User login
Viral Season 2024-2025: Try for An Ounce of Prevention
We are quickly approaching the typical cold and flu season. But can we call anything typical since 2020? Since 2020, there have been different recommendations for prevention, testing, return to work, and treatment since our world was rocked by the pandemic. Now that we are in the “post-pandemic” era, family physicians and other primary care professionals are the front line for discussions on prevention, evaluation, and treatment of the typical upper-respiratory infections, influenza, and COVID-19.
Let’s start with prevention. We have all heard the old adage, an ounce of prevention is worth a pound of cure. In primary care, we need to focus on prevention. Vaccination is often one of our best tools against the myriad of infections we are hoping to help patients prevent during cold and flu season. Most recently, we have fall vaccinations aimed to prevent COVID-19, influenza, and respiratory syncytial virus (RSV).
The number and timing of each of these vaccinations has different recommendations based on a variety of factors including age, pregnancy status, and whether or not the patient is immunocompromised. For the 2024-2025 season, the Centers for Disease Control and Prevention has recommended updated vaccines for both influenza and COVID-19.1 They have also updated the RSV vaccine recommendations to “People 75 or older, or between 60-74 with certain chronic health conditions or living in a nursing home should get one dose of the RSV vaccine to provide an extra layer of protection.”2
In addition to vaccines as prevention, there is also hygiene, staying home when sick and away from others who are sick, following guidelines for where and when to wear a face mask, and the general tools of eating well, and getting sufficient sleep and exercise to help maintain the healthiest immune system.
Despite the best of intentions, there will still be many who experience viral infections in this upcoming season. The CDC is currently recommending persons to stay away from others for at least 24 hours after their symptoms improve and they are fever-free without antipyretics. In addition to isolation while sick, general symptom management is something that we can recommend for all of these illnesses.
There is more to consider, though, as our patients face these illnesses. The first question is how to determine the diagnosis — and if that diagnosis is even necessary. Unfortunately, many of these viral illnesses can look the same. They can all cause fevers, chills, and other upper respiratory symptoms. They are all fairly contagious. All of these viruses can cause serious illness associated with additional complications. It is not truly possible to determine which virus someone has by symptoms alone, our patients can have multiple viruses at the same time and diagnosis of one does not preclude having another.3
Instead, we truly do need a test for diagnosis. In-office testing is available for RSV, influenza, and COVID-19. Additionally, despite not being as freely available as they were during the pandemic, patients are able to do home COVID tests and then call in with their results. At the time of writing this, at-home rapid influenza tests have also been approved by the FDA but are not yet readily available to the public. These tests are important for determining if the patient is eligible for treatment. Both influenza and COVID-19 have antiviral treatments available to help decrease the severity of the illness and potentially the length of illness and time contagious. According to the CDC, both treatments are underutilized.
This could be because of a lack of testing and diagnosis. It may also be because of a lack of familiarity with the available treatments.4,5Influenza treatment is recommended as soon as possible for those with suspected or confirmed diagnosis, immediately for anyone hospitalized, anyone with severe, complicated, or progressing illness, and for those at high risk of severe illness including but not limited to those under 2 years old, those over 65, those who are pregnant, and those with many chronic conditions.
Treatment can also be used for those who are not high risk when diagnosed within 48 hours. In the United States, four antivirals are recommended to treat influenza: oseltamivir phosphate, zanamivir, peramivir, and baloxavir marboxil. For COVID-19, treatments are also available for mild or moderate disease in those at risk for severe disease. Both remdesivir and nimatrelvir with ritonavir are treatment options that can be used for COVID-19 infection. Unfortunately, no specific antiviral is available for the other viral illnesses we see often during this season.
In primary care, we have some important roles to play. We need to continue to discuss all methods of prevention. Not only do vaccine recommendations change at least annually, our patients’ situations change and we have to reassess them. Additionally, people often need to hear things more than once before committing — so it never hurts to continue having those conversations. Combining the conversation about vaccines with other prevention measures is also important so that it does not seem like we are only recommending one thing. We should also start talking about treatment options before our patients are sick. We can communicate what is available as long as they let us know they are sick early. We can also be there to help our patients determine when they are at risk for severe illness and when they should consider a higher level of care.
The availability of home testing gives us the opportunity to provide these treatments via telehealth and even potentially in times when these illnesses are everywhere — with standing orders with our clinical teams. Although it is a busy time for us in the clinic, “cold and flu” season is definitely one of those times when our primary care relationship can truly help our patients.
References
1. CDC Recommends Updated 2024-2025 COVID-19 and Flu Vaccines for Fall/Winter Virus Season. https://www.cdc.gov/media/releases/2024/s-t0627-vaccine-recommendations.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
2. CDC Updates RSV Vaccination Recommendation for Adults. https://www.cdc.gov/media/releases/2024/s-0626-vaccination-adults.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
3. Similarities and Differences between Flu and COVID-19. https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases.
4. Respiratory Virus Guidance. https://www.cdc.gov/respiratory-viruses/guidance/index.html. Accessed August 9, 2024. Source: National Center for Immunization and Respiratory Diseases.
5. Provider Toolkit: Preparing Patients for the Fall and Winter Virus Season. https://www.cdc.gov/respiratory-viruses/hcp/tools-resources/index.html. Accessed August 9, 2024. Source: Centers for Disease Control and Prevention.
We are quickly approaching the typical cold and flu season. But can we call anything typical since 2020? Since 2020, there have been different recommendations for prevention, testing, return to work, and treatment since our world was rocked by the pandemic. Now that we are in the “post-pandemic” era, family physicians and other primary care professionals are the front line for discussions on prevention, evaluation, and treatment of the typical upper-respiratory infections, influenza, and COVID-19.
Let’s start with prevention. We have all heard the old adage, an ounce of prevention is worth a pound of cure. In primary care, we need to focus on prevention. Vaccination is often one of our best tools against the myriad of infections we are hoping to help patients prevent during cold and flu season. Most recently, we have fall vaccinations aimed to prevent COVID-19, influenza, and respiratory syncytial virus (RSV).
The number and timing of each of these vaccinations has different recommendations based on a variety of factors including age, pregnancy status, and whether or not the patient is immunocompromised. For the 2024-2025 season, the Centers for Disease Control and Prevention has recommended updated vaccines for both influenza and COVID-19.1 They have also updated the RSV vaccine recommendations to “People 75 or older, or between 60-74 with certain chronic health conditions or living in a nursing home should get one dose of the RSV vaccine to provide an extra layer of protection.”2
In addition to vaccines as prevention, there is also hygiene, staying home when sick and away from others who are sick, following guidelines for where and when to wear a face mask, and the general tools of eating well, and getting sufficient sleep and exercise to help maintain the healthiest immune system.
Despite the best of intentions, there will still be many who experience viral infections in this upcoming season. The CDC is currently recommending persons to stay away from others for at least 24 hours after their symptoms improve and they are fever-free without antipyretics. In addition to isolation while sick, general symptom management is something that we can recommend for all of these illnesses.
There is more to consider, though, as our patients face these illnesses. The first question is how to determine the diagnosis — and if that diagnosis is even necessary. Unfortunately, many of these viral illnesses can look the same. They can all cause fevers, chills, and other upper respiratory symptoms. They are all fairly contagious. All of these viruses can cause serious illness associated with additional complications. It is not truly possible to determine which virus someone has by symptoms alone, our patients can have multiple viruses at the same time and diagnosis of one does not preclude having another.3
Instead, we truly do need a test for diagnosis. In-office testing is available for RSV, influenza, and COVID-19. Additionally, despite not being as freely available as they were during the pandemic, patients are able to do home COVID tests and then call in with their results. At the time of writing this, at-home rapid influenza tests have also been approved by the FDA but are not yet readily available to the public. These tests are important for determining if the patient is eligible for treatment. Both influenza and COVID-19 have antiviral treatments available to help decrease the severity of the illness and potentially the length of illness and time contagious. According to the CDC, both treatments are underutilized.
This could be because of a lack of testing and diagnosis. It may also be because of a lack of familiarity with the available treatments.4,5Influenza treatment is recommended as soon as possible for those with suspected or confirmed diagnosis, immediately for anyone hospitalized, anyone with severe, complicated, or progressing illness, and for those at high risk of severe illness including but not limited to those under 2 years old, those over 65, those who are pregnant, and those with many chronic conditions.
Treatment can also be used for those who are not high risk when diagnosed within 48 hours. In the United States, four antivirals are recommended to treat influenza: oseltamivir phosphate, zanamivir, peramivir, and baloxavir marboxil. For COVID-19, treatments are also available for mild or moderate disease in those at risk for severe disease. Both remdesivir and nimatrelvir with ritonavir are treatment options that can be used for COVID-19 infection. Unfortunately, no specific antiviral is available for the other viral illnesses we see often during this season.
In primary care, we have some important roles to play. We need to continue to discuss all methods of prevention. Not only do vaccine recommendations change at least annually, our patients’ situations change and we have to reassess them. Additionally, people often need to hear things more than once before committing — so it never hurts to continue having those conversations. Combining the conversation about vaccines with other prevention measures is also important so that it does not seem like we are only recommending one thing. We should also start talking about treatment options before our patients are sick. We can communicate what is available as long as they let us know they are sick early. We can also be there to help our patients determine when they are at risk for severe illness and when they should consider a higher level of care.
The availability of home testing gives us the opportunity to provide these treatments via telehealth and even potentially in times when these illnesses are everywhere — with standing orders with our clinical teams. Although it is a busy time for us in the clinic, “cold and flu” season is definitely one of those times when our primary care relationship can truly help our patients.
References
1. CDC Recommends Updated 2024-2025 COVID-19 and Flu Vaccines for Fall/Winter Virus Season. https://www.cdc.gov/media/releases/2024/s-t0627-vaccine-recommendations.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
2. CDC Updates RSV Vaccination Recommendation for Adults. https://www.cdc.gov/media/releases/2024/s-0626-vaccination-adults.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
3. Similarities and Differences between Flu and COVID-19. https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases.
4. Respiratory Virus Guidance. https://www.cdc.gov/respiratory-viruses/guidance/index.html. Accessed August 9, 2024. Source: National Center for Immunization and Respiratory Diseases.
5. Provider Toolkit: Preparing Patients for the Fall and Winter Virus Season. https://www.cdc.gov/respiratory-viruses/hcp/tools-resources/index.html. Accessed August 9, 2024. Source: Centers for Disease Control and Prevention.
We are quickly approaching the typical cold and flu season. But can we call anything typical since 2020? Since 2020, there have been different recommendations for prevention, testing, return to work, and treatment since our world was rocked by the pandemic. Now that we are in the “post-pandemic” era, family physicians and other primary care professionals are the front line for discussions on prevention, evaluation, and treatment of the typical upper-respiratory infections, influenza, and COVID-19.
Let’s start with prevention. We have all heard the old adage, an ounce of prevention is worth a pound of cure. In primary care, we need to focus on prevention. Vaccination is often one of our best tools against the myriad of infections we are hoping to help patients prevent during cold and flu season. Most recently, we have fall vaccinations aimed to prevent COVID-19, influenza, and respiratory syncytial virus (RSV).
The number and timing of each of these vaccinations has different recommendations based on a variety of factors including age, pregnancy status, and whether or not the patient is immunocompromised. For the 2024-2025 season, the Centers for Disease Control and Prevention has recommended updated vaccines for both influenza and COVID-19.1 They have also updated the RSV vaccine recommendations to “People 75 or older, or between 60-74 with certain chronic health conditions or living in a nursing home should get one dose of the RSV vaccine to provide an extra layer of protection.”2
In addition to vaccines as prevention, there is also hygiene, staying home when sick and away from others who are sick, following guidelines for where and when to wear a face mask, and the general tools of eating well, and getting sufficient sleep and exercise to help maintain the healthiest immune system.
Despite the best of intentions, there will still be many who experience viral infections in this upcoming season. The CDC is currently recommending persons to stay away from others for at least 24 hours after their symptoms improve and they are fever-free without antipyretics. In addition to isolation while sick, general symptom management is something that we can recommend for all of these illnesses.
There is more to consider, though, as our patients face these illnesses. The first question is how to determine the diagnosis — and if that diagnosis is even necessary. Unfortunately, many of these viral illnesses can look the same. They can all cause fevers, chills, and other upper respiratory symptoms. They are all fairly contagious. All of these viruses can cause serious illness associated with additional complications. It is not truly possible to determine which virus someone has by symptoms alone, our patients can have multiple viruses at the same time and diagnosis of one does not preclude having another.3
Instead, we truly do need a test for diagnosis. In-office testing is available for RSV, influenza, and COVID-19. Additionally, despite not being as freely available as they were during the pandemic, patients are able to do home COVID tests and then call in with their results. At the time of writing this, at-home rapid influenza tests have also been approved by the FDA but are not yet readily available to the public. These tests are important for determining if the patient is eligible for treatment. Both influenza and COVID-19 have antiviral treatments available to help decrease the severity of the illness and potentially the length of illness and time contagious. According to the CDC, both treatments are underutilized.
This could be because of a lack of testing and diagnosis. It may also be because of a lack of familiarity with the available treatments.4,5Influenza treatment is recommended as soon as possible for those with suspected or confirmed diagnosis, immediately for anyone hospitalized, anyone with severe, complicated, or progressing illness, and for those at high risk of severe illness including but not limited to those under 2 years old, those over 65, those who are pregnant, and those with many chronic conditions.
Treatment can also be used for those who are not high risk when diagnosed within 48 hours. In the United States, four antivirals are recommended to treat influenza: oseltamivir phosphate, zanamivir, peramivir, and baloxavir marboxil. For COVID-19, treatments are also available for mild or moderate disease in those at risk for severe disease. Both remdesivir and nimatrelvir with ritonavir are treatment options that can be used for COVID-19 infection. Unfortunately, no specific antiviral is available for the other viral illnesses we see often during this season.
In primary care, we have some important roles to play. We need to continue to discuss all methods of prevention. Not only do vaccine recommendations change at least annually, our patients’ situations change and we have to reassess them. Additionally, people often need to hear things more than once before committing — so it never hurts to continue having those conversations. Combining the conversation about vaccines with other prevention measures is also important so that it does not seem like we are only recommending one thing. We should also start talking about treatment options before our patients are sick. We can communicate what is available as long as they let us know they are sick early. We can also be there to help our patients determine when they are at risk for severe illness and when they should consider a higher level of care.
The availability of home testing gives us the opportunity to provide these treatments via telehealth and even potentially in times when these illnesses are everywhere — with standing orders with our clinical teams. Although it is a busy time for us in the clinic, “cold and flu” season is definitely one of those times when our primary care relationship can truly help our patients.
References
1. CDC Recommends Updated 2024-2025 COVID-19 and Flu Vaccines for Fall/Winter Virus Season. https://www.cdc.gov/media/releases/2024/s-t0627-vaccine-recommendations.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
2. CDC Updates RSV Vaccination Recommendation for Adults. https://www.cdc.gov/media/releases/2024/s-0626-vaccination-adults.html. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention.
3. Similarities and Differences between Flu and COVID-19. https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm. Accessed August 8, 2024. Source: Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases.
4. Respiratory Virus Guidance. https://www.cdc.gov/respiratory-viruses/guidance/index.html. Accessed August 9, 2024. Source: National Center for Immunization and Respiratory Diseases.
5. Provider Toolkit: Preparing Patients for the Fall and Winter Virus Season. https://www.cdc.gov/respiratory-viruses/hcp/tools-resources/index.html. Accessed August 9, 2024. Source: Centers for Disease Control and Prevention.
Study Identifies Oral Antibiotics Linked to Severe Cutaneous Reactions
according to a large, population-based, nested case-control study of older adults, spanning two decades.
The findings, published online in JAMA, “underscore the importance of judicious prescribing, with preferential use of antibiotics associated with a lower risk when clinically appropriate,” noted senior author David Juurlink, MD, PhD, professor of medicine; pediatrics; and health policy, management and evaluation at the University of Toronto, and head of the Clinical Pharmacology and Toxicology Division at Sunnybrook Health Sciences Centre, also in Toronto, Ontario, Canada, and coauthors.
“We hope our study raises awareness about the importance of drug allergy and gains support for future studies to improve drug allergy care,” lead author Erika Lee, MD, clinical immunology and allergy lecturer at the University of Toronto’s Drug Allergy Clinic, Sunnybrook Health Sciences Centre, said in an interview. “It is important to recognize symptoms and signs of a severe drug rash and promptly stop culprit drugs to prevent worsening reaction.”
Serious cADRs are “a group of rare but potentially life-threatening drug hypersensitivity reactions involving the skin and, frequently, internal organs,” the authors wrote. “Typically delayed in onset, these reactions include drug reaction with eosinophilia and systemic symptoms, Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN) — the most severe cADR, which has a reported mortality of 20%-40%,” they noted.
Speculation Without Data
Although it has been speculated that some oral antibiotics are more likely than others to be associated with serious cADRs, there have been no population-based studies examining this, they added.
The study included adults aged 66 years or older and used administrative health databases in Ontario, spanning from April 1, 2002, to March 31, 2022. Data on antibiotic use were taken from the Ontario Drug Benefit database. The Canadian Institute for Health Information (CIHI) National Ambulatory Care Reporting System was used to obtain data on emergency department (ED) visits for cADRs, while the CIHI Discharge Abstract Database was used to identify hospitalizations for cADRs. Finally, demographic information and outpatient healthcare utilization data were obtained from the Registered Persons Database and the Ontario Health Insurance Plan database, respectively.
A cohort of 21,758 older adults (median age, 75 years; 64.1% women) who had an ED visit or hospitalization for serious cADRs within 60 days of receiving antibiotic therapy was matched by age and sex with 87,025 antibiotic-treated controls who did not have a cutaneous reaction.
The median duration of antibiotic prescription was 7 days among cases and controls, and among the cases, the median latency period between antibiotic prescriptions and hospital visits for cADRs was 14 days. Most of the case patients went to the ED only (86.9%), and the rest were hospitalized.
The most commonly prescribed antibiotic class was penicillins (28.9%), followed by cephalosporins (18.2%), fluoroquinolones (16.5%), macrolides (14.8%), nitrofurantoin (8.6%), and sulfonamides (6.2%). Less commonly used antibiotics (“other” antibiotics) accounted for 6.9%.
Macrolide antibiotics were used as the reference because they are rarely associated with serious cADRs, noted the authors, and the multivariable analysis, adjusted for risk factors associated with serious cADRs, including malignancy, chronic liver disease, chronic kidney disease, and HIV.
After multivariable adjustment, relative to macrolides, sulfonamides were most strongly associated with serious cADRs (adjusted odds ratio [aOR], 2.9) but so were all other antibiotic classes, including cephalosporins (aOR, 2.6), “other” antibiotics (aOR, 2.3), nitrofurantoin (aOR, 2.2), penicillins (aOR, 1.4), and fluoroquinolones (aOR,1.3).
In the secondary analysis, the crude rate of ED visits or hospitalizations for cADRs was highest for cephalosporins (4.92 per 1000 prescriptions), followed by sulfonamides (3.22 per 1000 prescriptions). Among hospitalized patients, the median length of stay was 6 days, with 9.6% requiring transfer to a critical care unit and 5.3% dying in the hospital.
Hospitalizations, ED Visits Not Studied Previously
“Notably, the rate of antibiotic-associated serious cADRs leading to an ED visit or hospitalization has not been previously studied,” noted the authors. “We found that at least two hospital encounters for serious cADRs ensued for every 1000 antibiotic prescriptions. This rate is considerably higher than suggested by studies that examine only SJS/TEN and drug reaction with eosinophilia and systemic symptoms.”
Dr. Lee also emphasized the previously unreported findings about nitrofurantoin. “It is surprising to find that nitrofurantoin, a commonly prescribed antibiotic for urinary tract infection, is also associated with an increased risk of severe drug rash,” she said in an interview.
“This finding highlights a potential novel risk at a population-based level and should be further explored in other populations to verify this association,” the authors wrote.
Amesh Adalja, MD, a senior scholar at the Johns Hopkins Center for Health Security in Baltimore, Maryland, and a spokesperson for the Infectious Diseases Society of America, who was not involved in the study, agreed that the nitrofurantoin finding was surprising, but he was not surprised that sulfonamides were high on the list.
“The study reinforces that antibiotics are not benign medications to be dispensed injudiciously,” he said in an interview. “Antibiotics have risks, including serious skin reactions, as well as the fostering of antibiotic resistance. Clinicians should always first ask themselves if their patient actually merits an antibiotic and then assess what is the safest antibiotic for the purpose, bearing in mind that certain antibiotics are more likely to result in adverse reactions than others.”
The study was supported by the Canadian Institutes of Health Research. The study was conducted at ICES, which is funded in part by an annual grant from the Ontario Ministry of Health and Long-Term Care. One coauthor reported receiving compensation from the British Journal of Dermatology as reviewer and section editor, the American Academy of Dermatology as guidelines writer, Canadian Dermatology Today as manuscript writer, and the National Eczema Association and the Canadian Agency for Drugs and Technologies in Health as consultant; as well as receiving research grants to the coauthor’s institution from the National Eczema Association, Eczema Society of Canada, Canadian Dermatology Foundation, Canadian Institutes of Health Research, US National Institutes of Health, and PSI Foundation. Another coauthor reported receiving grants from AbbVie, Bausch Health, Celgene, Lilly, Incyte, Janssen, LEO Pharma, L’Oréal, Novartis, Organon, Pfizer, Sandoz, Amgen, and Boehringer Ingelheim; receiving payment or honoraria for speaking from Sanofi China; participating on advisory boards for LEO Pharma, Novartis, Sanofi, and Union Therapeutics; and receiving equipment donation from L’Oréal. Dr. Adalja reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
according to a large, population-based, nested case-control study of older adults, spanning two decades.
The findings, published online in JAMA, “underscore the importance of judicious prescribing, with preferential use of antibiotics associated with a lower risk when clinically appropriate,” noted senior author David Juurlink, MD, PhD, professor of medicine; pediatrics; and health policy, management and evaluation at the University of Toronto, and head of the Clinical Pharmacology and Toxicology Division at Sunnybrook Health Sciences Centre, also in Toronto, Ontario, Canada, and coauthors.
“We hope our study raises awareness about the importance of drug allergy and gains support for future studies to improve drug allergy care,” lead author Erika Lee, MD, clinical immunology and allergy lecturer at the University of Toronto’s Drug Allergy Clinic, Sunnybrook Health Sciences Centre, said in an interview. “It is important to recognize symptoms and signs of a severe drug rash and promptly stop culprit drugs to prevent worsening reaction.”
Serious cADRs are “a group of rare but potentially life-threatening drug hypersensitivity reactions involving the skin and, frequently, internal organs,” the authors wrote. “Typically delayed in onset, these reactions include drug reaction with eosinophilia and systemic symptoms, Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN) — the most severe cADR, which has a reported mortality of 20%-40%,” they noted.
Speculation Without Data
Although it has been speculated that some oral antibiotics are more likely than others to be associated with serious cADRs, there have been no population-based studies examining this, they added.
The study included adults aged 66 years or older and used administrative health databases in Ontario, spanning from April 1, 2002, to March 31, 2022. Data on antibiotic use were taken from the Ontario Drug Benefit database. The Canadian Institute for Health Information (CIHI) National Ambulatory Care Reporting System was used to obtain data on emergency department (ED) visits for cADRs, while the CIHI Discharge Abstract Database was used to identify hospitalizations for cADRs. Finally, demographic information and outpatient healthcare utilization data were obtained from the Registered Persons Database and the Ontario Health Insurance Plan database, respectively.
A cohort of 21,758 older adults (median age, 75 years; 64.1% women) who had an ED visit or hospitalization for serious cADRs within 60 days of receiving antibiotic therapy was matched by age and sex with 87,025 antibiotic-treated controls who did not have a cutaneous reaction.
The median duration of antibiotic prescription was 7 days among cases and controls, and among the cases, the median latency period between antibiotic prescriptions and hospital visits for cADRs was 14 days. Most of the case patients went to the ED only (86.9%), and the rest were hospitalized.
The most commonly prescribed antibiotic class was penicillins (28.9%), followed by cephalosporins (18.2%), fluoroquinolones (16.5%), macrolides (14.8%), nitrofurantoin (8.6%), and sulfonamides (6.2%). Less commonly used antibiotics (“other” antibiotics) accounted for 6.9%.
Macrolide antibiotics were used as the reference because they are rarely associated with serious cADRs, noted the authors, and the multivariable analysis, adjusted for risk factors associated with serious cADRs, including malignancy, chronic liver disease, chronic kidney disease, and HIV.
After multivariable adjustment, relative to macrolides, sulfonamides were most strongly associated with serious cADRs (adjusted odds ratio [aOR], 2.9) but so were all other antibiotic classes, including cephalosporins (aOR, 2.6), “other” antibiotics (aOR, 2.3), nitrofurantoin (aOR, 2.2), penicillins (aOR, 1.4), and fluoroquinolones (aOR,1.3).
In the secondary analysis, the crude rate of ED visits or hospitalizations for cADRs was highest for cephalosporins (4.92 per 1000 prescriptions), followed by sulfonamides (3.22 per 1000 prescriptions). Among hospitalized patients, the median length of stay was 6 days, with 9.6% requiring transfer to a critical care unit and 5.3% dying in the hospital.
Hospitalizations, ED Visits Not Studied Previously
“Notably, the rate of antibiotic-associated serious cADRs leading to an ED visit or hospitalization has not been previously studied,” noted the authors. “We found that at least two hospital encounters for serious cADRs ensued for every 1000 antibiotic prescriptions. This rate is considerably higher than suggested by studies that examine only SJS/TEN and drug reaction with eosinophilia and systemic symptoms.”
Dr. Lee also emphasized the previously unreported findings about nitrofurantoin. “It is surprising to find that nitrofurantoin, a commonly prescribed antibiotic for urinary tract infection, is also associated with an increased risk of severe drug rash,” she said in an interview.
“This finding highlights a potential novel risk at a population-based level and should be further explored in other populations to verify this association,” the authors wrote.
Amesh Adalja, MD, a senior scholar at the Johns Hopkins Center for Health Security in Baltimore, Maryland, and a spokesperson for the Infectious Diseases Society of America, who was not involved in the study, agreed that the nitrofurantoin finding was surprising, but he was not surprised that sulfonamides were high on the list.
“The study reinforces that antibiotics are not benign medications to be dispensed injudiciously,” he said in an interview. “Antibiotics have risks, including serious skin reactions, as well as the fostering of antibiotic resistance. Clinicians should always first ask themselves if their patient actually merits an antibiotic and then assess what is the safest antibiotic for the purpose, bearing in mind that certain antibiotics are more likely to result in adverse reactions than others.”
The study was supported by the Canadian Institutes of Health Research. The study was conducted at ICES, which is funded in part by an annual grant from the Ontario Ministry of Health and Long-Term Care. One coauthor reported receiving compensation from the British Journal of Dermatology as reviewer and section editor, the American Academy of Dermatology as guidelines writer, Canadian Dermatology Today as manuscript writer, and the National Eczema Association and the Canadian Agency for Drugs and Technologies in Health as consultant; as well as receiving research grants to the coauthor’s institution from the National Eczema Association, Eczema Society of Canada, Canadian Dermatology Foundation, Canadian Institutes of Health Research, US National Institutes of Health, and PSI Foundation. Another coauthor reported receiving grants from AbbVie, Bausch Health, Celgene, Lilly, Incyte, Janssen, LEO Pharma, L’Oréal, Novartis, Organon, Pfizer, Sandoz, Amgen, and Boehringer Ingelheim; receiving payment or honoraria for speaking from Sanofi China; participating on advisory boards for LEO Pharma, Novartis, Sanofi, and Union Therapeutics; and receiving equipment donation from L’Oréal. Dr. Adalja reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
according to a large, population-based, nested case-control study of older adults, spanning two decades.
The findings, published online in JAMA, “underscore the importance of judicious prescribing, with preferential use of antibiotics associated with a lower risk when clinically appropriate,” noted senior author David Juurlink, MD, PhD, professor of medicine; pediatrics; and health policy, management and evaluation at the University of Toronto, and head of the Clinical Pharmacology and Toxicology Division at Sunnybrook Health Sciences Centre, also in Toronto, Ontario, Canada, and coauthors.
“We hope our study raises awareness about the importance of drug allergy and gains support for future studies to improve drug allergy care,” lead author Erika Lee, MD, clinical immunology and allergy lecturer at the University of Toronto’s Drug Allergy Clinic, Sunnybrook Health Sciences Centre, said in an interview. “It is important to recognize symptoms and signs of a severe drug rash and promptly stop culprit drugs to prevent worsening reaction.”
Serious cADRs are “a group of rare but potentially life-threatening drug hypersensitivity reactions involving the skin and, frequently, internal organs,” the authors wrote. “Typically delayed in onset, these reactions include drug reaction with eosinophilia and systemic symptoms, Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN) — the most severe cADR, which has a reported mortality of 20%-40%,” they noted.
Speculation Without Data
Although it has been speculated that some oral antibiotics are more likely than others to be associated with serious cADRs, there have been no population-based studies examining this, they added.
The study included adults aged 66 years or older and used administrative health databases in Ontario, spanning from April 1, 2002, to March 31, 2022. Data on antibiotic use were taken from the Ontario Drug Benefit database. The Canadian Institute for Health Information (CIHI) National Ambulatory Care Reporting System was used to obtain data on emergency department (ED) visits for cADRs, while the CIHI Discharge Abstract Database was used to identify hospitalizations for cADRs. Finally, demographic information and outpatient healthcare utilization data were obtained from the Registered Persons Database and the Ontario Health Insurance Plan database, respectively.
A cohort of 21,758 older adults (median age, 75 years; 64.1% women) who had an ED visit or hospitalization for serious cADRs within 60 days of receiving antibiotic therapy was matched by age and sex with 87,025 antibiotic-treated controls who did not have a cutaneous reaction.
The median duration of antibiotic prescription was 7 days among cases and controls, and among the cases, the median latency period between antibiotic prescriptions and hospital visits for cADRs was 14 days. Most of the case patients went to the ED only (86.9%), and the rest were hospitalized.
The most commonly prescribed antibiotic class was penicillins (28.9%), followed by cephalosporins (18.2%), fluoroquinolones (16.5%), macrolides (14.8%), nitrofurantoin (8.6%), and sulfonamides (6.2%). Less commonly used antibiotics (“other” antibiotics) accounted for 6.9%.
Macrolide antibiotics were used as the reference because they are rarely associated with serious cADRs, noted the authors, and the multivariable analysis, adjusted for risk factors associated with serious cADRs, including malignancy, chronic liver disease, chronic kidney disease, and HIV.
After multivariable adjustment, relative to macrolides, sulfonamides were most strongly associated with serious cADRs (adjusted odds ratio [aOR], 2.9) but so were all other antibiotic classes, including cephalosporins (aOR, 2.6), “other” antibiotics (aOR, 2.3), nitrofurantoin (aOR, 2.2), penicillins (aOR, 1.4), and fluoroquinolones (aOR,1.3).
In the secondary analysis, the crude rate of ED visits or hospitalizations for cADRs was highest for cephalosporins (4.92 per 1000 prescriptions), followed by sulfonamides (3.22 per 1000 prescriptions). Among hospitalized patients, the median length of stay was 6 days, with 9.6% requiring transfer to a critical care unit and 5.3% dying in the hospital.
Hospitalizations, ED Visits Not Studied Previously
“Notably, the rate of antibiotic-associated serious cADRs leading to an ED visit or hospitalization has not been previously studied,” noted the authors. “We found that at least two hospital encounters for serious cADRs ensued for every 1000 antibiotic prescriptions. This rate is considerably higher than suggested by studies that examine only SJS/TEN and drug reaction with eosinophilia and systemic symptoms.”
Dr. Lee also emphasized the previously unreported findings about nitrofurantoin. “It is surprising to find that nitrofurantoin, a commonly prescribed antibiotic for urinary tract infection, is also associated with an increased risk of severe drug rash,” she said in an interview.
“This finding highlights a potential novel risk at a population-based level and should be further explored in other populations to verify this association,” the authors wrote.
Amesh Adalja, MD, a senior scholar at the Johns Hopkins Center for Health Security in Baltimore, Maryland, and a spokesperson for the Infectious Diseases Society of America, who was not involved in the study, agreed that the nitrofurantoin finding was surprising, but he was not surprised that sulfonamides were high on the list.
“The study reinforces that antibiotics are not benign medications to be dispensed injudiciously,” he said in an interview. “Antibiotics have risks, including serious skin reactions, as well as the fostering of antibiotic resistance. Clinicians should always first ask themselves if their patient actually merits an antibiotic and then assess what is the safest antibiotic for the purpose, bearing in mind that certain antibiotics are more likely to result in adverse reactions than others.”
The study was supported by the Canadian Institutes of Health Research. The study was conducted at ICES, which is funded in part by an annual grant from the Ontario Ministry of Health and Long-Term Care. One coauthor reported receiving compensation from the British Journal of Dermatology as reviewer and section editor, the American Academy of Dermatology as guidelines writer, Canadian Dermatology Today as manuscript writer, and the National Eczema Association and the Canadian Agency for Drugs and Technologies in Health as consultant; as well as receiving research grants to the coauthor’s institution from the National Eczema Association, Eczema Society of Canada, Canadian Dermatology Foundation, Canadian Institutes of Health Research, US National Institutes of Health, and PSI Foundation. Another coauthor reported receiving grants from AbbVie, Bausch Health, Celgene, Lilly, Incyte, Janssen, LEO Pharma, L’Oréal, Novartis, Organon, Pfizer, Sandoz, Amgen, and Boehringer Ingelheim; receiving payment or honoraria for speaking from Sanofi China; participating on advisory boards for LEO Pharma, Novartis, Sanofi, and Union Therapeutics; and receiving equipment donation from L’Oréal. Dr. Adalja reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM JAMA
Comment on “Erythrodermic Pityriasis Rubra Pilaris Following COVID-19 Vaccination”
To the Editor:
We read with interest the case report from Abdelkader et al1 (Cutis. 2024;113:E22-E24) of a 32-year-old man who received the Sinopharm BBIBP COVID-19 vaccine (BBIBP-CorV) and experienced acute-onset erythroderma and severe itching. The patient did not disclose any recent medication intake and had no noteworthy medical history. Physical examination revealed palmoplantar keratoderma, keratotic follicular papules on the legs and feet, and typical orange-red erythroderma. The laboratory workup was normal, including a negative test result for HIV infection.
The absence of details regarding the patient’s history of allergic reactions or sensitivities is one possible shortcoming in this case report and may have given important information about the possible reason for the erythroderma that occurred following vaccination. Furthermore, more research into the precise Sinopharm BBIBP vaccine ingredients that may have caused the skin reaction would have been helpful in deciphering the underlying mechanisms.
Larger-scale studies examining the frequency of cutaneous reactions following COVID-19 vaccination with various vaccine formulations may be the focus of future research efforts and could assist in determining the risk factors for experiencing such reactions, which would enable health care providers to offer advice on vaccination alternatives or preventative measures for those who are more vulnerable. Furthermore, collaboration among dermatologists and allergists could improve patient outcomes and improve management.
By highlighting an uncommon but noteworthy dermatologic manifestation following COVID-19 immunization, this case report emphasizes how crucial it is to keep an eye out for and report any possible side effects linked to vaccinations to protect patient safety. Subsequent investigations should concentrate on enhancing comprehension of the pathophysiology of cutaneous reactions following immunization and devising tactics to alleviate these hazards. Working together, researchers and health care professionals can effectively tackle the issues raised by these newly discovered vaccine-related skin responses.
1. Abdelkader HA, Khedr H, El-Komy MH. Erythrodermic pityriasis rubra pilaris following COVID-19 vaccination. Cutis. 2024;113:E22-E24. doi:10.12788/cutis.1010
To the Editor:
We read with interest the case report from Abdelkader et al1 (Cutis. 2024;113:E22-E24) of a 32-year-old man who received the Sinopharm BBIBP COVID-19 vaccine (BBIBP-CorV) and experienced acute-onset erythroderma and severe itching. The patient did not disclose any recent medication intake and had no noteworthy medical history. Physical examination revealed palmoplantar keratoderma, keratotic follicular papules on the legs and feet, and typical orange-red erythroderma. The laboratory workup was normal, including a negative test result for HIV infection.
The absence of details regarding the patient’s history of allergic reactions or sensitivities is one possible shortcoming in this case report and may have given important information about the possible reason for the erythroderma that occurred following vaccination. Furthermore, more research into the precise Sinopharm BBIBP vaccine ingredients that may have caused the skin reaction would have been helpful in deciphering the underlying mechanisms.
Larger-scale studies examining the frequency of cutaneous reactions following COVID-19 vaccination with various vaccine formulations may be the focus of future research efforts and could assist in determining the risk factors for experiencing such reactions, which would enable health care providers to offer advice on vaccination alternatives or preventative measures for those who are more vulnerable. Furthermore, collaboration among dermatologists and allergists could improve patient outcomes and improve management.
By highlighting an uncommon but noteworthy dermatologic manifestation following COVID-19 immunization, this case report emphasizes how crucial it is to keep an eye out for and report any possible side effects linked to vaccinations to protect patient safety. Subsequent investigations should concentrate on enhancing comprehension of the pathophysiology of cutaneous reactions following immunization and devising tactics to alleviate these hazards. Working together, researchers and health care professionals can effectively tackle the issues raised by these newly discovered vaccine-related skin responses.
To the Editor:
We read with interest the case report from Abdelkader et al1 (Cutis. 2024;113:E22-E24) of a 32-year-old man who received the Sinopharm BBIBP COVID-19 vaccine (BBIBP-CorV) and experienced acute-onset erythroderma and severe itching. The patient did not disclose any recent medication intake and had no noteworthy medical history. Physical examination revealed palmoplantar keratoderma, keratotic follicular papules on the legs and feet, and typical orange-red erythroderma. The laboratory workup was normal, including a negative test result for HIV infection.
The absence of details regarding the patient’s history of allergic reactions or sensitivities is one possible shortcoming in this case report and may have given important information about the possible reason for the erythroderma that occurred following vaccination. Furthermore, more research into the precise Sinopharm BBIBP vaccine ingredients that may have caused the skin reaction would have been helpful in deciphering the underlying mechanisms.
Larger-scale studies examining the frequency of cutaneous reactions following COVID-19 vaccination with various vaccine formulations may be the focus of future research efforts and could assist in determining the risk factors for experiencing such reactions, which would enable health care providers to offer advice on vaccination alternatives or preventative measures for those who are more vulnerable. Furthermore, collaboration among dermatologists and allergists could improve patient outcomes and improve management.
By highlighting an uncommon but noteworthy dermatologic manifestation following COVID-19 immunization, this case report emphasizes how crucial it is to keep an eye out for and report any possible side effects linked to vaccinations to protect patient safety. Subsequent investigations should concentrate on enhancing comprehension of the pathophysiology of cutaneous reactions following immunization and devising tactics to alleviate these hazards. Working together, researchers and health care professionals can effectively tackle the issues raised by these newly discovered vaccine-related skin responses.
1. Abdelkader HA, Khedr H, El-Komy MH. Erythrodermic pityriasis rubra pilaris following COVID-19 vaccination. Cutis. 2024;113:E22-E24. doi:10.12788/cutis.1010
1. Abdelkader HA, Khedr H, El-Komy MH. Erythrodermic pityriasis rubra pilaris following COVID-19 vaccination. Cutis. 2024;113:E22-E24. doi:10.12788/cutis.1010
How Safe is Anti–IL-6 Therapy During Pregnancy?
TOPLINE:
The maternal and neonatal outcomes in pregnant women treated with anti–interleukin (IL)-6 therapy for COVID-19 are largely favorable, with transient neonatal cytopenia observed in around one third of the babies being the only possible adverse outcome that could be related to anti–IL-6 therapy.
METHODOLOGY:
- Despite guidance, very few pregnant women with COVID-19 are offered evidence-based therapies such as anti–IL-6 due to concerns regarding fetal safety in later pregnancy.
- In this retrospective study, researchers evaluated maternal and neonatal outcomes in 25 pregnant women with COVID-19 (mean age at admission, 33 years) treated with anti–IL-6 (tocilizumab or sarilumab) at two tertiary hospitals in London.
- Most women (n = 16) received anti–IL-6 in the third trimester of pregnancy, whereas nine received it during the second trimester.
- Maternal and neonatal outcomes were assessed through medical record reviews and maternal medicine networks, with follow-up for 12 months.
- The women included in the study constituted a high-risk population with severe COVID-19; 24 required level two or three critical care. All women were receiving at least three concomitant medications due to their critical illness.
TAKEAWAY:
- Overall, 24 of 25 women treated with IL-6 receptor antibodies survived until hospital discharge.
- The sole death occurred in a woman with severe COVID-19 pneumonitis who later developed myocarditis and cardiac arrest. The physicians believed that these complications were more likely due to severe COVID-19 rather than anti–IL-6 therapy.
- All pregnancies resulted in live births; however, 16 babies had to be delivered preterm due to COVID-19 complications.
- Transient cytopenia was observed in 6 of 19 babies in whom a full blood count was performed. All the six babies were premature, with cytopenia resolving within 7 days in four babies; one baby died from complications associated with extreme prematurity.
IN PRACTICE:
“Although the authors found mild, transitory cytopenia in some (6 of 19) exposed infants, most had been delivered prematurely due to progressive COVID-19–related morbidity, and distinguishing drug effects from similar prematurity-related effects is difficult,” wrote Steven L. Clark, MD, from the Department of Obstetrics and Gynecology, Baylor College of Medicine, Houston, in an accompanying editorial.
SOURCE:
The study was led by Melanie Nana, MRCP, from the Department of Obstetric Medicine, St Thomas’ Hospital, London, England. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study was retrospective in design, which may have introduced bias. The small sample size of 25 women may have limited the generalizability of the findings. Additionally, the study did not include a control group, which made it difficult to attribute outcomes solely to anti–IL-6 therapy. The lack of long-term follow-up data on the neonates also limited the understanding of potential long-term effects.
DISCLOSURES:
This study did not receive any funding. Some authors, including the lead author, received speaker fees, grants, or consultancy fees from academic institutions or pharmaceutical companies or had other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The maternal and neonatal outcomes in pregnant women treated with anti–interleukin (IL)-6 therapy for COVID-19 are largely favorable, with transient neonatal cytopenia observed in around one third of the babies being the only possible adverse outcome that could be related to anti–IL-6 therapy.
METHODOLOGY:
- Despite guidance, very few pregnant women with COVID-19 are offered evidence-based therapies such as anti–IL-6 due to concerns regarding fetal safety in later pregnancy.
- In this retrospective study, researchers evaluated maternal and neonatal outcomes in 25 pregnant women with COVID-19 (mean age at admission, 33 years) treated with anti–IL-6 (tocilizumab or sarilumab) at two tertiary hospitals in London.
- Most women (n = 16) received anti–IL-6 in the third trimester of pregnancy, whereas nine received it during the second trimester.
- Maternal and neonatal outcomes were assessed through medical record reviews and maternal medicine networks, with follow-up for 12 months.
- The women included in the study constituted a high-risk population with severe COVID-19; 24 required level two or three critical care. All women were receiving at least three concomitant medications due to their critical illness.
TAKEAWAY:
- Overall, 24 of 25 women treated with IL-6 receptor antibodies survived until hospital discharge.
- The sole death occurred in a woman with severe COVID-19 pneumonitis who later developed myocarditis and cardiac arrest. The physicians believed that these complications were more likely due to severe COVID-19 rather than anti–IL-6 therapy.
- All pregnancies resulted in live births; however, 16 babies had to be delivered preterm due to COVID-19 complications.
- Transient cytopenia was observed in 6 of 19 babies in whom a full blood count was performed. All the six babies were premature, with cytopenia resolving within 7 days in four babies; one baby died from complications associated with extreme prematurity.
IN PRACTICE:
“Although the authors found mild, transitory cytopenia in some (6 of 19) exposed infants, most had been delivered prematurely due to progressive COVID-19–related morbidity, and distinguishing drug effects from similar prematurity-related effects is difficult,” wrote Steven L. Clark, MD, from the Department of Obstetrics and Gynecology, Baylor College of Medicine, Houston, in an accompanying editorial.
SOURCE:
The study was led by Melanie Nana, MRCP, from the Department of Obstetric Medicine, St Thomas’ Hospital, London, England. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study was retrospective in design, which may have introduced bias. The small sample size of 25 women may have limited the generalizability of the findings. Additionally, the study did not include a control group, which made it difficult to attribute outcomes solely to anti–IL-6 therapy. The lack of long-term follow-up data on the neonates also limited the understanding of potential long-term effects.
DISCLOSURES:
This study did not receive any funding. Some authors, including the lead author, received speaker fees, grants, or consultancy fees from academic institutions or pharmaceutical companies or had other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
The maternal and neonatal outcomes in pregnant women treated with anti–interleukin (IL)-6 therapy for COVID-19 are largely favorable, with transient neonatal cytopenia observed in around one third of the babies being the only possible adverse outcome that could be related to anti–IL-6 therapy.
METHODOLOGY:
- Despite guidance, very few pregnant women with COVID-19 are offered evidence-based therapies such as anti–IL-6 due to concerns regarding fetal safety in later pregnancy.
- In this retrospective study, researchers evaluated maternal and neonatal outcomes in 25 pregnant women with COVID-19 (mean age at admission, 33 years) treated with anti–IL-6 (tocilizumab or sarilumab) at two tertiary hospitals in London.
- Most women (n = 16) received anti–IL-6 in the third trimester of pregnancy, whereas nine received it during the second trimester.
- Maternal and neonatal outcomes were assessed through medical record reviews and maternal medicine networks, with follow-up for 12 months.
- The women included in the study constituted a high-risk population with severe COVID-19; 24 required level two or three critical care. All women were receiving at least three concomitant medications due to their critical illness.
TAKEAWAY:
- Overall, 24 of 25 women treated with IL-6 receptor antibodies survived until hospital discharge.
- The sole death occurred in a woman with severe COVID-19 pneumonitis who later developed myocarditis and cardiac arrest. The physicians believed that these complications were more likely due to severe COVID-19 rather than anti–IL-6 therapy.
- All pregnancies resulted in live births; however, 16 babies had to be delivered preterm due to COVID-19 complications.
- Transient cytopenia was observed in 6 of 19 babies in whom a full blood count was performed. All the six babies were premature, with cytopenia resolving within 7 days in four babies; one baby died from complications associated with extreme prematurity.
IN PRACTICE:
“Although the authors found mild, transitory cytopenia in some (6 of 19) exposed infants, most had been delivered prematurely due to progressive COVID-19–related morbidity, and distinguishing drug effects from similar prematurity-related effects is difficult,” wrote Steven L. Clark, MD, from the Department of Obstetrics and Gynecology, Baylor College of Medicine, Houston, in an accompanying editorial.
SOURCE:
The study was led by Melanie Nana, MRCP, from the Department of Obstetric Medicine, St Thomas’ Hospital, London, England. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study was retrospective in design, which may have introduced bias. The small sample size of 25 women may have limited the generalizability of the findings. Additionally, the study did not include a control group, which made it difficult to attribute outcomes solely to anti–IL-6 therapy. The lack of long-term follow-up data on the neonates also limited the understanding of potential long-term effects.
DISCLOSURES:
This study did not receive any funding. Some authors, including the lead author, received speaker fees, grants, or consultancy fees from academic institutions or pharmaceutical companies or had other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Saxophone Penis: A Forgotten Manifestation of Hidradenitis Suppurativa
To the Editor:
Hidradenitis suppurativa (HS) is a multifactorial chronic inflammatory skin disease affecting 1% to 4% of Europeans. It is characterized by recurrent inflamed nodules, abscesses, and sinus tracts in intertriginous regions.1 The genital area is affected in 11% of cases2 and usually is connected to severe forms of HS in both men and women.3 The prevalence of HS-associated genital lymphedema remains unknown.
Saxophone penis is a specific penile malformation characterized by a saxophone shape due to inflammation of the major penile lymphatic vessels that cause fibrosis of the surrounding connective tissue. Poor blood flow further causes contracture and distortion of the penile axis.4 Saxophone penis also has been associated with primary lymphedema, lymphogranuloma venereum, filariasis,5 and administration of paraffin injections.6 We describe 3 men with HS who presented with saxophone penis.
A 33-year-old man with Hurley stage III HS presented with a medical history of groin lesions and progressive penoscrotal edema of 13 years’ duration. He had a body mass index (BMI) of 37, no family history of HS or comorbidities, and a 15-year history of smoking 20 cigarettes per day. After repeated surgical drainage of the HS lesions as well as antibiotic treatment with clindamycin 600 mg/d and rifampicin 600 mg/d, the patient was kept on a maintenance therapy with adalimumab 40 mg/wk. Due to lack of response, treatment was discontinued at week 16. Clindamycin and rifampicin 300 mg were immediately reintroduced with no benefit on the genital lesions. The patient underwent genital reconstruction, including penile degloving, scrotoplasty, infrapubic fat pad removal, and perineoplasty (Figure 1). The patient currently is not undergoing any therapies.
A 55-year-old man presented with Hurley stage II HS of 33 years’ duration. He had a BMI of 52; a history of hypertension, hyperuricemia, severe hip and knee osteoarthritis, and orchiopexy in childhood; a smoking history of 40 cigarettes per day; and an alcohol consumption history of 200 mL per day since 18 years of age. He had radical excision of axillary lesions 8 years prior. One year later, he was treated with concomitant clindamycin and rifampicin 300 mg twice daily for 3 months with no desirable effects. Adalimumab 40 mg/wk was initiated. After 12 weeks of treatment, he experienced 80% improvement in all areas except the genital region. He continued adalimumab for 3 years with good clinical response in all HS-affected sites except the genital region.
A 66-year-old man presented with Hurley stage III HS of 37 years’ duration. He had a smoking history of 10 cigarettes per day for 30 years, a BMI of 24.6, and a medical history of long-standing hypertension and hypothyroidism. A 3-month course of clindamycin and rifampicin 600 mg/d was ineffective; adalimumab 40 mg/wk was initiated. All affected areas improved, except for the saxophone penis. He continues his fifth year of therapy with adalimumab (Figure 2).

Hidradenitis suppurativa is associated with chronic pain, purulent malodor, and scarring with structural deformity. Repetitive inflammation causes fibrosis, scar formation, and soft-tissue destruction of lymphatic vessels, leading to lymphedema; primary lymphedema of the genitals in men has been reported to result in a saxophone penis.4
The only approved biologic treatments for moderate to severe HS are the tumor necrosis factor α inhibitor adalimumab and anti-IL-17 secukinumab.1 All 3 of our patients with HS were treated with adalimumab with reasonable success; however, the penile condition remained refractory, which we speculate may be due to adalimumab’s ability to control only active inflammatory lesions but not scars or fibrotic tissue.7 Higher adalimumab dosages were unlikely to be beneficial for their penile condition; some improvements have been reported following fluoroquinolone therapy. To our knowledge, there is no effective medical treatment for saxophone penis. However, surgery showed good results in one of our patients. Among our 3 adalimumab-treated patients, only 1 patient had corrective surgery that resulted in improvement in the penile deformity, further confirming adalimumab’s limited role in genital lymphedema.7 Extensive resection of the lymphedematous tissue, scrotoplasty, and Charles procedure are treatment options.8
Genital lymphedema has been associated with lymphangiectasia, lymphangioma circumscriptum, infections, and neoplasms such as lymphangiosarcoma and squamous cell carcinoma.9 Our patients reported discomfort, hygiene issues, and swelling. One patient reported micturition, and 2 patients reported sexual dysfunction.
Saxophone penis remains a disabling sequela of HS. Early diagnosis and treatment of HS may help prevent development of this condition.
- Lee EY, Alhusayen R, Lansang P, et al. What is hidradenitis suppurativa? Can Fam Physician. 2017;63:114-120.
- Fertitta L, Hotz C, Wolkenstein P, et al. Efficacy and satisfaction of surgical treatment for hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34:839-845.
- Micieli R, Alavi A. Lymphedema in patients with hidradenitis suppurativa: a systematic review of published literature. Int J Dermatol. 2018;57:1471-1480.
- Maatouk I, Moutran R. Saxophone penis. JAMA Dermatol. 2013;149:802.
- Koley S, Mandal RK. Saxophone penis after unilateral inguinal bubo of lymphogranuloma venereum. Indian J Sex Transm Dis AIDS. 2013;34:149-151.
- D’Antuono A, Lambertini M, Gaspari V, et al. Visual dermatology: self-induced chronic saxophone penis due to paraffin injections. J Cutan Med Surg. 2019;23:330.
- Musumeci ML, Scilletta A, Sorci F, et al. Genital lymphedema associated with hidradenitis suppurativa unresponsive to adalimumab treatment. JAAD Case Rep. 2019;5:326-328.
- Jain V, Singh S, Garge S, et al. Saxophone penis due to primary lymphoedema. J Indian Assoc Pediatr Surg. 2009;14:230-231.
- Moosbrugger EA, Mutasim DF. Hidradenitis suppurativa complicated by severe lymphedema and lymphangiectasias. J Am Acad Dermatol. 2011;64:1223-1224.
To the Editor:
Hidradenitis suppurativa (HS) is a multifactorial chronic inflammatory skin disease affecting 1% to 4% of Europeans. It is characterized by recurrent inflamed nodules, abscesses, and sinus tracts in intertriginous regions.1 The genital area is affected in 11% of cases2 and usually is connected to severe forms of HS in both men and women.3 The prevalence of HS-associated genital lymphedema remains unknown.
Saxophone penis is a specific penile malformation characterized by a saxophone shape due to inflammation of the major penile lymphatic vessels that cause fibrosis of the surrounding connective tissue. Poor blood flow further causes contracture and distortion of the penile axis.4 Saxophone penis also has been associated with primary lymphedema, lymphogranuloma venereum, filariasis,5 and administration of paraffin injections.6 We describe 3 men with HS who presented with saxophone penis.
A 33-year-old man with Hurley stage III HS presented with a medical history of groin lesions and progressive penoscrotal edema of 13 years’ duration. He had a body mass index (BMI) of 37, no family history of HS or comorbidities, and a 15-year history of smoking 20 cigarettes per day. After repeated surgical drainage of the HS lesions as well as antibiotic treatment with clindamycin 600 mg/d and rifampicin 600 mg/d, the patient was kept on a maintenance therapy with adalimumab 40 mg/wk. Due to lack of response, treatment was discontinued at week 16. Clindamycin and rifampicin 300 mg were immediately reintroduced with no benefit on the genital lesions. The patient underwent genital reconstruction, including penile degloving, scrotoplasty, infrapubic fat pad removal, and perineoplasty (Figure 1). The patient currently is not undergoing any therapies.
A 55-year-old man presented with Hurley stage II HS of 33 years’ duration. He had a BMI of 52; a history of hypertension, hyperuricemia, severe hip and knee osteoarthritis, and orchiopexy in childhood; a smoking history of 40 cigarettes per day; and an alcohol consumption history of 200 mL per day since 18 years of age. He had radical excision of axillary lesions 8 years prior. One year later, he was treated with concomitant clindamycin and rifampicin 300 mg twice daily for 3 months with no desirable effects. Adalimumab 40 mg/wk was initiated. After 12 weeks of treatment, he experienced 80% improvement in all areas except the genital region. He continued adalimumab for 3 years with good clinical response in all HS-affected sites except the genital region.
A 66-year-old man presented with Hurley stage III HS of 37 years’ duration. He had a smoking history of 10 cigarettes per day for 30 years, a BMI of 24.6, and a medical history of long-standing hypertension and hypothyroidism. A 3-month course of clindamycin and rifampicin 600 mg/d was ineffective; adalimumab 40 mg/wk was initiated. All affected areas improved, except for the saxophone penis. He continues his fifth year of therapy with adalimumab (Figure 2).
Hidradenitis suppurativa is associated with chronic pain, purulent malodor, and scarring with structural deformity. Repetitive inflammation causes fibrosis, scar formation, and soft-tissue destruction of lymphatic vessels, leading to lymphedema; primary lymphedema of the genitals in men has been reported to result in a saxophone penis.4
The only approved biologic treatments for moderate to severe HS are the tumor necrosis factor α inhibitor adalimumab and anti-IL-17 secukinumab.1 All 3 of our patients with HS were treated with adalimumab with reasonable success; however, the penile condition remained refractory, which we speculate may be due to adalimumab’s ability to control only active inflammatory lesions but not scars or fibrotic tissue.7 Higher adalimumab dosages were unlikely to be beneficial for their penile condition; some improvements have been reported following fluoroquinolone therapy. To our knowledge, there is no effective medical treatment for saxophone penis. However, surgery showed good results in one of our patients. Among our 3 adalimumab-treated patients, only 1 patient had corrective surgery that resulted in improvement in the penile deformity, further confirming adalimumab’s limited role in genital lymphedema.7 Extensive resection of the lymphedematous tissue, scrotoplasty, and Charles procedure are treatment options.8
Genital lymphedema has been associated with lymphangiectasia, lymphangioma circumscriptum, infections, and neoplasms such as lymphangiosarcoma and squamous cell carcinoma.9 Our patients reported discomfort, hygiene issues, and swelling. One patient reported micturition, and 2 patients reported sexual dysfunction.
Saxophone penis remains a disabling sequela of HS. Early diagnosis and treatment of HS may help prevent development of this condition.
To the Editor:
Hidradenitis suppurativa (HS) is a multifactorial chronic inflammatory skin disease affecting 1% to 4% of Europeans. It is characterized by recurrent inflamed nodules, abscesses, and sinus tracts in intertriginous regions.1 The genital area is affected in 11% of cases2 and usually is connected to severe forms of HS in both men and women.3 The prevalence of HS-associated genital lymphedema remains unknown.
Saxophone penis is a specific penile malformation characterized by a saxophone shape due to inflammation of the major penile lymphatic vessels that cause fibrosis of the surrounding connective tissue. Poor blood flow further causes contracture and distortion of the penile axis.4 Saxophone penis also has been associated with primary lymphedema, lymphogranuloma venereum, filariasis,5 and administration of paraffin injections.6 We describe 3 men with HS who presented with saxophone penis.
A 33-year-old man with Hurley stage III HS presented with a medical history of groin lesions and progressive penoscrotal edema of 13 years’ duration. He had a body mass index (BMI) of 37, no family history of HS or comorbidities, and a 15-year history of smoking 20 cigarettes per day. After repeated surgical drainage of the HS lesions as well as antibiotic treatment with clindamycin 600 mg/d and rifampicin 600 mg/d, the patient was kept on a maintenance therapy with adalimumab 40 mg/wk. Due to lack of response, treatment was discontinued at week 16. Clindamycin and rifampicin 300 mg were immediately reintroduced with no benefit on the genital lesions. The patient underwent genital reconstruction, including penile degloving, scrotoplasty, infrapubic fat pad removal, and perineoplasty (Figure 1). The patient currently is not undergoing any therapies.
A 55-year-old man presented with Hurley stage II HS of 33 years’ duration. He had a BMI of 52; a history of hypertension, hyperuricemia, severe hip and knee osteoarthritis, and orchiopexy in childhood; a smoking history of 40 cigarettes per day; and an alcohol consumption history of 200 mL per day since 18 years of age. He had radical excision of axillary lesions 8 years prior. One year later, he was treated with concomitant clindamycin and rifampicin 300 mg twice daily for 3 months with no desirable effects. Adalimumab 40 mg/wk was initiated. After 12 weeks of treatment, he experienced 80% improvement in all areas except the genital region. He continued adalimumab for 3 years with good clinical response in all HS-affected sites except the genital region.
A 66-year-old man presented with Hurley stage III HS of 37 years’ duration. He had a smoking history of 10 cigarettes per day for 30 years, a BMI of 24.6, and a medical history of long-standing hypertension and hypothyroidism. A 3-month course of clindamycin and rifampicin 600 mg/d was ineffective; adalimumab 40 mg/wk was initiated. All affected areas improved, except for the saxophone penis. He continues his fifth year of therapy with adalimumab (Figure 2).
Hidradenitis suppurativa is associated with chronic pain, purulent malodor, and scarring with structural deformity. Repetitive inflammation causes fibrosis, scar formation, and soft-tissue destruction of lymphatic vessels, leading to lymphedema; primary lymphedema of the genitals in men has been reported to result in a saxophone penis.4
The only approved biologic treatments for moderate to severe HS are the tumor necrosis factor α inhibitor adalimumab and anti-IL-17 secukinumab.1 All 3 of our patients with HS were treated with adalimumab with reasonable success; however, the penile condition remained refractory, which we speculate may be due to adalimumab’s ability to control only active inflammatory lesions but not scars or fibrotic tissue.7 Higher adalimumab dosages were unlikely to be beneficial for their penile condition; some improvements have been reported following fluoroquinolone therapy. To our knowledge, there is no effective medical treatment for saxophone penis. However, surgery showed good results in one of our patients. Among our 3 adalimumab-treated patients, only 1 patient had corrective surgery that resulted in improvement in the penile deformity, further confirming adalimumab’s limited role in genital lymphedema.7 Extensive resection of the lymphedematous tissue, scrotoplasty, and Charles procedure are treatment options.8
Genital lymphedema has been associated with lymphangiectasia, lymphangioma circumscriptum, infections, and neoplasms such as lymphangiosarcoma and squamous cell carcinoma.9 Our patients reported discomfort, hygiene issues, and swelling. One patient reported micturition, and 2 patients reported sexual dysfunction.
Saxophone penis remains a disabling sequela of HS. Early diagnosis and treatment of HS may help prevent development of this condition.
- Lee EY, Alhusayen R, Lansang P, et al. What is hidradenitis suppurativa? Can Fam Physician. 2017;63:114-120.
- Fertitta L, Hotz C, Wolkenstein P, et al. Efficacy and satisfaction of surgical treatment for hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34:839-845.
- Micieli R, Alavi A. Lymphedema in patients with hidradenitis suppurativa: a systematic review of published literature. Int J Dermatol. 2018;57:1471-1480.
- Maatouk I, Moutran R. Saxophone penis. JAMA Dermatol. 2013;149:802.
- Koley S, Mandal RK. Saxophone penis after unilateral inguinal bubo of lymphogranuloma venereum. Indian J Sex Transm Dis AIDS. 2013;34:149-151.
- D’Antuono A, Lambertini M, Gaspari V, et al. Visual dermatology: self-induced chronic saxophone penis due to paraffin injections. J Cutan Med Surg. 2019;23:330.
- Musumeci ML, Scilletta A, Sorci F, et al. Genital lymphedema associated with hidradenitis suppurativa unresponsive to adalimumab treatment. JAAD Case Rep. 2019;5:326-328.
- Jain V, Singh S, Garge S, et al. Saxophone penis due to primary lymphoedema. J Indian Assoc Pediatr Surg. 2009;14:230-231.
- Moosbrugger EA, Mutasim DF. Hidradenitis suppurativa complicated by severe lymphedema and lymphangiectasias. J Am Acad Dermatol. 2011;64:1223-1224.
- Lee EY, Alhusayen R, Lansang P, et al. What is hidradenitis suppurativa? Can Fam Physician. 2017;63:114-120.
- Fertitta L, Hotz C, Wolkenstein P, et al. Efficacy and satisfaction of surgical treatment for hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34:839-845.
- Micieli R, Alavi A. Lymphedema in patients with hidradenitis suppurativa: a systematic review of published literature. Int J Dermatol. 2018;57:1471-1480.
- Maatouk I, Moutran R. Saxophone penis. JAMA Dermatol. 2013;149:802.
- Koley S, Mandal RK. Saxophone penis after unilateral inguinal bubo of lymphogranuloma venereum. Indian J Sex Transm Dis AIDS. 2013;34:149-151.
- D’Antuono A, Lambertini M, Gaspari V, et al. Visual dermatology: self-induced chronic saxophone penis due to paraffin injections. J Cutan Med Surg. 2019;23:330.
- Musumeci ML, Scilletta A, Sorci F, et al. Genital lymphedema associated with hidradenitis suppurativa unresponsive to adalimumab treatment. JAAD Case Rep. 2019;5:326-328.
- Jain V, Singh S, Garge S, et al. Saxophone penis due to primary lymphoedema. J Indian Assoc Pediatr Surg. 2009;14:230-231.
- Moosbrugger EA, Mutasim DF. Hidradenitis suppurativa complicated by severe lymphedema and lymphangiectasias. J Am Acad Dermatol. 2011;64:1223-1224.
Practice Points
- Hidradenitis suppurativa (HS) is a multifactorial chronic inflammatory skin disease.
- Saxophone penis is a specific penile malformation characterized by a saxophone shape due to inflammation.
- Repetitive inflammation within the context of HS may cause structural deformity of the penis, resulting in a saxophone penis.
- Early diagnosis and treatment of HS may help prevent development of this condition.

Painful Anal Lesions in a Patient With HIV
The Diagnosis: Condyloma Latum
Laboratory test results were notable for a rapid plasma reagin titer of 1:512, a positive Treponema pallidum particle agglutination test, negative rectal nucleic acid amplification tests for gonorrhea and chlamydia, and a negative herpes simplex virus polymerase chain reaction. A VDRL test of cerebrospinal fluid from a lumbar puncture was negative. Histopathology of the punch biopsy sample revealed marked verrucous epidermal hyperplasia without keratinocytic atypia and with mixed inflammation (Figure 1), while immunohistochemical staining showed numerus T pallidum organisms (Figure 2). A diagnosis of condyloma latum was made based on the laboratory, lumbar puncture, and punch biopsy results. Due to a penicillin allergy, the patient was treated with oral doxycycline for 14 days. On follow-up at day 12 of therapy, he reported cessation of rectal pain, and resolution of anal lesions was noted on physical examination.
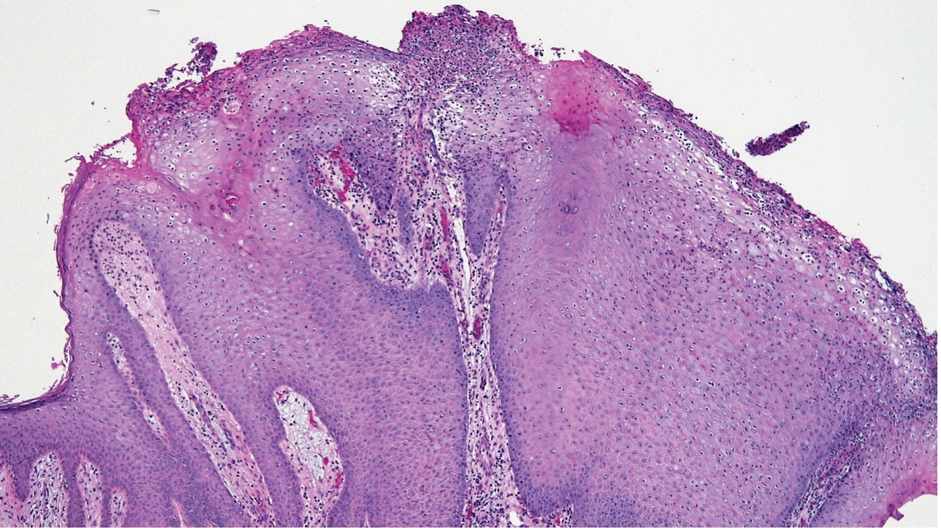
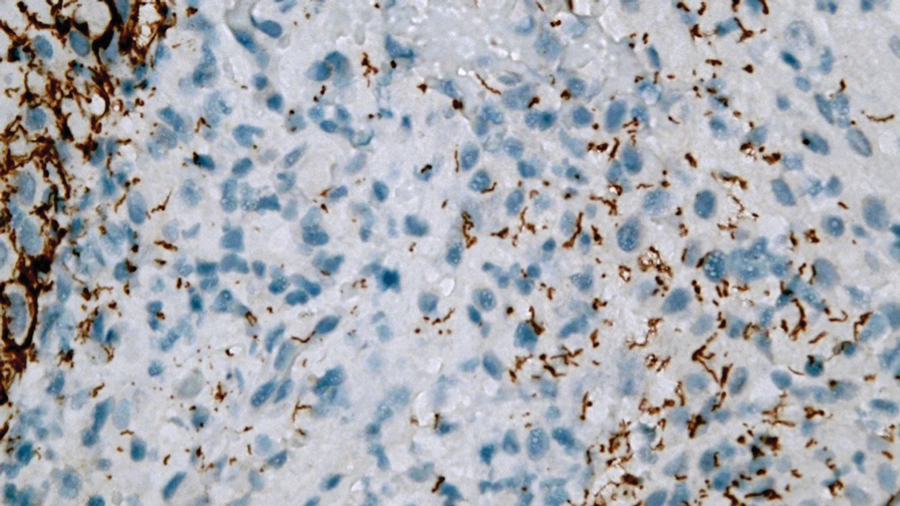
Condylomata lata are highly infectious cutaneous lesions that can manifest during secondary syphilis.1 They typically are described as white or gray, raised, flatappearing plaques and occur in moist areas or skin folds including the anus, scrotum, and vulva. However, these lesions also have been reported in the axillae, umbilicus, nasolabial folds, and other anatomic areas.1,2 The lesions can be painful and often manifest in multiples, especially in patients living with HIV.3
Condylomata lata can have a verrucous appearance and may mimic other anogenital lesions, such as condylomata acuminata, genital herpes, and malignant tumors, leading to an initial misdiagnosis.1,2 Condylomata lata should always be included in the differential when evaluating anogenital lesions. Other conditions in the differential diagnosis include psoriasis, typically manifesting as erythematous plaques with silver scale, and molluscum contagiosum, appearing as small umbilicated papules on physical examination.
Condylomata lata have been reported to occur in 6% to 23% of patients with secondary syphilis.1 Although secondary syphilis more typically manifests with a diffuse maculopapular rash, condylomata lata may be the sole dermatologic manifestation.4
Histopathology of condylomata lata consists of epithelial hyperplasia as well as lymphocytic and plasma cell infiltrates. It is diagnosed by serologic testing as well as immunohistochemical staining or dark-field microscopy.
First-line treatment of secondary syphilis is a single dose of benzathine penicillin G administered intramuscularly.5 However, a 14-day course of oral doxycycline can be used in patients with a penicillin allergy. When compliance and follow-up cannot be guaranteed, penicillin desensitization and treatment with benzathine penicillin G is recommended. Clinical evaluation and repeat serologic testing should be performed at 6 and 12 months follow-up, or more frequently if clinically indicated.5
- Pourang A, Fung MA, Tartar D, et al. Condyloma lata in secondary syphilis. JAAD Case Rep. 2021;10:18-21. doi:10.1016/j.jdcr.2021.01.025
- Liu Z, Wang L, Zhang G, et al. Warty mucosal lesions: oral condyloma lata of secondary syphilis. Indian J Dermatol Venereol Leprol. 2017;83:277. doi:10.4103/0378-6323.191129
- Rompalo AM, Joesoef MR, O’Donnell JA, et al; Syphilis and HIV Study Group. Clinical manifestations of early syphilis by HIV status and gender: results of the syphilis and HIV study. Sex Transm Dis.2001;28:158-165.
- Kumar P, Das A, Mondal A. Secondary syphilis: an unusual presentation. Indian J Sex Transm Dis AIDS. 2017;38:98-99. doi:10.4103/0253-7184.194318
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70:1-187. doi:10.15585/mmwr.rr7004a1
The Diagnosis: Condyloma Latum
Laboratory test results were notable for a rapid plasma reagin titer of 1:512, a positive Treponema pallidum particle agglutination test, negative rectal nucleic acid amplification tests for gonorrhea and chlamydia, and a negative herpes simplex virus polymerase chain reaction. A VDRL test of cerebrospinal fluid from a lumbar puncture was negative. Histopathology of the punch biopsy sample revealed marked verrucous epidermal hyperplasia without keratinocytic atypia and with mixed inflammation (Figure 1), while immunohistochemical staining showed numerus T pallidum organisms (Figure 2). A diagnosis of condyloma latum was made based on the laboratory, lumbar puncture, and punch biopsy results. Due to a penicillin allergy, the patient was treated with oral doxycycline for 14 days. On follow-up at day 12 of therapy, he reported cessation of rectal pain, and resolution of anal lesions was noted on physical examination.
Condylomata lata are highly infectious cutaneous lesions that can manifest during secondary syphilis.1 They typically are described as white or gray, raised, flatappearing plaques and occur in moist areas or skin folds including the anus, scrotum, and vulva. However, these lesions also have been reported in the axillae, umbilicus, nasolabial folds, and other anatomic areas.1,2 The lesions can be painful and often manifest in multiples, especially in patients living with HIV.3
Condylomata lata can have a verrucous appearance and may mimic other anogenital lesions, such as condylomata acuminata, genital herpes, and malignant tumors, leading to an initial misdiagnosis.1,2 Condylomata lata should always be included in the differential when evaluating anogenital lesions. Other conditions in the differential diagnosis include psoriasis, typically manifesting as erythematous plaques with silver scale, and molluscum contagiosum, appearing as small umbilicated papules on physical examination.
Condylomata lata have been reported to occur in 6% to 23% of patients with secondary syphilis.1 Although secondary syphilis more typically manifests with a diffuse maculopapular rash, condylomata lata may be the sole dermatologic manifestation.4
Histopathology of condylomata lata consists of epithelial hyperplasia as well as lymphocytic and plasma cell infiltrates. It is diagnosed by serologic testing as well as immunohistochemical staining or dark-field microscopy.
First-line treatment of secondary syphilis is a single dose of benzathine penicillin G administered intramuscularly.5 However, a 14-day course of oral doxycycline can be used in patients with a penicillin allergy. When compliance and follow-up cannot be guaranteed, penicillin desensitization and treatment with benzathine penicillin G is recommended. Clinical evaluation and repeat serologic testing should be performed at 6 and 12 months follow-up, or more frequently if clinically indicated.5
The Diagnosis: Condyloma Latum
Laboratory test results were notable for a rapid plasma reagin titer of 1:512, a positive Treponema pallidum particle agglutination test, negative rectal nucleic acid amplification tests for gonorrhea and chlamydia, and a negative herpes simplex virus polymerase chain reaction. A VDRL test of cerebrospinal fluid from a lumbar puncture was negative. Histopathology of the punch biopsy sample revealed marked verrucous epidermal hyperplasia without keratinocytic atypia and with mixed inflammation (Figure 1), while immunohistochemical staining showed numerus T pallidum organisms (Figure 2). A diagnosis of condyloma latum was made based on the laboratory, lumbar puncture, and punch biopsy results. Due to a penicillin allergy, the patient was treated with oral doxycycline for 14 days. On follow-up at day 12 of therapy, he reported cessation of rectal pain, and resolution of anal lesions was noted on physical examination.
Condylomata lata are highly infectious cutaneous lesions that can manifest during secondary syphilis.1 They typically are described as white or gray, raised, flatappearing plaques and occur in moist areas or skin folds including the anus, scrotum, and vulva. However, these lesions also have been reported in the axillae, umbilicus, nasolabial folds, and other anatomic areas.1,2 The lesions can be painful and often manifest in multiples, especially in patients living with HIV.3
Condylomata lata can have a verrucous appearance and may mimic other anogenital lesions, such as condylomata acuminata, genital herpes, and malignant tumors, leading to an initial misdiagnosis.1,2 Condylomata lata should always be included in the differential when evaluating anogenital lesions. Other conditions in the differential diagnosis include psoriasis, typically manifesting as erythematous plaques with silver scale, and molluscum contagiosum, appearing as small umbilicated papules on physical examination.
Condylomata lata have been reported to occur in 6% to 23% of patients with secondary syphilis.1 Although secondary syphilis more typically manifests with a diffuse maculopapular rash, condylomata lata may be the sole dermatologic manifestation.4
Histopathology of condylomata lata consists of epithelial hyperplasia as well as lymphocytic and plasma cell infiltrates. It is diagnosed by serologic testing as well as immunohistochemical staining or dark-field microscopy.
First-line treatment of secondary syphilis is a single dose of benzathine penicillin G administered intramuscularly.5 However, a 14-day course of oral doxycycline can be used in patients with a penicillin allergy. When compliance and follow-up cannot be guaranteed, penicillin desensitization and treatment with benzathine penicillin G is recommended. Clinical evaluation and repeat serologic testing should be performed at 6 and 12 months follow-up, or more frequently if clinically indicated.5
- Pourang A, Fung MA, Tartar D, et al. Condyloma lata in secondary syphilis. JAAD Case Rep. 2021;10:18-21. doi:10.1016/j.jdcr.2021.01.025
- Liu Z, Wang L, Zhang G, et al. Warty mucosal lesions: oral condyloma lata of secondary syphilis. Indian J Dermatol Venereol Leprol. 2017;83:277. doi:10.4103/0378-6323.191129
- Rompalo AM, Joesoef MR, O’Donnell JA, et al; Syphilis and HIV Study Group. Clinical manifestations of early syphilis by HIV status and gender: results of the syphilis and HIV study. Sex Transm Dis.2001;28:158-165.
- Kumar P, Das A, Mondal A. Secondary syphilis: an unusual presentation. Indian J Sex Transm Dis AIDS. 2017;38:98-99. doi:10.4103/0253-7184.194318
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70:1-187. doi:10.15585/mmwr.rr7004a1
- Pourang A, Fung MA, Tartar D, et al. Condyloma lata in secondary syphilis. JAAD Case Rep. 2021;10:18-21. doi:10.1016/j.jdcr.2021.01.025
- Liu Z, Wang L, Zhang G, et al. Warty mucosal lesions: oral condyloma lata of secondary syphilis. Indian J Dermatol Venereol Leprol. 2017;83:277. doi:10.4103/0378-6323.191129
- Rompalo AM, Joesoef MR, O’Donnell JA, et al; Syphilis and HIV Study Group. Clinical manifestations of early syphilis by HIV status and gender: results of the syphilis and HIV study. Sex Transm Dis.2001;28:158-165.
- Kumar P, Das A, Mondal A. Secondary syphilis: an unusual presentation. Indian J Sex Transm Dis AIDS. 2017;38:98-99. doi:10.4103/0253-7184.194318
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70:1-187. doi:10.15585/mmwr.rr7004a1
A 24-year-old man presented to the emergency department with rectal pain and lesions of 3 weeks’ duration that were progressively worsening. He had a medical history of poorly controlled HIV, cerebral toxoplasmosis, and genital herpes, as well as a social history of sexual activity with other men.
He had been diagnosed with HIV 7 years prior and had been off therapy until 1 year prior to the current presentation, when he was hospitalized with encephalopathy (CD4 count, <50 cells/mm3). A diagnosis of cerebral toxoplasmosis was made, and he began a treatment regimen of sulfadiazine, pyrimethamine, and leucovorin, as well as bictegravir, emtricitabine, and tenofovir alafenamide. Since then, the patient admitted to difficulty with medication adherence.
Rapid plasma reagin, gonorrhea, and chlamydia testing were negative during a routine workup 6 months prior to the current presentation. He initially presented to an urgent care clinic for evaluation of the rectal pain and lesions and was treated empirically with topical podofilox. He presented to the emergency department 1 week later (3 weeks after symptom onset) with anal warts and apparent vesicular lesions. Empiric treatment with oral valacyclovir was prescribed.
Despite these treatments, the rectal pain became severe—especially upon sitting, defecation, and physical exertion—prompting further evaluation. Physical examination revealed soft, flat-topped, moist-appearing, gray plaques with minimal surrounding erythema at the anus. Laboratory test results demonstrated a CD4 count of 161 cells/mm3 and an HIV viral load of 137 copies/mL.


Identifying, Treating Lyme Disease in Primary Care
Geographic spread of the ticks that most often cause Lyme disease in the United States and a rise in incidence of bites, resulting in 476,000 new US cases a year, have increased the chances that physicians who have never encountered a patient with Lyme disease will see their first cases.
“It’s increasing in areas where it was not seen before,” Steven E. Schutzer, MD, with the Department of Medicine, Rutgers New Jersey Medical School, Newark, said in an interview. Dr. Schutzer coauthored a report on diagnosing and treating Lyme disease with Patricia K. Coyle, MD, Department of Neurology, Renaissance School of Medicine at Stony Brook University, Stony Brook, New York.
The report, a Curbside Consult published in New England Journal of Medicine Evidence, comes amid high season for Lyme disease. Bites from an ixodid (hard shield) tick — almost always the source of the disease in the United States — are most common from April through October.
Identifying the Bite
About 70%-90% of the time, Lyme disease will be signaled by erythema migrans (EM) or lesion expanding from the tick bite site, the authors wrote. The “classic” presentation looks like a bullseye, but most of the time the skin will show a variation of that, the authors noted.
“The presence of EM is considered the best clinical diagnostic marker for Lyme disease,” they wrote.
Other dermatologic conditions, however, can complicate diagnosis: “EM mimickers include contact dermatitis, other arthropod bites, fixed drug eruptions, granuloma annulare, cellulitis, dermatophytosis, and systemic lupus erythematosus,” they wrote.
Testing Steps
“The current recommendation is to do two-step testing almost simultaneously,” Dr. Schutzer said in an interview. The first, he said, is an ELISA (enzyme-linked immunosorbent assay)-type test and the second one, used for years, has been a pictoral view of a Western immunoblot showing which antigens of the Lyme bacteria, Borrelia burgdorferi, the antibodies are reacting to.
However, the pictoral view is subjective and some of the antigens could be cross-reactive. So the U.S. Food and Drug Administration (FDA) “has been allowing newer substitutes like a second ELISA-like assay that often uses more recombinant, less cross-reactive antigen targets,” he said. The authors advised that, “The second-tier test should not be performed alone without the first tier.”
Dr. Schutzer advised physicians to check with the lab they plan to use before sending samples.
“If you’re a practicing physician and you know you’re using a particular laboratory, you should familiarize yourself with them, talking to one of the clinical pathologists involved in advance to know what the limitations are.” Take the time to talk with the person overseeing the test and get tips on how they want the sample transported and how the cases should be reported, he said.
If the patient has neurological symptoms, he said, before treating talk with a neurologist who can advise whether, for instance, a spinal tap is in order or whether an emergency department visit is appropriate.
“If you just start proceeding you may mess up the diagnostic signs that could show up in a lab test. Don’t be hesitant to ask for extra input from colleagues,” Dr. Schutzer said.
Suspicion in Endemic Areas
On Long Island, New York, where Lyme disease is endemic, internist Ian Storch, DO, said he sees “a few cases a season.
“We have a lot of people over the summer going to the Hamptons and areas out east for the weekend and tick bites are not uncommon,” he said. “People panic.”
He said one thing it’s important to tell patients is that the tick has to be on the skin for 48-72 hours to transmit the disease. If individuals were in a wooded area and were fine before they got there and the tick was attached for less than 2 days, “they’re usually fine.”
Another issue, Dr. Storch said, is patients sometimes want to get tested for Lyme disease immediately after a tick bite. But the antibody test doesn’t turn positive for weeks, he noted, and you can get a false-negative result. “If you’re worried and you really want to test, you need to wait 6 weeks to do the blood test.”
In his region, he said that although a tick bite is a red flag, he may also suspect Lyme disease when a patient presents with otherwise unexplained joint pain, weakness, lethargy, or fever. “In our area, those are things that would make you test for Lyme.”
He also urged consideration of Lyme in this new age of long COVID. Weakness, fatigue, and lethargy are also classic symptoms of long COVID, he noted. “Keep Lyme disease in your differential because there is a lot of overlap with chronic Lyme disease,” Dr. Storch said.
Discerning Lyme from Southern Tick–Associated Rash Illness
Bonnie M. Word, MD, director of the Houston Travel Medicine Clinic in Texas, where Lyme disease is not endemic, said Lyme disease “will not and should not be on the initial differential diagnosis for those residing in nonendemic areas unless a history of travel to an endemic area is obtained.”
She noted the typical EM rash may not be as distinct or easy to discern on black and brown skin. In addition, she said, EM may have many variations in presentation, such as a crusted center or faint borders, which could lead to a delay in diagnosis and treatment. She suggested consulting the CDC guidance on Lyme disease rashes.
Another challenge in diagnosis, she said, is the patient who presents with what appears to be a classic EM lesion but does not live in a Lyme-endemic area. In Texas, Southern Tick–Associated Rash Illness (STARI) may present with a similar lesion, she said.
“It is transmitted by the Lone Star Tick, which is found in the southeast and south-central US,” Dr. Word said. “However, its habitat is moving northward and westerly,” she said.
Adding Lyme disease to the differential diagnosis is reasonable, she said, if a patient presents with neurologic symptoms “such as a facial palsy, meningitis, radiculitis, and carditis if in addition to their symptoms there is evidence of an epidemiologic link to a Lyme-endemic region.”
She noted that a detailed travel history is important as “Lyme is also endemic in Eastern Canada, Europe, states of the former Soviet Union, China, Mongolia, and Japan.”
Primary care physicians play a critical role in evaluating, diagnosing, and treating most cases of early Lyme disease, thus limiting the number of people who will develop disseminated or late Lyme disease, she said. “The two latter manifestations are most often treated by infectious disease, neurology, or rheumatology specialists.”
Treatment*
Treatment is tailored to the clinical situation, Dr. Schutzer and Dr. Coyle write. A watch-and-wait approach may be appropriate in an asymptomatic but concerned person, even in an endemic area if the person has no known tick bite and no EM lesion.
If there is high risk of an infected ixodid tick bite in a high-incidence area and the tick was attached for at least 36 hours but less than 72 hours, one dose of doxycycline has been recommended as prophylaxis.
When a diagnosis of early nondisseminated Lyme disease is made after observation of an EM lesion, oral antibiotics are typically used to treat for 10 to 14 days. Suggested oral antibiotics and doses are 100 mg of doxycycline twice a day, 500 mg of amoxicillin three times a day, or 500 mg of cefuroxime twice a day, the authors write.
Dr. Schutzer said he hopes the paper serves as a refresher for those physicians who regularly see Lyme disease cases and also helps those newly included in the disease’s spreading regions.
“The earlier you diagnose it, the earlier you can treat it and the better the chance for a favorable outcome,” he said.
Dr. Schutzer, Dr. Coyle, Dr. Storch, and Dr. Word reported no relevant financial relationships.
*This story was updated on August, 2, 2024.
Geographic spread of the ticks that most often cause Lyme disease in the United States and a rise in incidence of bites, resulting in 476,000 new US cases a year, have increased the chances that physicians who have never encountered a patient with Lyme disease will see their first cases.
“It’s increasing in areas where it was not seen before,” Steven E. Schutzer, MD, with the Department of Medicine, Rutgers New Jersey Medical School, Newark, said in an interview. Dr. Schutzer coauthored a report on diagnosing and treating Lyme disease with Patricia K. Coyle, MD, Department of Neurology, Renaissance School of Medicine at Stony Brook University, Stony Brook, New York.
The report, a Curbside Consult published in New England Journal of Medicine Evidence, comes amid high season for Lyme disease. Bites from an ixodid (hard shield) tick — almost always the source of the disease in the United States — are most common from April through October.
Identifying the Bite
About 70%-90% of the time, Lyme disease will be signaled by erythema migrans (EM) or lesion expanding from the tick bite site, the authors wrote. The “classic” presentation looks like a bullseye, but most of the time the skin will show a variation of that, the authors noted.
“The presence of EM is considered the best clinical diagnostic marker for Lyme disease,” they wrote.
Other dermatologic conditions, however, can complicate diagnosis: “EM mimickers include contact dermatitis, other arthropod bites, fixed drug eruptions, granuloma annulare, cellulitis, dermatophytosis, and systemic lupus erythematosus,” they wrote.
Testing Steps
“The current recommendation is to do two-step testing almost simultaneously,” Dr. Schutzer said in an interview. The first, he said, is an ELISA (enzyme-linked immunosorbent assay)-type test and the second one, used for years, has been a pictoral view of a Western immunoblot showing which antigens of the Lyme bacteria, Borrelia burgdorferi, the antibodies are reacting to.
However, the pictoral view is subjective and some of the antigens could be cross-reactive. So the U.S. Food and Drug Administration (FDA) “has been allowing newer substitutes like a second ELISA-like assay that often uses more recombinant, less cross-reactive antigen targets,” he said. The authors advised that, “The second-tier test should not be performed alone without the first tier.”
Dr. Schutzer advised physicians to check with the lab they plan to use before sending samples.
“If you’re a practicing physician and you know you’re using a particular laboratory, you should familiarize yourself with them, talking to one of the clinical pathologists involved in advance to know what the limitations are.” Take the time to talk with the person overseeing the test and get tips on how they want the sample transported and how the cases should be reported, he said.
If the patient has neurological symptoms, he said, before treating talk with a neurologist who can advise whether, for instance, a spinal tap is in order or whether an emergency department visit is appropriate.
“If you just start proceeding you may mess up the diagnostic signs that could show up in a lab test. Don’t be hesitant to ask for extra input from colleagues,” Dr. Schutzer said.
Suspicion in Endemic Areas
On Long Island, New York, where Lyme disease is endemic, internist Ian Storch, DO, said he sees “a few cases a season.
“We have a lot of people over the summer going to the Hamptons and areas out east for the weekend and tick bites are not uncommon,” he said. “People panic.”
He said one thing it’s important to tell patients is that the tick has to be on the skin for 48-72 hours to transmit the disease. If individuals were in a wooded area and were fine before they got there and the tick was attached for less than 2 days, “they’re usually fine.”
Another issue, Dr. Storch said, is patients sometimes want to get tested for Lyme disease immediately after a tick bite. But the antibody test doesn’t turn positive for weeks, he noted, and you can get a false-negative result. “If you’re worried and you really want to test, you need to wait 6 weeks to do the blood test.”
In his region, he said that although a tick bite is a red flag, he may also suspect Lyme disease when a patient presents with otherwise unexplained joint pain, weakness, lethargy, or fever. “In our area, those are things that would make you test for Lyme.”
He also urged consideration of Lyme in this new age of long COVID. Weakness, fatigue, and lethargy are also classic symptoms of long COVID, he noted. “Keep Lyme disease in your differential because there is a lot of overlap with chronic Lyme disease,” Dr. Storch said.
Discerning Lyme from Southern Tick–Associated Rash Illness
Bonnie M. Word, MD, director of the Houston Travel Medicine Clinic in Texas, where Lyme disease is not endemic, said Lyme disease “will not and should not be on the initial differential diagnosis for those residing in nonendemic areas unless a history of travel to an endemic area is obtained.”
She noted the typical EM rash may not be as distinct or easy to discern on black and brown skin. In addition, she said, EM may have many variations in presentation, such as a crusted center or faint borders, which could lead to a delay in diagnosis and treatment. She suggested consulting the CDC guidance on Lyme disease rashes.
Another challenge in diagnosis, she said, is the patient who presents with what appears to be a classic EM lesion but does not live in a Lyme-endemic area. In Texas, Southern Tick–Associated Rash Illness (STARI) may present with a similar lesion, she said.
“It is transmitted by the Lone Star Tick, which is found in the southeast and south-central US,” Dr. Word said. “However, its habitat is moving northward and westerly,” she said.
Adding Lyme disease to the differential diagnosis is reasonable, she said, if a patient presents with neurologic symptoms “such as a facial palsy, meningitis, radiculitis, and carditis if in addition to their symptoms there is evidence of an epidemiologic link to a Lyme-endemic region.”
She noted that a detailed travel history is important as “Lyme is also endemic in Eastern Canada, Europe, states of the former Soviet Union, China, Mongolia, and Japan.”
Primary care physicians play a critical role in evaluating, diagnosing, and treating most cases of early Lyme disease, thus limiting the number of people who will develop disseminated or late Lyme disease, she said. “The two latter manifestations are most often treated by infectious disease, neurology, or rheumatology specialists.”
Treatment*
Treatment is tailored to the clinical situation, Dr. Schutzer and Dr. Coyle write. A watch-and-wait approach may be appropriate in an asymptomatic but concerned person, even in an endemic area if the person has no known tick bite and no EM lesion.
If there is high risk of an infected ixodid tick bite in a high-incidence area and the tick was attached for at least 36 hours but less than 72 hours, one dose of doxycycline has been recommended as prophylaxis.
When a diagnosis of early nondisseminated Lyme disease is made after observation of an EM lesion, oral antibiotics are typically used to treat for 10 to 14 days. Suggested oral antibiotics and doses are 100 mg of doxycycline twice a day, 500 mg of amoxicillin three times a day, or 500 mg of cefuroxime twice a day, the authors write.
Dr. Schutzer said he hopes the paper serves as a refresher for those physicians who regularly see Lyme disease cases and also helps those newly included in the disease’s spreading regions.
“The earlier you diagnose it, the earlier you can treat it and the better the chance for a favorable outcome,” he said.
Dr. Schutzer, Dr. Coyle, Dr. Storch, and Dr. Word reported no relevant financial relationships.
*This story was updated on August, 2, 2024.
Geographic spread of the ticks that most often cause Lyme disease in the United States and a rise in incidence of bites, resulting in 476,000 new US cases a year, have increased the chances that physicians who have never encountered a patient with Lyme disease will see their first cases.
“It’s increasing in areas where it was not seen before,” Steven E. Schutzer, MD, with the Department of Medicine, Rutgers New Jersey Medical School, Newark, said in an interview. Dr. Schutzer coauthored a report on diagnosing and treating Lyme disease with Patricia K. Coyle, MD, Department of Neurology, Renaissance School of Medicine at Stony Brook University, Stony Brook, New York.
The report, a Curbside Consult published in New England Journal of Medicine Evidence, comes amid high season for Lyme disease. Bites from an ixodid (hard shield) tick — almost always the source of the disease in the United States — are most common from April through October.
Identifying the Bite
About 70%-90% of the time, Lyme disease will be signaled by erythema migrans (EM) or lesion expanding from the tick bite site, the authors wrote. The “classic” presentation looks like a bullseye, but most of the time the skin will show a variation of that, the authors noted.
“The presence of EM is considered the best clinical diagnostic marker for Lyme disease,” they wrote.
Other dermatologic conditions, however, can complicate diagnosis: “EM mimickers include contact dermatitis, other arthropod bites, fixed drug eruptions, granuloma annulare, cellulitis, dermatophytosis, and systemic lupus erythematosus,” they wrote.
Testing Steps
“The current recommendation is to do two-step testing almost simultaneously,” Dr. Schutzer said in an interview. The first, he said, is an ELISA (enzyme-linked immunosorbent assay)-type test and the second one, used for years, has been a pictoral view of a Western immunoblot showing which antigens of the Lyme bacteria, Borrelia burgdorferi, the antibodies are reacting to.
However, the pictoral view is subjective and some of the antigens could be cross-reactive. So the U.S. Food and Drug Administration (FDA) “has been allowing newer substitutes like a second ELISA-like assay that often uses more recombinant, less cross-reactive antigen targets,” he said. The authors advised that, “The second-tier test should not be performed alone without the first tier.”
Dr. Schutzer advised physicians to check with the lab they plan to use before sending samples.
“If you’re a practicing physician and you know you’re using a particular laboratory, you should familiarize yourself with them, talking to one of the clinical pathologists involved in advance to know what the limitations are.” Take the time to talk with the person overseeing the test and get tips on how they want the sample transported and how the cases should be reported, he said.
If the patient has neurological symptoms, he said, before treating talk with a neurologist who can advise whether, for instance, a spinal tap is in order or whether an emergency department visit is appropriate.
“If you just start proceeding you may mess up the diagnostic signs that could show up in a lab test. Don’t be hesitant to ask for extra input from colleagues,” Dr. Schutzer said.
Suspicion in Endemic Areas
On Long Island, New York, where Lyme disease is endemic, internist Ian Storch, DO, said he sees “a few cases a season.
“We have a lot of people over the summer going to the Hamptons and areas out east for the weekend and tick bites are not uncommon,” he said. “People panic.”
He said one thing it’s important to tell patients is that the tick has to be on the skin for 48-72 hours to transmit the disease. If individuals were in a wooded area and were fine before they got there and the tick was attached for less than 2 days, “they’re usually fine.”
Another issue, Dr. Storch said, is patients sometimes want to get tested for Lyme disease immediately after a tick bite. But the antibody test doesn’t turn positive for weeks, he noted, and you can get a false-negative result. “If you’re worried and you really want to test, you need to wait 6 weeks to do the blood test.”
In his region, he said that although a tick bite is a red flag, he may also suspect Lyme disease when a patient presents with otherwise unexplained joint pain, weakness, lethargy, or fever. “In our area, those are things that would make you test for Lyme.”
He also urged consideration of Lyme in this new age of long COVID. Weakness, fatigue, and lethargy are also classic symptoms of long COVID, he noted. “Keep Lyme disease in your differential because there is a lot of overlap with chronic Lyme disease,” Dr. Storch said.
Discerning Lyme from Southern Tick–Associated Rash Illness
Bonnie M. Word, MD, director of the Houston Travel Medicine Clinic in Texas, where Lyme disease is not endemic, said Lyme disease “will not and should not be on the initial differential diagnosis for those residing in nonendemic areas unless a history of travel to an endemic area is obtained.”
She noted the typical EM rash may not be as distinct or easy to discern on black and brown skin. In addition, she said, EM may have many variations in presentation, such as a crusted center or faint borders, which could lead to a delay in diagnosis and treatment. She suggested consulting the CDC guidance on Lyme disease rashes.
Another challenge in diagnosis, she said, is the patient who presents with what appears to be a classic EM lesion but does not live in a Lyme-endemic area. In Texas, Southern Tick–Associated Rash Illness (STARI) may present with a similar lesion, she said.
“It is transmitted by the Lone Star Tick, which is found in the southeast and south-central US,” Dr. Word said. “However, its habitat is moving northward and westerly,” she said.
Adding Lyme disease to the differential diagnosis is reasonable, she said, if a patient presents with neurologic symptoms “such as a facial palsy, meningitis, radiculitis, and carditis if in addition to their symptoms there is evidence of an epidemiologic link to a Lyme-endemic region.”
She noted that a detailed travel history is important as “Lyme is also endemic in Eastern Canada, Europe, states of the former Soviet Union, China, Mongolia, and Japan.”
Primary care physicians play a critical role in evaluating, diagnosing, and treating most cases of early Lyme disease, thus limiting the number of people who will develop disseminated or late Lyme disease, she said. “The two latter manifestations are most often treated by infectious disease, neurology, or rheumatology specialists.”
Treatment*
Treatment is tailored to the clinical situation, Dr. Schutzer and Dr. Coyle write. A watch-and-wait approach may be appropriate in an asymptomatic but concerned person, even in an endemic area if the person has no known tick bite and no EM lesion.
If there is high risk of an infected ixodid tick bite in a high-incidence area and the tick was attached for at least 36 hours but less than 72 hours, one dose of doxycycline has been recommended as prophylaxis.
When a diagnosis of early nondisseminated Lyme disease is made after observation of an EM lesion, oral antibiotics are typically used to treat for 10 to 14 days. Suggested oral antibiotics and doses are 100 mg of doxycycline twice a day, 500 mg of amoxicillin three times a day, or 500 mg of cefuroxime twice a day, the authors write.
Dr. Schutzer said he hopes the paper serves as a refresher for those physicians who regularly see Lyme disease cases and also helps those newly included in the disease’s spreading regions.
“The earlier you diagnose it, the earlier you can treat it and the better the chance for a favorable outcome,” he said.
Dr. Schutzer, Dr. Coyle, Dr. Storch, and Dr. Word reported no relevant financial relationships.
*This story was updated on August, 2, 2024.
Shortage of Blood Bottles Could Disrupt Care
Hospitals and laboratories across the United States are grappling with a shortage of Becton Dickinson BACTEC blood culture bottles that threatens to extend at least until September.
In a health advisory, the Centers for Disease Control and Prevention (CDC) warned that the critical shortage could lead to “delays in diagnosis, misdiagnosis, or other challenges” in the management of patients with infectious diseases.
Healthcare providers, laboratories, healthcare facility administrators, and state, tribal, local, and territorial health departments affected by the shortage “should immediately begin to assess their situations and develop plans and options to mitigate the potential impact,” according to the health advisory.
What to Do
To reduce the impact of the shortage, facilities are urged to:
- Determine the type of blood culture bottles they have
- Optimize the use of blood cultures at their facility
- Take steps to prevent blood culture contamination
- Ensure that the appropriate volume of blood is collected for culture
- Assess alternate options for blood cultures
- Work with a nearby facility or send samples to another laboratory
Health departments are advised to contact hospitals and laboratories in their jurisdictions to determine whether the shortage will affect them. Health departments are also encouraged to educate others on the supply shortage, optimal use of blood cultures, and mechanisms for reporting supply chain shortages or interruptions to the Food and Drug Administration (FDA), as well as to help with communication between laboratories and facilities willing to assist others in need.
To further assist affected providers, the CDC, in collaboration with the Infectious Diseases Society of America, hosted a webinar with speakers from Johns Hopkins University, Massachusetts General Hospital, and Vanderbilt University, who shared what their institutions are doing to cope with the shortage and protect patients.
Why It Happened
In June, Becton Dickinson warned its customers that they may experience “intermittent delays” in the supply of some BACTEC blood culture media over the coming months because of reduced availability of plastic bottles from its supplier.
In a July 22 update, the company said the supplier issues were “more complex” than originally communicated and it is taking steps to “resolve this challenge as quickly as possible.”
In July, the FDA published a letter to healthcare providers acknowledging the supply disruptions and recommended strategies to preserve the supply for patients at highest risk.
Becton Dickinson has promised an update by September to this “dynamic and evolving situation.”
A version of this article appeared on Medscape.com.
Hospitals and laboratories across the United States are grappling with a shortage of Becton Dickinson BACTEC blood culture bottles that threatens to extend at least until September.
In a health advisory, the Centers for Disease Control and Prevention (CDC) warned that the critical shortage could lead to “delays in diagnosis, misdiagnosis, or other challenges” in the management of patients with infectious diseases.
Healthcare providers, laboratories, healthcare facility administrators, and state, tribal, local, and territorial health departments affected by the shortage “should immediately begin to assess their situations and develop plans and options to mitigate the potential impact,” according to the health advisory.
What to Do
To reduce the impact of the shortage, facilities are urged to:
- Determine the type of blood culture bottles they have
- Optimize the use of blood cultures at their facility
- Take steps to prevent blood culture contamination
- Ensure that the appropriate volume of blood is collected for culture
- Assess alternate options for blood cultures
- Work with a nearby facility or send samples to another laboratory
Health departments are advised to contact hospitals and laboratories in their jurisdictions to determine whether the shortage will affect them. Health departments are also encouraged to educate others on the supply shortage, optimal use of blood cultures, and mechanisms for reporting supply chain shortages or interruptions to the Food and Drug Administration (FDA), as well as to help with communication between laboratories and facilities willing to assist others in need.
To further assist affected providers, the CDC, in collaboration with the Infectious Diseases Society of America, hosted a webinar with speakers from Johns Hopkins University, Massachusetts General Hospital, and Vanderbilt University, who shared what their institutions are doing to cope with the shortage and protect patients.
Why It Happened
In June, Becton Dickinson warned its customers that they may experience “intermittent delays” in the supply of some BACTEC blood culture media over the coming months because of reduced availability of plastic bottles from its supplier.
In a July 22 update, the company said the supplier issues were “more complex” than originally communicated and it is taking steps to “resolve this challenge as quickly as possible.”
In July, the FDA published a letter to healthcare providers acknowledging the supply disruptions and recommended strategies to preserve the supply for patients at highest risk.
Becton Dickinson has promised an update by September to this “dynamic and evolving situation.”
A version of this article appeared on Medscape.com.
Hospitals and laboratories across the United States are grappling with a shortage of Becton Dickinson BACTEC blood culture bottles that threatens to extend at least until September.
In a health advisory, the Centers for Disease Control and Prevention (CDC) warned that the critical shortage could lead to “delays in diagnosis, misdiagnosis, or other challenges” in the management of patients with infectious diseases.
Healthcare providers, laboratories, healthcare facility administrators, and state, tribal, local, and territorial health departments affected by the shortage “should immediately begin to assess their situations and develop plans and options to mitigate the potential impact,” according to the health advisory.
What to Do
To reduce the impact of the shortage, facilities are urged to:
- Determine the type of blood culture bottles they have
- Optimize the use of blood cultures at their facility
- Take steps to prevent blood culture contamination
- Ensure that the appropriate volume of blood is collected for culture
- Assess alternate options for blood cultures
- Work with a nearby facility or send samples to another laboratory
Health departments are advised to contact hospitals and laboratories in their jurisdictions to determine whether the shortage will affect them. Health departments are also encouraged to educate others on the supply shortage, optimal use of blood cultures, and mechanisms for reporting supply chain shortages or interruptions to the Food and Drug Administration (FDA), as well as to help with communication between laboratories and facilities willing to assist others in need.
To further assist affected providers, the CDC, in collaboration with the Infectious Diseases Society of America, hosted a webinar with speakers from Johns Hopkins University, Massachusetts General Hospital, and Vanderbilt University, who shared what their institutions are doing to cope with the shortage and protect patients.
Why It Happened
In June, Becton Dickinson warned its customers that they may experience “intermittent delays” in the supply of some BACTEC blood culture media over the coming months because of reduced availability of plastic bottles from its supplier.
In a July 22 update, the company said the supplier issues were “more complex” than originally communicated and it is taking steps to “resolve this challenge as quickly as possible.”
In July, the FDA published a letter to healthcare providers acknowledging the supply disruptions and recommended strategies to preserve the supply for patients at highest risk.
Becton Dickinson has promised an update by September to this “dynamic and evolving situation.”
A version of this article appeared on Medscape.com.
‘Doesn’t Fit Anything I Trained for’: Committee Examines Treatment for Chronic Illness After Lyme Disease
WASHINGTON — Advancing treatment for what has been variably called chronic Lyme and posttreatment Lyme disease (PTLD) is under the eyes of a National Academies of Science, Engineering, and Medicine (NASEM) committee of experts for the first time — a year after the NASEM shone a spotlight on the need to accelerate research on chronic illnesses that follow known or suspected infections.
The committee will not make recommendations on specific approaches to diagnosis and treatment when it issues a report in early 2025 but will instead present “consensus findings” on treatment for chronic illness associated with Lyme disease, including recommendations for advancing treatment.
It’s an area void of the US Food and Drug Administration–approved therapies, void of any consensus on the off-label use of medications, and without any current standard of care or proven mechanisms and pathophysiology, said John Aucott, MD, director of the Johns Hopkins Medicine Lyme Disease Clinical Research Center, Baltimore, one of the invited speakers at a public meeting held by the NASEM in Washington, DC.
“The best way to look at this illness is not from the silos of infectious disease or the silos of rheumatology; you have to look across disciplines,” Dr. Aucott, also associate professor of medicine in the Division of Rheumatology, told the committee. “The story doesn’t fit anything I trained for in my infectious disease fellowship. Even today, I’d posit that PTLD is like an island — it’s still not connected to a lot of the mainstream of medicine.”
Rhisa Parera, who wrote and directed a 2021 documentary, Your Labs Are Normal, was one of several invited speakers who amplified the patient voice. Starting around age 7, she had pain in her knees, spine, and hips and vivid nightmares. In high school, she developed gastrointestinal issues, and in college, she developed debilitating neurologic symptoms.
Depression was her eventual diagnosis after having seen “every specialist in the book,” she said. At age 29, she received a positive western blot test and a Lyme disease diagnosis, at which point “I was prescribed 4 weeks of doxycycline and left in the dark,” the 34-year-old Black patient told the committee. Her health improved only after she began working with an “LLMD,” or Lyme-literate medical doctor (a term used in the patient community), while she lived with her mother and did not work, she said.
“I don’t share my Lyme disease history with other doctors. It’s pointless when you have those who will laugh at you, say you’re fine if you were treated, or just deny the disease completely,” Ms. Parera said. “We need this to be taught in medical school. It’s a literal emergency.”
Incidence and Potential Mechanisms
Limited research has suggested that 10%-20% of patients with Lyme disease develop persistent symptoms after standard antibiotic treatment advised by the Infectious Diseases Society of America (IDSA), Dr. Aucott said. (On its web page on chronic symptoms, the Centers for Disease Control and Prevention presents a more conservative range of 5%-10%.)
His own prospective cohort study at Johns Hopkins, published in 2022, found that 13.7% of 234 patients with prior Lyme disease met symptom and functional impact criteria for PTLD, compared with 4.1% of 49 participants without a history of Lyme disease — a statistically significant difference that he said should “put to rest” the question of “is it real?”
PTLD is the research case definition proposed by the IDSA in 2006; it requires that patients have prior documented Lyme disease, no other specific comorbidities, and specific symptoms (fatigue, widespread musculoskeletal pain, and/or cognitive difficulties) causing significant functional impact at least 6 months from their initial diagnosis and treatment.
In the real world, however, where diagnostics for acute Lyme disease are often inaccurate, erythema migrans is often absent, and the symptomatology of Lyme IACI is variable (and where there is no approved laboratory test or objective biomarker for diagnosing Lyme IACI), PTLD represents only a subset of a broader, heterogeneous population with persistent symptoms.
The term “Lyme IACI,” pronounced “Lyme eye-ACK-ee” at the meeting, builds on conversations at the 2023 NASEM workshop on infection-associated chronic illnesses and “encompasses a variety of terms that are used,” including PTLD, PTLD syndrome, persistent Lyme disease, and chronic Lyme disease, according to committee documents. Symptoms are distinct from the known complications of Lyme disease, such as arthritis or carditis.
The findings from Dr. Aucott’s SLICE cohort likely represent “the best outcome,” he said. They’re “probably not generalizable to a community setting where we see lots of missed diagnoses and delayed diagnoses,” as well as other tick-borne coinfections.
One of the challenges in designing future trials, in fact, relates to enrollment criteria and whether to use strict inclusion and exclusion criteria associated with the IDSA definition or take a broader approach to trial enrollment, he and others said. “You want to enroll patients for whom there’s no controversy that they’ve had Lyme infection ... for a study people believe in,” Dr. Aucott said during a discussion period, noting that it’s typical to screen over 100 patients to find one enrollee. “But it’s a tension we’re having.”
Timothy Sellati, PhD, chief scientific officer of the Global Lyme Alliance, urged change. “It’s really important to try to figure out how to alter our thinking on identifying and diagnosing chronic Lyme patients because they need to be recruited into clinical trials,” he said during his presentation.
“We think the best way to do this is to [develop and] employ composite diagnostic testing” that looks at unique Borrelia signatures (eg, protein, DNA, RNA, or metabolites), genetic and/or epigenetic signatures, inflammation signatures, T-cell-independent antibody signatures, and other elements, Dr. Sellati said.
Researchers designing treatment trials also face unknowns, Dr. Aucott and others said, about the role of potential mechanisms of Lyme IACI, from persistent Borrelia burgdorferi (or Borrelia mayonii) infection or the persistence of bacterial remnants (eg, nucleic acids or peptidoglycans) to infection-triggered pathology such as persistent immune dysregulation, chronic inflammation, autoimmunity, microbiome alterations, and dysautonomia and other neural network alterations.
The NASEM’s spotlight on Lyme IACI follows its long COVID-driven push last year to advance a common research agenda in infection-associated chronic illnesses. Investigators see common symptoms and potential shared mechanisms between long COVID, Lyme IACI, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), and other complex chronic illnesses following infections.
At the Lyme IACI meeting, invited speakers described parts of the research landscape. Avindra Nath, MD, of the National Institute of Neurological Disorders and Stroke, for instance, described a recently published deep phenotyping study of 17 patients with ME/CFS that found decreased central catecholamine synthesis, circuit dysfunction of integrative brain regions, and immune profiling differences (eg, defects in B-cell maturation or T-cell exhaustion), compared with matched controls, that suggest the persistence of microbial antigens.
And John Leong, MD, PhD, of Tufts University, Boston, described his lab’s focus on understanding the microbe-host interactions that enable bloodstream dissemination and tissue invasion of B burgdorferi to take hold, increasing the risk for persistent symptoms. Other research at Tufts, he noted during a discussion period, has demonstrated the persistence of B burgdorferi to antibiotics in microtiter dishes. “Those organisms that survive are really difficult to eradicate in vitro,” Dr. Leong said.
Other physician investigators described research on nociplastic pain — a category of pain that can be triggered by infections, causing both amplified sensory processing and augmented central nervous system pain — and on whether reactivation of the Epstein-Barr virus could potentiate autoimmunity in the context of Borrelia infection.
Researchers are ready to test therapies while pathophysiology is unraveled — provided there is funding, Dr. Aucott said. The Clinical Trials Network for Lyme and Other Tick-Borne Diseases, coordinated by Brian Fallon, MD, of Columbia University, New York City, and funded several years ago by the Steven & Alexandra Cohen Foundation, has a slate of small pilot studies underway or being planned that address potential mechanisms (eg, studies of pulse intravenous ceftriaxone, tetracycline, transauricular vagus nerve stimulation, and mast cell modulation). And should full multisite trials be designed and funded, the network is ready with an infrastructure.
Need for Patient-Centered Outcomes
Persistent symptomatology is on the NIH’s radar screen. Efforts to understand causes were part of a strategic tick-borne disease research plan developed by the NIH in 2019. And in 2023, the National Institute of Allergy and Infectious Diseases (NIAID) funded seven projects addressing persistent symptoms that will run through 2028, C. Benjamin Beard, PhD, deputy division director of the CDC’s Division of Vector-Borne Disease, said at the NASEM committee meeting.
Patient advocates maintained that too much emphasis is placed on tick biology and pathophysiology. When Wendy Adams, research grant director and advisory board member of the Bay Area Lyme Foundation, and a colleague analyzed NIAID tick-borne disease funding from 2013 to 2021, they found that 75% of the funding went toward basic research, 15% to translational research, and “only 3% went to clinical research,” Ms. Adams told the committee.
Only 3% of the basic research budget was spent on coinfections, she said, and only 1% was spent on neurologic disease associated with tick-borne infections, both of which are survey-defined patient priorities. Moreover, “12% of the overall NIAID [tick-borne diseases] budget was spent on tick biology,” she said.
Research needs to involve community physicians who are utilizing the guidelines and approaches of the International Lyme and Associated Diseases Society to treat most patients with Lyme IACI, Ms. Adams said. “They have data to be mined,” she said, as does LymeDisease.org, which maintains a patient registry, MyLymeData, with over 18,000 patients. The organization has published two treatment studies, including one on antibiotic treatment response.
Lorraine Johnson, JD, MBA, CEO of LymeDisease.org and principal investigator of MyLymeData, stressed the importance of using patient-centered outcomes that incorporate minimal clinically important differences (MCIDs). “A change in the SF-36 score [without consideration of MCIDs] is not inherently important or meaningful to patients,” she said, referring to the SF-36 survey of health-related quality of life.
“This may seem like an esoteric issue, but two of the four clinical trials done [on retreatment of] persistent Lyme disease used the SF-36 as their outcome measure, and those studies, led by [Mark] Klempner, concluded that retreatment was not effective,” Ms. Johnson said. “Patients have been and continue to be harmed by [this research] because they’re told by physicians that antibiotics don’t work.”
A 2012 biostatistical review of these four RCTs — trials that helped inform the 2006 IDSA treatment guidelines — concluded that the Klempner studies “set the bar for treatment success too high,” Ms. Johnson said. Three of the four trials were likely underpowered to detect clinically meaningful treatment effects, the review also found.
The NASEM committee will hold additional public meetings and review a wide range of literature through this year. The formation of the committee was recommended by the US Department of Health and Human Services Tick-Borne Disease Working Group that was established by Congress in 2016 and concluded its work in 2022. The committee’s work is funded by the Cohen Foundation.
A version of this article appeared on Medscape.com.
WASHINGTON — Advancing treatment for what has been variably called chronic Lyme and posttreatment Lyme disease (PTLD) is under the eyes of a National Academies of Science, Engineering, and Medicine (NASEM) committee of experts for the first time — a year after the NASEM shone a spotlight on the need to accelerate research on chronic illnesses that follow known or suspected infections.
The committee will not make recommendations on specific approaches to diagnosis and treatment when it issues a report in early 2025 but will instead present “consensus findings” on treatment for chronic illness associated with Lyme disease, including recommendations for advancing treatment.
It’s an area void of the US Food and Drug Administration–approved therapies, void of any consensus on the off-label use of medications, and without any current standard of care or proven mechanisms and pathophysiology, said John Aucott, MD, director of the Johns Hopkins Medicine Lyme Disease Clinical Research Center, Baltimore, one of the invited speakers at a public meeting held by the NASEM in Washington, DC.
“The best way to look at this illness is not from the silos of infectious disease or the silos of rheumatology; you have to look across disciplines,” Dr. Aucott, also associate professor of medicine in the Division of Rheumatology, told the committee. “The story doesn’t fit anything I trained for in my infectious disease fellowship. Even today, I’d posit that PTLD is like an island — it’s still not connected to a lot of the mainstream of medicine.”
Rhisa Parera, who wrote and directed a 2021 documentary, Your Labs Are Normal, was one of several invited speakers who amplified the patient voice. Starting around age 7, she had pain in her knees, spine, and hips and vivid nightmares. In high school, she developed gastrointestinal issues, and in college, she developed debilitating neurologic symptoms.
Depression was her eventual diagnosis after having seen “every specialist in the book,” she said. At age 29, she received a positive western blot test and a Lyme disease diagnosis, at which point “I was prescribed 4 weeks of doxycycline and left in the dark,” the 34-year-old Black patient told the committee. Her health improved only after she began working with an “LLMD,” or Lyme-literate medical doctor (a term used in the patient community), while she lived with her mother and did not work, she said.
“I don’t share my Lyme disease history with other doctors. It’s pointless when you have those who will laugh at you, say you’re fine if you were treated, or just deny the disease completely,” Ms. Parera said. “We need this to be taught in medical school. It’s a literal emergency.”
Incidence and Potential Mechanisms
Limited research has suggested that 10%-20% of patients with Lyme disease develop persistent symptoms after standard antibiotic treatment advised by the Infectious Diseases Society of America (IDSA), Dr. Aucott said. (On its web page on chronic symptoms, the Centers for Disease Control and Prevention presents a more conservative range of 5%-10%.)
His own prospective cohort study at Johns Hopkins, published in 2022, found that 13.7% of 234 patients with prior Lyme disease met symptom and functional impact criteria for PTLD, compared with 4.1% of 49 participants without a history of Lyme disease — a statistically significant difference that he said should “put to rest” the question of “is it real?”
PTLD is the research case definition proposed by the IDSA in 2006; it requires that patients have prior documented Lyme disease, no other specific comorbidities, and specific symptoms (fatigue, widespread musculoskeletal pain, and/or cognitive difficulties) causing significant functional impact at least 6 months from their initial diagnosis and treatment.
In the real world, however, where diagnostics for acute Lyme disease are often inaccurate, erythema migrans is often absent, and the symptomatology of Lyme IACI is variable (and where there is no approved laboratory test or objective biomarker for diagnosing Lyme IACI), PTLD represents only a subset of a broader, heterogeneous population with persistent symptoms.
The term “Lyme IACI,” pronounced “Lyme eye-ACK-ee” at the meeting, builds on conversations at the 2023 NASEM workshop on infection-associated chronic illnesses and “encompasses a variety of terms that are used,” including PTLD, PTLD syndrome, persistent Lyme disease, and chronic Lyme disease, according to committee documents. Symptoms are distinct from the known complications of Lyme disease, such as arthritis or carditis.
The findings from Dr. Aucott’s SLICE cohort likely represent “the best outcome,” he said. They’re “probably not generalizable to a community setting where we see lots of missed diagnoses and delayed diagnoses,” as well as other tick-borne coinfections.
One of the challenges in designing future trials, in fact, relates to enrollment criteria and whether to use strict inclusion and exclusion criteria associated with the IDSA definition or take a broader approach to trial enrollment, he and others said. “You want to enroll patients for whom there’s no controversy that they’ve had Lyme infection ... for a study people believe in,” Dr. Aucott said during a discussion period, noting that it’s typical to screen over 100 patients to find one enrollee. “But it’s a tension we’re having.”
Timothy Sellati, PhD, chief scientific officer of the Global Lyme Alliance, urged change. “It’s really important to try to figure out how to alter our thinking on identifying and diagnosing chronic Lyme patients because they need to be recruited into clinical trials,” he said during his presentation.
“We think the best way to do this is to [develop and] employ composite diagnostic testing” that looks at unique Borrelia signatures (eg, protein, DNA, RNA, or metabolites), genetic and/or epigenetic signatures, inflammation signatures, T-cell-independent antibody signatures, and other elements, Dr. Sellati said.
Researchers designing treatment trials also face unknowns, Dr. Aucott and others said, about the role of potential mechanisms of Lyme IACI, from persistent Borrelia burgdorferi (or Borrelia mayonii) infection or the persistence of bacterial remnants (eg, nucleic acids or peptidoglycans) to infection-triggered pathology such as persistent immune dysregulation, chronic inflammation, autoimmunity, microbiome alterations, and dysautonomia and other neural network alterations.
The NASEM’s spotlight on Lyme IACI follows its long COVID-driven push last year to advance a common research agenda in infection-associated chronic illnesses. Investigators see common symptoms and potential shared mechanisms between long COVID, Lyme IACI, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), and other complex chronic illnesses following infections.
At the Lyme IACI meeting, invited speakers described parts of the research landscape. Avindra Nath, MD, of the National Institute of Neurological Disorders and Stroke, for instance, described a recently published deep phenotyping study of 17 patients with ME/CFS that found decreased central catecholamine synthesis, circuit dysfunction of integrative brain regions, and immune profiling differences (eg, defects in B-cell maturation or T-cell exhaustion), compared with matched controls, that suggest the persistence of microbial antigens.
And John Leong, MD, PhD, of Tufts University, Boston, described his lab’s focus on understanding the microbe-host interactions that enable bloodstream dissemination and tissue invasion of B burgdorferi to take hold, increasing the risk for persistent symptoms. Other research at Tufts, he noted during a discussion period, has demonstrated the persistence of B burgdorferi to antibiotics in microtiter dishes. “Those organisms that survive are really difficult to eradicate in vitro,” Dr. Leong said.
Other physician investigators described research on nociplastic pain — a category of pain that can be triggered by infections, causing both amplified sensory processing and augmented central nervous system pain — and on whether reactivation of the Epstein-Barr virus could potentiate autoimmunity in the context of Borrelia infection.
Researchers are ready to test therapies while pathophysiology is unraveled — provided there is funding, Dr. Aucott said. The Clinical Trials Network for Lyme and Other Tick-Borne Diseases, coordinated by Brian Fallon, MD, of Columbia University, New York City, and funded several years ago by the Steven & Alexandra Cohen Foundation, has a slate of small pilot studies underway or being planned that address potential mechanisms (eg, studies of pulse intravenous ceftriaxone, tetracycline, transauricular vagus nerve stimulation, and mast cell modulation). And should full multisite trials be designed and funded, the network is ready with an infrastructure.
Need for Patient-Centered Outcomes
Persistent symptomatology is on the NIH’s radar screen. Efforts to understand causes were part of a strategic tick-borne disease research plan developed by the NIH in 2019. And in 2023, the National Institute of Allergy and Infectious Diseases (NIAID) funded seven projects addressing persistent symptoms that will run through 2028, C. Benjamin Beard, PhD, deputy division director of the CDC’s Division of Vector-Borne Disease, said at the NASEM committee meeting.
Patient advocates maintained that too much emphasis is placed on tick biology and pathophysiology. When Wendy Adams, research grant director and advisory board member of the Bay Area Lyme Foundation, and a colleague analyzed NIAID tick-borne disease funding from 2013 to 2021, they found that 75% of the funding went toward basic research, 15% to translational research, and “only 3% went to clinical research,” Ms. Adams told the committee.
Only 3% of the basic research budget was spent on coinfections, she said, and only 1% was spent on neurologic disease associated with tick-borne infections, both of which are survey-defined patient priorities. Moreover, “12% of the overall NIAID [tick-borne diseases] budget was spent on tick biology,” she said.
Research needs to involve community physicians who are utilizing the guidelines and approaches of the International Lyme and Associated Diseases Society to treat most patients with Lyme IACI, Ms. Adams said. “They have data to be mined,” she said, as does LymeDisease.org, which maintains a patient registry, MyLymeData, with over 18,000 patients. The organization has published two treatment studies, including one on antibiotic treatment response.
Lorraine Johnson, JD, MBA, CEO of LymeDisease.org and principal investigator of MyLymeData, stressed the importance of using patient-centered outcomes that incorporate minimal clinically important differences (MCIDs). “A change in the SF-36 score [without consideration of MCIDs] is not inherently important or meaningful to patients,” she said, referring to the SF-36 survey of health-related quality of life.
“This may seem like an esoteric issue, but two of the four clinical trials done [on retreatment of] persistent Lyme disease used the SF-36 as their outcome measure, and those studies, led by [Mark] Klempner, concluded that retreatment was not effective,” Ms. Johnson said. “Patients have been and continue to be harmed by [this research] because they’re told by physicians that antibiotics don’t work.”
A 2012 biostatistical review of these four RCTs — trials that helped inform the 2006 IDSA treatment guidelines — concluded that the Klempner studies “set the bar for treatment success too high,” Ms. Johnson said. Three of the four trials were likely underpowered to detect clinically meaningful treatment effects, the review also found.
The NASEM committee will hold additional public meetings and review a wide range of literature through this year. The formation of the committee was recommended by the US Department of Health and Human Services Tick-Borne Disease Working Group that was established by Congress in 2016 and concluded its work in 2022. The committee’s work is funded by the Cohen Foundation.
A version of this article appeared on Medscape.com.
WASHINGTON — Advancing treatment for what has been variably called chronic Lyme and posttreatment Lyme disease (PTLD) is under the eyes of a National Academies of Science, Engineering, and Medicine (NASEM) committee of experts for the first time — a year after the NASEM shone a spotlight on the need to accelerate research on chronic illnesses that follow known or suspected infections.
The committee will not make recommendations on specific approaches to diagnosis and treatment when it issues a report in early 2025 but will instead present “consensus findings” on treatment for chronic illness associated with Lyme disease, including recommendations for advancing treatment.
It’s an area void of the US Food and Drug Administration–approved therapies, void of any consensus on the off-label use of medications, and without any current standard of care or proven mechanisms and pathophysiology, said John Aucott, MD, director of the Johns Hopkins Medicine Lyme Disease Clinical Research Center, Baltimore, one of the invited speakers at a public meeting held by the NASEM in Washington, DC.
“The best way to look at this illness is not from the silos of infectious disease or the silos of rheumatology; you have to look across disciplines,” Dr. Aucott, also associate professor of medicine in the Division of Rheumatology, told the committee. “The story doesn’t fit anything I trained for in my infectious disease fellowship. Even today, I’d posit that PTLD is like an island — it’s still not connected to a lot of the mainstream of medicine.”
Rhisa Parera, who wrote and directed a 2021 documentary, Your Labs Are Normal, was one of several invited speakers who amplified the patient voice. Starting around age 7, she had pain in her knees, spine, and hips and vivid nightmares. In high school, she developed gastrointestinal issues, and in college, she developed debilitating neurologic symptoms.
Depression was her eventual diagnosis after having seen “every specialist in the book,” she said. At age 29, she received a positive western blot test and a Lyme disease diagnosis, at which point “I was prescribed 4 weeks of doxycycline and left in the dark,” the 34-year-old Black patient told the committee. Her health improved only after she began working with an “LLMD,” or Lyme-literate medical doctor (a term used in the patient community), while she lived with her mother and did not work, she said.
“I don’t share my Lyme disease history with other doctors. It’s pointless when you have those who will laugh at you, say you’re fine if you were treated, or just deny the disease completely,” Ms. Parera said. “We need this to be taught in medical school. It’s a literal emergency.”
Incidence and Potential Mechanisms
Limited research has suggested that 10%-20% of patients with Lyme disease develop persistent symptoms after standard antibiotic treatment advised by the Infectious Diseases Society of America (IDSA), Dr. Aucott said. (On its web page on chronic symptoms, the Centers for Disease Control and Prevention presents a more conservative range of 5%-10%.)
His own prospective cohort study at Johns Hopkins, published in 2022, found that 13.7% of 234 patients with prior Lyme disease met symptom and functional impact criteria for PTLD, compared with 4.1% of 49 participants without a history of Lyme disease — a statistically significant difference that he said should “put to rest” the question of “is it real?”
PTLD is the research case definition proposed by the IDSA in 2006; it requires that patients have prior documented Lyme disease, no other specific comorbidities, and specific symptoms (fatigue, widespread musculoskeletal pain, and/or cognitive difficulties) causing significant functional impact at least 6 months from their initial diagnosis and treatment.
In the real world, however, where diagnostics for acute Lyme disease are often inaccurate, erythema migrans is often absent, and the symptomatology of Lyme IACI is variable (and where there is no approved laboratory test or objective biomarker for diagnosing Lyme IACI), PTLD represents only a subset of a broader, heterogeneous population with persistent symptoms.
The term “Lyme IACI,” pronounced “Lyme eye-ACK-ee” at the meeting, builds on conversations at the 2023 NASEM workshop on infection-associated chronic illnesses and “encompasses a variety of terms that are used,” including PTLD, PTLD syndrome, persistent Lyme disease, and chronic Lyme disease, according to committee documents. Symptoms are distinct from the known complications of Lyme disease, such as arthritis or carditis.
The findings from Dr. Aucott’s SLICE cohort likely represent “the best outcome,” he said. They’re “probably not generalizable to a community setting where we see lots of missed diagnoses and delayed diagnoses,” as well as other tick-borne coinfections.
One of the challenges in designing future trials, in fact, relates to enrollment criteria and whether to use strict inclusion and exclusion criteria associated with the IDSA definition or take a broader approach to trial enrollment, he and others said. “You want to enroll patients for whom there’s no controversy that they’ve had Lyme infection ... for a study people believe in,” Dr. Aucott said during a discussion period, noting that it’s typical to screen over 100 patients to find one enrollee. “But it’s a tension we’re having.”
Timothy Sellati, PhD, chief scientific officer of the Global Lyme Alliance, urged change. “It’s really important to try to figure out how to alter our thinking on identifying and diagnosing chronic Lyme patients because they need to be recruited into clinical trials,” he said during his presentation.
“We think the best way to do this is to [develop and] employ composite diagnostic testing” that looks at unique Borrelia signatures (eg, protein, DNA, RNA, or metabolites), genetic and/or epigenetic signatures, inflammation signatures, T-cell-independent antibody signatures, and other elements, Dr. Sellati said.
Researchers designing treatment trials also face unknowns, Dr. Aucott and others said, about the role of potential mechanisms of Lyme IACI, from persistent Borrelia burgdorferi (or Borrelia mayonii) infection or the persistence of bacterial remnants (eg, nucleic acids or peptidoglycans) to infection-triggered pathology such as persistent immune dysregulation, chronic inflammation, autoimmunity, microbiome alterations, and dysautonomia and other neural network alterations.
The NASEM’s spotlight on Lyme IACI follows its long COVID-driven push last year to advance a common research agenda in infection-associated chronic illnesses. Investigators see common symptoms and potential shared mechanisms between long COVID, Lyme IACI, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), and other complex chronic illnesses following infections.
At the Lyme IACI meeting, invited speakers described parts of the research landscape. Avindra Nath, MD, of the National Institute of Neurological Disorders and Stroke, for instance, described a recently published deep phenotyping study of 17 patients with ME/CFS that found decreased central catecholamine synthesis, circuit dysfunction of integrative brain regions, and immune profiling differences (eg, defects in B-cell maturation or T-cell exhaustion), compared with matched controls, that suggest the persistence of microbial antigens.
And John Leong, MD, PhD, of Tufts University, Boston, described his lab’s focus on understanding the microbe-host interactions that enable bloodstream dissemination and tissue invasion of B burgdorferi to take hold, increasing the risk for persistent symptoms. Other research at Tufts, he noted during a discussion period, has demonstrated the persistence of B burgdorferi to antibiotics in microtiter dishes. “Those organisms that survive are really difficult to eradicate in vitro,” Dr. Leong said.
Other physician investigators described research on nociplastic pain — a category of pain that can be triggered by infections, causing both amplified sensory processing and augmented central nervous system pain — and on whether reactivation of the Epstein-Barr virus could potentiate autoimmunity in the context of Borrelia infection.
Researchers are ready to test therapies while pathophysiology is unraveled — provided there is funding, Dr. Aucott said. The Clinical Trials Network for Lyme and Other Tick-Borne Diseases, coordinated by Brian Fallon, MD, of Columbia University, New York City, and funded several years ago by the Steven & Alexandra Cohen Foundation, has a slate of small pilot studies underway or being planned that address potential mechanisms (eg, studies of pulse intravenous ceftriaxone, tetracycline, transauricular vagus nerve stimulation, and mast cell modulation). And should full multisite trials be designed and funded, the network is ready with an infrastructure.
Need for Patient-Centered Outcomes
Persistent symptomatology is on the NIH’s radar screen. Efforts to understand causes were part of a strategic tick-borne disease research plan developed by the NIH in 2019. And in 2023, the National Institute of Allergy and Infectious Diseases (NIAID) funded seven projects addressing persistent symptoms that will run through 2028, C. Benjamin Beard, PhD, deputy division director of the CDC’s Division of Vector-Borne Disease, said at the NASEM committee meeting.
Patient advocates maintained that too much emphasis is placed on tick biology and pathophysiology. When Wendy Adams, research grant director and advisory board member of the Bay Area Lyme Foundation, and a colleague analyzed NIAID tick-borne disease funding from 2013 to 2021, they found that 75% of the funding went toward basic research, 15% to translational research, and “only 3% went to clinical research,” Ms. Adams told the committee.
Only 3% of the basic research budget was spent on coinfections, she said, and only 1% was spent on neurologic disease associated with tick-borne infections, both of which are survey-defined patient priorities. Moreover, “12% of the overall NIAID [tick-borne diseases] budget was spent on tick biology,” she said.
Research needs to involve community physicians who are utilizing the guidelines and approaches of the International Lyme and Associated Diseases Society to treat most patients with Lyme IACI, Ms. Adams said. “They have data to be mined,” she said, as does LymeDisease.org, which maintains a patient registry, MyLymeData, with over 18,000 patients. The organization has published two treatment studies, including one on antibiotic treatment response.
Lorraine Johnson, JD, MBA, CEO of LymeDisease.org and principal investigator of MyLymeData, stressed the importance of using patient-centered outcomes that incorporate minimal clinically important differences (MCIDs). “A change in the SF-36 score [without consideration of MCIDs] is not inherently important or meaningful to patients,” she said, referring to the SF-36 survey of health-related quality of life.
“This may seem like an esoteric issue, but two of the four clinical trials done [on retreatment of] persistent Lyme disease used the SF-36 as their outcome measure, and those studies, led by [Mark] Klempner, concluded that retreatment was not effective,” Ms. Johnson said. “Patients have been and continue to be harmed by [this research] because they’re told by physicians that antibiotics don’t work.”
A 2012 biostatistical review of these four RCTs — trials that helped inform the 2006 IDSA treatment guidelines — concluded that the Klempner studies “set the bar for treatment success too high,” Ms. Johnson said. Three of the four trials were likely underpowered to detect clinically meaningful treatment effects, the review also found.
The NASEM committee will hold additional public meetings and review a wide range of literature through this year. The formation of the committee was recommended by the US Department of Health and Human Services Tick-Borne Disease Working Group that was established by Congress in 2016 and concluded its work in 2022. The committee’s work is funded by the Cohen Foundation.
A version of this article appeared on Medscape.com.
Twice-Yearly PrEP Gives ‘Huge’ 100% Protection
Twice-yearly injections are 100% effective in preventing new infections, according to the final results from the PURPOSE 1 trial of lenacapavir.
For weeks, the HIV community has been talking about this highly anticipated clinical trial and whether the strong — and to many, surprising — interim results would hold at final presentation at the International AIDS Conference 2024 in Munich, Germany.
Presenting the results, Linda-Gail Bekker, MD, director of the Desmond Tutu HIV Center at the University of Cape Town, South Africa, reported zero new infections in those who got the shots in the study of about 5000 young women. In the group given daily oral preexposure prophylaxis (PrEP), roughly 2% contracted HIV from infected partners.
“A twice-yearly PrEP choice could overcome some of the adherence and persistence challenges and contribute critically to our quest to reduce HIV infection in women around the world,” Dr. Bekker said about the results, which were published simultaneously in The New England Journal of Medicine.
PURPOSE 1 confirmed that lenacapavir is a “breakthrough” for HIV prevention, said International AIDS Society president Sharon Lewin, PhD, MBBS. It has “huge public health potential,” said Dr. Lewin, the AIDS 2024 conference cochair and director of the Peter Doherty Institute for Infection and Immunity at the University of Melbourne in Australia.
Lenacapavir is a novel, first-in-class multistage HIV-1 capsid inhibitor with a long half-life, which enables the twice-yearly dosing.
PURPOSE 1 enrolled women aged 15-25 years who were at risk for HIV in South Africa and Uganda, with a primary endpoint of HIV infection. Because of the previously announced interim results, which showed the injection was preventing infections, study sponsor Gilead Sciences discontinued the randomized phase of the trial and shifted to an open-label design for lenacapavir.
“One hundred percent efficacy is more that we could ever have hoped for a potential prevention efficacy,” said Christoph Spinner, MD, MBA, an infectious disease specialist at the University Hospital of the Technical University of Munich and AIDS 2024 conference cochair.
Dr. Spinner added that while this is the first study of lenacapavir for PrEP, it’s also the first to explore outcomes of emtricitabine-tenofovir in cisgender women.
Strong Adherence Rates
The twice-yearly injection demonstrated adherence rates above 90% in the trial for both the 6- and 12-month injection intervals.
“Adherence was 91.5% at week 26 and 92.8% at week 52,” Dr. Bekker reported.
The trial compared three PrEP options including the lenacapavir injection to once-daily oral emtricitabine 200 mg and tenofovir-alafenamide 25 mg (F/TAF) and once-daily emtricitabine 200 mg and tenofovir–disoproxil fumarate 300 mg (F/TDF).
“Most participants in both the F/TAF and F/TDF groups had low adherence, and this declined over time,” Dr. Bekker reported. At 52 weeks, the vast majority of patients on both oral therapies had low adherence with dosing, defined at less than two doses a week.
Dr. Bekker called the adherence to the oral agents in this trial “disappointing.”
Findings from the trial underscore the challenges of adherence to a daily oral medication, Rochelle Walensky, MD, and Lindsey Baden, MD, from the Harvard Kennedy School of Government and Harvard Business School in Cambridge, Massachusetts, wrote in an editorial accompanying the published results.
With almost 92% attendance for the twice-yearly lenacapavir injections, the “well-done,” large, randomized, controlled trial “exemplifies not only that women can dependably adhere to this administration schedule, but also that levels of an HIV-1 capsid inhibitor can remain high enough over a period of 6 months to reliably prevent infection,” they added.
Another key focus of the presentation was adverse events. The rate of adverse events grade 3 or more in the lenacapavir arm was 4.1%, Bekker said, which is slightly lower than the rates in the oral arms. The rates of serious adverse events were 2.8% for lenacapavir, 4% for F/TAF and 3.3% for F/TDF.
Injection Site Reactions
Injection site reactions occurred in 68% of the lenacapavir group, including 63% with subcutaneous nodules.
The injection can form “a drug depot which may be palpable as a nodule,” Dr. Bekker said. In the placebo group, 34% of patients had injection-site reactions and 16% had nodules. Nearly all injection-site reactions were grade 1 or 2, she said. “Higher grade injection-site reactions were rare and not serious and occurred in a similar percentage in lenacapavir and placebo,” she said.
Overall, more than 25,000 injections of lenacapavir have been given, Dr. Bekker said, and four patients discontinued treatment because of injection-site reactions. “Reporting of injection-site reactions, including nodules, decreased with subsequent doses,” she said.
Contraception was not a requirement for enrollment in the study, Dr. Bekker pointed out, and pregnancy outcomes across the treatment arms were similar to the general population.
First in a Series of Trials
This is the first in a series of PURPOSE trials, Bekker reported. The phase 3 PURPOSE 2 trial, enrolling 3000 gay men, transgender women, transgender men and gender nonbinary people who have sex with male partners, is the second pivotal trial now underway.
Three other smaller trials are in the clinic in the United States and Europe.
PURPOSE 1 participants will continue to access lenacapavir until the product is available in South Africa and Uganda, Dr. Bekker said. Trial sponsor Gilead Sciences is also developing a direct licensing program to expedite generic access to the drug in high-incidence, resource-limited countries, she said.
Dr. Walensky and Dr. Baden report that lenacapavir currently costs about $43,000 annually in the United States. “But the results of the PURPOSE 1 trial have now created a moral imperative to make lenacapavir broadly accessible and affordable as PrEP” to people who were enrolled, as well as all those who are similarly eligible and could benefit.
So now we have a PrEP product with high efficacy, they added. “That is great news for science but not (yet) great for women.”
Given the high pregnancy rate among participants in the PURPOSE 1 trial, Dr. Walensky and Dr. Baden point out the assessment of lenacapavir safety is a priority. They are also interested in learning more about drug resistance with this new option.
“I f approved and delivered — rapidly, affordably, and equitably — to those who need or want it, this long-acting tool could help accelerate global progress in HIV prevention,” Dr. Lewin said.
Now, she added, “we eagerly await results from PURPOSE 2.”
A version of this article first appeared on Medscape.com.
Twice-yearly injections are 100% effective in preventing new infections, according to the final results from the PURPOSE 1 trial of lenacapavir.
For weeks, the HIV community has been talking about this highly anticipated clinical trial and whether the strong — and to many, surprising — interim results would hold at final presentation at the International AIDS Conference 2024 in Munich, Germany.
Presenting the results, Linda-Gail Bekker, MD, director of the Desmond Tutu HIV Center at the University of Cape Town, South Africa, reported zero new infections in those who got the shots in the study of about 5000 young women. In the group given daily oral preexposure prophylaxis (PrEP), roughly 2% contracted HIV from infected partners.
“A twice-yearly PrEP choice could overcome some of the adherence and persistence challenges and contribute critically to our quest to reduce HIV infection in women around the world,” Dr. Bekker said about the results, which were published simultaneously in The New England Journal of Medicine.
PURPOSE 1 confirmed that lenacapavir is a “breakthrough” for HIV prevention, said International AIDS Society president Sharon Lewin, PhD, MBBS. It has “huge public health potential,” said Dr. Lewin, the AIDS 2024 conference cochair and director of the Peter Doherty Institute for Infection and Immunity at the University of Melbourne in Australia.
Lenacapavir is a novel, first-in-class multistage HIV-1 capsid inhibitor with a long half-life, which enables the twice-yearly dosing.
PURPOSE 1 enrolled women aged 15-25 years who were at risk for HIV in South Africa and Uganda, with a primary endpoint of HIV infection. Because of the previously announced interim results, which showed the injection was preventing infections, study sponsor Gilead Sciences discontinued the randomized phase of the trial and shifted to an open-label design for lenacapavir.
“One hundred percent efficacy is more that we could ever have hoped for a potential prevention efficacy,” said Christoph Spinner, MD, MBA, an infectious disease specialist at the University Hospital of the Technical University of Munich and AIDS 2024 conference cochair.
Dr. Spinner added that while this is the first study of lenacapavir for PrEP, it’s also the first to explore outcomes of emtricitabine-tenofovir in cisgender women.
Strong Adherence Rates
The twice-yearly injection demonstrated adherence rates above 90% in the trial for both the 6- and 12-month injection intervals.
“Adherence was 91.5% at week 26 and 92.8% at week 52,” Dr. Bekker reported.
The trial compared three PrEP options including the lenacapavir injection to once-daily oral emtricitabine 200 mg and tenofovir-alafenamide 25 mg (F/TAF) and once-daily emtricitabine 200 mg and tenofovir–disoproxil fumarate 300 mg (F/TDF).
“Most participants in both the F/TAF and F/TDF groups had low adherence, and this declined over time,” Dr. Bekker reported. At 52 weeks, the vast majority of patients on both oral therapies had low adherence with dosing, defined at less than two doses a week.
Dr. Bekker called the adherence to the oral agents in this trial “disappointing.”
Findings from the trial underscore the challenges of adherence to a daily oral medication, Rochelle Walensky, MD, and Lindsey Baden, MD, from the Harvard Kennedy School of Government and Harvard Business School in Cambridge, Massachusetts, wrote in an editorial accompanying the published results.
With almost 92% attendance for the twice-yearly lenacapavir injections, the “well-done,” large, randomized, controlled trial “exemplifies not only that women can dependably adhere to this administration schedule, but also that levels of an HIV-1 capsid inhibitor can remain high enough over a period of 6 months to reliably prevent infection,” they added.
Another key focus of the presentation was adverse events. The rate of adverse events grade 3 or more in the lenacapavir arm was 4.1%, Bekker said, which is slightly lower than the rates in the oral arms. The rates of serious adverse events were 2.8% for lenacapavir, 4% for F/TAF and 3.3% for F/TDF.
Injection Site Reactions
Injection site reactions occurred in 68% of the lenacapavir group, including 63% with subcutaneous nodules.
The injection can form “a drug depot which may be palpable as a nodule,” Dr. Bekker said. In the placebo group, 34% of patients had injection-site reactions and 16% had nodules. Nearly all injection-site reactions were grade 1 or 2, she said. “Higher grade injection-site reactions were rare and not serious and occurred in a similar percentage in lenacapavir and placebo,” she said.
Overall, more than 25,000 injections of lenacapavir have been given, Dr. Bekker said, and four patients discontinued treatment because of injection-site reactions. “Reporting of injection-site reactions, including nodules, decreased with subsequent doses,” she said.
Contraception was not a requirement for enrollment in the study, Dr. Bekker pointed out, and pregnancy outcomes across the treatment arms were similar to the general population.
First in a Series of Trials
This is the first in a series of PURPOSE trials, Bekker reported. The phase 3 PURPOSE 2 trial, enrolling 3000 gay men, transgender women, transgender men and gender nonbinary people who have sex with male partners, is the second pivotal trial now underway.
Three other smaller trials are in the clinic in the United States and Europe.
PURPOSE 1 participants will continue to access lenacapavir until the product is available in South Africa and Uganda, Dr. Bekker said. Trial sponsor Gilead Sciences is also developing a direct licensing program to expedite generic access to the drug in high-incidence, resource-limited countries, she said.
Dr. Walensky and Dr. Baden report that lenacapavir currently costs about $43,000 annually in the United States. “But the results of the PURPOSE 1 trial have now created a moral imperative to make lenacapavir broadly accessible and affordable as PrEP” to people who were enrolled, as well as all those who are similarly eligible and could benefit.
So now we have a PrEP product with high efficacy, they added. “That is great news for science but not (yet) great for women.”
Given the high pregnancy rate among participants in the PURPOSE 1 trial, Dr. Walensky and Dr. Baden point out the assessment of lenacapavir safety is a priority. They are also interested in learning more about drug resistance with this new option.
“I f approved and delivered — rapidly, affordably, and equitably — to those who need or want it, this long-acting tool could help accelerate global progress in HIV prevention,” Dr. Lewin said.
Now, she added, “we eagerly await results from PURPOSE 2.”
A version of this article first appeared on Medscape.com.
Twice-yearly injections are 100% effective in preventing new infections, according to the final results from the PURPOSE 1 trial of lenacapavir.
For weeks, the HIV community has been talking about this highly anticipated clinical trial and whether the strong — and to many, surprising — interim results would hold at final presentation at the International AIDS Conference 2024 in Munich, Germany.
Presenting the results, Linda-Gail Bekker, MD, director of the Desmond Tutu HIV Center at the University of Cape Town, South Africa, reported zero new infections in those who got the shots in the study of about 5000 young women. In the group given daily oral preexposure prophylaxis (PrEP), roughly 2% contracted HIV from infected partners.
“A twice-yearly PrEP choice could overcome some of the adherence and persistence challenges and contribute critically to our quest to reduce HIV infection in women around the world,” Dr. Bekker said about the results, which were published simultaneously in The New England Journal of Medicine.
PURPOSE 1 confirmed that lenacapavir is a “breakthrough” for HIV prevention, said International AIDS Society president Sharon Lewin, PhD, MBBS. It has “huge public health potential,” said Dr. Lewin, the AIDS 2024 conference cochair and director of the Peter Doherty Institute for Infection and Immunity at the University of Melbourne in Australia.
Lenacapavir is a novel, first-in-class multistage HIV-1 capsid inhibitor with a long half-life, which enables the twice-yearly dosing.
PURPOSE 1 enrolled women aged 15-25 years who were at risk for HIV in South Africa and Uganda, with a primary endpoint of HIV infection. Because of the previously announced interim results, which showed the injection was preventing infections, study sponsor Gilead Sciences discontinued the randomized phase of the trial and shifted to an open-label design for lenacapavir.
“One hundred percent efficacy is more that we could ever have hoped for a potential prevention efficacy,” said Christoph Spinner, MD, MBA, an infectious disease specialist at the University Hospital of the Technical University of Munich and AIDS 2024 conference cochair.
Dr. Spinner added that while this is the first study of lenacapavir for PrEP, it’s also the first to explore outcomes of emtricitabine-tenofovir in cisgender women.
Strong Adherence Rates
The twice-yearly injection demonstrated adherence rates above 90% in the trial for both the 6- and 12-month injection intervals.
“Adherence was 91.5% at week 26 and 92.8% at week 52,” Dr. Bekker reported.
The trial compared three PrEP options including the lenacapavir injection to once-daily oral emtricitabine 200 mg and tenofovir-alafenamide 25 mg (F/TAF) and once-daily emtricitabine 200 mg and tenofovir–disoproxil fumarate 300 mg (F/TDF).
“Most participants in both the F/TAF and F/TDF groups had low adherence, and this declined over time,” Dr. Bekker reported. At 52 weeks, the vast majority of patients on both oral therapies had low adherence with dosing, defined at less than two doses a week.
Dr. Bekker called the adherence to the oral agents in this trial “disappointing.”
Findings from the trial underscore the challenges of adherence to a daily oral medication, Rochelle Walensky, MD, and Lindsey Baden, MD, from the Harvard Kennedy School of Government and Harvard Business School in Cambridge, Massachusetts, wrote in an editorial accompanying the published results.
With almost 92% attendance for the twice-yearly lenacapavir injections, the “well-done,” large, randomized, controlled trial “exemplifies not only that women can dependably adhere to this administration schedule, but also that levels of an HIV-1 capsid inhibitor can remain high enough over a period of 6 months to reliably prevent infection,” they added.
Another key focus of the presentation was adverse events. The rate of adverse events grade 3 or more in the lenacapavir arm was 4.1%, Bekker said, which is slightly lower than the rates in the oral arms. The rates of serious adverse events were 2.8% for lenacapavir, 4% for F/TAF and 3.3% for F/TDF.
Injection Site Reactions
Injection site reactions occurred in 68% of the lenacapavir group, including 63% with subcutaneous nodules.
The injection can form “a drug depot which may be palpable as a nodule,” Dr. Bekker said. In the placebo group, 34% of patients had injection-site reactions and 16% had nodules. Nearly all injection-site reactions were grade 1 or 2, she said. “Higher grade injection-site reactions were rare and not serious and occurred in a similar percentage in lenacapavir and placebo,” she said.
Overall, more than 25,000 injections of lenacapavir have been given, Dr. Bekker said, and four patients discontinued treatment because of injection-site reactions. “Reporting of injection-site reactions, including nodules, decreased with subsequent doses,” she said.
Contraception was not a requirement for enrollment in the study, Dr. Bekker pointed out, and pregnancy outcomes across the treatment arms were similar to the general population.
First in a Series of Trials
This is the first in a series of PURPOSE trials, Bekker reported. The phase 3 PURPOSE 2 trial, enrolling 3000 gay men, transgender women, transgender men and gender nonbinary people who have sex with male partners, is the second pivotal trial now underway.
Three other smaller trials are in the clinic in the United States and Europe.
PURPOSE 1 participants will continue to access lenacapavir until the product is available in South Africa and Uganda, Dr. Bekker said. Trial sponsor Gilead Sciences is also developing a direct licensing program to expedite generic access to the drug in high-incidence, resource-limited countries, she said.
Dr. Walensky and Dr. Baden report that lenacapavir currently costs about $43,000 annually in the United States. “But the results of the PURPOSE 1 trial have now created a moral imperative to make lenacapavir broadly accessible and affordable as PrEP” to people who were enrolled, as well as all those who are similarly eligible and could benefit.
So now we have a PrEP product with high efficacy, they added. “That is great news for science but not (yet) great for women.”
Given the high pregnancy rate among participants in the PURPOSE 1 trial, Dr. Walensky and Dr. Baden point out the assessment of lenacapavir safety is a priority. They are also interested in learning more about drug resistance with this new option.
“I f approved and delivered — rapidly, affordably, and equitably — to those who need or want it, this long-acting tool could help accelerate global progress in HIV prevention,” Dr. Lewin said.
Now, she added, “we eagerly await results from PURPOSE 2.”
A version of this article first appeared on Medscape.com.
FROM AIDS 2024