User login
The Epidemiology and Clinical Manifestations of Community-Acquired Methicillin-Resistant Staphylococcus aureus
A 65-year-old male with no significant past medical history, recently returned from a trip to the Democratic Republic of the Congo, presented with pain, swelling, and ulceration of his right lower leg. The symptoms had progressed despite oral amoxicillin/clavulanate. Evaluation at the time of admission revealed a large fluid collection in the anterior calf with extensive subcutaneous edema. Blood cultures were positive for methicillin–resistant S. aureus susceptible to clindamycin, erythromycin, tetracycline, trimethoprim-sulfamethoxazole, gentamicin, and tetracycline. His infection was successfully treated with surgical debridement, wound care, and vancomycin.
In 1941, Skinner and colleagues described the seriousness of S. aureus bloodstream infections in their series of 122 consecutive patients. The mortality rate was greater than 80% (1). Despite early success with penicillin the subsequent decades have shown this organism to be capable of elaborating resistance mechanisms that make therapy increasingly difficult (2). Methicillin resistance, which first appeared in the 1960s, has come to characterize many of the S. aureus isolates that are identified in the hospital. Recently, distinct strains of methicillin-resistant S. aureus (MRSA) are more commonly being identified in patients presenting for care from the community. This review will discuss recent developments in the clinical presentation and epidemiology of community-acquired MRSA in adults.
Definitions and Epidemiology
For infection control and epidemiological purposes, infections have been traditionally termed nosocomial if they 1) were not incubating at the time of presentation, 2) developed more than 72 hours after hospital admission, or 3) occurred in patients who were recently discharged from the hospital or who reside in a long-term care or skilled nursing facility. Beyond epidemiology, these definitions have been useful in helping the practicing clinician to employ effective empirical antibiotic therapy. The delivery of health care has evolved, however, and the distinction between outpatients and inpatients has been blurred. A broader term that has been suggested for infectious maladies in experienced patients who have moved in and out of the hospital is “healthcare associated” infections (3).
The evolving understanding of the origin of an infection has influenced efforts to define community MRSA. The term “community onset” or “community associated” MRSA can be used to describe a methicillin-resistant S. aureus infection that began incubating outside the hospital. If a patient has historical ties to a traditional treatment setting, the infection is most likely healthcare associated. Notable risk factors include hospitalization or stay in a nursing facility within the past year, use of broad-spectrum antibiotics, surgery, dialysis, intravenous drug use, or the presence of an indwelling vascular catheter. A MRSA infection in a patient presenting from home without any healthcare risk factors can be deemed “community acquired” MRSA (CaMRSA) (4).
A further understanding of CaMRSA can be gleaned from molecular studies of the organism. Methicillin resistance is mediated by a genetic element called staphylococcal cassette chromosome mecA (SCCmecA). MecA codes for a novel penicillin binding protein, PBP 2a, which is not inhibited by beta-lactam antibiotics (2). There are at least 5 types of SCCmecA. Types I through III are typically present in nosocomial MRSA strains. CaMRSA is distinguishable by the presence of SCCmecA IV (4-6).
Another distinctive feature of CaMRSA is the presence of the Panton-Valentine leukocidin (PVL). Previous work has shown that only 2–3% of strains of S. aureus produce this toxin (7). However this virulence factor, encoded by the genes lukS-PV and lukF-PV, appears to be expressed much more commonly in CaMRSA.
The difficulties with defining CaMRSA have influenced attempts to understand its prevalence. The key question in reviewing the available studies is how rigorous an attempt was made to exclude those patients who had significant healthcare contact. Salgado and colleagues performed a meta-analysis to try to determine the prevalence of true CaMRSA. They found that a significant number of subjects included in prevalence studies had identifiable healthcare risk factors, and that when this was accounted for, the overall prevalence of CaMRSA was less than 0.24% (8). The burden of CaMRSA infection will vary however based on location, and certain areas of the United States have demonstrated a higher prevalence. Researchers from the Emerging Infections Program Network examined CaMRSA in Atlanta, Baltimore, and Minnesota and found the prevalence to range from 8% to 20% (9). Of note, only 41% of suspected cases of CaMRSA were confirmed through interviews.
So what is CaMRSA? An acceptable working definition is a methicillin-resistant S. aureus infection occurring in a patient without a history of healthcare risk factors due to an isolate carrying SCCmecA type IV. The isolate is also likely to express the PVL virulence factor. This definition combines what is known about both the clinical and molecular epidemiology of these strains. Further research and time is likely to result in modifications to our understanding of this emerging phenomenon.
Antibiotic Susceptibility Patterns
CaMRSA strains have unique susceptibility patterns compared with traditional MRSA strains. As noted above, SCCmecA codes for methicillin resistance in S. aureus. SCCmecA types II and III are large genetic elements that usually code for resistance to multiple antibiotics. In contrast, type IV is smaller and results in decreased susceptibility to betalactams alone. CaMRSA strains are identifiable as being susceptible to clindamycin, trimethoprim-sulfamethoxazole, and the aminoglycosides (4). Susceptibility to clindamycin must be interpreted cautiously in strains that are erythromycin resistant. If erythromycin resistance is due to an inactivating enzyme (a ribosomal methylase) resistance to clindamycin can be induced. This macrolide-lincosamide-streptogramin–inducible phenotype can be identified in the microbiology lab by performing an erythromycin induction test (D-test). Clinical failures have been described when clindamycin has been used in the presence of this inducible phenotype (10).
Outbreaks
As with many infectious diseases, outbreaks first brought the problem of CaMRSA to wider attention. The first well-described outbreak occurred in the early 1980s among intravenous drug users in Detroit (11). Reports in the early 1990s focused on MRSA infections in young children without risk factors for resistant infection (12). Overwhelming, fatal sepsis due to MRSA was described in 4 pediatric patients in Minnesota and North Dakota. A fulminant, necrotizing pneumonia characterized 3 of the cases (13). Subsequently numerous outbreaks have been described among prison inmates, sexual partners, and competitive sports participants (14-16).
Two well-documented outbreaks have been described in football players. Begier and colleagues identified an outbreak that involved 10 players on the same college football team. Molecular typing demonstrated all recovered isolates to be of the same strain and to carry SCCmecA and the PVL gene. The case-control analysis showed an association between infection and playing wide receiver or cornerback, turf burns, and body shaving (17). An investigation of 8 MRSA infections among professional football players similarly showed all recovered strains to be clonal and to harbor SCCmecA IV and the PVL locus. In contrast to the college outbreak, these investigators found an association between being a lineman or a linebacker and disease. Turf burns were again a significant risk factor (18).
Both of these outbreaks, although geographically separate, were found to be due to the same strain of MRSA, clone USA300-0114. This clone has also been demonstrated as the predominant cause of CaMRSA in other communities (15,19). This would seem to indicate greater fitness of this particular strain that has allowed it to spread widely (20).
Clinical Manifestations
In general, CaMRSA has been reported to cause a similar spectrum of disease as methicillin-susceptible S. aureus (MSSA). As mentioned above, it appears to be seen mostly in otherwise healthy, young individuals. In the population based surveillance project of Fridkin et al., 77% of patients with community MRSA had skin and soft tissue infections (9). Invasive disease was observed in 6%. Similarly, Naimi and colleagues found skin and soft tissue infections in 75% of the subjects in their study of community-associated MRSA in Minnesota (21).
There is concern that CaMRSA may be associated with a greater likelihood of disease compared with other S. aureus strains. Ellis et al. prospectively evaluated active-duty soldiers found to be colonized with CaMRSA. Of the 24 colonized, 38% or 9 individuals developed soft-tissue infections as compared with 3% of those colonized with MSSA. Eight of nine affected patients had abscesses. All 9 of the available clinical isolates were positive for the PVL gene and the presence of this virulence factor was associated with an increased risk of invasive disease (22). Other authors have found an association between PVL-carrying strains of S. aureus and disease and it is perhaps this characteristic, not methicillin resistance, that assists the organism in causing disease in otherwise healthy individuals (23,24). The observed high prevalence of the PVL virulence factor among CaMRSA has been described as the “convergence of resistance and virulence” (25).
Severe disease has also been described due to strains of CaMRSA. Francis described 4 patients with necrotizing pneumonia due to CaMRSA similar to the pediatric cases referred to above. The isolates from all 4 patients carried PVL and SCCmecA IV genes and were of the USA300 strain group (26). Of note, all 4 patients initially had influenza-like illnesses, demonstrating again the association between influenza and staphylococcal pneumonia. This also signifies these presentations were potentially vaccine preventable. Recently, necrotizing fasciitis caused by CaMRSA strains, all again characterized as having PVL genes, has been described (27). This new phenomenon expands the differential diagnosis of causes of this life-threatening soft-tissue syndrome and influences empirical antibiotic selection.
A 41-year-old with Crohn’s disease treated with infliximab undergoes ventral hernia repair. She has a past surgical history of multiple abdominal surgeries. Three weeks postoperatively she is readmitted with a superinfected hematoma requiring operative drainage. Cultures reveal MRSA, susceptible to erythromycin, clindamycin, vancomycin, gentamicin, tetracycline, and trimethoprim-sulfamethoxazole.
The work to date on this new aspect of resistance in S. aureus intimates a trend similar to that previously experienced with penicillin resistance. Penicillinase-producing strains, first recognized in 1944, became increasingly common among hospital isolates after the second World War (28,29). By the 1970s, penicillin-resistant staphylococci had become widespread in the Community as well. Currently, identification of a penicillin-susceptible S. aureus isolate is uncommon.
The potential for further increases in the prevalence of methicillin resistance among staphylococci lies with the SCCmecA complex. Acquisition of this determinant from another resistant clone of either S. aureus or a coagulase-negative staphylococcus is the necessary first step in the process of becoming methicillin resistant. Types I through III are large, and this has been an obstacle to frequent transfers to MSSA strains. The result of this dynamic is that hospital-acquired MRSA to this point has descended from a relatively small number of clones as compared with the wide heterogeneity seen in susceptible S. aureus (30). As mentioned above, SCCmecA IV is smaller and can therefore more easily insert into many different MSSA strains without a loss of fitness. In fact type IV strains have been shown in vitro to replicate faster than hospital MRSA strains (20). This may allow MRSA to begin to displace MSSA as the predominant community phenotype in a manner similar to that in which penicillin-susceptible S. aureus was replaced.
A similar phenomenon may occur in hospitals wherein a typical CaMRSA strain may become the predominant hospital clone. This has been described already in 1 hospital where SCCmecA IV became the major determinant of methicillin resistance in the hospital (31). The trend was identifiable by a “more susceptible” antibiogram of MRSA strains. Future epidemiological surveillance will be necessary as the potential exists for resistant strains to continue to cross the increasingly more permeable barrier between traditional healthcare and the community.
Management
Increasing resistance to S. aureus has several implications for clinicians. Fundamental principles in the management of infectious syndromes become even more important, particularly source control of suppurative foci through debridement and drainage. An added benefit of such procedures is that they facilitate the establishment of a microbiological diagnosis. Clinicians and microbiologists will need to continue to work together closely so as to be aware of resistance trends in their community. In situations where the pathogen is not identified and treatment is prescribed empirically, follow-up is crucial.
Obviously, the emergence of CaMRSA has limited antibiotic choices. Clindamycin, trimethoprim-sulfamethoxazole, and doxycycline remain therapeutic options in the appropriate clinical situation. The severe clinical manifestations described above require consideration of empirical vancomycin in the treatment of patients presenting seriously ill with infectious syndromes that could be potentially due to S. aureus while awaiting culture results. The most extensive experience for inpatient use is with this agent. Linezolid, daptomycin, and quinupristin-dalfopristin are newer agents with activity against MRSA that have been reviewed elsewhere (32,33). Growing experience with these agents has provided options in situations where vancomycin cannot be used. It has also emphasized some of their limitations. Daptomycin and quinupristin-dalfopristin are only given parenterally, while linezolid can be given both orally and intravenously. Expense impacts the use of all three especially outside the hospital. Treatment-limiting cytopenias and peripheral and optic neuropathy have been described with linezolid when it is has been employed for extended courses of therapy. Daptomycin is inhibited by surfactant and therefore should not be used for suspected pulmonary infections. Quinupristin-dalfopristin’s use can be limited by disabling myalgias and the need for central venous access. More data about the use of these newer agents for invasive infections are needed before they can be considered superior to vancomycin.
Dr. Fraser may be reached at frasert@ccf.org.
Dr. Fraser is a member of the Wyeth Emerging Pathogens speakers’ bureau and has participated in a local advisory panel for GlaxoSmithKline. There is no conflict of interest to disclose for this work.
References
- Skinner D, Keefer CS. Significance of bacteremia caused by Staphylococcus aureus. Arch Intern Med. 1941;68:851-75.
- Lowy FD. Antimicrobial resistance: the example of Staphylococcus aureus. J Clin Invest. 2003;111:1265-73.
- Friedman ND, Kaye KS, Stout JE, et al. Health care-associated bloodstream infections in adults: a reason to change the accepted definition of community-acquired infections. Ann Intern Med. 2002;137:791-7.
- Said-Salim B, Mathema B, Kreiswirth BN. Community-acquired methicillin-resistant Staphylococcus aureus: an emerging pathogen. Infect Control Hosp Epidemiol. 2003;24:451-5.
- Carleton HA, Diep BA, Charlebois ED, Sensabaugh GF, Perdreau-Remington F. Community-adapted methicillin-resistant Staphylococcus aureus (MRSA): population dynamics of an expanding community reservoir of MRSA. J Infect Dis. 2004;190:1730-8.
- Daum RS, Ito T, Hiramatsu K, et al. A novel methicillin-resistance cassette in community-acquired methicillin resistant Staphylococcus aureus isolates of diverse genetic backgrounds. J Infect Dis. 2002:186;1344-7.
- Dinges MM, Orwin PM, Schlievert PM. Exotoxins of Staphylococcus aureus. Clin Microbiol Rev. 2000;13:16-34.
- Salgado CD, Farr BM, Calfee DP. Community-acquired methicillin-resistant Staphylococcus aureus: a metaanalysis of prevalence and risk factors. Clin Infect Dis. 2003;36:131-9.
- Fridkin SK, Hageman JC, Morrison M, et al. Methicillinresistant Staphylococcus aureus disease in three communities. N Engl J Med. 2005;352:1436-44.
- Siberry GK, Tekle T, Carroll K, Dick J. Failure of clindamycin treatment of methicillin-resistant Staphylococcus aureus expressing inducible clindamycin resistance in vitro. Clin Infect Dis. 2003;37:1257-60.
- Saravolatz LD, Markowitz N, Arking L, Pohlod D, Fisher E. Methicillin-resistant Staphylococcus aureus. Epidemiologic observations during a community-acquired outbreak. Ann Intern Med. 1982;96:11-6.
- Herold BC, Immergluck LC, Maranan MC, et al. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA. 1998;279:593-598.
- Centers for Disease Control and Prevention. Four pediatric deaths from community acquired methicillin resistant Staphylococcus aureus—Minnesota and North Dakota, 1997-1999. MMWR Morb Mortal Wkly Rep. 1999;48:707-10.
- Centers for Disease Control and Prevention. Methicillin-resistant Staphylococcus aureus infections in correctional facilities—Georgia, California, and Texas, 2001-2003. MMWR Morb Mortal Wkly Rep. 2003;52:992-6.
- Centers for Disease Control and Prevention. Public Health Dispatch: outbreaks of community-associated methicillin-resistant Staphylococcus aureus skin infections—Los Angeles County, California, 2002-2003. MMWR Morb Mortal Wkly Rep. 2003;52:88.
- Lindenmayer JD, Schoenfeld S, O’Grady R, Carney JK. Methicillin-resistant Staphylococcus aureus in a high school wrestling team and the surrounding community. Arch Int Med. 1998;158:895-9.
- Begier EM, Frenette K, Barrett NL, et al. A high-morbidity outbreak of methicillin-resistant Staphylococcus aureus among players on a college football team, facilitated by cosmetic body shaving and turf burns. Clin Infect Dis. 2004;39:1446-53.
- Kazakova SV, Hagerman JC, Matava M, et al. A clone of methicillin-resistant Staphylococcus aureus among professional football players. N Engl J Med. 2005;352: 468-75.
- McDougal LK, Steward CD, Killgore GE, Chaitram JM, McAllister SK, Tenover FC. Pulsed-field gel electrophoresis typing of oxacillin-resistant Staphylococcus aureus isolates from the United States: establishing a national database. J Clin Microbiol. 2003;41:5113-20.
- Deresinski S. Methicillin-resistant Staphylococcus aureus: an evolutionary, epidemiologic, and therapeutic odyssey. Clin Infect Dis. 2005;40:562-73.
- Naimi TS, LeDell KH, Como-Sabetti K, et al. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA. 2003;290:2976-84.
- Ellis MW, Hospenthal DR, Dooley DP, Gray PJ, Murray CK. Natural history of methicillin-resistant Staphylococcus aureus colonization and infection in soldiers. Clin Infect Dis. 2004;39:971-9.
- Yamasaki O, Kaneko J, Morizane S, et al. The association between Staphylococcus aureus strains carrying panton-valentine leukocidin genes and the development of deep-seated follicular infection. Clin Infect Dis. 2005;40:381-5.
- Hsu LY, Koh TH, Kurup A, Low J, Chlebicki MP, Tan BH. High incidence of Panton-Valentine leukocidin-producing Staphylococcus aureus in a tertiary care public hospital in Singapore. Clin Infect Dis. 2005;40:486-9.
- Chambers HF. Community-associated MRSA–resistance and virulence converge. N Engl J Med. 2005;352:1485-7.
- Francis JS, Doherty MC, Lopatin U, et al. Severe community-onset pneumonia in healthy adults caused by methicillin-resistant Staphylococcus aureus carrying the Panton-Valentine leukocidin genes. Clin Infect Dis. 2005;40:100-7.
- Miller LG, Perdreau-Remington F, Rieg G, et al. Necrotizing fasciitis caused by community-associated methicillin-resistant Staphylococcus aureus in Los Angeles. N Engl J Med. 2005;352:1445-53.
- Kirby WMM. Extraction of a highly potent penicillin inactivator from penicillin resistant staphylococci. Science. 1944;99:452-3.
- Chambers HF. The changing epidemiology of Staphylococcus aureus? Emerg Infect Dis. 2001;7:178-82.
- Kreiswirth B, Kornblum J, Arbeit RD, et al. Evidence for a clonal origin of methicillin resistance in Staphylococcus aureus. Science. 1993;259:227-30.
- Donnio PY, Preney L, Gautier-Lerestif AL, Avril JL, Lafforgue N. Changes in staphylococcal chromosome type and antibiotic resistance profile in methicillin-resistant Staphylococcus aureus isolates from a French hospital over an 11 year period. J Antimicrob Chemother. 2004;53:808-13.
- Eliopoulos GM. Quinupristin-dalfopristin and linezolid: evidence and opinion. Clin Infect Dis. 2003;36: 473-81.
- Carpenter CF, Chambers HF. Daptomycin: another novel agent for treating infections due to drug-resistant gram-positive pathogens. Clin Infect Dis. 2004;38: 994-1000.
A 65-year-old male with no significant past medical history, recently returned from a trip to the Democratic Republic of the Congo, presented with pain, swelling, and ulceration of his right lower leg. The symptoms had progressed despite oral amoxicillin/clavulanate. Evaluation at the time of admission revealed a large fluid collection in the anterior calf with extensive subcutaneous edema. Blood cultures were positive for methicillin–resistant S. aureus susceptible to clindamycin, erythromycin, tetracycline, trimethoprim-sulfamethoxazole, gentamicin, and tetracycline. His infection was successfully treated with surgical debridement, wound care, and vancomycin.
In 1941, Skinner and colleagues described the seriousness of S. aureus bloodstream infections in their series of 122 consecutive patients. The mortality rate was greater than 80% (1). Despite early success with penicillin the subsequent decades have shown this organism to be capable of elaborating resistance mechanisms that make therapy increasingly difficult (2). Methicillin resistance, which first appeared in the 1960s, has come to characterize many of the S. aureus isolates that are identified in the hospital. Recently, distinct strains of methicillin-resistant S. aureus (MRSA) are more commonly being identified in patients presenting for care from the community. This review will discuss recent developments in the clinical presentation and epidemiology of community-acquired MRSA in adults.
Definitions and Epidemiology
For infection control and epidemiological purposes, infections have been traditionally termed nosocomial if they 1) were not incubating at the time of presentation, 2) developed more than 72 hours after hospital admission, or 3) occurred in patients who were recently discharged from the hospital or who reside in a long-term care or skilled nursing facility. Beyond epidemiology, these definitions have been useful in helping the practicing clinician to employ effective empirical antibiotic therapy. The delivery of health care has evolved, however, and the distinction between outpatients and inpatients has been blurred. A broader term that has been suggested for infectious maladies in experienced patients who have moved in and out of the hospital is “healthcare associated” infections (3).
The evolving understanding of the origin of an infection has influenced efforts to define community MRSA. The term “community onset” or “community associated” MRSA can be used to describe a methicillin-resistant S. aureus infection that began incubating outside the hospital. If a patient has historical ties to a traditional treatment setting, the infection is most likely healthcare associated. Notable risk factors include hospitalization or stay in a nursing facility within the past year, use of broad-spectrum antibiotics, surgery, dialysis, intravenous drug use, or the presence of an indwelling vascular catheter. A MRSA infection in a patient presenting from home without any healthcare risk factors can be deemed “community acquired” MRSA (CaMRSA) (4).
A further understanding of CaMRSA can be gleaned from molecular studies of the organism. Methicillin resistance is mediated by a genetic element called staphylococcal cassette chromosome mecA (SCCmecA). MecA codes for a novel penicillin binding protein, PBP 2a, which is not inhibited by beta-lactam antibiotics (2). There are at least 5 types of SCCmecA. Types I through III are typically present in nosocomial MRSA strains. CaMRSA is distinguishable by the presence of SCCmecA IV (4-6).
Another distinctive feature of CaMRSA is the presence of the Panton-Valentine leukocidin (PVL). Previous work has shown that only 2–3% of strains of S. aureus produce this toxin (7). However this virulence factor, encoded by the genes lukS-PV and lukF-PV, appears to be expressed much more commonly in CaMRSA.
The difficulties with defining CaMRSA have influenced attempts to understand its prevalence. The key question in reviewing the available studies is how rigorous an attempt was made to exclude those patients who had significant healthcare contact. Salgado and colleagues performed a meta-analysis to try to determine the prevalence of true CaMRSA. They found that a significant number of subjects included in prevalence studies had identifiable healthcare risk factors, and that when this was accounted for, the overall prevalence of CaMRSA was less than 0.24% (8). The burden of CaMRSA infection will vary however based on location, and certain areas of the United States have demonstrated a higher prevalence. Researchers from the Emerging Infections Program Network examined CaMRSA in Atlanta, Baltimore, and Minnesota and found the prevalence to range from 8% to 20% (9). Of note, only 41% of suspected cases of CaMRSA were confirmed through interviews.
So what is CaMRSA? An acceptable working definition is a methicillin-resistant S. aureus infection occurring in a patient without a history of healthcare risk factors due to an isolate carrying SCCmecA type IV. The isolate is also likely to express the PVL virulence factor. This definition combines what is known about both the clinical and molecular epidemiology of these strains. Further research and time is likely to result in modifications to our understanding of this emerging phenomenon.
Antibiotic Susceptibility Patterns
CaMRSA strains have unique susceptibility patterns compared with traditional MRSA strains. As noted above, SCCmecA codes for methicillin resistance in S. aureus. SCCmecA types II and III are large genetic elements that usually code for resistance to multiple antibiotics. In contrast, type IV is smaller and results in decreased susceptibility to betalactams alone. CaMRSA strains are identifiable as being susceptible to clindamycin, trimethoprim-sulfamethoxazole, and the aminoglycosides (4). Susceptibility to clindamycin must be interpreted cautiously in strains that are erythromycin resistant. If erythromycin resistance is due to an inactivating enzyme (a ribosomal methylase) resistance to clindamycin can be induced. This macrolide-lincosamide-streptogramin–inducible phenotype can be identified in the microbiology lab by performing an erythromycin induction test (D-test). Clinical failures have been described when clindamycin has been used in the presence of this inducible phenotype (10).
Outbreaks
As with many infectious diseases, outbreaks first brought the problem of CaMRSA to wider attention. The first well-described outbreak occurred in the early 1980s among intravenous drug users in Detroit (11). Reports in the early 1990s focused on MRSA infections in young children without risk factors for resistant infection (12). Overwhelming, fatal sepsis due to MRSA was described in 4 pediatric patients in Minnesota and North Dakota. A fulminant, necrotizing pneumonia characterized 3 of the cases (13). Subsequently numerous outbreaks have been described among prison inmates, sexual partners, and competitive sports participants (14-16).
Two well-documented outbreaks have been described in football players. Begier and colleagues identified an outbreak that involved 10 players on the same college football team. Molecular typing demonstrated all recovered isolates to be of the same strain and to carry SCCmecA and the PVL gene. The case-control analysis showed an association between infection and playing wide receiver or cornerback, turf burns, and body shaving (17). An investigation of 8 MRSA infections among professional football players similarly showed all recovered strains to be clonal and to harbor SCCmecA IV and the PVL locus. In contrast to the college outbreak, these investigators found an association between being a lineman or a linebacker and disease. Turf burns were again a significant risk factor (18).
Both of these outbreaks, although geographically separate, were found to be due to the same strain of MRSA, clone USA300-0114. This clone has also been demonstrated as the predominant cause of CaMRSA in other communities (15,19). This would seem to indicate greater fitness of this particular strain that has allowed it to spread widely (20).
Clinical Manifestations
In general, CaMRSA has been reported to cause a similar spectrum of disease as methicillin-susceptible S. aureus (MSSA). As mentioned above, it appears to be seen mostly in otherwise healthy, young individuals. In the population based surveillance project of Fridkin et al., 77% of patients with community MRSA had skin and soft tissue infections (9). Invasive disease was observed in 6%. Similarly, Naimi and colleagues found skin and soft tissue infections in 75% of the subjects in their study of community-associated MRSA in Minnesota (21).
There is concern that CaMRSA may be associated with a greater likelihood of disease compared with other S. aureus strains. Ellis et al. prospectively evaluated active-duty soldiers found to be colonized with CaMRSA. Of the 24 colonized, 38% or 9 individuals developed soft-tissue infections as compared with 3% of those colonized with MSSA. Eight of nine affected patients had abscesses. All 9 of the available clinical isolates were positive for the PVL gene and the presence of this virulence factor was associated with an increased risk of invasive disease (22). Other authors have found an association between PVL-carrying strains of S. aureus and disease and it is perhaps this characteristic, not methicillin resistance, that assists the organism in causing disease in otherwise healthy individuals (23,24). The observed high prevalence of the PVL virulence factor among CaMRSA has been described as the “convergence of resistance and virulence” (25).
Severe disease has also been described due to strains of CaMRSA. Francis described 4 patients with necrotizing pneumonia due to CaMRSA similar to the pediatric cases referred to above. The isolates from all 4 patients carried PVL and SCCmecA IV genes and were of the USA300 strain group (26). Of note, all 4 patients initially had influenza-like illnesses, demonstrating again the association between influenza and staphylococcal pneumonia. This also signifies these presentations were potentially vaccine preventable. Recently, necrotizing fasciitis caused by CaMRSA strains, all again characterized as having PVL genes, has been described (27). This new phenomenon expands the differential diagnosis of causes of this life-threatening soft-tissue syndrome and influences empirical antibiotic selection.
A 41-year-old with Crohn’s disease treated with infliximab undergoes ventral hernia repair. She has a past surgical history of multiple abdominal surgeries. Three weeks postoperatively she is readmitted with a superinfected hematoma requiring operative drainage. Cultures reveal MRSA, susceptible to erythromycin, clindamycin, vancomycin, gentamicin, tetracycline, and trimethoprim-sulfamethoxazole.
The work to date on this new aspect of resistance in S. aureus intimates a trend similar to that previously experienced with penicillin resistance. Penicillinase-producing strains, first recognized in 1944, became increasingly common among hospital isolates after the second World War (28,29). By the 1970s, penicillin-resistant staphylococci had become widespread in the Community as well. Currently, identification of a penicillin-susceptible S. aureus isolate is uncommon.
The potential for further increases in the prevalence of methicillin resistance among staphylococci lies with the SCCmecA complex. Acquisition of this determinant from another resistant clone of either S. aureus or a coagulase-negative staphylococcus is the necessary first step in the process of becoming methicillin resistant. Types I through III are large, and this has been an obstacle to frequent transfers to MSSA strains. The result of this dynamic is that hospital-acquired MRSA to this point has descended from a relatively small number of clones as compared with the wide heterogeneity seen in susceptible S. aureus (30). As mentioned above, SCCmecA IV is smaller and can therefore more easily insert into many different MSSA strains without a loss of fitness. In fact type IV strains have been shown in vitro to replicate faster than hospital MRSA strains (20). This may allow MRSA to begin to displace MSSA as the predominant community phenotype in a manner similar to that in which penicillin-susceptible S. aureus was replaced.
A similar phenomenon may occur in hospitals wherein a typical CaMRSA strain may become the predominant hospital clone. This has been described already in 1 hospital where SCCmecA IV became the major determinant of methicillin resistance in the hospital (31). The trend was identifiable by a “more susceptible” antibiogram of MRSA strains. Future epidemiological surveillance will be necessary as the potential exists for resistant strains to continue to cross the increasingly more permeable barrier between traditional healthcare and the community.
Management
Increasing resistance to S. aureus has several implications for clinicians. Fundamental principles in the management of infectious syndromes become even more important, particularly source control of suppurative foci through debridement and drainage. An added benefit of such procedures is that they facilitate the establishment of a microbiological diagnosis. Clinicians and microbiologists will need to continue to work together closely so as to be aware of resistance trends in their community. In situations where the pathogen is not identified and treatment is prescribed empirically, follow-up is crucial.
Obviously, the emergence of CaMRSA has limited antibiotic choices. Clindamycin, trimethoprim-sulfamethoxazole, and doxycycline remain therapeutic options in the appropriate clinical situation. The severe clinical manifestations described above require consideration of empirical vancomycin in the treatment of patients presenting seriously ill with infectious syndromes that could be potentially due to S. aureus while awaiting culture results. The most extensive experience for inpatient use is with this agent. Linezolid, daptomycin, and quinupristin-dalfopristin are newer agents with activity against MRSA that have been reviewed elsewhere (32,33). Growing experience with these agents has provided options in situations where vancomycin cannot be used. It has also emphasized some of their limitations. Daptomycin and quinupristin-dalfopristin are only given parenterally, while linezolid can be given both orally and intravenously. Expense impacts the use of all three especially outside the hospital. Treatment-limiting cytopenias and peripheral and optic neuropathy have been described with linezolid when it is has been employed for extended courses of therapy. Daptomycin is inhibited by surfactant and therefore should not be used for suspected pulmonary infections. Quinupristin-dalfopristin’s use can be limited by disabling myalgias and the need for central venous access. More data about the use of these newer agents for invasive infections are needed before they can be considered superior to vancomycin.
Dr. Fraser may be reached at frasert@ccf.org.
Dr. Fraser is a member of the Wyeth Emerging Pathogens speakers’ bureau and has participated in a local advisory panel for GlaxoSmithKline. There is no conflict of interest to disclose for this work.
References
- Skinner D, Keefer CS. Significance of bacteremia caused by Staphylococcus aureus. Arch Intern Med. 1941;68:851-75.
- Lowy FD. Antimicrobial resistance: the example of Staphylococcus aureus. J Clin Invest. 2003;111:1265-73.
- Friedman ND, Kaye KS, Stout JE, et al. Health care-associated bloodstream infections in adults: a reason to change the accepted definition of community-acquired infections. Ann Intern Med. 2002;137:791-7.
- Said-Salim B, Mathema B, Kreiswirth BN. Community-acquired methicillin-resistant Staphylococcus aureus: an emerging pathogen. Infect Control Hosp Epidemiol. 2003;24:451-5.
- Carleton HA, Diep BA, Charlebois ED, Sensabaugh GF, Perdreau-Remington F. Community-adapted methicillin-resistant Staphylococcus aureus (MRSA): population dynamics of an expanding community reservoir of MRSA. J Infect Dis. 2004;190:1730-8.
- Daum RS, Ito T, Hiramatsu K, et al. A novel methicillin-resistance cassette in community-acquired methicillin resistant Staphylococcus aureus isolates of diverse genetic backgrounds. J Infect Dis. 2002:186;1344-7.
- Dinges MM, Orwin PM, Schlievert PM. Exotoxins of Staphylococcus aureus. Clin Microbiol Rev. 2000;13:16-34.
- Salgado CD, Farr BM, Calfee DP. Community-acquired methicillin-resistant Staphylococcus aureus: a metaanalysis of prevalence and risk factors. Clin Infect Dis. 2003;36:131-9.
- Fridkin SK, Hageman JC, Morrison M, et al. Methicillinresistant Staphylococcus aureus disease in three communities. N Engl J Med. 2005;352:1436-44.
- Siberry GK, Tekle T, Carroll K, Dick J. Failure of clindamycin treatment of methicillin-resistant Staphylococcus aureus expressing inducible clindamycin resistance in vitro. Clin Infect Dis. 2003;37:1257-60.
- Saravolatz LD, Markowitz N, Arking L, Pohlod D, Fisher E. Methicillin-resistant Staphylococcus aureus. Epidemiologic observations during a community-acquired outbreak. Ann Intern Med. 1982;96:11-6.
- Herold BC, Immergluck LC, Maranan MC, et al. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA. 1998;279:593-598.
- Centers for Disease Control and Prevention. Four pediatric deaths from community acquired methicillin resistant Staphylococcus aureus—Minnesota and North Dakota, 1997-1999. MMWR Morb Mortal Wkly Rep. 1999;48:707-10.
- Centers for Disease Control and Prevention. Methicillin-resistant Staphylococcus aureus infections in correctional facilities—Georgia, California, and Texas, 2001-2003. MMWR Morb Mortal Wkly Rep. 2003;52:992-6.
- Centers for Disease Control and Prevention. Public Health Dispatch: outbreaks of community-associated methicillin-resistant Staphylococcus aureus skin infections—Los Angeles County, California, 2002-2003. MMWR Morb Mortal Wkly Rep. 2003;52:88.
- Lindenmayer JD, Schoenfeld S, O’Grady R, Carney JK. Methicillin-resistant Staphylococcus aureus in a high school wrestling team and the surrounding community. Arch Int Med. 1998;158:895-9.
- Begier EM, Frenette K, Barrett NL, et al. A high-morbidity outbreak of methicillin-resistant Staphylococcus aureus among players on a college football team, facilitated by cosmetic body shaving and turf burns. Clin Infect Dis. 2004;39:1446-53.
- Kazakova SV, Hagerman JC, Matava M, et al. A clone of methicillin-resistant Staphylococcus aureus among professional football players. N Engl J Med. 2005;352: 468-75.
- McDougal LK, Steward CD, Killgore GE, Chaitram JM, McAllister SK, Tenover FC. Pulsed-field gel electrophoresis typing of oxacillin-resistant Staphylococcus aureus isolates from the United States: establishing a national database. J Clin Microbiol. 2003;41:5113-20.
- Deresinski S. Methicillin-resistant Staphylococcus aureus: an evolutionary, epidemiologic, and therapeutic odyssey. Clin Infect Dis. 2005;40:562-73.
- Naimi TS, LeDell KH, Como-Sabetti K, et al. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA. 2003;290:2976-84.
- Ellis MW, Hospenthal DR, Dooley DP, Gray PJ, Murray CK. Natural history of methicillin-resistant Staphylococcus aureus colonization and infection in soldiers. Clin Infect Dis. 2004;39:971-9.
- Yamasaki O, Kaneko J, Morizane S, et al. The association between Staphylococcus aureus strains carrying panton-valentine leukocidin genes and the development of deep-seated follicular infection. Clin Infect Dis. 2005;40:381-5.
- Hsu LY, Koh TH, Kurup A, Low J, Chlebicki MP, Tan BH. High incidence of Panton-Valentine leukocidin-producing Staphylococcus aureus in a tertiary care public hospital in Singapore. Clin Infect Dis. 2005;40:486-9.
- Chambers HF. Community-associated MRSA–resistance and virulence converge. N Engl J Med. 2005;352:1485-7.
- Francis JS, Doherty MC, Lopatin U, et al. Severe community-onset pneumonia in healthy adults caused by methicillin-resistant Staphylococcus aureus carrying the Panton-Valentine leukocidin genes. Clin Infect Dis. 2005;40:100-7.
- Miller LG, Perdreau-Remington F, Rieg G, et al. Necrotizing fasciitis caused by community-associated methicillin-resistant Staphylococcus aureus in Los Angeles. N Engl J Med. 2005;352:1445-53.
- Kirby WMM. Extraction of a highly potent penicillin inactivator from penicillin resistant staphylococci. Science. 1944;99:452-3.
- Chambers HF. The changing epidemiology of Staphylococcus aureus? Emerg Infect Dis. 2001;7:178-82.
- Kreiswirth B, Kornblum J, Arbeit RD, et al. Evidence for a clonal origin of methicillin resistance in Staphylococcus aureus. Science. 1993;259:227-30.
- Donnio PY, Preney L, Gautier-Lerestif AL, Avril JL, Lafforgue N. Changes in staphylococcal chromosome type and antibiotic resistance profile in methicillin-resistant Staphylococcus aureus isolates from a French hospital over an 11 year period. J Antimicrob Chemother. 2004;53:808-13.
- Eliopoulos GM. Quinupristin-dalfopristin and linezolid: evidence and opinion. Clin Infect Dis. 2003;36: 473-81.
- Carpenter CF, Chambers HF. Daptomycin: another novel agent for treating infections due to drug-resistant gram-positive pathogens. Clin Infect Dis. 2004;38: 994-1000.
A 65-year-old male with no significant past medical history, recently returned from a trip to the Democratic Republic of the Congo, presented with pain, swelling, and ulceration of his right lower leg. The symptoms had progressed despite oral amoxicillin/clavulanate. Evaluation at the time of admission revealed a large fluid collection in the anterior calf with extensive subcutaneous edema. Blood cultures were positive for methicillin–resistant S. aureus susceptible to clindamycin, erythromycin, tetracycline, trimethoprim-sulfamethoxazole, gentamicin, and tetracycline. His infection was successfully treated with surgical debridement, wound care, and vancomycin.
In 1941, Skinner and colleagues described the seriousness of S. aureus bloodstream infections in their series of 122 consecutive patients. The mortality rate was greater than 80% (1). Despite early success with penicillin the subsequent decades have shown this organism to be capable of elaborating resistance mechanisms that make therapy increasingly difficult (2). Methicillin resistance, which first appeared in the 1960s, has come to characterize many of the S. aureus isolates that are identified in the hospital. Recently, distinct strains of methicillin-resistant S. aureus (MRSA) are more commonly being identified in patients presenting for care from the community. This review will discuss recent developments in the clinical presentation and epidemiology of community-acquired MRSA in adults.
Definitions and Epidemiology
For infection control and epidemiological purposes, infections have been traditionally termed nosocomial if they 1) were not incubating at the time of presentation, 2) developed more than 72 hours after hospital admission, or 3) occurred in patients who were recently discharged from the hospital or who reside in a long-term care or skilled nursing facility. Beyond epidemiology, these definitions have been useful in helping the practicing clinician to employ effective empirical antibiotic therapy. The delivery of health care has evolved, however, and the distinction between outpatients and inpatients has been blurred. A broader term that has been suggested for infectious maladies in experienced patients who have moved in and out of the hospital is “healthcare associated” infections (3).
The evolving understanding of the origin of an infection has influenced efforts to define community MRSA. The term “community onset” or “community associated” MRSA can be used to describe a methicillin-resistant S. aureus infection that began incubating outside the hospital. If a patient has historical ties to a traditional treatment setting, the infection is most likely healthcare associated. Notable risk factors include hospitalization or stay in a nursing facility within the past year, use of broad-spectrum antibiotics, surgery, dialysis, intravenous drug use, or the presence of an indwelling vascular catheter. A MRSA infection in a patient presenting from home without any healthcare risk factors can be deemed “community acquired” MRSA (CaMRSA) (4).
A further understanding of CaMRSA can be gleaned from molecular studies of the organism. Methicillin resistance is mediated by a genetic element called staphylococcal cassette chromosome mecA (SCCmecA). MecA codes for a novel penicillin binding protein, PBP 2a, which is not inhibited by beta-lactam antibiotics (2). There are at least 5 types of SCCmecA. Types I through III are typically present in nosocomial MRSA strains. CaMRSA is distinguishable by the presence of SCCmecA IV (4-6).
Another distinctive feature of CaMRSA is the presence of the Panton-Valentine leukocidin (PVL). Previous work has shown that only 2–3% of strains of S. aureus produce this toxin (7). However this virulence factor, encoded by the genes lukS-PV and lukF-PV, appears to be expressed much more commonly in CaMRSA.
The difficulties with defining CaMRSA have influenced attempts to understand its prevalence. The key question in reviewing the available studies is how rigorous an attempt was made to exclude those patients who had significant healthcare contact. Salgado and colleagues performed a meta-analysis to try to determine the prevalence of true CaMRSA. They found that a significant number of subjects included in prevalence studies had identifiable healthcare risk factors, and that when this was accounted for, the overall prevalence of CaMRSA was less than 0.24% (8). The burden of CaMRSA infection will vary however based on location, and certain areas of the United States have demonstrated a higher prevalence. Researchers from the Emerging Infections Program Network examined CaMRSA in Atlanta, Baltimore, and Minnesota and found the prevalence to range from 8% to 20% (9). Of note, only 41% of suspected cases of CaMRSA were confirmed through interviews.
So what is CaMRSA? An acceptable working definition is a methicillin-resistant S. aureus infection occurring in a patient without a history of healthcare risk factors due to an isolate carrying SCCmecA type IV. The isolate is also likely to express the PVL virulence factor. This definition combines what is known about both the clinical and molecular epidemiology of these strains. Further research and time is likely to result in modifications to our understanding of this emerging phenomenon.
Antibiotic Susceptibility Patterns
CaMRSA strains have unique susceptibility patterns compared with traditional MRSA strains. As noted above, SCCmecA codes for methicillin resistance in S. aureus. SCCmecA types II and III are large genetic elements that usually code for resistance to multiple antibiotics. In contrast, type IV is smaller and results in decreased susceptibility to betalactams alone. CaMRSA strains are identifiable as being susceptible to clindamycin, trimethoprim-sulfamethoxazole, and the aminoglycosides (4). Susceptibility to clindamycin must be interpreted cautiously in strains that are erythromycin resistant. If erythromycin resistance is due to an inactivating enzyme (a ribosomal methylase) resistance to clindamycin can be induced. This macrolide-lincosamide-streptogramin–inducible phenotype can be identified in the microbiology lab by performing an erythromycin induction test (D-test). Clinical failures have been described when clindamycin has been used in the presence of this inducible phenotype (10).
Outbreaks
As with many infectious diseases, outbreaks first brought the problem of CaMRSA to wider attention. The first well-described outbreak occurred in the early 1980s among intravenous drug users in Detroit (11). Reports in the early 1990s focused on MRSA infections in young children without risk factors for resistant infection (12). Overwhelming, fatal sepsis due to MRSA was described in 4 pediatric patients in Minnesota and North Dakota. A fulminant, necrotizing pneumonia characterized 3 of the cases (13). Subsequently numerous outbreaks have been described among prison inmates, sexual partners, and competitive sports participants (14-16).
Two well-documented outbreaks have been described in football players. Begier and colleagues identified an outbreak that involved 10 players on the same college football team. Molecular typing demonstrated all recovered isolates to be of the same strain and to carry SCCmecA and the PVL gene. The case-control analysis showed an association between infection and playing wide receiver or cornerback, turf burns, and body shaving (17). An investigation of 8 MRSA infections among professional football players similarly showed all recovered strains to be clonal and to harbor SCCmecA IV and the PVL locus. In contrast to the college outbreak, these investigators found an association between being a lineman or a linebacker and disease. Turf burns were again a significant risk factor (18).
Both of these outbreaks, although geographically separate, were found to be due to the same strain of MRSA, clone USA300-0114. This clone has also been demonstrated as the predominant cause of CaMRSA in other communities (15,19). This would seem to indicate greater fitness of this particular strain that has allowed it to spread widely (20).
Clinical Manifestations
In general, CaMRSA has been reported to cause a similar spectrum of disease as methicillin-susceptible S. aureus (MSSA). As mentioned above, it appears to be seen mostly in otherwise healthy, young individuals. In the population based surveillance project of Fridkin et al., 77% of patients with community MRSA had skin and soft tissue infections (9). Invasive disease was observed in 6%. Similarly, Naimi and colleagues found skin and soft tissue infections in 75% of the subjects in their study of community-associated MRSA in Minnesota (21).
There is concern that CaMRSA may be associated with a greater likelihood of disease compared with other S. aureus strains. Ellis et al. prospectively evaluated active-duty soldiers found to be colonized with CaMRSA. Of the 24 colonized, 38% or 9 individuals developed soft-tissue infections as compared with 3% of those colonized with MSSA. Eight of nine affected patients had abscesses. All 9 of the available clinical isolates were positive for the PVL gene and the presence of this virulence factor was associated with an increased risk of invasive disease (22). Other authors have found an association between PVL-carrying strains of S. aureus and disease and it is perhaps this characteristic, not methicillin resistance, that assists the organism in causing disease in otherwise healthy individuals (23,24). The observed high prevalence of the PVL virulence factor among CaMRSA has been described as the “convergence of resistance and virulence” (25).
Severe disease has also been described due to strains of CaMRSA. Francis described 4 patients with necrotizing pneumonia due to CaMRSA similar to the pediatric cases referred to above. The isolates from all 4 patients carried PVL and SCCmecA IV genes and were of the USA300 strain group (26). Of note, all 4 patients initially had influenza-like illnesses, demonstrating again the association between influenza and staphylococcal pneumonia. This also signifies these presentations were potentially vaccine preventable. Recently, necrotizing fasciitis caused by CaMRSA strains, all again characterized as having PVL genes, has been described (27). This new phenomenon expands the differential diagnosis of causes of this life-threatening soft-tissue syndrome and influences empirical antibiotic selection.
A 41-year-old with Crohn’s disease treated with infliximab undergoes ventral hernia repair. She has a past surgical history of multiple abdominal surgeries. Three weeks postoperatively she is readmitted with a superinfected hematoma requiring operative drainage. Cultures reveal MRSA, susceptible to erythromycin, clindamycin, vancomycin, gentamicin, tetracycline, and trimethoprim-sulfamethoxazole.
The work to date on this new aspect of resistance in S. aureus intimates a trend similar to that previously experienced with penicillin resistance. Penicillinase-producing strains, first recognized in 1944, became increasingly common among hospital isolates after the second World War (28,29). By the 1970s, penicillin-resistant staphylococci had become widespread in the Community as well. Currently, identification of a penicillin-susceptible S. aureus isolate is uncommon.
The potential for further increases in the prevalence of methicillin resistance among staphylococci lies with the SCCmecA complex. Acquisition of this determinant from another resistant clone of either S. aureus or a coagulase-negative staphylococcus is the necessary first step in the process of becoming methicillin resistant. Types I through III are large, and this has been an obstacle to frequent transfers to MSSA strains. The result of this dynamic is that hospital-acquired MRSA to this point has descended from a relatively small number of clones as compared with the wide heterogeneity seen in susceptible S. aureus (30). As mentioned above, SCCmecA IV is smaller and can therefore more easily insert into many different MSSA strains without a loss of fitness. In fact type IV strains have been shown in vitro to replicate faster than hospital MRSA strains (20). This may allow MRSA to begin to displace MSSA as the predominant community phenotype in a manner similar to that in which penicillin-susceptible S. aureus was replaced.
A similar phenomenon may occur in hospitals wherein a typical CaMRSA strain may become the predominant hospital clone. This has been described already in 1 hospital where SCCmecA IV became the major determinant of methicillin resistance in the hospital (31). The trend was identifiable by a “more susceptible” antibiogram of MRSA strains. Future epidemiological surveillance will be necessary as the potential exists for resistant strains to continue to cross the increasingly more permeable barrier between traditional healthcare and the community.
Management
Increasing resistance to S. aureus has several implications for clinicians. Fundamental principles in the management of infectious syndromes become even more important, particularly source control of suppurative foci through debridement and drainage. An added benefit of such procedures is that they facilitate the establishment of a microbiological diagnosis. Clinicians and microbiologists will need to continue to work together closely so as to be aware of resistance trends in their community. In situations where the pathogen is not identified and treatment is prescribed empirically, follow-up is crucial.
Obviously, the emergence of CaMRSA has limited antibiotic choices. Clindamycin, trimethoprim-sulfamethoxazole, and doxycycline remain therapeutic options in the appropriate clinical situation. The severe clinical manifestations described above require consideration of empirical vancomycin in the treatment of patients presenting seriously ill with infectious syndromes that could be potentially due to S. aureus while awaiting culture results. The most extensive experience for inpatient use is with this agent. Linezolid, daptomycin, and quinupristin-dalfopristin are newer agents with activity against MRSA that have been reviewed elsewhere (32,33). Growing experience with these agents has provided options in situations where vancomycin cannot be used. It has also emphasized some of their limitations. Daptomycin and quinupristin-dalfopristin are only given parenterally, while linezolid can be given both orally and intravenously. Expense impacts the use of all three especially outside the hospital. Treatment-limiting cytopenias and peripheral and optic neuropathy have been described with linezolid when it is has been employed for extended courses of therapy. Daptomycin is inhibited by surfactant and therefore should not be used for suspected pulmonary infections. Quinupristin-dalfopristin’s use can be limited by disabling myalgias and the need for central venous access. More data about the use of these newer agents for invasive infections are needed before they can be considered superior to vancomycin.
Dr. Fraser may be reached at frasert@ccf.org.
Dr. Fraser is a member of the Wyeth Emerging Pathogens speakers’ bureau and has participated in a local advisory panel for GlaxoSmithKline. There is no conflict of interest to disclose for this work.
References
- Skinner D, Keefer CS. Significance of bacteremia caused by Staphylococcus aureus. Arch Intern Med. 1941;68:851-75.
- Lowy FD. Antimicrobial resistance: the example of Staphylococcus aureus. J Clin Invest. 2003;111:1265-73.
- Friedman ND, Kaye KS, Stout JE, et al. Health care-associated bloodstream infections in adults: a reason to change the accepted definition of community-acquired infections. Ann Intern Med. 2002;137:791-7.
- Said-Salim B, Mathema B, Kreiswirth BN. Community-acquired methicillin-resistant Staphylococcus aureus: an emerging pathogen. Infect Control Hosp Epidemiol. 2003;24:451-5.
- Carleton HA, Diep BA, Charlebois ED, Sensabaugh GF, Perdreau-Remington F. Community-adapted methicillin-resistant Staphylococcus aureus (MRSA): population dynamics of an expanding community reservoir of MRSA. J Infect Dis. 2004;190:1730-8.
- Daum RS, Ito T, Hiramatsu K, et al. A novel methicillin-resistance cassette in community-acquired methicillin resistant Staphylococcus aureus isolates of diverse genetic backgrounds. J Infect Dis. 2002:186;1344-7.
- Dinges MM, Orwin PM, Schlievert PM. Exotoxins of Staphylococcus aureus. Clin Microbiol Rev. 2000;13:16-34.
- Salgado CD, Farr BM, Calfee DP. Community-acquired methicillin-resistant Staphylococcus aureus: a metaanalysis of prevalence and risk factors. Clin Infect Dis. 2003;36:131-9.
- Fridkin SK, Hageman JC, Morrison M, et al. Methicillinresistant Staphylococcus aureus disease in three communities. N Engl J Med. 2005;352:1436-44.
- Siberry GK, Tekle T, Carroll K, Dick J. Failure of clindamycin treatment of methicillin-resistant Staphylococcus aureus expressing inducible clindamycin resistance in vitro. Clin Infect Dis. 2003;37:1257-60.
- Saravolatz LD, Markowitz N, Arking L, Pohlod D, Fisher E. Methicillin-resistant Staphylococcus aureus. Epidemiologic observations during a community-acquired outbreak. Ann Intern Med. 1982;96:11-6.
- Herold BC, Immergluck LC, Maranan MC, et al. Community-acquired methicillin-resistant Staphylococcus aureus in children with no identified predisposing risk. JAMA. 1998;279:593-598.
- Centers for Disease Control and Prevention. Four pediatric deaths from community acquired methicillin resistant Staphylococcus aureus—Minnesota and North Dakota, 1997-1999. MMWR Morb Mortal Wkly Rep. 1999;48:707-10.
- Centers for Disease Control and Prevention. Methicillin-resistant Staphylococcus aureus infections in correctional facilities—Georgia, California, and Texas, 2001-2003. MMWR Morb Mortal Wkly Rep. 2003;52:992-6.
- Centers for Disease Control and Prevention. Public Health Dispatch: outbreaks of community-associated methicillin-resistant Staphylococcus aureus skin infections—Los Angeles County, California, 2002-2003. MMWR Morb Mortal Wkly Rep. 2003;52:88.
- Lindenmayer JD, Schoenfeld S, O’Grady R, Carney JK. Methicillin-resistant Staphylococcus aureus in a high school wrestling team and the surrounding community. Arch Int Med. 1998;158:895-9.
- Begier EM, Frenette K, Barrett NL, et al. A high-morbidity outbreak of methicillin-resistant Staphylococcus aureus among players on a college football team, facilitated by cosmetic body shaving and turf burns. Clin Infect Dis. 2004;39:1446-53.
- Kazakova SV, Hagerman JC, Matava M, et al. A clone of methicillin-resistant Staphylococcus aureus among professional football players. N Engl J Med. 2005;352: 468-75.
- McDougal LK, Steward CD, Killgore GE, Chaitram JM, McAllister SK, Tenover FC. Pulsed-field gel electrophoresis typing of oxacillin-resistant Staphylococcus aureus isolates from the United States: establishing a national database. J Clin Microbiol. 2003;41:5113-20.
- Deresinski S. Methicillin-resistant Staphylococcus aureus: an evolutionary, epidemiologic, and therapeutic odyssey. Clin Infect Dis. 2005;40:562-73.
- Naimi TS, LeDell KH, Como-Sabetti K, et al. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA. 2003;290:2976-84.
- Ellis MW, Hospenthal DR, Dooley DP, Gray PJ, Murray CK. Natural history of methicillin-resistant Staphylococcus aureus colonization and infection in soldiers. Clin Infect Dis. 2004;39:971-9.
- Yamasaki O, Kaneko J, Morizane S, et al. The association between Staphylococcus aureus strains carrying panton-valentine leukocidin genes and the development of deep-seated follicular infection. Clin Infect Dis. 2005;40:381-5.
- Hsu LY, Koh TH, Kurup A, Low J, Chlebicki MP, Tan BH. High incidence of Panton-Valentine leukocidin-producing Staphylococcus aureus in a tertiary care public hospital in Singapore. Clin Infect Dis. 2005;40:486-9.
- Chambers HF. Community-associated MRSA–resistance and virulence converge. N Engl J Med. 2005;352:1485-7.
- Francis JS, Doherty MC, Lopatin U, et al. Severe community-onset pneumonia in healthy adults caused by methicillin-resistant Staphylococcus aureus carrying the Panton-Valentine leukocidin genes. Clin Infect Dis. 2005;40:100-7.
- Miller LG, Perdreau-Remington F, Rieg G, et al. Necrotizing fasciitis caused by community-associated methicillin-resistant Staphylococcus aureus in Los Angeles. N Engl J Med. 2005;352:1445-53.
- Kirby WMM. Extraction of a highly potent penicillin inactivator from penicillin resistant staphylococci. Science. 1944;99:452-3.
- Chambers HF. The changing epidemiology of Staphylococcus aureus? Emerg Infect Dis. 2001;7:178-82.
- Kreiswirth B, Kornblum J, Arbeit RD, et al. Evidence for a clonal origin of methicillin resistance in Staphylococcus aureus. Science. 1993;259:227-30.
- Donnio PY, Preney L, Gautier-Lerestif AL, Avril JL, Lafforgue N. Changes in staphylococcal chromosome type and antibiotic resistance profile in methicillin-resistant Staphylococcus aureus isolates from a French hospital over an 11 year period. J Antimicrob Chemother. 2004;53:808-13.
- Eliopoulos GM. Quinupristin-dalfopristin and linezolid: evidence and opinion. Clin Infect Dis. 2003;36: 473-81.
- Carpenter CF, Chambers HF. Daptomycin: another novel agent for treating infections due to drug-resistant gram-positive pathogens. Clin Infect Dis. 2004;38: 994-1000.
Infective Endocarditis
Introduction
A 55-year-old heroin addict presented to the emergency department, complaining of shaking chills and fevers for 2 weeks. On examination, there was a loud holosystolic murmur, maximally audible in the epigastric space, and a pulsatile liver. Subcutaneous nodular lesions were noted on his palms. Blood cultures grew Pseudomonas aeruginosa. After nearly completing a prolonged course of intravenous antibiotic therapy, the patient died in his washroom from an overdose of heroin. This sad tale, often tragically repeated, represents a continuing challenge to the medical community. The patients’ palm lesions noted were
Osler’s nodes, originally described in 1908 by Sir William Osler, considered by many the father of internal medicine. Osler was born in 1849 and died in 1919. He was an astute clinician and educator, with professorships at McGill University, University of Pennsylvania, Johns Hopkins University, and Oxford University. Osler defined “chronic” infectious endocarditis as an illness lasting longer than 3 months and characterized by low grade fevers. This syndrome was distinct from a “malignant” form, which resulted in early death. Blood cultures usually grew streptococci or, occasionally, staphylococci. Osler made a practice of following his patients to the autopsy table. Vegetations on valves from patients who died of the chronic form looked more like “warts,” and were neither ”ulcerating or very large.” Osler thought anti-streptococcal vaccines might be of some benefit. There was little else to offer. Regardless of the form, nearly all patients died.
In this review, I discuss current methods for the diagnosis and management of infective endocarditis. Cases seen in recent years will illustrate key points.
Case 1 A 39-year-old computer programmer complained of occipital headaches, migratory muscle pains, afternoon fevers, and a 15-pound weight loss for 2 months. He had previously enjoyed excellent health. On examination his temperature was 38.0°C. An apical systolic heart murmur was noted. A transthoracic echocardiogram (TTE) showed mitral regurgitation, with a probable vegetation on the mitral valve. Blood cultures were drawn and the patient was admitted to the hospital. The next day, a transesophageal echocardiogram (TEE) showed perforation of the posterior mitral leaflet. That evening, the patient developed severe right flank pain. CT scan showed infarcts in the right kidney and spleen. The next day the patient underwent urgent mitral valve repair and was dismissed 5 days later to complete a course of intravenous ceftriaxone. All blood cultures grew viridans streptococci, exquisitely susceptible to penicillin.
Comment: This patient represents classic “subacute” bacterial endocarditis with fever, weight loss, and a heart murmur. In most cases, he would be cured with medical therapy alone. However, a TEE showed a lesion that was not appreciated on the initial TTE, and he required urgent surgery to restore a failing mitral valve.
Although the patient had no identified skin or mucosal lesions, when present these suggest the diagnosis. The subconjunctivial sacs and soft palate should be examined for petechiae, the nail beds for splinter hemorrhages, and digits for Janeway lesions.
Osler’s definition of endocarditis included remittent fever, history of valvular heart disease, embolic features, skin lesions, and heart failure. These remain useful bedside observations, and positive blood cultures usually clinch the diagnosis. Perhaps the most important technical advance in recent years for diagnosis is the echocardiogram. The major Duke criteria, published in 1994, include a predictable bacterial organism in blood culture, multiple positive blood cultures with the same organism, or an echocardiogram with definite vegetation, abscess, or valve dehiscence. Any two of the above suffice for diagnosis of probable endocarditis. Accepted minor criteria consist of predisposing lesions, history of intravenous drug abuse, temperature higher than 38°C, vasculitis, skin lesions, or “suggestive” echocardiographic or microbiologic findings. Five of these, or three with one major criterion, support the diagnosis. Transesophageal is superior to transthoracic echocardiography and should be performed if the TTE is equivocal or non-diagnostic.
Case 2 A 31-year-old warehouse manager with progressive dyspnea was transferred from an outside hospital. His illness began 8 months earlier with a dry cough and progressive fatigue. His past history was negative except for an asymptomatic heart murmur. On examination, he was pale and diaphoretic with a temperature of 36°C, pulse 110, and blood pressure of 108/56mm Hg. Neck veins were distended beats/min; loud heart murmurs and diffuse airway crackles were heard. The spleen was palpable. Blood cultures were drawn and antibiotics started.
As the patient was being wheeled for urgent heart surgery, he suffered a huge left-sided stroke. Contrast studies showed a leaking basilar artery aneurysm with subarachnoid hemorrhage. Once his neurologic problem stabilized, urgent mitral and aortic valve replacement was performed. Both valves were severely damaged and rife with vegetations. Admission blood cultures grew viridans streptococci, susceptible to penicillin. After prolonged hospitalization, the patient was transferred for continued care to a rehabilitation unit closer to home.
Comment: Neurologic complications of endocarditis are more common than generally appreciated, and occur in at least one third of patients at the time of diagnosis. Stroke is the most frequent finding, but encephalopathy, retinal embolic lesions, mycotic aneurysm, brain abscess, and meningitis can also occur. Fortunately, most neurologic problems resolve with medical management, but as seen in this patient, some are devastating and have permanent sequelae.
Organisms responsible for the majority of cases of native valve endocarditis are streptococci, as was true in Osler’s time. Staphylococcus aureus is next in frequency, followed by gram-negative bacilli, fungi, coagulase-negative staphylococci, and a poorly-defined category of “culture negative” cases. Therapy for infection caused by penicillin-susceptible streptococci is straightforward. The preferred agent is intravenous penicillin or ampicillin, with ceftraxione or vancomycin as alternatives. Streptococci less susceptible to penicillin, including nutritionally variant organisms, are treated more vigorously with a penicillin and low-dose aminoglycoside.
The HACEK group of gram-negative bacteria (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, and Kingella species) often produce large vegetations. Embolic lesions to major organs or extremities are a fairly common presenting feature. Treatment with ceftriaxone or ampicillin plus gentamicin is usually successful.
“Culture negative” endocarditis includes infections due to microorganisms difficult to culture on standard media. These uncommon pathogens include Bartonella, Brucella, Chlamydia, Coxiella, Francisella, Legionella, and Tropheryma whippeli.
Bartonella endocarditis has been reported in the homeless population. Blood cultures are usually negative. Serology is helpful. More recently, polymerase drain reactions (PCR) from resected valve tissue have proven useful. Treatment of choice is ampicillin plus gentamicin, but mortality remains approximately 25%.
Patients with endocarditis due to Coxiella burnetii (Q fever) are likewise difficult to diagnose. They may not have fever. However, there is generally underlying valvular heart disease, and frequently patients are immunosuppressed. Vegetations are rarely detected on echocardiogram. Routine blood cultures are negative. Fortunately, serology is quite specific for the diagnosis. A combination of doxycycline and chloroquine is the current treatment of choice.
PCR and special immunohistochemical techniques may be useful in the diagnosis of these unusual etiologies. Unfortunately, the methodology is not currently available at most hospitals. Broad-range PCR on surgical tissue help to identify more typical organisms (staphylococci and streptococci), whose growth may be suppressed by conventional antibiotic therapy. Although promising, PCR technology may lack specificity in these cases.
Case 3 A 61-year-old executive was admitted with a 4 week history of fevers and fatigue. Three months earlier he had undergone a bovine aortic valve replacement with mitral valve repair. Blood cultures drawn by a local physician grew methicillin-resistant Staphylococcus epidermidis (MRSE). Despite antibiotics, the patient’s fatigue persisted and he returned for further evaluation. On examination, he was afebrile, with a resting pulse of 71 beats/min and a blood pressure of 135/63mm Hg. However, he was very pale. Loud systolic and diastolic murmurs were heard throughout the precordium. His spleen was enlarged and very soft.
The patient underwent urgent reoperation. At surgery, partial aortic valve dehiscence as a result of a large subprosthetic abscess was discovered. Both aortic and mitral valve were replaced. Admission and operative cultures were negative on antibiotic therapy.
Comment: This is a classic presentation of early-onset prosthetic valve endocarditis. Usual organisms are S. epidermidis and S. aureus Streptococci, vancomycin-resistant enterococci (VRE), diphtheroids, gram-negative bacilli, and fungi (yeast and molds) are all seen in this setting, albeit less frequently.
S. epidermidis is of special interest because it produces hemolysins, grows very slowly on cell surfaces, and binds to host and foreign proteins. This biofilm creates a barrier to host defenses and appears to neutralize certain antibiotics. In addition there is clonal variability, with some isolates fully susceptible to oxacillin, while other clones are resistant.
Standard therapy for staphylococcal prosthetic valve endocarditis is oxacillin with gentamicin and rifampin. For oxacillin-resistant species, vancomycin is substituted. Prosthetic valve enterococcal endocarditis resistant to both penicillin and vancomycin is a growing concern. Some medical centers report VRE colonization rates as high as 30%. Therapy is daunting. For strains with a minimum inhibitory concentrations (MIC) less than 128 gr/mL to ampicillin, ampicillin/sulbactam plus an aminoglycoside has been recommended. For strains totally resistant to ampicillin, quinupristin/dalfopristin, linezolid, or daptomycin may be tried, but the overall success rate is probably no better than 50%.
Case 4 A 31-year-old automobile mechanic underwent aortic valve and graft replacement for severe aortic regurgitation with a large aneurysm of the ascending aorta. His post-operative course was complicated by massive bleeding at the distal graft anastomosis, and respiratory failure. After prolonged hospitalization, the patient was discharged improved, but 2 days later he complained of blurred vision and fevers. His wife noted a green hue from his right pupil. The patient was readmitted and started on intravenous acyclovir for presumed acute retinal necrosis. However, several days later, vitrectomy fluid grew Pseudoallescheria boydii.
Therapy was switched to intravenous miconazole but, shortly afterward, the patient suffered a cardiac arrest. Although his pulse and blood pressure were restored, he remained comatose and support was withdrawn. At autopsy, invasive prosthetic aortic valve and graft endocarditis was noted. Blood and tissue cultures also grew P. boydii.
Comment: Fungal prosthetic valve endocarditis is a devastating disease. Predisposing factors are prolonged use of central vascular catheters, often for antibiotic therapy or parenteral nutrition, and immunosuppression. Most success has been reported combining surgery with intravenous antifungal therapy. Patients should be continued on oral suppressive therapy afterward to prevent relapse later in life.
“Pacemaker endocarditis,” seen with increasing frequency, applies to pacemakers, defibrillators, or combinations thereof. Usual causes are skin flora microbes (staphylococci and Propionibacterium species) that gain access through a generator pocket wound. An echocardiogram may not show vegetations unless they extend to the tricuspid valve. Removal of all hardware, combined with intravenous antibiotic therapy, is necessary for cure. Some impacted leads require open heart surgery for removal.
Hospital-associated bacteremia from another source may spread to a heart valve or pacemaker lead, causing endocarditis. S. aureus bacteremia from intravenous catheters, hemodialysis fistula, and surgical wounds is most likely to do this. Patients on hemodialysis may be colonized with methicillin-resistant S. aureus (MRSA), a risk factor for infection. While intra-nasal mupirocin ointment may reduce MRSA colonization transiently, it is probably not effective for long-term prophylaxis.
Case 5 A 54-year-old accountant was admitted with chills and palpitations for several days. A bovine aortic valve prosthesis had been implanted 2 years earlier. The patient had complained of intermittent fevers for 6 months. A single blood culture had grown Propionibacterium acnes. Although a TEE was interpreted as normal, he was treated with intravenous vancomycin. Follow-up blood cultures were negative and a TTE was read as normal.
On examination, the patient was acutely ill with distended neck veins. His pulse was 50 beats/min and blood pressure 110/50mm Hg. Systolic and diastolic murmurs were present. Blood cultures were drawn, and antibiotics started.
An electrocardiogram showed heart block. A temporary pacemaker was placed. A TEE revealed a huge atrial septal abscess with a fistula from the right atrium to the aorta. The patient was taken emergently to surgery, where the prosthesis was found to have nearly completely dehisced. The fistula was resected and the aortic valve replaced with a homograft. Postoperatively the patient remained in cardiogenic shock and died. Admission blood and valve cultures subsequently grew P. acnes.
Comment and Conclusions
Continued fevers despite appropriate antibiotic and medical management are cause for alarm. Ring abscesses may develop. This is a clear indication for surgical intervention. Fevers may also be caused by embolic events (arterial or venous), drug reactions, and intravascular catheter-related infections. Close monitoring is necessary to avoid major events. Vigilance should be maintained for widening pulse pressures and rhythm disturbances as these are ominous signs of progressive infection.
Indications for urgent surgery include progressive valvular dysfunction; aortic root, ring or septal abscesses; large vegetations (greater than l cm in diameter); and organisms such as VRE, MRSA, Pseudomonas species, and fungi refractive to antimicrobial therapy. It is important to note that, even with appropriate therapy and a bacteriologic “cure,” about one half of patients will have enough valve damage to require surgery later in life.
Despite our best efforts, the death rate from infective endocarditis remains in the range of 10–20%. Death is more likely with prosthetic valve endocarditis and when the organism is S. aureus. Patients still succumb from congestive heart failure, embolic phenomenon, and ruptured mycotic aneurysms, just as they did during Osler’s time.
It is clear there is room for improvement in the diagnosis and management of endocarditis. First, we must continue to refine microbiologic techniques, to allow diagnosis more quickly and accurately. Second, we must develop more effective antimicrobial therapy, especially for pathogens resistant to conventional antimicrobials. Third, we must learn how to combat biofilms. Perhaps in the future we can avoid removal of foreign materials. Finally, we must follow our patients closely and pursue timely surgical intervention when indicated. In recent years this has become more difficult, because patients, once stabilized, are often discharged home or to a skilled nursing facility to complete antibiotic therapy.
While we have learned more about infective endocarditis over the past quarter century, the challenges we face today are greater than ever before.
References
- Osler W. Chronic infectious endocarditis. Q J Med. 1909;2: 219-30.
- Mylonakis E, Calderwood SB. Infective endocarditis in adults. N Engl J Med. 2001;345:1318-30.
- Durack DT, Lukes AS, Bright KD, et al: New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Am J Med. 1994;96:200-9.
- Salgado AV, Furlan AJ, Keys TF. Neurologic complications of endocarditis: a 12 year experience. Neurology. 1989;39:173-8.
- Wilson WR, Karchmer AW, Dajani AS, et al: Antibiotic treatment of adults with infective endocarditis due to streptococci, enterococci, staphylococci and HACEK micro organisms. JAMA. 1995;274:1706-13.
- Lepidi H, Houpikian P, Liang Z, Raoult D. Cardiac valves in patients with Q-fever endocarditis. J Infect Dis. 2003;187: 1097-106.
- Bosshard PP, Kronenberg A, Zbinden R, et al. Etiologic diagnosis of infective endocarditis by broad-range PCR. Clin Infect Dis. 2003;37:167-72.
- Keys TF. Early-onset prosthetic valve endocarditis. Cleve Clin J Med. 1993;60:455-9.
- Proctor RA. Coagulase-negative staphylococcal infection: a diagnostic and therapeutic challenge. Clin Infect Dis. 2000;31:31-3.
- Melgar GR, Nasser RM, Gordon SM, et al. Fungal prosthetic-valve endocarditis in 16 patients: an 11-year experience in a tertiary care hospital. Medicine. 1997;76:94-103.
- Fowler VG, Sanders LL, Kong LK, et al. Infective endocarditis due to Staphylococcus aureus. Clin Infect Dis. 1999;28:106-14.
- Douglas A, Moore-Gillon J, Eykyn S. Fever during treatment of infective endocarditis. Lancet. 1986;1:1341-3.
- Tornos MP, Permanyer-Miralda G, Olona J, et al. Long term complications of native valve endocarditis in non-addicts: a 15 year follow up study. Ann Intern Med. 1992;117:567-72.
- Andrews MM, Von Reyn CF. Patients election criteria and management guidelines for outpatient parenteral antibiotic therapy for native valve infective endocarditis. Clin Infect Dis. 2001;32:203-9.
Introduction
A 55-year-old heroin addict presented to the emergency department, complaining of shaking chills and fevers for 2 weeks. On examination, there was a loud holosystolic murmur, maximally audible in the epigastric space, and a pulsatile liver. Subcutaneous nodular lesions were noted on his palms. Blood cultures grew Pseudomonas aeruginosa. After nearly completing a prolonged course of intravenous antibiotic therapy, the patient died in his washroom from an overdose of heroin. This sad tale, often tragically repeated, represents a continuing challenge to the medical community. The patients’ palm lesions noted were
Osler’s nodes, originally described in 1908 by Sir William Osler, considered by many the father of internal medicine. Osler was born in 1849 and died in 1919. He was an astute clinician and educator, with professorships at McGill University, University of Pennsylvania, Johns Hopkins University, and Oxford University. Osler defined “chronic” infectious endocarditis as an illness lasting longer than 3 months and characterized by low grade fevers. This syndrome was distinct from a “malignant” form, which resulted in early death. Blood cultures usually grew streptococci or, occasionally, staphylococci. Osler made a practice of following his patients to the autopsy table. Vegetations on valves from patients who died of the chronic form looked more like “warts,” and were neither ”ulcerating or very large.” Osler thought anti-streptococcal vaccines might be of some benefit. There was little else to offer. Regardless of the form, nearly all patients died.
In this review, I discuss current methods for the diagnosis and management of infective endocarditis. Cases seen in recent years will illustrate key points.
Case 1 A 39-year-old computer programmer complained of occipital headaches, migratory muscle pains, afternoon fevers, and a 15-pound weight loss for 2 months. He had previously enjoyed excellent health. On examination his temperature was 38.0°C. An apical systolic heart murmur was noted. A transthoracic echocardiogram (TTE) showed mitral regurgitation, with a probable vegetation on the mitral valve. Blood cultures were drawn and the patient was admitted to the hospital. The next day, a transesophageal echocardiogram (TEE) showed perforation of the posterior mitral leaflet. That evening, the patient developed severe right flank pain. CT scan showed infarcts in the right kidney and spleen. The next day the patient underwent urgent mitral valve repair and was dismissed 5 days later to complete a course of intravenous ceftriaxone. All blood cultures grew viridans streptococci, exquisitely susceptible to penicillin.
Comment: This patient represents classic “subacute” bacterial endocarditis with fever, weight loss, and a heart murmur. In most cases, he would be cured with medical therapy alone. However, a TEE showed a lesion that was not appreciated on the initial TTE, and he required urgent surgery to restore a failing mitral valve.
Although the patient had no identified skin or mucosal lesions, when present these suggest the diagnosis. The subconjunctivial sacs and soft palate should be examined for petechiae, the nail beds for splinter hemorrhages, and digits for Janeway lesions.
Osler’s definition of endocarditis included remittent fever, history of valvular heart disease, embolic features, skin lesions, and heart failure. These remain useful bedside observations, and positive blood cultures usually clinch the diagnosis. Perhaps the most important technical advance in recent years for diagnosis is the echocardiogram. The major Duke criteria, published in 1994, include a predictable bacterial organism in blood culture, multiple positive blood cultures with the same organism, or an echocardiogram with definite vegetation, abscess, or valve dehiscence. Any two of the above suffice for diagnosis of probable endocarditis. Accepted minor criteria consist of predisposing lesions, history of intravenous drug abuse, temperature higher than 38°C, vasculitis, skin lesions, or “suggestive” echocardiographic or microbiologic findings. Five of these, or three with one major criterion, support the diagnosis. Transesophageal is superior to transthoracic echocardiography and should be performed if the TTE is equivocal or non-diagnostic.
Case 2 A 31-year-old warehouse manager with progressive dyspnea was transferred from an outside hospital. His illness began 8 months earlier with a dry cough and progressive fatigue. His past history was negative except for an asymptomatic heart murmur. On examination, he was pale and diaphoretic with a temperature of 36°C, pulse 110, and blood pressure of 108/56mm Hg. Neck veins were distended beats/min; loud heart murmurs and diffuse airway crackles were heard. The spleen was palpable. Blood cultures were drawn and antibiotics started.
As the patient was being wheeled for urgent heart surgery, he suffered a huge left-sided stroke. Contrast studies showed a leaking basilar artery aneurysm with subarachnoid hemorrhage. Once his neurologic problem stabilized, urgent mitral and aortic valve replacement was performed. Both valves were severely damaged and rife with vegetations. Admission blood cultures grew viridans streptococci, susceptible to penicillin. After prolonged hospitalization, the patient was transferred for continued care to a rehabilitation unit closer to home.
Comment: Neurologic complications of endocarditis are more common than generally appreciated, and occur in at least one third of patients at the time of diagnosis. Stroke is the most frequent finding, but encephalopathy, retinal embolic lesions, mycotic aneurysm, brain abscess, and meningitis can also occur. Fortunately, most neurologic problems resolve with medical management, but as seen in this patient, some are devastating and have permanent sequelae.
Organisms responsible for the majority of cases of native valve endocarditis are streptococci, as was true in Osler’s time. Staphylococcus aureus is next in frequency, followed by gram-negative bacilli, fungi, coagulase-negative staphylococci, and a poorly-defined category of “culture negative” cases. Therapy for infection caused by penicillin-susceptible streptococci is straightforward. The preferred agent is intravenous penicillin or ampicillin, with ceftraxione or vancomycin as alternatives. Streptococci less susceptible to penicillin, including nutritionally variant organisms, are treated more vigorously with a penicillin and low-dose aminoglycoside.
The HACEK group of gram-negative bacteria (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, and Kingella species) often produce large vegetations. Embolic lesions to major organs or extremities are a fairly common presenting feature. Treatment with ceftriaxone or ampicillin plus gentamicin is usually successful.
“Culture negative” endocarditis includes infections due to microorganisms difficult to culture on standard media. These uncommon pathogens include Bartonella, Brucella, Chlamydia, Coxiella, Francisella, Legionella, and Tropheryma whippeli.
Bartonella endocarditis has been reported in the homeless population. Blood cultures are usually negative. Serology is helpful. More recently, polymerase drain reactions (PCR) from resected valve tissue have proven useful. Treatment of choice is ampicillin plus gentamicin, but mortality remains approximately 25%.
Patients with endocarditis due to Coxiella burnetii (Q fever) are likewise difficult to diagnose. They may not have fever. However, there is generally underlying valvular heart disease, and frequently patients are immunosuppressed. Vegetations are rarely detected on echocardiogram. Routine blood cultures are negative. Fortunately, serology is quite specific for the diagnosis. A combination of doxycycline and chloroquine is the current treatment of choice.
PCR and special immunohistochemical techniques may be useful in the diagnosis of these unusual etiologies. Unfortunately, the methodology is not currently available at most hospitals. Broad-range PCR on surgical tissue help to identify more typical organisms (staphylococci and streptococci), whose growth may be suppressed by conventional antibiotic therapy. Although promising, PCR technology may lack specificity in these cases.
Case 3 A 61-year-old executive was admitted with a 4 week history of fevers and fatigue. Three months earlier he had undergone a bovine aortic valve replacement with mitral valve repair. Blood cultures drawn by a local physician grew methicillin-resistant Staphylococcus epidermidis (MRSE). Despite antibiotics, the patient’s fatigue persisted and he returned for further evaluation. On examination, he was afebrile, with a resting pulse of 71 beats/min and a blood pressure of 135/63mm Hg. However, he was very pale. Loud systolic and diastolic murmurs were heard throughout the precordium. His spleen was enlarged and very soft.
The patient underwent urgent reoperation. At surgery, partial aortic valve dehiscence as a result of a large subprosthetic abscess was discovered. Both aortic and mitral valve were replaced. Admission and operative cultures were negative on antibiotic therapy.
Comment: This is a classic presentation of early-onset prosthetic valve endocarditis. Usual organisms are S. epidermidis and S. aureus Streptococci, vancomycin-resistant enterococci (VRE), diphtheroids, gram-negative bacilli, and fungi (yeast and molds) are all seen in this setting, albeit less frequently.
S. epidermidis is of special interest because it produces hemolysins, grows very slowly on cell surfaces, and binds to host and foreign proteins. This biofilm creates a barrier to host defenses and appears to neutralize certain antibiotics. In addition there is clonal variability, with some isolates fully susceptible to oxacillin, while other clones are resistant.
Standard therapy for staphylococcal prosthetic valve endocarditis is oxacillin with gentamicin and rifampin. For oxacillin-resistant species, vancomycin is substituted. Prosthetic valve enterococcal endocarditis resistant to both penicillin and vancomycin is a growing concern. Some medical centers report VRE colonization rates as high as 30%. Therapy is daunting. For strains with a minimum inhibitory concentrations (MIC) less than 128 gr/mL to ampicillin, ampicillin/sulbactam plus an aminoglycoside has been recommended. For strains totally resistant to ampicillin, quinupristin/dalfopristin, linezolid, or daptomycin may be tried, but the overall success rate is probably no better than 50%.
Case 4 A 31-year-old automobile mechanic underwent aortic valve and graft replacement for severe aortic regurgitation with a large aneurysm of the ascending aorta. His post-operative course was complicated by massive bleeding at the distal graft anastomosis, and respiratory failure. After prolonged hospitalization, the patient was discharged improved, but 2 days later he complained of blurred vision and fevers. His wife noted a green hue from his right pupil. The patient was readmitted and started on intravenous acyclovir for presumed acute retinal necrosis. However, several days later, vitrectomy fluid grew Pseudoallescheria boydii.
Therapy was switched to intravenous miconazole but, shortly afterward, the patient suffered a cardiac arrest. Although his pulse and blood pressure were restored, he remained comatose and support was withdrawn. At autopsy, invasive prosthetic aortic valve and graft endocarditis was noted. Blood and tissue cultures also grew P. boydii.
Comment: Fungal prosthetic valve endocarditis is a devastating disease. Predisposing factors are prolonged use of central vascular catheters, often for antibiotic therapy or parenteral nutrition, and immunosuppression. Most success has been reported combining surgery with intravenous antifungal therapy. Patients should be continued on oral suppressive therapy afterward to prevent relapse later in life.
“Pacemaker endocarditis,” seen with increasing frequency, applies to pacemakers, defibrillators, or combinations thereof. Usual causes are skin flora microbes (staphylococci and Propionibacterium species) that gain access through a generator pocket wound. An echocardiogram may not show vegetations unless they extend to the tricuspid valve. Removal of all hardware, combined with intravenous antibiotic therapy, is necessary for cure. Some impacted leads require open heart surgery for removal.
Hospital-associated bacteremia from another source may spread to a heart valve or pacemaker lead, causing endocarditis. S. aureus bacteremia from intravenous catheters, hemodialysis fistula, and surgical wounds is most likely to do this. Patients on hemodialysis may be colonized with methicillin-resistant S. aureus (MRSA), a risk factor for infection. While intra-nasal mupirocin ointment may reduce MRSA colonization transiently, it is probably not effective for long-term prophylaxis.
Case 5 A 54-year-old accountant was admitted with chills and palpitations for several days. A bovine aortic valve prosthesis had been implanted 2 years earlier. The patient had complained of intermittent fevers for 6 months. A single blood culture had grown Propionibacterium acnes. Although a TEE was interpreted as normal, he was treated with intravenous vancomycin. Follow-up blood cultures were negative and a TTE was read as normal.
On examination, the patient was acutely ill with distended neck veins. His pulse was 50 beats/min and blood pressure 110/50mm Hg. Systolic and diastolic murmurs were present. Blood cultures were drawn, and antibiotics started.
An electrocardiogram showed heart block. A temporary pacemaker was placed. A TEE revealed a huge atrial septal abscess with a fistula from the right atrium to the aorta. The patient was taken emergently to surgery, where the prosthesis was found to have nearly completely dehisced. The fistula was resected and the aortic valve replaced with a homograft. Postoperatively the patient remained in cardiogenic shock and died. Admission blood and valve cultures subsequently grew P. acnes.
Comment and Conclusions
Continued fevers despite appropriate antibiotic and medical management are cause for alarm. Ring abscesses may develop. This is a clear indication for surgical intervention. Fevers may also be caused by embolic events (arterial or venous), drug reactions, and intravascular catheter-related infections. Close monitoring is necessary to avoid major events. Vigilance should be maintained for widening pulse pressures and rhythm disturbances as these are ominous signs of progressive infection.
Indications for urgent surgery include progressive valvular dysfunction; aortic root, ring or septal abscesses; large vegetations (greater than l cm in diameter); and organisms such as VRE, MRSA, Pseudomonas species, and fungi refractive to antimicrobial therapy. It is important to note that, even with appropriate therapy and a bacteriologic “cure,” about one half of patients will have enough valve damage to require surgery later in life.
Despite our best efforts, the death rate from infective endocarditis remains in the range of 10–20%. Death is more likely with prosthetic valve endocarditis and when the organism is S. aureus. Patients still succumb from congestive heart failure, embolic phenomenon, and ruptured mycotic aneurysms, just as they did during Osler’s time.
It is clear there is room for improvement in the diagnosis and management of endocarditis. First, we must continue to refine microbiologic techniques, to allow diagnosis more quickly and accurately. Second, we must develop more effective antimicrobial therapy, especially for pathogens resistant to conventional antimicrobials. Third, we must learn how to combat biofilms. Perhaps in the future we can avoid removal of foreign materials. Finally, we must follow our patients closely and pursue timely surgical intervention when indicated. In recent years this has become more difficult, because patients, once stabilized, are often discharged home or to a skilled nursing facility to complete antibiotic therapy.
While we have learned more about infective endocarditis over the past quarter century, the challenges we face today are greater than ever before.
References
- Osler W. Chronic infectious endocarditis. Q J Med. 1909;2: 219-30.
- Mylonakis E, Calderwood SB. Infective endocarditis in adults. N Engl J Med. 2001;345:1318-30.
- Durack DT, Lukes AS, Bright KD, et al: New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Am J Med. 1994;96:200-9.
- Salgado AV, Furlan AJ, Keys TF. Neurologic complications of endocarditis: a 12 year experience. Neurology. 1989;39:173-8.
- Wilson WR, Karchmer AW, Dajani AS, et al: Antibiotic treatment of adults with infective endocarditis due to streptococci, enterococci, staphylococci and HACEK micro organisms. JAMA. 1995;274:1706-13.
- Lepidi H, Houpikian P, Liang Z, Raoult D. Cardiac valves in patients with Q-fever endocarditis. J Infect Dis. 2003;187: 1097-106.
- Bosshard PP, Kronenberg A, Zbinden R, et al. Etiologic diagnosis of infective endocarditis by broad-range PCR. Clin Infect Dis. 2003;37:167-72.
- Keys TF. Early-onset prosthetic valve endocarditis. Cleve Clin J Med. 1993;60:455-9.
- Proctor RA. Coagulase-negative staphylococcal infection: a diagnostic and therapeutic challenge. Clin Infect Dis. 2000;31:31-3.
- Melgar GR, Nasser RM, Gordon SM, et al. Fungal prosthetic-valve endocarditis in 16 patients: an 11-year experience in a tertiary care hospital. Medicine. 1997;76:94-103.
- Fowler VG, Sanders LL, Kong LK, et al. Infective endocarditis due to Staphylococcus aureus. Clin Infect Dis. 1999;28:106-14.
- Douglas A, Moore-Gillon J, Eykyn S. Fever during treatment of infective endocarditis. Lancet. 1986;1:1341-3.
- Tornos MP, Permanyer-Miralda G, Olona J, et al. Long term complications of native valve endocarditis in non-addicts: a 15 year follow up study. Ann Intern Med. 1992;117:567-72.
- Andrews MM, Von Reyn CF. Patients election criteria and management guidelines for outpatient parenteral antibiotic therapy for native valve infective endocarditis. Clin Infect Dis. 2001;32:203-9.
Introduction
A 55-year-old heroin addict presented to the emergency department, complaining of shaking chills and fevers for 2 weeks. On examination, there was a loud holosystolic murmur, maximally audible in the epigastric space, and a pulsatile liver. Subcutaneous nodular lesions were noted on his palms. Blood cultures grew Pseudomonas aeruginosa. After nearly completing a prolonged course of intravenous antibiotic therapy, the patient died in his washroom from an overdose of heroin. This sad tale, often tragically repeated, represents a continuing challenge to the medical community. The patients’ palm lesions noted were
Osler’s nodes, originally described in 1908 by Sir William Osler, considered by many the father of internal medicine. Osler was born in 1849 and died in 1919. He was an astute clinician and educator, with professorships at McGill University, University of Pennsylvania, Johns Hopkins University, and Oxford University. Osler defined “chronic” infectious endocarditis as an illness lasting longer than 3 months and characterized by low grade fevers. This syndrome was distinct from a “malignant” form, which resulted in early death. Blood cultures usually grew streptococci or, occasionally, staphylococci. Osler made a practice of following his patients to the autopsy table. Vegetations on valves from patients who died of the chronic form looked more like “warts,” and were neither ”ulcerating or very large.” Osler thought anti-streptococcal vaccines might be of some benefit. There was little else to offer. Regardless of the form, nearly all patients died.
In this review, I discuss current methods for the diagnosis and management of infective endocarditis. Cases seen in recent years will illustrate key points.
Case 1 A 39-year-old computer programmer complained of occipital headaches, migratory muscle pains, afternoon fevers, and a 15-pound weight loss for 2 months. He had previously enjoyed excellent health. On examination his temperature was 38.0°C. An apical systolic heart murmur was noted. A transthoracic echocardiogram (TTE) showed mitral regurgitation, with a probable vegetation on the mitral valve. Blood cultures were drawn and the patient was admitted to the hospital. The next day, a transesophageal echocardiogram (TEE) showed perforation of the posterior mitral leaflet. That evening, the patient developed severe right flank pain. CT scan showed infarcts in the right kidney and spleen. The next day the patient underwent urgent mitral valve repair and was dismissed 5 days later to complete a course of intravenous ceftriaxone. All blood cultures grew viridans streptococci, exquisitely susceptible to penicillin.
Comment: This patient represents classic “subacute” bacterial endocarditis with fever, weight loss, and a heart murmur. In most cases, he would be cured with medical therapy alone. However, a TEE showed a lesion that was not appreciated on the initial TTE, and he required urgent surgery to restore a failing mitral valve.
Although the patient had no identified skin or mucosal lesions, when present these suggest the diagnosis. The subconjunctivial sacs and soft palate should be examined for petechiae, the nail beds for splinter hemorrhages, and digits for Janeway lesions.
Osler’s definition of endocarditis included remittent fever, history of valvular heart disease, embolic features, skin lesions, and heart failure. These remain useful bedside observations, and positive blood cultures usually clinch the diagnosis. Perhaps the most important technical advance in recent years for diagnosis is the echocardiogram. The major Duke criteria, published in 1994, include a predictable bacterial organism in blood culture, multiple positive blood cultures with the same organism, or an echocardiogram with definite vegetation, abscess, or valve dehiscence. Any two of the above suffice for diagnosis of probable endocarditis. Accepted minor criteria consist of predisposing lesions, history of intravenous drug abuse, temperature higher than 38°C, vasculitis, skin lesions, or “suggestive” echocardiographic or microbiologic findings. Five of these, or three with one major criterion, support the diagnosis. Transesophageal is superior to transthoracic echocardiography and should be performed if the TTE is equivocal or non-diagnostic.
Case 2 A 31-year-old warehouse manager with progressive dyspnea was transferred from an outside hospital. His illness began 8 months earlier with a dry cough and progressive fatigue. His past history was negative except for an asymptomatic heart murmur. On examination, he was pale and diaphoretic with a temperature of 36°C, pulse 110, and blood pressure of 108/56mm Hg. Neck veins were distended beats/min; loud heart murmurs and diffuse airway crackles were heard. The spleen was palpable. Blood cultures were drawn and antibiotics started.
As the patient was being wheeled for urgent heart surgery, he suffered a huge left-sided stroke. Contrast studies showed a leaking basilar artery aneurysm with subarachnoid hemorrhage. Once his neurologic problem stabilized, urgent mitral and aortic valve replacement was performed. Both valves were severely damaged and rife with vegetations. Admission blood cultures grew viridans streptococci, susceptible to penicillin. After prolonged hospitalization, the patient was transferred for continued care to a rehabilitation unit closer to home.
Comment: Neurologic complications of endocarditis are more common than generally appreciated, and occur in at least one third of patients at the time of diagnosis. Stroke is the most frequent finding, but encephalopathy, retinal embolic lesions, mycotic aneurysm, brain abscess, and meningitis can also occur. Fortunately, most neurologic problems resolve with medical management, but as seen in this patient, some are devastating and have permanent sequelae.
Organisms responsible for the majority of cases of native valve endocarditis are streptococci, as was true in Osler’s time. Staphylococcus aureus is next in frequency, followed by gram-negative bacilli, fungi, coagulase-negative staphylococci, and a poorly-defined category of “culture negative” cases. Therapy for infection caused by penicillin-susceptible streptococci is straightforward. The preferred agent is intravenous penicillin or ampicillin, with ceftraxione or vancomycin as alternatives. Streptococci less susceptible to penicillin, including nutritionally variant organisms, are treated more vigorously with a penicillin and low-dose aminoglycoside.
The HACEK group of gram-negative bacteria (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, and Kingella species) often produce large vegetations. Embolic lesions to major organs or extremities are a fairly common presenting feature. Treatment with ceftriaxone or ampicillin plus gentamicin is usually successful.
“Culture negative” endocarditis includes infections due to microorganisms difficult to culture on standard media. These uncommon pathogens include Bartonella, Brucella, Chlamydia, Coxiella, Francisella, Legionella, and Tropheryma whippeli.
Bartonella endocarditis has been reported in the homeless population. Blood cultures are usually negative. Serology is helpful. More recently, polymerase drain reactions (PCR) from resected valve tissue have proven useful. Treatment of choice is ampicillin plus gentamicin, but mortality remains approximately 25%.
Patients with endocarditis due to Coxiella burnetii (Q fever) are likewise difficult to diagnose. They may not have fever. However, there is generally underlying valvular heart disease, and frequently patients are immunosuppressed. Vegetations are rarely detected on echocardiogram. Routine blood cultures are negative. Fortunately, serology is quite specific for the diagnosis. A combination of doxycycline and chloroquine is the current treatment of choice.
PCR and special immunohistochemical techniques may be useful in the diagnosis of these unusual etiologies. Unfortunately, the methodology is not currently available at most hospitals. Broad-range PCR on surgical tissue help to identify more typical organisms (staphylococci and streptococci), whose growth may be suppressed by conventional antibiotic therapy. Although promising, PCR technology may lack specificity in these cases.
Case 3 A 61-year-old executive was admitted with a 4 week history of fevers and fatigue. Three months earlier he had undergone a bovine aortic valve replacement with mitral valve repair. Blood cultures drawn by a local physician grew methicillin-resistant Staphylococcus epidermidis (MRSE). Despite antibiotics, the patient’s fatigue persisted and he returned for further evaluation. On examination, he was afebrile, with a resting pulse of 71 beats/min and a blood pressure of 135/63mm Hg. However, he was very pale. Loud systolic and diastolic murmurs were heard throughout the precordium. His spleen was enlarged and very soft.
The patient underwent urgent reoperation. At surgery, partial aortic valve dehiscence as a result of a large subprosthetic abscess was discovered. Both aortic and mitral valve were replaced. Admission and operative cultures were negative on antibiotic therapy.
Comment: This is a classic presentation of early-onset prosthetic valve endocarditis. Usual organisms are S. epidermidis and S. aureus Streptococci, vancomycin-resistant enterococci (VRE), diphtheroids, gram-negative bacilli, and fungi (yeast and molds) are all seen in this setting, albeit less frequently.
S. epidermidis is of special interest because it produces hemolysins, grows very slowly on cell surfaces, and binds to host and foreign proteins. This biofilm creates a barrier to host defenses and appears to neutralize certain antibiotics. In addition there is clonal variability, with some isolates fully susceptible to oxacillin, while other clones are resistant.
Standard therapy for staphylococcal prosthetic valve endocarditis is oxacillin with gentamicin and rifampin. For oxacillin-resistant species, vancomycin is substituted. Prosthetic valve enterococcal endocarditis resistant to both penicillin and vancomycin is a growing concern. Some medical centers report VRE colonization rates as high as 30%. Therapy is daunting. For strains with a minimum inhibitory concentrations (MIC) less than 128 gr/mL to ampicillin, ampicillin/sulbactam plus an aminoglycoside has been recommended. For strains totally resistant to ampicillin, quinupristin/dalfopristin, linezolid, or daptomycin may be tried, but the overall success rate is probably no better than 50%.
Case 4 A 31-year-old automobile mechanic underwent aortic valve and graft replacement for severe aortic regurgitation with a large aneurysm of the ascending aorta. His post-operative course was complicated by massive bleeding at the distal graft anastomosis, and respiratory failure. After prolonged hospitalization, the patient was discharged improved, but 2 days later he complained of blurred vision and fevers. His wife noted a green hue from his right pupil. The patient was readmitted and started on intravenous acyclovir for presumed acute retinal necrosis. However, several days later, vitrectomy fluid grew Pseudoallescheria boydii.
Therapy was switched to intravenous miconazole but, shortly afterward, the patient suffered a cardiac arrest. Although his pulse and blood pressure were restored, he remained comatose and support was withdrawn. At autopsy, invasive prosthetic aortic valve and graft endocarditis was noted. Blood and tissue cultures also grew P. boydii.
Comment: Fungal prosthetic valve endocarditis is a devastating disease. Predisposing factors are prolonged use of central vascular catheters, often for antibiotic therapy or parenteral nutrition, and immunosuppression. Most success has been reported combining surgery with intravenous antifungal therapy. Patients should be continued on oral suppressive therapy afterward to prevent relapse later in life.
“Pacemaker endocarditis,” seen with increasing frequency, applies to pacemakers, defibrillators, or combinations thereof. Usual causes are skin flora microbes (staphylococci and Propionibacterium species) that gain access through a generator pocket wound. An echocardiogram may not show vegetations unless they extend to the tricuspid valve. Removal of all hardware, combined with intravenous antibiotic therapy, is necessary for cure. Some impacted leads require open heart surgery for removal.
Hospital-associated bacteremia from another source may spread to a heart valve or pacemaker lead, causing endocarditis. S. aureus bacteremia from intravenous catheters, hemodialysis fistula, and surgical wounds is most likely to do this. Patients on hemodialysis may be colonized with methicillin-resistant S. aureus (MRSA), a risk factor for infection. While intra-nasal mupirocin ointment may reduce MRSA colonization transiently, it is probably not effective for long-term prophylaxis.
Case 5 A 54-year-old accountant was admitted with chills and palpitations for several days. A bovine aortic valve prosthesis had been implanted 2 years earlier. The patient had complained of intermittent fevers for 6 months. A single blood culture had grown Propionibacterium acnes. Although a TEE was interpreted as normal, he was treated with intravenous vancomycin. Follow-up blood cultures were negative and a TTE was read as normal.
On examination, the patient was acutely ill with distended neck veins. His pulse was 50 beats/min and blood pressure 110/50mm Hg. Systolic and diastolic murmurs were present. Blood cultures were drawn, and antibiotics started.
An electrocardiogram showed heart block. A temporary pacemaker was placed. A TEE revealed a huge atrial septal abscess with a fistula from the right atrium to the aorta. The patient was taken emergently to surgery, where the prosthesis was found to have nearly completely dehisced. The fistula was resected and the aortic valve replaced with a homograft. Postoperatively the patient remained in cardiogenic shock and died. Admission blood and valve cultures subsequently grew P. acnes.
Comment and Conclusions
Continued fevers despite appropriate antibiotic and medical management are cause for alarm. Ring abscesses may develop. This is a clear indication for surgical intervention. Fevers may also be caused by embolic events (arterial or venous), drug reactions, and intravascular catheter-related infections. Close monitoring is necessary to avoid major events. Vigilance should be maintained for widening pulse pressures and rhythm disturbances as these are ominous signs of progressive infection.
Indications for urgent surgery include progressive valvular dysfunction; aortic root, ring or septal abscesses; large vegetations (greater than l cm in diameter); and organisms such as VRE, MRSA, Pseudomonas species, and fungi refractive to antimicrobial therapy. It is important to note that, even with appropriate therapy and a bacteriologic “cure,” about one half of patients will have enough valve damage to require surgery later in life.
Despite our best efforts, the death rate from infective endocarditis remains in the range of 10–20%. Death is more likely with prosthetic valve endocarditis and when the organism is S. aureus. Patients still succumb from congestive heart failure, embolic phenomenon, and ruptured mycotic aneurysms, just as they did during Osler’s time.
It is clear there is room for improvement in the diagnosis and management of endocarditis. First, we must continue to refine microbiologic techniques, to allow diagnosis more quickly and accurately. Second, we must develop more effective antimicrobial therapy, especially for pathogens resistant to conventional antimicrobials. Third, we must learn how to combat biofilms. Perhaps in the future we can avoid removal of foreign materials. Finally, we must follow our patients closely and pursue timely surgical intervention when indicated. In recent years this has become more difficult, because patients, once stabilized, are often discharged home or to a skilled nursing facility to complete antibiotic therapy.
While we have learned more about infective endocarditis over the past quarter century, the challenges we face today are greater than ever before.
References
- Osler W. Chronic infectious endocarditis. Q J Med. 1909;2: 219-30.
- Mylonakis E, Calderwood SB. Infective endocarditis in adults. N Engl J Med. 2001;345:1318-30.
- Durack DT, Lukes AS, Bright KD, et al: New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Am J Med. 1994;96:200-9.
- Salgado AV, Furlan AJ, Keys TF. Neurologic complications of endocarditis: a 12 year experience. Neurology. 1989;39:173-8.
- Wilson WR, Karchmer AW, Dajani AS, et al: Antibiotic treatment of adults with infective endocarditis due to streptococci, enterococci, staphylococci and HACEK micro organisms. JAMA. 1995;274:1706-13.
- Lepidi H, Houpikian P, Liang Z, Raoult D. Cardiac valves in patients with Q-fever endocarditis. J Infect Dis. 2003;187: 1097-106.
- Bosshard PP, Kronenberg A, Zbinden R, et al. Etiologic diagnosis of infective endocarditis by broad-range PCR. Clin Infect Dis. 2003;37:167-72.
- Keys TF. Early-onset prosthetic valve endocarditis. Cleve Clin J Med. 1993;60:455-9.
- Proctor RA. Coagulase-negative staphylococcal infection: a diagnostic and therapeutic challenge. Clin Infect Dis. 2000;31:31-3.
- Melgar GR, Nasser RM, Gordon SM, et al. Fungal prosthetic-valve endocarditis in 16 patients: an 11-year experience in a tertiary care hospital. Medicine. 1997;76:94-103.
- Fowler VG, Sanders LL, Kong LK, et al. Infective endocarditis due to Staphylococcus aureus. Clin Infect Dis. 1999;28:106-14.
- Douglas A, Moore-Gillon J, Eykyn S. Fever during treatment of infective endocarditis. Lancet. 1986;1:1341-3.
- Tornos MP, Permanyer-Miralda G, Olona J, et al. Long term complications of native valve endocarditis in non-addicts: a 15 year follow up study. Ann Intern Med. 1992;117:567-72.
- Andrews MM, Von Reyn CF. Patients election criteria and management guidelines for outpatient parenteral antibiotic therapy for native valve infective endocarditis. Clin Infect Dis. 2001;32:203-9.
Acute Bacterial Meningitis in Adults
Background Acute bacterial meningitis is an inflammation of the meninges, which results from bacterially mediated recruitment and activation of inflammatory cells in the cerebrospinal fluid (CSF). Bacterial meningitis was an almost invariably fatal disease at the start of the 20th century. With the development of and advancements in antimicrobial therapy, however, there has been a significant reduction in the mortality rate, although this has remained stable during the past 20 years (1). One large study of adults with community-acquired bacterial meningitis reported an overall mortality rate of 21%, including a 30% mortality rate associated with Streptococcus pneumoniae meningitis and a 7% mortality rate for Neisseria meningitidis (2). In adults, the most commonly identified organisms are S. pneumoniae (40–50%), Neisseria meningitidis (14–37%), and Listeria monocytogenes (4–10%) (2-4).
Clinical Presentation
Bacterial meningitis is a serious illness that often progresses rapidly. The classic clinical presentation consists of fever, nuchal rigidity, and mental status change (3). One large review of 10 critically appraised studies showed that almost all (99–100%) of the patients with bacterial meningitis presented with at least one of these clinical findings; and 95% of the patients had at least 2 of the clinical findings (5). In contrast, less than half of the patients presented with all 3 findings. Thus, in the absence of all 3 of these classic findings, the diagnosis of meningitis can virtually be dismissed, and further evaluation for meningitis need not be pursued. Individually, fever was the most common presenting finding, with a sensitivity of 85%. Nuchal rigidity had a sensitivity of 70%, and mental status change was 67%. While these physical examination findings may be of value in determining the diagnosis of bacterial meningitis, the accuracy of the clinical history including features such as headache, nausea and vomiting, and neck pain was too low to be of use clinically.
Signs of meningeal irritation may be of benefit in the clinical diagnosis of bacterial meningitis. Kernig’s and Brudzinski’s signs were first described nearly a century ago and have been used by most clinicians in the clinical realm; however, their diagnostic utility has been evaluated only in a limited number of studies. Kernig’s sign is positive when a patient in the supine position with his/her hips flexed at 90 degrees develops pain in the lower back or posterior thigh during an attempt to extend the knee. Brudzinski’s sign is positive when a patient in the supine position whose neck is passively flexed responds with flexion of his/her knees and hips. Recently, a bedside maneuver called jolt accentuation of headache was found to be potentially useful. In this maneuver, the patient is asked to turn his/her head horizontally 2–3 times per second, and a worsening headache is considered a positive sign. A small study showed that this maneuver had 97% sensitivity and 60% specificity for patients with CSF pleocytosis (6).
Other clinical manifestations in patients with bacterial meningitis include photophobia, seizure, rash, focal neurologic deficits, and signs of increased intracranial pressure. While these various findings may be present in many patients with bacterial meningitis, their sensitivities have been found to be low. Thus, their clinical utility in ruling out the diagnosis of bacterial meningitis is limited (5).
Laboratory Findings
Any patient who presents with a reasonable likelihood of having bacterial meningitis should undergo a lumbar puncture (LP) to evaluate the CSF as soon as possible. The initial CSF study should measure the opening pressure. One study demonstrated that 39% of patients with bacterial meningitis had opening pressures greater than 300 mg H20 (3). Other CSF laboratory studies should be sent for analysis in 4 sterile tubes filled with approximately 1 mL of CSF each. The first tube is typically reserved for gram stain and culture. The gram stain is positive in about 70% of patients with bacterial meningitis, and the culture will be positive in about 80% of cases. The second tube is sent for protein and glucose levels. Patients who have markedly elevated CSF protein counts (>500 mg/dL) and low glucose levels (<45 mg/dL, or ratio of serum: CSF glucose levels <0.4) are likely to have bacterial meningitis. The third tube is sent for cell count and differential. Patients with bacterial meningitis are likely to have >10 WBC/μL that are predominantly polymorphonucleocytes and have few or no red blood cells in the absence of a traumatic LP. We recommend the fourth tube be used for any viral, fungal, or other miscellaneous studies. In addition to the CSF studies, other diagnostic evaluations should include blood cultures, complete blood count with platelets and differential (CBCPD), and basic chemistry labs.
The CSF studies described above are the primary tools in diagnosing bacterial meningitis; however, there are other studies that may be helpful in certain clinical settings. Latex agglutination tests for bacterial antigens may be used in cases in which bacterial meningitis remains a possible diagnosis despite negative CSF studies. This test is available for S. pneumoniae, N. meningitidis, H. influenzae type B, group B Streptococcus, and E. coli. The polymerase chain reaction (PCR) test of the CSF has been developed for some bacterial pathogens including S. pneumoniae, N. meningitidis, H. influenzae type B, and Mycobacterium tuberculosis. The limulus amebocyte lysate assay is a very sensitive test for gram-negative endotoxins, which may aid in identifying gram-negative organisms as potential pathogens in the CSF. While these alternative CSF diagnostic tests are available, many laboratories do not perform the tests on site and require send-out to a specialty laboratory. The time required for this may negate the clinical utility of these tests.
Role of Brain Imaging
The decision to obtain a brain imaging study prior to performing an LP has been a controversial issue for both patient safety and medical-legal reasons. Two large studies have been published in an attempt to derive a clinically useful decision analysis tool (7,8). In summary, the studies found that 5 clinical features were associated with an abnormal head cranial tomography (CT) scan. These were:
- Age >60 years
- Immunocompromised state
- Any history of central nervous system (CNS) disease
- A history of seizure within 1 week prior to presentation
- Presence of a focal neurologic abnormality, including altered level of consciousness, inability to answer or follow 2 consecutive requests, gaze palsy, abnormal visual fields, facial palsy, arm or leg drift, and abnormal language.
In patients with none of these findings, there was a 97% negative predictive value of having an abnormal CT scan, with the few patients with positive scans nonetheless tolerating LP without adverse effects. Thus, in patients with none of these findings, it appears that an LP can safely be performed without obtaining a CT scan. One study also demonstrated that patients who underwent a CT scan prior to their LP waited, on average, 2 hours longer to get an LP; with antibiotic administration delayed by an average of 1 hour (8). Antibiotic administration should not be delayed in any patient suspected of having bacterial meningitis, whether brain imaging is performed or not.
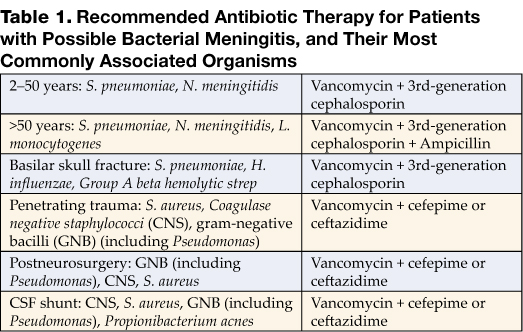
Differential Diagnosis
Given the severe nature of this disease, the diagnosis of bacterial meningitis must be differentiated from other conditions that may present in similar ways. Infectious causes that may present similarly to bacterial meningitis include other types of meningitis (viral, tuberculous, Lyme disease, syphilitic), viral encephalitis, Rocky Mountain spotted fever, fungal meningitis, parasitic causes, brain abscess, and epidural and subdural empyema. Other infectious etiologies not originating from the CNS may be mistaken for bacterial meningitis when these patients present with concomitant mental-status changes. This is especially common in elderly patients with pneumonia and urinary tract infections. Other noninfectious considerations include a CNS bleed such as a subarachnoid hemorrhage, drug-induced aseptic meningitis, and CNS vasculitis.
Treatment
When the patient’s presentation is suggestive of bacterial meningitis, empiric antibiotics should be administered without delay, while awaiting diagnostic evaluation. The initial dose of antibiotics should not alter the results of the diagnostic studies significantly. The choice of antibiotics is based upon the most likely offending organism from epidemiologic data and underlying predisposing conditions. S. pneumoniae and N. meningitidis are the 2 most common causes of bacterial meningitis in adults.
The development of antibiotic resistance by S. pneumoniae to penicillin and cephalosporins has been one of the major developments in the past 20 years. Due to this resistance, the recommended empiric therapy is a combination of a third-generation cephalosporin (ceftriaxone or cefotaxime) and vancomycin. For special cases, additional or alternative therapy should be given. Ampicillin should be added for patients at risk for Listeria monocytogenes; and postsurgical or post-trauma patients should have expanded coverage to include staphylococcal and gram-negative infections. Table 1 lists the recommended antibiotic therapy for patients with possible bacterial meningitis, along with the most commonly associated organisms.
Once the offending organism has been identified, antibiotic therapy should be narrowed to target the bacteria based on laboratory minimal inhibitory concentrations (MIC). The antibiotic should also have excellent CSF penetration and bactericidal activity. For S. pneumoniae that are susceptible to penicillin, penicillin G and ampicillin remain the therapy of choice (9). The increasing trend toward antibiotic resistance by S. pneumoniae has increased the use of vancomycin as therapy. In patients with resistant strains of S. pneumoniae, however, vancomycin should not be used alone. Vancomycin should be used in combination with a third-generation cephalosporin while keeping the serum vancomycin levels in the range of 15–20 μg/mL (10). It is imperative that the treatment course outlined be completed through its full duration. Table 2 lists specific antibiotic therapy with dosages and recommended duration of therapy based on isolated organisms.
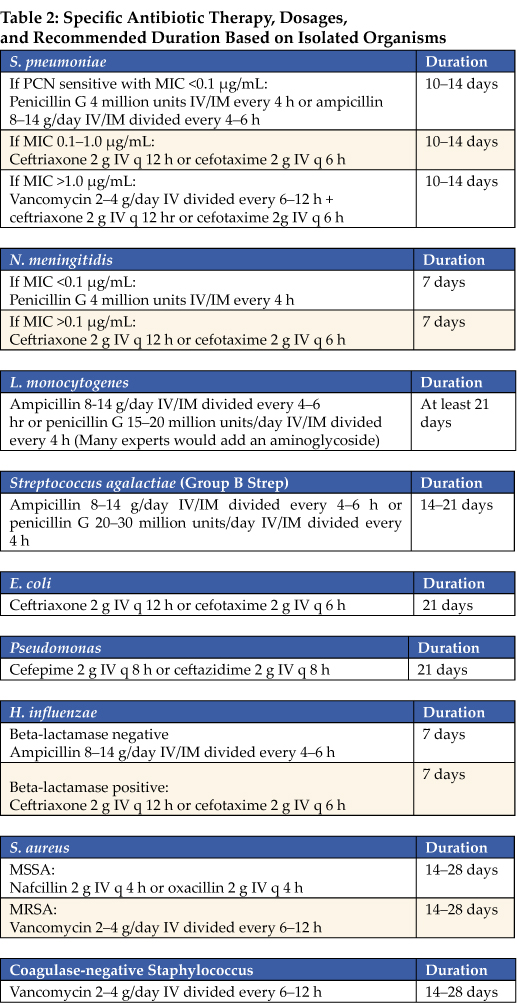
Adjunctive Therapy
The release and production of inflammatory cytokines in bacterial meningitis is thought to be a major cause of adverse outcomes. To counteract this inflammatory process, use of adjunctive steroids in patients with bacterial meningitis has been evaluated. Initial data from children with bacterial meningitis, mostly due to H. influenzae and S. pneumoniae, demonstrated improved neurologic outcomes, with significant reductions in deafness, in patients treated with dexamethasone as an adjunctive therapy to antibiotics (11). In adults with bacterial meningitis, a recent major trial demonstrated that treatment with adjunctive steroids, along with antibiotics, led to significant improvement in mortality and morbidity in patients with meningitis due to S. pneumoniae (12). Among patients with meningococcal meningitis, there was a trend toward improved outcomes. Patients with suspected pneumococcal meningitis should receive their first dose of dexamethasone 20–30 minutes prior to or at the same time as the initial antibiotic administration. The recommended dose and duration is 0.15 mg/kg every 6 hours for 2 to 4 days. The use of dexamethasone appears to have no benefit if administered after antibiotics have already been given, and data are lacking for patients with meningitis due to organisms other than S. pneumoniae. Most experts recommend against the use of adjunctive corticosteroids in these cases (10-13). Several questions, however, remain unanswered with regard to adjunctive corticosteroid use. These include the optimal duration of treatment, whether the penetration of vancomycin into the CSF is significantly decreased by dexamethasone, and whether they should be administered to immunocompromised patients (14).
Prevention
Currently, prevention of some types of bacterial meningitis can be accomplished by appropriate use of vaccines, or through antibiotic chemoprophylaxis in certain situations. For adults, vaccines are available against the 2 most common causes of bacterial meningitis. The 23 polyvalent pneumococcal vaccine is recommended for all adults >65 years of age and for anyone age >2 with a compromised immune status. The meningococcal vaccine is available as a quadravalent vaccine (serotypes A, C, Y, and W-135) and should be administered to anyone with functional asplenia, terminal complement deficiencies, those traveling to endemic areas of meningococcal meningitis, and any college freshman requesting the vaccine who will be living in college dormitories (15).
Antibiotic chemoprophylaxis can be administered to individuals who have had close contact with an index patient with meningococcal meningitis. Antibiotics should be administered as soon as exposure has been determined. There are several options available for meningococcal meningitis exposure. Ciprofloxacin is probably the simplest regimen due to its 1-time 500-mg oral dose. Other options include rifampin 600 mg every 12 hours ×4 doses and ceftriaxone 250 mg IM as a 1-time dose. Pregnant women should avoid ciprofloxacin and rifampin due to their potential teratogenic effects.
Prognosis and Follow-up
Prognosis of bacterial meningitis is closely linked to the causative organism, the severity of disease at the time of presentation, and the speed at which the disease progresses. One large retrospective study demonstrated in-hospital mortality rates of 25% for S. pneumoniae, 10% for N. meningitidis, and 21% for L. monocytogenes. Conditions associated with an increased risk of mortality included age >60, state of obtundation on admission, and development of seizure within 24 hours of admission. This study also showed that 21% of patients developed some type of neurologic deficits, and, overall, 9% had persistence of these deficits at time of discharge (3). Another study showed that baseline features of hypotension, mental status changes, and seizures were associated with increased mortality and neurologic morbidity (16). A more recent large study evaluating the efficacy of adjunctive corticosteroids reported a mortality rate of 15% in the control arm, with mortality of 34% in patients infected with S. pneumoniae (12). Another study suggested that if patients had a rapid progression of their disease, this seemed to correlate with worse outcomes. These investigators found an uncertain correlation between antibiotic timing and unfavorable outcomes (16).
Patients discharged from the hospital should have close follow-up with their primary care physician or infectious disease specialist. Evaluation in the short-term should focus on any complications that may have developed as a result of the bacterial meningitis; such as mental status change, seizure, focal neurologic deficits, and hearing loss. Long-term evaluations should also address cognitive functioning and the neuropsychiatric well-being of the patient, in addition to those issues addressed during short-term follow-up (11, 12).
Dr. Kim may be reached at seoungk@umich.edu.
References
- Swartz, Morton N. Bacterial Meningitis—A View of the Past 90 Years. N Engl J Med. 2004;351:1826-8.
- van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M. Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med. 2004;351:1849-59.
- Durand ML, Calderwood SB, Weber DJ, et al. Acute Bacterial Meningitis in Adults. A review of 493 episodes. N Engl J Med. 1993;328:21-8.
- Schuchat A, Robinson K, Wenger J, et al. Bacterial meningitis in the United States in 1995. Active Surveillance Team. N Engl J Med. 1997;337:970-6.
- Attia J, Hatala R, Cook DJ, Wong JG. The rational clinical examination. Does this adult patient have acute meningitis? JAMA. 1999;282:175-181.
- Uchihara T, Tsukagoshi H. Jolt accentuation of headache: the most sensitive sign of CSF pleocytosis. Headache. 1991;31:167-71.
- Gopal AK, Whitehouse JD, Simel DL, Corey RG. Cranial computed tomography before lumbar puncture: a prospective clinical evaluation. Arch Intern Med. 1999;159:2681-5.
- Hasbun R, Abrahams J, Jekel J, Quagliarello VJ. Computed tomography of the head before LP in adults with suspected meningitis. N Engl J Med. 2001;345:1727-33.
- Quagliarello VJ, Scheld WM. Treatment of bacterial meningitis. N Engl J Med. 1997;336:708-16.
- Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice Guidelines for the Management of Bacterial Meningitis. Clin Infect Dis. 2004;39:1267-84.
- McIntyre PB, Berkey CS, King SM, et al. Dexamethasone as adjunctive therapy in bacterial meningitis. A meta-analysis of randomized clinical trials since 1988. JAMA. 1997;278:928-31.
- de Gans J, van de Beek D Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002;347:1549-56.
- van de Beek D, de Gans J, McIntyre P, Prasad K. Steroids in adults with acute bacterial meningitis: a systematic review. Lancet Infect Dis 2004;4: 139-43.
- Pile JC, Longworth DL. Should adults with suspected acute bacterial meningitis get adjunctive corticosteroids? Cleve Clin J Med. 2005;72:67-70.
- Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 1997;4613-21.
- Aronin SI, Peduzzi P, Quagliarello VJ. Community-acquired bacterial meningitis: risk stratification for adverse clinical outcome and effect of antibiotic timing. Ann Intern Med. 1998;129:862-9.
Background Acute bacterial meningitis is an inflammation of the meninges, which results from bacterially mediated recruitment and activation of inflammatory cells in the cerebrospinal fluid (CSF). Bacterial meningitis was an almost invariably fatal disease at the start of the 20th century. With the development of and advancements in antimicrobial therapy, however, there has been a significant reduction in the mortality rate, although this has remained stable during the past 20 years (1). One large study of adults with community-acquired bacterial meningitis reported an overall mortality rate of 21%, including a 30% mortality rate associated with Streptococcus pneumoniae meningitis and a 7% mortality rate for Neisseria meningitidis (2). In adults, the most commonly identified organisms are S. pneumoniae (40–50%), Neisseria meningitidis (14–37%), and Listeria monocytogenes (4–10%) (2-4).
Clinical Presentation
Bacterial meningitis is a serious illness that often progresses rapidly. The classic clinical presentation consists of fever, nuchal rigidity, and mental status change (3). One large review of 10 critically appraised studies showed that almost all (99–100%) of the patients with bacterial meningitis presented with at least one of these clinical findings; and 95% of the patients had at least 2 of the clinical findings (5). In contrast, less than half of the patients presented with all 3 findings. Thus, in the absence of all 3 of these classic findings, the diagnosis of meningitis can virtually be dismissed, and further evaluation for meningitis need not be pursued. Individually, fever was the most common presenting finding, with a sensitivity of 85%. Nuchal rigidity had a sensitivity of 70%, and mental status change was 67%. While these physical examination findings may be of value in determining the diagnosis of bacterial meningitis, the accuracy of the clinical history including features such as headache, nausea and vomiting, and neck pain was too low to be of use clinically.
Signs of meningeal irritation may be of benefit in the clinical diagnosis of bacterial meningitis. Kernig’s and Brudzinski’s signs were first described nearly a century ago and have been used by most clinicians in the clinical realm; however, their diagnostic utility has been evaluated only in a limited number of studies. Kernig’s sign is positive when a patient in the supine position with his/her hips flexed at 90 degrees develops pain in the lower back or posterior thigh during an attempt to extend the knee. Brudzinski’s sign is positive when a patient in the supine position whose neck is passively flexed responds with flexion of his/her knees and hips. Recently, a bedside maneuver called jolt accentuation of headache was found to be potentially useful. In this maneuver, the patient is asked to turn his/her head horizontally 2–3 times per second, and a worsening headache is considered a positive sign. A small study showed that this maneuver had 97% sensitivity and 60% specificity for patients with CSF pleocytosis (6).
Other clinical manifestations in patients with bacterial meningitis include photophobia, seizure, rash, focal neurologic deficits, and signs of increased intracranial pressure. While these various findings may be present in many patients with bacterial meningitis, their sensitivities have been found to be low. Thus, their clinical utility in ruling out the diagnosis of bacterial meningitis is limited (5).
Laboratory Findings
Any patient who presents with a reasonable likelihood of having bacterial meningitis should undergo a lumbar puncture (LP) to evaluate the CSF as soon as possible. The initial CSF study should measure the opening pressure. One study demonstrated that 39% of patients with bacterial meningitis had opening pressures greater than 300 mg H20 (3). Other CSF laboratory studies should be sent for analysis in 4 sterile tubes filled with approximately 1 mL of CSF each. The first tube is typically reserved for gram stain and culture. The gram stain is positive in about 70% of patients with bacterial meningitis, and the culture will be positive in about 80% of cases. The second tube is sent for protein and glucose levels. Patients who have markedly elevated CSF protein counts (>500 mg/dL) and low glucose levels (<45 mg/dL, or ratio of serum: CSF glucose levels <0.4) are likely to have bacterial meningitis. The third tube is sent for cell count and differential. Patients with bacterial meningitis are likely to have >10 WBC/μL that are predominantly polymorphonucleocytes and have few or no red blood cells in the absence of a traumatic LP. We recommend the fourth tube be used for any viral, fungal, or other miscellaneous studies. In addition to the CSF studies, other diagnostic evaluations should include blood cultures, complete blood count with platelets and differential (CBCPD), and basic chemistry labs.
The CSF studies described above are the primary tools in diagnosing bacterial meningitis; however, there are other studies that may be helpful in certain clinical settings. Latex agglutination tests for bacterial antigens may be used in cases in which bacterial meningitis remains a possible diagnosis despite negative CSF studies. This test is available for S. pneumoniae, N. meningitidis, H. influenzae type B, group B Streptococcus, and E. coli. The polymerase chain reaction (PCR) test of the CSF has been developed for some bacterial pathogens including S. pneumoniae, N. meningitidis, H. influenzae type B, and Mycobacterium tuberculosis. The limulus amebocyte lysate assay is a very sensitive test for gram-negative endotoxins, which may aid in identifying gram-negative organisms as potential pathogens in the CSF. While these alternative CSF diagnostic tests are available, many laboratories do not perform the tests on site and require send-out to a specialty laboratory. The time required for this may negate the clinical utility of these tests.
Role of Brain Imaging
The decision to obtain a brain imaging study prior to performing an LP has been a controversial issue for both patient safety and medical-legal reasons. Two large studies have been published in an attempt to derive a clinically useful decision analysis tool (7,8). In summary, the studies found that 5 clinical features were associated with an abnormal head cranial tomography (CT) scan. These were:
- Age >60 years
- Immunocompromised state
- Any history of central nervous system (CNS) disease
- A history of seizure within 1 week prior to presentation
- Presence of a focal neurologic abnormality, including altered level of consciousness, inability to answer or follow 2 consecutive requests, gaze palsy, abnormal visual fields, facial palsy, arm or leg drift, and abnormal language.
In patients with none of these findings, there was a 97% negative predictive value of having an abnormal CT scan, with the few patients with positive scans nonetheless tolerating LP without adverse effects. Thus, in patients with none of these findings, it appears that an LP can safely be performed without obtaining a CT scan. One study also demonstrated that patients who underwent a CT scan prior to their LP waited, on average, 2 hours longer to get an LP; with antibiotic administration delayed by an average of 1 hour (8). Antibiotic administration should not be delayed in any patient suspected of having bacterial meningitis, whether brain imaging is performed or not.
Differential Diagnosis
Given the severe nature of this disease, the diagnosis of bacterial meningitis must be differentiated from other conditions that may present in similar ways. Infectious causes that may present similarly to bacterial meningitis include other types of meningitis (viral, tuberculous, Lyme disease, syphilitic), viral encephalitis, Rocky Mountain spotted fever, fungal meningitis, parasitic causes, brain abscess, and epidural and subdural empyema. Other infectious etiologies not originating from the CNS may be mistaken for bacterial meningitis when these patients present with concomitant mental-status changes. This is especially common in elderly patients with pneumonia and urinary tract infections. Other noninfectious considerations include a CNS bleed such as a subarachnoid hemorrhage, drug-induced aseptic meningitis, and CNS vasculitis.
Treatment
When the patient’s presentation is suggestive of bacterial meningitis, empiric antibiotics should be administered without delay, while awaiting diagnostic evaluation. The initial dose of antibiotics should not alter the results of the diagnostic studies significantly. The choice of antibiotics is based upon the most likely offending organism from epidemiologic data and underlying predisposing conditions. S. pneumoniae and N. meningitidis are the 2 most common causes of bacterial meningitis in adults.
The development of antibiotic resistance by S. pneumoniae to penicillin and cephalosporins has been one of the major developments in the past 20 years. Due to this resistance, the recommended empiric therapy is a combination of a third-generation cephalosporin (ceftriaxone or cefotaxime) and vancomycin. For special cases, additional or alternative therapy should be given. Ampicillin should be added for patients at risk for Listeria monocytogenes; and postsurgical or post-trauma patients should have expanded coverage to include staphylococcal and gram-negative infections. Table 1 lists the recommended antibiotic therapy for patients with possible bacterial meningitis, along with the most commonly associated organisms.
Once the offending organism has been identified, antibiotic therapy should be narrowed to target the bacteria based on laboratory minimal inhibitory concentrations (MIC). The antibiotic should also have excellent CSF penetration and bactericidal activity. For S. pneumoniae that are susceptible to penicillin, penicillin G and ampicillin remain the therapy of choice (9). The increasing trend toward antibiotic resistance by S. pneumoniae has increased the use of vancomycin as therapy. In patients with resistant strains of S. pneumoniae, however, vancomycin should not be used alone. Vancomycin should be used in combination with a third-generation cephalosporin while keeping the serum vancomycin levels in the range of 15–20 μg/mL (10). It is imperative that the treatment course outlined be completed through its full duration. Table 2 lists specific antibiotic therapy with dosages and recommended duration of therapy based on isolated organisms.
Adjunctive Therapy
The release and production of inflammatory cytokines in bacterial meningitis is thought to be a major cause of adverse outcomes. To counteract this inflammatory process, use of adjunctive steroids in patients with bacterial meningitis has been evaluated. Initial data from children with bacterial meningitis, mostly due to H. influenzae and S. pneumoniae, demonstrated improved neurologic outcomes, with significant reductions in deafness, in patients treated with dexamethasone as an adjunctive therapy to antibiotics (11). In adults with bacterial meningitis, a recent major trial demonstrated that treatment with adjunctive steroids, along with antibiotics, led to significant improvement in mortality and morbidity in patients with meningitis due to S. pneumoniae (12). Among patients with meningococcal meningitis, there was a trend toward improved outcomes. Patients with suspected pneumococcal meningitis should receive their first dose of dexamethasone 20–30 minutes prior to or at the same time as the initial antibiotic administration. The recommended dose and duration is 0.15 mg/kg every 6 hours for 2 to 4 days. The use of dexamethasone appears to have no benefit if administered after antibiotics have already been given, and data are lacking for patients with meningitis due to organisms other than S. pneumoniae. Most experts recommend against the use of adjunctive corticosteroids in these cases (10-13). Several questions, however, remain unanswered with regard to adjunctive corticosteroid use. These include the optimal duration of treatment, whether the penetration of vancomycin into the CSF is significantly decreased by dexamethasone, and whether they should be administered to immunocompromised patients (14).
Prevention
Currently, prevention of some types of bacterial meningitis can be accomplished by appropriate use of vaccines, or through antibiotic chemoprophylaxis in certain situations. For adults, vaccines are available against the 2 most common causes of bacterial meningitis. The 23 polyvalent pneumococcal vaccine is recommended for all adults >65 years of age and for anyone age >2 with a compromised immune status. The meningococcal vaccine is available as a quadravalent vaccine (serotypes A, C, Y, and W-135) and should be administered to anyone with functional asplenia, terminal complement deficiencies, those traveling to endemic areas of meningococcal meningitis, and any college freshman requesting the vaccine who will be living in college dormitories (15).
Antibiotic chemoprophylaxis can be administered to individuals who have had close contact with an index patient with meningococcal meningitis. Antibiotics should be administered as soon as exposure has been determined. There are several options available for meningococcal meningitis exposure. Ciprofloxacin is probably the simplest regimen due to its 1-time 500-mg oral dose. Other options include rifampin 600 mg every 12 hours ×4 doses and ceftriaxone 250 mg IM as a 1-time dose. Pregnant women should avoid ciprofloxacin and rifampin due to their potential teratogenic effects.
Prognosis and Follow-up
Prognosis of bacterial meningitis is closely linked to the causative organism, the severity of disease at the time of presentation, and the speed at which the disease progresses. One large retrospective study demonstrated in-hospital mortality rates of 25% for S. pneumoniae, 10% for N. meningitidis, and 21% for L. monocytogenes. Conditions associated with an increased risk of mortality included age >60, state of obtundation on admission, and development of seizure within 24 hours of admission. This study also showed that 21% of patients developed some type of neurologic deficits, and, overall, 9% had persistence of these deficits at time of discharge (3). Another study showed that baseline features of hypotension, mental status changes, and seizures were associated with increased mortality and neurologic morbidity (16). A more recent large study evaluating the efficacy of adjunctive corticosteroids reported a mortality rate of 15% in the control arm, with mortality of 34% in patients infected with S. pneumoniae (12). Another study suggested that if patients had a rapid progression of their disease, this seemed to correlate with worse outcomes. These investigators found an uncertain correlation between antibiotic timing and unfavorable outcomes (16).
Patients discharged from the hospital should have close follow-up with their primary care physician or infectious disease specialist. Evaluation in the short-term should focus on any complications that may have developed as a result of the bacterial meningitis; such as mental status change, seizure, focal neurologic deficits, and hearing loss. Long-term evaluations should also address cognitive functioning and the neuropsychiatric well-being of the patient, in addition to those issues addressed during short-term follow-up (11, 12).
Dr. Kim may be reached at seoungk@umich.edu.
References
- Swartz, Morton N. Bacterial Meningitis—A View of the Past 90 Years. N Engl J Med. 2004;351:1826-8.
- van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M. Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med. 2004;351:1849-59.
- Durand ML, Calderwood SB, Weber DJ, et al. Acute Bacterial Meningitis in Adults. A review of 493 episodes. N Engl J Med. 1993;328:21-8.
- Schuchat A, Robinson K, Wenger J, et al. Bacterial meningitis in the United States in 1995. Active Surveillance Team. N Engl J Med. 1997;337:970-6.
- Attia J, Hatala R, Cook DJ, Wong JG. The rational clinical examination. Does this adult patient have acute meningitis? JAMA. 1999;282:175-181.
- Uchihara T, Tsukagoshi H. Jolt accentuation of headache: the most sensitive sign of CSF pleocytosis. Headache. 1991;31:167-71.
- Gopal AK, Whitehouse JD, Simel DL, Corey RG. Cranial computed tomography before lumbar puncture: a prospective clinical evaluation. Arch Intern Med. 1999;159:2681-5.
- Hasbun R, Abrahams J, Jekel J, Quagliarello VJ. Computed tomography of the head before LP in adults with suspected meningitis. N Engl J Med. 2001;345:1727-33.
- Quagliarello VJ, Scheld WM. Treatment of bacterial meningitis. N Engl J Med. 1997;336:708-16.
- Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice Guidelines for the Management of Bacterial Meningitis. Clin Infect Dis. 2004;39:1267-84.
- McIntyre PB, Berkey CS, King SM, et al. Dexamethasone as adjunctive therapy in bacterial meningitis. A meta-analysis of randomized clinical trials since 1988. JAMA. 1997;278:928-31.
- de Gans J, van de Beek D Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002;347:1549-56.
- van de Beek D, de Gans J, McIntyre P, Prasad K. Steroids in adults with acute bacterial meningitis: a systematic review. Lancet Infect Dis 2004;4: 139-43.
- Pile JC, Longworth DL. Should adults with suspected acute bacterial meningitis get adjunctive corticosteroids? Cleve Clin J Med. 2005;72:67-70.
- Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 1997;4613-21.
- Aronin SI, Peduzzi P, Quagliarello VJ. Community-acquired bacterial meningitis: risk stratification for adverse clinical outcome and effect of antibiotic timing. Ann Intern Med. 1998;129:862-9.
Background Acute bacterial meningitis is an inflammation of the meninges, which results from bacterially mediated recruitment and activation of inflammatory cells in the cerebrospinal fluid (CSF). Bacterial meningitis was an almost invariably fatal disease at the start of the 20th century. With the development of and advancements in antimicrobial therapy, however, there has been a significant reduction in the mortality rate, although this has remained stable during the past 20 years (1). One large study of adults with community-acquired bacterial meningitis reported an overall mortality rate of 21%, including a 30% mortality rate associated with Streptococcus pneumoniae meningitis and a 7% mortality rate for Neisseria meningitidis (2). In adults, the most commonly identified organisms are S. pneumoniae (40–50%), Neisseria meningitidis (14–37%), and Listeria monocytogenes (4–10%) (2-4).
Clinical Presentation
Bacterial meningitis is a serious illness that often progresses rapidly. The classic clinical presentation consists of fever, nuchal rigidity, and mental status change (3). One large review of 10 critically appraised studies showed that almost all (99–100%) of the patients with bacterial meningitis presented with at least one of these clinical findings; and 95% of the patients had at least 2 of the clinical findings (5). In contrast, less than half of the patients presented with all 3 findings. Thus, in the absence of all 3 of these classic findings, the diagnosis of meningitis can virtually be dismissed, and further evaluation for meningitis need not be pursued. Individually, fever was the most common presenting finding, with a sensitivity of 85%. Nuchal rigidity had a sensitivity of 70%, and mental status change was 67%. While these physical examination findings may be of value in determining the diagnosis of bacterial meningitis, the accuracy of the clinical history including features such as headache, nausea and vomiting, and neck pain was too low to be of use clinically.
Signs of meningeal irritation may be of benefit in the clinical diagnosis of bacterial meningitis. Kernig’s and Brudzinski’s signs were first described nearly a century ago and have been used by most clinicians in the clinical realm; however, their diagnostic utility has been evaluated only in a limited number of studies. Kernig’s sign is positive when a patient in the supine position with his/her hips flexed at 90 degrees develops pain in the lower back or posterior thigh during an attempt to extend the knee. Brudzinski’s sign is positive when a patient in the supine position whose neck is passively flexed responds with flexion of his/her knees and hips. Recently, a bedside maneuver called jolt accentuation of headache was found to be potentially useful. In this maneuver, the patient is asked to turn his/her head horizontally 2–3 times per second, and a worsening headache is considered a positive sign. A small study showed that this maneuver had 97% sensitivity and 60% specificity for patients with CSF pleocytosis (6).
Other clinical manifestations in patients with bacterial meningitis include photophobia, seizure, rash, focal neurologic deficits, and signs of increased intracranial pressure. While these various findings may be present in many patients with bacterial meningitis, their sensitivities have been found to be low. Thus, their clinical utility in ruling out the diagnosis of bacterial meningitis is limited (5).
Laboratory Findings
Any patient who presents with a reasonable likelihood of having bacterial meningitis should undergo a lumbar puncture (LP) to evaluate the CSF as soon as possible. The initial CSF study should measure the opening pressure. One study demonstrated that 39% of patients with bacterial meningitis had opening pressures greater than 300 mg H20 (3). Other CSF laboratory studies should be sent for analysis in 4 sterile tubes filled with approximately 1 mL of CSF each. The first tube is typically reserved for gram stain and culture. The gram stain is positive in about 70% of patients with bacterial meningitis, and the culture will be positive in about 80% of cases. The second tube is sent for protein and glucose levels. Patients who have markedly elevated CSF protein counts (>500 mg/dL) and low glucose levels (<45 mg/dL, or ratio of serum: CSF glucose levels <0.4) are likely to have bacterial meningitis. The third tube is sent for cell count and differential. Patients with bacterial meningitis are likely to have >10 WBC/μL that are predominantly polymorphonucleocytes and have few or no red blood cells in the absence of a traumatic LP. We recommend the fourth tube be used for any viral, fungal, or other miscellaneous studies. In addition to the CSF studies, other diagnostic evaluations should include blood cultures, complete blood count with platelets and differential (CBCPD), and basic chemistry labs.
The CSF studies described above are the primary tools in diagnosing bacterial meningitis; however, there are other studies that may be helpful in certain clinical settings. Latex agglutination tests for bacterial antigens may be used in cases in which bacterial meningitis remains a possible diagnosis despite negative CSF studies. This test is available for S. pneumoniae, N. meningitidis, H. influenzae type B, group B Streptococcus, and E. coli. The polymerase chain reaction (PCR) test of the CSF has been developed for some bacterial pathogens including S. pneumoniae, N. meningitidis, H. influenzae type B, and Mycobacterium tuberculosis. The limulus amebocyte lysate assay is a very sensitive test for gram-negative endotoxins, which may aid in identifying gram-negative organisms as potential pathogens in the CSF. While these alternative CSF diagnostic tests are available, many laboratories do not perform the tests on site and require send-out to a specialty laboratory. The time required for this may negate the clinical utility of these tests.
Role of Brain Imaging
The decision to obtain a brain imaging study prior to performing an LP has been a controversial issue for both patient safety and medical-legal reasons. Two large studies have been published in an attempt to derive a clinically useful decision analysis tool (7,8). In summary, the studies found that 5 clinical features were associated with an abnormal head cranial tomography (CT) scan. These were:
- Age >60 years
- Immunocompromised state
- Any history of central nervous system (CNS) disease
- A history of seizure within 1 week prior to presentation
- Presence of a focal neurologic abnormality, including altered level of consciousness, inability to answer or follow 2 consecutive requests, gaze palsy, abnormal visual fields, facial palsy, arm or leg drift, and abnormal language.
In patients with none of these findings, there was a 97% negative predictive value of having an abnormal CT scan, with the few patients with positive scans nonetheless tolerating LP without adverse effects. Thus, in patients with none of these findings, it appears that an LP can safely be performed without obtaining a CT scan. One study also demonstrated that patients who underwent a CT scan prior to their LP waited, on average, 2 hours longer to get an LP; with antibiotic administration delayed by an average of 1 hour (8). Antibiotic administration should not be delayed in any patient suspected of having bacterial meningitis, whether brain imaging is performed or not.
Differential Diagnosis
Given the severe nature of this disease, the diagnosis of bacterial meningitis must be differentiated from other conditions that may present in similar ways. Infectious causes that may present similarly to bacterial meningitis include other types of meningitis (viral, tuberculous, Lyme disease, syphilitic), viral encephalitis, Rocky Mountain spotted fever, fungal meningitis, parasitic causes, brain abscess, and epidural and subdural empyema. Other infectious etiologies not originating from the CNS may be mistaken for bacterial meningitis when these patients present with concomitant mental-status changes. This is especially common in elderly patients with pneumonia and urinary tract infections. Other noninfectious considerations include a CNS bleed such as a subarachnoid hemorrhage, drug-induced aseptic meningitis, and CNS vasculitis.
Treatment
When the patient’s presentation is suggestive of bacterial meningitis, empiric antibiotics should be administered without delay, while awaiting diagnostic evaluation. The initial dose of antibiotics should not alter the results of the diagnostic studies significantly. The choice of antibiotics is based upon the most likely offending organism from epidemiologic data and underlying predisposing conditions. S. pneumoniae and N. meningitidis are the 2 most common causes of bacterial meningitis in adults.
The development of antibiotic resistance by S. pneumoniae to penicillin and cephalosporins has been one of the major developments in the past 20 years. Due to this resistance, the recommended empiric therapy is a combination of a third-generation cephalosporin (ceftriaxone or cefotaxime) and vancomycin. For special cases, additional or alternative therapy should be given. Ampicillin should be added for patients at risk for Listeria monocytogenes; and postsurgical or post-trauma patients should have expanded coverage to include staphylococcal and gram-negative infections. Table 1 lists the recommended antibiotic therapy for patients with possible bacterial meningitis, along with the most commonly associated organisms.
Once the offending organism has been identified, antibiotic therapy should be narrowed to target the bacteria based on laboratory minimal inhibitory concentrations (MIC). The antibiotic should also have excellent CSF penetration and bactericidal activity. For S. pneumoniae that are susceptible to penicillin, penicillin G and ampicillin remain the therapy of choice (9). The increasing trend toward antibiotic resistance by S. pneumoniae has increased the use of vancomycin as therapy. In patients with resistant strains of S. pneumoniae, however, vancomycin should not be used alone. Vancomycin should be used in combination with a third-generation cephalosporin while keeping the serum vancomycin levels in the range of 15–20 μg/mL (10). It is imperative that the treatment course outlined be completed through its full duration. Table 2 lists specific antibiotic therapy with dosages and recommended duration of therapy based on isolated organisms.
Adjunctive Therapy
The release and production of inflammatory cytokines in bacterial meningitis is thought to be a major cause of adverse outcomes. To counteract this inflammatory process, use of adjunctive steroids in patients with bacterial meningitis has been evaluated. Initial data from children with bacterial meningitis, mostly due to H. influenzae and S. pneumoniae, demonstrated improved neurologic outcomes, with significant reductions in deafness, in patients treated with dexamethasone as an adjunctive therapy to antibiotics (11). In adults with bacterial meningitis, a recent major trial demonstrated that treatment with adjunctive steroids, along with antibiotics, led to significant improvement in mortality and morbidity in patients with meningitis due to S. pneumoniae (12). Among patients with meningococcal meningitis, there was a trend toward improved outcomes. Patients with suspected pneumococcal meningitis should receive their first dose of dexamethasone 20–30 minutes prior to or at the same time as the initial antibiotic administration. The recommended dose and duration is 0.15 mg/kg every 6 hours for 2 to 4 days. The use of dexamethasone appears to have no benefit if administered after antibiotics have already been given, and data are lacking for patients with meningitis due to organisms other than S. pneumoniae. Most experts recommend against the use of adjunctive corticosteroids in these cases (10-13). Several questions, however, remain unanswered with regard to adjunctive corticosteroid use. These include the optimal duration of treatment, whether the penetration of vancomycin into the CSF is significantly decreased by dexamethasone, and whether they should be administered to immunocompromised patients (14).
Prevention
Currently, prevention of some types of bacterial meningitis can be accomplished by appropriate use of vaccines, or through antibiotic chemoprophylaxis in certain situations. For adults, vaccines are available against the 2 most common causes of bacterial meningitis. The 23 polyvalent pneumococcal vaccine is recommended for all adults >65 years of age and for anyone age >2 with a compromised immune status. The meningococcal vaccine is available as a quadravalent vaccine (serotypes A, C, Y, and W-135) and should be administered to anyone with functional asplenia, terminal complement deficiencies, those traveling to endemic areas of meningococcal meningitis, and any college freshman requesting the vaccine who will be living in college dormitories (15).
Antibiotic chemoprophylaxis can be administered to individuals who have had close contact with an index patient with meningococcal meningitis. Antibiotics should be administered as soon as exposure has been determined. There are several options available for meningococcal meningitis exposure. Ciprofloxacin is probably the simplest regimen due to its 1-time 500-mg oral dose. Other options include rifampin 600 mg every 12 hours ×4 doses and ceftriaxone 250 mg IM as a 1-time dose. Pregnant women should avoid ciprofloxacin and rifampin due to their potential teratogenic effects.
Prognosis and Follow-up
Prognosis of bacterial meningitis is closely linked to the causative organism, the severity of disease at the time of presentation, and the speed at which the disease progresses. One large retrospective study demonstrated in-hospital mortality rates of 25% for S. pneumoniae, 10% for N. meningitidis, and 21% for L. monocytogenes. Conditions associated with an increased risk of mortality included age >60, state of obtundation on admission, and development of seizure within 24 hours of admission. This study also showed that 21% of patients developed some type of neurologic deficits, and, overall, 9% had persistence of these deficits at time of discharge (3). Another study showed that baseline features of hypotension, mental status changes, and seizures were associated with increased mortality and neurologic morbidity (16). A more recent large study evaluating the efficacy of adjunctive corticosteroids reported a mortality rate of 15% in the control arm, with mortality of 34% in patients infected with S. pneumoniae (12). Another study suggested that if patients had a rapid progression of their disease, this seemed to correlate with worse outcomes. These investigators found an uncertain correlation between antibiotic timing and unfavorable outcomes (16).
Patients discharged from the hospital should have close follow-up with their primary care physician or infectious disease specialist. Evaluation in the short-term should focus on any complications that may have developed as a result of the bacterial meningitis; such as mental status change, seizure, focal neurologic deficits, and hearing loss. Long-term evaluations should also address cognitive functioning and the neuropsychiatric well-being of the patient, in addition to those issues addressed during short-term follow-up (11, 12).
Dr. Kim may be reached at seoungk@umich.edu.
References
- Swartz, Morton N. Bacterial Meningitis—A View of the Past 90 Years. N Engl J Med. 2004;351:1826-8.
- van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M. Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med. 2004;351:1849-59.
- Durand ML, Calderwood SB, Weber DJ, et al. Acute Bacterial Meningitis in Adults. A review of 493 episodes. N Engl J Med. 1993;328:21-8.
- Schuchat A, Robinson K, Wenger J, et al. Bacterial meningitis in the United States in 1995. Active Surveillance Team. N Engl J Med. 1997;337:970-6.
- Attia J, Hatala R, Cook DJ, Wong JG. The rational clinical examination. Does this adult patient have acute meningitis? JAMA. 1999;282:175-181.
- Uchihara T, Tsukagoshi H. Jolt accentuation of headache: the most sensitive sign of CSF pleocytosis. Headache. 1991;31:167-71.
- Gopal AK, Whitehouse JD, Simel DL, Corey RG. Cranial computed tomography before lumbar puncture: a prospective clinical evaluation. Arch Intern Med. 1999;159:2681-5.
- Hasbun R, Abrahams J, Jekel J, Quagliarello VJ. Computed tomography of the head before LP in adults with suspected meningitis. N Engl J Med. 2001;345:1727-33.
- Quagliarello VJ, Scheld WM. Treatment of bacterial meningitis. N Engl J Med. 1997;336:708-16.
- Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice Guidelines for the Management of Bacterial Meningitis. Clin Infect Dis. 2004;39:1267-84.
- McIntyre PB, Berkey CS, King SM, et al. Dexamethasone as adjunctive therapy in bacterial meningitis. A meta-analysis of randomized clinical trials since 1988. JAMA. 1997;278:928-31.
- de Gans J, van de Beek D Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002;347:1549-56.
- van de Beek D, de Gans J, McIntyre P, Prasad K. Steroids in adults with acute bacterial meningitis: a systematic review. Lancet Infect Dis 2004;4: 139-43.
- Pile JC, Longworth DL. Should adults with suspected acute bacterial meningitis get adjunctive corticosteroids? Cleve Clin J Med. 2005;72:67-70.
- Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 1997;4613-21.
- Aronin SI, Peduzzi P, Quagliarello VJ. Community-acquired bacterial meningitis: risk stratification for adverse clinical outcome and effect of antibiotic timing. Ann Intern Med. 1998;129:862-9.