User login
Patients with cancer get valuable second opinion for free
Halfway through her first round of chemotherapy, with hair falling out, weight down, and her brain in a fog, Carolyn Hackett sat down for a Zoom meeting with a team of oncologists.
She didn’t even want a second opinion, but a friend had insisted that she get one, and she had agreed for the sake of their friendship.
But that Zoom meeting likely saved her life. The team of five specialists who had been reviewing her case for a week explained that she had been misdiagnosed. The original pathologist was mistaken. She didn’t have Hodgkin lymphoma; her cancer was really non-Hodgkin T-cell lymphoma. And the chemotherapy regimen she was in the middle of would do nothing to stop it.
The panel of doctors who populated Hackett’s computer screen during that December 2020 Zoom call were all volunteers with an organization called thesecondopinion, based in San Francisco.
The group, organized in 1969, currently offers free second opinions to at least three California patients with cancer each week. Patients meet for an average of 30-40 minutes – though there is really no limit – with a panel of doctors who have expertise in their specific case.
More than 70 cancer-related specialists, both current and retired, make up the roster of volunteers. A paid staffer rounds up a patient’s medical records, imaging and pathology slides. And a team of four to five doctors spends a week reviewing each case.
Then they meet directly with the patient and their doctor to answer questions and deliver their consensus.
Ms. Hackett was in disbelief after her meeting with thesecondopinion. Her diagnosis had gone from bad to worse, but the new information had changed her life. Without it, she would have surely continued chemotherapy and died.
On top of the new acccurate diagnosis, Ms. Hackett said it was a relief and reassurance when the team of volunteer doctors honored and included her oncologist. “I’m a nurse,” she said, and so she knows through experience that medicine comes with egos and frequent risk of lawsuits. But the team from thesecondopinion never criticized her doctor – after all, it wasn’t his mistake anyway – nor did they suggest legal action. Instead, they immediately included him as part of the team and sent him a letter detailing the panel concensus, she said, which made her feel safe.
Second opinions are big business
“And rightly so,” says Alan Venook, MD, a professor of medicine at UCSF with experience and expertise in gastrointestinal malignancies who was approached for comment but is not associated with thesecondopinion. Cancer is an increasingly a sub-specialized area, and every patient should get a second opinion, he said in an interview.
What is unique to an appointment with thesecondopinion, however, is the price tag – $0.
By comparison, a virtual second opinion at the Cleveland Clinic comes at a flat rate of $1,850, and at the Dana-Farber Cancer Institute, Boston, the cost is $2,400.
At UCSF, a second opinion from Dr. Venook and his colleagues will cost patients a couple thousand dollars out-of-pocket, he said. “Many patients don’t have the luxury of paying for a second opinion,” he said.
More than looking for misdiagnosis
Research shows that getting a second opinion can significantly change the course of a patient’s disease and treatment. A 2017 study by the Mayo Clinic found that at their institution, around 22% of second opinions changed the diagnosis, and 66% of patients received a refined or redefined diagnosis.
However, a misdiagnosis – such the case presented by Ms. Hackett – is a rare occurrence at thesecondopinion, said Howard Kleckner, MD, a medical oncologist and the organization’s medical director.
“We aren’t in the business to look for mistakes,” he said.
More often, thesecondopinion panels are about clarifying and helping patients understand the disease and options they have.”People with cancer need to make a peace with it and make peace with the treatment,” Dr. Kleckner said.
He estimates that 90% of the patients that come to the group already have the right diagnosis and treatment plan because, he says, there are “very good doctors in the state and in the Bay Area in particular.”
And even in the case of the remaining 10% of patients whose second opinion differs from their first, it’s largely a case of differences in the staging the disease or treatment options, Dr. Kleckner said.
“We aren’t coming up with brilliant suggestions. Often we are agreeing with what’s already been said,” said David Lakes, MD, a retired medical oncologist who has been volunteering with thesecondopinion for more than 30 years. “But we often see people understand for the first time.”
Both Dr. Kleckner and Dr. Lakes say that the organization attracts a certain kind of doctor, who tends to be an excellent communicator and really cares about helping the patients.
Many of these doctors are retired, but they want to keep doing the work, and they understand which pieces of information are most important for patients to know, Dr. Kleckner told this news organization. They are also willing to do this kind of work even when they won’t get paid, Dr. Kleckner said.
Part of that comes with gray hair and storied careers, Dr. Lakes added. “Retired people have experience and judgment and communication skills that a lot of younger doctors don’t have,” he commented. They often have more experience with some of the tough stuff, like exploring the goals of treatment, discontinuing treatment, and end-of-life care, and they also have more time to engage patients on their emotional health, he said.
Dr. Venook said that the services provided free-of-charge by these volunteers is “laudable,” and their thorough review of all the diagnostic information is “to their credit.” But he questions whether every second opinion provided by the organization is an expert one, since the doctors are no longer practicing. Oncology is a particularly fast-moving field, with many new developments and novel drugs launched in recent years.
“Second opinions are incredibly helpful but [have] to be [provided] by a knowledgeable expert who gets all the details and gives it serious thought,” Dr. Venook said.
Dr. Lakes says that he is constantly evaluating whether he is entitled to keep offering second opinions when he isn’t practicing; so far the answer remains a yes. Although he now has to spend more time researching treatment options like biologics, he still feels adept at engaging with patients and helping patients understand where they are in their illness and the potential benefits of fourth- or fifth-line treatments.
Another strength of thesecondopinion model lies in numbers. Most of the time second opinions are given by one doctor, Dr. Kleckner pointed out. In contrast, thesecondopinion provides the patient with access to a whole team of specialists.
“Sometimes people on the panels don’t completely agree,” Dr. Lakes said. So, before meeting with the patient on Zoom, the doctors review the case together for about half an hour and come up with a consensus. This way there’s no mixed messaging and as little anxiety for the patient as possible, he said.
The fact that patients have direct access to the panel of experts who review their cases is unique in itself, Dr. Kleckner said.
Many hospitals have tumor boards, but they are reserved for physicians, he pointed out. Patients get to hear the board’s opinion secondhand through their primary doctor or oncologist.
But at thesecondopinion, the patient gets to engage with the doctors directly. There is time to review up to four questions that the patient has submitted before the meeting and also time for any additional questions that may have arisen during the course of the meeting.
In oncology, and medicine in general, patients are often shuffled from one specialist to another, Dr. Lakes said. But often, there is no one who takes a steps back to see the whole picture.
That’s part of what thesecondopinion offers, he said. “We have the time, the experience, and no skin in the game. We can think about [the cases] in an intellectual way without feeling like we are in the hot seat or in charge.”
Thanks to her second opinion, Ms. Hackett was able to get connected with an oncologist in San Francisco who specializes in the type of cancer she actually had. She went on to receive nine rounds of a monoclonal antibody treatment formulated for her specific cancer. She is now in remission 6 months after finishing that therapy.
Scans in late July showed that she was cancer-free and doing really well. “I’m so grateful to them. I’m so impressed with thesecondopinion, I can’t believe it,” she said. “I’m alive because of them.”
A version of this article first appeared on Medscape.com.
Halfway through her first round of chemotherapy, with hair falling out, weight down, and her brain in a fog, Carolyn Hackett sat down for a Zoom meeting with a team of oncologists.
She didn’t even want a second opinion, but a friend had insisted that she get one, and she had agreed for the sake of their friendship.
But that Zoom meeting likely saved her life. The team of five specialists who had been reviewing her case for a week explained that she had been misdiagnosed. The original pathologist was mistaken. She didn’t have Hodgkin lymphoma; her cancer was really non-Hodgkin T-cell lymphoma. And the chemotherapy regimen she was in the middle of would do nothing to stop it.
The panel of doctors who populated Hackett’s computer screen during that December 2020 Zoom call were all volunteers with an organization called thesecondopinion, based in San Francisco.
The group, organized in 1969, currently offers free second opinions to at least three California patients with cancer each week. Patients meet for an average of 30-40 minutes – though there is really no limit – with a panel of doctors who have expertise in their specific case.
More than 70 cancer-related specialists, both current and retired, make up the roster of volunteers. A paid staffer rounds up a patient’s medical records, imaging and pathology slides. And a team of four to five doctors spends a week reviewing each case.
Then they meet directly with the patient and their doctor to answer questions and deliver their consensus.
Ms. Hackett was in disbelief after her meeting with thesecondopinion. Her diagnosis had gone from bad to worse, but the new information had changed her life. Without it, she would have surely continued chemotherapy and died.
On top of the new acccurate diagnosis, Ms. Hackett said it was a relief and reassurance when the team of volunteer doctors honored and included her oncologist. “I’m a nurse,” she said, and so she knows through experience that medicine comes with egos and frequent risk of lawsuits. But the team from thesecondopinion never criticized her doctor – after all, it wasn’t his mistake anyway – nor did they suggest legal action. Instead, they immediately included him as part of the team and sent him a letter detailing the panel concensus, she said, which made her feel safe.
Second opinions are big business
“And rightly so,” says Alan Venook, MD, a professor of medicine at UCSF with experience and expertise in gastrointestinal malignancies who was approached for comment but is not associated with thesecondopinion. Cancer is an increasingly a sub-specialized area, and every patient should get a second opinion, he said in an interview.
What is unique to an appointment with thesecondopinion, however, is the price tag – $0.
By comparison, a virtual second opinion at the Cleveland Clinic comes at a flat rate of $1,850, and at the Dana-Farber Cancer Institute, Boston, the cost is $2,400.
At UCSF, a second opinion from Dr. Venook and his colleagues will cost patients a couple thousand dollars out-of-pocket, he said. “Many patients don’t have the luxury of paying for a second opinion,” he said.
More than looking for misdiagnosis
Research shows that getting a second opinion can significantly change the course of a patient’s disease and treatment. A 2017 study by the Mayo Clinic found that at their institution, around 22% of second opinions changed the diagnosis, and 66% of patients received a refined or redefined diagnosis.
However, a misdiagnosis – such the case presented by Ms. Hackett – is a rare occurrence at thesecondopinion, said Howard Kleckner, MD, a medical oncologist and the organization’s medical director.
“We aren’t in the business to look for mistakes,” he said.
More often, thesecondopinion panels are about clarifying and helping patients understand the disease and options they have.”People with cancer need to make a peace with it and make peace with the treatment,” Dr. Kleckner said.
He estimates that 90% of the patients that come to the group already have the right diagnosis and treatment plan because, he says, there are “very good doctors in the state and in the Bay Area in particular.”
And even in the case of the remaining 10% of patients whose second opinion differs from their first, it’s largely a case of differences in the staging the disease or treatment options, Dr. Kleckner said.
“We aren’t coming up with brilliant suggestions. Often we are agreeing with what’s already been said,” said David Lakes, MD, a retired medical oncologist who has been volunteering with thesecondopinion for more than 30 years. “But we often see people understand for the first time.”
Both Dr. Kleckner and Dr. Lakes say that the organization attracts a certain kind of doctor, who tends to be an excellent communicator and really cares about helping the patients.
Many of these doctors are retired, but they want to keep doing the work, and they understand which pieces of information are most important for patients to know, Dr. Kleckner told this news organization. They are also willing to do this kind of work even when they won’t get paid, Dr. Kleckner said.
Part of that comes with gray hair and storied careers, Dr. Lakes added. “Retired people have experience and judgment and communication skills that a lot of younger doctors don’t have,” he commented. They often have more experience with some of the tough stuff, like exploring the goals of treatment, discontinuing treatment, and end-of-life care, and they also have more time to engage patients on their emotional health, he said.
Dr. Venook said that the services provided free-of-charge by these volunteers is “laudable,” and their thorough review of all the diagnostic information is “to their credit.” But he questions whether every second opinion provided by the organization is an expert one, since the doctors are no longer practicing. Oncology is a particularly fast-moving field, with many new developments and novel drugs launched in recent years.
“Second opinions are incredibly helpful but [have] to be [provided] by a knowledgeable expert who gets all the details and gives it serious thought,” Dr. Venook said.
Dr. Lakes says that he is constantly evaluating whether he is entitled to keep offering second opinions when he isn’t practicing; so far the answer remains a yes. Although he now has to spend more time researching treatment options like biologics, he still feels adept at engaging with patients and helping patients understand where they are in their illness and the potential benefits of fourth- or fifth-line treatments.
Another strength of thesecondopinion model lies in numbers. Most of the time second opinions are given by one doctor, Dr. Kleckner pointed out. In contrast, thesecondopinion provides the patient with access to a whole team of specialists.
“Sometimes people on the panels don’t completely agree,” Dr. Lakes said. So, before meeting with the patient on Zoom, the doctors review the case together for about half an hour and come up with a consensus. This way there’s no mixed messaging and as little anxiety for the patient as possible, he said.
The fact that patients have direct access to the panel of experts who review their cases is unique in itself, Dr. Kleckner said.
Many hospitals have tumor boards, but they are reserved for physicians, he pointed out. Patients get to hear the board’s opinion secondhand through their primary doctor or oncologist.
But at thesecondopinion, the patient gets to engage with the doctors directly. There is time to review up to four questions that the patient has submitted before the meeting and also time for any additional questions that may have arisen during the course of the meeting.
In oncology, and medicine in general, patients are often shuffled from one specialist to another, Dr. Lakes said. But often, there is no one who takes a steps back to see the whole picture.
That’s part of what thesecondopinion offers, he said. “We have the time, the experience, and no skin in the game. We can think about [the cases] in an intellectual way without feeling like we are in the hot seat or in charge.”
Thanks to her second opinion, Ms. Hackett was able to get connected with an oncologist in San Francisco who specializes in the type of cancer she actually had. She went on to receive nine rounds of a monoclonal antibody treatment formulated for her specific cancer. She is now in remission 6 months after finishing that therapy.
Scans in late July showed that she was cancer-free and doing really well. “I’m so grateful to them. I’m so impressed with thesecondopinion, I can’t believe it,” she said. “I’m alive because of them.”
A version of this article first appeared on Medscape.com.
Halfway through her first round of chemotherapy, with hair falling out, weight down, and her brain in a fog, Carolyn Hackett sat down for a Zoom meeting with a team of oncologists.
She didn’t even want a second opinion, but a friend had insisted that she get one, and she had agreed for the sake of their friendship.
But that Zoom meeting likely saved her life. The team of five specialists who had been reviewing her case for a week explained that she had been misdiagnosed. The original pathologist was mistaken. She didn’t have Hodgkin lymphoma; her cancer was really non-Hodgkin T-cell lymphoma. And the chemotherapy regimen she was in the middle of would do nothing to stop it.
The panel of doctors who populated Hackett’s computer screen during that December 2020 Zoom call were all volunteers with an organization called thesecondopinion, based in San Francisco.
The group, organized in 1969, currently offers free second opinions to at least three California patients with cancer each week. Patients meet for an average of 30-40 minutes – though there is really no limit – with a panel of doctors who have expertise in their specific case.
More than 70 cancer-related specialists, both current and retired, make up the roster of volunteers. A paid staffer rounds up a patient’s medical records, imaging and pathology slides. And a team of four to five doctors spends a week reviewing each case.
Then they meet directly with the patient and their doctor to answer questions and deliver their consensus.
Ms. Hackett was in disbelief after her meeting with thesecondopinion. Her diagnosis had gone from bad to worse, but the new information had changed her life. Without it, she would have surely continued chemotherapy and died.
On top of the new acccurate diagnosis, Ms. Hackett said it was a relief and reassurance when the team of volunteer doctors honored and included her oncologist. “I’m a nurse,” she said, and so she knows through experience that medicine comes with egos and frequent risk of lawsuits. But the team from thesecondopinion never criticized her doctor – after all, it wasn’t his mistake anyway – nor did they suggest legal action. Instead, they immediately included him as part of the team and sent him a letter detailing the panel concensus, she said, which made her feel safe.
Second opinions are big business
“And rightly so,” says Alan Venook, MD, a professor of medicine at UCSF with experience and expertise in gastrointestinal malignancies who was approached for comment but is not associated with thesecondopinion. Cancer is an increasingly a sub-specialized area, and every patient should get a second opinion, he said in an interview.
What is unique to an appointment with thesecondopinion, however, is the price tag – $0.
By comparison, a virtual second opinion at the Cleveland Clinic comes at a flat rate of $1,850, and at the Dana-Farber Cancer Institute, Boston, the cost is $2,400.
At UCSF, a second opinion from Dr. Venook and his colleagues will cost patients a couple thousand dollars out-of-pocket, he said. “Many patients don’t have the luxury of paying for a second opinion,” he said.
More than looking for misdiagnosis
Research shows that getting a second opinion can significantly change the course of a patient’s disease and treatment. A 2017 study by the Mayo Clinic found that at their institution, around 22% of second opinions changed the diagnosis, and 66% of patients received a refined or redefined diagnosis.
However, a misdiagnosis – such the case presented by Ms. Hackett – is a rare occurrence at thesecondopinion, said Howard Kleckner, MD, a medical oncologist and the organization’s medical director.
“We aren’t in the business to look for mistakes,” he said.
More often, thesecondopinion panels are about clarifying and helping patients understand the disease and options they have.”People with cancer need to make a peace with it and make peace with the treatment,” Dr. Kleckner said.
He estimates that 90% of the patients that come to the group already have the right diagnosis and treatment plan because, he says, there are “very good doctors in the state and in the Bay Area in particular.”
And even in the case of the remaining 10% of patients whose second opinion differs from their first, it’s largely a case of differences in the staging the disease or treatment options, Dr. Kleckner said.
“We aren’t coming up with brilliant suggestions. Often we are agreeing with what’s already been said,” said David Lakes, MD, a retired medical oncologist who has been volunteering with thesecondopinion for more than 30 years. “But we often see people understand for the first time.”
Both Dr. Kleckner and Dr. Lakes say that the organization attracts a certain kind of doctor, who tends to be an excellent communicator and really cares about helping the patients.
Many of these doctors are retired, but they want to keep doing the work, and they understand which pieces of information are most important for patients to know, Dr. Kleckner told this news organization. They are also willing to do this kind of work even when they won’t get paid, Dr. Kleckner said.
Part of that comes with gray hair and storied careers, Dr. Lakes added. “Retired people have experience and judgment and communication skills that a lot of younger doctors don’t have,” he commented. They often have more experience with some of the tough stuff, like exploring the goals of treatment, discontinuing treatment, and end-of-life care, and they also have more time to engage patients on their emotional health, he said.
Dr. Venook said that the services provided free-of-charge by these volunteers is “laudable,” and their thorough review of all the diagnostic information is “to their credit.” But he questions whether every second opinion provided by the organization is an expert one, since the doctors are no longer practicing. Oncology is a particularly fast-moving field, with many new developments and novel drugs launched in recent years.
“Second opinions are incredibly helpful but [have] to be [provided] by a knowledgeable expert who gets all the details and gives it serious thought,” Dr. Venook said.
Dr. Lakes says that he is constantly evaluating whether he is entitled to keep offering second opinions when he isn’t practicing; so far the answer remains a yes. Although he now has to spend more time researching treatment options like biologics, he still feels adept at engaging with patients and helping patients understand where they are in their illness and the potential benefits of fourth- or fifth-line treatments.
Another strength of thesecondopinion model lies in numbers. Most of the time second opinions are given by one doctor, Dr. Kleckner pointed out. In contrast, thesecondopinion provides the patient with access to a whole team of specialists.
“Sometimes people on the panels don’t completely agree,” Dr. Lakes said. So, before meeting with the patient on Zoom, the doctors review the case together for about half an hour and come up with a consensus. This way there’s no mixed messaging and as little anxiety for the patient as possible, he said.
The fact that patients have direct access to the panel of experts who review their cases is unique in itself, Dr. Kleckner said.
Many hospitals have tumor boards, but they are reserved for physicians, he pointed out. Patients get to hear the board’s opinion secondhand through their primary doctor or oncologist.
But at thesecondopinion, the patient gets to engage with the doctors directly. There is time to review up to four questions that the patient has submitted before the meeting and also time for any additional questions that may have arisen during the course of the meeting.
In oncology, and medicine in general, patients are often shuffled from one specialist to another, Dr. Lakes said. But often, there is no one who takes a steps back to see the whole picture.
That’s part of what thesecondopinion offers, he said. “We have the time, the experience, and no skin in the game. We can think about [the cases] in an intellectual way without feeling like we are in the hot seat or in charge.”
Thanks to her second opinion, Ms. Hackett was able to get connected with an oncologist in San Francisco who specializes in the type of cancer she actually had. She went on to receive nine rounds of a monoclonal antibody treatment formulated for her specific cancer. She is now in remission 6 months after finishing that therapy.
Scans in late July showed that she was cancer-free and doing really well. “I’m so grateful to them. I’m so impressed with thesecondopinion, I can’t believe it,” she said. “I’m alive because of them.”
A version of this article first appeared on Medscape.com.
Weight-loss surgery has a big effect on marriage
Kristal was only in her mid-30s when she decided to have surgery. Her doctor said it was too early. But the Oregon mom of three had found herself in the hospital twice for obesity-related lung complications before her 35th birthday. So she got the gastric sleeve.
And at first it seemed like the best decision for her and her family. She was losing weight – 100 pounds in 16 months – and so was her husband. The whole family was more active and seemed to have more energy. But then her husband’s weight began to creep back up.
While she joined a running group and signed up for half-marathons, her husband’s depression and drinking worsened. The healthier lifestyle they’d shared was now an unspoken wedge between them.
And the added attention Kristal was getting from men and women because of her thinner size only added to the tension. After 30 years together and 22 years of marriage, the high school sweethearts divorced in June 2021. Kristal’s weight loss wasn’t the only problem, but she and her ex-husband believe it was the beginning of the end.
An unexpected outcome?
New research from the University of Pittsburgh found that Kristal’s experience is a common one. The study looked at data from 1,441 bariatric surgery patients and found that never-married patients were over 50% more likely to get married, and married patients were more than twice as likely to get divorced, compared to the general U.S. population.
This U.S. data follows two Scandinavian studies from 2018 and 2020 that found similar relationship changes after bariatric surgery. But the postsurgery divorce rate in the United States was only about half that found in the Danish and Swedish studies, according to the new study published in Annals of Surgery.
It’s important to note that even with an increase in the divorce rate, most marriages in the study were unchanged, said epidemiologist and lead author Wendy King, PhD. In fact, 81% of couples were still married 5 years after surgery. But where the U.S. population has a divorce rate of 3.5%, bariatric patients in the study had an 8% divorce rate. Likewise, those who’d never been married before the surgery had a marriage rate of 18%, compared to 7% in the U.S. population.
Surgery certainly isn’t a death sentence for a patient’s love life. But the uptick in marriage and divorce suggests bariatric surgery significantly impacts how people engage in relationships.
“It makes sense,” said clinical psychologist Rachel Goldman, PhD, who specializes in health and wellness issues and bariatric surgery cases in New York City. “People are changing their lifestyle.” And those changes don’t start or stop the day of surgery, they begin as soon as someone decides to have surgery and continue as a lifelong process, she said.
For some patients, these healthy habits may offer a “new lease on life,” said Dr. King. According to the study, patients who had better physical health after surgery were more likely to get married.
But the continual lifestyle changes can dramatically impact the rituals of existing relationships, said Dr. Goldman. Maybe a couple loved to go out and enjoy an extravagant meal before surgery, or they had ice cream and watched a movie every Friday. The habit changes that come with bariatric surgery can require one partner to focus less on those rituals.
These sorts of changes may leave one or both people feeling like their partner is turning away from them, said Don Cole, DMin, a relationship therapist and clinical director at the Gottman Institute in Seattle, a think tank focused on the science of relationships. The person who had surgery may feel unsupported in the new journey if the partner keeps advocating for unhealthy habits, he said. And the person who didn’t have surgery may feel cast aside by the partner’s new health priorities.
Changes, even those that are positive and healthy, create a kind of crisis for relationships, Dr. Cole said. It’s not just bariatric surgery. Bringing a baby into the home, infertility treatments, and substance abuse recovery are all considered positive changes that are also predictors of relationship dissatisfaction and divorce, he said.
A couple could have a range of emotions after one partner gets bariatric surgery, Dr. Cole said. Unfortunately, “my experience as a therapist says they aren’t that good [at talking about it],” he said.
But bariatric surgery isn’t the only thing at play in these relationship changes, according to the study. Married patients had a much lower chance of separation or divorce (13%) than patients who were unmarried but living together (44%) by 5 years after surgery. Similarly, most people who were already separated either got divorced or resumed being married. It’s as if the surgery and lifestyle changes served as a catalyst for people who already had one foot out of (or in) the door, Dr. Goldman said.
A high sexual desire after surgery was also a predictor of divorce. In fact, there were more things before surgery that impacted divorce than surgery-related changes. It’s possible that many of these patients are “on the path toward change already,” Dr. King said. “Who knows how much the surgery had to do with it.”
Dr. Goldman recalled a patient who, before surgery, had very low self-worth. She wasn’t satisfied with her relationship but admitted to staying because she didn’t believe she could do any better than her current partner. After surgery, her perspective radically changed. She started to get healthier, invested in her education, and changed jobs. And when her partner refused to join her in making changes, she left. Maybe some of these patients “were already thinking about leaving but just didn’t have the confidence,” Dr. Goldman said.
Still, it’s critical that patients receive more counseling on how choosing to have bariatric surgery can impact their relationship before and after their weight loss procedure, Dr. King said. It should be the standard of care.
Currently, relationship-specific counseling isn’t required, Dr. Goldman said. Most programs do require a psychosocial evaluation before surgery, “but they are quite varied.” And even in programs where relationships are mentioned, there often isn’t a psychologist or licensed mental health professional on the team.
Since Dr. King’s previous research on substance abuse after bariatric surgery changed common practice in the field, Dr. Goldman said she hopes the new data will have a similar influence and relationship counseling will become the norm.
Dr. Cole actually had bariatric surgery. He recalled potential relationship issues were briefly mentioned. Someone at the clinic said if his marriage felt challenged, he should seek help from a professional, and that was it.
For Dr. Cole, there were unexpected negative feelings of shame and disappointment after surgery. He felt the extreme weight loss was all his colleagues could talk about and was very disappointed when there was no change in his chronic pain, a primary reason he had the procedure.
Fortunately, he could talk to his wife – also is a relationship therapist at Gottman – about the range of emotions. “One of the things that we know that creates a deep sense of trust is [when] I know my partner is there for me when I’m not well,” Dr. Cole said.
But these negative emotions can be the very things that feel most difficult to talk about or hear from a partner. It’s hard to share our own negative feelings and to hear someone else’s, Dr. Cole said.
He advises creating a new “ritual of connection: moments in time when you plan to turn toward one another.”
That could be a daily walk, where you intentionally talk about the surgery-related changes that both of you have had. Dr. Cole said to ask yourself, “Are we intentional about turning toward one another in those [challenging] moments?”
A version of this article first appeared on WebMD.com.
Kristal was only in her mid-30s when she decided to have surgery. Her doctor said it was too early. But the Oregon mom of three had found herself in the hospital twice for obesity-related lung complications before her 35th birthday. So she got the gastric sleeve.
And at first it seemed like the best decision for her and her family. She was losing weight – 100 pounds in 16 months – and so was her husband. The whole family was more active and seemed to have more energy. But then her husband’s weight began to creep back up.
While she joined a running group and signed up for half-marathons, her husband’s depression and drinking worsened. The healthier lifestyle they’d shared was now an unspoken wedge between them.
And the added attention Kristal was getting from men and women because of her thinner size only added to the tension. After 30 years together and 22 years of marriage, the high school sweethearts divorced in June 2021. Kristal’s weight loss wasn’t the only problem, but she and her ex-husband believe it was the beginning of the end.
An unexpected outcome?
New research from the University of Pittsburgh found that Kristal’s experience is a common one. The study looked at data from 1,441 bariatric surgery patients and found that never-married patients were over 50% more likely to get married, and married patients were more than twice as likely to get divorced, compared to the general U.S. population.
This U.S. data follows two Scandinavian studies from 2018 and 2020 that found similar relationship changes after bariatric surgery. But the postsurgery divorce rate in the United States was only about half that found in the Danish and Swedish studies, according to the new study published in Annals of Surgery.
It’s important to note that even with an increase in the divorce rate, most marriages in the study were unchanged, said epidemiologist and lead author Wendy King, PhD. In fact, 81% of couples were still married 5 years after surgery. But where the U.S. population has a divorce rate of 3.5%, bariatric patients in the study had an 8% divorce rate. Likewise, those who’d never been married before the surgery had a marriage rate of 18%, compared to 7% in the U.S. population.
Surgery certainly isn’t a death sentence for a patient’s love life. But the uptick in marriage and divorce suggests bariatric surgery significantly impacts how people engage in relationships.
“It makes sense,” said clinical psychologist Rachel Goldman, PhD, who specializes in health and wellness issues and bariatric surgery cases in New York City. “People are changing their lifestyle.” And those changes don’t start or stop the day of surgery, they begin as soon as someone decides to have surgery and continue as a lifelong process, she said.
For some patients, these healthy habits may offer a “new lease on life,” said Dr. King. According to the study, patients who had better physical health after surgery were more likely to get married.
But the continual lifestyle changes can dramatically impact the rituals of existing relationships, said Dr. Goldman. Maybe a couple loved to go out and enjoy an extravagant meal before surgery, or they had ice cream and watched a movie every Friday. The habit changes that come with bariatric surgery can require one partner to focus less on those rituals.
These sorts of changes may leave one or both people feeling like their partner is turning away from them, said Don Cole, DMin, a relationship therapist and clinical director at the Gottman Institute in Seattle, a think tank focused on the science of relationships. The person who had surgery may feel unsupported in the new journey if the partner keeps advocating for unhealthy habits, he said. And the person who didn’t have surgery may feel cast aside by the partner’s new health priorities.
Changes, even those that are positive and healthy, create a kind of crisis for relationships, Dr. Cole said. It’s not just bariatric surgery. Bringing a baby into the home, infertility treatments, and substance abuse recovery are all considered positive changes that are also predictors of relationship dissatisfaction and divorce, he said.
A couple could have a range of emotions after one partner gets bariatric surgery, Dr. Cole said. Unfortunately, “my experience as a therapist says they aren’t that good [at talking about it],” he said.
But bariatric surgery isn’t the only thing at play in these relationship changes, according to the study. Married patients had a much lower chance of separation or divorce (13%) than patients who were unmarried but living together (44%) by 5 years after surgery. Similarly, most people who were already separated either got divorced or resumed being married. It’s as if the surgery and lifestyle changes served as a catalyst for people who already had one foot out of (or in) the door, Dr. Goldman said.
A high sexual desire after surgery was also a predictor of divorce. In fact, there were more things before surgery that impacted divorce than surgery-related changes. It’s possible that many of these patients are “on the path toward change already,” Dr. King said. “Who knows how much the surgery had to do with it.”
Dr. Goldman recalled a patient who, before surgery, had very low self-worth. She wasn’t satisfied with her relationship but admitted to staying because she didn’t believe she could do any better than her current partner. After surgery, her perspective radically changed. She started to get healthier, invested in her education, and changed jobs. And when her partner refused to join her in making changes, she left. Maybe some of these patients “were already thinking about leaving but just didn’t have the confidence,” Dr. Goldman said.
Still, it’s critical that patients receive more counseling on how choosing to have bariatric surgery can impact their relationship before and after their weight loss procedure, Dr. King said. It should be the standard of care.
Currently, relationship-specific counseling isn’t required, Dr. Goldman said. Most programs do require a psychosocial evaluation before surgery, “but they are quite varied.” And even in programs where relationships are mentioned, there often isn’t a psychologist or licensed mental health professional on the team.
Since Dr. King’s previous research on substance abuse after bariatric surgery changed common practice in the field, Dr. Goldman said she hopes the new data will have a similar influence and relationship counseling will become the norm.
Dr. Cole actually had bariatric surgery. He recalled potential relationship issues were briefly mentioned. Someone at the clinic said if his marriage felt challenged, he should seek help from a professional, and that was it.
For Dr. Cole, there were unexpected negative feelings of shame and disappointment after surgery. He felt the extreme weight loss was all his colleagues could talk about and was very disappointed when there was no change in his chronic pain, a primary reason he had the procedure.
Fortunately, he could talk to his wife – also is a relationship therapist at Gottman – about the range of emotions. “One of the things that we know that creates a deep sense of trust is [when] I know my partner is there for me when I’m not well,” Dr. Cole said.
But these negative emotions can be the very things that feel most difficult to talk about or hear from a partner. It’s hard to share our own negative feelings and to hear someone else’s, Dr. Cole said.
He advises creating a new “ritual of connection: moments in time when you plan to turn toward one another.”
That could be a daily walk, where you intentionally talk about the surgery-related changes that both of you have had. Dr. Cole said to ask yourself, “Are we intentional about turning toward one another in those [challenging] moments?”
A version of this article first appeared on WebMD.com.
Kristal was only in her mid-30s when she decided to have surgery. Her doctor said it was too early. But the Oregon mom of three had found herself in the hospital twice for obesity-related lung complications before her 35th birthday. So she got the gastric sleeve.
And at first it seemed like the best decision for her and her family. She was losing weight – 100 pounds in 16 months – and so was her husband. The whole family was more active and seemed to have more energy. But then her husband’s weight began to creep back up.
While she joined a running group and signed up for half-marathons, her husband’s depression and drinking worsened. The healthier lifestyle they’d shared was now an unspoken wedge between them.
And the added attention Kristal was getting from men and women because of her thinner size only added to the tension. After 30 years together and 22 years of marriage, the high school sweethearts divorced in June 2021. Kristal’s weight loss wasn’t the only problem, but she and her ex-husband believe it was the beginning of the end.
An unexpected outcome?
New research from the University of Pittsburgh found that Kristal’s experience is a common one. The study looked at data from 1,441 bariatric surgery patients and found that never-married patients were over 50% more likely to get married, and married patients were more than twice as likely to get divorced, compared to the general U.S. population.
This U.S. data follows two Scandinavian studies from 2018 and 2020 that found similar relationship changes after bariatric surgery. But the postsurgery divorce rate in the United States was only about half that found in the Danish and Swedish studies, according to the new study published in Annals of Surgery.
It’s important to note that even with an increase in the divorce rate, most marriages in the study were unchanged, said epidemiologist and lead author Wendy King, PhD. In fact, 81% of couples were still married 5 years after surgery. But where the U.S. population has a divorce rate of 3.5%, bariatric patients in the study had an 8% divorce rate. Likewise, those who’d never been married before the surgery had a marriage rate of 18%, compared to 7% in the U.S. population.
Surgery certainly isn’t a death sentence for a patient’s love life. But the uptick in marriage and divorce suggests bariatric surgery significantly impacts how people engage in relationships.
“It makes sense,” said clinical psychologist Rachel Goldman, PhD, who specializes in health and wellness issues and bariatric surgery cases in New York City. “People are changing their lifestyle.” And those changes don’t start or stop the day of surgery, they begin as soon as someone decides to have surgery and continue as a lifelong process, she said.
For some patients, these healthy habits may offer a “new lease on life,” said Dr. King. According to the study, patients who had better physical health after surgery were more likely to get married.
But the continual lifestyle changes can dramatically impact the rituals of existing relationships, said Dr. Goldman. Maybe a couple loved to go out and enjoy an extravagant meal before surgery, or they had ice cream and watched a movie every Friday. The habit changes that come with bariatric surgery can require one partner to focus less on those rituals.
These sorts of changes may leave one or both people feeling like their partner is turning away from them, said Don Cole, DMin, a relationship therapist and clinical director at the Gottman Institute in Seattle, a think tank focused on the science of relationships. The person who had surgery may feel unsupported in the new journey if the partner keeps advocating for unhealthy habits, he said. And the person who didn’t have surgery may feel cast aside by the partner’s new health priorities.
Changes, even those that are positive and healthy, create a kind of crisis for relationships, Dr. Cole said. It’s not just bariatric surgery. Bringing a baby into the home, infertility treatments, and substance abuse recovery are all considered positive changes that are also predictors of relationship dissatisfaction and divorce, he said.
A couple could have a range of emotions after one partner gets bariatric surgery, Dr. Cole said. Unfortunately, “my experience as a therapist says they aren’t that good [at talking about it],” he said.
But bariatric surgery isn’t the only thing at play in these relationship changes, according to the study. Married patients had a much lower chance of separation or divorce (13%) than patients who were unmarried but living together (44%) by 5 years after surgery. Similarly, most people who were already separated either got divorced or resumed being married. It’s as if the surgery and lifestyle changes served as a catalyst for people who already had one foot out of (or in) the door, Dr. Goldman said.
A high sexual desire after surgery was also a predictor of divorce. In fact, there were more things before surgery that impacted divorce than surgery-related changes. It’s possible that many of these patients are “on the path toward change already,” Dr. King said. “Who knows how much the surgery had to do with it.”
Dr. Goldman recalled a patient who, before surgery, had very low self-worth. She wasn’t satisfied with her relationship but admitted to staying because she didn’t believe she could do any better than her current partner. After surgery, her perspective radically changed. She started to get healthier, invested in her education, and changed jobs. And when her partner refused to join her in making changes, she left. Maybe some of these patients “were already thinking about leaving but just didn’t have the confidence,” Dr. Goldman said.
Still, it’s critical that patients receive more counseling on how choosing to have bariatric surgery can impact their relationship before and after their weight loss procedure, Dr. King said. It should be the standard of care.
Currently, relationship-specific counseling isn’t required, Dr. Goldman said. Most programs do require a psychosocial evaluation before surgery, “but they are quite varied.” And even in programs where relationships are mentioned, there often isn’t a psychologist or licensed mental health professional on the team.
Since Dr. King’s previous research on substance abuse after bariatric surgery changed common practice in the field, Dr. Goldman said she hopes the new data will have a similar influence and relationship counseling will become the norm.
Dr. Cole actually had bariatric surgery. He recalled potential relationship issues were briefly mentioned. Someone at the clinic said if his marriage felt challenged, he should seek help from a professional, and that was it.
For Dr. Cole, there were unexpected negative feelings of shame and disappointment after surgery. He felt the extreme weight loss was all his colleagues could talk about and was very disappointed when there was no change in his chronic pain, a primary reason he had the procedure.
Fortunately, he could talk to his wife – also is a relationship therapist at Gottman – about the range of emotions. “One of the things that we know that creates a deep sense of trust is [when] I know my partner is there for me when I’m not well,” Dr. Cole said.
But these negative emotions can be the very things that feel most difficult to talk about or hear from a partner. It’s hard to share our own negative feelings and to hear someone else’s, Dr. Cole said.
He advises creating a new “ritual of connection: moments in time when you plan to turn toward one another.”
That could be a daily walk, where you intentionally talk about the surgery-related changes that both of you have had. Dr. Cole said to ask yourself, “Are we intentional about turning toward one another in those [challenging] moments?”
A version of this article first appeared on WebMD.com.
FROM ANNALS OF SURGERY
HPV testing plus cytology catches two times more cervical lesions
, according to a new study.
The study, which analyzed data from Mexico’s population-based hrHPV screening program over 6 years, confirms the importance of HPV screening for catching high-grade cervical lesions early.
“Our results provide evidence that hrHPV testing is the best strategy for a timely diagnosis of CIN2+ lesions while avoiding overtreatment of young women,” the study authors write. “Many countries now use hrHPV testing as the primary screening method, given it has higher sensitivity and detects more cervical cancer precursor lesions, such as CIN2+.”
According to Erik Jansen, MSc, the analysis supports recent updates to U.S. screening standards and confirms findings from previous trials, which show that HPV testing significantly improves prevention of cervical cancer.
“The significance of this paper is that the data reported is from a long follow-up in a country that implemented HPV screening on a large scale,” Mr. Jansen, PhD candidate in the Department of Public Health, Erasmus University Medical Center, Rotterdam, the Netherlands, told this news organization.
The study, conducted by Mexico’s National Institute of Public Health, analyzed screening data from the country’s public cervical cancer prevention program from 2010 to 2015. More than 2 million women aged 34 to 65 who had hrHPV-based screening tests followed by cytologic triage if they were HPV positive were included, as were 2.8 million women of the same age who received cytologic testing alone.
In the hrHPV group, 1.2% of women (n = 24,276) received referrals to colposcopy versus 3.1% of women (n = 90,980) in the cytology group. And among all women, only 0.8% who had abnormal results (n = 16,459) in the HPV went for a colposcopy versus 1.5% (n = 43,638) in the cytology group.
Overall, the authors found that 13.3 colposcopies were required to detect a single CIN2+ case in the cytology group compared to 5.7 colposcopies in the hrHPV with cytologic triage group.
The authors also note that the cost of colposcopies was three times lower in the HPV testing group and that the positive predictive value of hrHPV testing with cytologic triage was 17.5% versus 7.5% for cytology alone.
“The positive predictive value did not change for either screening strategy whether or not women lost to follow-up were taken into account,” the authors write.
Although Mr. Jansen noted that the findings are important, he also pointed to several limitations – namely, the significant loss to follow-up in the HPV group.
The HPV testing and cytologic triage happened in separate visits, and under the two-visit protocol, more than 50% of women who tested positive for HPV didn’t return for cytology. Such a significant loss to follow-up may call some of the findings into question, Mr. Jansen noted.
For instance, the rate of colposcopy referrals does not account for HPV-positive women who skipped their cytology screening. Assuming the same HPV risk for women who received cytology and those who did not, Mr. Jansen calculated that without any loss to follow-up, the colposcopy referral rate would have increased from the reported 1.2% to 2.6%, which is much closer to the 3.1% of the women referred in the cytology arm.
The lower colposcopy costs in the HPV group were also likely due, in part, to the loss to follow-up, which is not necessarily a good thing, Mr. Jansen said.
Still, “this study does confirm the finding that a primary HPV screening program is more effective than cytology [alone],” Mr. Jansen said.
Co-author Eduardo Franco reported receiving grants and personal fees from MSD and has a pending patent, “Methylation Markers in Cervical Cancer.” All other authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
, according to a new study.
The study, which analyzed data from Mexico’s population-based hrHPV screening program over 6 years, confirms the importance of HPV screening for catching high-grade cervical lesions early.
“Our results provide evidence that hrHPV testing is the best strategy for a timely diagnosis of CIN2+ lesions while avoiding overtreatment of young women,” the study authors write. “Many countries now use hrHPV testing as the primary screening method, given it has higher sensitivity and detects more cervical cancer precursor lesions, such as CIN2+.”
According to Erik Jansen, MSc, the analysis supports recent updates to U.S. screening standards and confirms findings from previous trials, which show that HPV testing significantly improves prevention of cervical cancer.
“The significance of this paper is that the data reported is from a long follow-up in a country that implemented HPV screening on a large scale,” Mr. Jansen, PhD candidate in the Department of Public Health, Erasmus University Medical Center, Rotterdam, the Netherlands, told this news organization.
The study, conducted by Mexico’s National Institute of Public Health, analyzed screening data from the country’s public cervical cancer prevention program from 2010 to 2015. More than 2 million women aged 34 to 65 who had hrHPV-based screening tests followed by cytologic triage if they were HPV positive were included, as were 2.8 million women of the same age who received cytologic testing alone.
In the hrHPV group, 1.2% of women (n = 24,276) received referrals to colposcopy versus 3.1% of women (n = 90,980) in the cytology group. And among all women, only 0.8% who had abnormal results (n = 16,459) in the HPV went for a colposcopy versus 1.5% (n = 43,638) in the cytology group.
Overall, the authors found that 13.3 colposcopies were required to detect a single CIN2+ case in the cytology group compared to 5.7 colposcopies in the hrHPV with cytologic triage group.
The authors also note that the cost of colposcopies was three times lower in the HPV testing group and that the positive predictive value of hrHPV testing with cytologic triage was 17.5% versus 7.5% for cytology alone.
“The positive predictive value did not change for either screening strategy whether or not women lost to follow-up were taken into account,” the authors write.
Although Mr. Jansen noted that the findings are important, he also pointed to several limitations – namely, the significant loss to follow-up in the HPV group.
The HPV testing and cytologic triage happened in separate visits, and under the two-visit protocol, more than 50% of women who tested positive for HPV didn’t return for cytology. Such a significant loss to follow-up may call some of the findings into question, Mr. Jansen noted.
For instance, the rate of colposcopy referrals does not account for HPV-positive women who skipped their cytology screening. Assuming the same HPV risk for women who received cytology and those who did not, Mr. Jansen calculated that without any loss to follow-up, the colposcopy referral rate would have increased from the reported 1.2% to 2.6%, which is much closer to the 3.1% of the women referred in the cytology arm.
The lower colposcopy costs in the HPV group were also likely due, in part, to the loss to follow-up, which is not necessarily a good thing, Mr. Jansen said.
Still, “this study does confirm the finding that a primary HPV screening program is more effective than cytology [alone],” Mr. Jansen said.
Co-author Eduardo Franco reported receiving grants and personal fees from MSD and has a pending patent, “Methylation Markers in Cervical Cancer.” All other authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
, according to a new study.
The study, which analyzed data from Mexico’s population-based hrHPV screening program over 6 years, confirms the importance of HPV screening for catching high-grade cervical lesions early.
“Our results provide evidence that hrHPV testing is the best strategy for a timely diagnosis of CIN2+ lesions while avoiding overtreatment of young women,” the study authors write. “Many countries now use hrHPV testing as the primary screening method, given it has higher sensitivity and detects more cervical cancer precursor lesions, such as CIN2+.”
According to Erik Jansen, MSc, the analysis supports recent updates to U.S. screening standards and confirms findings from previous trials, which show that HPV testing significantly improves prevention of cervical cancer.
“The significance of this paper is that the data reported is from a long follow-up in a country that implemented HPV screening on a large scale,” Mr. Jansen, PhD candidate in the Department of Public Health, Erasmus University Medical Center, Rotterdam, the Netherlands, told this news organization.
The study, conducted by Mexico’s National Institute of Public Health, analyzed screening data from the country’s public cervical cancer prevention program from 2010 to 2015. More than 2 million women aged 34 to 65 who had hrHPV-based screening tests followed by cytologic triage if they were HPV positive were included, as were 2.8 million women of the same age who received cytologic testing alone.
In the hrHPV group, 1.2% of women (n = 24,276) received referrals to colposcopy versus 3.1% of women (n = 90,980) in the cytology group. And among all women, only 0.8% who had abnormal results (n = 16,459) in the HPV went for a colposcopy versus 1.5% (n = 43,638) in the cytology group.
Overall, the authors found that 13.3 colposcopies were required to detect a single CIN2+ case in the cytology group compared to 5.7 colposcopies in the hrHPV with cytologic triage group.
The authors also note that the cost of colposcopies was three times lower in the HPV testing group and that the positive predictive value of hrHPV testing with cytologic triage was 17.5% versus 7.5% for cytology alone.
“The positive predictive value did not change for either screening strategy whether or not women lost to follow-up were taken into account,” the authors write.
Although Mr. Jansen noted that the findings are important, he also pointed to several limitations – namely, the significant loss to follow-up in the HPV group.
The HPV testing and cytologic triage happened in separate visits, and under the two-visit protocol, more than 50% of women who tested positive for HPV didn’t return for cytology. Such a significant loss to follow-up may call some of the findings into question, Mr. Jansen noted.
For instance, the rate of colposcopy referrals does not account for HPV-positive women who skipped their cytology screening. Assuming the same HPV risk for women who received cytology and those who did not, Mr. Jansen calculated that without any loss to follow-up, the colposcopy referral rate would have increased from the reported 1.2% to 2.6%, which is much closer to the 3.1% of the women referred in the cytology arm.
The lower colposcopy costs in the HPV group were also likely due, in part, to the loss to follow-up, which is not necessarily a good thing, Mr. Jansen said.
Still, “this study does confirm the finding that a primary HPV screening program is more effective than cytology [alone],” Mr. Jansen said.
Co-author Eduardo Franco reported receiving grants and personal fees from MSD and has a pending patent, “Methylation Markers in Cervical Cancer.” All other authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Large analysis confirms safety of nipple-sparing mastectomy
A new analysis of over 22,000 mastectomy patients confirms what smaller studies have indicated: Patients who undergo nipple-sparing mastectomy have overall and disease-free survival similar to that of those who receive a total mastectomy.
When nipple-sparing mastectomy was introduced, many experts felt uneasy about opting for the less invasive procedure, recalled Rosa Hwang, MD, associate medical director for breast surgery at MD Anderson Cancer Center in Houston. “The concern was leaving all this skin,” said Dr. Hwang. “Are you going to leave cancer behind” and increase the risk of local recurrence?
Over the past 2 decades, the number of patients undergoing nipple-sparing mastectomy increased and, in turn, studies began to demonstrate the safety of the procedure.
However, large analyses evaluating long-term outcomes – namely, overall survival and breast cancer-specific survival – of nipple-sparing mastectomy were still lacking.
The latest study, published online Nov. 20 in Annals of Surgical Oncology, compared the long-term prognosis and survival benefits of nipple-sparing to total mastectomy in thousands of women. The analysis, which pulled data from the SEER cancer database, included 5,765 patients who underwent the nipple-sparing procedure and 17,289 patients who had a total mastectomy.
The authors found that overall survival and breast cancer–specific survival were similar for women undergoing nipple-sparing mastectomy and those receiving a total mastectomy. In fact, over the long-term, the nipple-sparing group slightly edged out the total mastectomy group in overall survival (94.61% vs. 93% at 5 years and 86.34% vs. 83.48% at 10 years, respectively) and in breast cancer-specific survival rates (96.16% vs. 95.74% at 5 years, and 92.2% vs. 91.37% at 10 years). The differences, however, were not significant.
The study also found that certain subgroups – including White women, women over age 46, those with a median household income of $70,000 or more, hormone receptor-positive, and HER2 negative – had significantly better overall survival rate with the nipple-sparing procedure (P < .05). However, the authors noted, the survival advantage in the nipple-sparing group did not extend to breast cancer–specific survival.
Dr. Hwang, who was not involved in the current analysis, said the significant overall survival result in the subgroup analysis was surprising because “there’s no biological reason why one would expect that to be true.”
Given that the subgroups did not demonstrate better breast cancer–specific survival, Dr. Hwang believes the overall survival finding may have more to do with comorbidities, which the study did not account for, than type of mastectomy.
When choosing who is eligible for a nipple-sparing mastectomy, “We’re more selective,” Dr. Hwang said. For instance, patients with uncontrolled diabetes or who smoke are unlikely to be candidates. “So, I think it’s possible that medical comorbidities and medical conditions between these groups [were] different.”
According to the authors, coding inconsistencies represent another possible weakness of the study. From 1998 to 2010, “the term ‘nipple-sparing mastectomy’ was coded as a [total mastectomy] with the ‘subcutaneous mastectomy’ code.” It’s possible that some patients receiving the nipple-sparing procedure before 2011 were not appropriately coded in the current study.
Moving forward, a large prospective study that includes comorbidities would be helpful, but overall the study helps validate that “nipple-sparing mastectomy is a safe operation for selected patients,” Dr. Hwang said.
A version of this article first appeared on Medscape.com.
A new analysis of over 22,000 mastectomy patients confirms what smaller studies have indicated: Patients who undergo nipple-sparing mastectomy have overall and disease-free survival similar to that of those who receive a total mastectomy.
When nipple-sparing mastectomy was introduced, many experts felt uneasy about opting for the less invasive procedure, recalled Rosa Hwang, MD, associate medical director for breast surgery at MD Anderson Cancer Center in Houston. “The concern was leaving all this skin,” said Dr. Hwang. “Are you going to leave cancer behind” and increase the risk of local recurrence?
Over the past 2 decades, the number of patients undergoing nipple-sparing mastectomy increased and, in turn, studies began to demonstrate the safety of the procedure.
However, large analyses evaluating long-term outcomes – namely, overall survival and breast cancer-specific survival – of nipple-sparing mastectomy were still lacking.
The latest study, published online Nov. 20 in Annals of Surgical Oncology, compared the long-term prognosis and survival benefits of nipple-sparing to total mastectomy in thousands of women. The analysis, which pulled data from the SEER cancer database, included 5,765 patients who underwent the nipple-sparing procedure and 17,289 patients who had a total mastectomy.
The authors found that overall survival and breast cancer–specific survival were similar for women undergoing nipple-sparing mastectomy and those receiving a total mastectomy. In fact, over the long-term, the nipple-sparing group slightly edged out the total mastectomy group in overall survival (94.61% vs. 93% at 5 years and 86.34% vs. 83.48% at 10 years, respectively) and in breast cancer-specific survival rates (96.16% vs. 95.74% at 5 years, and 92.2% vs. 91.37% at 10 years). The differences, however, were not significant.
The study also found that certain subgroups – including White women, women over age 46, those with a median household income of $70,000 or more, hormone receptor-positive, and HER2 negative – had significantly better overall survival rate with the nipple-sparing procedure (P < .05). However, the authors noted, the survival advantage in the nipple-sparing group did not extend to breast cancer–specific survival.
Dr. Hwang, who was not involved in the current analysis, said the significant overall survival result in the subgroup analysis was surprising because “there’s no biological reason why one would expect that to be true.”
Given that the subgroups did not demonstrate better breast cancer–specific survival, Dr. Hwang believes the overall survival finding may have more to do with comorbidities, which the study did not account for, than type of mastectomy.
When choosing who is eligible for a nipple-sparing mastectomy, “We’re more selective,” Dr. Hwang said. For instance, patients with uncontrolled diabetes or who smoke are unlikely to be candidates. “So, I think it’s possible that medical comorbidities and medical conditions between these groups [were] different.”
According to the authors, coding inconsistencies represent another possible weakness of the study. From 1998 to 2010, “the term ‘nipple-sparing mastectomy’ was coded as a [total mastectomy] with the ‘subcutaneous mastectomy’ code.” It’s possible that some patients receiving the nipple-sparing procedure before 2011 were not appropriately coded in the current study.
Moving forward, a large prospective study that includes comorbidities would be helpful, but overall the study helps validate that “nipple-sparing mastectomy is a safe operation for selected patients,” Dr. Hwang said.
A version of this article first appeared on Medscape.com.
A new analysis of over 22,000 mastectomy patients confirms what smaller studies have indicated: Patients who undergo nipple-sparing mastectomy have overall and disease-free survival similar to that of those who receive a total mastectomy.
When nipple-sparing mastectomy was introduced, many experts felt uneasy about opting for the less invasive procedure, recalled Rosa Hwang, MD, associate medical director for breast surgery at MD Anderson Cancer Center in Houston. “The concern was leaving all this skin,” said Dr. Hwang. “Are you going to leave cancer behind” and increase the risk of local recurrence?
Over the past 2 decades, the number of patients undergoing nipple-sparing mastectomy increased and, in turn, studies began to demonstrate the safety of the procedure.
However, large analyses evaluating long-term outcomes – namely, overall survival and breast cancer-specific survival – of nipple-sparing mastectomy were still lacking.
The latest study, published online Nov. 20 in Annals of Surgical Oncology, compared the long-term prognosis and survival benefits of nipple-sparing to total mastectomy in thousands of women. The analysis, which pulled data from the SEER cancer database, included 5,765 patients who underwent the nipple-sparing procedure and 17,289 patients who had a total mastectomy.
The authors found that overall survival and breast cancer–specific survival were similar for women undergoing nipple-sparing mastectomy and those receiving a total mastectomy. In fact, over the long-term, the nipple-sparing group slightly edged out the total mastectomy group in overall survival (94.61% vs. 93% at 5 years and 86.34% vs. 83.48% at 10 years, respectively) and in breast cancer-specific survival rates (96.16% vs. 95.74% at 5 years, and 92.2% vs. 91.37% at 10 years). The differences, however, were not significant.
The study also found that certain subgroups – including White women, women over age 46, those with a median household income of $70,000 or more, hormone receptor-positive, and HER2 negative – had significantly better overall survival rate with the nipple-sparing procedure (P < .05). However, the authors noted, the survival advantage in the nipple-sparing group did not extend to breast cancer–specific survival.
Dr. Hwang, who was not involved in the current analysis, said the significant overall survival result in the subgroup analysis was surprising because “there’s no biological reason why one would expect that to be true.”
Given that the subgroups did not demonstrate better breast cancer–specific survival, Dr. Hwang believes the overall survival finding may have more to do with comorbidities, which the study did not account for, than type of mastectomy.
When choosing who is eligible for a nipple-sparing mastectomy, “We’re more selective,” Dr. Hwang said. For instance, patients with uncontrolled diabetes or who smoke are unlikely to be candidates. “So, I think it’s possible that medical comorbidities and medical conditions between these groups [were] different.”
According to the authors, coding inconsistencies represent another possible weakness of the study. From 1998 to 2010, “the term ‘nipple-sparing mastectomy’ was coded as a [total mastectomy] with the ‘subcutaneous mastectomy’ code.” It’s possible that some patients receiving the nipple-sparing procedure before 2011 were not appropriately coded in the current study.
Moving forward, a large prospective study that includes comorbidities would be helpful, but overall the study helps validate that “nipple-sparing mastectomy is a safe operation for selected patients,” Dr. Hwang said.
A version of this article first appeared on Medscape.com.
Tiny worms sniff out early-stage pancreatic cancer
Research shows Caenorhabditis elegans are attracted to the odor certain chemicals give off – a behavior known as attractive chemotaxis – and early evidence indicates these scents may include human cancer cell secretions, cancer tissues, and urine from patients with colorectal, gastric, and breast cancers.
According to the recent analysis, published in Oncotarget, these small worms may be hot on the trail of pancreatic cancer–related compounds too. The researchers found that C. elegans were significantly more attracted to patients with early-stage pancreatic cancer versus healthy controls.
There is a huge need for research like this that explores strategies to detect pancreatic cancer early, but it’s far too soon to tell how, or if, this particular approach will be clinically relevant, according to Neeha Zaidi, MD, assistant professor of oncology and a medical oncologist specializing in pancreatic cancer at John Hopkins Medicine, Baltimore, who was not involved in the current analysis.
Right now, few diagnostic markers exist for identifying pancreatic ductal adenocarcinomas (PDACs), which account for 90% of pancreatic cancers. PDACs remain one of the deadliest cancers, with a 5-year survival rate of 9%.
A combination of surgical resection and chemotherapy is the only curative treatment, and just 20% of patients are eligible, Dr. Zaidi said. The majority are identified after the disease has metastasized.
However, patients’ 5-year survival rate improves markedly – as high as 85% – if the condition is caught sooner.
In the current study, the researchers first exposed C. elegans to the urine of 83 patients from cancer centers across Japan who had various stages of pancreatic cancer before and after undergoing surgical resection. Using an assay, which takes 30 minutes and 50-100 nematodes per test, C. elegans showed significantly higher chemotaxis toward preoperative urine, compared with postoperative urine.
In a second, closed-labeled arm, the nematodes were exposed to the urine of 28 randomized participants – 11 of whom had early-stage pancreatic cancer (0 or IA), plus 17 healthy volunteers. In this instance as well, C. elegans showed significantly higher chemotaxis in patients with early-stage pancreatic cancer, compared with healthy volunteers (P = .034).
According to the authors, C. elegans “had a higher sensitivity for detecting early pancreatic cancer compared to existing diagnostic markers.” And while this strategy needs to be further validated, they believe early detection of pancreatic cancer using C. elegans “can certainly be expected in the near future.”
The study aligns with previous research, showing that wild-type C. elegans are sensitive to scent and that these critters can smell cancer. Other studies have also found that sniffer canines can detect volatile organic compounds – including biomarkers of certain cancers – in the urine and breath of cancer patients. But training an adequate number of these canines for the clinic isn’t feasible, while C. elegans are far more compact and affordable.
According to Dr. Zaidi, a scent test using C. elegans “seems pretty feasible” and cost effective, but whether this approach will “change our care has yet to be determined.”
The authors, for instance, don’t specify how the scent test will be used, though Dr. Zaidi suspects it would be most relevant for following patients with a higher risk of pancreatic cancer. Alternatively, it could be used as a screening test, but that’s a massive undertaking and “this is way too early to tell if it’s going to be helpful to use this test on a broad scale,” Dr. Zaidi said.
To validate the approach, researchers would also need to know what exactly the C. elegans are smelling and to test it in a much larger number of patients, Dr. Zaidi said. The mere 11 patients with cancer in the blinded portion of the study are not sufficient to draw any major conclusions.
The study also claims a high sensitivity, but what about specificity, Dr. Zaidi said. In other words, are there a lot of false positives?
In addition, a deeper look at the participants shows the two groups – early PDAC and healthy volunteers – were not adequately balanced. The median age of the diseased patients was 70, and the healthy volunteers was 39.
“This is a big difference,” Eithne Costello, PhD, professor of molecular oncology at Liverpool (England) University, said in an interview. “It [also] appears the controls are all of one sex (either all male or all female), while the cancer group is mixed.”
The authors attributed these shortcomings to the small population they had to work with: There simply aren’t many patients whose pancreatic cancer is detected early. Dr. Zaidi agreed that patients with pancreatic cancer stage 0 or IA are extremely difficult to come by.
Even still, researchers need to understand the mechanisms behind this approach and see it work in a much larger group of patients, Dr. Zaidi said.
The study was supported in part by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology. The authors reported institutional endowments received from Hirotsu Bio Science, Kinshu-kai Medical, IDEA Consultants, Ono Pharmaceutical, and others. Two coauthors are employees of Hirotsu Bio Science.
A version of this article first appeared on Medscape.com.
Research shows Caenorhabditis elegans are attracted to the odor certain chemicals give off – a behavior known as attractive chemotaxis – and early evidence indicates these scents may include human cancer cell secretions, cancer tissues, and urine from patients with colorectal, gastric, and breast cancers.
According to the recent analysis, published in Oncotarget, these small worms may be hot on the trail of pancreatic cancer–related compounds too. The researchers found that C. elegans were significantly more attracted to patients with early-stage pancreatic cancer versus healthy controls.
There is a huge need for research like this that explores strategies to detect pancreatic cancer early, but it’s far too soon to tell how, or if, this particular approach will be clinically relevant, according to Neeha Zaidi, MD, assistant professor of oncology and a medical oncologist specializing in pancreatic cancer at John Hopkins Medicine, Baltimore, who was not involved in the current analysis.
Right now, few diagnostic markers exist for identifying pancreatic ductal adenocarcinomas (PDACs), which account for 90% of pancreatic cancers. PDACs remain one of the deadliest cancers, with a 5-year survival rate of 9%.
A combination of surgical resection and chemotherapy is the only curative treatment, and just 20% of patients are eligible, Dr. Zaidi said. The majority are identified after the disease has metastasized.
However, patients’ 5-year survival rate improves markedly – as high as 85% – if the condition is caught sooner.
In the current study, the researchers first exposed C. elegans to the urine of 83 patients from cancer centers across Japan who had various stages of pancreatic cancer before and after undergoing surgical resection. Using an assay, which takes 30 minutes and 50-100 nematodes per test, C. elegans showed significantly higher chemotaxis toward preoperative urine, compared with postoperative urine.
In a second, closed-labeled arm, the nematodes were exposed to the urine of 28 randomized participants – 11 of whom had early-stage pancreatic cancer (0 or IA), plus 17 healthy volunteers. In this instance as well, C. elegans showed significantly higher chemotaxis in patients with early-stage pancreatic cancer, compared with healthy volunteers (P = .034).
According to the authors, C. elegans “had a higher sensitivity for detecting early pancreatic cancer compared to existing diagnostic markers.” And while this strategy needs to be further validated, they believe early detection of pancreatic cancer using C. elegans “can certainly be expected in the near future.”
The study aligns with previous research, showing that wild-type C. elegans are sensitive to scent and that these critters can smell cancer. Other studies have also found that sniffer canines can detect volatile organic compounds – including biomarkers of certain cancers – in the urine and breath of cancer patients. But training an adequate number of these canines for the clinic isn’t feasible, while C. elegans are far more compact and affordable.
According to Dr. Zaidi, a scent test using C. elegans “seems pretty feasible” and cost effective, but whether this approach will “change our care has yet to be determined.”
The authors, for instance, don’t specify how the scent test will be used, though Dr. Zaidi suspects it would be most relevant for following patients with a higher risk of pancreatic cancer. Alternatively, it could be used as a screening test, but that’s a massive undertaking and “this is way too early to tell if it’s going to be helpful to use this test on a broad scale,” Dr. Zaidi said.
To validate the approach, researchers would also need to know what exactly the C. elegans are smelling and to test it in a much larger number of patients, Dr. Zaidi said. The mere 11 patients with cancer in the blinded portion of the study are not sufficient to draw any major conclusions.
The study also claims a high sensitivity, but what about specificity, Dr. Zaidi said. In other words, are there a lot of false positives?
In addition, a deeper look at the participants shows the two groups – early PDAC and healthy volunteers – were not adequately balanced. The median age of the diseased patients was 70, and the healthy volunteers was 39.
“This is a big difference,” Eithne Costello, PhD, professor of molecular oncology at Liverpool (England) University, said in an interview. “It [also] appears the controls are all of one sex (either all male or all female), while the cancer group is mixed.”
The authors attributed these shortcomings to the small population they had to work with: There simply aren’t many patients whose pancreatic cancer is detected early. Dr. Zaidi agreed that patients with pancreatic cancer stage 0 or IA are extremely difficult to come by.
Even still, researchers need to understand the mechanisms behind this approach and see it work in a much larger group of patients, Dr. Zaidi said.
The study was supported in part by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology. The authors reported institutional endowments received from Hirotsu Bio Science, Kinshu-kai Medical, IDEA Consultants, Ono Pharmaceutical, and others. Two coauthors are employees of Hirotsu Bio Science.
A version of this article first appeared on Medscape.com.
Research shows Caenorhabditis elegans are attracted to the odor certain chemicals give off – a behavior known as attractive chemotaxis – and early evidence indicates these scents may include human cancer cell secretions, cancer tissues, and urine from patients with colorectal, gastric, and breast cancers.
According to the recent analysis, published in Oncotarget, these small worms may be hot on the trail of pancreatic cancer–related compounds too. The researchers found that C. elegans were significantly more attracted to patients with early-stage pancreatic cancer versus healthy controls.
There is a huge need for research like this that explores strategies to detect pancreatic cancer early, but it’s far too soon to tell how, or if, this particular approach will be clinically relevant, according to Neeha Zaidi, MD, assistant professor of oncology and a medical oncologist specializing in pancreatic cancer at John Hopkins Medicine, Baltimore, who was not involved in the current analysis.
Right now, few diagnostic markers exist for identifying pancreatic ductal adenocarcinomas (PDACs), which account for 90% of pancreatic cancers. PDACs remain one of the deadliest cancers, with a 5-year survival rate of 9%.
A combination of surgical resection and chemotherapy is the only curative treatment, and just 20% of patients are eligible, Dr. Zaidi said. The majority are identified after the disease has metastasized.
However, patients’ 5-year survival rate improves markedly – as high as 85% – if the condition is caught sooner.
In the current study, the researchers first exposed C. elegans to the urine of 83 patients from cancer centers across Japan who had various stages of pancreatic cancer before and after undergoing surgical resection. Using an assay, which takes 30 minutes and 50-100 nematodes per test, C. elegans showed significantly higher chemotaxis toward preoperative urine, compared with postoperative urine.
In a second, closed-labeled arm, the nematodes were exposed to the urine of 28 randomized participants – 11 of whom had early-stage pancreatic cancer (0 or IA), plus 17 healthy volunteers. In this instance as well, C. elegans showed significantly higher chemotaxis in patients with early-stage pancreatic cancer, compared with healthy volunteers (P = .034).
According to the authors, C. elegans “had a higher sensitivity for detecting early pancreatic cancer compared to existing diagnostic markers.” And while this strategy needs to be further validated, they believe early detection of pancreatic cancer using C. elegans “can certainly be expected in the near future.”
The study aligns with previous research, showing that wild-type C. elegans are sensitive to scent and that these critters can smell cancer. Other studies have also found that sniffer canines can detect volatile organic compounds – including biomarkers of certain cancers – in the urine and breath of cancer patients. But training an adequate number of these canines for the clinic isn’t feasible, while C. elegans are far more compact and affordable.
According to Dr. Zaidi, a scent test using C. elegans “seems pretty feasible” and cost effective, but whether this approach will “change our care has yet to be determined.”
The authors, for instance, don’t specify how the scent test will be used, though Dr. Zaidi suspects it would be most relevant for following patients with a higher risk of pancreatic cancer. Alternatively, it could be used as a screening test, but that’s a massive undertaking and “this is way too early to tell if it’s going to be helpful to use this test on a broad scale,” Dr. Zaidi said.
To validate the approach, researchers would also need to know what exactly the C. elegans are smelling and to test it in a much larger number of patients, Dr. Zaidi said. The mere 11 patients with cancer in the blinded portion of the study are not sufficient to draw any major conclusions.
The study also claims a high sensitivity, but what about specificity, Dr. Zaidi said. In other words, are there a lot of false positives?
In addition, a deeper look at the participants shows the two groups – early PDAC and healthy volunteers – were not adequately balanced. The median age of the diseased patients was 70, and the healthy volunteers was 39.
“This is a big difference,” Eithne Costello, PhD, professor of molecular oncology at Liverpool (England) University, said in an interview. “It [also] appears the controls are all of one sex (either all male or all female), while the cancer group is mixed.”
The authors attributed these shortcomings to the small population they had to work with: There simply aren’t many patients whose pancreatic cancer is detected early. Dr. Zaidi agreed that patients with pancreatic cancer stage 0 or IA are extremely difficult to come by.
Even still, researchers need to understand the mechanisms behind this approach and see it work in a much larger group of patients, Dr. Zaidi said.
The study was supported in part by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology. The authors reported institutional endowments received from Hirotsu Bio Science, Kinshu-kai Medical, IDEA Consultants, Ono Pharmaceutical, and others. Two coauthors are employees of Hirotsu Bio Science.
A version of this article first appeared on Medscape.com.
Alcohol ups risk for atrial fibrillation episode hours later
Consuming alcohol increases the risk for an atrial fibrillation (AF) episode hours later, according to a study published online Aug. 30 in Annals of Internal Medicine.

Past research has associated long-term alcohol consumption with the development of AF, and abstinence from alcohol has been associated with a lower overall AF burden. However, lead study author Greg Marcus, MD, a cardioelectrophysiolgist at the University of California, San Francisco, noted that many patients say that alcohol is a trigger for discrete AF episodes.
To test whether that was possible, the researchers enrolled 100 patients who had a history of AF events and who consumed at least one drink per month. Participants wore a transdermal alcohol sensor and an ambulatory, single-lead electrocardiogram device for 4 weeks. They were instructed to press a button on the electrocardiogram device each time they consumed a standard alcoholic beverage. In addition, blood samples were tested for phosphatidylethanol (PEth) at the participants’ 2-week and 4-week visits. PEth is a phospholipid formed in the blood after alcohol intake. It remains in the blood for up to 4 weeks after alcohol consumption.
The study findings confirmed what the patients had reported. The odds of an AF episode were 38% greater with every 0.1% increase in peak blood alcohol concentration over the previous 12 hours (odds ratio [OR], 1.38; 95% confidence interval, 1.04-1.83; P = .024). Moreover, an episode of AF was associated with twofold greater odds (OR, 2.02; 95% CI, 1.38-3.17) of having consumed one alcoholic drink in the past 4 hours. It was associated with more than threefold greater odds of having consumed two or more drinks (OR, 3.58; 95% CI, 1.63-7.89).
“The major takeaway is, among atrial fibrillation patients, consuming alcohol substantially heightened their risk for any given atrial fibrillation event in the subsequent few hours,” Dr. Marcus said. “The more alcohol consumed, the higher that risk.”
The acute effect of alcohol on these arrhythmias also means that modifying alcohol consumption could immediately benefit some patients. “These data combined with other evidence suggest that recommending minimizing or completely eliminating alcohol will likely be helpful to them,” Dr. Marcus said.
The study’s reliance on wearables and sensors was impressive, said Mariann R. Piano, PhD, director of the Center for Research Development and Scholarship, Vanderbilt University, Nashville, Tenn. Often, these types of studies are “self-reported and confounded by recall bias,” she said. But this study passively documented arrhythmia events and blood alcohol level without any patient input. The additional measures of alcohol consumption were used to validate the blood alcohol sensor.
The study’s focus on patients with a history of AF highlighted a high-risk patient group, according to Dr. Piano, who coauthored an editorial about the study. However, the findings may not be applicable to the general population.
Dr. Marcus said alcohol’s role in causing these types of arrhythmias is probably a matter of degree. AF patients are more prone to events than is the general population and are therefore more sensitive to alcohol, he said. But excessive alcohol consumption could increase the chance of AF in the general population.
The study is not without its limitations, however. For instance, “it would have been really ideal if we knew what that blood alcohol was” before an episode, Dr. Piano said. The number of drinks is a good start, but two drinks can affect persons differently, depending on their weight and height. Also, baseline PEth values suggest that patients had been drinking before the study, she said. Ideally, patients could have been asked to abstain from alcohol for a period before the study to determine a negative baseline PEth value and minimize the effects of previous drinking on AF episodes.
Moving forward, this research should inform how clinicians care for their AF patients, both experts agree. “We need to talk to patients about how much they drink,” Dr. Piano said. In addition, patients should be advised to closely monitor what they’re drinking.
“This definitely sharpens the focus of the importance of a thorough alcohol history when we see an atrial fibrillation patient and to counsel them to reduce or eliminate alcohol, even among those that don’t have alcohol use disorders,” Dr. Marcus said.
Preliminary results of the study were presented as a late-breaking clinical trials presentation at the American College of Cardiology meeting in May.
Dr. Marcus has received grants from Baylis, Jawbone, and Eight Sleep and has received personal fees from InCarda and Johnson & Johnson. Coauthors have received personal fees from VivaLNK, Huba Pharmaceuticals, Johnson & Johnson, and Merck and grants from Samsung and Amgen Inc. The editorialists have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Consuming alcohol increases the risk for an atrial fibrillation (AF) episode hours later, according to a study published online Aug. 30 in Annals of Internal Medicine.
Past research has associated long-term alcohol consumption with the development of AF, and abstinence from alcohol has been associated with a lower overall AF burden. However, lead study author Greg Marcus, MD, a cardioelectrophysiolgist at the University of California, San Francisco, noted that many patients say that alcohol is a trigger for discrete AF episodes.
To test whether that was possible, the researchers enrolled 100 patients who had a history of AF events and who consumed at least one drink per month. Participants wore a transdermal alcohol sensor and an ambulatory, single-lead electrocardiogram device for 4 weeks. They were instructed to press a button on the electrocardiogram device each time they consumed a standard alcoholic beverage. In addition, blood samples were tested for phosphatidylethanol (PEth) at the participants’ 2-week and 4-week visits. PEth is a phospholipid formed in the blood after alcohol intake. It remains in the blood for up to 4 weeks after alcohol consumption.
The study findings confirmed what the patients had reported. The odds of an AF episode were 38% greater with every 0.1% increase in peak blood alcohol concentration over the previous 12 hours (odds ratio [OR], 1.38; 95% confidence interval, 1.04-1.83; P = .024). Moreover, an episode of AF was associated with twofold greater odds (OR, 2.02; 95% CI, 1.38-3.17) of having consumed one alcoholic drink in the past 4 hours. It was associated with more than threefold greater odds of having consumed two or more drinks (OR, 3.58; 95% CI, 1.63-7.89).
“The major takeaway is, among atrial fibrillation patients, consuming alcohol substantially heightened their risk for any given atrial fibrillation event in the subsequent few hours,” Dr. Marcus said. “The more alcohol consumed, the higher that risk.”
The acute effect of alcohol on these arrhythmias also means that modifying alcohol consumption could immediately benefit some patients. “These data combined with other evidence suggest that recommending minimizing or completely eliminating alcohol will likely be helpful to them,” Dr. Marcus said.
The study’s reliance on wearables and sensors was impressive, said Mariann R. Piano, PhD, director of the Center for Research Development and Scholarship, Vanderbilt University, Nashville, Tenn. Often, these types of studies are “self-reported and confounded by recall bias,” she said. But this study passively documented arrhythmia events and blood alcohol level without any patient input. The additional measures of alcohol consumption were used to validate the blood alcohol sensor.
The study’s focus on patients with a history of AF highlighted a high-risk patient group, according to Dr. Piano, who coauthored an editorial about the study. However, the findings may not be applicable to the general population.
Dr. Marcus said alcohol’s role in causing these types of arrhythmias is probably a matter of degree. AF patients are more prone to events than is the general population and are therefore more sensitive to alcohol, he said. But excessive alcohol consumption could increase the chance of AF in the general population.
The study is not without its limitations, however. For instance, “it would have been really ideal if we knew what that blood alcohol was” before an episode, Dr. Piano said. The number of drinks is a good start, but two drinks can affect persons differently, depending on their weight and height. Also, baseline PEth values suggest that patients had been drinking before the study, she said. Ideally, patients could have been asked to abstain from alcohol for a period before the study to determine a negative baseline PEth value and minimize the effects of previous drinking on AF episodes.
Moving forward, this research should inform how clinicians care for their AF patients, both experts agree. “We need to talk to patients about how much they drink,” Dr. Piano said. In addition, patients should be advised to closely monitor what they’re drinking.
“This definitely sharpens the focus of the importance of a thorough alcohol history when we see an atrial fibrillation patient and to counsel them to reduce or eliminate alcohol, even among those that don’t have alcohol use disorders,” Dr. Marcus said.
Preliminary results of the study were presented as a late-breaking clinical trials presentation at the American College of Cardiology meeting in May.
Dr. Marcus has received grants from Baylis, Jawbone, and Eight Sleep and has received personal fees from InCarda and Johnson & Johnson. Coauthors have received personal fees from VivaLNK, Huba Pharmaceuticals, Johnson & Johnson, and Merck and grants from Samsung and Amgen Inc. The editorialists have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Consuming alcohol increases the risk for an atrial fibrillation (AF) episode hours later, according to a study published online Aug. 30 in Annals of Internal Medicine.
Past research has associated long-term alcohol consumption with the development of AF, and abstinence from alcohol has been associated with a lower overall AF burden. However, lead study author Greg Marcus, MD, a cardioelectrophysiolgist at the University of California, San Francisco, noted that many patients say that alcohol is a trigger for discrete AF episodes.
To test whether that was possible, the researchers enrolled 100 patients who had a history of AF events and who consumed at least one drink per month. Participants wore a transdermal alcohol sensor and an ambulatory, single-lead electrocardiogram device for 4 weeks. They were instructed to press a button on the electrocardiogram device each time they consumed a standard alcoholic beverage. In addition, blood samples were tested for phosphatidylethanol (PEth) at the participants’ 2-week and 4-week visits. PEth is a phospholipid formed in the blood after alcohol intake. It remains in the blood for up to 4 weeks after alcohol consumption.
The study findings confirmed what the patients had reported. The odds of an AF episode were 38% greater with every 0.1% increase in peak blood alcohol concentration over the previous 12 hours (odds ratio [OR], 1.38; 95% confidence interval, 1.04-1.83; P = .024). Moreover, an episode of AF was associated with twofold greater odds (OR, 2.02; 95% CI, 1.38-3.17) of having consumed one alcoholic drink in the past 4 hours. It was associated with more than threefold greater odds of having consumed two or more drinks (OR, 3.58; 95% CI, 1.63-7.89).
“The major takeaway is, among atrial fibrillation patients, consuming alcohol substantially heightened their risk for any given atrial fibrillation event in the subsequent few hours,” Dr. Marcus said. “The more alcohol consumed, the higher that risk.”
The acute effect of alcohol on these arrhythmias also means that modifying alcohol consumption could immediately benefit some patients. “These data combined with other evidence suggest that recommending minimizing or completely eliminating alcohol will likely be helpful to them,” Dr. Marcus said.
The study’s reliance on wearables and sensors was impressive, said Mariann R. Piano, PhD, director of the Center for Research Development and Scholarship, Vanderbilt University, Nashville, Tenn. Often, these types of studies are “self-reported and confounded by recall bias,” she said. But this study passively documented arrhythmia events and blood alcohol level without any patient input. The additional measures of alcohol consumption were used to validate the blood alcohol sensor.
The study’s focus on patients with a history of AF highlighted a high-risk patient group, according to Dr. Piano, who coauthored an editorial about the study. However, the findings may not be applicable to the general population.
Dr. Marcus said alcohol’s role in causing these types of arrhythmias is probably a matter of degree. AF patients are more prone to events than is the general population and are therefore more sensitive to alcohol, he said. But excessive alcohol consumption could increase the chance of AF in the general population.
The study is not without its limitations, however. For instance, “it would have been really ideal if we knew what that blood alcohol was” before an episode, Dr. Piano said. The number of drinks is a good start, but two drinks can affect persons differently, depending on their weight and height. Also, baseline PEth values suggest that patients had been drinking before the study, she said. Ideally, patients could have been asked to abstain from alcohol for a period before the study to determine a negative baseline PEth value and minimize the effects of previous drinking on AF episodes.
Moving forward, this research should inform how clinicians care for their AF patients, both experts agree. “We need to talk to patients about how much they drink,” Dr. Piano said. In addition, patients should be advised to closely monitor what they’re drinking.
“This definitely sharpens the focus of the importance of a thorough alcohol history when we see an atrial fibrillation patient and to counsel them to reduce or eliminate alcohol, even among those that don’t have alcohol use disorders,” Dr. Marcus said.
Preliminary results of the study were presented as a late-breaking clinical trials presentation at the American College of Cardiology meeting in May.
Dr. Marcus has received grants from Baylis, Jawbone, and Eight Sleep and has received personal fees from InCarda and Johnson & Johnson. Coauthors have received personal fees from VivaLNK, Huba Pharmaceuticals, Johnson & Johnson, and Merck and grants from Samsung and Amgen Inc. The editorialists have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Med student kicked out for microaggression dustup sues school
Kieran Bhattacharya was slated to graduate from University of Virginia (UVA) Medical School in 2021. But in late 2018, he was suspended. In early 2019, the University Threat Assessment Team went a step further, issuing Mr. Bhattacharya a no-trespass warning.
Mr. Bhattacharya claims the unraveling of his medical training was because of questions he asked at a UVA-hosted panel on microaggressions that took place 1 month before his suspension. His attorneys argue that, after making some admittedly less-than-collegial statements at a forum, the institution branded him as a threat. The school counters that Mr. Bhattacharya had a pattern of concerning, unprofessional behavior. The matter will now be settled in court.
UVA initially attempted to have Mr. Bhattacharya’s suit thrown out. A federal judge did dismiss three of four counts; however, he also ruled the lawsuit could move forward on the grounds that Mr. Bhattacharya’s First Amendment right to free speech was infringed.
Supporters claim that Mr. Bhattacharya was a student in good standing with the university, until he spoke publicly at the panel. They say the discipline he’s faced for those remarks is an egregious breach of free speech. Several experts say his case highlights the use – or rather misuse – of professionalism policies to undermine student freedoms and valuable discourse.
UVA argues that it’s not so simple and that the facts considered by the judge this spring were only part of the story. According to the defense, Mr. Bhattacharya’s side leaves out key details leading up to his suspension. The institution says Mr. Bhattacharya did and said things that provoked medical school officials to question the safety of the campus and his fitness to practice medicine. This news organization attempted to contact Mr. Bhattacharya several times through his attorneys and did not receive a response.
What happened at the microaggression panel
On this, both parties agree: A panel on microaggressions took place on Oct. 25, 2018. Mr. Bhattacharya, then a 2nd-year UVA medical student, was the first volunteer to speak when the floor was opened for questioning.
“Thank you for your presentation,” said Mr. Bhattacharya, according to an audio recording of the event. “I had a few questions, just to clarify your definition of microaggressions.” He then asked his first question: “Is it a requirement, to be a victim of microaggression, that you are a member of a marginalized group?”
The presenter, Beverly Colwell Adams, PhD, associate professor emeritus in the department of psychology and previously the assistant dean of UVA’s College of Arts and Sciences, said it was not. But before she could go on to explain, Mr. Bhattacharya interrupted, speaking quickly. “But in the definition, it just said you had to be a member of a marginalized group, in the definition you used on the last slide. So that’s contradictory.” Dr. Adams responded. “What I had there is kind of the generalized definition,” she said. “In fact, I extend it beyond that.”
Mr. Bhattacharya asked a second question – to which Dr. Adams responded – about defining a marginalized group. Then, during a third question about differentiating between microaggressions and unintentional rude statements, Mr. Bhattacharya sped up again, repeating some of Dr. Adams’ own presentation back to her. He then asked if she had done any other research on microaggression, after calling the evidence she provided “one anecdotal case.” Dr. Adams responded with an example.
Mr. Bhattacharya’s fourth question was then intercepted by a fellow panelist, Sara Rasmussen, MD. She offered an anecdote about her own experience with microaggression, as a person from rural West Virginia. She offered some advice on understanding the impact of your actions and then advised, “You have to learn to uncouple the intent of what you’re saying and the impact it has on the audience.”
Mr. Bhattacharya briefly disagreed with Dr. Rasmussen, and then called the evidence Dr. Adams presented “anecdotal” a second time. At that point, Dr. Rasmussen interrupted him to say that Dr. Adams had offered “a lot of citations from the literature” and then called on another student to ask a question.
In total, Mr. Bhattacharya engaged with the panel for just over 5 minutes. He is now arguing in court that those 5 minutes forever changed his life.
Blindsided
After the event, according to court documents, Nora Kern, MD, and one of the panelists filed a professionalism concern card about Mr. Bhattacharya’s discourse. “This student asked a series of questions that were quite antagonistic toward the panel. He pressed on and stated one faculty member was being contradictory. His level of frustration/anger seemed to escalate until another faculty member defused the situation by calling on another student for questions,” Dr. Kern wrote on the card that was later included in Mr. Bhattacharya’s case filing.
According to Regina Rini, PhD, Canada research chair in philosophy of moral and social cognition at York University in Toronto, there are two layers to Mr. Bhattacharya’s discussion with the panel. She told this news organization that the first level is the content of the conversation: “His very first question was a very reasonable one.” Since the 1970s, when Chester Pierce first coined the term microaggression, most experts have agreed that the action must be directed at a person within a marginalized group. “It sounds like the presenter has a nuanced view,” Dr. Rini said. She added that his “was a fair question to ask.”
However, Dr. Rini said the second layer – the way conversation took place – is a separate concern. “Maybe two rounds of questions later, he starts speaking quickly” and fires off multiple questions one after the other, when asking if Dr. Adams had any evidence, and called her support anecdotal, Dr. Rini said. “That’s not a cooperative attempt to hear an answer.”
“He’s a little antagonistic,” Alana Nichols, JD, MD, attorney and a medical pediatrics intern at the University of Alabama at Birmingham, said after listening to the recording. “He did sound like he had an agenda and was not being receptive to what they were saying.” However, Dr. Nichols said, “What brought me pause as someone in medicine was the way it escalated.”
After Dr. Kern filed the professionalism concern card, two faculty members contacted Mr. Bhattacharya. Christine Peterson, MD, assistant dean for medical education, emailed to ask if he wanted to discuss how to navigate uncomfortable conversations and how to cope with “unintended consequences of conversations.” The day after the panel, John Densmore, MD, associate dean for admissions and student affairs, emailed Mr. Bhattacharya, asking to meet the following week.
Mr. Bhattacharya met with both deans. Dr. Peterson only briefly mentioned the panel. Dr. Densmore didn’t at all, according to court documents. Dr. Densmore also didn’t mention the professionalism concern card to Mr. Bhattacharya. However, the Academic Standards and Achievement Committee discussed it about 2 weeks later, at their monthly meeting.
Dr. Kern was the only voting member present who actually witnessed the microaggression panel. Dr. Peterson was there as a guest. The committee voted unanimously to send Mr. Bhattacharya a letter, reminding him of the importance of showing respect to everyone. The letter was sent the following day, Nov. 14, 2018. Mr. Bhattacharya still had no knowledge of the professionalism concern card.
On Nov. 26, Dr. Densmore sent Mr. Bhattacharya an email that read: “We were notified by the Dean of Students Office that you were heading back to Charlottesville. You will need to be seen by CAPS [Counseling and Psychological Services] before you can return to classes.”
On Nov. 27, court records show Mr. Bhattacharya emailed Dr. Densmore, questioning the school’s ability to mandate psychiatric evaluation. The decision was reinforced with an email from the then senior associate dean for education at UVA Medical School. Mr. Bhattacharya was not permitted to return to class without the evaluation.
“If I were in his situation, I would feel kind of blindsided,” Dr. Nichols said. Mr. Bhattacharya met with two deans immediately after the event, during which he said his conduct with the panel was barely or not at all mentioned. To him, the situation could well have seemed to be over, Dr. Nichols said. In her opinion, as a lawyer and doctor in training, the situation “escalated very quickly and not very transparently.”
More than microaggressions
UVA points to an entirely different timeline. In fact, the school claims that neither Mr. Bhattacharya’s statements at the panel nor the tone with which he spoke there had any bearing on the decision to suspend him.
According to court documents, UVA denies that Mr. Bhattacharya “ever faced discipline because of the content of [his] speech at the panel discussion.” It also denies that the mandate for psychological evaluation was related to or in any way triggered by his behavior at the panel discussion.
UVA’s official statement on the case states: “The student in question was dismissed from the School of Medicine after a series of incidents and repeated instances of erratic behavior that raised security concerns as well as questions about his professionalism and fitness to practice medicine.”
The university cites two such incidents. The first is a meeting with Dr. Densmore at which Mr. Bhattacharya’s behavior was so concerning that he was escorted to the counseling center. After meeting with the counselor, Mr. Bhattacharya was involuntarily hospitalized afterward. At a second meeting with Dr. Densmore, UVA’s filing alleges that Mr. Bhattacharya’s behavior was so “erratic, aggressive, and concerning” that Dr. Densmore called the police. The school also cites a second involuntarily hospitalization and a restraining order against Mr. Bhattacharya by his girlfriend, a fellow medical student, as reasons for his suspension.
Mr. Bhattacharya’s girlfriend, Angel Hsu, a recent graduate of UVA medical school, has since been added to the list of defendants. Mr. Bhattacharya’s attorneys have called her a third-party coconspirator, working with Dr. Peterson and Dr. Densmore to have Mr. Bhattacharya removed from the university. Mr. Bhattacharya alleges that Dr. Hsu’s schemes started when he broke up with her the day before the microaggression panel. He claims that, during their relationship, she admitted to framing two other men for sexual misconduct during her undergraduate education at Emory. All of this is detailed in the 87-page document filed by Mr. Bhattacharya’s attorneys regarding his relationship with Dr. Hsu.
Alex Morey, JD, an attorney at the Foundation for Individual Rights in Education, said Mr. Bhattacharya is also alleged to have exhibited other threatening behavior on social media and in chat rooms. However, if Mr. Bhattacharya was suspended for reasons other than what he said at the panel, Ms. Morey said, the burden of proof is on the school. They’ll need to prove that the incidents listed, and not his speech, are the motivation for Mr. Bhattacharya’s removal from the program. “We haven’t seen [that] yet,” she said.
In a statement sent to this news organization by UVA Health Public Information Officer Eric Swensen, the school said, “It is worth noting, however, that the court’s recent ruling is based only on the facts as alleged by the plaintiff and must accept all of those allegations as true at this stage of the proceedings.”
Problems with professionalism policies
The case brings into focus concerns about professionalism policies in medical education. “Traditionally it’s been assumed that a physician has certain values, attributes, and behaviors that constitute professionals, which, in some ways, boil down to inspiring trust in him or her,” said Edward Krupat, PhD, associate professor of medicine at Harvard University.
However, many feel that these binding codes of student conduct allow institutions to inhibit civil rights under the guise of professionalism, a standard critics say is inconsistently and often ill-defined.
“They just didn’t like what he said and the way he said it,” Ms. Morey said about Mr. Bhattacharya. “That is not the same as someone engaging in behavior that fundamentally undermines the profession they are in.”
UVA Health’s professionalism policy prohibits conduct that is perceived as rude and says that a pattern of unprofessionalism – defined as three or more recorded events – or one egregious act of unprofessionalism can be punished with removal from the school. What remains to be seen is documented proof of the specific unprofessional or egregious acts that got Mr. Bhattacharya suspended. “Clearly it’s subjective,” Dr. Krupat said. And “there’s an ever-widening gray area” when it comes to these policies.
In a 2020 study of 108 medical graduates, Dr. Krupat and his collaborators found that those who had to go before their review board for professionalism concerns as students were more than five times more likely undergo disciplinary review during residency. They were two times more likely to be sued or sanctioned during their practice.
Dr. Krupat said that a traditional approach would be to look at the list of documented offenses and ask, “Would this be your first choice for a physician?” If the facts the dean alleges are true of Mr. Bhattacharya, then the answer may be no, Dr. Krupat said, based on his limited familiarity with the case. However, he said the situation may be “more complex than the dean says.”
What is unlikely, according to Dr. Krupat, is that medical staff were eager to quickly get rid of a student. In his experience, medical faculty often take extra precautions to understand, justify, and support medical students. There’s even a term in the medical education literature to describe faculty’s unrelenting tendency to stick with students: “failure to fail.” Dr. Krupat finds it “highly unusual that someone would say something in a gray area and be asked to leave.”
What a ruling may mean
Despite the many seemingly contradictory and gray areas, Ms. Morey sees it as cut-and-dried. “It’s a pretty clear First Amendment violation,” she said in an interview. “It’s been one of the more egregious cases we’ve seen lately.”
There are exceptions to free speech on college campuses, Ms. Morey said. Students have First Amendment rights; however, in the classroom setting, the professor and school also have the right to maintain an orderly environment. The panel opened the floor for questions. Thus, Mr. Bhattacharya’s counsel is arguing that the faculty essentially turned the program over to the students. According to Ms. Morey, because UVA hasn’t been able to prove that Mr. Bhattacharya’s discourse caused a “material disruption,” the First Amendment suit is moving forward.
“In a Q&A, the school has essentially created a public forum,” Ms. Morey said. “What they can’t do is open a forum for public speech and punish the speech [they] don’t like.” She said that the courts have historically ruled that a student still has their rights.
“A ruling against Kieran Bhattacharya, in this case, would hugely undermine the First Amendment rights of professional students at every program across the country,” Ms. Morey said.
However, Dr. Nichols said that there have also been cases where the judiciary chooses not to get involved with the self-governing of an individual institution. “It could be an uphill battle for the student,” she said. If UVA can prove their claim that Bhattacharya’s pattern of behavior – and not his commentary on microaggressions – is what put others at risk and was the cause of suspension, then the school’s decision will likely hold.
Dr. Krupat said this case comes at a time when everyone – both students and faculty – feel like they are walking on eggshells. Power dynamics are rightfully being called into question but “a pendulum stuck at one end never just swings to the middle and stops,” he said. Students are frightened that faculty will be insensitive. Faculty fear that if they give negative feedback they might be accused of bias. He does think this tension is “something that will resolve itself for the better in the future,” he said.
The jury trial is currently set for early January 2022. In the meantime, First Amendment advocates are “heartened” that the judge allowed the case to proceed while those concerned with professionalism policies continue to closely watch what happens next.
A version of this article first appeared on Medscape.com.
Kieran Bhattacharya was slated to graduate from University of Virginia (UVA) Medical School in 2021. But in late 2018, he was suspended. In early 2019, the University Threat Assessment Team went a step further, issuing Mr. Bhattacharya a no-trespass warning.
Mr. Bhattacharya claims the unraveling of his medical training was because of questions he asked at a UVA-hosted panel on microaggressions that took place 1 month before his suspension. His attorneys argue that, after making some admittedly less-than-collegial statements at a forum, the institution branded him as a threat. The school counters that Mr. Bhattacharya had a pattern of concerning, unprofessional behavior. The matter will now be settled in court.
UVA initially attempted to have Mr. Bhattacharya’s suit thrown out. A federal judge did dismiss three of four counts; however, he also ruled the lawsuit could move forward on the grounds that Mr. Bhattacharya’s First Amendment right to free speech was infringed.
Supporters claim that Mr. Bhattacharya was a student in good standing with the university, until he spoke publicly at the panel. They say the discipline he’s faced for those remarks is an egregious breach of free speech. Several experts say his case highlights the use – or rather misuse – of professionalism policies to undermine student freedoms and valuable discourse.
UVA argues that it’s not so simple and that the facts considered by the judge this spring were only part of the story. According to the defense, Mr. Bhattacharya’s side leaves out key details leading up to his suspension. The institution says Mr. Bhattacharya did and said things that provoked medical school officials to question the safety of the campus and his fitness to practice medicine. This news organization attempted to contact Mr. Bhattacharya several times through his attorneys and did not receive a response.
What happened at the microaggression panel
On this, both parties agree: A panel on microaggressions took place on Oct. 25, 2018. Mr. Bhattacharya, then a 2nd-year UVA medical student, was the first volunteer to speak when the floor was opened for questioning.
“Thank you for your presentation,” said Mr. Bhattacharya, according to an audio recording of the event. “I had a few questions, just to clarify your definition of microaggressions.” He then asked his first question: “Is it a requirement, to be a victim of microaggression, that you are a member of a marginalized group?”
The presenter, Beverly Colwell Adams, PhD, associate professor emeritus in the department of psychology and previously the assistant dean of UVA’s College of Arts and Sciences, said it was not. But before she could go on to explain, Mr. Bhattacharya interrupted, speaking quickly. “But in the definition, it just said you had to be a member of a marginalized group, in the definition you used on the last slide. So that’s contradictory.” Dr. Adams responded. “What I had there is kind of the generalized definition,” she said. “In fact, I extend it beyond that.”
Mr. Bhattacharya asked a second question – to which Dr. Adams responded – about defining a marginalized group. Then, during a third question about differentiating between microaggressions and unintentional rude statements, Mr. Bhattacharya sped up again, repeating some of Dr. Adams’ own presentation back to her. He then asked if she had done any other research on microaggression, after calling the evidence she provided “one anecdotal case.” Dr. Adams responded with an example.
Mr. Bhattacharya’s fourth question was then intercepted by a fellow panelist, Sara Rasmussen, MD. She offered an anecdote about her own experience with microaggression, as a person from rural West Virginia. She offered some advice on understanding the impact of your actions and then advised, “You have to learn to uncouple the intent of what you’re saying and the impact it has on the audience.”
Mr. Bhattacharya briefly disagreed with Dr. Rasmussen, and then called the evidence Dr. Adams presented “anecdotal” a second time. At that point, Dr. Rasmussen interrupted him to say that Dr. Adams had offered “a lot of citations from the literature” and then called on another student to ask a question.
In total, Mr. Bhattacharya engaged with the panel for just over 5 minutes. He is now arguing in court that those 5 minutes forever changed his life.
Blindsided
After the event, according to court documents, Nora Kern, MD, and one of the panelists filed a professionalism concern card about Mr. Bhattacharya’s discourse. “This student asked a series of questions that were quite antagonistic toward the panel. He pressed on and stated one faculty member was being contradictory. His level of frustration/anger seemed to escalate until another faculty member defused the situation by calling on another student for questions,” Dr. Kern wrote on the card that was later included in Mr. Bhattacharya’s case filing.
According to Regina Rini, PhD, Canada research chair in philosophy of moral and social cognition at York University in Toronto, there are two layers to Mr. Bhattacharya’s discussion with the panel. She told this news organization that the first level is the content of the conversation: “His very first question was a very reasonable one.” Since the 1970s, when Chester Pierce first coined the term microaggression, most experts have agreed that the action must be directed at a person within a marginalized group. “It sounds like the presenter has a nuanced view,” Dr. Rini said. She added that his “was a fair question to ask.”
However, Dr. Rini said the second layer – the way conversation took place – is a separate concern. “Maybe two rounds of questions later, he starts speaking quickly” and fires off multiple questions one after the other, when asking if Dr. Adams had any evidence, and called her support anecdotal, Dr. Rini said. “That’s not a cooperative attempt to hear an answer.”
“He’s a little antagonistic,” Alana Nichols, JD, MD, attorney and a medical pediatrics intern at the University of Alabama at Birmingham, said after listening to the recording. “He did sound like he had an agenda and was not being receptive to what they were saying.” However, Dr. Nichols said, “What brought me pause as someone in medicine was the way it escalated.”
After Dr. Kern filed the professionalism concern card, two faculty members contacted Mr. Bhattacharya. Christine Peterson, MD, assistant dean for medical education, emailed to ask if he wanted to discuss how to navigate uncomfortable conversations and how to cope with “unintended consequences of conversations.” The day after the panel, John Densmore, MD, associate dean for admissions and student affairs, emailed Mr. Bhattacharya, asking to meet the following week.
Mr. Bhattacharya met with both deans. Dr. Peterson only briefly mentioned the panel. Dr. Densmore didn’t at all, according to court documents. Dr. Densmore also didn’t mention the professionalism concern card to Mr. Bhattacharya. However, the Academic Standards and Achievement Committee discussed it about 2 weeks later, at their monthly meeting.
Dr. Kern was the only voting member present who actually witnessed the microaggression panel. Dr. Peterson was there as a guest. The committee voted unanimously to send Mr. Bhattacharya a letter, reminding him of the importance of showing respect to everyone. The letter was sent the following day, Nov. 14, 2018. Mr. Bhattacharya still had no knowledge of the professionalism concern card.
On Nov. 26, Dr. Densmore sent Mr. Bhattacharya an email that read: “We were notified by the Dean of Students Office that you were heading back to Charlottesville. You will need to be seen by CAPS [Counseling and Psychological Services] before you can return to classes.”
On Nov. 27, court records show Mr. Bhattacharya emailed Dr. Densmore, questioning the school’s ability to mandate psychiatric evaluation. The decision was reinforced with an email from the then senior associate dean for education at UVA Medical School. Mr. Bhattacharya was not permitted to return to class without the evaluation.
“If I were in his situation, I would feel kind of blindsided,” Dr. Nichols said. Mr. Bhattacharya met with two deans immediately after the event, during which he said his conduct with the panel was barely or not at all mentioned. To him, the situation could well have seemed to be over, Dr. Nichols said. In her opinion, as a lawyer and doctor in training, the situation “escalated very quickly and not very transparently.”
More than microaggressions
UVA points to an entirely different timeline. In fact, the school claims that neither Mr. Bhattacharya’s statements at the panel nor the tone with which he spoke there had any bearing on the decision to suspend him.
According to court documents, UVA denies that Mr. Bhattacharya “ever faced discipline because of the content of [his] speech at the panel discussion.” It also denies that the mandate for psychological evaluation was related to or in any way triggered by his behavior at the panel discussion.
UVA’s official statement on the case states: “The student in question was dismissed from the School of Medicine after a series of incidents and repeated instances of erratic behavior that raised security concerns as well as questions about his professionalism and fitness to practice medicine.”
The university cites two such incidents. The first is a meeting with Dr. Densmore at which Mr. Bhattacharya’s behavior was so concerning that he was escorted to the counseling center. After meeting with the counselor, Mr. Bhattacharya was involuntarily hospitalized afterward. At a second meeting with Dr. Densmore, UVA’s filing alleges that Mr. Bhattacharya’s behavior was so “erratic, aggressive, and concerning” that Dr. Densmore called the police. The school also cites a second involuntarily hospitalization and a restraining order against Mr. Bhattacharya by his girlfriend, a fellow medical student, as reasons for his suspension.
Mr. Bhattacharya’s girlfriend, Angel Hsu, a recent graduate of UVA medical school, has since been added to the list of defendants. Mr. Bhattacharya’s attorneys have called her a third-party coconspirator, working with Dr. Peterson and Dr. Densmore to have Mr. Bhattacharya removed from the university. Mr. Bhattacharya alleges that Dr. Hsu’s schemes started when he broke up with her the day before the microaggression panel. He claims that, during their relationship, she admitted to framing two other men for sexual misconduct during her undergraduate education at Emory. All of this is detailed in the 87-page document filed by Mr. Bhattacharya’s attorneys regarding his relationship with Dr. Hsu.
Alex Morey, JD, an attorney at the Foundation for Individual Rights in Education, said Mr. Bhattacharya is also alleged to have exhibited other threatening behavior on social media and in chat rooms. However, if Mr. Bhattacharya was suspended for reasons other than what he said at the panel, Ms. Morey said, the burden of proof is on the school. They’ll need to prove that the incidents listed, and not his speech, are the motivation for Mr. Bhattacharya’s removal from the program. “We haven’t seen [that] yet,” she said.
In a statement sent to this news organization by UVA Health Public Information Officer Eric Swensen, the school said, “It is worth noting, however, that the court’s recent ruling is based only on the facts as alleged by the plaintiff and must accept all of those allegations as true at this stage of the proceedings.”
Problems with professionalism policies
The case brings into focus concerns about professionalism policies in medical education. “Traditionally it’s been assumed that a physician has certain values, attributes, and behaviors that constitute professionals, which, in some ways, boil down to inspiring trust in him or her,” said Edward Krupat, PhD, associate professor of medicine at Harvard University.
However, many feel that these binding codes of student conduct allow institutions to inhibit civil rights under the guise of professionalism, a standard critics say is inconsistently and often ill-defined.
“They just didn’t like what he said and the way he said it,” Ms. Morey said about Mr. Bhattacharya. “That is not the same as someone engaging in behavior that fundamentally undermines the profession they are in.”
UVA Health’s professionalism policy prohibits conduct that is perceived as rude and says that a pattern of unprofessionalism – defined as three or more recorded events – or one egregious act of unprofessionalism can be punished with removal from the school. What remains to be seen is documented proof of the specific unprofessional or egregious acts that got Mr. Bhattacharya suspended. “Clearly it’s subjective,” Dr. Krupat said. And “there’s an ever-widening gray area” when it comes to these policies.
In a 2020 study of 108 medical graduates, Dr. Krupat and his collaborators found that those who had to go before their review board for professionalism concerns as students were more than five times more likely undergo disciplinary review during residency. They were two times more likely to be sued or sanctioned during their practice.
Dr. Krupat said that a traditional approach would be to look at the list of documented offenses and ask, “Would this be your first choice for a physician?” If the facts the dean alleges are true of Mr. Bhattacharya, then the answer may be no, Dr. Krupat said, based on his limited familiarity with the case. However, he said the situation may be “more complex than the dean says.”
What is unlikely, according to Dr. Krupat, is that medical staff were eager to quickly get rid of a student. In his experience, medical faculty often take extra precautions to understand, justify, and support medical students. There’s even a term in the medical education literature to describe faculty’s unrelenting tendency to stick with students: “failure to fail.” Dr. Krupat finds it “highly unusual that someone would say something in a gray area and be asked to leave.”
What a ruling may mean
Despite the many seemingly contradictory and gray areas, Ms. Morey sees it as cut-and-dried. “It’s a pretty clear First Amendment violation,” she said in an interview. “It’s been one of the more egregious cases we’ve seen lately.”
There are exceptions to free speech on college campuses, Ms. Morey said. Students have First Amendment rights; however, in the classroom setting, the professor and school also have the right to maintain an orderly environment. The panel opened the floor for questions. Thus, Mr. Bhattacharya’s counsel is arguing that the faculty essentially turned the program over to the students. According to Ms. Morey, because UVA hasn’t been able to prove that Mr. Bhattacharya’s discourse caused a “material disruption,” the First Amendment suit is moving forward.
“In a Q&A, the school has essentially created a public forum,” Ms. Morey said. “What they can’t do is open a forum for public speech and punish the speech [they] don’t like.” She said that the courts have historically ruled that a student still has their rights.
“A ruling against Kieran Bhattacharya, in this case, would hugely undermine the First Amendment rights of professional students at every program across the country,” Ms. Morey said.
However, Dr. Nichols said that there have also been cases where the judiciary chooses not to get involved with the self-governing of an individual institution. “It could be an uphill battle for the student,” she said. If UVA can prove their claim that Bhattacharya’s pattern of behavior – and not his commentary on microaggressions – is what put others at risk and was the cause of suspension, then the school’s decision will likely hold.
Dr. Krupat said this case comes at a time when everyone – both students and faculty – feel like they are walking on eggshells. Power dynamics are rightfully being called into question but “a pendulum stuck at one end never just swings to the middle and stops,” he said. Students are frightened that faculty will be insensitive. Faculty fear that if they give negative feedback they might be accused of bias. He does think this tension is “something that will resolve itself for the better in the future,” he said.
The jury trial is currently set for early January 2022. In the meantime, First Amendment advocates are “heartened” that the judge allowed the case to proceed while those concerned with professionalism policies continue to closely watch what happens next.
A version of this article first appeared on Medscape.com.
Kieran Bhattacharya was slated to graduate from University of Virginia (UVA) Medical School in 2021. But in late 2018, he was suspended. In early 2019, the University Threat Assessment Team went a step further, issuing Mr. Bhattacharya a no-trespass warning.
Mr. Bhattacharya claims the unraveling of his medical training was because of questions he asked at a UVA-hosted panel on microaggressions that took place 1 month before his suspension. His attorneys argue that, after making some admittedly less-than-collegial statements at a forum, the institution branded him as a threat. The school counters that Mr. Bhattacharya had a pattern of concerning, unprofessional behavior. The matter will now be settled in court.
UVA initially attempted to have Mr. Bhattacharya’s suit thrown out. A federal judge did dismiss three of four counts; however, he also ruled the lawsuit could move forward on the grounds that Mr. Bhattacharya’s First Amendment right to free speech was infringed.
Supporters claim that Mr. Bhattacharya was a student in good standing with the university, until he spoke publicly at the panel. They say the discipline he’s faced for those remarks is an egregious breach of free speech. Several experts say his case highlights the use – or rather misuse – of professionalism policies to undermine student freedoms and valuable discourse.
UVA argues that it’s not so simple and that the facts considered by the judge this spring were only part of the story. According to the defense, Mr. Bhattacharya’s side leaves out key details leading up to his suspension. The institution says Mr. Bhattacharya did and said things that provoked medical school officials to question the safety of the campus and his fitness to practice medicine. This news organization attempted to contact Mr. Bhattacharya several times through his attorneys and did not receive a response.
What happened at the microaggression panel
On this, both parties agree: A panel on microaggressions took place on Oct. 25, 2018. Mr. Bhattacharya, then a 2nd-year UVA medical student, was the first volunteer to speak when the floor was opened for questioning.
“Thank you for your presentation,” said Mr. Bhattacharya, according to an audio recording of the event. “I had a few questions, just to clarify your definition of microaggressions.” He then asked his first question: “Is it a requirement, to be a victim of microaggression, that you are a member of a marginalized group?”
The presenter, Beverly Colwell Adams, PhD, associate professor emeritus in the department of psychology and previously the assistant dean of UVA’s College of Arts and Sciences, said it was not. But before she could go on to explain, Mr. Bhattacharya interrupted, speaking quickly. “But in the definition, it just said you had to be a member of a marginalized group, in the definition you used on the last slide. So that’s contradictory.” Dr. Adams responded. “What I had there is kind of the generalized definition,” she said. “In fact, I extend it beyond that.”
Mr. Bhattacharya asked a second question – to which Dr. Adams responded – about defining a marginalized group. Then, during a third question about differentiating between microaggressions and unintentional rude statements, Mr. Bhattacharya sped up again, repeating some of Dr. Adams’ own presentation back to her. He then asked if she had done any other research on microaggression, after calling the evidence she provided “one anecdotal case.” Dr. Adams responded with an example.
Mr. Bhattacharya’s fourth question was then intercepted by a fellow panelist, Sara Rasmussen, MD. She offered an anecdote about her own experience with microaggression, as a person from rural West Virginia. She offered some advice on understanding the impact of your actions and then advised, “You have to learn to uncouple the intent of what you’re saying and the impact it has on the audience.”
Mr. Bhattacharya briefly disagreed with Dr. Rasmussen, and then called the evidence Dr. Adams presented “anecdotal” a second time. At that point, Dr. Rasmussen interrupted him to say that Dr. Adams had offered “a lot of citations from the literature” and then called on another student to ask a question.
In total, Mr. Bhattacharya engaged with the panel for just over 5 minutes. He is now arguing in court that those 5 minutes forever changed his life.
Blindsided
After the event, according to court documents, Nora Kern, MD, and one of the panelists filed a professionalism concern card about Mr. Bhattacharya’s discourse. “This student asked a series of questions that were quite antagonistic toward the panel. He pressed on and stated one faculty member was being contradictory. His level of frustration/anger seemed to escalate until another faculty member defused the situation by calling on another student for questions,” Dr. Kern wrote on the card that was later included in Mr. Bhattacharya’s case filing.
According to Regina Rini, PhD, Canada research chair in philosophy of moral and social cognition at York University in Toronto, there are two layers to Mr. Bhattacharya’s discussion with the panel. She told this news organization that the first level is the content of the conversation: “His very first question was a very reasonable one.” Since the 1970s, when Chester Pierce first coined the term microaggression, most experts have agreed that the action must be directed at a person within a marginalized group. “It sounds like the presenter has a nuanced view,” Dr. Rini said. She added that his “was a fair question to ask.”
However, Dr. Rini said the second layer – the way conversation took place – is a separate concern. “Maybe two rounds of questions later, he starts speaking quickly” and fires off multiple questions one after the other, when asking if Dr. Adams had any evidence, and called her support anecdotal, Dr. Rini said. “That’s not a cooperative attempt to hear an answer.”
“He’s a little antagonistic,” Alana Nichols, JD, MD, attorney and a medical pediatrics intern at the University of Alabama at Birmingham, said after listening to the recording. “He did sound like he had an agenda and was not being receptive to what they were saying.” However, Dr. Nichols said, “What brought me pause as someone in medicine was the way it escalated.”
After Dr. Kern filed the professionalism concern card, two faculty members contacted Mr. Bhattacharya. Christine Peterson, MD, assistant dean for medical education, emailed to ask if he wanted to discuss how to navigate uncomfortable conversations and how to cope with “unintended consequences of conversations.” The day after the panel, John Densmore, MD, associate dean for admissions and student affairs, emailed Mr. Bhattacharya, asking to meet the following week.
Mr. Bhattacharya met with both deans. Dr. Peterson only briefly mentioned the panel. Dr. Densmore didn’t at all, according to court documents. Dr. Densmore also didn’t mention the professionalism concern card to Mr. Bhattacharya. However, the Academic Standards and Achievement Committee discussed it about 2 weeks later, at their monthly meeting.
Dr. Kern was the only voting member present who actually witnessed the microaggression panel. Dr. Peterson was there as a guest. The committee voted unanimously to send Mr. Bhattacharya a letter, reminding him of the importance of showing respect to everyone. The letter was sent the following day, Nov. 14, 2018. Mr. Bhattacharya still had no knowledge of the professionalism concern card.
On Nov. 26, Dr. Densmore sent Mr. Bhattacharya an email that read: “We were notified by the Dean of Students Office that you were heading back to Charlottesville. You will need to be seen by CAPS [Counseling and Psychological Services] before you can return to classes.”
On Nov. 27, court records show Mr. Bhattacharya emailed Dr. Densmore, questioning the school’s ability to mandate psychiatric evaluation. The decision was reinforced with an email from the then senior associate dean for education at UVA Medical School. Mr. Bhattacharya was not permitted to return to class without the evaluation.
“If I were in his situation, I would feel kind of blindsided,” Dr. Nichols said. Mr. Bhattacharya met with two deans immediately after the event, during which he said his conduct with the panel was barely or not at all mentioned. To him, the situation could well have seemed to be over, Dr. Nichols said. In her opinion, as a lawyer and doctor in training, the situation “escalated very quickly and not very transparently.”
More than microaggressions
UVA points to an entirely different timeline. In fact, the school claims that neither Mr. Bhattacharya’s statements at the panel nor the tone with which he spoke there had any bearing on the decision to suspend him.
According to court documents, UVA denies that Mr. Bhattacharya “ever faced discipline because of the content of [his] speech at the panel discussion.” It also denies that the mandate for psychological evaluation was related to or in any way triggered by his behavior at the panel discussion.
UVA’s official statement on the case states: “The student in question was dismissed from the School of Medicine after a series of incidents and repeated instances of erratic behavior that raised security concerns as well as questions about his professionalism and fitness to practice medicine.”
The university cites two such incidents. The first is a meeting with Dr. Densmore at which Mr. Bhattacharya’s behavior was so concerning that he was escorted to the counseling center. After meeting with the counselor, Mr. Bhattacharya was involuntarily hospitalized afterward. At a second meeting with Dr. Densmore, UVA’s filing alleges that Mr. Bhattacharya’s behavior was so “erratic, aggressive, and concerning” that Dr. Densmore called the police. The school also cites a second involuntarily hospitalization and a restraining order against Mr. Bhattacharya by his girlfriend, a fellow medical student, as reasons for his suspension.
Mr. Bhattacharya’s girlfriend, Angel Hsu, a recent graduate of UVA medical school, has since been added to the list of defendants. Mr. Bhattacharya’s attorneys have called her a third-party coconspirator, working with Dr. Peterson and Dr. Densmore to have Mr. Bhattacharya removed from the university. Mr. Bhattacharya alleges that Dr. Hsu’s schemes started when he broke up with her the day before the microaggression panel. He claims that, during their relationship, she admitted to framing two other men for sexual misconduct during her undergraduate education at Emory. All of this is detailed in the 87-page document filed by Mr. Bhattacharya’s attorneys regarding his relationship with Dr. Hsu.
Alex Morey, JD, an attorney at the Foundation for Individual Rights in Education, said Mr. Bhattacharya is also alleged to have exhibited other threatening behavior on social media and in chat rooms. However, if Mr. Bhattacharya was suspended for reasons other than what he said at the panel, Ms. Morey said, the burden of proof is on the school. They’ll need to prove that the incidents listed, and not his speech, are the motivation for Mr. Bhattacharya’s removal from the program. “We haven’t seen [that] yet,” she said.
In a statement sent to this news organization by UVA Health Public Information Officer Eric Swensen, the school said, “It is worth noting, however, that the court’s recent ruling is based only on the facts as alleged by the plaintiff and must accept all of those allegations as true at this stage of the proceedings.”
Problems with professionalism policies
The case brings into focus concerns about professionalism policies in medical education. “Traditionally it’s been assumed that a physician has certain values, attributes, and behaviors that constitute professionals, which, in some ways, boil down to inspiring trust in him or her,” said Edward Krupat, PhD, associate professor of medicine at Harvard University.
However, many feel that these binding codes of student conduct allow institutions to inhibit civil rights under the guise of professionalism, a standard critics say is inconsistently and often ill-defined.
“They just didn’t like what he said and the way he said it,” Ms. Morey said about Mr. Bhattacharya. “That is not the same as someone engaging in behavior that fundamentally undermines the profession they are in.”
UVA Health’s professionalism policy prohibits conduct that is perceived as rude and says that a pattern of unprofessionalism – defined as three or more recorded events – or one egregious act of unprofessionalism can be punished with removal from the school. What remains to be seen is documented proof of the specific unprofessional or egregious acts that got Mr. Bhattacharya suspended. “Clearly it’s subjective,” Dr. Krupat said. And “there’s an ever-widening gray area” when it comes to these policies.
In a 2020 study of 108 medical graduates, Dr. Krupat and his collaborators found that those who had to go before their review board for professionalism concerns as students were more than five times more likely undergo disciplinary review during residency. They were two times more likely to be sued or sanctioned during their practice.
Dr. Krupat said that a traditional approach would be to look at the list of documented offenses and ask, “Would this be your first choice for a physician?” If the facts the dean alleges are true of Mr. Bhattacharya, then the answer may be no, Dr. Krupat said, based on his limited familiarity with the case. However, he said the situation may be “more complex than the dean says.”
What is unlikely, according to Dr. Krupat, is that medical staff were eager to quickly get rid of a student. In his experience, medical faculty often take extra precautions to understand, justify, and support medical students. There’s even a term in the medical education literature to describe faculty’s unrelenting tendency to stick with students: “failure to fail.” Dr. Krupat finds it “highly unusual that someone would say something in a gray area and be asked to leave.”
What a ruling may mean
Despite the many seemingly contradictory and gray areas, Ms. Morey sees it as cut-and-dried. “It’s a pretty clear First Amendment violation,” she said in an interview. “It’s been one of the more egregious cases we’ve seen lately.”
There are exceptions to free speech on college campuses, Ms. Morey said. Students have First Amendment rights; however, in the classroom setting, the professor and school also have the right to maintain an orderly environment. The panel opened the floor for questions. Thus, Mr. Bhattacharya’s counsel is arguing that the faculty essentially turned the program over to the students. According to Ms. Morey, because UVA hasn’t been able to prove that Mr. Bhattacharya’s discourse caused a “material disruption,” the First Amendment suit is moving forward.
“In a Q&A, the school has essentially created a public forum,” Ms. Morey said. “What they can’t do is open a forum for public speech and punish the speech [they] don’t like.” She said that the courts have historically ruled that a student still has their rights.
“A ruling against Kieran Bhattacharya, in this case, would hugely undermine the First Amendment rights of professional students at every program across the country,” Ms. Morey said.
However, Dr. Nichols said that there have also been cases where the judiciary chooses not to get involved with the self-governing of an individual institution. “It could be an uphill battle for the student,” she said. If UVA can prove their claim that Bhattacharya’s pattern of behavior – and not his commentary on microaggressions – is what put others at risk and was the cause of suspension, then the school’s decision will likely hold.
Dr. Krupat said this case comes at a time when everyone – both students and faculty – feel like they are walking on eggshells. Power dynamics are rightfully being called into question but “a pendulum stuck at one end never just swings to the middle and stops,” he said. Students are frightened that faculty will be insensitive. Faculty fear that if they give negative feedback they might be accused of bias. He does think this tension is “something that will resolve itself for the better in the future,” he said.
The jury trial is currently set for early January 2022. In the meantime, First Amendment advocates are “heartened” that the judge allowed the case to proceed while those concerned with professionalism policies continue to closely watch what happens next.
A version of this article first appeared on Medscape.com.
ED docs are cleaning up the messes of medical tourism
It was a typical, busy evening shift in the emergency department (ED) when Steve Carroll, DO, an emergency medicine physician in the Philadelphia area, noticed an odd listing on the tracking board. In the waiting room, there was someone whose chief complaint was that she needed to have surgical drains pulled.
According to the woman’s chart, she’d undergone liposuction in Miami a week before. The surgeon had effectively relinquished all follow-up care to the woman’s local ED.
Dr. Carroll searched the name of her surgeon and found that his site “specifically advertised medical tourism,” Dr. Carroll said. The site lured patients with the idea of recovering by the beach and that a local nurse would come to their room every day.
But when Dr. Carroll told the patient that her surgeon should be the one who removes the drains, she became concerned. She didn’t know that her surgeon wasn’t providing the standard of care, he said. Somewhat appalled that a board-certified plastic surgeon would place the burden of follow-up care on an ED doctor hundreds of miles away, Dr. Carroll posted the case to Twitter and several Facebook groups.
“Yes I could refuse to take [the drains] out but that’s not patient-centered care,” Dr. Carroll wrote in a Twitter thread. “It’s unfairly shifting routine outpatient surgical followup (and liability) onto me and extra cost to [the patient].” Comments from ED physicians and sympathetic surgeons across the country flowed in. Dr. Carroll quickly realized his situation was part of a much larger problem than he’d thought.
Dr. Carroll’s patient told him that the Miami surgery cost less than undergoing the surgery locally; that’s why she’d made the trip. She’s not alone. Traveling to get the lowest price for a plastic surgery procedure has been a rising phenomenon since the early 2000s, according to the American Society of Plastic Surgeons (ASPS). Many countries are actively fostering their medical tourism industries, as are states such as Florida.
People have long traveled to get the best medical care. But “medical tourism is completely different,” said Alan Matarasso, MD, FACS, a Manhattan-based plastic surgeon and member of the ASPS Executive Committee. “People [are] traveling to get a simultaneous vacation or lower cost,” he said.
Choosing facilities on the basis of these criteria comes with myriad problems, and the quality of medical care may be lower. It’s difficult to verify the credentials of the surgeons, anesthesiologists, and facilities involved. Medical records can be in a different language, and traveling immediately after surgery increases the risk for pulmonary embolism and death, not to mention the added complications of traveling and being a surgical patient during the COVID-19 pandemic, he said.
Typically, surgeons are protective of their patients. But Murtaza Akhter, MD, an emergency medicine physician based in Miami, says it’s the opposite with the medical tourism surgeons whose patients regularly end up in his ED. “There’s almost no ownership,” he said. “Every time, [the patients] say, ‘My doctor isn’t responding,’ or they said go to the ER.” And that’s before they’ve even made it out of Miami.
The most common cosmetic surgery complications Dr. Akhter sees occur in patients who’ve undergone so-called Brazilian butt lifts. They show up in his ED face down, suffering from severe blood loss. He has them undergo a transfusion and maybe some imaging, but if they need a higher degree of care, they have to be transferred. “There’s a reason it’s cheaper,” he said.
Medical tourism mishaps are such a regular occurrence in Miami that no one flinches when the patients show up in the ED, Dr. Akhter said. He had begun to think he was overreacting to the problem until he saw Dr. Carroll’s Twitter thread.
“Since it’s daily, I just thought maybe I had gone crazy and that it’s considered normal for plastic surgeons to do this. Thanks for making me feel sane again,” Dr. Akhter tweeted in a reply to Dr. Carroll.
There are no reliable data as to of how often or where such surgeries are occurring or of patients’ outcomes. But Nicholas Genes, MD, an ED physician in Manhattan, says he sees far more postsurgical patients who traveled for their procedures than ones who underwent surgery locally. He can’t say for certain whether that’s because procedures performed by doctors in New York City have fewer complications or the physicians just handle postprocedure problems themselves.
In a 2021 systematic review of aesthetic breast surgeries performed through medical tourism, researchers found that of 171 patients who traveled for surgery, 88 (51%) had a total of 106 complications that required returning to the operating room and undergoing general anesthesia. They also found that 39% of breast augmentation implant surgeries required either a unilateral or bilateral explantation procedure after patients returned home.
The rate of complications was higher than the study authors had expected. “These are totally elective procedures,” Dr. Matarasso said. “They should be optimized.” And high rates of complications come with hefty price tags.
The cost of managing these complications, which falls to the home healthcare system or the patient themselves, can range from $5,500 (determined on the basis of data from a 2019 study in the United Kingdom) to as much as $123,000, researchers in New York City calculated, if the patient develops a complicated mycobacterium infection.
“In your effort to get a good deal or around the system, you could still end up with a lot of extensive medical bills if something goes wrong,” Dr. Genes said.
The liability dilemma
Many of the ED physicians Dr. Carroll heard from said that they wouldn’t have treated the woman who needed to have drains removed. Unlike the Brazilian-butt-lifts-gone-wrong in Miami or the complications Dr. Genes sees in New York City, Dr. Carroll’s patient wasn’t in a state of emergency. Most ED physicians said they would have sent her on her way to find a surgeon.
“In general, we shouldn’t be doing things we aren’t trained to do. It’s sort of a slippery slope,” Dr. Genes said. He’s comfortable with removing stitches, but for surgical drains and plastic apparatuses, “I don’t feel particularly well trained. I’d have to consult a colleague in general surgery,” he said. When he does get one of these patients, he works the phones to find a plastic surgeon who will see the patient, something he says their original plastic surgeon should have done.
“Sitting there with the patient, I felt a little bad for her,” Dr. Carroll said. “I knew if I didn’t do it, it would be weeks while she bounced around to urgent care, primary care, and finally found a surgeon.” But by removing the drains, he did shift some of the liability to himself. “If she developed a wound infection, then I’m on the hook for [that],” he said. “If I send her away, I have less liability but didn’t quite do the right thing for the patient.”
In replies to Dr. Carroll’s thread, some doctors debated whether these types of cases, particularly those in which surgeons forgo follow-up care, could be considered medical abandonment. Legal experts say that’s not exactly the case, at least it would not be the case with Dr. Carroll’s patient.
“I don’t think they’ve abandoned the patient; I think they’ve abandoned care,” said Michael Flynn, JD, professor of personal injury law at Nova Southeastern University, in Fort Lauderdale–Davie, Fla. “And that abandonment of follow-up care, if it falls below the standard of what medical professionals should do, then it’s malpractice.”
“The doctor didn’t just walk away and become unreachable,” said Bernard Black, JD, a medical malpractice attorney and law professor at Northwestern University, in Evanston, Ill. Technically, the surgeon referred the patient to the ED. Mr. Black agreed that it sounds more like a question of malpractice, “but without real damages, there’s no claim.”
Even if not illegal, sending these patients to the ED is still highly unethical, Dr. Carroll said. The authors of a 2014 article in Aesthetic Plastic Surgery concur: “It is the duty and ethical responsibility of plastic surgeons to prevent unnecessary complications following tourism medicine by adequately counseling patients, defining perioperative treatment protocols, and reporting complications to regional and specialty-specific governing bodies,” they write.
Sometimes patients need to travel, Dr. Matarasso said. Recently, three out-of-state patients came to him for procedures. Two stayed in Manhattan until their follow-up care was finished; he arranged care elsewhere for the third. It’s the operating surgeon’s job to connect patients with someone who can provide follow-up care when they go home, Dr. Matarasso said. If a surgeon doesn’t have a connection in a patient’s home city, the ASPS has a referral service to help, he said.
“My frustration was never with the patient,” Dr. Carroll said. “No one should feel bad about coming to an ED for literally anything, and I mean that. My frustration is with the surgeon who didn’t go the one extra step to arrange her follow-up.”
A version of this article first appeared on Medscape.com.
It was a typical, busy evening shift in the emergency department (ED) when Steve Carroll, DO, an emergency medicine physician in the Philadelphia area, noticed an odd listing on the tracking board. In the waiting room, there was someone whose chief complaint was that she needed to have surgical drains pulled.
According to the woman’s chart, she’d undergone liposuction in Miami a week before. The surgeon had effectively relinquished all follow-up care to the woman’s local ED.
Dr. Carroll searched the name of her surgeon and found that his site “specifically advertised medical tourism,” Dr. Carroll said. The site lured patients with the idea of recovering by the beach and that a local nurse would come to their room every day.
But when Dr. Carroll told the patient that her surgeon should be the one who removes the drains, she became concerned. She didn’t know that her surgeon wasn’t providing the standard of care, he said. Somewhat appalled that a board-certified plastic surgeon would place the burden of follow-up care on an ED doctor hundreds of miles away, Dr. Carroll posted the case to Twitter and several Facebook groups.
“Yes I could refuse to take [the drains] out but that’s not patient-centered care,” Dr. Carroll wrote in a Twitter thread. “It’s unfairly shifting routine outpatient surgical followup (and liability) onto me and extra cost to [the patient].” Comments from ED physicians and sympathetic surgeons across the country flowed in. Dr. Carroll quickly realized his situation was part of a much larger problem than he’d thought.
Dr. Carroll’s patient told him that the Miami surgery cost less than undergoing the surgery locally; that’s why she’d made the trip. She’s not alone. Traveling to get the lowest price for a plastic surgery procedure has been a rising phenomenon since the early 2000s, according to the American Society of Plastic Surgeons (ASPS). Many countries are actively fostering their medical tourism industries, as are states such as Florida.
People have long traveled to get the best medical care. But “medical tourism is completely different,” said Alan Matarasso, MD, FACS, a Manhattan-based plastic surgeon and member of the ASPS Executive Committee. “People [are] traveling to get a simultaneous vacation or lower cost,” he said.
Choosing facilities on the basis of these criteria comes with myriad problems, and the quality of medical care may be lower. It’s difficult to verify the credentials of the surgeons, anesthesiologists, and facilities involved. Medical records can be in a different language, and traveling immediately after surgery increases the risk for pulmonary embolism and death, not to mention the added complications of traveling and being a surgical patient during the COVID-19 pandemic, he said.
Typically, surgeons are protective of their patients. But Murtaza Akhter, MD, an emergency medicine physician based in Miami, says it’s the opposite with the medical tourism surgeons whose patients regularly end up in his ED. “There’s almost no ownership,” he said. “Every time, [the patients] say, ‘My doctor isn’t responding,’ or they said go to the ER.” And that’s before they’ve even made it out of Miami.
The most common cosmetic surgery complications Dr. Akhter sees occur in patients who’ve undergone so-called Brazilian butt lifts. They show up in his ED face down, suffering from severe blood loss. He has them undergo a transfusion and maybe some imaging, but if they need a higher degree of care, they have to be transferred. “There’s a reason it’s cheaper,” he said.
Medical tourism mishaps are such a regular occurrence in Miami that no one flinches when the patients show up in the ED, Dr. Akhter said. He had begun to think he was overreacting to the problem until he saw Dr. Carroll’s Twitter thread.
“Since it’s daily, I just thought maybe I had gone crazy and that it’s considered normal for plastic surgeons to do this. Thanks for making me feel sane again,” Dr. Akhter tweeted in a reply to Dr. Carroll.
There are no reliable data as to of how often or where such surgeries are occurring or of patients’ outcomes. But Nicholas Genes, MD, an ED physician in Manhattan, says he sees far more postsurgical patients who traveled for their procedures than ones who underwent surgery locally. He can’t say for certain whether that’s because procedures performed by doctors in New York City have fewer complications or the physicians just handle postprocedure problems themselves.
In a 2021 systematic review of aesthetic breast surgeries performed through medical tourism, researchers found that of 171 patients who traveled for surgery, 88 (51%) had a total of 106 complications that required returning to the operating room and undergoing general anesthesia. They also found that 39% of breast augmentation implant surgeries required either a unilateral or bilateral explantation procedure after patients returned home.
The rate of complications was higher than the study authors had expected. “These are totally elective procedures,” Dr. Matarasso said. “They should be optimized.” And high rates of complications come with hefty price tags.
The cost of managing these complications, which falls to the home healthcare system or the patient themselves, can range from $5,500 (determined on the basis of data from a 2019 study in the United Kingdom) to as much as $123,000, researchers in New York City calculated, if the patient develops a complicated mycobacterium infection.
“In your effort to get a good deal or around the system, you could still end up with a lot of extensive medical bills if something goes wrong,” Dr. Genes said.
The liability dilemma
Many of the ED physicians Dr. Carroll heard from said that they wouldn’t have treated the woman who needed to have drains removed. Unlike the Brazilian-butt-lifts-gone-wrong in Miami or the complications Dr. Genes sees in New York City, Dr. Carroll’s patient wasn’t in a state of emergency. Most ED physicians said they would have sent her on her way to find a surgeon.
“In general, we shouldn’t be doing things we aren’t trained to do. It’s sort of a slippery slope,” Dr. Genes said. He’s comfortable with removing stitches, but for surgical drains and plastic apparatuses, “I don’t feel particularly well trained. I’d have to consult a colleague in general surgery,” he said. When he does get one of these patients, he works the phones to find a plastic surgeon who will see the patient, something he says their original plastic surgeon should have done.
“Sitting there with the patient, I felt a little bad for her,” Dr. Carroll said. “I knew if I didn’t do it, it would be weeks while she bounced around to urgent care, primary care, and finally found a surgeon.” But by removing the drains, he did shift some of the liability to himself. “If she developed a wound infection, then I’m on the hook for [that],” he said. “If I send her away, I have less liability but didn’t quite do the right thing for the patient.”
In replies to Dr. Carroll’s thread, some doctors debated whether these types of cases, particularly those in which surgeons forgo follow-up care, could be considered medical abandonment. Legal experts say that’s not exactly the case, at least it would not be the case with Dr. Carroll’s patient.
“I don’t think they’ve abandoned the patient; I think they’ve abandoned care,” said Michael Flynn, JD, professor of personal injury law at Nova Southeastern University, in Fort Lauderdale–Davie, Fla. “And that abandonment of follow-up care, if it falls below the standard of what medical professionals should do, then it’s malpractice.”
“The doctor didn’t just walk away and become unreachable,” said Bernard Black, JD, a medical malpractice attorney and law professor at Northwestern University, in Evanston, Ill. Technically, the surgeon referred the patient to the ED. Mr. Black agreed that it sounds more like a question of malpractice, “but without real damages, there’s no claim.”
Even if not illegal, sending these patients to the ED is still highly unethical, Dr. Carroll said. The authors of a 2014 article in Aesthetic Plastic Surgery concur: “It is the duty and ethical responsibility of plastic surgeons to prevent unnecessary complications following tourism medicine by adequately counseling patients, defining perioperative treatment protocols, and reporting complications to regional and specialty-specific governing bodies,” they write.
Sometimes patients need to travel, Dr. Matarasso said. Recently, three out-of-state patients came to him for procedures. Two stayed in Manhattan until their follow-up care was finished; he arranged care elsewhere for the third. It’s the operating surgeon’s job to connect patients with someone who can provide follow-up care when they go home, Dr. Matarasso said. If a surgeon doesn’t have a connection in a patient’s home city, the ASPS has a referral service to help, he said.
“My frustration was never with the patient,” Dr. Carroll said. “No one should feel bad about coming to an ED for literally anything, and I mean that. My frustration is with the surgeon who didn’t go the one extra step to arrange her follow-up.”
A version of this article first appeared on Medscape.com.
It was a typical, busy evening shift in the emergency department (ED) when Steve Carroll, DO, an emergency medicine physician in the Philadelphia area, noticed an odd listing on the tracking board. In the waiting room, there was someone whose chief complaint was that she needed to have surgical drains pulled.
According to the woman’s chart, she’d undergone liposuction in Miami a week before. The surgeon had effectively relinquished all follow-up care to the woman’s local ED.
Dr. Carroll searched the name of her surgeon and found that his site “specifically advertised medical tourism,” Dr. Carroll said. The site lured patients with the idea of recovering by the beach and that a local nurse would come to their room every day.
But when Dr. Carroll told the patient that her surgeon should be the one who removes the drains, she became concerned. She didn’t know that her surgeon wasn’t providing the standard of care, he said. Somewhat appalled that a board-certified plastic surgeon would place the burden of follow-up care on an ED doctor hundreds of miles away, Dr. Carroll posted the case to Twitter and several Facebook groups.
“Yes I could refuse to take [the drains] out but that’s not patient-centered care,” Dr. Carroll wrote in a Twitter thread. “It’s unfairly shifting routine outpatient surgical followup (and liability) onto me and extra cost to [the patient].” Comments from ED physicians and sympathetic surgeons across the country flowed in. Dr. Carroll quickly realized his situation was part of a much larger problem than he’d thought.
Dr. Carroll’s patient told him that the Miami surgery cost less than undergoing the surgery locally; that’s why she’d made the trip. She’s not alone. Traveling to get the lowest price for a plastic surgery procedure has been a rising phenomenon since the early 2000s, according to the American Society of Plastic Surgeons (ASPS). Many countries are actively fostering their medical tourism industries, as are states such as Florida.
People have long traveled to get the best medical care. But “medical tourism is completely different,” said Alan Matarasso, MD, FACS, a Manhattan-based plastic surgeon and member of the ASPS Executive Committee. “People [are] traveling to get a simultaneous vacation or lower cost,” he said.
Choosing facilities on the basis of these criteria comes with myriad problems, and the quality of medical care may be lower. It’s difficult to verify the credentials of the surgeons, anesthesiologists, and facilities involved. Medical records can be in a different language, and traveling immediately after surgery increases the risk for pulmonary embolism and death, not to mention the added complications of traveling and being a surgical patient during the COVID-19 pandemic, he said.
Typically, surgeons are protective of their patients. But Murtaza Akhter, MD, an emergency medicine physician based in Miami, says it’s the opposite with the medical tourism surgeons whose patients regularly end up in his ED. “There’s almost no ownership,” he said. “Every time, [the patients] say, ‘My doctor isn’t responding,’ or they said go to the ER.” And that’s before they’ve even made it out of Miami.
The most common cosmetic surgery complications Dr. Akhter sees occur in patients who’ve undergone so-called Brazilian butt lifts. They show up in his ED face down, suffering from severe blood loss. He has them undergo a transfusion and maybe some imaging, but if they need a higher degree of care, they have to be transferred. “There’s a reason it’s cheaper,” he said.
Medical tourism mishaps are such a regular occurrence in Miami that no one flinches when the patients show up in the ED, Dr. Akhter said. He had begun to think he was overreacting to the problem until he saw Dr. Carroll’s Twitter thread.
“Since it’s daily, I just thought maybe I had gone crazy and that it’s considered normal for plastic surgeons to do this. Thanks for making me feel sane again,” Dr. Akhter tweeted in a reply to Dr. Carroll.
There are no reliable data as to of how often or where such surgeries are occurring or of patients’ outcomes. But Nicholas Genes, MD, an ED physician in Manhattan, says he sees far more postsurgical patients who traveled for their procedures than ones who underwent surgery locally. He can’t say for certain whether that’s because procedures performed by doctors in New York City have fewer complications or the physicians just handle postprocedure problems themselves.
In a 2021 systematic review of aesthetic breast surgeries performed through medical tourism, researchers found that of 171 patients who traveled for surgery, 88 (51%) had a total of 106 complications that required returning to the operating room and undergoing general anesthesia. They also found that 39% of breast augmentation implant surgeries required either a unilateral or bilateral explantation procedure after patients returned home.
The rate of complications was higher than the study authors had expected. “These are totally elective procedures,” Dr. Matarasso said. “They should be optimized.” And high rates of complications come with hefty price tags.
The cost of managing these complications, which falls to the home healthcare system or the patient themselves, can range from $5,500 (determined on the basis of data from a 2019 study in the United Kingdom) to as much as $123,000, researchers in New York City calculated, if the patient develops a complicated mycobacterium infection.
“In your effort to get a good deal or around the system, you could still end up with a lot of extensive medical bills if something goes wrong,” Dr. Genes said.
The liability dilemma
Many of the ED physicians Dr. Carroll heard from said that they wouldn’t have treated the woman who needed to have drains removed. Unlike the Brazilian-butt-lifts-gone-wrong in Miami or the complications Dr. Genes sees in New York City, Dr. Carroll’s patient wasn’t in a state of emergency. Most ED physicians said they would have sent her on her way to find a surgeon.
“In general, we shouldn’t be doing things we aren’t trained to do. It’s sort of a slippery slope,” Dr. Genes said. He’s comfortable with removing stitches, but for surgical drains and plastic apparatuses, “I don’t feel particularly well trained. I’d have to consult a colleague in general surgery,” he said. When he does get one of these patients, he works the phones to find a plastic surgeon who will see the patient, something he says their original plastic surgeon should have done.
“Sitting there with the patient, I felt a little bad for her,” Dr. Carroll said. “I knew if I didn’t do it, it would be weeks while she bounced around to urgent care, primary care, and finally found a surgeon.” But by removing the drains, he did shift some of the liability to himself. “If she developed a wound infection, then I’m on the hook for [that],” he said. “If I send her away, I have less liability but didn’t quite do the right thing for the patient.”
In replies to Dr. Carroll’s thread, some doctors debated whether these types of cases, particularly those in which surgeons forgo follow-up care, could be considered medical abandonment. Legal experts say that’s not exactly the case, at least it would not be the case with Dr. Carroll’s patient.
“I don’t think they’ve abandoned the patient; I think they’ve abandoned care,” said Michael Flynn, JD, professor of personal injury law at Nova Southeastern University, in Fort Lauderdale–Davie, Fla. “And that abandonment of follow-up care, if it falls below the standard of what medical professionals should do, then it’s malpractice.”
“The doctor didn’t just walk away and become unreachable,” said Bernard Black, JD, a medical malpractice attorney and law professor at Northwestern University, in Evanston, Ill. Technically, the surgeon referred the patient to the ED. Mr. Black agreed that it sounds more like a question of malpractice, “but without real damages, there’s no claim.”
Even if not illegal, sending these patients to the ED is still highly unethical, Dr. Carroll said. The authors of a 2014 article in Aesthetic Plastic Surgery concur: “It is the duty and ethical responsibility of plastic surgeons to prevent unnecessary complications following tourism medicine by adequately counseling patients, defining perioperative treatment protocols, and reporting complications to regional and specialty-specific governing bodies,” they write.
Sometimes patients need to travel, Dr. Matarasso said. Recently, three out-of-state patients came to him for procedures. Two stayed in Manhattan until their follow-up care was finished; he arranged care elsewhere for the third. It’s the operating surgeon’s job to connect patients with someone who can provide follow-up care when they go home, Dr. Matarasso said. If a surgeon doesn’t have a connection in a patient’s home city, the ASPS has a referral service to help, he said.
“My frustration was never with the patient,” Dr. Carroll said. “No one should feel bad about coming to an ED for literally anything, and I mean that. My frustration is with the surgeon who didn’t go the one extra step to arrange her follow-up.”
A version of this article first appeared on Medscape.com.
Injectable monoclonal antibodies prevent COVID-19 in trial
according to results of a randomized, double-blind, placebo-controlled clinical trial published online August 4, 2021, in the New England Journal of Medicine.
The cocktail of the monoclonal antibodies casirivimab and imdevimab (REGEN-COV, Regeneron Pharmaceuticals) reduced participants’ relative risk of infection by 72%, compared with placebo within the first week. After the first week, risk reduction increased to 93%.
“Long after you would be exposed by your household, there is an enduring effect that prevents you from community spread,” said David Wohl, MD, professor of medicine in the division of infectious diseases at the University of North Carolina at Chapel Hill, who was a site investigator for the trial but not a study author.
Participants were enrolled within 96 hours after someone in their household tested positive for SARS-CoV-2. Participants were randomly assigned to receive 1,200 mg of REGEN-COV subcutaneously or a placebo. Based on serologic testing, study participants showed no evidence of current or previous SARS-CoV-2 infection. The median age of participants was 42.9, but 45% were male teenagers (ages 12-17).
In the group that received REGEN-COV, 11 out of 753 participants developed symptomatic COVID-19, compared with 59 out of 752 participants who received placebo. The relative risk reduction for the study’s 4-week period was 81.4% (P < .001). Of the participants that did develop a SARS-CoV-2 infection, those that received REGEN-COV were less likely to be symptomatic. Asymptomatic infections developed in 25 participants who received REGEN-COV versus 48 in the placebo group. The relative risk of developing any SARS-CoV-2 infection, symptomatic or asymptomatic, was reduced by 66.4% with REGEN-COV (P < .001).
Among the patients who were symptomatic, symptoms subsided within a median of 1.2 weeks for the group that received REGEN-COV, 2 weeks earlier than the placebo group. These patients also had a shorter duration of a high viral load (>104 copies/mL). Few adverse events were reported in the treatment or placebo groups. Monoclonal antibodies “seem to be incredibly safe,” Dr. Wohl said.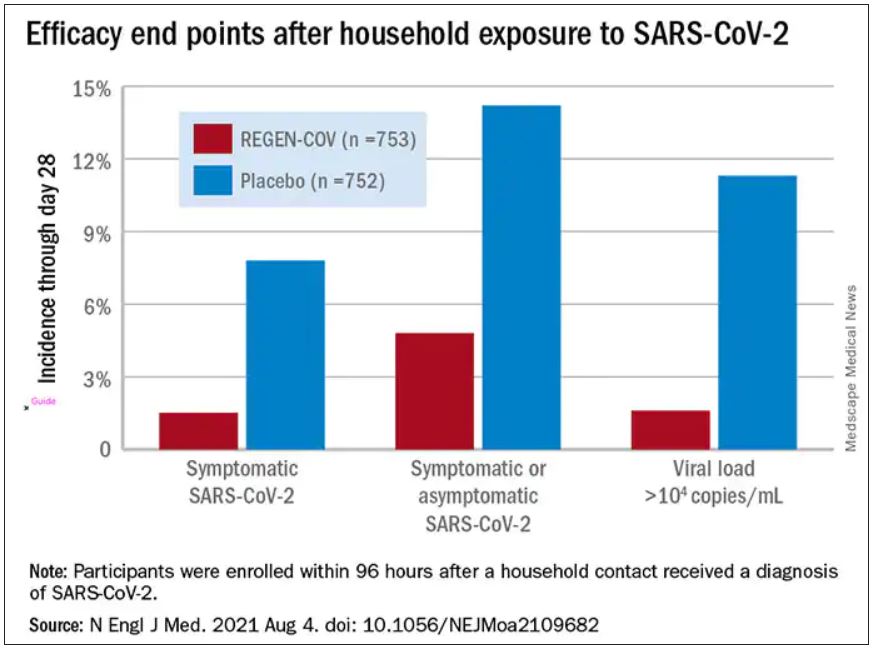
“These monoclonal antibodies have proven they can reduce the viral replication in the nose,” said study author Myron Cohen, MD, an infectious disease specialist and professor of epidemiology at the University of North Carolina.
The Food and Drug Administration first granted REGEN-COV emergency use authorization (EUA) in November 2020 for use in patients with mild or moderate COVID-19 who were also at high risk for progressing to severe COVID-19. At that time, the cocktail of monoclonal antibodies was delivered by a single intravenous infusion.
In January, Regeneron first announced the success of this trial of the subcutaneous injection for exposed household contacts based on early results, and in June of 2021, the FDA expanded the EUA to include a subcutaneous delivery when IV is not feasible. On July 30, the EUA was expanded again to include prophylactic use in exposed patients based on these trial results.
The U.S. government has purchased approximately 1.5 million doses of REGEN-COV from Regeneron and has agreed to make the treatments free of charge to patients.
But despite being free, available, and backed by promising data, monoclonal antibodies as a therapeutic answer to COVID-19 still hasn’t really taken off. “The problem is, it first requires knowledge and awareness,” Dr. Wohl said. “A lot [of people] don’t know this exists. To be honest, vaccination has taken up all the oxygen in the room.”
Dr. Cohen agreed. One reason for the slow uptake may be because the drug supply is owned by the government and not a pharmaceutical company. There hasn’t been a typical marketing push to make physicians and consumers aware. Additionally, “the logistics are daunting,” Dr. Cohen said. The office spaces where many physicians care for patients “often aren’t appropriate for patients who think they have SARS-CoV-2.”
“Right now, there’s not a mechanism” to administer the drug to people who could benefit from it, Dr. Wohl said. Eligible patients are either immunocompromised and unlikely to mount a sufficient immune response with vaccination, or not fully vaccinated. They should have been exposed to an infected individual or have a high likelihood of exposure due to where they live, such as in a prison or nursing home. Local doctors are unlikely to be the primary administrators of the drug, Dr. Wohl added. “How do we operationalize this for people who fit the criteria?”
There’s also an issue of timing. REGEN-COV is most effective when given early, Dr. Cohen said. “[Monoclonal antibodies] really only work well in the replication phase.” Many patients who would be eligible delay care until they’ve had symptoms for several days, when REGEN-COV would no longer have the desired effect.
Eventually, Dr. Wohl suspects demand will increase when people realize REGEN-COV can help those with COVID-19 and those who have been exposed. But before then, “we do have to think about how to integrate this into a workflow people can access without being confused.”
The trial was done before there was widespread vaccination, so it’s unclear what the results mean for people who have been vaccinated. Dr. Cohen and Dr. Wohl said there are ongoing conversations about whether monoclonal antibodies could be complementary to vaccination and if there’s potential for continued monthly use of these therapies.
Cohen and Wohl reported no relevant financial relationships. The trial was supported by Regeneron Pharmaceuticals, F. Hoffmann–La Roche, the National Institute of Allergy and Infectious Diseases, NIH, and the COVID-19 Prevention Network.
A version of this article first appeared on Medscape.com.
according to results of a randomized, double-blind, placebo-controlled clinical trial published online August 4, 2021, in the New England Journal of Medicine.
The cocktail of the monoclonal antibodies casirivimab and imdevimab (REGEN-COV, Regeneron Pharmaceuticals) reduced participants’ relative risk of infection by 72%, compared with placebo within the first week. After the first week, risk reduction increased to 93%.
“Long after you would be exposed by your household, there is an enduring effect that prevents you from community spread,” said David Wohl, MD, professor of medicine in the division of infectious diseases at the University of North Carolina at Chapel Hill, who was a site investigator for the trial but not a study author.
Participants were enrolled within 96 hours after someone in their household tested positive for SARS-CoV-2. Participants were randomly assigned to receive 1,200 mg of REGEN-COV subcutaneously or a placebo. Based on serologic testing, study participants showed no evidence of current or previous SARS-CoV-2 infection. The median age of participants was 42.9, but 45% were male teenagers (ages 12-17).
In the group that received REGEN-COV, 11 out of 753 participants developed symptomatic COVID-19, compared with 59 out of 752 participants who received placebo. The relative risk reduction for the study’s 4-week period was 81.4% (P < .001). Of the participants that did develop a SARS-CoV-2 infection, those that received REGEN-COV were less likely to be symptomatic. Asymptomatic infections developed in 25 participants who received REGEN-COV versus 48 in the placebo group. The relative risk of developing any SARS-CoV-2 infection, symptomatic or asymptomatic, was reduced by 66.4% with REGEN-COV (P < .001).
Among the patients who were symptomatic, symptoms subsided within a median of 1.2 weeks for the group that received REGEN-COV, 2 weeks earlier than the placebo group. These patients also had a shorter duration of a high viral load (>104 copies/mL). Few adverse events were reported in the treatment or placebo groups. Monoclonal antibodies “seem to be incredibly safe,” Dr. Wohl said.
“These monoclonal antibodies have proven they can reduce the viral replication in the nose,” said study author Myron Cohen, MD, an infectious disease specialist and professor of epidemiology at the University of North Carolina.
The Food and Drug Administration first granted REGEN-COV emergency use authorization (EUA) in November 2020 for use in patients with mild or moderate COVID-19 who were also at high risk for progressing to severe COVID-19. At that time, the cocktail of monoclonal antibodies was delivered by a single intravenous infusion.
In January, Regeneron first announced the success of this trial of the subcutaneous injection for exposed household contacts based on early results, and in June of 2021, the FDA expanded the EUA to include a subcutaneous delivery when IV is not feasible. On July 30, the EUA was expanded again to include prophylactic use in exposed patients based on these trial results.
The U.S. government has purchased approximately 1.5 million doses of REGEN-COV from Regeneron and has agreed to make the treatments free of charge to patients.
But despite being free, available, and backed by promising data, monoclonal antibodies as a therapeutic answer to COVID-19 still hasn’t really taken off. “The problem is, it first requires knowledge and awareness,” Dr. Wohl said. “A lot [of people] don’t know this exists. To be honest, vaccination has taken up all the oxygen in the room.”
Dr. Cohen agreed. One reason for the slow uptake may be because the drug supply is owned by the government and not a pharmaceutical company. There hasn’t been a typical marketing push to make physicians and consumers aware. Additionally, “the logistics are daunting,” Dr. Cohen said. The office spaces where many physicians care for patients “often aren’t appropriate for patients who think they have SARS-CoV-2.”
“Right now, there’s not a mechanism” to administer the drug to people who could benefit from it, Dr. Wohl said. Eligible patients are either immunocompromised and unlikely to mount a sufficient immune response with vaccination, or not fully vaccinated. They should have been exposed to an infected individual or have a high likelihood of exposure due to where they live, such as in a prison or nursing home. Local doctors are unlikely to be the primary administrators of the drug, Dr. Wohl added. “How do we operationalize this for people who fit the criteria?”
There’s also an issue of timing. REGEN-COV is most effective when given early, Dr. Cohen said. “[Monoclonal antibodies] really only work well in the replication phase.” Many patients who would be eligible delay care until they’ve had symptoms for several days, when REGEN-COV would no longer have the desired effect.
Eventually, Dr. Wohl suspects demand will increase when people realize REGEN-COV can help those with COVID-19 and those who have been exposed. But before then, “we do have to think about how to integrate this into a workflow people can access without being confused.”
The trial was done before there was widespread vaccination, so it’s unclear what the results mean for people who have been vaccinated. Dr. Cohen and Dr. Wohl said there are ongoing conversations about whether monoclonal antibodies could be complementary to vaccination and if there’s potential for continued monthly use of these therapies.
Cohen and Wohl reported no relevant financial relationships. The trial was supported by Regeneron Pharmaceuticals, F. Hoffmann–La Roche, the National Institute of Allergy and Infectious Diseases, NIH, and the COVID-19 Prevention Network.
A version of this article first appeared on Medscape.com.
according to results of a randomized, double-blind, placebo-controlled clinical trial published online August 4, 2021, in the New England Journal of Medicine.
The cocktail of the monoclonal antibodies casirivimab and imdevimab (REGEN-COV, Regeneron Pharmaceuticals) reduced participants’ relative risk of infection by 72%, compared with placebo within the first week. After the first week, risk reduction increased to 93%.
“Long after you would be exposed by your household, there is an enduring effect that prevents you from community spread,” said David Wohl, MD, professor of medicine in the division of infectious diseases at the University of North Carolina at Chapel Hill, who was a site investigator for the trial but not a study author.
Participants were enrolled within 96 hours after someone in their household tested positive for SARS-CoV-2. Participants were randomly assigned to receive 1,200 mg of REGEN-COV subcutaneously or a placebo. Based on serologic testing, study participants showed no evidence of current or previous SARS-CoV-2 infection. The median age of participants was 42.9, but 45% were male teenagers (ages 12-17).
In the group that received REGEN-COV, 11 out of 753 participants developed symptomatic COVID-19, compared with 59 out of 752 participants who received placebo. The relative risk reduction for the study’s 4-week period was 81.4% (P < .001). Of the participants that did develop a SARS-CoV-2 infection, those that received REGEN-COV were less likely to be symptomatic. Asymptomatic infections developed in 25 participants who received REGEN-COV versus 48 in the placebo group. The relative risk of developing any SARS-CoV-2 infection, symptomatic or asymptomatic, was reduced by 66.4% with REGEN-COV (P < .001).
Among the patients who were symptomatic, symptoms subsided within a median of 1.2 weeks for the group that received REGEN-COV, 2 weeks earlier than the placebo group. These patients also had a shorter duration of a high viral load (>104 copies/mL). Few adverse events were reported in the treatment or placebo groups. Monoclonal antibodies “seem to be incredibly safe,” Dr. Wohl said.
“These monoclonal antibodies have proven they can reduce the viral replication in the nose,” said study author Myron Cohen, MD, an infectious disease specialist and professor of epidemiology at the University of North Carolina.
The Food and Drug Administration first granted REGEN-COV emergency use authorization (EUA) in November 2020 for use in patients with mild or moderate COVID-19 who were also at high risk for progressing to severe COVID-19. At that time, the cocktail of monoclonal antibodies was delivered by a single intravenous infusion.
In January, Regeneron first announced the success of this trial of the subcutaneous injection for exposed household contacts based on early results, and in June of 2021, the FDA expanded the EUA to include a subcutaneous delivery when IV is not feasible. On July 30, the EUA was expanded again to include prophylactic use in exposed patients based on these trial results.
The U.S. government has purchased approximately 1.5 million doses of REGEN-COV from Regeneron and has agreed to make the treatments free of charge to patients.
But despite being free, available, and backed by promising data, monoclonal antibodies as a therapeutic answer to COVID-19 still hasn’t really taken off. “The problem is, it first requires knowledge and awareness,” Dr. Wohl said. “A lot [of people] don’t know this exists. To be honest, vaccination has taken up all the oxygen in the room.”
Dr. Cohen agreed. One reason for the slow uptake may be because the drug supply is owned by the government and not a pharmaceutical company. There hasn’t been a typical marketing push to make physicians and consumers aware. Additionally, “the logistics are daunting,” Dr. Cohen said. The office spaces where many physicians care for patients “often aren’t appropriate for patients who think they have SARS-CoV-2.”
“Right now, there’s not a mechanism” to administer the drug to people who could benefit from it, Dr. Wohl said. Eligible patients are either immunocompromised and unlikely to mount a sufficient immune response with vaccination, or not fully vaccinated. They should have been exposed to an infected individual or have a high likelihood of exposure due to where they live, such as in a prison or nursing home. Local doctors are unlikely to be the primary administrators of the drug, Dr. Wohl added. “How do we operationalize this for people who fit the criteria?”
There’s also an issue of timing. REGEN-COV is most effective when given early, Dr. Cohen said. “[Monoclonal antibodies] really only work well in the replication phase.” Many patients who would be eligible delay care until they’ve had symptoms for several days, when REGEN-COV would no longer have the desired effect.
Eventually, Dr. Wohl suspects demand will increase when people realize REGEN-COV can help those with COVID-19 and those who have been exposed. But before then, “we do have to think about how to integrate this into a workflow people can access without being confused.”
The trial was done before there was widespread vaccination, so it’s unclear what the results mean for people who have been vaccinated. Dr. Cohen and Dr. Wohl said there are ongoing conversations about whether monoclonal antibodies could be complementary to vaccination and if there’s potential for continued monthly use of these therapies.
Cohen and Wohl reported no relevant financial relationships. The trial was supported by Regeneron Pharmaceuticals, F. Hoffmann–La Roche, the National Institute of Allergy and Infectious Diseases, NIH, and the COVID-19 Prevention Network.
A version of this article first appeared on Medscape.com.
Midodrine reduces fainting in young patients
.
Vasovagal syncope is the most common cause of fainting and is often triggered by dehydration and upright posture, according to Johns Hopkins Medicine. But it can also be caused by stimuli like the sight of blood or sudden emotional distress. The stimulus causes the heart rate and blood pressure to drop rapidly, according to the Mayo Clinic.
The randomized, placebo-controlled, double-blind trial included 133 patients with recurrent vasovagal syncope and was published in Annals of Internal Medicine. Those that received midodrine were less likely to have one syncope episode (28 of 66 [42%]), compared with those that took the placebo (41 of 67 [61%]). The absolute risk reduction for vasovagal syncope was 19 percentage points (95% confidence interval, 2-36 percentage points).
The study included patients from 25 university hospitals in Canada, the United States, Mexico, and the United Kingdom, who were followed for 12 months. The trial participants were highly symptomatic for vasovagal syncope, having experienced a median of 23 episodes in their lifetime and 5 syncope episodes in the last year, and they had no comorbid conditions.
“We don’t have many arrows in our quiver,” said Robert Sheldon, MD, PhD, a cardiologist at University of Calgary (Alta.) and lead author of the study, referring to the lack of evidence-based treatments for syncope.
For 20 years Dr. Sheldon’s lab has been testing drugs that showed some potential. While a previous study of fludrocortisone (Florinef ) showed some benefit, “[midodrine] was the first to be unequivocally, slam-dunk positive,” he said in an interview.
Earlier trials of midodrine
Other studies have shown midodrine to prevent syncope on tilt tests. There have been two randomized trials where midodrine significantly reduced vasovagal syncope, but one of these was short and in children, and the other one was open label with no placebo control.
“Risk reduction was very high in previous studies,” Dr. Sheldon said in an interview. But, because they were open label, there was a huge placebo effect, he noted.
“There were no adequately done, adequately powered [studies] that have been positive,” Dr. Sheldon added.
New study methods and outcomes
The study published in Annals of Internal Medicine this week included patients over 18 years of age with a Calgary Syncope Symptom Score of at least 2. All were educated on lifestyle measures that can prevent syncopes before beginning to take 5 mg of study drug or placebo three times daily, 4 hours apart.
In these cases, the study authors wrote, “taking medication three times a day seems worth the effort.” But in patients with a lower frequency of episodes, midodrine might not have an adequate payoff.
These results are “impressive,” said Roopinder K. Sandhu, MD, MPH, clinical electrophysiologist at Cedar-Sinai in Los Angeles. “This study demonstrated that midodrine is the first medical therapy, in addition to education and lifestyle measures, to unequivocally pass the scrutiny of an international, placebo-controlled, RCT to show a significant reduction in syncope recurrence in a younger population with frequent syncope events.”
“[Taking midodrine] doesn’t carry the long-term consequence of pacemakers,” she added.
Study limitations
Limitations of the new study include its small size and short observation period, the authors wrote. Additionally, a large proportion of patients enrolled were also from a single center in Calgary that specializes in syncope care. Twenty-seven patients in the trial stopped taking their assigned medication during the year observation period, but the authors concluded these participants “likely would bias the results against midodrine.”
For doctors considering midodrine for their patients, it’s critical to confirm the diagnosis and to try patient education first, Dr. Sheldon advised.
Lifestyle factors like hydration, adequate sodium intake, and squatting or lying down when the syncope is coming on can sufficiently suppress syncopes in two-thirds of patients, he noted.
This is a treatment for young people, Dr. Sandhu said. The median age in the trial was 35, so patients taking midodrine should be younger than 50. Midodrine is also not effective in patients with high blood pressure or heart failure, she said.
“[Midodrine] is easy to use but kind of a pain at first,” Dr. Sheldon noted. Every patient should start out taking 5 mg doses, three times a day – during waking hours. But then you have to adjust the dosage, “and it’s tricky,” he said.
If a patient experiences goosebumps or the sensation of worms crawling in the hair, the dose might be too much, Dr. Sheldon noted.
If the patient is still fainting, first consider when they are fainting, he said. If it’s around the time they should take another dose, it might be trough effect.
Dr. Sandhu was not involved in the study, but Cedar Sinai was a participating center, and she considers Dr. Sheldon to be a mentor. Dr. Sandhu also noted that she has published papers with Dr. Sheldon, who reported no conflicts.
.
Vasovagal syncope is the most common cause of fainting and is often triggered by dehydration and upright posture, according to Johns Hopkins Medicine. But it can also be caused by stimuli like the sight of blood or sudden emotional distress. The stimulus causes the heart rate and blood pressure to drop rapidly, according to the Mayo Clinic.
The randomized, placebo-controlled, double-blind trial included 133 patients with recurrent vasovagal syncope and was published in Annals of Internal Medicine. Those that received midodrine were less likely to have one syncope episode (28 of 66 [42%]), compared with those that took the placebo (41 of 67 [61%]). The absolute risk reduction for vasovagal syncope was 19 percentage points (95% confidence interval, 2-36 percentage points).
The study included patients from 25 university hospitals in Canada, the United States, Mexico, and the United Kingdom, who were followed for 12 months. The trial participants were highly symptomatic for vasovagal syncope, having experienced a median of 23 episodes in their lifetime and 5 syncope episodes in the last year, and they had no comorbid conditions.
“We don’t have many arrows in our quiver,” said Robert Sheldon, MD, PhD, a cardiologist at University of Calgary (Alta.) and lead author of the study, referring to the lack of evidence-based treatments for syncope.
For 20 years Dr. Sheldon’s lab has been testing drugs that showed some potential. While a previous study of fludrocortisone (Florinef ) showed some benefit, “[midodrine] was the first to be unequivocally, slam-dunk positive,” he said in an interview.
Earlier trials of midodrine
Other studies have shown midodrine to prevent syncope on tilt tests. There have been two randomized trials where midodrine significantly reduced vasovagal syncope, but one of these was short and in children, and the other one was open label with no placebo control.
“Risk reduction was very high in previous studies,” Dr. Sheldon said in an interview. But, because they were open label, there was a huge placebo effect, he noted.
“There were no adequately done, adequately powered [studies] that have been positive,” Dr. Sheldon added.
New study methods and outcomes
The study published in Annals of Internal Medicine this week included patients over 18 years of age with a Calgary Syncope Symptom Score of at least 2. All were educated on lifestyle measures that can prevent syncopes before beginning to take 5 mg of study drug or placebo three times daily, 4 hours apart.
In these cases, the study authors wrote, “taking medication three times a day seems worth the effort.” But in patients with a lower frequency of episodes, midodrine might not have an adequate payoff.
These results are “impressive,” said Roopinder K. Sandhu, MD, MPH, clinical electrophysiologist at Cedar-Sinai in Los Angeles. “This study demonstrated that midodrine is the first medical therapy, in addition to education and lifestyle measures, to unequivocally pass the scrutiny of an international, placebo-controlled, RCT to show a significant reduction in syncope recurrence in a younger population with frequent syncope events.”
“[Taking midodrine] doesn’t carry the long-term consequence of pacemakers,” she added.
Study limitations
Limitations of the new study include its small size and short observation period, the authors wrote. Additionally, a large proportion of patients enrolled were also from a single center in Calgary that specializes in syncope care. Twenty-seven patients in the trial stopped taking their assigned medication during the year observation period, but the authors concluded these participants “likely would bias the results against midodrine.”
For doctors considering midodrine for their patients, it’s critical to confirm the diagnosis and to try patient education first, Dr. Sheldon advised.
Lifestyle factors like hydration, adequate sodium intake, and squatting or lying down when the syncope is coming on can sufficiently suppress syncopes in two-thirds of patients, he noted.
This is a treatment for young people, Dr. Sandhu said. The median age in the trial was 35, so patients taking midodrine should be younger than 50. Midodrine is also not effective in patients with high blood pressure or heart failure, she said.
“[Midodrine] is easy to use but kind of a pain at first,” Dr. Sheldon noted. Every patient should start out taking 5 mg doses, three times a day – during waking hours. But then you have to adjust the dosage, “and it’s tricky,” he said.
If a patient experiences goosebumps or the sensation of worms crawling in the hair, the dose might be too much, Dr. Sheldon noted.
If the patient is still fainting, first consider when they are fainting, he said. If it’s around the time they should take another dose, it might be trough effect.
Dr. Sandhu was not involved in the study, but Cedar Sinai was a participating center, and she considers Dr. Sheldon to be a mentor. Dr. Sandhu also noted that she has published papers with Dr. Sheldon, who reported no conflicts.
.
Vasovagal syncope is the most common cause of fainting and is often triggered by dehydration and upright posture, according to Johns Hopkins Medicine. But it can also be caused by stimuli like the sight of blood or sudden emotional distress. The stimulus causes the heart rate and blood pressure to drop rapidly, according to the Mayo Clinic.
The randomized, placebo-controlled, double-blind trial included 133 patients with recurrent vasovagal syncope and was published in Annals of Internal Medicine. Those that received midodrine were less likely to have one syncope episode (28 of 66 [42%]), compared with those that took the placebo (41 of 67 [61%]). The absolute risk reduction for vasovagal syncope was 19 percentage points (95% confidence interval, 2-36 percentage points).
The study included patients from 25 university hospitals in Canada, the United States, Mexico, and the United Kingdom, who were followed for 12 months. The trial participants were highly symptomatic for vasovagal syncope, having experienced a median of 23 episodes in their lifetime and 5 syncope episodes in the last year, and they had no comorbid conditions.
“We don’t have many arrows in our quiver,” said Robert Sheldon, MD, PhD, a cardiologist at University of Calgary (Alta.) and lead author of the study, referring to the lack of evidence-based treatments for syncope.
For 20 years Dr. Sheldon’s lab has been testing drugs that showed some potential. While a previous study of fludrocortisone (Florinef ) showed some benefit, “[midodrine] was the first to be unequivocally, slam-dunk positive,” he said in an interview.
Earlier trials of midodrine
Other studies have shown midodrine to prevent syncope on tilt tests. There have been two randomized trials where midodrine significantly reduced vasovagal syncope, but one of these was short and in children, and the other one was open label with no placebo control.
“Risk reduction was very high in previous studies,” Dr. Sheldon said in an interview. But, because they were open label, there was a huge placebo effect, he noted.
“There were no adequately done, adequately powered [studies] that have been positive,” Dr. Sheldon added.
New study methods and outcomes
The study published in Annals of Internal Medicine this week included patients over 18 years of age with a Calgary Syncope Symptom Score of at least 2. All were educated on lifestyle measures that can prevent syncopes before beginning to take 5 mg of study drug or placebo three times daily, 4 hours apart.
In these cases, the study authors wrote, “taking medication three times a day seems worth the effort.” But in patients with a lower frequency of episodes, midodrine might not have an adequate payoff.
These results are “impressive,” said Roopinder K. Sandhu, MD, MPH, clinical electrophysiologist at Cedar-Sinai in Los Angeles. “This study demonstrated that midodrine is the first medical therapy, in addition to education and lifestyle measures, to unequivocally pass the scrutiny of an international, placebo-controlled, RCT to show a significant reduction in syncope recurrence in a younger population with frequent syncope events.”
“[Taking midodrine] doesn’t carry the long-term consequence of pacemakers,” she added.
Study limitations
Limitations of the new study include its small size and short observation period, the authors wrote. Additionally, a large proportion of patients enrolled were also from a single center in Calgary that specializes in syncope care. Twenty-seven patients in the trial stopped taking their assigned medication during the year observation period, but the authors concluded these participants “likely would bias the results against midodrine.”
For doctors considering midodrine for their patients, it’s critical to confirm the diagnosis and to try patient education first, Dr. Sheldon advised.
Lifestyle factors like hydration, adequate sodium intake, and squatting or lying down when the syncope is coming on can sufficiently suppress syncopes in two-thirds of patients, he noted.
This is a treatment for young people, Dr. Sandhu said. The median age in the trial was 35, so patients taking midodrine should be younger than 50. Midodrine is also not effective in patients with high blood pressure or heart failure, she said.
“[Midodrine] is easy to use but kind of a pain at first,” Dr. Sheldon noted. Every patient should start out taking 5 mg doses, three times a day – during waking hours. But then you have to adjust the dosage, “and it’s tricky,” he said.
If a patient experiences goosebumps or the sensation of worms crawling in the hair, the dose might be too much, Dr. Sheldon noted.
If the patient is still fainting, first consider when they are fainting, he said. If it’s around the time they should take another dose, it might be trough effect.
Dr. Sandhu was not involved in the study, but Cedar Sinai was a participating center, and she considers Dr. Sheldon to be a mentor. Dr. Sandhu also noted that she has published papers with Dr. Sheldon, who reported no conflicts.
FROM ANNALS OF INTERNAL MEDICINE