User login
US Experience With Infliximab Biosimilars Suggests Need for More Development Incentives
TOPLINE:
Uptake of infliximab biosimilars rose slowly across private insurance, Medicaid, and Medicare when two were available in the United States during 2016-2020 but increased significantly through 2022 after the third biosimilar became available in July 2020. However, prescriptions in Medicare still lagged behind those in private insurance and Medicaid.
METHODOLOGY:
- Researchers analyzed electronic health records from over 1100 US rheumatologists who participated in a national registry, the Rheumatology Informatics System for Effectiveness (RISE), for all infliximab administrations (bio-originator or biosimilar) to patients older than 18 years from April 2016 to September 2022.
- They conducted an interrupted time series to account for autocorrelation and model the effect of each infliximab biosimilar release (infliximab-dyyb in November 2016, infliximab-abda in July 2017, and infliximab-axxq in July 2020) on uptake across Medicare, Medicaid, and private insurers.
TAKEAWAY:
- The researchers identified 659,988 infliximab administrations for 37,560 unique patients, with 52% on Medicare, 4.8% on Medicaid, and 43% on private insurance.
- Biosimilar uptake rose slowly with average annual increases < 5% from 2016 to June 2020 (Medicare, 3.2%; Medicaid, 5.2%; private insurance, 1.8%).
- After the third biosimilar release in July 2020, the average annual increase reached 13% for Medicaid and 16.4% for private insurance but remained low for Medicare (5.6%).
- By September 2022, biosimilar uptake was higher for Medicaid (43.8%) and private insurance (38.5%) than for Medicare (24%).
IN PRACTICE:
“Our results suggest policymakers may need to do more to allow biosimilars to get a foothold in the market by incentivizing the development and entry of multiple biosimilars, address anticompetitive pricing strategies, and may need to amend Medicare policy to [incentivize] uptake in order to ensure a competitive and sustainable biosimilar market that gradually reduces total drug expenditures and out-of-pocket costs over time,” wrote the authors of the study.
SOURCE:
The study was led by Eric T. Roberts, PhD, University of California, San Francisco. It was published online on July 30, 2024, in Arthritis & Rheumatology.
LIMITATIONS:
First, while the biosimilar introductions are likely catalysts for many changes in the market, some changes in slopes may also be attributable to the natural growth of the market over time. Second, this study may neither be generalizable to academic medical centers, which are underrepresented in RISE, nor be generalizable to infliximab prescriptions from other specialties. Third, uptake among privately insured patients changed shortly after November-December 2020, raising the possibility that the delay reflected negotiations between insurance companies and relevant entities regarding formulary coverage.
DISCLOSURES:
This study was funded by grants from the Agency for Healthcare Research and Quality and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. One author disclosed receiving consulting fees from Pfizer, AstraZeneca, and Bristol-Myers Squibb and grant funding from AstraZeneca, the Bristol-Myers Squibb Foundation, and Aurinia.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Uptake of infliximab biosimilars rose slowly across private insurance, Medicaid, and Medicare when two were available in the United States during 2016-2020 but increased significantly through 2022 after the third biosimilar became available in July 2020. However, prescriptions in Medicare still lagged behind those in private insurance and Medicaid.
METHODOLOGY:
- Researchers analyzed electronic health records from over 1100 US rheumatologists who participated in a national registry, the Rheumatology Informatics System for Effectiveness (RISE), for all infliximab administrations (bio-originator or biosimilar) to patients older than 18 years from April 2016 to September 2022.
- They conducted an interrupted time series to account for autocorrelation and model the effect of each infliximab biosimilar release (infliximab-dyyb in November 2016, infliximab-abda in July 2017, and infliximab-axxq in July 2020) on uptake across Medicare, Medicaid, and private insurers.
TAKEAWAY:
- The researchers identified 659,988 infliximab administrations for 37,560 unique patients, with 52% on Medicare, 4.8% on Medicaid, and 43% on private insurance.
- Biosimilar uptake rose slowly with average annual increases < 5% from 2016 to June 2020 (Medicare, 3.2%; Medicaid, 5.2%; private insurance, 1.8%).
- After the third biosimilar release in July 2020, the average annual increase reached 13% for Medicaid and 16.4% for private insurance but remained low for Medicare (5.6%).
- By September 2022, biosimilar uptake was higher for Medicaid (43.8%) and private insurance (38.5%) than for Medicare (24%).
IN PRACTICE:
“Our results suggest policymakers may need to do more to allow biosimilars to get a foothold in the market by incentivizing the development and entry of multiple biosimilars, address anticompetitive pricing strategies, and may need to amend Medicare policy to [incentivize] uptake in order to ensure a competitive and sustainable biosimilar market that gradually reduces total drug expenditures and out-of-pocket costs over time,” wrote the authors of the study.
SOURCE:
The study was led by Eric T. Roberts, PhD, University of California, San Francisco. It was published online on July 30, 2024, in Arthritis & Rheumatology.
LIMITATIONS:
First, while the biosimilar introductions are likely catalysts for many changes in the market, some changes in slopes may also be attributable to the natural growth of the market over time. Second, this study may neither be generalizable to academic medical centers, which are underrepresented in RISE, nor be generalizable to infliximab prescriptions from other specialties. Third, uptake among privately insured patients changed shortly after November-December 2020, raising the possibility that the delay reflected negotiations between insurance companies and relevant entities regarding formulary coverage.
DISCLOSURES:
This study was funded by grants from the Agency for Healthcare Research and Quality and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. One author disclosed receiving consulting fees from Pfizer, AstraZeneca, and Bristol-Myers Squibb and grant funding from AstraZeneca, the Bristol-Myers Squibb Foundation, and Aurinia.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Uptake of infliximab biosimilars rose slowly across private insurance, Medicaid, and Medicare when two were available in the United States during 2016-2020 but increased significantly through 2022 after the third biosimilar became available in July 2020. However, prescriptions in Medicare still lagged behind those in private insurance and Medicaid.
METHODOLOGY:
- Researchers analyzed electronic health records from over 1100 US rheumatologists who participated in a national registry, the Rheumatology Informatics System for Effectiveness (RISE), for all infliximab administrations (bio-originator or biosimilar) to patients older than 18 years from April 2016 to September 2022.
- They conducted an interrupted time series to account for autocorrelation and model the effect of each infliximab biosimilar release (infliximab-dyyb in November 2016, infliximab-abda in July 2017, and infliximab-axxq in July 2020) on uptake across Medicare, Medicaid, and private insurers.
TAKEAWAY:
- The researchers identified 659,988 infliximab administrations for 37,560 unique patients, with 52% on Medicare, 4.8% on Medicaid, and 43% on private insurance.
- Biosimilar uptake rose slowly with average annual increases < 5% from 2016 to June 2020 (Medicare, 3.2%; Medicaid, 5.2%; private insurance, 1.8%).
- After the third biosimilar release in July 2020, the average annual increase reached 13% for Medicaid and 16.4% for private insurance but remained low for Medicare (5.6%).
- By September 2022, biosimilar uptake was higher for Medicaid (43.8%) and private insurance (38.5%) than for Medicare (24%).
IN PRACTICE:
“Our results suggest policymakers may need to do more to allow biosimilars to get a foothold in the market by incentivizing the development and entry of multiple biosimilars, address anticompetitive pricing strategies, and may need to amend Medicare policy to [incentivize] uptake in order to ensure a competitive and sustainable biosimilar market that gradually reduces total drug expenditures and out-of-pocket costs over time,” wrote the authors of the study.
SOURCE:
The study was led by Eric T. Roberts, PhD, University of California, San Francisco. It was published online on July 30, 2024, in Arthritis & Rheumatology.
LIMITATIONS:
First, while the biosimilar introductions are likely catalysts for many changes in the market, some changes in slopes may also be attributable to the natural growth of the market over time. Second, this study may neither be generalizable to academic medical centers, which are underrepresented in RISE, nor be generalizable to infliximab prescriptions from other specialties. Third, uptake among privately insured patients changed shortly after November-December 2020, raising the possibility that the delay reflected negotiations between insurance companies and relevant entities regarding formulary coverage.
DISCLOSURES:
This study was funded by grants from the Agency for Healthcare Research and Quality and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. One author disclosed receiving consulting fees from Pfizer, AstraZeneca, and Bristol-Myers Squibb and grant funding from AstraZeneca, the Bristol-Myers Squibb Foundation, and Aurinia.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Trends in Rheumatic Disease Pain Management Show Decline in Opioid Use
TOPLINE:
Since 2014, opioid use for autoimmune rheumatic decreased by 15% annually while other management modalities increased or stabilized.
METHODOLOGY:
- Researchers analyzed de-identified US claims data from the MarketScan Database from 2007-2021.
- The study included nearly 142,000 patients with autoimmune rheumatic diseases: 10,927 with ankylosing spondylitis (AS); 21,438 with psoriatic arthritis (PsA); 71,393 with rheumatoid arthritis (RA); 16,718 with Sjögren disease; 18,018 with systemic lupus erythematosus; and 3468 with systemic sclerosis.
- Primary outcome was opioid use annual trends, with secondary outcomes including trends in the use of anticonvulsants, antidepressants, skeletal muscle relaxants, nonsteroidal anti-inflammatory drugs (NSAIDs), topical pain medications, and physical or occupational therapy.
TAKEAWAY:
- The incidence of opioid use increased annually by 4% until 2014 and decreased annually by 15% after 2014.
- NSAID use increased 2% annually until 2014, then declined by 5% afterward.
- The proportion of patients utilizing physical therapy or anticonvulsants doubled from 2008 to 2020.
- NSAID prescriptions were highest in AS, PsA, and RA, while they were lowest in Sjögren disease and systemic sclerosis.
IN PRACTICE:
“Our work, along with the published literature, highlights the need for future studies to evaluate the effectiveness of pain management modality changes over time and to understand the possible effects that changes have had on outcomes such as quality of life, disability, health status, and function,” wrote the authors of the study.
SOURCE:
The study was led by Titilola Falasinnu, PhD, Stanford University School of Medicine, Stanford, California. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study relied on administrative claims data, which did not contain information on use of over-the-counter medications like NSAIDs and topical analgesics. The study did not include the duration of pain treatment modalities, making it difficult to differentiate between acute and chronic use. The analysis did not include race or ethnicity, which is important for understanding pain outcomes across different sociodemographic groups.
DISCLOSURES:
The study was supported by grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Since 2014, opioid use for autoimmune rheumatic decreased by 15% annually while other management modalities increased or stabilized.
METHODOLOGY:
- Researchers analyzed de-identified US claims data from the MarketScan Database from 2007-2021.
- The study included nearly 142,000 patients with autoimmune rheumatic diseases: 10,927 with ankylosing spondylitis (AS); 21,438 with psoriatic arthritis (PsA); 71,393 with rheumatoid arthritis (RA); 16,718 with Sjögren disease; 18,018 with systemic lupus erythematosus; and 3468 with systemic sclerosis.
- Primary outcome was opioid use annual trends, with secondary outcomes including trends in the use of anticonvulsants, antidepressants, skeletal muscle relaxants, nonsteroidal anti-inflammatory drugs (NSAIDs), topical pain medications, and physical or occupational therapy.
TAKEAWAY:
- The incidence of opioid use increased annually by 4% until 2014 and decreased annually by 15% after 2014.
- NSAID use increased 2% annually until 2014, then declined by 5% afterward.
- The proportion of patients utilizing physical therapy or anticonvulsants doubled from 2008 to 2020.
- NSAID prescriptions were highest in AS, PsA, and RA, while they were lowest in Sjögren disease and systemic sclerosis.
IN PRACTICE:
“Our work, along with the published literature, highlights the need for future studies to evaluate the effectiveness of pain management modality changes over time and to understand the possible effects that changes have had on outcomes such as quality of life, disability, health status, and function,” wrote the authors of the study.
SOURCE:
The study was led by Titilola Falasinnu, PhD, Stanford University School of Medicine, Stanford, California. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study relied on administrative claims data, which did not contain information on use of over-the-counter medications like NSAIDs and topical analgesics. The study did not include the duration of pain treatment modalities, making it difficult to differentiate between acute and chronic use. The analysis did not include race or ethnicity, which is important for understanding pain outcomes across different sociodemographic groups.
DISCLOSURES:
The study was supported by grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Since 2014, opioid use for autoimmune rheumatic decreased by 15% annually while other management modalities increased or stabilized.
METHODOLOGY:
- Researchers analyzed de-identified US claims data from the MarketScan Database from 2007-2021.
- The study included nearly 142,000 patients with autoimmune rheumatic diseases: 10,927 with ankylosing spondylitis (AS); 21,438 with psoriatic arthritis (PsA); 71,393 with rheumatoid arthritis (RA); 16,718 with Sjögren disease; 18,018 with systemic lupus erythematosus; and 3468 with systemic sclerosis.
- Primary outcome was opioid use annual trends, with secondary outcomes including trends in the use of anticonvulsants, antidepressants, skeletal muscle relaxants, nonsteroidal anti-inflammatory drugs (NSAIDs), topical pain medications, and physical or occupational therapy.
TAKEAWAY:
- The incidence of opioid use increased annually by 4% until 2014 and decreased annually by 15% after 2014.
- NSAID use increased 2% annually until 2014, then declined by 5% afterward.
- The proportion of patients utilizing physical therapy or anticonvulsants doubled from 2008 to 2020.
- NSAID prescriptions were highest in AS, PsA, and RA, while they were lowest in Sjögren disease and systemic sclerosis.
IN PRACTICE:
“Our work, along with the published literature, highlights the need for future studies to evaluate the effectiveness of pain management modality changes over time and to understand the possible effects that changes have had on outcomes such as quality of life, disability, health status, and function,” wrote the authors of the study.
SOURCE:
The study was led by Titilola Falasinnu, PhD, Stanford University School of Medicine, Stanford, California. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study relied on administrative claims data, which did not contain information on use of over-the-counter medications like NSAIDs and topical analgesics. The study did not include the duration of pain treatment modalities, making it difficult to differentiate between acute and chronic use. The analysis did not include race or ethnicity, which is important for understanding pain outcomes across different sociodemographic groups.
DISCLOSURES:
The study was supported by grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Financial Hardship Common With Rheumatologic Disease: How Can Doctors Help?
Many patients struggle with healthcare costs and basic expenses, according to new research.
People with rheumatologic diseases often experience a hidden symptom: financial toxicity or significant economic strain from out-of-pocket costs. A new study of 41,502 patients published in JCR: Journal of Clinical Rheumatology showed that 20% of those with rheumatologic diseases faced financial hardship from medical expenses, with 55% of those unable to pay their bills.
Compared with patients who do not have rheumatologic diseases, and after clinical and sociodemographic factors were controlled for, patients with rheumatologic diseases were:
- 29% more likely to have high levels of financial hardship — difficulty paying; needing to pay over time; or inability to pay bills for doctors, dentists, hospitals, therapists, medication, equipment, nursing homes, or home care.
- 53% more likely to have high levels of financial distress — significant worry about having enough money for retirement, paying medical costs in the event of a serious illness or accident, maintaining their standard of living, paying their usual healthcare costs, and affording their normal monthly bills and housing costs.
- 29% more likely to experience food insecurity, defined as limited or uncertain access to adequate food.
- 58% more likely to report cost-related medication nonadherence — skipping doses, taking less medication, or delaying filling a prescription to save money.
People who were younger than 64 years, male, Black, or uninsured had higher odds of experiencing financial hardship, financial distress, food insecurity, and cost-related medication nonadherence.
This study highlights “just how costly everyday rheumatologic conditions can be for your average American,” said lead study author Troy Amen, MD, MBA, an orthopedic surgery resident at the Hospital for Special Surgery in New York City. These diseases can be disabling, limiting a patient’s ability to work at the very time when expensive medications are needed.
“It’s critical for clinicians to recognize how common the financial burden from healthcare costs can be, and only then can they take steps to better support patients,” said G. Caleb Alexander, MD, MS, professor of epidemiology at Johns Hopkins University in Baltimore, who was not involved in the study.
Here’s how healthcare providers can help.
Consider skipped medication a red flag. It’s often the first sign of a financial concern. “Sometimes with these problems, it looks like simple medication noncompliance, but it’s really a more complex form of nonadherence,” said Susan M. Goodman, MD, professor of clinical medicine at Weill Cornell Medicine in New York City and a coauthor of the study. “And I think if someone’s not taking the medication that had been very helpful, it does behoove the physician to try and figure out why that is.”
Normalize the issue to help patients open up. “I will often say, ‘You know, many, many patients don’t take their medicines exactly as prescribed. About how many days a week do you take this medicine?’” said Dr. Alexander. “If you ask in a nonconfrontational, supportive manner, I’ve found that patients are quite candid.”
Don’t assume insurance has it covered. If patients are uninsured, help them enroll in (or renew) insurance coverage. But don’t assume insurance will solve the whole problem. “There are many people who, although they do have coverage, still can’t afford their medications,” said Dr. Goodman.
For products on high formulary tiers, the patient’s monthly cost can be hundreds to thousands of dollars. “Over the past 10-20 years, we’ve seen remarkable technological innovation in the types of medicines being brought to market, and here, I’m referring primarily to biologics and medicines made from living cells,” said Dr. Alexander, “but many of these have a price tag that is simply astronomical, and insurers aren’t going to bear the brunt of these costs alone.”
Biosimilars can be a bit more affordable, but “the dirty little secret of biosimilars is that they’re not really very much less expensive,” said Dr. Goodman. “If your patient is doing well on a drug that gets dropped from their insurance plan’s formulary, or if they switch to a plan that doesn’t cover it, try calling and advocating for an exception. It’s an uphill battle, but it sometimes works,” she said.
If not? Help your patients apply for a patient assistance program. Many drug manufacturers offer copay assistance through their websites, and nonprofit patient assistance organizations such as the PAN Foundation, the Patient Advocate Foundation’s Co-Pay Relief Program, or The Assistance Fund can also help fill the gaps. One study published in the Journal of Managed Care and Specialty Pharmacy showed that in patients with rheumatoid arthritis, copay assistance was associated with 79% lower odds of prescription abandonment (failure to fill within 30 days of health plan approval).
Beware of “shiny penny syndrome.” It’s easy to get excited about new, innovative medications, especially when sales reps provide plenty of free samples. “There is a tendency to treat every new medicine as if it’s a bright shiny object in the streambed, and you know that’s not always the case,” said Dr. Alexander. “So, I think we have to be careful, especially in settings when we’re talking about ultra–high-cost medicines, that we’re aware of the burden these medicines may place on patients and that we’re navigating that with patients together, and not simply leaving that as a conversation that never happens in the exam room.”
Maybe there’s an older, time-tested drug that works just as well as the newer, more expensive one. Perhaps there is a slightly less effective medicine that costs a lot less. “These are cost–quality trade-offs that clinicians and patients should be navigating together,” said Dr. Alexander. For example, in a patient with rheumatoid arthritis, a tumor necrosis factor alpha inhibitor might work similarly to or almost as well as an interleukin inhibitor, the newer and typically more expensive choice.
“Some clinicians may find it quite unpalatable to be potentially compromising on safety or efficacy in the interest of reducing the cost of therapies, but as former Surgeon General C. Everett Koop said, ‘Drugs don’t work in patients who don’t take them,’ ” said Dr. Alexander. “So, if the choice is for someone not to be taking a treatment, or to be taking one that may be a little bit less good, I’ll take the latter.”
Consider the patient’s broader care team. Encourage patients to discuss costs with their other healthcare providers. For patients taking multiple medications, a few adjustments could make a big impact on their wallets. Primary care providers or other specialists might recommend some older and less expensive, but still effective, drugs, such as thiazides for hypertension or metformin for type 2 diabetes. Another option might be to simplify the patient’s regimen or include some fixed-dose combination pills in place of two others.
And if no one has referred the patient to a medical social worker, make the connection. A social worker can put patients in touch with local agencies that can help them with food, housing, and other nonmedical costs.
Talk about this problem with anyone who will listen. One of the best ways to help patients with rheumatologic diseases is to ensure that decision-makers don’t overlook them. Professional societies such as the American College of Rheumatology can be great resources for advocacy in Washington, DC. Political movements can make drugs more affordable — for example, insulin prices have dropped in recent years because of political pressure, said Dr. Goodman.
“A lot of our national policy now focuses on aiding patients with single high-cost events, but we hope studies like these can really get policymakers to think through how to better support patients with chronic conditions that may have been historically ignored, such as patients with rheumatologic disease,” said Dr. Amen.
The first step is raising awareness and telling your story. “As providers, we are often [at the] forefront in witnessing how chronic conditions and their associated costs can negatively affect patients’ lives and even alter clinical outcomes,” Dr. Amen added. “By publishing data and sharing meaningful patient stories and clinical vignettes, we can begin to advocate and humanize these patients to policymakers.”
Information on study funding was not available. All authors reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Many patients struggle with healthcare costs and basic expenses, according to new research.
People with rheumatologic diseases often experience a hidden symptom: financial toxicity or significant economic strain from out-of-pocket costs. A new study of 41,502 patients published in JCR: Journal of Clinical Rheumatology showed that 20% of those with rheumatologic diseases faced financial hardship from medical expenses, with 55% of those unable to pay their bills.
Compared with patients who do not have rheumatologic diseases, and after clinical and sociodemographic factors were controlled for, patients with rheumatologic diseases were:
- 29% more likely to have high levels of financial hardship — difficulty paying; needing to pay over time; or inability to pay bills for doctors, dentists, hospitals, therapists, medication, equipment, nursing homes, or home care.
- 53% more likely to have high levels of financial distress — significant worry about having enough money for retirement, paying medical costs in the event of a serious illness or accident, maintaining their standard of living, paying their usual healthcare costs, and affording their normal monthly bills and housing costs.
- 29% more likely to experience food insecurity, defined as limited or uncertain access to adequate food.
- 58% more likely to report cost-related medication nonadherence — skipping doses, taking less medication, or delaying filling a prescription to save money.
People who were younger than 64 years, male, Black, or uninsured had higher odds of experiencing financial hardship, financial distress, food insecurity, and cost-related medication nonadherence.
This study highlights “just how costly everyday rheumatologic conditions can be for your average American,” said lead study author Troy Amen, MD, MBA, an orthopedic surgery resident at the Hospital for Special Surgery in New York City. These diseases can be disabling, limiting a patient’s ability to work at the very time when expensive medications are needed.
“It’s critical for clinicians to recognize how common the financial burden from healthcare costs can be, and only then can they take steps to better support patients,” said G. Caleb Alexander, MD, MS, professor of epidemiology at Johns Hopkins University in Baltimore, who was not involved in the study.
Here’s how healthcare providers can help.
Consider skipped medication a red flag. It’s often the first sign of a financial concern. “Sometimes with these problems, it looks like simple medication noncompliance, but it’s really a more complex form of nonadherence,” said Susan M. Goodman, MD, professor of clinical medicine at Weill Cornell Medicine in New York City and a coauthor of the study. “And I think if someone’s not taking the medication that had been very helpful, it does behoove the physician to try and figure out why that is.”
Normalize the issue to help patients open up. “I will often say, ‘You know, many, many patients don’t take their medicines exactly as prescribed. About how many days a week do you take this medicine?’” said Dr. Alexander. “If you ask in a nonconfrontational, supportive manner, I’ve found that patients are quite candid.”
Don’t assume insurance has it covered. If patients are uninsured, help them enroll in (or renew) insurance coverage. But don’t assume insurance will solve the whole problem. “There are many people who, although they do have coverage, still can’t afford their medications,” said Dr. Goodman.
For products on high formulary tiers, the patient’s monthly cost can be hundreds to thousands of dollars. “Over the past 10-20 years, we’ve seen remarkable technological innovation in the types of medicines being brought to market, and here, I’m referring primarily to biologics and medicines made from living cells,” said Dr. Alexander, “but many of these have a price tag that is simply astronomical, and insurers aren’t going to bear the brunt of these costs alone.”
Biosimilars can be a bit more affordable, but “the dirty little secret of biosimilars is that they’re not really very much less expensive,” said Dr. Goodman. “If your patient is doing well on a drug that gets dropped from their insurance plan’s formulary, or if they switch to a plan that doesn’t cover it, try calling and advocating for an exception. It’s an uphill battle, but it sometimes works,” she said.
If not? Help your patients apply for a patient assistance program. Many drug manufacturers offer copay assistance through their websites, and nonprofit patient assistance organizations such as the PAN Foundation, the Patient Advocate Foundation’s Co-Pay Relief Program, or The Assistance Fund can also help fill the gaps. One study published in the Journal of Managed Care and Specialty Pharmacy showed that in patients with rheumatoid arthritis, copay assistance was associated with 79% lower odds of prescription abandonment (failure to fill within 30 days of health plan approval).
Beware of “shiny penny syndrome.” It’s easy to get excited about new, innovative medications, especially when sales reps provide plenty of free samples. “There is a tendency to treat every new medicine as if it’s a bright shiny object in the streambed, and you know that’s not always the case,” said Dr. Alexander. “So, I think we have to be careful, especially in settings when we’re talking about ultra–high-cost medicines, that we’re aware of the burden these medicines may place on patients and that we’re navigating that with patients together, and not simply leaving that as a conversation that never happens in the exam room.”
Maybe there’s an older, time-tested drug that works just as well as the newer, more expensive one. Perhaps there is a slightly less effective medicine that costs a lot less. “These are cost–quality trade-offs that clinicians and patients should be navigating together,” said Dr. Alexander. For example, in a patient with rheumatoid arthritis, a tumor necrosis factor alpha inhibitor might work similarly to or almost as well as an interleukin inhibitor, the newer and typically more expensive choice.
“Some clinicians may find it quite unpalatable to be potentially compromising on safety or efficacy in the interest of reducing the cost of therapies, but as former Surgeon General C. Everett Koop said, ‘Drugs don’t work in patients who don’t take them,’ ” said Dr. Alexander. “So, if the choice is for someone not to be taking a treatment, or to be taking one that may be a little bit less good, I’ll take the latter.”
Consider the patient’s broader care team. Encourage patients to discuss costs with their other healthcare providers. For patients taking multiple medications, a few adjustments could make a big impact on their wallets. Primary care providers or other specialists might recommend some older and less expensive, but still effective, drugs, such as thiazides for hypertension or metformin for type 2 diabetes. Another option might be to simplify the patient’s regimen or include some fixed-dose combination pills in place of two others.
And if no one has referred the patient to a medical social worker, make the connection. A social worker can put patients in touch with local agencies that can help them with food, housing, and other nonmedical costs.
Talk about this problem with anyone who will listen. One of the best ways to help patients with rheumatologic diseases is to ensure that decision-makers don’t overlook them. Professional societies such as the American College of Rheumatology can be great resources for advocacy in Washington, DC. Political movements can make drugs more affordable — for example, insulin prices have dropped in recent years because of political pressure, said Dr. Goodman.
“A lot of our national policy now focuses on aiding patients with single high-cost events, but we hope studies like these can really get policymakers to think through how to better support patients with chronic conditions that may have been historically ignored, such as patients with rheumatologic disease,” said Dr. Amen.
The first step is raising awareness and telling your story. “As providers, we are often [at the] forefront in witnessing how chronic conditions and their associated costs can negatively affect patients’ lives and even alter clinical outcomes,” Dr. Amen added. “By publishing data and sharing meaningful patient stories and clinical vignettes, we can begin to advocate and humanize these patients to policymakers.”
Information on study funding was not available. All authors reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Many patients struggle with healthcare costs and basic expenses, according to new research.
People with rheumatologic diseases often experience a hidden symptom: financial toxicity or significant economic strain from out-of-pocket costs. A new study of 41,502 patients published in JCR: Journal of Clinical Rheumatology showed that 20% of those with rheumatologic diseases faced financial hardship from medical expenses, with 55% of those unable to pay their bills.
Compared with patients who do not have rheumatologic diseases, and after clinical and sociodemographic factors were controlled for, patients with rheumatologic diseases were:
- 29% more likely to have high levels of financial hardship — difficulty paying; needing to pay over time; or inability to pay bills for doctors, dentists, hospitals, therapists, medication, equipment, nursing homes, or home care.
- 53% more likely to have high levels of financial distress — significant worry about having enough money for retirement, paying medical costs in the event of a serious illness or accident, maintaining their standard of living, paying their usual healthcare costs, and affording their normal monthly bills and housing costs.
- 29% more likely to experience food insecurity, defined as limited or uncertain access to adequate food.
- 58% more likely to report cost-related medication nonadherence — skipping doses, taking less medication, or delaying filling a prescription to save money.
People who were younger than 64 years, male, Black, or uninsured had higher odds of experiencing financial hardship, financial distress, food insecurity, and cost-related medication nonadherence.
This study highlights “just how costly everyday rheumatologic conditions can be for your average American,” said lead study author Troy Amen, MD, MBA, an orthopedic surgery resident at the Hospital for Special Surgery in New York City. These diseases can be disabling, limiting a patient’s ability to work at the very time when expensive medications are needed.
“It’s critical for clinicians to recognize how common the financial burden from healthcare costs can be, and only then can they take steps to better support patients,” said G. Caleb Alexander, MD, MS, professor of epidemiology at Johns Hopkins University in Baltimore, who was not involved in the study.
Here’s how healthcare providers can help.
Consider skipped medication a red flag. It’s often the first sign of a financial concern. “Sometimes with these problems, it looks like simple medication noncompliance, but it’s really a more complex form of nonadherence,” said Susan M. Goodman, MD, professor of clinical medicine at Weill Cornell Medicine in New York City and a coauthor of the study. “And I think if someone’s not taking the medication that had been very helpful, it does behoove the physician to try and figure out why that is.”
Normalize the issue to help patients open up. “I will often say, ‘You know, many, many patients don’t take their medicines exactly as prescribed. About how many days a week do you take this medicine?’” said Dr. Alexander. “If you ask in a nonconfrontational, supportive manner, I’ve found that patients are quite candid.”
Don’t assume insurance has it covered. If patients are uninsured, help them enroll in (or renew) insurance coverage. But don’t assume insurance will solve the whole problem. “There are many people who, although they do have coverage, still can’t afford their medications,” said Dr. Goodman.
For products on high formulary tiers, the patient’s monthly cost can be hundreds to thousands of dollars. “Over the past 10-20 years, we’ve seen remarkable technological innovation in the types of medicines being brought to market, and here, I’m referring primarily to biologics and medicines made from living cells,” said Dr. Alexander, “but many of these have a price tag that is simply astronomical, and insurers aren’t going to bear the brunt of these costs alone.”
Biosimilars can be a bit more affordable, but “the dirty little secret of biosimilars is that they’re not really very much less expensive,” said Dr. Goodman. “If your patient is doing well on a drug that gets dropped from their insurance plan’s formulary, or if they switch to a plan that doesn’t cover it, try calling and advocating for an exception. It’s an uphill battle, but it sometimes works,” she said.
If not? Help your patients apply for a patient assistance program. Many drug manufacturers offer copay assistance through their websites, and nonprofit patient assistance organizations such as the PAN Foundation, the Patient Advocate Foundation’s Co-Pay Relief Program, or The Assistance Fund can also help fill the gaps. One study published in the Journal of Managed Care and Specialty Pharmacy showed that in patients with rheumatoid arthritis, copay assistance was associated with 79% lower odds of prescription abandonment (failure to fill within 30 days of health plan approval).
Beware of “shiny penny syndrome.” It’s easy to get excited about new, innovative medications, especially when sales reps provide plenty of free samples. “There is a tendency to treat every new medicine as if it’s a bright shiny object in the streambed, and you know that’s not always the case,” said Dr. Alexander. “So, I think we have to be careful, especially in settings when we’re talking about ultra–high-cost medicines, that we’re aware of the burden these medicines may place on patients and that we’re navigating that with patients together, and not simply leaving that as a conversation that never happens in the exam room.”
Maybe there’s an older, time-tested drug that works just as well as the newer, more expensive one. Perhaps there is a slightly less effective medicine that costs a lot less. “These are cost–quality trade-offs that clinicians and patients should be navigating together,” said Dr. Alexander. For example, in a patient with rheumatoid arthritis, a tumor necrosis factor alpha inhibitor might work similarly to or almost as well as an interleukin inhibitor, the newer and typically more expensive choice.
“Some clinicians may find it quite unpalatable to be potentially compromising on safety or efficacy in the interest of reducing the cost of therapies, but as former Surgeon General C. Everett Koop said, ‘Drugs don’t work in patients who don’t take them,’ ” said Dr. Alexander. “So, if the choice is for someone not to be taking a treatment, or to be taking one that may be a little bit less good, I’ll take the latter.”
Consider the patient’s broader care team. Encourage patients to discuss costs with their other healthcare providers. For patients taking multiple medications, a few adjustments could make a big impact on their wallets. Primary care providers or other specialists might recommend some older and less expensive, but still effective, drugs, such as thiazides for hypertension or metformin for type 2 diabetes. Another option might be to simplify the patient’s regimen or include some fixed-dose combination pills in place of two others.
And if no one has referred the patient to a medical social worker, make the connection. A social worker can put patients in touch with local agencies that can help them with food, housing, and other nonmedical costs.
Talk about this problem with anyone who will listen. One of the best ways to help patients with rheumatologic diseases is to ensure that decision-makers don’t overlook them. Professional societies such as the American College of Rheumatology can be great resources for advocacy in Washington, DC. Political movements can make drugs more affordable — for example, insulin prices have dropped in recent years because of political pressure, said Dr. Goodman.
“A lot of our national policy now focuses on aiding patients with single high-cost events, but we hope studies like these can really get policymakers to think through how to better support patients with chronic conditions that may have been historically ignored, such as patients with rheumatologic disease,” said Dr. Amen.
The first step is raising awareness and telling your story. “As providers, we are often [at the] forefront in witnessing how chronic conditions and their associated costs can negatively affect patients’ lives and even alter clinical outcomes,” Dr. Amen added. “By publishing data and sharing meaningful patient stories and clinical vignettes, we can begin to advocate and humanize these patients to policymakers.”
Information on study funding was not available. All authors reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Functional Limitations in Axial Spondyloarthritis Benefit From Long-term Exercise Therapy
TOPLINE:
Long-term, supervised exercise therapy significantly improves the functional ability and quality of life in patients with axial spondyloarthritis (axSpA) and severe functional limitations.
METHODOLOGY:
- This 52-week study evaluated the effectiveness of personalized exercise therapy in adults with axSpA and severe functional limitations.
- Overall, 214 participants were randomly allocated to either a personalized exercise therapy regimen or usual care for 52 weeks.
- The supervised exercise therapy regimen consisted of various exercises, patient education, goal setting, and physical activity promotion for up to 64 sessions.
- The primary endpoint was a change in the highest-ranked Patient-Specific Complaints Numeric Rating Scale (PSC1) score at 52 weeks, and secondary endpoints included measures of physical functioning and quality of life.
TAKEAWAY:
- At 52 weeks, the exercise group showed a greater improvement in the primary outcome measure (PSC1) than the usual-care group, with a mean difference of −1.8 (95% CI, −2.4 to −1.2).
- Exercise therapy led to significant improvements in functional disability and physical quality of life.
- No serious adverse events related to the intervention were reported, highlighting the safety of exercise therapy.
IN PRACTICE:
“If guided by a trained physical therapist applying a personalized approach, people with severe functional limitations due to an unfavorable course or comorbidities can be just as responsive to training as people with axSpA without severe limitations,” the authors wrote.
SOURCE:
The study was led by Maria A.T. van Wissen, Department of Orthopaedics, Leiden University Medical Center, Leiden, the Netherlands, and published online in Rheumatology.
LIMITATIONS:
The study’s reliance on self-reported data for axSpA treatment-related medication may have compromised accuracy. Additionally, the lack of information on medication changes during the study period could affect result interpretation.
DISCLOSURES:
The study was supported by grants from the Netherlands Organization for Health Research and Development; Ministry of Health, Welfare and Sport; Royal Dutch Society for Physical Therapy; and Dutch Arthritis Society. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Long-term, supervised exercise therapy significantly improves the functional ability and quality of life in patients with axial spondyloarthritis (axSpA) and severe functional limitations.
METHODOLOGY:
- This 52-week study evaluated the effectiveness of personalized exercise therapy in adults with axSpA and severe functional limitations.
- Overall, 214 participants were randomly allocated to either a personalized exercise therapy regimen or usual care for 52 weeks.
- The supervised exercise therapy regimen consisted of various exercises, patient education, goal setting, and physical activity promotion for up to 64 sessions.
- The primary endpoint was a change in the highest-ranked Patient-Specific Complaints Numeric Rating Scale (PSC1) score at 52 weeks, and secondary endpoints included measures of physical functioning and quality of life.
TAKEAWAY:
- At 52 weeks, the exercise group showed a greater improvement in the primary outcome measure (PSC1) than the usual-care group, with a mean difference of −1.8 (95% CI, −2.4 to −1.2).
- Exercise therapy led to significant improvements in functional disability and physical quality of life.
- No serious adverse events related to the intervention were reported, highlighting the safety of exercise therapy.
IN PRACTICE:
“If guided by a trained physical therapist applying a personalized approach, people with severe functional limitations due to an unfavorable course or comorbidities can be just as responsive to training as people with axSpA without severe limitations,” the authors wrote.
SOURCE:
The study was led by Maria A.T. van Wissen, Department of Orthopaedics, Leiden University Medical Center, Leiden, the Netherlands, and published online in Rheumatology.
LIMITATIONS:
The study’s reliance on self-reported data for axSpA treatment-related medication may have compromised accuracy. Additionally, the lack of information on medication changes during the study period could affect result interpretation.
DISCLOSURES:
The study was supported by grants from the Netherlands Organization for Health Research and Development; Ministry of Health, Welfare and Sport; Royal Dutch Society for Physical Therapy; and Dutch Arthritis Society. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Long-term, supervised exercise therapy significantly improves the functional ability and quality of life in patients with axial spondyloarthritis (axSpA) and severe functional limitations.
METHODOLOGY:
- This 52-week study evaluated the effectiveness of personalized exercise therapy in adults with axSpA and severe functional limitations.
- Overall, 214 participants were randomly allocated to either a personalized exercise therapy regimen or usual care for 52 weeks.
- The supervised exercise therapy regimen consisted of various exercises, patient education, goal setting, and physical activity promotion for up to 64 sessions.
- The primary endpoint was a change in the highest-ranked Patient-Specific Complaints Numeric Rating Scale (PSC1) score at 52 weeks, and secondary endpoints included measures of physical functioning and quality of life.
TAKEAWAY:
- At 52 weeks, the exercise group showed a greater improvement in the primary outcome measure (PSC1) than the usual-care group, with a mean difference of −1.8 (95% CI, −2.4 to −1.2).
- Exercise therapy led to significant improvements in functional disability and physical quality of life.
- No serious adverse events related to the intervention were reported, highlighting the safety of exercise therapy.
IN PRACTICE:
“If guided by a trained physical therapist applying a personalized approach, people with severe functional limitations due to an unfavorable course or comorbidities can be just as responsive to training as people with axSpA without severe limitations,” the authors wrote.
SOURCE:
The study was led by Maria A.T. van Wissen, Department of Orthopaedics, Leiden University Medical Center, Leiden, the Netherlands, and published online in Rheumatology.
LIMITATIONS:
The study’s reliance on self-reported data for axSpA treatment-related medication may have compromised accuracy. Additionally, the lack of information on medication changes during the study period could affect result interpretation.
DISCLOSURES:
The study was supported by grants from the Netherlands Organization for Health Research and Development; Ministry of Health, Welfare and Sport; Royal Dutch Society for Physical Therapy; and Dutch Arthritis Society. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Debate Over Axial Involvement in Psoriatic Arthritis Still Unresolved Despite New Studies
VIENNA — While there is no doubt that some people with psoriatic arthritis (PsA) have axial symptoms, data presented at the annual European Congress of Rheumatology do not appear to add much to what is already known about axial PsA or to further the cause of differentiating it from axial spondyloarthritis (axSpA).
In both the AXIS study and Reuma.pt, around one in three patients with PsA were found to have axial involvement. Notably, the percentage of people with axial PsA was found to vary according to how imaging information was interpreted in the AXIS study. Both studies were discussed during the Axial Involvement in PsA and SpA session at EULAR 2024.
The One-Million-Dollar Question
“So, the one-million-dollar question: What is it, really?” Philippe Carron, MD, PhD, Ghent University Hospital, Ghent, Belgium, said in the presentation that started the session. Despite PsA being described more than 60 years ago, “we still have no internationally accepted definition or a consensus on how we should define these patients and how we should screen them,” he said.
“There are some believers that it is just a form of axial SpA with concomitant psoriasis, but also some people that think that the axial PsA is a typical disease, with typical characteristics which are different from axial disease,” Dr. Carron said.
The lack of consensus makes it difficult to estimate just how many people have axial PsA. Reported prevalences range from 5% to 70%, “all caused by which criteria that you’re using to define axial involvement,” Dr. Carron added.
There are, however, two things that can be agreed upon, according to Dr. Carron. First, the prevalence of axial involvement in people with early PsA is “much, much lower” than that of more established disease. Second, exclusive axial involvement is seen in “just a minority of PsA patients.” Most people with axial disease also have peripheral disease, he added.
Imaging findings in axial PsA “are quite similar to those seen in axial SpA,” although Dr. Carron also said that there were some distinct differences. Radiographic sacroiliitis occurs in around 25%-50% of people with axial PsA, and atypical syndesmophytes are more often found in people with axial PsA than in those with axSpA.
Shared Characteristics
But are axial PsA and axSpA separate diseases or part of the same disease continuum? That’s a question that is still very much open for debate, said Sofia Ramiro, MD, PhD, a senior researcher at Leiden University Medical Center, Leiden, the Netherlands, and rheumatology consultant at Zuyderland Medical Center in Heerlen, the Netherlands.
While many studies have looked to answer this question, there is a big methodological problem — the studies largely cannot be compared as they have used different definitions of axSpA.
Take a patient with inflammatory back pain, psoriasis, and oligoarthritis, Dr. Ramiro said. If the patient goes to one rheumatologist, they may get a diagnosis of axSpA, but if they go to a different rheumatologist, they may get a diagnosis of axial PsA.
“This is influenced by training, expertise, by beliefs, and by belonging to ASAS [Assessment of Spondyloarthritis International Society] or to GRAPPA [Group for Research and Assessment of Psoriasis and Psoriatic Arthritis],” Dr. Ramiro suggested. It’s “a diagnostic bias” that is very difficult to overcome and makes direct comparisons between patient populations recruited into clinical studies “extremely challenging.”
To confuse matters more, axial PsA and axSpA share common characteristics: Inflammatory back pain, HLA-B27 positivity, elevated levels of C-reactive protein (CRP) or a higher erythrocyte sedimentation rate, and structural lesions in the sacroiliac joints and spine.
AXIS Study ‘Gives Answers’
More research into factors associated with axial PsA need to be performed to try to help define the condition and enable classification and ultimately treatment guidelines. This is where the AXIS study comes in.
The AXIS study is a joint project of ASAS and GRAPPA that was started in January 2019 with the aim of defining a homogeneous subgroup of patients who could be studied.
“The objectives of the AXIS study are to determine the frequency of axial involvement in patients with PsA; to identify the frequency of active inflammatory and structural changes on imaging; and to identify factors associated with the presence of axial involvement in PsA,” Murat Torgutalp, MD, of Charité – Universitätsmedizin Berlin, Berlin, Germany, said at EULAR 2024.
The study population consisted of 409 consecutively recruited patients diagnosed with PsA according to CASPAR (Classification for Psoriatic Arthritis) criteria; all have had PsA for up to 10 years and were untreated with biologic or targeted synthetic disease modifying drugs at the time of inclusion.
Dr. Torgutalp, who is the study’s primary research coordinator, reported that a diagnosis of PsA was made in 37% of the population when local investigators considered available clinical, laboratory, and imaging data. However, patients’ imaging data were also centrally assessed, and when the local investigators were party to the expert imaging interpretations, the percentage of people diagnosed with PsA dropped to 27%.
“When we looked at the clinical characteristics, the presence of the back pain, particularly inflammatory back pain, HLA-B27 positivity, elevated CRP, and presence of active, inflammatory and structural changes in the sacroiliac joints and spine were associated with the final conclusion on the presence of axial involvement,” Dr. Torgutalp said.
Despite the title of his presentation being “The Axis Study Gives Answers,” Dr. Torgutalp presented lots of data without giving much insight into how they might be used. He concluded that “overall, there was a trend toward overestimation of the presence of imaging changes indicative of axial involvement across all imaging modalities” by the local investigators.
Dennis McGonagle, MB, MCH, BAO, PhD, of the University of Leeds, Leeds, England,said in an interview that the AXIS study “is a noble, international effort across multiple countries to try and better understand axial PsA.”
Dr. McGonagle, who was not involved in the study, added: “A lot of data are being generated, and a lot of analysis needs to be done to drill down to get a clear message that could influence practice.”
Axial PsA in the Portuguese Population
Separately, Catarina Abreu, a rheumatology intern at Hospital Garcia de Orta, Almada, Portugal, presented some real-world data on axial PsA from Reuma.pt.
Of 2304 patients, 854 (37.1%) reportedly had axial PsA, which had been defined as physician-reported spondylitis or the presence of imaging findings suggestive of axial involvement. This included radiographic- or MRI-detected sacroiliitis or syndesmophytes seen on axial x-rays.
The majority (78.2%) of those with an axial PsA diagnosis had concomitant peripheral involvement, with 8.1% having exclusive axial disease.
About 70% of the axial PsA diagnoses had been made using clinical or laboratory findings alone, and 30% of diagnoses was based on imaging results. Of the latter, Ms. Abreu noted that patients who had imaging data available were more likely to be HLA-B27 positive and less likely to have dactylitis, with respective odds ratios (ORs) of 3.10 and 2.42.
Individuals with axial PsA were more likely to have enthesitis (OR, 1.92), although no data were available on whether this was axial or peripheral enthesitis. Tobacco exposure was also linked to an increased chance of having axial PsA (OR, 1.66).
Ms. Abreu noted that the “scarce number of available imaging exams” and other missing data in Reuma.pt may have led to an underdiagnosis of axial PsA.
“The difference that we found between axial and peripheral [PsA] are similar to the differences found in other studies that compared axial psoriatic arthritis with axial spondyloarthritis,” Ms. Abreu said.
“So, we leave with the question that was already left before here: If these are different diseases or just different phenotypes of the same disease, and what implications will this have in the future?” Ms. Abreu concluded.
Dr. Carron received educational grants, speaker fees, or honoraria for other consultancy work from AbbVie, UCB, Pfizer, Eli Lilly, Novartis, Janssen, and Galapagos/Alfasigma. Dr. Ramiro is an ASAS executive committee member and received research grants or consulting/speaker fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp and Dohme, Novartis, Pfizer, Sanofi, and UCB. AXIS is supported by unrestricted research grants from AbbVie, Galapagos, Janssen, Eli Lilly, Novartis, Pfizer, and UCB. Dr. Torgutalp is the primary research coordinator for the study; he reported no financial conflicts of interest. The Reuma.pt registry was developed with the financial support of the pharmaceutical industry and is currently supported by AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp and Dohme, Novartis, Pfizer, and Sobi. Ms. Abreu reported no financial conflicts of interest.
A version of this article appeared on Medscape.com.
VIENNA — While there is no doubt that some people with psoriatic arthritis (PsA) have axial symptoms, data presented at the annual European Congress of Rheumatology do not appear to add much to what is already known about axial PsA or to further the cause of differentiating it from axial spondyloarthritis (axSpA).
In both the AXIS study and Reuma.pt, around one in three patients with PsA were found to have axial involvement. Notably, the percentage of people with axial PsA was found to vary according to how imaging information was interpreted in the AXIS study. Both studies were discussed during the Axial Involvement in PsA and SpA session at EULAR 2024.
The One-Million-Dollar Question
“So, the one-million-dollar question: What is it, really?” Philippe Carron, MD, PhD, Ghent University Hospital, Ghent, Belgium, said in the presentation that started the session. Despite PsA being described more than 60 years ago, “we still have no internationally accepted definition or a consensus on how we should define these patients and how we should screen them,” he said.
“There are some believers that it is just a form of axial SpA with concomitant psoriasis, but also some people that think that the axial PsA is a typical disease, with typical characteristics which are different from axial disease,” Dr. Carron said.
The lack of consensus makes it difficult to estimate just how many people have axial PsA. Reported prevalences range from 5% to 70%, “all caused by which criteria that you’re using to define axial involvement,” Dr. Carron added.
There are, however, two things that can be agreed upon, according to Dr. Carron. First, the prevalence of axial involvement in people with early PsA is “much, much lower” than that of more established disease. Second, exclusive axial involvement is seen in “just a minority of PsA patients.” Most people with axial disease also have peripheral disease, he added.
Imaging findings in axial PsA “are quite similar to those seen in axial SpA,” although Dr. Carron also said that there were some distinct differences. Radiographic sacroiliitis occurs in around 25%-50% of people with axial PsA, and atypical syndesmophytes are more often found in people with axial PsA than in those with axSpA.
Shared Characteristics
But are axial PsA and axSpA separate diseases or part of the same disease continuum? That’s a question that is still very much open for debate, said Sofia Ramiro, MD, PhD, a senior researcher at Leiden University Medical Center, Leiden, the Netherlands, and rheumatology consultant at Zuyderland Medical Center in Heerlen, the Netherlands.
While many studies have looked to answer this question, there is a big methodological problem — the studies largely cannot be compared as they have used different definitions of axSpA.
Take a patient with inflammatory back pain, psoriasis, and oligoarthritis, Dr. Ramiro said. If the patient goes to one rheumatologist, they may get a diagnosis of axSpA, but if they go to a different rheumatologist, they may get a diagnosis of axial PsA.
“This is influenced by training, expertise, by beliefs, and by belonging to ASAS [Assessment of Spondyloarthritis International Society] or to GRAPPA [Group for Research and Assessment of Psoriasis and Psoriatic Arthritis],” Dr. Ramiro suggested. It’s “a diagnostic bias” that is very difficult to overcome and makes direct comparisons between patient populations recruited into clinical studies “extremely challenging.”
To confuse matters more, axial PsA and axSpA share common characteristics: Inflammatory back pain, HLA-B27 positivity, elevated levels of C-reactive protein (CRP) or a higher erythrocyte sedimentation rate, and structural lesions in the sacroiliac joints and spine.
AXIS Study ‘Gives Answers’
More research into factors associated with axial PsA need to be performed to try to help define the condition and enable classification and ultimately treatment guidelines. This is where the AXIS study comes in.
The AXIS study is a joint project of ASAS and GRAPPA that was started in January 2019 with the aim of defining a homogeneous subgroup of patients who could be studied.
“The objectives of the AXIS study are to determine the frequency of axial involvement in patients with PsA; to identify the frequency of active inflammatory and structural changes on imaging; and to identify factors associated with the presence of axial involvement in PsA,” Murat Torgutalp, MD, of Charité – Universitätsmedizin Berlin, Berlin, Germany, said at EULAR 2024.
The study population consisted of 409 consecutively recruited patients diagnosed with PsA according to CASPAR (Classification for Psoriatic Arthritis) criteria; all have had PsA for up to 10 years and were untreated with biologic or targeted synthetic disease modifying drugs at the time of inclusion.
Dr. Torgutalp, who is the study’s primary research coordinator, reported that a diagnosis of PsA was made in 37% of the population when local investigators considered available clinical, laboratory, and imaging data. However, patients’ imaging data were also centrally assessed, and when the local investigators were party to the expert imaging interpretations, the percentage of people diagnosed with PsA dropped to 27%.
“When we looked at the clinical characteristics, the presence of the back pain, particularly inflammatory back pain, HLA-B27 positivity, elevated CRP, and presence of active, inflammatory and structural changes in the sacroiliac joints and spine were associated with the final conclusion on the presence of axial involvement,” Dr. Torgutalp said.
Despite the title of his presentation being “The Axis Study Gives Answers,” Dr. Torgutalp presented lots of data without giving much insight into how they might be used. He concluded that “overall, there was a trend toward overestimation of the presence of imaging changes indicative of axial involvement across all imaging modalities” by the local investigators.
Dennis McGonagle, MB, MCH, BAO, PhD, of the University of Leeds, Leeds, England,said in an interview that the AXIS study “is a noble, international effort across multiple countries to try and better understand axial PsA.”
Dr. McGonagle, who was not involved in the study, added: “A lot of data are being generated, and a lot of analysis needs to be done to drill down to get a clear message that could influence practice.”
Axial PsA in the Portuguese Population
Separately, Catarina Abreu, a rheumatology intern at Hospital Garcia de Orta, Almada, Portugal, presented some real-world data on axial PsA from Reuma.pt.
Of 2304 patients, 854 (37.1%) reportedly had axial PsA, which had been defined as physician-reported spondylitis or the presence of imaging findings suggestive of axial involvement. This included radiographic- or MRI-detected sacroiliitis or syndesmophytes seen on axial x-rays.
The majority (78.2%) of those with an axial PsA diagnosis had concomitant peripheral involvement, with 8.1% having exclusive axial disease.
About 70% of the axial PsA diagnoses had been made using clinical or laboratory findings alone, and 30% of diagnoses was based on imaging results. Of the latter, Ms. Abreu noted that patients who had imaging data available were more likely to be HLA-B27 positive and less likely to have dactylitis, with respective odds ratios (ORs) of 3.10 and 2.42.
Individuals with axial PsA were more likely to have enthesitis (OR, 1.92), although no data were available on whether this was axial or peripheral enthesitis. Tobacco exposure was also linked to an increased chance of having axial PsA (OR, 1.66).
Ms. Abreu noted that the “scarce number of available imaging exams” and other missing data in Reuma.pt may have led to an underdiagnosis of axial PsA.
“The difference that we found between axial and peripheral [PsA] are similar to the differences found in other studies that compared axial psoriatic arthritis with axial spondyloarthritis,” Ms. Abreu said.
“So, we leave with the question that was already left before here: If these are different diseases or just different phenotypes of the same disease, and what implications will this have in the future?” Ms. Abreu concluded.
Dr. Carron received educational grants, speaker fees, or honoraria for other consultancy work from AbbVie, UCB, Pfizer, Eli Lilly, Novartis, Janssen, and Galapagos/Alfasigma. Dr. Ramiro is an ASAS executive committee member and received research grants or consulting/speaker fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp and Dohme, Novartis, Pfizer, Sanofi, and UCB. AXIS is supported by unrestricted research grants from AbbVie, Galapagos, Janssen, Eli Lilly, Novartis, Pfizer, and UCB. Dr. Torgutalp is the primary research coordinator for the study; he reported no financial conflicts of interest. The Reuma.pt registry was developed with the financial support of the pharmaceutical industry and is currently supported by AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp and Dohme, Novartis, Pfizer, and Sobi. Ms. Abreu reported no financial conflicts of interest.
A version of this article appeared on Medscape.com.
VIENNA — While there is no doubt that some people with psoriatic arthritis (PsA) have axial symptoms, data presented at the annual European Congress of Rheumatology do not appear to add much to what is already known about axial PsA or to further the cause of differentiating it from axial spondyloarthritis (axSpA).
In both the AXIS study and Reuma.pt, around one in three patients with PsA were found to have axial involvement. Notably, the percentage of people with axial PsA was found to vary according to how imaging information was interpreted in the AXIS study. Both studies were discussed during the Axial Involvement in PsA and SpA session at EULAR 2024.
The One-Million-Dollar Question
“So, the one-million-dollar question: What is it, really?” Philippe Carron, MD, PhD, Ghent University Hospital, Ghent, Belgium, said in the presentation that started the session. Despite PsA being described more than 60 years ago, “we still have no internationally accepted definition or a consensus on how we should define these patients and how we should screen them,” he said.
“There are some believers that it is just a form of axial SpA with concomitant psoriasis, but also some people that think that the axial PsA is a typical disease, with typical characteristics which are different from axial disease,” Dr. Carron said.
The lack of consensus makes it difficult to estimate just how many people have axial PsA. Reported prevalences range from 5% to 70%, “all caused by which criteria that you’re using to define axial involvement,” Dr. Carron added.
There are, however, two things that can be agreed upon, according to Dr. Carron. First, the prevalence of axial involvement in people with early PsA is “much, much lower” than that of more established disease. Second, exclusive axial involvement is seen in “just a minority of PsA patients.” Most people with axial disease also have peripheral disease, he added.
Imaging findings in axial PsA “are quite similar to those seen in axial SpA,” although Dr. Carron also said that there were some distinct differences. Radiographic sacroiliitis occurs in around 25%-50% of people with axial PsA, and atypical syndesmophytes are more often found in people with axial PsA than in those with axSpA.
Shared Characteristics
But are axial PsA and axSpA separate diseases or part of the same disease continuum? That’s a question that is still very much open for debate, said Sofia Ramiro, MD, PhD, a senior researcher at Leiden University Medical Center, Leiden, the Netherlands, and rheumatology consultant at Zuyderland Medical Center in Heerlen, the Netherlands.
While many studies have looked to answer this question, there is a big methodological problem — the studies largely cannot be compared as they have used different definitions of axSpA.
Take a patient with inflammatory back pain, psoriasis, and oligoarthritis, Dr. Ramiro said. If the patient goes to one rheumatologist, they may get a diagnosis of axSpA, but if they go to a different rheumatologist, they may get a diagnosis of axial PsA.
“This is influenced by training, expertise, by beliefs, and by belonging to ASAS [Assessment of Spondyloarthritis International Society] or to GRAPPA [Group for Research and Assessment of Psoriasis and Psoriatic Arthritis],” Dr. Ramiro suggested. It’s “a diagnostic bias” that is very difficult to overcome and makes direct comparisons between patient populations recruited into clinical studies “extremely challenging.”
To confuse matters more, axial PsA and axSpA share common characteristics: Inflammatory back pain, HLA-B27 positivity, elevated levels of C-reactive protein (CRP) or a higher erythrocyte sedimentation rate, and structural lesions in the sacroiliac joints and spine.
AXIS Study ‘Gives Answers’
More research into factors associated with axial PsA need to be performed to try to help define the condition and enable classification and ultimately treatment guidelines. This is where the AXIS study comes in.
The AXIS study is a joint project of ASAS and GRAPPA that was started in January 2019 with the aim of defining a homogeneous subgroup of patients who could be studied.
“The objectives of the AXIS study are to determine the frequency of axial involvement in patients with PsA; to identify the frequency of active inflammatory and structural changes on imaging; and to identify factors associated with the presence of axial involvement in PsA,” Murat Torgutalp, MD, of Charité – Universitätsmedizin Berlin, Berlin, Germany, said at EULAR 2024.
The study population consisted of 409 consecutively recruited patients diagnosed with PsA according to CASPAR (Classification for Psoriatic Arthritis) criteria; all have had PsA for up to 10 years and were untreated with biologic or targeted synthetic disease modifying drugs at the time of inclusion.
Dr. Torgutalp, who is the study’s primary research coordinator, reported that a diagnosis of PsA was made in 37% of the population when local investigators considered available clinical, laboratory, and imaging data. However, patients’ imaging data were also centrally assessed, and when the local investigators were party to the expert imaging interpretations, the percentage of people diagnosed with PsA dropped to 27%.
“When we looked at the clinical characteristics, the presence of the back pain, particularly inflammatory back pain, HLA-B27 positivity, elevated CRP, and presence of active, inflammatory and structural changes in the sacroiliac joints and spine were associated with the final conclusion on the presence of axial involvement,” Dr. Torgutalp said.
Despite the title of his presentation being “The Axis Study Gives Answers,” Dr. Torgutalp presented lots of data without giving much insight into how they might be used. He concluded that “overall, there was a trend toward overestimation of the presence of imaging changes indicative of axial involvement across all imaging modalities” by the local investigators.
Dennis McGonagle, MB, MCH, BAO, PhD, of the University of Leeds, Leeds, England,said in an interview that the AXIS study “is a noble, international effort across multiple countries to try and better understand axial PsA.”
Dr. McGonagle, who was not involved in the study, added: “A lot of data are being generated, and a lot of analysis needs to be done to drill down to get a clear message that could influence practice.”
Axial PsA in the Portuguese Population
Separately, Catarina Abreu, a rheumatology intern at Hospital Garcia de Orta, Almada, Portugal, presented some real-world data on axial PsA from Reuma.pt.
Of 2304 patients, 854 (37.1%) reportedly had axial PsA, which had been defined as physician-reported spondylitis or the presence of imaging findings suggestive of axial involvement. This included radiographic- or MRI-detected sacroiliitis or syndesmophytes seen on axial x-rays.
The majority (78.2%) of those with an axial PsA diagnosis had concomitant peripheral involvement, with 8.1% having exclusive axial disease.
About 70% of the axial PsA diagnoses had been made using clinical or laboratory findings alone, and 30% of diagnoses was based on imaging results. Of the latter, Ms. Abreu noted that patients who had imaging data available were more likely to be HLA-B27 positive and less likely to have dactylitis, with respective odds ratios (ORs) of 3.10 and 2.42.
Individuals with axial PsA were more likely to have enthesitis (OR, 1.92), although no data were available on whether this was axial or peripheral enthesitis. Tobacco exposure was also linked to an increased chance of having axial PsA (OR, 1.66).
Ms. Abreu noted that the “scarce number of available imaging exams” and other missing data in Reuma.pt may have led to an underdiagnosis of axial PsA.
“The difference that we found between axial and peripheral [PsA] are similar to the differences found in other studies that compared axial psoriatic arthritis with axial spondyloarthritis,” Ms. Abreu said.
“So, we leave with the question that was already left before here: If these are different diseases or just different phenotypes of the same disease, and what implications will this have in the future?” Ms. Abreu concluded.
Dr. Carron received educational grants, speaker fees, or honoraria for other consultancy work from AbbVie, UCB, Pfizer, Eli Lilly, Novartis, Janssen, and Galapagos/Alfasigma. Dr. Ramiro is an ASAS executive committee member and received research grants or consulting/speaker fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp and Dohme, Novartis, Pfizer, Sanofi, and UCB. AXIS is supported by unrestricted research grants from AbbVie, Galapagos, Janssen, Eli Lilly, Novartis, Pfizer, and UCB. Dr. Torgutalp is the primary research coordinator for the study; he reported no financial conflicts of interest. The Reuma.pt registry was developed with the financial support of the pharmaceutical industry and is currently supported by AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp and Dohme, Novartis, Pfizer, and Sobi. Ms. Abreu reported no financial conflicts of interest.
A version of this article appeared on Medscape.com.
FROM EULAR 2024
Patient-Driven Care Plus Telemonitoring Yields Promising Results for Spondyloarthritis
VIENNA — People with spondyloarthritis (SpA) who have low or stable disease activity can effectively and safely be managed using a model of patient-initiated care with or without remote monitoring, suggested the results of two separate trials presented at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting.
In the 18-month, single-center ReMonit study that included 243 people with axial SpA (axSpA), patient-initiated care was found to be noninferior for keeping them in a low-disease activity state, compared with both usual hospital follow-up and remote digital monitoring.
Meanwhile, in the 12-month, multicenter TeleSpA study, which included 200 patients with any type of SpA, the number of hospital visits needed by people who were randomly assigned to receive patient-initiated care together with asynchronous telemonitoring was significantly lower than for the usual-care group, with no detriment to the participants’ overall health outcomes or safety. Moreover, the strategy was deemed cost-effective from a healthcare provision perspective.
Time to Rationalize Healthcare Resources?
People with chronic rheumatic diseases such as axSpA require long-term follow-up in specialist healthcare centers, Inger Jorid Berg, MD, PhD, of Diakonhjemmet Hospital in Oslo, Norway, said when she presented the findings of the ReMonit study as a late-breaking abstract.

“Traditionally, this has been offered as prescheduled face-to-face consultations at an outpatient clinic, but remote monitoring and patient-initiated care may allow for more targeted and efficient uses of healthcare resources,” Dr. Berg said.
“The end goal of what you’re trying to do is increase the efficiency of outpatient care and provide more patient-tailored care,” Kasper Hermans, MD, said in an interview. He presented the results of the TeleSpA study.
Dr. Hermans, who is a rheumatology fellow and PhD candidate at Maastricht University, Maastricht, the Netherlands, observed during his presentation at EULAR 2024 that there is an increasing demand for rheumatology services but an expected shortfall in the future workforce. Thus, “sustainable alternative strategies are needed for optimizing the efficiency of care,” he said.
People need to have timely access to care, Dr. Hermans stressed, but perhaps alternatives to the traditional models of care where patients are seen routinely every 6 or 12 months are needed, particularly as prior work had suggested that around one-third of people who were seen by a rheumatologist perhaps did not need to be.
A strategy of patient-initiated care — which is where people are seen by a healthcare provider only if they feel that they need to and request a consultation — is therefore an attractive proposition, particularly if it is backed up with remote monitoring, which is what the TeleSpA study was testing.
Two Distinct Studies
ReMonit and TeleSpA were two distinct studies. While both were noninferiority trials and involved patient-initiated care and telemonitoring of outpatients with SpA, that is where the similarities generally end.
Notably, ReMonit included a very specific population of patients — all had a diagnosis of axSpA and were being treated with a tumor necrosis factor (TNF) inhibitor and had been on a stable dose for the last 6 months. For inclusion, they also had to have inactive disease or low disease activity, as indicated by an Ankylosing Spondylitis Disease Activity Score (ASDAS) < 2.1.
ReMonit’s telemonitoring strategy involved participants completing monthly questionnaires using the Dignio smartphone app. Patients first completed the Patient Global Assessment (PGA) and noted whether they had experienced a flare in their disease. If they had a flare or their PGA score was 3 or higher, then they were asked to also complete the Bath Ankylosing Spondyloarthritis Disease Activity Index (BASDAI). If the BASDAI score was 4 or more, then the patient was called by a study nurse and offered a consultation.
“Patients in all three groups were recommended to take blood samples at the general practitioner’s or at the hospital every third month as a safety procedure when using TNF inhibitors,” Dr. Berg said.
The primary outcome was the proportion of people who remained with low disease activity (ASDAS < 2.1) at 6, 12, and 18 months in each of the three arms of the trial, which were patient-initiated care (n = 81), monthly remote monitoring (n = 80), or usual follow-up in the hospital every 6 months (n = 82).
TeleSpA on the other hand was a “much more pragmatic trial, much closer to actual care,” Dr. Hermans said. “We included axial spondyloarthritis, peripheral spondyloarthritis, or patients who had both axial and peripheral disease, including patients with psoriatic arthritis,” he said, adding that their inclusion was regardless of their baseline ASDAS based on C-reactive protein (ASDAS-CRP).
This means that patients who would otherwise have been classified at baseline as having high disease activity (by ASDAS-CRP or similar disease activity measures) could be included. The main proviso was that both the patient and their rheumatologist had to define the condition as being stable with an acceptable level of symptom control and no immediate plans to change treatment within the next 3 months.
TeleSpA’s remote monitoring strategy involved the use of SpA-Net, which Dr. Hermans and coinvestigators have described previously as “an ongoing, disease-specific, prospective, web-based registry for monitoring SpA in daily practice.” This captures a host of clinical and laboratory test information.
SpA-Net was used in both arms of the study. However, while the 100 participants in the standard-care arm completed questionnaires and had tests before every in-person visit that had been prescheduled with their rheumatologist, the 100 individuals in the patient-initiated care arm had no prescheduled in-person visits except for being seen at the start and end of the study. These patients were reminded via email to complete the necessary SpA-Net registry questionnaires at 6 months.
The primary outcome for TeleSpA was the total number of rheumatology visits, including both physical and telephone or video consultations, within a 1-year period.
ReMonit Results
Berg reported that similar percentages of patients remained in a low disease activity state at 6, 12, and 18 months, regardless of the group that they had been randomized into, and that there was little change seen within the individual groups.
For instance, at 6, 12, and 18 months, 92%, 91%, and 92% of individuals in the patient-initiated arm had an ASDAS of < 2.1. Corresponding percentages for the usual-care arm were 96%, 93%, and 90% and for the remote-monitoring arm were 96%, 96%, and 94%.
Both patient-initiated care and remote monitoring were noninferior to usual care, and patient-initiated care was also noninferior to remote monitoring. There were no differences between the trial arms in terms of disease activity, measured using either ASDAS or BASDAI, at 6, 12, or 18 months.
Dr. Berg stated that “patient satisfaction was high in all three follow-up strategies, and there was the lowest resource use with patient-initiated care.” She concluded that “remote monitoring and patient-initiated care could be implemented in the follow-up of patients with axial spondyloarthritis and low disease activity.”
TeleSpA Results
In TeleSpA, people in the patient-initiated care and telemonitoring arm were seen a mean of 1.9 times over the course of the 1-year follow-up vs 2.6 for people in the usual care arm. The reduction was caused in part by the decrease in physical visits (1.4 vs 2.0) as there were the same mean number of telephone visits in each group. Overall, there was a 25.4% reduction in consultations comparing the patient-initiated care and telemonitoring arm with the usual-care arm.
Importantly, the intervention was noninferior regarding all of the predefined health outcomes: ASDAS, BASDAI, pain assessed using a visual analog scale, patient global assessment, and physician global assessment.
And more than 90% of participants in both groups reported having an overall good experience with their care.
Dr. Hermans noted after his presentation that an additional study had been performed where “we actively engaged with patients in the intervention group as well as healthcare providers to ask them what their experiences were with the intervention, how we could possibly improve it, and whether or not they thought that it was a valid approach to follow-up after the end of the study. And results were very, very reassuring.”
In terms of safety, eight serious adverse events were reported, but none were related to the study intervention, Dr. Hermans said.
Dr. Hermans reported that there was “negligible difference” in the 1-year quality-adjusted life-years (+0.004, in favor of the intervention overall) and that, while healthcare costs were lower at €243/year for the entire intervention period, societal costs were higher, at €513/year vs usual care. The latter was thought to be “due to an unexpected rise in absenteeism that we think was most likely due to a small amount of outliers,” Dr. Hermans said.
Nonetheless, using at willingness-to-pay threshold of €20,000/ quality-adjusted life year, he reported that the added value of patient-initiated care with remote monitoring yielded a potential net monetary benefit of +€322 from a healthcare perspective for the entire intervention period.
“We believe that these results support the fast-paced adoption of remote care interventions,” Dr. Hermans said. “In the context that I described earlier, of decreasing healthcare personnel and rising costs, we believe that this could be a valuable approach for follow-up for patients with stable axSpA.”
ReMonit was sponsored by Diakonhjemmet Hospital, and TeleSpA was sponsored by Maastricht University Medical Center, with funding from the Dutch Arthritis Society. Dr. Berg and Dr. Hermans had no relevant conflicts of interest to report.
A version of this article first appeared on Medscape.com.
Editor’s Note: This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
VIENNA — People with spondyloarthritis (SpA) who have low or stable disease activity can effectively and safely be managed using a model of patient-initiated care with or without remote monitoring, suggested the results of two separate trials presented at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting.
In the 18-month, single-center ReMonit study that included 243 people with axial SpA (axSpA), patient-initiated care was found to be noninferior for keeping them in a low-disease activity state, compared with both usual hospital follow-up and remote digital monitoring.
Meanwhile, in the 12-month, multicenter TeleSpA study, which included 200 patients with any type of SpA, the number of hospital visits needed by people who were randomly assigned to receive patient-initiated care together with asynchronous telemonitoring was significantly lower than for the usual-care group, with no detriment to the participants’ overall health outcomes or safety. Moreover, the strategy was deemed cost-effective from a healthcare provision perspective.
Time to Rationalize Healthcare Resources?
People with chronic rheumatic diseases such as axSpA require long-term follow-up in specialist healthcare centers, Inger Jorid Berg, MD, PhD, of Diakonhjemmet Hospital in Oslo, Norway, said when she presented the findings of the ReMonit study as a late-breaking abstract.
“Traditionally, this has been offered as prescheduled face-to-face consultations at an outpatient clinic, but remote monitoring and patient-initiated care may allow for more targeted and efficient uses of healthcare resources,” Dr. Berg said.
“The end goal of what you’re trying to do is increase the efficiency of outpatient care and provide more patient-tailored care,” Kasper Hermans, MD, said in an interview. He presented the results of the TeleSpA study.
Dr. Hermans, who is a rheumatology fellow and PhD candidate at Maastricht University, Maastricht, the Netherlands, observed during his presentation at EULAR 2024 that there is an increasing demand for rheumatology services but an expected shortfall in the future workforce. Thus, “sustainable alternative strategies are needed for optimizing the efficiency of care,” he said.
People need to have timely access to care, Dr. Hermans stressed, but perhaps alternatives to the traditional models of care where patients are seen routinely every 6 or 12 months are needed, particularly as prior work had suggested that around one-third of people who were seen by a rheumatologist perhaps did not need to be.
A strategy of patient-initiated care — which is where people are seen by a healthcare provider only if they feel that they need to and request a consultation — is therefore an attractive proposition, particularly if it is backed up with remote monitoring, which is what the TeleSpA study was testing.
Two Distinct Studies
ReMonit and TeleSpA were two distinct studies. While both were noninferiority trials and involved patient-initiated care and telemonitoring of outpatients with SpA, that is where the similarities generally end.
Notably, ReMonit included a very specific population of patients — all had a diagnosis of axSpA and were being treated with a tumor necrosis factor (TNF) inhibitor and had been on a stable dose for the last 6 months. For inclusion, they also had to have inactive disease or low disease activity, as indicated by an Ankylosing Spondylitis Disease Activity Score (ASDAS) < 2.1.
ReMonit’s telemonitoring strategy involved participants completing monthly questionnaires using the Dignio smartphone app. Patients first completed the Patient Global Assessment (PGA) and noted whether they had experienced a flare in their disease. If they had a flare or their PGA score was 3 or higher, then they were asked to also complete the Bath Ankylosing Spondyloarthritis Disease Activity Index (BASDAI). If the BASDAI score was 4 or more, then the patient was called by a study nurse and offered a consultation.
“Patients in all three groups were recommended to take blood samples at the general practitioner’s or at the hospital every third month as a safety procedure when using TNF inhibitors,” Dr. Berg said.
The primary outcome was the proportion of people who remained with low disease activity (ASDAS < 2.1) at 6, 12, and 18 months in each of the three arms of the trial, which were patient-initiated care (n = 81), monthly remote monitoring (n = 80), or usual follow-up in the hospital every 6 months (n = 82).
TeleSpA on the other hand was a “much more pragmatic trial, much closer to actual care,” Dr. Hermans said. “We included axial spondyloarthritis, peripheral spondyloarthritis, or patients who had both axial and peripheral disease, including patients with psoriatic arthritis,” he said, adding that their inclusion was regardless of their baseline ASDAS based on C-reactive protein (ASDAS-CRP).
This means that patients who would otherwise have been classified at baseline as having high disease activity (by ASDAS-CRP or similar disease activity measures) could be included. The main proviso was that both the patient and their rheumatologist had to define the condition as being stable with an acceptable level of symptom control and no immediate plans to change treatment within the next 3 months.
TeleSpA’s remote monitoring strategy involved the use of SpA-Net, which Dr. Hermans and coinvestigators have described previously as “an ongoing, disease-specific, prospective, web-based registry for monitoring SpA in daily practice.” This captures a host of clinical and laboratory test information.
SpA-Net was used in both arms of the study. However, while the 100 participants in the standard-care arm completed questionnaires and had tests before every in-person visit that had been prescheduled with their rheumatologist, the 100 individuals in the patient-initiated care arm had no prescheduled in-person visits except for being seen at the start and end of the study. These patients were reminded via email to complete the necessary SpA-Net registry questionnaires at 6 months.
The primary outcome for TeleSpA was the total number of rheumatology visits, including both physical and telephone or video consultations, within a 1-year period.
ReMonit Results
Berg reported that similar percentages of patients remained in a low disease activity state at 6, 12, and 18 months, regardless of the group that they had been randomized into, and that there was little change seen within the individual groups.
For instance, at 6, 12, and 18 months, 92%, 91%, and 92% of individuals in the patient-initiated arm had an ASDAS of < 2.1. Corresponding percentages for the usual-care arm were 96%, 93%, and 90% and for the remote-monitoring arm were 96%, 96%, and 94%.
Both patient-initiated care and remote monitoring were noninferior to usual care, and patient-initiated care was also noninferior to remote monitoring. There were no differences between the trial arms in terms of disease activity, measured using either ASDAS or BASDAI, at 6, 12, or 18 months.
Dr. Berg stated that “patient satisfaction was high in all three follow-up strategies, and there was the lowest resource use with patient-initiated care.” She concluded that “remote monitoring and patient-initiated care could be implemented in the follow-up of patients with axial spondyloarthritis and low disease activity.”
TeleSpA Results
In TeleSpA, people in the patient-initiated care and telemonitoring arm were seen a mean of 1.9 times over the course of the 1-year follow-up vs 2.6 for people in the usual care arm. The reduction was caused in part by the decrease in physical visits (1.4 vs 2.0) as there were the same mean number of telephone visits in each group. Overall, there was a 25.4% reduction in consultations comparing the patient-initiated care and telemonitoring arm with the usual-care arm.
Importantly, the intervention was noninferior regarding all of the predefined health outcomes: ASDAS, BASDAI, pain assessed using a visual analog scale, patient global assessment, and physician global assessment.
And more than 90% of participants in both groups reported having an overall good experience with their care.
Dr. Hermans noted after his presentation that an additional study had been performed where “we actively engaged with patients in the intervention group as well as healthcare providers to ask them what their experiences were with the intervention, how we could possibly improve it, and whether or not they thought that it was a valid approach to follow-up after the end of the study. And results were very, very reassuring.”
In terms of safety, eight serious adverse events were reported, but none were related to the study intervention, Dr. Hermans said.
Dr. Hermans reported that there was “negligible difference” in the 1-year quality-adjusted life-years (+0.004, in favor of the intervention overall) and that, while healthcare costs were lower at €243/year for the entire intervention period, societal costs were higher, at €513/year vs usual care. The latter was thought to be “due to an unexpected rise in absenteeism that we think was most likely due to a small amount of outliers,” Dr. Hermans said.
Nonetheless, using at willingness-to-pay threshold of €20,000/ quality-adjusted life year, he reported that the added value of patient-initiated care with remote monitoring yielded a potential net monetary benefit of +€322 from a healthcare perspective for the entire intervention period.
“We believe that these results support the fast-paced adoption of remote care interventions,” Dr. Hermans said. “In the context that I described earlier, of decreasing healthcare personnel and rising costs, we believe that this could be a valuable approach for follow-up for patients with stable axSpA.”
ReMonit was sponsored by Diakonhjemmet Hospital, and TeleSpA was sponsored by Maastricht University Medical Center, with funding from the Dutch Arthritis Society. Dr. Berg and Dr. Hermans had no relevant conflicts of interest to report.
A version of this article first appeared on Medscape.com.
Editor’s Note: This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
VIENNA — People with spondyloarthritis (SpA) who have low or stable disease activity can effectively and safely be managed using a model of patient-initiated care with or without remote monitoring, suggested the results of two separate trials presented at the European Alliance of Associations for Rheumatology (EULAR) 2024 Annual Meeting.
In the 18-month, single-center ReMonit study that included 243 people with axial SpA (axSpA), patient-initiated care was found to be noninferior for keeping them in a low-disease activity state, compared with both usual hospital follow-up and remote digital monitoring.
Meanwhile, in the 12-month, multicenter TeleSpA study, which included 200 patients with any type of SpA, the number of hospital visits needed by people who were randomly assigned to receive patient-initiated care together with asynchronous telemonitoring was significantly lower than for the usual-care group, with no detriment to the participants’ overall health outcomes or safety. Moreover, the strategy was deemed cost-effective from a healthcare provision perspective.
Time to Rationalize Healthcare Resources?
People with chronic rheumatic diseases such as axSpA require long-term follow-up in specialist healthcare centers, Inger Jorid Berg, MD, PhD, of Diakonhjemmet Hospital in Oslo, Norway, said when she presented the findings of the ReMonit study as a late-breaking abstract.
“Traditionally, this has been offered as prescheduled face-to-face consultations at an outpatient clinic, but remote monitoring and patient-initiated care may allow for more targeted and efficient uses of healthcare resources,” Dr. Berg said.
“The end goal of what you’re trying to do is increase the efficiency of outpatient care and provide more patient-tailored care,” Kasper Hermans, MD, said in an interview. He presented the results of the TeleSpA study.
Dr. Hermans, who is a rheumatology fellow and PhD candidate at Maastricht University, Maastricht, the Netherlands, observed during his presentation at EULAR 2024 that there is an increasing demand for rheumatology services but an expected shortfall in the future workforce. Thus, “sustainable alternative strategies are needed for optimizing the efficiency of care,” he said.
People need to have timely access to care, Dr. Hermans stressed, but perhaps alternatives to the traditional models of care where patients are seen routinely every 6 or 12 months are needed, particularly as prior work had suggested that around one-third of people who were seen by a rheumatologist perhaps did not need to be.
A strategy of patient-initiated care — which is where people are seen by a healthcare provider only if they feel that they need to and request a consultation — is therefore an attractive proposition, particularly if it is backed up with remote monitoring, which is what the TeleSpA study was testing.
Two Distinct Studies
ReMonit and TeleSpA were two distinct studies. While both were noninferiority trials and involved patient-initiated care and telemonitoring of outpatients with SpA, that is where the similarities generally end.
Notably, ReMonit included a very specific population of patients — all had a diagnosis of axSpA and were being treated with a tumor necrosis factor (TNF) inhibitor and had been on a stable dose for the last 6 months. For inclusion, they also had to have inactive disease or low disease activity, as indicated by an Ankylosing Spondylitis Disease Activity Score (ASDAS) < 2.1.
ReMonit’s telemonitoring strategy involved participants completing monthly questionnaires using the Dignio smartphone app. Patients first completed the Patient Global Assessment (PGA) and noted whether they had experienced a flare in their disease. If they had a flare or their PGA score was 3 or higher, then they were asked to also complete the Bath Ankylosing Spondyloarthritis Disease Activity Index (BASDAI). If the BASDAI score was 4 or more, then the patient was called by a study nurse and offered a consultation.
“Patients in all three groups were recommended to take blood samples at the general practitioner’s or at the hospital every third month as a safety procedure when using TNF inhibitors,” Dr. Berg said.
The primary outcome was the proportion of people who remained with low disease activity (ASDAS < 2.1) at 6, 12, and 18 months in each of the three arms of the trial, which were patient-initiated care (n = 81), monthly remote monitoring (n = 80), or usual follow-up in the hospital every 6 months (n = 82).
TeleSpA on the other hand was a “much more pragmatic trial, much closer to actual care,” Dr. Hermans said. “We included axial spondyloarthritis, peripheral spondyloarthritis, or patients who had both axial and peripheral disease, including patients with psoriatic arthritis,” he said, adding that their inclusion was regardless of their baseline ASDAS based on C-reactive protein (ASDAS-CRP).
This means that patients who would otherwise have been classified at baseline as having high disease activity (by ASDAS-CRP or similar disease activity measures) could be included. The main proviso was that both the patient and their rheumatologist had to define the condition as being stable with an acceptable level of symptom control and no immediate plans to change treatment within the next 3 months.
TeleSpA’s remote monitoring strategy involved the use of SpA-Net, which Dr. Hermans and coinvestigators have described previously as “an ongoing, disease-specific, prospective, web-based registry for monitoring SpA in daily practice.” This captures a host of clinical and laboratory test information.
SpA-Net was used in both arms of the study. However, while the 100 participants in the standard-care arm completed questionnaires and had tests before every in-person visit that had been prescheduled with their rheumatologist, the 100 individuals in the patient-initiated care arm had no prescheduled in-person visits except for being seen at the start and end of the study. These patients were reminded via email to complete the necessary SpA-Net registry questionnaires at 6 months.
The primary outcome for TeleSpA was the total number of rheumatology visits, including both physical and telephone or video consultations, within a 1-year period.
ReMonit Results
Berg reported that similar percentages of patients remained in a low disease activity state at 6, 12, and 18 months, regardless of the group that they had been randomized into, and that there was little change seen within the individual groups.
For instance, at 6, 12, and 18 months, 92%, 91%, and 92% of individuals in the patient-initiated arm had an ASDAS of < 2.1. Corresponding percentages for the usual-care arm were 96%, 93%, and 90% and for the remote-monitoring arm were 96%, 96%, and 94%.
Both patient-initiated care and remote monitoring were noninferior to usual care, and patient-initiated care was also noninferior to remote monitoring. There were no differences between the trial arms in terms of disease activity, measured using either ASDAS or BASDAI, at 6, 12, or 18 months.
Dr. Berg stated that “patient satisfaction was high in all three follow-up strategies, and there was the lowest resource use with patient-initiated care.” She concluded that “remote monitoring and patient-initiated care could be implemented in the follow-up of patients with axial spondyloarthritis and low disease activity.”
TeleSpA Results
In TeleSpA, people in the patient-initiated care and telemonitoring arm were seen a mean of 1.9 times over the course of the 1-year follow-up vs 2.6 for people in the usual care arm. The reduction was caused in part by the decrease in physical visits (1.4 vs 2.0) as there were the same mean number of telephone visits in each group. Overall, there was a 25.4% reduction in consultations comparing the patient-initiated care and telemonitoring arm with the usual-care arm.
Importantly, the intervention was noninferior regarding all of the predefined health outcomes: ASDAS, BASDAI, pain assessed using a visual analog scale, patient global assessment, and physician global assessment.
And more than 90% of participants in both groups reported having an overall good experience with their care.
Dr. Hermans noted after his presentation that an additional study had been performed where “we actively engaged with patients in the intervention group as well as healthcare providers to ask them what their experiences were with the intervention, how we could possibly improve it, and whether or not they thought that it was a valid approach to follow-up after the end of the study. And results were very, very reassuring.”
In terms of safety, eight serious adverse events were reported, but none were related to the study intervention, Dr. Hermans said.
Dr. Hermans reported that there was “negligible difference” in the 1-year quality-adjusted life-years (+0.004, in favor of the intervention overall) and that, while healthcare costs were lower at €243/year for the entire intervention period, societal costs were higher, at €513/year vs usual care. The latter was thought to be “due to an unexpected rise in absenteeism that we think was most likely due to a small amount of outliers,” Dr. Hermans said.
Nonetheless, using at willingness-to-pay threshold of €20,000/ quality-adjusted life year, he reported that the added value of patient-initiated care with remote monitoring yielded a potential net monetary benefit of +€322 from a healthcare perspective for the entire intervention period.
“We believe that these results support the fast-paced adoption of remote care interventions,” Dr. Hermans said. “In the context that I described earlier, of decreasing healthcare personnel and rising costs, we believe that this could be a valuable approach for follow-up for patients with stable axSpA.”
ReMonit was sponsored by Diakonhjemmet Hospital, and TeleSpA was sponsored by Maastricht University Medical Center, with funding from the Dutch Arthritis Society. Dr. Berg and Dr. Hermans had no relevant conflicts of interest to report.
A version of this article first appeared on Medscape.com.
Editor’s Note: This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
FROM EULAR 2024
What’s in a Name: Defining Difficult-to-Treat axSpA and PsA
Despite an expanding arsenal of disease-modifying antirheumatic drugs (DMARDs), many patients with axial spondyloarthritis (axSpA) and psoriatic arthritis (PsA) still struggle to reach remission even after trying multiple advanced treatments.
Now, international groups of experts are working to better define these “difficult-to-treat” patients to both inform care and improve selection of participants for future clinical trials.
“The idea is rather simple, and the need is relatively ubiquitous,” Denis Poddubnyy, MD, of the Charité – Universitätsmedizin Berlin and the German Rheumatism Research Center Berlin, both in Berlin, Germany, said in an interview. He is the co-primary investigator for the ongoing Assessment of SpondyloArthritis International Society (ASAS) project to develop a consensus definition of difficult-to-treat axSpA.
According to ASAS, only 40%-50% of patients with axSpA achieve a 40% improvement in ASAS response criteria (ASAS40), and few (10%-20%) achieve remission in the first 4-6 months of treatment.

“If you look into current clinical guidelines, you will see that there is no clear guidance,” on how to manage these patients, Dr. Poddubnyy continued. “In other similar recommendations for the treatment of axSpA, the only point which is clearly made with regards to nonresponders to effective anti-inflammatory treatment is to ‘check the diagnosis.’”
Multiple Reasons for Nonresponse
“While the term difficult-to-treat can refer to refractory disease, that is not the only reason why a patient might not be responding to medication. In fact, it’s likely that truly biologically refractory disease makes up only a fraction of cases that respond inadequately to treatment,” said Shikha Singla, MD, who directs the psoriatic arthritis program at the Medical College of Wisconsin in Milwaukee. She is also involved with the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) initiative to define Difficult-to-Treat and Complex-to-Manage PsA.

“Apart from the persistent articular and periarticular inflammation, there could be multiple noninflammatory factors that may be contributing to this treatment-resistant disease, including comorbid conditions such as obesity, cardiovascular disease, fibromyalgia, and even social factors such as limited access to medications,” she told this news organization. “Given these complexities, it is a matter of supreme importance to recognize and carefully delineate the elements that contribute to treatment refractory disease: Is it truly the inflammation, or are there noninflammatory components that are causing the treatment failure, or a combination of the two?”
Other contributing factors could be depression, hypersensitization, and comorbidities that prevent certain treatment approaches, added Fabian Proft, MD, also of Charité – Universitätsmedizin Berlin. Dr. Proft discussed these difficult-to-treat definition efforts at the recent Spondyloarthritis Research and Treatment Network (SPARTAN) annual meeting held in Cleveland. Patients also might not be taking their medication regularly and may be seeking alternative medicine approaches, he said.

“There is a quite clear consensus within the community” that differentiation between these two groups is needed, Dr. Proft said.
The Definitions
Terminology for these two groups can vary by professional society. The European Alliance of Associations for Rheumatology (EULAR) published a definition for “difficult-to-treat” rheumatoid arthritis (RA) that includes cases with “both inflammatory activity and/or noninflammatory complaints.”
The definition includes three criteria:
1) Treatment according to EULAR recommendation and failure of at least two biologic DMARDs (bDMARDs) or targeted synthetic DMARDs (tsDMARDs) (with different mechanisms of action) after failing conventional synthetic DMARD therapy (unless contraindicated)
2) Signs suggestive of active/progressive disease, including at least one of the following:
- Moderate disease activity (according to validated composite measures including joint counts)
- Signs (including acute phase reactants and imaging) and/or symptoms suggestive of active disease, whether joint-related or other
- Inability to taper glucocorticoid treatment
- Rapid radiographic progression (with or without signs of active disease)
- RA symptoms that are causing a reduction in quality of life
3) Symptom/sign management perceived as problematic by the rheumatologist or the patient
All three criteria must be met.
Both GRAPPA and ASAS plan to use the term “difficult-to-treat” or “treatment refractory” to describe true biologically refractory inflammatory disease and are categorizing the larger, heterogeneous group of nonresponders as “difficult-to-manage” (ASAS) or “complex-to-manage” (GRAPPA).
According to Dr. Poddubnyy, the agreed ASAS definition of difficult-to-manage has several similarities with EULAR’s RA definition, including three pillars:
- Treatment according to existing recommendations and failure of at least two different bDMARDs or tsDMARDs with different mechanisms
- Having signs and symptoms of disease (measured by high disease activity by certain disease activity indexes, persistently elevated C-reactive protein, inflammation on MRI, or rapid radiographic spinal progression)
- Symptoms/signs of disease that are considered problematic by the provider or patient
The definition was approved in January, and the manuscript is in the works, Dr. Poddubnyy said.
The GRAPPA project on PsA is still in its early stages, which so far has included a comprehensive literature review as well as a survey of GRAPPA members across 47 countries. The group is generally in agreement that two separate definitions for nonresponse to treatment are necessary, and that the “difficult-to-treat” definition — which identifies true refractory disease — should include objective signs of inflammation, Dr. Singla said.
Looking Forward
The next step of the ASAS project is to “define the pathway” from difficult-to-manage axSpA to treatment refractory disease, Dr. Poddubnyy said.
“What should be ruled out in order to exclude so-called noninflammatory causes of pain?” he continued. “It will require some Delphi exercises and [a] consensus approach.”
Proft anticipates that this treatment refractory definition in both axSpA and PsA will be most useful in research, rather than clinical practice.
“It is really important to have unified definition criteria to shape as homogeneous a cohort as possible,” he said, for future clinical trials in this population.
On the other hand, the complex/difficult-to-manage definition may be more useful for clinical practice, Dr. Proft thought.
“If you see a patient not responding to treatment, the easiest thing you can do would be to change treatment,” like swapping one biologic for another, Dr. Poddubnyy added, “but this would not be the right approach in every patient.” One goal of these initiatives is to give guidance on “what things should be looked after or excluded before you conclude this is biological [nonresponse],” he said.
Dr. Singla consults for AbbVie, Janssen, and UCB and received research funding from Eli Lilly. Dr. Poddubnyy disclosed serving as a speaker, consultant, and/or research grant recipient for multiple companies including AbbVie, Lilly, Merck Sharp and Dohme, Novartis, Pfizer, GlaxoSmithKline, Novartis, and UCB. Dr. Proft reported receiving research grants, consultant fees, or support for attending meetings and/or travel from Amgen, AbbVie, Bristol Myers Squibb, Celgene, Eli Lilly, Janssen, Merck Sharp and Dohme, Novartis, Pfizer, Roche, UCB, Medscape Medical News, Galapagos, and Hexal. Dr. Proft also participants on a data safety monitoring board or advisory board for AbbVie, Celgene, Janssen, Novartis, and UCB.
A version of this article appeared on Medscape.com.
Despite an expanding arsenal of disease-modifying antirheumatic drugs (DMARDs), many patients with axial spondyloarthritis (axSpA) and psoriatic arthritis (PsA) still struggle to reach remission even after trying multiple advanced treatments.
Now, international groups of experts are working to better define these “difficult-to-treat” patients to both inform care and improve selection of participants for future clinical trials.
“The idea is rather simple, and the need is relatively ubiquitous,” Denis Poddubnyy, MD, of the Charité – Universitätsmedizin Berlin and the German Rheumatism Research Center Berlin, both in Berlin, Germany, said in an interview. He is the co-primary investigator for the ongoing Assessment of SpondyloArthritis International Society (ASAS) project to develop a consensus definition of difficult-to-treat axSpA.
According to ASAS, only 40%-50% of patients with axSpA achieve a 40% improvement in ASAS response criteria (ASAS40), and few (10%-20%) achieve remission in the first 4-6 months of treatment.
“If you look into current clinical guidelines, you will see that there is no clear guidance,” on how to manage these patients, Dr. Poddubnyy continued. “In other similar recommendations for the treatment of axSpA, the only point which is clearly made with regards to nonresponders to effective anti-inflammatory treatment is to ‘check the diagnosis.’”
Multiple Reasons for Nonresponse
“While the term difficult-to-treat can refer to refractory disease, that is not the only reason why a patient might not be responding to medication. In fact, it’s likely that truly biologically refractory disease makes up only a fraction of cases that respond inadequately to treatment,” said Shikha Singla, MD, who directs the psoriatic arthritis program at the Medical College of Wisconsin in Milwaukee. She is also involved with the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) initiative to define Difficult-to-Treat and Complex-to-Manage PsA.
“Apart from the persistent articular and periarticular inflammation, there could be multiple noninflammatory factors that may be contributing to this treatment-resistant disease, including comorbid conditions such as obesity, cardiovascular disease, fibromyalgia, and even social factors such as limited access to medications,” she told this news organization. “Given these complexities, it is a matter of supreme importance to recognize and carefully delineate the elements that contribute to treatment refractory disease: Is it truly the inflammation, or are there noninflammatory components that are causing the treatment failure, or a combination of the two?”
Other contributing factors could be depression, hypersensitization, and comorbidities that prevent certain treatment approaches, added Fabian Proft, MD, also of Charité – Universitätsmedizin Berlin. Dr. Proft discussed these difficult-to-treat definition efforts at the recent Spondyloarthritis Research and Treatment Network (SPARTAN) annual meeting held in Cleveland. Patients also might not be taking their medication regularly and may be seeking alternative medicine approaches, he said.
“There is a quite clear consensus within the community” that differentiation between these two groups is needed, Dr. Proft said.
The Definitions
Terminology for these two groups can vary by professional society. The European Alliance of Associations for Rheumatology (EULAR) published a definition for “difficult-to-treat” rheumatoid arthritis (RA) that includes cases with “both inflammatory activity and/or noninflammatory complaints.”
The definition includes three criteria:
1) Treatment according to EULAR recommendation and failure of at least two biologic DMARDs (bDMARDs) or targeted synthetic DMARDs (tsDMARDs) (with different mechanisms of action) after failing conventional synthetic DMARD therapy (unless contraindicated)
2) Signs suggestive of active/progressive disease, including at least one of the following:
- Moderate disease activity (according to validated composite measures including joint counts)
- Signs (including acute phase reactants and imaging) and/or symptoms suggestive of active disease, whether joint-related or other
- Inability to taper glucocorticoid treatment
- Rapid radiographic progression (with or without signs of active disease)
- RA symptoms that are causing a reduction in quality of life
3) Symptom/sign management perceived as problematic by the rheumatologist or the patient
All three criteria must be met.
Both GRAPPA and ASAS plan to use the term “difficult-to-treat” or “treatment refractory” to describe true biologically refractory inflammatory disease and are categorizing the larger, heterogeneous group of nonresponders as “difficult-to-manage” (ASAS) or “complex-to-manage” (GRAPPA).
According to Dr. Poddubnyy, the agreed ASAS definition of difficult-to-manage has several similarities with EULAR’s RA definition, including three pillars:
- Treatment according to existing recommendations and failure of at least two different bDMARDs or tsDMARDs with different mechanisms
- Having signs and symptoms of disease (measured by high disease activity by certain disease activity indexes, persistently elevated C-reactive protein, inflammation on MRI, or rapid radiographic spinal progression)
- Symptoms/signs of disease that are considered problematic by the provider or patient
The definition was approved in January, and the manuscript is in the works, Dr. Poddubnyy said.
The GRAPPA project on PsA is still in its early stages, which so far has included a comprehensive literature review as well as a survey of GRAPPA members across 47 countries. The group is generally in agreement that two separate definitions for nonresponse to treatment are necessary, and that the “difficult-to-treat” definition — which identifies true refractory disease — should include objective signs of inflammation, Dr. Singla said.
Looking Forward
The next step of the ASAS project is to “define the pathway” from difficult-to-manage axSpA to treatment refractory disease, Dr. Poddubnyy said.
“What should be ruled out in order to exclude so-called noninflammatory causes of pain?” he continued. “It will require some Delphi exercises and [a] consensus approach.”
Proft anticipates that this treatment refractory definition in both axSpA and PsA will be most useful in research, rather than clinical practice.
“It is really important to have unified definition criteria to shape as homogeneous a cohort as possible,” he said, for future clinical trials in this population.
On the other hand, the complex/difficult-to-manage definition may be more useful for clinical practice, Dr. Proft thought.
“If you see a patient not responding to treatment, the easiest thing you can do would be to change treatment,” like swapping one biologic for another, Dr. Poddubnyy added, “but this would not be the right approach in every patient.” One goal of these initiatives is to give guidance on “what things should be looked after or excluded before you conclude this is biological [nonresponse],” he said.
Dr. Singla consults for AbbVie, Janssen, and UCB and received research funding from Eli Lilly. Dr. Poddubnyy disclosed serving as a speaker, consultant, and/or research grant recipient for multiple companies including AbbVie, Lilly, Merck Sharp and Dohme, Novartis, Pfizer, GlaxoSmithKline, Novartis, and UCB. Dr. Proft reported receiving research grants, consultant fees, or support for attending meetings and/or travel from Amgen, AbbVie, Bristol Myers Squibb, Celgene, Eli Lilly, Janssen, Merck Sharp and Dohme, Novartis, Pfizer, Roche, UCB, Medscape Medical News, Galapagos, and Hexal. Dr. Proft also participants on a data safety monitoring board or advisory board for AbbVie, Celgene, Janssen, Novartis, and UCB.
A version of this article appeared on Medscape.com.
Despite an expanding arsenal of disease-modifying antirheumatic drugs (DMARDs), many patients with axial spondyloarthritis (axSpA) and psoriatic arthritis (PsA) still struggle to reach remission even after trying multiple advanced treatments.
Now, international groups of experts are working to better define these “difficult-to-treat” patients to both inform care and improve selection of participants for future clinical trials.
“The idea is rather simple, and the need is relatively ubiquitous,” Denis Poddubnyy, MD, of the Charité – Universitätsmedizin Berlin and the German Rheumatism Research Center Berlin, both in Berlin, Germany, said in an interview. He is the co-primary investigator for the ongoing Assessment of SpondyloArthritis International Society (ASAS) project to develop a consensus definition of difficult-to-treat axSpA.
According to ASAS, only 40%-50% of patients with axSpA achieve a 40% improvement in ASAS response criteria (ASAS40), and few (10%-20%) achieve remission in the first 4-6 months of treatment.
“If you look into current clinical guidelines, you will see that there is no clear guidance,” on how to manage these patients, Dr. Poddubnyy continued. “In other similar recommendations for the treatment of axSpA, the only point which is clearly made with regards to nonresponders to effective anti-inflammatory treatment is to ‘check the diagnosis.’”
Multiple Reasons for Nonresponse
“While the term difficult-to-treat can refer to refractory disease, that is not the only reason why a patient might not be responding to medication. In fact, it’s likely that truly biologically refractory disease makes up only a fraction of cases that respond inadequately to treatment,” said Shikha Singla, MD, who directs the psoriatic arthritis program at the Medical College of Wisconsin in Milwaukee. She is also involved with the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) initiative to define Difficult-to-Treat and Complex-to-Manage PsA.
“Apart from the persistent articular and periarticular inflammation, there could be multiple noninflammatory factors that may be contributing to this treatment-resistant disease, including comorbid conditions such as obesity, cardiovascular disease, fibromyalgia, and even social factors such as limited access to medications,” she told this news organization. “Given these complexities, it is a matter of supreme importance to recognize and carefully delineate the elements that contribute to treatment refractory disease: Is it truly the inflammation, or are there noninflammatory components that are causing the treatment failure, or a combination of the two?”
Other contributing factors could be depression, hypersensitization, and comorbidities that prevent certain treatment approaches, added Fabian Proft, MD, also of Charité – Universitätsmedizin Berlin. Dr. Proft discussed these difficult-to-treat definition efforts at the recent Spondyloarthritis Research and Treatment Network (SPARTAN) annual meeting held in Cleveland. Patients also might not be taking their medication regularly and may be seeking alternative medicine approaches, he said.
“There is a quite clear consensus within the community” that differentiation between these two groups is needed, Dr. Proft said.
The Definitions
Terminology for these two groups can vary by professional society. The European Alliance of Associations for Rheumatology (EULAR) published a definition for “difficult-to-treat” rheumatoid arthritis (RA) that includes cases with “both inflammatory activity and/or noninflammatory complaints.”
The definition includes three criteria:
1) Treatment according to EULAR recommendation and failure of at least two biologic DMARDs (bDMARDs) or targeted synthetic DMARDs (tsDMARDs) (with different mechanisms of action) after failing conventional synthetic DMARD therapy (unless contraindicated)
2) Signs suggestive of active/progressive disease, including at least one of the following:
- Moderate disease activity (according to validated composite measures including joint counts)
- Signs (including acute phase reactants and imaging) and/or symptoms suggestive of active disease, whether joint-related or other
- Inability to taper glucocorticoid treatment
- Rapid radiographic progression (with or without signs of active disease)
- RA symptoms that are causing a reduction in quality of life
3) Symptom/sign management perceived as problematic by the rheumatologist or the patient
All three criteria must be met.
Both GRAPPA and ASAS plan to use the term “difficult-to-treat” or “treatment refractory” to describe true biologically refractory inflammatory disease and are categorizing the larger, heterogeneous group of nonresponders as “difficult-to-manage” (ASAS) or “complex-to-manage” (GRAPPA).
According to Dr. Poddubnyy, the agreed ASAS definition of difficult-to-manage has several similarities with EULAR’s RA definition, including three pillars:
- Treatment according to existing recommendations and failure of at least two different bDMARDs or tsDMARDs with different mechanisms
- Having signs and symptoms of disease (measured by high disease activity by certain disease activity indexes, persistently elevated C-reactive protein, inflammation on MRI, or rapid radiographic spinal progression)
- Symptoms/signs of disease that are considered problematic by the provider or patient
The definition was approved in January, and the manuscript is in the works, Dr. Poddubnyy said.
The GRAPPA project on PsA is still in its early stages, which so far has included a comprehensive literature review as well as a survey of GRAPPA members across 47 countries. The group is generally in agreement that two separate definitions for nonresponse to treatment are necessary, and that the “difficult-to-treat” definition — which identifies true refractory disease — should include objective signs of inflammation, Dr. Singla said.
Looking Forward
The next step of the ASAS project is to “define the pathway” from difficult-to-manage axSpA to treatment refractory disease, Dr. Poddubnyy said.
“What should be ruled out in order to exclude so-called noninflammatory causes of pain?” he continued. “It will require some Delphi exercises and [a] consensus approach.”
Proft anticipates that this treatment refractory definition in both axSpA and PsA will be most useful in research, rather than clinical practice.
“It is really important to have unified definition criteria to shape as homogeneous a cohort as possible,” he said, for future clinical trials in this population.
On the other hand, the complex/difficult-to-manage definition may be more useful for clinical practice, Dr. Proft thought.
“If you see a patient not responding to treatment, the easiest thing you can do would be to change treatment,” like swapping one biologic for another, Dr. Poddubnyy added, “but this would not be the right approach in every patient.” One goal of these initiatives is to give guidance on “what things should be looked after or excluded before you conclude this is biological [nonresponse],” he said.
Dr. Singla consults for AbbVie, Janssen, and UCB and received research funding from Eli Lilly. Dr. Poddubnyy disclosed serving as a speaker, consultant, and/or research grant recipient for multiple companies including AbbVie, Lilly, Merck Sharp and Dohme, Novartis, Pfizer, GlaxoSmithKline, Novartis, and UCB. Dr. Proft reported receiving research grants, consultant fees, or support for attending meetings and/or travel from Amgen, AbbVie, Bristol Myers Squibb, Celgene, Eli Lilly, Janssen, Merck Sharp and Dohme, Novartis, Pfizer, Roche, UCB, Medscape Medical News, Galapagos, and Hexal. Dr. Proft also participants on a data safety monitoring board or advisory board for AbbVie, Celgene, Janssen, Novartis, and UCB.
A version of this article appeared on Medscape.com.
FROM SPARTAN 2024
Clear Coverage Preference for Humira Over Biosimilars Seen in Most Medicare Part D Plans
Despite the influx of adalimumab biosimilars entering the market in 2023, Humira remains on top.
As of January 2024, both high and low concentrations of Humira, the originator adalimumab product, are nearly universally covered by Medicare Part D plans, while only half of these plans covered adalimumab biosimilars, according to a new research letter published online on June 6, 2024, in JAMA.
Of the plans that covered both, only 1.5% had lower-tier placement for biosimilars.
“This study of formulary coverage helps explain limited uptake of adalimumab biosimilars,” wrote the authors, led by Matthew J. Klebanoff, MD, of the University of Pennsylvania, Philadelphia. “Subpar biosimilar adoption will not only undermine their potential to reduce spending but also may deter investments in biosimilar development.”
The analysis included the formulary and enrollment files for 5609 Medicare Part D plans, representing 44.4 million beneficiaries. Drug list prices and whole acquisition costs (WAC) were pulled from the Red Book database, which provides prices for prescription and over-the-counter drugs as well as medical devices and supplies.
Nearly all (98.9%) of Part D plans covered the high-concentration (100 mg/mL) version of adalimumab with a WAC of $6923. This higher concentration is the most popular formulation of the drug, making up an estimated 85% of prescriptions. By comparison, 26.8% of plans covered the high-concentration version of adalimumab-adaz (Hyrimoz), with a WAC 5% less than the reference product.
The unbranded version of adalimumab-adaz, sold at an 81% discount from the reference product, was covered by 13% of plans. Only 4.6% of plans covered high-concentration adalimumab-bwwd (Hadlima), manufactured by Samsung Bioepis.
In January 2024, no high-concentration adalimumab biosimilar had been granted interchangeability status by the US Food and Drug Administration (FDA). Adalimumab-ryvk (Simlandi) was the first biosimilar to receive this designation and was launched in late May 2024.
Coverage for the lower concentration of adalimumab was nearly universal (98.7% of plans). About half of the plans (50.7%) covered adalimumab-adbm (Cyltezo) at a 5% discount. Adalimumab-adbm (Boehringer Ingelheim) was the first interchangeable Humira biosimilar approved by the FDA, but it is only interchangeable with the less popular, lower concentration formulation of adalimumab.
All other biosimilars were covered by less than 5% of Medicare Part D plans, even with some having a WAC 86% below Humira.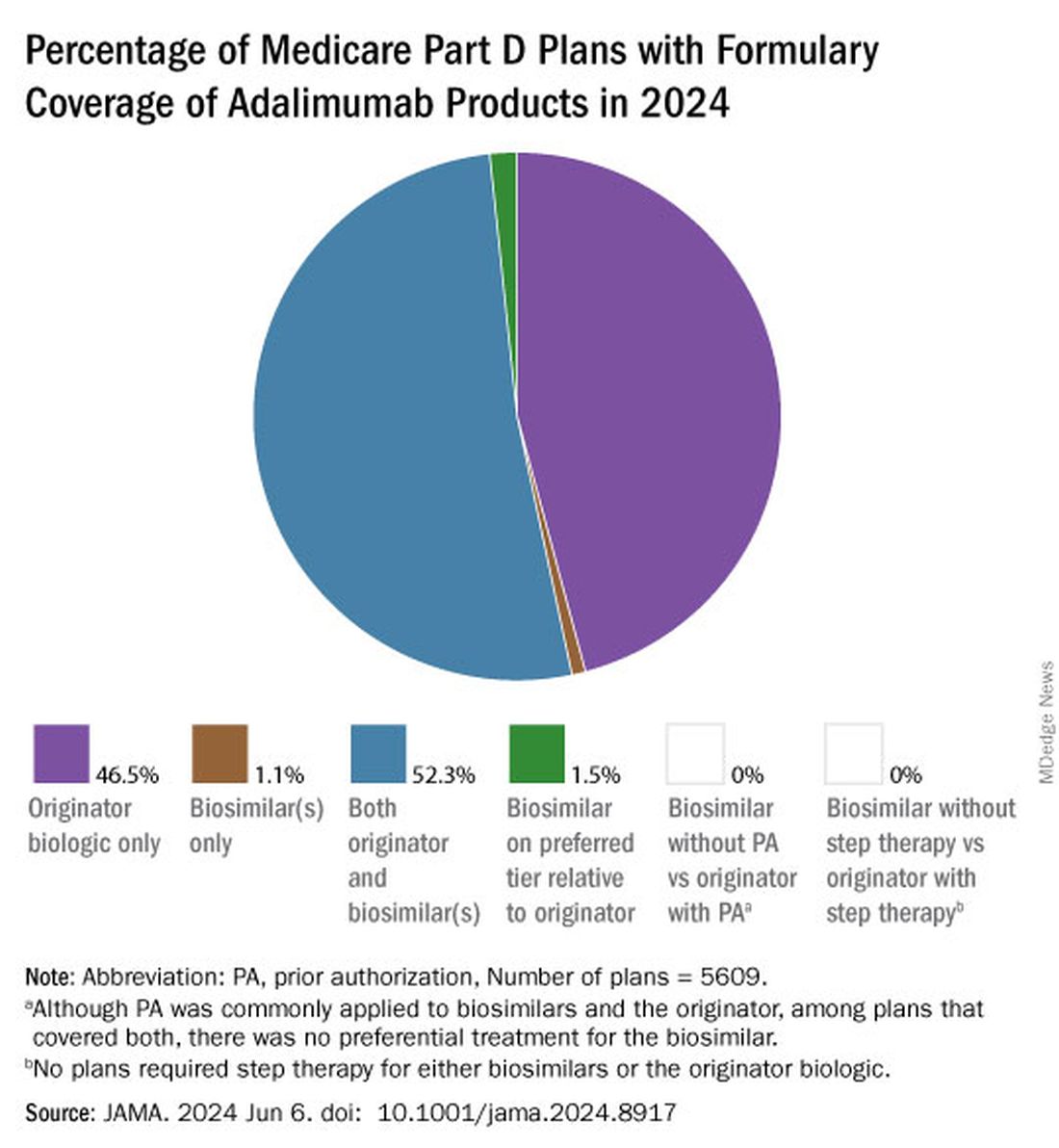
Few plans (1.5%) had biosimilars on preferred tiers compared with the reference product, and no plans used prior authorization to incentivize use of biosimilars. Most plans preferred the higher-priced version of adalimumab biosimilars, which appeals to pharmacy benefit managers who can therefore receive higher rebates, the authors noted.
“Ultimately, biosimilars’ true effect on spending will depend not on their list price but rather on their net price (after rebates) and their influence on originator biologics’ net price,” they wrote. They pointed to the 38% drop in Humira’s annual net price at the end of 2023 compared with the prior year.
“Despite this price decrease, biosimilars offer far greater potential savings: Several adalimumab biosimilars have list prices that are less than half of Humira’s net price,” the authors continued, and encouraged policy makers to mandate coverage for these lower-priced options.
Dr. Klebanoff was supported by a grant from the Health Resources and Services Administration. Two coauthors were supported by a grant from the National Institute on Aging. One author reported receiving consulting fees from AbbVie, which manufactures Humira.
A version of this article appeared on Medscape.com .
Despite the influx of adalimumab biosimilars entering the market in 2023, Humira remains on top.
As of January 2024, both high and low concentrations of Humira, the originator adalimumab product, are nearly universally covered by Medicare Part D plans, while only half of these plans covered adalimumab biosimilars, according to a new research letter published online on June 6, 2024, in JAMA.
Of the plans that covered both, only 1.5% had lower-tier placement for biosimilars.
“This study of formulary coverage helps explain limited uptake of adalimumab biosimilars,” wrote the authors, led by Matthew J. Klebanoff, MD, of the University of Pennsylvania, Philadelphia. “Subpar biosimilar adoption will not only undermine their potential to reduce spending but also may deter investments in biosimilar development.”
The analysis included the formulary and enrollment files for 5609 Medicare Part D plans, representing 44.4 million beneficiaries. Drug list prices and whole acquisition costs (WAC) were pulled from the Red Book database, which provides prices for prescription and over-the-counter drugs as well as medical devices and supplies.
Nearly all (98.9%) of Part D plans covered the high-concentration (100 mg/mL) version of adalimumab with a WAC of $6923. This higher concentration is the most popular formulation of the drug, making up an estimated 85% of prescriptions. By comparison, 26.8% of plans covered the high-concentration version of adalimumab-adaz (Hyrimoz), with a WAC 5% less than the reference product.
The unbranded version of adalimumab-adaz, sold at an 81% discount from the reference product, was covered by 13% of plans. Only 4.6% of plans covered high-concentration adalimumab-bwwd (Hadlima), manufactured by Samsung Bioepis.
In January 2024, no high-concentration adalimumab biosimilar had been granted interchangeability status by the US Food and Drug Administration (FDA). Adalimumab-ryvk (Simlandi) was the first biosimilar to receive this designation and was launched in late May 2024.
Coverage for the lower concentration of adalimumab was nearly universal (98.7% of plans). About half of the plans (50.7%) covered adalimumab-adbm (Cyltezo) at a 5% discount. Adalimumab-adbm (Boehringer Ingelheim) was the first interchangeable Humira biosimilar approved by the FDA, but it is only interchangeable with the less popular, lower concentration formulation of adalimumab.
All other biosimilars were covered by less than 5% of Medicare Part D plans, even with some having a WAC 86% below Humira.
Few plans (1.5%) had biosimilars on preferred tiers compared with the reference product, and no plans used prior authorization to incentivize use of biosimilars. Most plans preferred the higher-priced version of adalimumab biosimilars, which appeals to pharmacy benefit managers who can therefore receive higher rebates, the authors noted.
“Ultimately, biosimilars’ true effect on spending will depend not on their list price but rather on their net price (after rebates) and their influence on originator biologics’ net price,” they wrote. They pointed to the 38% drop in Humira’s annual net price at the end of 2023 compared with the prior year.
“Despite this price decrease, biosimilars offer far greater potential savings: Several adalimumab biosimilars have list prices that are less than half of Humira’s net price,” the authors continued, and encouraged policy makers to mandate coverage for these lower-priced options.
Dr. Klebanoff was supported by a grant from the Health Resources and Services Administration. Two coauthors were supported by a grant from the National Institute on Aging. One author reported receiving consulting fees from AbbVie, which manufactures Humira.
A version of this article appeared on Medscape.com .
Despite the influx of adalimumab biosimilars entering the market in 2023, Humira remains on top.
As of January 2024, both high and low concentrations of Humira, the originator adalimumab product, are nearly universally covered by Medicare Part D plans, while only half of these plans covered adalimumab biosimilars, according to a new research letter published online on June 6, 2024, in JAMA.
Of the plans that covered both, only 1.5% had lower-tier placement for biosimilars.
“This study of formulary coverage helps explain limited uptake of adalimumab biosimilars,” wrote the authors, led by Matthew J. Klebanoff, MD, of the University of Pennsylvania, Philadelphia. “Subpar biosimilar adoption will not only undermine their potential to reduce spending but also may deter investments in biosimilar development.”
The analysis included the formulary and enrollment files for 5609 Medicare Part D plans, representing 44.4 million beneficiaries. Drug list prices and whole acquisition costs (WAC) were pulled from the Red Book database, which provides prices for prescription and over-the-counter drugs as well as medical devices and supplies.
Nearly all (98.9%) of Part D plans covered the high-concentration (100 mg/mL) version of adalimumab with a WAC of $6923. This higher concentration is the most popular formulation of the drug, making up an estimated 85% of prescriptions. By comparison, 26.8% of plans covered the high-concentration version of adalimumab-adaz (Hyrimoz), with a WAC 5% less than the reference product.
The unbranded version of adalimumab-adaz, sold at an 81% discount from the reference product, was covered by 13% of plans. Only 4.6% of plans covered high-concentration adalimumab-bwwd (Hadlima), manufactured by Samsung Bioepis.
In January 2024, no high-concentration adalimumab biosimilar had been granted interchangeability status by the US Food and Drug Administration (FDA). Adalimumab-ryvk (Simlandi) was the first biosimilar to receive this designation and was launched in late May 2024.
Coverage for the lower concentration of adalimumab was nearly universal (98.7% of plans). About half of the plans (50.7%) covered adalimumab-adbm (Cyltezo) at a 5% discount. Adalimumab-adbm (Boehringer Ingelheim) was the first interchangeable Humira biosimilar approved by the FDA, but it is only interchangeable with the less popular, lower concentration formulation of adalimumab.
All other biosimilars were covered by less than 5% of Medicare Part D plans, even with some having a WAC 86% below Humira.
Few plans (1.5%) had biosimilars on preferred tiers compared with the reference product, and no plans used prior authorization to incentivize use of biosimilars. Most plans preferred the higher-priced version of adalimumab biosimilars, which appeals to pharmacy benefit managers who can therefore receive higher rebates, the authors noted.
“Ultimately, biosimilars’ true effect on spending will depend not on their list price but rather on their net price (after rebates) and their influence on originator biologics’ net price,” they wrote. They pointed to the 38% drop in Humira’s annual net price at the end of 2023 compared with the prior year.
“Despite this price decrease, biosimilars offer far greater potential savings: Several adalimumab biosimilars have list prices that are less than half of Humira’s net price,” the authors continued, and encouraged policy makers to mandate coverage for these lower-priced options.
Dr. Klebanoff was supported by a grant from the Health Resources and Services Administration. Two coauthors were supported by a grant from the National Institute on Aging. One author reported receiving consulting fees from AbbVie, which manufactures Humira.
A version of this article appeared on Medscape.com .
FROM JAMA
Spondyloarthritis Screening Study Finds ‘High Burden of Need’ in Patients With Inflammatory Bowel Disease
More than 40% of patients with inflammatory bowel disease (IBD) screened positive for joint pain symptomatic of spondyloarthritis (SpA), according to a new study.
Of these patients, 75% did not have any history of arthritis.
“What we know is that a substantial proportion of patients with IBD do report musculoskeletal symptoms, and inflammatory back pain stands out as being one of the more frequent symptoms reported,” said Reem Jan, MBBS, a rheumatologist at the University of Chicago Medicine. She presented the study findings during the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN) in Cleveland.
“Yet a minority of these patients are evaluated by rheumatologists. So that suggests there’s a high burden of need in the IBD population to have this joint pain evaluated and addressed,” she said during her presentation.
She presented preliminary data from an ongoing project to better understand the prevalence of inflammatory arthritis in IBD — estimates range from 17% to 39%— and the risk factors for developing arthritis in this patient population.
Study Details
Researchers enrolled patients from outpatient gastroenterology clinics or procedure units at NYU Langone Health, New York City; Brigham and Women’s Hospital, Boston; University of Colorado Anschutz Medical Campus, Aurora, Colorado; Mayo Clinic, Rochester, Minnesota; University of Chicago Medicine Inflammatory Bowel Disease Center, Chicago; and Icahn School of Medicine at Mount Sinai, New York City. Additional patients were recruited from Mercy Health, a community health system in Ohio.
Upon entry into the study, participants completed a survey documenting their history with joint pain. The survey combined questions from the DETAIL and the IBIS questionnaires.
Between January 2021 and December 2022, 669 patients joined the study. In total, 41% of patients (n = 275) screened positive.
“What really stood out to us was that of all the positive screens, only about a quarter of those patients were known to have SpA,” Dr. Jan said during her presentation. “[This] means 75% of the patients who screened positive were not known to have any type of arthritic disease.”
In addition, only 24% (n = 65) of all patients who screened positive — including those with a SpA diagnosis — had seen a rheumatologist in the previous year.
Among these patients, inflammatory back pain was the most commonly reported symptom, followed by painful swelling of peripheral joints and heel pain.
Excluding patients with a SpA diagnosis, researchers also investigated which characteristics were associated with a higher likelihood of screening positive in the questionnaire. The analysis, including 588 patients, identified the following risk factors:
- Female sex: Odds ratio (OR), 2.0; 95% CI, 1.4-2.9
- Older age: OR, 1.02; 95% CI, 1.01-1.4
- History of smoking: OR, 1.7; 95% CI, 1.1-2.6
- History of prior IBD-related surgery: OR, 1.60; 95% CI, 1.1-2.5
- History of biologic or small molecule therapy: OR, 2.3; 95% CI, 1.4-4.0
Future Directions
Commenting on the study, Mark Hwang, MD, a rheumatologist at UTHealth Houston, noted that it was “very interesting to see the fairly large, positive rates” of joint pain in patients with IBD, which certainly have clinical implications. However, it is not yet known if any of these patients went on to be diagnosed with SpA.
Jan noted that potential next steps include a follow-up analysis of patients who screened positive to see how many went on to see a rheumatologist and which patients were ultimately diagnosed with SpA or other inflammatory arthritis conditions.
These findings are a first step, Dr. Hwang said, and will likely “help further establish some of the validity of these questionnaires by testing in different patient populations,” he noted.
The ultimate goal is to “develop really good strategies to risk stratify IBD patients with the greatest need of rheumatologist consultation,” Dr. Jan said. “We certainly don’t want to see all these patients, so how can we figure out who really needs to be seen?”
Funding information was not available for this study. Dr. Hwang is conducting two clinical trials for psoriatic arthritis sponsored by Janssen and Eli Lilly. Dr. Jan reported no relevant disclosures.
A version of this article appeared on Medscape.com.
More than 40% of patients with inflammatory bowel disease (IBD) screened positive for joint pain symptomatic of spondyloarthritis (SpA), according to a new study.
Of these patients, 75% did not have any history of arthritis.
“What we know is that a substantial proportion of patients with IBD do report musculoskeletal symptoms, and inflammatory back pain stands out as being one of the more frequent symptoms reported,” said Reem Jan, MBBS, a rheumatologist at the University of Chicago Medicine. She presented the study findings during the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN) in Cleveland.
“Yet a minority of these patients are evaluated by rheumatologists. So that suggests there’s a high burden of need in the IBD population to have this joint pain evaluated and addressed,” she said during her presentation.
She presented preliminary data from an ongoing project to better understand the prevalence of inflammatory arthritis in IBD — estimates range from 17% to 39%— and the risk factors for developing arthritis in this patient population.
Study Details
Researchers enrolled patients from outpatient gastroenterology clinics or procedure units at NYU Langone Health, New York City; Brigham and Women’s Hospital, Boston; University of Colorado Anschutz Medical Campus, Aurora, Colorado; Mayo Clinic, Rochester, Minnesota; University of Chicago Medicine Inflammatory Bowel Disease Center, Chicago; and Icahn School of Medicine at Mount Sinai, New York City. Additional patients were recruited from Mercy Health, a community health system in Ohio.
Upon entry into the study, participants completed a survey documenting their history with joint pain. The survey combined questions from the DETAIL and the IBIS questionnaires.
Between January 2021 and December 2022, 669 patients joined the study. In total, 41% of patients (n = 275) screened positive.
“What really stood out to us was that of all the positive screens, only about a quarter of those patients were known to have SpA,” Dr. Jan said during her presentation. “[This] means 75% of the patients who screened positive were not known to have any type of arthritic disease.”
In addition, only 24% (n = 65) of all patients who screened positive — including those with a SpA diagnosis — had seen a rheumatologist in the previous year.
Among these patients, inflammatory back pain was the most commonly reported symptom, followed by painful swelling of peripheral joints and heel pain.
Excluding patients with a SpA diagnosis, researchers also investigated which characteristics were associated with a higher likelihood of screening positive in the questionnaire. The analysis, including 588 patients, identified the following risk factors:
- Female sex: Odds ratio (OR), 2.0; 95% CI, 1.4-2.9
- Older age: OR, 1.02; 95% CI, 1.01-1.4
- History of smoking: OR, 1.7; 95% CI, 1.1-2.6
- History of prior IBD-related surgery: OR, 1.60; 95% CI, 1.1-2.5
- History of biologic or small molecule therapy: OR, 2.3; 95% CI, 1.4-4.0
Future Directions
Commenting on the study, Mark Hwang, MD, a rheumatologist at UTHealth Houston, noted that it was “very interesting to see the fairly large, positive rates” of joint pain in patients with IBD, which certainly have clinical implications. However, it is not yet known if any of these patients went on to be diagnosed with SpA.
Jan noted that potential next steps include a follow-up analysis of patients who screened positive to see how many went on to see a rheumatologist and which patients were ultimately diagnosed with SpA or other inflammatory arthritis conditions.
These findings are a first step, Dr. Hwang said, and will likely “help further establish some of the validity of these questionnaires by testing in different patient populations,” he noted.
The ultimate goal is to “develop really good strategies to risk stratify IBD patients with the greatest need of rheumatologist consultation,” Dr. Jan said. “We certainly don’t want to see all these patients, so how can we figure out who really needs to be seen?”
Funding information was not available for this study. Dr. Hwang is conducting two clinical trials for psoriatic arthritis sponsored by Janssen and Eli Lilly. Dr. Jan reported no relevant disclosures.
A version of this article appeared on Medscape.com.
More than 40% of patients with inflammatory bowel disease (IBD) screened positive for joint pain symptomatic of spondyloarthritis (SpA), according to a new study.
Of these patients, 75% did not have any history of arthritis.
“What we know is that a substantial proportion of patients with IBD do report musculoskeletal symptoms, and inflammatory back pain stands out as being one of the more frequent symptoms reported,” said Reem Jan, MBBS, a rheumatologist at the University of Chicago Medicine. She presented the study findings during the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN) in Cleveland.
“Yet a minority of these patients are evaluated by rheumatologists. So that suggests there’s a high burden of need in the IBD population to have this joint pain evaluated and addressed,” she said during her presentation.
She presented preliminary data from an ongoing project to better understand the prevalence of inflammatory arthritis in IBD — estimates range from 17% to 39%— and the risk factors for developing arthritis in this patient population.
Study Details
Researchers enrolled patients from outpatient gastroenterology clinics or procedure units at NYU Langone Health, New York City; Brigham and Women’s Hospital, Boston; University of Colorado Anschutz Medical Campus, Aurora, Colorado; Mayo Clinic, Rochester, Minnesota; University of Chicago Medicine Inflammatory Bowel Disease Center, Chicago; and Icahn School of Medicine at Mount Sinai, New York City. Additional patients were recruited from Mercy Health, a community health system in Ohio.
Upon entry into the study, participants completed a survey documenting their history with joint pain. The survey combined questions from the DETAIL and the IBIS questionnaires.
Between January 2021 and December 2022, 669 patients joined the study. In total, 41% of patients (n = 275) screened positive.
“What really stood out to us was that of all the positive screens, only about a quarter of those patients were known to have SpA,” Dr. Jan said during her presentation. “[This] means 75% of the patients who screened positive were not known to have any type of arthritic disease.”
In addition, only 24% (n = 65) of all patients who screened positive — including those with a SpA diagnosis — had seen a rheumatologist in the previous year.
Among these patients, inflammatory back pain was the most commonly reported symptom, followed by painful swelling of peripheral joints and heel pain.
Excluding patients with a SpA diagnosis, researchers also investigated which characteristics were associated with a higher likelihood of screening positive in the questionnaire. The analysis, including 588 patients, identified the following risk factors:
- Female sex: Odds ratio (OR), 2.0; 95% CI, 1.4-2.9
- Older age: OR, 1.02; 95% CI, 1.01-1.4
- History of smoking: OR, 1.7; 95% CI, 1.1-2.6
- History of prior IBD-related surgery: OR, 1.60; 95% CI, 1.1-2.5
- History of biologic or small molecule therapy: OR, 2.3; 95% CI, 1.4-4.0
Future Directions
Commenting on the study, Mark Hwang, MD, a rheumatologist at UTHealth Houston, noted that it was “very interesting to see the fairly large, positive rates” of joint pain in patients with IBD, which certainly have clinical implications. However, it is not yet known if any of these patients went on to be diagnosed with SpA.
Jan noted that potential next steps include a follow-up analysis of patients who screened positive to see how many went on to see a rheumatologist and which patients were ultimately diagnosed with SpA or other inflammatory arthritis conditions.
These findings are a first step, Dr. Hwang said, and will likely “help further establish some of the validity of these questionnaires by testing in different patient populations,” he noted.
The ultimate goal is to “develop really good strategies to risk stratify IBD patients with the greatest need of rheumatologist consultation,” Dr. Jan said. “We certainly don’t want to see all these patients, so how can we figure out who really needs to be seen?”
Funding information was not available for this study. Dr. Hwang is conducting two clinical trials for psoriatic arthritis sponsored by Janssen and Eli Lilly. Dr. Jan reported no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM SPARTAN 2024
High NSAID Use in Patients With Axial Spondyloarthritis May Not Raise Risk for Hypertension
TOPLINE:
Patients with axial spondyloarthritis (axSpA) who reported high nonsteroidal anti-inflammatory drug (NSAID) use did not have a higher risk for hypertension than those who reported low NSAID use.
METHODOLOGY:
- NSAIDs are first-line therapy for axSpA and are associated with a high risk for hypertension in the general population, but it’s unknown whether NSAID use increases the risk for hypertension in patients with axSpA, who are already at higher risk for cardiovascular disease and hypertension than the general population
- This study used the DESIR cohort, a multicenter cohort of patients with recent-onset axSpA in France, including 631 individuals aged 18-50 years who did not have hypertension at baseline and had 6 years of follow-up.
- NSAID use was evaluated at each follow-up visit, using the Assessment of Spondyloarthritis International Society NSAID index.
- A score ≥ 50 was categorized as high use, and a score < 50 was considered low use.
- The primary outcome was hypertension, defined by the use of antihypertensive medication, self-reported hypertension, and/or systolic blood pressure (BP) ≥ 140 mm Hg or diastolic BP ≥ 90 mm Hg on at least two visits.
TAKEAWAY:
- A total of 39% of patients were categorized as high NSAID users.
- Over 6 years of follow-up, 70 patients (11%) developed hypertension.
- There was no significant association between high NSAID use and the risk for hypertension.
IN PRACTICE:
The study is too preliminary to have practice application.
SOURCE:
The research was led and presented by Jose Meade-Aguilar, MD, of Boston University School of Medicine, at the Spondyloarthritis Research and Treatment Network (SPARTAN) 2024 annual meeting in Cleveland.
LIMITATIONS:
The study had a low number of hypertension events, which could be due to the younger age of participants and earlier disease stage. The study was observational, so residual or unmeasured confounding is possible.
DISCLOSURES:
The DESIR cohort study is financially supported by unrestricted grants from both the French Society for Rheumatology and Pfizer France. One coauthor reported receiving research grants and/or consultancy fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp & Dohme, Novartis, Pfizer, UCB, and Sanofi. Another coauthor reported receiving research grants from UCB and consulting fees from Eli Lilly, Novartis, Pfizer, and UCB. The remaining authors had no financial, relational, or commercial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients with axial spondyloarthritis (axSpA) who reported high nonsteroidal anti-inflammatory drug (NSAID) use did not have a higher risk for hypertension than those who reported low NSAID use.
METHODOLOGY:
- NSAIDs are first-line therapy for axSpA and are associated with a high risk for hypertension in the general population, but it’s unknown whether NSAID use increases the risk for hypertension in patients with axSpA, who are already at higher risk for cardiovascular disease and hypertension than the general population
- This study used the DESIR cohort, a multicenter cohort of patients with recent-onset axSpA in France, including 631 individuals aged 18-50 years who did not have hypertension at baseline and had 6 years of follow-up.
- NSAID use was evaluated at each follow-up visit, using the Assessment of Spondyloarthritis International Society NSAID index.
- A score ≥ 50 was categorized as high use, and a score < 50 was considered low use.
- The primary outcome was hypertension, defined by the use of antihypertensive medication, self-reported hypertension, and/or systolic blood pressure (BP) ≥ 140 mm Hg or diastolic BP ≥ 90 mm Hg on at least two visits.
TAKEAWAY:
- A total of 39% of patients were categorized as high NSAID users.
- Over 6 years of follow-up, 70 patients (11%) developed hypertension.
- There was no significant association between high NSAID use and the risk for hypertension.
IN PRACTICE:
The study is too preliminary to have practice application.
SOURCE:
The research was led and presented by Jose Meade-Aguilar, MD, of Boston University School of Medicine, at the Spondyloarthritis Research and Treatment Network (SPARTAN) 2024 annual meeting in Cleveland.
LIMITATIONS:
The study had a low number of hypertension events, which could be due to the younger age of participants and earlier disease stage. The study was observational, so residual or unmeasured confounding is possible.
DISCLOSURES:
The DESIR cohort study is financially supported by unrestricted grants from both the French Society for Rheumatology and Pfizer France. One coauthor reported receiving research grants and/or consultancy fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp & Dohme, Novartis, Pfizer, UCB, and Sanofi. Another coauthor reported receiving research grants from UCB and consulting fees from Eli Lilly, Novartis, Pfizer, and UCB. The remaining authors had no financial, relational, or commercial conflicts to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients with axial spondyloarthritis (axSpA) who reported high nonsteroidal anti-inflammatory drug (NSAID) use did not have a higher risk for hypertension than those who reported low NSAID use.
METHODOLOGY:
- NSAIDs are first-line therapy for axSpA and are associated with a high risk for hypertension in the general population, but it’s unknown whether NSAID use increases the risk for hypertension in patients with axSpA, who are already at higher risk for cardiovascular disease and hypertension than the general population
- This study used the DESIR cohort, a multicenter cohort of patients with recent-onset axSpA in France, including 631 individuals aged 18-50 years who did not have hypertension at baseline and had 6 years of follow-up.
- NSAID use was evaluated at each follow-up visit, using the Assessment of Spondyloarthritis International Society NSAID index.
- A score ≥ 50 was categorized as high use, and a score < 50 was considered low use.
- The primary outcome was hypertension, defined by the use of antihypertensive medication, self-reported hypertension, and/or systolic blood pressure (BP) ≥ 140 mm Hg or diastolic BP ≥ 90 mm Hg on at least two visits.
TAKEAWAY:
- A total of 39% of patients were categorized as high NSAID users.
- Over 6 years of follow-up, 70 patients (11%) developed hypertension.
- There was no significant association between high NSAID use and the risk for hypertension.
IN PRACTICE:
The study is too preliminary to have practice application.
SOURCE:
The research was led and presented by Jose Meade-Aguilar, MD, of Boston University School of Medicine, at the Spondyloarthritis Research and Treatment Network (SPARTAN) 2024 annual meeting in Cleveland.
LIMITATIONS:
The study had a low number of hypertension events, which could be due to the younger age of participants and earlier disease stage. The study was observational, so residual or unmeasured confounding is possible.
DISCLOSURES:
The DESIR cohort study is financially supported by unrestricted grants from both the French Society for Rheumatology and Pfizer France. One coauthor reported receiving research grants and/or consultancy fees from AbbVie, Eli Lilly, Galapagos, Janssen, Merck Sharp & Dohme, Novartis, Pfizer, UCB, and Sanofi. Another coauthor reported receiving research grants from UCB and consulting fees from Eli Lilly, Novartis, Pfizer, and UCB. The remaining authors had no financial, relational, or commercial conflicts to disclose.
A version of this article appeared on Medscape.com.