User login
Knowing My Limits
The records came in by fax. A patient who’d recently moved here and needed to connect with a local neurologist.
When I had time, I flipped through the records. He needed ongoing treatment for a rare neurological disease that I’d heard of, but wasn’t otherwise familiar with. It didn’t even exist in the textbooks or conferences when I was in residency. I’d never seen a case of it, just read about it here and there in journals.
I looked it up, reviewed current treatment options, monitoring, and other knowledge about it, then stared at the notes for a minute. Finally, after thinking it over, I attached a sticky note for my secretary that, if the person called, to redirect them to one of the local subspecialty neurology centers.
I have nothing against this patient, but realistically he would be better served seeing someone with time to keep up on advancements in esoteric disorders, not a general neurologist like myself.
Isn’t that why we have subspecialty centers?
Some of it is also me. There was a time in my career when keeping up on newly discovered disorders and their treatments was, well, cool. But after 25 years in practice, that changes.
It’s important to be at least somewhat aware of new developments (such as in this case) as you may encounter them, and need to know when it’s something you can handle and when to send it elsewhere.
Driving home that afternoon I thought, “I’m an old dog. I don’t want to learn new tricks.” Maybe that’s all it is. There are other neurologists my age and older who thrive on the challenge of learning about and treating new and rare disorders that were unknown when they started out. There’s nothing wrong with that.
But I’ve never pretended to be an academic or sub-sub-specialist. My patients depend on me to stay up to date on the large number of commonly seen neurological disorders, and I do my best to do that.
It ain’t easy being an old dog.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
The records came in by fax. A patient who’d recently moved here and needed to connect with a local neurologist.
When I had time, I flipped through the records. He needed ongoing treatment for a rare neurological disease that I’d heard of, but wasn’t otherwise familiar with. It didn’t even exist in the textbooks or conferences when I was in residency. I’d never seen a case of it, just read about it here and there in journals.
I looked it up, reviewed current treatment options, monitoring, and other knowledge about it, then stared at the notes for a minute. Finally, after thinking it over, I attached a sticky note for my secretary that, if the person called, to redirect them to one of the local subspecialty neurology centers.
I have nothing against this patient, but realistically he would be better served seeing someone with time to keep up on advancements in esoteric disorders, not a general neurologist like myself.
Isn’t that why we have subspecialty centers?
Some of it is also me. There was a time in my career when keeping up on newly discovered disorders and their treatments was, well, cool. But after 25 years in practice, that changes.
It’s important to be at least somewhat aware of new developments (such as in this case) as you may encounter them, and need to know when it’s something you can handle and when to send it elsewhere.
Driving home that afternoon I thought, “I’m an old dog. I don’t want to learn new tricks.” Maybe that’s all it is. There are other neurologists my age and older who thrive on the challenge of learning about and treating new and rare disorders that were unknown when they started out. There’s nothing wrong with that.
But I’ve never pretended to be an academic or sub-sub-specialist. My patients depend on me to stay up to date on the large number of commonly seen neurological disorders, and I do my best to do that.
It ain’t easy being an old dog.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
The records came in by fax. A patient who’d recently moved here and needed to connect with a local neurologist.
When I had time, I flipped through the records. He needed ongoing treatment for a rare neurological disease that I’d heard of, but wasn’t otherwise familiar with. It didn’t even exist in the textbooks or conferences when I was in residency. I’d never seen a case of it, just read about it here and there in journals.
I looked it up, reviewed current treatment options, monitoring, and other knowledge about it, then stared at the notes for a minute. Finally, after thinking it over, I attached a sticky note for my secretary that, if the person called, to redirect them to one of the local subspecialty neurology centers.
I have nothing against this patient, but realistically he would be better served seeing someone with time to keep up on advancements in esoteric disorders, not a general neurologist like myself.
Isn’t that why we have subspecialty centers?
Some of it is also me. There was a time in my career when keeping up on newly discovered disorders and their treatments was, well, cool. But after 25 years in practice, that changes.
It’s important to be at least somewhat aware of new developments (such as in this case) as you may encounter them, and need to know when it’s something you can handle and when to send it elsewhere.
Driving home that afternoon I thought, “I’m an old dog. I don’t want to learn new tricks.” Maybe that’s all it is. There are other neurologists my age and older who thrive on the challenge of learning about and treating new and rare disorders that were unknown when they started out. There’s nothing wrong with that.
But I’ve never pretended to be an academic or sub-sub-specialist. My patients depend on me to stay up to date on the large number of commonly seen neurological disorders, and I do my best to do that.
It ain’t easy being an old dog.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Losing Weight, Decreasing Alcohol, and Improving Sex Life?
Richard* was a master-of-the-universe type. He went to Wharton, ran a large hedge fund, and lived in Greenwich, Connecticut. His three children attended Ivy League schools. He played golf on the weekends and ate three healthy meals per day. There was just one issue: He had gained 90 pounds since the 1990s from consuming six to seven alcoholic beverages per day. He already had one DUI under his belt, and his marriage was on shaky ground. He had tried to address his alcohol abuse disorder on multiple occasions: He went to a yearlong class on alcoholism, saw a psychologist for cognitive-behavioral therapy, and joined Alcoholics Anonymous, all to no avail.
When I met him in December 2023, he had hit rock bottom and was willing to try anything.
At our first visit, I prescribed him weekly tirzepatide (Zepbound) off label, along with a small dose of naltrexone.
Richard shared some feedback after his first 2 weeks:
The naltrexone works great and is strong ... small dose for me effective ... I haven’t wanted to drink and when I do I can’t finish a glass over 2 hours … went from 25 drinks a week to about 4 … don’t notice other side effects … sleeping better too.
And after 6 weeks:
Some more feedback … on week 6-7 and all going well ... drinking very little alcohol and still on half tab of naltrexone ... that works well and have no side effects ... the Zepbound works well too. I do get hungry a few days after the shot but still don’t crave sugar or bad snacks … weight down 21 pounds since started … 292 to 271.
And finally, after 8 weeks:
Looking at my last text to you I see the progress … been incredible ... now down 35 pounds and at 257 … continue to feel excellent with plenty of energy … want to exercise more ... and no temptation to eat or drink unhealthy stuff ... I’m very happy this has surpassed my expectations on how fast it’s worked and I don’t feel any side effects. Marriage has never been better … all thanks to you.
Tirzepatide contains two hormones, glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), that are naturally produced by our bodies after meals. Scientists recently learned that the GLP-1 system contributes to the feedback loop of addictive behaviors. Increasing synthetic GLP-1, through medications like tirzepatide, appears to minimize addictive behaviors by limiting their ability to upregulate the brain’s production of dopamine.
Dopamine is a neurotransmitter produced in the brain’s reward center, which regulates how people experience pleasure and control impulses. Dopamine reinforces the pleasure experienced by certain behaviors like drinking, smoking, and eating sweets. These new medications reduce the amount of dopamine released after these activities and thereby lower the motivation to repeat these behaviors.
Contrary to some reports in the news, the vast majority of my male patients using these medications for alcohol abuse disorder experience concurrent increases in testosterone, for two reasons: (1) testosterone increases as body mass index decreases and (2) chronic alcohol use can damage the cells in the testicles that produce testosterone and also decrease the brain’s ability to stimulate the testicles to produce testosterone.
At his most recent checkup last month, Richard’s testosterone had risen from borderline to robust levels, his libido and sleep had improved, and he reported never having felt so healthy or confident. Fingers crossed that the US Food and Drug Administration won’t wait too long before approving this class of medications for more than just diabetes, heart disease, and obesity.
*Patient’s name has been changed.
Dr. Messer is clinical assistant professor, Icahn School of Medicine at Mount Sinai, New York, and associate professor, Zucker School of Medicine at Hofstra University, Hempstead, New York. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Richard* was a master-of-the-universe type. He went to Wharton, ran a large hedge fund, and lived in Greenwich, Connecticut. His three children attended Ivy League schools. He played golf on the weekends and ate three healthy meals per day. There was just one issue: He had gained 90 pounds since the 1990s from consuming six to seven alcoholic beverages per day. He already had one DUI under his belt, and his marriage was on shaky ground. He had tried to address his alcohol abuse disorder on multiple occasions: He went to a yearlong class on alcoholism, saw a psychologist for cognitive-behavioral therapy, and joined Alcoholics Anonymous, all to no avail.
When I met him in December 2023, he had hit rock bottom and was willing to try anything.
At our first visit, I prescribed him weekly tirzepatide (Zepbound) off label, along with a small dose of naltrexone.
Richard shared some feedback after his first 2 weeks:
The naltrexone works great and is strong ... small dose for me effective ... I haven’t wanted to drink and when I do I can’t finish a glass over 2 hours … went from 25 drinks a week to about 4 … don’t notice other side effects … sleeping better too.
And after 6 weeks:
Some more feedback … on week 6-7 and all going well ... drinking very little alcohol and still on half tab of naltrexone ... that works well and have no side effects ... the Zepbound works well too. I do get hungry a few days after the shot but still don’t crave sugar or bad snacks … weight down 21 pounds since started … 292 to 271.
And finally, after 8 weeks:
Looking at my last text to you I see the progress … been incredible ... now down 35 pounds and at 257 … continue to feel excellent with plenty of energy … want to exercise more ... and no temptation to eat or drink unhealthy stuff ... I’m very happy this has surpassed my expectations on how fast it’s worked and I don’t feel any side effects. Marriage has never been better … all thanks to you.
Tirzepatide contains two hormones, glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), that are naturally produced by our bodies after meals. Scientists recently learned that the GLP-1 system contributes to the feedback loop of addictive behaviors. Increasing synthetic GLP-1, through medications like tirzepatide, appears to minimize addictive behaviors by limiting their ability to upregulate the brain’s production of dopamine.
Dopamine is a neurotransmitter produced in the brain’s reward center, which regulates how people experience pleasure and control impulses. Dopamine reinforces the pleasure experienced by certain behaviors like drinking, smoking, and eating sweets. These new medications reduce the amount of dopamine released after these activities and thereby lower the motivation to repeat these behaviors.
Contrary to some reports in the news, the vast majority of my male patients using these medications for alcohol abuse disorder experience concurrent increases in testosterone, for two reasons: (1) testosterone increases as body mass index decreases and (2) chronic alcohol use can damage the cells in the testicles that produce testosterone and also decrease the brain’s ability to stimulate the testicles to produce testosterone.
At his most recent checkup last month, Richard’s testosterone had risen from borderline to robust levels, his libido and sleep had improved, and he reported never having felt so healthy or confident. Fingers crossed that the US Food and Drug Administration won’t wait too long before approving this class of medications for more than just diabetes, heart disease, and obesity.
*Patient’s name has been changed.
Dr. Messer is clinical assistant professor, Icahn School of Medicine at Mount Sinai, New York, and associate professor, Zucker School of Medicine at Hofstra University, Hempstead, New York. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Richard* was a master-of-the-universe type. He went to Wharton, ran a large hedge fund, and lived in Greenwich, Connecticut. His three children attended Ivy League schools. He played golf on the weekends and ate three healthy meals per day. There was just one issue: He had gained 90 pounds since the 1990s from consuming six to seven alcoholic beverages per day. He already had one DUI under his belt, and his marriage was on shaky ground. He had tried to address his alcohol abuse disorder on multiple occasions: He went to a yearlong class on alcoholism, saw a psychologist for cognitive-behavioral therapy, and joined Alcoholics Anonymous, all to no avail.
When I met him in December 2023, he had hit rock bottom and was willing to try anything.
At our first visit, I prescribed him weekly tirzepatide (Zepbound) off label, along with a small dose of naltrexone.
Richard shared some feedback after his first 2 weeks:
The naltrexone works great and is strong ... small dose for me effective ... I haven’t wanted to drink and when I do I can’t finish a glass over 2 hours … went from 25 drinks a week to about 4 … don’t notice other side effects … sleeping better too.
And after 6 weeks:
Some more feedback … on week 6-7 and all going well ... drinking very little alcohol and still on half tab of naltrexone ... that works well and have no side effects ... the Zepbound works well too. I do get hungry a few days after the shot but still don’t crave sugar or bad snacks … weight down 21 pounds since started … 292 to 271.
And finally, after 8 weeks:
Looking at my last text to you I see the progress … been incredible ... now down 35 pounds and at 257 … continue to feel excellent with plenty of energy … want to exercise more ... and no temptation to eat or drink unhealthy stuff ... I’m very happy this has surpassed my expectations on how fast it’s worked and I don’t feel any side effects. Marriage has never been better … all thanks to you.
Tirzepatide contains two hormones, glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), that are naturally produced by our bodies after meals. Scientists recently learned that the GLP-1 system contributes to the feedback loop of addictive behaviors. Increasing synthetic GLP-1, through medications like tirzepatide, appears to minimize addictive behaviors by limiting their ability to upregulate the brain’s production of dopamine.
Dopamine is a neurotransmitter produced in the brain’s reward center, which regulates how people experience pleasure and control impulses. Dopamine reinforces the pleasure experienced by certain behaviors like drinking, smoking, and eating sweets. These new medications reduce the amount of dopamine released after these activities and thereby lower the motivation to repeat these behaviors.
Contrary to some reports in the news, the vast majority of my male patients using these medications for alcohol abuse disorder experience concurrent increases in testosterone, for two reasons: (1) testosterone increases as body mass index decreases and (2) chronic alcohol use can damage the cells in the testicles that produce testosterone and also decrease the brain’s ability to stimulate the testicles to produce testosterone.
At his most recent checkup last month, Richard’s testosterone had risen from borderline to robust levels, his libido and sleep had improved, and he reported never having felt so healthy or confident. Fingers crossed that the US Food and Drug Administration won’t wait too long before approving this class of medications for more than just diabetes, heart disease, and obesity.
*Patient’s name has been changed.
Dr. Messer is clinical assistant professor, Icahn School of Medicine at Mount Sinai, New York, and associate professor, Zucker School of Medicine at Hofstra University, Hempstead, New York. She has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Is Semaglutide the ‘New Statin’? Not So Fast
There has been much hyperbole since the presentation of results from the SELECT cardiovascular outcomes trial (CVOT) at this year’s European Congress on Obesity, which led many to herald semaglutide as the “new statin.”
In the SELECT CVOT, participants with overweight or obesity (body mass index [BMI] ≥ 27), established cardiovascular disease (CVD), and no history of type 2 diabetes were administered the injectable glucagon-like peptide 1 (GLP-1) receptor agonist semaglutide (Wegovy) at a 2.4-mg dose weekly. Treatment resulted in a significant 20% relative risk reduction in major adverse CV events (a composite endpoint comprising CV death, nonfatal myocardial infarction, or nonfatal stroke). Importantly, SELECT was a trial on secondary prevention of CVD.
The CV benefits of semaglutide were notably independent of baseline weight or amount of weight lost. This suggests that the underlying driver of improved CV outcomes with semaglutide extends beyond simple reduction in obesity and perhaps indicates a direct effect on vasculature and reduction in atherosclerosis, although this remains unproven.
Not All Risk Reduction Is Equal
Much of the sensationalist coverage in the lay press focused on the 20% relative risk reduction figure. This endpoint is often more impressive and headline-grabbing than the absolute risk reduction, which provides a clearer view of a treatment’s real-world impact.
In SELECT, the absolute risk reduction was 1.5 percentage points, which translated into a number needed to treat (NNT) of 67 over 34 months to prevent one primary outcome of a major adverse CV event.
Lower NNTs suggest more effective treatments because fewer people need to be treated to prevent one clinical event, such as the major adverse CV events used in SELECT.
Semaglutide vs Statins
How does the clinical effectiveness observed in the SELECT trial compare with that observed in statin trials when it comes to the secondary prevention of CVD?
The seminal 4S study published in 1994 explored the impact of simvastatin on all-cause mortality among people with previous myocardial infarction or angina and hyperlipidemia (mean baseline BMI, 26). After 5.4 years of follow-up, the trial was stopped early owing to a 3.3-percentage point absolute risk reduction in all-cause mortality (NNT, 30; relative risk reduction, 28%). The NNT to prevent one death from CV causes was 31, and the NNT to prevent one major coronary event was lower, at 15.
Other statin secondary prevention trials, such as the LIPID and MIRACL studies, demonstrated similarly low NNTs.
So, you can see that the NNTs for statins in secondary prevention are much lower than with semaglutide in SELECT. Furthermore, the benefits of semaglutide in preventing CVD in people living with overweight/obesity have yet to be elucidated.
In contrast, we already have published evidence showing the benefits of statins in the primary prevention of CVD, albeit with higher and more variable NNTs than in the statin secondary prevention studies.
The benefits of statins are also postulated to extend beyond their impact on lowering low-density lipoprotein cholesterol. Statins have been suggested to have anti-inflammatory and plaque-stabilizing effects, among other pleiotropic benefits.
We also currently lack evidence for the cost-effectiveness of semaglutide for CV risk reduction. Assessing economic viability and use in health care systems, such as the UK’s National Health Service, involves comparing the cost of semaglutide against the health care savings from prevented CV events. Health economic studies are vital to determine whether the benefits justify the expense. In contrast, the cost-effectiveness of statins is well established, particularly for high-risk individuals.
Advantages of GLP-1s Should Not Be Overlooked
Of course, statins don’t provide the significant weight loss benefits of semaglutide.
Additional data from SELECT presented at the 2024 European Congress on Obesity demonstrated that participants lost a mean of 10.2% body weight and 7.7 cm from their waist circumference after 4 years. Moreover, after 2 years, 12% of individuals randomized to semaglutide had returned to a normal BMI, and nearly half were no longer living with obesity.
Although the CV benefits of semaglutide were independent of weight reduction, this level of weight loss is clinically meaningful and will reduce the risk of many other cardiometabolic conditions including type 2 diabetes, metabolic dysfunction–associated steatotic liver disease, and obstructive sleep apnea/hypopnea syndrome, as well as improve low mood, depression, and overall quality of life. Additionally, obesity is now a risk factor for 13 different types of cancer, including bowel, breast, and pancreatic cancer, so facilitating a return to a healthier body weight will also mitigate future risk for cancer.
Sticking With Our Cornerstone Therapy, For Now
In conclusion, I do not believe that semaglutide is the “new statin.” Statins are the cornerstone of primary and secondary prevention of CVD in a wide range of comorbidities, as evidenced in multiple large and high-quality trials dating back over 30 years.
However, there is no doubt that the GLP-1 receptor agonist class is the most significant therapeutic advance for the management of obesity and comorbidities to date.
The SELECT CVOT data uniquely position semaglutide as a secondary CVD prevention agent on top of guideline-driven management for people living with overweight/obesity and established CVD. Additionally, the clinically meaningful weight loss achieved with semaglutide will impact the risk of developing many other cardiometabolic conditions, as well as improve mental health and overall quality of life.
Dr. Fernando, GP Partner, North Berwick Health Centre, North Berwick, Scotland, creates concise clinical aide-mémoire for primary and secondary care to make life easier for health care professionals and ultimately to improve the lives of patients. He is very active on social media (X handle @drkevinfernando), where he posts hot topics in type 2 diabetes and CVRM. He recently has forayed into YouTube (@DrKevinFernando) and TikTok (@drkevinfernando) with patient-facing video content. Dr. Fernando has been elected to Fellowship of the Royal College of General Practitioners, the Royal College of Physicians of Edinburgh, and the Academy of Medical Educators for his work in diabetes and medical education. He has disclosed the following relevant financial relationships: Serve(d) as a speaker or a member of a speakers bureau for AstraZeneca; Boehringer Ingelheim; Lilly; Menarini; Bayer; Dexcom; Novartis; Novo Nordisk; Amgen; and Daiichi Sankyo; received income in an amount equal to or greater than $250 from AstraZeneca; Boehringer Ingelheim; Lilly; Menarini; Bayer; Dexcom; Novartis; Novo Nordisk; Amgen; and Daiichi Sankyo.
A version of this article first appeared on Medscape.com.
There has been much hyperbole since the presentation of results from the SELECT cardiovascular outcomes trial (CVOT) at this year’s European Congress on Obesity, which led many to herald semaglutide as the “new statin.”
In the SELECT CVOT, participants with overweight or obesity (body mass index [BMI] ≥ 27), established cardiovascular disease (CVD), and no history of type 2 diabetes were administered the injectable glucagon-like peptide 1 (GLP-1) receptor agonist semaglutide (Wegovy) at a 2.4-mg dose weekly. Treatment resulted in a significant 20% relative risk reduction in major adverse CV events (a composite endpoint comprising CV death, nonfatal myocardial infarction, or nonfatal stroke). Importantly, SELECT was a trial on secondary prevention of CVD.
The CV benefits of semaglutide were notably independent of baseline weight or amount of weight lost. This suggests that the underlying driver of improved CV outcomes with semaglutide extends beyond simple reduction in obesity and perhaps indicates a direct effect on vasculature and reduction in atherosclerosis, although this remains unproven.
Not All Risk Reduction Is Equal
Much of the sensationalist coverage in the lay press focused on the 20% relative risk reduction figure. This endpoint is often more impressive and headline-grabbing than the absolute risk reduction, which provides a clearer view of a treatment’s real-world impact.
In SELECT, the absolute risk reduction was 1.5 percentage points, which translated into a number needed to treat (NNT) of 67 over 34 months to prevent one primary outcome of a major adverse CV event.
Lower NNTs suggest more effective treatments because fewer people need to be treated to prevent one clinical event, such as the major adverse CV events used in SELECT.
Semaglutide vs Statins
How does the clinical effectiveness observed in the SELECT trial compare with that observed in statin trials when it comes to the secondary prevention of CVD?
The seminal 4S study published in 1994 explored the impact of simvastatin on all-cause mortality among people with previous myocardial infarction or angina and hyperlipidemia (mean baseline BMI, 26). After 5.4 years of follow-up, the trial was stopped early owing to a 3.3-percentage point absolute risk reduction in all-cause mortality (NNT, 30; relative risk reduction, 28%). The NNT to prevent one death from CV causes was 31, and the NNT to prevent one major coronary event was lower, at 15.
Other statin secondary prevention trials, such as the LIPID and MIRACL studies, demonstrated similarly low NNTs.
So, you can see that the NNTs for statins in secondary prevention are much lower than with semaglutide in SELECT. Furthermore, the benefits of semaglutide in preventing CVD in people living with overweight/obesity have yet to be elucidated.
In contrast, we already have published evidence showing the benefits of statins in the primary prevention of CVD, albeit with higher and more variable NNTs than in the statin secondary prevention studies.
The benefits of statins are also postulated to extend beyond their impact on lowering low-density lipoprotein cholesterol. Statins have been suggested to have anti-inflammatory and plaque-stabilizing effects, among other pleiotropic benefits.
We also currently lack evidence for the cost-effectiveness of semaglutide for CV risk reduction. Assessing economic viability and use in health care systems, such as the UK’s National Health Service, involves comparing the cost of semaglutide against the health care savings from prevented CV events. Health economic studies are vital to determine whether the benefits justify the expense. In contrast, the cost-effectiveness of statins is well established, particularly for high-risk individuals.
Advantages of GLP-1s Should Not Be Overlooked
Of course, statins don’t provide the significant weight loss benefits of semaglutide.
Additional data from SELECT presented at the 2024 European Congress on Obesity demonstrated that participants lost a mean of 10.2% body weight and 7.7 cm from their waist circumference after 4 years. Moreover, after 2 years, 12% of individuals randomized to semaglutide had returned to a normal BMI, and nearly half were no longer living with obesity.
Although the CV benefits of semaglutide were independent of weight reduction, this level of weight loss is clinically meaningful and will reduce the risk of many other cardiometabolic conditions including type 2 diabetes, metabolic dysfunction–associated steatotic liver disease, and obstructive sleep apnea/hypopnea syndrome, as well as improve low mood, depression, and overall quality of life. Additionally, obesity is now a risk factor for 13 different types of cancer, including bowel, breast, and pancreatic cancer, so facilitating a return to a healthier body weight will also mitigate future risk for cancer.
Sticking With Our Cornerstone Therapy, For Now
In conclusion, I do not believe that semaglutide is the “new statin.” Statins are the cornerstone of primary and secondary prevention of CVD in a wide range of comorbidities, as evidenced in multiple large and high-quality trials dating back over 30 years.
However, there is no doubt that the GLP-1 receptor agonist class is the most significant therapeutic advance for the management of obesity and comorbidities to date.
The SELECT CVOT data uniquely position semaglutide as a secondary CVD prevention agent on top of guideline-driven management for people living with overweight/obesity and established CVD. Additionally, the clinically meaningful weight loss achieved with semaglutide will impact the risk of developing many other cardiometabolic conditions, as well as improve mental health and overall quality of life.
Dr. Fernando, GP Partner, North Berwick Health Centre, North Berwick, Scotland, creates concise clinical aide-mémoire for primary and secondary care to make life easier for health care professionals and ultimately to improve the lives of patients. He is very active on social media (X handle @drkevinfernando), where he posts hot topics in type 2 diabetes and CVRM. He recently has forayed into YouTube (@DrKevinFernando) and TikTok (@drkevinfernando) with patient-facing video content. Dr. Fernando has been elected to Fellowship of the Royal College of General Practitioners, the Royal College of Physicians of Edinburgh, and the Academy of Medical Educators for his work in diabetes and medical education. He has disclosed the following relevant financial relationships: Serve(d) as a speaker or a member of a speakers bureau for AstraZeneca; Boehringer Ingelheim; Lilly; Menarini; Bayer; Dexcom; Novartis; Novo Nordisk; Amgen; and Daiichi Sankyo; received income in an amount equal to or greater than $250 from AstraZeneca; Boehringer Ingelheim; Lilly; Menarini; Bayer; Dexcom; Novartis; Novo Nordisk; Amgen; and Daiichi Sankyo.
A version of this article first appeared on Medscape.com.
There has been much hyperbole since the presentation of results from the SELECT cardiovascular outcomes trial (CVOT) at this year’s European Congress on Obesity, which led many to herald semaglutide as the “new statin.”
In the SELECT CVOT, participants with overweight or obesity (body mass index [BMI] ≥ 27), established cardiovascular disease (CVD), and no history of type 2 diabetes were administered the injectable glucagon-like peptide 1 (GLP-1) receptor agonist semaglutide (Wegovy) at a 2.4-mg dose weekly. Treatment resulted in a significant 20% relative risk reduction in major adverse CV events (a composite endpoint comprising CV death, nonfatal myocardial infarction, or nonfatal stroke). Importantly, SELECT was a trial on secondary prevention of CVD.
The CV benefits of semaglutide were notably independent of baseline weight or amount of weight lost. This suggests that the underlying driver of improved CV outcomes with semaglutide extends beyond simple reduction in obesity and perhaps indicates a direct effect on vasculature and reduction in atherosclerosis, although this remains unproven.
Not All Risk Reduction Is Equal
Much of the sensationalist coverage in the lay press focused on the 20% relative risk reduction figure. This endpoint is often more impressive and headline-grabbing than the absolute risk reduction, which provides a clearer view of a treatment’s real-world impact.
In SELECT, the absolute risk reduction was 1.5 percentage points, which translated into a number needed to treat (NNT) of 67 over 34 months to prevent one primary outcome of a major adverse CV event.
Lower NNTs suggest more effective treatments because fewer people need to be treated to prevent one clinical event, such as the major adverse CV events used in SELECT.
Semaglutide vs Statins
How does the clinical effectiveness observed in the SELECT trial compare with that observed in statin trials when it comes to the secondary prevention of CVD?
The seminal 4S study published in 1994 explored the impact of simvastatin on all-cause mortality among people with previous myocardial infarction or angina and hyperlipidemia (mean baseline BMI, 26). After 5.4 years of follow-up, the trial was stopped early owing to a 3.3-percentage point absolute risk reduction in all-cause mortality (NNT, 30; relative risk reduction, 28%). The NNT to prevent one death from CV causes was 31, and the NNT to prevent one major coronary event was lower, at 15.
Other statin secondary prevention trials, such as the LIPID and MIRACL studies, demonstrated similarly low NNTs.
So, you can see that the NNTs for statins in secondary prevention are much lower than with semaglutide in SELECT. Furthermore, the benefits of semaglutide in preventing CVD in people living with overweight/obesity have yet to be elucidated.
In contrast, we already have published evidence showing the benefits of statins in the primary prevention of CVD, albeit with higher and more variable NNTs than in the statin secondary prevention studies.
The benefits of statins are also postulated to extend beyond their impact on lowering low-density lipoprotein cholesterol. Statins have been suggested to have anti-inflammatory and plaque-stabilizing effects, among other pleiotropic benefits.
We also currently lack evidence for the cost-effectiveness of semaglutide for CV risk reduction. Assessing economic viability and use in health care systems, such as the UK’s National Health Service, involves comparing the cost of semaglutide against the health care savings from prevented CV events. Health economic studies are vital to determine whether the benefits justify the expense. In contrast, the cost-effectiveness of statins is well established, particularly for high-risk individuals.
Advantages of GLP-1s Should Not Be Overlooked
Of course, statins don’t provide the significant weight loss benefits of semaglutide.
Additional data from SELECT presented at the 2024 European Congress on Obesity demonstrated that participants lost a mean of 10.2% body weight and 7.7 cm from their waist circumference after 4 years. Moreover, after 2 years, 12% of individuals randomized to semaglutide had returned to a normal BMI, and nearly half were no longer living with obesity.
Although the CV benefits of semaglutide were independent of weight reduction, this level of weight loss is clinically meaningful and will reduce the risk of many other cardiometabolic conditions including type 2 diabetes, metabolic dysfunction–associated steatotic liver disease, and obstructive sleep apnea/hypopnea syndrome, as well as improve low mood, depression, and overall quality of life. Additionally, obesity is now a risk factor for 13 different types of cancer, including bowel, breast, and pancreatic cancer, so facilitating a return to a healthier body weight will also mitigate future risk for cancer.
Sticking With Our Cornerstone Therapy, For Now
In conclusion, I do not believe that semaglutide is the “new statin.” Statins are the cornerstone of primary and secondary prevention of CVD in a wide range of comorbidities, as evidenced in multiple large and high-quality trials dating back over 30 years.
However, there is no doubt that the GLP-1 receptor agonist class is the most significant therapeutic advance for the management of obesity and comorbidities to date.
The SELECT CVOT data uniquely position semaglutide as a secondary CVD prevention agent on top of guideline-driven management for people living with overweight/obesity and established CVD. Additionally, the clinically meaningful weight loss achieved with semaglutide will impact the risk of developing many other cardiometabolic conditions, as well as improve mental health and overall quality of life.
Dr. Fernando, GP Partner, North Berwick Health Centre, North Berwick, Scotland, creates concise clinical aide-mémoire for primary and secondary care to make life easier for health care professionals and ultimately to improve the lives of patients. He is very active on social media (X handle @drkevinfernando), where he posts hot topics in type 2 diabetes and CVRM. He recently has forayed into YouTube (@DrKevinFernando) and TikTok (@drkevinfernando) with patient-facing video content. Dr. Fernando has been elected to Fellowship of the Royal College of General Practitioners, the Royal College of Physicians of Edinburgh, and the Academy of Medical Educators for his work in diabetes and medical education. He has disclosed the following relevant financial relationships: Serve(d) as a speaker or a member of a speakers bureau for AstraZeneca; Boehringer Ingelheim; Lilly; Menarini; Bayer; Dexcom; Novartis; Novo Nordisk; Amgen; and Daiichi Sankyo; received income in an amount equal to or greater than $250 from AstraZeneca; Boehringer Ingelheim; Lilly; Menarini; Bayer; Dexcom; Novartis; Novo Nordisk; Amgen; and Daiichi Sankyo.
A version of this article first appeared on Medscape.com.
Low-Field MRIs
Recently, “low field” MRIs have been in the news, with the promise that they’ll be safer and easier. People can go in them with their cell phones, car keys in pockets, no ear plugs needed for the noise, etc. They’re cheaper to build and can be plugged into a standard outlet.
That’s all well and good, but what about accuracy and image quality?
That’s a big question. Even proponents of the technology say it’s not as good as what we see with 3T MRI, so they’re trying to compensate by using AI and other software protocols to enhance the pictures. Allegedly it looks good, but so far only healthy volunteers have been scanned. How will it do with a small low-grade glioma or other subtle (but important) findings? We don’t know yet.
Personally, I think having to give up your iPhone and car keys for an hour, and put in foam ear plugs, are small trade-offs to get an accurate diagnosis.
Of course, I’m also approaching this as someone who deals with brain imaging. Maybe for other structures, like a knee, that kind of detail isn’t as necessary (or maybe it is. I’m definitely not in that field).
So, as with so many things that make it into the popular press, they likely have potential, but are still not ready for prime time.
This sort of stuff always gets my office phones ringing. Patients see a blurb about it on the news or Facebook and assume it’s available now, so they want one. They seem to think the new MRI is like Bones McCoy’s tricorder. I take the scanner off my belt, wave it over them, and the answer comes up on the screen. The fact that the unit still weighs over a ton is hidden at the bottom of the blurb, if it’s even mentioned at all.
There’s also the likelihood that this sort of thing is going to be taken to the public, in the same way carotid Dopplers have been. Marketed to the worried well with celebrity endorsements and taglines like “see what your doctor won’t look for.” Of course, MRIs are chock full of things like nonspecific white matter changes, disc bulges, tiny meningiomas, and a host of other incidental findings that cause panic in cyberchondriacs. Who then call us.
But that’s another story.
I understand that for some parts of the world a comparatively inexpensive, transportable, MRI that requires less shielding and power is a HUGE deal. Its availability can make the difference between life and death.
I’m not knocking the technology. I’m sure it will be useful. But, like so much in medicine, it’s not here yet.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Recently, “low field” MRIs have been in the news, with the promise that they’ll be safer and easier. People can go in them with their cell phones, car keys in pockets, no ear plugs needed for the noise, etc. They’re cheaper to build and can be plugged into a standard outlet.
That’s all well and good, but what about accuracy and image quality?
That’s a big question. Even proponents of the technology say it’s not as good as what we see with 3T MRI, so they’re trying to compensate by using AI and other software protocols to enhance the pictures. Allegedly it looks good, but so far only healthy volunteers have been scanned. How will it do with a small low-grade glioma or other subtle (but important) findings? We don’t know yet.
Personally, I think having to give up your iPhone and car keys for an hour, and put in foam ear plugs, are small trade-offs to get an accurate diagnosis.
Of course, I’m also approaching this as someone who deals with brain imaging. Maybe for other structures, like a knee, that kind of detail isn’t as necessary (or maybe it is. I’m definitely not in that field).
So, as with so many things that make it into the popular press, they likely have potential, but are still not ready for prime time.
This sort of stuff always gets my office phones ringing. Patients see a blurb about it on the news or Facebook and assume it’s available now, so they want one. They seem to think the new MRI is like Bones McCoy’s tricorder. I take the scanner off my belt, wave it over them, and the answer comes up on the screen. The fact that the unit still weighs over a ton is hidden at the bottom of the blurb, if it’s even mentioned at all.
There’s also the likelihood that this sort of thing is going to be taken to the public, in the same way carotid Dopplers have been. Marketed to the worried well with celebrity endorsements and taglines like “see what your doctor won’t look for.” Of course, MRIs are chock full of things like nonspecific white matter changes, disc bulges, tiny meningiomas, and a host of other incidental findings that cause panic in cyberchondriacs. Who then call us.
But that’s another story.
I understand that for some parts of the world a comparatively inexpensive, transportable, MRI that requires less shielding and power is a HUGE deal. Its availability can make the difference between life and death.
I’m not knocking the technology. I’m sure it will be useful. But, like so much in medicine, it’s not here yet.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Recently, “low field” MRIs have been in the news, with the promise that they’ll be safer and easier. People can go in them with their cell phones, car keys in pockets, no ear plugs needed for the noise, etc. They’re cheaper to build and can be plugged into a standard outlet.
That’s all well and good, but what about accuracy and image quality?
That’s a big question. Even proponents of the technology say it’s not as good as what we see with 3T MRI, so they’re trying to compensate by using AI and other software protocols to enhance the pictures. Allegedly it looks good, but so far only healthy volunteers have been scanned. How will it do with a small low-grade glioma or other subtle (but important) findings? We don’t know yet.
Personally, I think having to give up your iPhone and car keys for an hour, and put in foam ear plugs, are small trade-offs to get an accurate diagnosis.
Of course, I’m also approaching this as someone who deals with brain imaging. Maybe for other structures, like a knee, that kind of detail isn’t as necessary (or maybe it is. I’m definitely not in that field).
So, as with so many things that make it into the popular press, they likely have potential, but are still not ready for prime time.
This sort of stuff always gets my office phones ringing. Patients see a blurb about it on the news or Facebook and assume it’s available now, so they want one. They seem to think the new MRI is like Bones McCoy’s tricorder. I take the scanner off my belt, wave it over them, and the answer comes up on the screen. The fact that the unit still weighs over a ton is hidden at the bottom of the blurb, if it’s even mentioned at all.
There’s also the likelihood that this sort of thing is going to be taken to the public, in the same way carotid Dopplers have been. Marketed to the worried well with celebrity endorsements and taglines like “see what your doctor won’t look for.” Of course, MRIs are chock full of things like nonspecific white matter changes, disc bulges, tiny meningiomas, and a host of other incidental findings that cause panic in cyberchondriacs. Who then call us.
But that’s another story.
I understand that for some parts of the world a comparatively inexpensive, transportable, MRI that requires less shielding and power is a HUGE deal. Its availability can make the difference between life and death.
I’m not knocking the technology. I’m sure it will be useful. But, like so much in medicine, it’s not here yet.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
The Value of Early Education
Early education is right up there with motherhood and apple pie as unarguable positive concepts. How could exposing young children to a school-like atmosphere not be a benefit, particularly in communities dominated by socioeconomic challenges? While there are some questions about the value of playing Mozart to infants, early education in the traditional sense continues to be viewed as a key strategy for providing young children a preschool foundation on which a successful academic career can be built. Several oft-cited randomized controlled trials have fueled both private and public interest and funding.
However, a recent commentary published in Science suggests that all programs are “not unequivocally positive and much more research is needed.” “Worrisome results in Tennessee,” “Success in Boston,” and “Largely null results for Headstart” are just a few of the article’s section titles and convey a sense of the inconsistency the investigators found as they reviewed early education systems around the country.
While there may be some politicians who may attempt to use the results of this investigation as a reason to cancel public funding of underperforming early education programs, the authors avoid this baby-and-the-bathwater conclusion. Instead, they urge more rigorous research “to understand how effective programs can be designed and implemented.”
The kind of re-thinking and brainstorming these investigators suggest takes time. While we’re waiting for this process to gain traction, this might be a good time to consider some of the benefits of early education that we don’t usually consider when our focus is on academic metrics.
A recent paper in Children’s Health Care by investigators at the Boston University Medical Center and School of Medicine considered the diet of children attending preschool. Looking at the dietary records of more than 300 children attending 30 childcare centers, the researchers found that the children’s diets before arrival at daycare was less healthy than while they were in daycare. “The hour after pickup appeared to be the least healthful” of any of the time periods surveyed. Of course, we will all conjure up images of what this chaotic post-daycare pickup may look like and cut the harried parents and grandparents some slack when it comes to nutritional choices. However, the bottom line is that for the group of children surveyed being in preschool or daycare protected them from a less healthy diet they were being provided outside of school hours.
Our recent experience with pandemic-related school closures provides more evidence that being in school was superior to any remote experience academically. School-age children and adolescents gained weight when school closures were the norm. Play patterns for children shifted from outdoor play to indoor play — often dominated by more sedentary video games. Both fatal and non-fatal gun-related injuries surged during the pandemic and, by far, the majority of these occur in the home and not at school.
Stepping back to look at this broader picture that includes diet, physical activity, and safety — not to mention the benefits of socialization — leads one to arrive at the unfortunate conclusion that Of course there will be those who point to the belief that schools are petri dishes putting children at greater risk for respiratory infections. On the other hand, we must accept that schools haven’t proved to be a major factor in the spread of COVID that many had feared.
The authors of the study in Science are certainly correct in recommending a more thorough investigation into the academic benefits of preschool education. However, we must keep in mind that preschool offers an environment that can be a positive influence on young children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Early education is right up there with motherhood and apple pie as unarguable positive concepts. How could exposing young children to a school-like atmosphere not be a benefit, particularly in communities dominated by socioeconomic challenges? While there are some questions about the value of playing Mozart to infants, early education in the traditional sense continues to be viewed as a key strategy for providing young children a preschool foundation on which a successful academic career can be built. Several oft-cited randomized controlled trials have fueled both private and public interest and funding.
However, a recent commentary published in Science suggests that all programs are “not unequivocally positive and much more research is needed.” “Worrisome results in Tennessee,” “Success in Boston,” and “Largely null results for Headstart” are just a few of the article’s section titles and convey a sense of the inconsistency the investigators found as they reviewed early education systems around the country.
While there may be some politicians who may attempt to use the results of this investigation as a reason to cancel public funding of underperforming early education programs, the authors avoid this baby-and-the-bathwater conclusion. Instead, they urge more rigorous research “to understand how effective programs can be designed and implemented.”
The kind of re-thinking and brainstorming these investigators suggest takes time. While we’re waiting for this process to gain traction, this might be a good time to consider some of the benefits of early education that we don’t usually consider when our focus is on academic metrics.
A recent paper in Children’s Health Care by investigators at the Boston University Medical Center and School of Medicine considered the diet of children attending preschool. Looking at the dietary records of more than 300 children attending 30 childcare centers, the researchers found that the children’s diets before arrival at daycare was less healthy than while they were in daycare. “The hour after pickup appeared to be the least healthful” of any of the time periods surveyed. Of course, we will all conjure up images of what this chaotic post-daycare pickup may look like and cut the harried parents and grandparents some slack when it comes to nutritional choices. However, the bottom line is that for the group of children surveyed being in preschool or daycare protected them from a less healthy diet they were being provided outside of school hours.
Our recent experience with pandemic-related school closures provides more evidence that being in school was superior to any remote experience academically. School-age children and adolescents gained weight when school closures were the norm. Play patterns for children shifted from outdoor play to indoor play — often dominated by more sedentary video games. Both fatal and non-fatal gun-related injuries surged during the pandemic and, by far, the majority of these occur in the home and not at school.
Stepping back to look at this broader picture that includes diet, physical activity, and safety — not to mention the benefits of socialization — leads one to arrive at the unfortunate conclusion that Of course there will be those who point to the belief that schools are petri dishes putting children at greater risk for respiratory infections. On the other hand, we must accept that schools haven’t proved to be a major factor in the spread of COVID that many had feared.
The authors of the study in Science are certainly correct in recommending a more thorough investigation into the academic benefits of preschool education. However, we must keep in mind that preschool offers an environment that can be a positive influence on young children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Early education is right up there with motherhood and apple pie as unarguable positive concepts. How could exposing young children to a school-like atmosphere not be a benefit, particularly in communities dominated by socioeconomic challenges? While there are some questions about the value of playing Mozart to infants, early education in the traditional sense continues to be viewed as a key strategy for providing young children a preschool foundation on which a successful academic career can be built. Several oft-cited randomized controlled trials have fueled both private and public interest and funding.
However, a recent commentary published in Science suggests that all programs are “not unequivocally positive and much more research is needed.” “Worrisome results in Tennessee,” “Success in Boston,” and “Largely null results for Headstart” are just a few of the article’s section titles and convey a sense of the inconsistency the investigators found as they reviewed early education systems around the country.
While there may be some politicians who may attempt to use the results of this investigation as a reason to cancel public funding of underperforming early education programs, the authors avoid this baby-and-the-bathwater conclusion. Instead, they urge more rigorous research “to understand how effective programs can be designed and implemented.”
The kind of re-thinking and brainstorming these investigators suggest takes time. While we’re waiting for this process to gain traction, this might be a good time to consider some of the benefits of early education that we don’t usually consider when our focus is on academic metrics.
A recent paper in Children’s Health Care by investigators at the Boston University Medical Center and School of Medicine considered the diet of children attending preschool. Looking at the dietary records of more than 300 children attending 30 childcare centers, the researchers found that the children’s diets before arrival at daycare was less healthy than while they were in daycare. “The hour after pickup appeared to be the least healthful” of any of the time periods surveyed. Of course, we will all conjure up images of what this chaotic post-daycare pickup may look like and cut the harried parents and grandparents some slack when it comes to nutritional choices. However, the bottom line is that for the group of children surveyed being in preschool or daycare protected them from a less healthy diet they were being provided outside of school hours.
Our recent experience with pandemic-related school closures provides more evidence that being in school was superior to any remote experience academically. School-age children and adolescents gained weight when school closures were the norm. Play patterns for children shifted from outdoor play to indoor play — often dominated by more sedentary video games. Both fatal and non-fatal gun-related injuries surged during the pandemic and, by far, the majority of these occur in the home and not at school.
Stepping back to look at this broader picture that includes diet, physical activity, and safety — not to mention the benefits of socialization — leads one to arrive at the unfortunate conclusion that Of course there will be those who point to the belief that schools are petri dishes putting children at greater risk for respiratory infections. On the other hand, we must accept that schools haven’t proved to be a major factor in the spread of COVID that many had feared.
The authors of the study in Science are certainly correct in recommending a more thorough investigation into the academic benefits of preschool education. However, we must keep in mind that preschool offers an environment that can be a positive influence on young children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Calcium and CV Risk: Are Supplements and Vitamin D to Blame?
This transcript has been edited for clarity.
Tricia Ward: Hi. I’m Tricia Ward, from theheart.org/Medscape Cardiology. I’m joined today by Dr Matthew Budoff. He is professor of medicine at UCLA and the endowed chair of preventive cardiology at the Lundquist Institute. Welcome, Dr Budoff.
Matthew J. Budoff, MD: Thank you.
Dietary Calcium vs Coronary Calcium
Ms. Ward: The reason I wanted to talk to you today is because there have been some recent studies linking calcium supplements to an increased risk for cardiovascular disease. I’m old enough to remember when we used to tell people that dietary calcium and coronary calcium weren’t connected and weren’t the same. Were we wrong?
Dr. Budoff: I think there’s a large amount of mixed data out there still. The US Preventive Services Task Force looked into this a number of years ago and said there’s no association between calcium supplementation and increased risk for cardiovascular disease.
As you mentioned, there are a couple of newer studies that point us toward a relationship. I think that we still have a little bit of a mixed bag, but we need to dive a little deeper into that to figure out what’s going on.
Ms. Ward: Does it appear to be connected to calcium in the form of supplements vs calcium from foods?
Dr. Budoff: We looked very carefully at dietary calcium in the MESA study, the multiethnic study of atherosclerosis. There is no relationship between dietary calcium intake and coronary calcium or cardiovascular events. We’re talking mostly about supplements now when we talk about this increased risk that we’re seeing.
Does Vitamin D Exacerbate Risk?
Ms. Ward: Because it’s seen with supplements, is that likely because that’s a much higher concentration of calcium coming in or do you think it’s something inherent in its being in the form of a supplement?
Dr. Budoff: I think there are two things. One, it’s definitely a higher concentration all at once. You get many more milligrams at a time when you take a supplement than if you had a high-calcium food or drink.
Also, most supplements have vitamin D as well. I think vitamin D and calcium work synergistically. When you give them both together simultaneously, I think that may have more of a potentiating effect that might exacerbate any potential risk.
Ms. Ward: Is there any reason to think there might be a difference in type of calcium supplement? I always think of the chalky tablet form vs calcium chews.
Dr. Budoff: I’m not aware of a difference in the supplement type. I think the vitamin D issue is a big problem because we all have patients who take thousands of units of vitamin D — just crazy numbers. People advocate really high numbers and that stays in the system.
Personally, I think part of the explanation is that with very high levels of vitamin D on top of calcium supplementation, you now absorb it better. You now get it into the bone, but maybe also into the coronary arteries. If you’re very high in vitamin D and then are taking a large calcium supplement, it might be the calcium/vitamin D combination that’s giving us some trouble. I think people on vitamin D supplements really need to watch their levels and not get supratherapeutic.
Ms. Ward: With the vitamin D?
Dr. Budoff: With the vitamin D.
Diabetes and Renal Function
Ms. Ward: In some of the studies, there seems to be a higher risk in patients with diabetes. Is there any reason why that would be?
Dr. Budoff: I can’t think of a reason exactly why with diabetes per se, except for renal disease. Patients with diabetes have more intrinsic renal disease, proteinuria, and even a reduced eGFR. We’ve seen that the kidney is very strongly tied to this. We have a very strong relationship, in work I’ve done a decade ago now, showing that calcium supplementation (in the form of phosphate binders) in patients on dialysis or with advanced renal disease is linked to much higher coronary calcium progression.
We did prospective, randomized trials showing that calcium intake as binders to reduce phosphorus led to more coronary calcium. We always thought that was just relegated to the renal population, and there might be an overlap here with the diabetes and more renal disease. I have a feeling that it has to do with more of that. It might be regulation of parathyroid hormone as well, which might be more abnormal in patients with diabetes.
Avoid Supratherapeutic Vitamin D Levels
Ms. Ward:: What are you telling your patients?
Dr. Budoff: I tell patients with normal kidney function that the bone will modulate 99.9% of the calcium uptake. If they have osteopenia or osteoporosis, regardless of their calcium score, I’m very comfortable putting them on supplements.
I’m a little more cautious with the vitamin D levels, and I keep an eye on that and regulate how much vitamin D they get based on their levels. I get them into the normal range, but I don’t want them supratherapeutic. You can even follow their calcium score. Again, we’ve shown that if you’re taking too much calcium, your calcium score will go up. I can just check it again in a couple of years to make sure that it’s safe.
Ms. Ward:: In terms of vitamin D levels, when you’re saying “supratherapeutic,” what levels do you consider a safe amount to take?
Dr. Budoff: I’d like them under 100 ng/mL as far as their upper level. Normal is around 70 ng/mL at most labs. I try to keep them in the normal range. I don’t even want them to be high-normal if I’m going to be concomitantly giving them calcium supplements. Of course, if they have renal insufficiency, then I’m much more cautious. We’ve even seen calcium supplements raise the serum calcium, which you never see with dietary calcium. That’s another potential proof that it might be too much too fast.
For renal patients, even in mild renal insufficiency, maybe even in diabetes where we’ve seen a signal, maybe aim lower in the amount of calcium supplementation if diet is insufficient, and aim a little lower in vitamin D targets, and I think you’ll be in a safer place.
Ms. Ward: Is there anything else you want to add?
Dr. Budoff: The evidence is still evolving. I’d say that it’s interesting and maybe a little frustrating that we don’t have a final answer on all of this. I would stay tuned for more data because we’re looking at many of the epidemiologic studies to try to see what happens in the real world, with both dietary intake of calcium and calcium supplementation.
Ms. Ward: Thank you very much for joining me today.
Dr. Budoff: It’s a pleasure. Thanks for having me.
Dr. Budoff disclosed being a speaker for Amarin Pharma.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Tricia Ward: Hi. I’m Tricia Ward, from theheart.org/Medscape Cardiology. I’m joined today by Dr Matthew Budoff. He is professor of medicine at UCLA and the endowed chair of preventive cardiology at the Lundquist Institute. Welcome, Dr Budoff.
Matthew J. Budoff, MD: Thank you.
Dietary Calcium vs Coronary Calcium
Ms. Ward: The reason I wanted to talk to you today is because there have been some recent studies linking calcium supplements to an increased risk for cardiovascular disease. I’m old enough to remember when we used to tell people that dietary calcium and coronary calcium weren’t connected and weren’t the same. Were we wrong?
Dr. Budoff: I think there’s a large amount of mixed data out there still. The US Preventive Services Task Force looked into this a number of years ago and said there’s no association between calcium supplementation and increased risk for cardiovascular disease.
As you mentioned, there are a couple of newer studies that point us toward a relationship. I think that we still have a little bit of a mixed bag, but we need to dive a little deeper into that to figure out what’s going on.
Ms. Ward: Does it appear to be connected to calcium in the form of supplements vs calcium from foods?
Dr. Budoff: We looked very carefully at dietary calcium in the MESA study, the multiethnic study of atherosclerosis. There is no relationship between dietary calcium intake and coronary calcium or cardiovascular events. We’re talking mostly about supplements now when we talk about this increased risk that we’re seeing.
Does Vitamin D Exacerbate Risk?
Ms. Ward: Because it’s seen with supplements, is that likely because that’s a much higher concentration of calcium coming in or do you think it’s something inherent in its being in the form of a supplement?
Dr. Budoff: I think there are two things. One, it’s definitely a higher concentration all at once. You get many more milligrams at a time when you take a supplement than if you had a high-calcium food or drink.
Also, most supplements have vitamin D as well. I think vitamin D and calcium work synergistically. When you give them both together simultaneously, I think that may have more of a potentiating effect that might exacerbate any potential risk.
Ms. Ward: Is there any reason to think there might be a difference in type of calcium supplement? I always think of the chalky tablet form vs calcium chews.
Dr. Budoff: I’m not aware of a difference in the supplement type. I think the vitamin D issue is a big problem because we all have patients who take thousands of units of vitamin D — just crazy numbers. People advocate really high numbers and that stays in the system.
Personally, I think part of the explanation is that with very high levels of vitamin D on top of calcium supplementation, you now absorb it better. You now get it into the bone, but maybe also into the coronary arteries. If you’re very high in vitamin D and then are taking a large calcium supplement, it might be the calcium/vitamin D combination that’s giving us some trouble. I think people on vitamin D supplements really need to watch their levels and not get supratherapeutic.
Ms. Ward: With the vitamin D?
Dr. Budoff: With the vitamin D.
Diabetes and Renal Function
Ms. Ward: In some of the studies, there seems to be a higher risk in patients with diabetes. Is there any reason why that would be?
Dr. Budoff: I can’t think of a reason exactly why with diabetes per se, except for renal disease. Patients with diabetes have more intrinsic renal disease, proteinuria, and even a reduced eGFR. We’ve seen that the kidney is very strongly tied to this. We have a very strong relationship, in work I’ve done a decade ago now, showing that calcium supplementation (in the form of phosphate binders) in patients on dialysis or with advanced renal disease is linked to much higher coronary calcium progression.
We did prospective, randomized trials showing that calcium intake as binders to reduce phosphorus led to more coronary calcium. We always thought that was just relegated to the renal population, and there might be an overlap here with the diabetes and more renal disease. I have a feeling that it has to do with more of that. It might be regulation of parathyroid hormone as well, which might be more abnormal in patients with diabetes.
Avoid Supratherapeutic Vitamin D Levels
Ms. Ward:: What are you telling your patients?
Dr. Budoff: I tell patients with normal kidney function that the bone will modulate 99.9% of the calcium uptake. If they have osteopenia or osteoporosis, regardless of their calcium score, I’m very comfortable putting them on supplements.
I’m a little more cautious with the vitamin D levels, and I keep an eye on that and regulate how much vitamin D they get based on their levels. I get them into the normal range, but I don’t want them supratherapeutic. You can even follow their calcium score. Again, we’ve shown that if you’re taking too much calcium, your calcium score will go up. I can just check it again in a couple of years to make sure that it’s safe.
Ms. Ward:: In terms of vitamin D levels, when you’re saying “supratherapeutic,” what levels do you consider a safe amount to take?
Dr. Budoff: I’d like them under 100 ng/mL as far as their upper level. Normal is around 70 ng/mL at most labs. I try to keep them in the normal range. I don’t even want them to be high-normal if I’m going to be concomitantly giving them calcium supplements. Of course, if they have renal insufficiency, then I’m much more cautious. We’ve even seen calcium supplements raise the serum calcium, which you never see with dietary calcium. That’s another potential proof that it might be too much too fast.
For renal patients, even in mild renal insufficiency, maybe even in diabetes where we’ve seen a signal, maybe aim lower in the amount of calcium supplementation if diet is insufficient, and aim a little lower in vitamin D targets, and I think you’ll be in a safer place.
Ms. Ward: Is there anything else you want to add?
Dr. Budoff: The evidence is still evolving. I’d say that it’s interesting and maybe a little frustrating that we don’t have a final answer on all of this. I would stay tuned for more data because we’re looking at many of the epidemiologic studies to try to see what happens in the real world, with both dietary intake of calcium and calcium supplementation.
Ms. Ward: Thank you very much for joining me today.
Dr. Budoff: It’s a pleasure. Thanks for having me.
Dr. Budoff disclosed being a speaker for Amarin Pharma.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Tricia Ward: Hi. I’m Tricia Ward, from theheart.org/Medscape Cardiology. I’m joined today by Dr Matthew Budoff. He is professor of medicine at UCLA and the endowed chair of preventive cardiology at the Lundquist Institute. Welcome, Dr Budoff.
Matthew J. Budoff, MD: Thank you.
Dietary Calcium vs Coronary Calcium
Ms. Ward: The reason I wanted to talk to you today is because there have been some recent studies linking calcium supplements to an increased risk for cardiovascular disease. I’m old enough to remember when we used to tell people that dietary calcium and coronary calcium weren’t connected and weren’t the same. Were we wrong?
Dr. Budoff: I think there’s a large amount of mixed data out there still. The US Preventive Services Task Force looked into this a number of years ago and said there’s no association between calcium supplementation and increased risk for cardiovascular disease.
As you mentioned, there are a couple of newer studies that point us toward a relationship. I think that we still have a little bit of a mixed bag, but we need to dive a little deeper into that to figure out what’s going on.
Ms. Ward: Does it appear to be connected to calcium in the form of supplements vs calcium from foods?
Dr. Budoff: We looked very carefully at dietary calcium in the MESA study, the multiethnic study of atherosclerosis. There is no relationship between dietary calcium intake and coronary calcium or cardiovascular events. We’re talking mostly about supplements now when we talk about this increased risk that we’re seeing.
Does Vitamin D Exacerbate Risk?
Ms. Ward: Because it’s seen with supplements, is that likely because that’s a much higher concentration of calcium coming in or do you think it’s something inherent in its being in the form of a supplement?
Dr. Budoff: I think there are two things. One, it’s definitely a higher concentration all at once. You get many more milligrams at a time when you take a supplement than if you had a high-calcium food or drink.
Also, most supplements have vitamin D as well. I think vitamin D and calcium work synergistically. When you give them both together simultaneously, I think that may have more of a potentiating effect that might exacerbate any potential risk.
Ms. Ward: Is there any reason to think there might be a difference in type of calcium supplement? I always think of the chalky tablet form vs calcium chews.
Dr. Budoff: I’m not aware of a difference in the supplement type. I think the vitamin D issue is a big problem because we all have patients who take thousands of units of vitamin D — just crazy numbers. People advocate really high numbers and that stays in the system.
Personally, I think part of the explanation is that with very high levels of vitamin D on top of calcium supplementation, you now absorb it better. You now get it into the bone, but maybe also into the coronary arteries. If you’re very high in vitamin D and then are taking a large calcium supplement, it might be the calcium/vitamin D combination that’s giving us some trouble. I think people on vitamin D supplements really need to watch their levels and not get supratherapeutic.
Ms. Ward: With the vitamin D?
Dr. Budoff: With the vitamin D.
Diabetes and Renal Function
Ms. Ward: In some of the studies, there seems to be a higher risk in patients with diabetes. Is there any reason why that would be?
Dr. Budoff: I can’t think of a reason exactly why with diabetes per se, except for renal disease. Patients with diabetes have more intrinsic renal disease, proteinuria, and even a reduced eGFR. We’ve seen that the kidney is very strongly tied to this. We have a very strong relationship, in work I’ve done a decade ago now, showing that calcium supplementation (in the form of phosphate binders) in patients on dialysis or with advanced renal disease is linked to much higher coronary calcium progression.
We did prospective, randomized trials showing that calcium intake as binders to reduce phosphorus led to more coronary calcium. We always thought that was just relegated to the renal population, and there might be an overlap here with the diabetes and more renal disease. I have a feeling that it has to do with more of that. It might be regulation of parathyroid hormone as well, which might be more abnormal in patients with diabetes.
Avoid Supratherapeutic Vitamin D Levels
Ms. Ward:: What are you telling your patients?
Dr. Budoff: I tell patients with normal kidney function that the bone will modulate 99.9% of the calcium uptake. If they have osteopenia or osteoporosis, regardless of their calcium score, I’m very comfortable putting them on supplements.
I’m a little more cautious with the vitamin D levels, and I keep an eye on that and regulate how much vitamin D they get based on their levels. I get them into the normal range, but I don’t want them supratherapeutic. You can even follow their calcium score. Again, we’ve shown that if you’re taking too much calcium, your calcium score will go up. I can just check it again in a couple of years to make sure that it’s safe.
Ms. Ward:: In terms of vitamin D levels, when you’re saying “supratherapeutic,” what levels do you consider a safe amount to take?
Dr. Budoff: I’d like them under 100 ng/mL as far as their upper level. Normal is around 70 ng/mL at most labs. I try to keep them in the normal range. I don’t even want them to be high-normal if I’m going to be concomitantly giving them calcium supplements. Of course, if they have renal insufficiency, then I’m much more cautious. We’ve even seen calcium supplements raise the serum calcium, which you never see with dietary calcium. That’s another potential proof that it might be too much too fast.
For renal patients, even in mild renal insufficiency, maybe even in diabetes where we’ve seen a signal, maybe aim lower in the amount of calcium supplementation if diet is insufficient, and aim a little lower in vitamin D targets, and I think you’ll be in a safer place.
Ms. Ward: Is there anything else you want to add?
Dr. Budoff: The evidence is still evolving. I’d say that it’s interesting and maybe a little frustrating that we don’t have a final answer on all of this. I would stay tuned for more data because we’re looking at many of the epidemiologic studies to try to see what happens in the real world, with both dietary intake of calcium and calcium supplementation.
Ms. Ward: Thank you very much for joining me today.
Dr. Budoff: It’s a pleasure. Thanks for having me.
Dr. Budoff disclosed being a speaker for Amarin Pharma.
A version of this article appeared on Medscape.com.
In the Future, a Robot Intensivist May Save Your Life
This transcript has been edited for clarity.
They call it the “golden hour”: 60 minutes, give or take, when the chance to save the life of a trauma victim is at its greatest. If the patient can be resuscitated and stabilized in that time window, they stand a good chance of surviving. If not, well, they don’t.
But resuscitation is complicated. It requires blood products, fluids, vasopressors — all given in precise doses in response to rapidly changing hemodynamics. To do it right takes specialized training, advanced life support (ALS). If the patient is in a remote area or an area without ALS-certified emergency medical services, or is far from the nearest trauma center, that golden hour is lost. And the patient may be as well.
But we live in the future. We have robots in factories, self-driving cars, autonomous drones. Why not an autonomous trauma doctor? If you are in a life-threatening accident, would you want to be treated ... by a robot?
Enter “resuscitation based on functional hemodynamic monitoring,” or “ReFit,” introduced in this article appearing in the journal Intensive Care Medicine Experimental.
The idea behind ReFit is straightforward. Resuscitation after trauma should be based on hitting key hemodynamic targets using the tools we have available in the field: blood, fluids, pressors. The researchers wanted to develop a closed-loop system, something that could be used by minimally trained personnel. The input to the system? Hemodynamic data, provided through a single measurement device, an arterial catheter. The output: blood, fluids, and pressors, delivered intravenously.
The body (a prototype) of the system looks like this. You can see various pumps labeled with various fluids, electronic controllers, and so forth.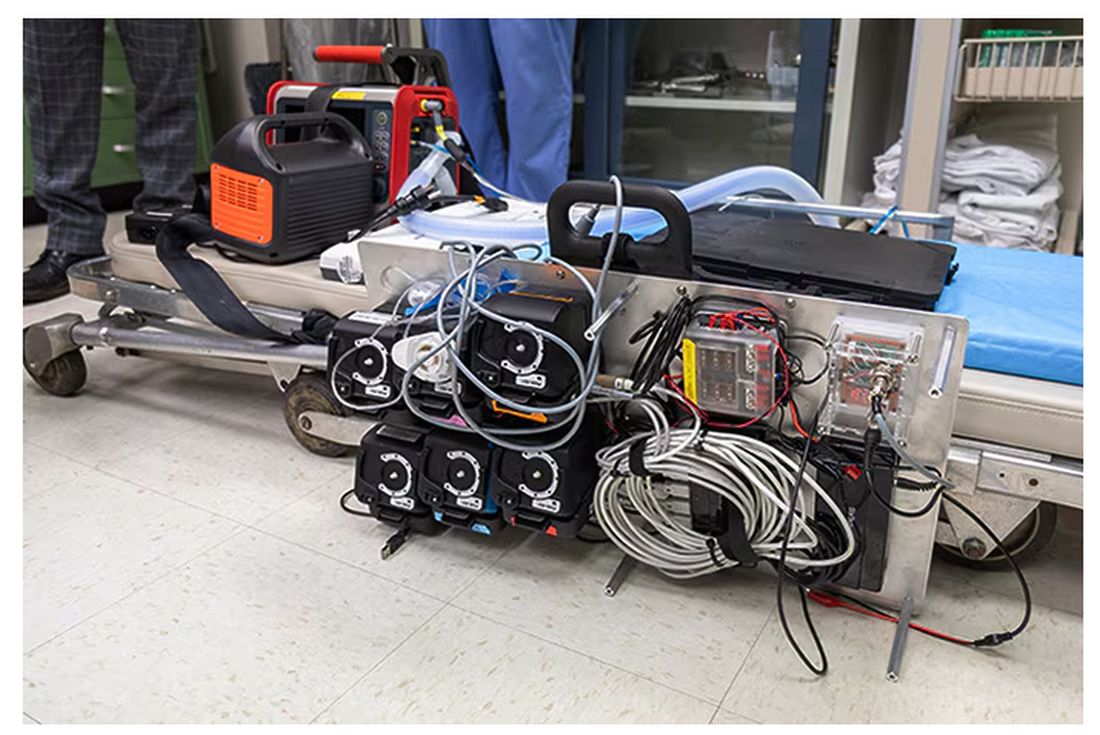
If that’s the body, then this is the brain – a ruggedized laptop interpreting a readout of that arterial catheter.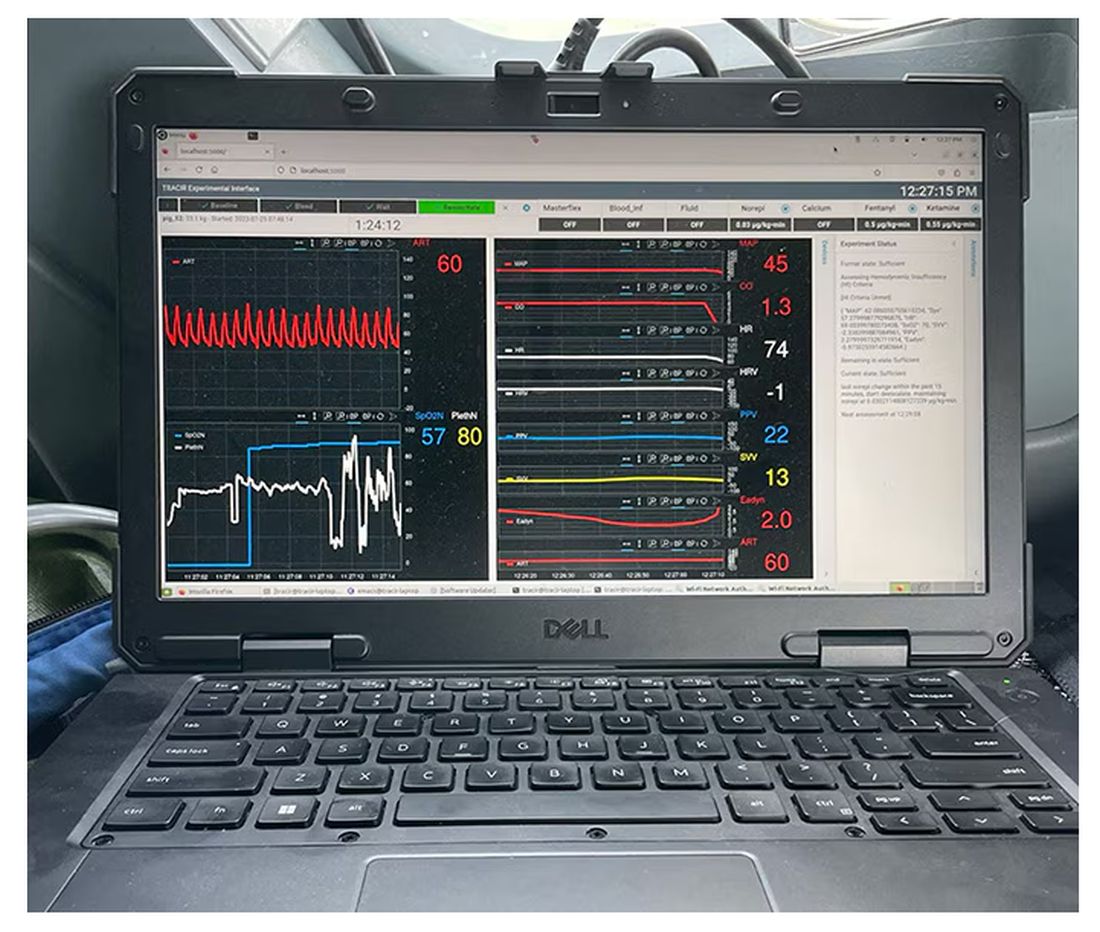
If that’s the brain, then the ReFit algorithm is the mind. The algorithm does its best to leverage all the data it can, so I want to walk through it in a bit of detail.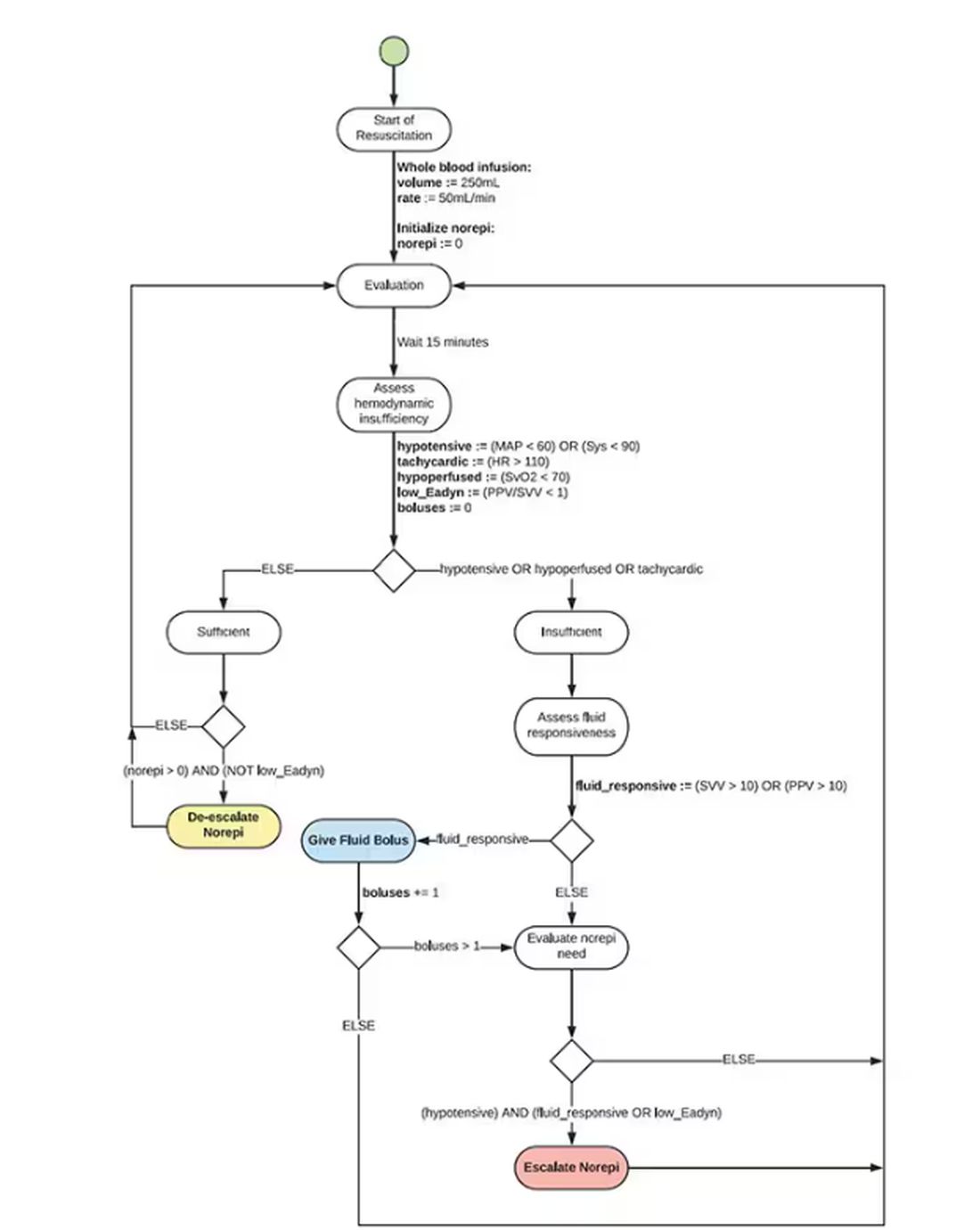
First, check to see whether the patient is stable, defined as a heart rate < 110 beats/min and a mean arterial pressure > 60 mm Hg. If not, you’re off to the races, starting with a bolus of whole blood.
Next, the algorithm gets really interesting. If the patient is still unstable, the computer assesses fluid responsiveness by giving a test dose of fluid and measuring the pulse pressure variation. Greater pulse pressure variation means more fluid responsiveness and the algorithm gives more fluid. Less pulse pressure variation leads the algorithm to uptitrate pressors — in this case, norepinephrine.
This cycle of evaluation and response keeps repeating. The computer titrates fluids and pressors up and down entirely on its own, in theory freeing the human team members to do other things, like getting the patient to a trauma center for definitive care.
So, how do you test whether something like this works? Clearly, you don’t want the trial run of a system like this to be used on a real human suffering from a real traumatic injury.
Once again, we have animals to thank for research advances — in this case, pigs. Fifteen pigs are described in the study. To simulate a severe, hemorrhagic trauma, they were anesthetized and the liver was lacerated. They were then observed passively until the mean arterial pressure had dropped to below 40 mm Hg.
This is a pretty severe injury. Three unfortunate animals served as controls, two of which died within the 3-hour time window of the study. Eight animals were plugged into the ReFit system.
For a window into what happens during this process, let’s take a look at the mean arterial pressure and heart rate readouts for one of the animals. You see that the blood pressure starts to fall precipitously after the liver laceration. The heart rate quickly picks up to compensate, raising the mean arterial pressure a bit, but this would be unsustainable with ongoing bleeding.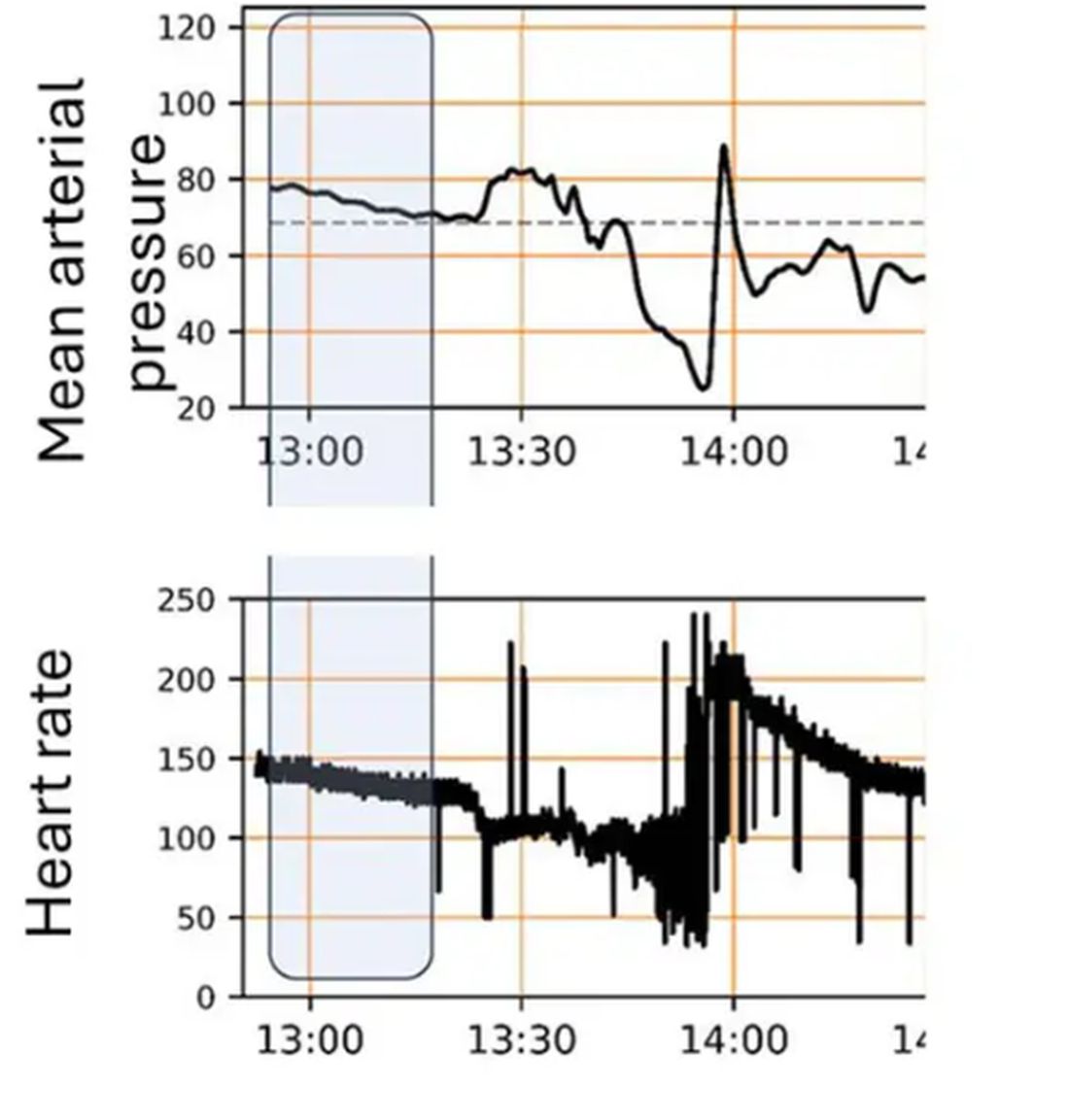
Here, the ReFit system takes over. Autonomously, the system administers two units of blood, followed by fluids, and then norepinephrine or further fluids per the protocol I described earlier. 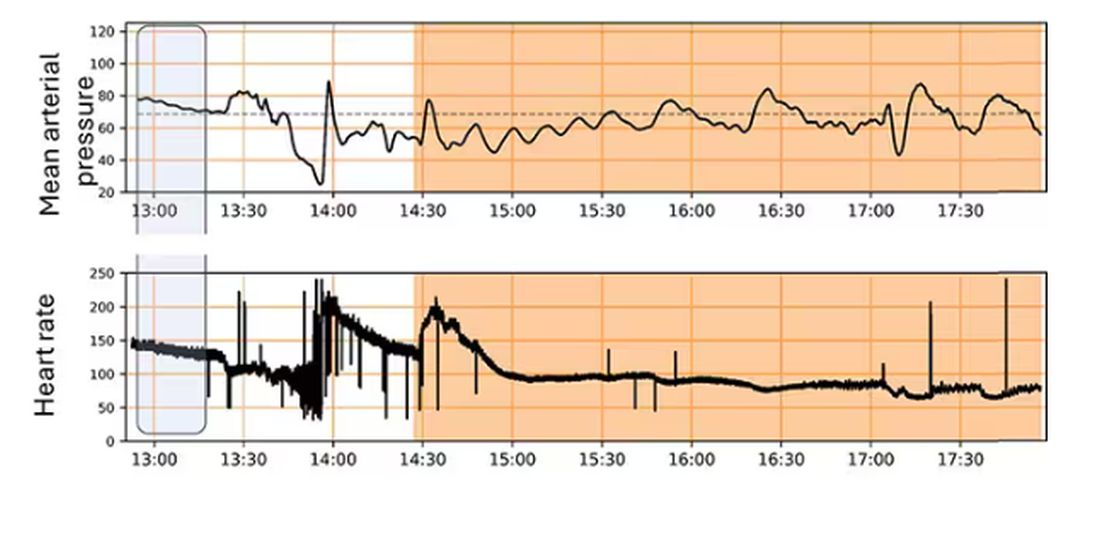
The practical upshot of all of this is stabilization, despite an as-yet untreated liver laceration.
Could an experienced ALS provider do this? Of course. But, as I mentioned before, you aren’t always near an experienced ALS provider.
This is all well and good in the lab, but in the real world, you actually need to transport a trauma patient. The researchers tried this also. To prove feasibility, four pigs were taken from the lab to the top of the University of Pittsburgh Medical Center, flown to Allegheny County Airport and back. Total time before liver laceration repair? Three hours. And all four survived.
It won’t surprise you to hear that this work was funded by the Department of Defense. You can see how a system like this, made a bit more rugged, a bit smaller, and a bit more self-contained could have real uses in the battlefield. But trauma is not unique to war, and something that can extend the time you have to safely transport a patient to definitive care — well, that’s worth its weight in golden hours.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
They call it the “golden hour”: 60 minutes, give or take, when the chance to save the life of a trauma victim is at its greatest. If the patient can be resuscitated and stabilized in that time window, they stand a good chance of surviving. If not, well, they don’t.
But resuscitation is complicated. It requires blood products, fluids, vasopressors — all given in precise doses in response to rapidly changing hemodynamics. To do it right takes specialized training, advanced life support (ALS). If the patient is in a remote area or an area without ALS-certified emergency medical services, or is far from the nearest trauma center, that golden hour is lost. And the patient may be as well.
But we live in the future. We have robots in factories, self-driving cars, autonomous drones. Why not an autonomous trauma doctor? If you are in a life-threatening accident, would you want to be treated ... by a robot?
Enter “resuscitation based on functional hemodynamic monitoring,” or “ReFit,” introduced in this article appearing in the journal Intensive Care Medicine Experimental.
The idea behind ReFit is straightforward. Resuscitation after trauma should be based on hitting key hemodynamic targets using the tools we have available in the field: blood, fluids, pressors. The researchers wanted to develop a closed-loop system, something that could be used by minimally trained personnel. The input to the system? Hemodynamic data, provided through a single measurement device, an arterial catheter. The output: blood, fluids, and pressors, delivered intravenously.
The body (a prototype) of the system looks like this. You can see various pumps labeled with various fluids, electronic controllers, and so forth.
If that’s the body, then this is the brain – a ruggedized laptop interpreting a readout of that arterial catheter.
If that’s the brain, then the ReFit algorithm is the mind. The algorithm does its best to leverage all the data it can, so I want to walk through it in a bit of detail.
First, check to see whether the patient is stable, defined as a heart rate < 110 beats/min and a mean arterial pressure > 60 mm Hg. If not, you’re off to the races, starting with a bolus of whole blood.
Next, the algorithm gets really interesting. If the patient is still unstable, the computer assesses fluid responsiveness by giving a test dose of fluid and measuring the pulse pressure variation. Greater pulse pressure variation means more fluid responsiveness and the algorithm gives more fluid. Less pulse pressure variation leads the algorithm to uptitrate pressors — in this case, norepinephrine.
This cycle of evaluation and response keeps repeating. The computer titrates fluids and pressors up and down entirely on its own, in theory freeing the human team members to do other things, like getting the patient to a trauma center for definitive care.
So, how do you test whether something like this works? Clearly, you don’t want the trial run of a system like this to be used on a real human suffering from a real traumatic injury.
Once again, we have animals to thank for research advances — in this case, pigs. Fifteen pigs are described in the study. To simulate a severe, hemorrhagic trauma, they were anesthetized and the liver was lacerated. They were then observed passively until the mean arterial pressure had dropped to below 40 mm Hg.
This is a pretty severe injury. Three unfortunate animals served as controls, two of which died within the 3-hour time window of the study. Eight animals were plugged into the ReFit system.
For a window into what happens during this process, let’s take a look at the mean arterial pressure and heart rate readouts for one of the animals. You see that the blood pressure starts to fall precipitously after the liver laceration. The heart rate quickly picks up to compensate, raising the mean arterial pressure a bit, but this would be unsustainable with ongoing bleeding.
Here, the ReFit system takes over. Autonomously, the system administers two units of blood, followed by fluids, and then norepinephrine or further fluids per the protocol I described earlier.
The practical upshot of all of this is stabilization, despite an as-yet untreated liver laceration.
Could an experienced ALS provider do this? Of course. But, as I mentioned before, you aren’t always near an experienced ALS provider.
This is all well and good in the lab, but in the real world, you actually need to transport a trauma patient. The researchers tried this also. To prove feasibility, four pigs were taken from the lab to the top of the University of Pittsburgh Medical Center, flown to Allegheny County Airport and back. Total time before liver laceration repair? Three hours. And all four survived.
It won’t surprise you to hear that this work was funded by the Department of Defense. You can see how a system like this, made a bit more rugged, a bit smaller, and a bit more self-contained could have real uses in the battlefield. But trauma is not unique to war, and something that can extend the time you have to safely transport a patient to definitive care — well, that’s worth its weight in golden hours.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
They call it the “golden hour”: 60 minutes, give or take, when the chance to save the life of a trauma victim is at its greatest. If the patient can be resuscitated and stabilized in that time window, they stand a good chance of surviving. If not, well, they don’t.
But resuscitation is complicated. It requires blood products, fluids, vasopressors — all given in precise doses in response to rapidly changing hemodynamics. To do it right takes specialized training, advanced life support (ALS). If the patient is in a remote area or an area without ALS-certified emergency medical services, or is far from the nearest trauma center, that golden hour is lost. And the patient may be as well.
But we live in the future. We have robots in factories, self-driving cars, autonomous drones. Why not an autonomous trauma doctor? If you are in a life-threatening accident, would you want to be treated ... by a robot?
Enter “resuscitation based on functional hemodynamic monitoring,” or “ReFit,” introduced in this article appearing in the journal Intensive Care Medicine Experimental.
The idea behind ReFit is straightforward. Resuscitation after trauma should be based on hitting key hemodynamic targets using the tools we have available in the field: blood, fluids, pressors. The researchers wanted to develop a closed-loop system, something that could be used by minimally trained personnel. The input to the system? Hemodynamic data, provided through a single measurement device, an arterial catheter. The output: blood, fluids, and pressors, delivered intravenously.
The body (a prototype) of the system looks like this. You can see various pumps labeled with various fluids, electronic controllers, and so forth.
If that’s the body, then this is the brain – a ruggedized laptop interpreting a readout of that arterial catheter.
If that’s the brain, then the ReFit algorithm is the mind. The algorithm does its best to leverage all the data it can, so I want to walk through it in a bit of detail.
First, check to see whether the patient is stable, defined as a heart rate < 110 beats/min and a mean arterial pressure > 60 mm Hg. If not, you’re off to the races, starting with a bolus of whole blood.
Next, the algorithm gets really interesting. If the patient is still unstable, the computer assesses fluid responsiveness by giving a test dose of fluid and measuring the pulse pressure variation. Greater pulse pressure variation means more fluid responsiveness and the algorithm gives more fluid. Less pulse pressure variation leads the algorithm to uptitrate pressors — in this case, norepinephrine.
This cycle of evaluation and response keeps repeating. The computer titrates fluids and pressors up and down entirely on its own, in theory freeing the human team members to do other things, like getting the patient to a trauma center for definitive care.
So, how do you test whether something like this works? Clearly, you don’t want the trial run of a system like this to be used on a real human suffering from a real traumatic injury.
Once again, we have animals to thank for research advances — in this case, pigs. Fifteen pigs are described in the study. To simulate a severe, hemorrhagic trauma, they were anesthetized and the liver was lacerated. They were then observed passively until the mean arterial pressure had dropped to below 40 mm Hg.
This is a pretty severe injury. Three unfortunate animals served as controls, two of which died within the 3-hour time window of the study. Eight animals were plugged into the ReFit system.
For a window into what happens during this process, let’s take a look at the mean arterial pressure and heart rate readouts for one of the animals. You see that the blood pressure starts to fall precipitously after the liver laceration. The heart rate quickly picks up to compensate, raising the mean arterial pressure a bit, but this would be unsustainable with ongoing bleeding.
Here, the ReFit system takes over. Autonomously, the system administers two units of blood, followed by fluids, and then norepinephrine or further fluids per the protocol I described earlier.
The practical upshot of all of this is stabilization, despite an as-yet untreated liver laceration.
Could an experienced ALS provider do this? Of course. But, as I mentioned before, you aren’t always near an experienced ALS provider.
This is all well and good in the lab, but in the real world, you actually need to transport a trauma patient. The researchers tried this also. To prove feasibility, four pigs were taken from the lab to the top of the University of Pittsburgh Medical Center, flown to Allegheny County Airport and back. Total time before liver laceration repair? Three hours. And all four survived.
It won’t surprise you to hear that this work was funded by the Department of Defense. You can see how a system like this, made a bit more rugged, a bit smaller, and a bit more self-contained could have real uses in the battlefield. But trauma is not unique to war, and something that can extend the time you have to safely transport a patient to definitive care — well, that’s worth its weight in golden hours.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
When It Comes to Medicine, ‘Women Are Not Small Men’
Welcome everyone. I’m Dr. John White. I’m the chief medical officer at WebMD. Does your biologic sex impact your health? Does it have any play in how you’re diagnosed, how you’re treated in terms of what symptoms you have? Of course it does. We all know that. But that’s not something that many people believed 5, 10 years ago, certainly not 20 years ago. And it was only because of leaders like my guest today, Phyllis Greenberger, who really championed the need for research on women’s health. She has a new book out, which I love. It’s called Sex Cells: the Fight to Overcome Bias and Discrimination in Women’s Healthcare. Please welcome my very good friend, Phyllis Greenberger.
Thank you.
Phyllis, It’s great to see you today.
It’s great to see you as well.
Now, you and I have been talking about this for easily 2 decades.
At least.
And some people think, oh, of course it makes sense. Although I saw you disagreeing that not everyone still believes that. But what has been that journey? Why has it been so hard to make people understand, as you point out early on in your book, women are not smaller men?
I think the basic reason was that it was just believed that men and women were the same except for their reproductive organs. So minus the reproductive organs, whether it was a device, a diagnostic, or therapeutic, if it was used and successful on a male, that it would be successful on a female. We’re really very far from understanding the differences, and there’s still a lot of distrust and disbelief and ignorance about it. And so there’s still a long way to go.
But you talk about that in the book, that there’s still a long way to go. Why is that? What’s the biggest obstacle? Is it just misinformation, lack of information? People don’t understand the science? There’s still resistance in some areas. Why is that?
I think it’s misinformation, and I gave a presentation, I don’t know how many years ago, at least 20 years ago, about the curriculum. And at the time, there was no women’s health in the curriculum. It was health. So if it was on cardiovascular issues or on osteoporosis, it was sort of the basic. And at the time, there would maybe be one woman whose job was women’s health, and she’d have an office, and otherwise there was nothing. And maybe they talked about breast cancer, who knows. But I spoke to someone just the other day, in view of all the attention that the book is getting now, whether that’s changed, whether it’s necessary and required. And she said it’s not. So, it’s not necessarily on the curriculum of all research and medical institutions, and even if women’s health, quote unquote, is on the curriculum, it doesn’t mean that they’re really looking at sex differences. And the difference is obvious. I mean, gender is really, it’s a social construct, but biological sex is how disease occurs and develops. And so if you’re not looking, and because there’s so little research now on sex differences that I don’t even know, I mean, how much you could actually teach.
So what needs to change? This book is a manifesto in many ways in how we need to include women; we need to make research more inclusive of everyone. But we’re not there yet. So what needs to change, Phyllis?
During this whole saga of trying to get people to listen to me and to the society, we really started out just looking at clinical trials and that, as you mentioned, I mean, there are issues in rural communities. There’s travel issues for women and child care. There’s a lot of disbelief or fear of clinical trials in some ethnicities. I do think, going to the future, that technology can help that. I mean, if people have broadband, which of course is also an issue in rural areas.
What could women do today? What should women listeners hear and then be doing? Should they be saying something to their doctor? Should they be asking specific questions? When they interact with the health care system, how can they make sure they’re getting the best care that’s appropriate for them when we know that sex cells matter?
Well, that’s a good question. It depends on, frankly, if your doctor is aware of this, if he or she has learned anything about this in school, which, I had already said, we’re not sure about that because research is still ongoing and there’s so much we don’t know. So I mean, you used to think, or I used to think, that you go to, you want a physician who’s older and more experienced. But now I think you should be going to a physician who’s younger and hopefully has learned about this, because the physicians that were educated years ago and have been practicing for 20, 30 years, I don’t know how much they know about this, whether they’re even aware of it.
Phyllis, you are a woman of action. You’ve lived in the DC area. You have championed legislative reforms, executive agendas. What do you want done now? What needs to be changed today? The curriculum is going to take time, but what else needs to change?
That’s a good question. I mean, if curriculum is going to take a while and you can ask your doctor if he prescribes the medication, whether it’s been tested on women, but then if it hasn’t been tested on women, but it’s the only thing that there is for your condition, I mean, so it’s very difficult. The Biden administration, as you know, just allocated a hundred million dollars for women’s health research.
What do you hope to accomplish with this book?
Well, what I’m hoping is that I spoke to someone at AMWA and I’m hoping — and AMWA is an association for women medical students. And I’m hoping that’s the audience. The audience needs to be. I mean, obviously everybody that I know that’s not a doctor that’s read it, found it fascinating and didn’t know a lot of the stuff that was in it. So I think it’s an interesting book anyway, and I think women should be aware of it. But really I think it needs to be for medical students.
And to your credit, you built the Society for Women’s Health Research into a powerful force in Washington under your tenure in really promoting the need for Office of Women’s Health and Research in general. The book is entitled Sex Cells, the Fight to Overcome Bias and Discrimination in Women’s Healthcare. Phyllis Greenberger, thank you so much for all that you’ve done for women’s health, for women’s research. We wouldn’t be where we are today if it wasn’t for you. So thanks.
Thank you very much, John. Thank you. I appreciate the opportunity.
Dr. Whyte, is chief medical officer, WebMD, New York, NY. He has disclosed no relevant financial relationships. Ms. Greenberger is a women’s health advocate and author of “Sex Cells: The Fight to Overcome Bias and Discrimination in Women’s Healthcare”
This interview originally appeared on WebMD on May 23, 2024. A version of this article appeared on Medscape.com .
Welcome everyone. I’m Dr. John White. I’m the chief medical officer at WebMD. Does your biologic sex impact your health? Does it have any play in how you’re diagnosed, how you’re treated in terms of what symptoms you have? Of course it does. We all know that. But that’s not something that many people believed 5, 10 years ago, certainly not 20 years ago. And it was only because of leaders like my guest today, Phyllis Greenberger, who really championed the need for research on women’s health. She has a new book out, which I love. It’s called Sex Cells: the Fight to Overcome Bias and Discrimination in Women’s Healthcare. Please welcome my very good friend, Phyllis Greenberger.
Thank you.
Phyllis, It’s great to see you today.
It’s great to see you as well.
Now, you and I have been talking about this for easily 2 decades.
At least.
And some people think, oh, of course it makes sense. Although I saw you disagreeing that not everyone still believes that. But what has been that journey? Why has it been so hard to make people understand, as you point out early on in your book, women are not smaller men?
I think the basic reason was that it was just believed that men and women were the same except for their reproductive organs. So minus the reproductive organs, whether it was a device, a diagnostic, or therapeutic, if it was used and successful on a male, that it would be successful on a female. We’re really very far from understanding the differences, and there’s still a lot of distrust and disbelief and ignorance about it. And so there’s still a long way to go.
But you talk about that in the book, that there’s still a long way to go. Why is that? What’s the biggest obstacle? Is it just misinformation, lack of information? People don’t understand the science? There’s still resistance in some areas. Why is that?
I think it’s misinformation, and I gave a presentation, I don’t know how many years ago, at least 20 years ago, about the curriculum. And at the time, there was no women’s health in the curriculum. It was health. So if it was on cardiovascular issues or on osteoporosis, it was sort of the basic. And at the time, there would maybe be one woman whose job was women’s health, and she’d have an office, and otherwise there was nothing. And maybe they talked about breast cancer, who knows. But I spoke to someone just the other day, in view of all the attention that the book is getting now, whether that’s changed, whether it’s necessary and required. And she said it’s not. So, it’s not necessarily on the curriculum of all research and medical institutions, and even if women’s health, quote unquote, is on the curriculum, it doesn’t mean that they’re really looking at sex differences. And the difference is obvious. I mean, gender is really, it’s a social construct, but biological sex is how disease occurs and develops. And so if you’re not looking, and because there’s so little research now on sex differences that I don’t even know, I mean, how much you could actually teach.
So what needs to change? This book is a manifesto in many ways in how we need to include women; we need to make research more inclusive of everyone. But we’re not there yet. So what needs to change, Phyllis?
During this whole saga of trying to get people to listen to me and to the society, we really started out just looking at clinical trials and that, as you mentioned, I mean, there are issues in rural communities. There’s travel issues for women and child care. There’s a lot of disbelief or fear of clinical trials in some ethnicities. I do think, going to the future, that technology can help that. I mean, if people have broadband, which of course is also an issue in rural areas.
What could women do today? What should women listeners hear and then be doing? Should they be saying something to their doctor? Should they be asking specific questions? When they interact with the health care system, how can they make sure they’re getting the best care that’s appropriate for them when we know that sex cells matter?
Well, that’s a good question. It depends on, frankly, if your doctor is aware of this, if he or she has learned anything about this in school, which, I had already said, we’re not sure about that because research is still ongoing and there’s so much we don’t know. So I mean, you used to think, or I used to think, that you go to, you want a physician who’s older and more experienced. But now I think you should be going to a physician who’s younger and hopefully has learned about this, because the physicians that were educated years ago and have been practicing for 20, 30 years, I don’t know how much they know about this, whether they’re even aware of it.
Phyllis, you are a woman of action. You’ve lived in the DC area. You have championed legislative reforms, executive agendas. What do you want done now? What needs to be changed today? The curriculum is going to take time, but what else needs to change?
That’s a good question. I mean, if curriculum is going to take a while and you can ask your doctor if he prescribes the medication, whether it’s been tested on women, but then if it hasn’t been tested on women, but it’s the only thing that there is for your condition, I mean, so it’s very difficult. The Biden administration, as you know, just allocated a hundred million dollars for women’s health research.
What do you hope to accomplish with this book?
Well, what I’m hoping is that I spoke to someone at AMWA and I’m hoping — and AMWA is an association for women medical students. And I’m hoping that’s the audience. The audience needs to be. I mean, obviously everybody that I know that’s not a doctor that’s read it, found it fascinating and didn’t know a lot of the stuff that was in it. So I think it’s an interesting book anyway, and I think women should be aware of it. But really I think it needs to be for medical students.
And to your credit, you built the Society for Women’s Health Research into a powerful force in Washington under your tenure in really promoting the need for Office of Women’s Health and Research in general. The book is entitled Sex Cells, the Fight to Overcome Bias and Discrimination in Women’s Healthcare. Phyllis Greenberger, thank you so much for all that you’ve done for women’s health, for women’s research. We wouldn’t be where we are today if it wasn’t for you. So thanks.
Thank you very much, John. Thank you. I appreciate the opportunity.
Dr. Whyte, is chief medical officer, WebMD, New York, NY. He has disclosed no relevant financial relationships. Ms. Greenberger is a women’s health advocate and author of “Sex Cells: The Fight to Overcome Bias and Discrimination in Women’s Healthcare”
This interview originally appeared on WebMD on May 23, 2024. A version of this article appeared on Medscape.com .
Welcome everyone. I’m Dr. John White. I’m the chief medical officer at WebMD. Does your biologic sex impact your health? Does it have any play in how you’re diagnosed, how you’re treated in terms of what symptoms you have? Of course it does. We all know that. But that’s not something that many people believed 5, 10 years ago, certainly not 20 years ago. And it was only because of leaders like my guest today, Phyllis Greenberger, who really championed the need for research on women’s health. She has a new book out, which I love. It’s called Sex Cells: the Fight to Overcome Bias and Discrimination in Women’s Healthcare. Please welcome my very good friend, Phyllis Greenberger.
Thank you.
Phyllis, It’s great to see you today.
It’s great to see you as well.
Now, you and I have been talking about this for easily 2 decades.
At least.
And some people think, oh, of course it makes sense. Although I saw you disagreeing that not everyone still believes that. But what has been that journey? Why has it been so hard to make people understand, as you point out early on in your book, women are not smaller men?
I think the basic reason was that it was just believed that men and women were the same except for their reproductive organs. So minus the reproductive organs, whether it was a device, a diagnostic, or therapeutic, if it was used and successful on a male, that it would be successful on a female. We’re really very far from understanding the differences, and there’s still a lot of distrust and disbelief and ignorance about it. And so there’s still a long way to go.
But you talk about that in the book, that there’s still a long way to go. Why is that? What’s the biggest obstacle? Is it just misinformation, lack of information? People don’t understand the science? There’s still resistance in some areas. Why is that?
I think it’s misinformation, and I gave a presentation, I don’t know how many years ago, at least 20 years ago, about the curriculum. And at the time, there was no women’s health in the curriculum. It was health. So if it was on cardiovascular issues or on osteoporosis, it was sort of the basic. And at the time, there would maybe be one woman whose job was women’s health, and she’d have an office, and otherwise there was nothing. And maybe they talked about breast cancer, who knows. But I spoke to someone just the other day, in view of all the attention that the book is getting now, whether that’s changed, whether it’s necessary and required. And she said it’s not. So, it’s not necessarily on the curriculum of all research and medical institutions, and even if women’s health, quote unquote, is on the curriculum, it doesn’t mean that they’re really looking at sex differences. And the difference is obvious. I mean, gender is really, it’s a social construct, but biological sex is how disease occurs and develops. And so if you’re not looking, and because there’s so little research now on sex differences that I don’t even know, I mean, how much you could actually teach.
So what needs to change? This book is a manifesto in many ways in how we need to include women; we need to make research more inclusive of everyone. But we’re not there yet. So what needs to change, Phyllis?
During this whole saga of trying to get people to listen to me and to the society, we really started out just looking at clinical trials and that, as you mentioned, I mean, there are issues in rural communities. There’s travel issues for women and child care. There’s a lot of disbelief or fear of clinical trials in some ethnicities. I do think, going to the future, that technology can help that. I mean, if people have broadband, which of course is also an issue in rural areas.
What could women do today? What should women listeners hear and then be doing? Should they be saying something to their doctor? Should they be asking specific questions? When they interact with the health care system, how can they make sure they’re getting the best care that’s appropriate for them when we know that sex cells matter?
Well, that’s a good question. It depends on, frankly, if your doctor is aware of this, if he or she has learned anything about this in school, which, I had already said, we’re not sure about that because research is still ongoing and there’s so much we don’t know. So I mean, you used to think, or I used to think, that you go to, you want a physician who’s older and more experienced. But now I think you should be going to a physician who’s younger and hopefully has learned about this, because the physicians that were educated years ago and have been practicing for 20, 30 years, I don’t know how much they know about this, whether they’re even aware of it.
Phyllis, you are a woman of action. You’ve lived in the DC area. You have championed legislative reforms, executive agendas. What do you want done now? What needs to be changed today? The curriculum is going to take time, but what else needs to change?
That’s a good question. I mean, if curriculum is going to take a while and you can ask your doctor if he prescribes the medication, whether it’s been tested on women, but then if it hasn’t been tested on women, but it’s the only thing that there is for your condition, I mean, so it’s very difficult. The Biden administration, as you know, just allocated a hundred million dollars for women’s health research.
What do you hope to accomplish with this book?
Well, what I’m hoping is that I spoke to someone at AMWA and I’m hoping — and AMWA is an association for women medical students. And I’m hoping that’s the audience. The audience needs to be. I mean, obviously everybody that I know that’s not a doctor that’s read it, found it fascinating and didn’t know a lot of the stuff that was in it. So I think it’s an interesting book anyway, and I think women should be aware of it. But really I think it needs to be for medical students.
And to your credit, you built the Society for Women’s Health Research into a powerful force in Washington under your tenure in really promoting the need for Office of Women’s Health and Research in general. The book is entitled Sex Cells, the Fight to Overcome Bias and Discrimination in Women’s Healthcare. Phyllis Greenberger, thank you so much for all that you’ve done for women’s health, for women’s research. We wouldn’t be where we are today if it wasn’t for you. So thanks.
Thank you very much, John. Thank you. I appreciate the opportunity.
Dr. Whyte, is chief medical officer, WebMD, New York, NY. He has disclosed no relevant financial relationships. Ms. Greenberger is a women’s health advocate and author of “Sex Cells: The Fight to Overcome Bias and Discrimination in Women’s Healthcare”
This interview originally appeared on WebMD on May 23, 2024. A version of this article appeared on Medscape.com .
Staving Off Obsolescence
I don’t write many checks anymore.
When I started my practice in 2000 I wrote a lot. Paychecks for my staff, my rent, insurance, IRA contributions, federal & state withholding, payments on my EMG machine, pretty much everything.
Checks are old. We’ve been using them in some form for roughly 2000 years.
But the online world has changed a lot of that. Now I write maybe 2-3 a month. I could probably do fewer, but haven’t bothered to set those accounts up that way.
I recently was down to my last few checks, so ordered replacements. The minimum order was 600. As I unpacked the box I realized they’re probably the last ones I’ll need, both because checks are gradually passing by and because there are more days behind in my neurology career than ahead.
The checks are a minor thing, but they do make you think. Certainly we’re in the last generation of people who will ever need to use paper checks. Some phrases like “blank check” will likely be with us long after they’re gone (like “dialing a phone”), but the real deal is heading the same way as 8-Track and VHS tapes.
As my 600 checks dwindle down, realistically, so will my career. There is no rewind button on life. I have no desire to leave medicine right now, but the passage of time changes things.
Does that mean I, like my checks, am also getting obsolete?
I hope not. I’d like to think I still have something to offer. I have 30 years of neurology experience behind me, and try to keep up to date on my field. My patients and staff depend on me to bring my best to the office every day.
I hope to stay that way to the end. I’d rather leave voluntarily, still at the top of my game. Even if I end up leaving a few unused checks behind.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
I don’t write many checks anymore.
When I started my practice in 2000 I wrote a lot. Paychecks for my staff, my rent, insurance, IRA contributions, federal & state withholding, payments on my EMG machine, pretty much everything.
Checks are old. We’ve been using them in some form for roughly 2000 years.
But the online world has changed a lot of that. Now I write maybe 2-3 a month. I could probably do fewer, but haven’t bothered to set those accounts up that way.
I recently was down to my last few checks, so ordered replacements. The minimum order was 600. As I unpacked the box I realized they’re probably the last ones I’ll need, both because checks are gradually passing by and because there are more days behind in my neurology career than ahead.
The checks are a minor thing, but they do make you think. Certainly we’re in the last generation of people who will ever need to use paper checks. Some phrases like “blank check” will likely be with us long after they’re gone (like “dialing a phone”), but the real deal is heading the same way as 8-Track and VHS tapes.
As my 600 checks dwindle down, realistically, so will my career. There is no rewind button on life. I have no desire to leave medicine right now, but the passage of time changes things.
Does that mean I, like my checks, am also getting obsolete?
I hope not. I’d like to think I still have something to offer. I have 30 years of neurology experience behind me, and try to keep up to date on my field. My patients and staff depend on me to bring my best to the office every day.
I hope to stay that way to the end. I’d rather leave voluntarily, still at the top of my game. Even if I end up leaving a few unused checks behind.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
I don’t write many checks anymore.
When I started my practice in 2000 I wrote a lot. Paychecks for my staff, my rent, insurance, IRA contributions, federal & state withholding, payments on my EMG machine, pretty much everything.
Checks are old. We’ve been using them in some form for roughly 2000 years.
But the online world has changed a lot of that. Now I write maybe 2-3 a month. I could probably do fewer, but haven’t bothered to set those accounts up that way.
I recently was down to my last few checks, so ordered replacements. The minimum order was 600. As I unpacked the box I realized they’re probably the last ones I’ll need, both because checks are gradually passing by and because there are more days behind in my neurology career than ahead.
The checks are a minor thing, but they do make you think. Certainly we’re in the last generation of people who will ever need to use paper checks. Some phrases like “blank check” will likely be with us long after they’re gone (like “dialing a phone”), but the real deal is heading the same way as 8-Track and VHS tapes.
As my 600 checks dwindle down, realistically, so will my career. There is no rewind button on life. I have no desire to leave medicine right now, but the passage of time changes things.
Does that mean I, like my checks, am also getting obsolete?
I hope not. I’d like to think I still have something to offer. I have 30 years of neurology experience behind me, and try to keep up to date on my field. My patients and staff depend on me to bring my best to the office every day.
I hope to stay that way to the end. I’d rather leave voluntarily, still at the top of my game. Even if I end up leaving a few unused checks behind.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Rethinking the Rebels
Each month I set out on an expedition to find a topic for this column. I came across a new book Rebel Health by Susannah Fox that I thought might be a good one. It’s both a treatise on the shortcomings of healthcare and a Baedeker for patients on how to find their way to being better served. Her argument is that many patients’ needs are unmet and their conditions are often invisible to us in mainstream healthcare. We fail to find solutions to help them. Patients would benefit from more open access to their records and more resources to take control of their own health, she argues. A few chapters in, I thought, “Oh, here we go, another diatribe on doctors and how we care most about how to keep patients in their rightful, subordinate place.” The “Rebel” title is provocative and implies patients need to overthrow the status quo. Well, I am part of the establishment. I stopped reading. This book doesn’t apply to me, I thought.
After all, I’m a healthcare progressive, right? My notes and results have been open for years. I encourage shared decision-making and try to empower patients as much as treat them. The idea that I or my colleagues are unwilling to do whatever is necessary to meet our patients’ needs was maddening. We dedicate our lives to it. My young daughter often greets me in the morning by asking if I’ll be working tonight. Most nights, I am — answering patient messages, collaborating with colleagues to help patients, keeping up with medical knowledge. I was angry at what felt like unjust criticism, especially that we’d neglect patients because their problems are not obvious or worse, there is not enough money to be made helping them. Harrumph.
That’s when I realized the best thing for me was to read the entire book and digest the arguments. I pride myself on being well-read, but I fall into a common trap: the podcasts I listen to, news I consume, and books I read mostly affirm my beliefs. It is a healthy choice to seek dispositive data and contrasting stories rather than always feeding our personal opinions.
Rebel Health was not written by Robespierre. It was penned by a thoughtful, articulate patient advocate with over 20 years experience. She has far more bona fides than I could achieve in two lifetimes. In the book, she reminds us that She describes four patient archetypes: seekers, networkers, solvers, and champions, and offers a four-quadrant model to visualize how some patients are unhelped by our current healthcare system. She advocates for frictionless, open access to health data and tries to inspire patients to connect, innovate, and create to fill the voids that exist in healthcare. We have come a long way from the immured system of a decade ago; much of that is the result of patient advocates. But healthcare is still too costly, too fragmented and too many patients unhelped. “Community is a superpower,” she writes. I agree, we should assemble all the heroes in the universe for this challenge.
Fox also tells stories of patients who solved diagnostic dilemmas through their own research and advocacy. I thought of my own contrasting experiences of patients whose DIY care was based on misinformation and how their false confidence led to poorer outcomes for them. I want to share with her readers how physicians feel hurt when patients question our competence or place the opinion of an adversarial Redditor over ours. Physicians are sometimes wrong and often in doubt. Most of us care deeply about our patients regardless of how visible their diagnosis or how easy they are to appease.
We don’t have time to engage back-and-forth on an insignificantly abnormal test they find in their open chart or why B12 and hormone testing would not be helpful for their disease. It’s also not the patients’ fault. Having unfettered access to their data might add work, but it also adds value. They are trying to learn and be active in their care. Physicians are frustrated mostly because we don’t have time to meet these unmet needs. Everyone is trying their best and we all want the same thing: patients to be satisfied and well.
As for learning the skill of being open-minded, an excellent reference is Adam Grant’s Think Again. It’s inspiring and instructive of how we can all be more open, including how to have productive arguments rather than fruitless fights. We live in divisive times. Perhaps if we all put in effort to be open-minded, push down righteous indignation, and advance more honest humility we’d all be a bit better off.
Patients are the primary audience for the Rebel Health book. Yet, as we care about them and we all want to make healthcare better, it is worth reading in its entirety. I told my daughter I don’t have to work tonight because I’ve written my article this month. When she’s a little older, I’ll tell her all about it. To be successful, she’ll have to be as open-minded as she is smart. She can learn both.
I have no conflict of interest in the book.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Each month I set out on an expedition to find a topic for this column. I came across a new book Rebel Health by Susannah Fox that I thought might be a good one. It’s both a treatise on the shortcomings of healthcare and a Baedeker for patients on how to find their way to being better served. Her argument is that many patients’ needs are unmet and their conditions are often invisible to us in mainstream healthcare. We fail to find solutions to help them. Patients would benefit from more open access to their records and more resources to take control of their own health, she argues. A few chapters in, I thought, “Oh, here we go, another diatribe on doctors and how we care most about how to keep patients in their rightful, subordinate place.” The “Rebel” title is provocative and implies patients need to overthrow the status quo. Well, I am part of the establishment. I stopped reading. This book doesn’t apply to me, I thought.
After all, I’m a healthcare progressive, right? My notes and results have been open for years. I encourage shared decision-making and try to empower patients as much as treat them. The idea that I or my colleagues are unwilling to do whatever is necessary to meet our patients’ needs was maddening. We dedicate our lives to it. My young daughter often greets me in the morning by asking if I’ll be working tonight. Most nights, I am — answering patient messages, collaborating with colleagues to help patients, keeping up with medical knowledge. I was angry at what felt like unjust criticism, especially that we’d neglect patients because their problems are not obvious or worse, there is not enough money to be made helping them. Harrumph.
That’s when I realized the best thing for me was to read the entire book and digest the arguments. I pride myself on being well-read, but I fall into a common trap: the podcasts I listen to, news I consume, and books I read mostly affirm my beliefs. It is a healthy choice to seek dispositive data and contrasting stories rather than always feeding our personal opinions.
Rebel Health was not written by Robespierre. It was penned by a thoughtful, articulate patient advocate with over 20 years experience. She has far more bona fides than I could achieve in two lifetimes. In the book, she reminds us that She describes four patient archetypes: seekers, networkers, solvers, and champions, and offers a four-quadrant model to visualize how some patients are unhelped by our current healthcare system. She advocates for frictionless, open access to health data and tries to inspire patients to connect, innovate, and create to fill the voids that exist in healthcare. We have come a long way from the immured system of a decade ago; much of that is the result of patient advocates. But healthcare is still too costly, too fragmented and too many patients unhelped. “Community is a superpower,” she writes. I agree, we should assemble all the heroes in the universe for this challenge.
Fox also tells stories of patients who solved diagnostic dilemmas through their own research and advocacy. I thought of my own contrasting experiences of patients whose DIY care was based on misinformation and how their false confidence led to poorer outcomes for them. I want to share with her readers how physicians feel hurt when patients question our competence or place the opinion of an adversarial Redditor over ours. Physicians are sometimes wrong and often in doubt. Most of us care deeply about our patients regardless of how visible their diagnosis or how easy they are to appease.
We don’t have time to engage back-and-forth on an insignificantly abnormal test they find in their open chart or why B12 and hormone testing would not be helpful for their disease. It’s also not the patients’ fault. Having unfettered access to their data might add work, but it also adds value. They are trying to learn and be active in their care. Physicians are frustrated mostly because we don’t have time to meet these unmet needs. Everyone is trying their best and we all want the same thing: patients to be satisfied and well.
As for learning the skill of being open-minded, an excellent reference is Adam Grant’s Think Again. It’s inspiring and instructive of how we can all be more open, including how to have productive arguments rather than fruitless fights. We live in divisive times. Perhaps if we all put in effort to be open-minded, push down righteous indignation, and advance more honest humility we’d all be a bit better off.
Patients are the primary audience for the Rebel Health book. Yet, as we care about them and we all want to make healthcare better, it is worth reading in its entirety. I told my daughter I don’t have to work tonight because I’ve written my article this month. When she’s a little older, I’ll tell her all about it. To be successful, she’ll have to be as open-minded as she is smart. She can learn both.
I have no conflict of interest in the book.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Each month I set out on an expedition to find a topic for this column. I came across a new book Rebel Health by Susannah Fox that I thought might be a good one. It’s both a treatise on the shortcomings of healthcare and a Baedeker for patients on how to find their way to being better served. Her argument is that many patients’ needs are unmet and their conditions are often invisible to us in mainstream healthcare. We fail to find solutions to help them. Patients would benefit from more open access to their records and more resources to take control of their own health, she argues. A few chapters in, I thought, “Oh, here we go, another diatribe on doctors and how we care most about how to keep patients in their rightful, subordinate place.” The “Rebel” title is provocative and implies patients need to overthrow the status quo. Well, I am part of the establishment. I stopped reading. This book doesn’t apply to me, I thought.
After all, I’m a healthcare progressive, right? My notes and results have been open for years. I encourage shared decision-making and try to empower patients as much as treat them. The idea that I or my colleagues are unwilling to do whatever is necessary to meet our patients’ needs was maddening. We dedicate our lives to it. My young daughter often greets me in the morning by asking if I’ll be working tonight. Most nights, I am — answering patient messages, collaborating with colleagues to help patients, keeping up with medical knowledge. I was angry at what felt like unjust criticism, especially that we’d neglect patients because their problems are not obvious or worse, there is not enough money to be made helping them. Harrumph.
That’s when I realized the best thing for me was to read the entire book and digest the arguments. I pride myself on being well-read, but I fall into a common trap: the podcasts I listen to, news I consume, and books I read mostly affirm my beliefs. It is a healthy choice to seek dispositive data and contrasting stories rather than always feeding our personal opinions.
Rebel Health was not written by Robespierre. It was penned by a thoughtful, articulate patient advocate with over 20 years experience. She has far more bona fides than I could achieve in two lifetimes. In the book, she reminds us that She describes four patient archetypes: seekers, networkers, solvers, and champions, and offers a four-quadrant model to visualize how some patients are unhelped by our current healthcare system. She advocates for frictionless, open access to health data and tries to inspire patients to connect, innovate, and create to fill the voids that exist in healthcare. We have come a long way from the immured system of a decade ago; much of that is the result of patient advocates. But healthcare is still too costly, too fragmented and too many patients unhelped. “Community is a superpower,” she writes. I agree, we should assemble all the heroes in the universe for this challenge.
Fox also tells stories of patients who solved diagnostic dilemmas through their own research and advocacy. I thought of my own contrasting experiences of patients whose DIY care was based on misinformation and how their false confidence led to poorer outcomes for them. I want to share with her readers how physicians feel hurt when patients question our competence or place the opinion of an adversarial Redditor over ours. Physicians are sometimes wrong and often in doubt. Most of us care deeply about our patients regardless of how visible their diagnosis or how easy they are to appease.
We don’t have time to engage back-and-forth on an insignificantly abnormal test they find in their open chart or why B12 and hormone testing would not be helpful for their disease. It’s also not the patients’ fault. Having unfettered access to their data might add work, but it also adds value. They are trying to learn and be active in their care. Physicians are frustrated mostly because we don’t have time to meet these unmet needs. Everyone is trying their best and we all want the same thing: patients to be satisfied and well.
As for learning the skill of being open-minded, an excellent reference is Adam Grant’s Think Again. It’s inspiring and instructive of how we can all be more open, including how to have productive arguments rather than fruitless fights. We live in divisive times. Perhaps if we all put in effort to be open-minded, push down righteous indignation, and advance more honest humility we’d all be a bit better off.
Patients are the primary audience for the Rebel Health book. Yet, as we care about them and we all want to make healthcare better, it is worth reading in its entirety. I told my daughter I don’t have to work tonight because I’ve written my article this month. When she’s a little older, I’ll tell her all about it. To be successful, she’ll have to be as open-minded as she is smart. She can learn both.
I have no conflict of interest in the book.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.