User login
Helping survivors in the aftermath of suicide loss
The loss of a loved one to suicide is often experienced as “devastating.”1 While survivors of suicide loss may be able to move through the grief process without clinical support,2 the traumatic and stigmatizing nature of suicide is likely to make its aftermath more challenging to navigate than other types of loss. Sanford et al3 found that more than two-thirds of suicide loss survivors sought therapy after their loss. Further, when individuals facing these challenges present for treatment, clinicians often face challenges of their own.
Very few clinicians are trained in general grief processes,4 and even those specifically trained in grief and loss have been shown to “miss” several of the common clinical features that are unique to suicide loss.3 In my professional experience, the intensity and duration of suicide grief are often greater than they are for other losses, and many survivors of suicide loss have reported that others, including clinicians, have “pathologized” this, rather than having understood it as normative under the circumstances.
Although there is extensive literature on the aftermath of suicide for surviving loved ones, very few controlled studies have assessed interventions specifically for this population. Yet the U.S. Guidelines for Suicide Postvention5 explicitly call for improved training for those who work with suicide loss survivors, as well as research on these interventions. Jordan and McGann6 noted, “Without a full knowledge of suicide and its aftermath, it is very possible to make clinical errors which can hamper treatment.” This article summarizes what is currently known about the general experience of suicide bereavement and optimal interventions in treatment.
What makes suicide loss unique?
Suicide bereavement is distinct from other types of loss in 3 significant ways7:
- the thematic content of the grief
- the social processes surrounding the survivor
- the impact that suicide has on family systems.
Additionally, the perceived intentionality and preventability of a suicide death, as well as its stigmatized and traumatic nature, differentiate it from other types of traumatic loss.7 These elements are all likely to affect the nature, intensity, and duration of the grief.
Stigma and suicide. Stigma associated with suicide is well documented.8 Former U.S. Surgeon General David Satcher9 specifically described stigma toward suicide as one of the biggest barriers to prevention. In addition, researchers have found that the stigma associated with suicide “spills over” to the bereaved family members. Doka10,11 refers to “disenfranchised grief,” in which bereaved individuals receive the message that their grief is not legitimate, and as a result, they are likely to internalize this view. Studies have shown that individuals bereaved by suicide are also stigmatized, and are believed to be more psychologically disturbed, less likable, more blameworthy, more ashamed, and more in need of professional help than other bereaved individuals.8,12-20
These judgments often mirror suicide loss survivors’ self-punitive assessments, which then become exacerbated by and intertwined with both externally imposed and internalized stigma. Thus, it is not uncommon for survivors of suicide loss to question their own right to grieve, to report low expectations of social support, and to feel compelled to deny or hide the mode of death. To the extent that they are actively grieving, survivors of suicide loss often feel that they must do so in isolation. Thus, the perception of stigma, whether external or internalized, can have a profound effect on decisions about disclosure, requesting support, and ultimately on one’s ability to integrate the loss. Indeed, Feigelman et al21 found that stigmatization after suicide was specifically associated with ongoing grief difficulties, depression, and suicidal ideation.
Continue to: Traumatic nature of suicide
Traumatic nature of suicide. Suicide loss is also quite traumatic, and posttraumatic stress disorder (PTSD) symptoms such as shock, horror, disbelief, and intrusive/perseverative thoughts and questions, particularly in the earlier stages of grief, are common. Sanford et al3 found that the higher the level of “perceived closeness” to the deceased, the more likely that survivors of suicide loss would experience PTSD symptoms. In addition, the dramatic loss of social support following a suicide loss may itself be traumatic, which can serve to compound these difficulties. Notably, Sanford et al3 found that even for those survivors of suicide loss in treatment who endorsed PTSD symptoms, many of their treating clinicians did not assess or diagnose this disorder, thus missing an important component for treatment.
Increased risk for suicidality. Studies have shown that individuals who have lost a loved one to suicide are themselves at heightened risk for suicidal ideation and behaviors.22-27 Therefore, an assessment for suicide risk is always advisable. However, it is important to note that suicidal ideation is not uncommon and can serve different functions for survivors of suicide loss without necessarily progressing to a plan for acting on such ideations. Survivors of suicide loss may wish to “join” their loved one; to understand or identify with the mental state of the deceased; to punish themselves for failing to prevent the suicide; or to end their own pain through death. Therefore, it is crucial to assess the nature and function of expressed ideation (in addition to the presence or absence of plans) before assigning the level of risk.
Elements of suicide grief
After the loss of a loved one to suicide, the path to healing is often complex, with survivors of suicide loss enduring the following challenges:
Existential assumptions are shattered. Several authors28-30 have found that suicide loss is also likely to shatter survivors’ existential assumptions regarding their worldviews, roles, and identities, as well as religious and spiritual beliefs. As one survivor of suicide loss in my practice noted, “The world is gone, nothing is predictable anymore, and it’s no longer safe to assume anything.” Others have described feeling “fragmented” in ways they had never before experienced, and many have reported difficulties in “trusting” their own judgment, the stability of the world, and relationships. “Why?” becomes an emergent and insistent question in the survivor’s efforts to understand the suicide and (ideally) reassemble a coherent narrative around the loss.
Increased duration and intensity of grief. The duration of the grief process is likely to be affected by the traumatic nature of suicide loss, the differential social support accorded to its survivors, and the difficulty in finding systems that can validate and normalize the unique elements in suicide bereavement. The stigmatized reactions of others, particularly when internalized, can present barriers to the processing of grief. In addition, the intensity of the trauma and existential impact, as well as the perseverative nature of several of the unique themes (Box 1), can also prolong the processing and increase the intensity of suicide grief. Clinicians would do well to recognize the relatively “normative” nature of the increased duration and intensity, rather than seeing it as immediately indicative of a DSM diagnosis of complicated/prolonged grief disorder.
Box 1
Common themes in the suicide grief process
Several common themes are likely to emerge during the suicide grief process. Guilt and a sense of failure—around what one did and did not do—can be pervasive and persistent, and are often present even when not objectively warranted.
Anger and blame directed towards the deceased, other family members, and clinicians who had been treating the deceased may also be present, and may be used in efforts to deflect guilt. Any of these themes may be enlisted to create a deceptively simple narrative for understanding the reasons for the suicide.
Shame is often present, and certainly exacerbated by both external and internalized stigma. Feelings of rejection, betrayal, and abandonment by the deceased are also common, as well as fear/hypervigilance regarding the possibility of losing others to suicide. Given the intensity of suicide grief, it has been my observation that there may also be fear in relation to one's own mental status, as many otherwise healthy survivors of suicide loss have described feeling like they're "going crazy." Finally, there may also be relief, particularly if the deceased had been suffering from chronic psychiatric distress or had been cruel or abusive.
Continue to: Family disruption
Family disruption. It is not uncommon for a suicide loss to result in family disruption.6,31-32 This may manifest in the blaming of family members for “sins of omission or commission,”6 conflicts around the disclosure of the suicide both within and outside of the family, discordant grieving styles, and difficulties in understanding and attending to the needs of one’s children while grieving oneself.
Despite the common elements often seen in suicide grief, it is crucial to recognize that this process is not “one size fits all.” Not only are there individual variants, but Grad et al33 found gender-based differences in grieving styles, and cultural issues such as the “meanings” assigned to suicide, and culturally sanctioned grief rituals and behaviors that are also likely to affect how grief is experienced and expressed. In addition, personal variants such as closeness/conflicts with the deceased, histories of previous trauma or loss, pre-existing psychiatric disorders, and attachment orientation34 are likely to impact the grief process.
Losing close friends and colleagues may be similarly traumatic, but these survivors of suicide loss often receive even less social support than those who have kinship losses. Finally, when a suicide loss occurs in a professional capacity (such as the loss of a patient), this is likely to have many additional implications for one’s professional functions and identity.35
Interventions to help survivors
Several goals and “tasks” are involved in the suicide bereavement process (Box 21,6,30,36-40). These can be achieved through the following interventions: Support groups. Many survivors find that support groups that focus on suicide loss are extremely helpful, and research has supported this.1,4,41-44 Interactions with other suicide loss survivors provide hope, connection, and an “antidote” to stigma and shame. Optimally, group facilitators provide education, validation and normalization of the grief trajectory, and facilitate the sharing of both loss experiences and current functioning between group members. As a result, group participants often report renewed connections, increased efficacy in giving and accepting support, and decreased distress (including reductions in PTSD and depressive symptoms). The American Association of Suicidology (www.suicidology.org) and American Foundation of Suicide Prevention (www.afsp.org) provide contact information for suicide loss survivor groups (by geographical area) as well as information about online support groups.
Box 2
Goals and 'tasks' in suicide bereavement
The following goals and "tasks" should be part of the process of suicide bereavement:
- Reduce symptoms of posttraumatic stress disorder and other psychiatric disorders. Given the traumatic nature of the loss, an important goal is to understand and reduce posttraumatic stress disorder and other psychiatric symptoms, and incrementally improving functionality in relation to these.
- Integrate the loss. Recent authors36-38 have highlighted the need for survivors of suicide loss to "bear" and integrate the loss, as opposed to the concept of "getting over it." In these paradigms, the loss becomes an important part of one's identity, and eventually ceases to define it. Optimally, the "whole person" is remembered, not just the suicide. Part of this involves a reinvestment in life, with the acceptance of a "new normal" that takes the loss into account. It is not unusual for survivors of suicide loss to report some guilt in "moving on" and/or experiencing pleasure; often this is felt as a "betrayal" of the deceased.
- Create meaning from the loss. A major goal for those who have lost a loved one to suicide is the ability to find and/or create meaning from the loss. This would include the creation of a loss narrative39 that incorporates both ambiguity and complexity, as well as a regained/renewed sense of purpose in ongoing life.
- Develop ambiguity tolerance. A related "task" in suicide grief is the development of ambiguity tolerance, which generally includes an understanding of the complexity underlying suicide, the ability to offer oneself a "fair trial"30 in relation to one's realistic degree of responsibility, and the acceptance that many questions may remain unanswerable. In addition, in concert with the current understanding of "continuing bonds,"40 survivors should attempt to attend to the ongoing relationship with the deceased, including any "unfinished business."6
- Develop skills to manage stigmatized social responses and/or changes in family and social relationships.
- Memorialize and honor the deceased. Healing for survivors is facilitated by memorializations, which both validate the mourning process itself while also paying tribute to the richness of the deceased person's life.
- Post-traumatic growth. The relatively new understanding of "post-traumatic" growth is certainly applicable to the "unexpected gifts" many survivors of suicide loss report after they have moved through suicide grief. This includes greater understanding toward oneself, other survivors of suicide loss, and suicidal individuals; gratitude toward those who have provided support; and a desire to "use" their newfound understanding of suicide and suicide grief in ways to honor the deceased and benefit others. Feigelman et al1 found that many longer-term survivors of suicide loss engaged in both direct service and social activism around suicide pre- and postvention.
Individual treatment. The limited research on individual treatment for suicide loss survivors suggests that while most participants find it generally helpful, a significant number of others report that their therapists lack knowledge of suicide grief and endorse stigmatizing attitudes toward suicide and suicide loss survivors.45-46 In addition, Sanford et al3 found that survivors of suicide loss who endorsed PTSD symptoms were not assessed, diagnosed, or treated for these symptoms.
Continue to: This speaks to the importance of understanding what is...
This speaks to the importance of understanding what is “normative” for survivors of suicide loss. In general, “normalization” and psychoeducation about the suicide grief trajectory can play an important role in work with survivors of suicide loss, even in the presence of diagnosable disorders. While PTSD, depressive symptoms, and suicidal ideation are not uncommon in suicide loss survivors, and certainly may warrant clinical assessment and treatment, it can be helpful (and less stigmatizing) for your patients to know that these diagnoses are relatively common and understandable in the context of this devastating experience. For instance, survivors of suicide loss often report feeling relieved when clinicians explain the connections between traumatic loss and PTSD and/or depressive symptoms, and this can also help to relieve secondary anxiety about “going crazy.” Many survivors of suicide loss also describe feeling as though they are functioning on “autopilot” in the earlier stages of grief; it can help them understand the “function” of compartmentalization as potentially adaptive in the short run.
Suicide loss survivors may also find it helpful to learn about suicidal states of mind and their relationships to any types of mental illness their loved ones had struggled with.47
Your role: Help survivors integrate the loss
Before beginning treatment with an individual who has lost a loved one to suicide, clinicians should thoroughly explore their own understanding of and experience with suicide, including assumptions around causation, internalized stigma about suicidal individuals and survivors of suicide loss, their own history of suicide loss or suicidality, cultural/religious attitudes, and anxiety/defenses associated with the topic of suicide. These factors, particularly when unexamined, are likely to impact the treatment relationship and one’s clinical efficacy.
In concert with the existing literature, consider the potential goals and tasks involved in the integration of the individual’s suicide loss, along with any individual factors/variants that may impact the grief trajectory. Kosminsky and Jordon34 described the role of the clinician in this situation as a “transitional attachment figure” who facilitates the management and integration of the loss into the creation of what survivors of suicide loss have termed a “new normal.”
Because suicide loss is often associated with PTSD and other psychiatric illnesses (eg, depression, suicidality, substance abuse), it is essential to balance the assessment and treatment of these issues with attention to grief issues as needed. Again, to the extent that such issues have arisen primarily in the wake of the suicide loss, it can be helpful for patients to understand their connection to the context of the loss.
Continue to: Ideally, the clinician should...
Ideally, the clinician should be “present” with the patient’s pain, normative guilt, and rumination, without attempting to quickly eliminate or “fix” it or provide premature reassurance that the survivor of suicide loss “did nothing wrong.” Rather, as Jordan6 suggests, the clinician should act to promote a “fair trial” with respect to the patient’s guilt and blame, with an understanding of the “tyranny of hindsight.” The promotion of ambiguity tolerance should also play a role in coming to terms with many questions that may remain unanswered.
Optimally, clinicians should encourage patients to attend to their ongoing relationship with the deceased, particularly in the service of resolving “unfinished business,” ultimately integrating the loss into memories of the whole person. In line with this, survivors of suicide loss may be encouraged to create a narrative of the loss that incorporates both complexity and ambiguity. In the service of supporting the suicide loss survivor’s reinvestment in life, it is often helpful to facilitate their ability to anticipate and cope with triggers, such as anniversaries, birthdays, or holidays, as well as to develop and use skills for managing difficult or stigmatizing social or cultural reactions.
Any disruptions in family functioning should also be addressed. Psychoeducation about discordant grieving styles (particularly around gender) and the support of children’s grief may be helpful, and referrals to family or couples therapists should be considered as needed. Finally, the facilitation of suicide loss survivors’ creation of memorializations or rituals can help promote healing and make their loss meaningful.
Bottom Line
Losing a loved one to suicide is often a devastating and traumatic experience, but with optimal support, most survivors are ultimately able to integrate the loss and grow as a result. Understanding the suicide grief trajectory, as well as general guidelines for treatment, will facilitate healing and growth in the aftermath of suicide loss.
Related Resources
- Jordan JR, McIntosh JL. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011.
- American Association of Suicidology. http://www.suicidology.org/.
- American Foundation for Suicide Prevention. https://afsp.org/.
1. Feigelman W, Jordan JR, McIntosh JL, et al. Devastating losses: how parents cope with the death of a child to suicide or drugs. New York, NY: Springer; 2012.
2. McIntosh JL. Research on survivors of suicide. In: Stimming MT, Stimming M, eds. Before their time: adult children’s experiences of parental suicide. Philadelphia, PA: Temple University Press; 1999:157-180.
3. Sanford RL, Cerel J, McGann VL, et al. Suicide loss survivors’ experiences with therapy: Implications for clinical practice. Community Ment Health J. 2016;5(2):551-558.
4. Jordan JR, McMenamy J. Interventions for suicide survivors: a review of the literature. Suicide Life Threat Behav. 2004;34(4):337-349.
5. Survivors of Suicide Loss Task Force. Responding to grief, trauma, & distress after a suicide: U.S. national guidelines. Washington, DC: National Action Alliance for Suicide Prevention; 2015.
6. Jordan JR, McGann V. Clinical work with suicide loss survivors: implications of the U.S. postvention guidelines. Death Stud. 2017;41(10):659-672.
7. Jordan JR. Is suicide bereavement different? A reassessment of the literature. Suicide Life Threat Behav. 2001;31(1):91-102.
8. Cvinar JG. Do suicide survivors suffer social stigma: a review of the literature. Perspect Psychiatr Care. 2005;41(1):14-21.
9. U.S. Public Health Service. The Surgeon General’s call to action to prevent suicide. Washington, DC: Department of Health and Human Services; 1999.
10. Doka KJ. Disenfranchised grief: recognizing hidden sorrow. Lexington, MA: Lexington; 1989.
11. Doka KJ. Disenfranchised grief: new directions, challenges, and strategies for practice. Champaign, IL: Research Press; 2002.
12. McIntosh JL. Suicide survivors: the aftermath of suicide and suicidal behavior. In: Bryant CD, ed. Handbook of death & dying. Vol. 1. Thousand Oaks, CA: SAGE Publications; 2003:339-350.
13. Jordan, JR, McIntosh, JL. Is suicide bereavement different? A framework for rethinking the question. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:19-42.
14. Dunne EJ, McIntosh JL, Dunne-Maxim K, eds. Suicide and its aftermath: understanding and counseling the survivors. New York, NY: W.W. Norton & Co.; 1987.
15. Harwood D, Hawton K, Hope T, et al. The grief experiences and needs of bereaved relatives and friends of older people dying through suicide: a descriptive and case-control study. J Affect Disord. 2002;72(2):185-194.
16. Armour, M. Violent death: understanding the context of traumatic and stigmatized grief. J Hum Behav Soc Environ. 2006;14(4):53-90.
17. Van Dongen CJ. Social context of postsuicide bereavement. Death Stud. 1993;17(2):125-141.
18. Calhoun LG, Allen BG. Social reactions to the survivor of a suicide in the family: A review of the literature. Omega – Journal of Death and Dying. 1991;23(2):95-107.
19. Range LM. When a loss is due to suicide: unique aspects of bereavement. In: Harvey JH, ed. Perspectives on loss: a sourcebook. Philadelphia, PA: Brunner/Mazel; 1998:213-220.
20. Sveen CA, Walby FA. Suicide survivors’ mental health and grief reactions: a systematic review of controlled studies. Suicide Life Threat Behav. 2008;38(1):13-29.
21. Feigelman W, Gorman BS, Jordan JR. Stigmatization and suicide bereavement. Death Stud. 2009;33(7):591-608.
22. Shneidman ES. Foreword. In: Cain AC, ed. Survivors of suicide. Springfield, IL: Charles C. Thomas; 1972:ix-xi.
23. Jordan JR, McIntosh, JL. Suicide bereavement: Why study survivors of suicide loss? In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:3-18.
24. Agerbo E. Midlife suicide risk, partner’s psychiatric illness, spouse and child bereavement by suicide or other modes of death: a gender specific study. J Epidemiol Community Health. 2005;59(5):407-412.
25. Hedström P, Liu KY, Nordvik MK. Interaction domains and suicide: a population-based panel study of suicides in Stockholm, 1991-1999. Soc Forces. 2008;87(2):713-740.
26. Qin P, Agerbo E, Mortensen PB. Suicide risk in relation to family history of completed suicide and psychiatric disorders: a nested case-control study based on longitudinal registers. Lancet. 2002;360(9340):1126-1130.
27. Qin P, Mortensen PB. The impact of parental status on the risk of completed suicide. Arch Gen Psychiatry. 2003;60(8):797-802.
28. Neimeyer RA, Sands D. Suicide loss and the quest for meaning. In: Andriessen K, Krysinska K, Grad OT, eds. Postvention in action: the international handbook of suicide bereavement support. Cambridge, MA: Hogrefe; 2017:71-84.
29. Sands DC, Jordan JR, Neimeyer RA. The meanings of suicide: A narrative approach to healing. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:249-282.
30. Jordan JR. Principles of grief counseling with adult survivors. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:179-224.
31. Cerel J, Jordan JR, Duberstein PR. The impact of suicide on the family. Crisis. 2008;29:38-44.
32. Kaslow NJ, Samples TC, Rhodes M, et al. A family-oriented and culturally sensitive postvention approach with suicide survivors. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:301-323.
33. Grad OT, Treven M, Krysinska K. Suicide bereavement and gender. In: Andriessen K, Krysinska K, Grad OT, eds. Postvention in action: the international handbook of suicide bereavement support. Cambridge, MA: Hogrefe; 2017:39-49.
34. Kosminsky PS, Jordan JR. Attachment-informed grief therapy: the clinician’s guide to foundations and applications. New York, NY: Routledge; 2016.
35. Gutin N, McGann VL, Jordan JR. The impact of suicide on professional caregivers. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:93-111.
36. Jordan JR. Bereavement after suicide. Psychiatr Ann. 2008;38(10):679-685.
37. Jordan JR. After suicide: clinical work with survivors. Grief Matters. 2009;12(1):4-9.
38. Neimeyer, RA. Traumatic loss and the reconstruction of meaning. J Palliat Med. 2002;5(6):935-942; discussion 942-943.
39. Neimeyer R, ed. Meaning reconstruction & the experience of loss. Washington, DC: American Psychological Association; 2001.
40. Klass, D. Sorrow and solace: Neglected areas in bereavement research. Death Stud. 2013;37(7):597-616.
41. Farberow NL. The Los Angeles Survivors-After-Suicide program: an evaluation. Crisis. 1992;13(1):23-34.
42. McDaid C, Trowman R, Golder S, et al. Interventions for people bereaved through suicide: systematic review. Br J Psychiatry. 2008;193(6):438-443.
43. Groos AD, Shakespeare-Finch J. Positive experiences for participants in suicide bereavement groups: a grounded theory model. Death Stud. 2013;37(1):1-24.
44. Jordan JR. Group work with suicide survivors. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:283-300.
45. Wilson A, Marshall A. The support needs and experiences of suicidally bereaved family and friends. Death Stud. 2010;34(7):625-640.
46. McKinnon JM, Chonody J. Exploring the formal supports used by people bereaved through suicide: a qualitative study. Soc Work Ment Health. 2014;12(3):231-248.
47. Myers MF, Fine C. Touched by suicide: hope and healing after loss. New York, NY: Gotham Books; 2006.
The loss of a loved one to suicide is often experienced as “devastating.”1 While survivors of suicide loss may be able to move through the grief process without clinical support,2 the traumatic and stigmatizing nature of suicide is likely to make its aftermath more challenging to navigate than other types of loss. Sanford et al3 found that more than two-thirds of suicide loss survivors sought therapy after their loss. Further, when individuals facing these challenges present for treatment, clinicians often face challenges of their own.
Very few clinicians are trained in general grief processes,4 and even those specifically trained in grief and loss have been shown to “miss” several of the common clinical features that are unique to suicide loss.3 In my professional experience, the intensity and duration of suicide grief are often greater than they are for other losses, and many survivors of suicide loss have reported that others, including clinicians, have “pathologized” this, rather than having understood it as normative under the circumstances.
Although there is extensive literature on the aftermath of suicide for surviving loved ones, very few controlled studies have assessed interventions specifically for this population. Yet the U.S. Guidelines for Suicide Postvention5 explicitly call for improved training for those who work with suicide loss survivors, as well as research on these interventions. Jordan and McGann6 noted, “Without a full knowledge of suicide and its aftermath, it is very possible to make clinical errors which can hamper treatment.” This article summarizes what is currently known about the general experience of suicide bereavement and optimal interventions in treatment.
What makes suicide loss unique?
Suicide bereavement is distinct from other types of loss in 3 significant ways7:
- the thematic content of the grief
- the social processes surrounding the survivor
- the impact that suicide has on family systems.
Additionally, the perceived intentionality and preventability of a suicide death, as well as its stigmatized and traumatic nature, differentiate it from other types of traumatic loss.7 These elements are all likely to affect the nature, intensity, and duration of the grief.
Stigma and suicide. Stigma associated with suicide is well documented.8 Former U.S. Surgeon General David Satcher9 specifically described stigma toward suicide as one of the biggest barriers to prevention. In addition, researchers have found that the stigma associated with suicide “spills over” to the bereaved family members. Doka10,11 refers to “disenfranchised grief,” in which bereaved individuals receive the message that their grief is not legitimate, and as a result, they are likely to internalize this view. Studies have shown that individuals bereaved by suicide are also stigmatized, and are believed to be more psychologically disturbed, less likable, more blameworthy, more ashamed, and more in need of professional help than other bereaved individuals.8,12-20
These judgments often mirror suicide loss survivors’ self-punitive assessments, which then become exacerbated by and intertwined with both externally imposed and internalized stigma. Thus, it is not uncommon for survivors of suicide loss to question their own right to grieve, to report low expectations of social support, and to feel compelled to deny or hide the mode of death. To the extent that they are actively grieving, survivors of suicide loss often feel that they must do so in isolation. Thus, the perception of stigma, whether external or internalized, can have a profound effect on decisions about disclosure, requesting support, and ultimately on one’s ability to integrate the loss. Indeed, Feigelman et al21 found that stigmatization after suicide was specifically associated with ongoing grief difficulties, depression, and suicidal ideation.
Continue to: Traumatic nature of suicide
Traumatic nature of suicide. Suicide loss is also quite traumatic, and posttraumatic stress disorder (PTSD) symptoms such as shock, horror, disbelief, and intrusive/perseverative thoughts and questions, particularly in the earlier stages of grief, are common. Sanford et al3 found that the higher the level of “perceived closeness” to the deceased, the more likely that survivors of suicide loss would experience PTSD symptoms. In addition, the dramatic loss of social support following a suicide loss may itself be traumatic, which can serve to compound these difficulties. Notably, Sanford et al3 found that even for those survivors of suicide loss in treatment who endorsed PTSD symptoms, many of their treating clinicians did not assess or diagnose this disorder, thus missing an important component for treatment.
Increased risk for suicidality. Studies have shown that individuals who have lost a loved one to suicide are themselves at heightened risk for suicidal ideation and behaviors.22-27 Therefore, an assessment for suicide risk is always advisable. However, it is important to note that suicidal ideation is not uncommon and can serve different functions for survivors of suicide loss without necessarily progressing to a plan for acting on such ideations. Survivors of suicide loss may wish to “join” their loved one; to understand or identify with the mental state of the deceased; to punish themselves for failing to prevent the suicide; or to end their own pain through death. Therefore, it is crucial to assess the nature and function of expressed ideation (in addition to the presence or absence of plans) before assigning the level of risk.
Elements of suicide grief
After the loss of a loved one to suicide, the path to healing is often complex, with survivors of suicide loss enduring the following challenges:
Existential assumptions are shattered. Several authors28-30 have found that suicide loss is also likely to shatter survivors’ existential assumptions regarding their worldviews, roles, and identities, as well as religious and spiritual beliefs. As one survivor of suicide loss in my practice noted, “The world is gone, nothing is predictable anymore, and it’s no longer safe to assume anything.” Others have described feeling “fragmented” in ways they had never before experienced, and many have reported difficulties in “trusting” their own judgment, the stability of the world, and relationships. “Why?” becomes an emergent and insistent question in the survivor’s efforts to understand the suicide and (ideally) reassemble a coherent narrative around the loss.
Increased duration and intensity of grief. The duration of the grief process is likely to be affected by the traumatic nature of suicide loss, the differential social support accorded to its survivors, and the difficulty in finding systems that can validate and normalize the unique elements in suicide bereavement. The stigmatized reactions of others, particularly when internalized, can present barriers to the processing of grief. In addition, the intensity of the trauma and existential impact, as well as the perseverative nature of several of the unique themes (Box 1), can also prolong the processing and increase the intensity of suicide grief. Clinicians would do well to recognize the relatively “normative” nature of the increased duration and intensity, rather than seeing it as immediately indicative of a DSM diagnosis of complicated/prolonged grief disorder.
Box 1
Common themes in the suicide grief process
Several common themes are likely to emerge during the suicide grief process. Guilt and a sense of failure—around what one did and did not do—can be pervasive and persistent, and are often present even when not objectively warranted.
Anger and blame directed towards the deceased, other family members, and clinicians who had been treating the deceased may also be present, and may be used in efforts to deflect guilt. Any of these themes may be enlisted to create a deceptively simple narrative for understanding the reasons for the suicide.
Shame is often present, and certainly exacerbated by both external and internalized stigma. Feelings of rejection, betrayal, and abandonment by the deceased are also common, as well as fear/hypervigilance regarding the possibility of losing others to suicide. Given the intensity of suicide grief, it has been my observation that there may also be fear in relation to one's own mental status, as many otherwise healthy survivors of suicide loss have described feeling like they're "going crazy." Finally, there may also be relief, particularly if the deceased had been suffering from chronic psychiatric distress or had been cruel or abusive.
Continue to: Family disruption
Family disruption. It is not uncommon for a suicide loss to result in family disruption.6,31-32 This may manifest in the blaming of family members for “sins of omission or commission,”6 conflicts around the disclosure of the suicide both within and outside of the family, discordant grieving styles, and difficulties in understanding and attending to the needs of one’s children while grieving oneself.
Despite the common elements often seen in suicide grief, it is crucial to recognize that this process is not “one size fits all.” Not only are there individual variants, but Grad et al33 found gender-based differences in grieving styles, and cultural issues such as the “meanings” assigned to suicide, and culturally sanctioned grief rituals and behaviors that are also likely to affect how grief is experienced and expressed. In addition, personal variants such as closeness/conflicts with the deceased, histories of previous trauma or loss, pre-existing psychiatric disorders, and attachment orientation34 are likely to impact the grief process.
Losing close friends and colleagues may be similarly traumatic, but these survivors of suicide loss often receive even less social support than those who have kinship losses. Finally, when a suicide loss occurs in a professional capacity (such as the loss of a patient), this is likely to have many additional implications for one’s professional functions and identity.35
Interventions to help survivors
Several goals and “tasks” are involved in the suicide bereavement process (Box 21,6,30,36-40). These can be achieved through the following interventions: Support groups. Many survivors find that support groups that focus on suicide loss are extremely helpful, and research has supported this.1,4,41-44 Interactions with other suicide loss survivors provide hope, connection, and an “antidote” to stigma and shame. Optimally, group facilitators provide education, validation and normalization of the grief trajectory, and facilitate the sharing of both loss experiences and current functioning between group members. As a result, group participants often report renewed connections, increased efficacy in giving and accepting support, and decreased distress (including reductions in PTSD and depressive symptoms). The American Association of Suicidology (www.suicidology.org) and American Foundation of Suicide Prevention (www.afsp.org) provide contact information for suicide loss survivor groups (by geographical area) as well as information about online support groups.
Box 2
Goals and 'tasks' in suicide bereavement
The following goals and "tasks" should be part of the process of suicide bereavement:
- Reduce symptoms of posttraumatic stress disorder and other psychiatric disorders. Given the traumatic nature of the loss, an important goal is to understand and reduce posttraumatic stress disorder and other psychiatric symptoms, and incrementally improving functionality in relation to these.
- Integrate the loss. Recent authors36-38 have highlighted the need for survivors of suicide loss to "bear" and integrate the loss, as opposed to the concept of "getting over it." In these paradigms, the loss becomes an important part of one's identity, and eventually ceases to define it. Optimally, the "whole person" is remembered, not just the suicide. Part of this involves a reinvestment in life, with the acceptance of a "new normal" that takes the loss into account. It is not unusual for survivors of suicide loss to report some guilt in "moving on" and/or experiencing pleasure; often this is felt as a "betrayal" of the deceased.
- Create meaning from the loss. A major goal for those who have lost a loved one to suicide is the ability to find and/or create meaning from the loss. This would include the creation of a loss narrative39 that incorporates both ambiguity and complexity, as well as a regained/renewed sense of purpose in ongoing life.
- Develop ambiguity tolerance. A related "task" in suicide grief is the development of ambiguity tolerance, which generally includes an understanding of the complexity underlying suicide, the ability to offer oneself a "fair trial"30 in relation to one's realistic degree of responsibility, and the acceptance that many questions may remain unanswerable. In addition, in concert with the current understanding of "continuing bonds,"40 survivors should attempt to attend to the ongoing relationship with the deceased, including any "unfinished business."6
- Develop skills to manage stigmatized social responses and/or changes in family and social relationships.
- Memorialize and honor the deceased. Healing for survivors is facilitated by memorializations, which both validate the mourning process itself while also paying tribute to the richness of the deceased person's life.
- Post-traumatic growth. The relatively new understanding of "post-traumatic" growth is certainly applicable to the "unexpected gifts" many survivors of suicide loss report after they have moved through suicide grief. This includes greater understanding toward oneself, other survivors of suicide loss, and suicidal individuals; gratitude toward those who have provided support; and a desire to "use" their newfound understanding of suicide and suicide grief in ways to honor the deceased and benefit others. Feigelman et al1 found that many longer-term survivors of suicide loss engaged in both direct service and social activism around suicide pre- and postvention.
Individual treatment. The limited research on individual treatment for suicide loss survivors suggests that while most participants find it generally helpful, a significant number of others report that their therapists lack knowledge of suicide grief and endorse stigmatizing attitudes toward suicide and suicide loss survivors.45-46 In addition, Sanford et al3 found that survivors of suicide loss who endorsed PTSD symptoms were not assessed, diagnosed, or treated for these symptoms.
Continue to: This speaks to the importance of understanding what is...
This speaks to the importance of understanding what is “normative” for survivors of suicide loss. In general, “normalization” and psychoeducation about the suicide grief trajectory can play an important role in work with survivors of suicide loss, even in the presence of diagnosable disorders. While PTSD, depressive symptoms, and suicidal ideation are not uncommon in suicide loss survivors, and certainly may warrant clinical assessment and treatment, it can be helpful (and less stigmatizing) for your patients to know that these diagnoses are relatively common and understandable in the context of this devastating experience. For instance, survivors of suicide loss often report feeling relieved when clinicians explain the connections between traumatic loss and PTSD and/or depressive symptoms, and this can also help to relieve secondary anxiety about “going crazy.” Many survivors of suicide loss also describe feeling as though they are functioning on “autopilot” in the earlier stages of grief; it can help them understand the “function” of compartmentalization as potentially adaptive in the short run.
Suicide loss survivors may also find it helpful to learn about suicidal states of mind and their relationships to any types of mental illness their loved ones had struggled with.47
Your role: Help survivors integrate the loss
Before beginning treatment with an individual who has lost a loved one to suicide, clinicians should thoroughly explore their own understanding of and experience with suicide, including assumptions around causation, internalized stigma about suicidal individuals and survivors of suicide loss, their own history of suicide loss or suicidality, cultural/religious attitudes, and anxiety/defenses associated with the topic of suicide. These factors, particularly when unexamined, are likely to impact the treatment relationship and one’s clinical efficacy.
In concert with the existing literature, consider the potential goals and tasks involved in the integration of the individual’s suicide loss, along with any individual factors/variants that may impact the grief trajectory. Kosminsky and Jordon34 described the role of the clinician in this situation as a “transitional attachment figure” who facilitates the management and integration of the loss into the creation of what survivors of suicide loss have termed a “new normal.”
Because suicide loss is often associated with PTSD and other psychiatric illnesses (eg, depression, suicidality, substance abuse), it is essential to balance the assessment and treatment of these issues with attention to grief issues as needed. Again, to the extent that such issues have arisen primarily in the wake of the suicide loss, it can be helpful for patients to understand their connection to the context of the loss.
Continue to: Ideally, the clinician should...
Ideally, the clinician should be “present” with the patient’s pain, normative guilt, and rumination, without attempting to quickly eliminate or “fix” it or provide premature reassurance that the survivor of suicide loss “did nothing wrong.” Rather, as Jordan6 suggests, the clinician should act to promote a “fair trial” with respect to the patient’s guilt and blame, with an understanding of the “tyranny of hindsight.” The promotion of ambiguity tolerance should also play a role in coming to terms with many questions that may remain unanswered.
Optimally, clinicians should encourage patients to attend to their ongoing relationship with the deceased, particularly in the service of resolving “unfinished business,” ultimately integrating the loss into memories of the whole person. In line with this, survivors of suicide loss may be encouraged to create a narrative of the loss that incorporates both complexity and ambiguity. In the service of supporting the suicide loss survivor’s reinvestment in life, it is often helpful to facilitate their ability to anticipate and cope with triggers, such as anniversaries, birthdays, or holidays, as well as to develop and use skills for managing difficult or stigmatizing social or cultural reactions.
Any disruptions in family functioning should also be addressed. Psychoeducation about discordant grieving styles (particularly around gender) and the support of children’s grief may be helpful, and referrals to family or couples therapists should be considered as needed. Finally, the facilitation of suicide loss survivors’ creation of memorializations or rituals can help promote healing and make their loss meaningful.
Bottom Line
Losing a loved one to suicide is often a devastating and traumatic experience, but with optimal support, most survivors are ultimately able to integrate the loss and grow as a result. Understanding the suicide grief trajectory, as well as general guidelines for treatment, will facilitate healing and growth in the aftermath of suicide loss.
Related Resources
- Jordan JR, McIntosh JL. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011.
- American Association of Suicidology. http://www.suicidology.org/.
- American Foundation for Suicide Prevention. https://afsp.org/.
The loss of a loved one to suicide is often experienced as “devastating.”1 While survivors of suicide loss may be able to move through the grief process without clinical support,2 the traumatic and stigmatizing nature of suicide is likely to make its aftermath more challenging to navigate than other types of loss. Sanford et al3 found that more than two-thirds of suicide loss survivors sought therapy after their loss. Further, when individuals facing these challenges present for treatment, clinicians often face challenges of their own.
Very few clinicians are trained in general grief processes,4 and even those specifically trained in grief and loss have been shown to “miss” several of the common clinical features that are unique to suicide loss.3 In my professional experience, the intensity and duration of suicide grief are often greater than they are for other losses, and many survivors of suicide loss have reported that others, including clinicians, have “pathologized” this, rather than having understood it as normative under the circumstances.
Although there is extensive literature on the aftermath of suicide for surviving loved ones, very few controlled studies have assessed interventions specifically for this population. Yet the U.S. Guidelines for Suicide Postvention5 explicitly call for improved training for those who work with suicide loss survivors, as well as research on these interventions. Jordan and McGann6 noted, “Without a full knowledge of suicide and its aftermath, it is very possible to make clinical errors which can hamper treatment.” This article summarizes what is currently known about the general experience of suicide bereavement and optimal interventions in treatment.
What makes suicide loss unique?
Suicide bereavement is distinct from other types of loss in 3 significant ways7:
- the thematic content of the grief
- the social processes surrounding the survivor
- the impact that suicide has on family systems.
Additionally, the perceived intentionality and preventability of a suicide death, as well as its stigmatized and traumatic nature, differentiate it from other types of traumatic loss.7 These elements are all likely to affect the nature, intensity, and duration of the grief.
Stigma and suicide. Stigma associated with suicide is well documented.8 Former U.S. Surgeon General David Satcher9 specifically described stigma toward suicide as one of the biggest barriers to prevention. In addition, researchers have found that the stigma associated with suicide “spills over” to the bereaved family members. Doka10,11 refers to “disenfranchised grief,” in which bereaved individuals receive the message that their grief is not legitimate, and as a result, they are likely to internalize this view. Studies have shown that individuals bereaved by suicide are also stigmatized, and are believed to be more psychologically disturbed, less likable, more blameworthy, more ashamed, and more in need of professional help than other bereaved individuals.8,12-20
These judgments often mirror suicide loss survivors’ self-punitive assessments, which then become exacerbated by and intertwined with both externally imposed and internalized stigma. Thus, it is not uncommon for survivors of suicide loss to question their own right to grieve, to report low expectations of social support, and to feel compelled to deny or hide the mode of death. To the extent that they are actively grieving, survivors of suicide loss often feel that they must do so in isolation. Thus, the perception of stigma, whether external or internalized, can have a profound effect on decisions about disclosure, requesting support, and ultimately on one’s ability to integrate the loss. Indeed, Feigelman et al21 found that stigmatization after suicide was specifically associated with ongoing grief difficulties, depression, and suicidal ideation.
Continue to: Traumatic nature of suicide
Traumatic nature of suicide. Suicide loss is also quite traumatic, and posttraumatic stress disorder (PTSD) symptoms such as shock, horror, disbelief, and intrusive/perseverative thoughts and questions, particularly in the earlier stages of grief, are common. Sanford et al3 found that the higher the level of “perceived closeness” to the deceased, the more likely that survivors of suicide loss would experience PTSD symptoms. In addition, the dramatic loss of social support following a suicide loss may itself be traumatic, which can serve to compound these difficulties. Notably, Sanford et al3 found that even for those survivors of suicide loss in treatment who endorsed PTSD symptoms, many of their treating clinicians did not assess or diagnose this disorder, thus missing an important component for treatment.
Increased risk for suicidality. Studies have shown that individuals who have lost a loved one to suicide are themselves at heightened risk for suicidal ideation and behaviors.22-27 Therefore, an assessment for suicide risk is always advisable. However, it is important to note that suicidal ideation is not uncommon and can serve different functions for survivors of suicide loss without necessarily progressing to a plan for acting on such ideations. Survivors of suicide loss may wish to “join” their loved one; to understand or identify with the mental state of the deceased; to punish themselves for failing to prevent the suicide; or to end their own pain through death. Therefore, it is crucial to assess the nature and function of expressed ideation (in addition to the presence or absence of plans) before assigning the level of risk.
Elements of suicide grief
After the loss of a loved one to suicide, the path to healing is often complex, with survivors of suicide loss enduring the following challenges:
Existential assumptions are shattered. Several authors28-30 have found that suicide loss is also likely to shatter survivors’ existential assumptions regarding their worldviews, roles, and identities, as well as religious and spiritual beliefs. As one survivor of suicide loss in my practice noted, “The world is gone, nothing is predictable anymore, and it’s no longer safe to assume anything.” Others have described feeling “fragmented” in ways they had never before experienced, and many have reported difficulties in “trusting” their own judgment, the stability of the world, and relationships. “Why?” becomes an emergent and insistent question in the survivor’s efforts to understand the suicide and (ideally) reassemble a coherent narrative around the loss.
Increased duration and intensity of grief. The duration of the grief process is likely to be affected by the traumatic nature of suicide loss, the differential social support accorded to its survivors, and the difficulty in finding systems that can validate and normalize the unique elements in suicide bereavement. The stigmatized reactions of others, particularly when internalized, can present barriers to the processing of grief. In addition, the intensity of the trauma and existential impact, as well as the perseverative nature of several of the unique themes (Box 1), can also prolong the processing and increase the intensity of suicide grief. Clinicians would do well to recognize the relatively “normative” nature of the increased duration and intensity, rather than seeing it as immediately indicative of a DSM diagnosis of complicated/prolonged grief disorder.
Box 1
Common themes in the suicide grief process
Several common themes are likely to emerge during the suicide grief process. Guilt and a sense of failure—around what one did and did not do—can be pervasive and persistent, and are often present even when not objectively warranted.
Anger and blame directed towards the deceased, other family members, and clinicians who had been treating the deceased may also be present, and may be used in efforts to deflect guilt. Any of these themes may be enlisted to create a deceptively simple narrative for understanding the reasons for the suicide.
Shame is often present, and certainly exacerbated by both external and internalized stigma. Feelings of rejection, betrayal, and abandonment by the deceased are also common, as well as fear/hypervigilance regarding the possibility of losing others to suicide. Given the intensity of suicide grief, it has been my observation that there may also be fear in relation to one's own mental status, as many otherwise healthy survivors of suicide loss have described feeling like they're "going crazy." Finally, there may also be relief, particularly if the deceased had been suffering from chronic psychiatric distress or had been cruel or abusive.
Continue to: Family disruption
Family disruption. It is not uncommon for a suicide loss to result in family disruption.6,31-32 This may manifest in the blaming of family members for “sins of omission or commission,”6 conflicts around the disclosure of the suicide both within and outside of the family, discordant grieving styles, and difficulties in understanding and attending to the needs of one’s children while grieving oneself.
Despite the common elements often seen in suicide grief, it is crucial to recognize that this process is not “one size fits all.” Not only are there individual variants, but Grad et al33 found gender-based differences in grieving styles, and cultural issues such as the “meanings” assigned to suicide, and culturally sanctioned grief rituals and behaviors that are also likely to affect how grief is experienced and expressed. In addition, personal variants such as closeness/conflicts with the deceased, histories of previous trauma or loss, pre-existing psychiatric disorders, and attachment orientation34 are likely to impact the grief process.
Losing close friends and colleagues may be similarly traumatic, but these survivors of suicide loss often receive even less social support than those who have kinship losses. Finally, when a suicide loss occurs in a professional capacity (such as the loss of a patient), this is likely to have many additional implications for one’s professional functions and identity.35
Interventions to help survivors
Several goals and “tasks” are involved in the suicide bereavement process (Box 21,6,30,36-40). These can be achieved through the following interventions: Support groups. Many survivors find that support groups that focus on suicide loss are extremely helpful, and research has supported this.1,4,41-44 Interactions with other suicide loss survivors provide hope, connection, and an “antidote” to stigma and shame. Optimally, group facilitators provide education, validation and normalization of the grief trajectory, and facilitate the sharing of both loss experiences and current functioning between group members. As a result, group participants often report renewed connections, increased efficacy in giving and accepting support, and decreased distress (including reductions in PTSD and depressive symptoms). The American Association of Suicidology (www.suicidology.org) and American Foundation of Suicide Prevention (www.afsp.org) provide contact information for suicide loss survivor groups (by geographical area) as well as information about online support groups.
Box 2
Goals and 'tasks' in suicide bereavement
The following goals and "tasks" should be part of the process of suicide bereavement:
- Reduce symptoms of posttraumatic stress disorder and other psychiatric disorders. Given the traumatic nature of the loss, an important goal is to understand and reduce posttraumatic stress disorder and other psychiatric symptoms, and incrementally improving functionality in relation to these.
- Integrate the loss. Recent authors36-38 have highlighted the need for survivors of suicide loss to "bear" and integrate the loss, as opposed to the concept of "getting over it." In these paradigms, the loss becomes an important part of one's identity, and eventually ceases to define it. Optimally, the "whole person" is remembered, not just the suicide. Part of this involves a reinvestment in life, with the acceptance of a "new normal" that takes the loss into account. It is not unusual for survivors of suicide loss to report some guilt in "moving on" and/or experiencing pleasure; often this is felt as a "betrayal" of the deceased.
- Create meaning from the loss. A major goal for those who have lost a loved one to suicide is the ability to find and/or create meaning from the loss. This would include the creation of a loss narrative39 that incorporates both ambiguity and complexity, as well as a regained/renewed sense of purpose in ongoing life.
- Develop ambiguity tolerance. A related "task" in suicide grief is the development of ambiguity tolerance, which generally includes an understanding of the complexity underlying suicide, the ability to offer oneself a "fair trial"30 in relation to one's realistic degree of responsibility, and the acceptance that many questions may remain unanswerable. In addition, in concert with the current understanding of "continuing bonds,"40 survivors should attempt to attend to the ongoing relationship with the deceased, including any "unfinished business."6
- Develop skills to manage stigmatized social responses and/or changes in family and social relationships.
- Memorialize and honor the deceased. Healing for survivors is facilitated by memorializations, which both validate the mourning process itself while also paying tribute to the richness of the deceased person's life.
- Post-traumatic growth. The relatively new understanding of "post-traumatic" growth is certainly applicable to the "unexpected gifts" many survivors of suicide loss report after they have moved through suicide grief. This includes greater understanding toward oneself, other survivors of suicide loss, and suicidal individuals; gratitude toward those who have provided support; and a desire to "use" their newfound understanding of suicide and suicide grief in ways to honor the deceased and benefit others. Feigelman et al1 found that many longer-term survivors of suicide loss engaged in both direct service and social activism around suicide pre- and postvention.
Individual treatment. The limited research on individual treatment for suicide loss survivors suggests that while most participants find it generally helpful, a significant number of others report that their therapists lack knowledge of suicide grief and endorse stigmatizing attitudes toward suicide and suicide loss survivors.45-46 In addition, Sanford et al3 found that survivors of suicide loss who endorsed PTSD symptoms were not assessed, diagnosed, or treated for these symptoms.
Continue to: This speaks to the importance of understanding what is...
This speaks to the importance of understanding what is “normative” for survivors of suicide loss. In general, “normalization” and psychoeducation about the suicide grief trajectory can play an important role in work with survivors of suicide loss, even in the presence of diagnosable disorders. While PTSD, depressive symptoms, and suicidal ideation are not uncommon in suicide loss survivors, and certainly may warrant clinical assessment and treatment, it can be helpful (and less stigmatizing) for your patients to know that these diagnoses are relatively common and understandable in the context of this devastating experience. For instance, survivors of suicide loss often report feeling relieved when clinicians explain the connections between traumatic loss and PTSD and/or depressive symptoms, and this can also help to relieve secondary anxiety about “going crazy.” Many survivors of suicide loss also describe feeling as though they are functioning on “autopilot” in the earlier stages of grief; it can help them understand the “function” of compartmentalization as potentially adaptive in the short run.
Suicide loss survivors may also find it helpful to learn about suicidal states of mind and their relationships to any types of mental illness their loved ones had struggled with.47
Your role: Help survivors integrate the loss
Before beginning treatment with an individual who has lost a loved one to suicide, clinicians should thoroughly explore their own understanding of and experience with suicide, including assumptions around causation, internalized stigma about suicidal individuals and survivors of suicide loss, their own history of suicide loss or suicidality, cultural/religious attitudes, and anxiety/defenses associated with the topic of suicide. These factors, particularly when unexamined, are likely to impact the treatment relationship and one’s clinical efficacy.
In concert with the existing literature, consider the potential goals and tasks involved in the integration of the individual’s suicide loss, along with any individual factors/variants that may impact the grief trajectory. Kosminsky and Jordon34 described the role of the clinician in this situation as a “transitional attachment figure” who facilitates the management and integration of the loss into the creation of what survivors of suicide loss have termed a “new normal.”
Because suicide loss is often associated with PTSD and other psychiatric illnesses (eg, depression, suicidality, substance abuse), it is essential to balance the assessment and treatment of these issues with attention to grief issues as needed. Again, to the extent that such issues have arisen primarily in the wake of the suicide loss, it can be helpful for patients to understand their connection to the context of the loss.
Continue to: Ideally, the clinician should...
Ideally, the clinician should be “present” with the patient’s pain, normative guilt, and rumination, without attempting to quickly eliminate or “fix” it or provide premature reassurance that the survivor of suicide loss “did nothing wrong.” Rather, as Jordan6 suggests, the clinician should act to promote a “fair trial” with respect to the patient’s guilt and blame, with an understanding of the “tyranny of hindsight.” The promotion of ambiguity tolerance should also play a role in coming to terms with many questions that may remain unanswered.
Optimally, clinicians should encourage patients to attend to their ongoing relationship with the deceased, particularly in the service of resolving “unfinished business,” ultimately integrating the loss into memories of the whole person. In line with this, survivors of suicide loss may be encouraged to create a narrative of the loss that incorporates both complexity and ambiguity. In the service of supporting the suicide loss survivor’s reinvestment in life, it is often helpful to facilitate their ability to anticipate and cope with triggers, such as anniversaries, birthdays, or holidays, as well as to develop and use skills for managing difficult or stigmatizing social or cultural reactions.
Any disruptions in family functioning should also be addressed. Psychoeducation about discordant grieving styles (particularly around gender) and the support of children’s grief may be helpful, and referrals to family or couples therapists should be considered as needed. Finally, the facilitation of suicide loss survivors’ creation of memorializations or rituals can help promote healing and make their loss meaningful.
Bottom Line
Losing a loved one to suicide is often a devastating and traumatic experience, but with optimal support, most survivors are ultimately able to integrate the loss and grow as a result. Understanding the suicide grief trajectory, as well as general guidelines for treatment, will facilitate healing and growth in the aftermath of suicide loss.
Related Resources
- Jordan JR, McIntosh JL. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011.
- American Association of Suicidology. http://www.suicidology.org/.
- American Foundation for Suicide Prevention. https://afsp.org/.
1. Feigelman W, Jordan JR, McIntosh JL, et al. Devastating losses: how parents cope with the death of a child to suicide or drugs. New York, NY: Springer; 2012.
2. McIntosh JL. Research on survivors of suicide. In: Stimming MT, Stimming M, eds. Before their time: adult children’s experiences of parental suicide. Philadelphia, PA: Temple University Press; 1999:157-180.
3. Sanford RL, Cerel J, McGann VL, et al. Suicide loss survivors’ experiences with therapy: Implications for clinical practice. Community Ment Health J. 2016;5(2):551-558.
4. Jordan JR, McMenamy J. Interventions for suicide survivors: a review of the literature. Suicide Life Threat Behav. 2004;34(4):337-349.
5. Survivors of Suicide Loss Task Force. Responding to grief, trauma, & distress after a suicide: U.S. national guidelines. Washington, DC: National Action Alliance for Suicide Prevention; 2015.
6. Jordan JR, McGann V. Clinical work with suicide loss survivors: implications of the U.S. postvention guidelines. Death Stud. 2017;41(10):659-672.
7. Jordan JR. Is suicide bereavement different? A reassessment of the literature. Suicide Life Threat Behav. 2001;31(1):91-102.
8. Cvinar JG. Do suicide survivors suffer social stigma: a review of the literature. Perspect Psychiatr Care. 2005;41(1):14-21.
9. U.S. Public Health Service. The Surgeon General’s call to action to prevent suicide. Washington, DC: Department of Health and Human Services; 1999.
10. Doka KJ. Disenfranchised grief: recognizing hidden sorrow. Lexington, MA: Lexington; 1989.
11. Doka KJ. Disenfranchised grief: new directions, challenges, and strategies for practice. Champaign, IL: Research Press; 2002.
12. McIntosh JL. Suicide survivors: the aftermath of suicide and suicidal behavior. In: Bryant CD, ed. Handbook of death & dying. Vol. 1. Thousand Oaks, CA: SAGE Publications; 2003:339-350.
13. Jordan, JR, McIntosh, JL. Is suicide bereavement different? A framework for rethinking the question. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:19-42.
14. Dunne EJ, McIntosh JL, Dunne-Maxim K, eds. Suicide and its aftermath: understanding and counseling the survivors. New York, NY: W.W. Norton & Co.; 1987.
15. Harwood D, Hawton K, Hope T, et al. The grief experiences and needs of bereaved relatives and friends of older people dying through suicide: a descriptive and case-control study. J Affect Disord. 2002;72(2):185-194.
16. Armour, M. Violent death: understanding the context of traumatic and stigmatized grief. J Hum Behav Soc Environ. 2006;14(4):53-90.
17. Van Dongen CJ. Social context of postsuicide bereavement. Death Stud. 1993;17(2):125-141.
18. Calhoun LG, Allen BG. Social reactions to the survivor of a suicide in the family: A review of the literature. Omega – Journal of Death and Dying. 1991;23(2):95-107.
19. Range LM. When a loss is due to suicide: unique aspects of bereavement. In: Harvey JH, ed. Perspectives on loss: a sourcebook. Philadelphia, PA: Brunner/Mazel; 1998:213-220.
20. Sveen CA, Walby FA. Suicide survivors’ mental health and grief reactions: a systematic review of controlled studies. Suicide Life Threat Behav. 2008;38(1):13-29.
21. Feigelman W, Gorman BS, Jordan JR. Stigmatization and suicide bereavement. Death Stud. 2009;33(7):591-608.
22. Shneidman ES. Foreword. In: Cain AC, ed. Survivors of suicide. Springfield, IL: Charles C. Thomas; 1972:ix-xi.
23. Jordan JR, McIntosh, JL. Suicide bereavement: Why study survivors of suicide loss? In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:3-18.
24. Agerbo E. Midlife suicide risk, partner’s psychiatric illness, spouse and child bereavement by suicide or other modes of death: a gender specific study. J Epidemiol Community Health. 2005;59(5):407-412.
25. Hedström P, Liu KY, Nordvik MK. Interaction domains and suicide: a population-based panel study of suicides in Stockholm, 1991-1999. Soc Forces. 2008;87(2):713-740.
26. Qin P, Agerbo E, Mortensen PB. Suicide risk in relation to family history of completed suicide and psychiatric disorders: a nested case-control study based on longitudinal registers. Lancet. 2002;360(9340):1126-1130.
27. Qin P, Mortensen PB. The impact of parental status on the risk of completed suicide. Arch Gen Psychiatry. 2003;60(8):797-802.
28. Neimeyer RA, Sands D. Suicide loss and the quest for meaning. In: Andriessen K, Krysinska K, Grad OT, eds. Postvention in action: the international handbook of suicide bereavement support. Cambridge, MA: Hogrefe; 2017:71-84.
29. Sands DC, Jordan JR, Neimeyer RA. The meanings of suicide: A narrative approach to healing. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:249-282.
30. Jordan JR. Principles of grief counseling with adult survivors. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:179-224.
31. Cerel J, Jordan JR, Duberstein PR. The impact of suicide on the family. Crisis. 2008;29:38-44.
32. Kaslow NJ, Samples TC, Rhodes M, et al. A family-oriented and culturally sensitive postvention approach with suicide survivors. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:301-323.
33. Grad OT, Treven M, Krysinska K. Suicide bereavement and gender. In: Andriessen K, Krysinska K, Grad OT, eds. Postvention in action: the international handbook of suicide bereavement support. Cambridge, MA: Hogrefe; 2017:39-49.
34. Kosminsky PS, Jordan JR. Attachment-informed grief therapy: the clinician’s guide to foundations and applications. New York, NY: Routledge; 2016.
35. Gutin N, McGann VL, Jordan JR. The impact of suicide on professional caregivers. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:93-111.
36. Jordan JR. Bereavement after suicide. Psychiatr Ann. 2008;38(10):679-685.
37. Jordan JR. After suicide: clinical work with survivors. Grief Matters. 2009;12(1):4-9.
38. Neimeyer, RA. Traumatic loss and the reconstruction of meaning. J Palliat Med. 2002;5(6):935-942; discussion 942-943.
39. Neimeyer R, ed. Meaning reconstruction & the experience of loss. Washington, DC: American Psychological Association; 2001.
40. Klass, D. Sorrow and solace: Neglected areas in bereavement research. Death Stud. 2013;37(7):597-616.
41. Farberow NL. The Los Angeles Survivors-After-Suicide program: an evaluation. Crisis. 1992;13(1):23-34.
42. McDaid C, Trowman R, Golder S, et al. Interventions for people bereaved through suicide: systematic review. Br J Psychiatry. 2008;193(6):438-443.
43. Groos AD, Shakespeare-Finch J. Positive experiences for participants in suicide bereavement groups: a grounded theory model. Death Stud. 2013;37(1):1-24.
44. Jordan JR. Group work with suicide survivors. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:283-300.
45. Wilson A, Marshall A. The support needs and experiences of suicidally bereaved family and friends. Death Stud. 2010;34(7):625-640.
46. McKinnon JM, Chonody J. Exploring the formal supports used by people bereaved through suicide: a qualitative study. Soc Work Ment Health. 2014;12(3):231-248.
47. Myers MF, Fine C. Touched by suicide: hope and healing after loss. New York, NY: Gotham Books; 2006.
1. Feigelman W, Jordan JR, McIntosh JL, et al. Devastating losses: how parents cope with the death of a child to suicide or drugs. New York, NY: Springer; 2012.
2. McIntosh JL. Research on survivors of suicide. In: Stimming MT, Stimming M, eds. Before their time: adult children’s experiences of parental suicide. Philadelphia, PA: Temple University Press; 1999:157-180.
3. Sanford RL, Cerel J, McGann VL, et al. Suicide loss survivors’ experiences with therapy: Implications for clinical practice. Community Ment Health J. 2016;5(2):551-558.
4. Jordan JR, McMenamy J. Interventions for suicide survivors: a review of the literature. Suicide Life Threat Behav. 2004;34(4):337-349.
5. Survivors of Suicide Loss Task Force. Responding to grief, trauma, & distress after a suicide: U.S. national guidelines. Washington, DC: National Action Alliance for Suicide Prevention; 2015.
6. Jordan JR, McGann V. Clinical work with suicide loss survivors: implications of the U.S. postvention guidelines. Death Stud. 2017;41(10):659-672.
7. Jordan JR. Is suicide bereavement different? A reassessment of the literature. Suicide Life Threat Behav. 2001;31(1):91-102.
8. Cvinar JG. Do suicide survivors suffer social stigma: a review of the literature. Perspect Psychiatr Care. 2005;41(1):14-21.
9. U.S. Public Health Service. The Surgeon General’s call to action to prevent suicide. Washington, DC: Department of Health and Human Services; 1999.
10. Doka KJ. Disenfranchised grief: recognizing hidden sorrow. Lexington, MA: Lexington; 1989.
11. Doka KJ. Disenfranchised grief: new directions, challenges, and strategies for practice. Champaign, IL: Research Press; 2002.
12. McIntosh JL. Suicide survivors: the aftermath of suicide and suicidal behavior. In: Bryant CD, ed. Handbook of death & dying. Vol. 1. Thousand Oaks, CA: SAGE Publications; 2003:339-350.
13. Jordan, JR, McIntosh, JL. Is suicide bereavement different? A framework for rethinking the question. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:19-42.
14. Dunne EJ, McIntosh JL, Dunne-Maxim K, eds. Suicide and its aftermath: understanding and counseling the survivors. New York, NY: W.W. Norton & Co.; 1987.
15. Harwood D, Hawton K, Hope T, et al. The grief experiences and needs of bereaved relatives and friends of older people dying through suicide: a descriptive and case-control study. J Affect Disord. 2002;72(2):185-194.
16. Armour, M. Violent death: understanding the context of traumatic and stigmatized grief. J Hum Behav Soc Environ. 2006;14(4):53-90.
17. Van Dongen CJ. Social context of postsuicide bereavement. Death Stud. 1993;17(2):125-141.
18. Calhoun LG, Allen BG. Social reactions to the survivor of a suicide in the family: A review of the literature. Omega – Journal of Death and Dying. 1991;23(2):95-107.
19. Range LM. When a loss is due to suicide: unique aspects of bereavement. In: Harvey JH, ed. Perspectives on loss: a sourcebook. Philadelphia, PA: Brunner/Mazel; 1998:213-220.
20. Sveen CA, Walby FA. Suicide survivors’ mental health and grief reactions: a systematic review of controlled studies. Suicide Life Threat Behav. 2008;38(1):13-29.
21. Feigelman W, Gorman BS, Jordan JR. Stigmatization and suicide bereavement. Death Stud. 2009;33(7):591-608.
22. Shneidman ES. Foreword. In: Cain AC, ed. Survivors of suicide. Springfield, IL: Charles C. Thomas; 1972:ix-xi.
23. Jordan JR, McIntosh, JL. Suicide bereavement: Why study survivors of suicide loss? In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:3-18.
24. Agerbo E. Midlife suicide risk, partner’s psychiatric illness, spouse and child bereavement by suicide or other modes of death: a gender specific study. J Epidemiol Community Health. 2005;59(5):407-412.
25. Hedström P, Liu KY, Nordvik MK. Interaction domains and suicide: a population-based panel study of suicides in Stockholm, 1991-1999. Soc Forces. 2008;87(2):713-740.
26. Qin P, Agerbo E, Mortensen PB. Suicide risk in relation to family history of completed suicide and psychiatric disorders: a nested case-control study based on longitudinal registers. Lancet. 2002;360(9340):1126-1130.
27. Qin P, Mortensen PB. The impact of parental status on the risk of completed suicide. Arch Gen Psychiatry. 2003;60(8):797-802.
28. Neimeyer RA, Sands D. Suicide loss and the quest for meaning. In: Andriessen K, Krysinska K, Grad OT, eds. Postvention in action: the international handbook of suicide bereavement support. Cambridge, MA: Hogrefe; 2017:71-84.
29. Sands DC, Jordan JR, Neimeyer RA. The meanings of suicide: A narrative approach to healing. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:249-282.
30. Jordan JR. Principles of grief counseling with adult survivors. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:179-224.
31. Cerel J, Jordan JR, Duberstein PR. The impact of suicide on the family. Crisis. 2008;29:38-44.
32. Kaslow NJ, Samples TC, Rhodes M, et al. A family-oriented and culturally sensitive postvention approach with suicide survivors. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:301-323.
33. Grad OT, Treven M, Krysinska K. Suicide bereavement and gender. In: Andriessen K, Krysinska K, Grad OT, eds. Postvention in action: the international handbook of suicide bereavement support. Cambridge, MA: Hogrefe; 2017:39-49.
34. Kosminsky PS, Jordan JR. Attachment-informed grief therapy: the clinician’s guide to foundations and applications. New York, NY: Routledge; 2016.
35. Gutin N, McGann VL, Jordan JR. The impact of suicide on professional caregivers. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:93-111.
36. Jordan JR. Bereavement after suicide. Psychiatr Ann. 2008;38(10):679-685.
37. Jordan JR. After suicide: clinical work with survivors. Grief Matters. 2009;12(1):4-9.
38. Neimeyer, RA. Traumatic loss and the reconstruction of meaning. J Palliat Med. 2002;5(6):935-942; discussion 942-943.
39. Neimeyer R, ed. Meaning reconstruction & the experience of loss. Washington, DC: American Psychological Association; 2001.
40. Klass, D. Sorrow and solace: Neglected areas in bereavement research. Death Stud. 2013;37(7):597-616.
41. Farberow NL. The Los Angeles Survivors-After-Suicide program: an evaluation. Crisis. 1992;13(1):23-34.
42. McDaid C, Trowman R, Golder S, et al. Interventions for people bereaved through suicide: systematic review. Br J Psychiatry. 2008;193(6):438-443.
43. Groos AD, Shakespeare-Finch J. Positive experiences for participants in suicide bereavement groups: a grounded theory model. Death Stud. 2013;37(1):1-24.
44. Jordan JR. Group work with suicide survivors. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge/Taylor & Francis Group; 2011:283-300.
45. Wilson A, Marshall A. The support needs and experiences of suicidally bereaved family and friends. Death Stud. 2010;34(7):625-640.
46. McKinnon JM, Chonody J. Exploring the formal supports used by people bereaved through suicide: a qualitative study. Soc Work Ment Health. 2014;12(3):231-248.
47. Myers MF, Fine C. Touched by suicide: hope and healing after loss. New York, NY: Gotham Books; 2006.

Survey-Based Priming Intervention Linked to Improved Communication with the Seriously Ill
Study Overview
Objective. To evaluate the efficacy of an intervention targeting both patients and clinicians intended to increase goals-of-care conversations.
Design. Multicenter cluster-randomized controlled trial.
Setting and participants. Clinicians (physicians or nurse practitioners) were recruited between February 2014 and November 2015 from 2 large health centers in the Pacific Northwest and were eligible if they provided primary or specialty care and had at least 5 eligible patients in their panels. Using the electronic health record (EHR) and clinic schedules, study staff identified and contacted (via mail or telephone) consecutive patients cared for by participating clinicians between March 2014 and May 2016 with the following eligibility criteria: age 18 years or older, 2 or more visits with the clinician in the last 18 months, and 1 or more qualifying conditions. Qualifying conditions included (1) metastatic cancer or inoperable lung cancer; (2) COPD with FEV1 values below 35% of that predicted or oxygen dependence, restrictive lung disease with a total lung capacity below 50% of that predicted, or cystic fibrosis with FEV1 below 30% of that predicted; (3) New York Heart Association class III or IV heart failure, pulmonary arterial hypertension, or left ventricular assist device or implantable cardioverter defibrillator implant; 4) cirrhosis or end-stage liver disease; (5) dialysis-dependent renal failure and diabetes; (6) age 75 or older with one or more life-limiting chronic illness; (7) age 90 or older; (8) hospitalization in the last 18 months with a life-limiting illness; (9) Charlson comorbidity index of 6 or higher. The qualifying criteria were selected to identify a median survival of approximately 2 years, suggesting relevance of goals-of-care discussions.
Intervention. The intervention was the patient-specific Jumpstart-Tips intervention, intended to prime clinicians and patients for a brief discussion of goals of care during a routine clinic visit. Patients in the intervention group received a survey to assess their preferences, barriers and facilitators for communication about end-of-life care. Survey responses were used to (1) generate an abstracted version of the patient’s preferences, (2) identify the most important communication barrier or facilitator, and (3) provide communication tips based on curricular materials from VitalTalk (http://vitaltalk.org) tailored to patient responses. The 1-page communication guide, called Jumpstart-Tips, was sent to clinicians 1 or 2 days prior to the target clinic visit date. Patients also received 1-page patient-specific Jumpstart-Tips forms, which summarized their survey responses and provided suggestions for having a goals-of-care conversation with the clinician. Patients in the control group completed the same surveys, but no information was provided to the patients or clinicians. Clinicians were randomly assigned in a 1:1 ratio to intervention or enhanced usual care.
Main outcome measures. The primary outcome was patient-reported occurrence of goals-of-care communication, which was evaluated using a validated dichotomous survey item. Other outcomes included clinician documentation of a goals-of-care conversation in the medical record, patient-reported quality of communication (measured using Quality of Communication questionnaire) at 2 weeks, patient reports of goal-concordant care at 3 months, and patient-reported symptoms of depression and anxiety at 3 and 6 months. All analyses included covariate adjustment for the baseline measure of the outcome and adjustment for other variables found to confound the association between randomization group and outcome.
Main results. Of 485 potentially eligible clinicians, 65 clinicians were randomized to the intervention group and 69 were randomized to the control group. Of these 132 clinicians, 124 had patients participating in the study: 537 out of 917 eligible patients enrolled, with 249 allocated to intervention and 288 to usual care.
Patients in the intervention group were more likely to report a goals-of-care conversation with their provider among all patients (74%, n = 137 vs 31%, n = 66; P n = 112 vs 28%, n = 44; P n = 140 vs 17%, n = 45; P n = 114 vs 17%, n = 34; P
Patients in the intervention group also reported higher quality ratings of goals-of-care conversations at the target visit (mean values, 4.6 v 2.1, P = 0.01, on the 4-indicator construct). Additionally, intervention members reported statistically significant higher ratings on 3 of the 7 individual quality-of-communication survey items.
Patient-assessed goal concordant care did not increase significantly overall (70% vs 57%; P = 0.08) but did increase for patients with stable goals between 3-month follow-up and last prior assessment (73% vs 57%; P = 0.03). Symptoms of depression or anxiety were not different between groups at 3 or 6 months.
Conclusion. The Jumpstart-Tips intervention was associated with an increase in patient reports and clinician documentation of goals-of-care communication. Increased patient-reported goal-concordant care among patients with stable goals was also associated with the intervention. Statistical significance was not detected for changes in depression or anxiety as a result of the intervention. The impact on goals-of-care discussion between patients and caregivers is suggestive of enhanced patient-centered care; however, further studies are needed to evaluate whether this communication is associated with changes in health care delivery.
Commentary
Previous research has shown that patients with serious illness who discuss their goals-of-care fare better in terms of quality of life and reducing intensity of care at the end-of-life [1]. However, providers often fail to or inadequately discuss goals of care with seriously ill patients [2,3]. This contributes to the lack of concordance between patient wishes, particularly related to end-of-life care, and clinical plans of care [4,5]. Addressing this gap between care provided and care desired, as well as providing high-quality, patient-centered care is needed.
Access to palliative care providers (who are trained to address these priorities) in the outpatient setting lags, despite an increase in specialists [6,7]. Thus, primary and specialty care providers in the outpatient setting are best positioned to align their care strategy with the goals of their patients. However, there have been limited results in showing that goals-of-care communication can be improved within the practice setting [8,9]. A randomized clinical trial among hospitalized seniors at the end-of-life showed an association where those who received advanced care planning with had improved quality of life, reduced care at dying, and reduced psychological distress among family [10]. However, in another randomized trial, simulation-based communication training compared with usual education among internal medicine and nurse practitioner trainees did not improve quality of communication about end-of-life care or quality of end-of-life care but was associated with a small increase in patients’ depressive symptoms [11]. A recent 2018 literature review of strategies used to facilitate the discussion of advance care planning with older adults in primary care settings identified effective interventions, including delivering education using various delivery methods, computer-generated triggers for primary care physicians (PCPs), inclusion of multidisciplinary professionals for content delivery, and patient preparation for PCP visit [12].
This article adds to the literature by demonstrating the feasibility and impact of implementing an intervention to increase communication about goals of care and end-of-life care. Further, this study highlights how communication that is bilateral, predetermined, and structured can be integrated into primary care. Strengths of the study include the use of randomization; deployment of validated survey tools; and confirmatory factor analysis to assess whether the survey variables are consistent with the hypothesized constructs. In addition, study staff were blinded when extracting data from the EHR record around discussions and documentation of goals-of-care conversations during patient visits. However, several limitations are present. There may be limited generalizability as the study was performed at low-scale, across one region as well as selection bias among clinicians participating in the study. Clinicians were not blinded of their assignment, which may have influenced their behaviors to discuss and document goals-of-care conversations.
Applications for Clinical Practice
Increasing quality communication around the end of life and understanding of a patient’s goals is important. Good communication can facilitate the development of a comprehensive treatment plan that is medically sound and concordant with the patient’s wishes and values. Clinicians and practices should consider adopting approaches to communication priming and accurate documentation, including: (1) incorporating/automating Jumpstart-Tips forms into practice (and tailoring as needed); (2) identifying similar education material that can serve as a primer for patients; (3) creating a pre-visit form for patients/caregivers to document and inform the clinician of their goals prior to the visit; (4) incorporating a standard EHR note to document and update goals-of-care discussion at each visit; and (5) more broadly encouraging (or providing training for) clinicians to practice bilateral communications with patients during visits.
—Ronald Sanchez, MPH, and Katrina F. Mateo, MPH
1. Wright AA, Zhang B, Ray A, et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 2008;300:1665–73.
2. Anderson WG, Chase R, Pantilat SZ, et al. Code status discussions between attending hospitalist physicians and medical patients at hospital admission. J Gen Intern Med 2011;26:359–66.
3. Osborn TR, Curtis JR, Nielsen EL, et al. Identifying elements of ICU care that families report as important but unsatisfactory: decision-making, control, and ICU atmosphere. Chest 2012;142:1185–92.
4. Covinsky KE, Fuller JD, Yaffe K, et al. Communication and decision-making in seriously ill patients: findings of the SUPPORT project. The Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments. J Am Geriatr Soc 2000;48:S187–93.
5. Heyland DK, Dodek P, Rocker G, et al. What matters most in end-of-life care: perceptions of seriously ill patients and their family members. CMAJ 2006;174:627–33
6. Dumanovsky T, Augustin R, Rogers M, Lettang K, Meier DE, Morrison RS. The growth of palliative care in U.S. hospitals: a status report. J Palliat Med 2016;19:8–15.
7. Dumanovsky T, Rogers M, Spragens LH, Morrison RS, Meier DE. Impact of staffing on access to palliative care in U.S. hospitals. J Palliat Med 2015;18:998–9.
8. Roze des Ordons, AL, Sharma N, Heyland DK, et al. Strategies for effective goals of care discussions and decision-making: perspectives from a multi-centre survey of Canadian hospital-based healthcare providers. BMC Palliative Care, 2015;14:38.
9. You JJ, Dodek P, Lamontagne F, et al. What really matters in end-of-life discussions? Perspectives of patients in hospital with serious illness and their families. CMAJ 2014;18:E679–E687.
10. Detering KM, Hancock AD, Reade MC, Silvester W. The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ. 2010;340:c1345.
11. Curtis JR, Back AL, Ford DW, et al. Effect of communication skills training for residents and nurse practitioners on quality of communication with patients with serious illness: a randomized trial. JAMA 2013;310:2271–81.
12. Solis GR, Mancera BM, Shen MJ. Strategies used to facilitate the discussion of advance care planning with older adults in primary care settings: A literature review. J Am Assoc Nurse Pract 2018;30:270–9.
Study Overview
Objective. To evaluate the efficacy of an intervention targeting both patients and clinicians intended to increase goals-of-care conversations.
Design. Multicenter cluster-randomized controlled trial.
Setting and participants. Clinicians (physicians or nurse practitioners) were recruited between February 2014 and November 2015 from 2 large health centers in the Pacific Northwest and were eligible if they provided primary or specialty care and had at least 5 eligible patients in their panels. Using the electronic health record (EHR) and clinic schedules, study staff identified and contacted (via mail or telephone) consecutive patients cared for by participating clinicians between March 2014 and May 2016 with the following eligibility criteria: age 18 years or older, 2 or more visits with the clinician in the last 18 months, and 1 or more qualifying conditions. Qualifying conditions included (1) metastatic cancer or inoperable lung cancer; (2) COPD with FEV1 values below 35% of that predicted or oxygen dependence, restrictive lung disease with a total lung capacity below 50% of that predicted, or cystic fibrosis with FEV1 below 30% of that predicted; (3) New York Heart Association class III or IV heart failure, pulmonary arterial hypertension, or left ventricular assist device or implantable cardioverter defibrillator implant; 4) cirrhosis or end-stage liver disease; (5) dialysis-dependent renal failure and diabetes; (6) age 75 or older with one or more life-limiting chronic illness; (7) age 90 or older; (8) hospitalization in the last 18 months with a life-limiting illness; (9) Charlson comorbidity index of 6 or higher. The qualifying criteria were selected to identify a median survival of approximately 2 years, suggesting relevance of goals-of-care discussions.
Intervention. The intervention was the patient-specific Jumpstart-Tips intervention, intended to prime clinicians and patients for a brief discussion of goals of care during a routine clinic visit. Patients in the intervention group received a survey to assess their preferences, barriers and facilitators for communication about end-of-life care. Survey responses were used to (1) generate an abstracted version of the patient’s preferences, (2) identify the most important communication barrier or facilitator, and (3) provide communication tips based on curricular materials from VitalTalk (http://vitaltalk.org) tailored to patient responses. The 1-page communication guide, called Jumpstart-Tips, was sent to clinicians 1 or 2 days prior to the target clinic visit date. Patients also received 1-page patient-specific Jumpstart-Tips forms, which summarized their survey responses and provided suggestions for having a goals-of-care conversation with the clinician. Patients in the control group completed the same surveys, but no information was provided to the patients or clinicians. Clinicians were randomly assigned in a 1:1 ratio to intervention or enhanced usual care.
Main outcome measures. The primary outcome was patient-reported occurrence of goals-of-care communication, which was evaluated using a validated dichotomous survey item. Other outcomes included clinician documentation of a goals-of-care conversation in the medical record, patient-reported quality of communication (measured using Quality of Communication questionnaire) at 2 weeks, patient reports of goal-concordant care at 3 months, and patient-reported symptoms of depression and anxiety at 3 and 6 months. All analyses included covariate adjustment for the baseline measure of the outcome and adjustment for other variables found to confound the association between randomization group and outcome.
Main results. Of 485 potentially eligible clinicians, 65 clinicians were randomized to the intervention group and 69 were randomized to the control group. Of these 132 clinicians, 124 had patients participating in the study: 537 out of 917 eligible patients enrolled, with 249 allocated to intervention and 288 to usual care.
Patients in the intervention group were more likely to report a goals-of-care conversation with their provider among all patients (74%, n = 137 vs 31%, n = 66; P n = 112 vs 28%, n = 44; P n = 140 vs 17%, n = 45; P n = 114 vs 17%, n = 34; P
Patients in the intervention group also reported higher quality ratings of goals-of-care conversations at the target visit (mean values, 4.6 v 2.1, P = 0.01, on the 4-indicator construct). Additionally, intervention members reported statistically significant higher ratings on 3 of the 7 individual quality-of-communication survey items.
Patient-assessed goal concordant care did not increase significantly overall (70% vs 57%; P = 0.08) but did increase for patients with stable goals between 3-month follow-up and last prior assessment (73% vs 57%; P = 0.03). Symptoms of depression or anxiety were not different between groups at 3 or 6 months.
Conclusion. The Jumpstart-Tips intervention was associated with an increase in patient reports and clinician documentation of goals-of-care communication. Increased patient-reported goal-concordant care among patients with stable goals was also associated with the intervention. Statistical significance was not detected for changes in depression or anxiety as a result of the intervention. The impact on goals-of-care discussion between patients and caregivers is suggestive of enhanced patient-centered care; however, further studies are needed to evaluate whether this communication is associated with changes in health care delivery.
Commentary
Previous research has shown that patients with serious illness who discuss their goals-of-care fare better in terms of quality of life and reducing intensity of care at the end-of-life [1]. However, providers often fail to or inadequately discuss goals of care with seriously ill patients [2,3]. This contributes to the lack of concordance between patient wishes, particularly related to end-of-life care, and clinical plans of care [4,5]. Addressing this gap between care provided and care desired, as well as providing high-quality, patient-centered care is needed.
Access to palliative care providers (who are trained to address these priorities) in the outpatient setting lags, despite an increase in specialists [6,7]. Thus, primary and specialty care providers in the outpatient setting are best positioned to align their care strategy with the goals of their patients. However, there have been limited results in showing that goals-of-care communication can be improved within the practice setting [8,9]. A randomized clinical trial among hospitalized seniors at the end-of-life showed an association where those who received advanced care planning with had improved quality of life, reduced care at dying, and reduced psychological distress among family [10]. However, in another randomized trial, simulation-based communication training compared with usual education among internal medicine and nurse practitioner trainees did not improve quality of communication about end-of-life care or quality of end-of-life care but was associated with a small increase in patients’ depressive symptoms [11]. A recent 2018 literature review of strategies used to facilitate the discussion of advance care planning with older adults in primary care settings identified effective interventions, including delivering education using various delivery methods, computer-generated triggers for primary care physicians (PCPs), inclusion of multidisciplinary professionals for content delivery, and patient preparation for PCP visit [12].
This article adds to the literature by demonstrating the feasibility and impact of implementing an intervention to increase communication about goals of care and end-of-life care. Further, this study highlights how communication that is bilateral, predetermined, and structured can be integrated into primary care. Strengths of the study include the use of randomization; deployment of validated survey tools; and confirmatory factor analysis to assess whether the survey variables are consistent with the hypothesized constructs. In addition, study staff were blinded when extracting data from the EHR record around discussions and documentation of goals-of-care conversations during patient visits. However, several limitations are present. There may be limited generalizability as the study was performed at low-scale, across one region as well as selection bias among clinicians participating in the study. Clinicians were not blinded of their assignment, which may have influenced their behaviors to discuss and document goals-of-care conversations.
Applications for Clinical Practice
Increasing quality communication around the end of life and understanding of a patient’s goals is important. Good communication can facilitate the development of a comprehensive treatment plan that is medically sound and concordant with the patient’s wishes and values. Clinicians and practices should consider adopting approaches to communication priming and accurate documentation, including: (1) incorporating/automating Jumpstart-Tips forms into practice (and tailoring as needed); (2) identifying similar education material that can serve as a primer for patients; (3) creating a pre-visit form for patients/caregivers to document and inform the clinician of their goals prior to the visit; (4) incorporating a standard EHR note to document and update goals-of-care discussion at each visit; and (5) more broadly encouraging (or providing training for) clinicians to practice bilateral communications with patients during visits.
—Ronald Sanchez, MPH, and Katrina F. Mateo, MPH
Study Overview
Objective. To evaluate the efficacy of an intervention targeting both patients and clinicians intended to increase goals-of-care conversations.
Design. Multicenter cluster-randomized controlled trial.
Setting and participants. Clinicians (physicians or nurse practitioners) were recruited between February 2014 and November 2015 from 2 large health centers in the Pacific Northwest and were eligible if they provided primary or specialty care and had at least 5 eligible patients in their panels. Using the electronic health record (EHR) and clinic schedules, study staff identified and contacted (via mail or telephone) consecutive patients cared for by participating clinicians between March 2014 and May 2016 with the following eligibility criteria: age 18 years or older, 2 or more visits with the clinician in the last 18 months, and 1 or more qualifying conditions. Qualifying conditions included (1) metastatic cancer or inoperable lung cancer; (2) COPD with FEV1 values below 35% of that predicted or oxygen dependence, restrictive lung disease with a total lung capacity below 50% of that predicted, or cystic fibrosis with FEV1 below 30% of that predicted; (3) New York Heart Association class III or IV heart failure, pulmonary arterial hypertension, or left ventricular assist device or implantable cardioverter defibrillator implant; 4) cirrhosis or end-stage liver disease; (5) dialysis-dependent renal failure and diabetes; (6) age 75 or older with one or more life-limiting chronic illness; (7) age 90 or older; (8) hospitalization in the last 18 months with a life-limiting illness; (9) Charlson comorbidity index of 6 or higher. The qualifying criteria were selected to identify a median survival of approximately 2 years, suggesting relevance of goals-of-care discussions.
Intervention. The intervention was the patient-specific Jumpstart-Tips intervention, intended to prime clinicians and patients for a brief discussion of goals of care during a routine clinic visit. Patients in the intervention group received a survey to assess their preferences, barriers and facilitators for communication about end-of-life care. Survey responses were used to (1) generate an abstracted version of the patient’s preferences, (2) identify the most important communication barrier or facilitator, and (3) provide communication tips based on curricular materials from VitalTalk (http://vitaltalk.org) tailored to patient responses. The 1-page communication guide, called Jumpstart-Tips, was sent to clinicians 1 or 2 days prior to the target clinic visit date. Patients also received 1-page patient-specific Jumpstart-Tips forms, which summarized their survey responses and provided suggestions for having a goals-of-care conversation with the clinician. Patients in the control group completed the same surveys, but no information was provided to the patients or clinicians. Clinicians were randomly assigned in a 1:1 ratio to intervention or enhanced usual care.
Main outcome measures. The primary outcome was patient-reported occurrence of goals-of-care communication, which was evaluated using a validated dichotomous survey item. Other outcomes included clinician documentation of a goals-of-care conversation in the medical record, patient-reported quality of communication (measured using Quality of Communication questionnaire) at 2 weeks, patient reports of goal-concordant care at 3 months, and patient-reported symptoms of depression and anxiety at 3 and 6 months. All analyses included covariate adjustment for the baseline measure of the outcome and adjustment for other variables found to confound the association between randomization group and outcome.
Main results. Of 485 potentially eligible clinicians, 65 clinicians were randomized to the intervention group and 69 were randomized to the control group. Of these 132 clinicians, 124 had patients participating in the study: 537 out of 917 eligible patients enrolled, with 249 allocated to intervention and 288 to usual care.
Patients in the intervention group were more likely to report a goals-of-care conversation with their provider among all patients (74%, n = 137 vs 31%, n = 66; P n = 112 vs 28%, n = 44; P n = 140 vs 17%, n = 45; P n = 114 vs 17%, n = 34; P
Patients in the intervention group also reported higher quality ratings of goals-of-care conversations at the target visit (mean values, 4.6 v 2.1, P = 0.01, on the 4-indicator construct). Additionally, intervention members reported statistically significant higher ratings on 3 of the 7 individual quality-of-communication survey items.
Patient-assessed goal concordant care did not increase significantly overall (70% vs 57%; P = 0.08) but did increase for patients with stable goals between 3-month follow-up and last prior assessment (73% vs 57%; P = 0.03). Symptoms of depression or anxiety were not different between groups at 3 or 6 months.
Conclusion. The Jumpstart-Tips intervention was associated with an increase in patient reports and clinician documentation of goals-of-care communication. Increased patient-reported goal-concordant care among patients with stable goals was also associated with the intervention. Statistical significance was not detected for changes in depression or anxiety as a result of the intervention. The impact on goals-of-care discussion between patients and caregivers is suggestive of enhanced patient-centered care; however, further studies are needed to evaluate whether this communication is associated with changes in health care delivery.
Commentary
Previous research has shown that patients with serious illness who discuss their goals-of-care fare better in terms of quality of life and reducing intensity of care at the end-of-life [1]. However, providers often fail to or inadequately discuss goals of care with seriously ill patients [2,3]. This contributes to the lack of concordance between patient wishes, particularly related to end-of-life care, and clinical plans of care [4,5]. Addressing this gap between care provided and care desired, as well as providing high-quality, patient-centered care is needed.
Access to palliative care providers (who are trained to address these priorities) in the outpatient setting lags, despite an increase in specialists [6,7]. Thus, primary and specialty care providers in the outpatient setting are best positioned to align their care strategy with the goals of their patients. However, there have been limited results in showing that goals-of-care communication can be improved within the practice setting [8,9]. A randomized clinical trial among hospitalized seniors at the end-of-life showed an association where those who received advanced care planning with had improved quality of life, reduced care at dying, and reduced psychological distress among family [10]. However, in another randomized trial, simulation-based communication training compared with usual education among internal medicine and nurse practitioner trainees did not improve quality of communication about end-of-life care or quality of end-of-life care but was associated with a small increase in patients’ depressive symptoms [11]. A recent 2018 literature review of strategies used to facilitate the discussion of advance care planning with older adults in primary care settings identified effective interventions, including delivering education using various delivery methods, computer-generated triggers for primary care physicians (PCPs), inclusion of multidisciplinary professionals for content delivery, and patient preparation for PCP visit [12].
This article adds to the literature by demonstrating the feasibility and impact of implementing an intervention to increase communication about goals of care and end-of-life care. Further, this study highlights how communication that is bilateral, predetermined, and structured can be integrated into primary care. Strengths of the study include the use of randomization; deployment of validated survey tools; and confirmatory factor analysis to assess whether the survey variables are consistent with the hypothesized constructs. In addition, study staff were blinded when extracting data from the EHR record around discussions and documentation of goals-of-care conversations during patient visits. However, several limitations are present. There may be limited generalizability as the study was performed at low-scale, across one region as well as selection bias among clinicians participating in the study. Clinicians were not blinded of their assignment, which may have influenced their behaviors to discuss and document goals-of-care conversations.
Applications for Clinical Practice
Increasing quality communication around the end of life and understanding of a patient’s goals is important. Good communication can facilitate the development of a comprehensive treatment plan that is medically sound and concordant with the patient’s wishes and values. Clinicians and practices should consider adopting approaches to communication priming and accurate documentation, including: (1) incorporating/automating Jumpstart-Tips forms into practice (and tailoring as needed); (2) identifying similar education material that can serve as a primer for patients; (3) creating a pre-visit form for patients/caregivers to document and inform the clinician of their goals prior to the visit; (4) incorporating a standard EHR note to document and update goals-of-care discussion at each visit; and (5) more broadly encouraging (or providing training for) clinicians to practice bilateral communications with patients during visits.
—Ronald Sanchez, MPH, and Katrina F. Mateo, MPH
1. Wright AA, Zhang B, Ray A, et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 2008;300:1665–73.
2. Anderson WG, Chase R, Pantilat SZ, et al. Code status discussions between attending hospitalist physicians and medical patients at hospital admission. J Gen Intern Med 2011;26:359–66.
3. Osborn TR, Curtis JR, Nielsen EL, et al. Identifying elements of ICU care that families report as important but unsatisfactory: decision-making, control, and ICU atmosphere. Chest 2012;142:1185–92.
4. Covinsky KE, Fuller JD, Yaffe K, et al. Communication and decision-making in seriously ill patients: findings of the SUPPORT project. The Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments. J Am Geriatr Soc 2000;48:S187–93.
5. Heyland DK, Dodek P, Rocker G, et al. What matters most in end-of-life care: perceptions of seriously ill patients and their family members. CMAJ 2006;174:627–33
6. Dumanovsky T, Augustin R, Rogers M, Lettang K, Meier DE, Morrison RS. The growth of palliative care in U.S. hospitals: a status report. J Palliat Med 2016;19:8–15.
7. Dumanovsky T, Rogers M, Spragens LH, Morrison RS, Meier DE. Impact of staffing on access to palliative care in U.S. hospitals. J Palliat Med 2015;18:998–9.
8. Roze des Ordons, AL, Sharma N, Heyland DK, et al. Strategies for effective goals of care discussions and decision-making: perspectives from a multi-centre survey of Canadian hospital-based healthcare providers. BMC Palliative Care, 2015;14:38.
9. You JJ, Dodek P, Lamontagne F, et al. What really matters in end-of-life discussions? Perspectives of patients in hospital with serious illness and their families. CMAJ 2014;18:E679–E687.
10. Detering KM, Hancock AD, Reade MC, Silvester W. The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ. 2010;340:c1345.
11. Curtis JR, Back AL, Ford DW, et al. Effect of communication skills training for residents and nurse practitioners on quality of communication with patients with serious illness: a randomized trial. JAMA 2013;310:2271–81.
12. Solis GR, Mancera BM, Shen MJ. Strategies used to facilitate the discussion of advance care planning with older adults in primary care settings: A literature review. J Am Assoc Nurse Pract 2018;30:270–9.
1. Wright AA, Zhang B, Ray A, et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 2008;300:1665–73.
2. Anderson WG, Chase R, Pantilat SZ, et al. Code status discussions between attending hospitalist physicians and medical patients at hospital admission. J Gen Intern Med 2011;26:359–66.
3. Osborn TR, Curtis JR, Nielsen EL, et al. Identifying elements of ICU care that families report as important but unsatisfactory: decision-making, control, and ICU atmosphere. Chest 2012;142:1185–92.
4. Covinsky KE, Fuller JD, Yaffe K, et al. Communication and decision-making in seriously ill patients: findings of the SUPPORT project. The Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments. J Am Geriatr Soc 2000;48:S187–93.
5. Heyland DK, Dodek P, Rocker G, et al. What matters most in end-of-life care: perceptions of seriously ill patients and their family members. CMAJ 2006;174:627–33
6. Dumanovsky T, Augustin R, Rogers M, Lettang K, Meier DE, Morrison RS. The growth of palliative care in U.S. hospitals: a status report. J Palliat Med 2016;19:8–15.
7. Dumanovsky T, Rogers M, Spragens LH, Morrison RS, Meier DE. Impact of staffing on access to palliative care in U.S. hospitals. J Palliat Med 2015;18:998–9.
8. Roze des Ordons, AL, Sharma N, Heyland DK, et al. Strategies for effective goals of care discussions and decision-making: perspectives from a multi-centre survey of Canadian hospital-based healthcare providers. BMC Palliative Care, 2015;14:38.
9. You JJ, Dodek P, Lamontagne F, et al. What really matters in end-of-life discussions? Perspectives of patients in hospital with serious illness and their families. CMAJ 2014;18:E679–E687.
10. Detering KM, Hancock AD, Reade MC, Silvester W. The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ. 2010;340:c1345.
11. Curtis JR, Back AL, Ford DW, et al. Effect of communication skills training for residents and nurse practitioners on quality of communication with patients with serious illness: a randomized trial. JAMA 2013;310:2271–81.
12. Solis GR, Mancera BM, Shen MJ. Strategies used to facilitate the discussion of advance care planning with older adults in primary care settings: A literature review. J Am Assoc Nurse Pract 2018;30:270–9.
Approaches to Enhancing Patient-Centered Communication In Caring For Hispanic/Latino Patients With Diabetes
From the University of Texas at El Paso, El Paso, TX.
Abstract
- Objective: To demonstrate the applied use of recommended cultural competency communication tools.
- Methods: An overview of several cultural competency tools is presented and vignettes are used to demonstrate the use of these tools with Hispanic patients with diabetes.
- Results: Three communication mnemonic instruments, ie, BELIEF, ETHNIC, and BATHE, may be useful for engaging health professionals in patient-centered communication with their Hispanic patients and shared decision making. Health professionals can also employ nonjudgmental probing as part of engaging patients in setting diabetes treatment goals.
- Conclusion: Health professionals are in an influential position to leverage a patient- and culture-centered communication style to improve communication with Hispanic patients. Using mnemonic tools can help facilitate this communication and improve health professionals’ understanding on how cultural and social factors influence diabetes management in this population.
Key words: Hispanic/Latino; diabetes; patient-centered communication; cultural-competency.
The 2017 American Diabetes Association (ADA) Standards of Medical Care recommend that health professionals engage in a patient-centered communication style with patient to facilitate shared decision-making and improve diabetes outcomes. The ADA defines patient-centered communication as “a style that uses active listening, elicits patient preferences and beliefs, and assesses literacy, numeracy, and potential barriers to care” [1]. One of the main goals of using patient-centered communication is to create a collaborative, personal, and non-judgmental relationship with patients. These guidelines, however, provide less direction on the type of communication skills training that would facilitate this type of communication, particularly as it relates to ethnic/racial minority groups most at risk for diabetes and related complications.
The US Hispanic/Latino population, in particular, is a group that is burdened by the diabetes epidemic, with a prevalence that is 130% higher than non-Hispanic whites [2]. It is widely known that certain social determinants of health, like socioeconomic status, social injustices, poor access to health care, food insecurity, or living in environments that do not support health behaviors, all contribute to health disparities for Hispanics/Latinos [3]. Understanding how Hispanics/Latinos cope with these social determinants of health is important for health care professionals, and a patient-centered communication style is an ideal approach for active listening and eliciting information about the social barriers/challenges that may influence diabetes self-care. However, there is some evidence that suggests this approach is not fully used by health care professionals when communicating with Hispanics/Latinos with diabetes, and Hispanics/Latinos continue to be more likely to experience disparities in the quality of diabetes care they receive compared to non-Hispanic whites [4–9]. One of the identified contributors to these disparities is the poor communication between physicians and Hispanic/Latino patients [10–16]. Given that health care professionals are the primary source of health care and diabetes information for Hispanics/Latinos, it is important for health professionals to enhance their patient-centered communications skills to improve the quality of care that is provided to this population [12].
Cultural Competence and Patient-Centered Communication
Not all health professional communication skills are perceived as unsatisfactory by Hispanic/Latino patients with diabetes. In fact, Hispanics/Latinos report a positive provider-patient clinical interaction when health professionals display cultural competency skills [15,17–20]. Moreover, evidence suggest that Hispanic/Latino patients with diabetes reported better quality of care and improved self-management behaviors with a culturally competent provider [18–20]. Cultural competency is described as “understanding and responding effectively to the cultural and linguistic needs brought by the patient to the health care encounter” and “valuing diversity, provider self-assessment, managing dynamics of differences, acquiring and institutionalizing knowledge, and adapting to diversity and the cultural context of individuals served” [9,11,12]. One approach for gaining cultural competency skills is to understand how the disease process is conceptualized within a culture and how that influences a patient’s own theory about their disease etiology, prognosis, and outcome [21]. This approach is known as culture-centered in the health communications literature and may be useful when communicating with Hispanic/Latino patients with diabetes because there is extensive literature describing unique indigenous Latin American explanatory models for diabetes [22–26].
Language Discordance in Physician-Patient Communication
The process of patient-physician communication includes “attending to one another and begin interpreting one another’s verbal and nonverbal” interactions [9]. A conventional assumption regarding the disparities in diabetes care quality for Hispanic/Latino patients is that it stems from language discordant patient-physician interactions, which result in errors in the provision of diabetes information and treatment instructions regarding medications and self-care behaviors [9]. While language is a contributing factor, the US Census reports that over half of US Hispanics/Latinos are bilingual and speak English “very well” [27]. Thus, other underlying mechanisms must be contributing to patient-physician miscommunication and suboptimal diabetes outcomes. Moreover, the findings from studies of patient-physician language concordance and diabetes management are inconsistent. For example, language concordance between Hispanic/Latino patients and physicians is associated with improvement in HbA1c but not self-care behaviors (ie, healthy eating, self-monitoring, medicine adherence, exercise) [20]. Thus, there is need to move beyond spoken language to address elements of interpersonal communication around diabetes care through addressing cultural health beliefs and explanatory models of diabetes.
Cultural Explanatory Models of Diabetes
Explanatory models for diabetes among Hispanics/Latinos are diverse and often include a biomedical framework (eg, obesity, unhealthy eating, sedentary lifestyle, genetics); however, there is one unique indigenous belief that continues to be held within this population. Specifically, there is a cultural belief that diabetes is caused by strong or negative emotions, like fright sickness (susto), stress (estres), anger (coraje), or nerves (nervios) [22–26]. Although this cultural belief has been in existence long before scientific evidence has shown the bi-directional relationship between stress/depression and diabetes, the integration of emotions in diabetes self-management in patient-provider communication has not been standardized [28–31]. Health professionals’ interest in how patients view their own disease process may help build rapport with patients. Enhancing health professionals’ cultural competency skills can be a critical first step for improving patient-provider communication. For instance, it can (1) present an opportunity to integrate cultural belief systems into diabetes care for Hispanics/Latinos, (2) open the door for other important conversations about Hispanic/Latino patients’ psychosocial and familial environment and identify barriers or motivators in diabetes self-management, and (3) build rapport and trust between the health professional and patient.
Additionally, inquiring about emotional beliefs or emotions about diabetes in general can help improve the patient-provider relationship, giving Hispanic/Latino patients a sense that their provider cares about their feelings and emotional well-being. For example, in a study conducted by Concha et al, a Hispanic/Latino male patient with diabetes expresses his appreciation of his doctor for attending to his emotional problems and suggests that his diabetes is in control because of the encouragement he receives from the doctor [22].
…I believe the doctors..can encourage one with ..diabetes… I am very grateful to God before anything that till today I have my sugar controlled. I am a diabetic, but controlled. And Dr. [name omitted], he’s a blessing from God. He knows my body like my mother….Because whatever little thing, he attends to me, he gives me a lot of encouragement with my emotional problems. He sent me to a counselor, I have a specialist for my problem with my urinary tracts. I have attention, I have all the attention from the doctor…
Inquiring about emotional well-being may also be beneficial because Hispanics/Latinos with diabetes have reported that they would feel more comfortable talking to a professional about personal problems compared to Hispanics/Latinos without diabetes [32]. Having a physical illness may provide an opportunity for these patients to discuss stress or depression in tandem with diabetes to diminish any possible stigma or shame associated with having a mental health problem. It is important for health care providers to be aware of emotional or social problems that may be negatively influencing diabetes self-care behaviors.
Models of Effective Cross-Cultural Communication
Cultural competency training for health professionals is one strategy for reducing health disparities and ensuring that racial/ethnic populations receive “equitable, effective, and culturally appropriate clinical care” [9,11,12,33]. The Association of American Medical Colleges’ guide for cultural competence education in medical school cites several models of effective cross-cultural communication for physicians and/or physician assistants [34]. I describe 3 communication tools below that may help health care professionals initiate conversations and aid them in understanding how to better manage sociocultural and environmental issues that may impede patients’ ability to manage diabetes. For each tool, a vignette is offered that illustrates how the tool may be used in communicating with Hispanic/Latino patients.
BELIEF
The BELIEF instrument (Dobbie 2003) is a teaching tool designed to elicit patients’ health beliefs and to assist preclinical medical students or medical professionals in understanding how explanatory models of a disease influence patient engagement in care. The BELIEF instrument is straightforward and can be easily implemented into clinical case vignettes and or role-play as part of cultural competency training [35]. The specific questions corresponding to the BELIEF prompts are
- B: Beliefs about health (What caused your illness/problem?)
- E: Explanation (Why did it happen at this time?)
- L: Learn (Help me understand your belief/opinion)
- I: Impact (How is this illness/problem impacting your life?)
- E: Empathy (This must be very hard for you)
- F: Feelings (How are you feeling about it?)
Vignette 1
The following vignette is a conversation between a Spanish-speaking Hispanic women, a language interpreter, and medical professional. The patient, Mrs. Chavez, has come into the clinic for the third time after experiencing symptoms due to hypoglycemia. Mrs. Chavez believes stress may have something to do with her hypoglycemia but is not quite sure how. By using the BELIEF mnemonic, the medical professional is able to ask more about the stress that led into a discussion about how stress actually influenced her eating and medication intake behaviors. Through this probing, the medical professional was able to identify the possible cause of her hypoglycemia and work with Mrs. Chavez on finding a solution every time she experiences the stressful event. The vignette also demonstrates how interpreters may share cultural information that may clarify problems.
Medical Professional: Mrs. Chavez, I see you are here again for hypoglycemia. Can you tell me what has happened? Do you have your medications with you today?
Interpreter: Sra. Chavez, entiendo que está aquí nuevamente por hipoglucemia. ¿Puedes decirme qué ha pasado? ¿Tiene sus medicamentos con usted hoy?
Mrs. Chavez: Si, me ha sentido débil y mareado.
Interpreter: Yes I have felt faint and dizzy?
Medical Professional: Have you been taking your metformin as prescribed?
Interpreter: ¿Ha estado tomando su metformin según lo recetado?
Mrs. Chavez: Si (YES).
Medical Professional: We might have to consider adjusting your dosage.
Interpreter: Es posible que tengamos que considerar ajustar su dosis.
Mrs. Chavez privately to the Interpreter: ¿no es posible que las emociones o nervios puedan causar algo? He escuchado que este puede ser el problema?
Interpreter to Mrs. Chavez: Déjame preguntarle al doctor, si?
Let me ask the doctor, yes? (Mrs. Chavez, nods in agreement)
Interpreter to Medical Professional: She is asking if emotions or nervousness could be the cause. She has heard that this could be the problem.
Medical Profesional to Interpreter: What does she mean?
Interpreter: There is a cultural belief that stress or nerves can cause diabetes or affect diabetes. You may want to ask about this.
Medical Professional: Yes emotions like stress can cause changes in you glucose. (Beliefs) Do you believe that some emotions are causing your hypoglycemia?
Interpreter: Sí, las emociones como el estrés pueden provocar cambios en la glucosa. ¿Crees que algunas emociones están causando tu hipoglucemia?
Mrs. Chavez: (Shrugs shoulders).
Medical Professional: I see here in your records, that the other two times you had hypoglycemica were 1 month and 3 months ago. (Beliefs) What do you think caused these events and (Explanation) why do you think it happened during these times?
Interpreter: Veo aquí en sus registros que las otras dos veces que tuvo hipoglucemia fueron hace 1 mes y 3 meses. ¿Qué crees que causó estos eventos y por qué crees que sucedió durante estos tiempos?
Mrs. Chavez: Pues, no sé.
Interpreter: Well I don’t know.
Medical Professional: (Learn) Help me understand what you think happened 3 and 1 month ago and this month that may have caused your glucose to drop. What was happening emotionally during these times? Do you remember?
Interpreter: Ayúdame a entender lo que piensas que sucedió hace 3 y 1 meses y este mes, puede haber causado que tu glucosa baje. ¿Qué estaba pasando emocionalmente durante este tiempo? ¿Te acuerdas?
Mrs. Chavez: Hmm. Pues, hace 3 meses fui a visitar a mi madre y hace 1 meses fui a visitar a mi hermano al norte.
Interpreter: Hmm. Well 3 months ago I went to visit my mother and 1 months ago I went to visit my brother up north.
Medical Professional: (Learn) How were those trips for you. Did you have fun? What types of emotions were you feeling during these trips?
Interpreter: ¿Cómo fueron esos viajes para ti? ¿Te divertiste? ¿Qué tipo de emociones sentías durante estos viajes?
Mrs. Chavez: Pues, yo estaba muy estresado durante mis viajes.
Interpreter: Well, I was very stressed during my trips.
Medical Professional: (Learn) Would you like to share why you were stressed? What was happening for you to feel so stressed?
Interpreter: ¿Te gustaría compartir por qué estabas estresado? ¿Qué estaba pasando para que te sientas tan estresado?
Mrs. Chavez: Bueno, tenemos muchos problemas familiares y conflictos. Hay muchos argumentos familiares y se vuelve estresante.
Interpreter: Well we have a lot of family problems and conflict. There are a lot of family arguments and it gets stressful.
Medical Professional: (Impact) How do you think this has affected your glucose?
Interpreter: ¿Cómo crees que esto ha afectado tu glucosa?
Mrs. Chavez: No lo sé.
Interpreter: I don’t know.
Medical Professional: (Learn) Do you think the stress maybe led you to forget to take your medication or affected your eating?
Interprter: ¿Crees que el estrés puede llevarte a olvidarte de tomar tu medicación o afectó su alimentación?
Mrs. Chavez: Pues si y no comí. Estaba demasiado estresado para comer. Raramente comí mientras estaba allí. Estaba tan estresado que no tenía apetito.
Interpreter: Well yes and I didn’t eat. I was too stressed to eat. I rarely ate while I was there. I was so stressed i did not have an appetite.
Medical Professional: (Empathy) Mrs. Chavez, that must have been very hard for you. I’m sorry you have had to feel this way. (Feelings) Is this how you feel everytime you visit your family?
Interpreter: Sra. Chávez, eso debe haber sido muy difícil para usted. Lamento que hayas tenido que sentirte de esta manera. ¿Es así como te sientes cada vez que visitas a tu familia?
Mrs. Chavez: Sí, todos se involucran en los problemas familiares y es muy estresante visitarlos, pero tengo que ir a ayudar a mi madre porque mi hermano está enfermo y no puede ayudarla. Soy el único que está cerca y mis otros hermanos discuten sobre lo que debería hacer. Tengo que estar ahí. Tengo que visitar.
Interpreter: Yes, everyone gets involved in the family problems and it is very stressful to visit but I have to go to help my mom because my brother is sick and can’t help her. I’m the only one close by and my other siblings argue about what I should do. I have to be there. I have to visit.
Medical Profesional: (Empathy) Yes, that must be very difficult for you. Okay, now I understand what is happening. Your visits are necessary but it seems like the stress is affecting your eating patterns and whether you remember to take your metformin. How do you feel if we come up with a plan for when you visit your family now that we know what might be causing your hypoglycemia? Do you think it is a good idea to take high glucose snacks or candy and have them with you on the trip so when you feel dizzy or faint you can eat them?
Interpreter: Sí, eso debe ser muy difícil para ti. De acuerdo, ahora entiendo lo que está pasando. Sus visitas son necesarias, pero parece que el estrés está afectando sus patrones de alimentación y si recuerda tomar su metformina. ¿Cómo se siente si elaboramos un plan para su familia ahora que sabemos lo que podría estar causando su hipoglucemia? ¿Cree que es una buena idea tomar refrigerios con alto contenido de glucosa o dulces y llevarlos consigo durante el viaje para que cuando se sienta mareado o desmayado pueda comerlos?
Mrs. Chavez: Sí, por supuesto. Ni siquiera me di cuenta de eso hasta ahora que hablamos sobre eso. Tienes razón, no he estado comiendo bien cuando lo visito. Me siento terrible cuando estoy allí como si quisiera desmayarme.
Interpreter: Yes of course. I didn’t even really realize that until now that we talked about it. You are right, I haven’t been eating right when I visit. I feel terrible when I am there like I want to faint.
Medical Professional: Mrs. Chavez, sometimes it is helpful to talk about our stress and problems we encournter in life, just to talk through it. Is this something you would be interested in? If so, we can arrange for you to come talk to the social worker.
Interpreter: Sra. Chavez, a veces es útil hablar sobre nuestro estrés y los problemas que alegramos en la vida, solo para hablar sobre ello. ¿Esto es algo que te interesaría? Si tu quieres, podemos hacer arreglos para que vengas a hablar con el trabajador social.
Mrs. Chavez: Tal vez, no estoy seguro, pero tal vez
Interpreter: Maybe, I’m not sure but maybe.
Medical Professional: Okay, you let me know if this is something you would like to do. You can call and let us know and I’ll ask again during our next visit and see how you are dealing with the stress when you visit your family.
Interpreter: De acuerdo, dime si esto es algo que te gustaría hacer. Puede llamar y dejarnos saber, y volveré a preguntar durante nuestra próxima visita y verá cómo lidia con el estrés cuando visita a su familia.
ETHNIC
The ETHNIC interviewing tool (Levin SJ 2000) can be used to explore cross cultural issues and facilitate collaboration during clinical encounters and is designed for clinical students or health professionals permitted to diagnose and provide therapeutic interventions [36]. The specific questions corresponding to the ETHNIC prompts:
- E: Explanation (How do you explain your illness?)
- T: Treatment (What treatment have you tried?)
- H: Healers (Have you sought any advice from folk healers?)
- N: Negotiate (mutually acceptable options)
- I: Intervention (agreed on)
- C: Collaboration (with patient, family, and healers)
Vignette 2
The second vignette is a discussion between a conscientious patient, Mrs. Rodriguez, and her doctor. Mrs. Rodriguez is determined to keep her glucose levels within optimal range by eating healthy and living a natural lifestyle. Included in her natural lifestyle is the use of herbs from her garden and herbal supplements sold to her by her neighbor. Because her numbers have been in the normal range she discontinues her prescribed medication to rely on natural products. However, a trip with family members interrupts her daily routine, which is replaced with fast foods and little rest. Upon returning from her trip her glucose levels increase and she cannot decrease her glucose numbers.
Medical Professional: Good morning Mrs. Rodriguez. I see you are here today for high blood sugar because of your diabetes. (Explanation) Can you share why you think you have recently had higher numbers than normal?
Mrs. Rodriguez: Good morning Doctor. Yes, I am usually very good with my numbers but lately they have gone up and I know why.
Medical Professional: Yes, that is good that you have had your glucose managed. (Explanation) What has caused your numbers to go up Mrs. Rodriguez?
Mrs. Rodriguez: All this American food. I went on a trip to visit my daughter and all we did was eat out, hamburgers, fast food restaurants. They do not cook at home and we were always doing something so I could not cook. It was terrible, all we did was keep busy out and about, I was tired. I spent so much money on food that has chemicals. Look at me now. I can’t seem to get my numbers down.
Medical Professional: Oh, I understand. Yes, a trip can sometimes mess with our routine. (Treatment) Since you have been good at managing your glucose in the past what have you been doing now to get your glucose in normal range?
Mrs. Rodriguez: Well I have been doing the same thing I have always been doing. Eating healthy, resting, gardening, and praying.
Medical Professional: Gardening? That’s really nice. What do you garden?
Mrs. Rodriguez: Oh I love gardening. I plant all types of herbs, vegetables, flowers.
Medical Professional: That is so good Mrs. Rodriguez. I wish I had more time to garden. Do you use your own vegetable and herbs when you cook?
Mrs. Rodriguez: Haha. Yes of course. That is why my sugar was fine before I went on this trip. I rely on my garden to keep me healthy.
Medical Professional: There are so many herbs that are helpful for diabetes. (Treatment) Do you use any to help with your diabetes?
Mrs. Rodriguez: Well yes, in fact, I do. I know you doctors don’t like us to use our herbs but I do. And that was what keeps my sugars normal.
Medical Professional: Oh Mrs. Rodriguez, yes sometimes you hear doctors say this but some herbs are helpful. We just like to know what other things our patients do so we know how to make sure your medications work with certain herbs. (Treatment) I know many people use nopal (cactus), do you eat nopal?
Mrs. Rodriguez: ¿Como no? (of course). I eat them all the time. I make my morning licuado (drink); a little bit of parsley, oregano, oatmeal, lemon, nopal mixed with milk and yogurt.
Medical Professional: (Treatment) Sounds good, what else do you use?
Mrs. Rodriguez: Oh you know other things. Apple cider, cinnamon, cayenne.
Medical Professional: All from your garden?
Mrs. Rodriguez: Yes.
Medical Professional: (Treatment) Do you use any type of herbal supplements from stores or online?
Mrs. Rodriguez: My neighbor sells supplements specifically for diabetes. I started to use a natural supplement with cinnamon, vitamin D, and fish oil. All very natural.
Medical Professional: (Healer) Oh does your neighbor also have diabetes?
Mrs. Rodriguez: No, she sells products. But she sells to many people with diabetes and the supplement works. We get together and she tells us about how they work.
Medical Professional: Do you know the name of this supplement Mrs. Rodriguez?
Mrs. Rodriguez: Oh, gluco…something, it has a heart in the name. But I read the ingredients and it has only natural ingredients. (An FDA banned supplement for false claims)
Medical Professional: Oh I see. I may be familiar with that. Can you bring the supplement along with the medications I have prescribed? I just want to make sure there is not interaction between the two. To get your glucose back to normal I want to make sure we think of every possible situation that could be causing your high numbers. (Treatment) How have you been taking the supplement and the prescribed medications?
Mrs. Rodriguez: Well, I have not refilled your prescription. I was doing so well with my numbers, I’d rather go natural than take all those chemicals.
Medical Professional: Oh, I see Mrs. Rodriguez. Okay, you have done so well controlling your glucose before your trip and now we are in a situation where your numbers are not coming down so let’s try to figure this out. I’d like to learn more about this supplement, so for our next visit can you bring in your supplements so I can take a look at it? (Negotiate) We can then talk about the benefits or cautions. But in the meantime I’d like you to refill your medication and take as followed to see if that helps your sugars. (Negotiate) What do you think? Is this possible?
Mrs. Rodriguez: Oh Doctor, I just don’t like taking chemicals.
Medical Professional: I understand Mrs. Rodriguez. You did take them to start when you first came in for diabetes, is this correct?
Mrs. Rodriguez: Well yes but, I slowly got off them.
Medical Professional: I know it’s difficult to take medications every day but they can help in addition to your healthy eating. I know you are concerned about medications but for now we have to focus on getting your numbers down or your diabetes could become worse and we don’t want you to get there. Do you agree? (Negotiating process)
Mrs. Rodriguez: Well, I am concerned about my numbers.
Medical Professional: (Intervention) Okay well let’s try to get back to where you were before the trip. Let’s get you back on the medication and let’s see if this helps. (Negotiate) For the next visit would you be willing to bring any supplements you are taking along with the medication? (Collaboration) We can talk about the benefits and cautions for the medications and supplements. How does this sound?
Mrs. Rodriguez: Well, I am here to fix my numbers. I have everything I take in a box so I can bring that.
Medical Professional: Yes that would be great. (Collaboration) We can both talk about your daily routine and what have you learned about the supplement, any information or papers that you have, in addition to the medication I prescribed.
Mrs. Rodriguez: Yes I can do that.
Medical Professional: Thank you Mrs. Rodriguez. (Intervention) Also, I’ll have the nurse call you today or tomorrow and you can give her the name of the supplement and she’ll make sure the drug store has a refill for you. Would this work for you Mrs. Rodriguez?
Mrs. Rodriguez: Yes Doctor. You can call me. I’ll have the list ready.
BATHE
Unlike the BELIEF and ETHNIC instruments, the BATHE mnemonic (Lieberman 1999)
- B: Background (What is going on in your life?)
- A: Affect (How do you feel about what is going on?)
- T: Trouble (What troubles you most?)
- H: Handling (How are you handling that?)
- E: Empathy (This must be very difficult for you)
Vignette 3
The last vignette features Mr. Gonzalez, who typically shows a positive outlook on life when visiting his doctor. He is a patient who would not necessarily discuss his emotions if not asked specific questions about his emotional well-being.
Medical Professional: Hello Mr. Gonzalez. (Background) How are you doing today? What’s new? What’s going on in your life lately?
Mr. Gonzalez: Hey, Doctor! I’m good you know just living day to day.
Medical Professional: Good. (Affect) So how is your diabetes treating you day to day? How are you feeling with life and managing your diabetes?
Mr. Gonzalez: Ah well you know, just dealing with it as best as I can.
Medical Professional: Ah okay. As best as you can. (Troubles) What troubles you the most about managing diabetes?
Mr. Gonzalez: Well you know the aches and pains. But what can I do.
Medical Professional: (Affect) How do you feel about those aches and pains?
Mr. Gonzalez: Well it does limit me. I can’t move as well as I use to.
Medical Professional: (Handling) Hmm. I see. How are you handling those aches and pains? What are you doing to relieve it?
Mr. Gonzalez: I do my best with pain cream.
Medical Professional: (Empathy) Pains and aches, that must be difficult. (Affect) How do the aches and pains make you feel?
Mr. Gonzalez: Ahh, Doc, it’s not the same. You know I can’t do the same things anymore.
Medical Professional: (Background) What do you mean? What is not the same anymore?
Mr. Gonzalez: This diabetes, I’m not the same person. I use to be able to be there for my family and community and now I feel like I can’t be there for them the way I use to. I use to be the strong one for my family, helping those in need, and now I’m limited, my body is limited.
Medical Professional: (Affect) How do you feel about that? How does it make you feel emotionally and physically?
Mr. Gonzalez: Bad. I feel bad about it.
Medical Professional: Bad emotionally or physically?
Mr. Gonzalez: Both
Medical Professional: I see. (Handling) How are you dealing with the emotional part of it?
Mr. Gonzalez: I don’t know. I don’t know how.
Medical Professional: (Empathy) Dealing with diabetes and how it makes your body feel can be very emotionally distressing. It is common to feel this way but I want to make sure we also work on how you feel emotionally or how your emotions is affecting your diabetes.
Conclusion
Three mnemonic tools have been suggested to initiate patient-centered and culture-centered communication with patients. Beyond the use of these instruments, there are 2 key skills that are essential for engaging a Hispanic/Latino patient. The first is a non-judgmental, warm communication approach, and the second is astute probing. Once when I was interpreting for a Spanish-speaking Hispanic/Latino patient and English-speaking doctor, the patient expressed to me that she felt that the medical professionals “tienen una cultura fría” (“have a cold culture”), and she did not feel comfortable sharing more about herself because of it. It is also important for medical professionals to be aware of a patient’s doublespeak as a way to share enough information but not all information to keep from being judged by medical professionals. Thus, non-judgmental probing can uncover important information that may be useful for collaborative goal setting and treatment decisions.
The management of diabetes is multifaceted and complex, particularly for populations who face social barriers and challenges. The Hispanic/Latino population is more likely to encounter disparities in access to quality health care and disparities in social determinants of health compared to non-Hispanic whites [4–9]. Therefore, it is important for health professionals to engage Hispanic/Latino patients in self-care by eliciting information that best facilitates collaborative goal setting. Health professionals are in an influential position to leverage a communication style that is empathetic, trusting, and open, setting the tone for a positive patient-physician encounter and, in turn, positive patient outcomes [18–20].
Corresponding author: Jeannie Belinda Concha, PhD, MPH, Dept. of Public Health Sciences, The University of Texas at El Paso, 500 W. University Ave., El Paso, TX 79968, jeannie@utep.edu.
Funding support: Support for this research was provided by the Office of Research and Sponsored Projects at The University of Texas at El Paso.
Financial disclosures: None.
1. American Diabetes Association. American Diabetes Association Standards of Medical Care in Diabetes. Diabetes Care 2017; 40: Suppl 1.
2. Dominguez K, Penman-Aguilar A, Chang MH, et al. Vital signs: Leading causes of death, prevalence of diseases and risk factors, and use of health services among Hispanics in the United States, 2009–2013. MMWR 2015;64:1–10.
3. Commission on Social Determinants of Heath. Closing the gap in a generation: health equity through action on the social determinants of health. Final report on the Commission on Social Determinants of Health. Geneva, World Health Organization. Accessed 10 Sept 2017 at http://apps.who.int/iris/bitstream/10665/43943/1/9789241563703_eng.pdf.
4. Laiterapong N, Fairchild PC, Chou CH, et al. Revisiting disparities in quality of care among US adults with diabetes in the era of individualized care, NHANES 2007-2010. Med Care 2015;53:25–31.
5. Vaccaro JA, Feaster DJ, Lobar SL, et al. Medical advice and diabetes self-management reported by Mexican-American, Black, and White-non-Hispanic adults across the United States. BMC Public Health 2012;12:185.
6. Correa-de-Araujo R, McDermott K, Moy E. Gender differences across racial and ethnic groups in quality of care for diabetes. Women Health Iss 2006;16:56–65.
7. Chawla N, Rodriguez MA, Babey SH, Brown ER. Health policy fact sheet: diabetes among Latinos in California; disparities in access and management. UCLA Center for Health Policy Research. Accessed 1 Aug 2017 at http://healthpolicy.ucla.edu/publications/Documents/PDF/Diabetes%20among%20Latinos%20in%20California%20Disparities%20in%20Access%20and%20Management.pdf.
8. Pu J, Chewning B. Racial differences in diabetes preventive care. Res Social Adm Pharm 2013;9:790–6.
9. Institute of Medicine. Unequal treatment: Confronting racial and ethnic disparities in healthcare. Washington, DC: National Academies Press; 2003.
10. Saha S, Arbeaez JJ, Cooper LA. Patient-physician relationships and racial disparities in the quality of care. Am J Public Health 2003;93:1713–9.
11. What is cultural and linguistic competence?: Definitions, February 2003. Agency for Healthcare Research and Quality, Rockville, MD. Accessed 28 Aug 2017 at http://www.ahrq.gov/pprofessionals/systems/primary -care/cultural-competence-mco/cultcompdef.html.
12. U.S. Department of Health and Human Services, Office of Minority Health. 2000. Assuring cultural competence in health care: Recommendations for National Standards and an outcomes-focused research agenda. Accessed 17 August 2017 at http://www.omhrc.gov/clas/finalpo.htm.
13. Zhao X. Relationships between sources of health information and diabetes knowledge in the US Hispanic population. Health Commun 2014;29:574–85.
14. Perchman ML, Flannagan D, Ferrer RL, Matamoras M. Communication compete c e, self-care behaviors, and glucose control in patients with type 2 diabetes. Patient Educ Couns 2009;77:55–9.
15. Reimann JOF, Talavera GA, Salmon M, et al. Cultural competence among physicians treating Mexican Americans who have diabetes: a structural model. Soc Sci Med 2004;59:2195–205.
16. Gordon HS, Gerber BS. What we’ve got here is a failure to communication. J Gen Intern Med 2011;26:104–6.
17. Gonzalez A, Salas D, Umpierrez GE. Special considerations on the management of Latino patients with type 2 diabetes mellitus. Curr Med Res Opin 2011;27:969–79.
18. Peek ME, Cargill A, Juang ES. Diabetes health disparities: A systematic review of health care interventions. Med Care Res Rev 2007;64(5 Supp):101S–156S.
19. Kutob RM, Bormanis J, Crago M, et al. Assessing culturally competent diabetes care with unannounced standardized patients. Fam Med 2013;45:400–8.
20. Weller SC, Baer RD, Garcia de Alba Garcia J, Salcedo Rocha AL. Are differences between patient and provider explanatory models of diabetes associated with patient self-management and glycemic control? J Health Care Poor Underserved 2013:24;1498–510.
21. Duta MJ. Communicating about culture and health: Theorizing culture-centered and cultural sensitivity approaches. Commun Theory 2007;17:304–28.
22. Concha JB, Mayer SD, Mezuk B, Avula D. Diabetes causation beliefs among Spanish speaking patients. Diabetes Educ 2015:42:116–25.
23. Arcury TA, Skelly AH, Gesler WM, et al. Diabetes meanings among those without diabetes: explanatory models of immigrant Latinos in rural North Carolina. Soc Sci Med 2004;59:2183–3.
24. Daniulaityte R. Making sense of diabetes: cultural models, gender and individual adjustment to type 2 diabetes in a Mexican community. Soc Sci Med 2004;59:1899–912.
25. Poss J, Jezewski MA. The role and meaning of susto in Mexican American’s explanatory model of type 2 diabetes. Med Anthropol Q 2002;16:360–77.
26. Weller SC, Baer RD, Pachter LM, et al. Latino beliefs about diabetes. Diabetes Care 1999;22:722–8.
27. United States Census Bureau. Language use. Accessed Sept 2017 at https://www.census.gov/topics/population/language-use/about.html.
28. Mezuk B, Albrecht S, Eaton WW, Golden SH. Depression and type 2 diabetes over the lifespan: a meta-analysis. Diabetes Care 2008;31:2383–90.
29. Li C, Ford ES, Strine TW, Mokdad AH. Prevalence of depression among US adults with diabetes. Diabetes Care 2007;31:105–7.
30. Ali S, Stone MA, Peters JL, Davies MJ, Khunti K. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 2006;24:1069–78.
31. Li C, Barker L, Ford ES, et al. Diabetes and anxiety In US adults: findings from the 2006 Behavioral Risk Factor Surveillance System. Diabetes Med 2008;25:878–81.
32. Concha JB, Mezuk B, Duran B. Culture-centered approaches: the relevance of assessing emotional health for Latinos with type 2 diabetes. BMJ Open Diab Res Care 2015;3.
33. Bentancourt JR, Green AR, Carillo Je, Park ER. Cultural competence and health care: Key perspectives and trends. Health Affairs 2015;24:499–506.
34. Association of American Medical Colleges. Cultural Competence Education 2005. Accessed Feb 2016 at https://www.aamc.org/download/54338/data/.
35. Dobbie AE, Medrano M, Tysinger J, Olney C. The BELIEF Instrument: A preclinical teaching tool to elicit patients’ health beliefs. Family Med 2003;35:316–9.
36. Levin SJ, Like RC, Gottlieb JE. ETHNIC: A framework for culturally competent ethical practice. Patient Care 2003;34:188–9.
37. Stuart MR, Leibermann JR. The fifteen-minute hour: applied psychotherapy for the primary care physician. New York: Praeger.
38. Pace EJ, Somerville NJ, Enyoha C, et al. Effects of a brief psychosocial intervention on inpatient satisfaction: a randomized control trial. Fam Med 2017;49:675–8.
From the University of Texas at El Paso, El Paso, TX.
Abstract
- Objective: To demonstrate the applied use of recommended cultural competency communication tools.
- Methods: An overview of several cultural competency tools is presented and vignettes are used to demonstrate the use of these tools with Hispanic patients with diabetes.
- Results: Three communication mnemonic instruments, ie, BELIEF, ETHNIC, and BATHE, may be useful for engaging health professionals in patient-centered communication with their Hispanic patients and shared decision making. Health professionals can also employ nonjudgmental probing as part of engaging patients in setting diabetes treatment goals.
- Conclusion: Health professionals are in an influential position to leverage a patient- and culture-centered communication style to improve communication with Hispanic patients. Using mnemonic tools can help facilitate this communication and improve health professionals’ understanding on how cultural and social factors influence diabetes management in this population.
Key words: Hispanic/Latino; diabetes; patient-centered communication; cultural-competency.
The 2017 American Diabetes Association (ADA) Standards of Medical Care recommend that health professionals engage in a patient-centered communication style with patient to facilitate shared decision-making and improve diabetes outcomes. The ADA defines patient-centered communication as “a style that uses active listening, elicits patient preferences and beliefs, and assesses literacy, numeracy, and potential barriers to care” [1]. One of the main goals of using patient-centered communication is to create a collaborative, personal, and non-judgmental relationship with patients. These guidelines, however, provide less direction on the type of communication skills training that would facilitate this type of communication, particularly as it relates to ethnic/racial minority groups most at risk for diabetes and related complications.
The US Hispanic/Latino population, in particular, is a group that is burdened by the diabetes epidemic, with a prevalence that is 130% higher than non-Hispanic whites [2]. It is widely known that certain social determinants of health, like socioeconomic status, social injustices, poor access to health care, food insecurity, or living in environments that do not support health behaviors, all contribute to health disparities for Hispanics/Latinos [3]. Understanding how Hispanics/Latinos cope with these social determinants of health is important for health care professionals, and a patient-centered communication style is an ideal approach for active listening and eliciting information about the social barriers/challenges that may influence diabetes self-care. However, there is some evidence that suggests this approach is not fully used by health care professionals when communicating with Hispanics/Latinos with diabetes, and Hispanics/Latinos continue to be more likely to experience disparities in the quality of diabetes care they receive compared to non-Hispanic whites [4–9]. One of the identified contributors to these disparities is the poor communication between physicians and Hispanic/Latino patients [10–16]. Given that health care professionals are the primary source of health care and diabetes information for Hispanics/Latinos, it is important for health professionals to enhance their patient-centered communications skills to improve the quality of care that is provided to this population [12].
Cultural Competence and Patient-Centered Communication
Not all health professional communication skills are perceived as unsatisfactory by Hispanic/Latino patients with diabetes. In fact, Hispanics/Latinos report a positive provider-patient clinical interaction when health professionals display cultural competency skills [15,17–20]. Moreover, evidence suggest that Hispanic/Latino patients with diabetes reported better quality of care and improved self-management behaviors with a culturally competent provider [18–20]. Cultural competency is described as “understanding and responding effectively to the cultural and linguistic needs brought by the patient to the health care encounter” and “valuing diversity, provider self-assessment, managing dynamics of differences, acquiring and institutionalizing knowledge, and adapting to diversity and the cultural context of individuals served” [9,11,12]. One approach for gaining cultural competency skills is to understand how the disease process is conceptualized within a culture and how that influences a patient’s own theory about their disease etiology, prognosis, and outcome [21]. This approach is known as culture-centered in the health communications literature and may be useful when communicating with Hispanic/Latino patients with diabetes because there is extensive literature describing unique indigenous Latin American explanatory models for diabetes [22–26].
Language Discordance in Physician-Patient Communication
The process of patient-physician communication includes “attending to one another and begin interpreting one another’s verbal and nonverbal” interactions [9]. A conventional assumption regarding the disparities in diabetes care quality for Hispanic/Latino patients is that it stems from language discordant patient-physician interactions, which result in errors in the provision of diabetes information and treatment instructions regarding medications and self-care behaviors [9]. While language is a contributing factor, the US Census reports that over half of US Hispanics/Latinos are bilingual and speak English “very well” [27]. Thus, other underlying mechanisms must be contributing to patient-physician miscommunication and suboptimal diabetes outcomes. Moreover, the findings from studies of patient-physician language concordance and diabetes management are inconsistent. For example, language concordance between Hispanic/Latino patients and physicians is associated with improvement in HbA1c but not self-care behaviors (ie, healthy eating, self-monitoring, medicine adherence, exercise) [20]. Thus, there is need to move beyond spoken language to address elements of interpersonal communication around diabetes care through addressing cultural health beliefs and explanatory models of diabetes.
Cultural Explanatory Models of Diabetes
Explanatory models for diabetes among Hispanics/Latinos are diverse and often include a biomedical framework (eg, obesity, unhealthy eating, sedentary lifestyle, genetics); however, there is one unique indigenous belief that continues to be held within this population. Specifically, there is a cultural belief that diabetes is caused by strong or negative emotions, like fright sickness (susto), stress (estres), anger (coraje), or nerves (nervios) [22–26]. Although this cultural belief has been in existence long before scientific evidence has shown the bi-directional relationship between stress/depression and diabetes, the integration of emotions in diabetes self-management in patient-provider communication has not been standardized [28–31]. Health professionals’ interest in how patients view their own disease process may help build rapport with patients. Enhancing health professionals’ cultural competency skills can be a critical first step for improving patient-provider communication. For instance, it can (1) present an opportunity to integrate cultural belief systems into diabetes care for Hispanics/Latinos, (2) open the door for other important conversations about Hispanic/Latino patients’ psychosocial and familial environment and identify barriers or motivators in diabetes self-management, and (3) build rapport and trust between the health professional and patient.
Additionally, inquiring about emotional beliefs or emotions about diabetes in general can help improve the patient-provider relationship, giving Hispanic/Latino patients a sense that their provider cares about their feelings and emotional well-being. For example, in a study conducted by Concha et al, a Hispanic/Latino male patient with diabetes expresses his appreciation of his doctor for attending to his emotional problems and suggests that his diabetes is in control because of the encouragement he receives from the doctor [22].
…I believe the doctors..can encourage one with ..diabetes… I am very grateful to God before anything that till today I have my sugar controlled. I am a diabetic, but controlled. And Dr. [name omitted], he’s a blessing from God. He knows my body like my mother….Because whatever little thing, he attends to me, he gives me a lot of encouragement with my emotional problems. He sent me to a counselor, I have a specialist for my problem with my urinary tracts. I have attention, I have all the attention from the doctor…
Inquiring about emotional well-being may also be beneficial because Hispanics/Latinos with diabetes have reported that they would feel more comfortable talking to a professional about personal problems compared to Hispanics/Latinos without diabetes [32]. Having a physical illness may provide an opportunity for these patients to discuss stress or depression in tandem with diabetes to diminish any possible stigma or shame associated with having a mental health problem. It is important for health care providers to be aware of emotional or social problems that may be negatively influencing diabetes self-care behaviors.
Models of Effective Cross-Cultural Communication
Cultural competency training for health professionals is one strategy for reducing health disparities and ensuring that racial/ethnic populations receive “equitable, effective, and culturally appropriate clinical care” [9,11,12,33]. The Association of American Medical Colleges’ guide for cultural competence education in medical school cites several models of effective cross-cultural communication for physicians and/or physician assistants [34]. I describe 3 communication tools below that may help health care professionals initiate conversations and aid them in understanding how to better manage sociocultural and environmental issues that may impede patients’ ability to manage diabetes. For each tool, a vignette is offered that illustrates how the tool may be used in communicating with Hispanic/Latino patients.
BELIEF
The BELIEF instrument (Dobbie 2003) is a teaching tool designed to elicit patients’ health beliefs and to assist preclinical medical students or medical professionals in understanding how explanatory models of a disease influence patient engagement in care. The BELIEF instrument is straightforward and can be easily implemented into clinical case vignettes and or role-play as part of cultural competency training [35]. The specific questions corresponding to the BELIEF prompts are
- B: Beliefs about health (What caused your illness/problem?)
- E: Explanation (Why did it happen at this time?)
- L: Learn (Help me understand your belief/opinion)
- I: Impact (How is this illness/problem impacting your life?)
- E: Empathy (This must be very hard for you)
- F: Feelings (How are you feeling about it?)
Vignette 1
The following vignette is a conversation between a Spanish-speaking Hispanic women, a language interpreter, and medical professional. The patient, Mrs. Chavez, has come into the clinic for the third time after experiencing symptoms due to hypoglycemia. Mrs. Chavez believes stress may have something to do with her hypoglycemia but is not quite sure how. By using the BELIEF mnemonic, the medical professional is able to ask more about the stress that led into a discussion about how stress actually influenced her eating and medication intake behaviors. Through this probing, the medical professional was able to identify the possible cause of her hypoglycemia and work with Mrs. Chavez on finding a solution every time she experiences the stressful event. The vignette also demonstrates how interpreters may share cultural information that may clarify problems.
Medical Professional: Mrs. Chavez, I see you are here again for hypoglycemia. Can you tell me what has happened? Do you have your medications with you today?
Interpreter: Sra. Chavez, entiendo que está aquí nuevamente por hipoglucemia. ¿Puedes decirme qué ha pasado? ¿Tiene sus medicamentos con usted hoy?
Mrs. Chavez: Si, me ha sentido débil y mareado.
Interpreter: Yes I have felt faint and dizzy?
Medical Professional: Have you been taking your metformin as prescribed?
Interpreter: ¿Ha estado tomando su metformin según lo recetado?
Mrs. Chavez: Si (YES).
Medical Professional: We might have to consider adjusting your dosage.
Interpreter: Es posible que tengamos que considerar ajustar su dosis.
Mrs. Chavez privately to the Interpreter: ¿no es posible que las emociones o nervios puedan causar algo? He escuchado que este puede ser el problema?
Interpreter to Mrs. Chavez: Déjame preguntarle al doctor, si?
Let me ask the doctor, yes? (Mrs. Chavez, nods in agreement)
Interpreter to Medical Professional: She is asking if emotions or nervousness could be the cause. She has heard that this could be the problem.
Medical Profesional to Interpreter: What does she mean?
Interpreter: There is a cultural belief that stress or nerves can cause diabetes or affect diabetes. You may want to ask about this.
Medical Professional: Yes emotions like stress can cause changes in you glucose. (Beliefs) Do you believe that some emotions are causing your hypoglycemia?
Interpreter: Sí, las emociones como el estrés pueden provocar cambios en la glucosa. ¿Crees que algunas emociones están causando tu hipoglucemia?
Mrs. Chavez: (Shrugs shoulders).
Medical Professional: I see here in your records, that the other two times you had hypoglycemica were 1 month and 3 months ago. (Beliefs) What do you think caused these events and (Explanation) why do you think it happened during these times?
Interpreter: Veo aquí en sus registros que las otras dos veces que tuvo hipoglucemia fueron hace 1 mes y 3 meses. ¿Qué crees que causó estos eventos y por qué crees que sucedió durante estos tiempos?
Mrs. Chavez: Pues, no sé.
Interpreter: Well I don’t know.
Medical Professional: (Learn) Help me understand what you think happened 3 and 1 month ago and this month that may have caused your glucose to drop. What was happening emotionally during these times? Do you remember?
Interpreter: Ayúdame a entender lo que piensas que sucedió hace 3 y 1 meses y este mes, puede haber causado que tu glucosa baje. ¿Qué estaba pasando emocionalmente durante este tiempo? ¿Te acuerdas?
Mrs. Chavez: Hmm. Pues, hace 3 meses fui a visitar a mi madre y hace 1 meses fui a visitar a mi hermano al norte.
Interpreter: Hmm. Well 3 months ago I went to visit my mother and 1 months ago I went to visit my brother up north.
Medical Professional: (Learn) How were those trips for you. Did you have fun? What types of emotions were you feeling during these trips?
Interpreter: ¿Cómo fueron esos viajes para ti? ¿Te divertiste? ¿Qué tipo de emociones sentías durante estos viajes?
Mrs. Chavez: Pues, yo estaba muy estresado durante mis viajes.
Interpreter: Well, I was very stressed during my trips.
Medical Professional: (Learn) Would you like to share why you were stressed? What was happening for you to feel so stressed?
Interpreter: ¿Te gustaría compartir por qué estabas estresado? ¿Qué estaba pasando para que te sientas tan estresado?
Mrs. Chavez: Bueno, tenemos muchos problemas familiares y conflictos. Hay muchos argumentos familiares y se vuelve estresante.
Interpreter: Well we have a lot of family problems and conflict. There are a lot of family arguments and it gets stressful.
Medical Professional: (Impact) How do you think this has affected your glucose?
Interpreter: ¿Cómo crees que esto ha afectado tu glucosa?
Mrs. Chavez: No lo sé.
Interpreter: I don’t know.
Medical Professional: (Learn) Do you think the stress maybe led you to forget to take your medication or affected your eating?
Interprter: ¿Crees que el estrés puede llevarte a olvidarte de tomar tu medicación o afectó su alimentación?
Mrs. Chavez: Pues si y no comí. Estaba demasiado estresado para comer. Raramente comí mientras estaba allí. Estaba tan estresado que no tenía apetito.
Interpreter: Well yes and I didn’t eat. I was too stressed to eat. I rarely ate while I was there. I was so stressed i did not have an appetite.
Medical Professional: (Empathy) Mrs. Chavez, that must have been very hard for you. I’m sorry you have had to feel this way. (Feelings) Is this how you feel everytime you visit your family?
Interpreter: Sra. Chávez, eso debe haber sido muy difícil para usted. Lamento que hayas tenido que sentirte de esta manera. ¿Es así como te sientes cada vez que visitas a tu familia?
Mrs. Chavez: Sí, todos se involucran en los problemas familiares y es muy estresante visitarlos, pero tengo que ir a ayudar a mi madre porque mi hermano está enfermo y no puede ayudarla. Soy el único que está cerca y mis otros hermanos discuten sobre lo que debería hacer. Tengo que estar ahí. Tengo que visitar.
Interpreter: Yes, everyone gets involved in the family problems and it is very stressful to visit but I have to go to help my mom because my brother is sick and can’t help her. I’m the only one close by and my other siblings argue about what I should do. I have to be there. I have to visit.
Medical Profesional: (Empathy) Yes, that must be very difficult for you. Okay, now I understand what is happening. Your visits are necessary but it seems like the stress is affecting your eating patterns and whether you remember to take your metformin. How do you feel if we come up with a plan for when you visit your family now that we know what might be causing your hypoglycemia? Do you think it is a good idea to take high glucose snacks or candy and have them with you on the trip so when you feel dizzy or faint you can eat them?
Interpreter: Sí, eso debe ser muy difícil para ti. De acuerdo, ahora entiendo lo que está pasando. Sus visitas son necesarias, pero parece que el estrés está afectando sus patrones de alimentación y si recuerda tomar su metformina. ¿Cómo se siente si elaboramos un plan para su familia ahora que sabemos lo que podría estar causando su hipoglucemia? ¿Cree que es una buena idea tomar refrigerios con alto contenido de glucosa o dulces y llevarlos consigo durante el viaje para que cuando se sienta mareado o desmayado pueda comerlos?
Mrs. Chavez: Sí, por supuesto. Ni siquiera me di cuenta de eso hasta ahora que hablamos sobre eso. Tienes razón, no he estado comiendo bien cuando lo visito. Me siento terrible cuando estoy allí como si quisiera desmayarme.
Interpreter: Yes of course. I didn’t even really realize that until now that we talked about it. You are right, I haven’t been eating right when I visit. I feel terrible when I am there like I want to faint.
Medical Professional: Mrs. Chavez, sometimes it is helpful to talk about our stress and problems we encournter in life, just to talk through it. Is this something you would be interested in? If so, we can arrange for you to come talk to the social worker.
Interpreter: Sra. Chavez, a veces es útil hablar sobre nuestro estrés y los problemas que alegramos en la vida, solo para hablar sobre ello. ¿Esto es algo que te interesaría? Si tu quieres, podemos hacer arreglos para que vengas a hablar con el trabajador social.
Mrs. Chavez: Tal vez, no estoy seguro, pero tal vez
Interpreter: Maybe, I’m not sure but maybe.
Medical Professional: Okay, you let me know if this is something you would like to do. You can call and let us know and I’ll ask again during our next visit and see how you are dealing with the stress when you visit your family.
Interpreter: De acuerdo, dime si esto es algo que te gustaría hacer. Puede llamar y dejarnos saber, y volveré a preguntar durante nuestra próxima visita y verá cómo lidia con el estrés cuando visita a su familia.
ETHNIC
The ETHNIC interviewing tool (Levin SJ 2000) can be used to explore cross cultural issues and facilitate collaboration during clinical encounters and is designed for clinical students or health professionals permitted to diagnose and provide therapeutic interventions [36]. The specific questions corresponding to the ETHNIC prompts:
- E: Explanation (How do you explain your illness?)
- T: Treatment (What treatment have you tried?)
- H: Healers (Have you sought any advice from folk healers?)
- N: Negotiate (mutually acceptable options)
- I: Intervention (agreed on)
- C: Collaboration (with patient, family, and healers)
Vignette 2
The second vignette is a discussion between a conscientious patient, Mrs. Rodriguez, and her doctor. Mrs. Rodriguez is determined to keep her glucose levels within optimal range by eating healthy and living a natural lifestyle. Included in her natural lifestyle is the use of herbs from her garden and herbal supplements sold to her by her neighbor. Because her numbers have been in the normal range she discontinues her prescribed medication to rely on natural products. However, a trip with family members interrupts her daily routine, which is replaced with fast foods and little rest. Upon returning from her trip her glucose levels increase and she cannot decrease her glucose numbers.
Medical Professional: Good morning Mrs. Rodriguez. I see you are here today for high blood sugar because of your diabetes. (Explanation) Can you share why you think you have recently had higher numbers than normal?
Mrs. Rodriguez: Good morning Doctor. Yes, I am usually very good with my numbers but lately they have gone up and I know why.
Medical Professional: Yes, that is good that you have had your glucose managed. (Explanation) What has caused your numbers to go up Mrs. Rodriguez?
Mrs. Rodriguez: All this American food. I went on a trip to visit my daughter and all we did was eat out, hamburgers, fast food restaurants. They do not cook at home and we were always doing something so I could not cook. It was terrible, all we did was keep busy out and about, I was tired. I spent so much money on food that has chemicals. Look at me now. I can’t seem to get my numbers down.
Medical Professional: Oh, I understand. Yes, a trip can sometimes mess with our routine. (Treatment) Since you have been good at managing your glucose in the past what have you been doing now to get your glucose in normal range?
Mrs. Rodriguez: Well I have been doing the same thing I have always been doing. Eating healthy, resting, gardening, and praying.
Medical Professional: Gardening? That’s really nice. What do you garden?
Mrs. Rodriguez: Oh I love gardening. I plant all types of herbs, vegetables, flowers.
Medical Professional: That is so good Mrs. Rodriguez. I wish I had more time to garden. Do you use your own vegetable and herbs when you cook?
Mrs. Rodriguez: Haha. Yes of course. That is why my sugar was fine before I went on this trip. I rely on my garden to keep me healthy.
Medical Professional: There are so many herbs that are helpful for diabetes. (Treatment) Do you use any to help with your diabetes?
Mrs. Rodriguez: Well yes, in fact, I do. I know you doctors don’t like us to use our herbs but I do. And that was what keeps my sugars normal.
Medical Professional: Oh Mrs. Rodriguez, yes sometimes you hear doctors say this but some herbs are helpful. We just like to know what other things our patients do so we know how to make sure your medications work with certain herbs. (Treatment) I know many people use nopal (cactus), do you eat nopal?
Mrs. Rodriguez: ¿Como no? (of course). I eat them all the time. I make my morning licuado (drink); a little bit of parsley, oregano, oatmeal, lemon, nopal mixed with milk and yogurt.
Medical Professional: (Treatment) Sounds good, what else do you use?
Mrs. Rodriguez: Oh you know other things. Apple cider, cinnamon, cayenne.
Medical Professional: All from your garden?
Mrs. Rodriguez: Yes.
Medical Professional: (Treatment) Do you use any type of herbal supplements from stores or online?
Mrs. Rodriguez: My neighbor sells supplements specifically for diabetes. I started to use a natural supplement with cinnamon, vitamin D, and fish oil. All very natural.
Medical Professional: (Healer) Oh does your neighbor also have diabetes?
Mrs. Rodriguez: No, she sells products. But she sells to many people with diabetes and the supplement works. We get together and she tells us about how they work.
Medical Professional: Do you know the name of this supplement Mrs. Rodriguez?
Mrs. Rodriguez: Oh, gluco…something, it has a heart in the name. But I read the ingredients and it has only natural ingredients. (An FDA banned supplement for false claims)
Medical Professional: Oh I see. I may be familiar with that. Can you bring the supplement along with the medications I have prescribed? I just want to make sure there is not interaction between the two. To get your glucose back to normal I want to make sure we think of every possible situation that could be causing your high numbers. (Treatment) How have you been taking the supplement and the prescribed medications?
Mrs. Rodriguez: Well, I have not refilled your prescription. I was doing so well with my numbers, I’d rather go natural than take all those chemicals.
Medical Professional: Oh, I see Mrs. Rodriguez. Okay, you have done so well controlling your glucose before your trip and now we are in a situation where your numbers are not coming down so let’s try to figure this out. I’d like to learn more about this supplement, so for our next visit can you bring in your supplements so I can take a look at it? (Negotiate) We can then talk about the benefits or cautions. But in the meantime I’d like you to refill your medication and take as followed to see if that helps your sugars. (Negotiate) What do you think? Is this possible?
Mrs. Rodriguez: Oh Doctor, I just don’t like taking chemicals.
Medical Professional: I understand Mrs. Rodriguez. You did take them to start when you first came in for diabetes, is this correct?
Mrs. Rodriguez: Well yes but, I slowly got off them.
Medical Professional: I know it’s difficult to take medications every day but they can help in addition to your healthy eating. I know you are concerned about medications but for now we have to focus on getting your numbers down or your diabetes could become worse and we don’t want you to get there. Do you agree? (Negotiating process)
Mrs. Rodriguez: Well, I am concerned about my numbers.
Medical Professional: (Intervention) Okay well let’s try to get back to where you were before the trip. Let’s get you back on the medication and let’s see if this helps. (Negotiate) For the next visit would you be willing to bring any supplements you are taking along with the medication? (Collaboration) We can talk about the benefits and cautions for the medications and supplements. How does this sound?
Mrs. Rodriguez: Well, I am here to fix my numbers. I have everything I take in a box so I can bring that.
Medical Professional: Yes that would be great. (Collaboration) We can both talk about your daily routine and what have you learned about the supplement, any information or papers that you have, in addition to the medication I prescribed.
Mrs. Rodriguez: Yes I can do that.
Medical Professional: Thank you Mrs. Rodriguez. (Intervention) Also, I’ll have the nurse call you today or tomorrow and you can give her the name of the supplement and she’ll make sure the drug store has a refill for you. Would this work for you Mrs. Rodriguez?
Mrs. Rodriguez: Yes Doctor. You can call me. I’ll have the list ready.
BATHE
Unlike the BELIEF and ETHNIC instruments, the BATHE mnemonic (Lieberman 1999)
- B: Background (What is going on in your life?)
- A: Affect (How do you feel about what is going on?)
- T: Trouble (What troubles you most?)
- H: Handling (How are you handling that?)
- E: Empathy (This must be very difficult for you)
Vignette 3
The last vignette features Mr. Gonzalez, who typically shows a positive outlook on life when visiting his doctor. He is a patient who would not necessarily discuss his emotions if not asked specific questions about his emotional well-being.
Medical Professional: Hello Mr. Gonzalez. (Background) How are you doing today? What’s new? What’s going on in your life lately?
Mr. Gonzalez: Hey, Doctor! I’m good you know just living day to day.
Medical Professional: Good. (Affect) So how is your diabetes treating you day to day? How are you feeling with life and managing your diabetes?
Mr. Gonzalez: Ah well you know, just dealing with it as best as I can.
Medical Professional: Ah okay. As best as you can. (Troubles) What troubles you the most about managing diabetes?
Mr. Gonzalez: Well you know the aches and pains. But what can I do.
Medical Professional: (Affect) How do you feel about those aches and pains?
Mr. Gonzalez: Well it does limit me. I can’t move as well as I use to.
Medical Professional: (Handling) Hmm. I see. How are you handling those aches and pains? What are you doing to relieve it?
Mr. Gonzalez: I do my best with pain cream.
Medical Professional: (Empathy) Pains and aches, that must be difficult. (Affect) How do the aches and pains make you feel?
Mr. Gonzalez: Ahh, Doc, it’s not the same. You know I can’t do the same things anymore.
Medical Professional: (Background) What do you mean? What is not the same anymore?
Mr. Gonzalez: This diabetes, I’m not the same person. I use to be able to be there for my family and community and now I feel like I can’t be there for them the way I use to. I use to be the strong one for my family, helping those in need, and now I’m limited, my body is limited.
Medical Professional: (Affect) How do you feel about that? How does it make you feel emotionally and physically?
Mr. Gonzalez: Bad. I feel bad about it.
Medical Professional: Bad emotionally or physically?
Mr. Gonzalez: Both
Medical Professional: I see. (Handling) How are you dealing with the emotional part of it?
Mr. Gonzalez: I don’t know. I don’t know how.
Medical Professional: (Empathy) Dealing with diabetes and how it makes your body feel can be very emotionally distressing. It is common to feel this way but I want to make sure we also work on how you feel emotionally or how your emotions is affecting your diabetes.
Conclusion
Three mnemonic tools have been suggested to initiate patient-centered and culture-centered communication with patients. Beyond the use of these instruments, there are 2 key skills that are essential for engaging a Hispanic/Latino patient. The first is a non-judgmental, warm communication approach, and the second is astute probing. Once when I was interpreting for a Spanish-speaking Hispanic/Latino patient and English-speaking doctor, the patient expressed to me that she felt that the medical professionals “tienen una cultura fría” (“have a cold culture”), and she did not feel comfortable sharing more about herself because of it. It is also important for medical professionals to be aware of a patient’s doublespeak as a way to share enough information but not all information to keep from being judged by medical professionals. Thus, non-judgmental probing can uncover important information that may be useful for collaborative goal setting and treatment decisions.
The management of diabetes is multifaceted and complex, particularly for populations who face social barriers and challenges. The Hispanic/Latino population is more likely to encounter disparities in access to quality health care and disparities in social determinants of health compared to non-Hispanic whites [4–9]. Therefore, it is important for health professionals to engage Hispanic/Latino patients in self-care by eliciting information that best facilitates collaborative goal setting. Health professionals are in an influential position to leverage a communication style that is empathetic, trusting, and open, setting the tone for a positive patient-physician encounter and, in turn, positive patient outcomes [18–20].
Corresponding author: Jeannie Belinda Concha, PhD, MPH, Dept. of Public Health Sciences, The University of Texas at El Paso, 500 W. University Ave., El Paso, TX 79968, jeannie@utep.edu.
Funding support: Support for this research was provided by the Office of Research and Sponsored Projects at The University of Texas at El Paso.
Financial disclosures: None.
From the University of Texas at El Paso, El Paso, TX.
Abstract
- Objective: To demonstrate the applied use of recommended cultural competency communication tools.
- Methods: An overview of several cultural competency tools is presented and vignettes are used to demonstrate the use of these tools with Hispanic patients with diabetes.
- Results: Three communication mnemonic instruments, ie, BELIEF, ETHNIC, and BATHE, may be useful for engaging health professionals in patient-centered communication with their Hispanic patients and shared decision making. Health professionals can also employ nonjudgmental probing as part of engaging patients in setting diabetes treatment goals.
- Conclusion: Health professionals are in an influential position to leverage a patient- and culture-centered communication style to improve communication with Hispanic patients. Using mnemonic tools can help facilitate this communication and improve health professionals’ understanding on how cultural and social factors influence diabetes management in this population.
Key words: Hispanic/Latino; diabetes; patient-centered communication; cultural-competency.
The 2017 American Diabetes Association (ADA) Standards of Medical Care recommend that health professionals engage in a patient-centered communication style with patient to facilitate shared decision-making and improve diabetes outcomes. The ADA defines patient-centered communication as “a style that uses active listening, elicits patient preferences and beliefs, and assesses literacy, numeracy, and potential barriers to care” [1]. One of the main goals of using patient-centered communication is to create a collaborative, personal, and non-judgmental relationship with patients. These guidelines, however, provide less direction on the type of communication skills training that would facilitate this type of communication, particularly as it relates to ethnic/racial minority groups most at risk for diabetes and related complications.
The US Hispanic/Latino population, in particular, is a group that is burdened by the diabetes epidemic, with a prevalence that is 130% higher than non-Hispanic whites [2]. It is widely known that certain social determinants of health, like socioeconomic status, social injustices, poor access to health care, food insecurity, or living in environments that do not support health behaviors, all contribute to health disparities for Hispanics/Latinos [3]. Understanding how Hispanics/Latinos cope with these social determinants of health is important for health care professionals, and a patient-centered communication style is an ideal approach for active listening and eliciting information about the social barriers/challenges that may influence diabetes self-care. However, there is some evidence that suggests this approach is not fully used by health care professionals when communicating with Hispanics/Latinos with diabetes, and Hispanics/Latinos continue to be more likely to experience disparities in the quality of diabetes care they receive compared to non-Hispanic whites [4–9]. One of the identified contributors to these disparities is the poor communication between physicians and Hispanic/Latino patients [10–16]. Given that health care professionals are the primary source of health care and diabetes information for Hispanics/Latinos, it is important for health professionals to enhance their patient-centered communications skills to improve the quality of care that is provided to this population [12].
Cultural Competence and Patient-Centered Communication
Not all health professional communication skills are perceived as unsatisfactory by Hispanic/Latino patients with diabetes. In fact, Hispanics/Latinos report a positive provider-patient clinical interaction when health professionals display cultural competency skills [15,17–20]. Moreover, evidence suggest that Hispanic/Latino patients with diabetes reported better quality of care and improved self-management behaviors with a culturally competent provider [18–20]. Cultural competency is described as “understanding and responding effectively to the cultural and linguistic needs brought by the patient to the health care encounter” and “valuing diversity, provider self-assessment, managing dynamics of differences, acquiring and institutionalizing knowledge, and adapting to diversity and the cultural context of individuals served” [9,11,12]. One approach for gaining cultural competency skills is to understand how the disease process is conceptualized within a culture and how that influences a patient’s own theory about their disease etiology, prognosis, and outcome [21]. This approach is known as culture-centered in the health communications literature and may be useful when communicating with Hispanic/Latino patients with diabetes because there is extensive literature describing unique indigenous Latin American explanatory models for diabetes [22–26].
Language Discordance in Physician-Patient Communication
The process of patient-physician communication includes “attending to one another and begin interpreting one another’s verbal and nonverbal” interactions [9]. A conventional assumption regarding the disparities in diabetes care quality for Hispanic/Latino patients is that it stems from language discordant patient-physician interactions, which result in errors in the provision of diabetes information and treatment instructions regarding medications and self-care behaviors [9]. While language is a contributing factor, the US Census reports that over half of US Hispanics/Latinos are bilingual and speak English “very well” [27]. Thus, other underlying mechanisms must be contributing to patient-physician miscommunication and suboptimal diabetes outcomes. Moreover, the findings from studies of patient-physician language concordance and diabetes management are inconsistent. For example, language concordance between Hispanic/Latino patients and physicians is associated with improvement in HbA1c but not self-care behaviors (ie, healthy eating, self-monitoring, medicine adherence, exercise) [20]. Thus, there is need to move beyond spoken language to address elements of interpersonal communication around diabetes care through addressing cultural health beliefs and explanatory models of diabetes.
Cultural Explanatory Models of Diabetes
Explanatory models for diabetes among Hispanics/Latinos are diverse and often include a biomedical framework (eg, obesity, unhealthy eating, sedentary lifestyle, genetics); however, there is one unique indigenous belief that continues to be held within this population. Specifically, there is a cultural belief that diabetes is caused by strong or negative emotions, like fright sickness (susto), stress (estres), anger (coraje), or nerves (nervios) [22–26]. Although this cultural belief has been in existence long before scientific evidence has shown the bi-directional relationship between stress/depression and diabetes, the integration of emotions in diabetes self-management in patient-provider communication has not been standardized [28–31]. Health professionals’ interest in how patients view their own disease process may help build rapport with patients. Enhancing health professionals’ cultural competency skills can be a critical first step for improving patient-provider communication. For instance, it can (1) present an opportunity to integrate cultural belief systems into diabetes care for Hispanics/Latinos, (2) open the door for other important conversations about Hispanic/Latino patients’ psychosocial and familial environment and identify barriers or motivators in diabetes self-management, and (3) build rapport and trust between the health professional and patient.
Additionally, inquiring about emotional beliefs or emotions about diabetes in general can help improve the patient-provider relationship, giving Hispanic/Latino patients a sense that their provider cares about their feelings and emotional well-being. For example, in a study conducted by Concha et al, a Hispanic/Latino male patient with diabetes expresses his appreciation of his doctor for attending to his emotional problems and suggests that his diabetes is in control because of the encouragement he receives from the doctor [22].
…I believe the doctors..can encourage one with ..diabetes… I am very grateful to God before anything that till today I have my sugar controlled. I am a diabetic, but controlled. And Dr. [name omitted], he’s a blessing from God. He knows my body like my mother….Because whatever little thing, he attends to me, he gives me a lot of encouragement with my emotional problems. He sent me to a counselor, I have a specialist for my problem with my urinary tracts. I have attention, I have all the attention from the doctor…
Inquiring about emotional well-being may also be beneficial because Hispanics/Latinos with diabetes have reported that they would feel more comfortable talking to a professional about personal problems compared to Hispanics/Latinos without diabetes [32]. Having a physical illness may provide an opportunity for these patients to discuss stress or depression in tandem with diabetes to diminish any possible stigma or shame associated with having a mental health problem. It is important for health care providers to be aware of emotional or social problems that may be negatively influencing diabetes self-care behaviors.
Models of Effective Cross-Cultural Communication
Cultural competency training for health professionals is one strategy for reducing health disparities and ensuring that racial/ethnic populations receive “equitable, effective, and culturally appropriate clinical care” [9,11,12,33]. The Association of American Medical Colleges’ guide for cultural competence education in medical school cites several models of effective cross-cultural communication for physicians and/or physician assistants [34]. I describe 3 communication tools below that may help health care professionals initiate conversations and aid them in understanding how to better manage sociocultural and environmental issues that may impede patients’ ability to manage diabetes. For each tool, a vignette is offered that illustrates how the tool may be used in communicating with Hispanic/Latino patients.
BELIEF
The BELIEF instrument (Dobbie 2003) is a teaching tool designed to elicit patients’ health beliefs and to assist preclinical medical students or medical professionals in understanding how explanatory models of a disease influence patient engagement in care. The BELIEF instrument is straightforward and can be easily implemented into clinical case vignettes and or role-play as part of cultural competency training [35]. The specific questions corresponding to the BELIEF prompts are
- B: Beliefs about health (What caused your illness/problem?)
- E: Explanation (Why did it happen at this time?)
- L: Learn (Help me understand your belief/opinion)
- I: Impact (How is this illness/problem impacting your life?)
- E: Empathy (This must be very hard for you)
- F: Feelings (How are you feeling about it?)
Vignette 1
The following vignette is a conversation between a Spanish-speaking Hispanic women, a language interpreter, and medical professional. The patient, Mrs. Chavez, has come into the clinic for the third time after experiencing symptoms due to hypoglycemia. Mrs. Chavez believes stress may have something to do with her hypoglycemia but is not quite sure how. By using the BELIEF mnemonic, the medical professional is able to ask more about the stress that led into a discussion about how stress actually influenced her eating and medication intake behaviors. Through this probing, the medical professional was able to identify the possible cause of her hypoglycemia and work with Mrs. Chavez on finding a solution every time she experiences the stressful event. The vignette also demonstrates how interpreters may share cultural information that may clarify problems.
Medical Professional: Mrs. Chavez, I see you are here again for hypoglycemia. Can you tell me what has happened? Do you have your medications with you today?
Interpreter: Sra. Chavez, entiendo que está aquí nuevamente por hipoglucemia. ¿Puedes decirme qué ha pasado? ¿Tiene sus medicamentos con usted hoy?
Mrs. Chavez: Si, me ha sentido débil y mareado.
Interpreter: Yes I have felt faint and dizzy?
Medical Professional: Have you been taking your metformin as prescribed?
Interpreter: ¿Ha estado tomando su metformin según lo recetado?
Mrs. Chavez: Si (YES).
Medical Professional: We might have to consider adjusting your dosage.
Interpreter: Es posible que tengamos que considerar ajustar su dosis.
Mrs. Chavez privately to the Interpreter: ¿no es posible que las emociones o nervios puedan causar algo? He escuchado que este puede ser el problema?
Interpreter to Mrs. Chavez: Déjame preguntarle al doctor, si?
Let me ask the doctor, yes? (Mrs. Chavez, nods in agreement)
Interpreter to Medical Professional: She is asking if emotions or nervousness could be the cause. She has heard that this could be the problem.
Medical Profesional to Interpreter: What does she mean?
Interpreter: There is a cultural belief that stress or nerves can cause diabetes or affect diabetes. You may want to ask about this.
Medical Professional: Yes emotions like stress can cause changes in you glucose. (Beliefs) Do you believe that some emotions are causing your hypoglycemia?
Interpreter: Sí, las emociones como el estrés pueden provocar cambios en la glucosa. ¿Crees que algunas emociones están causando tu hipoglucemia?
Mrs. Chavez: (Shrugs shoulders).
Medical Professional: I see here in your records, that the other two times you had hypoglycemica were 1 month and 3 months ago. (Beliefs) What do you think caused these events and (Explanation) why do you think it happened during these times?
Interpreter: Veo aquí en sus registros que las otras dos veces que tuvo hipoglucemia fueron hace 1 mes y 3 meses. ¿Qué crees que causó estos eventos y por qué crees que sucedió durante estos tiempos?
Mrs. Chavez: Pues, no sé.
Interpreter: Well I don’t know.
Medical Professional: (Learn) Help me understand what you think happened 3 and 1 month ago and this month that may have caused your glucose to drop. What was happening emotionally during these times? Do you remember?
Interpreter: Ayúdame a entender lo que piensas que sucedió hace 3 y 1 meses y este mes, puede haber causado que tu glucosa baje. ¿Qué estaba pasando emocionalmente durante este tiempo? ¿Te acuerdas?
Mrs. Chavez: Hmm. Pues, hace 3 meses fui a visitar a mi madre y hace 1 meses fui a visitar a mi hermano al norte.
Interpreter: Hmm. Well 3 months ago I went to visit my mother and 1 months ago I went to visit my brother up north.
Medical Professional: (Learn) How were those trips for you. Did you have fun? What types of emotions were you feeling during these trips?
Interpreter: ¿Cómo fueron esos viajes para ti? ¿Te divertiste? ¿Qué tipo de emociones sentías durante estos viajes?
Mrs. Chavez: Pues, yo estaba muy estresado durante mis viajes.
Interpreter: Well, I was very stressed during my trips.
Medical Professional: (Learn) Would you like to share why you were stressed? What was happening for you to feel so stressed?
Interpreter: ¿Te gustaría compartir por qué estabas estresado? ¿Qué estaba pasando para que te sientas tan estresado?
Mrs. Chavez: Bueno, tenemos muchos problemas familiares y conflictos. Hay muchos argumentos familiares y se vuelve estresante.
Interpreter: Well we have a lot of family problems and conflict. There are a lot of family arguments and it gets stressful.
Medical Professional: (Impact) How do you think this has affected your glucose?
Interpreter: ¿Cómo crees que esto ha afectado tu glucosa?
Mrs. Chavez: No lo sé.
Interpreter: I don’t know.
Medical Professional: (Learn) Do you think the stress maybe led you to forget to take your medication or affected your eating?
Interprter: ¿Crees que el estrés puede llevarte a olvidarte de tomar tu medicación o afectó su alimentación?
Mrs. Chavez: Pues si y no comí. Estaba demasiado estresado para comer. Raramente comí mientras estaba allí. Estaba tan estresado que no tenía apetito.
Interpreter: Well yes and I didn’t eat. I was too stressed to eat. I rarely ate while I was there. I was so stressed i did not have an appetite.
Medical Professional: (Empathy) Mrs. Chavez, that must have been very hard for you. I’m sorry you have had to feel this way. (Feelings) Is this how you feel everytime you visit your family?
Interpreter: Sra. Chávez, eso debe haber sido muy difícil para usted. Lamento que hayas tenido que sentirte de esta manera. ¿Es así como te sientes cada vez que visitas a tu familia?
Mrs. Chavez: Sí, todos se involucran en los problemas familiares y es muy estresante visitarlos, pero tengo que ir a ayudar a mi madre porque mi hermano está enfermo y no puede ayudarla. Soy el único que está cerca y mis otros hermanos discuten sobre lo que debería hacer. Tengo que estar ahí. Tengo que visitar.
Interpreter: Yes, everyone gets involved in the family problems and it is very stressful to visit but I have to go to help my mom because my brother is sick and can’t help her. I’m the only one close by and my other siblings argue about what I should do. I have to be there. I have to visit.
Medical Profesional: (Empathy) Yes, that must be very difficult for you. Okay, now I understand what is happening. Your visits are necessary but it seems like the stress is affecting your eating patterns and whether you remember to take your metformin. How do you feel if we come up with a plan for when you visit your family now that we know what might be causing your hypoglycemia? Do you think it is a good idea to take high glucose snacks or candy and have them with you on the trip so when you feel dizzy or faint you can eat them?
Interpreter: Sí, eso debe ser muy difícil para ti. De acuerdo, ahora entiendo lo que está pasando. Sus visitas son necesarias, pero parece que el estrés está afectando sus patrones de alimentación y si recuerda tomar su metformina. ¿Cómo se siente si elaboramos un plan para su familia ahora que sabemos lo que podría estar causando su hipoglucemia? ¿Cree que es una buena idea tomar refrigerios con alto contenido de glucosa o dulces y llevarlos consigo durante el viaje para que cuando se sienta mareado o desmayado pueda comerlos?
Mrs. Chavez: Sí, por supuesto. Ni siquiera me di cuenta de eso hasta ahora que hablamos sobre eso. Tienes razón, no he estado comiendo bien cuando lo visito. Me siento terrible cuando estoy allí como si quisiera desmayarme.
Interpreter: Yes of course. I didn’t even really realize that until now that we talked about it. You are right, I haven’t been eating right when I visit. I feel terrible when I am there like I want to faint.
Medical Professional: Mrs. Chavez, sometimes it is helpful to talk about our stress and problems we encournter in life, just to talk through it. Is this something you would be interested in? If so, we can arrange for you to come talk to the social worker.
Interpreter: Sra. Chavez, a veces es útil hablar sobre nuestro estrés y los problemas que alegramos en la vida, solo para hablar sobre ello. ¿Esto es algo que te interesaría? Si tu quieres, podemos hacer arreglos para que vengas a hablar con el trabajador social.
Mrs. Chavez: Tal vez, no estoy seguro, pero tal vez
Interpreter: Maybe, I’m not sure but maybe.
Medical Professional: Okay, you let me know if this is something you would like to do. You can call and let us know and I’ll ask again during our next visit and see how you are dealing with the stress when you visit your family.
Interpreter: De acuerdo, dime si esto es algo que te gustaría hacer. Puede llamar y dejarnos saber, y volveré a preguntar durante nuestra próxima visita y verá cómo lidia con el estrés cuando visita a su familia.
ETHNIC
The ETHNIC interviewing tool (Levin SJ 2000) can be used to explore cross cultural issues and facilitate collaboration during clinical encounters and is designed for clinical students or health professionals permitted to diagnose and provide therapeutic interventions [36]. The specific questions corresponding to the ETHNIC prompts:
- E: Explanation (How do you explain your illness?)
- T: Treatment (What treatment have you tried?)
- H: Healers (Have you sought any advice from folk healers?)
- N: Negotiate (mutually acceptable options)
- I: Intervention (agreed on)
- C: Collaboration (with patient, family, and healers)
Vignette 2
The second vignette is a discussion between a conscientious patient, Mrs. Rodriguez, and her doctor. Mrs. Rodriguez is determined to keep her glucose levels within optimal range by eating healthy and living a natural lifestyle. Included in her natural lifestyle is the use of herbs from her garden and herbal supplements sold to her by her neighbor. Because her numbers have been in the normal range she discontinues her prescribed medication to rely on natural products. However, a trip with family members interrupts her daily routine, which is replaced with fast foods and little rest. Upon returning from her trip her glucose levels increase and she cannot decrease her glucose numbers.
Medical Professional: Good morning Mrs. Rodriguez. I see you are here today for high blood sugar because of your diabetes. (Explanation) Can you share why you think you have recently had higher numbers than normal?
Mrs. Rodriguez: Good morning Doctor. Yes, I am usually very good with my numbers but lately they have gone up and I know why.
Medical Professional: Yes, that is good that you have had your glucose managed. (Explanation) What has caused your numbers to go up Mrs. Rodriguez?
Mrs. Rodriguez: All this American food. I went on a trip to visit my daughter and all we did was eat out, hamburgers, fast food restaurants. They do not cook at home and we were always doing something so I could not cook. It was terrible, all we did was keep busy out and about, I was tired. I spent so much money on food that has chemicals. Look at me now. I can’t seem to get my numbers down.
Medical Professional: Oh, I understand. Yes, a trip can sometimes mess with our routine. (Treatment) Since you have been good at managing your glucose in the past what have you been doing now to get your glucose in normal range?
Mrs. Rodriguez: Well I have been doing the same thing I have always been doing. Eating healthy, resting, gardening, and praying.
Medical Professional: Gardening? That’s really nice. What do you garden?
Mrs. Rodriguez: Oh I love gardening. I plant all types of herbs, vegetables, flowers.
Medical Professional: That is so good Mrs. Rodriguez. I wish I had more time to garden. Do you use your own vegetable and herbs when you cook?
Mrs. Rodriguez: Haha. Yes of course. That is why my sugar was fine before I went on this trip. I rely on my garden to keep me healthy.
Medical Professional: There are so many herbs that are helpful for diabetes. (Treatment) Do you use any to help with your diabetes?
Mrs. Rodriguez: Well yes, in fact, I do. I know you doctors don’t like us to use our herbs but I do. And that was what keeps my sugars normal.
Medical Professional: Oh Mrs. Rodriguez, yes sometimes you hear doctors say this but some herbs are helpful. We just like to know what other things our patients do so we know how to make sure your medications work with certain herbs. (Treatment) I know many people use nopal (cactus), do you eat nopal?
Mrs. Rodriguez: ¿Como no? (of course). I eat them all the time. I make my morning licuado (drink); a little bit of parsley, oregano, oatmeal, lemon, nopal mixed with milk and yogurt.
Medical Professional: (Treatment) Sounds good, what else do you use?
Mrs. Rodriguez: Oh you know other things. Apple cider, cinnamon, cayenne.
Medical Professional: All from your garden?
Mrs. Rodriguez: Yes.
Medical Professional: (Treatment) Do you use any type of herbal supplements from stores or online?
Mrs. Rodriguez: My neighbor sells supplements specifically for diabetes. I started to use a natural supplement with cinnamon, vitamin D, and fish oil. All very natural.
Medical Professional: (Healer) Oh does your neighbor also have diabetes?
Mrs. Rodriguez: No, she sells products. But she sells to many people with diabetes and the supplement works. We get together and she tells us about how they work.
Medical Professional: Do you know the name of this supplement Mrs. Rodriguez?
Mrs. Rodriguez: Oh, gluco…something, it has a heart in the name. But I read the ingredients and it has only natural ingredients. (An FDA banned supplement for false claims)
Medical Professional: Oh I see. I may be familiar with that. Can you bring the supplement along with the medications I have prescribed? I just want to make sure there is not interaction between the two. To get your glucose back to normal I want to make sure we think of every possible situation that could be causing your high numbers. (Treatment) How have you been taking the supplement and the prescribed medications?
Mrs. Rodriguez: Well, I have not refilled your prescription. I was doing so well with my numbers, I’d rather go natural than take all those chemicals.
Medical Professional: Oh, I see Mrs. Rodriguez. Okay, you have done so well controlling your glucose before your trip and now we are in a situation where your numbers are not coming down so let’s try to figure this out. I’d like to learn more about this supplement, so for our next visit can you bring in your supplements so I can take a look at it? (Negotiate) We can then talk about the benefits or cautions. But in the meantime I’d like you to refill your medication and take as followed to see if that helps your sugars. (Negotiate) What do you think? Is this possible?
Mrs. Rodriguez: Oh Doctor, I just don’t like taking chemicals.
Medical Professional: I understand Mrs. Rodriguez. You did take them to start when you first came in for diabetes, is this correct?
Mrs. Rodriguez: Well yes but, I slowly got off them.
Medical Professional: I know it’s difficult to take medications every day but they can help in addition to your healthy eating. I know you are concerned about medications but for now we have to focus on getting your numbers down or your diabetes could become worse and we don’t want you to get there. Do you agree? (Negotiating process)
Mrs. Rodriguez: Well, I am concerned about my numbers.
Medical Professional: (Intervention) Okay well let’s try to get back to where you were before the trip. Let’s get you back on the medication and let’s see if this helps. (Negotiate) For the next visit would you be willing to bring any supplements you are taking along with the medication? (Collaboration) We can talk about the benefits and cautions for the medications and supplements. How does this sound?
Mrs. Rodriguez: Well, I am here to fix my numbers. I have everything I take in a box so I can bring that.
Medical Professional: Yes that would be great. (Collaboration) We can both talk about your daily routine and what have you learned about the supplement, any information or papers that you have, in addition to the medication I prescribed.
Mrs. Rodriguez: Yes I can do that.
Medical Professional: Thank you Mrs. Rodriguez. (Intervention) Also, I’ll have the nurse call you today or tomorrow and you can give her the name of the supplement and she’ll make sure the drug store has a refill for you. Would this work for you Mrs. Rodriguez?
Mrs. Rodriguez: Yes Doctor. You can call me. I’ll have the list ready.
BATHE
Unlike the BELIEF and ETHNIC instruments, the BATHE mnemonic (Lieberman 1999)
- B: Background (What is going on in your life?)
- A: Affect (How do you feel about what is going on?)
- T: Trouble (What troubles you most?)
- H: Handling (How are you handling that?)
- E: Empathy (This must be very difficult for you)
Vignette 3
The last vignette features Mr. Gonzalez, who typically shows a positive outlook on life when visiting his doctor. He is a patient who would not necessarily discuss his emotions if not asked specific questions about his emotional well-being.
Medical Professional: Hello Mr. Gonzalez. (Background) How are you doing today? What’s new? What’s going on in your life lately?
Mr. Gonzalez: Hey, Doctor! I’m good you know just living day to day.
Medical Professional: Good. (Affect) So how is your diabetes treating you day to day? How are you feeling with life and managing your diabetes?
Mr. Gonzalez: Ah well you know, just dealing with it as best as I can.
Medical Professional: Ah okay. As best as you can. (Troubles) What troubles you the most about managing diabetes?
Mr. Gonzalez: Well you know the aches and pains. But what can I do.
Medical Professional: (Affect) How do you feel about those aches and pains?
Mr. Gonzalez: Well it does limit me. I can’t move as well as I use to.
Medical Professional: (Handling) Hmm. I see. How are you handling those aches and pains? What are you doing to relieve it?
Mr. Gonzalez: I do my best with pain cream.
Medical Professional: (Empathy) Pains and aches, that must be difficult. (Affect) How do the aches and pains make you feel?
Mr. Gonzalez: Ahh, Doc, it’s not the same. You know I can’t do the same things anymore.
Medical Professional: (Background) What do you mean? What is not the same anymore?
Mr. Gonzalez: This diabetes, I’m not the same person. I use to be able to be there for my family and community and now I feel like I can’t be there for them the way I use to. I use to be the strong one for my family, helping those in need, and now I’m limited, my body is limited.
Medical Professional: (Affect) How do you feel about that? How does it make you feel emotionally and physically?
Mr. Gonzalez: Bad. I feel bad about it.
Medical Professional: Bad emotionally or physically?
Mr. Gonzalez: Both
Medical Professional: I see. (Handling) How are you dealing with the emotional part of it?
Mr. Gonzalez: I don’t know. I don’t know how.
Medical Professional: (Empathy) Dealing with diabetes and how it makes your body feel can be very emotionally distressing. It is common to feel this way but I want to make sure we also work on how you feel emotionally or how your emotions is affecting your diabetes.
Conclusion
Three mnemonic tools have been suggested to initiate patient-centered and culture-centered communication with patients. Beyond the use of these instruments, there are 2 key skills that are essential for engaging a Hispanic/Latino patient. The first is a non-judgmental, warm communication approach, and the second is astute probing. Once when I was interpreting for a Spanish-speaking Hispanic/Latino patient and English-speaking doctor, the patient expressed to me that she felt that the medical professionals “tienen una cultura fría” (“have a cold culture”), and she did not feel comfortable sharing more about herself because of it. It is also important for medical professionals to be aware of a patient’s doublespeak as a way to share enough information but not all information to keep from being judged by medical professionals. Thus, non-judgmental probing can uncover important information that may be useful for collaborative goal setting and treatment decisions.
The management of diabetes is multifaceted and complex, particularly for populations who face social barriers and challenges. The Hispanic/Latino population is more likely to encounter disparities in access to quality health care and disparities in social determinants of health compared to non-Hispanic whites [4–9]. Therefore, it is important for health professionals to engage Hispanic/Latino patients in self-care by eliciting information that best facilitates collaborative goal setting. Health professionals are in an influential position to leverage a communication style that is empathetic, trusting, and open, setting the tone for a positive patient-physician encounter and, in turn, positive patient outcomes [18–20].
Corresponding author: Jeannie Belinda Concha, PhD, MPH, Dept. of Public Health Sciences, The University of Texas at El Paso, 500 W. University Ave., El Paso, TX 79968, jeannie@utep.edu.
Funding support: Support for this research was provided by the Office of Research and Sponsored Projects at The University of Texas at El Paso.
Financial disclosures: None.
1. American Diabetes Association. American Diabetes Association Standards of Medical Care in Diabetes. Diabetes Care 2017; 40: Suppl 1.
2. Dominguez K, Penman-Aguilar A, Chang MH, et al. Vital signs: Leading causes of death, prevalence of diseases and risk factors, and use of health services among Hispanics in the United States, 2009–2013. MMWR 2015;64:1–10.
3. Commission on Social Determinants of Heath. Closing the gap in a generation: health equity through action on the social determinants of health. Final report on the Commission on Social Determinants of Health. Geneva, World Health Organization. Accessed 10 Sept 2017 at http://apps.who.int/iris/bitstream/10665/43943/1/9789241563703_eng.pdf.
4. Laiterapong N, Fairchild PC, Chou CH, et al. Revisiting disparities in quality of care among US adults with diabetes in the era of individualized care, NHANES 2007-2010. Med Care 2015;53:25–31.
5. Vaccaro JA, Feaster DJ, Lobar SL, et al. Medical advice and diabetes self-management reported by Mexican-American, Black, and White-non-Hispanic adults across the United States. BMC Public Health 2012;12:185.
6. Correa-de-Araujo R, McDermott K, Moy E. Gender differences across racial and ethnic groups in quality of care for diabetes. Women Health Iss 2006;16:56–65.
7. Chawla N, Rodriguez MA, Babey SH, Brown ER. Health policy fact sheet: diabetes among Latinos in California; disparities in access and management. UCLA Center for Health Policy Research. Accessed 1 Aug 2017 at http://healthpolicy.ucla.edu/publications/Documents/PDF/Diabetes%20among%20Latinos%20in%20California%20Disparities%20in%20Access%20and%20Management.pdf.
8. Pu J, Chewning B. Racial differences in diabetes preventive care. Res Social Adm Pharm 2013;9:790–6.
9. Institute of Medicine. Unequal treatment: Confronting racial and ethnic disparities in healthcare. Washington, DC: National Academies Press; 2003.
10. Saha S, Arbeaez JJ, Cooper LA. Patient-physician relationships and racial disparities in the quality of care. Am J Public Health 2003;93:1713–9.
11. What is cultural and linguistic competence?: Definitions, February 2003. Agency for Healthcare Research and Quality, Rockville, MD. Accessed 28 Aug 2017 at http://www.ahrq.gov/pprofessionals/systems/primary -care/cultural-competence-mco/cultcompdef.html.
12. U.S. Department of Health and Human Services, Office of Minority Health. 2000. Assuring cultural competence in health care: Recommendations for National Standards and an outcomes-focused research agenda. Accessed 17 August 2017 at http://www.omhrc.gov/clas/finalpo.htm.
13. Zhao X. Relationships between sources of health information and diabetes knowledge in the US Hispanic population. Health Commun 2014;29:574–85.
14. Perchman ML, Flannagan D, Ferrer RL, Matamoras M. Communication compete c e, self-care behaviors, and glucose control in patients with type 2 diabetes. Patient Educ Couns 2009;77:55–9.
15. Reimann JOF, Talavera GA, Salmon M, et al. Cultural competence among physicians treating Mexican Americans who have diabetes: a structural model. Soc Sci Med 2004;59:2195–205.
16. Gordon HS, Gerber BS. What we’ve got here is a failure to communication. J Gen Intern Med 2011;26:104–6.
17. Gonzalez A, Salas D, Umpierrez GE. Special considerations on the management of Latino patients with type 2 diabetes mellitus. Curr Med Res Opin 2011;27:969–79.
18. Peek ME, Cargill A, Juang ES. Diabetes health disparities: A systematic review of health care interventions. Med Care Res Rev 2007;64(5 Supp):101S–156S.
19. Kutob RM, Bormanis J, Crago M, et al. Assessing culturally competent diabetes care with unannounced standardized patients. Fam Med 2013;45:400–8.
20. Weller SC, Baer RD, Garcia de Alba Garcia J, Salcedo Rocha AL. Are differences between patient and provider explanatory models of diabetes associated with patient self-management and glycemic control? J Health Care Poor Underserved 2013:24;1498–510.
21. Duta MJ. Communicating about culture and health: Theorizing culture-centered and cultural sensitivity approaches. Commun Theory 2007;17:304–28.
22. Concha JB, Mayer SD, Mezuk B, Avula D. Diabetes causation beliefs among Spanish speaking patients. Diabetes Educ 2015:42:116–25.
23. Arcury TA, Skelly AH, Gesler WM, et al. Diabetes meanings among those without diabetes: explanatory models of immigrant Latinos in rural North Carolina. Soc Sci Med 2004;59:2183–3.
24. Daniulaityte R. Making sense of diabetes: cultural models, gender and individual adjustment to type 2 diabetes in a Mexican community. Soc Sci Med 2004;59:1899–912.
25. Poss J, Jezewski MA. The role and meaning of susto in Mexican American’s explanatory model of type 2 diabetes. Med Anthropol Q 2002;16:360–77.
26. Weller SC, Baer RD, Pachter LM, et al. Latino beliefs about diabetes. Diabetes Care 1999;22:722–8.
27. United States Census Bureau. Language use. Accessed Sept 2017 at https://www.census.gov/topics/population/language-use/about.html.
28. Mezuk B, Albrecht S, Eaton WW, Golden SH. Depression and type 2 diabetes over the lifespan: a meta-analysis. Diabetes Care 2008;31:2383–90.
29. Li C, Ford ES, Strine TW, Mokdad AH. Prevalence of depression among US adults with diabetes. Diabetes Care 2007;31:105–7.
30. Ali S, Stone MA, Peters JL, Davies MJ, Khunti K. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 2006;24:1069–78.
31. Li C, Barker L, Ford ES, et al. Diabetes and anxiety In US adults: findings from the 2006 Behavioral Risk Factor Surveillance System. Diabetes Med 2008;25:878–81.
32. Concha JB, Mezuk B, Duran B. Culture-centered approaches: the relevance of assessing emotional health for Latinos with type 2 diabetes. BMJ Open Diab Res Care 2015;3.
33. Bentancourt JR, Green AR, Carillo Je, Park ER. Cultural competence and health care: Key perspectives and trends. Health Affairs 2015;24:499–506.
34. Association of American Medical Colleges. Cultural Competence Education 2005. Accessed Feb 2016 at https://www.aamc.org/download/54338/data/.
35. Dobbie AE, Medrano M, Tysinger J, Olney C. The BELIEF Instrument: A preclinical teaching tool to elicit patients’ health beliefs. Family Med 2003;35:316–9.
36. Levin SJ, Like RC, Gottlieb JE. ETHNIC: A framework for culturally competent ethical practice. Patient Care 2003;34:188–9.
37. Stuart MR, Leibermann JR. The fifteen-minute hour: applied psychotherapy for the primary care physician. New York: Praeger.
38. Pace EJ, Somerville NJ, Enyoha C, et al. Effects of a brief psychosocial intervention on inpatient satisfaction: a randomized control trial. Fam Med 2017;49:675–8.
1. American Diabetes Association. American Diabetes Association Standards of Medical Care in Diabetes. Diabetes Care 2017; 40: Suppl 1.
2. Dominguez K, Penman-Aguilar A, Chang MH, et al. Vital signs: Leading causes of death, prevalence of diseases and risk factors, and use of health services among Hispanics in the United States, 2009–2013. MMWR 2015;64:1–10.
3. Commission on Social Determinants of Heath. Closing the gap in a generation: health equity through action on the social determinants of health. Final report on the Commission on Social Determinants of Health. Geneva, World Health Organization. Accessed 10 Sept 2017 at http://apps.who.int/iris/bitstream/10665/43943/1/9789241563703_eng.pdf.
4. Laiterapong N, Fairchild PC, Chou CH, et al. Revisiting disparities in quality of care among US adults with diabetes in the era of individualized care, NHANES 2007-2010. Med Care 2015;53:25–31.
5. Vaccaro JA, Feaster DJ, Lobar SL, et al. Medical advice and diabetes self-management reported by Mexican-American, Black, and White-non-Hispanic adults across the United States. BMC Public Health 2012;12:185.
6. Correa-de-Araujo R, McDermott K, Moy E. Gender differences across racial and ethnic groups in quality of care for diabetes. Women Health Iss 2006;16:56–65.
7. Chawla N, Rodriguez MA, Babey SH, Brown ER. Health policy fact sheet: diabetes among Latinos in California; disparities in access and management. UCLA Center for Health Policy Research. Accessed 1 Aug 2017 at http://healthpolicy.ucla.edu/publications/Documents/PDF/Diabetes%20among%20Latinos%20in%20California%20Disparities%20in%20Access%20and%20Management.pdf.
8. Pu J, Chewning B. Racial differences in diabetes preventive care. Res Social Adm Pharm 2013;9:790–6.
9. Institute of Medicine. Unequal treatment: Confronting racial and ethnic disparities in healthcare. Washington, DC: National Academies Press; 2003.
10. Saha S, Arbeaez JJ, Cooper LA. Patient-physician relationships and racial disparities in the quality of care. Am J Public Health 2003;93:1713–9.
11. What is cultural and linguistic competence?: Definitions, February 2003. Agency for Healthcare Research and Quality, Rockville, MD. Accessed 28 Aug 2017 at http://www.ahrq.gov/pprofessionals/systems/primary -care/cultural-competence-mco/cultcompdef.html.
12. U.S. Department of Health and Human Services, Office of Minority Health. 2000. Assuring cultural competence in health care: Recommendations for National Standards and an outcomes-focused research agenda. Accessed 17 August 2017 at http://www.omhrc.gov/clas/finalpo.htm.
13. Zhao X. Relationships between sources of health information and diabetes knowledge in the US Hispanic population. Health Commun 2014;29:574–85.
14. Perchman ML, Flannagan D, Ferrer RL, Matamoras M. Communication compete c e, self-care behaviors, and glucose control in patients with type 2 diabetes. Patient Educ Couns 2009;77:55–9.
15. Reimann JOF, Talavera GA, Salmon M, et al. Cultural competence among physicians treating Mexican Americans who have diabetes: a structural model. Soc Sci Med 2004;59:2195–205.
16. Gordon HS, Gerber BS. What we’ve got here is a failure to communication. J Gen Intern Med 2011;26:104–6.
17. Gonzalez A, Salas D, Umpierrez GE. Special considerations on the management of Latino patients with type 2 diabetes mellitus. Curr Med Res Opin 2011;27:969–79.
18. Peek ME, Cargill A, Juang ES. Diabetes health disparities: A systematic review of health care interventions. Med Care Res Rev 2007;64(5 Supp):101S–156S.
19. Kutob RM, Bormanis J, Crago M, et al. Assessing culturally competent diabetes care with unannounced standardized patients. Fam Med 2013;45:400–8.
20. Weller SC, Baer RD, Garcia de Alba Garcia J, Salcedo Rocha AL. Are differences between patient and provider explanatory models of diabetes associated with patient self-management and glycemic control? J Health Care Poor Underserved 2013:24;1498–510.
21. Duta MJ. Communicating about culture and health: Theorizing culture-centered and cultural sensitivity approaches. Commun Theory 2007;17:304–28.
22. Concha JB, Mayer SD, Mezuk B, Avula D. Diabetes causation beliefs among Spanish speaking patients. Diabetes Educ 2015:42:116–25.
23. Arcury TA, Skelly AH, Gesler WM, et al. Diabetes meanings among those without diabetes: explanatory models of immigrant Latinos in rural North Carolina. Soc Sci Med 2004;59:2183–3.
24. Daniulaityte R. Making sense of diabetes: cultural models, gender and individual adjustment to type 2 diabetes in a Mexican community. Soc Sci Med 2004;59:1899–912.
25. Poss J, Jezewski MA. The role and meaning of susto in Mexican American’s explanatory model of type 2 diabetes. Med Anthropol Q 2002;16:360–77.
26. Weller SC, Baer RD, Pachter LM, et al. Latino beliefs about diabetes. Diabetes Care 1999;22:722–8.
27. United States Census Bureau. Language use. Accessed Sept 2017 at https://www.census.gov/topics/population/language-use/about.html.
28. Mezuk B, Albrecht S, Eaton WW, Golden SH. Depression and type 2 diabetes over the lifespan: a meta-analysis. Diabetes Care 2008;31:2383–90.
29. Li C, Ford ES, Strine TW, Mokdad AH. Prevalence of depression among US adults with diabetes. Diabetes Care 2007;31:105–7.
30. Ali S, Stone MA, Peters JL, Davies MJ, Khunti K. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 2006;24:1069–78.
31. Li C, Barker L, Ford ES, et al. Diabetes and anxiety In US adults: findings from the 2006 Behavioral Risk Factor Surveillance System. Diabetes Med 2008;25:878–81.
32. Concha JB, Mezuk B, Duran B. Culture-centered approaches: the relevance of assessing emotional health for Latinos with type 2 diabetes. BMJ Open Diab Res Care 2015;3.
33. Bentancourt JR, Green AR, Carillo Je, Park ER. Cultural competence and health care: Key perspectives and trends. Health Affairs 2015;24:499–506.
34. Association of American Medical Colleges. Cultural Competence Education 2005. Accessed Feb 2016 at https://www.aamc.org/download/54338/data/.
35. Dobbie AE, Medrano M, Tysinger J, Olney C. The BELIEF Instrument: A preclinical teaching tool to elicit patients’ health beliefs. Family Med 2003;35:316–9.
36. Levin SJ, Like RC, Gottlieb JE. ETHNIC: A framework for culturally competent ethical practice. Patient Care 2003;34:188–9.
37. Stuart MR, Leibermann JR. The fifteen-minute hour: applied psychotherapy for the primary care physician. New York: Praeger.
38. Pace EJ, Somerville NJ, Enyoha C, et al. Effects of a brief psychosocial intervention on inpatient satisfaction: a randomized control trial. Fam Med 2017;49:675–8.
Which interventions are effective in managing parental vaccine refusal?
EVIDENCE SUMMARY
A systematic review analyzed 30 predominantly US studies with more than 8000 patients published between 1990 and 2012 (4 RCTs, 7 nonrandomized clinical trials, 13 before/after intervention trials, and 6 evaluation studies) to evaluate interventions that decreased parental vaccine refusal and hesitancy.1 Interventions included: change in state law, changes in state and school policies, and family-centered education initiatives.
Four studies that evaluated the impact of state laws concerning personal exemption (in addition to religious exemption) consistently found that total nonmedical exemption rates were higher in states that allowed personal exemptions. One nationwide survey found that total nonmedical exemption rates were 2.54 times higher (95% confidence interval [CI], 1.68-3.83) in states that allowed personal exemption than in states where only religious nonmedical exemption was allowed.
Fifteen studies evaluated the impact of educational initiatives on parental attitude towards vaccination; 8 of them reported statistically significant changes. None of the studies demonstrated a change in vaccination rates, however. Citing the generally low quality of the studies, the review authors concluded that they didn’t have convincing evidence that educational interventions reduced vaccine hesitancy.
Herd immunity is an iffy motivator
A systematic review analyzed 29 studies from western nations (17 qualitative and 12 quantitative, 4650 patients) regarding willingness to immunize children for the benefit of the community.2 Of the 17 qualitative studies, only 2 (164 patients) identified benefit to others as a motivating factor in parents’ decisions to immunize their children. In the 12 quantitative studies, a wide range of parents (1% to 60%) rated the concept of benefit to others as a reason for immunization. Overall, approximately one-third of parents listed herd immunity as a motivating reason. The authors concluded that the high heterogeneity of the studies made it unclear whether herd immunity was a motivating factor in childhood immunizations.
Multifaceted interventions, education, and tailored approaches may all work
A systematic review of international studies published between 2007 and 2013 investigated interventions to increase uptake of routinely recommended immunizations in groups with vaccine hesitancy and reduced use.3 Authors identified 189 articles (trial types and number of patients not given) that provided outcome measures.
Interventions that resulted in at least a 25% increase in vaccine uptake were primarily multifaceted, including elements of: targeting undervaccinated populations, improving access or convenience, educational initiatives, and mandates. Interventions that produced a greater than 20% increase in knowledge were generally educational interventions embedded in routine processes such as clinic visits.
The authors noted wide variation between studies in effect size, settings, and target populations. They concluded that interventions tailored to specific populations and concerns were likely to work best.
Corrective information doesn’t help with the most worried parents
A subsequent RCT tested whether correcting the myth that the flu vaccine can give people the flu would reduce belief in the misconception, increase perceptions that the flu vaccine is safe, and increase vaccination intent.4 Respondents to a national online poll of 1000 people received one of 3 interventions: correctional education (information debunking the myth), risk education (information about the risks of influenza infection), or no additional education.
Corrective information about the flu vaccine reduced the false belief that the vaccine can cause the flu by 15% to 20% and that the flu vaccine is unsafe by 5% to 10% (data from graphs; P<.05 for both effects). However, corrective information actually decreased parental intention to vaccinate among the group most concerned about the adverse effects of the vaccine (data from graph and text: +5% in the low-concern group vs −18% in the high-concern group; P<.05).
A presumptive approach works—but at a cost
A subsequent observational study videotaped 111 patient-provider vaccine discussions.5 Researchers categorized the initiation of the vaccine discussion as presumptive (eg, “We have to do some shots.”) or participatory (eg, “What do you want to do about shots?”). Using a presumptive style was more likely to result in acceptance of all recommended vaccines by the end of the visit (90% vs 17%; P<.05), but it decreased the chance of a highly rated visit experience (63% vs 95%; P<.05).
RECOMMENDATIONS
The 2015 Centers for Disease Control and Prevention (CDC) Pink Book recommends a combination of strategies, aimed at both providers and the public, for increasing and maintaining high immunization rates. The Pink Book advises providers to be ready to address vaccine safety concerns raised by parents.6
In a 2012 guideline, the CDC encouraged providers to listen attentively, be ready with scientific information and reliable resources, and use appropriate anecdotes in communicating with vaccine-hesitant parents.7 The guideline recommended against excluding families who refuse vaccination from the practice.
1. Sadaf A, Richards JL, Glanz J, et al. A systematic review of interventions for reducing parental vaccine refusal and vaccine hesitancy. Vaccine. 2013;31:4293-42304.
2. Quadri-Sheriff M, Hendrix K, Downs S, et al. The role of herd immunity in parents’ decision to vaccinate children: a systematic review. Pediatrics. 2012;130:522-530.
3. Jarrett C, Wilson R, O’Leary M, et al. Strategies for addressing vaccine hesitancy: a systematic review. Vaccine. 2015;33:4180-4190.
4. Nyhan B, Reifler J. Does correcting myths about the flu vaccine work? An experimental evaluation of the effects of corrective information. Vaccine. 2015;33:459-464.
5. Opel DJ, Mangione-Smith R, Robinson JD, et al. The influence of provider communication behaviors on parental vaccine acceptance and visit experience. Am J Public Health. 2015;105:1998-2004.
6. Centers for Disease Control and Prevention. Immunization Strategies for Healthcare Practices and Providers. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/strat.html. Accessed May 11, 2016.
7. Centers for Disease Control and Prevention. Provider Resources for Vaccine Conversations with Parents. Available at: http://www.cdc.gov/vaccines/hcp/conversations/about-vacc-conversations.html. Accessed May 11, 2016.
EVIDENCE SUMMARY
A systematic review analyzed 30 predominantly US studies with more than 8000 patients published between 1990 and 2012 (4 RCTs, 7 nonrandomized clinical trials, 13 before/after intervention trials, and 6 evaluation studies) to evaluate interventions that decreased parental vaccine refusal and hesitancy.1 Interventions included: change in state law, changes in state and school policies, and family-centered education initiatives.
Four studies that evaluated the impact of state laws concerning personal exemption (in addition to religious exemption) consistently found that total nonmedical exemption rates were higher in states that allowed personal exemptions. One nationwide survey found that total nonmedical exemption rates were 2.54 times higher (95% confidence interval [CI], 1.68-3.83) in states that allowed personal exemption than in states where only religious nonmedical exemption was allowed.
Fifteen studies evaluated the impact of educational initiatives on parental attitude towards vaccination; 8 of them reported statistically significant changes. None of the studies demonstrated a change in vaccination rates, however. Citing the generally low quality of the studies, the review authors concluded that they didn’t have convincing evidence that educational interventions reduced vaccine hesitancy.
Herd immunity is an iffy motivator
A systematic review analyzed 29 studies from western nations (17 qualitative and 12 quantitative, 4650 patients) regarding willingness to immunize children for the benefit of the community.2 Of the 17 qualitative studies, only 2 (164 patients) identified benefit to others as a motivating factor in parents’ decisions to immunize their children. In the 12 quantitative studies, a wide range of parents (1% to 60%) rated the concept of benefit to others as a reason for immunization. Overall, approximately one-third of parents listed herd immunity as a motivating reason. The authors concluded that the high heterogeneity of the studies made it unclear whether herd immunity was a motivating factor in childhood immunizations.
Multifaceted interventions, education, and tailored approaches may all work
A systematic review of international studies published between 2007 and 2013 investigated interventions to increase uptake of routinely recommended immunizations in groups with vaccine hesitancy and reduced use.3 Authors identified 189 articles (trial types and number of patients not given) that provided outcome measures.
Interventions that resulted in at least a 25% increase in vaccine uptake were primarily multifaceted, including elements of: targeting undervaccinated populations, improving access or convenience, educational initiatives, and mandates. Interventions that produced a greater than 20% increase in knowledge were generally educational interventions embedded in routine processes such as clinic visits.
The authors noted wide variation between studies in effect size, settings, and target populations. They concluded that interventions tailored to specific populations and concerns were likely to work best.
Corrective information doesn’t help with the most worried parents
A subsequent RCT tested whether correcting the myth that the flu vaccine can give people the flu would reduce belief in the misconception, increase perceptions that the flu vaccine is safe, and increase vaccination intent.4 Respondents to a national online poll of 1000 people received one of 3 interventions: correctional education (information debunking the myth), risk education (information about the risks of influenza infection), or no additional education.
Corrective information about the flu vaccine reduced the false belief that the vaccine can cause the flu by 15% to 20% and that the flu vaccine is unsafe by 5% to 10% (data from graphs; P<.05 for both effects). However, corrective information actually decreased parental intention to vaccinate among the group most concerned about the adverse effects of the vaccine (data from graph and text: +5% in the low-concern group vs −18% in the high-concern group; P<.05).
A presumptive approach works—but at a cost
A subsequent observational study videotaped 111 patient-provider vaccine discussions.5 Researchers categorized the initiation of the vaccine discussion as presumptive (eg, “We have to do some shots.”) or participatory (eg, “What do you want to do about shots?”). Using a presumptive style was more likely to result in acceptance of all recommended vaccines by the end of the visit (90% vs 17%; P<.05), but it decreased the chance of a highly rated visit experience (63% vs 95%; P<.05).
RECOMMENDATIONS
The 2015 Centers for Disease Control and Prevention (CDC) Pink Book recommends a combination of strategies, aimed at both providers and the public, for increasing and maintaining high immunization rates. The Pink Book advises providers to be ready to address vaccine safety concerns raised by parents.6
In a 2012 guideline, the CDC encouraged providers to listen attentively, be ready with scientific information and reliable resources, and use appropriate anecdotes in communicating with vaccine-hesitant parents.7 The guideline recommended against excluding families who refuse vaccination from the practice.
EVIDENCE SUMMARY
A systematic review analyzed 30 predominantly US studies with more than 8000 patients published between 1990 and 2012 (4 RCTs, 7 nonrandomized clinical trials, 13 before/after intervention trials, and 6 evaluation studies) to evaluate interventions that decreased parental vaccine refusal and hesitancy.1 Interventions included: change in state law, changes in state and school policies, and family-centered education initiatives.
Four studies that evaluated the impact of state laws concerning personal exemption (in addition to religious exemption) consistently found that total nonmedical exemption rates were higher in states that allowed personal exemptions. One nationwide survey found that total nonmedical exemption rates were 2.54 times higher (95% confidence interval [CI], 1.68-3.83) in states that allowed personal exemption than in states where only religious nonmedical exemption was allowed.
Fifteen studies evaluated the impact of educational initiatives on parental attitude towards vaccination; 8 of them reported statistically significant changes. None of the studies demonstrated a change in vaccination rates, however. Citing the generally low quality of the studies, the review authors concluded that they didn’t have convincing evidence that educational interventions reduced vaccine hesitancy.
Herd immunity is an iffy motivator
A systematic review analyzed 29 studies from western nations (17 qualitative and 12 quantitative, 4650 patients) regarding willingness to immunize children for the benefit of the community.2 Of the 17 qualitative studies, only 2 (164 patients) identified benefit to others as a motivating factor in parents’ decisions to immunize their children. In the 12 quantitative studies, a wide range of parents (1% to 60%) rated the concept of benefit to others as a reason for immunization. Overall, approximately one-third of parents listed herd immunity as a motivating reason. The authors concluded that the high heterogeneity of the studies made it unclear whether herd immunity was a motivating factor in childhood immunizations.
Multifaceted interventions, education, and tailored approaches may all work
A systematic review of international studies published between 2007 and 2013 investigated interventions to increase uptake of routinely recommended immunizations in groups with vaccine hesitancy and reduced use.3 Authors identified 189 articles (trial types and number of patients not given) that provided outcome measures.
Interventions that resulted in at least a 25% increase in vaccine uptake were primarily multifaceted, including elements of: targeting undervaccinated populations, improving access or convenience, educational initiatives, and mandates. Interventions that produced a greater than 20% increase in knowledge were generally educational interventions embedded in routine processes such as clinic visits.
The authors noted wide variation between studies in effect size, settings, and target populations. They concluded that interventions tailored to specific populations and concerns were likely to work best.
Corrective information doesn’t help with the most worried parents
A subsequent RCT tested whether correcting the myth that the flu vaccine can give people the flu would reduce belief in the misconception, increase perceptions that the flu vaccine is safe, and increase vaccination intent.4 Respondents to a national online poll of 1000 people received one of 3 interventions: correctional education (information debunking the myth), risk education (information about the risks of influenza infection), or no additional education.
Corrective information about the flu vaccine reduced the false belief that the vaccine can cause the flu by 15% to 20% and that the flu vaccine is unsafe by 5% to 10% (data from graphs; P<.05 for both effects). However, corrective information actually decreased parental intention to vaccinate among the group most concerned about the adverse effects of the vaccine (data from graph and text: +5% in the low-concern group vs −18% in the high-concern group; P<.05).
A presumptive approach works—but at a cost
A subsequent observational study videotaped 111 patient-provider vaccine discussions.5 Researchers categorized the initiation of the vaccine discussion as presumptive (eg, “We have to do some shots.”) or participatory (eg, “What do you want to do about shots?”). Using a presumptive style was more likely to result in acceptance of all recommended vaccines by the end of the visit (90% vs 17%; P<.05), but it decreased the chance of a highly rated visit experience (63% vs 95%; P<.05).
RECOMMENDATIONS
The 2015 Centers for Disease Control and Prevention (CDC) Pink Book recommends a combination of strategies, aimed at both providers and the public, for increasing and maintaining high immunization rates. The Pink Book advises providers to be ready to address vaccine safety concerns raised by parents.6
In a 2012 guideline, the CDC encouraged providers to listen attentively, be ready with scientific information and reliable resources, and use appropriate anecdotes in communicating with vaccine-hesitant parents.7 The guideline recommended against excluding families who refuse vaccination from the practice.
1. Sadaf A, Richards JL, Glanz J, et al. A systematic review of interventions for reducing parental vaccine refusal and vaccine hesitancy. Vaccine. 2013;31:4293-42304.
2. Quadri-Sheriff M, Hendrix K, Downs S, et al. The role of herd immunity in parents’ decision to vaccinate children: a systematic review. Pediatrics. 2012;130:522-530.
3. Jarrett C, Wilson R, O’Leary M, et al. Strategies for addressing vaccine hesitancy: a systematic review. Vaccine. 2015;33:4180-4190.
4. Nyhan B, Reifler J. Does correcting myths about the flu vaccine work? An experimental evaluation of the effects of corrective information. Vaccine. 2015;33:459-464.
5. Opel DJ, Mangione-Smith R, Robinson JD, et al. The influence of provider communication behaviors on parental vaccine acceptance and visit experience. Am J Public Health. 2015;105:1998-2004.
6. Centers for Disease Control and Prevention. Immunization Strategies for Healthcare Practices and Providers. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/strat.html. Accessed May 11, 2016.
7. Centers for Disease Control and Prevention. Provider Resources for Vaccine Conversations with Parents. Available at: http://www.cdc.gov/vaccines/hcp/conversations/about-vacc-conversations.html. Accessed May 11, 2016.
1. Sadaf A, Richards JL, Glanz J, et al. A systematic review of interventions for reducing parental vaccine refusal and vaccine hesitancy. Vaccine. 2013;31:4293-42304.
2. Quadri-Sheriff M, Hendrix K, Downs S, et al. The role of herd immunity in parents’ decision to vaccinate children: a systematic review. Pediatrics. 2012;130:522-530.
3. Jarrett C, Wilson R, O’Leary M, et al. Strategies for addressing vaccine hesitancy: a systematic review. Vaccine. 2015;33:4180-4190.
4. Nyhan B, Reifler J. Does correcting myths about the flu vaccine work? An experimental evaluation of the effects of corrective information. Vaccine. 2015;33:459-464.
5. Opel DJ, Mangione-Smith R, Robinson JD, et al. The influence of provider communication behaviors on parental vaccine acceptance and visit experience. Am J Public Health. 2015;105:1998-2004.
6. Centers for Disease Control and Prevention. Immunization Strategies for Healthcare Practices and Providers. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/strat.html. Accessed May 11, 2016.
7. Centers for Disease Control and Prevention. Provider Resources for Vaccine Conversations with Parents. Available at: http://www.cdc.gov/vaccines/hcp/conversations/about-vacc-conversations.html. Accessed May 11, 2016.
Evidence-based answers from the Family Physicians Inquiries Network
EVIDENCE-BASED ANSWER:
It’s unclear whether educational initiatives alone alter vaccine refusal. Although about a third of parents cite herd immunity as motivation for vaccination, its efficacy in addressing vaccine hesitancy isn’t clear (strength of recommendation [SOR]: B, systematic reviews not limited to randomized controlled trials [RCTs]).
Multifaceted interventions (encompassing improved access to vaccines, immunization mandates, and patient education) may produce a ≥25% increase in vaccine uptake in groups with vaccine hesitancy and low utilization (SOR: B, extrapolated from a meta-analysis across diverse cultures).
Correcting false information about influenza vaccination improves perceptions about the vaccine, but may decrease intention to vaccinate in parents who already have strong concerns about safety (SOR: C, low-quality RCT).
Discussions about vaccines that are more paternalistic (presumptive rather than participatory) are associated with higher vaccination rates, but lower visit satisfaction (SOR: C, observational study).
Providers should thoroughly address patient concerns about safety and encourage vaccine use (SOR: C, expert opinion).

A Talking Map for Family Meetings in the Intensive Care Unit
From the Department of Neurology, Duke University Medical Center, Durham, NC (Dr. McFarlin), the Department of Psychosocial Oncology and Palliative Care, Dana-Farber Cancer Institute, Boston, MA (Dr. Tulsky), Harborview Medical Center, University of Washington, Seattle, WA (Dr. Back), and Department of Medicine, University of Pittsburgh, Pittsburgh, PA (Dr. Arnold).
Abstract
- Objective: To describe the use of a cognitive map for navigating family meetings with surrogate decision makers of patients in an intensive care unit.
- Methods: Descriptive report and discussion using an illustrative case to outline the steps in the cognitive map.
- Results: The use of cognitive maps has improved the ability of physicians to efficiently perform a specific communication skill. During a “goals of care” conversation, the cognitive map follows these steps: (1) Gather the clinical team for a pre-meeting, (2) Introduce everyone, (3) Use the “ask-tell-ask” strategy to communicate information, (4) Respond to emotion, (5) Highlight the patient’s voice, (6) Plan next steps, (7) Reflect on the meeting with the team. Providing this map of key communication skills will help faculty teach learners the core components of a family meeting.
- Conclusion: Practicing the behaviors demonstrated in the cognitive map may increase clinician skill during difficult conversations. Improving communication with surrogate decision makers will increase the support we offer to critically ill patients and their loved ones.
Key words: intensive care unit; communication; family meeting; critical illness; decision making; end of life care.
Family members of patients in the ICU value high-quality communication with the medical team. In fact, family members report that physicians’ communication skills are often more important than their medical skills [1]. Multiple professional societies, including the American Thoracic Society and the Society of Critical Care Medicine, define communication with families as a key component of high-quality critical care. Effective physician-patient communication improves measureable outcomes including decreased ICU length of stay [2] and may reduce distress amongst patients’ families [3]. The American College of Chest Physicians position statement on Palliative and End-of-Life Care for Patients with Cardiopulmonary Diseases urges physicians to develop curricula that incorporate interpersonal communication skills into training [4].
Unfortunately, such high-quality communication is not the norm. Surrogate decision makers are often displeased with the frequency of communication, the limited availability of attending physicians, and report feeling excluded from discussions [5]. When family meetings do occur, surrogate decision makers report inadequate understanding of diagnosis, prognosis, and treatment plans [6].
Physicians also find family meetings difficult. Intensivists worry that high-quality family meetings are time consuming and difficult to do in a busy ICU [7]. Critical care fellows report not feeling adequately trained to conduct family meetings [8]. It makes sense that untrained clinicians would want to avoid a conversation that is emotionally charged, particularly if one is unsure how to respond effectively.
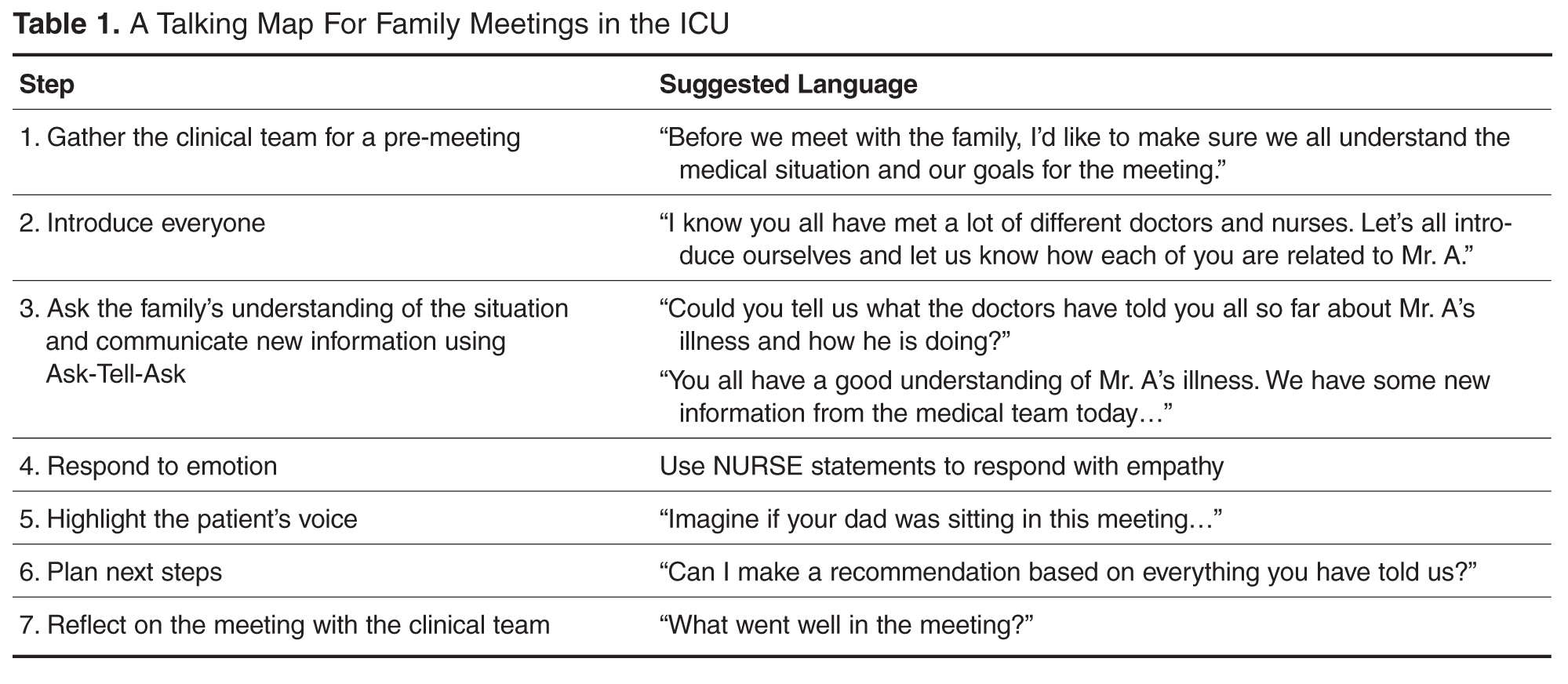
The Case of Mr. A
Thomas A. is a 79-year-old man admitted to the medical intensive care unit 7 days earlier with a large left middle cerebral artery territory infarction. Given his decreased mental status, on admission he was intubated for airway protection. He is awake but aphasic and unable to follow any commands or move his right side. The neurology consultants do not feel this will improve. He has significant secretions and episodes of hypoxia. He has also developed acute on chronic kidney injury and may need to start dialysis. The social worker explains that his need for dialysis limits his placement options and that he will not be able to be discharged to home. Given his lack of improvement the team is concerned he will need a tracheostomy and feeding tube placed in order to safely continue this level of care. A family meeting is arranged to understand Mr. A’s goals of care.
Talking Map Basics
Before each step is discussed in detail, some definitions are needed. “Family” can be defined as anyone important enough, biologically related or not, to be present at a conversation with a clinician [10]. Second, a “family meeting” is a planned event between the family and interdisciplinary members of the ICU team as well as any other health care providers who have been involved in the patient’s care. The meeting takes place in a private space and at a time that is scheduled with the families’ needs in mind. Thus it is different from having families present on rounds or one-off meetings with particular clinicians.
Goals of care meetings are typically held when, in the clinicians’ view, the current treatments are not achieving the previously stated goals. Thus, the meeting has 2 purposes: first, to give the family the bad news that the current plan is not working and second, to develop a new plan based on the patient’s values. The family’s job, as surrogate decision maker, is to provide information about what would be most important to the patient. The clinician’s job is to suggest treatment plans that have the best probability of matching the patient’s values.
Not all of these tasks need be done at once. Some families will not be able to move from hearing bad news to making a decision without having time to first reflect and grieve. Others will need to confer with other family members privately before deciding on a plan. In many cases, a time-limited trial may be the right option with a plan for subsequent meetings. Given this, we recommend checking in with the family between each step to ensure that they feel safe moving ahead. For example, one might ask “Is it OK if we talk about what happens next?”
Talking Map Steps in Detail
1. Gather the Clinical Team for a Pre-Meeting
ICU care involves a large interdisciplinary care team. A “meeting before the meeting” with the entire clinical team is an opportunity to reach consensus on prognosis and therapeutic options, share prior interactions with family, and determine goals for the family meeting. It is also helpful to clarify team members’ roles at the meeting and to choose a primary facilitator. All of this helps to ensure that the family receives a consistent message during the meeting. The pre-meeting is also an opportunity to ask a team member to observe the communication skills of the facilitator and be prepared to give feedback after the meeting.
At this time, the team should also create the proper environment for the family meeting. This includes a quiet room free of interruptions with ample seating, available tissues, and transferred pagers and cell phones.
The intensivist and bedside nurse should always be present at the family meeting, and it is best when the same attending can be at subsequent family meetings Their consistent dual presence provides the uniform communication from the team, can reduce anxiety in family members and the collaboration reduces ICU nurse and physician burnout [11]. For illnesses that involve a specific disease or organ system, it is important to have the specialist at the meeting who can provide the appropriate expertise.
The Pre-Meeting
A family meeting was scheduled in the family meeting room for 3 pm, after morning rounds. Thirty minutes prior to the meeting the medical team, including the MICU intensivist, the bedside nurse, the neurology attending who has been involved in the care, the case manager and 2 residents sat to discuss Mr. A’s care. The neurology team confirmed that this stroke was considered very large and would result in a level of disability that could only be cared for in a nursing home and would require both a tracheostomy and feeding tube for safe care. The bedside nurse relayed that the family had asked if Mr. A. would ever recover enough to get back to his home. The neurology team shared they did not expect much improvement at all. Given the worsening renal failure and need for dialysis the case manager reminded the team that Mr. A’s nursing home placements were limited. The team decided that the intensivist would lead the meeting as she had updated various family members on rounds for the past 4 days and would be on service for another week. The team decided that their goal for the meeting was to make sure the family understands that Mr. A’s several medical illnesses portend a poor prognosis. They recognized this may be breaking bad news to the family. They also wanted to better understand what Mr. A would have thought given this situation. The residents were asked to watch for the family’s responses when the team delivered the news.
2. Introduce Everyone
Each meeting should start with formal introductions. Even if most providers know most family members it is a polite way to start the meeting. Introducing each family member present and how they know the patient provides insight into how the family is constructed and makes decisions. For example, the entire family may defer to the daughter who introduces herself as a nurse. In other situations, although there is one legal decision maker, the family may explain that they make decisions by consensus.
Each member of the treating team should also introduce themselves. Even if the clinician has been working with the family, it is polite to be formal and give your name and role. Given the number of people the family sees every day, one should not assume that the family remembers all of the clinicians.
In teaching hospitals, providers should also help the family understand their level of training. Surrogates do not always understand the different roles or level of training between students, residents and fellows, advanced practice providers, consultants and their attending physicians. Uncertainty about the roles can lead to family members feeling as though they are receiving contradictory information. Family satisfaction decreases when multiple attending physicians are involved in a patient’s care [12]. When possible, a consistent presence among providers at family meetings is always best.
3. Ask the Family's Understanding of the Situation (Ask-Tell-Ask)
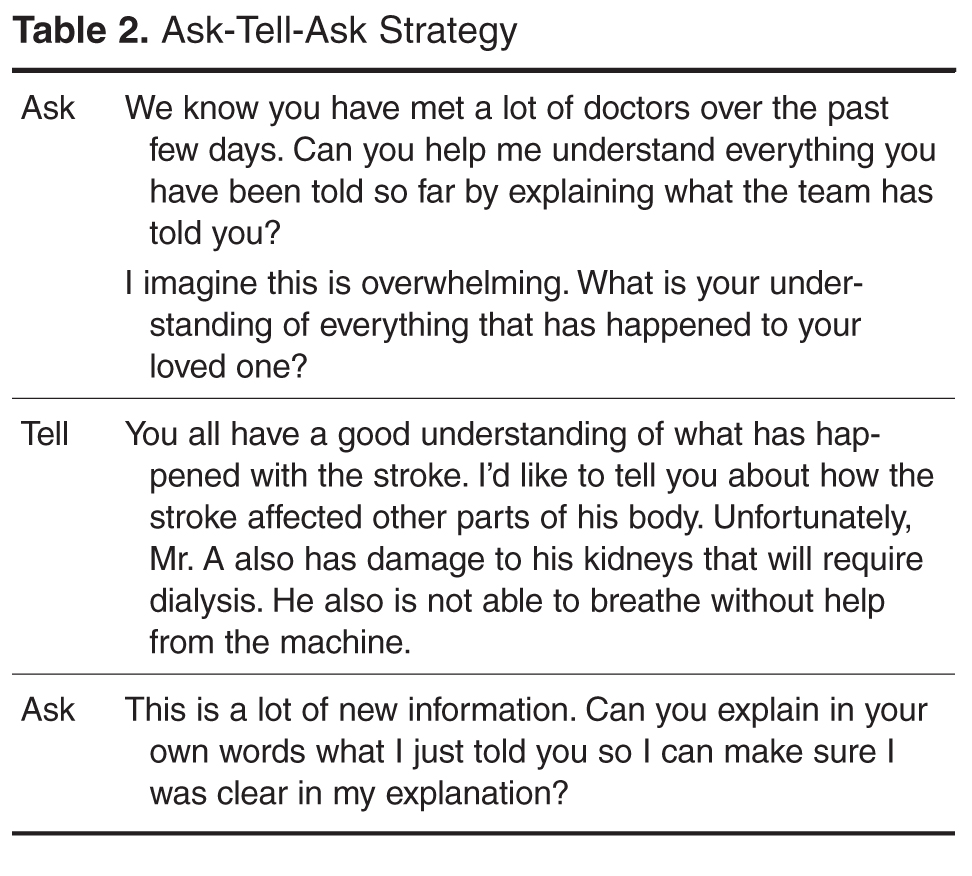
Asking the family to explain the situation in their own language reveals how well they understand the medical facts and helps the medical team determine what information will be most helpful to the family. An opening statement might be “We have all seen your dad and talked to many of his providers. It would help us all be on the same page if you can you tell me what the doctors are telling you?” Starting with the family’s understanding builds trust with the medical team as it creates an opportunity for the family to lead the meeting and indicates that the team is available to listen to their concerns. Asking surrogates for their understanding allows them to tell their story and not hear a reiteration of things they already know. Providing time for the family to share their perspective of the care elicits family’s concerns.
In a large meeting, ensure that all members of the family have an opportunity to communicate their concerns. Does a particular person do all of the talking? Are there individuals that do not speak at all? One way to further understand unspoken concerns during the meeting is to ask “I notice you have been quiet, what questions do you have that I can answer?” There may be several rounds of “asking” in order to ensure all the family members’ concerns are heard. Letting the family tell what they have heard helps the clinicians get a better idea of their health literacy. Do they explain information using technical data or jargon? Finally, as the family talks the clinicians can determine how surprising the “serious news” will be to them. For example, if the family says they know their dad is doing much worse and may die, the information to be delivered can be truncated. However if family incorrectly thinks their dad is doing better or is uncertain they will be much more surprised by the serious news.
After providing time for the family to express their understanding, tell them the information the team needs to communicate. When delivering serious news it is important to focus on the key 1 to 2 points you want the family to take away from the meeting. Typically when health care professionals talk to each other, they talk about every medical detail. Families find this amount of information overwhelming and are not sure what is most important, asking “So what does that mean?” Focusing on the “headline” helps the family focus on what you think the most important piece of information is. Studies suggest that what families most want to know is what the information means for the patient’s future and what treatments are possible. After delivering the new information, stop to allow the family space to think about what you said. If you are giving serious news, you will know they have heard what you said as they will get emotional (see next step).
Checking for understanding is the final “ask” in Ask-Tell-Ask. Begin by asking “What questions do you have?” Data in primary care has shown that patients are more likely to ask questions if you ask “what questions do you have” rather than “do you have any questions?” It is important to continue to ask this question until the family has asked all their questions. Often the family’s tough questions do not come until they get more comfortable and confident in the health care team. In cases where one family member is dominant it might also help to say “What questions do others have?” Next, using techniques like the “teach back” model the physician should check in to see what the family is taking away from the conversation. If a family understands, they can “teach back” the information accurately. This “ask” can be done in a way that does not make the family feel they are being tested: “I am not always clear when I communicate. Do you mind telling me back in your own words what you thought I said so I know we are on the same page?” This also provides an opportunity to answer any new questions that arise. Hearing the information directly from the family can allow the team to clarify any misconceptions and give insight into any emotional responses that the family might have.
4. Respond to Emotion
Discussing serious news in the ICU setting naturally leads to an emotional reaction. The clinician’s ability to notice emotional cues and respond with empathy is a key communication skill in family meetings [13]. Emotional reactions impede individual’s ability to process cognitive information and make it hard to think cognitively about what should be done next.
Physicians miss opportunities to respond to emotion in family meetings [14]. Missed opportunities lead to decreased family satisfaction and may lead to treatment decisions not consistent with the wishes of their loved ones. Empathic responses improve the family-clinician relationship and helps build trust and rapport [15]. Well- placed empathic statements may help surrogates disclose concerns that help the physician better understand the goals and values of the family and patient. Families also can more fully process cognitive information when their emotional responses have been attended to.
Physicians can develop the capacity to recognize and respond to the emotional cues family members are delivering. Intensivists should actively look for the emotions, the empathic opportunity, that are displayed by the family. This emotion is the “data” that will help lead to an empathic response. A family that just received bad news typically responds by showing emotion. Clues that emotions are present include: the family asking the same questions multiple times; using emotional words such as “sad” or “frustrated;” existential questions that do not have a cognitive answer such as “Why did God let this happen?;” or non-verbal cues like tears and hand wringing.
Sometimes the emotional responses are more difficult to recognize. Families may continue to ask for more cognitive information after hearing bad news. Someone keeps asking “Why did his kidney function worsen?” or “I thought the team said the chest x-ray looked better.” It is tempting to start answering these questions with more medical facts. However, if the question comes after bad news, it is usually an expression of frustration or sadness rather than a request for more information. Rather than giving information, it might help to acknowledge this by saying “I imagine this new is overwhelming.”
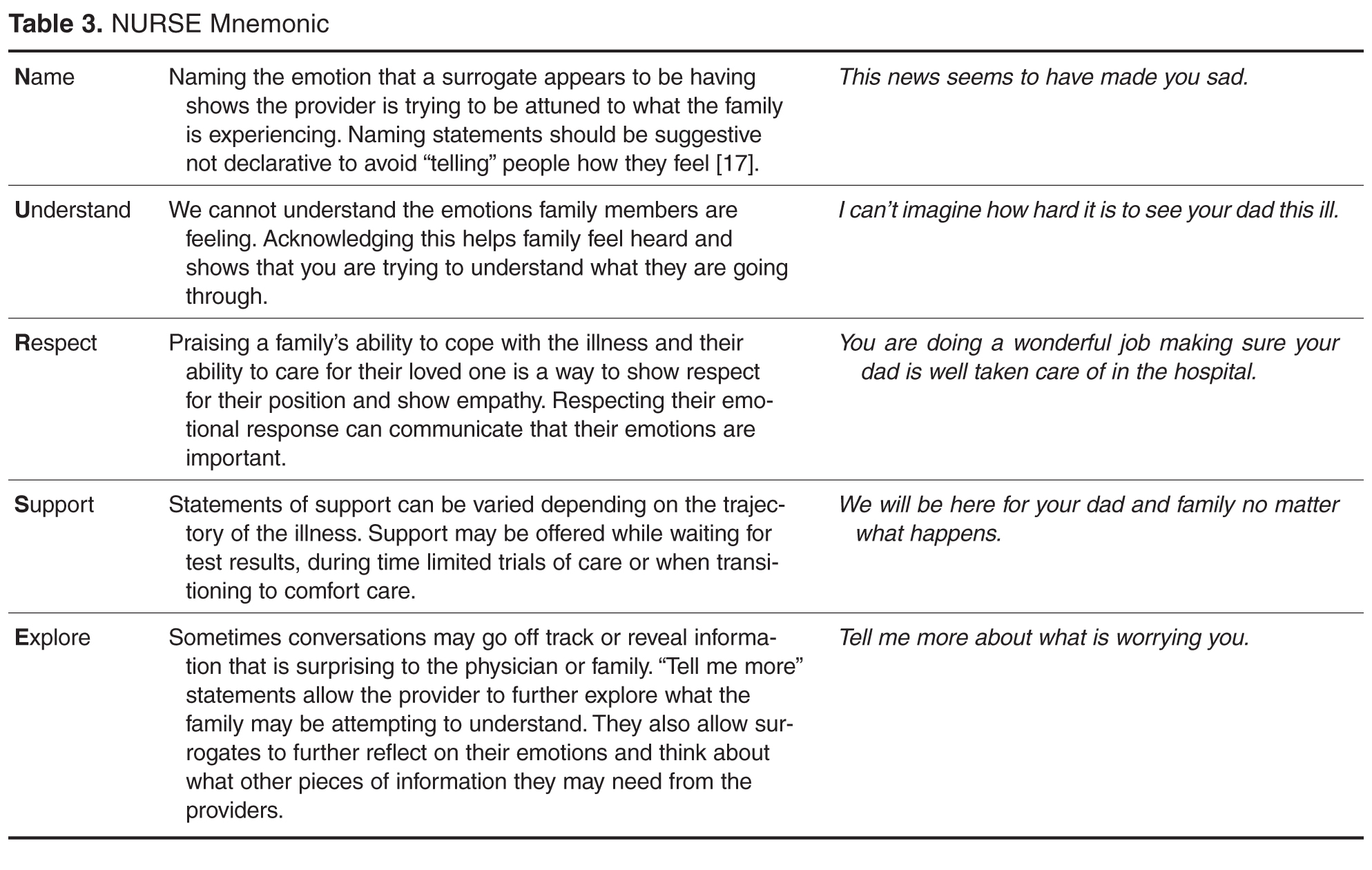
5. Highlight the Patient’s Voice
Family meetings are often used to develop new treatment plans (given that the old plans are not working). In these situations, it is essential to understand what the incapacitated patient would say if they were part of the family meeting. The surrogate’s primary role is to represent the patient’s voice. To do this, surrogates need assistance in applying their critically ill loved one’s thoughts and values to complex, possibly life limiting, situations. Surrogate decision makers struggle with the decisions’ emotional impact, as well as how to reconcile their desires with their loved one’s wishes [18]. This can lead them to make decisions that conflict with the loved one’s values [19] as well as emotional sequelae such as PTSD and depression [20].
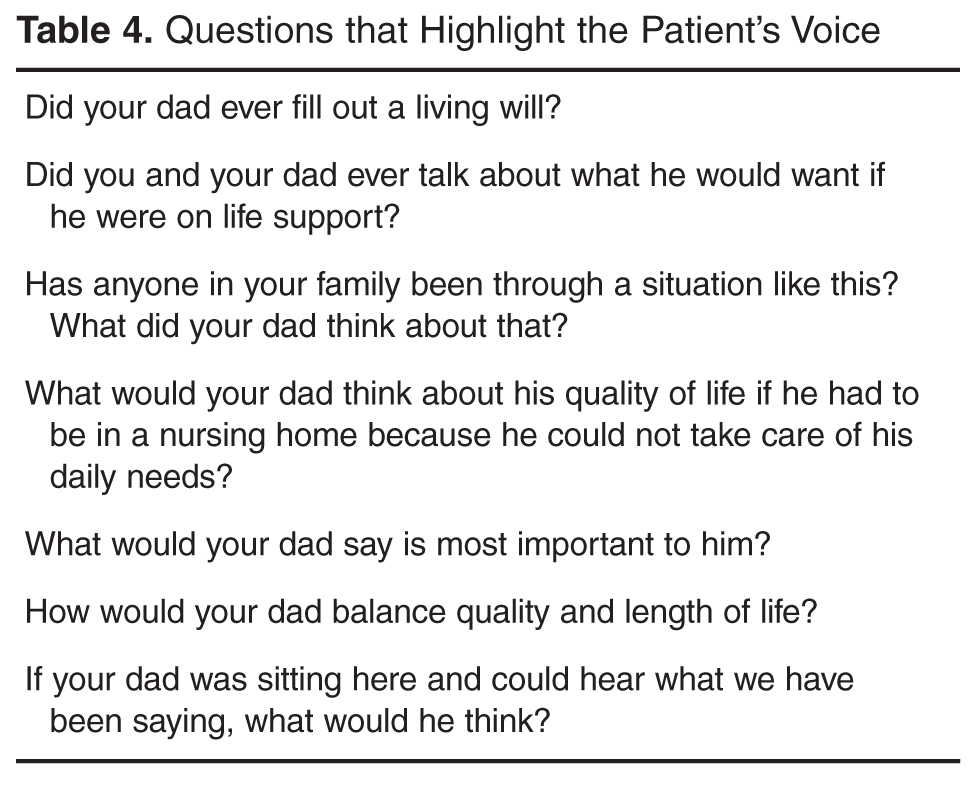
As families reflect on their loved one’s values, conflicting desires will arise. For example, someone may have wanted to live as long as possible and also values independence. Or someone may value their ability to think clearly more than being physically well but would not want to be physically dependent on artificial life support. Exploring which values would be more important can help resolve these conflicts.
Clinicians should check for understanding while family members are identifying the values of their loved ones. Providing the family with a summary of what you have heard will help ensure a more accurate understanding of these crucial issues. A summary statement might be, “It sounds like you are saying your dad really valued his independence. He enjoyed being able to take care of his loved ones and himself. Is that right?”
6. Plan Next Steps
The family meeting serves to attend to family emotion and allow space to elicit patients’ values. Following a family meeting surrogate decision makers may be able to begin to consider the next steps in their loved one’s care. If bad news was delivered they may need space to adjust to a different future than they expected. Using an empathic statement of support “We will continue to make sure we communicate with you as we work together to plan next steps” will reassure a family that they have time and space to plan for the future.
Families vary regarding how much physician input they desire in planning next steps [21]. You can explicitly ask how the team can best help the family with decisions: “Some families like to hear the options for next steps from the team and make a decision, other families like to hear a recommendation from the team. What would be the most helpful for you?” Throughout the course of an illness a surrogate’s preference for decision making may change and clinicians should be responsive to those changing needs.
If the surrogate wants a clinician’s recommendation, 3 points are worth stressing. First, the recommendation should be personalized to this patient and his values. The goal is to reveal how the understanding of the patient’s values led to the treatment plan offered. Second, the recommendation should focus primarily on what will be done to achieve the patient’s values. Focusing on what the clinicians will do may help the family feel that the clinicians are still “trying” and not abandoning their loved one. In this case, the team will continue medical care that will help the patient regain/maintain independence. Only after talking about what will be done should the clinician point out that certain interventions will not achieve the patient’s goals and thus will not be done:
“It sounds like your father really valued his independence and that this illness has really taken that away. Knowing this, would it be helpful for me to make a recommendation for next steps?” “I think we should continue providing excellent medical care for your father in hopes he can get better and go home. One the other hand, if he gets worse, we should not use therapies such as CPR or dialysis that are unlikely to help him regain his independence.”
Finally, be concrete when planning next steps. If a time-limited trial of a therapy is proposed, make sure the family understands what a successful and unsuccessful trial will look like. Make plans to meet again on a specific date in order to ensure the family understands the progress being made. If a transition to comfort care is agreed upon, ensure support of the entire family during the next hours to days and offer services such as chaplaincy or child life specialists.
A family may not agree with the recommendation and back and forth discussion can help create a plan that is in line with their understanding of the illness. Rather than convincing, a clinician should keep an open mind about why they and the surrogate disagree. Do they have different views about the patient’s future? Did the medical team misunderstand the patient’s values? Are there emotional factors that inhibit the surrogate’s ability to attend to the discussion? It is only by learning where the disagreement is that a clinician can move the conversation forward.
A surrogate may ask about a therapy that is not beneficial or may increase distress to the patient. The use of “I wish” or “I worry” statements can be helpful at these points. These specific phrases recognize the surrogate’s desire to do more but also imply that the therapies are not helpful.
“I wish that his ability to communicate and tell you what he wants would get better with a little more time as well.”
“I worry that waiting 2 more weeks for improvement will actually cause complications to occur.”
7. Reflect
Family meetings have an impact on both the family and the medical team. Following the meeting, a short debriefing with the clinical team can be helpful. Summarizing the events of the meeting ensures clarity about the treatment plan going forward. It provides team members a chance to discuss conflicts that may have arisen. It allows the participants in the meeting to reflect on what communication skills they used and how they can improve their skills going forward.
Conclusion
Family meetings with surrogate decision makers must navigate multiple agendas of the family and providers. The goal of excellent communication with surrogates in an ICU should be to understand the patient’s goals and values and seek to make treatment plans that align with their perspective. This talking map provides a conceptual framework for physicians to guide a family through these conversations. The framework creates an opportunity to focus on the patient’s values and preferences for care while allowing space to attend to emotional responses to reduce the distress inherent in surrogate decision-making. Practicing the behaviors demonstrated in the talking map may increase clinician skill during difficult conversations. Improving communication with surrogate decision makers will increase the support we offer to critically ill patients and their loved ones.
Corresponding author: Jessica McFarlin, MD, jessmcfarlin@gmail.com.
Funding/support: Dr. Arnold receives support though the Leo H. Criep Chair in Patient Care.
Financial disclosures: None.
1. Hickey M. What are the needs of families of critically ill patients? A review of the literature since 1976. Heart Lung 1990;19:401–15.
2. Mosenthal AC, Murphy PA, Barker LK, et al. Changing culture around end-of-life care in the trauma intensive care unit. J Trauma 2008;64:1587–93.
3. Lautrette A, Darmon M, Megarbane B, et al. A communication strategy and brochure for relatives of patients dying in the ICU. N Engl J Med 2007;356:469–78.
4. Selecky PA, Eliasson AH, Hall RI, et al. Palliative and end-of-life care for patients with cardiopulmonary diseases. Chest 2005;128:3599–610.
5. Henrich NJ, Dodek P, Heyland D, et al. Qualitative analysis of an intensive care unit family satisfaction survey. Crit Care Med 2011;39:1000–5.
6. Azoulet E, Chevret S, Leleu G, et al. Half the families of intensive care unit patients experience inadequate communication with physicians. Crit Care Med 2000;28:3044–9.
7. Curtis JR. Communicating about end-of-life care with patients and families in the intensive care unit. Crit Care Clin 2004;20:363–80.
8. Hope AA, Hsieh SJ, Howes JM, et al. Let’s talk critical. Development and evaluation of a communication skills training program for critical care fellows. Ann Am Thorac Soc 2015;12:505–11.
9. Back AL, Arnold RM, Baile WF, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Intern Med 2007;167:453–60.
10. Vital Talk. Conduct a family conference. Accessed 27 June 2016 at www.vitaltalk.org/clinicians/family.
11. Kramer M, Schmalenberg C. Securing “good” nurse/physician relationships. Nurs Manage 2003;34:34–8.
12. Johnson D, Wilson M, Cavanaugh B, et al. Measuring the ability to meet family needs in an intensive care unit. Crit Care Med 1998;26:266–71.
13. Back AL, Arnold RM. “Isn’t there anything more you can do?’’: when empathic statements work, and when they don’t. J Palliat Med 2013;16:1429–32.
14. Curtis JR, Engelberg RA, Wenrich MD. Missed opportunities during family conferences about end-of-life care in the intensive care unit. Am J Respir Crit Care Med 2005;171:844–9.
15. Pollak KI, Arnold RM, Jeffreys AS, et al. Oncologist communication about emotion during visits with patients with advanced cancer. J Clin Oncol 2007;36:5748–52.
16. Back AL, Arnold RM, Tulsky JA. Mastering communication with seriously ill patients: balancing honesty with empathy and hope. Cambridge: Cambridge University Press; 2009.
17. Back AL, Arnold RM, Baile WF, et al. Approaching difficult communication tasks in oncology. CA Cancer J Clin 2005;55:164–77.
18. Schenker Y, White D, Crowley-Matoka M, et al. “It hurts to know…and it helps”: exploring how surrogates in the ICU cope with prognostic information. J Palliat Med 2013;16:243–9.
19. Scheunemann LP, Arnold RM, White DB. The facilitated values history: helping surrogates make authentic decisions for incapacitated patients with advanced illness. Am J Respir Crit Care Med 2012;186:480–6.
20. Azoulay E, Pochard F, Kentish-Barnes N, et al. Risk of post-traumatic stress symptoms in family members of intensive care unit patients. Am J Respir Crit Care Med 2005;171:987–94.
21. White DB, Braddock CH, Bereknyei et al. Toward shared decision making at the end of life in intensive care units: opportunities for improvement. Arch Intern Med 2007;167:461–7.
From the Department of Neurology, Duke University Medical Center, Durham, NC (Dr. McFarlin), the Department of Psychosocial Oncology and Palliative Care, Dana-Farber Cancer Institute, Boston, MA (Dr. Tulsky), Harborview Medical Center, University of Washington, Seattle, WA (Dr. Back), and Department of Medicine, University of Pittsburgh, Pittsburgh, PA (Dr. Arnold).
Abstract
- Objective: To describe the use of a cognitive map for navigating family meetings with surrogate decision makers of patients in an intensive care unit.
- Methods: Descriptive report and discussion using an illustrative case to outline the steps in the cognitive map.
- Results: The use of cognitive maps has improved the ability of physicians to efficiently perform a specific communication skill. During a “goals of care” conversation, the cognitive map follows these steps: (1) Gather the clinical team for a pre-meeting, (2) Introduce everyone, (3) Use the “ask-tell-ask” strategy to communicate information, (4) Respond to emotion, (5) Highlight the patient’s voice, (6) Plan next steps, (7) Reflect on the meeting with the team. Providing this map of key communication skills will help faculty teach learners the core components of a family meeting.
- Conclusion: Practicing the behaviors demonstrated in the cognitive map may increase clinician skill during difficult conversations. Improving communication with surrogate decision makers will increase the support we offer to critically ill patients and their loved ones.
Key words: intensive care unit; communication; family meeting; critical illness; decision making; end of life care.
Family members of patients in the ICU value high-quality communication with the medical team. In fact, family members report that physicians’ communication skills are often more important than their medical skills [1]. Multiple professional societies, including the American Thoracic Society and the Society of Critical Care Medicine, define communication with families as a key component of high-quality critical care. Effective physician-patient communication improves measureable outcomes including decreased ICU length of stay [2] and may reduce distress amongst patients’ families [3]. The American College of Chest Physicians position statement on Palliative and End-of-Life Care for Patients with Cardiopulmonary Diseases urges physicians to develop curricula that incorporate interpersonal communication skills into training [4].
Unfortunately, such high-quality communication is not the norm. Surrogate decision makers are often displeased with the frequency of communication, the limited availability of attending physicians, and report feeling excluded from discussions [5]. When family meetings do occur, surrogate decision makers report inadequate understanding of diagnosis, prognosis, and treatment plans [6].
Physicians also find family meetings difficult. Intensivists worry that high-quality family meetings are time consuming and difficult to do in a busy ICU [7]. Critical care fellows report not feeling adequately trained to conduct family meetings [8]. It makes sense that untrained clinicians would want to avoid a conversation that is emotionally charged, particularly if one is unsure how to respond effectively.
The Case of Mr. A
Thomas A. is a 79-year-old man admitted to the medical intensive care unit 7 days earlier with a large left middle cerebral artery territory infarction. Given his decreased mental status, on admission he was intubated for airway protection. He is awake but aphasic and unable to follow any commands or move his right side. The neurology consultants do not feel this will improve. He has significant secretions and episodes of hypoxia. He has also developed acute on chronic kidney injury and may need to start dialysis. The social worker explains that his need for dialysis limits his placement options and that he will not be able to be discharged to home. Given his lack of improvement the team is concerned he will need a tracheostomy and feeding tube placed in order to safely continue this level of care. A family meeting is arranged to understand Mr. A’s goals of care.
Talking Map Basics
Before each step is discussed in detail, some definitions are needed. “Family” can be defined as anyone important enough, biologically related or not, to be present at a conversation with a clinician [10]. Second, a “family meeting” is a planned event between the family and interdisciplinary members of the ICU team as well as any other health care providers who have been involved in the patient’s care. The meeting takes place in a private space and at a time that is scheduled with the families’ needs in mind. Thus it is different from having families present on rounds or one-off meetings with particular clinicians.
Goals of care meetings are typically held when, in the clinicians’ view, the current treatments are not achieving the previously stated goals. Thus, the meeting has 2 purposes: first, to give the family the bad news that the current plan is not working and second, to develop a new plan based on the patient’s values. The family’s job, as surrogate decision maker, is to provide information about what would be most important to the patient. The clinician’s job is to suggest treatment plans that have the best probability of matching the patient’s values.
Not all of these tasks need be done at once. Some families will not be able to move from hearing bad news to making a decision without having time to first reflect and grieve. Others will need to confer with other family members privately before deciding on a plan. In many cases, a time-limited trial may be the right option with a plan for subsequent meetings. Given this, we recommend checking in with the family between each step to ensure that they feel safe moving ahead. For example, one might ask “Is it OK if we talk about what happens next?”
Talking Map Steps in Detail
1. Gather the Clinical Team for a Pre-Meeting
ICU care involves a large interdisciplinary care team. A “meeting before the meeting” with the entire clinical team is an opportunity to reach consensus on prognosis and therapeutic options, share prior interactions with family, and determine goals for the family meeting. It is also helpful to clarify team members’ roles at the meeting and to choose a primary facilitator. All of this helps to ensure that the family receives a consistent message during the meeting. The pre-meeting is also an opportunity to ask a team member to observe the communication skills of the facilitator and be prepared to give feedback after the meeting.
At this time, the team should also create the proper environment for the family meeting. This includes a quiet room free of interruptions with ample seating, available tissues, and transferred pagers and cell phones.
The intensivist and bedside nurse should always be present at the family meeting, and it is best when the same attending can be at subsequent family meetings Their consistent dual presence provides the uniform communication from the team, can reduce anxiety in family members and the collaboration reduces ICU nurse and physician burnout [11]. For illnesses that involve a specific disease or organ system, it is important to have the specialist at the meeting who can provide the appropriate expertise.
The Pre-Meeting
A family meeting was scheduled in the family meeting room for 3 pm, after morning rounds. Thirty minutes prior to the meeting the medical team, including the MICU intensivist, the bedside nurse, the neurology attending who has been involved in the care, the case manager and 2 residents sat to discuss Mr. A’s care. The neurology team confirmed that this stroke was considered very large and would result in a level of disability that could only be cared for in a nursing home and would require both a tracheostomy and feeding tube for safe care. The bedside nurse relayed that the family had asked if Mr. A. would ever recover enough to get back to his home. The neurology team shared they did not expect much improvement at all. Given the worsening renal failure and need for dialysis the case manager reminded the team that Mr. A’s nursing home placements were limited. The team decided that the intensivist would lead the meeting as she had updated various family members on rounds for the past 4 days and would be on service for another week. The team decided that their goal for the meeting was to make sure the family understands that Mr. A’s several medical illnesses portend a poor prognosis. They recognized this may be breaking bad news to the family. They also wanted to better understand what Mr. A would have thought given this situation. The residents were asked to watch for the family’s responses when the team delivered the news.
2. Introduce Everyone
Each meeting should start with formal introductions. Even if most providers know most family members it is a polite way to start the meeting. Introducing each family member present and how they know the patient provides insight into how the family is constructed and makes decisions. For example, the entire family may defer to the daughter who introduces herself as a nurse. In other situations, although there is one legal decision maker, the family may explain that they make decisions by consensus.
Each member of the treating team should also introduce themselves. Even if the clinician has been working with the family, it is polite to be formal and give your name and role. Given the number of people the family sees every day, one should not assume that the family remembers all of the clinicians.
In teaching hospitals, providers should also help the family understand their level of training. Surrogates do not always understand the different roles or level of training between students, residents and fellows, advanced practice providers, consultants and their attending physicians. Uncertainty about the roles can lead to family members feeling as though they are receiving contradictory information. Family satisfaction decreases when multiple attending physicians are involved in a patient’s care [12]. When possible, a consistent presence among providers at family meetings is always best.
3. Ask the Family's Understanding of the Situation (Ask-Tell-Ask)
Asking the family to explain the situation in their own language reveals how well they understand the medical facts and helps the medical team determine what information will be most helpful to the family. An opening statement might be “We have all seen your dad and talked to many of his providers. It would help us all be on the same page if you can you tell me what the doctors are telling you?” Starting with the family’s understanding builds trust with the medical team as it creates an opportunity for the family to lead the meeting and indicates that the team is available to listen to their concerns. Asking surrogates for their understanding allows them to tell their story and not hear a reiteration of things they already know. Providing time for the family to share their perspective of the care elicits family’s concerns.
In a large meeting, ensure that all members of the family have an opportunity to communicate their concerns. Does a particular person do all of the talking? Are there individuals that do not speak at all? One way to further understand unspoken concerns during the meeting is to ask “I notice you have been quiet, what questions do you have that I can answer?” There may be several rounds of “asking” in order to ensure all the family members’ concerns are heard. Letting the family tell what they have heard helps the clinicians get a better idea of their health literacy. Do they explain information using technical data or jargon? Finally, as the family talks the clinicians can determine how surprising the “serious news” will be to them. For example, if the family says they know their dad is doing much worse and may die, the information to be delivered can be truncated. However if family incorrectly thinks their dad is doing better or is uncertain they will be much more surprised by the serious news.
After providing time for the family to express their understanding, tell them the information the team needs to communicate. When delivering serious news it is important to focus on the key 1 to 2 points you want the family to take away from the meeting. Typically when health care professionals talk to each other, they talk about every medical detail. Families find this amount of information overwhelming and are not sure what is most important, asking “So what does that mean?” Focusing on the “headline” helps the family focus on what you think the most important piece of information is. Studies suggest that what families most want to know is what the information means for the patient’s future and what treatments are possible. After delivering the new information, stop to allow the family space to think about what you said. If you are giving serious news, you will know they have heard what you said as they will get emotional (see next step).
Checking for understanding is the final “ask” in Ask-Tell-Ask. Begin by asking “What questions do you have?” Data in primary care has shown that patients are more likely to ask questions if you ask “what questions do you have” rather than “do you have any questions?” It is important to continue to ask this question until the family has asked all their questions. Often the family’s tough questions do not come until they get more comfortable and confident in the health care team. In cases where one family member is dominant it might also help to say “What questions do others have?” Next, using techniques like the “teach back” model the physician should check in to see what the family is taking away from the conversation. If a family understands, they can “teach back” the information accurately. This “ask” can be done in a way that does not make the family feel they are being tested: “I am not always clear when I communicate. Do you mind telling me back in your own words what you thought I said so I know we are on the same page?” This also provides an opportunity to answer any new questions that arise. Hearing the information directly from the family can allow the team to clarify any misconceptions and give insight into any emotional responses that the family might have.
4. Respond to Emotion
Discussing serious news in the ICU setting naturally leads to an emotional reaction. The clinician’s ability to notice emotional cues and respond with empathy is a key communication skill in family meetings [13]. Emotional reactions impede individual’s ability to process cognitive information and make it hard to think cognitively about what should be done next.
Physicians miss opportunities to respond to emotion in family meetings [14]. Missed opportunities lead to decreased family satisfaction and may lead to treatment decisions not consistent with the wishes of their loved ones. Empathic responses improve the family-clinician relationship and helps build trust and rapport [15]. Well- placed empathic statements may help surrogates disclose concerns that help the physician better understand the goals and values of the family and patient. Families also can more fully process cognitive information when their emotional responses have been attended to.
Physicians can develop the capacity to recognize and respond to the emotional cues family members are delivering. Intensivists should actively look for the emotions, the empathic opportunity, that are displayed by the family. This emotion is the “data” that will help lead to an empathic response. A family that just received bad news typically responds by showing emotion. Clues that emotions are present include: the family asking the same questions multiple times; using emotional words such as “sad” or “frustrated;” existential questions that do not have a cognitive answer such as “Why did God let this happen?;” or non-verbal cues like tears and hand wringing.
Sometimes the emotional responses are more difficult to recognize. Families may continue to ask for more cognitive information after hearing bad news. Someone keeps asking “Why did his kidney function worsen?” or “I thought the team said the chest x-ray looked better.” It is tempting to start answering these questions with more medical facts. However, if the question comes after bad news, it is usually an expression of frustration or sadness rather than a request for more information. Rather than giving information, it might help to acknowledge this by saying “I imagine this new is overwhelming.”
5. Highlight the Patient’s Voice
Family meetings are often used to develop new treatment plans (given that the old plans are not working). In these situations, it is essential to understand what the incapacitated patient would say if they were part of the family meeting. The surrogate’s primary role is to represent the patient’s voice. To do this, surrogates need assistance in applying their critically ill loved one’s thoughts and values to complex, possibly life limiting, situations. Surrogate decision makers struggle with the decisions’ emotional impact, as well as how to reconcile their desires with their loved one’s wishes [18]. This can lead them to make decisions that conflict with the loved one’s values [19] as well as emotional sequelae such as PTSD and depression [20].
As families reflect on their loved one’s values, conflicting desires will arise. For example, someone may have wanted to live as long as possible and also values independence. Or someone may value their ability to think clearly more than being physically well but would not want to be physically dependent on artificial life support. Exploring which values would be more important can help resolve these conflicts.
Clinicians should check for understanding while family members are identifying the values of their loved ones. Providing the family with a summary of what you have heard will help ensure a more accurate understanding of these crucial issues. A summary statement might be, “It sounds like you are saying your dad really valued his independence. He enjoyed being able to take care of his loved ones and himself. Is that right?”
6. Plan Next Steps
The family meeting serves to attend to family emotion and allow space to elicit patients’ values. Following a family meeting surrogate decision makers may be able to begin to consider the next steps in their loved one’s care. If bad news was delivered they may need space to adjust to a different future than they expected. Using an empathic statement of support “We will continue to make sure we communicate with you as we work together to plan next steps” will reassure a family that they have time and space to plan for the future.
Families vary regarding how much physician input they desire in planning next steps [21]. You can explicitly ask how the team can best help the family with decisions: “Some families like to hear the options for next steps from the team and make a decision, other families like to hear a recommendation from the team. What would be the most helpful for you?” Throughout the course of an illness a surrogate’s preference for decision making may change and clinicians should be responsive to those changing needs.
If the surrogate wants a clinician’s recommendation, 3 points are worth stressing. First, the recommendation should be personalized to this patient and his values. The goal is to reveal how the understanding of the patient’s values led to the treatment plan offered. Second, the recommendation should focus primarily on what will be done to achieve the patient’s values. Focusing on what the clinicians will do may help the family feel that the clinicians are still “trying” and not abandoning their loved one. In this case, the team will continue medical care that will help the patient regain/maintain independence. Only after talking about what will be done should the clinician point out that certain interventions will not achieve the patient’s goals and thus will not be done:
“It sounds like your father really valued his independence and that this illness has really taken that away. Knowing this, would it be helpful for me to make a recommendation for next steps?” “I think we should continue providing excellent medical care for your father in hopes he can get better and go home. One the other hand, if he gets worse, we should not use therapies such as CPR or dialysis that are unlikely to help him regain his independence.”
Finally, be concrete when planning next steps. If a time-limited trial of a therapy is proposed, make sure the family understands what a successful and unsuccessful trial will look like. Make plans to meet again on a specific date in order to ensure the family understands the progress being made. If a transition to comfort care is agreed upon, ensure support of the entire family during the next hours to days and offer services such as chaplaincy or child life specialists.
A family may not agree with the recommendation and back and forth discussion can help create a plan that is in line with their understanding of the illness. Rather than convincing, a clinician should keep an open mind about why they and the surrogate disagree. Do they have different views about the patient’s future? Did the medical team misunderstand the patient’s values? Are there emotional factors that inhibit the surrogate’s ability to attend to the discussion? It is only by learning where the disagreement is that a clinician can move the conversation forward.
A surrogate may ask about a therapy that is not beneficial or may increase distress to the patient. The use of “I wish” or “I worry” statements can be helpful at these points. These specific phrases recognize the surrogate’s desire to do more but also imply that the therapies are not helpful.
“I wish that his ability to communicate and tell you what he wants would get better with a little more time as well.”
“I worry that waiting 2 more weeks for improvement will actually cause complications to occur.”
7. Reflect
Family meetings have an impact on both the family and the medical team. Following the meeting, a short debriefing with the clinical team can be helpful. Summarizing the events of the meeting ensures clarity about the treatment plan going forward. It provides team members a chance to discuss conflicts that may have arisen. It allows the participants in the meeting to reflect on what communication skills they used and how they can improve their skills going forward.
Conclusion
Family meetings with surrogate decision makers must navigate multiple agendas of the family and providers. The goal of excellent communication with surrogates in an ICU should be to understand the patient’s goals and values and seek to make treatment plans that align with their perspective. This talking map provides a conceptual framework for physicians to guide a family through these conversations. The framework creates an opportunity to focus on the patient’s values and preferences for care while allowing space to attend to emotional responses to reduce the distress inherent in surrogate decision-making. Practicing the behaviors demonstrated in the talking map may increase clinician skill during difficult conversations. Improving communication with surrogate decision makers will increase the support we offer to critically ill patients and their loved ones.
Corresponding author: Jessica McFarlin, MD, jessmcfarlin@gmail.com.
Funding/support: Dr. Arnold receives support though the Leo H. Criep Chair in Patient Care.
Financial disclosures: None.
From the Department of Neurology, Duke University Medical Center, Durham, NC (Dr. McFarlin), the Department of Psychosocial Oncology and Palliative Care, Dana-Farber Cancer Institute, Boston, MA (Dr. Tulsky), Harborview Medical Center, University of Washington, Seattle, WA (Dr. Back), and Department of Medicine, University of Pittsburgh, Pittsburgh, PA (Dr. Arnold).
Abstract
- Objective: To describe the use of a cognitive map for navigating family meetings with surrogate decision makers of patients in an intensive care unit.
- Methods: Descriptive report and discussion using an illustrative case to outline the steps in the cognitive map.
- Results: The use of cognitive maps has improved the ability of physicians to efficiently perform a specific communication skill. During a “goals of care” conversation, the cognitive map follows these steps: (1) Gather the clinical team for a pre-meeting, (2) Introduce everyone, (3) Use the “ask-tell-ask” strategy to communicate information, (4) Respond to emotion, (5) Highlight the patient’s voice, (6) Plan next steps, (7) Reflect on the meeting with the team. Providing this map of key communication skills will help faculty teach learners the core components of a family meeting.
- Conclusion: Practicing the behaviors demonstrated in the cognitive map may increase clinician skill during difficult conversations. Improving communication with surrogate decision makers will increase the support we offer to critically ill patients and their loved ones.
Key words: intensive care unit; communication; family meeting; critical illness; decision making; end of life care.
Family members of patients in the ICU value high-quality communication with the medical team. In fact, family members report that physicians’ communication skills are often more important than their medical skills [1]. Multiple professional societies, including the American Thoracic Society and the Society of Critical Care Medicine, define communication with families as a key component of high-quality critical care. Effective physician-patient communication improves measureable outcomes including decreased ICU length of stay [2] and may reduce distress amongst patients’ families [3]. The American College of Chest Physicians position statement on Palliative and End-of-Life Care for Patients with Cardiopulmonary Diseases urges physicians to develop curricula that incorporate interpersonal communication skills into training [4].
Unfortunately, such high-quality communication is not the norm. Surrogate decision makers are often displeased with the frequency of communication, the limited availability of attending physicians, and report feeling excluded from discussions [5]. When family meetings do occur, surrogate decision makers report inadequate understanding of diagnosis, prognosis, and treatment plans [6].
Physicians also find family meetings difficult. Intensivists worry that high-quality family meetings are time consuming and difficult to do in a busy ICU [7]. Critical care fellows report not feeling adequately trained to conduct family meetings [8]. It makes sense that untrained clinicians would want to avoid a conversation that is emotionally charged, particularly if one is unsure how to respond effectively.
The Case of Mr. A
Thomas A. is a 79-year-old man admitted to the medical intensive care unit 7 days earlier with a large left middle cerebral artery territory infarction. Given his decreased mental status, on admission he was intubated for airway protection. He is awake but aphasic and unable to follow any commands or move his right side. The neurology consultants do not feel this will improve. He has significant secretions and episodes of hypoxia. He has also developed acute on chronic kidney injury and may need to start dialysis. The social worker explains that his need for dialysis limits his placement options and that he will not be able to be discharged to home. Given his lack of improvement the team is concerned he will need a tracheostomy and feeding tube placed in order to safely continue this level of care. A family meeting is arranged to understand Mr. A’s goals of care.
Talking Map Basics
Before each step is discussed in detail, some definitions are needed. “Family” can be defined as anyone important enough, biologically related or not, to be present at a conversation with a clinician [10]. Second, a “family meeting” is a planned event between the family and interdisciplinary members of the ICU team as well as any other health care providers who have been involved in the patient’s care. The meeting takes place in a private space and at a time that is scheduled with the families’ needs in mind. Thus it is different from having families present on rounds or one-off meetings with particular clinicians.
Goals of care meetings are typically held when, in the clinicians’ view, the current treatments are not achieving the previously stated goals. Thus, the meeting has 2 purposes: first, to give the family the bad news that the current plan is not working and second, to develop a new plan based on the patient’s values. The family’s job, as surrogate decision maker, is to provide information about what would be most important to the patient. The clinician’s job is to suggest treatment plans that have the best probability of matching the patient’s values.
Not all of these tasks need be done at once. Some families will not be able to move from hearing bad news to making a decision without having time to first reflect and grieve. Others will need to confer with other family members privately before deciding on a plan. In many cases, a time-limited trial may be the right option with a plan for subsequent meetings. Given this, we recommend checking in with the family between each step to ensure that they feel safe moving ahead. For example, one might ask “Is it OK if we talk about what happens next?”
Talking Map Steps in Detail
1. Gather the Clinical Team for a Pre-Meeting
ICU care involves a large interdisciplinary care team. A “meeting before the meeting” with the entire clinical team is an opportunity to reach consensus on prognosis and therapeutic options, share prior interactions with family, and determine goals for the family meeting. It is also helpful to clarify team members’ roles at the meeting and to choose a primary facilitator. All of this helps to ensure that the family receives a consistent message during the meeting. The pre-meeting is also an opportunity to ask a team member to observe the communication skills of the facilitator and be prepared to give feedback after the meeting.
At this time, the team should also create the proper environment for the family meeting. This includes a quiet room free of interruptions with ample seating, available tissues, and transferred pagers and cell phones.
The intensivist and bedside nurse should always be present at the family meeting, and it is best when the same attending can be at subsequent family meetings Their consistent dual presence provides the uniform communication from the team, can reduce anxiety in family members and the collaboration reduces ICU nurse and physician burnout [11]. For illnesses that involve a specific disease or organ system, it is important to have the specialist at the meeting who can provide the appropriate expertise.
The Pre-Meeting
A family meeting was scheduled in the family meeting room for 3 pm, after morning rounds. Thirty minutes prior to the meeting the medical team, including the MICU intensivist, the bedside nurse, the neurology attending who has been involved in the care, the case manager and 2 residents sat to discuss Mr. A’s care. The neurology team confirmed that this stroke was considered very large and would result in a level of disability that could only be cared for in a nursing home and would require both a tracheostomy and feeding tube for safe care. The bedside nurse relayed that the family had asked if Mr. A. would ever recover enough to get back to his home. The neurology team shared they did not expect much improvement at all. Given the worsening renal failure and need for dialysis the case manager reminded the team that Mr. A’s nursing home placements were limited. The team decided that the intensivist would lead the meeting as she had updated various family members on rounds for the past 4 days and would be on service for another week. The team decided that their goal for the meeting was to make sure the family understands that Mr. A’s several medical illnesses portend a poor prognosis. They recognized this may be breaking bad news to the family. They also wanted to better understand what Mr. A would have thought given this situation. The residents were asked to watch for the family’s responses when the team delivered the news.
2. Introduce Everyone
Each meeting should start with formal introductions. Even if most providers know most family members it is a polite way to start the meeting. Introducing each family member present and how they know the patient provides insight into how the family is constructed and makes decisions. For example, the entire family may defer to the daughter who introduces herself as a nurse. In other situations, although there is one legal decision maker, the family may explain that they make decisions by consensus.
Each member of the treating team should also introduce themselves. Even if the clinician has been working with the family, it is polite to be formal and give your name and role. Given the number of people the family sees every day, one should not assume that the family remembers all of the clinicians.
In teaching hospitals, providers should also help the family understand their level of training. Surrogates do not always understand the different roles or level of training between students, residents and fellows, advanced practice providers, consultants and their attending physicians. Uncertainty about the roles can lead to family members feeling as though they are receiving contradictory information. Family satisfaction decreases when multiple attending physicians are involved in a patient’s care [12]. When possible, a consistent presence among providers at family meetings is always best.
3. Ask the Family's Understanding of the Situation (Ask-Tell-Ask)
Asking the family to explain the situation in their own language reveals how well they understand the medical facts and helps the medical team determine what information will be most helpful to the family. An opening statement might be “We have all seen your dad and talked to many of his providers. It would help us all be on the same page if you can you tell me what the doctors are telling you?” Starting with the family’s understanding builds trust with the medical team as it creates an opportunity for the family to lead the meeting and indicates that the team is available to listen to their concerns. Asking surrogates for their understanding allows them to tell their story and not hear a reiteration of things they already know. Providing time for the family to share their perspective of the care elicits family’s concerns.
In a large meeting, ensure that all members of the family have an opportunity to communicate their concerns. Does a particular person do all of the talking? Are there individuals that do not speak at all? One way to further understand unspoken concerns during the meeting is to ask “I notice you have been quiet, what questions do you have that I can answer?” There may be several rounds of “asking” in order to ensure all the family members’ concerns are heard. Letting the family tell what they have heard helps the clinicians get a better idea of their health literacy. Do they explain information using technical data or jargon? Finally, as the family talks the clinicians can determine how surprising the “serious news” will be to them. For example, if the family says they know their dad is doing much worse and may die, the information to be delivered can be truncated. However if family incorrectly thinks their dad is doing better or is uncertain they will be much more surprised by the serious news.
After providing time for the family to express their understanding, tell them the information the team needs to communicate. When delivering serious news it is important to focus on the key 1 to 2 points you want the family to take away from the meeting. Typically when health care professionals talk to each other, they talk about every medical detail. Families find this amount of information overwhelming and are not sure what is most important, asking “So what does that mean?” Focusing on the “headline” helps the family focus on what you think the most important piece of information is. Studies suggest that what families most want to know is what the information means for the patient’s future and what treatments are possible. After delivering the new information, stop to allow the family space to think about what you said. If you are giving serious news, you will know they have heard what you said as they will get emotional (see next step).
Checking for understanding is the final “ask” in Ask-Tell-Ask. Begin by asking “What questions do you have?” Data in primary care has shown that patients are more likely to ask questions if you ask “what questions do you have” rather than “do you have any questions?” It is important to continue to ask this question until the family has asked all their questions. Often the family’s tough questions do not come until they get more comfortable and confident in the health care team. In cases where one family member is dominant it might also help to say “What questions do others have?” Next, using techniques like the “teach back” model the physician should check in to see what the family is taking away from the conversation. If a family understands, they can “teach back” the information accurately. This “ask” can be done in a way that does not make the family feel they are being tested: “I am not always clear when I communicate. Do you mind telling me back in your own words what you thought I said so I know we are on the same page?” This also provides an opportunity to answer any new questions that arise. Hearing the information directly from the family can allow the team to clarify any misconceptions and give insight into any emotional responses that the family might have.
4. Respond to Emotion
Discussing serious news in the ICU setting naturally leads to an emotional reaction. The clinician’s ability to notice emotional cues and respond with empathy is a key communication skill in family meetings [13]. Emotional reactions impede individual’s ability to process cognitive information and make it hard to think cognitively about what should be done next.
Physicians miss opportunities to respond to emotion in family meetings [14]. Missed opportunities lead to decreased family satisfaction and may lead to treatment decisions not consistent with the wishes of their loved ones. Empathic responses improve the family-clinician relationship and helps build trust and rapport [15]. Well- placed empathic statements may help surrogates disclose concerns that help the physician better understand the goals and values of the family and patient. Families also can more fully process cognitive information when their emotional responses have been attended to.
Physicians can develop the capacity to recognize and respond to the emotional cues family members are delivering. Intensivists should actively look for the emotions, the empathic opportunity, that are displayed by the family. This emotion is the “data” that will help lead to an empathic response. A family that just received bad news typically responds by showing emotion. Clues that emotions are present include: the family asking the same questions multiple times; using emotional words such as “sad” or “frustrated;” existential questions that do not have a cognitive answer such as “Why did God let this happen?;” or non-verbal cues like tears and hand wringing.
Sometimes the emotional responses are more difficult to recognize. Families may continue to ask for more cognitive information after hearing bad news. Someone keeps asking “Why did his kidney function worsen?” or “I thought the team said the chest x-ray looked better.” It is tempting to start answering these questions with more medical facts. However, if the question comes after bad news, it is usually an expression of frustration or sadness rather than a request for more information. Rather than giving information, it might help to acknowledge this by saying “I imagine this new is overwhelming.”
5. Highlight the Patient’s Voice
Family meetings are often used to develop new treatment plans (given that the old plans are not working). In these situations, it is essential to understand what the incapacitated patient would say if they were part of the family meeting. The surrogate’s primary role is to represent the patient’s voice. To do this, surrogates need assistance in applying their critically ill loved one’s thoughts and values to complex, possibly life limiting, situations. Surrogate decision makers struggle with the decisions’ emotional impact, as well as how to reconcile their desires with their loved one’s wishes [18]. This can lead them to make decisions that conflict with the loved one’s values [19] as well as emotional sequelae such as PTSD and depression [20].
As families reflect on their loved one’s values, conflicting desires will arise. For example, someone may have wanted to live as long as possible and also values independence. Or someone may value their ability to think clearly more than being physically well but would not want to be physically dependent on artificial life support. Exploring which values would be more important can help resolve these conflicts.
Clinicians should check for understanding while family members are identifying the values of their loved ones. Providing the family with a summary of what you have heard will help ensure a more accurate understanding of these crucial issues. A summary statement might be, “It sounds like you are saying your dad really valued his independence. He enjoyed being able to take care of his loved ones and himself. Is that right?”
6. Plan Next Steps
The family meeting serves to attend to family emotion and allow space to elicit patients’ values. Following a family meeting surrogate decision makers may be able to begin to consider the next steps in their loved one’s care. If bad news was delivered they may need space to adjust to a different future than they expected. Using an empathic statement of support “We will continue to make sure we communicate with you as we work together to plan next steps” will reassure a family that they have time and space to plan for the future.
Families vary regarding how much physician input they desire in planning next steps [21]. You can explicitly ask how the team can best help the family with decisions: “Some families like to hear the options for next steps from the team and make a decision, other families like to hear a recommendation from the team. What would be the most helpful for you?” Throughout the course of an illness a surrogate’s preference for decision making may change and clinicians should be responsive to those changing needs.
If the surrogate wants a clinician’s recommendation, 3 points are worth stressing. First, the recommendation should be personalized to this patient and his values. The goal is to reveal how the understanding of the patient’s values led to the treatment plan offered. Second, the recommendation should focus primarily on what will be done to achieve the patient’s values. Focusing on what the clinicians will do may help the family feel that the clinicians are still “trying” and not abandoning their loved one. In this case, the team will continue medical care that will help the patient regain/maintain independence. Only after talking about what will be done should the clinician point out that certain interventions will not achieve the patient’s goals and thus will not be done:
“It sounds like your father really valued his independence and that this illness has really taken that away. Knowing this, would it be helpful for me to make a recommendation for next steps?” “I think we should continue providing excellent medical care for your father in hopes he can get better and go home. One the other hand, if he gets worse, we should not use therapies such as CPR or dialysis that are unlikely to help him regain his independence.”
Finally, be concrete when planning next steps. If a time-limited trial of a therapy is proposed, make sure the family understands what a successful and unsuccessful trial will look like. Make plans to meet again on a specific date in order to ensure the family understands the progress being made. If a transition to comfort care is agreed upon, ensure support of the entire family during the next hours to days and offer services such as chaplaincy or child life specialists.
A family may not agree with the recommendation and back and forth discussion can help create a plan that is in line with their understanding of the illness. Rather than convincing, a clinician should keep an open mind about why they and the surrogate disagree. Do they have different views about the patient’s future? Did the medical team misunderstand the patient’s values? Are there emotional factors that inhibit the surrogate’s ability to attend to the discussion? It is only by learning where the disagreement is that a clinician can move the conversation forward.
A surrogate may ask about a therapy that is not beneficial or may increase distress to the patient. The use of “I wish” or “I worry” statements can be helpful at these points. These specific phrases recognize the surrogate’s desire to do more but also imply that the therapies are not helpful.
“I wish that his ability to communicate and tell you what he wants would get better with a little more time as well.”
“I worry that waiting 2 more weeks for improvement will actually cause complications to occur.”
7. Reflect
Family meetings have an impact on both the family and the medical team. Following the meeting, a short debriefing with the clinical team can be helpful. Summarizing the events of the meeting ensures clarity about the treatment plan going forward. It provides team members a chance to discuss conflicts that may have arisen. It allows the participants in the meeting to reflect on what communication skills they used and how they can improve their skills going forward.
Conclusion
Family meetings with surrogate decision makers must navigate multiple agendas of the family and providers. The goal of excellent communication with surrogates in an ICU should be to understand the patient’s goals and values and seek to make treatment plans that align with their perspective. This talking map provides a conceptual framework for physicians to guide a family through these conversations. The framework creates an opportunity to focus on the patient’s values and preferences for care while allowing space to attend to emotional responses to reduce the distress inherent in surrogate decision-making. Practicing the behaviors demonstrated in the talking map may increase clinician skill during difficult conversations. Improving communication with surrogate decision makers will increase the support we offer to critically ill patients and their loved ones.
Corresponding author: Jessica McFarlin, MD, jessmcfarlin@gmail.com.
Funding/support: Dr. Arnold receives support though the Leo H. Criep Chair in Patient Care.
Financial disclosures: None.
1. Hickey M. What are the needs of families of critically ill patients? A review of the literature since 1976. Heart Lung 1990;19:401–15.
2. Mosenthal AC, Murphy PA, Barker LK, et al. Changing culture around end-of-life care in the trauma intensive care unit. J Trauma 2008;64:1587–93.
3. Lautrette A, Darmon M, Megarbane B, et al. A communication strategy and brochure for relatives of patients dying in the ICU. N Engl J Med 2007;356:469–78.
4. Selecky PA, Eliasson AH, Hall RI, et al. Palliative and end-of-life care for patients with cardiopulmonary diseases. Chest 2005;128:3599–610.
5. Henrich NJ, Dodek P, Heyland D, et al. Qualitative analysis of an intensive care unit family satisfaction survey. Crit Care Med 2011;39:1000–5.
6. Azoulet E, Chevret S, Leleu G, et al. Half the families of intensive care unit patients experience inadequate communication with physicians. Crit Care Med 2000;28:3044–9.
7. Curtis JR. Communicating about end-of-life care with patients and families in the intensive care unit. Crit Care Clin 2004;20:363–80.
8. Hope AA, Hsieh SJ, Howes JM, et al. Let’s talk critical. Development and evaluation of a communication skills training program for critical care fellows. Ann Am Thorac Soc 2015;12:505–11.
9. Back AL, Arnold RM, Baile WF, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Intern Med 2007;167:453–60.
10. Vital Talk. Conduct a family conference. Accessed 27 June 2016 at www.vitaltalk.org/clinicians/family.
11. Kramer M, Schmalenberg C. Securing “good” nurse/physician relationships. Nurs Manage 2003;34:34–8.
12. Johnson D, Wilson M, Cavanaugh B, et al. Measuring the ability to meet family needs in an intensive care unit. Crit Care Med 1998;26:266–71.
13. Back AL, Arnold RM. “Isn’t there anything more you can do?’’: when empathic statements work, and when they don’t. J Palliat Med 2013;16:1429–32.
14. Curtis JR, Engelberg RA, Wenrich MD. Missed opportunities during family conferences about end-of-life care in the intensive care unit. Am J Respir Crit Care Med 2005;171:844–9.
15. Pollak KI, Arnold RM, Jeffreys AS, et al. Oncologist communication about emotion during visits with patients with advanced cancer. J Clin Oncol 2007;36:5748–52.
16. Back AL, Arnold RM, Tulsky JA. Mastering communication with seriously ill patients: balancing honesty with empathy and hope. Cambridge: Cambridge University Press; 2009.
17. Back AL, Arnold RM, Baile WF, et al. Approaching difficult communication tasks in oncology. CA Cancer J Clin 2005;55:164–77.
18. Schenker Y, White D, Crowley-Matoka M, et al. “It hurts to know…and it helps”: exploring how surrogates in the ICU cope with prognostic information. J Palliat Med 2013;16:243–9.
19. Scheunemann LP, Arnold RM, White DB. The facilitated values history: helping surrogates make authentic decisions for incapacitated patients with advanced illness. Am J Respir Crit Care Med 2012;186:480–6.
20. Azoulay E, Pochard F, Kentish-Barnes N, et al. Risk of post-traumatic stress symptoms in family members of intensive care unit patients. Am J Respir Crit Care Med 2005;171:987–94.
21. White DB, Braddock CH, Bereknyei et al. Toward shared decision making at the end of life in intensive care units: opportunities for improvement. Arch Intern Med 2007;167:461–7.
1. Hickey M. What are the needs of families of critically ill patients? A review of the literature since 1976. Heart Lung 1990;19:401–15.
2. Mosenthal AC, Murphy PA, Barker LK, et al. Changing culture around end-of-life care in the trauma intensive care unit. J Trauma 2008;64:1587–93.
3. Lautrette A, Darmon M, Megarbane B, et al. A communication strategy and brochure for relatives of patients dying in the ICU. N Engl J Med 2007;356:469–78.
4. Selecky PA, Eliasson AH, Hall RI, et al. Palliative and end-of-life care for patients with cardiopulmonary diseases. Chest 2005;128:3599–610.
5. Henrich NJ, Dodek P, Heyland D, et al. Qualitative analysis of an intensive care unit family satisfaction survey. Crit Care Med 2011;39:1000–5.
6. Azoulet E, Chevret S, Leleu G, et al. Half the families of intensive care unit patients experience inadequate communication with physicians. Crit Care Med 2000;28:3044–9.
7. Curtis JR. Communicating about end-of-life care with patients and families in the intensive care unit. Crit Care Clin 2004;20:363–80.
8. Hope AA, Hsieh SJ, Howes JM, et al. Let’s talk critical. Development and evaluation of a communication skills training program for critical care fellows. Ann Am Thorac Soc 2015;12:505–11.
9. Back AL, Arnold RM, Baile WF, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Intern Med 2007;167:453–60.
10. Vital Talk. Conduct a family conference. Accessed 27 June 2016 at www.vitaltalk.org/clinicians/family.
11. Kramer M, Schmalenberg C. Securing “good” nurse/physician relationships. Nurs Manage 2003;34:34–8.
12. Johnson D, Wilson M, Cavanaugh B, et al. Measuring the ability to meet family needs in an intensive care unit. Crit Care Med 1998;26:266–71.
13. Back AL, Arnold RM. “Isn’t there anything more you can do?’’: when empathic statements work, and when they don’t. J Palliat Med 2013;16:1429–32.
14. Curtis JR, Engelberg RA, Wenrich MD. Missed opportunities during family conferences about end-of-life care in the intensive care unit. Am J Respir Crit Care Med 2005;171:844–9.
15. Pollak KI, Arnold RM, Jeffreys AS, et al. Oncologist communication about emotion during visits with patients with advanced cancer. J Clin Oncol 2007;36:5748–52.
16. Back AL, Arnold RM, Tulsky JA. Mastering communication with seriously ill patients: balancing honesty with empathy and hope. Cambridge: Cambridge University Press; 2009.
17. Back AL, Arnold RM, Baile WF, et al. Approaching difficult communication tasks in oncology. CA Cancer J Clin 2005;55:164–77.
18. Schenker Y, White D, Crowley-Matoka M, et al. “It hurts to know…and it helps”: exploring how surrogates in the ICU cope with prognostic information. J Palliat Med 2013;16:243–9.
19. Scheunemann LP, Arnold RM, White DB. The facilitated values history: helping surrogates make authentic decisions for incapacitated patients with advanced illness. Am J Respir Crit Care Med 2012;186:480–6.
20. Azoulay E, Pochard F, Kentish-Barnes N, et al. Risk of post-traumatic stress symptoms in family members of intensive care unit patients. Am J Respir Crit Care Med 2005;171:987–94.
21. White DB, Braddock CH, Bereknyei et al. Toward shared decision making at the end of life in intensive care units: opportunities for improvement. Arch Intern Med 2007;167:461–7.
Patient-Physician Communication and Diabetes Self-Care
Abstract
- Objective: To summarize the current literature, research findings, and interventions for self-care communication in the physician-patient relationship.
- Methods: Literature review.
- Results: Diabetes management requires patients to follow complex self-care recommendations for nutrition, physical activity, blood glucose monitoring, and medication. Adherence to these recommendations improves glycemic control and mitigates the risk of diabetes complications; however, many patients struggle to follow these behaviors in everyday life. In the physician-patient relationship, self-care communication is largely influenced by interpersonal trust. Physicians need to incorporate interpersonal and relational skills to establish a trusting relationship. Physician-level barriers to self-care communication include lack of time, lack of collaboration and teamwork among health care providers, lack of patients’ access to resources, and lack of psychosocial support for diabetes patients. Among patients, psychosocial barriers and health literacy may affect willingness to discuss self-care. Motivational interviewing techniques may be helpful for improving communication around patient self-management and promotion of healthy behaviors.
- Conclusion: Physicians can assist patients with their diabetes self-care by discussing self-care challenges during medical visits.
Diabetes is one of the most significant and growing chronic health problems in the world, affecting approximately 415 million people [1]. Diabetes is marked by the body’s inability to make insulin as well as the body’s inability to effectively use the insulin it produces [2]. Diagnosis of diabetes has increased sharply in recent decades and is expected to increase even more, with the largest increases in middle- and low-income countries [3]. Diabetes is a leading cause of blindness, kidney failure, myocardial infarction, stroke, and amputation [3], and in 2015 it accounted for 5 million deaths worldwide [1]. Further, diabetes’s costs to society represent 12% ($673 billion) of global health expenditures [1]. By 2040, models predict that 642 million people will be diagnosed with diabetes and costs will continue to grow as the population ages [1]. Thus, prevention of diabetes is the ultimate goal; however, more effective management for individuals already diagnosed with diabetes is critical to reduce the risk of complications and the economic burden of the disease.
Diabetes management requires patients to perform complex self-care regimens, including weight reduction, frequent blood glucose monitoring, taking oral and/or insulin medications, engaging in physical activity, adhering to diabetes nutrition guidelines, and attending clinic appointments [4–9]. These self-care behaviors are critically linked to improved glycemic control, however, integrating them into one’s daily life can be challenging [10–12]. Recent National Health and Nutrition Examination Survey (NHANES) data show that approximately half of adults with diabetes are not meeting recommended goals for diabetes care [13]. Physicians can assist patients with their diabetes self-care by scheduling frequent follow-up visits and discussing self-care challenges with their patients [14].
In this review, we discuss the current literature on physician-patient communication and diabetes self-care. First, we discuss the qualities of an effective physician-patient relationship followed by the importance of self-care communication in diabetes care. Next, we discuss barriers and facilitators to self-care communication. Finally, we review interventions for improving physician-patient communication in diabetes self-care.
Qualities of an Effective Physician-Patient Relationship
Successful diabetes care requires teamwork between physicians and patients [15]. Two components of successful teamwork are physician-patient communication and shared decision-making, both of which have been shown to improve patient satisfaction, adherence to treatment plans and health outcomes [16–23]. In shared decision-making, the physician and patient share medical information [24–26]. Specifically, the physician presents different treatment options to the patient and describes the risks and benefits of each option. Then the patient expresses his or her preferences for treatment to ensure that the care provided aligns with the patient’s values and needs [27]. Thus, shared decision-making in the treatment relationship is predicated on effective communication between the physician and patient [19].
Effective physician-patient communication is supported by continuous care [19,28], a secure attachment style [29, 30], shared goals [19], a mutual understanding of respective roles and tasks [15,31–33], and a bond characterized by liking, confidence, and trust [19,28,31]. Trust is paramount in physician-patient communication. Interpersonal trust and social trust are the 2 predominant types [34]. Interpersonal trust refers to the relationship the patient has with the physician, specifically the confidence the patient has in the physician as well as the responsibility, competence, compassion, and regard the physician has for the patient’s welfare [34–36]. For patients and physicians, interpersonal trust is developed over time with repeated interactions [34–36]. On the other hand, social trust refers to the beliefs of honesty, integrity, and reliability in others [36]. Social trust is influenced by social constructs, including the media and institutions of higher education [36].
In the physician-patient relationship, self-care communication is largely influenced by interpersonal trust. A patient’s trust can be acquired through multiple medical appointments with the physician. Further, how the patient is treated during these appointments as well as how much time and attention the physician invests in the patient’s care influences the level of interpersonal trust. A high level of trust in the relationship can lead to in improvements in adherence to self-care, continuity of care, physician-patient communication, and overall quality of the physician-patient relationship [37–39].
In the diabetes physician-patient relationship, minimal research has explored how trust in one’s physician impacts self-care communication. In a study by Beverly and colleagues, diabetes patients emphasized the importance of a trusting physician-patient relationship for diabetes care [27]. Another study by Ritholz and colleagues found that physicians and patients both stress the importance of developing trust to facilitate self-care communication [40]. Specifically, trust as well as acceptance from the physician contributes to open and honest self-care communication in the physician-patient diabetes relationship[40]. Additional research is needed to determine whether a high level of physician-patient trust is associated with increased self-care behaviors and improved diabetes outcomes over time.
Importance of Diabetes Self-Care Communication
Diabetes self-care communication in the physician-patient relationship increases patient satisfaction, improves adherence to treatment regimens, and leads to better clinical outcomes [22,41–43]. For physicians, effective self-care communication requires the performance of specific communication tasks and behaviors, including collecting a medical history, explaining a diagnosis and prognosis, and providing clear and concise therapeutic instructions [44]. In addition, physicians must incorporate interpersonal and relational skills to establish a trusting relationship [44,45]. Both physicians and patients agree that a trusting treatment relationship is a requirement for open and honest self-care communication [45]. For patients, effective communication necessitates the disclosure of self-care successes and failures [46]. Diabetes patients face challenging self-care regimens, and these challenges can interfere with glycemic control and increase the risk for diabetes complications [47,48]. For this reason, patients must feel comfortable discussing their self-are challenges so that their physician can individualize treatment prescriptions and recommendations, thereby increasing the likelihood of treatment success.
Barriers to Self-Care Communication
Physician-patient self-care communication is essential to improving patient adherence [29,49] yet numerous barriers exist that undermine effective physician-patient self-care communication. From the physician perspective, the most commonly cited barrier to self-care communication is time [50]. A recent study of family medicine practices found that the time physicians spent discussing self-care with their patients varied from 1 to 17 minutes, suggesting that time is a major barrier to self-care communication [51]. Other barriers include lack of collaboration and teamwork among health care providers, lack of patients’ access to resources, and lack of psychosocial support for patients with diabetes [50]. Relatedly, Beverly and colleagues [52] found that physicians often feel inadequately trained to address diabetes patients’ psychosocial issues and this perceived lack of expertise may contribute to physicians feeling overwhelmed and frustrated within the physician-patient relationship, which may hinder open self-care communication.
For patients, barriers tend to differ from those perceived by physicians. A qualitative study using semi-structured interviews with patients and clinicians, and direct observation of clinical encounters at an inner-city family practice training site, revealed different perceptions of the term “control” between physicians and patients. In practice, physicians used the term “control” to focus on the management of blood glucose levels rather than trying to understand the patients’ understanding of diabetes and subsequent treatment goals. Differing viewpoints contributed to frustration and hindered effective communication [53]. In another qualitative study with physicians and patients, both noted that patients were reluctant to discuss self-care for fear being judged or shamed about food intake and weight [45]. This finding was supported in a quantitative follow-up study assessing patient reluctance to discuss self-care. Thirty percent of surveyed patients reported reluctance to discussing self-care with their physicians for fear of being judged, not wanting to disappoint their doctors, guilt, and shame [14]. Interestingly, patients reporting elevated depressive symptoms were more likely to be reluctant to discuss their self-care [14]. Cognitive behavioral changes (eg, cognitive distortions, avoidance behavior, attention deficits) associated with major depression and depressive symptoms may impair patients’ ability to recall self-care information. Also, patients reporting more depressive symptoms may be more socially withdrawn during a medical appointment, and thus less willing to communicate with their physician about self-care.
Other studies found that psychosocial factors such as diabetes distress [54,55] and pessimistic attitudes [56–59], cultural differences [60–66], lack of family and social support [60,67–70], lack of readiness to change behavior [71], introversion and social isolation [72,73], hypo-glycemia fear [74,75] and ineffectual coping styles [76,77] interfere with self-care and glycemic control. Further, low health literacy is associated with difficulty adhering to self-care, particular medication regimens, and negative health outcomes [78].
In summary psychosocial barriers and health literacy may affect a patients’ willingness to discuss self-care during a medical visit. Therefore, routine assessment of psychosocial factors and health literacy may be necessary to address a patient’s barriers to self-care as well as to promote open and honest self-care communication. Interventions and evidenced-based approaches that address psychosocial factors, health literacy, and physician-patient self-care communication are needed.
Facilitators to Self-Care Communication
Despite numerous barriers to self-care communication, several factors promote self-care communication in the physician-patient relationship. For example, direct and non-accusatory communication from physicians as well as providing patients with hope for living with diabetes both support physician-patient self-care communication [45]. A recent systematic review by Sohal and colleagues [79] found that trust in physicians, the use of culturally appropriate exercise and dietary advice, and increasing family involvement improved physician-patient communication and diabetes self-care [79]. Lastly, a study by Schillinger and colleagues [80] found that physician assessment of patient recall and comprehension of new concepts during medical visits improved diabetes outcomes [80].
Patient-Physician Self-Care Communication Interventions
One of the more successful interventions for improving diabetes self-care and patient-physician communication is motivational interviewing (MI). MI is a non-judgmental communication style designed to explore a patient’s intrinsic motivation to change health behaviors [81]. Inherent to MI is the belief that motivation for change is malleable and that it can be transformed in the context of the patient-physician relationship [81]. MI is a patient-centered method designed to empower a patient’s ability and responsibility to make health-related decisions, with the physician supporting the patient’s autonomy in the process [82]. Recent meta-analyses and systematic reviews [83–87] showed that MI interventions improve self-care behaviors and glycemic control in the short-term; long-term effects of MI on self-care and glycemia remain inconclusive. More high-quality research is needed to evaluate the MI training content of these interventions in order to determine its long-term effectiveness and replicate outcomes in various healthcare settings [87].
Other studies not included in the meta-analyses and reviews found MI interventions improved self-care behaviors [88–90], glycemic control [90,91], and quality of life [91]. A qualitative study exploring diabetes patients’ experiences with MI and self-care behaviors revealed that patients’ appreciate when providers initiate discussions that result in new ways of thinking about self-care and promote a sense of well-being in patients [92]. New research utilizing patient navigators to connect diabetes patients’ to their primary care providers showed MI techniques improved patient self-efficacy and glycemic control [93]. Another study, an internet-based incentives study, found that the application of a brief MI interviewing session improved blood glucose monitoring in adolescents with type 1 diabetes [94]. Thus, creative strategies that employ MI techniques in collaboration with other members of the health care team (ie, patient navigation [93], telehealth [89], health coaching [95], internet-based tools [94]) hold promise for improving self-care and patient-physician communication. Increased collaboration with members of the health care team (eg, certified diabetes educators, nurses, dietitians, pharmacists, exercise physiologists), community health workers [96,97] and peer mentors [98,99] may help reinforce messages, promote shared decision-making, improve diabetes outcomes, increase patient satisfaction, and reduce medical costs [100].
Few other interventions have directly addressed physician-patient diabetes self-care communication. One older study examined the effectiveness of an intervention designed to increase of diabetes patients’ involvement in medical decision-making [16]. Patients randomized to the intervention arm participated in a 20-minute session prior to meeting with their physician, in which researchers reviewed their medical chart and used systematic prompts to encourage patients to negotiate medical decisions with their physician. Patients in the control arm received standard educational materials in a session of equal length. Patients in the intervention arm improved glycemia and elicited twice the amount of medical information from their physician compared to controls [16]. These findings suggest that brief interventions prior to medical appointments can improve patient communication, self-care behavior, and in turn, diabetes outcomes [16].
A recent study evaluated the effectiveness of a training program in communication skills for pediatric diabetes care providers in the UK [101, 102]. In this cluster randomized controlled trial, pediatric providers allocated to the Talking Diabetes intervention participated in web-based material and face-to-face seminars designed to prepare providers for constructive self-care conversations with patients as well as skills for promoting behavior change. The psychoeducational training emphasized shared decision-making and utilized motivational interviewing techniques [101]. Twenty-six centers and 693 young people with type 1 diabetes participated in the study [102]. At 12-month follow-up, the Talking Diabetes intervention did not demonstrate improvements in glycemic control. Further, the intervention had a negative effect on patients’ quality of life but a short-term improvement in coping [102]. Interestingly, parents of patients in the intervention arm reported greater continuity of care, which suggests that parents benefited more from the intervention than their children. Future communication interventions targeting the pediatric population should provide ongoing support to children of physicians exposed to interventions such as Talking Diabetes [102].
Currently, 3 ongoing studies aim to improve self-care and clinical outcomes via physician-patient communication interventions. A study by Ricci-Cabello and colleagues [103] aims to improve diabetes self-care by enhancing patient-physician communication in an underserved community of adults with uncontrolled type 2 diabetes. In this 3-arm randomized controlled trial, patients allocated to groups A and B received communication skills training and graphic feedback about glycosylated hemoglobin A1c levels; patients in group C received usual care. Patients in group B also received telephone reinforcement [103]. The second study, by Billimek and colleagues, aims to improve physician-patient communication about medication regimens via diabetes coaching [104]. In this intervention, 190 Mexican-American adult patients with type 2 diabetes were randomly assigned to complete a Coached Care visit with trained community health workers or a Coached Care visit plus the EMPATHy software toolkit, a computer-based activity with strategies and resources to overcome self-care barriers. The primary endpoints are (1) the development of care plan that addresses everyday barriers to medication adherence and (2) completion of a concrete behavioral goal [104]. Finally, the third study, by Grant and colleagues, aims to improve physician-patient communication via a pre-visit prioritization of diabetes concerns. In this controlled, cluster-randomized, multisite trial, primary care physicians were randomized to the Pre-Visit Prioritization for Complex Patients with Diabetes or the control group [105]. The Pre-Visit Prioritization IT-tool is designed to help patients identify one or two concerns prior to a medical visit and then send these priorities to the primary care physician via an electronic health record. The overall goal of the intervention is to improve communication of self-care concerns during a medical visit [105]. Findings from these 3 interventions are forthcoming; findings may provide evidence for validated interventions that improve physician-patient self-care communication in diabetes.
Techniques to Improve Self-Care Communication
Incorporating communication skills in continuing medical education and diabetes education may improve self-care communication in the physician-patient relationship. Educational programs that teach physicians how to provide consistent messages, repeat information, reinforce and offer feedback regarding specific self-care behaviors, and problem-solve self-care challenges may improve patients’ willingness to discuss self-care [14,106]. Most patients will remember only a small portion of the information given to them during medical visit. Studies that compare how much information patients retain versus how much information physicians provide show that patients forget 31% to 71% of information [107]. Therefore, physicians need techniques that promote open self-care communication during a visit. The following techniques can help physicians improve self-care communication [108]:
- Discuss the most important self-care information first; patients tend to remember the information that is presented first.
- Use the phrase “This is very important…” when discussing key points because patients will remember things that are perceived as important.
- Deliver simple, clear, and concrete instructions; patients are more likely to forget complex or confusing instructions. For example, “Check your blood glucose every morning within five minutes of waking up and before you eat breakfast” is more specific and easier to follow than “Check your blood glucose”.
- Ask open-ended questions to allow patients to verbalize feelings or concerns about their diabetes self-care.
- Employ MI techniques to help patients who are struggling to initiate and adhere to self-care behaviors. MI tools, such as the Readiness Ruler, Self-Evaluation Rulers, Decisional Balance Matrix, and Health Behavior Menu (Figure), may help patients and physicians discuss self-care behaviors during a medical visit [109].
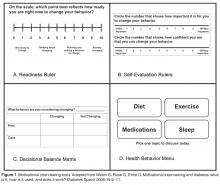
– Express empathy by reflective listening and asking patients for permission before offering information or advice about diabetes self-care.
– Roll with resistance by engaging the patient in the process of problem solving rather than opposing a patient’s resistance to change behaviors.
– Develop discrepancy by helping the patient recognize that there is an inconsistency between his/her behavior and personal goals.
– Support self-efficacy by empowering the patient to believe that he/she can change behaviors.
6. Demonstrate active listening skills by reflecting and summarizing the patient’s statements. Reflecting and summarizing show the patient that the physician has been listening to concerns and understands what the patient is saying. This is also an opportunity to correct any miscommunications from the visit.
7. Write down instructions or provide handouts to the patient to help reinforce learning and information retention.
8. Ask patients to write a list of questions a few days prior to the medical appointment and bring it with them. Patients are more likely to remember information about issues they have previously considered that directly relate to them.
9. Consider collaborating with community health workers, patient navigators, peer mentors, and other members of the healthcare team to improve communication, diabetes outcomes, and patient satisfaction.
Summary
Physician-patient self-care communication is essential to achieving optimal diabetes outcomes [15,22,33,110] Patients’ ability to inform physicians about their self-care challenges [14], and physicians’ ability to respond to patients’ self-care reports directly and in non-accusatory language, are vital factors in effective diabetes care [45]. Interventions and education that promote open and honest conversations are particularly important given patients’ well-documented struggles achieving self-care and glycemic goals [111] and physicians’ feelings of inadequacy, frustration, and fatigue when they are not making an impact on patients’ outcomes [48,112]. More research is needed to determine the best strategies to improve self-care communication in the physician-patient relationship.
Corresponding author: Elizabeth A. Beverly, PhD, Department of Family Medicine, Ohio University Heritage College of Osteopathic Medicine, Athens, OH 45701, beverle1@ohio.edu.
Financial disclosures: None.
Author contributions: drafting of article, EAB, MFW, ABC, KEP, NNI; critical revision of the article, EAB, MFW, ABC, KEP, NNI.
1. Anderson E, Kian EM. Examining media contestation of masculinity and head trauma in the National Football League. J Men Masculinities 2011;1–22.
2. CDC. National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011.
3. Bandura A. Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice Hall; 1986.
4. Jacobson AM, Adler AG, Derby L, et al. Clinic attendance and glycemic control. Study of contrasting groups of patients with IDDM. Diabetes Care 1991;14:599–601.
5. Dyer PH, Lloyd CE, Lancashire RJ, et al. Factors associated with clinic non-attendance in adults with type 1 diabetes mellitus. Diab Med 1998;15:339–43.
6. Conn VS, Hafdahl AR, Mehr DR, et al. Metabolic effects of interventions to increase exercise in adults with type 2 diabetes. Diabetologia 2007;50:913–21.
7. Maiorana A, O’Driscoll G, Goodman C, et al. Combined aerobic and resistance exercise improves glycemic control and fitness in type 2 diabetes. Diab Res Clin Pract 2002;56:115–23.
8. Pi-Sunyer FX, Maggio CA, McCarron DA, et al. Multicenter randomized trial of a comprehensive prepared meal program in type 2 diabetes. Diabetes Care 1999;22:191–7.
9. Delahanty LM, Halford BN. The role of diet behaviors in achieving improved glycemic control in intensively treated patients in the Diabetes Control and Complications Trial. Diabetes Care 1993;16:1453–8.
10. Gafarian CT, Heiby EM, Blair P, Singer F. The Diabetes Time Management Questionnaire. Diabetes Educ 1999;25:585–92.
11. Wdowik MJ, Kendall PA, Harris MA. College students with diabetes: using focus groups and interviews to determine psychosocial issues and barriers to control. Diabetes Educ 1997;23:558–62.
12. Rubin RR, Peyrot M. Psychological issues and treatment for people with diabetes. J Clin Psychol 2001;57:457–78.
13. Ali MK, Bullard KM, Gregg EW. Achievement of goals in U.S. Diabetes Care, 1999-2010. N Engl J Med 2013;369:287–8.
14. Beverly EA, Ganda OP, Ritholz MD, et al. Look who’s (not) talking: diabetic patients’ willingness to discuss self-care with physicians. Diabetes Care 2012;35:1466–72.
15. Heisler M, Vijan S, Anderson RM, et al. When do patients and their physicians agree on diabetes treatment goals and strategies, and what difference does it make? J Gen Intern Med 2003;18:893–902.
16. Greenfield S, Kaplan SH, Ware JE Jr, et al. Patients’ participation in medical care: effects on blood sugar control and quality of life in diabetes. J Gen Intern Med 1988;3:448–57.
17. Greenfield S, Kaplan S, Ware JE Jr. Expanding patient involvement in care. Effects on patient outcomes. Ann Intern Med 1985;102:520–8.
18. Anderson RM, Funnell MM, Butler PM, et al. Patient empowerment. Results of a randomized controlled trial. Diabetes Care 1995;18:943–9.
19. Von Korff M, Gruman J, Schaefer J, et al. Collaborative management of chronic illness. Ann Intern Med 1997;127:1097–102.
20. Campbell SM, Hann M, Hacker J, et al. Identifying predictors of high quality care in English general practice: observational study. BMJ 2001;323:784–7.
21. Bower P, Campbell S, Bojke C, Sibbald B. Team structure, team climate and the quality of care in primary care: an observational study. Qual Saf Health Care 2003;12:273–9.
22. Piette JD, Schillinger D, Potter MB, Heisler M. Dimensions of patient-provider communication and diabetes self-care in an ethnically diverse population. J Gen Intern Med 2003;18:624-33.
23. Kerr EA, Smith DM, Kaplan SH, Hayward RA. The association between three different measures of health status and satisfaction among patients with diabetes. Med Care Res Rev 2003;60:158-77.
24. Oshima Lee E, Emanuel EJ. Shared decision making to improve care and reduce costs. N Engl J Med 2013;368:6-8.
25. Barry MJ, Edgman-Levitan S. Shared decision making--pinnacle of patient-centered care. N Engl J Med 2012;366:780–1.
26. Truog RD. Patients and doctors--evolution of a relationship. N Engl J Med 2012;366:581–5.
27. Beverly EA, Wray LA, LaCoe CL, Gabbay R. Listening to older adults’ values and preferences for type 2 diabetes care: a qualitative study. Diabetes Spectrum 2014;27:44–9.
28. Bordin ES. The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy 1979;26:252–60.
29. Ciechanowski PS, Katon WJ, Russo JE, Walker EA. The patient-provider relationship: attachment theory and adherence to treatment in diabetes. Am J Psychiatry 2001;158:29–35.
30. Ciechanowski P, Russo J, Katon W, et al. Influence of patient attachment style on self-care and outcomes in diabetes. Psychosom Med 2004;66:720–8.
31. Jahng KH, Martin LR, Golin CE, DiMatteo MR. Preferences for medical collaboration: patient-physician congruence and patient outcomes. Patient Educ Couns 2005;57:308–14.
32. Street RL Jr, Krupat E, Bell RA, et al. Beliefs about control in the physician-patient relationship: effect on communication in medical encounters. J Gen Intern Med 2003;18:609–16.
33. Heisler M, Bouknight RR, Hayward RA, et al. The relative importance of physician communication, participatory decision making, and patient understanding in diabetes self-management. J Gen Intern Med 2002;17:243–52.
34. Mechanic D. Changing medical organization and the erosion of trust. Milbank Q 1996;74:171–89.
35. Mechanic D, Schlesinger M. The impact of managed care on patients’ trust in medical care and their physicians. JAMA 1996;275:1693–7.
36. Pearson SD, Raeke LH. Patients’ trust in physicians: many theories, few measures, and little data. J Gen Intern Med 2000;15:509–13.
37. Jones DE, Carson KA, Bleich SN, Cooper LA. Patient trust in physicians and adoption of lifestyle behaviors to control high blood pressure. Patient Educ Couns 2012;89:57–62.
38. Mostashari F, Riley E, Selwyn PA, Altice FL. Acceptance and adherence with antiretroviral therapy among HIV-infected women in a correctional facility. J Acquired Immun Def Syndr Hum Retrovir 1998;18:341–8.
39. Cooper-Patrick L, Gallo JJ, Gonzales JJ, et al. Race, gender, and partnership in the patient-physician relationship. JAMA 1999;282:583–9.
40. Ritholz MD, Beverly EA, Brooks KM, et al. Barriers and facilitators to self-care communication during medical appointments in the United States for adults with type 2 diabetes. Chronic Illn 2014;10:303–13.
41. Aikens JE, Bingham R, Piette JD. Patient-provider communication and self-care behavior among type 2 diabetes patients. Diabetes Educ 2005;31:681–90.
42. Bundesmann R, Kaplowitz SA. Provider communication and patient participation in diabetes self-care. Patient Educ Couns 2011;85:143–7.
43. Heisler M, Cole I, Weir D, et al. Does physician communication influence older patients’ diabetes self-management and glycemic control? Results from the Health and Retirement Study (HRS). J Gerontol A Biol Sci Med Sci 2007;62:1435–42.
44. Duffy FD, Gordon GH, Whelan G, et al. Assessing competence in communication and interpersonal skills: the Kalamazoo II report. Acad Med 2004;79:495–507.
45. Ritholz MD, Beverly EA, Brooks KM, et al. Barriers and facilitators to self-care communication during medical appointments in the United States for adults with type 2 diabetes. Chronic Illn 2014;10:303–13.
46. Ciechanowski P, Katon WJ. The interpersonal experience of health care through the eyes of patients with diabetes. Soc Sci Med 2006;63:3067–79.
47. Diabetes Control and Complications Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329:977–86.
48. Peyrot M, Rubin RR, Lauritzen T, et al. Psychosocial problems and barriers to improved diabetes management: results of the Cross-National Diabetes Attitudes, Wishes and Needs (DAWN) Study. Diab Med 2005;22:1379–85.
49. DiMatteo MR, Linn LS, Chang BL, Cope DW. Affect and neutrality in physician behavior: a study of patients’ values and satisfaction. J Behav Med 1985;8:397–409.
50. Stuckey HL, Vallis M, Kovacs Burns K, et al. “I do my best to listen to patients”: qualitative insights into DAWN2 (Diabetes Psychosocial Care From the Perspective of Health Care Professionals in the Second Diabetes Attitudes, Wishes and Needs Study). Clin Ther 2015;37:1986–98.
51. Kruse RL, Olsberg JE, Oliver DP, et al. Patient-provider communication about diabetes self-care activities. Fam Med 2013;45:319–22.
52. Beverly EA, Hultgren BA, Brooks KM, et al. Understanding physicians’ challenges when treating type 2 diabetic patients’ social and emotional difficulties: a qualitative study. Diabetes Care 2011;34:1086–8.
53. Freeman J, Loewe R. Barriers to communication about diabetes mellitus. Patients’ and physicians’ different view of the disease. J Fam Pract 2000;49:507–12.
54. Gonzalez JS, Delahanty LM, Safren SA, et al. Differentiating symptoms of depression from diabetes-specific distress: relationships with self-care in type 2 diabetes. Diabetologia 2008;51:1822–5.
55. Fisher L, Hessler DM, Polonsky WH, Mullan J. When is diabetes distress clinically meaningful?: establishing cut points for the Diabetes Distress Scale. Diabetes Care 2012;35:259–64.
56. Polonsky WH, Anderson BJ, Lohrer PA, et al. Assessment of diabetes-related distress. Diabetes Care 1995;18:754–60.
57. Welch G, Weinger K, Anderson B, Polonsky WH. Responsiveness of the Problem Areas In Diabetes (PAID) questionnaire. Diabetic Med 2003;20:69–72.
58. Weinger K, Kinsley BT, Bajaj M, et al. Diabetes-related emotional distress: A barrier to improving glycemic control during intensive diabetes treatment. Abstract. Diabetes 1997;46:Supp1:268A.
59. Weinger K, Jacobson AM. Psychosocial and quality of life correlates of glycemic control during intensive treatment of type 1 diabetes. Patient Educ Couns 2001;42:123–31.
60. Fisher L, Chesla CA, Skaff MM, et al. The family and disease management in Hispanic and European-American patients with type 2 diabetes. Diabetes Care 2000;23:267–72.
61. Wen LK, Parchman ML, Shepherd MD. Family support and diet barriers among older Hispanic adults with type 2 diabetes. Fam Med 2004;36:423–30.
62. Chesla CA, Fisher L, Mullan JT, et al. Family and disease management in African-American patients with type 2 diabetes. Diabetes Care 2004;27:2850–5.
63. Brown SA, Harrist RB, Villagomez ET, et al. Gender and treatment differences in knowledge, health beliefs, and metabolic control in Mexican Americans with type 2 diabetes. Diabetes Educ 2000;26:425–38.
64. Fisher L, Chesla CA, Chun KM, et al. Patient-appraised couple emotion management and disease management among Chinese American patients with type 2 diabetes. J Fam Psychol 2004;18:302–10.
65. Akimoto M, Fukunishi I, Kanno K, et al. Psychosocial predictors of relapse among diabetes patients: a 2-year follow-up after inpatient diabetes education. Psychosomatics 2004;45:343–9.
66. Samuel-Hodge CD, Headen SW, Skelly AH, et al. Influences on day-to-day self-management of type 2 diabetes among African-American women: spirituality, the multi-caregiver role, and other social context factors. Diabetes Care 2000;23:928–33.
67. Wing RR, Marcus MD, Epstein LH, Jawad A. A “family-based” approach to the treatment of obese type II diabetic patients. J Consult Clin Psychol 1991;59:156–62.
68. Trief PM, Ploutz-Snyder R, Britton KD, Weinstock RS. The relationship between marital quality and adherence to the diabetes care regimen. Ann Behav Med 2004;27:148–54.
69. Gleeson-Kreig J, Bernal H, Woolley S. The role of social support in the self-management of diabetes mellitus among a Hispanic population. Pub Health Nurs 2002;19:215–22.
70. Wen LK, Shepherd MD, Parchman ML. Family support, diet, and exercise among older Mexican Americans with type 2 diabetes. Diabetes Educ 2004;30:980–93.
71. Ruggiero L. Helping people with diabetes change behavior: from theory to practice. Diab Spectrum 2000;13:125–32.
72. Orr DP, Golden MP, Myers G, Marrero DG. Characteristics of adolescents with poorly controlled diabetes referred to a tertiary care center. Diabetes Care 1983;6:170–5.
73. Lane JD, Stabler B, Ross SL, et al. Psychological predictors of glucose control in patients with IDDM. Diabetes Care 1988;11:798–800.
74. Irvine AA, Cox D, Gonder-Frederick L. Fear of hypoglycemia: relationship to physical and psychological symptoms in patients with insulin-dependent diabetes mellitus. Health Psychology 1992;11:135–8.
75. Irvine A, Cox D, Gonder-Frederick L. The fear of hypoglycemia scale. In: Bradley C, editor. Handbook of psychology and diabetes. Harwood Academic; 1994.
76. Peyrot MF, McMurry JF Jr. Stress buffering and glycemic control. The role of coping styles. Diabetes Care 1992;15:842–6.
77. Peyrot M, McMurry JF Jr, Kruger DF. A biopsychosocial model of glycemic control in diabetes: stress, coping and regimen adherence. J Health Soc Behav 1999;40:141–58.
78. Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med 2011;155:97–107.
79. Sohal S, Sohal P, King-Shier KM, Khan NA. Barriers and facilitators for type-2 diabetes management in South Asians: a systematic review. PloS One 2015:1–15.
80. Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med 2003;163:83–90.
81. Miller WR, Rollnick S. Motivational interviewing: preparing people for change. New York: Guilford Press; 2002.
82. Powell PW, Corathers SD, Raymond J, Streisand R. New approaches to providing individualized diabetes care in the 21st century. Curr Diabetes Rev 2015;11:222–30.
83. Jones AJ, Gladstone BP, Lubeck M, et al. Motivational interventions in the management of HbA1c levels: A systematic review and meta-analysis. Prim Care Diabetes 2014;8:91–100.
84. Song D, Xu TZ, Sun QH. Effect of motivational interviewing on self-management in patients with type 2 diabetes mellitus: a meta-analysis. Intl J Nurs Sci 2014;1:291–7.
85. Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs 2014;23:8–14.
86. Noordman J, van der Weijden T, van Dulmen S. Communication-related behavior change techniques used in face-to-face lifestyle interventions in primary care: a systematic review of the literature. Patient Educ Couns 2012;89:227–44.
87. Soderlund LL, Madson MB, Rubak S, Nilsen P. A systematic review of motivational interviewing training for general health care practitioners. Patient Educ Couns 2011;84:16–26.
88. Kang SH, Kim BG, Lee GM. Justification of continuous packed-bed reactor for retroviral vector production from amphotropic PsiCRIP murine producer cell. Cytotechnology 2000;34(1–2):151–8.
89. Holmen H, Torbjornsen A, Wahl AK, et al. A mobile health intervention for self-management and lifestyle change for persons with type 2 diabetes, part 2: one-year results from the Norwegian randomized controlled trial RENEWING HEALTH. JMIR mHealth uHealth 2014;2(4):e57.
90. Chlebowy DO, El-Mallakh P, Myers J, et al. Motivational interviewing to improve diabetes outcomes in African Americans adults with diabetes. West J Nurs Res 2015;37:566–80.
91. Kang HY, Gu MO. [Development and effects of a motivational interviewing self-management program for elderly patients with diabetes mellitus]. J Kor Acad Nurs 2015;45:533–43.
92. Brobeck E, Odencrants S, Bergh H, Hildingh C. Patients’ experiences of lifestyle discussions based on motivational interviewing: a qualitative study. BMC Nursing 2014;13:13.
93. Loskutova NY, Tsai AG, Fisher EB, et al. Patient navigators connecting patients to community resources to improve diabetes outcomes. J Am Board Fam Med 2016;29:78–89.
94. Raiff BR, Barry VB, Ridenour TA, Jitnarin N. Internet-based incentives increase blood glucose testing with a non-adherent, diverse sample of teens with type 1 diabetes mellitus: a randomized controlled Trial. Trans Behav Med 2016;6:179–88.
95. Sahlen KG, Johansson H, Nystrom L, Lindholm L. Health coaching to promote healthier lifestyle among older people at moderate risk for cardiovascular diseases, diabetes and depression: a study protocol for a randomized controlled trial in Sweden. BMC Public Health 2013;13:199.
96. Kane EP, Collinsworth AW, Schmidt KL, et al. Improving diabetes care and outcomes with community health workers. Fam Pract 2016;33:523–8.
97. Wagner JA, Bermudez-Millan A, Damio G, et al. A randomized, controlled trial of a stress management intervention for Latinos with type 2 diabetes delivered by community health workers: Outcomes for psychological wellbeing, glycemic control, and cortisol. Diabetes Res Clin Pract 2016;120:162–70.
98. Rogers EA, Hessler DM, Bodenheimer TS, et al. Diabetes peer coaching: do “better patients” make better coaches? Diabetes Educ 2014;40:107–15.
99. Long JA, Jahnle EC, Richardson DM, et al. Peer mentoring and financial incentives to improve glucose control in African American veterans: a randomized trial. Ann Intern Med 2012;156:416–24.
100. Mundt MP, Agneessens F, Tuan WJ, et al. Primary care team communication networks, team climate, quality of care, and medical costs for patients with diabetes: A cross-sectional study. Int J Nurs Stud 2016;58:1–11.
101. Fisher L, Mullan JT, Arean P, et al. Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care 2010;33:23–8.
102. Fisher L, Glasgow RE, Strycker LA. The relationship between diabetes distress and clinical depression with glycemic control among patients with type 2 diabetes. Diabetes Care 2010;33:1034–6.
103. Ricci-Cabello I, Olry de Labry-Lima A, Bolivar-Munoz J, et al. Effectiveness of two interventions based on improving patient-practitioner communication on diabetes self-management in patients with low educational level: study protocol of a clustered randomized trial in primary care. BMC Health Serv Res 2013;13:433.
104. Billimek J, Guzman H, Angulo MA. Effectiveness and feasibility of a software tool to help patients communicate with doctors about problems they face with their medication regimen (EMPATHy): study protocol for a randomized controlled trial. Trials 2015;16:145.
105. Grant RW, Uratsu CS, Estacio KR, et al. Pre-Visit Prioritization for complex patients with diabetes: Randomized trial design and implementation within an integrated health care system. Contemp Clin Trials 2016;47:196–201.
106. Ritholz MD, Beverly EA, Abrahamson MJ, et al. Physicians’ perceptions of the type 2 diabetes multidisciplinary treatment team: a qualitative study. Diabetes Educ 2011.
107. Ley P. Satisfaction, compliance and communication. Br J Clin Psychol 1982;21:241–54.
108. Weinger K, Smaldone A, Beverly EA. Psychosocial and educational implications of diabetic foot complications. In: Veves A, Giurini JM, LoGerfo FW, editors. The diabetic foot: medical and surgical management. Boston: Springer; 2012:503–18.
109. Welch G, Rose G, Ernst D. Motivational interviewing and diabetes: what is it, how is it used, and does it work? Diabetes Spectr 2006;19:5–11.
110. Kaplan SH, Greenfield S, Ware JE Jr. Assessing the effects of physician-patient interactions on the outcomes of chronic disease. Med Care 1989;27(3 Suppl):S110–27.
111. Nelson KM, Reiber G, Boyko EJ. Diet and exercise among adults with type 2 diabetes: findings from the third national health and nutrition examination survey (NHANES III). Diabetes Care 2002;25:1722–8.
112. Wens J, Vermeire E, Royen PV, et al. GPs’ perspectives of type 2 diabetes patients’ adherence to treatment: A qualitative analysis of barriers and solutions. BMC Fam Pract 2005;6:20.
Abstract
- Objective: To summarize the current literature, research findings, and interventions for self-care communication in the physician-patient relationship.
- Methods: Literature review.
- Results: Diabetes management requires patients to follow complex self-care recommendations for nutrition, physical activity, blood glucose monitoring, and medication. Adherence to these recommendations improves glycemic control and mitigates the risk of diabetes complications; however, many patients struggle to follow these behaviors in everyday life. In the physician-patient relationship, self-care communication is largely influenced by interpersonal trust. Physicians need to incorporate interpersonal and relational skills to establish a trusting relationship. Physician-level barriers to self-care communication include lack of time, lack of collaboration and teamwork among health care providers, lack of patients’ access to resources, and lack of psychosocial support for diabetes patients. Among patients, psychosocial barriers and health literacy may affect willingness to discuss self-care. Motivational interviewing techniques may be helpful for improving communication around patient self-management and promotion of healthy behaviors.
- Conclusion: Physicians can assist patients with their diabetes self-care by discussing self-care challenges during medical visits.
Diabetes is one of the most significant and growing chronic health problems in the world, affecting approximately 415 million people [1]. Diabetes is marked by the body’s inability to make insulin as well as the body’s inability to effectively use the insulin it produces [2]. Diagnosis of diabetes has increased sharply in recent decades and is expected to increase even more, with the largest increases in middle- and low-income countries [3]. Diabetes is a leading cause of blindness, kidney failure, myocardial infarction, stroke, and amputation [3], and in 2015 it accounted for 5 million deaths worldwide [1]. Further, diabetes’s costs to society represent 12% ($673 billion) of global health expenditures [1]. By 2040, models predict that 642 million people will be diagnosed with diabetes and costs will continue to grow as the population ages [1]. Thus, prevention of diabetes is the ultimate goal; however, more effective management for individuals already diagnosed with diabetes is critical to reduce the risk of complications and the economic burden of the disease.
Diabetes management requires patients to perform complex self-care regimens, including weight reduction, frequent blood glucose monitoring, taking oral and/or insulin medications, engaging in physical activity, adhering to diabetes nutrition guidelines, and attending clinic appointments [4–9]. These self-care behaviors are critically linked to improved glycemic control, however, integrating them into one’s daily life can be challenging [10–12]. Recent National Health and Nutrition Examination Survey (NHANES) data show that approximately half of adults with diabetes are not meeting recommended goals for diabetes care [13]. Physicians can assist patients with their diabetes self-care by scheduling frequent follow-up visits and discussing self-care challenges with their patients [14].
In this review, we discuss the current literature on physician-patient communication and diabetes self-care. First, we discuss the qualities of an effective physician-patient relationship followed by the importance of self-care communication in diabetes care. Next, we discuss barriers and facilitators to self-care communication. Finally, we review interventions for improving physician-patient communication in diabetes self-care.
Qualities of an Effective Physician-Patient Relationship
Successful diabetes care requires teamwork between physicians and patients [15]. Two components of successful teamwork are physician-patient communication and shared decision-making, both of which have been shown to improve patient satisfaction, adherence to treatment plans and health outcomes [16–23]. In shared decision-making, the physician and patient share medical information [24–26]. Specifically, the physician presents different treatment options to the patient and describes the risks and benefits of each option. Then the patient expresses his or her preferences for treatment to ensure that the care provided aligns with the patient’s values and needs [27]. Thus, shared decision-making in the treatment relationship is predicated on effective communication between the physician and patient [19].
Effective physician-patient communication is supported by continuous care [19,28], a secure attachment style [29, 30], shared goals [19], a mutual understanding of respective roles and tasks [15,31–33], and a bond characterized by liking, confidence, and trust [19,28,31]. Trust is paramount in physician-patient communication. Interpersonal trust and social trust are the 2 predominant types [34]. Interpersonal trust refers to the relationship the patient has with the physician, specifically the confidence the patient has in the physician as well as the responsibility, competence, compassion, and regard the physician has for the patient’s welfare [34–36]. For patients and physicians, interpersonal trust is developed over time with repeated interactions [34–36]. On the other hand, social trust refers to the beliefs of honesty, integrity, and reliability in others [36]. Social trust is influenced by social constructs, including the media and institutions of higher education [36].
In the physician-patient relationship, self-care communication is largely influenced by interpersonal trust. A patient’s trust can be acquired through multiple medical appointments with the physician. Further, how the patient is treated during these appointments as well as how much time and attention the physician invests in the patient’s care influences the level of interpersonal trust. A high level of trust in the relationship can lead to in improvements in adherence to self-care, continuity of care, physician-patient communication, and overall quality of the physician-patient relationship [37–39].
In the diabetes physician-patient relationship, minimal research has explored how trust in one’s physician impacts self-care communication. In a study by Beverly and colleagues, diabetes patients emphasized the importance of a trusting physician-patient relationship for diabetes care [27]. Another study by Ritholz and colleagues found that physicians and patients both stress the importance of developing trust to facilitate self-care communication [40]. Specifically, trust as well as acceptance from the physician contributes to open and honest self-care communication in the physician-patient diabetes relationship[40]. Additional research is needed to determine whether a high level of physician-patient trust is associated with increased self-care behaviors and improved diabetes outcomes over time.
Importance of Diabetes Self-Care Communication
Diabetes self-care communication in the physician-patient relationship increases patient satisfaction, improves adherence to treatment regimens, and leads to better clinical outcomes [22,41–43]. For physicians, effective self-care communication requires the performance of specific communication tasks and behaviors, including collecting a medical history, explaining a diagnosis and prognosis, and providing clear and concise therapeutic instructions [44]. In addition, physicians must incorporate interpersonal and relational skills to establish a trusting relationship [44,45]. Both physicians and patients agree that a trusting treatment relationship is a requirement for open and honest self-care communication [45]. For patients, effective communication necessitates the disclosure of self-care successes and failures [46]. Diabetes patients face challenging self-care regimens, and these challenges can interfere with glycemic control and increase the risk for diabetes complications [47,48]. For this reason, patients must feel comfortable discussing their self-are challenges so that their physician can individualize treatment prescriptions and recommendations, thereby increasing the likelihood of treatment success.
Barriers to Self-Care Communication
Physician-patient self-care communication is essential to improving patient adherence [29,49] yet numerous barriers exist that undermine effective physician-patient self-care communication. From the physician perspective, the most commonly cited barrier to self-care communication is time [50]. A recent study of family medicine practices found that the time physicians spent discussing self-care with their patients varied from 1 to 17 minutes, suggesting that time is a major barrier to self-care communication [51]. Other barriers include lack of collaboration and teamwork among health care providers, lack of patients’ access to resources, and lack of psychosocial support for patients with diabetes [50]. Relatedly, Beverly and colleagues [52] found that physicians often feel inadequately trained to address diabetes patients’ psychosocial issues and this perceived lack of expertise may contribute to physicians feeling overwhelmed and frustrated within the physician-patient relationship, which may hinder open self-care communication.
For patients, barriers tend to differ from those perceived by physicians. A qualitative study using semi-structured interviews with patients and clinicians, and direct observation of clinical encounters at an inner-city family practice training site, revealed different perceptions of the term “control” between physicians and patients. In practice, physicians used the term “control” to focus on the management of blood glucose levels rather than trying to understand the patients’ understanding of diabetes and subsequent treatment goals. Differing viewpoints contributed to frustration and hindered effective communication [53]. In another qualitative study with physicians and patients, both noted that patients were reluctant to discuss self-care for fear being judged or shamed about food intake and weight [45]. This finding was supported in a quantitative follow-up study assessing patient reluctance to discuss self-care. Thirty percent of surveyed patients reported reluctance to discussing self-care with their physicians for fear of being judged, not wanting to disappoint their doctors, guilt, and shame [14]. Interestingly, patients reporting elevated depressive symptoms were more likely to be reluctant to discuss their self-care [14]. Cognitive behavioral changes (eg, cognitive distortions, avoidance behavior, attention deficits) associated with major depression and depressive symptoms may impair patients’ ability to recall self-care information. Also, patients reporting more depressive symptoms may be more socially withdrawn during a medical appointment, and thus less willing to communicate with their physician about self-care.
Other studies found that psychosocial factors such as diabetes distress [54,55] and pessimistic attitudes [56–59], cultural differences [60–66], lack of family and social support [60,67–70], lack of readiness to change behavior [71], introversion and social isolation [72,73], hypo-glycemia fear [74,75] and ineffectual coping styles [76,77] interfere with self-care and glycemic control. Further, low health literacy is associated with difficulty adhering to self-care, particular medication regimens, and negative health outcomes [78].
In summary psychosocial barriers and health literacy may affect a patients’ willingness to discuss self-care during a medical visit. Therefore, routine assessment of psychosocial factors and health literacy may be necessary to address a patient’s barriers to self-care as well as to promote open and honest self-care communication. Interventions and evidenced-based approaches that address psychosocial factors, health literacy, and physician-patient self-care communication are needed.
Facilitators to Self-Care Communication
Despite numerous barriers to self-care communication, several factors promote self-care communication in the physician-patient relationship. For example, direct and non-accusatory communication from physicians as well as providing patients with hope for living with diabetes both support physician-patient self-care communication [45]. A recent systematic review by Sohal and colleagues [79] found that trust in physicians, the use of culturally appropriate exercise and dietary advice, and increasing family involvement improved physician-patient communication and diabetes self-care [79]. Lastly, a study by Schillinger and colleagues [80] found that physician assessment of patient recall and comprehension of new concepts during medical visits improved diabetes outcomes [80].
Patient-Physician Self-Care Communication Interventions
One of the more successful interventions for improving diabetes self-care and patient-physician communication is motivational interviewing (MI). MI is a non-judgmental communication style designed to explore a patient’s intrinsic motivation to change health behaviors [81]. Inherent to MI is the belief that motivation for change is malleable and that it can be transformed in the context of the patient-physician relationship [81]. MI is a patient-centered method designed to empower a patient’s ability and responsibility to make health-related decisions, with the physician supporting the patient’s autonomy in the process [82]. Recent meta-analyses and systematic reviews [83–87] showed that MI interventions improve self-care behaviors and glycemic control in the short-term; long-term effects of MI on self-care and glycemia remain inconclusive. More high-quality research is needed to evaluate the MI training content of these interventions in order to determine its long-term effectiveness and replicate outcomes in various healthcare settings [87].
Other studies not included in the meta-analyses and reviews found MI interventions improved self-care behaviors [88–90], glycemic control [90,91], and quality of life [91]. A qualitative study exploring diabetes patients’ experiences with MI and self-care behaviors revealed that patients’ appreciate when providers initiate discussions that result in new ways of thinking about self-care and promote a sense of well-being in patients [92]. New research utilizing patient navigators to connect diabetes patients’ to their primary care providers showed MI techniques improved patient self-efficacy and glycemic control [93]. Another study, an internet-based incentives study, found that the application of a brief MI interviewing session improved blood glucose monitoring in adolescents with type 1 diabetes [94]. Thus, creative strategies that employ MI techniques in collaboration with other members of the health care team (ie, patient navigation [93], telehealth [89], health coaching [95], internet-based tools [94]) hold promise for improving self-care and patient-physician communication. Increased collaboration with members of the health care team (eg, certified diabetes educators, nurses, dietitians, pharmacists, exercise physiologists), community health workers [96,97] and peer mentors [98,99] may help reinforce messages, promote shared decision-making, improve diabetes outcomes, increase patient satisfaction, and reduce medical costs [100].
Few other interventions have directly addressed physician-patient diabetes self-care communication. One older study examined the effectiveness of an intervention designed to increase of diabetes patients’ involvement in medical decision-making [16]. Patients randomized to the intervention arm participated in a 20-minute session prior to meeting with their physician, in which researchers reviewed their medical chart and used systematic prompts to encourage patients to negotiate medical decisions with their physician. Patients in the control arm received standard educational materials in a session of equal length. Patients in the intervention arm improved glycemia and elicited twice the amount of medical information from their physician compared to controls [16]. These findings suggest that brief interventions prior to medical appointments can improve patient communication, self-care behavior, and in turn, diabetes outcomes [16].
A recent study evaluated the effectiveness of a training program in communication skills for pediatric diabetes care providers in the UK [101, 102]. In this cluster randomized controlled trial, pediatric providers allocated to the Talking Diabetes intervention participated in web-based material and face-to-face seminars designed to prepare providers for constructive self-care conversations with patients as well as skills for promoting behavior change. The psychoeducational training emphasized shared decision-making and utilized motivational interviewing techniques [101]. Twenty-six centers and 693 young people with type 1 diabetes participated in the study [102]. At 12-month follow-up, the Talking Diabetes intervention did not demonstrate improvements in glycemic control. Further, the intervention had a negative effect on patients’ quality of life but a short-term improvement in coping [102]. Interestingly, parents of patients in the intervention arm reported greater continuity of care, which suggests that parents benefited more from the intervention than their children. Future communication interventions targeting the pediatric population should provide ongoing support to children of physicians exposed to interventions such as Talking Diabetes [102].
Currently, 3 ongoing studies aim to improve self-care and clinical outcomes via physician-patient communication interventions. A study by Ricci-Cabello and colleagues [103] aims to improve diabetes self-care by enhancing patient-physician communication in an underserved community of adults with uncontrolled type 2 diabetes. In this 3-arm randomized controlled trial, patients allocated to groups A and B received communication skills training and graphic feedback about glycosylated hemoglobin A1c levels; patients in group C received usual care. Patients in group B also received telephone reinforcement [103]. The second study, by Billimek and colleagues, aims to improve physician-patient communication about medication regimens via diabetes coaching [104]. In this intervention, 190 Mexican-American adult patients with type 2 diabetes were randomly assigned to complete a Coached Care visit with trained community health workers or a Coached Care visit plus the EMPATHy software toolkit, a computer-based activity with strategies and resources to overcome self-care barriers. The primary endpoints are (1) the development of care plan that addresses everyday barriers to medication adherence and (2) completion of a concrete behavioral goal [104]. Finally, the third study, by Grant and colleagues, aims to improve physician-patient communication via a pre-visit prioritization of diabetes concerns. In this controlled, cluster-randomized, multisite trial, primary care physicians were randomized to the Pre-Visit Prioritization for Complex Patients with Diabetes or the control group [105]. The Pre-Visit Prioritization IT-tool is designed to help patients identify one or two concerns prior to a medical visit and then send these priorities to the primary care physician via an electronic health record. The overall goal of the intervention is to improve communication of self-care concerns during a medical visit [105]. Findings from these 3 interventions are forthcoming; findings may provide evidence for validated interventions that improve physician-patient self-care communication in diabetes.
Techniques to Improve Self-Care Communication
Incorporating communication skills in continuing medical education and diabetes education may improve self-care communication in the physician-patient relationship. Educational programs that teach physicians how to provide consistent messages, repeat information, reinforce and offer feedback regarding specific self-care behaviors, and problem-solve self-care challenges may improve patients’ willingness to discuss self-care [14,106]. Most patients will remember only a small portion of the information given to them during medical visit. Studies that compare how much information patients retain versus how much information physicians provide show that patients forget 31% to 71% of information [107]. Therefore, physicians need techniques that promote open self-care communication during a visit. The following techniques can help physicians improve self-care communication [108]:
- Discuss the most important self-care information first; patients tend to remember the information that is presented first.
- Use the phrase “This is very important…” when discussing key points because patients will remember things that are perceived as important.
- Deliver simple, clear, and concrete instructions; patients are more likely to forget complex or confusing instructions. For example, “Check your blood glucose every morning within five minutes of waking up and before you eat breakfast” is more specific and easier to follow than “Check your blood glucose”.
- Ask open-ended questions to allow patients to verbalize feelings or concerns about their diabetes self-care.
- Employ MI techniques to help patients who are struggling to initiate and adhere to self-care behaviors. MI tools, such as the Readiness Ruler, Self-Evaluation Rulers, Decisional Balance Matrix, and Health Behavior Menu (Figure), may help patients and physicians discuss self-care behaviors during a medical visit [109].
– Express empathy by reflective listening and asking patients for permission before offering information or advice about diabetes self-care.
– Roll with resistance by engaging the patient in the process of problem solving rather than opposing a patient’s resistance to change behaviors.
– Develop discrepancy by helping the patient recognize that there is an inconsistency between his/her behavior and personal goals.
– Support self-efficacy by empowering the patient to believe that he/she can change behaviors.
6. Demonstrate active listening skills by reflecting and summarizing the patient’s statements. Reflecting and summarizing show the patient that the physician has been listening to concerns and understands what the patient is saying. This is also an opportunity to correct any miscommunications from the visit.
7. Write down instructions or provide handouts to the patient to help reinforce learning and information retention.
8. Ask patients to write a list of questions a few days prior to the medical appointment and bring it with them. Patients are more likely to remember information about issues they have previously considered that directly relate to them.
9. Consider collaborating with community health workers, patient navigators, peer mentors, and other members of the healthcare team to improve communication, diabetes outcomes, and patient satisfaction.
Summary
Physician-patient self-care communication is essential to achieving optimal diabetes outcomes [15,22,33,110] Patients’ ability to inform physicians about their self-care challenges [14], and physicians’ ability to respond to patients’ self-care reports directly and in non-accusatory language, are vital factors in effective diabetes care [45]. Interventions and education that promote open and honest conversations are particularly important given patients’ well-documented struggles achieving self-care and glycemic goals [111] and physicians’ feelings of inadequacy, frustration, and fatigue when they are not making an impact on patients’ outcomes [48,112]. More research is needed to determine the best strategies to improve self-care communication in the physician-patient relationship.
Corresponding author: Elizabeth A. Beverly, PhD, Department of Family Medicine, Ohio University Heritage College of Osteopathic Medicine, Athens, OH 45701, beverle1@ohio.edu.
Financial disclosures: None.
Author contributions: drafting of article, EAB, MFW, ABC, KEP, NNI; critical revision of the article, EAB, MFW, ABC, KEP, NNI.
Abstract
- Objective: To summarize the current literature, research findings, and interventions for self-care communication in the physician-patient relationship.
- Methods: Literature review.
- Results: Diabetes management requires patients to follow complex self-care recommendations for nutrition, physical activity, blood glucose monitoring, and medication. Adherence to these recommendations improves glycemic control and mitigates the risk of diabetes complications; however, many patients struggle to follow these behaviors in everyday life. In the physician-patient relationship, self-care communication is largely influenced by interpersonal trust. Physicians need to incorporate interpersonal and relational skills to establish a trusting relationship. Physician-level barriers to self-care communication include lack of time, lack of collaboration and teamwork among health care providers, lack of patients’ access to resources, and lack of psychosocial support for diabetes patients. Among patients, psychosocial barriers and health literacy may affect willingness to discuss self-care. Motivational interviewing techniques may be helpful for improving communication around patient self-management and promotion of healthy behaviors.
- Conclusion: Physicians can assist patients with their diabetes self-care by discussing self-care challenges during medical visits.
Diabetes is one of the most significant and growing chronic health problems in the world, affecting approximately 415 million people [1]. Diabetes is marked by the body’s inability to make insulin as well as the body’s inability to effectively use the insulin it produces [2]. Diagnosis of diabetes has increased sharply in recent decades and is expected to increase even more, with the largest increases in middle- and low-income countries [3]. Diabetes is a leading cause of blindness, kidney failure, myocardial infarction, stroke, and amputation [3], and in 2015 it accounted for 5 million deaths worldwide [1]. Further, diabetes’s costs to society represent 12% ($673 billion) of global health expenditures [1]. By 2040, models predict that 642 million people will be diagnosed with diabetes and costs will continue to grow as the population ages [1]. Thus, prevention of diabetes is the ultimate goal; however, more effective management for individuals already diagnosed with diabetes is critical to reduce the risk of complications and the economic burden of the disease.
Diabetes management requires patients to perform complex self-care regimens, including weight reduction, frequent blood glucose monitoring, taking oral and/or insulin medications, engaging in physical activity, adhering to diabetes nutrition guidelines, and attending clinic appointments [4–9]. These self-care behaviors are critically linked to improved glycemic control, however, integrating them into one’s daily life can be challenging [10–12]. Recent National Health and Nutrition Examination Survey (NHANES) data show that approximately half of adults with diabetes are not meeting recommended goals for diabetes care [13]. Physicians can assist patients with their diabetes self-care by scheduling frequent follow-up visits and discussing self-care challenges with their patients [14].
In this review, we discuss the current literature on physician-patient communication and diabetes self-care. First, we discuss the qualities of an effective physician-patient relationship followed by the importance of self-care communication in diabetes care. Next, we discuss barriers and facilitators to self-care communication. Finally, we review interventions for improving physician-patient communication in diabetes self-care.
Qualities of an Effective Physician-Patient Relationship
Successful diabetes care requires teamwork between physicians and patients [15]. Two components of successful teamwork are physician-patient communication and shared decision-making, both of which have been shown to improve patient satisfaction, adherence to treatment plans and health outcomes [16–23]. In shared decision-making, the physician and patient share medical information [24–26]. Specifically, the physician presents different treatment options to the patient and describes the risks and benefits of each option. Then the patient expresses his or her preferences for treatment to ensure that the care provided aligns with the patient’s values and needs [27]. Thus, shared decision-making in the treatment relationship is predicated on effective communication between the physician and patient [19].
Effective physician-patient communication is supported by continuous care [19,28], a secure attachment style [29, 30], shared goals [19], a mutual understanding of respective roles and tasks [15,31–33], and a bond characterized by liking, confidence, and trust [19,28,31]. Trust is paramount in physician-patient communication. Interpersonal trust and social trust are the 2 predominant types [34]. Interpersonal trust refers to the relationship the patient has with the physician, specifically the confidence the patient has in the physician as well as the responsibility, competence, compassion, and regard the physician has for the patient’s welfare [34–36]. For patients and physicians, interpersonal trust is developed over time with repeated interactions [34–36]. On the other hand, social trust refers to the beliefs of honesty, integrity, and reliability in others [36]. Social trust is influenced by social constructs, including the media and institutions of higher education [36].
In the physician-patient relationship, self-care communication is largely influenced by interpersonal trust. A patient’s trust can be acquired through multiple medical appointments with the physician. Further, how the patient is treated during these appointments as well as how much time and attention the physician invests in the patient’s care influences the level of interpersonal trust. A high level of trust in the relationship can lead to in improvements in adherence to self-care, continuity of care, physician-patient communication, and overall quality of the physician-patient relationship [37–39].
In the diabetes physician-patient relationship, minimal research has explored how trust in one’s physician impacts self-care communication. In a study by Beverly and colleagues, diabetes patients emphasized the importance of a trusting physician-patient relationship for diabetes care [27]. Another study by Ritholz and colleagues found that physicians and patients both stress the importance of developing trust to facilitate self-care communication [40]. Specifically, trust as well as acceptance from the physician contributes to open and honest self-care communication in the physician-patient diabetes relationship[40]. Additional research is needed to determine whether a high level of physician-patient trust is associated with increased self-care behaviors and improved diabetes outcomes over time.
Importance of Diabetes Self-Care Communication
Diabetes self-care communication in the physician-patient relationship increases patient satisfaction, improves adherence to treatment regimens, and leads to better clinical outcomes [22,41–43]. For physicians, effective self-care communication requires the performance of specific communication tasks and behaviors, including collecting a medical history, explaining a diagnosis and prognosis, and providing clear and concise therapeutic instructions [44]. In addition, physicians must incorporate interpersonal and relational skills to establish a trusting relationship [44,45]. Both physicians and patients agree that a trusting treatment relationship is a requirement for open and honest self-care communication [45]. For patients, effective communication necessitates the disclosure of self-care successes and failures [46]. Diabetes patients face challenging self-care regimens, and these challenges can interfere with glycemic control and increase the risk for diabetes complications [47,48]. For this reason, patients must feel comfortable discussing their self-are challenges so that their physician can individualize treatment prescriptions and recommendations, thereby increasing the likelihood of treatment success.
Barriers to Self-Care Communication
Physician-patient self-care communication is essential to improving patient adherence [29,49] yet numerous barriers exist that undermine effective physician-patient self-care communication. From the physician perspective, the most commonly cited barrier to self-care communication is time [50]. A recent study of family medicine practices found that the time physicians spent discussing self-care with their patients varied from 1 to 17 minutes, suggesting that time is a major barrier to self-care communication [51]. Other barriers include lack of collaboration and teamwork among health care providers, lack of patients’ access to resources, and lack of psychosocial support for patients with diabetes [50]. Relatedly, Beverly and colleagues [52] found that physicians often feel inadequately trained to address diabetes patients’ psychosocial issues and this perceived lack of expertise may contribute to physicians feeling overwhelmed and frustrated within the physician-patient relationship, which may hinder open self-care communication.
For patients, barriers tend to differ from those perceived by physicians. A qualitative study using semi-structured interviews with patients and clinicians, and direct observation of clinical encounters at an inner-city family practice training site, revealed different perceptions of the term “control” between physicians and patients. In practice, physicians used the term “control” to focus on the management of blood glucose levels rather than trying to understand the patients’ understanding of diabetes and subsequent treatment goals. Differing viewpoints contributed to frustration and hindered effective communication [53]. In another qualitative study with physicians and patients, both noted that patients were reluctant to discuss self-care for fear being judged or shamed about food intake and weight [45]. This finding was supported in a quantitative follow-up study assessing patient reluctance to discuss self-care. Thirty percent of surveyed patients reported reluctance to discussing self-care with their physicians for fear of being judged, not wanting to disappoint their doctors, guilt, and shame [14]. Interestingly, patients reporting elevated depressive symptoms were more likely to be reluctant to discuss their self-care [14]. Cognitive behavioral changes (eg, cognitive distortions, avoidance behavior, attention deficits) associated with major depression and depressive symptoms may impair patients’ ability to recall self-care information. Also, patients reporting more depressive symptoms may be more socially withdrawn during a medical appointment, and thus less willing to communicate with their physician about self-care.
Other studies found that psychosocial factors such as diabetes distress [54,55] and pessimistic attitudes [56–59], cultural differences [60–66], lack of family and social support [60,67–70], lack of readiness to change behavior [71], introversion and social isolation [72,73], hypo-glycemia fear [74,75] and ineffectual coping styles [76,77] interfere with self-care and glycemic control. Further, low health literacy is associated with difficulty adhering to self-care, particular medication regimens, and negative health outcomes [78].
In summary psychosocial barriers and health literacy may affect a patients’ willingness to discuss self-care during a medical visit. Therefore, routine assessment of psychosocial factors and health literacy may be necessary to address a patient’s barriers to self-care as well as to promote open and honest self-care communication. Interventions and evidenced-based approaches that address psychosocial factors, health literacy, and physician-patient self-care communication are needed.
Facilitators to Self-Care Communication
Despite numerous barriers to self-care communication, several factors promote self-care communication in the physician-patient relationship. For example, direct and non-accusatory communication from physicians as well as providing patients with hope for living with diabetes both support physician-patient self-care communication [45]. A recent systematic review by Sohal and colleagues [79] found that trust in physicians, the use of culturally appropriate exercise and dietary advice, and increasing family involvement improved physician-patient communication and diabetes self-care [79]. Lastly, a study by Schillinger and colleagues [80] found that physician assessment of patient recall and comprehension of new concepts during medical visits improved diabetes outcomes [80].
Patient-Physician Self-Care Communication Interventions
One of the more successful interventions for improving diabetes self-care and patient-physician communication is motivational interviewing (MI). MI is a non-judgmental communication style designed to explore a patient’s intrinsic motivation to change health behaviors [81]. Inherent to MI is the belief that motivation for change is malleable and that it can be transformed in the context of the patient-physician relationship [81]. MI is a patient-centered method designed to empower a patient’s ability and responsibility to make health-related decisions, with the physician supporting the patient’s autonomy in the process [82]. Recent meta-analyses and systematic reviews [83–87] showed that MI interventions improve self-care behaviors and glycemic control in the short-term; long-term effects of MI on self-care and glycemia remain inconclusive. More high-quality research is needed to evaluate the MI training content of these interventions in order to determine its long-term effectiveness and replicate outcomes in various healthcare settings [87].
Other studies not included in the meta-analyses and reviews found MI interventions improved self-care behaviors [88–90], glycemic control [90,91], and quality of life [91]. A qualitative study exploring diabetes patients’ experiences with MI and self-care behaviors revealed that patients’ appreciate when providers initiate discussions that result in new ways of thinking about self-care and promote a sense of well-being in patients [92]. New research utilizing patient navigators to connect diabetes patients’ to their primary care providers showed MI techniques improved patient self-efficacy and glycemic control [93]. Another study, an internet-based incentives study, found that the application of a brief MI interviewing session improved blood glucose monitoring in adolescents with type 1 diabetes [94]. Thus, creative strategies that employ MI techniques in collaboration with other members of the health care team (ie, patient navigation [93], telehealth [89], health coaching [95], internet-based tools [94]) hold promise for improving self-care and patient-physician communication. Increased collaboration with members of the health care team (eg, certified diabetes educators, nurses, dietitians, pharmacists, exercise physiologists), community health workers [96,97] and peer mentors [98,99] may help reinforce messages, promote shared decision-making, improve diabetes outcomes, increase patient satisfaction, and reduce medical costs [100].
Few other interventions have directly addressed physician-patient diabetes self-care communication. One older study examined the effectiveness of an intervention designed to increase of diabetes patients’ involvement in medical decision-making [16]. Patients randomized to the intervention arm participated in a 20-minute session prior to meeting with their physician, in which researchers reviewed their medical chart and used systematic prompts to encourage patients to negotiate medical decisions with their physician. Patients in the control arm received standard educational materials in a session of equal length. Patients in the intervention arm improved glycemia and elicited twice the amount of medical information from their physician compared to controls [16]. These findings suggest that brief interventions prior to medical appointments can improve patient communication, self-care behavior, and in turn, diabetes outcomes [16].
A recent study evaluated the effectiveness of a training program in communication skills for pediatric diabetes care providers in the UK [101, 102]. In this cluster randomized controlled trial, pediatric providers allocated to the Talking Diabetes intervention participated in web-based material and face-to-face seminars designed to prepare providers for constructive self-care conversations with patients as well as skills for promoting behavior change. The psychoeducational training emphasized shared decision-making and utilized motivational interviewing techniques [101]. Twenty-six centers and 693 young people with type 1 diabetes participated in the study [102]. At 12-month follow-up, the Talking Diabetes intervention did not demonstrate improvements in glycemic control. Further, the intervention had a negative effect on patients’ quality of life but a short-term improvement in coping [102]. Interestingly, parents of patients in the intervention arm reported greater continuity of care, which suggests that parents benefited more from the intervention than their children. Future communication interventions targeting the pediatric population should provide ongoing support to children of physicians exposed to interventions such as Talking Diabetes [102].
Currently, 3 ongoing studies aim to improve self-care and clinical outcomes via physician-patient communication interventions. A study by Ricci-Cabello and colleagues [103] aims to improve diabetes self-care by enhancing patient-physician communication in an underserved community of adults with uncontrolled type 2 diabetes. In this 3-arm randomized controlled trial, patients allocated to groups A and B received communication skills training and graphic feedback about glycosylated hemoglobin A1c levels; patients in group C received usual care. Patients in group B also received telephone reinforcement [103]. The second study, by Billimek and colleagues, aims to improve physician-patient communication about medication regimens via diabetes coaching [104]. In this intervention, 190 Mexican-American adult patients with type 2 diabetes were randomly assigned to complete a Coached Care visit with trained community health workers or a Coached Care visit plus the EMPATHy software toolkit, a computer-based activity with strategies and resources to overcome self-care barriers. The primary endpoints are (1) the development of care plan that addresses everyday barriers to medication adherence and (2) completion of a concrete behavioral goal [104]. Finally, the third study, by Grant and colleagues, aims to improve physician-patient communication via a pre-visit prioritization of diabetes concerns. In this controlled, cluster-randomized, multisite trial, primary care physicians were randomized to the Pre-Visit Prioritization for Complex Patients with Diabetes or the control group [105]. The Pre-Visit Prioritization IT-tool is designed to help patients identify one or two concerns prior to a medical visit and then send these priorities to the primary care physician via an electronic health record. The overall goal of the intervention is to improve communication of self-care concerns during a medical visit [105]. Findings from these 3 interventions are forthcoming; findings may provide evidence for validated interventions that improve physician-patient self-care communication in diabetes.
Techniques to Improve Self-Care Communication
Incorporating communication skills in continuing medical education and diabetes education may improve self-care communication in the physician-patient relationship. Educational programs that teach physicians how to provide consistent messages, repeat information, reinforce and offer feedback regarding specific self-care behaviors, and problem-solve self-care challenges may improve patients’ willingness to discuss self-care [14,106]. Most patients will remember only a small portion of the information given to them during medical visit. Studies that compare how much information patients retain versus how much information physicians provide show that patients forget 31% to 71% of information [107]. Therefore, physicians need techniques that promote open self-care communication during a visit. The following techniques can help physicians improve self-care communication [108]:
- Discuss the most important self-care information first; patients tend to remember the information that is presented first.
- Use the phrase “This is very important…” when discussing key points because patients will remember things that are perceived as important.
- Deliver simple, clear, and concrete instructions; patients are more likely to forget complex or confusing instructions. For example, “Check your blood glucose every morning within five minutes of waking up and before you eat breakfast” is more specific and easier to follow than “Check your blood glucose”.
- Ask open-ended questions to allow patients to verbalize feelings or concerns about their diabetes self-care.
- Employ MI techniques to help patients who are struggling to initiate and adhere to self-care behaviors. MI tools, such as the Readiness Ruler, Self-Evaluation Rulers, Decisional Balance Matrix, and Health Behavior Menu (Figure), may help patients and physicians discuss self-care behaviors during a medical visit [109].
– Express empathy by reflective listening and asking patients for permission before offering information or advice about diabetes self-care.
– Roll with resistance by engaging the patient in the process of problem solving rather than opposing a patient’s resistance to change behaviors.
– Develop discrepancy by helping the patient recognize that there is an inconsistency between his/her behavior and personal goals.
– Support self-efficacy by empowering the patient to believe that he/she can change behaviors.
6. Demonstrate active listening skills by reflecting and summarizing the patient’s statements. Reflecting and summarizing show the patient that the physician has been listening to concerns and understands what the patient is saying. This is also an opportunity to correct any miscommunications from the visit.
7. Write down instructions or provide handouts to the patient to help reinforce learning and information retention.
8. Ask patients to write a list of questions a few days prior to the medical appointment and bring it with them. Patients are more likely to remember information about issues they have previously considered that directly relate to them.
9. Consider collaborating with community health workers, patient navigators, peer mentors, and other members of the healthcare team to improve communication, diabetes outcomes, and patient satisfaction.
Summary
Physician-patient self-care communication is essential to achieving optimal diabetes outcomes [15,22,33,110] Patients’ ability to inform physicians about their self-care challenges [14], and physicians’ ability to respond to patients’ self-care reports directly and in non-accusatory language, are vital factors in effective diabetes care [45]. Interventions and education that promote open and honest conversations are particularly important given patients’ well-documented struggles achieving self-care and glycemic goals [111] and physicians’ feelings of inadequacy, frustration, and fatigue when they are not making an impact on patients’ outcomes [48,112]. More research is needed to determine the best strategies to improve self-care communication in the physician-patient relationship.
Corresponding author: Elizabeth A. Beverly, PhD, Department of Family Medicine, Ohio University Heritage College of Osteopathic Medicine, Athens, OH 45701, beverle1@ohio.edu.
Financial disclosures: None.
Author contributions: drafting of article, EAB, MFW, ABC, KEP, NNI; critical revision of the article, EAB, MFW, ABC, KEP, NNI.
1. Anderson E, Kian EM. Examining media contestation of masculinity and head trauma in the National Football League. J Men Masculinities 2011;1–22.
2. CDC. National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011.
3. Bandura A. Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice Hall; 1986.
4. Jacobson AM, Adler AG, Derby L, et al. Clinic attendance and glycemic control. Study of contrasting groups of patients with IDDM. Diabetes Care 1991;14:599–601.
5. Dyer PH, Lloyd CE, Lancashire RJ, et al. Factors associated with clinic non-attendance in adults with type 1 diabetes mellitus. Diab Med 1998;15:339–43.
6. Conn VS, Hafdahl AR, Mehr DR, et al. Metabolic effects of interventions to increase exercise in adults with type 2 diabetes. Diabetologia 2007;50:913–21.
7. Maiorana A, O’Driscoll G, Goodman C, et al. Combined aerobic and resistance exercise improves glycemic control and fitness in type 2 diabetes. Diab Res Clin Pract 2002;56:115–23.
8. Pi-Sunyer FX, Maggio CA, McCarron DA, et al. Multicenter randomized trial of a comprehensive prepared meal program in type 2 diabetes. Diabetes Care 1999;22:191–7.
9. Delahanty LM, Halford BN. The role of diet behaviors in achieving improved glycemic control in intensively treated patients in the Diabetes Control and Complications Trial. Diabetes Care 1993;16:1453–8.
10. Gafarian CT, Heiby EM, Blair P, Singer F. The Diabetes Time Management Questionnaire. Diabetes Educ 1999;25:585–92.
11. Wdowik MJ, Kendall PA, Harris MA. College students with diabetes: using focus groups and interviews to determine psychosocial issues and barriers to control. Diabetes Educ 1997;23:558–62.
12. Rubin RR, Peyrot M. Psychological issues and treatment for people with diabetes. J Clin Psychol 2001;57:457–78.
13. Ali MK, Bullard KM, Gregg EW. Achievement of goals in U.S. Diabetes Care, 1999-2010. N Engl J Med 2013;369:287–8.
14. Beverly EA, Ganda OP, Ritholz MD, et al. Look who’s (not) talking: diabetic patients’ willingness to discuss self-care with physicians. Diabetes Care 2012;35:1466–72.
15. Heisler M, Vijan S, Anderson RM, et al. When do patients and their physicians agree on diabetes treatment goals and strategies, and what difference does it make? J Gen Intern Med 2003;18:893–902.
16. Greenfield S, Kaplan SH, Ware JE Jr, et al. Patients’ participation in medical care: effects on blood sugar control and quality of life in diabetes. J Gen Intern Med 1988;3:448–57.
17. Greenfield S, Kaplan S, Ware JE Jr. Expanding patient involvement in care. Effects on patient outcomes. Ann Intern Med 1985;102:520–8.
18. Anderson RM, Funnell MM, Butler PM, et al. Patient empowerment. Results of a randomized controlled trial. Diabetes Care 1995;18:943–9.
19. Von Korff M, Gruman J, Schaefer J, et al. Collaborative management of chronic illness. Ann Intern Med 1997;127:1097–102.
20. Campbell SM, Hann M, Hacker J, et al. Identifying predictors of high quality care in English general practice: observational study. BMJ 2001;323:784–7.
21. Bower P, Campbell S, Bojke C, Sibbald B. Team structure, team climate and the quality of care in primary care: an observational study. Qual Saf Health Care 2003;12:273–9.
22. Piette JD, Schillinger D, Potter MB, Heisler M. Dimensions of patient-provider communication and diabetes self-care in an ethnically diverse population. J Gen Intern Med 2003;18:624-33.
23. Kerr EA, Smith DM, Kaplan SH, Hayward RA. The association between three different measures of health status and satisfaction among patients with diabetes. Med Care Res Rev 2003;60:158-77.
24. Oshima Lee E, Emanuel EJ. Shared decision making to improve care and reduce costs. N Engl J Med 2013;368:6-8.
25. Barry MJ, Edgman-Levitan S. Shared decision making--pinnacle of patient-centered care. N Engl J Med 2012;366:780–1.
26. Truog RD. Patients and doctors--evolution of a relationship. N Engl J Med 2012;366:581–5.
27. Beverly EA, Wray LA, LaCoe CL, Gabbay R. Listening to older adults’ values and preferences for type 2 diabetes care: a qualitative study. Diabetes Spectrum 2014;27:44–9.
28. Bordin ES. The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy 1979;26:252–60.
29. Ciechanowski PS, Katon WJ, Russo JE, Walker EA. The patient-provider relationship: attachment theory and adherence to treatment in diabetes. Am J Psychiatry 2001;158:29–35.
30. Ciechanowski P, Russo J, Katon W, et al. Influence of patient attachment style on self-care and outcomes in diabetes. Psychosom Med 2004;66:720–8.
31. Jahng KH, Martin LR, Golin CE, DiMatteo MR. Preferences for medical collaboration: patient-physician congruence and patient outcomes. Patient Educ Couns 2005;57:308–14.
32. Street RL Jr, Krupat E, Bell RA, et al. Beliefs about control in the physician-patient relationship: effect on communication in medical encounters. J Gen Intern Med 2003;18:609–16.
33. Heisler M, Bouknight RR, Hayward RA, et al. The relative importance of physician communication, participatory decision making, and patient understanding in diabetes self-management. J Gen Intern Med 2002;17:243–52.
34. Mechanic D. Changing medical organization and the erosion of trust. Milbank Q 1996;74:171–89.
35. Mechanic D, Schlesinger M. The impact of managed care on patients’ trust in medical care and their physicians. JAMA 1996;275:1693–7.
36. Pearson SD, Raeke LH. Patients’ trust in physicians: many theories, few measures, and little data. J Gen Intern Med 2000;15:509–13.
37. Jones DE, Carson KA, Bleich SN, Cooper LA. Patient trust in physicians and adoption of lifestyle behaviors to control high blood pressure. Patient Educ Couns 2012;89:57–62.
38. Mostashari F, Riley E, Selwyn PA, Altice FL. Acceptance and adherence with antiretroviral therapy among HIV-infected women in a correctional facility. J Acquired Immun Def Syndr Hum Retrovir 1998;18:341–8.
39. Cooper-Patrick L, Gallo JJ, Gonzales JJ, et al. Race, gender, and partnership in the patient-physician relationship. JAMA 1999;282:583–9.
40. Ritholz MD, Beverly EA, Brooks KM, et al. Barriers and facilitators to self-care communication during medical appointments in the United States for adults with type 2 diabetes. Chronic Illn 2014;10:303–13.
41. Aikens JE, Bingham R, Piette JD. Patient-provider communication and self-care behavior among type 2 diabetes patients. Diabetes Educ 2005;31:681–90.
42. Bundesmann R, Kaplowitz SA. Provider communication and patient participation in diabetes self-care. Patient Educ Couns 2011;85:143–7.
43. Heisler M, Cole I, Weir D, et al. Does physician communication influence older patients’ diabetes self-management and glycemic control? Results from the Health and Retirement Study (HRS). J Gerontol A Biol Sci Med Sci 2007;62:1435–42.
44. Duffy FD, Gordon GH, Whelan G, et al. Assessing competence in communication and interpersonal skills: the Kalamazoo II report. Acad Med 2004;79:495–507.
45. Ritholz MD, Beverly EA, Brooks KM, et al. Barriers and facilitators to self-care communication during medical appointments in the United States for adults with type 2 diabetes. Chronic Illn 2014;10:303–13.
46. Ciechanowski P, Katon WJ. The interpersonal experience of health care through the eyes of patients with diabetes. Soc Sci Med 2006;63:3067–79.
47. Diabetes Control and Complications Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329:977–86.
48. Peyrot M, Rubin RR, Lauritzen T, et al. Psychosocial problems and barriers to improved diabetes management: results of the Cross-National Diabetes Attitudes, Wishes and Needs (DAWN) Study. Diab Med 2005;22:1379–85.
49. DiMatteo MR, Linn LS, Chang BL, Cope DW. Affect and neutrality in physician behavior: a study of patients’ values and satisfaction. J Behav Med 1985;8:397–409.
50. Stuckey HL, Vallis M, Kovacs Burns K, et al. “I do my best to listen to patients”: qualitative insights into DAWN2 (Diabetes Psychosocial Care From the Perspective of Health Care Professionals in the Second Diabetes Attitudes, Wishes and Needs Study). Clin Ther 2015;37:1986–98.
51. Kruse RL, Olsberg JE, Oliver DP, et al. Patient-provider communication about diabetes self-care activities. Fam Med 2013;45:319–22.
52. Beverly EA, Hultgren BA, Brooks KM, et al. Understanding physicians’ challenges when treating type 2 diabetic patients’ social and emotional difficulties: a qualitative study. Diabetes Care 2011;34:1086–8.
53. Freeman J, Loewe R. Barriers to communication about diabetes mellitus. Patients’ and physicians’ different view of the disease. J Fam Pract 2000;49:507–12.
54. Gonzalez JS, Delahanty LM, Safren SA, et al. Differentiating symptoms of depression from diabetes-specific distress: relationships with self-care in type 2 diabetes. Diabetologia 2008;51:1822–5.
55. Fisher L, Hessler DM, Polonsky WH, Mullan J. When is diabetes distress clinically meaningful?: establishing cut points for the Diabetes Distress Scale. Diabetes Care 2012;35:259–64.
56. Polonsky WH, Anderson BJ, Lohrer PA, et al. Assessment of diabetes-related distress. Diabetes Care 1995;18:754–60.
57. Welch G, Weinger K, Anderson B, Polonsky WH. Responsiveness of the Problem Areas In Diabetes (PAID) questionnaire. Diabetic Med 2003;20:69–72.
58. Weinger K, Kinsley BT, Bajaj M, et al. Diabetes-related emotional distress: A barrier to improving glycemic control during intensive diabetes treatment. Abstract. Diabetes 1997;46:Supp1:268A.
59. Weinger K, Jacobson AM. Psychosocial and quality of life correlates of glycemic control during intensive treatment of type 1 diabetes. Patient Educ Couns 2001;42:123–31.
60. Fisher L, Chesla CA, Skaff MM, et al. The family and disease management in Hispanic and European-American patients with type 2 diabetes. Diabetes Care 2000;23:267–72.
61. Wen LK, Parchman ML, Shepherd MD. Family support and diet barriers among older Hispanic adults with type 2 diabetes. Fam Med 2004;36:423–30.
62. Chesla CA, Fisher L, Mullan JT, et al. Family and disease management in African-American patients with type 2 diabetes. Diabetes Care 2004;27:2850–5.
63. Brown SA, Harrist RB, Villagomez ET, et al. Gender and treatment differences in knowledge, health beliefs, and metabolic control in Mexican Americans with type 2 diabetes. Diabetes Educ 2000;26:425–38.
64. Fisher L, Chesla CA, Chun KM, et al. Patient-appraised couple emotion management and disease management among Chinese American patients with type 2 diabetes. J Fam Psychol 2004;18:302–10.
65. Akimoto M, Fukunishi I, Kanno K, et al. Psychosocial predictors of relapse among diabetes patients: a 2-year follow-up after inpatient diabetes education. Psychosomatics 2004;45:343–9.
66. Samuel-Hodge CD, Headen SW, Skelly AH, et al. Influences on day-to-day self-management of type 2 diabetes among African-American women: spirituality, the multi-caregiver role, and other social context factors. Diabetes Care 2000;23:928–33.
67. Wing RR, Marcus MD, Epstein LH, Jawad A. A “family-based” approach to the treatment of obese type II diabetic patients. J Consult Clin Psychol 1991;59:156–62.
68. Trief PM, Ploutz-Snyder R, Britton KD, Weinstock RS. The relationship between marital quality and adherence to the diabetes care regimen. Ann Behav Med 2004;27:148–54.
69. Gleeson-Kreig J, Bernal H, Woolley S. The role of social support in the self-management of diabetes mellitus among a Hispanic population. Pub Health Nurs 2002;19:215–22.
70. Wen LK, Shepherd MD, Parchman ML. Family support, diet, and exercise among older Mexican Americans with type 2 diabetes. Diabetes Educ 2004;30:980–93.
71. Ruggiero L. Helping people with diabetes change behavior: from theory to practice. Diab Spectrum 2000;13:125–32.
72. Orr DP, Golden MP, Myers G, Marrero DG. Characteristics of adolescents with poorly controlled diabetes referred to a tertiary care center. Diabetes Care 1983;6:170–5.
73. Lane JD, Stabler B, Ross SL, et al. Psychological predictors of glucose control in patients with IDDM. Diabetes Care 1988;11:798–800.
74. Irvine AA, Cox D, Gonder-Frederick L. Fear of hypoglycemia: relationship to physical and psychological symptoms in patients with insulin-dependent diabetes mellitus. Health Psychology 1992;11:135–8.
75. Irvine A, Cox D, Gonder-Frederick L. The fear of hypoglycemia scale. In: Bradley C, editor. Handbook of psychology and diabetes. Harwood Academic; 1994.
76. Peyrot MF, McMurry JF Jr. Stress buffering and glycemic control. The role of coping styles. Diabetes Care 1992;15:842–6.
77. Peyrot M, McMurry JF Jr, Kruger DF. A biopsychosocial model of glycemic control in diabetes: stress, coping and regimen adherence. J Health Soc Behav 1999;40:141–58.
78. Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med 2011;155:97–107.
79. Sohal S, Sohal P, King-Shier KM, Khan NA. Barriers and facilitators for type-2 diabetes management in South Asians: a systematic review. PloS One 2015:1–15.
80. Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med 2003;163:83–90.
81. Miller WR, Rollnick S. Motivational interviewing: preparing people for change. New York: Guilford Press; 2002.
82. Powell PW, Corathers SD, Raymond J, Streisand R. New approaches to providing individualized diabetes care in the 21st century. Curr Diabetes Rev 2015;11:222–30.
83. Jones AJ, Gladstone BP, Lubeck M, et al. Motivational interventions in the management of HbA1c levels: A systematic review and meta-analysis. Prim Care Diabetes 2014;8:91–100.
84. Song D, Xu TZ, Sun QH. Effect of motivational interviewing on self-management in patients with type 2 diabetes mellitus: a meta-analysis. Intl J Nurs Sci 2014;1:291–7.
85. Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs 2014;23:8–14.
86. Noordman J, van der Weijden T, van Dulmen S. Communication-related behavior change techniques used in face-to-face lifestyle interventions in primary care: a systematic review of the literature. Patient Educ Couns 2012;89:227–44.
87. Soderlund LL, Madson MB, Rubak S, Nilsen P. A systematic review of motivational interviewing training for general health care practitioners. Patient Educ Couns 2011;84:16–26.
88. Kang SH, Kim BG, Lee GM. Justification of continuous packed-bed reactor for retroviral vector production from amphotropic PsiCRIP murine producer cell. Cytotechnology 2000;34(1–2):151–8.
89. Holmen H, Torbjornsen A, Wahl AK, et al. A mobile health intervention for self-management and lifestyle change for persons with type 2 diabetes, part 2: one-year results from the Norwegian randomized controlled trial RENEWING HEALTH. JMIR mHealth uHealth 2014;2(4):e57.
90. Chlebowy DO, El-Mallakh P, Myers J, et al. Motivational interviewing to improve diabetes outcomes in African Americans adults with diabetes. West J Nurs Res 2015;37:566–80.
91. Kang HY, Gu MO. [Development and effects of a motivational interviewing self-management program for elderly patients with diabetes mellitus]. J Kor Acad Nurs 2015;45:533–43.
92. Brobeck E, Odencrants S, Bergh H, Hildingh C. Patients’ experiences of lifestyle discussions based on motivational interviewing: a qualitative study. BMC Nursing 2014;13:13.
93. Loskutova NY, Tsai AG, Fisher EB, et al. Patient navigators connecting patients to community resources to improve diabetes outcomes. J Am Board Fam Med 2016;29:78–89.
94. Raiff BR, Barry VB, Ridenour TA, Jitnarin N. Internet-based incentives increase blood glucose testing with a non-adherent, diverse sample of teens with type 1 diabetes mellitus: a randomized controlled Trial. Trans Behav Med 2016;6:179–88.
95. Sahlen KG, Johansson H, Nystrom L, Lindholm L. Health coaching to promote healthier lifestyle among older people at moderate risk for cardiovascular diseases, diabetes and depression: a study protocol for a randomized controlled trial in Sweden. BMC Public Health 2013;13:199.
96. Kane EP, Collinsworth AW, Schmidt KL, et al. Improving diabetes care and outcomes with community health workers. Fam Pract 2016;33:523–8.
97. Wagner JA, Bermudez-Millan A, Damio G, et al. A randomized, controlled trial of a stress management intervention for Latinos with type 2 diabetes delivered by community health workers: Outcomes for psychological wellbeing, glycemic control, and cortisol. Diabetes Res Clin Pract 2016;120:162–70.
98. Rogers EA, Hessler DM, Bodenheimer TS, et al. Diabetes peer coaching: do “better patients” make better coaches? Diabetes Educ 2014;40:107–15.
99. Long JA, Jahnle EC, Richardson DM, et al. Peer mentoring and financial incentives to improve glucose control in African American veterans: a randomized trial. Ann Intern Med 2012;156:416–24.
100. Mundt MP, Agneessens F, Tuan WJ, et al. Primary care team communication networks, team climate, quality of care, and medical costs for patients with diabetes: A cross-sectional study. Int J Nurs Stud 2016;58:1–11.
101. Fisher L, Mullan JT, Arean P, et al. Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care 2010;33:23–8.
102. Fisher L, Glasgow RE, Strycker LA. The relationship between diabetes distress and clinical depression with glycemic control among patients with type 2 diabetes. Diabetes Care 2010;33:1034–6.
103. Ricci-Cabello I, Olry de Labry-Lima A, Bolivar-Munoz J, et al. Effectiveness of two interventions based on improving patient-practitioner communication on diabetes self-management in patients with low educational level: study protocol of a clustered randomized trial in primary care. BMC Health Serv Res 2013;13:433.
104. Billimek J, Guzman H, Angulo MA. Effectiveness and feasibility of a software tool to help patients communicate with doctors about problems they face with their medication regimen (EMPATHy): study protocol for a randomized controlled trial. Trials 2015;16:145.
105. Grant RW, Uratsu CS, Estacio KR, et al. Pre-Visit Prioritization for complex patients with diabetes: Randomized trial design and implementation within an integrated health care system. Contemp Clin Trials 2016;47:196–201.
106. Ritholz MD, Beverly EA, Abrahamson MJ, et al. Physicians’ perceptions of the type 2 diabetes multidisciplinary treatment team: a qualitative study. Diabetes Educ 2011.
107. Ley P. Satisfaction, compliance and communication. Br J Clin Psychol 1982;21:241–54.
108. Weinger K, Smaldone A, Beverly EA. Psychosocial and educational implications of diabetic foot complications. In: Veves A, Giurini JM, LoGerfo FW, editors. The diabetic foot: medical and surgical management. Boston: Springer; 2012:503–18.
109. Welch G, Rose G, Ernst D. Motivational interviewing and diabetes: what is it, how is it used, and does it work? Diabetes Spectr 2006;19:5–11.
110. Kaplan SH, Greenfield S, Ware JE Jr. Assessing the effects of physician-patient interactions on the outcomes of chronic disease. Med Care 1989;27(3 Suppl):S110–27.
111. Nelson KM, Reiber G, Boyko EJ. Diet and exercise among adults with type 2 diabetes: findings from the third national health and nutrition examination survey (NHANES III). Diabetes Care 2002;25:1722–8.
112. Wens J, Vermeire E, Royen PV, et al. GPs’ perspectives of type 2 diabetes patients’ adherence to treatment: A qualitative analysis of barriers and solutions. BMC Fam Pract 2005;6:20.
1. Anderson E, Kian EM. Examining media contestation of masculinity and head trauma in the National Football League. J Men Masculinities 2011;1–22.
2. CDC. National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011.
3. Bandura A. Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice Hall; 1986.
4. Jacobson AM, Adler AG, Derby L, et al. Clinic attendance and glycemic control. Study of contrasting groups of patients with IDDM. Diabetes Care 1991;14:599–601.
5. Dyer PH, Lloyd CE, Lancashire RJ, et al. Factors associated with clinic non-attendance in adults with type 1 diabetes mellitus. Diab Med 1998;15:339–43.
6. Conn VS, Hafdahl AR, Mehr DR, et al. Metabolic effects of interventions to increase exercise in adults with type 2 diabetes. Diabetologia 2007;50:913–21.
7. Maiorana A, O’Driscoll G, Goodman C, et al. Combined aerobic and resistance exercise improves glycemic control and fitness in type 2 diabetes. Diab Res Clin Pract 2002;56:115–23.
8. Pi-Sunyer FX, Maggio CA, McCarron DA, et al. Multicenter randomized trial of a comprehensive prepared meal program in type 2 diabetes. Diabetes Care 1999;22:191–7.
9. Delahanty LM, Halford BN. The role of diet behaviors in achieving improved glycemic control in intensively treated patients in the Diabetes Control and Complications Trial. Diabetes Care 1993;16:1453–8.
10. Gafarian CT, Heiby EM, Blair P, Singer F. The Diabetes Time Management Questionnaire. Diabetes Educ 1999;25:585–92.
11. Wdowik MJ, Kendall PA, Harris MA. College students with diabetes: using focus groups and interviews to determine psychosocial issues and barriers to control. Diabetes Educ 1997;23:558–62.
12. Rubin RR, Peyrot M. Psychological issues and treatment for people with diabetes. J Clin Psychol 2001;57:457–78.
13. Ali MK, Bullard KM, Gregg EW. Achievement of goals in U.S. Diabetes Care, 1999-2010. N Engl J Med 2013;369:287–8.
14. Beverly EA, Ganda OP, Ritholz MD, et al. Look who’s (not) talking: diabetic patients’ willingness to discuss self-care with physicians. Diabetes Care 2012;35:1466–72.
15. Heisler M, Vijan S, Anderson RM, et al. When do patients and their physicians agree on diabetes treatment goals and strategies, and what difference does it make? J Gen Intern Med 2003;18:893–902.
16. Greenfield S, Kaplan SH, Ware JE Jr, et al. Patients’ participation in medical care: effects on blood sugar control and quality of life in diabetes. J Gen Intern Med 1988;3:448–57.
17. Greenfield S, Kaplan S, Ware JE Jr. Expanding patient involvement in care. Effects on patient outcomes. Ann Intern Med 1985;102:520–8.
18. Anderson RM, Funnell MM, Butler PM, et al. Patient empowerment. Results of a randomized controlled trial. Diabetes Care 1995;18:943–9.
19. Von Korff M, Gruman J, Schaefer J, et al. Collaborative management of chronic illness. Ann Intern Med 1997;127:1097–102.
20. Campbell SM, Hann M, Hacker J, et al. Identifying predictors of high quality care in English general practice: observational study. BMJ 2001;323:784–7.
21. Bower P, Campbell S, Bojke C, Sibbald B. Team structure, team climate and the quality of care in primary care: an observational study. Qual Saf Health Care 2003;12:273–9.
22. Piette JD, Schillinger D, Potter MB, Heisler M. Dimensions of patient-provider communication and diabetes self-care in an ethnically diverse population. J Gen Intern Med 2003;18:624-33.
23. Kerr EA, Smith DM, Kaplan SH, Hayward RA. The association between three different measures of health status and satisfaction among patients with diabetes. Med Care Res Rev 2003;60:158-77.
24. Oshima Lee E, Emanuel EJ. Shared decision making to improve care and reduce costs. N Engl J Med 2013;368:6-8.
25. Barry MJ, Edgman-Levitan S. Shared decision making--pinnacle of patient-centered care. N Engl J Med 2012;366:780–1.
26. Truog RD. Patients and doctors--evolution of a relationship. N Engl J Med 2012;366:581–5.
27. Beverly EA, Wray LA, LaCoe CL, Gabbay R. Listening to older adults’ values and preferences for type 2 diabetes care: a qualitative study. Diabetes Spectrum 2014;27:44–9.
28. Bordin ES. The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy 1979;26:252–60.
29. Ciechanowski PS, Katon WJ, Russo JE, Walker EA. The patient-provider relationship: attachment theory and adherence to treatment in diabetes. Am J Psychiatry 2001;158:29–35.
30. Ciechanowski P, Russo J, Katon W, et al. Influence of patient attachment style on self-care and outcomes in diabetes. Psychosom Med 2004;66:720–8.
31. Jahng KH, Martin LR, Golin CE, DiMatteo MR. Preferences for medical collaboration: patient-physician congruence and patient outcomes. Patient Educ Couns 2005;57:308–14.
32. Street RL Jr, Krupat E, Bell RA, et al. Beliefs about control in the physician-patient relationship: effect on communication in medical encounters. J Gen Intern Med 2003;18:609–16.
33. Heisler M, Bouknight RR, Hayward RA, et al. The relative importance of physician communication, participatory decision making, and patient understanding in diabetes self-management. J Gen Intern Med 2002;17:243–52.
34. Mechanic D. Changing medical organization and the erosion of trust. Milbank Q 1996;74:171–89.
35. Mechanic D, Schlesinger M. The impact of managed care on patients’ trust in medical care and their physicians. JAMA 1996;275:1693–7.
36. Pearson SD, Raeke LH. Patients’ trust in physicians: many theories, few measures, and little data. J Gen Intern Med 2000;15:509–13.
37. Jones DE, Carson KA, Bleich SN, Cooper LA. Patient trust in physicians and adoption of lifestyle behaviors to control high blood pressure. Patient Educ Couns 2012;89:57–62.
38. Mostashari F, Riley E, Selwyn PA, Altice FL. Acceptance and adherence with antiretroviral therapy among HIV-infected women in a correctional facility. J Acquired Immun Def Syndr Hum Retrovir 1998;18:341–8.
39. Cooper-Patrick L, Gallo JJ, Gonzales JJ, et al. Race, gender, and partnership in the patient-physician relationship. JAMA 1999;282:583–9.
40. Ritholz MD, Beverly EA, Brooks KM, et al. Barriers and facilitators to self-care communication during medical appointments in the United States for adults with type 2 diabetes. Chronic Illn 2014;10:303–13.
41. Aikens JE, Bingham R, Piette JD. Patient-provider communication and self-care behavior among type 2 diabetes patients. Diabetes Educ 2005;31:681–90.
42. Bundesmann R, Kaplowitz SA. Provider communication and patient participation in diabetes self-care. Patient Educ Couns 2011;85:143–7.
43. Heisler M, Cole I, Weir D, et al. Does physician communication influence older patients’ diabetes self-management and glycemic control? Results from the Health and Retirement Study (HRS). J Gerontol A Biol Sci Med Sci 2007;62:1435–42.
44. Duffy FD, Gordon GH, Whelan G, et al. Assessing competence in communication and interpersonal skills: the Kalamazoo II report. Acad Med 2004;79:495–507.
45. Ritholz MD, Beverly EA, Brooks KM, et al. Barriers and facilitators to self-care communication during medical appointments in the United States for adults with type 2 diabetes. Chronic Illn 2014;10:303–13.
46. Ciechanowski P, Katon WJ. The interpersonal experience of health care through the eyes of patients with diabetes. Soc Sci Med 2006;63:3067–79.
47. Diabetes Control and Complications Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329:977–86.
48. Peyrot M, Rubin RR, Lauritzen T, et al. Psychosocial problems and barriers to improved diabetes management: results of the Cross-National Diabetes Attitudes, Wishes and Needs (DAWN) Study. Diab Med 2005;22:1379–85.
49. DiMatteo MR, Linn LS, Chang BL, Cope DW. Affect and neutrality in physician behavior: a study of patients’ values and satisfaction. J Behav Med 1985;8:397–409.
50. Stuckey HL, Vallis M, Kovacs Burns K, et al. “I do my best to listen to patients”: qualitative insights into DAWN2 (Diabetes Psychosocial Care From the Perspective of Health Care Professionals in the Second Diabetes Attitudes, Wishes and Needs Study). Clin Ther 2015;37:1986–98.
51. Kruse RL, Olsberg JE, Oliver DP, et al. Patient-provider communication about diabetes self-care activities. Fam Med 2013;45:319–22.
52. Beverly EA, Hultgren BA, Brooks KM, et al. Understanding physicians’ challenges when treating type 2 diabetic patients’ social and emotional difficulties: a qualitative study. Diabetes Care 2011;34:1086–8.
53. Freeman J, Loewe R. Barriers to communication about diabetes mellitus. Patients’ and physicians’ different view of the disease. J Fam Pract 2000;49:507–12.
54. Gonzalez JS, Delahanty LM, Safren SA, et al. Differentiating symptoms of depression from diabetes-specific distress: relationships with self-care in type 2 diabetes. Diabetologia 2008;51:1822–5.
55. Fisher L, Hessler DM, Polonsky WH, Mullan J. When is diabetes distress clinically meaningful?: establishing cut points for the Diabetes Distress Scale. Diabetes Care 2012;35:259–64.
56. Polonsky WH, Anderson BJ, Lohrer PA, et al. Assessment of diabetes-related distress. Diabetes Care 1995;18:754–60.
57. Welch G, Weinger K, Anderson B, Polonsky WH. Responsiveness of the Problem Areas In Diabetes (PAID) questionnaire. Diabetic Med 2003;20:69–72.
58. Weinger K, Kinsley BT, Bajaj M, et al. Diabetes-related emotional distress: A barrier to improving glycemic control during intensive diabetes treatment. Abstract. Diabetes 1997;46:Supp1:268A.
59. Weinger K, Jacobson AM. Psychosocial and quality of life correlates of glycemic control during intensive treatment of type 1 diabetes. Patient Educ Couns 2001;42:123–31.
60. Fisher L, Chesla CA, Skaff MM, et al. The family and disease management in Hispanic and European-American patients with type 2 diabetes. Diabetes Care 2000;23:267–72.
61. Wen LK, Parchman ML, Shepherd MD. Family support and diet barriers among older Hispanic adults with type 2 diabetes. Fam Med 2004;36:423–30.
62. Chesla CA, Fisher L, Mullan JT, et al. Family and disease management in African-American patients with type 2 diabetes. Diabetes Care 2004;27:2850–5.
63. Brown SA, Harrist RB, Villagomez ET, et al. Gender and treatment differences in knowledge, health beliefs, and metabolic control in Mexican Americans with type 2 diabetes. Diabetes Educ 2000;26:425–38.
64. Fisher L, Chesla CA, Chun KM, et al. Patient-appraised couple emotion management and disease management among Chinese American patients with type 2 diabetes. J Fam Psychol 2004;18:302–10.
65. Akimoto M, Fukunishi I, Kanno K, et al. Psychosocial predictors of relapse among diabetes patients: a 2-year follow-up after inpatient diabetes education. Psychosomatics 2004;45:343–9.
66. Samuel-Hodge CD, Headen SW, Skelly AH, et al. Influences on day-to-day self-management of type 2 diabetes among African-American women: spirituality, the multi-caregiver role, and other social context factors. Diabetes Care 2000;23:928–33.
67. Wing RR, Marcus MD, Epstein LH, Jawad A. A “family-based” approach to the treatment of obese type II diabetic patients. J Consult Clin Psychol 1991;59:156–62.
68. Trief PM, Ploutz-Snyder R, Britton KD, Weinstock RS. The relationship between marital quality and adherence to the diabetes care regimen. Ann Behav Med 2004;27:148–54.
69. Gleeson-Kreig J, Bernal H, Woolley S. The role of social support in the self-management of diabetes mellitus among a Hispanic population. Pub Health Nurs 2002;19:215–22.
70. Wen LK, Shepherd MD, Parchman ML. Family support, diet, and exercise among older Mexican Americans with type 2 diabetes. Diabetes Educ 2004;30:980–93.
71. Ruggiero L. Helping people with diabetes change behavior: from theory to practice. Diab Spectrum 2000;13:125–32.
72. Orr DP, Golden MP, Myers G, Marrero DG. Characteristics of adolescents with poorly controlled diabetes referred to a tertiary care center. Diabetes Care 1983;6:170–5.
73. Lane JD, Stabler B, Ross SL, et al. Psychological predictors of glucose control in patients with IDDM. Diabetes Care 1988;11:798–800.
74. Irvine AA, Cox D, Gonder-Frederick L. Fear of hypoglycemia: relationship to physical and psychological symptoms in patients with insulin-dependent diabetes mellitus. Health Psychology 1992;11:135–8.
75. Irvine A, Cox D, Gonder-Frederick L. The fear of hypoglycemia scale. In: Bradley C, editor. Handbook of psychology and diabetes. Harwood Academic; 1994.
76. Peyrot MF, McMurry JF Jr. Stress buffering and glycemic control. The role of coping styles. Diabetes Care 1992;15:842–6.
77. Peyrot M, McMurry JF Jr, Kruger DF. A biopsychosocial model of glycemic control in diabetes: stress, coping and regimen adherence. J Health Soc Behav 1999;40:141–58.
78. Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med 2011;155:97–107.
79. Sohal S, Sohal P, King-Shier KM, Khan NA. Barriers and facilitators for type-2 diabetes management in South Asians: a systematic review. PloS One 2015:1–15.
80. Schillinger D, Piette J, Grumbach K, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med 2003;163:83–90.
81. Miller WR, Rollnick S. Motivational interviewing: preparing people for change. New York: Guilford Press; 2002.
82. Powell PW, Corathers SD, Raymond J, Streisand R. New approaches to providing individualized diabetes care in the 21st century. Curr Diabetes Rev 2015;11:222–30.
83. Jones AJ, Gladstone BP, Lubeck M, et al. Motivational interventions in the management of HbA1c levels: A systematic review and meta-analysis. Prim Care Diabetes 2014;8:91–100.
84. Song D, Xu TZ, Sun QH. Effect of motivational interviewing on self-management in patients with type 2 diabetes mellitus: a meta-analysis. Intl J Nurs Sci 2014;1:291–7.
85. Clifford Mulimba A, Byron-Daniel J. Motivational interviewing-based interventions and diabetes mellitus. Br J Nurs 2014;23:8–14.
86. Noordman J, van der Weijden T, van Dulmen S. Communication-related behavior change techniques used in face-to-face lifestyle interventions in primary care: a systematic review of the literature. Patient Educ Couns 2012;89:227–44.
87. Soderlund LL, Madson MB, Rubak S, Nilsen P. A systematic review of motivational interviewing training for general health care practitioners. Patient Educ Couns 2011;84:16–26.
88. Kang SH, Kim BG, Lee GM. Justification of continuous packed-bed reactor for retroviral vector production from amphotropic PsiCRIP murine producer cell. Cytotechnology 2000;34(1–2):151–8.
89. Holmen H, Torbjornsen A, Wahl AK, et al. A mobile health intervention for self-management and lifestyle change for persons with type 2 diabetes, part 2: one-year results from the Norwegian randomized controlled trial RENEWING HEALTH. JMIR mHealth uHealth 2014;2(4):e57.
90. Chlebowy DO, El-Mallakh P, Myers J, et al. Motivational interviewing to improve diabetes outcomes in African Americans adults with diabetes. West J Nurs Res 2015;37:566–80.
91. Kang HY, Gu MO. [Development and effects of a motivational interviewing self-management program for elderly patients with diabetes mellitus]. J Kor Acad Nurs 2015;45:533–43.
92. Brobeck E, Odencrants S, Bergh H, Hildingh C. Patients’ experiences of lifestyle discussions based on motivational interviewing: a qualitative study. BMC Nursing 2014;13:13.
93. Loskutova NY, Tsai AG, Fisher EB, et al. Patient navigators connecting patients to community resources to improve diabetes outcomes. J Am Board Fam Med 2016;29:78–89.
94. Raiff BR, Barry VB, Ridenour TA, Jitnarin N. Internet-based incentives increase blood glucose testing with a non-adherent, diverse sample of teens with type 1 diabetes mellitus: a randomized controlled Trial. Trans Behav Med 2016;6:179–88.
95. Sahlen KG, Johansson H, Nystrom L, Lindholm L. Health coaching to promote healthier lifestyle among older people at moderate risk for cardiovascular diseases, diabetes and depression: a study protocol for a randomized controlled trial in Sweden. BMC Public Health 2013;13:199.
96. Kane EP, Collinsworth AW, Schmidt KL, et al. Improving diabetes care and outcomes with community health workers. Fam Pract 2016;33:523–8.
97. Wagner JA, Bermudez-Millan A, Damio G, et al. A randomized, controlled trial of a stress management intervention for Latinos with type 2 diabetes delivered by community health workers: Outcomes for psychological wellbeing, glycemic control, and cortisol. Diabetes Res Clin Pract 2016;120:162–70.
98. Rogers EA, Hessler DM, Bodenheimer TS, et al. Diabetes peer coaching: do “better patients” make better coaches? Diabetes Educ 2014;40:107–15.
99. Long JA, Jahnle EC, Richardson DM, et al. Peer mentoring and financial incentives to improve glucose control in African American veterans: a randomized trial. Ann Intern Med 2012;156:416–24.
100. Mundt MP, Agneessens F, Tuan WJ, et al. Primary care team communication networks, team climate, quality of care, and medical costs for patients with diabetes: A cross-sectional study. Int J Nurs Stud 2016;58:1–11.
101. Fisher L, Mullan JT, Arean P, et al. Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care 2010;33:23–8.
102. Fisher L, Glasgow RE, Strycker LA. The relationship between diabetes distress and clinical depression with glycemic control among patients with type 2 diabetes. Diabetes Care 2010;33:1034–6.
103. Ricci-Cabello I, Olry de Labry-Lima A, Bolivar-Munoz J, et al. Effectiveness of two interventions based on improving patient-practitioner communication on diabetes self-management in patients with low educational level: study protocol of a clustered randomized trial in primary care. BMC Health Serv Res 2013;13:433.
104. Billimek J, Guzman H, Angulo MA. Effectiveness and feasibility of a software tool to help patients communicate with doctors about problems they face with their medication regimen (EMPATHy): study protocol for a randomized controlled trial. Trials 2015;16:145.
105. Grant RW, Uratsu CS, Estacio KR, et al. Pre-Visit Prioritization for complex patients with diabetes: Randomized trial design and implementation within an integrated health care system. Contemp Clin Trials 2016;47:196–201.
106. Ritholz MD, Beverly EA, Abrahamson MJ, et al. Physicians’ perceptions of the type 2 diabetes multidisciplinary treatment team: a qualitative study. Diabetes Educ 2011.
107. Ley P. Satisfaction, compliance and communication. Br J Clin Psychol 1982;21:241–54.
108. Weinger K, Smaldone A, Beverly EA. Psychosocial and educational implications of diabetic foot complications. In: Veves A, Giurini JM, LoGerfo FW, editors. The diabetic foot: medical and surgical management. Boston: Springer; 2012:503–18.
109. Welch G, Rose G, Ernst D. Motivational interviewing and diabetes: what is it, how is it used, and does it work? Diabetes Spectr 2006;19:5–11.
110. Kaplan SH, Greenfield S, Ware JE Jr. Assessing the effects of physician-patient interactions on the outcomes of chronic disease. Med Care 1989;27(3 Suppl):S110–27.
111. Nelson KM, Reiber G, Boyko EJ. Diet and exercise among adults with type 2 diabetes: findings from the third national health and nutrition examination survey (NHANES III). Diabetes Care 2002;25:1722–8.
112. Wens J, Vermeire E, Royen PV, et al. GPs’ perspectives of type 2 diabetes patients’ adherence to treatment: A qualitative analysis of barriers and solutions. BMC Fam Pract 2005;6:20.
Fertility and Fertility Preservation: Scripts to Support Oncology Nurses in Discussions with Adolescent and Young Adult Patients
From the Moffitt Cancer Center, Tampa, FL (Dr. Vadaparampil, Ms. Bowman, Ms. Sehovic, Dr. Quinn), Memorial Sloan Kettering Cancer Center, New York, NY (Ms. Kelvin), and Edward Via College of Osteopathic Medicine, Auburn, AL (Ms. Murphy).
Abstract
- Objective: To describe a script-based approach to assist oncology nurses in fertility discussions with their adolescent and young adult (AYA) patients.
- Methods: Scripts were developed by a team that included experts in fertility and reproductive health, health education, health communication, and clinical care of AYA patients. Individual scripts for females, males, and survivors were created and accompanied by a flyer and frequently asked questions sheet. The script and supplementary materials were then vetted by oncology nurses who participated in the Educating Nurses about Reproductive Health Issues in Cancer Healthcare (ENRICH) training program.
- Results: The scripts were rated as helpful and socially appropriate with minor concerns noted about awkward wording and medical jargon.
- Conclusion: The updated scripts provide one approach for nurses to become more adept at discussing the topic of infertility and FP with AYA oncology patients and survivors.
In the United States, over 70,000 adolescents and young adults (AYAs) are diagnosed with cancer each year [1,2]. Treatments are available that are associated with improved survival for these cancers. Unfortunately, cancer treatment may significantly impact AYA survivors’ future fertility. Infertility or premature ovarian failure can occur during or after cancer treatment (eg, chemotherapy, radiation) for females, and males may be temporarily or permanently azoospermic [3]. There are a number of established methods of fertility preservation (FP) that are available; these include oocyte and embryo cryopreservation and ovarian transposition for females and sperm banking for males [3]. Experimental options for males include testicular tissue freezing and for females ovarian tissue cryopreservation.
The American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network [4,5] recommend discussing FP with patients of reproductive age, ideally before initiation of treatment. In 2013, ASCO updated guidelines extending the responsibility for discussion and referral for FP beyond the medical oncologist to explicitly include other physician specialties, nurses, and allied health care professionals in the oncology care setting [3]. However, multiple publications, including patient surveys and interviews, physician surveys, and medical record abstraction studies suggest these discussions do not consistently take place. In an analysis of 156 practice groups submitting data as part of ASCO's Quality Oncology Practice Initiative, only ~15%–20% of practices routinely discussed infertility risks and FP options [6]. A recent review of medical charts of patients aged 18–45 treated in 2011 at 1 of 4 large U.S. cancer care institutions found that documentation of discussions for infertility risk was 26%, 24% for FP option discussion, and 13% for fertility specialist referral [7].
Oncology nurses play a key role in patients’ care and, compared to other health care providers, are more likely to have multiple interactions with patients prior to the initiation of treatment [8]. They are often attuned to the medical and psychosocial needs of the patient and family and can advocate for their needs and desires [9]. However, existing research finds few oncology nurses discuss this topic with AYA patients. Studies examining barriers have identified factors that may hinder discussions about infertility and FP with AYA oncology patients. These barriers include lack of knowledge about cancer related infertility and available FP procedures; access to reproductive endocrinologists or sperm banking clinics; time constraints in busy clinics and concerns about delaying treatment; discomforts discussing reproductive health; patient’s ability to afford FP; bias about the suitability of FP for young or unpartnered or LGBT patients or those with a poor prognosis; and personal religious or moral values about the use of assisted reproductive technologies [10–15].
Equipping nurses with content-specific communication may overcome some of the barriers described. A method often used in nursing education and communication interventions is scripting [16–18]. Scripting provides precise key words that ensure consistency in the message, no matter the messenger [19]. This paper reports on the development and refinement of a series of scripts to guide discussions about FP for male and female AYA patients and survivors.
Script Development
In 2003 Studer developed the AIDET (Acknowledge, Introduce, Duration, Explanation, and Thank you) model of communication for health professionals [19]. AIDET is an effective tool in facilitating communication practices among nurses and physicians in adult and pediatric settings [20–24]. The AIDET model was adapted by our team to develop AIDED: Assess, Introduce, Decide, Explain, and Discuss, a script-based approach to assist oncology nurses in fertility discussions with their AYA patients. Our team included experts in fertility and reproductive health, health education, health communication, as well as clinical and psychosocial care of AYA patients.
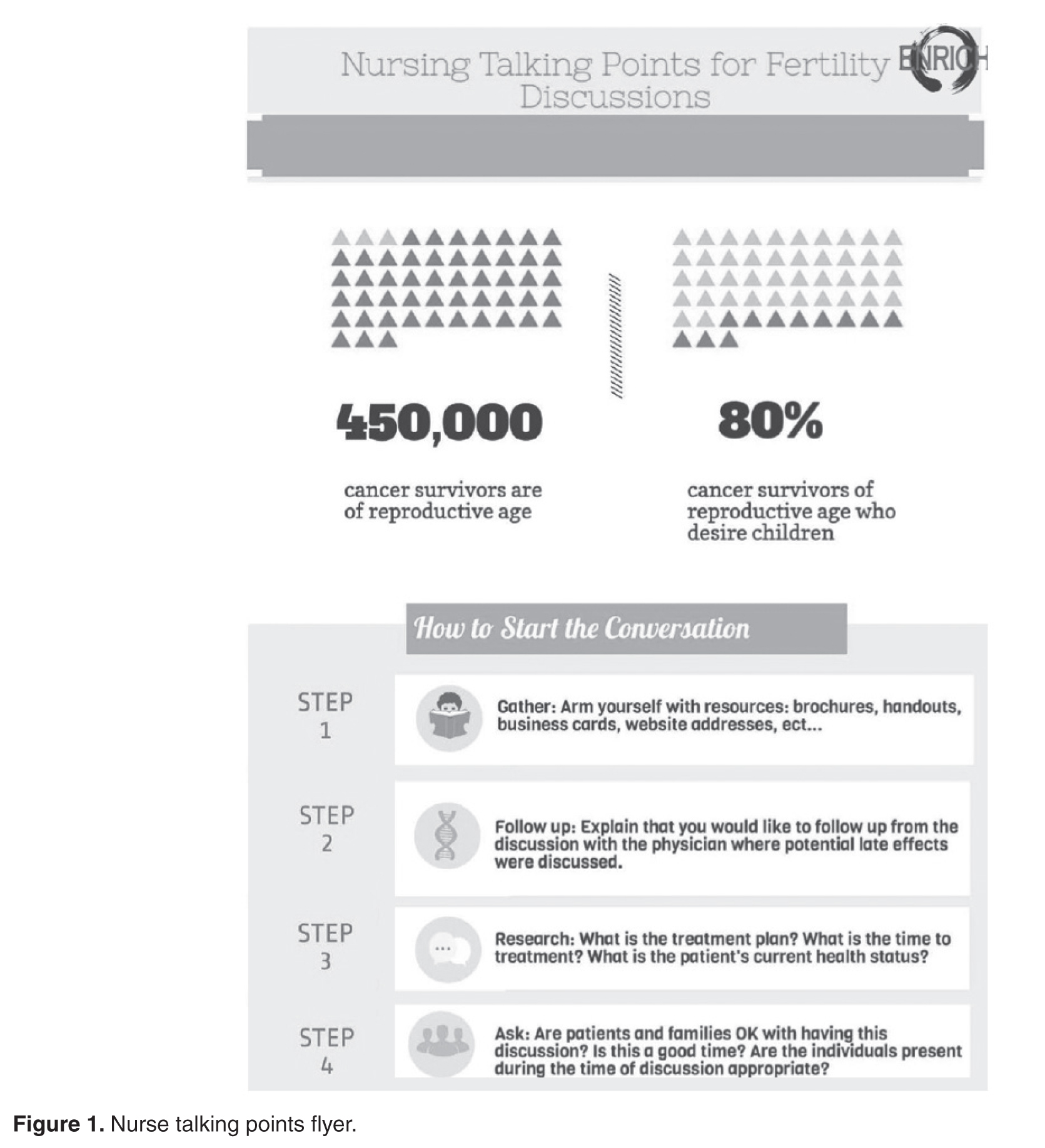
Educating Nurses 
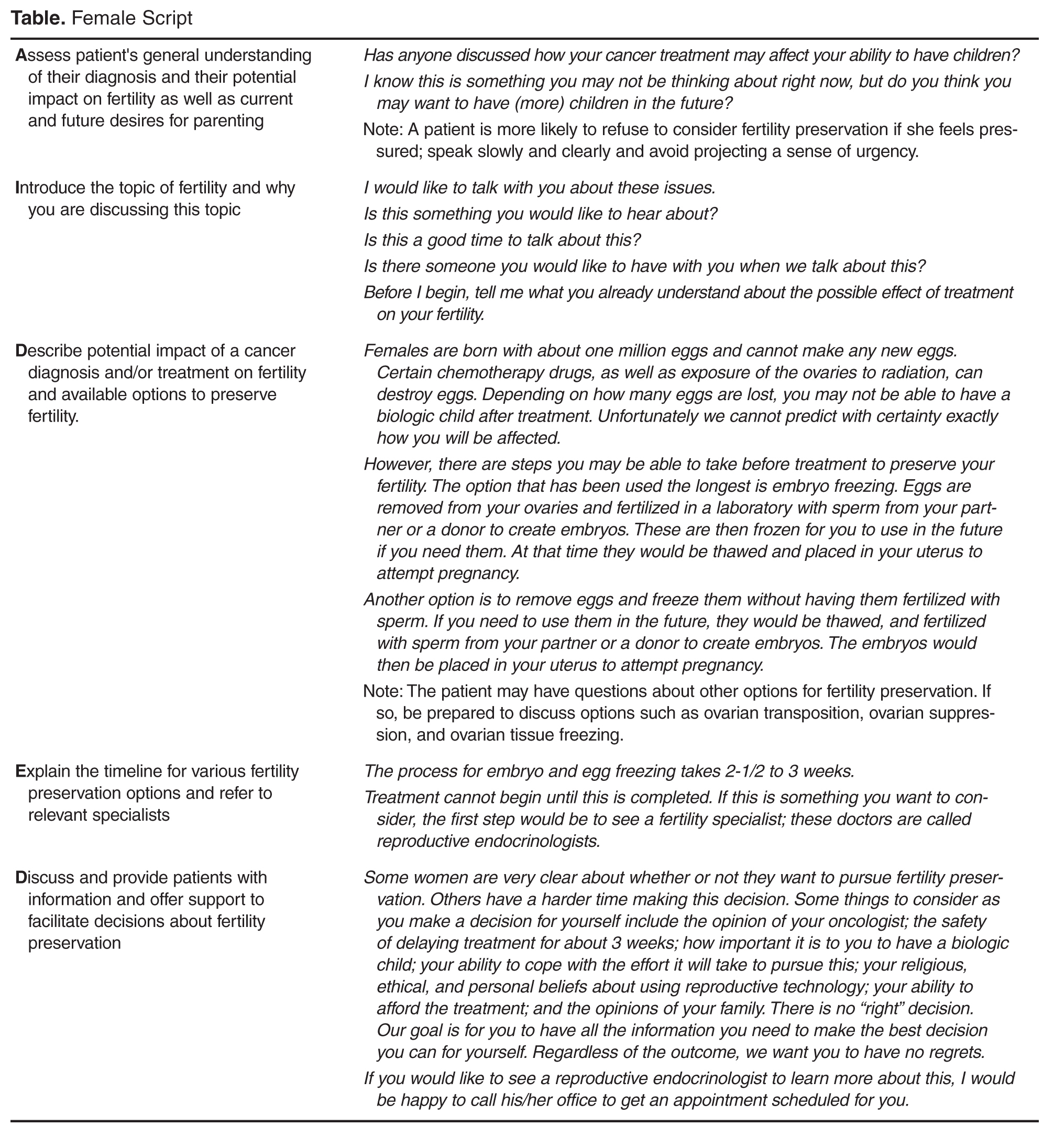
Benefits of Scripts
Communication difficulties may present an obstacle for oncology nurses to address the infertility, FP information, and supportive care needs of AYA cancer patients [15]. While guidelines from leading health and professional organizations support the need to discuss these issues with patients, implementation requires providing practical tools that meet the needs of nurses’ practice setting and patient population [26].
The use of scripts has a long history in the 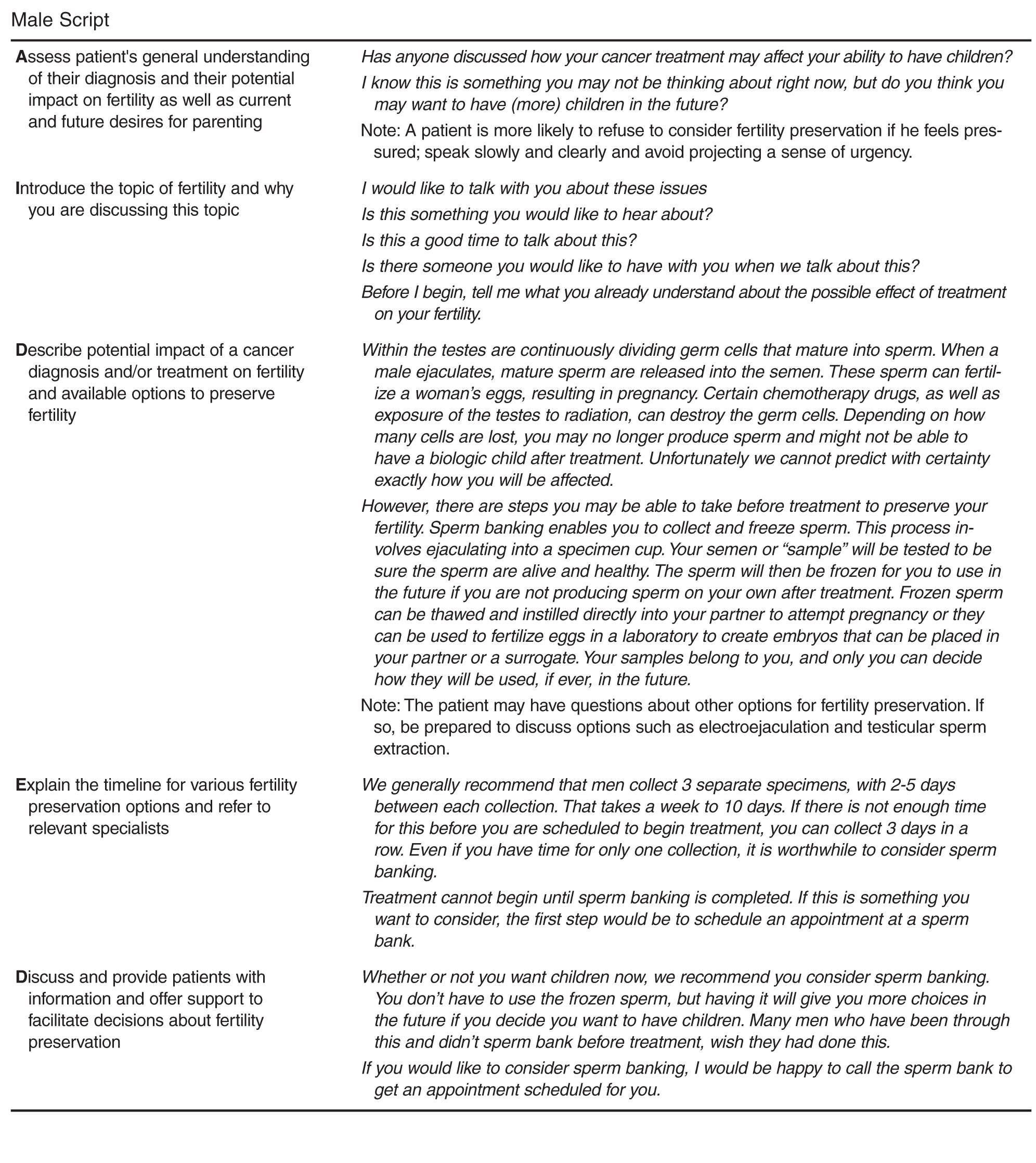
Conclusion

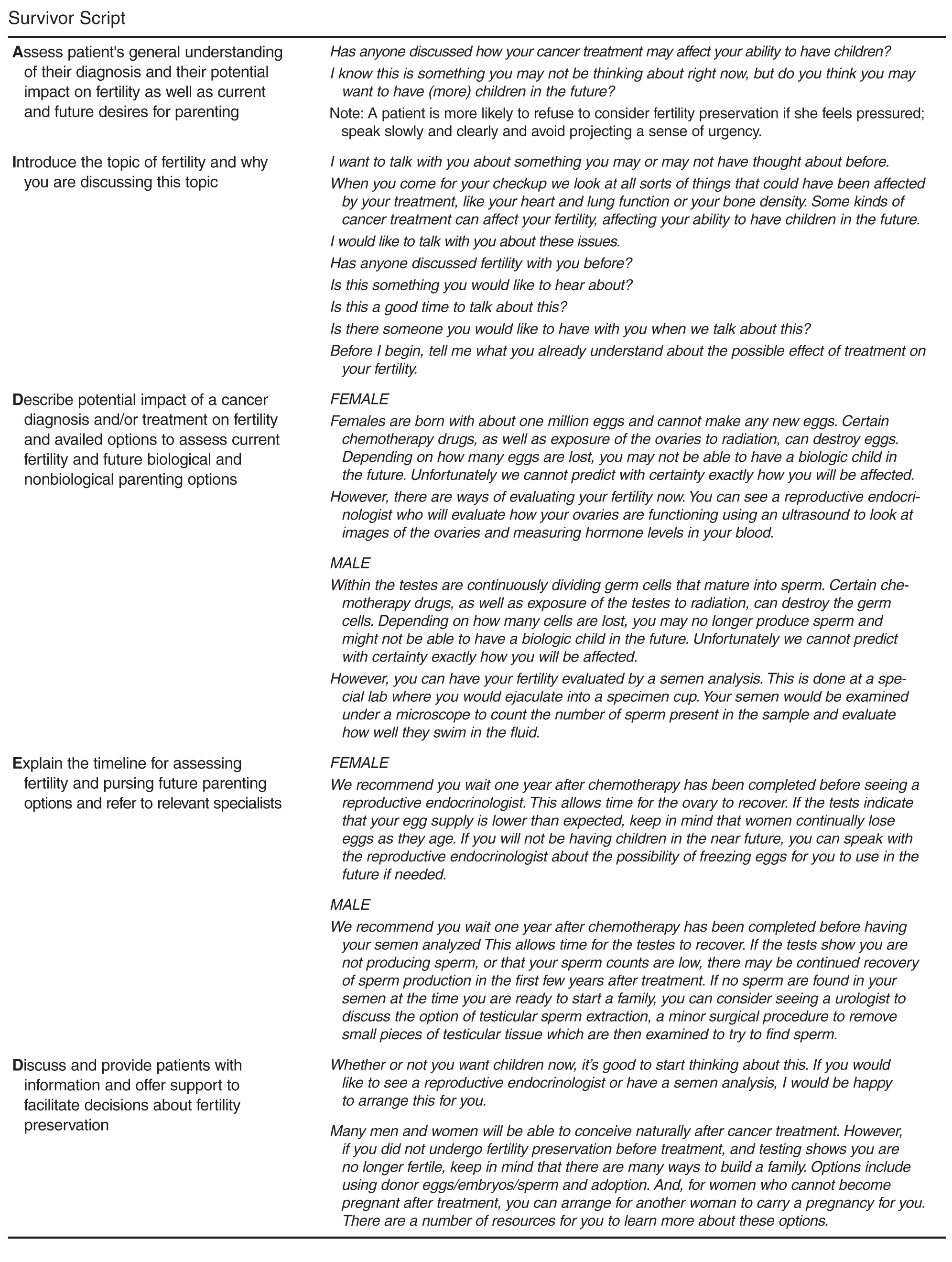
These scripts provide one approach for nurses to become more adept at discussing the topic of FP with AYA oncology patients. We will continue to update and refine these scripts and ultimately test their efficacy in improving psychosocial and behavioral outcomes for AYA patients. While scripts are effective, they must be updated to reflect relevant advances in clinical care. In addition, it is important to identify local resources to facilitate discussion and referral for those who seek additional information and or services related to FP. Such resources include psychosocial support, reproductive endocrinologists with expertise in the unique needs of AYA oncology patients, providers who accept pediatric patients (if needed), and financial assistance.
Corresponding author: Susan T. Vadaparampil, PhD, MPH, 12902 Magnolia Dr., MRC CANCONT, Tampa, FL 33612, susan.vadaparampil@moffitt.org.
Funding/support: ENRICH is funded by a National Cancer Institute R25 Training Grant: #5R25CA142519-05.
Financial disclosures: None.
1. Bleyer AOLM, O’Leary M, Barr L, Ries LAG. Cancer epidemiology in older adolescents and young adults 15 to 29 years of age, including SEER incidence and survival: 1975–2000. Bethesda, MD: National Cancer Institute; 2006.
2. Ward E, DeSantis C, Robbins A, et al. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin 2014;64: 83–103.
3. Loren AW, Mangu PB, Beck LN, et al. Fertility preservation for patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 2013;31:2500–10.
4. Lee SJ, Schover LR, Partridge AH, et al. American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. J Clin Oncol 2006;24:2917–31.
5. Coccia P, Altman J, Bhatia S, et al. Adolescent and young adult (AYA) oncology version 1.2012. National Comprehensive Cancer Network; 2012.
6. Neuss MN, Malin JL, Chan S, et al. Measuring the improving quality of outpatient care in medical oncology practices in the United States. J Clin Oncol 2013;31:1471–7.
7. Quinn GP, Block RG, Clayman ML, et al. If you did not document it, it did not happen: rates of documentation of discussion of infertility risk in adolescent and young adult oncology patients’ medical records. J Oncol Pract 2015;11: 137–44.
8. Cope D. Patients’ and physicians’ experinces with sperm banking and infertility issues related to cancer treatment. Clin J Oncol Nurs 2002;6:293–5.
9. Vaartio-Rajalin H, Leino-Kilpi H. Nurses as patient advocates in oncology care: activities based on literature. Clin J Oncol Nurs. 2011;15:526–32.
10. King LM, Quinn GP, Vadaparampil ST, et al. Oncology nurses’ perceptions of barriers to discussion of fertility preservation with patients with cancer. Clin J Oncol Nurs 2008; 12:467–76.
11. Clayton HB, Vadaparampil ST, Quinn GP, et al. Trends in clinical practice and nurses’ attitudes about fertility preservation for pediatric patients with cancer. Oncol Nurs Forum 2008;35:449–55.
12. Vadaparampil ST, Clayton H, Quinn GP, et al. Pediatric oncology nurses’ attitudes related to discussing fertility preservation with pediatric cancer patients and their families. J Pediatr Oncol Nurs 2007;24:255–63.
13. Kotronoulas G, Papadopoulou C, Patiraki E. Nurses’ knowledge, attitudes, and practices regarding provision of sexual health care in patients with cancer: critical review of the evidence. Support Care Cancer 2009;17:479–501.
14. Reebals JF, Brown R, Buckner EB. Nurse practice issues regarding sperm banking in adolescent male cancer patients. J Pediatr Oncol Nurs 2006;23:182–8.
15. Goossens J, Delbaere I, Beeckman D, et al. Communication difficulties and the experience of loneliness in patients with cancer dealing with fertility issues: a qualitative study. Oncol Nurs Forum 2015;42:34–43.
16. Mustard LW. Improving patient satisfaction through the consistent use of scripting by the nursing staff. JONAS Healthc Law Ethics Regul 2003;5:68–72.
17. Kuiper RA. Integration of innovative clinical reasoning pedagogies into a baccalaureate nursing curriculum. Creat Nurs 2013;19:128–39.
18. Handel DA, Fu R, Daya M, et al. The use of scripting at triage and its impact on elopements. Acad Emerg Med 2010; 17:495–500.
19. Studer Q. Hardwiring excellence: purpose, worthwhile work, making a difference. Gulf Breeze, FL: Fire Starter Publishing; 2003.
20. Katona A, Kunkel E, Arfaa J, et al. Methodology for delivering feedback to neurology house staff on communication skills using AIDET (Acknowledge, Introduce, Duration, Explanation, Thank You). Neurology 2014;82(10 Suppl):P1–328.
21. Prestia A , Dyess S. Maximizing caring relationships between nursing assistants and patients: Care partners. J Nurs Admin 2012;42:144–7.
22. Fisher MJ. A brief intervention to improve emotion-focused communication between newly licensed pediatric nurses and parents [dissertation]. Indianapolis: Indiana University; 2012.
23. Baker SJ. Key words: a prescriptive approach to reducing patient anxiety and improving safety. J Emerg Nurs 2011; 37:571–4.
24. Shupe R. Using skills validation and verification techniques to hardwire staff behaviors. J Emerg Nurs 2013;39:364–8.
25. Vadaparampil ST, Hutchins NM, Quinn GP. Reproductive health in the adolescent and young adult cancer patient: an innovative training program for oncology nurses. J Cancer Educ 2013;28:197–208.
26. Shekelle P, Woolf S, Grimshaw JM, et al. Developing clinical practice guidelines: reviewing, reporting, and publishing guidelines; updating guidelines; and the emerging issues of enhancing guideline implementability and accounting for comorbid conditions in guideline development. Implement Sci 2012;7:62.
27. Clayton JM, Adler JL, O’Callaghan A, et al. Intensive communication skills teaching for specialist training in palliative medicine: development and evaluation of an experiential workshop. J Palliat Med 2012;15:585–91.
28. Hymes DH. On communicative competence. In: Pride JB, Holmes J, editors. Sociolinguistics: selected readings. Harmondsworth: Penguin; 1972:269–93.
29. Asnani MR. Patient-physician communication. West Indian Med J 2009;58:357–61.
30. Clark PA. Medical practices’ sensitivity to patients’ needs: Opportunities and practices for improvement. J Ambulat Care Manage 2003;26:110–23.
31. Wanzer MB, Booth-Butterfield M, Gruber K. Perceptions of health care providers’ communication: Relationships between patient-centered communication and satisfaction. Health Care Commun 2004;16:363–84.
From the Moffitt Cancer Center, Tampa, FL (Dr. Vadaparampil, Ms. Bowman, Ms. Sehovic, Dr. Quinn), Memorial Sloan Kettering Cancer Center, New York, NY (Ms. Kelvin), and Edward Via College of Osteopathic Medicine, Auburn, AL (Ms. Murphy).
Abstract
- Objective: To describe a script-based approach to assist oncology nurses in fertility discussions with their adolescent and young adult (AYA) patients.
- Methods: Scripts were developed by a team that included experts in fertility and reproductive health, health education, health communication, and clinical care of AYA patients. Individual scripts for females, males, and survivors were created and accompanied by a flyer and frequently asked questions sheet. The script and supplementary materials were then vetted by oncology nurses who participated in the Educating Nurses about Reproductive Health Issues in Cancer Healthcare (ENRICH) training program.
- Results: The scripts were rated as helpful and socially appropriate with minor concerns noted about awkward wording and medical jargon.
- Conclusion: The updated scripts provide one approach for nurses to become more adept at discussing the topic of infertility and FP with AYA oncology patients and survivors.
In the United States, over 70,000 adolescents and young adults (AYAs) are diagnosed with cancer each year [1,2]. Treatments are available that are associated with improved survival for these cancers. Unfortunately, cancer treatment may significantly impact AYA survivors’ future fertility. Infertility or premature ovarian failure can occur during or after cancer treatment (eg, chemotherapy, radiation) for females, and males may be temporarily or permanently azoospermic [3]. There are a number of established methods of fertility preservation (FP) that are available; these include oocyte and embryo cryopreservation and ovarian transposition for females and sperm banking for males [3]. Experimental options for males include testicular tissue freezing and for females ovarian tissue cryopreservation.
The American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network [4,5] recommend discussing FP with patients of reproductive age, ideally before initiation of treatment. In 2013, ASCO updated guidelines extending the responsibility for discussion and referral for FP beyond the medical oncologist to explicitly include other physician specialties, nurses, and allied health care professionals in the oncology care setting [3]. However, multiple publications, including patient surveys and interviews, physician surveys, and medical record abstraction studies suggest these discussions do not consistently take place. In an analysis of 156 practice groups submitting data as part of ASCO's Quality Oncology Practice Initiative, only ~15%–20% of practices routinely discussed infertility risks and FP options [6]. A recent review of medical charts of patients aged 18–45 treated in 2011 at 1 of 4 large U.S. cancer care institutions found that documentation of discussions for infertility risk was 26%, 24% for FP option discussion, and 13% for fertility specialist referral [7].
Oncology nurses play a key role in patients’ care and, compared to other health care providers, are more likely to have multiple interactions with patients prior to the initiation of treatment [8]. They are often attuned to the medical and psychosocial needs of the patient and family and can advocate for their needs and desires [9]. However, existing research finds few oncology nurses discuss this topic with AYA patients. Studies examining barriers have identified factors that may hinder discussions about infertility and FP with AYA oncology patients. These barriers include lack of knowledge about cancer related infertility and available FP procedures; access to reproductive endocrinologists or sperm banking clinics; time constraints in busy clinics and concerns about delaying treatment; discomforts discussing reproductive health; patient’s ability to afford FP; bias about the suitability of FP for young or unpartnered or LGBT patients or those with a poor prognosis; and personal religious or moral values about the use of assisted reproductive technologies [10–15].
Equipping nurses with content-specific communication may overcome some of the barriers described. A method often used in nursing education and communication interventions is scripting [16–18]. Scripting provides precise key words that ensure consistency in the message, no matter the messenger [19]. This paper reports on the development and refinement of a series of scripts to guide discussions about FP for male and female AYA patients and survivors.
Script Development
In 2003 Studer developed the AIDET (Acknowledge, Introduce, Duration, Explanation, and Thank you) model of communication for health professionals [19]. AIDET is an effective tool in facilitating communication practices among nurses and physicians in adult and pediatric settings [20–24]. The AIDET model was adapted by our team to develop AIDED: Assess, Introduce, Decide, Explain, and Discuss, a script-based approach to assist oncology nurses in fertility discussions with their AYA patients. Our team included experts in fertility and reproductive health, health education, health communication, as well as clinical and psychosocial care of AYA patients.
Educating Nurses
Benefits of Scripts
Communication difficulties may present an obstacle for oncology nurses to address the infertility, FP information, and supportive care needs of AYA cancer patients [15]. While guidelines from leading health and professional organizations support the need to discuss these issues with patients, implementation requires providing practical tools that meet the needs of nurses’ practice setting and patient population [26].
The use of scripts has a long history in the
Conclusion
These scripts provide one approach for nurses to become more adept at discussing the topic of FP with AYA oncology patients. We will continue to update and refine these scripts and ultimately test their efficacy in improving psychosocial and behavioral outcomes for AYA patients. While scripts are effective, they must be updated to reflect relevant advances in clinical care. In addition, it is important to identify local resources to facilitate discussion and referral for those who seek additional information and or services related to FP. Such resources include psychosocial support, reproductive endocrinologists with expertise in the unique needs of AYA oncology patients, providers who accept pediatric patients (if needed), and financial assistance.
Corresponding author: Susan T. Vadaparampil, PhD, MPH, 12902 Magnolia Dr., MRC CANCONT, Tampa, FL 33612, susan.vadaparampil@moffitt.org.
Funding/support: ENRICH is funded by a National Cancer Institute R25 Training Grant: #5R25CA142519-05.
Financial disclosures: None.
From the Moffitt Cancer Center, Tampa, FL (Dr. Vadaparampil, Ms. Bowman, Ms. Sehovic, Dr. Quinn), Memorial Sloan Kettering Cancer Center, New York, NY (Ms. Kelvin), and Edward Via College of Osteopathic Medicine, Auburn, AL (Ms. Murphy).
Abstract
- Objective: To describe a script-based approach to assist oncology nurses in fertility discussions with their adolescent and young adult (AYA) patients.
- Methods: Scripts were developed by a team that included experts in fertility and reproductive health, health education, health communication, and clinical care of AYA patients. Individual scripts for females, males, and survivors were created and accompanied by a flyer and frequently asked questions sheet. The script and supplementary materials were then vetted by oncology nurses who participated in the Educating Nurses about Reproductive Health Issues in Cancer Healthcare (ENRICH) training program.
- Results: The scripts were rated as helpful and socially appropriate with minor concerns noted about awkward wording and medical jargon.
- Conclusion: The updated scripts provide one approach for nurses to become more adept at discussing the topic of infertility and FP with AYA oncology patients and survivors.
In the United States, over 70,000 adolescents and young adults (AYAs) are diagnosed with cancer each year [1,2]. Treatments are available that are associated with improved survival for these cancers. Unfortunately, cancer treatment may significantly impact AYA survivors’ future fertility. Infertility or premature ovarian failure can occur during or after cancer treatment (eg, chemotherapy, radiation) for females, and males may be temporarily or permanently azoospermic [3]. There are a number of established methods of fertility preservation (FP) that are available; these include oocyte and embryo cryopreservation and ovarian transposition for females and sperm banking for males [3]. Experimental options for males include testicular tissue freezing and for females ovarian tissue cryopreservation.
The American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network [4,5] recommend discussing FP with patients of reproductive age, ideally before initiation of treatment. In 2013, ASCO updated guidelines extending the responsibility for discussion and referral for FP beyond the medical oncologist to explicitly include other physician specialties, nurses, and allied health care professionals in the oncology care setting [3]. However, multiple publications, including patient surveys and interviews, physician surveys, and medical record abstraction studies suggest these discussions do not consistently take place. In an analysis of 156 practice groups submitting data as part of ASCO's Quality Oncology Practice Initiative, only ~15%–20% of practices routinely discussed infertility risks and FP options [6]. A recent review of medical charts of patients aged 18–45 treated in 2011 at 1 of 4 large U.S. cancer care institutions found that documentation of discussions for infertility risk was 26%, 24% for FP option discussion, and 13% for fertility specialist referral [7].
Oncology nurses play a key role in patients’ care and, compared to other health care providers, are more likely to have multiple interactions with patients prior to the initiation of treatment [8]. They are often attuned to the medical and psychosocial needs of the patient and family and can advocate for their needs and desires [9]. However, existing research finds few oncology nurses discuss this topic with AYA patients. Studies examining barriers have identified factors that may hinder discussions about infertility and FP with AYA oncology patients. These barriers include lack of knowledge about cancer related infertility and available FP procedures; access to reproductive endocrinologists or sperm banking clinics; time constraints in busy clinics and concerns about delaying treatment; discomforts discussing reproductive health; patient’s ability to afford FP; bias about the suitability of FP for young or unpartnered or LGBT patients or those with a poor prognosis; and personal religious or moral values about the use of assisted reproductive technologies [10–15].
Equipping nurses with content-specific communication may overcome some of the barriers described. A method often used in nursing education and communication interventions is scripting [16–18]. Scripting provides precise key words that ensure consistency in the message, no matter the messenger [19]. This paper reports on the development and refinement of a series of scripts to guide discussions about FP for male and female AYA patients and survivors.
Script Development
In 2003 Studer developed the AIDET (Acknowledge, Introduce, Duration, Explanation, and Thank you) model of communication for health professionals [19]. AIDET is an effective tool in facilitating communication practices among nurses and physicians in adult and pediatric settings [20–24]. The AIDET model was adapted by our team to develop AIDED: Assess, Introduce, Decide, Explain, and Discuss, a script-based approach to assist oncology nurses in fertility discussions with their AYA patients. Our team included experts in fertility and reproductive health, health education, health communication, as well as clinical and psychosocial care of AYA patients.
Educating Nurses
Benefits of Scripts
Communication difficulties may present an obstacle for oncology nurses to address the infertility, FP information, and supportive care needs of AYA cancer patients [15]. While guidelines from leading health and professional organizations support the need to discuss these issues with patients, implementation requires providing practical tools that meet the needs of nurses’ practice setting and patient population [26].
The use of scripts has a long history in the
Conclusion
These scripts provide one approach for nurses to become more adept at discussing the topic of FP with AYA oncology patients. We will continue to update and refine these scripts and ultimately test their efficacy in improving psychosocial and behavioral outcomes for AYA patients. While scripts are effective, they must be updated to reflect relevant advances in clinical care. In addition, it is important to identify local resources to facilitate discussion and referral for those who seek additional information and or services related to FP. Such resources include psychosocial support, reproductive endocrinologists with expertise in the unique needs of AYA oncology patients, providers who accept pediatric patients (if needed), and financial assistance.
Corresponding author: Susan T. Vadaparampil, PhD, MPH, 12902 Magnolia Dr., MRC CANCONT, Tampa, FL 33612, susan.vadaparampil@moffitt.org.
Funding/support: ENRICH is funded by a National Cancer Institute R25 Training Grant: #5R25CA142519-05.
Financial disclosures: None.
1. Bleyer AOLM, O’Leary M, Barr L, Ries LAG. Cancer epidemiology in older adolescents and young adults 15 to 29 years of age, including SEER incidence and survival: 1975–2000. Bethesda, MD: National Cancer Institute; 2006.
2. Ward E, DeSantis C, Robbins A, et al. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin 2014;64: 83–103.
3. Loren AW, Mangu PB, Beck LN, et al. Fertility preservation for patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 2013;31:2500–10.
4. Lee SJ, Schover LR, Partridge AH, et al. American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. J Clin Oncol 2006;24:2917–31.
5. Coccia P, Altman J, Bhatia S, et al. Adolescent and young adult (AYA) oncology version 1.2012. National Comprehensive Cancer Network; 2012.
6. Neuss MN, Malin JL, Chan S, et al. Measuring the improving quality of outpatient care in medical oncology practices in the United States. J Clin Oncol 2013;31:1471–7.
7. Quinn GP, Block RG, Clayman ML, et al. If you did not document it, it did not happen: rates of documentation of discussion of infertility risk in adolescent and young adult oncology patients’ medical records. J Oncol Pract 2015;11: 137–44.
8. Cope D. Patients’ and physicians’ experinces with sperm banking and infertility issues related to cancer treatment. Clin J Oncol Nurs 2002;6:293–5.
9. Vaartio-Rajalin H, Leino-Kilpi H. Nurses as patient advocates in oncology care: activities based on literature. Clin J Oncol Nurs. 2011;15:526–32.
10. King LM, Quinn GP, Vadaparampil ST, et al. Oncology nurses’ perceptions of barriers to discussion of fertility preservation with patients with cancer. Clin J Oncol Nurs 2008; 12:467–76.
11. Clayton HB, Vadaparampil ST, Quinn GP, et al. Trends in clinical practice and nurses’ attitudes about fertility preservation for pediatric patients with cancer. Oncol Nurs Forum 2008;35:449–55.
12. Vadaparampil ST, Clayton H, Quinn GP, et al. Pediatric oncology nurses’ attitudes related to discussing fertility preservation with pediatric cancer patients and their families. J Pediatr Oncol Nurs 2007;24:255–63.
13. Kotronoulas G, Papadopoulou C, Patiraki E. Nurses’ knowledge, attitudes, and practices regarding provision of sexual health care in patients with cancer: critical review of the evidence. Support Care Cancer 2009;17:479–501.
14. Reebals JF, Brown R, Buckner EB. Nurse practice issues regarding sperm banking in adolescent male cancer patients. J Pediatr Oncol Nurs 2006;23:182–8.
15. Goossens J, Delbaere I, Beeckman D, et al. Communication difficulties and the experience of loneliness in patients with cancer dealing with fertility issues: a qualitative study. Oncol Nurs Forum 2015;42:34–43.
16. Mustard LW. Improving patient satisfaction through the consistent use of scripting by the nursing staff. JONAS Healthc Law Ethics Regul 2003;5:68–72.
17. Kuiper RA. Integration of innovative clinical reasoning pedagogies into a baccalaureate nursing curriculum. Creat Nurs 2013;19:128–39.
18. Handel DA, Fu R, Daya M, et al. The use of scripting at triage and its impact on elopements. Acad Emerg Med 2010; 17:495–500.
19. Studer Q. Hardwiring excellence: purpose, worthwhile work, making a difference. Gulf Breeze, FL: Fire Starter Publishing; 2003.
20. Katona A, Kunkel E, Arfaa J, et al. Methodology for delivering feedback to neurology house staff on communication skills using AIDET (Acknowledge, Introduce, Duration, Explanation, Thank You). Neurology 2014;82(10 Suppl):P1–328.
21. Prestia A , Dyess S. Maximizing caring relationships between nursing assistants and patients: Care partners. J Nurs Admin 2012;42:144–7.
22. Fisher MJ. A brief intervention to improve emotion-focused communication between newly licensed pediatric nurses and parents [dissertation]. Indianapolis: Indiana University; 2012.
23. Baker SJ. Key words: a prescriptive approach to reducing patient anxiety and improving safety. J Emerg Nurs 2011; 37:571–4.
24. Shupe R. Using skills validation and verification techniques to hardwire staff behaviors. J Emerg Nurs 2013;39:364–8.
25. Vadaparampil ST, Hutchins NM, Quinn GP. Reproductive health in the adolescent and young adult cancer patient: an innovative training program for oncology nurses. J Cancer Educ 2013;28:197–208.
26. Shekelle P, Woolf S, Grimshaw JM, et al. Developing clinical practice guidelines: reviewing, reporting, and publishing guidelines; updating guidelines; and the emerging issues of enhancing guideline implementability and accounting for comorbid conditions in guideline development. Implement Sci 2012;7:62.
27. Clayton JM, Adler JL, O’Callaghan A, et al. Intensive communication skills teaching for specialist training in palliative medicine: development and evaluation of an experiential workshop. J Palliat Med 2012;15:585–91.
28. Hymes DH. On communicative competence. In: Pride JB, Holmes J, editors. Sociolinguistics: selected readings. Harmondsworth: Penguin; 1972:269–93.
29. Asnani MR. Patient-physician communication. West Indian Med J 2009;58:357–61.
30. Clark PA. Medical practices’ sensitivity to patients’ needs: Opportunities and practices for improvement. J Ambulat Care Manage 2003;26:110–23.
31. Wanzer MB, Booth-Butterfield M, Gruber K. Perceptions of health care providers’ communication: Relationships between patient-centered communication and satisfaction. Health Care Commun 2004;16:363–84.
1. Bleyer AOLM, O’Leary M, Barr L, Ries LAG. Cancer epidemiology in older adolescents and young adults 15 to 29 years of age, including SEER incidence and survival: 1975–2000. Bethesda, MD: National Cancer Institute; 2006.
2. Ward E, DeSantis C, Robbins A, et al. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin 2014;64: 83–103.
3. Loren AW, Mangu PB, Beck LN, et al. Fertility preservation for patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 2013;31:2500–10.
4. Lee SJ, Schover LR, Partridge AH, et al. American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. J Clin Oncol 2006;24:2917–31.
5. Coccia P, Altman J, Bhatia S, et al. Adolescent and young adult (AYA) oncology version 1.2012. National Comprehensive Cancer Network; 2012.
6. Neuss MN, Malin JL, Chan S, et al. Measuring the improving quality of outpatient care in medical oncology practices in the United States. J Clin Oncol 2013;31:1471–7.
7. Quinn GP, Block RG, Clayman ML, et al. If you did not document it, it did not happen: rates of documentation of discussion of infertility risk in adolescent and young adult oncology patients’ medical records. J Oncol Pract 2015;11: 137–44.
8. Cope D. Patients’ and physicians’ experinces with sperm banking and infertility issues related to cancer treatment. Clin J Oncol Nurs 2002;6:293–5.
9. Vaartio-Rajalin H, Leino-Kilpi H. Nurses as patient advocates in oncology care: activities based on literature. Clin J Oncol Nurs. 2011;15:526–32.
10. King LM, Quinn GP, Vadaparampil ST, et al. Oncology nurses’ perceptions of barriers to discussion of fertility preservation with patients with cancer. Clin J Oncol Nurs 2008; 12:467–76.
11. Clayton HB, Vadaparampil ST, Quinn GP, et al. Trends in clinical practice and nurses’ attitudes about fertility preservation for pediatric patients with cancer. Oncol Nurs Forum 2008;35:449–55.
12. Vadaparampil ST, Clayton H, Quinn GP, et al. Pediatric oncology nurses’ attitudes related to discussing fertility preservation with pediatric cancer patients and their families. J Pediatr Oncol Nurs 2007;24:255–63.
13. Kotronoulas G, Papadopoulou C, Patiraki E. Nurses’ knowledge, attitudes, and practices regarding provision of sexual health care in patients with cancer: critical review of the evidence. Support Care Cancer 2009;17:479–501.
14. Reebals JF, Brown R, Buckner EB. Nurse practice issues regarding sperm banking in adolescent male cancer patients. J Pediatr Oncol Nurs 2006;23:182–8.
15. Goossens J, Delbaere I, Beeckman D, et al. Communication difficulties and the experience of loneliness in patients with cancer dealing with fertility issues: a qualitative study. Oncol Nurs Forum 2015;42:34–43.
16. Mustard LW. Improving patient satisfaction through the consistent use of scripting by the nursing staff. JONAS Healthc Law Ethics Regul 2003;5:68–72.
17. Kuiper RA. Integration of innovative clinical reasoning pedagogies into a baccalaureate nursing curriculum. Creat Nurs 2013;19:128–39.
18. Handel DA, Fu R, Daya M, et al. The use of scripting at triage and its impact on elopements. Acad Emerg Med 2010; 17:495–500.
19. Studer Q. Hardwiring excellence: purpose, worthwhile work, making a difference. Gulf Breeze, FL: Fire Starter Publishing; 2003.
20. Katona A, Kunkel E, Arfaa J, et al. Methodology for delivering feedback to neurology house staff on communication skills using AIDET (Acknowledge, Introduce, Duration, Explanation, Thank You). Neurology 2014;82(10 Suppl):P1–328.
21. Prestia A , Dyess S. Maximizing caring relationships between nursing assistants and patients: Care partners. J Nurs Admin 2012;42:144–7.
22. Fisher MJ. A brief intervention to improve emotion-focused communication between newly licensed pediatric nurses and parents [dissertation]. Indianapolis: Indiana University; 2012.
23. Baker SJ. Key words: a prescriptive approach to reducing patient anxiety and improving safety. J Emerg Nurs 2011; 37:571–4.
24. Shupe R. Using skills validation and verification techniques to hardwire staff behaviors. J Emerg Nurs 2013;39:364–8.
25. Vadaparampil ST, Hutchins NM, Quinn GP. Reproductive health in the adolescent and young adult cancer patient: an innovative training program for oncology nurses. J Cancer Educ 2013;28:197–208.
26. Shekelle P, Woolf S, Grimshaw JM, et al. Developing clinical practice guidelines: reviewing, reporting, and publishing guidelines; updating guidelines; and the emerging issues of enhancing guideline implementability and accounting for comorbid conditions in guideline development. Implement Sci 2012;7:62.
27. Clayton JM, Adler JL, O’Callaghan A, et al. Intensive communication skills teaching for specialist training in palliative medicine: development and evaluation of an experiential workshop. J Palliat Med 2012;15:585–91.
28. Hymes DH. On communicative competence. In: Pride JB, Holmes J, editors. Sociolinguistics: selected readings. Harmondsworth: Penguin; 1972:269–93.
29. Asnani MR. Patient-physician communication. West Indian Med J 2009;58:357–61.
30. Clark PA. Medical practices’ sensitivity to patients’ needs: Opportunities and practices for improvement. J Ambulat Care Manage 2003;26:110–23.
31. Wanzer MB, Booth-Butterfield M, Gruber K. Perceptions of health care providers’ communication: Relationships between patient-centered communication and satisfaction. Health Care Commun 2004;16:363–84.
Enhancing the Communication Skills of Critical Care Nurses: Focus on Prognosis and Goals of Care Discussions
From the University of California Irvine Health/Chao Family Comprehensive Cancer Center Orange, CA (Ms. Boyle) and the University of California San Francisco Medical Center, San Francisco, CA (Dr. Anderson).
Abstract
- Objective: To describe components of a unique interactive workshop focusing on the enhancement of critical care nurses’ communication skills within the realm of prognosis and goals of care discussions with family members and physicians.
- Methods: A series of one-day workshops were offered to critical care nurses practicing in the 5 University of California hospital settings. After workshop attendance, nurse participants were followed by workshop facilitators in their units to ensure new communication skills were being integrated into practice and to problem solve if barriers were met.
- Results: Improvement in nurses’ self-confidence in engaging in these discussions was seen. This confidence was sustained months following workshop participation.
- Conclusion: The combination of critical care nurse workshop participation that involved skill enhancement through role-playing, in combination with clinical follow-up with attendees, resulted in positive affirmation of nurse communication skills specific to prognosis and goals of care discussions with family members and physicians.
There is increasing evidence that in the absence of quality communication between professional caregivers and those they care for, negative outcomes may prevail, such as reduced patient/family satisfaction, lower health status awareness, and a decreased sense of being cared about and cared for [1–5]. Communication skill competency is a critical corollary of nursing practice. In the intensive care unit (ICU) setting, patients and families have cited skilled communication as a core element of high-quality care [3,6]. Proficiency in this realm enhances nurses’ understanding of the patient and family’s encounter with health care and provides a vehicle to gather information, inform, teach, and offer emotional support. Additionally, it identifies values, goals, health care preferences, worries and concerns, and facilitates the nurses’ coordination of care [7]. Despite this skill’s importance, however, it is generally not taught in basic education and until recently has been overlooked as a key competency [8,9].
Skilled communication in palliative and end-of-life care is pivotal for discussing prognosis and care planning. In the acute care setting this is particularly relevant as the majority of Americans die in hospitals versus their preferred site of home [10]. Additionally, 1 in 5 Americans die during or shortly after receiving care in an ICU [11]. Hence, while the ICU is a setting in which intensive effort to save lives is employed, it is also a setting where death frequently occurs. The complexity and highly emotive nature of critical care often results in family needs for information and support not being met [12]. A number of reasons for this occurrence have been proposed. In this paper, we will delineate barriers to critical care nurses’ involvement in prognosis and goals of care discussions, identify why nurse involvement in this communication is needed, describe a unique workshop exemplar with a sample role play that characterizes the workshop, and offer recommendations for colleagues interested in replicating similar education offerings.
Barriers to Communication
In the ICU, the sheer number of professionals families interact with may cause confusion. In particular, numerous medical consultants commonly offer opposing opinions. Additionally, each specialist may provide information that focuses on their area of expertise such that the “big picture” is not relayed to the patient and family. Emotional discomfort on the part of the health professional around discussions of poor prognosis, goals of care, and code status may prompt limiting discussion time with patients and families and even the avoidance of interpersonal exchanges [13–15]. Health professionals have also reported concern that end-of-life discussions will increase patient distress [16]. Among health care professionals, the subject of mortality may prompt personal anxiety, trigger unresolved grief, or fear that they will “become emotional” in front of the patient/family [7]. Lack of knowledge about cultural and religious norms has been cited as a barrier, as has time constraints [17,18]. Most frequently, inadequate or absent communication skill training is noted as a significant barrier [19,20]. Many ICU nurses also report feeling marginalized due their exclusion from goals of care and decision-making discussions with patients and families they know well [21,22].
Nurses As Key Palliative Care Communicators
Education efforts that foster communication proficiency during serious illness have traditionally focused on training physicians. Recently, nursing has become a focus of communication skill enhancement in recognition of nurses’ intense and protracted interactions with patients and families in the acute care setting. Nurses are the ‘constant’ in the patient and family’s journey through the fragmented health care system [21,23]. They often have the best knowledge of, and strongest relationship with, the family and often have had extensive discussions with them about their loved one’s status [24]. Nurses are aware of the patients’ symptom experiences and are privy to valuable information about the concerns and priorities of patients and families [12]. Additionally, having the most continuous presence, nurses have seen and heard interactions with clinicians from numerous disciplines. Nurses are the most visible, constant resource for patient and family education, information and support, and thus they perceive one of their most important roles to be that of advocate for the patient and family [20,21].
Communication Training Programs for Critical Care Nurses
Education is critical to enhance communication skills within palliative care [7,15,17,20,21,24]. The preferred teaching style within this realm is role play, where skills can be practiced and the affective component of engaging in sensitive discussions can be addressed [25–27]. Role play also demonstrates firsthand the importance of nonverbal communication (eg, body language, proximity, use of gestures, tone of voice) [7,20] and facilitates nurses’ gaining a sense of comfort with wordless communication [18].
Communication skills training programs have been designed to provide bedside critical care nurses with the tools they need to be active participants in discussions of prognosis, goals of care, and palliative care with families and physicians [27,28]. These programs have demonstrated improvement in nurses’ confidence to engage in key palliative care-related discussions. Essential elements of these programs include (1) delineation of the role of the bedside nurse in palliative care communication; (2) presentation and learner-centered practice of communication skills using role play; and (3) a reflection session focused on self-care and sustainability.
Across the 5 academic University of California medical centers (San Francisco, Davis, Los Angeles, Irvine, and San Diego), a communication training program based on this work has been implemented [29]. The one-day workshop, entitled IMPACT-ICU (Integrating Multidisciplinary Palliative Care into the ICU), has taught a total of 527 critical care nurses across the 5 centers. In addition to classroom training, the IMPACT-ICU program also includes proactive specialty palliative nursing support for bedside nurses by facilitating the availability of palliative care advanced practice nurses and nurse educators resources. This support helps nurses to apply the skills learned in the workshop in their practice. During rounds at the bedside, the nurse resources coach the bedside staff on the “how” and “when” of addressing palliative care needs. Education and support on a range of topics are offered, including clarifying goals and interventions provided by palliative care teams, the specifics of how to provide family emotional support and delivery of understandable information, the assessment and management of symptoms distress, and the nurses’ role in organizing and participating in family meetings. Case-specific consultations are also offered that address how to interface with resistant medical staff. The importance of nurse documentation of these varied exchanges is also emphasized.
IMPACT-ICU Workshop
A maximum of 15 nurses participate in each 8-hour workshop. The session begins with introductions and small group discussions about what the participants perceive to be the greatest barriers to goals of care discussions and fostering patient/family decision-making in the ICU. Participants are also asked to reflect on what they want to learn as a result of their workshop attendance.
A short didactic session then reviews the definition of palliative care and its core components, addresses the nurses’ role in communication within palliative care, a social worker’s perspective of what it is like to be a family member in the ICU, and the outline of the day. This includes delineation of expectations for involvement within the role plays and the various roles to be enacted. An emphasis is placed on the workshop being a safe place to explore and trial skills with the support of colleagues, and that practice is the optimum way to integrate communication expertise into the nurses’ skill set.
The “4 Cs” serves as the instructional basis for nurse communication skill enhancement [27]. This model outlines 4 key nursing roles in optimizing communication within palliative care:
Convening: Making sure multidisciplinary patient/family/clinician communication occurs.
Checking: Identifying the patient and family needs for information; ensuring that patients and families clearly receive desired information; ensuring that clinicians understand patient and family perspectives.
Caring: Naming emotions and responding to feeling.
Continuing: Following up after discussions to clarify and reinforce information and provide support.
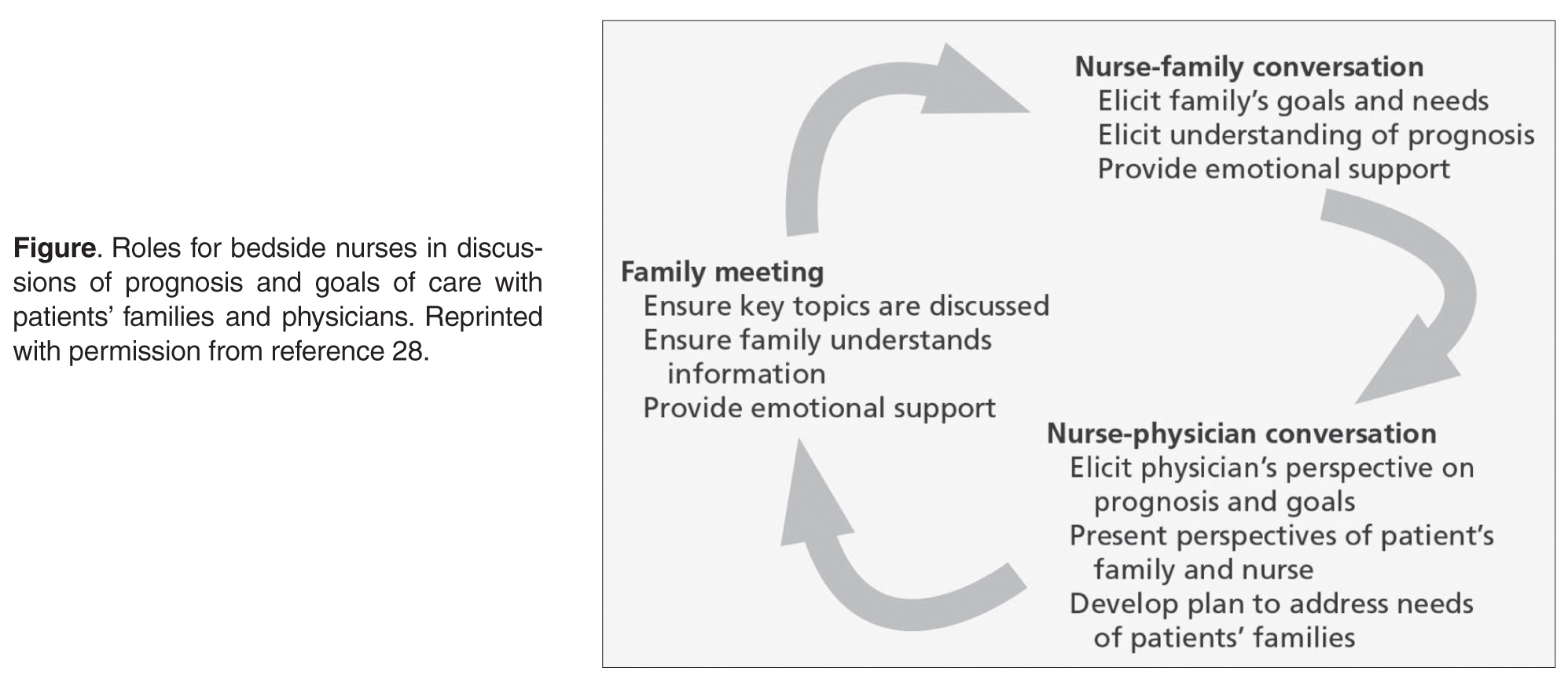
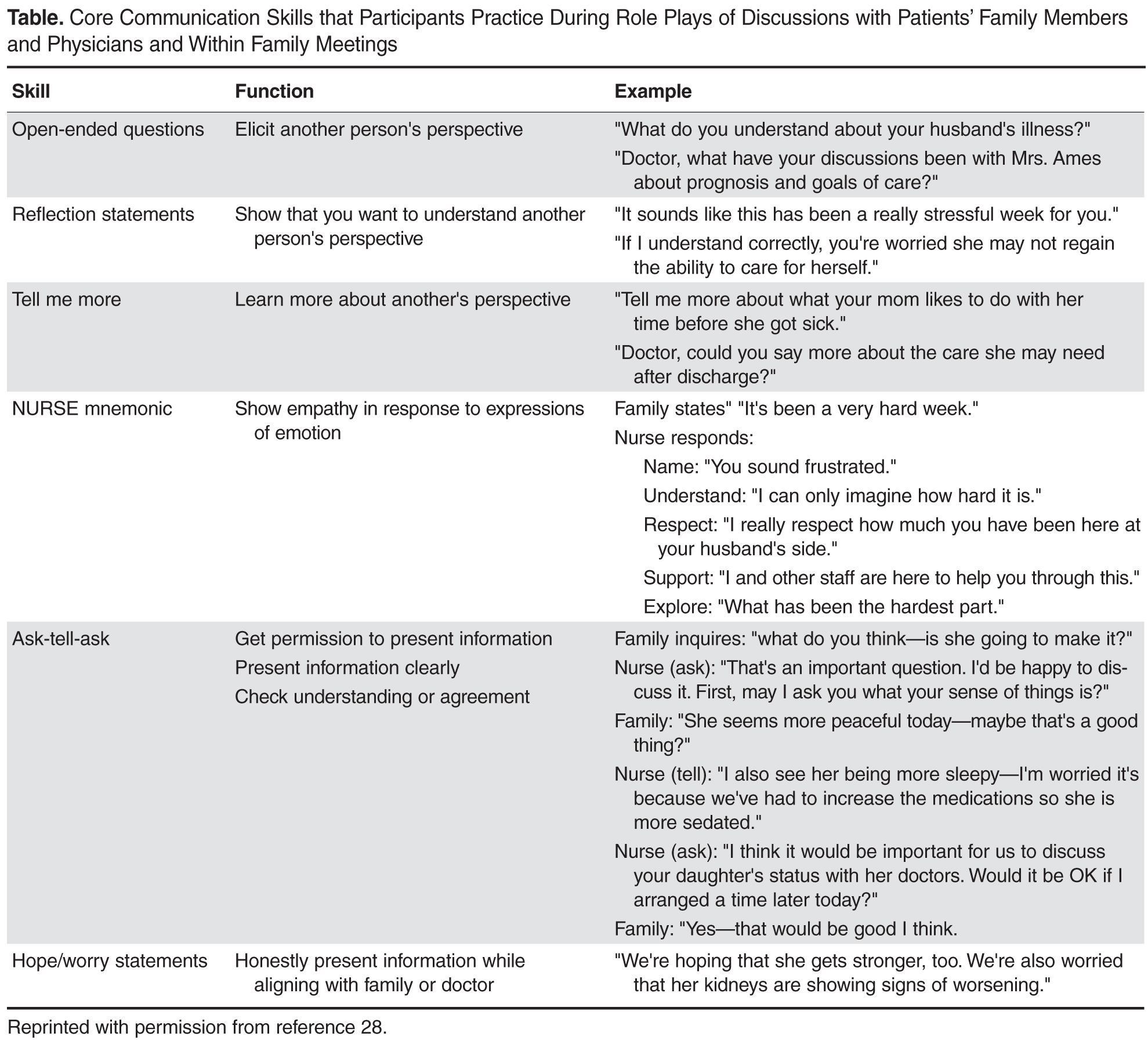
Sample Role Play
Facilitator: So our first role play is focused on eliciting patient and family perspectives and needs. I need a learner and someone to play the role of the family member.
Learner: I’ll give it a try.
Facilitator: Lisa, you’re going to do great. Who wants to play the family member?
Workshop Participant: I’ll do it.
Facilitator: So Mary (who has agreed to play the role of the wife), why don’t you read us the scenario. (She reads it out loud to the group).
Facilitator: Lisa, as the nurse, I want you to look at your guide and tell me what your goal is for this conversation with Mrs. Ames and then which skill you want to practice.
Learner: I think I want to try eliciting the patient and family’s needs for information and I’ll try “Tell Me More” statements.
Facilitator: Alright. So remember Lisa, if you feel the conversation isn’t going well, you can call a “time out.” I can do this as well if I feel you need to start over. I’ll also call a time out when I feel you have met your goal. Sound OK? Mary, do you have any questions playing the part of Mrs. Ames?
Wife Role: Well, how hard should I make this for her? Should I be one of those “difficult” family members?
Facilitator: Our goal here is not to “stump” you or make it particularly difficult. We want you to try out these skills and get a sense of your “comfort zone.” So let’s start with some basic communication skills, OK?
Wife Role: Alright.
Facilitator: Why don’t we set the stage, such that Lisa, you are Mr. Ames’ nurse assessing him at the start of your shift, when Mrs. Ames enters. This is the first time you have taken care of him. The night nurse has told you that he has been requiring increasing ventilator support and his renal function is declining. Per Mrs. Ames’ request, the night nurse called her to let her know how he was doing and Mrs. Ames told her she would be in shortly.
Wife Role: (nervously enters the room and grasps her husband’s hand and looks at the nurse). How’s he doing? Is he better? The night nurse called me and I was so worried I rushed over here.
Learner: (Turns to Mrs. Ames and extends her hand). Are you Mrs. Ames? I’m Lisa and I am going to be taking care of Mr. Ames today. Let me just finish my assessment and how about we talk then? Will that be OK? It will be just a few minutes.
Wife Role: Alright, I’ll be in the waiting area but please come get me as soon as you can.
Learner: I will. (Nurse then shortly comes into the waiting area and asks Mrs. Ames to come back into the ICU where she invites her to sit just outside Mr. Ames’ room). Mrs. Ames, how are you doing? This must be so stressful for you, having your husband in the ICU.
Wife Role: It’s awful. He’s never been in the hospital before this and look at him, all hooked up to machines. I’m so worried. He seems to be getting worse instead of better.
Learner: What’s your understanding of what is going on?
Wife Role: I really don’t know. One doctor comes in and says one thing and then another comes in and tells me the opposite. I’m so confused I don’t know what to think.
Learner: Would having a better idea of his condition from the doctors who are treating him help you have a better understanding?
Wife Role: Oh, yes, but they always seem in such a hurry.
Learner: What exactly would you like to know?
Wife: Well, I want to know when he can get off that breathing machine because we have been planning to go to our son’s house for Thanksgiving.
Facilitator: Time out. Lisa, did you meet your conversation goal?
Learner: Um, I’m not sure, I guess so.
Facilitator: (Turns to Observers). What do you think, did she meet her goal?
Observer: Yes, she determined Mrs. Ames’ need for more information and she asked her what she wanted to know exactly.
Facilitator: What else did we see Lisa do to enhance communication with Mrs. Ames?
Observer: Well, when Mrs. Ames rushed into the room and asked her for information, Lisa didn’t just jump in and spout out values for the ventilator and his output. She took the time to introduce herself and de-escalate Mrs. Ames’ anxiety and she followed up on her promise to come get her in the waiting room as soon as she could.
Facilitator: Why do you think was important?
Observer: It helps establish trust.
Facilitator: Did Lisa use the skill she wanted to try out?
Observer: Yes.
Facilitator: How do you know? What did you hear her say?
Observer: She said, “What’s your understanding of what is going on with Mr. Ames?”
Facilitator: Absolutely. Great job, Lisa. And who wants to take a guess at how long Lisa’s exchange with Mrs. Ames took?
Observer: Less than two minutes?
Facilitator: That’s right. So just as you consider how long it takes, and how proficient you are, in starting an IV or inserting a Foley catheter, when you have a goal in mind and have practiced the skills to do it well, any skill can be mastered.
Feedback
Participants in the workshops uniformly report an enhanced sense of self-confidence in their palliative care communication skills as a result of their participation [29]. Key to the success of the workshop is the ongoing contact by the workshop facilitators with participants. Rounding is routinely planned such that each participant is visited weekly by a workshop facilitator in their clinical area to determine if the bedside nurse has practiced the new skills and if so, how the interaction transpired. Positive feedback is given for attempts to engage in new behaviors and participants are reminded that with any new skill, repetitive trials are necessary to foster success.
Lessons Learned and Next Steps
One of our major lessons learned was recognizing that it was difficult for many critical care nurses to practice the new communication skills. Nurses are trained to fix problems and perform medico-technical tasks; “listening” has not always been recognized as real work [18]. We needed to reinforce that skills like eliciting another’s perspective or making reflection statements are equally important to those associated with behavioral/technical proficiency.
While our program has been successful, we recognize that the next step in fostering ideal palliative care communication is to provide education within an interdisciplinary context. We recommend that colleagues interested in replicating this or a similar education intervention, survey nurse participants prior to and following workshop participation to measure attitudes, self confidence and perceived barriers over time [30]. We hope to translate our positive experience into a program that engages multiple professionals in the enhancement of optimum palliative care communication proficiency.
Corresponding author: Deborah A. Boyle MSN, RN, AOCNS, Department of Nursing Quality, Research and Education, University of California, Irvine Health, 101 The City Drive, Bldg 22A, Room 3104, Orange, CA 92868.
1. Leung JM, Udris EM, Uman J, et al. The effect of end-of-life discussions on perceived quality of care and health status among patients with COPD. Chest 2012;142:128–33.
2. Osborn TR, Curtis JR, Nielsen EL, et al. Identifying elements of ICU care that families report as important but unsatisfactory: decision-making, control and ICU atmosphere. Chest 2012;142:1185–92.
3. Nelson JE, Puntillo K, Pronovost PJ, et al. In their own words: patients and families define high-quality palliative care in the ICU. Crit Care Med 2010;38:808–18.
4. Nels W, Gabrijel S, Kiss S, et al. Communication skill training significantly improves lung cancer patients understanding. J Palliat Care Med 2014;4:182.
5. Van Vliet LM, Epstein AS. Current state of the art and science of patient-clinician communication in progressive disease: patients’ need to know and feel known. J Clin Oncol 2014;32:3474-8.
6. Troug RD, Campbell ML, Curtis JR, et al. Recommendations for end of life care in the intensive care unit: a consensus statement by the American College of Critical Care Medicine. Crit Care Med 2008;36:953–63.
7. Dahlin CM, Wittenberg E. Communication in palliative care. In: Ferrell BR, Coyle N, Paice J, editors. Oxford textbook of palliative nursing. 4th ed. Oxford: Oxford University Press; 2014:81–109.
8. Baer L, Weinstein E. Improving oncology nurses’ communication skills for difficult conversations. Clin J Oncol Nurs 2013;17:E45–E51.
9. Treece PD. Communication in the intensive care unit about end of life care. AACN Adv Crit Care 2007;18:406–14.
10. Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end of life care at the last place of care. JAMA 2004;291:88–92.
11. Angus DC, Barnato AE, Linde-Zwirble WT, et al. Robert Wood Johnson Foundation ICU End-of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med 2004;32:638–43.
12. Hamric AB, Blackhall LJ. Nurse-physician perspectives on the care of dying patients in intensive care units: collaboration, moral distress, and ethical climate. Crit Care Med 2007;35:422–9.
13. Back AL, Trinidad SB, Hopley EK, Edwards KA. Reframing the goals of care conversation: “We’re in a different place.” J Palliat Med 2014;17:1010–24.
14. Aslakson RA, Wyskiel R, Thornton I, et al. Nurse perceived barriers to effective communication regarding prognosis and optimal end of life care for surgical ICU patients: a qualitative exploration. J Palliat Med 2012;15:910–5.
15. Erickson J. Bedside nurse involvement in end of life decision-making. Dimens Crit Care Nurs 2013;32:65–8.
16. Bernacki RE, Block SD for the American College of Physicians High Value Care Task Force. Communication about serious illness care goals: a review and synthesis of best practices. JAMA Intern Med 2014;174:1994–2003.
17. You JJ, Downar J, Fowler RA, et al. Barriers to goals of care discussion with ‘seriously’ ill hospitalized patients and their families: a multicenter survey of clinicians. JAMA Intern Med 2015;175:549–56.
18. Strang S, Henoch I, Danielson E, et al. Communication about existential issues with patients close to death: nurses’ reflections on content, process, and meaning. Psychooncology 2014;23:562–8.
19. Slatore CG, Hensen L, Gauzine L, et al. Communication by nurses in the intensive care unit: qualitative analysis of domains in patient-centered care. Am J Crit Care 2012;21:410–8.
20. Wittenberg-Lyles E, Goldsmith J, Platt CS. Palliative care communication. Sem Oncol Nurs 2014;30:280–6.
21. Fox MY. Improving communication with patients and families in the ICU: palliative care strategies for intensive care unit nurses. J Hospice Palliat Nurs 2014;16:93–8.
22. Beckstrand RL, Callister LC, Kirchhoff KT. Providing a ‘good death’: critical care nurses’ suggestions for improving end of life care. Am J Crit Care 2006;15:38–45.
23. Peereboom K, Coyle N. Facilitating goals of care discus.sions for patients with life-limiting disease: communication strategies for nurses. J Hospice Palliat Nurs 2012; 14:251–8.
24. Nelson JE, Cortez TB, Curtis JR, et al. Integrating palliative care in the ICU: the nurse in the leading role. J Hospice Palliat Nurs 2011;13:89–94.
25. Jors K, Seibel K, Bardenheuer H, et al. Education in end of life care: what do experienced professionals find important? J Cancer Educ 2015 March 15.
26. Roze des Ordons AL, Sharma N, Heyland DK, et al. Strategies for effective goals of care discussions and decision-making: perspective from a multi-centre survey of Canadian hospital-based health care providers. BMC Palliat Care 2015;14:38.
27. Krimshtein NS, Luhrs CA, Puntillo KA, et al. Training nurses for interdisciplinary communication with families in the ICU. J Palliat Med 2011;14:1325–32.
28. Milic MM, Puntillo K, Turner K, et al. Communicating with patients’ families and physicians about prognosis and goals of care. Am J Crit Care 2015;24:e56–e64.
29. Anderson W, Puntillo K, Barbour S, et al. The IMPACT-ICU Project: expanding palliative care nursing across University of California Centers ICUs to advance palliative care. Center to Advance Palliative Care (CAPC) national seminar. Nov 7–9, 2013. Dallas, TX.
30. Anderson WG, Puntillo K, Boyle D, et al. ICU bedside nurses’ involvement in palliative care communication: a multicenter survey. J Pain Symptom Manage. In press.
From the University of California Irvine Health/Chao Family Comprehensive Cancer Center Orange, CA (Ms. Boyle) and the University of California San Francisco Medical Center, San Francisco, CA (Dr. Anderson).
Abstract
- Objective: To describe components of a unique interactive workshop focusing on the enhancement of critical care nurses’ communication skills within the realm of prognosis and goals of care discussions with family members and physicians.
- Methods: A series of one-day workshops were offered to critical care nurses practicing in the 5 University of California hospital settings. After workshop attendance, nurse participants were followed by workshop facilitators in their units to ensure new communication skills were being integrated into practice and to problem solve if barriers were met.
- Results: Improvement in nurses’ self-confidence in engaging in these discussions was seen. This confidence was sustained months following workshop participation.
- Conclusion: The combination of critical care nurse workshop participation that involved skill enhancement through role-playing, in combination with clinical follow-up with attendees, resulted in positive affirmation of nurse communication skills specific to prognosis and goals of care discussions with family members and physicians.
There is increasing evidence that in the absence of quality communication between professional caregivers and those they care for, negative outcomes may prevail, such as reduced patient/family satisfaction, lower health status awareness, and a decreased sense of being cared about and cared for [1–5]. Communication skill competency is a critical corollary of nursing practice. In the intensive care unit (ICU) setting, patients and families have cited skilled communication as a core element of high-quality care [3,6]. Proficiency in this realm enhances nurses’ understanding of the patient and family’s encounter with health care and provides a vehicle to gather information, inform, teach, and offer emotional support. Additionally, it identifies values, goals, health care preferences, worries and concerns, and facilitates the nurses’ coordination of care [7]. Despite this skill’s importance, however, it is generally not taught in basic education and until recently has been overlooked as a key competency [8,9].
Skilled communication in palliative and end-of-life care is pivotal for discussing prognosis and care planning. In the acute care setting this is particularly relevant as the majority of Americans die in hospitals versus their preferred site of home [10]. Additionally, 1 in 5 Americans die during or shortly after receiving care in an ICU [11]. Hence, while the ICU is a setting in which intensive effort to save lives is employed, it is also a setting where death frequently occurs. The complexity and highly emotive nature of critical care often results in family needs for information and support not being met [12]. A number of reasons for this occurrence have been proposed. In this paper, we will delineate barriers to critical care nurses’ involvement in prognosis and goals of care discussions, identify why nurse involvement in this communication is needed, describe a unique workshop exemplar with a sample role play that characterizes the workshop, and offer recommendations for colleagues interested in replicating similar education offerings.
Barriers to Communication
In the ICU, the sheer number of professionals families interact with may cause confusion. In particular, numerous medical consultants commonly offer opposing opinions. Additionally, each specialist may provide information that focuses on their area of expertise such that the “big picture” is not relayed to the patient and family. Emotional discomfort on the part of the health professional around discussions of poor prognosis, goals of care, and code status may prompt limiting discussion time with patients and families and even the avoidance of interpersonal exchanges [13–15]. Health professionals have also reported concern that end-of-life discussions will increase patient distress [16]. Among health care professionals, the subject of mortality may prompt personal anxiety, trigger unresolved grief, or fear that they will “become emotional” in front of the patient/family [7]. Lack of knowledge about cultural and religious norms has been cited as a barrier, as has time constraints [17,18]. Most frequently, inadequate or absent communication skill training is noted as a significant barrier [19,20]. Many ICU nurses also report feeling marginalized due their exclusion from goals of care and decision-making discussions with patients and families they know well [21,22].
Nurses As Key Palliative Care Communicators
Education efforts that foster communication proficiency during serious illness have traditionally focused on training physicians. Recently, nursing has become a focus of communication skill enhancement in recognition of nurses’ intense and protracted interactions with patients and families in the acute care setting. Nurses are the ‘constant’ in the patient and family’s journey through the fragmented health care system [21,23]. They often have the best knowledge of, and strongest relationship with, the family and often have had extensive discussions with them about their loved one’s status [24]. Nurses are aware of the patients’ symptom experiences and are privy to valuable information about the concerns and priorities of patients and families [12]. Additionally, having the most continuous presence, nurses have seen and heard interactions with clinicians from numerous disciplines. Nurses are the most visible, constant resource for patient and family education, information and support, and thus they perceive one of their most important roles to be that of advocate for the patient and family [20,21].
Communication Training Programs for Critical Care Nurses
Education is critical to enhance communication skills within palliative care [7,15,17,20,21,24]. The preferred teaching style within this realm is role play, where skills can be practiced and the affective component of engaging in sensitive discussions can be addressed [25–27]. Role play also demonstrates firsthand the importance of nonverbal communication (eg, body language, proximity, use of gestures, tone of voice) [7,20] and facilitates nurses’ gaining a sense of comfort with wordless communication [18].
Communication skills training programs have been designed to provide bedside critical care nurses with the tools they need to be active participants in discussions of prognosis, goals of care, and palliative care with families and physicians [27,28]. These programs have demonstrated improvement in nurses’ confidence to engage in key palliative care-related discussions. Essential elements of these programs include (1) delineation of the role of the bedside nurse in palliative care communication; (2) presentation and learner-centered practice of communication skills using role play; and (3) a reflection session focused on self-care and sustainability.
Across the 5 academic University of California medical centers (San Francisco, Davis, Los Angeles, Irvine, and San Diego), a communication training program based on this work has been implemented [29]. The one-day workshop, entitled IMPACT-ICU (Integrating Multidisciplinary Palliative Care into the ICU), has taught a total of 527 critical care nurses across the 5 centers. In addition to classroom training, the IMPACT-ICU program also includes proactive specialty palliative nursing support for bedside nurses by facilitating the availability of palliative care advanced practice nurses and nurse educators resources. This support helps nurses to apply the skills learned in the workshop in their practice. During rounds at the bedside, the nurse resources coach the bedside staff on the “how” and “when” of addressing palliative care needs. Education and support on a range of topics are offered, including clarifying goals and interventions provided by palliative care teams, the specifics of how to provide family emotional support and delivery of understandable information, the assessment and management of symptoms distress, and the nurses’ role in organizing and participating in family meetings. Case-specific consultations are also offered that address how to interface with resistant medical staff. The importance of nurse documentation of these varied exchanges is also emphasized.
IMPACT-ICU Workshop
A maximum of 15 nurses participate in each 8-hour workshop. The session begins with introductions and small group discussions about what the participants perceive to be the greatest barriers to goals of care discussions and fostering patient/family decision-making in the ICU. Participants are also asked to reflect on what they want to learn as a result of their workshop attendance.
A short didactic session then reviews the definition of palliative care and its core components, addresses the nurses’ role in communication within palliative care, a social worker’s perspective of what it is like to be a family member in the ICU, and the outline of the day. This includes delineation of expectations for involvement within the role plays and the various roles to be enacted. An emphasis is placed on the workshop being a safe place to explore and trial skills with the support of colleagues, and that practice is the optimum way to integrate communication expertise into the nurses’ skill set.
The “4 Cs” serves as the instructional basis for nurse communication skill enhancement [27]. This model outlines 4 key nursing roles in optimizing communication within palliative care:
Convening: Making sure multidisciplinary patient/family/clinician communication occurs.
Checking: Identifying the patient and family needs for information; ensuring that patients and families clearly receive desired information; ensuring that clinicians understand patient and family perspectives.
Caring: Naming emotions and responding to feeling.
Continuing: Following up after discussions to clarify and reinforce information and provide support.
Sample Role Play
Facilitator: So our first role play is focused on eliciting patient and family perspectives and needs. I need a learner and someone to play the role of the family member.
Learner: I’ll give it a try.
Facilitator: Lisa, you’re going to do great. Who wants to play the family member?
Workshop Participant: I’ll do it.
Facilitator: So Mary (who has agreed to play the role of the wife), why don’t you read us the scenario. (She reads it out loud to the group).
Facilitator: Lisa, as the nurse, I want you to look at your guide and tell me what your goal is for this conversation with Mrs. Ames and then which skill you want to practice.
Learner: I think I want to try eliciting the patient and family’s needs for information and I’ll try “Tell Me More” statements.
Facilitator: Alright. So remember Lisa, if you feel the conversation isn’t going well, you can call a “time out.” I can do this as well if I feel you need to start over. I’ll also call a time out when I feel you have met your goal. Sound OK? Mary, do you have any questions playing the part of Mrs. Ames?
Wife Role: Well, how hard should I make this for her? Should I be one of those “difficult” family members?
Facilitator: Our goal here is not to “stump” you or make it particularly difficult. We want you to try out these skills and get a sense of your “comfort zone.” So let’s start with some basic communication skills, OK?
Wife Role: Alright.
Facilitator: Why don’t we set the stage, such that Lisa, you are Mr. Ames’ nurse assessing him at the start of your shift, when Mrs. Ames enters. This is the first time you have taken care of him. The night nurse has told you that he has been requiring increasing ventilator support and his renal function is declining. Per Mrs. Ames’ request, the night nurse called her to let her know how he was doing and Mrs. Ames told her she would be in shortly.
Wife Role: (nervously enters the room and grasps her husband’s hand and looks at the nurse). How’s he doing? Is he better? The night nurse called me and I was so worried I rushed over here.
Learner: (Turns to Mrs. Ames and extends her hand). Are you Mrs. Ames? I’m Lisa and I am going to be taking care of Mr. Ames today. Let me just finish my assessment and how about we talk then? Will that be OK? It will be just a few minutes.
Wife Role: Alright, I’ll be in the waiting area but please come get me as soon as you can.
Learner: I will. (Nurse then shortly comes into the waiting area and asks Mrs. Ames to come back into the ICU where she invites her to sit just outside Mr. Ames’ room). Mrs. Ames, how are you doing? This must be so stressful for you, having your husband in the ICU.
Wife Role: It’s awful. He’s never been in the hospital before this and look at him, all hooked up to machines. I’m so worried. He seems to be getting worse instead of better.
Learner: What’s your understanding of what is going on?
Wife Role: I really don’t know. One doctor comes in and says one thing and then another comes in and tells me the opposite. I’m so confused I don’t know what to think.
Learner: Would having a better idea of his condition from the doctors who are treating him help you have a better understanding?
Wife Role: Oh, yes, but they always seem in such a hurry.
Learner: What exactly would you like to know?
Wife: Well, I want to know when he can get off that breathing machine because we have been planning to go to our son’s house for Thanksgiving.
Facilitator: Time out. Lisa, did you meet your conversation goal?
Learner: Um, I’m not sure, I guess so.
Facilitator: (Turns to Observers). What do you think, did she meet her goal?
Observer: Yes, she determined Mrs. Ames’ need for more information and she asked her what she wanted to know exactly.
Facilitator: What else did we see Lisa do to enhance communication with Mrs. Ames?
Observer: Well, when Mrs. Ames rushed into the room and asked her for information, Lisa didn’t just jump in and spout out values for the ventilator and his output. She took the time to introduce herself and de-escalate Mrs. Ames’ anxiety and she followed up on her promise to come get her in the waiting room as soon as she could.
Facilitator: Why do you think was important?
Observer: It helps establish trust.
Facilitator: Did Lisa use the skill she wanted to try out?
Observer: Yes.
Facilitator: How do you know? What did you hear her say?
Observer: She said, “What’s your understanding of what is going on with Mr. Ames?”
Facilitator: Absolutely. Great job, Lisa. And who wants to take a guess at how long Lisa’s exchange with Mrs. Ames took?
Observer: Less than two minutes?
Facilitator: That’s right. So just as you consider how long it takes, and how proficient you are, in starting an IV or inserting a Foley catheter, when you have a goal in mind and have practiced the skills to do it well, any skill can be mastered.
Feedback
Participants in the workshops uniformly report an enhanced sense of self-confidence in their palliative care communication skills as a result of their participation [29]. Key to the success of the workshop is the ongoing contact by the workshop facilitators with participants. Rounding is routinely planned such that each participant is visited weekly by a workshop facilitator in their clinical area to determine if the bedside nurse has practiced the new skills and if so, how the interaction transpired. Positive feedback is given for attempts to engage in new behaviors and participants are reminded that with any new skill, repetitive trials are necessary to foster success.
Lessons Learned and Next Steps
One of our major lessons learned was recognizing that it was difficult for many critical care nurses to practice the new communication skills. Nurses are trained to fix problems and perform medico-technical tasks; “listening” has not always been recognized as real work [18]. We needed to reinforce that skills like eliciting another’s perspective or making reflection statements are equally important to those associated with behavioral/technical proficiency.
While our program has been successful, we recognize that the next step in fostering ideal palliative care communication is to provide education within an interdisciplinary context. We recommend that colleagues interested in replicating this or a similar education intervention, survey nurse participants prior to and following workshop participation to measure attitudes, self confidence and perceived barriers over time [30]. We hope to translate our positive experience into a program that engages multiple professionals in the enhancement of optimum palliative care communication proficiency.
Corresponding author: Deborah A. Boyle MSN, RN, AOCNS, Department of Nursing Quality, Research and Education, University of California, Irvine Health, 101 The City Drive, Bldg 22A, Room 3104, Orange, CA 92868.
From the University of California Irvine Health/Chao Family Comprehensive Cancer Center Orange, CA (Ms. Boyle) and the University of California San Francisco Medical Center, San Francisco, CA (Dr. Anderson).
Abstract
- Objective: To describe components of a unique interactive workshop focusing on the enhancement of critical care nurses’ communication skills within the realm of prognosis and goals of care discussions with family members and physicians.
- Methods: A series of one-day workshops were offered to critical care nurses practicing in the 5 University of California hospital settings. After workshop attendance, nurse participants were followed by workshop facilitators in their units to ensure new communication skills were being integrated into practice and to problem solve if barriers were met.
- Results: Improvement in nurses’ self-confidence in engaging in these discussions was seen. This confidence was sustained months following workshop participation.
- Conclusion: The combination of critical care nurse workshop participation that involved skill enhancement through role-playing, in combination with clinical follow-up with attendees, resulted in positive affirmation of nurse communication skills specific to prognosis and goals of care discussions with family members and physicians.
There is increasing evidence that in the absence of quality communication between professional caregivers and those they care for, negative outcomes may prevail, such as reduced patient/family satisfaction, lower health status awareness, and a decreased sense of being cared about and cared for [1–5]. Communication skill competency is a critical corollary of nursing practice. In the intensive care unit (ICU) setting, patients and families have cited skilled communication as a core element of high-quality care [3,6]. Proficiency in this realm enhances nurses’ understanding of the patient and family’s encounter with health care and provides a vehicle to gather information, inform, teach, and offer emotional support. Additionally, it identifies values, goals, health care preferences, worries and concerns, and facilitates the nurses’ coordination of care [7]. Despite this skill’s importance, however, it is generally not taught in basic education and until recently has been overlooked as a key competency [8,9].
Skilled communication in palliative and end-of-life care is pivotal for discussing prognosis and care planning. In the acute care setting this is particularly relevant as the majority of Americans die in hospitals versus their preferred site of home [10]. Additionally, 1 in 5 Americans die during or shortly after receiving care in an ICU [11]. Hence, while the ICU is a setting in which intensive effort to save lives is employed, it is also a setting where death frequently occurs. The complexity and highly emotive nature of critical care often results in family needs for information and support not being met [12]. A number of reasons for this occurrence have been proposed. In this paper, we will delineate barriers to critical care nurses’ involvement in prognosis and goals of care discussions, identify why nurse involvement in this communication is needed, describe a unique workshop exemplar with a sample role play that characterizes the workshop, and offer recommendations for colleagues interested in replicating similar education offerings.
Barriers to Communication
In the ICU, the sheer number of professionals families interact with may cause confusion. In particular, numerous medical consultants commonly offer opposing opinions. Additionally, each specialist may provide information that focuses on their area of expertise such that the “big picture” is not relayed to the patient and family. Emotional discomfort on the part of the health professional around discussions of poor prognosis, goals of care, and code status may prompt limiting discussion time with patients and families and even the avoidance of interpersonal exchanges [13–15]. Health professionals have also reported concern that end-of-life discussions will increase patient distress [16]. Among health care professionals, the subject of mortality may prompt personal anxiety, trigger unresolved grief, or fear that they will “become emotional” in front of the patient/family [7]. Lack of knowledge about cultural and religious norms has been cited as a barrier, as has time constraints [17,18]. Most frequently, inadequate or absent communication skill training is noted as a significant barrier [19,20]. Many ICU nurses also report feeling marginalized due their exclusion from goals of care and decision-making discussions with patients and families they know well [21,22].
Nurses As Key Palliative Care Communicators
Education efforts that foster communication proficiency during serious illness have traditionally focused on training physicians. Recently, nursing has become a focus of communication skill enhancement in recognition of nurses’ intense and protracted interactions with patients and families in the acute care setting. Nurses are the ‘constant’ in the patient and family’s journey through the fragmented health care system [21,23]. They often have the best knowledge of, and strongest relationship with, the family and often have had extensive discussions with them about their loved one’s status [24]. Nurses are aware of the patients’ symptom experiences and are privy to valuable information about the concerns and priorities of patients and families [12]. Additionally, having the most continuous presence, nurses have seen and heard interactions with clinicians from numerous disciplines. Nurses are the most visible, constant resource for patient and family education, information and support, and thus they perceive one of their most important roles to be that of advocate for the patient and family [20,21].
Communication Training Programs for Critical Care Nurses
Education is critical to enhance communication skills within palliative care [7,15,17,20,21,24]. The preferred teaching style within this realm is role play, where skills can be practiced and the affective component of engaging in sensitive discussions can be addressed [25–27]. Role play also demonstrates firsthand the importance of nonverbal communication (eg, body language, proximity, use of gestures, tone of voice) [7,20] and facilitates nurses’ gaining a sense of comfort with wordless communication [18].
Communication skills training programs have been designed to provide bedside critical care nurses with the tools they need to be active participants in discussions of prognosis, goals of care, and palliative care with families and physicians [27,28]. These programs have demonstrated improvement in nurses’ confidence to engage in key palliative care-related discussions. Essential elements of these programs include (1) delineation of the role of the bedside nurse in palliative care communication; (2) presentation and learner-centered practice of communication skills using role play; and (3) a reflection session focused on self-care and sustainability.
Across the 5 academic University of California medical centers (San Francisco, Davis, Los Angeles, Irvine, and San Diego), a communication training program based on this work has been implemented [29]. The one-day workshop, entitled IMPACT-ICU (Integrating Multidisciplinary Palliative Care into the ICU), has taught a total of 527 critical care nurses across the 5 centers. In addition to classroom training, the IMPACT-ICU program also includes proactive specialty palliative nursing support for bedside nurses by facilitating the availability of palliative care advanced practice nurses and nurse educators resources. This support helps nurses to apply the skills learned in the workshop in their practice. During rounds at the bedside, the nurse resources coach the bedside staff on the “how” and “when” of addressing palliative care needs. Education and support on a range of topics are offered, including clarifying goals and interventions provided by palliative care teams, the specifics of how to provide family emotional support and delivery of understandable information, the assessment and management of symptoms distress, and the nurses’ role in organizing and participating in family meetings. Case-specific consultations are also offered that address how to interface with resistant medical staff. The importance of nurse documentation of these varied exchanges is also emphasized.
IMPACT-ICU Workshop
A maximum of 15 nurses participate in each 8-hour workshop. The session begins with introductions and small group discussions about what the participants perceive to be the greatest barriers to goals of care discussions and fostering patient/family decision-making in the ICU. Participants are also asked to reflect on what they want to learn as a result of their workshop attendance.
A short didactic session then reviews the definition of palliative care and its core components, addresses the nurses’ role in communication within palliative care, a social worker’s perspective of what it is like to be a family member in the ICU, and the outline of the day. This includes delineation of expectations for involvement within the role plays and the various roles to be enacted. An emphasis is placed on the workshop being a safe place to explore and trial skills with the support of colleagues, and that practice is the optimum way to integrate communication expertise into the nurses’ skill set.
The “4 Cs” serves as the instructional basis for nurse communication skill enhancement [27]. This model outlines 4 key nursing roles in optimizing communication within palliative care:
Convening: Making sure multidisciplinary patient/family/clinician communication occurs.
Checking: Identifying the patient and family needs for information; ensuring that patients and families clearly receive desired information; ensuring that clinicians understand patient and family perspectives.
Caring: Naming emotions and responding to feeling.
Continuing: Following up after discussions to clarify and reinforce information and provide support.
Sample Role Play
Facilitator: So our first role play is focused on eliciting patient and family perspectives and needs. I need a learner and someone to play the role of the family member.
Learner: I’ll give it a try.
Facilitator: Lisa, you’re going to do great. Who wants to play the family member?
Workshop Participant: I’ll do it.
Facilitator: So Mary (who has agreed to play the role of the wife), why don’t you read us the scenario. (She reads it out loud to the group).
Facilitator: Lisa, as the nurse, I want you to look at your guide and tell me what your goal is for this conversation with Mrs. Ames and then which skill you want to practice.
Learner: I think I want to try eliciting the patient and family’s needs for information and I’ll try “Tell Me More” statements.
Facilitator: Alright. So remember Lisa, if you feel the conversation isn’t going well, you can call a “time out.” I can do this as well if I feel you need to start over. I’ll also call a time out when I feel you have met your goal. Sound OK? Mary, do you have any questions playing the part of Mrs. Ames?
Wife Role: Well, how hard should I make this for her? Should I be one of those “difficult” family members?
Facilitator: Our goal here is not to “stump” you or make it particularly difficult. We want you to try out these skills and get a sense of your “comfort zone.” So let’s start with some basic communication skills, OK?
Wife Role: Alright.
Facilitator: Why don’t we set the stage, such that Lisa, you are Mr. Ames’ nurse assessing him at the start of your shift, when Mrs. Ames enters. This is the first time you have taken care of him. The night nurse has told you that he has been requiring increasing ventilator support and his renal function is declining. Per Mrs. Ames’ request, the night nurse called her to let her know how he was doing and Mrs. Ames told her she would be in shortly.
Wife Role: (nervously enters the room and grasps her husband’s hand and looks at the nurse). How’s he doing? Is he better? The night nurse called me and I was so worried I rushed over here.
Learner: (Turns to Mrs. Ames and extends her hand). Are you Mrs. Ames? I’m Lisa and I am going to be taking care of Mr. Ames today. Let me just finish my assessment and how about we talk then? Will that be OK? It will be just a few minutes.
Wife Role: Alright, I’ll be in the waiting area but please come get me as soon as you can.
Learner: I will. (Nurse then shortly comes into the waiting area and asks Mrs. Ames to come back into the ICU where she invites her to sit just outside Mr. Ames’ room). Mrs. Ames, how are you doing? This must be so stressful for you, having your husband in the ICU.
Wife Role: It’s awful. He’s never been in the hospital before this and look at him, all hooked up to machines. I’m so worried. He seems to be getting worse instead of better.
Learner: What’s your understanding of what is going on?
Wife Role: I really don’t know. One doctor comes in and says one thing and then another comes in and tells me the opposite. I’m so confused I don’t know what to think.
Learner: Would having a better idea of his condition from the doctors who are treating him help you have a better understanding?
Wife Role: Oh, yes, but they always seem in such a hurry.
Learner: What exactly would you like to know?
Wife: Well, I want to know when he can get off that breathing machine because we have been planning to go to our son’s house for Thanksgiving.
Facilitator: Time out. Lisa, did you meet your conversation goal?
Learner: Um, I’m not sure, I guess so.
Facilitator: (Turns to Observers). What do you think, did she meet her goal?
Observer: Yes, she determined Mrs. Ames’ need for more information and she asked her what she wanted to know exactly.
Facilitator: What else did we see Lisa do to enhance communication with Mrs. Ames?
Observer: Well, when Mrs. Ames rushed into the room and asked her for information, Lisa didn’t just jump in and spout out values for the ventilator and his output. She took the time to introduce herself and de-escalate Mrs. Ames’ anxiety and she followed up on her promise to come get her in the waiting room as soon as she could.
Facilitator: Why do you think was important?
Observer: It helps establish trust.
Facilitator: Did Lisa use the skill she wanted to try out?
Observer: Yes.
Facilitator: How do you know? What did you hear her say?
Observer: She said, “What’s your understanding of what is going on with Mr. Ames?”
Facilitator: Absolutely. Great job, Lisa. And who wants to take a guess at how long Lisa’s exchange with Mrs. Ames took?
Observer: Less than two minutes?
Facilitator: That’s right. So just as you consider how long it takes, and how proficient you are, in starting an IV or inserting a Foley catheter, when you have a goal in mind and have practiced the skills to do it well, any skill can be mastered.
Feedback
Participants in the workshops uniformly report an enhanced sense of self-confidence in their palliative care communication skills as a result of their participation [29]. Key to the success of the workshop is the ongoing contact by the workshop facilitators with participants. Rounding is routinely planned such that each participant is visited weekly by a workshop facilitator in their clinical area to determine if the bedside nurse has practiced the new skills and if so, how the interaction transpired. Positive feedback is given for attempts to engage in new behaviors and participants are reminded that with any new skill, repetitive trials are necessary to foster success.
Lessons Learned and Next Steps
One of our major lessons learned was recognizing that it was difficult for many critical care nurses to practice the new communication skills. Nurses are trained to fix problems and perform medico-technical tasks; “listening” has not always been recognized as real work [18]. We needed to reinforce that skills like eliciting another’s perspective or making reflection statements are equally important to those associated with behavioral/technical proficiency.
While our program has been successful, we recognize that the next step in fostering ideal palliative care communication is to provide education within an interdisciplinary context. We recommend that colleagues interested in replicating this or a similar education intervention, survey nurse participants prior to and following workshop participation to measure attitudes, self confidence and perceived barriers over time [30]. We hope to translate our positive experience into a program that engages multiple professionals in the enhancement of optimum palliative care communication proficiency.
Corresponding author: Deborah A. Boyle MSN, RN, AOCNS, Department of Nursing Quality, Research and Education, University of California, Irvine Health, 101 The City Drive, Bldg 22A, Room 3104, Orange, CA 92868.
1. Leung JM, Udris EM, Uman J, et al. The effect of end-of-life discussions on perceived quality of care and health status among patients with COPD. Chest 2012;142:128–33.
2. Osborn TR, Curtis JR, Nielsen EL, et al. Identifying elements of ICU care that families report as important but unsatisfactory: decision-making, control and ICU atmosphere. Chest 2012;142:1185–92.
3. Nelson JE, Puntillo K, Pronovost PJ, et al. In their own words: patients and families define high-quality palliative care in the ICU. Crit Care Med 2010;38:808–18.
4. Nels W, Gabrijel S, Kiss S, et al. Communication skill training significantly improves lung cancer patients understanding. J Palliat Care Med 2014;4:182.
5. Van Vliet LM, Epstein AS. Current state of the art and science of patient-clinician communication in progressive disease: patients’ need to know and feel known. J Clin Oncol 2014;32:3474-8.
6. Troug RD, Campbell ML, Curtis JR, et al. Recommendations for end of life care in the intensive care unit: a consensus statement by the American College of Critical Care Medicine. Crit Care Med 2008;36:953–63.
7. Dahlin CM, Wittenberg E. Communication in palliative care. In: Ferrell BR, Coyle N, Paice J, editors. Oxford textbook of palliative nursing. 4th ed. Oxford: Oxford University Press; 2014:81–109.
8. Baer L, Weinstein E. Improving oncology nurses’ communication skills for difficult conversations. Clin J Oncol Nurs 2013;17:E45–E51.
9. Treece PD. Communication in the intensive care unit about end of life care. AACN Adv Crit Care 2007;18:406–14.
10. Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end of life care at the last place of care. JAMA 2004;291:88–92.
11. Angus DC, Barnato AE, Linde-Zwirble WT, et al. Robert Wood Johnson Foundation ICU End-of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med 2004;32:638–43.
12. Hamric AB, Blackhall LJ. Nurse-physician perspectives on the care of dying patients in intensive care units: collaboration, moral distress, and ethical climate. Crit Care Med 2007;35:422–9.
13. Back AL, Trinidad SB, Hopley EK, Edwards KA. Reframing the goals of care conversation: “We’re in a different place.” J Palliat Med 2014;17:1010–24.
14. Aslakson RA, Wyskiel R, Thornton I, et al. Nurse perceived barriers to effective communication regarding prognosis and optimal end of life care for surgical ICU patients: a qualitative exploration. J Palliat Med 2012;15:910–5.
15. Erickson J. Bedside nurse involvement in end of life decision-making. Dimens Crit Care Nurs 2013;32:65–8.
16. Bernacki RE, Block SD for the American College of Physicians High Value Care Task Force. Communication about serious illness care goals: a review and synthesis of best practices. JAMA Intern Med 2014;174:1994–2003.
17. You JJ, Downar J, Fowler RA, et al. Barriers to goals of care discussion with ‘seriously’ ill hospitalized patients and their families: a multicenter survey of clinicians. JAMA Intern Med 2015;175:549–56.
18. Strang S, Henoch I, Danielson E, et al. Communication about existential issues with patients close to death: nurses’ reflections on content, process, and meaning. Psychooncology 2014;23:562–8.
19. Slatore CG, Hensen L, Gauzine L, et al. Communication by nurses in the intensive care unit: qualitative analysis of domains in patient-centered care. Am J Crit Care 2012;21:410–8.
20. Wittenberg-Lyles E, Goldsmith J, Platt CS. Palliative care communication. Sem Oncol Nurs 2014;30:280–6.
21. Fox MY. Improving communication with patients and families in the ICU: palliative care strategies for intensive care unit nurses. J Hospice Palliat Nurs 2014;16:93–8.
22. Beckstrand RL, Callister LC, Kirchhoff KT. Providing a ‘good death’: critical care nurses’ suggestions for improving end of life care. Am J Crit Care 2006;15:38–45.
23. Peereboom K, Coyle N. Facilitating goals of care discus.sions for patients with life-limiting disease: communication strategies for nurses. J Hospice Palliat Nurs 2012; 14:251–8.
24. Nelson JE, Cortez TB, Curtis JR, et al. Integrating palliative care in the ICU: the nurse in the leading role. J Hospice Palliat Nurs 2011;13:89–94.
25. Jors K, Seibel K, Bardenheuer H, et al. Education in end of life care: what do experienced professionals find important? J Cancer Educ 2015 March 15.
26. Roze des Ordons AL, Sharma N, Heyland DK, et al. Strategies for effective goals of care discussions and decision-making: perspective from a multi-centre survey of Canadian hospital-based health care providers. BMC Palliat Care 2015;14:38.
27. Krimshtein NS, Luhrs CA, Puntillo KA, et al. Training nurses for interdisciplinary communication with families in the ICU. J Palliat Med 2011;14:1325–32.
28. Milic MM, Puntillo K, Turner K, et al. Communicating with patients’ families and physicians about prognosis and goals of care. Am J Crit Care 2015;24:e56–e64.
29. Anderson W, Puntillo K, Barbour S, et al. The IMPACT-ICU Project: expanding palliative care nursing across University of California Centers ICUs to advance palliative care. Center to Advance Palliative Care (CAPC) national seminar. Nov 7–9, 2013. Dallas, TX.
30. Anderson WG, Puntillo K, Boyle D, et al. ICU bedside nurses’ involvement in palliative care communication: a multicenter survey. J Pain Symptom Manage. In press.
1. Leung JM, Udris EM, Uman J, et al. The effect of end-of-life discussions on perceived quality of care and health status among patients with COPD. Chest 2012;142:128–33.
2. Osborn TR, Curtis JR, Nielsen EL, et al. Identifying elements of ICU care that families report as important but unsatisfactory: decision-making, control and ICU atmosphere. Chest 2012;142:1185–92.
3. Nelson JE, Puntillo K, Pronovost PJ, et al. In their own words: patients and families define high-quality palliative care in the ICU. Crit Care Med 2010;38:808–18.
4. Nels W, Gabrijel S, Kiss S, et al. Communication skill training significantly improves lung cancer patients understanding. J Palliat Care Med 2014;4:182.
5. Van Vliet LM, Epstein AS. Current state of the art and science of patient-clinician communication in progressive disease: patients’ need to know and feel known. J Clin Oncol 2014;32:3474-8.
6. Troug RD, Campbell ML, Curtis JR, et al. Recommendations for end of life care in the intensive care unit: a consensus statement by the American College of Critical Care Medicine. Crit Care Med 2008;36:953–63.
7. Dahlin CM, Wittenberg E. Communication in palliative care. In: Ferrell BR, Coyle N, Paice J, editors. Oxford textbook of palliative nursing. 4th ed. Oxford: Oxford University Press; 2014:81–109.
8. Baer L, Weinstein E. Improving oncology nurses’ communication skills for difficult conversations. Clin J Oncol Nurs 2013;17:E45–E51.
9. Treece PD. Communication in the intensive care unit about end of life care. AACN Adv Crit Care 2007;18:406–14.
10. Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end of life care at the last place of care. JAMA 2004;291:88–92.
11. Angus DC, Barnato AE, Linde-Zwirble WT, et al. Robert Wood Johnson Foundation ICU End-of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med 2004;32:638–43.
12. Hamric AB, Blackhall LJ. Nurse-physician perspectives on the care of dying patients in intensive care units: collaboration, moral distress, and ethical climate. Crit Care Med 2007;35:422–9.
13. Back AL, Trinidad SB, Hopley EK, Edwards KA. Reframing the goals of care conversation: “We’re in a different place.” J Palliat Med 2014;17:1010–24.
14. Aslakson RA, Wyskiel R, Thornton I, et al. Nurse perceived barriers to effective communication regarding prognosis and optimal end of life care for surgical ICU patients: a qualitative exploration. J Palliat Med 2012;15:910–5.
15. Erickson J. Bedside nurse involvement in end of life decision-making. Dimens Crit Care Nurs 2013;32:65–8.
16. Bernacki RE, Block SD for the American College of Physicians High Value Care Task Force. Communication about serious illness care goals: a review and synthesis of best practices. JAMA Intern Med 2014;174:1994–2003.
17. You JJ, Downar J, Fowler RA, et al. Barriers to goals of care discussion with ‘seriously’ ill hospitalized patients and their families: a multicenter survey of clinicians. JAMA Intern Med 2015;175:549–56.
18. Strang S, Henoch I, Danielson E, et al. Communication about existential issues with patients close to death: nurses’ reflections on content, process, and meaning. Psychooncology 2014;23:562–8.
19. Slatore CG, Hensen L, Gauzine L, et al. Communication by nurses in the intensive care unit: qualitative analysis of domains in patient-centered care. Am J Crit Care 2012;21:410–8.
20. Wittenberg-Lyles E, Goldsmith J, Platt CS. Palliative care communication. Sem Oncol Nurs 2014;30:280–6.
21. Fox MY. Improving communication with patients and families in the ICU: palliative care strategies for intensive care unit nurses. J Hospice Palliat Nurs 2014;16:93–8.
22. Beckstrand RL, Callister LC, Kirchhoff KT. Providing a ‘good death’: critical care nurses’ suggestions for improving end of life care. Am J Crit Care 2006;15:38–45.
23. Peereboom K, Coyle N. Facilitating goals of care discus.sions for patients with life-limiting disease: communication strategies for nurses. J Hospice Palliat Nurs 2012; 14:251–8.
24. Nelson JE, Cortez TB, Curtis JR, et al. Integrating palliative care in the ICU: the nurse in the leading role. J Hospice Palliat Nurs 2011;13:89–94.
25. Jors K, Seibel K, Bardenheuer H, et al. Education in end of life care: what do experienced professionals find important? J Cancer Educ 2015 March 15.
26. Roze des Ordons AL, Sharma N, Heyland DK, et al. Strategies for effective goals of care discussions and decision-making: perspective from a multi-centre survey of Canadian hospital-based health care providers. BMC Palliat Care 2015;14:38.
27. Krimshtein NS, Luhrs CA, Puntillo KA, et al. Training nurses for interdisciplinary communication with families in the ICU. J Palliat Med 2011;14:1325–32.
28. Milic MM, Puntillo K, Turner K, et al. Communicating with patients’ families and physicians about prognosis and goals of care. Am J Crit Care 2015;24:e56–e64.
29. Anderson W, Puntillo K, Barbour S, et al. The IMPACT-ICU Project: expanding palliative care nursing across University of California Centers ICUs to advance palliative care. Center to Advance Palliative Care (CAPC) national seminar. Nov 7–9, 2013. Dallas, TX.
30. Anderson WG, Puntillo K, Boyle D, et al. ICU bedside nurses’ involvement in palliative care communication: a multicenter survey. J Pain Symptom Manage. In press.
Delivering Bad News in the Context of Culture: A Patient-Centered Approach
From the University of Virginia School of Medicine, Charlottesville, VA.
Abstract
- Objective: To describe the impact of culture on delivering bad news to patients and to describe a patient-centered approach physicians can use when delivering bad news.
- Methods: Descriptive report and discussion utilizing an illustrative case.
- Results: Physicians often find it challenging to deliver bad news in a culturally sensitive manner. Patients vary in their preferences for how they receive bad news, both within and across cultural groups. A strategy to address these preferences is presented that integrates the ethnographic Kleinman model and the SPIKES model.
- Conclusion: Delivering bad news is a challenging endeavor for many physicians. Strategies are available to guide clinicians through these conversations in a manner that is culturally sensitive and patient-centered.
A 52-year-old patient from Mexico is seeing his physician because he has been experiencing some fatigue and abdominal pain. The doctor asks the patient about his symptoms with the aid of an interpreter (in all the dialogues, a Spanish interpreter is present).
Doctor: How can I help you today?
Patient: I think it’s probably nothing, but my wife is worried and wanted me to see you. I don’t quite feel myself, just a little more tired than usual.
Doctor: Do you have any other symptoms?
Patient: Well, I have been having some pain in my stomach, just a little crampy feeling down low. My wife says I have lost some weight and she wanted me to see a doctor. I haven’t been eating as much as I usually do. I just don’t have much of an appetite, especially when I get the pain.
The doctor goes on to ask some additional questions and conducts a physical examination. He discovers the patient lost 20 pounds since his last visit 8 months ago. He is worried that the patient may have something serious going on, possibly colon cancer. He recommends some testing to the patient.
Doctor: I would like to do some tests to see what is going on.
Patient: What kind of tests?
Doctor: A few blood tests and a colonoscopy. Do you know what that is?
Patient: Yes, my brother had one a few years ago.
Doctor: Ok, my nurse will set that up and explain what you will need to do. We’ll schedule another appointment for you to come back to discuss the results. You mentioned your wife. Would you like her or anyone else to be with you at that appointment?
Patient: Yes, my wife and son. My son knows a lot more about medical things than I do, and I know he would want to come.
The Need for Culturally Sensitive Care
The concept of one’s culture encompasses a host of components including how an individual identifies oneself as well as the language, customs, beliefs, and value system one utilizes. Culture, in turn, profoundly affects patients’ belief systems regarding health and wellness, disease and illness, and the delivery of health care services, including the use of healers and alternative providers [1].In order to provide culturally sensitive and high-quality care to diverse patient populations, it is important for providers to gain an understanding and sensitivity to the influences of culture on patients’ beliefs and behaviors [2].
The ability to provide care to people of different cultures is more important than ever before. In 2011, the number of legal and unauthorized immigrants in the United States rose to 40.4 million (13% of the population) and between 2007 and 2011 alone, this number rose by 2.4 million [3].According to a 2010 census bureau report, in the last 30 years the number of individuals over the age of 5 who spoke a language other than English in their home more than doubled, an increase that was 4 times greater than the rate of population growth [4].In addition, in 2009 the United States resettled more refugees than any other nation (60,000+) and this number reached almost 70,000 in 2013 [5,6].Patient populations in the United States are becoming increasingly diverse, and providers must have the skills to communicate effectively with these groups. A one-size-fits-all approach is not sufficient for our changing population.
The Challenges of Delivering Bad News and the Impact of Culture
Perhaps one of the most challenging communication scenarios faced by physicians is the need to deliver bad news to a patient. “Bad news” can be described as any information that adversely alters one’s expectations for the future [7].Clinicians from nearly all specialties are confronted with the task of giving bad news [8],and this is particularly true regarding cancer care. Among oncologists, 60% reported the need to break bad news to patients between 5 to 20 times per month, with 14% reporting greater than 20 times per month [9].The concept of giving bad news is often viewed as stressful by clinicians [10], and clinicians must be able to balance a myriad of elements, including patients’ emotional responses, information needs, uncertainties of disease progression and treatments, patients’ preferred level of involvement in decision making, patient expectations, involvement of family members, and how to maintain hope, among others [9,11]. Indeed, it seems that clinicians find it difficult to take into account the full spectrum of patient needs [8]. While the descriptive literature indicates that patient satisfaction and psychological well-being is improved when a patient-centered approach is utilized that attends to the emotional needs of patients [12], clinicians often focus on biomedical information, with less focus on patients’ psychosocial needs and their level of understanding [13–15].
Further, the interaction of patient culture and context with the complexity of the “bad news” interaction can be daunting, and clinicians have noted their diminished level of comfort in adjusting to these cultural preferences [16].The ability of clinicians to “match” the patient’s preferred level of involvement in decision making is associated with higher patient satisfaction with decision making and lower depression after 3 months [11],yet clinicians often find it difficult to determine which patients want to be involved in the decision making to a greater or lesser extent [12].In addition, words have different meanings when used in medical settings or in lay contexts [8],not to mention the challenges of translation when dealing with non–English-speaking patients. Yet, the manner in which clinicians deliver bad news can affect patients’ understanding of their disease, treatment options, and patients’ adjustment to the diagnosis [8],as well as patients’ expected quality of life and intentions to adhere to recommendations [17].
Information Disclosure
One of the key areas impacted by culture relates to preferred disclosure of medical information. Walsh et al noted in their review that the majority of patients in English-speaking countries wanted relatively full disclosure regarding their illness in comparison to individuals from other countries [18].As a further distinction, Blackhall et al noted that African Americans and European Americans were more likely to believe that a patient should be told of a terminal diagnosis than Mexican and Korean Americans [19].In addition, Mexican and Korean Americans were more likely to believe that clinicians should not discuss death and dying with patients, as it could be harmful. Fujimori noted that Asians are less likely to prefer discussions of life expectancy in contrast to Westerners [20].In a survey of Albanian nationals, < 50% of patients wanted to know their true diagnosis; however, individuals who were male, urban, and educated demonstrated a significantly greater preference for disclosure [21].In the Middle East, the concept of disclosure is highly variable in terms of both provider and patient preferences [22].
Involvement of Family Members
A second important area relates to the involvement of family members. Fujimori noted high variability of patient preferences for having family members present when discussing bad news. Of Japanese patients, 78% preferred to be told with family members present, with the number decreasing for Portugal (61%), Australia (53%-57%), and Ireland (40%). Eighty-one percent of the US patients did not want anyone else present. However, almost all placed high value on physician expertise and honesty [20]. Blackhall noted that Mexican and Korean Americans were more likely to favor a family-centered approach to decision making [19]. In addition, Orona indicated that Mexican-American and Chinese-American families felt it was their duty to protect their relatives from a cancer diagnosis to keep the patient’s remaining time free of worry [23]. Haggerty found mixed evidence for patient preferences regarding disclosure of cancer prognosis to family members [24].
Given these variations and complexities, it is natural to try to develop a system for managing them, eg, a list of traits or attributes one can apply to certain groups. For example, patients of Asian origin prefer _______. However, there is an inherent danger in doing this, as it leads to stereotyping [25]. Cultural factors also may be given inappropriate meaning. Specifically, a well-meaning clinician might attribute certain characteristics to a patient when in fact it has little bearing on the patient’s perspective [25]. In addition, given the nature of communication, travel, and the fact that many individuals identify with more than one cultural group, it may be inappropriate to attribute a singular cultural identity to a group in contemporary society. As a result, Kleinman [25] proposed an ethnographic approach as opposed to a cultural approach. Specifically, this involves understanding a patient and his/her illness from an individual’s perspective as opposed to the cultural collective.
Communication Skills to Help Deliver Bad News

Set Up the Interview
Before meeting with the patient, it is important to review the medical data and have a plan in mind for delivering the bad news. Schedule adequate time for discussion and avoid interruptions. Meet in a quiet, private room that is large enough to accommodate family members or friends whom the patient may have brought. In our case example, the patient has brought his wife and son to the appointment.
Doctor: Hello, Mr. Ruiz. (Turning to the patient’s wife and son) I am Dr. Simon.
Patient: Hello, Doctor. This is my wife, Maria, and son, Alejandro.
Doctor: Please have a seat. Are you comfortable?
Patient: Yes. We are anxious to hear the results of the tests.
Son: My father doesn’t always understand medical terms and I wanted to be here to help. I am very worried about him.
Doctor: I understand your concern and I will explain everything to you.
Assess the Patient’s Perception of the Problem
Before telling the patient the diagnosis, it is important to get an idea of the patient’s understanding of the problem, including what he calls it, what he thinks caused it, and how severe he thinks it is.
Doctor: Before I tell you the results, I would like to get a sense first of what you think is going on.
Patient: Well, I really don’t know for sure, but I know the pain is getting worse and I have been feeling weaker. The pain started right after my son’s wedding. There was a lot of food and I ate more than usual. Maybe it was something bad that I ate?
Doctor: (Turning to the wife and son) Do you have any thoughts about the illness?
Wife: I can see he is in pain a lot, even though he tries to hide it from me. I want to know what’s wrong. I am worried it could be something bad.
Obtain the Patient’s Invitation to Disclose the Information
It is important to know if the patient wants to be told the information about his or her diagnosis. Ideally, physicians should discuss this in general terms as part of routine care, before any bad news needs to be delivered. For example,
Doctor: There may come a time when I will need to tell you something bad about your health. Hopefully, that time will never come, but I want to know your preferences so I can honor them if the time does arise. Would you want to be told about this, or would you want someone else, perhaps someone in your family, to be told?
Patient: I appreciate your asking, Doctor. I haven’t really thought about it, but I get kind of nervous and upset when I hear bad news. I would rather you tell me when my wife and son can be there too.
Give Knowledge and Information to the Patient
It is important to provide information that is at a level that the patient can understand. Avoid the use of medical jargon. When speaking through an interpreter, the clinician may need to have a conversation with the interpreter before meeting the patient to explain the situation and the need to be sensitive. For example, if the clinician does not use the word “cancer” after determining from the patient or family the preference for an alternative word, be sure to inform the interpreter not to use the word “cancer.” Provide the information in small chunks and check in frequently to make sure the patient understands. Avoid language that takes away hope. If there is a family member who speaks English, there is a tendency to speak to that person rather than the patient directly. Avoid doing this unless the patient explicitly requests that the clinician speak directly to that individual. This is often the case with older patients. The following might take place at a subsequent appointment:
Doctor: Mr. Ruiz, you told me previously that you would like me to tell you the results of your tests, along with you wife and son. Unfortunately, I have some bad news to tell you. (Pause) The colonoscopy showed that you have a tumor in the colon, also called the large intestine. It is located in the part that we call the ascending colon (draws a picture to show them where this is). We will need to do some other scans to make sure that the tumor is just in the colon and has not spread. I am hopeful, though, that we have caught it fairly early and it has not spread. That would be the best situation. (Pause) Do you understand what I have told you so far?
Address the Patient’s and Family’s Emotions
Every patient will express their reactions to bad news differently, and their reactions may be different from what the physician might experience in a similar situation. Thus, the clinician should be self-aware and be prepared to respond to a variety of responses. It is important to express empathy and validate the patient’s and family reactions and emotions. If the patient does not express any emotion, the clinician should explore this carefully. It may require more than one visit for the patient to open up with his feelings.
Doctor: I am so sorry. I know that this must be a big shock for you.
Patient: I kind of figured it might be something bad, but it is still a shock. Even so, I am a religious man and I believe that I will get through this with the help of my wife and family.
Doctor: It sounds as if you have a great support system and get strength from your faith. You are lucky to have such a wonderful family and that will be a big help as we move forward.
Strategize and Summarize
Ask the patient if he or she is ready to have a discussion about treatment, including his or her goals of treatment. Continue to explore the patient’s knowledge, expectations and hopes. Always allow the patient to express his fears and concerns. Most importantly, let the patient know that you will share the responsibility of decision making with the patient and be there to support him.
Doctor: This is never easy and it’s a lot to take in. Would you like to discuss the next steps and possible treatments at this time or should we make another appointment after your CAT scan?
Patient: My wife is pretty upset and I think it might be better if we stop here for now. Is that ok?
Son: We want to come back as soon as we can after the CAT scan. In the meantime, can you provide me with some information or a good website to check out?
Doctor: Yes, of course. That sounds like a good plan.
Conclusion
The task of giving bad news is a necessity for physicians of most specialties and is often viewed as challenging and even stressful to some. However, the manner in which information is discussed with patients can impact patients’ satisfaction, understanding of their illness, adjustment to the diagnosis, expected quality of life, and intentions to adhere to recommendations [8,17]. Providing bad news in a culturally sensitive manner adds an additional level of complexity to an already challenging encounter. While an individual’s culture can strongly influence patient belief systems and utilization of care, there is an inherent danger when clinicians make assumptions about individuals’ culture and the role it plays in their lives. Instead of focusing on creating a mental list of cultural attributes, we recommend a patient-centered approach where few assumptions about the patient are made and instead, the clinician gains an understanding of each individual patient through queries and adjusts his/her approach and language according to each individual’s needs.
Corresponding author: Lisa K. Rollins, PhD, Dept. of Family Medicine, Univ.of Virginia, PO Box 800729, Charlottesville,VA 22908-0729, lkr2h@virginia.edu.
Financial disclosures: None.
1. Cultural competency – clear communication. National Institutes of Health (NIH). Accessed at www.nih.gov/clearcommunication/culturalcompetency.htm on 15 Jul 2014.
2. Betancourt JR, Green AR, Carrillo JE, Ananeh-Firempong O. Defining cultural competence: a practical framework for addressing racial/ethnic disparities in health and health care. Pub Health Rep 2003;118:293–302.
3. PEW research: Hispanic trends project, a nation of immigrants. Accessed at www.pewhispanic.org/2013/01/29/a-nation-of-immigrants/ on 31 Jul 2014.
4. U.S. Census Bureau. New census bureau report analyzes nation’s linguistic diversity. Accessed at www.census/gov/newsroom/releases/archives/american_community_survey_acs/cb10-cn58.html on 31 Jul 2014.
5. Immigration Policy Center. Refugees: a fact sheet. Accessed at www.immigrationpolicy.org on 28 May 2014.
6. U.S. Department of State. U.S. welcomes record number of refugees. Accessed at iipdigital.usembassy.gov/st/english/article/2013/10/20131023285033.html?CP.rss=true#axzz3GtyMkFSe on 28 May 2014.
7. Barclay JS, Blackhall L J, Tulsky JA. Communication strategies and cultural issues in the delivery of bad news. J Palliative Med 2007;10:958–77.
8. Fallowfield L, Jenkins V. Communicating sad, bad, and difficult news in medicine. Lancet 2004;363;312–9.
9. Baile WF, Buckman R, Lenzi R, et al. SPIKES—A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000;5:302–11.
10. Ptacek JT, McIntosh EG. Physician challenges in communicating bad news. J Behav Med 2009;32:380–7.
11. Vogel BA, Leonhart R, Helmes AW. Communication matters: the impact of communication and participation in decision making on breast cancer patients’ depression and quality of life. Patient Educ Couns 2009;77:391–7.
12. Hack TF, Degner LF, Parker PA. The communication goals and needs of cancer patients: a review. Psychooncology 2005;14:831–45.
13. Vail L, Sandhu H, Fisher J, et al. Hospital consultants breaking bad news with simulated patients: an analysis of communication using the roter interaction analysis system. Patient Educ Couns 2011;83:185–94.
14. Hack TF, Pickles T, Ruether JD, et al. Behind closed doors: systematic analysis of breast cancer consultation communication and predictors of satisfaction with communication.
Psychooncology 2010;19:626–36.
15. Cantwell BM, Ramirez A. Doctor-patient communication: a study of junior house officers. Med Educ 1997;31:17–21.
16. Rollins LK, Bradley EB, Hayden GF, et al. Responding to a changing nation: are faculty prepared for cross-cultural conversations and care? Fam Med 2013;45:736–9.
17. Burgers C, Beukeboom CJ, Sparks L. How the doc should (not) talk: when breaking bad news with negations influences patients’ immediate responses and medical adherence intentions. Patient Educ Couns 2012;89:267–73.
18. Walsh RA, Girgis A, Sanson-Fisher RW. Breaking bad news 2: what evidence is available to guide clinicians? Behav Med 1998;24:61–73.
19. Blackhall LJ, Murphy ST, Frank G, et al. Ethnicity and attitudes toward patient autonomy. JAMA 1995;274:820–5.
20. Fujimori M, Uchitomi Y. Preferences of cancer patients regarding communication of bad news: a systematic literature review. Jpn J Clin Oncol 2009;39:201–16.
21. Beqiri A, Toci E, Sallaku A, et al. Breaking bad news in a southeast european population: a survey among cancer patients in Albania. J Palliat Med 2012;15:1100–5.
22. Khalil RB. Attitudes, beliefs and perceptions regarding truth disclosure of cancer-related information in the Middle East: a review. Palliat Supp Care 2013;11:69–78.
23. Orona CJ, Koenig BA, Davis AJ. Cultural aspects of nondisclosure. Camb Q Healthc Ethics 1994;3:338–46.
24. Hagerty RG, Butow PN, Ellis PM, et al. Communicating prognosis in cancer care: a systematic review of the literature. Ann Oncol 2005;16:1005–53.
25. Kleinman A, Benson P. Anthropology in the clinic: the problem of cultural competency and how to fix it. PLoS Med 2006;3:1673–6.
From the University of Virginia School of Medicine, Charlottesville, VA.
Abstract
- Objective: To describe the impact of culture on delivering bad news to patients and to describe a patient-centered approach physicians can use when delivering bad news.
- Methods: Descriptive report and discussion utilizing an illustrative case.
- Results: Physicians often find it challenging to deliver bad news in a culturally sensitive manner. Patients vary in their preferences for how they receive bad news, both within and across cultural groups. A strategy to address these preferences is presented that integrates the ethnographic Kleinman model and the SPIKES model.
- Conclusion: Delivering bad news is a challenging endeavor for many physicians. Strategies are available to guide clinicians through these conversations in a manner that is culturally sensitive and patient-centered.
A 52-year-old patient from Mexico is seeing his physician because he has been experiencing some fatigue and abdominal pain. The doctor asks the patient about his symptoms with the aid of an interpreter (in all the dialogues, a Spanish interpreter is present).
Doctor: How can I help you today?
Patient: I think it’s probably nothing, but my wife is worried and wanted me to see you. I don’t quite feel myself, just a little more tired than usual.
Doctor: Do you have any other symptoms?
Patient: Well, I have been having some pain in my stomach, just a little crampy feeling down low. My wife says I have lost some weight and she wanted me to see a doctor. I haven’t been eating as much as I usually do. I just don’t have much of an appetite, especially when I get the pain.
The doctor goes on to ask some additional questions and conducts a physical examination. He discovers the patient lost 20 pounds since his last visit 8 months ago. He is worried that the patient may have something serious going on, possibly colon cancer. He recommends some testing to the patient.
Doctor: I would like to do some tests to see what is going on.
Patient: What kind of tests?
Doctor: A few blood tests and a colonoscopy. Do you know what that is?
Patient: Yes, my brother had one a few years ago.
Doctor: Ok, my nurse will set that up and explain what you will need to do. We’ll schedule another appointment for you to come back to discuss the results. You mentioned your wife. Would you like her or anyone else to be with you at that appointment?
Patient: Yes, my wife and son. My son knows a lot more about medical things than I do, and I know he would want to come.
The Need for Culturally Sensitive Care
The concept of one’s culture encompasses a host of components including how an individual identifies oneself as well as the language, customs, beliefs, and value system one utilizes. Culture, in turn, profoundly affects patients’ belief systems regarding health and wellness, disease and illness, and the delivery of health care services, including the use of healers and alternative providers [1].In order to provide culturally sensitive and high-quality care to diverse patient populations, it is important for providers to gain an understanding and sensitivity to the influences of culture on patients’ beliefs and behaviors [2].
The ability to provide care to people of different cultures is more important than ever before. In 2011, the number of legal and unauthorized immigrants in the United States rose to 40.4 million (13% of the population) and between 2007 and 2011 alone, this number rose by 2.4 million [3].According to a 2010 census bureau report, in the last 30 years the number of individuals over the age of 5 who spoke a language other than English in their home more than doubled, an increase that was 4 times greater than the rate of population growth [4].In addition, in 2009 the United States resettled more refugees than any other nation (60,000+) and this number reached almost 70,000 in 2013 [5,6].Patient populations in the United States are becoming increasingly diverse, and providers must have the skills to communicate effectively with these groups. A one-size-fits-all approach is not sufficient for our changing population.
The Challenges of Delivering Bad News and the Impact of Culture
Perhaps one of the most challenging communication scenarios faced by physicians is the need to deliver bad news to a patient. “Bad news” can be described as any information that adversely alters one’s expectations for the future [7].Clinicians from nearly all specialties are confronted with the task of giving bad news [8],and this is particularly true regarding cancer care. Among oncologists, 60% reported the need to break bad news to patients between 5 to 20 times per month, with 14% reporting greater than 20 times per month [9].The concept of giving bad news is often viewed as stressful by clinicians [10], and clinicians must be able to balance a myriad of elements, including patients’ emotional responses, information needs, uncertainties of disease progression and treatments, patients’ preferred level of involvement in decision making, patient expectations, involvement of family members, and how to maintain hope, among others [9,11]. Indeed, it seems that clinicians find it difficult to take into account the full spectrum of patient needs [8]. While the descriptive literature indicates that patient satisfaction and psychological well-being is improved when a patient-centered approach is utilized that attends to the emotional needs of patients [12], clinicians often focus on biomedical information, with less focus on patients’ psychosocial needs and their level of understanding [13–15].
Further, the interaction of patient culture and context with the complexity of the “bad news” interaction can be daunting, and clinicians have noted their diminished level of comfort in adjusting to these cultural preferences [16].The ability of clinicians to “match” the patient’s preferred level of involvement in decision making is associated with higher patient satisfaction with decision making and lower depression after 3 months [11],yet clinicians often find it difficult to determine which patients want to be involved in the decision making to a greater or lesser extent [12].In addition, words have different meanings when used in medical settings or in lay contexts [8],not to mention the challenges of translation when dealing with non–English-speaking patients. Yet, the manner in which clinicians deliver bad news can affect patients’ understanding of their disease, treatment options, and patients’ adjustment to the diagnosis [8],as well as patients’ expected quality of life and intentions to adhere to recommendations [17].
Information Disclosure
One of the key areas impacted by culture relates to preferred disclosure of medical information. Walsh et al noted in their review that the majority of patients in English-speaking countries wanted relatively full disclosure regarding their illness in comparison to individuals from other countries [18].As a further distinction, Blackhall et al noted that African Americans and European Americans were more likely to believe that a patient should be told of a terminal diagnosis than Mexican and Korean Americans [19].In addition, Mexican and Korean Americans were more likely to believe that clinicians should not discuss death and dying with patients, as it could be harmful. Fujimori noted that Asians are less likely to prefer discussions of life expectancy in contrast to Westerners [20].In a survey of Albanian nationals, < 50% of patients wanted to know their true diagnosis; however, individuals who were male, urban, and educated demonstrated a significantly greater preference for disclosure [21].In the Middle East, the concept of disclosure is highly variable in terms of both provider and patient preferences [22].
Involvement of Family Members
A second important area relates to the involvement of family members. Fujimori noted high variability of patient preferences for having family members present when discussing bad news. Of Japanese patients, 78% preferred to be told with family members present, with the number decreasing for Portugal (61%), Australia (53%-57%), and Ireland (40%). Eighty-one percent of the US patients did not want anyone else present. However, almost all placed high value on physician expertise and honesty [20]. Blackhall noted that Mexican and Korean Americans were more likely to favor a family-centered approach to decision making [19]. In addition, Orona indicated that Mexican-American and Chinese-American families felt it was their duty to protect their relatives from a cancer diagnosis to keep the patient’s remaining time free of worry [23]. Haggerty found mixed evidence for patient preferences regarding disclosure of cancer prognosis to family members [24].
Given these variations and complexities, it is natural to try to develop a system for managing them, eg, a list of traits or attributes one can apply to certain groups. For example, patients of Asian origin prefer _______. However, there is an inherent danger in doing this, as it leads to stereotyping [25]. Cultural factors also may be given inappropriate meaning. Specifically, a well-meaning clinician might attribute certain characteristics to a patient when in fact it has little bearing on the patient’s perspective [25]. In addition, given the nature of communication, travel, and the fact that many individuals identify with more than one cultural group, it may be inappropriate to attribute a singular cultural identity to a group in contemporary society. As a result, Kleinman [25] proposed an ethnographic approach as opposed to a cultural approach. Specifically, this involves understanding a patient and his/her illness from an individual’s perspective as opposed to the cultural collective.
Communication Skills to Help Deliver Bad News
Set Up the Interview
Before meeting with the patient, it is important to review the medical data and have a plan in mind for delivering the bad news. Schedule adequate time for discussion and avoid interruptions. Meet in a quiet, private room that is large enough to accommodate family members or friends whom the patient may have brought. In our case example, the patient has brought his wife and son to the appointment.
Doctor: Hello, Mr. Ruiz. (Turning to the patient’s wife and son) I am Dr. Simon.
Patient: Hello, Doctor. This is my wife, Maria, and son, Alejandro.
Doctor: Please have a seat. Are you comfortable?
Patient: Yes. We are anxious to hear the results of the tests.
Son: My father doesn’t always understand medical terms and I wanted to be here to help. I am very worried about him.
Doctor: I understand your concern and I will explain everything to you.
Assess the Patient’s Perception of the Problem
Before telling the patient the diagnosis, it is important to get an idea of the patient’s understanding of the problem, including what he calls it, what he thinks caused it, and how severe he thinks it is.
Doctor: Before I tell you the results, I would like to get a sense first of what you think is going on.
Patient: Well, I really don’t know for sure, but I know the pain is getting worse and I have been feeling weaker. The pain started right after my son’s wedding. There was a lot of food and I ate more than usual. Maybe it was something bad that I ate?
Doctor: (Turning to the wife and son) Do you have any thoughts about the illness?
Wife: I can see he is in pain a lot, even though he tries to hide it from me. I want to know what’s wrong. I am worried it could be something bad.
Obtain the Patient’s Invitation to Disclose the Information
It is important to know if the patient wants to be told the information about his or her diagnosis. Ideally, physicians should discuss this in general terms as part of routine care, before any bad news needs to be delivered. For example,
Doctor: There may come a time when I will need to tell you something bad about your health. Hopefully, that time will never come, but I want to know your preferences so I can honor them if the time does arise. Would you want to be told about this, or would you want someone else, perhaps someone in your family, to be told?
Patient: I appreciate your asking, Doctor. I haven’t really thought about it, but I get kind of nervous and upset when I hear bad news. I would rather you tell me when my wife and son can be there too.
Give Knowledge and Information to the Patient
It is important to provide information that is at a level that the patient can understand. Avoid the use of medical jargon. When speaking through an interpreter, the clinician may need to have a conversation with the interpreter before meeting the patient to explain the situation and the need to be sensitive. For example, if the clinician does not use the word “cancer” after determining from the patient or family the preference for an alternative word, be sure to inform the interpreter not to use the word “cancer.” Provide the information in small chunks and check in frequently to make sure the patient understands. Avoid language that takes away hope. If there is a family member who speaks English, there is a tendency to speak to that person rather than the patient directly. Avoid doing this unless the patient explicitly requests that the clinician speak directly to that individual. This is often the case with older patients. The following might take place at a subsequent appointment:
Doctor: Mr. Ruiz, you told me previously that you would like me to tell you the results of your tests, along with you wife and son. Unfortunately, I have some bad news to tell you. (Pause) The colonoscopy showed that you have a tumor in the colon, also called the large intestine. It is located in the part that we call the ascending colon (draws a picture to show them where this is). We will need to do some other scans to make sure that the tumor is just in the colon and has not spread. I am hopeful, though, that we have caught it fairly early and it has not spread. That would be the best situation. (Pause) Do you understand what I have told you so far?
Address the Patient’s and Family’s Emotions
Every patient will express their reactions to bad news differently, and their reactions may be different from what the physician might experience in a similar situation. Thus, the clinician should be self-aware and be prepared to respond to a variety of responses. It is important to express empathy and validate the patient’s and family reactions and emotions. If the patient does not express any emotion, the clinician should explore this carefully. It may require more than one visit for the patient to open up with his feelings.
Doctor: I am so sorry. I know that this must be a big shock for you.
Patient: I kind of figured it might be something bad, but it is still a shock. Even so, I am a religious man and I believe that I will get through this with the help of my wife and family.
Doctor: It sounds as if you have a great support system and get strength from your faith. You are lucky to have such a wonderful family and that will be a big help as we move forward.
Strategize and Summarize
Ask the patient if he or she is ready to have a discussion about treatment, including his or her goals of treatment. Continue to explore the patient’s knowledge, expectations and hopes. Always allow the patient to express his fears and concerns. Most importantly, let the patient know that you will share the responsibility of decision making with the patient and be there to support him.
Doctor: This is never easy and it’s a lot to take in. Would you like to discuss the next steps and possible treatments at this time or should we make another appointment after your CAT scan?
Patient: My wife is pretty upset and I think it might be better if we stop here for now. Is that ok?
Son: We want to come back as soon as we can after the CAT scan. In the meantime, can you provide me with some information or a good website to check out?
Doctor: Yes, of course. That sounds like a good plan.
Conclusion
The task of giving bad news is a necessity for physicians of most specialties and is often viewed as challenging and even stressful to some. However, the manner in which information is discussed with patients can impact patients’ satisfaction, understanding of their illness, adjustment to the diagnosis, expected quality of life, and intentions to adhere to recommendations [8,17]. Providing bad news in a culturally sensitive manner adds an additional level of complexity to an already challenging encounter. While an individual’s culture can strongly influence patient belief systems and utilization of care, there is an inherent danger when clinicians make assumptions about individuals’ culture and the role it plays in their lives. Instead of focusing on creating a mental list of cultural attributes, we recommend a patient-centered approach where few assumptions about the patient are made and instead, the clinician gains an understanding of each individual patient through queries and adjusts his/her approach and language according to each individual’s needs.
Corresponding author: Lisa K. Rollins, PhD, Dept. of Family Medicine, Univ.of Virginia, PO Box 800729, Charlottesville,VA 22908-0729, lkr2h@virginia.edu.
Financial disclosures: None.
From the University of Virginia School of Medicine, Charlottesville, VA.
Abstract
- Objective: To describe the impact of culture on delivering bad news to patients and to describe a patient-centered approach physicians can use when delivering bad news.
- Methods: Descriptive report and discussion utilizing an illustrative case.
- Results: Physicians often find it challenging to deliver bad news in a culturally sensitive manner. Patients vary in their preferences for how they receive bad news, both within and across cultural groups. A strategy to address these preferences is presented that integrates the ethnographic Kleinman model and the SPIKES model.
- Conclusion: Delivering bad news is a challenging endeavor for many physicians. Strategies are available to guide clinicians through these conversations in a manner that is culturally sensitive and patient-centered.
A 52-year-old patient from Mexico is seeing his physician because he has been experiencing some fatigue and abdominal pain. The doctor asks the patient about his symptoms with the aid of an interpreter (in all the dialogues, a Spanish interpreter is present).
Doctor: How can I help you today?
Patient: I think it’s probably nothing, but my wife is worried and wanted me to see you. I don’t quite feel myself, just a little more tired than usual.
Doctor: Do you have any other symptoms?
Patient: Well, I have been having some pain in my stomach, just a little crampy feeling down low. My wife says I have lost some weight and she wanted me to see a doctor. I haven’t been eating as much as I usually do. I just don’t have much of an appetite, especially when I get the pain.
The doctor goes on to ask some additional questions and conducts a physical examination. He discovers the patient lost 20 pounds since his last visit 8 months ago. He is worried that the patient may have something serious going on, possibly colon cancer. He recommends some testing to the patient.
Doctor: I would like to do some tests to see what is going on.
Patient: What kind of tests?
Doctor: A few blood tests and a colonoscopy. Do you know what that is?
Patient: Yes, my brother had one a few years ago.
Doctor: Ok, my nurse will set that up and explain what you will need to do. We’ll schedule another appointment for you to come back to discuss the results. You mentioned your wife. Would you like her or anyone else to be with you at that appointment?
Patient: Yes, my wife and son. My son knows a lot more about medical things than I do, and I know he would want to come.
The Need for Culturally Sensitive Care
The concept of one’s culture encompasses a host of components including how an individual identifies oneself as well as the language, customs, beliefs, and value system one utilizes. Culture, in turn, profoundly affects patients’ belief systems regarding health and wellness, disease and illness, and the delivery of health care services, including the use of healers and alternative providers [1].In order to provide culturally sensitive and high-quality care to diverse patient populations, it is important for providers to gain an understanding and sensitivity to the influences of culture on patients’ beliefs and behaviors [2].
The ability to provide care to people of different cultures is more important than ever before. In 2011, the number of legal and unauthorized immigrants in the United States rose to 40.4 million (13% of the population) and between 2007 and 2011 alone, this number rose by 2.4 million [3].According to a 2010 census bureau report, in the last 30 years the number of individuals over the age of 5 who spoke a language other than English in their home more than doubled, an increase that was 4 times greater than the rate of population growth [4].In addition, in 2009 the United States resettled more refugees than any other nation (60,000+) and this number reached almost 70,000 in 2013 [5,6].Patient populations in the United States are becoming increasingly diverse, and providers must have the skills to communicate effectively with these groups. A one-size-fits-all approach is not sufficient for our changing population.
The Challenges of Delivering Bad News and the Impact of Culture
Perhaps one of the most challenging communication scenarios faced by physicians is the need to deliver bad news to a patient. “Bad news” can be described as any information that adversely alters one’s expectations for the future [7].Clinicians from nearly all specialties are confronted with the task of giving bad news [8],and this is particularly true regarding cancer care. Among oncologists, 60% reported the need to break bad news to patients between 5 to 20 times per month, with 14% reporting greater than 20 times per month [9].The concept of giving bad news is often viewed as stressful by clinicians [10], and clinicians must be able to balance a myriad of elements, including patients’ emotional responses, information needs, uncertainties of disease progression and treatments, patients’ preferred level of involvement in decision making, patient expectations, involvement of family members, and how to maintain hope, among others [9,11]. Indeed, it seems that clinicians find it difficult to take into account the full spectrum of patient needs [8]. While the descriptive literature indicates that patient satisfaction and psychological well-being is improved when a patient-centered approach is utilized that attends to the emotional needs of patients [12], clinicians often focus on biomedical information, with less focus on patients’ psychosocial needs and their level of understanding [13–15].
Further, the interaction of patient culture and context with the complexity of the “bad news” interaction can be daunting, and clinicians have noted their diminished level of comfort in adjusting to these cultural preferences [16].The ability of clinicians to “match” the patient’s preferred level of involvement in decision making is associated with higher patient satisfaction with decision making and lower depression after 3 months [11],yet clinicians often find it difficult to determine which patients want to be involved in the decision making to a greater or lesser extent [12].In addition, words have different meanings when used in medical settings or in lay contexts [8],not to mention the challenges of translation when dealing with non–English-speaking patients. Yet, the manner in which clinicians deliver bad news can affect patients’ understanding of their disease, treatment options, and patients’ adjustment to the diagnosis [8],as well as patients’ expected quality of life and intentions to adhere to recommendations [17].
Information Disclosure
One of the key areas impacted by culture relates to preferred disclosure of medical information. Walsh et al noted in their review that the majority of patients in English-speaking countries wanted relatively full disclosure regarding their illness in comparison to individuals from other countries [18].As a further distinction, Blackhall et al noted that African Americans and European Americans were more likely to believe that a patient should be told of a terminal diagnosis than Mexican and Korean Americans [19].In addition, Mexican and Korean Americans were more likely to believe that clinicians should not discuss death and dying with patients, as it could be harmful. Fujimori noted that Asians are less likely to prefer discussions of life expectancy in contrast to Westerners [20].In a survey of Albanian nationals, < 50% of patients wanted to know their true diagnosis; however, individuals who were male, urban, and educated demonstrated a significantly greater preference for disclosure [21].In the Middle East, the concept of disclosure is highly variable in terms of both provider and patient preferences [22].
Involvement of Family Members
A second important area relates to the involvement of family members. Fujimori noted high variability of patient preferences for having family members present when discussing bad news. Of Japanese patients, 78% preferred to be told with family members present, with the number decreasing for Portugal (61%), Australia (53%-57%), and Ireland (40%). Eighty-one percent of the US patients did not want anyone else present. However, almost all placed high value on physician expertise and honesty [20]. Blackhall noted that Mexican and Korean Americans were more likely to favor a family-centered approach to decision making [19]. In addition, Orona indicated that Mexican-American and Chinese-American families felt it was their duty to protect their relatives from a cancer diagnosis to keep the patient’s remaining time free of worry [23]. Haggerty found mixed evidence for patient preferences regarding disclosure of cancer prognosis to family members [24].
Given these variations and complexities, it is natural to try to develop a system for managing them, eg, a list of traits or attributes one can apply to certain groups. For example, patients of Asian origin prefer _______. However, there is an inherent danger in doing this, as it leads to stereotyping [25]. Cultural factors also may be given inappropriate meaning. Specifically, a well-meaning clinician might attribute certain characteristics to a patient when in fact it has little bearing on the patient’s perspective [25]. In addition, given the nature of communication, travel, and the fact that many individuals identify with more than one cultural group, it may be inappropriate to attribute a singular cultural identity to a group in contemporary society. As a result, Kleinman [25] proposed an ethnographic approach as opposed to a cultural approach. Specifically, this involves understanding a patient and his/her illness from an individual’s perspective as opposed to the cultural collective.
Communication Skills to Help Deliver Bad News
Set Up the Interview
Before meeting with the patient, it is important to review the medical data and have a plan in mind for delivering the bad news. Schedule adequate time for discussion and avoid interruptions. Meet in a quiet, private room that is large enough to accommodate family members or friends whom the patient may have brought. In our case example, the patient has brought his wife and son to the appointment.
Doctor: Hello, Mr. Ruiz. (Turning to the patient’s wife and son) I am Dr. Simon.
Patient: Hello, Doctor. This is my wife, Maria, and son, Alejandro.
Doctor: Please have a seat. Are you comfortable?
Patient: Yes. We are anxious to hear the results of the tests.
Son: My father doesn’t always understand medical terms and I wanted to be here to help. I am very worried about him.
Doctor: I understand your concern and I will explain everything to you.
Assess the Patient’s Perception of the Problem
Before telling the patient the diagnosis, it is important to get an idea of the patient’s understanding of the problem, including what he calls it, what he thinks caused it, and how severe he thinks it is.
Doctor: Before I tell you the results, I would like to get a sense first of what you think is going on.
Patient: Well, I really don’t know for sure, but I know the pain is getting worse and I have been feeling weaker. The pain started right after my son’s wedding. There was a lot of food and I ate more than usual. Maybe it was something bad that I ate?
Doctor: (Turning to the wife and son) Do you have any thoughts about the illness?
Wife: I can see he is in pain a lot, even though he tries to hide it from me. I want to know what’s wrong. I am worried it could be something bad.
Obtain the Patient’s Invitation to Disclose the Information
It is important to know if the patient wants to be told the information about his or her diagnosis. Ideally, physicians should discuss this in general terms as part of routine care, before any bad news needs to be delivered. For example,
Doctor: There may come a time when I will need to tell you something bad about your health. Hopefully, that time will never come, but I want to know your preferences so I can honor them if the time does arise. Would you want to be told about this, or would you want someone else, perhaps someone in your family, to be told?
Patient: I appreciate your asking, Doctor. I haven’t really thought about it, but I get kind of nervous and upset when I hear bad news. I would rather you tell me when my wife and son can be there too.
Give Knowledge and Information to the Patient
It is important to provide information that is at a level that the patient can understand. Avoid the use of medical jargon. When speaking through an interpreter, the clinician may need to have a conversation with the interpreter before meeting the patient to explain the situation and the need to be sensitive. For example, if the clinician does not use the word “cancer” after determining from the patient or family the preference for an alternative word, be sure to inform the interpreter not to use the word “cancer.” Provide the information in small chunks and check in frequently to make sure the patient understands. Avoid language that takes away hope. If there is a family member who speaks English, there is a tendency to speak to that person rather than the patient directly. Avoid doing this unless the patient explicitly requests that the clinician speak directly to that individual. This is often the case with older patients. The following might take place at a subsequent appointment:
Doctor: Mr. Ruiz, you told me previously that you would like me to tell you the results of your tests, along with you wife and son. Unfortunately, I have some bad news to tell you. (Pause) The colonoscopy showed that you have a tumor in the colon, also called the large intestine. It is located in the part that we call the ascending colon (draws a picture to show them where this is). We will need to do some other scans to make sure that the tumor is just in the colon and has not spread. I am hopeful, though, that we have caught it fairly early and it has not spread. That would be the best situation. (Pause) Do you understand what I have told you so far?
Address the Patient’s and Family’s Emotions
Every patient will express their reactions to bad news differently, and their reactions may be different from what the physician might experience in a similar situation. Thus, the clinician should be self-aware and be prepared to respond to a variety of responses. It is important to express empathy and validate the patient’s and family reactions and emotions. If the patient does not express any emotion, the clinician should explore this carefully. It may require more than one visit for the patient to open up with his feelings.
Doctor: I am so sorry. I know that this must be a big shock for you.
Patient: I kind of figured it might be something bad, but it is still a shock. Even so, I am a religious man and I believe that I will get through this with the help of my wife and family.
Doctor: It sounds as if you have a great support system and get strength from your faith. You are lucky to have such a wonderful family and that will be a big help as we move forward.
Strategize and Summarize
Ask the patient if he or she is ready to have a discussion about treatment, including his or her goals of treatment. Continue to explore the patient’s knowledge, expectations and hopes. Always allow the patient to express his fears and concerns. Most importantly, let the patient know that you will share the responsibility of decision making with the patient and be there to support him.
Doctor: This is never easy and it’s a lot to take in. Would you like to discuss the next steps and possible treatments at this time or should we make another appointment after your CAT scan?
Patient: My wife is pretty upset and I think it might be better if we stop here for now. Is that ok?
Son: We want to come back as soon as we can after the CAT scan. In the meantime, can you provide me with some information or a good website to check out?
Doctor: Yes, of course. That sounds like a good plan.
Conclusion
The task of giving bad news is a necessity for physicians of most specialties and is often viewed as challenging and even stressful to some. However, the manner in which information is discussed with patients can impact patients’ satisfaction, understanding of their illness, adjustment to the diagnosis, expected quality of life, and intentions to adhere to recommendations [8,17]. Providing bad news in a culturally sensitive manner adds an additional level of complexity to an already challenging encounter. While an individual’s culture can strongly influence patient belief systems and utilization of care, there is an inherent danger when clinicians make assumptions about individuals’ culture and the role it plays in their lives. Instead of focusing on creating a mental list of cultural attributes, we recommend a patient-centered approach where few assumptions about the patient are made and instead, the clinician gains an understanding of each individual patient through queries and adjusts his/her approach and language according to each individual’s needs.
Corresponding author: Lisa K. Rollins, PhD, Dept. of Family Medicine, Univ.of Virginia, PO Box 800729, Charlottesville,VA 22908-0729, lkr2h@virginia.edu.
Financial disclosures: None.
1. Cultural competency – clear communication. National Institutes of Health (NIH). Accessed at www.nih.gov/clearcommunication/culturalcompetency.htm on 15 Jul 2014.
2. Betancourt JR, Green AR, Carrillo JE, Ananeh-Firempong O. Defining cultural competence: a practical framework for addressing racial/ethnic disparities in health and health care. Pub Health Rep 2003;118:293–302.
3. PEW research: Hispanic trends project, a nation of immigrants. Accessed at www.pewhispanic.org/2013/01/29/a-nation-of-immigrants/ on 31 Jul 2014.
4. U.S. Census Bureau. New census bureau report analyzes nation’s linguistic diversity. Accessed at www.census/gov/newsroom/releases/archives/american_community_survey_acs/cb10-cn58.html on 31 Jul 2014.
5. Immigration Policy Center. Refugees: a fact sheet. Accessed at www.immigrationpolicy.org on 28 May 2014.
6. U.S. Department of State. U.S. welcomes record number of refugees. Accessed at iipdigital.usembassy.gov/st/english/article/2013/10/20131023285033.html?CP.rss=true#axzz3GtyMkFSe on 28 May 2014.
7. Barclay JS, Blackhall L J, Tulsky JA. Communication strategies and cultural issues in the delivery of bad news. J Palliative Med 2007;10:958–77.
8. Fallowfield L, Jenkins V. Communicating sad, bad, and difficult news in medicine. Lancet 2004;363;312–9.
9. Baile WF, Buckman R, Lenzi R, et al. SPIKES—A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000;5:302–11.
10. Ptacek JT, McIntosh EG. Physician challenges in communicating bad news. J Behav Med 2009;32:380–7.
11. Vogel BA, Leonhart R, Helmes AW. Communication matters: the impact of communication and participation in decision making on breast cancer patients’ depression and quality of life. Patient Educ Couns 2009;77:391–7.
12. Hack TF, Degner LF, Parker PA. The communication goals and needs of cancer patients: a review. Psychooncology 2005;14:831–45.
13. Vail L, Sandhu H, Fisher J, et al. Hospital consultants breaking bad news with simulated patients: an analysis of communication using the roter interaction analysis system. Patient Educ Couns 2011;83:185–94.
14. Hack TF, Pickles T, Ruether JD, et al. Behind closed doors: systematic analysis of breast cancer consultation communication and predictors of satisfaction with communication.
Psychooncology 2010;19:626–36.
15. Cantwell BM, Ramirez A. Doctor-patient communication: a study of junior house officers. Med Educ 1997;31:17–21.
16. Rollins LK, Bradley EB, Hayden GF, et al. Responding to a changing nation: are faculty prepared for cross-cultural conversations and care? Fam Med 2013;45:736–9.
17. Burgers C, Beukeboom CJ, Sparks L. How the doc should (not) talk: when breaking bad news with negations influences patients’ immediate responses and medical adherence intentions. Patient Educ Couns 2012;89:267–73.
18. Walsh RA, Girgis A, Sanson-Fisher RW. Breaking bad news 2: what evidence is available to guide clinicians? Behav Med 1998;24:61–73.
19. Blackhall LJ, Murphy ST, Frank G, et al. Ethnicity and attitudes toward patient autonomy. JAMA 1995;274:820–5.
20. Fujimori M, Uchitomi Y. Preferences of cancer patients regarding communication of bad news: a systematic literature review. Jpn J Clin Oncol 2009;39:201–16.
21. Beqiri A, Toci E, Sallaku A, et al. Breaking bad news in a southeast european population: a survey among cancer patients in Albania. J Palliat Med 2012;15:1100–5.
22. Khalil RB. Attitudes, beliefs and perceptions regarding truth disclosure of cancer-related information in the Middle East: a review. Palliat Supp Care 2013;11:69–78.
23. Orona CJ, Koenig BA, Davis AJ. Cultural aspects of nondisclosure. Camb Q Healthc Ethics 1994;3:338–46.
24. Hagerty RG, Butow PN, Ellis PM, et al. Communicating prognosis in cancer care: a systematic review of the literature. Ann Oncol 2005;16:1005–53.
25. Kleinman A, Benson P. Anthropology in the clinic: the problem of cultural competency and how to fix it. PLoS Med 2006;3:1673–6.
1. Cultural competency – clear communication. National Institutes of Health (NIH). Accessed at www.nih.gov/clearcommunication/culturalcompetency.htm on 15 Jul 2014.
2. Betancourt JR, Green AR, Carrillo JE, Ananeh-Firempong O. Defining cultural competence: a practical framework for addressing racial/ethnic disparities in health and health care. Pub Health Rep 2003;118:293–302.
3. PEW research: Hispanic trends project, a nation of immigrants. Accessed at www.pewhispanic.org/2013/01/29/a-nation-of-immigrants/ on 31 Jul 2014.
4. U.S. Census Bureau. New census bureau report analyzes nation’s linguistic diversity. Accessed at www.census/gov/newsroom/releases/archives/american_community_survey_acs/cb10-cn58.html on 31 Jul 2014.
5. Immigration Policy Center. Refugees: a fact sheet. Accessed at www.immigrationpolicy.org on 28 May 2014.
6. U.S. Department of State. U.S. welcomes record number of refugees. Accessed at iipdigital.usembassy.gov/st/english/article/2013/10/20131023285033.html?CP.rss=true#axzz3GtyMkFSe on 28 May 2014.
7. Barclay JS, Blackhall L J, Tulsky JA. Communication strategies and cultural issues in the delivery of bad news. J Palliative Med 2007;10:958–77.
8. Fallowfield L, Jenkins V. Communicating sad, bad, and difficult news in medicine. Lancet 2004;363;312–9.
9. Baile WF, Buckman R, Lenzi R, et al. SPIKES—A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000;5:302–11.
10. Ptacek JT, McIntosh EG. Physician challenges in communicating bad news. J Behav Med 2009;32:380–7.
11. Vogel BA, Leonhart R, Helmes AW. Communication matters: the impact of communication and participation in decision making on breast cancer patients’ depression and quality of life. Patient Educ Couns 2009;77:391–7.
12. Hack TF, Degner LF, Parker PA. The communication goals and needs of cancer patients: a review. Psychooncology 2005;14:831–45.
13. Vail L, Sandhu H, Fisher J, et al. Hospital consultants breaking bad news with simulated patients: an analysis of communication using the roter interaction analysis system. Patient Educ Couns 2011;83:185–94.
14. Hack TF, Pickles T, Ruether JD, et al. Behind closed doors: systematic analysis of breast cancer consultation communication and predictors of satisfaction with communication.
Psychooncology 2010;19:626–36.
15. Cantwell BM, Ramirez A. Doctor-patient communication: a study of junior house officers. Med Educ 1997;31:17–21.
16. Rollins LK, Bradley EB, Hayden GF, et al. Responding to a changing nation: are faculty prepared for cross-cultural conversations and care? Fam Med 2013;45:736–9.
17. Burgers C, Beukeboom CJ, Sparks L. How the doc should (not) talk: when breaking bad news with negations influences patients’ immediate responses and medical adherence intentions. Patient Educ Couns 2012;89:267–73.
18. Walsh RA, Girgis A, Sanson-Fisher RW. Breaking bad news 2: what evidence is available to guide clinicians? Behav Med 1998;24:61–73.
19. Blackhall LJ, Murphy ST, Frank G, et al. Ethnicity and attitudes toward patient autonomy. JAMA 1995;274:820–5.
20. Fujimori M, Uchitomi Y. Preferences of cancer patients regarding communication of bad news: a systematic literature review. Jpn J Clin Oncol 2009;39:201–16.
21. Beqiri A, Toci E, Sallaku A, et al. Breaking bad news in a southeast european population: a survey among cancer patients in Albania. J Palliat Med 2012;15:1100–5.
22. Khalil RB. Attitudes, beliefs and perceptions regarding truth disclosure of cancer-related information in the Middle East: a review. Palliat Supp Care 2013;11:69–78.
23. Orona CJ, Koenig BA, Davis AJ. Cultural aspects of nondisclosure. Camb Q Healthc Ethics 1994;3:338–46.
24. Hagerty RG, Butow PN, Ellis PM, et al. Communicating prognosis in cancer care: a systematic review of the literature. Ann Oncol 2005;16:1005–53.
25. Kleinman A, Benson P. Anthropology in the clinic: the problem of cultural competency and how to fix it. PLoS Med 2006;3:1673–6.