User login
Skin Disease Education Foundation (SDEF): Las Vegas Dermatology Seminar
Novel treatments for AKN include laser hair removal, UVB
LAS VEGAS – Bothersome and even disfiguring for some, acne keloidalis nuchae (AKN) is a mysterious but common skin disorder mostly affecting men of African descent.
But an accurate clinical diagnosis and a flexible treatment approach can boost treatment success, said Dr. Andrew F. Alexis, chair of the department of dermatology, and director of the Skin of Color Center, Mount Sinai St Luke’s and Mount Sinai Roosevelt, New York.

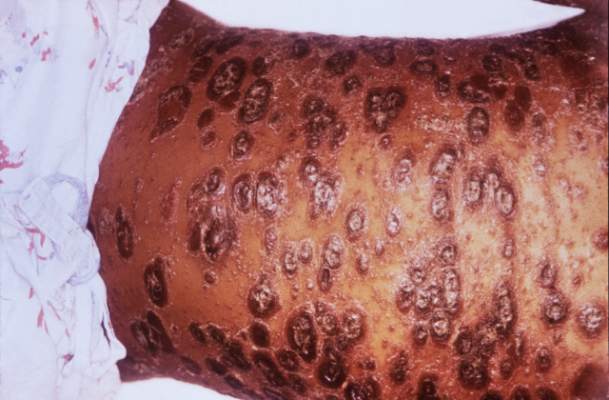
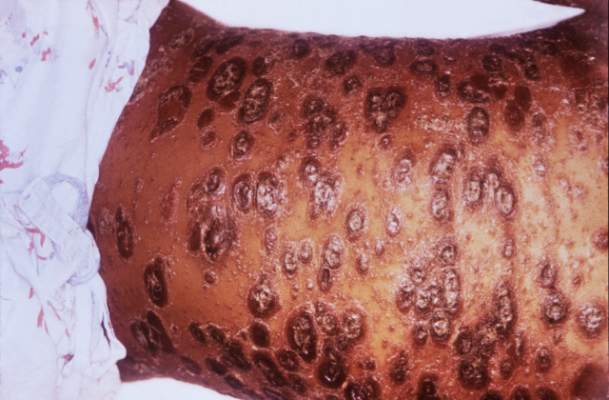
Speaking at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Alexis that the diagnosis can be made clinically, without the need for biopsies or skin scrapings. The condition is characterized by fibrotic, follicular papules, usually at the nape of the neck and on the occipital scalp. However, in more severe cases, the papules coalesce into a larger plaque. Occasionally, the characteristic scarring alopecia and keloidlike papules can be seen more toward the vertex of the scalp.
“We don’t really, truly know what the etiology of acne keloidalis nuchae is,” said Dr. Alexis, noting that many etiologies have been proposed. Some say it’s an epithelial elimination disorder, or a variant of lichen simplex chronicus. Many lay people may feel this is an ingrown hair disorder, but histopathologic studies have refuted this theory. These studies have also found no evidence of bacterial overgrowth in affected areas.
A newer and leading hypothesis is that AKN’s primary mechanism is fibrosis secondary to a mechanically induced folliculitis. At the very least, mechanical forces, even if they don’t cause the disorder, “certainly can exacerbate acne keloidalis nuchae, and short haircuts using electrical clippers may be a factor,” Dr. Alexis said. Support for this hypothesis can be found in two South African cross-sectional studies of nearly 2,000 men and boys: 86% of those with AKN reported receiving short haircuts with clippers. Among the adults reporting at least one episode of bleeding during a haircut, the odds ratio for having AKN was 3.45 (Int J Dermatol. 2011 Oct;50[10]:1212-6).

Therapy is multimodal, with some behavioral components, including avoidance of mechanical factors that can exacerbate AKN. In addition to low haircuts, tight-fitting caps and picking or scratching at the papules can worsen the condition.
Few studies exist to support one treatment regime over another for AKN, Dr. Alexis said. One small open label study of 20 individuals evaluated clobetasol 0.05% foam twice daily for two cycles of 2 weeks on and 2 weeks off treatment. Patients with persistent disease were then stepped down to 2 weeks of betamethasone valerate 0.12% foam twice daily. Overall, the mean papule/pustule count dropped by more than half, from 25 at baseline to 10 at 12 weeks, Dr. Alexis said (Cutis. 2005;75:317-21).
For larger papules and coalescent plaques, Dr. Alexis recommends intralesional triamcinolone acetonide at a concentration of 20-40mg/mL. “Don’t undertreat” and be sure to inject into, rather than under the lesion, he said. Concomitant topical class 1 or class 2 corticosteroids, such as clobetasol or fluocinonide, can be used along with injections. Addition of a topical antibiotic such as clindamycin can also accelerate resolution in his anecdotal experience.
Further recommendations based on practice experience include once-daily chlorhexidine washes of the affected area, as well as the addition of an oral tetracycline, such as doxycycline, when pustules are present or with more severe cases, Dr. Alexis said.
For some severely affected patients, surgical therapy may become the best treatment option. “You can inject all day long and still have disfiguring keloidlike plaque” in some patients with severe disease, he noted. Case series of both primary closure and healing by secondary intention have both shown good results. “Whichever camp you belong to, the key is to use a horizontal ellipse that includes the posterior hairline, and the depth of the excision must be down to the dermal-subcutaneous junction,” he said.

More recently, laser hair removal has been studied as a treatment alternative for AKN, Dr. Alexis pointed out. In a pilot study of 16 patients with AKN who received five sessions of laser hair removal, all had a marked reduction in papules and pustules at one year of follow-up (Eur J Dermatol. 2012 Sep-Oct;22[5]:645-50).
Another novel treatment approach used targeted UVB light with good results in a small split-scalp study. Pathology suggested the targeted skin was undergoing active matrix remodeling as a result of the UVB therapy (Br J Dermatol. 2014 Nov;171[5]:1156-63).
Dr. Alexis disclosed that he has received grants and research support from Allergan and Novartis, and speaker honoraria from Cipla. He has received consulting fees from Acclaris Therapeutics, Allergan, Amgen, Anacor, Bayer, Galderma, Johnson & Johnson, Leo, L’Oreal, Roche, Schick, Suneva, and Valeant.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Bothersome and even disfiguring for some, acne keloidalis nuchae (AKN) is a mysterious but common skin disorder mostly affecting men of African descent.
But an accurate clinical diagnosis and a flexible treatment approach can boost treatment success, said Dr. Andrew F. Alexis, chair of the department of dermatology, and director of the Skin of Color Center, Mount Sinai St Luke’s and Mount Sinai Roosevelt, New York.
Speaking at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Alexis that the diagnosis can be made clinically, without the need for biopsies or skin scrapings. The condition is characterized by fibrotic, follicular papules, usually at the nape of the neck and on the occipital scalp. However, in more severe cases, the papules coalesce into a larger plaque. Occasionally, the characteristic scarring alopecia and keloidlike papules can be seen more toward the vertex of the scalp.
“We don’t really, truly know what the etiology of acne keloidalis nuchae is,” said Dr. Alexis, noting that many etiologies have been proposed. Some say it’s an epithelial elimination disorder, or a variant of lichen simplex chronicus. Many lay people may feel this is an ingrown hair disorder, but histopathologic studies have refuted this theory. These studies have also found no evidence of bacterial overgrowth in affected areas.
A newer and leading hypothesis is that AKN’s primary mechanism is fibrosis secondary to a mechanically induced folliculitis. At the very least, mechanical forces, even if they don’t cause the disorder, “certainly can exacerbate acne keloidalis nuchae, and short haircuts using electrical clippers may be a factor,” Dr. Alexis said. Support for this hypothesis can be found in two South African cross-sectional studies of nearly 2,000 men and boys: 86% of those with AKN reported receiving short haircuts with clippers. Among the adults reporting at least one episode of bleeding during a haircut, the odds ratio for having AKN was 3.45 (Int J Dermatol. 2011 Oct;50[10]:1212-6).
Therapy is multimodal, with some behavioral components, including avoidance of mechanical factors that can exacerbate AKN. In addition to low haircuts, tight-fitting caps and picking or scratching at the papules can worsen the condition.
Few studies exist to support one treatment regime over another for AKN, Dr. Alexis said. One small open label study of 20 individuals evaluated clobetasol 0.05% foam twice daily for two cycles of 2 weeks on and 2 weeks off treatment. Patients with persistent disease were then stepped down to 2 weeks of betamethasone valerate 0.12% foam twice daily. Overall, the mean papule/pustule count dropped by more than half, from 25 at baseline to 10 at 12 weeks, Dr. Alexis said (Cutis. 2005;75:317-21).
For larger papules and coalescent plaques, Dr. Alexis recommends intralesional triamcinolone acetonide at a concentration of 20-40mg/mL. “Don’t undertreat” and be sure to inject into, rather than under the lesion, he said. Concomitant topical class 1 or class 2 corticosteroids, such as clobetasol or fluocinonide, can be used along with injections. Addition of a topical antibiotic such as clindamycin can also accelerate resolution in his anecdotal experience.
Further recommendations based on practice experience include once-daily chlorhexidine washes of the affected area, as well as the addition of an oral tetracycline, such as doxycycline, when pustules are present or with more severe cases, Dr. Alexis said.
For some severely affected patients, surgical therapy may become the best treatment option. “You can inject all day long and still have disfiguring keloidlike plaque” in some patients with severe disease, he noted. Case series of both primary closure and healing by secondary intention have both shown good results. “Whichever camp you belong to, the key is to use a horizontal ellipse that includes the posterior hairline, and the depth of the excision must be down to the dermal-subcutaneous junction,” he said.
More recently, laser hair removal has been studied as a treatment alternative for AKN, Dr. Alexis pointed out. In a pilot study of 16 patients with AKN who received five sessions of laser hair removal, all had a marked reduction in papules and pustules at one year of follow-up (Eur J Dermatol. 2012 Sep-Oct;22[5]:645-50).
Another novel treatment approach used targeted UVB light with good results in a small split-scalp study. Pathology suggested the targeted skin was undergoing active matrix remodeling as a result of the UVB therapy (Br J Dermatol. 2014 Nov;171[5]:1156-63).
Dr. Alexis disclosed that he has received grants and research support from Allergan and Novartis, and speaker honoraria from Cipla. He has received consulting fees from Acclaris Therapeutics, Allergan, Amgen, Anacor, Bayer, Galderma, Johnson & Johnson, Leo, L’Oreal, Roche, Schick, Suneva, and Valeant.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Bothersome and even disfiguring for some, acne keloidalis nuchae (AKN) is a mysterious but common skin disorder mostly affecting men of African descent.
But an accurate clinical diagnosis and a flexible treatment approach can boost treatment success, said Dr. Andrew F. Alexis, chair of the department of dermatology, and director of the Skin of Color Center, Mount Sinai St Luke’s and Mount Sinai Roosevelt, New York.
Speaking at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Alexis that the diagnosis can be made clinically, without the need for biopsies or skin scrapings. The condition is characterized by fibrotic, follicular papules, usually at the nape of the neck and on the occipital scalp. However, in more severe cases, the papules coalesce into a larger plaque. Occasionally, the characteristic scarring alopecia and keloidlike papules can be seen more toward the vertex of the scalp.
“We don’t really, truly know what the etiology of acne keloidalis nuchae is,” said Dr. Alexis, noting that many etiologies have been proposed. Some say it’s an epithelial elimination disorder, or a variant of lichen simplex chronicus. Many lay people may feel this is an ingrown hair disorder, but histopathologic studies have refuted this theory. These studies have also found no evidence of bacterial overgrowth in affected areas.
A newer and leading hypothesis is that AKN’s primary mechanism is fibrosis secondary to a mechanically induced folliculitis. At the very least, mechanical forces, even if they don’t cause the disorder, “certainly can exacerbate acne keloidalis nuchae, and short haircuts using electrical clippers may be a factor,” Dr. Alexis said. Support for this hypothesis can be found in two South African cross-sectional studies of nearly 2,000 men and boys: 86% of those with AKN reported receiving short haircuts with clippers. Among the adults reporting at least one episode of bleeding during a haircut, the odds ratio for having AKN was 3.45 (Int J Dermatol. 2011 Oct;50[10]:1212-6).
Therapy is multimodal, with some behavioral components, including avoidance of mechanical factors that can exacerbate AKN. In addition to low haircuts, tight-fitting caps and picking or scratching at the papules can worsen the condition.
Few studies exist to support one treatment regime over another for AKN, Dr. Alexis said. One small open label study of 20 individuals evaluated clobetasol 0.05% foam twice daily for two cycles of 2 weeks on and 2 weeks off treatment. Patients with persistent disease were then stepped down to 2 weeks of betamethasone valerate 0.12% foam twice daily. Overall, the mean papule/pustule count dropped by more than half, from 25 at baseline to 10 at 12 weeks, Dr. Alexis said (Cutis. 2005;75:317-21).
For larger papules and coalescent plaques, Dr. Alexis recommends intralesional triamcinolone acetonide at a concentration of 20-40mg/mL. “Don’t undertreat” and be sure to inject into, rather than under the lesion, he said. Concomitant topical class 1 or class 2 corticosteroids, such as clobetasol or fluocinonide, can be used along with injections. Addition of a topical antibiotic such as clindamycin can also accelerate resolution in his anecdotal experience.
Further recommendations based on practice experience include once-daily chlorhexidine washes of the affected area, as well as the addition of an oral tetracycline, such as doxycycline, when pustules are present or with more severe cases, Dr. Alexis said.
For some severely affected patients, surgical therapy may become the best treatment option. “You can inject all day long and still have disfiguring keloidlike plaque” in some patients with severe disease, he noted. Case series of both primary closure and healing by secondary intention have both shown good results. “Whichever camp you belong to, the key is to use a horizontal ellipse that includes the posterior hairline, and the depth of the excision must be down to the dermal-subcutaneous junction,” he said.
More recently, laser hair removal has been studied as a treatment alternative for AKN, Dr. Alexis pointed out. In a pilot study of 16 patients with AKN who received five sessions of laser hair removal, all had a marked reduction in papules and pustules at one year of follow-up (Eur J Dermatol. 2012 Sep-Oct;22[5]:645-50).
Another novel treatment approach used targeted UVB light with good results in a small split-scalp study. Pathology suggested the targeted skin was undergoing active matrix remodeling as a result of the UVB therapy (Br J Dermatol. 2014 Nov;171[5]:1156-63).
Dr. Alexis disclosed that he has received grants and research support from Allergan and Novartis, and speaker honoraria from Cipla. He has received consulting fees from Acclaris Therapeutics, Allergan, Amgen, Anacor, Bayer, Galderma, Johnson & Johnson, Leo, L’Oreal, Roche, Schick, Suneva, and Valeant.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR

For skin rejuvenation, pick the right light-based technique
LAS VEGAS – Technologies to address the many skin changes associated with photoaging run the gamut from nonablative to ablative – and choosing the right technology for a given patient is a balancing act, according to Dr. Mathew Avram.
“Basically, it’s a trade-off between increased efficacy and increased side effects and downtime,” Dr. Avram said at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.

Dr. Avram, director of the Massachusetts General Hospital dermatology, laser, and cosmetic center, Boston, said that traditional resurfacing remains the preferred method for repairing photodamaged skin. “One treatment provides reproducible, excellent results,” but at the cost of a significant amount of wound care and prolonged downtime. Potential adverse effects also include clear lines of demarcation with improper feathering, prolonged erythema, permanent hypopigmentation, infection, and scarring, he added.
For these reasons, the popularity of traditional resurfacing to treat photodamaged skin has declined over time as nonablative and intermediate techniques have arisen.
Intense pulsed light (IPL) is a nonlaser, nonablative technique that can produce overall skin rejuvenation, a “side effect” that patients often notice after they receive IPL for vascular lesions or hyperpigmentation. The benefits tend to be modest, even after several treatments, so this is not usually performed as a standalone technique for skin laxity or rhytides.
Nonablative fractional lasers act by creating thousands of microscopic wounds that are “columns of thermal coagulation,” leaving an intact stratum corneum, said Dr. Avram, who is also faculty director for laser and cosmetic training, Harvard Medical School, Boston.
The most common reason for treatment with a nonablative laser is mild to moderate wrinkles, though it can also be used for various pigmentation issues, as well as acne, surgical, and burn scars.
Although side effects are typically minor, the devices can be used off face, and there’s no worry about lines of demarcation; improvement is also more modest and will happen only with multiple treatments. “Fractional treatments give you fractional results,” Dr. Avram commented.
“You want to think about your treatment in terms of the pathology of what you’re treating,” he added, noting that fractional resurfacing can target both epidermal and dermal conditions. Examples of epidermal conditions that benefit from superficial treatment include dermatoheliosis, lentigines, and melasma.
Acne scars and deep wrinkles should receive deeper treatment in order to create thermal damage to the dermis proper, which, over a period of months, will trigger collagen remodeling and new collagen formation. Pulse energy will determine the depth and width of the zone of coagulation in the skin, so higher energy should be used with deeper skin pathology, Dr. Avram said.
Dermatologists also need to consider density of treatment – what percent of the skin is treated. “These devices go from about 5% to about 48% of skin coverage,” and increased density is really what increases the intensity of treatment, he noted. High-density treatment will result in more redness and swelling and has a greater potential for hyperpigmentation, but will not necessarily yield increased benefit in treatment outcomes, he added.
Pretreatment considerations should include assessing the patient’s expectations and availability for downtime post procedure. Treatment planning should also consider the patient’s skin type and probability for sun exposure. Patients should know they will see only partial improvement in wrinkles, scars, and pigmentation, and should expect some discomfort during the procedure and some side effects and healing time post procedure. Patients with a history of herpes labialis should receive valacyclovir 500 mg twice daily, beginning the day before treatment and continuing for 5-7 days, Dr. Avram said.
Cold-air cooling makes the treatment both safer and more comfortable, he pointed out. Topical compounded anesthesia including higher percentages of lidocaine and tetracaine can also be effective. Though local injected anesthesia can be effective in focal treatment of scars, the injection should be deep, and treatment should not begin immediately. This allows the lidocaine to disperse, minimizing the risk of ulceration from the thermal instability that a depot of lidocaine could cause, he said.
Fractional lasers can also be effective for treating background dermatoheliosis, as opposed to targeted treatment of individual lentigines. “Fractional is going to be great for clearing background damage,” Dr. Avram said.
A hybrid technique called ablative fractional photothermolysis creates tiny columns of ablation, while leaving the surrounding untreated tissue available as a reservoir for rapid healing. This technique will improve the more severe wrinkles that nonablative treatments don’t help, with less downtime than a fully ablative technique. Interestingly, patients have less postprocedure pain with this technique than with nonablative techniques, probably because the ablated channels offer a way for heat to escape the skin, he said
Dr. Avram disclosed that he is a paid consultant or has received honoraria from Invasix, Zeltiq Aesthetics, Galderma, and Kythera Biopharmaceuticals; that he is on the scientific advisory board of Cytrellis and Zeltiq; that he has intellectual property and royalty interests with Cytrellis; and that he has received research equipment from Cutera.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Technologies to address the many skin changes associated with photoaging run the gamut from nonablative to ablative – and choosing the right technology for a given patient is a balancing act, according to Dr. Mathew Avram.
“Basically, it’s a trade-off between increased efficacy and increased side effects and downtime,” Dr. Avram said at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Dr. Avram, director of the Massachusetts General Hospital dermatology, laser, and cosmetic center, Boston, said that traditional resurfacing remains the preferred method for repairing photodamaged skin. “One treatment provides reproducible, excellent results,” but at the cost of a significant amount of wound care and prolonged downtime. Potential adverse effects also include clear lines of demarcation with improper feathering, prolonged erythema, permanent hypopigmentation, infection, and scarring, he added.
For these reasons, the popularity of traditional resurfacing to treat photodamaged skin has declined over time as nonablative and intermediate techniques have arisen.
Intense pulsed light (IPL) is a nonlaser, nonablative technique that can produce overall skin rejuvenation, a “side effect” that patients often notice after they receive IPL for vascular lesions or hyperpigmentation. The benefits tend to be modest, even after several treatments, so this is not usually performed as a standalone technique for skin laxity or rhytides.
Nonablative fractional lasers act by creating thousands of microscopic wounds that are “columns of thermal coagulation,” leaving an intact stratum corneum, said Dr. Avram, who is also faculty director for laser and cosmetic training, Harvard Medical School, Boston.
The most common reason for treatment with a nonablative laser is mild to moderate wrinkles, though it can also be used for various pigmentation issues, as well as acne, surgical, and burn scars.
Although side effects are typically minor, the devices can be used off face, and there’s no worry about lines of demarcation; improvement is also more modest and will happen only with multiple treatments. “Fractional treatments give you fractional results,” Dr. Avram commented.
“You want to think about your treatment in terms of the pathology of what you’re treating,” he added, noting that fractional resurfacing can target both epidermal and dermal conditions. Examples of epidermal conditions that benefit from superficial treatment include dermatoheliosis, lentigines, and melasma.
Acne scars and deep wrinkles should receive deeper treatment in order to create thermal damage to the dermis proper, which, over a period of months, will trigger collagen remodeling and new collagen formation. Pulse energy will determine the depth and width of the zone of coagulation in the skin, so higher energy should be used with deeper skin pathology, Dr. Avram said.
Dermatologists also need to consider density of treatment – what percent of the skin is treated. “These devices go from about 5% to about 48% of skin coverage,” and increased density is really what increases the intensity of treatment, he noted. High-density treatment will result in more redness and swelling and has a greater potential for hyperpigmentation, but will not necessarily yield increased benefit in treatment outcomes, he added.
Pretreatment considerations should include assessing the patient’s expectations and availability for downtime post procedure. Treatment planning should also consider the patient’s skin type and probability for sun exposure. Patients should know they will see only partial improvement in wrinkles, scars, and pigmentation, and should expect some discomfort during the procedure and some side effects and healing time post procedure. Patients with a history of herpes labialis should receive valacyclovir 500 mg twice daily, beginning the day before treatment and continuing for 5-7 days, Dr. Avram said.
Cold-air cooling makes the treatment both safer and more comfortable, he pointed out. Topical compounded anesthesia including higher percentages of lidocaine and tetracaine can also be effective. Though local injected anesthesia can be effective in focal treatment of scars, the injection should be deep, and treatment should not begin immediately. This allows the lidocaine to disperse, minimizing the risk of ulceration from the thermal instability that a depot of lidocaine could cause, he said.
Fractional lasers can also be effective for treating background dermatoheliosis, as opposed to targeted treatment of individual lentigines. “Fractional is going to be great for clearing background damage,” Dr. Avram said.
A hybrid technique called ablative fractional photothermolysis creates tiny columns of ablation, while leaving the surrounding untreated tissue available as a reservoir for rapid healing. This technique will improve the more severe wrinkles that nonablative treatments don’t help, with less downtime than a fully ablative technique. Interestingly, patients have less postprocedure pain with this technique than with nonablative techniques, probably because the ablated channels offer a way for heat to escape the skin, he said
Dr. Avram disclosed that he is a paid consultant or has received honoraria from Invasix, Zeltiq Aesthetics, Galderma, and Kythera Biopharmaceuticals; that he is on the scientific advisory board of Cytrellis and Zeltiq; that he has intellectual property and royalty interests with Cytrellis; and that he has received research equipment from Cutera.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Technologies to address the many skin changes associated with photoaging run the gamut from nonablative to ablative – and choosing the right technology for a given patient is a balancing act, according to Dr. Mathew Avram.
“Basically, it’s a trade-off between increased efficacy and increased side effects and downtime,” Dr. Avram said at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Dr. Avram, director of the Massachusetts General Hospital dermatology, laser, and cosmetic center, Boston, said that traditional resurfacing remains the preferred method for repairing photodamaged skin. “One treatment provides reproducible, excellent results,” but at the cost of a significant amount of wound care and prolonged downtime. Potential adverse effects also include clear lines of demarcation with improper feathering, prolonged erythema, permanent hypopigmentation, infection, and scarring, he added.
For these reasons, the popularity of traditional resurfacing to treat photodamaged skin has declined over time as nonablative and intermediate techniques have arisen.
Intense pulsed light (IPL) is a nonlaser, nonablative technique that can produce overall skin rejuvenation, a “side effect” that patients often notice after they receive IPL for vascular lesions or hyperpigmentation. The benefits tend to be modest, even after several treatments, so this is not usually performed as a standalone technique for skin laxity or rhytides.
Nonablative fractional lasers act by creating thousands of microscopic wounds that are “columns of thermal coagulation,” leaving an intact stratum corneum, said Dr. Avram, who is also faculty director for laser and cosmetic training, Harvard Medical School, Boston.
The most common reason for treatment with a nonablative laser is mild to moderate wrinkles, though it can also be used for various pigmentation issues, as well as acne, surgical, and burn scars.
Although side effects are typically minor, the devices can be used off face, and there’s no worry about lines of demarcation; improvement is also more modest and will happen only with multiple treatments. “Fractional treatments give you fractional results,” Dr. Avram commented.
“You want to think about your treatment in terms of the pathology of what you’re treating,” he added, noting that fractional resurfacing can target both epidermal and dermal conditions. Examples of epidermal conditions that benefit from superficial treatment include dermatoheliosis, lentigines, and melasma.
Acne scars and deep wrinkles should receive deeper treatment in order to create thermal damage to the dermis proper, which, over a period of months, will trigger collagen remodeling and new collagen formation. Pulse energy will determine the depth and width of the zone of coagulation in the skin, so higher energy should be used with deeper skin pathology, Dr. Avram said.
Dermatologists also need to consider density of treatment – what percent of the skin is treated. “These devices go from about 5% to about 48% of skin coverage,” and increased density is really what increases the intensity of treatment, he noted. High-density treatment will result in more redness and swelling and has a greater potential for hyperpigmentation, but will not necessarily yield increased benefit in treatment outcomes, he added.
Pretreatment considerations should include assessing the patient’s expectations and availability for downtime post procedure. Treatment planning should also consider the patient’s skin type and probability for sun exposure. Patients should know they will see only partial improvement in wrinkles, scars, and pigmentation, and should expect some discomfort during the procedure and some side effects and healing time post procedure. Patients with a history of herpes labialis should receive valacyclovir 500 mg twice daily, beginning the day before treatment and continuing for 5-7 days, Dr. Avram said.
Cold-air cooling makes the treatment both safer and more comfortable, he pointed out. Topical compounded anesthesia including higher percentages of lidocaine and tetracaine can also be effective. Though local injected anesthesia can be effective in focal treatment of scars, the injection should be deep, and treatment should not begin immediately. This allows the lidocaine to disperse, minimizing the risk of ulceration from the thermal instability that a depot of lidocaine could cause, he said.
Fractional lasers can also be effective for treating background dermatoheliosis, as opposed to targeted treatment of individual lentigines. “Fractional is going to be great for clearing background damage,” Dr. Avram said.
A hybrid technique called ablative fractional photothermolysis creates tiny columns of ablation, while leaving the surrounding untreated tissue available as a reservoir for rapid healing. This technique will improve the more severe wrinkles that nonablative treatments don’t help, with less downtime than a fully ablative technique. Interestingly, patients have less postprocedure pain with this technique than with nonablative techniques, probably because the ablated channels offer a way for heat to escape the skin, he said
Dr. Avram disclosed that he is a paid consultant or has received honoraria from Invasix, Zeltiq Aesthetics, Galderma, and Kythera Biopharmaceuticals; that he is on the scientific advisory board of Cytrellis and Zeltiq; that he has intellectual property and royalty interests with Cytrellis; and that he has received research equipment from Cutera.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR

Common sense drives risk factor screening for systemic psoriasis therapy
LAS VEGAS – For a physician starting a patient on a systemic agent to treat psoriasis, deciding on risk factor screening and management strategies can be confusing. Who gets checked for what? Why? How often?
With a dearth of evidence to guide them, physicians should use what they know about psoriasis itself, as well as patient risk factors and the inherent risks of a given systemic therapy to guide screening, according to Dr. Kristina Callis Duffin of the department of dermatology, University of Utah, Salt Lake City.
Speaking at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Duffin said that in her practice, this means that all patients being considered for systemic therapy get baseline labs as recommended by the drug manufacturer, and risk-focused monitoring for cardiovascular disease, infection, and cancer. Basically, she noted, the strategy is, “How can we be effective at monitoring and surveying for those ‘bad guys’– those complications of therapy?”
“Some of this is really about using common sense and being a good physician,” she added.
To obtain a pertinent history, it’s worthwhile to formulate a directed intake questionnaire, Dr. Duffin said. Screening items should include history of recurrent infections; hepatitis, HIV, and TB status and risk; travel history; cardiovascular history, including lipid status; history of any liver or kidney problems; history and risk of diabetes mellitus; depression; personal or family history of multiple sclerosis; and history of cancer, including skin cancer, and blood disorders.
The social history should include pregnancy status and birth control method for women (as appropriate); and alcohol use for all patients. Patients should be current with age-appropriate recommended immunizations and cancer screenings.
Obtaining baseline lab tests for all patients before they start treatment with a systemic agent affords the opportunity to detect common metabolic abnormalities, such as diabetes, liver or kidney disease, and dyslipidemia, as well as rare but serious blood abnormalities, Dr. Duffin said. This approach respects the fact that “there is no question that cardiovascular risk factors are overrepresented in the moderate to severe psoriasis population.”
Published TB screening guidelines have universally recommended screening before initiating a biologic agent with a tuberculin skin test, unless the patient has had the BCG vaccine or is immunosuppressed. From there, interpretation of the tine test and further screening requires knowing the patient: “It’s all about pretest probability,” said Dr. Duffin, adding that physicians should not be afraid to use infectious disease consultants to help them sort out tricky cases.
In terms of ongoing management, communication and coordination are key. Continue to ask patients about symptoms of psoriatic arthritis, and make sure that you work with the patient’s primary care provider so that cardiovascular risk management, malignancy screening, and immunizations don’t fall through the cracks, she advised.
“Have a high index of suspicion for infection,” including deep fungal infections, she added. Though the literature does not report frequent cases of serious fungal infections, “there’s no question cases are unreported or numbers can be unclear in the registries.” Patients should know early signs of infection and know to seek care right away.
Patients should know to defer live vaccines, and the physician managing the care of psoriasis should be included in the planning and management process for any type of surgery, to oversee biologic administration. While probably slight, the risk of infection should be weighed against the risk of loss of efficacy in psoriasis or psoriatic arthritis treatment, Dr. Duffin said.
The baseline risk of solid tumors is elevated in patients with psoriasis, but “is not definitively elevated in patients on biologics,” she commented. The risk of nonmelanoma skin cancer, however, is definitely elevated for patients on biologic therapies, so an annual skin survey is a must for these patients, she said.
“Should we be discussing immunizations with our patients? Absolutely,”she added. All patients need the influenza vaccine and the pneumococcal vaccine, and for live virus immunizations, the dermatologist should coordinate administration with the primary care physician.
Managing these risks effectively can make a big difference in quality of life for patients who are able to start and stay on systemic therapy, said Dr. Duffin. The many risks of not treating psoriasis appropriately include not only the significant psychosocial impact, but also progression of psoriatic arthritis, progression of skin disease, and increased risk of heart disease and other cardiovascular comorbidities. “Our job is to treat to patient satisfaction and the best possible quality of life. A lot of this is about anticipation and communication,” she said.
Dr. Duffin reported receiving research support from and consulting for Amgen, Eli Lilly, Janssen, Stiefel, AbbVie, Bristol-Myers Squibb, Celgene, Novartis, and XenoPort; consulting and being on the scientific advisory board for Pfizer; and being on the scientific advisory board for Novartis, Eli Lilly, Janssen, Celgene, and XenoPort.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – For a physician starting a patient on a systemic agent to treat psoriasis, deciding on risk factor screening and management strategies can be confusing. Who gets checked for what? Why? How often?
With a dearth of evidence to guide them, physicians should use what they know about psoriasis itself, as well as patient risk factors and the inherent risks of a given systemic therapy to guide screening, according to Dr. Kristina Callis Duffin of the department of dermatology, University of Utah, Salt Lake City.
Speaking at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Duffin said that in her practice, this means that all patients being considered for systemic therapy get baseline labs as recommended by the drug manufacturer, and risk-focused monitoring for cardiovascular disease, infection, and cancer. Basically, she noted, the strategy is, “How can we be effective at monitoring and surveying for those ‘bad guys’– those complications of therapy?”
“Some of this is really about using common sense and being a good physician,” she added.
To obtain a pertinent history, it’s worthwhile to formulate a directed intake questionnaire, Dr. Duffin said. Screening items should include history of recurrent infections; hepatitis, HIV, and TB status and risk; travel history; cardiovascular history, including lipid status; history of any liver or kidney problems; history and risk of diabetes mellitus; depression; personal or family history of multiple sclerosis; and history of cancer, including skin cancer, and blood disorders.
The social history should include pregnancy status and birth control method for women (as appropriate); and alcohol use for all patients. Patients should be current with age-appropriate recommended immunizations and cancer screenings.
Obtaining baseline lab tests for all patients before they start treatment with a systemic agent affords the opportunity to detect common metabolic abnormalities, such as diabetes, liver or kidney disease, and dyslipidemia, as well as rare but serious blood abnormalities, Dr. Duffin said. This approach respects the fact that “there is no question that cardiovascular risk factors are overrepresented in the moderate to severe psoriasis population.”
Published TB screening guidelines have universally recommended screening before initiating a biologic agent with a tuberculin skin test, unless the patient has had the BCG vaccine or is immunosuppressed. From there, interpretation of the tine test and further screening requires knowing the patient: “It’s all about pretest probability,” said Dr. Duffin, adding that physicians should not be afraid to use infectious disease consultants to help them sort out tricky cases.
In terms of ongoing management, communication and coordination are key. Continue to ask patients about symptoms of psoriatic arthritis, and make sure that you work with the patient’s primary care provider so that cardiovascular risk management, malignancy screening, and immunizations don’t fall through the cracks, she advised.
“Have a high index of suspicion for infection,” including deep fungal infections, she added. Though the literature does not report frequent cases of serious fungal infections, “there’s no question cases are unreported or numbers can be unclear in the registries.” Patients should know early signs of infection and know to seek care right away.
Patients should know to defer live vaccines, and the physician managing the care of psoriasis should be included in the planning and management process for any type of surgery, to oversee biologic administration. While probably slight, the risk of infection should be weighed against the risk of loss of efficacy in psoriasis or psoriatic arthritis treatment, Dr. Duffin said.
The baseline risk of solid tumors is elevated in patients with psoriasis, but “is not definitively elevated in patients on biologics,” she commented. The risk of nonmelanoma skin cancer, however, is definitely elevated for patients on biologic therapies, so an annual skin survey is a must for these patients, she said.
“Should we be discussing immunizations with our patients? Absolutely,”she added. All patients need the influenza vaccine and the pneumococcal vaccine, and for live virus immunizations, the dermatologist should coordinate administration with the primary care physician.
Managing these risks effectively can make a big difference in quality of life for patients who are able to start and stay on systemic therapy, said Dr. Duffin. The many risks of not treating psoriasis appropriately include not only the significant psychosocial impact, but also progression of psoriatic arthritis, progression of skin disease, and increased risk of heart disease and other cardiovascular comorbidities. “Our job is to treat to patient satisfaction and the best possible quality of life. A lot of this is about anticipation and communication,” she said.
Dr. Duffin reported receiving research support from and consulting for Amgen, Eli Lilly, Janssen, Stiefel, AbbVie, Bristol-Myers Squibb, Celgene, Novartis, and XenoPort; consulting and being on the scientific advisory board for Pfizer; and being on the scientific advisory board for Novartis, Eli Lilly, Janssen, Celgene, and XenoPort.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – For a physician starting a patient on a systemic agent to treat psoriasis, deciding on risk factor screening and management strategies can be confusing. Who gets checked for what? Why? How often?
With a dearth of evidence to guide them, physicians should use what they know about psoriasis itself, as well as patient risk factors and the inherent risks of a given systemic therapy to guide screening, according to Dr. Kristina Callis Duffin of the department of dermatology, University of Utah, Salt Lake City.
Speaking at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Duffin said that in her practice, this means that all patients being considered for systemic therapy get baseline labs as recommended by the drug manufacturer, and risk-focused monitoring for cardiovascular disease, infection, and cancer. Basically, she noted, the strategy is, “How can we be effective at monitoring and surveying for those ‘bad guys’– those complications of therapy?”
“Some of this is really about using common sense and being a good physician,” she added.
To obtain a pertinent history, it’s worthwhile to formulate a directed intake questionnaire, Dr. Duffin said. Screening items should include history of recurrent infections; hepatitis, HIV, and TB status and risk; travel history; cardiovascular history, including lipid status; history of any liver or kidney problems; history and risk of diabetes mellitus; depression; personal or family history of multiple sclerosis; and history of cancer, including skin cancer, and blood disorders.
The social history should include pregnancy status and birth control method for women (as appropriate); and alcohol use for all patients. Patients should be current with age-appropriate recommended immunizations and cancer screenings.
Obtaining baseline lab tests for all patients before they start treatment with a systemic agent affords the opportunity to detect common metabolic abnormalities, such as diabetes, liver or kidney disease, and dyslipidemia, as well as rare but serious blood abnormalities, Dr. Duffin said. This approach respects the fact that “there is no question that cardiovascular risk factors are overrepresented in the moderate to severe psoriasis population.”
Published TB screening guidelines have universally recommended screening before initiating a biologic agent with a tuberculin skin test, unless the patient has had the BCG vaccine or is immunosuppressed. From there, interpretation of the tine test and further screening requires knowing the patient: “It’s all about pretest probability,” said Dr. Duffin, adding that physicians should not be afraid to use infectious disease consultants to help them sort out tricky cases.
In terms of ongoing management, communication and coordination are key. Continue to ask patients about symptoms of psoriatic arthritis, and make sure that you work with the patient’s primary care provider so that cardiovascular risk management, malignancy screening, and immunizations don’t fall through the cracks, she advised.
“Have a high index of suspicion for infection,” including deep fungal infections, she added. Though the literature does not report frequent cases of serious fungal infections, “there’s no question cases are unreported or numbers can be unclear in the registries.” Patients should know early signs of infection and know to seek care right away.
Patients should know to defer live vaccines, and the physician managing the care of psoriasis should be included in the planning and management process for any type of surgery, to oversee biologic administration. While probably slight, the risk of infection should be weighed against the risk of loss of efficacy in psoriasis or psoriatic arthritis treatment, Dr. Duffin said.
The baseline risk of solid tumors is elevated in patients with psoriasis, but “is not definitively elevated in patients on biologics,” she commented. The risk of nonmelanoma skin cancer, however, is definitely elevated for patients on biologic therapies, so an annual skin survey is a must for these patients, she said.
“Should we be discussing immunizations with our patients? Absolutely,”she added. All patients need the influenza vaccine and the pneumococcal vaccine, and for live virus immunizations, the dermatologist should coordinate administration with the primary care physician.
Managing these risks effectively can make a big difference in quality of life for patients who are able to start and stay on systemic therapy, said Dr. Duffin. The many risks of not treating psoriasis appropriately include not only the significant psychosocial impact, but also progression of psoriatic arthritis, progression of skin disease, and increased risk of heart disease and other cardiovascular comorbidities. “Our job is to treat to patient satisfaction and the best possible quality of life. A lot of this is about anticipation and communication,” she said.
Dr. Duffin reported receiving research support from and consulting for Amgen, Eli Lilly, Janssen, Stiefel, AbbVie, Bristol-Myers Squibb, Celgene, Novartis, and XenoPort; consulting and being on the scientific advisory board for Pfizer; and being on the scientific advisory board for Novartis, Eli Lilly, Janssen, Celgene, and XenoPort.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR
Practical tips help quell pseudofolliculitis barbae
LAS VEGAS – Stubble is okay, and not just because it’s trendy to sport a beard. This was a key message during a presentation on pseudofolliculitis barbae at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Changing up personal grooming habits is an important tactic for men who are plagued with pseudofolliculitis barbae, according to Dr. Andrew F. Alexis, chair of the department of dermatology and director of The Skin of Color Center, Mount Sinai St. Luke’s and Mount Sinai Roosevelt, New York.

This very common skin condition, affecting 45%-83% of men of African ancestry, is best managed by avoiding close shaving and preventing a sharp hair shaft tip. For those who don’t want a full beard for personal or professional reasons, using single blade razors, electric clippers, and even depilatories can help, he said.
All of these techniques prevent curly beard hairs from repenetrating or recurving before emergence – the underpinning of the pathology of pseudofolliculitis barbae. The embedded hairs eventually form a papular or pustular lesion that mimics infectious folliculitis. The inflammatory process can also prompt keloid formation in susceptible individuals.
Providing treatment options is important because the condition can be disfiguring, with such long-term physical sequelae as scarring beard alopecia and postinflammatory hyperpigmentation – changes in appearance that can have a significant psychosocial impact on affected men, Dr. Alexis said.
Therapies are centered around avoiding close shaving and/or preventing a sharp hair shaft tip.

One primary treatment is to stop shaving. “Embedded hairs spontaneously release after about one centimeter of growth,” Dr. Alexis said. This process can take up to 2 months, he said, but military studies dating back to the 1970s showed that the vast majority of pseudofolliculitis barbae cases resolved when service members stopped close shaving practices.
However, many patients want a clean-shaven appearance. “We can work with them to modify their shaving practices. Historically, we have recommended single-blade razors over multiple blade razors” because they shave less closely, he said, pointing out that razor manufacturers have funded studies that challenge this finding.
“Electric clippers are a very good alternative” to razors, Dr. Alexis said. A blade setting that allows at least 0.5-1 mm stubble is desirable.
Chemical depilatories, which act by weakening keratin disulfide bonds, can be effective, since depilated hair does not have a sharp, beveled tip on regrowth and is therefore less likely to repuncture the skin. Patients should be aware, though, that these substances can cause irritant contact dermatitis, he pointed out. Newer formulations are less caustic, but also less efficacious, he said.
In terms of practical tips, shaving technique is important. “Don’t assume the patient knows. There are all sorts of varying techniques out there,” some of which can exacerbate pseudofolliculitis barbae, Dr. Alexis said.
Before shaving, men should wash with a mild cleanser, using a gentle circular technique to free any entrapped hairs, then a moisturizing shaving cream. Razors should be changed every five to seven shaves, and shaving should always be done in the direction of beard growth without pulling on the skin.

Post shave, topical benzoyl peroxide 5%/clindamycin 1% can significantly reduce papules and pustules. Topical retinoids are another effective option. A low-potency steroid can be helpful for inflammatory symptoms.
For cases that just don’t respond to conservative and medical management, laser hair removal is an option. A recent military-funded split-face study found further improvement when topical eflornithine was added to long-pulse Nd:Yag laser therapy, Dr. Alexis said.
Affected individuals may find it difficult to modify shaving practices when uniformed service regulations or office dress codes require men to be close shaven; a note from a physician can be helpful. Dr. Alexis provides patients with a form letter to show their employers, explaining that the patient has a skin disorder that is exacerbated by shaving, and that the patient should be permitted to maintain a well-groomed beard. “I end up writing a lot of these for New York police officers,” he said.
Dr. Alexis disclosed that he has received grants and research support from Allergan and Novartis, and speaker honoraria from Cipla. He has received consulting fees from Aclaris, Allergan, Amgen, Anacor, Bayer, Galderma, Johnson & Johnson, Leo, L’Oreal, Roche, Schick, Suneva, and Valeant.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Stubble is okay, and not just because it’s trendy to sport a beard. This was a key message during a presentation on pseudofolliculitis barbae at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Changing up personal grooming habits is an important tactic for men who are plagued with pseudofolliculitis barbae, according to Dr. Andrew F. Alexis, chair of the department of dermatology and director of The Skin of Color Center, Mount Sinai St. Luke’s and Mount Sinai Roosevelt, New York.
This very common skin condition, affecting 45%-83% of men of African ancestry, is best managed by avoiding close shaving and preventing a sharp hair shaft tip. For those who don’t want a full beard for personal or professional reasons, using single blade razors, electric clippers, and even depilatories can help, he said.
All of these techniques prevent curly beard hairs from repenetrating or recurving before emergence – the underpinning of the pathology of pseudofolliculitis barbae. The embedded hairs eventually form a papular or pustular lesion that mimics infectious folliculitis. The inflammatory process can also prompt keloid formation in susceptible individuals.
Providing treatment options is important because the condition can be disfiguring, with such long-term physical sequelae as scarring beard alopecia and postinflammatory hyperpigmentation – changes in appearance that can have a significant psychosocial impact on affected men, Dr. Alexis said.
Therapies are centered around avoiding close shaving and/or preventing a sharp hair shaft tip.
One primary treatment is to stop shaving. “Embedded hairs spontaneously release after about one centimeter of growth,” Dr. Alexis said. This process can take up to 2 months, he said, but military studies dating back to the 1970s showed that the vast majority of pseudofolliculitis barbae cases resolved when service members stopped close shaving practices.
However, many patients want a clean-shaven appearance. “We can work with them to modify their shaving practices. Historically, we have recommended single-blade razors over multiple blade razors” because they shave less closely, he said, pointing out that razor manufacturers have funded studies that challenge this finding.
“Electric clippers are a very good alternative” to razors, Dr. Alexis said. A blade setting that allows at least 0.5-1 mm stubble is desirable.
Chemical depilatories, which act by weakening keratin disulfide bonds, can be effective, since depilated hair does not have a sharp, beveled tip on regrowth and is therefore less likely to repuncture the skin. Patients should be aware, though, that these substances can cause irritant contact dermatitis, he pointed out. Newer formulations are less caustic, but also less efficacious, he said.
In terms of practical tips, shaving technique is important. “Don’t assume the patient knows. There are all sorts of varying techniques out there,” some of which can exacerbate pseudofolliculitis barbae, Dr. Alexis said.
Before shaving, men should wash with a mild cleanser, using a gentle circular technique to free any entrapped hairs, then a moisturizing shaving cream. Razors should be changed every five to seven shaves, and shaving should always be done in the direction of beard growth without pulling on the skin.
Post shave, topical benzoyl peroxide 5%/clindamycin 1% can significantly reduce papules and pustules. Topical retinoids are another effective option. A low-potency steroid can be helpful for inflammatory symptoms.
For cases that just don’t respond to conservative and medical management, laser hair removal is an option. A recent military-funded split-face study found further improvement when topical eflornithine was added to long-pulse Nd:Yag laser therapy, Dr. Alexis said.
Affected individuals may find it difficult to modify shaving practices when uniformed service regulations or office dress codes require men to be close shaven; a note from a physician can be helpful. Dr. Alexis provides patients with a form letter to show their employers, explaining that the patient has a skin disorder that is exacerbated by shaving, and that the patient should be permitted to maintain a well-groomed beard. “I end up writing a lot of these for New York police officers,” he said.
Dr. Alexis disclosed that he has received grants and research support from Allergan and Novartis, and speaker honoraria from Cipla. He has received consulting fees from Aclaris, Allergan, Amgen, Anacor, Bayer, Galderma, Johnson & Johnson, Leo, L’Oreal, Roche, Schick, Suneva, and Valeant.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Stubble is okay, and not just because it’s trendy to sport a beard. This was a key message during a presentation on pseudofolliculitis barbae at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Changing up personal grooming habits is an important tactic for men who are plagued with pseudofolliculitis barbae, according to Dr. Andrew F. Alexis, chair of the department of dermatology and director of The Skin of Color Center, Mount Sinai St. Luke’s and Mount Sinai Roosevelt, New York.
This very common skin condition, affecting 45%-83% of men of African ancestry, is best managed by avoiding close shaving and preventing a sharp hair shaft tip. For those who don’t want a full beard for personal or professional reasons, using single blade razors, electric clippers, and even depilatories can help, he said.
All of these techniques prevent curly beard hairs from repenetrating or recurving before emergence – the underpinning of the pathology of pseudofolliculitis barbae. The embedded hairs eventually form a papular or pustular lesion that mimics infectious folliculitis. The inflammatory process can also prompt keloid formation in susceptible individuals.
Providing treatment options is important because the condition can be disfiguring, with such long-term physical sequelae as scarring beard alopecia and postinflammatory hyperpigmentation – changes in appearance that can have a significant psychosocial impact on affected men, Dr. Alexis said.
Therapies are centered around avoiding close shaving and/or preventing a sharp hair shaft tip.
One primary treatment is to stop shaving. “Embedded hairs spontaneously release after about one centimeter of growth,” Dr. Alexis said. This process can take up to 2 months, he said, but military studies dating back to the 1970s showed that the vast majority of pseudofolliculitis barbae cases resolved when service members stopped close shaving practices.
However, many patients want a clean-shaven appearance. “We can work with them to modify their shaving practices. Historically, we have recommended single-blade razors over multiple blade razors” because they shave less closely, he said, pointing out that razor manufacturers have funded studies that challenge this finding.
“Electric clippers are a very good alternative” to razors, Dr. Alexis said. A blade setting that allows at least 0.5-1 mm stubble is desirable.
Chemical depilatories, which act by weakening keratin disulfide bonds, can be effective, since depilated hair does not have a sharp, beveled tip on regrowth and is therefore less likely to repuncture the skin. Patients should be aware, though, that these substances can cause irritant contact dermatitis, he pointed out. Newer formulations are less caustic, but also less efficacious, he said.
In terms of practical tips, shaving technique is important. “Don’t assume the patient knows. There are all sorts of varying techniques out there,” some of which can exacerbate pseudofolliculitis barbae, Dr. Alexis said.
Before shaving, men should wash with a mild cleanser, using a gentle circular technique to free any entrapped hairs, then a moisturizing shaving cream. Razors should be changed every five to seven shaves, and shaving should always be done in the direction of beard growth without pulling on the skin.
Post shave, topical benzoyl peroxide 5%/clindamycin 1% can significantly reduce papules and pustules. Topical retinoids are another effective option. A low-potency steroid can be helpful for inflammatory symptoms.
For cases that just don’t respond to conservative and medical management, laser hair removal is an option. A recent military-funded split-face study found further improvement when topical eflornithine was added to long-pulse Nd:Yag laser therapy, Dr. Alexis said.
Affected individuals may find it difficult to modify shaving practices when uniformed service regulations or office dress codes require men to be close shaven; a note from a physician can be helpful. Dr. Alexis provides patients with a form letter to show their employers, explaining that the patient has a skin disorder that is exacerbated by shaving, and that the patient should be permitted to maintain a well-groomed beard. “I end up writing a lot of these for New York police officers,” he said.
Dr. Alexis disclosed that he has received grants and research support from Allergan and Novartis, and speaker honoraria from Cipla. He has received consulting fees from Aclaris, Allergan, Amgen, Anacor, Bayer, Galderma, Johnson & Johnson, Leo, L’Oreal, Roche, Schick, Suneva, and Valeant.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR

Topicals, PDT offer field treatment options for actinic keratoses
LAS VEGAS – The addition of field treatment to targeted lesion treatment may offer patients the best outcomes when addressing actinic keratoses (AKs), said Dr. David M. Pariser, professor of dermatology at Eastern Virginia Medical School, Norfolk, Virginia.
Speaking at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Pariser said that the rationale for treating AKs stems from the fact that not all AKs will transform to squamous cell carcinoma (SCC). “We don’t know which ones will and which ones won’t.” Though treatment can be guided by a shared decision-making approach, a personal history of multiple skin cancers is an obvious reason for concern, as is any drug-related or disease-related immunosuppression, he added.

Available treatments for AKs include cryosurgery, curettage, and electrodessication; photodynamic therapy (PDT); and topical agents, including 5-fluorouracil (5-FU), diclofenac, imiquimod, and ingenol mebutate.
“Cryosurgery is what most of us do for most AKs,” said Dr. Pariser, observing that this is a bread-and-butter procedure that is part of the backbone of most dermatology practices. Cryosurgery, curettage, and electrodessication are all used to treat discrete lesions, especially for higher-grade AKs.
However, Dr. Pariser noted that many AKs occur in a “field of cancerization.” This is a larger area of photodamaged skin; the skin may not appear grossly abnormal, but deranged areas will be diffusely evident with fluorescence detection, “indicating that all of this area was damaged,” he said.
PDT and topical agents effectively provide field treatment, and do not just address discrete lesions, although field treatment is technically an off-label use for these modalities, he added.
Lower concentrations and shorter courses of topical agents may be effective and better tolerated by patients, Dr. Pariser said. In clinical trials, for example, the efficacy of imiquimod 2.5% and 3.75% has been comparable to the stronger 5% formulation. Treatment cycles lasting 2 rather than 3 weeks have also shown similar efficacy. The greater palatability of these regimens to patients may increase real-world adherence as well.
Cure rates for PDT range from 67% to 92% for both the blue light–aminolevulinic acid modality and the red light–methyl aminolevulinate more commonly used in Europe. These modalities also treat a broad field, offer cure rates comparable to other topical modalities, and result in less scarring than destructive modalities, Dr. Pariser said.
The pain of PDT may be understandably off-putting for some patients, he commented. In the United States, investigators are experimenting with shorter incubation times for the ALA topical solutions. One study found comparable reductions in the number of AKs by the end of the study period for 1 versus 2 or 3 hours of incubation, and a 2-hour incubation period with spot treatment only was also similarly effective. Clearance rates ranged from about 70%-80%, and all were highly statistically significant, compared with the vehicle-only arm. However, “a second treatment at week 8 seems to be necessary for improved efficacy,” Dr. Pariser said.
Another treatment strategy currently being investigated is “painless PDT,” where the agent is applied and the field is illuminated immediately. Photo-bleaching degrades the protoporphyrins as they are produced, dramatically reducing patient discomfort. Efficacy is promising, he added.
In Europe, “daylight PDT” is being explored – the photosensitizing agent is applied, and the patient simply goes about his or her daily business in normal daylight. This is a nearly painless therapy and shows promise for efficacy. However, said Dr. Pariser, the realities of practice economics make it very unlikely that daylight PDT will catch on in the United States, since the daylight exposure does not represent a billable procedure.
Dr. Pariser reiterated that regardless of the modality, “field therapy has better long-term efficacy rates and better sustained clearance no matter which one of the agents we use, and combination therapy [of lesional and field treatment] seems to be the most effective.”
Dr. Pariser disclosed that he is an investigator and consultant for DUSA Pharmaceuticals, Photocure, and LEO Pharma, and that he discussed off-label uses of drugs and devices.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – The addition of field treatment to targeted lesion treatment may offer patients the best outcomes when addressing actinic keratoses (AKs), said Dr. David M. Pariser, professor of dermatology at Eastern Virginia Medical School, Norfolk, Virginia.
Speaking at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Pariser said that the rationale for treating AKs stems from the fact that not all AKs will transform to squamous cell carcinoma (SCC). “We don’t know which ones will and which ones won’t.” Though treatment can be guided by a shared decision-making approach, a personal history of multiple skin cancers is an obvious reason for concern, as is any drug-related or disease-related immunosuppression, he added.
Available treatments for AKs include cryosurgery, curettage, and electrodessication; photodynamic therapy (PDT); and topical agents, including 5-fluorouracil (5-FU), diclofenac, imiquimod, and ingenol mebutate.
“Cryosurgery is what most of us do for most AKs,” said Dr. Pariser, observing that this is a bread-and-butter procedure that is part of the backbone of most dermatology practices. Cryosurgery, curettage, and electrodessication are all used to treat discrete lesions, especially for higher-grade AKs.
However, Dr. Pariser noted that many AKs occur in a “field of cancerization.” This is a larger area of photodamaged skin; the skin may not appear grossly abnormal, but deranged areas will be diffusely evident with fluorescence detection, “indicating that all of this area was damaged,” he said.
PDT and topical agents effectively provide field treatment, and do not just address discrete lesions, although field treatment is technically an off-label use for these modalities, he added.
Lower concentrations and shorter courses of topical agents may be effective and better tolerated by patients, Dr. Pariser said. In clinical trials, for example, the efficacy of imiquimod 2.5% and 3.75% has been comparable to the stronger 5% formulation. Treatment cycles lasting 2 rather than 3 weeks have also shown similar efficacy. The greater palatability of these regimens to patients may increase real-world adherence as well.
Cure rates for PDT range from 67% to 92% for both the blue light–aminolevulinic acid modality and the red light–methyl aminolevulinate more commonly used in Europe. These modalities also treat a broad field, offer cure rates comparable to other topical modalities, and result in less scarring than destructive modalities, Dr. Pariser said.
The pain of PDT may be understandably off-putting for some patients, he commented. In the United States, investigators are experimenting with shorter incubation times for the ALA topical solutions. One study found comparable reductions in the number of AKs by the end of the study period for 1 versus 2 or 3 hours of incubation, and a 2-hour incubation period with spot treatment only was also similarly effective. Clearance rates ranged from about 70%-80%, and all were highly statistically significant, compared with the vehicle-only arm. However, “a second treatment at week 8 seems to be necessary for improved efficacy,” Dr. Pariser said.
Another treatment strategy currently being investigated is “painless PDT,” where the agent is applied and the field is illuminated immediately. Photo-bleaching degrades the protoporphyrins as they are produced, dramatically reducing patient discomfort. Efficacy is promising, he added.
In Europe, “daylight PDT” is being explored – the photosensitizing agent is applied, and the patient simply goes about his or her daily business in normal daylight. This is a nearly painless therapy and shows promise for efficacy. However, said Dr. Pariser, the realities of practice economics make it very unlikely that daylight PDT will catch on in the United States, since the daylight exposure does not represent a billable procedure.
Dr. Pariser reiterated that regardless of the modality, “field therapy has better long-term efficacy rates and better sustained clearance no matter which one of the agents we use, and combination therapy [of lesional and field treatment] seems to be the most effective.”
Dr. Pariser disclosed that he is an investigator and consultant for DUSA Pharmaceuticals, Photocure, and LEO Pharma, and that he discussed off-label uses of drugs and devices.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – The addition of field treatment to targeted lesion treatment may offer patients the best outcomes when addressing actinic keratoses (AKs), said Dr. David M. Pariser, professor of dermatology at Eastern Virginia Medical School, Norfolk, Virginia.
Speaking at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Pariser said that the rationale for treating AKs stems from the fact that not all AKs will transform to squamous cell carcinoma (SCC). “We don’t know which ones will and which ones won’t.” Though treatment can be guided by a shared decision-making approach, a personal history of multiple skin cancers is an obvious reason for concern, as is any drug-related or disease-related immunosuppression, he added.
Available treatments for AKs include cryosurgery, curettage, and electrodessication; photodynamic therapy (PDT); and topical agents, including 5-fluorouracil (5-FU), diclofenac, imiquimod, and ingenol mebutate.
“Cryosurgery is what most of us do for most AKs,” said Dr. Pariser, observing that this is a bread-and-butter procedure that is part of the backbone of most dermatology practices. Cryosurgery, curettage, and electrodessication are all used to treat discrete lesions, especially for higher-grade AKs.
However, Dr. Pariser noted that many AKs occur in a “field of cancerization.” This is a larger area of photodamaged skin; the skin may not appear grossly abnormal, but deranged areas will be diffusely evident with fluorescence detection, “indicating that all of this area was damaged,” he said.
PDT and topical agents effectively provide field treatment, and do not just address discrete lesions, although field treatment is technically an off-label use for these modalities, he added.
Lower concentrations and shorter courses of topical agents may be effective and better tolerated by patients, Dr. Pariser said. In clinical trials, for example, the efficacy of imiquimod 2.5% and 3.75% has been comparable to the stronger 5% formulation. Treatment cycles lasting 2 rather than 3 weeks have also shown similar efficacy. The greater palatability of these regimens to patients may increase real-world adherence as well.
Cure rates for PDT range from 67% to 92% for both the blue light–aminolevulinic acid modality and the red light–methyl aminolevulinate more commonly used in Europe. These modalities also treat a broad field, offer cure rates comparable to other topical modalities, and result in less scarring than destructive modalities, Dr. Pariser said.
The pain of PDT may be understandably off-putting for some patients, he commented. In the United States, investigators are experimenting with shorter incubation times for the ALA topical solutions. One study found comparable reductions in the number of AKs by the end of the study period for 1 versus 2 or 3 hours of incubation, and a 2-hour incubation period with spot treatment only was also similarly effective. Clearance rates ranged from about 70%-80%, and all were highly statistically significant, compared with the vehicle-only arm. However, “a second treatment at week 8 seems to be necessary for improved efficacy,” Dr. Pariser said.
Another treatment strategy currently being investigated is “painless PDT,” where the agent is applied and the field is illuminated immediately. Photo-bleaching degrades the protoporphyrins as they are produced, dramatically reducing patient discomfort. Efficacy is promising, he added.
In Europe, “daylight PDT” is being explored – the photosensitizing agent is applied, and the patient simply goes about his or her daily business in normal daylight. This is a nearly painless therapy and shows promise for efficacy. However, said Dr. Pariser, the realities of practice economics make it very unlikely that daylight PDT will catch on in the United States, since the daylight exposure does not represent a billable procedure.
Dr. Pariser reiterated that regardless of the modality, “field therapy has better long-term efficacy rates and better sustained clearance no matter which one of the agents we use, and combination therapy [of lesional and field treatment] seems to be the most effective.”
Dr. Pariser disclosed that he is an investigator and consultant for DUSA Pharmaceuticals, Photocure, and LEO Pharma, and that he discussed off-label uses of drugs and devices.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR

Busting eczema treatment myths: applying the evidence
LAS VEGAS – In the treatment of eczema, the gap between evidence and practice can be broad.
Dermatologists who treat atopic dermatitis confront many challenges – patients may be severely atopic, have a hard time being compliant with therapies, and have frequent recurrences, Dr. Robert Sidbury said at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. “It just is not easy,” he said.

However, even for challenging patients, physicians should be mindful of evidence-supported treatments and be attentive to practice gaps, said Dr. Sidbury, chief of the division of dermatology at the University of Washington’s Seattle Children’s Hospital.
Though the field is rapidly changing, the American Academy of Dermatology has issued practice guidelines that can help guide clinical treatment decisions, said Dr. Sidbury, who helped develop the AAD guidelines. He noted that prescribers may eventually feel the pain of the practice gap if AMA-driven performance measures are enforced.
At the meeting, Dr. Sidbury discussed areas in which many clinicians may have a practice gap in the treatment of eczema. Topping the list of non–evidence-based eczema care are overuse of steroids, oral antibiotics, and nonsedating antihistamines.
Practice gap: Many clinicians believe that topical steroids are more effective for atopic dermatitis when used twice daily.
Reality: “Randomized, controlled trials and a systematic review suggest that there is no benefit to twice-daily use of steroids,” over once-daily use, Dr. Sidbury said, though he admitted that he’s having a hard time breaking his own longstanding practice habit of prescribing twice- rather than once-daily dosing of topical corticosteroids. He pointed out that Dr. Hywel Williams, the director of the University of Nottingham’s Center of Evidence-Based Dermatology, England, calls this the “lowest-hanging fruit” in terms of cost savings, safety, and convenience to patients.
Practice gap: Unnecessary skin cultures can lead to overuse of systemic antibiotics in atopic dermatitis.
Reality: Colonization with Staphylococcus aureus occurs in more than 90% of adults with atopic dermatitis, but the vast majority of these patients are not infected. “Except for bleach baths in concert with intranasal mupirocin, no topical antistaphylococcal treatment has been shown to be clinically helpful in patients with atopic dermatitis,” Dr. Sidbury said.
“How do we know when eczema is infected? We know it when we see it. You are best served by using your clinical gestalt,” he added. Eczematous skin presents along a continuum, ranging from erythema, scaling, and crusting, to a frankly purulent appearance with clear infection, and clinical presentation and judgment should guide treatment. Barring frank infection, the evidence doesn’t support use of systemic antibiotics (Br J Dermatol. 2010 Jul;163 [1]:12-26).
Practice gap: Many patients with atopic dermatitis receive nonsedating antihistamines for itching.
Reality: There is no evidence that nonsedating antihistamines are beneficial unless the patient has concurrent rhinoconjunctivitis, so data don’t support their use “for the actual itch of eczema,” Dr. Sidbury said. In fact, the AMA-sponsored Physician Consortium for Performance Improvement nearly passed an overuse measure that would have penalized the prescription of nonsedating antihistamines in this setting, he said.
Practice gap: Systemic immunomodulatory therapy is used for pediatric atopic dermatitis, despite the lack of data that provide clear guidance.
Reality: The landscape here is a little more complicated, according to Dr. Sidbury. Among the systemic immunosuppressants, cyclosporine, methotrexate, azathioprine, and mycophenolate have the most evidence backing their use. However, there remains a lack of comparative studies and a lack of studies evaluating these therapies in the pediatric population, he said.
In general, Dr. Sidbury said that systemic therapy for atopic dermatitis is indicated only when control is inadequate despite truly optimized topical care, and the condition is having a “significant negative physical, psychological, or social impact” on the patient. Before beginning these potent systemic therapies, it’s important to assess that the patient and family are truly adherent to the topical treatment regime, and that adjunctive treatments like wet wraps and strict allergen avoidance are being followed. The Food and Drug Administration is beginning to include pediatric patients in clinical trials of systemic therapy for atopic dermatitis, so the quality of data should improve.
If systemic therapy is initiated, some clinical pearls can guide use, he said. Cyclosporine has the quickest onset of action and can be dosed at 3-6 mg/kg per day, divided into twice daily dosing. The maximum dose is 300 mg/day, and the microemulsion form is preferred. Overall, mycophenolate is the best-tolerated immunosuppressive. If methotrexate is chosen, it should be dosed at 0.2-0.7 mg/kg per week; liver function should be checked at 5-7 days after dosing, since methotrexate can cause a transient transaminitis. There are no standard recommendations to guide if or when to do liver biopsy recommendations in children receiving methotrexate. (J Am Acad Dermatol. 2014 Aug;71[2]:327-49).
Practice gap: Eczema appointments may only last 10-20 minutes.
Reality: “Proper eczema education takes much longer,” Dr. Sidbury said. Among patients and clinicians, there is still “rampant misinformation,” with persistence of fundamental knowledge gaps. “Studies repeatedly validate the role of education” in providing optimal care for eczema sufferers and their families, he emphasized (Pediatr Allergy Immunol. 2015 Jan 23. doi: 10.1111/pai.12338).
How is a busy physician to integrate all of these recommendations into practice and make sure patients are getting proper education? “Don’t reinvent the wheel – Google it!” Dr. Sidbury said. Resources from the National Eczema Association, among others, can help guide care. Eczema action plans that can be downloaded provide a roadmap for shared decision making; food allergy clinical practice guidelines help patients avoid allergens, and patients can further their knowledge when directed to reputable websites like the National Eczema Association and resources like www.eczemacenter.org, at Rady Children’s Hospital–San Diego.
Dr. Sidbury disclosed that he was a site principal investigator for an Anacor Pharmaceuticals–sponsored trial of a new topical anti-inflammatory agent for allergic dermatitis, and that he is on the Scientific Advisory Committee of the National Eczema Association.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – In the treatment of eczema, the gap between evidence and practice can be broad.
Dermatologists who treat atopic dermatitis confront many challenges – patients may be severely atopic, have a hard time being compliant with therapies, and have frequent recurrences, Dr. Robert Sidbury said at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. “It just is not easy,” he said.
However, even for challenging patients, physicians should be mindful of evidence-supported treatments and be attentive to practice gaps, said Dr. Sidbury, chief of the division of dermatology at the University of Washington’s Seattle Children’s Hospital.
Though the field is rapidly changing, the American Academy of Dermatology has issued practice guidelines that can help guide clinical treatment decisions, said Dr. Sidbury, who helped develop the AAD guidelines. He noted that prescribers may eventually feel the pain of the practice gap if AMA-driven performance measures are enforced.
At the meeting, Dr. Sidbury discussed areas in which many clinicians may have a practice gap in the treatment of eczema. Topping the list of non–evidence-based eczema care are overuse of steroids, oral antibiotics, and nonsedating antihistamines.
Practice gap: Many clinicians believe that topical steroids are more effective for atopic dermatitis when used twice daily.
Reality: “Randomized, controlled trials and a systematic review suggest that there is no benefit to twice-daily use of steroids,” over once-daily use, Dr. Sidbury said, though he admitted that he’s having a hard time breaking his own longstanding practice habit of prescribing twice- rather than once-daily dosing of topical corticosteroids. He pointed out that Dr. Hywel Williams, the director of the University of Nottingham’s Center of Evidence-Based Dermatology, England, calls this the “lowest-hanging fruit” in terms of cost savings, safety, and convenience to patients.
Practice gap: Unnecessary skin cultures can lead to overuse of systemic antibiotics in atopic dermatitis.
Reality: Colonization with Staphylococcus aureus occurs in more than 90% of adults with atopic dermatitis, but the vast majority of these patients are not infected. “Except for bleach baths in concert with intranasal mupirocin, no topical antistaphylococcal treatment has been shown to be clinically helpful in patients with atopic dermatitis,” Dr. Sidbury said.
“How do we know when eczema is infected? We know it when we see it. You are best served by using your clinical gestalt,” he added. Eczematous skin presents along a continuum, ranging from erythema, scaling, and crusting, to a frankly purulent appearance with clear infection, and clinical presentation and judgment should guide treatment. Barring frank infection, the evidence doesn’t support use of systemic antibiotics (Br J Dermatol. 2010 Jul;163 [1]:12-26).
Practice gap: Many patients with atopic dermatitis receive nonsedating antihistamines for itching.
Reality: There is no evidence that nonsedating antihistamines are beneficial unless the patient has concurrent rhinoconjunctivitis, so data don’t support their use “for the actual itch of eczema,” Dr. Sidbury said. In fact, the AMA-sponsored Physician Consortium for Performance Improvement nearly passed an overuse measure that would have penalized the prescription of nonsedating antihistamines in this setting, he said.
Practice gap: Systemic immunomodulatory therapy is used for pediatric atopic dermatitis, despite the lack of data that provide clear guidance.
Reality: The landscape here is a little more complicated, according to Dr. Sidbury. Among the systemic immunosuppressants, cyclosporine, methotrexate, azathioprine, and mycophenolate have the most evidence backing their use. However, there remains a lack of comparative studies and a lack of studies evaluating these therapies in the pediatric population, he said.
In general, Dr. Sidbury said that systemic therapy for atopic dermatitis is indicated only when control is inadequate despite truly optimized topical care, and the condition is having a “significant negative physical, psychological, or social impact” on the patient. Before beginning these potent systemic therapies, it’s important to assess that the patient and family are truly adherent to the topical treatment regime, and that adjunctive treatments like wet wraps and strict allergen avoidance are being followed. The Food and Drug Administration is beginning to include pediatric patients in clinical trials of systemic therapy for atopic dermatitis, so the quality of data should improve.
If systemic therapy is initiated, some clinical pearls can guide use, he said. Cyclosporine has the quickest onset of action and can be dosed at 3-6 mg/kg per day, divided into twice daily dosing. The maximum dose is 300 mg/day, and the microemulsion form is preferred. Overall, mycophenolate is the best-tolerated immunosuppressive. If methotrexate is chosen, it should be dosed at 0.2-0.7 mg/kg per week; liver function should be checked at 5-7 days after dosing, since methotrexate can cause a transient transaminitis. There are no standard recommendations to guide if or when to do liver biopsy recommendations in children receiving methotrexate. (J Am Acad Dermatol. 2014 Aug;71[2]:327-49).
Practice gap: Eczema appointments may only last 10-20 minutes.
Reality: “Proper eczema education takes much longer,” Dr. Sidbury said. Among patients and clinicians, there is still “rampant misinformation,” with persistence of fundamental knowledge gaps. “Studies repeatedly validate the role of education” in providing optimal care for eczema sufferers and their families, he emphasized (Pediatr Allergy Immunol. 2015 Jan 23. doi: 10.1111/pai.12338).
How is a busy physician to integrate all of these recommendations into practice and make sure patients are getting proper education? “Don’t reinvent the wheel – Google it!” Dr. Sidbury said. Resources from the National Eczema Association, among others, can help guide care. Eczema action plans that can be downloaded provide a roadmap for shared decision making; food allergy clinical practice guidelines help patients avoid allergens, and patients can further their knowledge when directed to reputable websites like the National Eczema Association and resources like www.eczemacenter.org, at Rady Children’s Hospital–San Diego.
Dr. Sidbury disclosed that he was a site principal investigator for an Anacor Pharmaceuticals–sponsored trial of a new topical anti-inflammatory agent for allergic dermatitis, and that he is on the Scientific Advisory Committee of the National Eczema Association.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – In the treatment of eczema, the gap between evidence and practice can be broad.
Dermatologists who treat atopic dermatitis confront many challenges – patients may be severely atopic, have a hard time being compliant with therapies, and have frequent recurrences, Dr. Robert Sidbury said at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar. “It just is not easy,” he said.
However, even for challenging patients, physicians should be mindful of evidence-supported treatments and be attentive to practice gaps, said Dr. Sidbury, chief of the division of dermatology at the University of Washington’s Seattle Children’s Hospital.
Though the field is rapidly changing, the American Academy of Dermatology has issued practice guidelines that can help guide clinical treatment decisions, said Dr. Sidbury, who helped develop the AAD guidelines. He noted that prescribers may eventually feel the pain of the practice gap if AMA-driven performance measures are enforced.
At the meeting, Dr. Sidbury discussed areas in which many clinicians may have a practice gap in the treatment of eczema. Topping the list of non–evidence-based eczema care are overuse of steroids, oral antibiotics, and nonsedating antihistamines.
Practice gap: Many clinicians believe that topical steroids are more effective for atopic dermatitis when used twice daily.
Reality: “Randomized, controlled trials and a systematic review suggest that there is no benefit to twice-daily use of steroids,” over once-daily use, Dr. Sidbury said, though he admitted that he’s having a hard time breaking his own longstanding practice habit of prescribing twice- rather than once-daily dosing of topical corticosteroids. He pointed out that Dr. Hywel Williams, the director of the University of Nottingham’s Center of Evidence-Based Dermatology, England, calls this the “lowest-hanging fruit” in terms of cost savings, safety, and convenience to patients.
Practice gap: Unnecessary skin cultures can lead to overuse of systemic antibiotics in atopic dermatitis.
Reality: Colonization with Staphylococcus aureus occurs in more than 90% of adults with atopic dermatitis, but the vast majority of these patients are not infected. “Except for bleach baths in concert with intranasal mupirocin, no topical antistaphylococcal treatment has been shown to be clinically helpful in patients with atopic dermatitis,” Dr. Sidbury said.
“How do we know when eczema is infected? We know it when we see it. You are best served by using your clinical gestalt,” he added. Eczematous skin presents along a continuum, ranging from erythema, scaling, and crusting, to a frankly purulent appearance with clear infection, and clinical presentation and judgment should guide treatment. Barring frank infection, the evidence doesn’t support use of systemic antibiotics (Br J Dermatol. 2010 Jul;163 [1]:12-26).
Practice gap: Many patients with atopic dermatitis receive nonsedating antihistamines for itching.
Reality: There is no evidence that nonsedating antihistamines are beneficial unless the patient has concurrent rhinoconjunctivitis, so data don’t support their use “for the actual itch of eczema,” Dr. Sidbury said. In fact, the AMA-sponsored Physician Consortium for Performance Improvement nearly passed an overuse measure that would have penalized the prescription of nonsedating antihistamines in this setting, he said.
Practice gap: Systemic immunomodulatory therapy is used for pediatric atopic dermatitis, despite the lack of data that provide clear guidance.
Reality: The landscape here is a little more complicated, according to Dr. Sidbury. Among the systemic immunosuppressants, cyclosporine, methotrexate, azathioprine, and mycophenolate have the most evidence backing their use. However, there remains a lack of comparative studies and a lack of studies evaluating these therapies in the pediatric population, he said.
In general, Dr. Sidbury said that systemic therapy for atopic dermatitis is indicated only when control is inadequate despite truly optimized topical care, and the condition is having a “significant negative physical, psychological, or social impact” on the patient. Before beginning these potent systemic therapies, it’s important to assess that the patient and family are truly adherent to the topical treatment regime, and that adjunctive treatments like wet wraps and strict allergen avoidance are being followed. The Food and Drug Administration is beginning to include pediatric patients in clinical trials of systemic therapy for atopic dermatitis, so the quality of data should improve.
If systemic therapy is initiated, some clinical pearls can guide use, he said. Cyclosporine has the quickest onset of action and can be dosed at 3-6 mg/kg per day, divided into twice daily dosing. The maximum dose is 300 mg/day, and the microemulsion form is preferred. Overall, mycophenolate is the best-tolerated immunosuppressive. If methotrexate is chosen, it should be dosed at 0.2-0.7 mg/kg per week; liver function should be checked at 5-7 days after dosing, since methotrexate can cause a transient transaminitis. There are no standard recommendations to guide if or when to do liver biopsy recommendations in children receiving methotrexate. (J Am Acad Dermatol. 2014 Aug;71[2]:327-49).
Practice gap: Eczema appointments may only last 10-20 minutes.
Reality: “Proper eczema education takes much longer,” Dr. Sidbury said. Among patients and clinicians, there is still “rampant misinformation,” with persistence of fundamental knowledge gaps. “Studies repeatedly validate the role of education” in providing optimal care for eczema sufferers and their families, he emphasized (Pediatr Allergy Immunol. 2015 Jan 23. doi: 10.1111/pai.12338).
How is a busy physician to integrate all of these recommendations into practice and make sure patients are getting proper education? “Don’t reinvent the wheel – Google it!” Dr. Sidbury said. Resources from the National Eczema Association, among others, can help guide care. Eczema action plans that can be downloaded provide a roadmap for shared decision making; food allergy clinical practice guidelines help patients avoid allergens, and patients can further their knowledge when directed to reputable websites like the National Eczema Association and resources like www.eczemacenter.org, at Rady Children’s Hospital–San Diego.
Dr. Sidbury disclosed that he was a site principal investigator for an Anacor Pharmaceuticals–sponsored trial of a new topical anti-inflammatory agent for allergic dermatitis, and that he is on the Scientific Advisory Committee of the National Eczema Association.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR

New antifungals effective with shorter treatment course for tinea pedis
LAS VEGAS – Tinea pedis plagues millions of patients yearly, and treatment is lengthy, cumbersome, and often ineffective.
But two potent new antifungals promise an easier treatment regimen and a higher rate of successful treatment outcomes, according to Dr. David M. Pariser, who shared data about luliconazole and a new formulation of naftifine as topical treatments for tinea infections, at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.

Dr. Pariser, professor in the department of dermatology at Eastern Virginia Medical School, Norfolk, pointed out that most antifungals currently approved for tinea pedis require at least daily – and sometimes twice daily – application for at least 4 weeks. Terbinafine and tolnaftate are the exceptions, with treatment periods ranging from 1-6 weeks for the two products, depending on clinical response.
A new formulation of naftifine hydrochloride 2%, (Naftin), a potent prescription topical allylamine antifungal available as a cream or a gel, has shown equivalent efficacy with just two weeks of treatment. Naftifine has lipophilic and keratinophilic properties; further, it has clinically significant anti-inflammatory and antibacterial effects, in addition to its potent fungicidal and fungistatic effects against dermatophytes, Dr. Pariser said at the meeting. The preparations are currently approved for topical treatment of tinea pedis, tinea cruris, and tinea corporis.
Notably, naftifine maintains a “clinically relevant therapeutic reservoir effect after treatment completion, with naftifine detected in the stratum corneum for up to 4 weeks posttreatment,” he said. This reservoir effect permits a significantly easier treatment regimen, with topical application of either formulation daily for just 2 weeks.
The clinical trials of naftifine HCl 2% with daily administration for 2 weeks showed equivalence with the 1% formulation administered for 4 weeks; the higher concentration was well tolerated and was effective in both the moccasin and interdigital distributions of tinea pedis involvement. Trials also showed the mycologic and clinical cure rates of naftifine 2% to be equivalent or superior to those of terbinafine, econazole, clotrimazole, miconazole, and tolnaftate.
Clinical trials showed treatment effectiveness – defined as 90% improvement over baseline and achieving “essentially normal skin” – in 52% of patients receiving naftifine 2%, compared with 20% of patients receiving vehicle only. Overall clinical success – defined as mycologic cure and either clinical cure of effective clinical treatment – was seen in 78% of the naftifine 2% patients, compared with 49% of the vehicle patients.
The second antifungal Dr. Pariser discussed is luliconazole (Luzu), a prescription topical imidazole that is available as a 1% cream. Luliconazole is also a broad-spectrum, potent antifungal with effects that persist several weeks after treatment. The preparation is at least as effective as bifonazole, terbinafine, and lanoconazole, both in vitro and in vivo, Dr. Pariser said.
In two parallel clinical trials comparing luliconazole 1% cream to its vehicle, treatment was effective (at least 90% clearing and with normal-appearing skin) in 48% and 33% of patients receiving luliconazole, compared with 10% and 15% of patients receiving vehicle alone.
An advantage of the topical agents is that there are generally no major systemic side effects, since there is minimal systemic absorption, Dr. Pariser noted. Allergic contact dermatitis may be a local reaction, but tends to be mild and transient, he said.
Clinicians should always be alert for tinea pedis when treating onychomycosis, said Dr. Pariser, and untreated tinea can contribute to recurrence of nail fungus. “If you don’t look for tinea, you might not find it, and you’ve missed a treatment opportunity,” he said.
Dr. Pariser disclosed that he is an investigator and consultant for Valeant and an investigator for Anacor Pharmaceuticals.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Tinea pedis plagues millions of patients yearly, and treatment is lengthy, cumbersome, and often ineffective.
But two potent new antifungals promise an easier treatment regimen and a higher rate of successful treatment outcomes, according to Dr. David M. Pariser, who shared data about luliconazole and a new formulation of naftifine as topical treatments for tinea infections, at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Dr. Pariser, professor in the department of dermatology at Eastern Virginia Medical School, Norfolk, pointed out that most antifungals currently approved for tinea pedis require at least daily – and sometimes twice daily – application for at least 4 weeks. Terbinafine and tolnaftate are the exceptions, with treatment periods ranging from 1-6 weeks for the two products, depending on clinical response.
A new formulation of naftifine hydrochloride 2%, (Naftin), a potent prescription topical allylamine antifungal available as a cream or a gel, has shown equivalent efficacy with just two weeks of treatment. Naftifine has lipophilic and keratinophilic properties; further, it has clinically significant anti-inflammatory and antibacterial effects, in addition to its potent fungicidal and fungistatic effects against dermatophytes, Dr. Pariser said at the meeting. The preparations are currently approved for topical treatment of tinea pedis, tinea cruris, and tinea corporis.
Notably, naftifine maintains a “clinically relevant therapeutic reservoir effect after treatment completion, with naftifine detected in the stratum corneum for up to 4 weeks posttreatment,” he said. This reservoir effect permits a significantly easier treatment regimen, with topical application of either formulation daily for just 2 weeks.
The clinical trials of naftifine HCl 2% with daily administration for 2 weeks showed equivalence with the 1% formulation administered for 4 weeks; the higher concentration was well tolerated and was effective in both the moccasin and interdigital distributions of tinea pedis involvement. Trials also showed the mycologic and clinical cure rates of naftifine 2% to be equivalent or superior to those of terbinafine, econazole, clotrimazole, miconazole, and tolnaftate.
Clinical trials showed treatment effectiveness – defined as 90% improvement over baseline and achieving “essentially normal skin” – in 52% of patients receiving naftifine 2%, compared with 20% of patients receiving vehicle only. Overall clinical success – defined as mycologic cure and either clinical cure of effective clinical treatment – was seen in 78% of the naftifine 2% patients, compared with 49% of the vehicle patients.
The second antifungal Dr. Pariser discussed is luliconazole (Luzu), a prescription topical imidazole that is available as a 1% cream. Luliconazole is also a broad-spectrum, potent antifungal with effects that persist several weeks after treatment. The preparation is at least as effective as bifonazole, terbinafine, and lanoconazole, both in vitro and in vivo, Dr. Pariser said.
In two parallel clinical trials comparing luliconazole 1% cream to its vehicle, treatment was effective (at least 90% clearing and with normal-appearing skin) in 48% and 33% of patients receiving luliconazole, compared with 10% and 15% of patients receiving vehicle alone.
An advantage of the topical agents is that there are generally no major systemic side effects, since there is minimal systemic absorption, Dr. Pariser noted. Allergic contact dermatitis may be a local reaction, but tends to be mild and transient, he said.
Clinicians should always be alert for tinea pedis when treating onychomycosis, said Dr. Pariser, and untreated tinea can contribute to recurrence of nail fungus. “If you don’t look for tinea, you might not find it, and you’ve missed a treatment opportunity,” he said.
Dr. Pariser disclosed that he is an investigator and consultant for Valeant and an investigator for Anacor Pharmaceuticals.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Tinea pedis plagues millions of patients yearly, and treatment is lengthy, cumbersome, and often ineffective.
But two potent new antifungals promise an easier treatment regimen and a higher rate of successful treatment outcomes, according to Dr. David M. Pariser, who shared data about luliconazole and a new formulation of naftifine as topical treatments for tinea infections, at the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Dr. Pariser, professor in the department of dermatology at Eastern Virginia Medical School, Norfolk, pointed out that most antifungals currently approved for tinea pedis require at least daily – and sometimes twice daily – application for at least 4 weeks. Terbinafine and tolnaftate are the exceptions, with treatment periods ranging from 1-6 weeks for the two products, depending on clinical response.
A new formulation of naftifine hydrochloride 2%, (Naftin), a potent prescription topical allylamine antifungal available as a cream or a gel, has shown equivalent efficacy with just two weeks of treatment. Naftifine has lipophilic and keratinophilic properties; further, it has clinically significant anti-inflammatory and antibacterial effects, in addition to its potent fungicidal and fungistatic effects against dermatophytes, Dr. Pariser said at the meeting. The preparations are currently approved for topical treatment of tinea pedis, tinea cruris, and tinea corporis.
Notably, naftifine maintains a “clinically relevant therapeutic reservoir effect after treatment completion, with naftifine detected in the stratum corneum for up to 4 weeks posttreatment,” he said. This reservoir effect permits a significantly easier treatment regimen, with topical application of either formulation daily for just 2 weeks.
The clinical trials of naftifine HCl 2% with daily administration for 2 weeks showed equivalence with the 1% formulation administered for 4 weeks; the higher concentration was well tolerated and was effective in both the moccasin and interdigital distributions of tinea pedis involvement. Trials also showed the mycologic and clinical cure rates of naftifine 2% to be equivalent or superior to those of terbinafine, econazole, clotrimazole, miconazole, and tolnaftate.
Clinical trials showed treatment effectiveness – defined as 90% improvement over baseline and achieving “essentially normal skin” – in 52% of patients receiving naftifine 2%, compared with 20% of patients receiving vehicle only. Overall clinical success – defined as mycologic cure and either clinical cure of effective clinical treatment – was seen in 78% of the naftifine 2% patients, compared with 49% of the vehicle patients.
The second antifungal Dr. Pariser discussed is luliconazole (Luzu), a prescription topical imidazole that is available as a 1% cream. Luliconazole is also a broad-spectrum, potent antifungal with effects that persist several weeks after treatment. The preparation is at least as effective as bifonazole, terbinafine, and lanoconazole, both in vitro and in vivo, Dr. Pariser said.
In two parallel clinical trials comparing luliconazole 1% cream to its vehicle, treatment was effective (at least 90% clearing and with normal-appearing skin) in 48% and 33% of patients receiving luliconazole, compared with 10% and 15% of patients receiving vehicle alone.
An advantage of the topical agents is that there are generally no major systemic side effects, since there is minimal systemic absorption, Dr. Pariser noted. Allergic contact dermatitis may be a local reaction, but tends to be mild and transient, he said.
Clinicians should always be alert for tinea pedis when treating onychomycosis, said Dr. Pariser, and untreated tinea can contribute to recurrence of nail fungus. “If you don’t look for tinea, you might not find it, and you’ve missed a treatment opportunity,” he said.
Dr. Pariser disclosed that he is an investigator and consultant for Valeant and an investigator for Anacor Pharmaceuticals.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
EXPERT ANALYSIS AT SDEF LAS VEGAS DERMATOLOGY SEMINAR

SDEF: Improved responses with newer topical onychomycosis treatments
LAS VEGAS – Better penetration through the nail is a key driver behind the increased efficacy of newer topical treatments for onychomycosis, affording a better chance for a clinical and mycologic cure without the potential for toxicity that comes with systemic treatments, according to Dr. David M. Pariser.
At the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Pariser, professor in the department of dermatology at Eastern Virginia Medical School, Norfolk, reviewed clinical trial data for 10% topical efinaconazole solution and 5% tavaborole topical solution, newer treatment options for the old problem of nail fungus. “New topical antifungals have improved the challenge of nail penetration,” which had been a key obstacle to efficacy with earlier topical treatments, he said.

Though topical treatments for onychomycosis avoid the risk of systemic side effects and the need for periodic blood tests to check liver function, historically, these treatments have not been very effective, he commented.
Ciclopirox (Penlac), one of the more efficacious treatments, achieves a cure rate of 5.5%-8.5%, and the buildup of the lacquer vehicle requires frequent nail debridement. Because of real or perceived risks, patients may be reluctant to take oral antifungals for onychomycosis, he said, noting that in addition to the potential for liver injury, use of these medications may also be limited by multiple drug-drug interactions.
The two new topical formulations he reviewed have a low molecular weight to allow better penetration through the dense, keratin-rich nail plate, Dr. Pariser said.
One of the topicals, 10% topical efinaconazole solution (Jublia), uses a formulation with low surface tension for good penetration with no surface buildup of vehicle material, achieving better nail penetration than do lacquer-based products, he noted.
A key efinaconazole study assessed clinical improvement in nail appearance in combination with mycologic cure, defined as negative findings on KOH prep exam and negative fungal culture. A complete cure was defined as a “totally clear target toenail and negative KOH/negative fungal culture,” and an “almost complete cure” was defined as mycologic cure, combined with no more than 5% clinically apparent involvement of the target toenail.

After double-blinded randomization into two parallel studies, patients applied either efinaconazole or the vehicle alone once daily at bedtime to the target toenail for 48 weeks. In the studies, 18% and 15% of those in the efinaconazole arm had achieved complete cure 52 weeks after beginning treatment, compared with 3% and 6% of the vehicle arm patients, respectively. However, for a pooled intent-to-treat population, the treatment arm saw a 28% cured or almost-cured rate, compared with 7% of the pooled vehicle-treated patients (P less than .001). Mycologic cure was achieved by 55% and 53% of the patients in the two efinaconazole arms, compared with 17% of the vehicle-only patients in each arm, according to Dr. Pariser.
Adverse events, similar between treatment arms, were mostly mild to moderate and localized, with dermatitis, vesicles, pain, and ingrown toenails the most commonly reported effects.
Tavaborole topical solution, 5% (Kerydin), is a boron-based compound that is highly water soluble, with broad antifungal activity that persists in the presence of keratin. As with efinaconazole, there is no product buildup, so nail debridement is not needed during treatment, Dr. Pariser said.
Two multicenter tavaborole trials compared the active tavaborole solution with a vehicle-only arm in a randomized, double-blind fashion, with product application daily for 48 weeks. The primary efficacy outcome for the trials was complete cure of the target great toenail at week 52. Secondary endpoints were a completely clear or almost clear (10% or less involvement of the target nail) target great toenail, as well as mycologic cure of the nail. Safety was measured by tracking adverse events, and local tolerability, as well as monitoring labs and ECG parameters.
A complete cure for the tavaborole trials required a completely clear nail on clinical exam, as well as negative mycology (negative KOH and negative fungal culture). At 52 weeks, 6.5% and 9.1% of the tavaborole-treated patients saw a complete cure, compared with 0.5% and 1.5% of vehicle-only patients in the two studies. Of those treated with tavaborole, 31.1% and 35.9% achieved mycologic cure, compared with 7.2% and 12.2% of those in the vehicle arm.
The rates of complete or almost complete clearing of the target great toenail for those in the tavaborole arms were 26.1% and 27.5%, compared with 9.3% and 14.6% in the vehicle arms. Predefined treatment success – a combination of mycologic cure and clear or almost clear target great toenail – was seen in 15.3% and 17.9% of the tavaborole-treated patients, compared with 1.5% and 3.9% of the vehicle-only patients (P less than or equal to .001 for all endpoints in both studies).
Treatment-related adverse events were generally mild and similar between the vehicle and treatment arms, with application site exfoliation, erythema, dermatitis, as well as ingrown toenails, the most commonly reported events for both arms.
Dr. Pariser noted that comparing efficacy of the newer agents directly is difficult, since the pivotal clinical trials for each had different designs, entry criteria, clinical assessments, and endpoints.
He disclosed that he is an investigator and consultant for Valeant, which manufactures the 10% topical efinaconazole solution, and an investigator for Anacor Pharmaceuticals, which markets tavaborole.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Better penetration through the nail is a key driver behind the increased efficacy of newer topical treatments for onychomycosis, affording a better chance for a clinical and mycologic cure without the potential for toxicity that comes with systemic treatments, according to Dr. David M. Pariser.
At the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Pariser, professor in the department of dermatology at Eastern Virginia Medical School, Norfolk, reviewed clinical trial data for 10% topical efinaconazole solution and 5% tavaborole topical solution, newer treatment options for the old problem of nail fungus. “New topical antifungals have improved the challenge of nail penetration,” which had been a key obstacle to efficacy with earlier topical treatments, he said.
Though topical treatments for onychomycosis avoid the risk of systemic side effects and the need for periodic blood tests to check liver function, historically, these treatments have not been very effective, he commented.
Ciclopirox (Penlac), one of the more efficacious treatments, achieves a cure rate of 5.5%-8.5%, and the buildup of the lacquer vehicle requires frequent nail debridement. Because of real or perceived risks, patients may be reluctant to take oral antifungals for onychomycosis, he said, noting that in addition to the potential for liver injury, use of these medications may also be limited by multiple drug-drug interactions.
The two new topical formulations he reviewed have a low molecular weight to allow better penetration through the dense, keratin-rich nail plate, Dr. Pariser said.
One of the topicals, 10% topical efinaconazole solution (Jublia), uses a formulation with low surface tension for good penetration with no surface buildup of vehicle material, achieving better nail penetration than do lacquer-based products, he noted.
A key efinaconazole study assessed clinical improvement in nail appearance in combination with mycologic cure, defined as negative findings on KOH prep exam and negative fungal culture. A complete cure was defined as a “totally clear target toenail and negative KOH/negative fungal culture,” and an “almost complete cure” was defined as mycologic cure, combined with no more than 5% clinically apparent involvement of the target toenail.
After double-blinded randomization into two parallel studies, patients applied either efinaconazole or the vehicle alone once daily at bedtime to the target toenail for 48 weeks. In the studies, 18% and 15% of those in the efinaconazole arm had achieved complete cure 52 weeks after beginning treatment, compared with 3% and 6% of the vehicle arm patients, respectively. However, for a pooled intent-to-treat population, the treatment arm saw a 28% cured or almost-cured rate, compared with 7% of the pooled vehicle-treated patients (P less than .001). Mycologic cure was achieved by 55% and 53% of the patients in the two efinaconazole arms, compared with 17% of the vehicle-only patients in each arm, according to Dr. Pariser.
Adverse events, similar between treatment arms, were mostly mild to moderate and localized, with dermatitis, vesicles, pain, and ingrown toenails the most commonly reported effects.
Tavaborole topical solution, 5% (Kerydin), is a boron-based compound that is highly water soluble, with broad antifungal activity that persists in the presence of keratin. As with efinaconazole, there is no product buildup, so nail debridement is not needed during treatment, Dr. Pariser said.
Two multicenter tavaborole trials compared the active tavaborole solution with a vehicle-only arm in a randomized, double-blind fashion, with product application daily for 48 weeks. The primary efficacy outcome for the trials was complete cure of the target great toenail at week 52. Secondary endpoints were a completely clear or almost clear (10% or less involvement of the target nail) target great toenail, as well as mycologic cure of the nail. Safety was measured by tracking adverse events, and local tolerability, as well as monitoring labs and ECG parameters.
A complete cure for the tavaborole trials required a completely clear nail on clinical exam, as well as negative mycology (negative KOH and negative fungal culture). At 52 weeks, 6.5% and 9.1% of the tavaborole-treated patients saw a complete cure, compared with 0.5% and 1.5% of vehicle-only patients in the two studies. Of those treated with tavaborole, 31.1% and 35.9% achieved mycologic cure, compared with 7.2% and 12.2% of those in the vehicle arm.
The rates of complete or almost complete clearing of the target great toenail for those in the tavaborole arms were 26.1% and 27.5%, compared with 9.3% and 14.6% in the vehicle arms. Predefined treatment success – a combination of mycologic cure and clear or almost clear target great toenail – was seen in 15.3% and 17.9% of the tavaborole-treated patients, compared with 1.5% and 3.9% of the vehicle-only patients (P less than or equal to .001 for all endpoints in both studies).
Treatment-related adverse events were generally mild and similar between the vehicle and treatment arms, with application site exfoliation, erythema, dermatitis, as well as ingrown toenails, the most commonly reported events for both arms.
Dr. Pariser noted that comparing efficacy of the newer agents directly is difficult, since the pivotal clinical trials for each had different designs, entry criteria, clinical assessments, and endpoints.
He disclosed that he is an investigator and consultant for Valeant, which manufactures the 10% topical efinaconazole solution, and an investigator for Anacor Pharmaceuticals, which markets tavaborole.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
LAS VEGAS – Better penetration through the nail is a key driver behind the increased efficacy of newer topical treatments for onychomycosis, affording a better chance for a clinical and mycologic cure without the potential for toxicity that comes with systemic treatments, according to Dr. David M. Pariser.
At the Skin Disease Education Foundation’s annual Las Vegas dermatology seminar, Dr. Pariser, professor in the department of dermatology at Eastern Virginia Medical School, Norfolk, reviewed clinical trial data for 10% topical efinaconazole solution and 5% tavaborole topical solution, newer treatment options for the old problem of nail fungus. “New topical antifungals have improved the challenge of nail penetration,” which had been a key obstacle to efficacy with earlier topical treatments, he said.
Though topical treatments for onychomycosis avoid the risk of systemic side effects and the need for periodic blood tests to check liver function, historically, these treatments have not been very effective, he commented.
Ciclopirox (Penlac), one of the more efficacious treatments, achieves a cure rate of 5.5%-8.5%, and the buildup of the lacquer vehicle requires frequent nail debridement. Because of real or perceived risks, patients may be reluctant to take oral antifungals for onychomycosis, he said, noting that in addition to the potential for liver injury, use of these medications may also be limited by multiple drug-drug interactions.
The two new topical formulations he reviewed have a low molecular weight to allow better penetration through the dense, keratin-rich nail plate, Dr. Pariser said.
One of the topicals, 10% topical efinaconazole solution (Jublia), uses a formulation with low surface tension for good penetration with no surface buildup of vehicle material, achieving better nail penetration than do lacquer-based products, he noted.
A key efinaconazole study assessed clinical improvement in nail appearance in combination with mycologic cure, defined as negative findings on KOH prep exam and negative fungal culture. A complete cure was defined as a “totally clear target toenail and negative KOH/negative fungal culture,” and an “almost complete cure” was defined as mycologic cure, combined with no more than 5% clinically apparent involvement of the target toenail.
After double-blinded randomization into two parallel studies, patients applied either efinaconazole or the vehicle alone once daily at bedtime to the target toenail for 48 weeks. In the studies, 18% and 15% of those in the efinaconazole arm had achieved complete cure 52 weeks after beginning treatment, compared with 3% and 6% of the vehicle arm patients, respectively. However, for a pooled intent-to-treat population, the treatment arm saw a 28% cured or almost-cured rate, compared with 7% of the pooled vehicle-treated patients (P less than .001). Mycologic cure was achieved by 55% and 53% of the patients in the two efinaconazole arms, compared with 17% of the vehicle-only patients in each arm, according to Dr. Pariser.
Adverse events, similar between treatment arms, were mostly mild to moderate and localized, with dermatitis, vesicles, pain, and ingrown toenails the most commonly reported effects.
Tavaborole topical solution, 5% (Kerydin), is a boron-based compound that is highly water soluble, with broad antifungal activity that persists in the presence of keratin. As with efinaconazole, there is no product buildup, so nail debridement is not needed during treatment, Dr. Pariser said.
Two multicenter tavaborole trials compared the active tavaborole solution with a vehicle-only arm in a randomized, double-blind fashion, with product application daily for 48 weeks. The primary efficacy outcome for the trials was complete cure of the target great toenail at week 52. Secondary endpoints were a completely clear or almost clear (10% or less involvement of the target nail) target great toenail, as well as mycologic cure of the nail. Safety was measured by tracking adverse events, and local tolerability, as well as monitoring labs and ECG parameters.
A complete cure for the tavaborole trials required a completely clear nail on clinical exam, as well as negative mycology (negative KOH and negative fungal culture). At 52 weeks, 6.5% and 9.1% of the tavaborole-treated patients saw a complete cure, compared with 0.5% and 1.5% of vehicle-only patients in the two studies. Of those treated with tavaborole, 31.1% and 35.9% achieved mycologic cure, compared with 7.2% and 12.2% of those in the vehicle arm.
The rates of complete or almost complete clearing of the target great toenail for those in the tavaborole arms were 26.1% and 27.5%, compared with 9.3% and 14.6% in the vehicle arms. Predefined treatment success – a combination of mycologic cure and clear or almost clear target great toenail – was seen in 15.3% and 17.9% of the tavaborole-treated patients, compared with 1.5% and 3.9% of the vehicle-only patients (P less than or equal to .001 for all endpoints in both studies).
Treatment-related adverse events were generally mild and similar between the vehicle and treatment arms, with application site exfoliation, erythema, dermatitis, as well as ingrown toenails, the most commonly reported events for both arms.
Dr. Pariser noted that comparing efficacy of the newer agents directly is difficult, since the pivotal clinical trials for each had different designs, entry criteria, clinical assessments, and endpoints.
He disclosed that he is an investigator and consultant for Valeant, which manufactures the 10% topical efinaconazole solution, and an investigator for Anacor Pharmaceuticals, which markets tavaborole.
SDEF and this news organization are owned by the same parent company.
On Twitter @karioakes
EXPERT ANALYSIS FROM SDEF LAS VEGAS DERMATOLOGY SEMINAR
