User login
50 years of pediatric residency: What has changed?
When Eileen Ouellette, MD, graduated from Boston’s Harvard Medical School in 1962, she was one of seven women in her class of 141 students. She went on to become one of only three women in pediatric residency at Massachusetts General Hospital later that year.
Free room and board was included in the program, Dr. Ouellette recalled, but her cramped room was poorly insulated and so small that she had to kneel on the bed to open her chest of drawers. The young doctor also soon learned that the women residents made less money than their male counterparts.
Dr. Ouellette, 79, now can laugh at the memory of her tiny room and tinier paycheck. The pediatric residents of today are entering a vastly different environment, she said. For starters, the average pay for medical residents in 2017 is $54,107. Women pediatric residents today far outnumber male residents. And most residents enjoy standard-sized rooms or apartments when completing their residencies.
Technology, for instance, greatly aids pediatric residents in their education today, said Renee Jenkins, MD, a professor at Howard University in Washington and a past AAP president.
Fewer hours, more hand-offs
During Dr. Ouellette’s residency from 1962 to 1965, sleep became a luxury. Of 168 hours in a week, residents were sometimes off for only 26 of them, she said.
“That was absolutely brutal,” she said. “You could not think of anything other than sleep. That became the primary focus of your whole life.”
“It didn’t seem crazy at the time,” said Dr. Stanton, founding dean of Seton Hall University Hackensack Meridian School of Medicine, South Orange, N.J. ”You developed the kind of bond with these families that it wouldn’t occur to you to go home.”
In the 1960s, there were no explicit limits on duty hours, according to Susan White, director of external communications for the Accreditation Council of Graduate Medical Education (ACGME). A “Guide for Residency Programs in Pediatrics,” published in 1968, recommended that “time off should be taken only when the service needs of the patients are assured and that “night and weekend duty provides a valuable educational experience. ... Duty of this type every second or third night and weekend is desirable.”
The guide predates the existence of the ACGME – established in 1981 – but it originated from a committee approved by the American Academy of Pediatrics, the American Board of Pediatrics, and the Council on Medical Education of the American Medical Association, according to Ms. White. While some residency programs changed their work hours over the years, the first mandated requirements for duty hours came in 1990 when ACGME set an 80-hour work week for four specialties: internal medicine, dermatology, ophthalmology, and preventive medicine. The council also limited on-call to every third night that year. In 2003, ACGME put in place duty hour requirements for all specialties.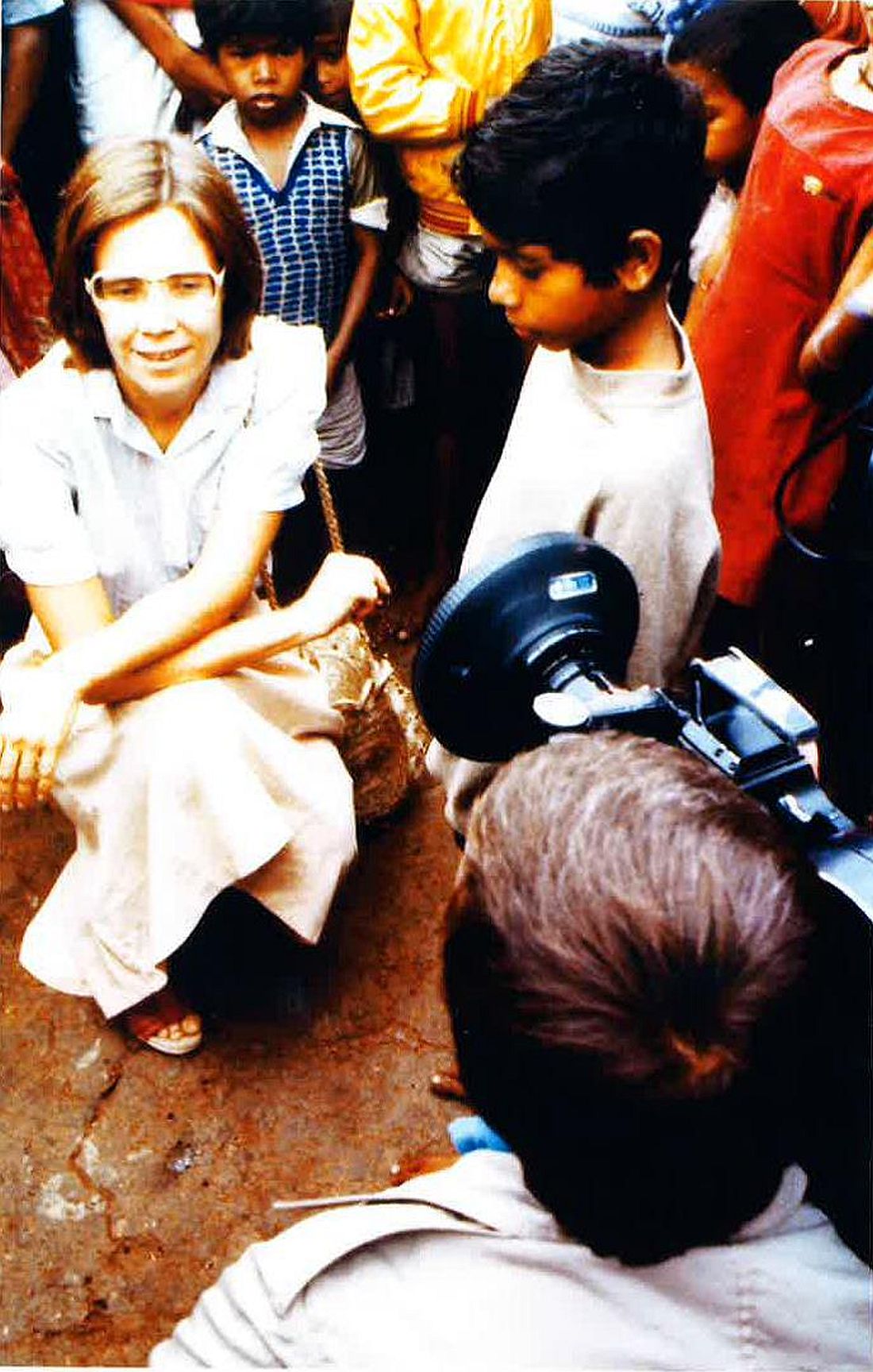
“The pediatric requirements currently in effect provide safeguards for the resident, guidelines for educational programs, specific competencies and medical knowledge, as well as communication skills, professionalism requirements, and standardized assessment,” Ms. White said.
Current limitations for duty hours are beneficial in terms of resident safety, but the restrictions can be a double-edged sword, Dr. Jenkins said.
A changing gender demographic
By the time Dr. Stanton graduated from Yale in 1976, about 15% of her class were women, a marked shift from just a few years earlier, she said.
“In my residency program, women made up a quarter of our group,” she recalled. “That was a big change.”
The number of women going into pediatric residency has steadily increased in the last 5 decades, now far surpassing the number of men. Of 8,933 pediatric residents from 2015 to 2016, 67% were female and 25% were male, (with 8% not reporting), according to ACGME data.
“
Pediatrics is a natural selection for women, especially for those who plan to raise families, said Antoinette Eaton, MD, a retired pediatrician who completed her residency in the late 1950s at what is now Nationwide Children’s Hospital in Columbus, Ohio. Pediatrics is a prime specialty for career and family balance, she said.
“I worked part time a lot during my career,” said Dr. Eaton, a past AAP president. “Always being responsible as a mother and to the house were very high priorities.”
Dr. Stanton agrees that pediatric practices are much more tolerant of part time work, allowing women to better juggle children and career. However, she notes that the decline of male pediatricians also can be negative for the field overall.
New focus, growing debt
The curriculum focus for pediatric residency, meanwhile, has changed significantly over the years, pediatricians say. Dr. Eaton recalls her residency being almost entirely focused on inpatient care. In fact, insurance companies often refused to pay for outpatient care in sharp contrast to today, she said.
“You had to admit the patient if you wanted insurance to pay for it,” she said. “For example, if you had a patient with cerebral palsy or special needs, I had to admit that patient for 3, 4, 5 days. It was really different than what you have today.”
As time has passed, pediatric requirements have changed to emphasize the need for balance between inpatient and outpatient care, with a focus on continuity of care in either setting, Ms. White said. Newer additions to the requirements include the competencies of professionalism, communication, and life-long learning.
“Over the years these setting have expanded to include inpatients in hospitals, clinics, emergency centers, intensive care units, and in the community, [including] schools and other settings,” she said. “The requirements have always emphasized the importance of having high-quality, board-certified faculty to provide bedside teaching and deliver lectures at conferences.”
Another marked change for pediatric residents is the accumulation of debt. After her medical education, Dr. Jenkins owed about $1,500, she recalls.
“Today, that’s a drop in the bucket,” she said. “For the most part, you stayed out of [debt] trouble. It was nothing compared to that kids have to pay now.”
In 2014, the average medical school student graduated with a median debt of $180,000, according to data from the Association of American Medical Colleges. The wide debt differences are attributed to more expensive medical education today, Dr. Jenkins said.
While debt has risen, clinical responsibilities for residents have dropped as physician extenders and advanced equipment have become commonplace.
When Dr. Ouellette was a resident in the 1960s, there were few technicians to assist and no CT scans or MRIs for imaging. Residents drew blood from and gave blood to patients themselves. They took x-rays and developed them, she said.
“We had to use our brains and figure out what was going on,” she said. “People don’t think so much now. They send x-rays or scans to someone else, rather than figuring out the answer. Medicine may not be as much fun now as it was back then.”
Dr. Eaton added that residents have more technical demands today, more regulations to follow, and more paperwork to complete than the residents of the past. However, she believes pediatrics remains a worthwhile medical path. Three of her four children became doctors, one of whom went into pediatrics.
“I’m very disturbed when people try to convince children not to go into medicine,” she said. “I think it’s still a wonderful and rewarding career.”
agallegos@frontlinemedcom.com
On Twitter @legal_med
*Clarification made on 4/21/17
When Eileen Ouellette, MD, graduated from Boston’s Harvard Medical School in 1962, she was one of seven women in her class of 141 students. She went on to become one of only three women in pediatric residency at Massachusetts General Hospital later that year.
Free room and board was included in the program, Dr. Ouellette recalled, but her cramped room was poorly insulated and so small that she had to kneel on the bed to open her chest of drawers. The young doctor also soon learned that the women residents made less money than their male counterparts.
Dr. Ouellette, 79, now can laugh at the memory of her tiny room and tinier paycheck. The pediatric residents of today are entering a vastly different environment, she said. For starters, the average pay for medical residents in 2017 is $54,107. Women pediatric residents today far outnumber male residents. And most residents enjoy standard-sized rooms or apartments when completing their residencies.
Technology, for instance, greatly aids pediatric residents in their education today, said Renee Jenkins, MD, a professor at Howard University in Washington and a past AAP president.
Fewer hours, more hand-offs
During Dr. Ouellette’s residency from 1962 to 1965, sleep became a luxury. Of 168 hours in a week, residents were sometimes off for only 26 of them, she said.
“That was absolutely brutal,” she said. “You could not think of anything other than sleep. That became the primary focus of your whole life.”
“It didn’t seem crazy at the time,” said Dr. Stanton, founding dean of Seton Hall University Hackensack Meridian School of Medicine, South Orange, N.J. ”You developed the kind of bond with these families that it wouldn’t occur to you to go home.”
In the 1960s, there were no explicit limits on duty hours, according to Susan White, director of external communications for the Accreditation Council of Graduate Medical Education (ACGME). A “Guide for Residency Programs in Pediatrics,” published in 1968, recommended that “time off should be taken only when the service needs of the patients are assured and that “night and weekend duty provides a valuable educational experience. ... Duty of this type every second or third night and weekend is desirable.”
The guide predates the existence of the ACGME – established in 1981 – but it originated from a committee approved by the American Academy of Pediatrics, the American Board of Pediatrics, and the Council on Medical Education of the American Medical Association, according to Ms. White. While some residency programs changed their work hours over the years, the first mandated requirements for duty hours came in 1990 when ACGME set an 80-hour work week for four specialties: internal medicine, dermatology, ophthalmology, and preventive medicine. The council also limited on-call to every third night that year. In 2003, ACGME put in place duty hour requirements for all specialties.
“The pediatric requirements currently in effect provide safeguards for the resident, guidelines for educational programs, specific competencies and medical knowledge, as well as communication skills, professionalism requirements, and standardized assessment,” Ms. White said.
Current limitations for duty hours are beneficial in terms of resident safety, but the restrictions can be a double-edged sword, Dr. Jenkins said.
A changing gender demographic
By the time Dr. Stanton graduated from Yale in 1976, about 15% of her class were women, a marked shift from just a few years earlier, she said.
“In my residency program, women made up a quarter of our group,” she recalled. “That was a big change.”
The number of women going into pediatric residency has steadily increased in the last 5 decades, now far surpassing the number of men. Of 8,933 pediatric residents from 2015 to 2016, 67% were female and 25% were male, (with 8% not reporting), according to ACGME data.
“
Pediatrics is a natural selection for women, especially for those who plan to raise families, said Antoinette Eaton, MD, a retired pediatrician who completed her residency in the late 1950s at what is now Nationwide Children’s Hospital in Columbus, Ohio. Pediatrics is a prime specialty for career and family balance, she said.
“I worked part time a lot during my career,” said Dr. Eaton, a past AAP president. “Always being responsible as a mother and to the house were very high priorities.”
Dr. Stanton agrees that pediatric practices are much more tolerant of part time work, allowing women to better juggle children and career. However, she notes that the decline of male pediatricians also can be negative for the field overall.
New focus, growing debt
The curriculum focus for pediatric residency, meanwhile, has changed significantly over the years, pediatricians say. Dr. Eaton recalls her residency being almost entirely focused on inpatient care. In fact, insurance companies often refused to pay for outpatient care in sharp contrast to today, she said.
“You had to admit the patient if you wanted insurance to pay for it,” she said. “For example, if you had a patient with cerebral palsy or special needs, I had to admit that patient for 3, 4, 5 days. It was really different than what you have today.”
As time has passed, pediatric requirements have changed to emphasize the need for balance between inpatient and outpatient care, with a focus on continuity of care in either setting, Ms. White said. Newer additions to the requirements include the competencies of professionalism, communication, and life-long learning.
“Over the years these setting have expanded to include inpatients in hospitals, clinics, emergency centers, intensive care units, and in the community, [including] schools and other settings,” she said. “The requirements have always emphasized the importance of having high-quality, board-certified faculty to provide bedside teaching and deliver lectures at conferences.”
Another marked change for pediatric residents is the accumulation of debt. After her medical education, Dr. Jenkins owed about $1,500, she recalls.
“Today, that’s a drop in the bucket,” she said. “For the most part, you stayed out of [debt] trouble. It was nothing compared to that kids have to pay now.”
In 2014, the average medical school student graduated with a median debt of $180,000, according to data from the Association of American Medical Colleges. The wide debt differences are attributed to more expensive medical education today, Dr. Jenkins said.
While debt has risen, clinical responsibilities for residents have dropped as physician extenders and advanced equipment have become commonplace.
When Dr. Ouellette was a resident in the 1960s, there were few technicians to assist and no CT scans or MRIs for imaging. Residents drew blood from and gave blood to patients themselves. They took x-rays and developed them, she said.
“We had to use our brains and figure out what was going on,” she said. “People don’t think so much now. They send x-rays or scans to someone else, rather than figuring out the answer. Medicine may not be as much fun now as it was back then.”
Dr. Eaton added that residents have more technical demands today, more regulations to follow, and more paperwork to complete than the residents of the past. However, she believes pediatrics remains a worthwhile medical path. Three of her four children became doctors, one of whom went into pediatrics.
“I’m very disturbed when people try to convince children not to go into medicine,” she said. “I think it’s still a wonderful and rewarding career.”
agallegos@frontlinemedcom.com
On Twitter @legal_med
*Clarification made on 4/21/17
When Eileen Ouellette, MD, graduated from Boston’s Harvard Medical School in 1962, she was one of seven women in her class of 141 students. She went on to become one of only three women in pediatric residency at Massachusetts General Hospital later that year.
Free room and board was included in the program, Dr. Ouellette recalled, but her cramped room was poorly insulated and so small that she had to kneel on the bed to open her chest of drawers. The young doctor also soon learned that the women residents made less money than their male counterparts.
Dr. Ouellette, 79, now can laugh at the memory of her tiny room and tinier paycheck. The pediatric residents of today are entering a vastly different environment, she said. For starters, the average pay for medical residents in 2017 is $54,107. Women pediatric residents today far outnumber male residents. And most residents enjoy standard-sized rooms or apartments when completing their residencies.
Technology, for instance, greatly aids pediatric residents in their education today, said Renee Jenkins, MD, a professor at Howard University in Washington and a past AAP president.
Fewer hours, more hand-offs
During Dr. Ouellette’s residency from 1962 to 1965, sleep became a luxury. Of 168 hours in a week, residents were sometimes off for only 26 of them, she said.
“That was absolutely brutal,” she said. “You could not think of anything other than sleep. That became the primary focus of your whole life.”
“It didn’t seem crazy at the time,” said Dr. Stanton, founding dean of Seton Hall University Hackensack Meridian School of Medicine, South Orange, N.J. ”You developed the kind of bond with these families that it wouldn’t occur to you to go home.”
In the 1960s, there were no explicit limits on duty hours, according to Susan White, director of external communications for the Accreditation Council of Graduate Medical Education (ACGME). A “Guide for Residency Programs in Pediatrics,” published in 1968, recommended that “time off should be taken only when the service needs of the patients are assured and that “night and weekend duty provides a valuable educational experience. ... Duty of this type every second or third night and weekend is desirable.”
The guide predates the existence of the ACGME – established in 1981 – but it originated from a committee approved by the American Academy of Pediatrics, the American Board of Pediatrics, and the Council on Medical Education of the American Medical Association, according to Ms. White. While some residency programs changed their work hours over the years, the first mandated requirements for duty hours came in 1990 when ACGME set an 80-hour work week for four specialties: internal medicine, dermatology, ophthalmology, and preventive medicine. The council also limited on-call to every third night that year. In 2003, ACGME put in place duty hour requirements for all specialties.
“The pediatric requirements currently in effect provide safeguards for the resident, guidelines for educational programs, specific competencies and medical knowledge, as well as communication skills, professionalism requirements, and standardized assessment,” Ms. White said.
Current limitations for duty hours are beneficial in terms of resident safety, but the restrictions can be a double-edged sword, Dr. Jenkins said.
A changing gender demographic
By the time Dr. Stanton graduated from Yale in 1976, about 15% of her class were women, a marked shift from just a few years earlier, she said.
“In my residency program, women made up a quarter of our group,” she recalled. “That was a big change.”
The number of women going into pediatric residency has steadily increased in the last 5 decades, now far surpassing the number of men. Of 8,933 pediatric residents from 2015 to 2016, 67% were female and 25% were male, (with 8% not reporting), according to ACGME data.
“
Pediatrics is a natural selection for women, especially for those who plan to raise families, said Antoinette Eaton, MD, a retired pediatrician who completed her residency in the late 1950s at what is now Nationwide Children’s Hospital in Columbus, Ohio. Pediatrics is a prime specialty for career and family balance, she said.
“I worked part time a lot during my career,” said Dr. Eaton, a past AAP president. “Always being responsible as a mother and to the house were very high priorities.”
Dr. Stanton agrees that pediatric practices are much more tolerant of part time work, allowing women to better juggle children and career. However, she notes that the decline of male pediatricians also can be negative for the field overall.
New focus, growing debt
The curriculum focus for pediatric residency, meanwhile, has changed significantly over the years, pediatricians say. Dr. Eaton recalls her residency being almost entirely focused on inpatient care. In fact, insurance companies often refused to pay for outpatient care in sharp contrast to today, she said.
“You had to admit the patient if you wanted insurance to pay for it,” she said. “For example, if you had a patient with cerebral palsy or special needs, I had to admit that patient for 3, 4, 5 days. It was really different than what you have today.”
As time has passed, pediatric requirements have changed to emphasize the need for balance between inpatient and outpatient care, with a focus on continuity of care in either setting, Ms. White said. Newer additions to the requirements include the competencies of professionalism, communication, and life-long learning.
“Over the years these setting have expanded to include inpatients in hospitals, clinics, emergency centers, intensive care units, and in the community, [including] schools and other settings,” she said. “The requirements have always emphasized the importance of having high-quality, board-certified faculty to provide bedside teaching and deliver lectures at conferences.”
Another marked change for pediatric residents is the accumulation of debt. After her medical education, Dr. Jenkins owed about $1,500, she recalls.
“Today, that’s a drop in the bucket,” she said. “For the most part, you stayed out of [debt] trouble. It was nothing compared to that kids have to pay now.”
In 2014, the average medical school student graduated with a median debt of $180,000, according to data from the Association of American Medical Colleges. The wide debt differences are attributed to more expensive medical education today, Dr. Jenkins said.
While debt has risen, clinical responsibilities for residents have dropped as physician extenders and advanced equipment have become commonplace.
When Dr. Ouellette was a resident in the 1960s, there were few technicians to assist and no CT scans or MRIs for imaging. Residents drew blood from and gave blood to patients themselves. They took x-rays and developed them, she said.
“We had to use our brains and figure out what was going on,” she said. “People don’t think so much now. They send x-rays or scans to someone else, rather than figuring out the answer. Medicine may not be as much fun now as it was back then.”
Dr. Eaton added that residents have more technical demands today, more regulations to follow, and more paperwork to complete than the residents of the past. However, she believes pediatrics remains a worthwhile medical path. Three of her four children became doctors, one of whom went into pediatrics.
“I’m very disturbed when people try to convince children not to go into medicine,” she said. “I think it’s still a wonderful and rewarding career.”
agallegos@frontlinemedcom.com
On Twitter @legal_med
*Clarification made on 4/21/17
Well-child care: Steady growth in breadth and content
Fifty years ago in 1967, the American Academy of Pediatrics published a “Suggested Schedule for Preventive Child Health Care.” It was, in essence, the first periodicity schedule for well-child visits.
Described by AAP officials at the time as an “amalgamation of schedules used in various clinics and private offices,” it charted out the frequency and basic content of visits from 1 month through 6 years of age, and offered a simple list of items to be considered for guidance and discussion in all visits from 6 years on.
It is updated in real time, and is accompanied by an expansive package of Bright Futures recommendations, guidelines, and tools (including forms, handouts, and questionnaires) for health promotion and guidance. Together, the Periodicity Schedule and Bright Futures guidance reflect decades of steady change in the breadth and content of well-child care – and more recently, in some of its processes.
“When I started practicing [in 1979], developmental surveillance meant asking a few questions about developmental milestones, observing, and maybe lifting a few questions from the Denver Scale [the Denver Developmental Screening Test] to support our surveillance,” said Joseph F. Hagan, Jr., MD, a pediatrician in Burlington, Vt., and coeditor of Bright Futures.
Jack Swanson, MD, a pediatrician in Ames, Iowa, and a member of the Bright Futures Steering Committee, has similar recollections of well-child care in the early 1970s. “The developmental milestones were just questions and nothing more formal. Nutrition was a big [anticipatory guidance] issue, and some safety,” he recalled.
In early pediatric visits, “parents were interested in Dr. [Benjamin] Spock’s recommendations about feeding and raising their baby… and we used to make our own [anticipatory guidance] handouts,” he said. And in the later years, “an adolescent visit used to be every 2 or 3 years.”
“During the Vietnam War, there weren’t enough people who were healthy enough, physically fit enough, to be mustered into the Army,” said Peter Rappo, MD, a pediatrician in Brockton, Mass., who chaired the AAP’s Committee on Practice and Ambulatory Medicine in the late 1990s.
Dr. Rappo became interested in the history of preventive pediatric care after discovering a Children’s Year Campaign (1918-1919) poster in an antiques market. The poster’s message – “The Health of the Child is the Power of the Nation” – remained relevant through the Vietnam War. “I’d like to think that [childhood preventive services] were all about the kids,” he said, “but at the end of the day, it was about military issues too.”
Still, interest in the 1960s in the long-term implications of early-life development fed research that eventually led to an explosion of new science in the 1990s on the importance of early brain development and early life experiences. This scientific literature combined with greater societal interest in school readiness helped drive development of research-based instruments for developmental screening, said pediatrician Edward L. Schor, MD, formerly a vice president at the Commonwealth Fund and now a senior vice president for programs and partnerships at Lucile Packard Foundation for Children’s Health.
“Development was the first topic … of screening instruments,” he said. The tools have “not only increased the quality of care, they also have increased the efficiency of care, because the time to ask and answer these questions was shifted to the waiting room.”
Their use is far from universal, but increasing. Results of the Periodic Surveys administered to a national random sample of AAP members show that pediatricians’ use of at least one formal screening instrument to identify children through 36 months of age at risk for developmental delay increased from 23% in 2002 to 45% in 2009 and 63% in 2016. (And in 2016, 81% reported “always/almost always” using at least one formal screening tool for autism.) The data was presented at the annual meeting of the Society of Developmental and Behavioral Pediatrics September 2016.
For Dr. Rappo’s practice in Massachusetts, the adoption of developmental and behavioral health screening questionnaires for all ages was spurred by a 2007 mandate requiring formal screening for children and adolescents in MassHealth, the state’s combined Medicaid–Children’s Health Insurance Program.
“We all knew intuitively this is what we should be doing, so we also sat down with insurers to talk about why this is important for kids,” he said. Reimbursement improved, and most importantly, he said, use of the tools “has tremendously improved our opportunities for opening up discussions with parents about developmental-behavioral issues.”
The well-child visit of 50 years ago was much more of “a physician-generated, physician-led visit,” said Dr. Swanson. “The pediatrician knew what was needed, and at the end, we’d ask if there were any questions. Today, the first question recommended by Bright Futures is ‘Do you have any questions for the visit?’”
According to a 2009 focus group study involving 282 pediatricians and 41 nurse-practitioners, clinicians agree that eliciting and prioritizing parent concerns is a top priority in well-child care. Yet there’s also some unease. Some said in the focus group discussions that they feel constrained by the Periodicity Schedule, for instance, or feel tension between inviting parents’ concerns while simultaneously addressing the content recommended by professional guidelines (Pediatrics. 2009 Sep;124[3]:849-57).
Indeed, policies and recommendations for health promotion and anticipatory guidance (some consensus-based, some evidence-based or evidence-informed) mushroomed throughout the 1980s and 1990s, Dr. Swanson said. Combined with the increase in recommended screenings through the 1990s and 2000s – and in recent years, the increasing need for discussions to address vaccine concerns, mental and behavioral health issues, and obesity and overweight problems – there are real pulls and tugs.
The time allotted to well-child visits may have increased slightly for some pediatricians – to just over 20 minutes – but overall, visit length hasn’t changed much over the past few decades. “It has pretty much stayed the same, averaging between 15 and 20 minutes,” said Dr. Schor.
Offering guidance to clinicians in prioritizing questions and issues has been a goal in the last two editions (2008 and 2016) of the Bright Futures recommendations – formally called the Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. “The joke was that if you did a Bright Futures well-child visit according to the old Bright Futures, you’d do one in the morning and one in the afternoon,” said Dr. Hagan.
The first edition came out in 1994, after a multidisciplinary group convened by the Maternal and Child Health Bureau at the Health Resources and Services Administration, and the Medicaid Bureau (then part of the Health Care Financing Administration) established the Bright Futures Children’s Health Charter to improve children’s health. The second edition was released in 2000 and updated in 2002, at which point the AAP established the Bright Futures National Center.
Previsit screening tools included in the new edition are aimed at assessing and prioritizing anticipatory guidance issues, Dr. Hagan said, noting too that the Periodicity Schedule and Bright Futures recommendations make distinctions between universal and selective screening. “By design,” he emphasized, “there’s more anticipatory guidance than you might ever accomplish in one visit, because we want to be thorough enough to provide a context – a schema – to deal with the issues.”
Oftentimes, he said, “what parents want to talk about is what you want to talk about.” And pediatricians “develop a skill set to temporize, to figure out what needs to be covered today, and what can be dealt with better at a later time,” Dr. Hagan said. “If you tell kids, for instance, ‘I can help you with this, I just have to get more information,’ they hear that there’s help on the way. Then you follow through.”
Overall, his well-child visits “have gotten much more involved with the emotional well-being of children.” Given that emotional issues and behavioral issues “tend to take a longer time to discuss and unravel,” he sets aside consultation times near the end of the day for families who need to discuss these issues.
And he routinely devotes time – starting at the 2-month visit – to discuss screen time and media use. “I believe that technology is making our children sick,” he said, noting that in his nearly 17 years of practice he has seen increasing numbers of children and adolescents with depression, anxiety, anger, and attention deficit/hyperactivity disorder. “The AAP has done a pretty good job of raising the point, but I don’t think it has hit home with parents yet.”
For Dr. Chung, electronic medical records and systems have enabled him to better flag issues for follow-up over the course of well-child visits, leading to “better longitudinal care.”
Surveys and questionnaires filled out by parents in his practice’s waiting room are scanned into charts, he noted, and adolescents can mark answers on a proprietary confidential risk questionnaire that subsequently gets scrambled so that no one but the provider can understand the responses.
Other potential impacts of electronic systems have yet to be realized, he and others said. Some pediatric practices, Dr. Schor said, have begun engaging with families ahead of well-child visits through the use of a computerized questionnaire that elicits areas and issues of interest. Such outreach may help families feel more invested and committed to attending the visits, particularly those that don’t involve immunizations or school/sport forms, he said.
Families are “not [always] buying what we’re selling [for well-child care],” said Dr. Schor, who has served on AAP committees and has written several well-cited articles on preventive pediatrics care.
Insurance coverage for well-child care got a boost in 2010 when Bright Futures was cited in the Affordable Care Act as the standard of what well-child care should accomplish, and its recommended screenings and services were required to be covered by insurers without cost-sharing.
In the long-run, he said, rethinking the roles of nonphysicians in anticipatory guidance and developmental and psychosocial screening – in interpreting results of questionnaires, for instance – may be essential for well-child care. Outside of large health care systems, “the use of personnel [has been] pretty much been unchanged over the years,” he said. “We need to ask, how can we use each individual’s skills and training most efficiently? How can we retrain and reorganize our patient flow?”
This may be especially important as well-child care increasingly considers family psychosocial issues such as housing, food insecurity, family violence, and other family social stressors. Maternal depression screening made its way into the Periodicity Schedule in February 2016, and Dr. Schor predicts that the schedule will include “family psychosocial risk screening” in another several years.
For now, the newly revised Bright Futures guidelines – and much of well-child care – places an increased emphasis on the social determinants of health, which Dr. Hagan said reflects the “long-standing, logical conclusion that we reached back in the 1990s – that if families are healthy, kids will be healthy … and that family health is also linked to community health.”
Fifty years ago in 1967, the American Academy of Pediatrics published a “Suggested Schedule for Preventive Child Health Care.” It was, in essence, the first periodicity schedule for well-child visits.
Described by AAP officials at the time as an “amalgamation of schedules used in various clinics and private offices,” it charted out the frequency and basic content of visits from 1 month through 6 years of age, and offered a simple list of items to be considered for guidance and discussion in all visits from 6 years on.
It is updated in real time, and is accompanied by an expansive package of Bright Futures recommendations, guidelines, and tools (including forms, handouts, and questionnaires) for health promotion and guidance. Together, the Periodicity Schedule and Bright Futures guidance reflect decades of steady change in the breadth and content of well-child care – and more recently, in some of its processes.
“When I started practicing [in 1979], developmental surveillance meant asking a few questions about developmental milestones, observing, and maybe lifting a few questions from the Denver Scale [the Denver Developmental Screening Test] to support our surveillance,” said Joseph F. Hagan, Jr., MD, a pediatrician in Burlington, Vt., and coeditor of Bright Futures.
Jack Swanson, MD, a pediatrician in Ames, Iowa, and a member of the Bright Futures Steering Committee, has similar recollections of well-child care in the early 1970s. “The developmental milestones were just questions and nothing more formal. Nutrition was a big [anticipatory guidance] issue, and some safety,” he recalled.
In early pediatric visits, “parents were interested in Dr. [Benjamin] Spock’s recommendations about feeding and raising their baby… and we used to make our own [anticipatory guidance] handouts,” he said. And in the later years, “an adolescent visit used to be every 2 or 3 years.”
“During the Vietnam War, there weren’t enough people who were healthy enough, physically fit enough, to be mustered into the Army,” said Peter Rappo, MD, a pediatrician in Brockton, Mass., who chaired the AAP’s Committee on Practice and Ambulatory Medicine in the late 1990s.
Dr. Rappo became interested in the history of preventive pediatric care after discovering a Children’s Year Campaign (1918-1919) poster in an antiques market. The poster’s message – “The Health of the Child is the Power of the Nation” – remained relevant through the Vietnam War. “I’d like to think that [childhood preventive services] were all about the kids,” he said, “but at the end of the day, it was about military issues too.”
Still, interest in the 1960s in the long-term implications of early-life development fed research that eventually led to an explosion of new science in the 1990s on the importance of early brain development and early life experiences. This scientific literature combined with greater societal interest in school readiness helped drive development of research-based instruments for developmental screening, said pediatrician Edward L. Schor, MD, formerly a vice president at the Commonwealth Fund and now a senior vice president for programs and partnerships at Lucile Packard Foundation for Children’s Health.
“Development was the first topic … of screening instruments,” he said. The tools have “not only increased the quality of care, they also have increased the efficiency of care, because the time to ask and answer these questions was shifted to the waiting room.”
Their use is far from universal, but increasing. Results of the Periodic Surveys administered to a national random sample of AAP members show that pediatricians’ use of at least one formal screening instrument to identify children through 36 months of age at risk for developmental delay increased from 23% in 2002 to 45% in 2009 and 63% in 2016. (And in 2016, 81% reported “always/almost always” using at least one formal screening tool for autism.) The data was presented at the annual meeting of the Society of Developmental and Behavioral Pediatrics September 2016.
For Dr. Rappo’s practice in Massachusetts, the adoption of developmental and behavioral health screening questionnaires for all ages was spurred by a 2007 mandate requiring formal screening for children and adolescents in MassHealth, the state’s combined Medicaid–Children’s Health Insurance Program.
“We all knew intuitively this is what we should be doing, so we also sat down with insurers to talk about why this is important for kids,” he said. Reimbursement improved, and most importantly, he said, use of the tools “has tremendously improved our opportunities for opening up discussions with parents about developmental-behavioral issues.”
The well-child visit of 50 years ago was much more of “a physician-generated, physician-led visit,” said Dr. Swanson. “The pediatrician knew what was needed, and at the end, we’d ask if there were any questions. Today, the first question recommended by Bright Futures is ‘Do you have any questions for the visit?’”
According to a 2009 focus group study involving 282 pediatricians and 41 nurse-practitioners, clinicians agree that eliciting and prioritizing parent concerns is a top priority in well-child care. Yet there’s also some unease. Some said in the focus group discussions that they feel constrained by the Periodicity Schedule, for instance, or feel tension between inviting parents’ concerns while simultaneously addressing the content recommended by professional guidelines (Pediatrics. 2009 Sep;124[3]:849-57).
Indeed, policies and recommendations for health promotion and anticipatory guidance (some consensus-based, some evidence-based or evidence-informed) mushroomed throughout the 1980s and 1990s, Dr. Swanson said. Combined with the increase in recommended screenings through the 1990s and 2000s – and in recent years, the increasing need for discussions to address vaccine concerns, mental and behavioral health issues, and obesity and overweight problems – there are real pulls and tugs.
The time allotted to well-child visits may have increased slightly for some pediatricians – to just over 20 minutes – but overall, visit length hasn’t changed much over the past few decades. “It has pretty much stayed the same, averaging between 15 and 20 minutes,” said Dr. Schor.
Offering guidance to clinicians in prioritizing questions and issues has been a goal in the last two editions (2008 and 2016) of the Bright Futures recommendations – formally called the Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. “The joke was that if you did a Bright Futures well-child visit according to the old Bright Futures, you’d do one in the morning and one in the afternoon,” said Dr. Hagan.
The first edition came out in 1994, after a multidisciplinary group convened by the Maternal and Child Health Bureau at the Health Resources and Services Administration, and the Medicaid Bureau (then part of the Health Care Financing Administration) established the Bright Futures Children’s Health Charter to improve children’s health. The second edition was released in 2000 and updated in 2002, at which point the AAP established the Bright Futures National Center.
Previsit screening tools included in the new edition are aimed at assessing and prioritizing anticipatory guidance issues, Dr. Hagan said, noting too that the Periodicity Schedule and Bright Futures recommendations make distinctions between universal and selective screening. “By design,” he emphasized, “there’s more anticipatory guidance than you might ever accomplish in one visit, because we want to be thorough enough to provide a context – a schema – to deal with the issues.”
Oftentimes, he said, “what parents want to talk about is what you want to talk about.” And pediatricians “develop a skill set to temporize, to figure out what needs to be covered today, and what can be dealt with better at a later time,” Dr. Hagan said. “If you tell kids, for instance, ‘I can help you with this, I just have to get more information,’ they hear that there’s help on the way. Then you follow through.”
Overall, his well-child visits “have gotten much more involved with the emotional well-being of children.” Given that emotional issues and behavioral issues “tend to take a longer time to discuss and unravel,” he sets aside consultation times near the end of the day for families who need to discuss these issues.
And he routinely devotes time – starting at the 2-month visit – to discuss screen time and media use. “I believe that technology is making our children sick,” he said, noting that in his nearly 17 years of practice he has seen increasing numbers of children and adolescents with depression, anxiety, anger, and attention deficit/hyperactivity disorder. “The AAP has done a pretty good job of raising the point, but I don’t think it has hit home with parents yet.”
For Dr. Chung, electronic medical records and systems have enabled him to better flag issues for follow-up over the course of well-child visits, leading to “better longitudinal care.”
Surveys and questionnaires filled out by parents in his practice’s waiting room are scanned into charts, he noted, and adolescents can mark answers on a proprietary confidential risk questionnaire that subsequently gets scrambled so that no one but the provider can understand the responses.
Other potential impacts of electronic systems have yet to be realized, he and others said. Some pediatric practices, Dr. Schor said, have begun engaging with families ahead of well-child visits through the use of a computerized questionnaire that elicits areas and issues of interest. Such outreach may help families feel more invested and committed to attending the visits, particularly those that don’t involve immunizations or school/sport forms, he said.
Families are “not [always] buying what we’re selling [for well-child care],” said Dr. Schor, who has served on AAP committees and has written several well-cited articles on preventive pediatrics care.
Insurance coverage for well-child care got a boost in 2010 when Bright Futures was cited in the Affordable Care Act as the standard of what well-child care should accomplish, and its recommended screenings and services were required to be covered by insurers without cost-sharing.
In the long-run, he said, rethinking the roles of nonphysicians in anticipatory guidance and developmental and psychosocial screening – in interpreting results of questionnaires, for instance – may be essential for well-child care. Outside of large health care systems, “the use of personnel [has been] pretty much been unchanged over the years,” he said. “We need to ask, how can we use each individual’s skills and training most efficiently? How can we retrain and reorganize our patient flow?”
This may be especially important as well-child care increasingly considers family psychosocial issues such as housing, food insecurity, family violence, and other family social stressors. Maternal depression screening made its way into the Periodicity Schedule in February 2016, and Dr. Schor predicts that the schedule will include “family psychosocial risk screening” in another several years.
For now, the newly revised Bright Futures guidelines – and much of well-child care – places an increased emphasis on the social determinants of health, which Dr. Hagan said reflects the “long-standing, logical conclusion that we reached back in the 1990s – that if families are healthy, kids will be healthy … and that family health is also linked to community health.”
Fifty years ago in 1967, the American Academy of Pediatrics published a “Suggested Schedule for Preventive Child Health Care.” It was, in essence, the first periodicity schedule for well-child visits.
Described by AAP officials at the time as an “amalgamation of schedules used in various clinics and private offices,” it charted out the frequency and basic content of visits from 1 month through 6 years of age, and offered a simple list of items to be considered for guidance and discussion in all visits from 6 years on.
It is updated in real time, and is accompanied by an expansive package of Bright Futures recommendations, guidelines, and tools (including forms, handouts, and questionnaires) for health promotion and guidance. Together, the Periodicity Schedule and Bright Futures guidance reflect decades of steady change in the breadth and content of well-child care – and more recently, in some of its processes.
“When I started practicing [in 1979], developmental surveillance meant asking a few questions about developmental milestones, observing, and maybe lifting a few questions from the Denver Scale [the Denver Developmental Screening Test] to support our surveillance,” said Joseph F. Hagan, Jr., MD, a pediatrician in Burlington, Vt., and coeditor of Bright Futures.
Jack Swanson, MD, a pediatrician in Ames, Iowa, and a member of the Bright Futures Steering Committee, has similar recollections of well-child care in the early 1970s. “The developmental milestones were just questions and nothing more formal. Nutrition was a big [anticipatory guidance] issue, and some safety,” he recalled.
In early pediatric visits, “parents were interested in Dr. [Benjamin] Spock’s recommendations about feeding and raising their baby… and we used to make our own [anticipatory guidance] handouts,” he said. And in the later years, “an adolescent visit used to be every 2 or 3 years.”
“During the Vietnam War, there weren’t enough people who were healthy enough, physically fit enough, to be mustered into the Army,” said Peter Rappo, MD, a pediatrician in Brockton, Mass., who chaired the AAP’s Committee on Practice and Ambulatory Medicine in the late 1990s.
Dr. Rappo became interested in the history of preventive pediatric care after discovering a Children’s Year Campaign (1918-1919) poster in an antiques market. The poster’s message – “The Health of the Child is the Power of the Nation” – remained relevant through the Vietnam War. “I’d like to think that [childhood preventive services] were all about the kids,” he said, “but at the end of the day, it was about military issues too.”
Still, interest in the 1960s in the long-term implications of early-life development fed research that eventually led to an explosion of new science in the 1990s on the importance of early brain development and early life experiences. This scientific literature combined with greater societal interest in school readiness helped drive development of research-based instruments for developmental screening, said pediatrician Edward L. Schor, MD, formerly a vice president at the Commonwealth Fund and now a senior vice president for programs and partnerships at Lucile Packard Foundation for Children’s Health.
“Development was the first topic … of screening instruments,” he said. The tools have “not only increased the quality of care, they also have increased the efficiency of care, because the time to ask and answer these questions was shifted to the waiting room.”
Their use is far from universal, but increasing. Results of the Periodic Surveys administered to a national random sample of AAP members show that pediatricians’ use of at least one formal screening instrument to identify children through 36 months of age at risk for developmental delay increased from 23% in 2002 to 45% in 2009 and 63% in 2016. (And in 2016, 81% reported “always/almost always” using at least one formal screening tool for autism.) The data was presented at the annual meeting of the Society of Developmental and Behavioral Pediatrics September 2016.
For Dr. Rappo’s practice in Massachusetts, the adoption of developmental and behavioral health screening questionnaires for all ages was spurred by a 2007 mandate requiring formal screening for children and adolescents in MassHealth, the state’s combined Medicaid–Children’s Health Insurance Program.
“We all knew intuitively this is what we should be doing, so we also sat down with insurers to talk about why this is important for kids,” he said. Reimbursement improved, and most importantly, he said, use of the tools “has tremendously improved our opportunities for opening up discussions with parents about developmental-behavioral issues.”
The well-child visit of 50 years ago was much more of “a physician-generated, physician-led visit,” said Dr. Swanson. “The pediatrician knew what was needed, and at the end, we’d ask if there were any questions. Today, the first question recommended by Bright Futures is ‘Do you have any questions for the visit?’”
According to a 2009 focus group study involving 282 pediatricians and 41 nurse-practitioners, clinicians agree that eliciting and prioritizing parent concerns is a top priority in well-child care. Yet there’s also some unease. Some said in the focus group discussions that they feel constrained by the Periodicity Schedule, for instance, or feel tension between inviting parents’ concerns while simultaneously addressing the content recommended by professional guidelines (Pediatrics. 2009 Sep;124[3]:849-57).
Indeed, policies and recommendations for health promotion and anticipatory guidance (some consensus-based, some evidence-based or evidence-informed) mushroomed throughout the 1980s and 1990s, Dr. Swanson said. Combined with the increase in recommended screenings through the 1990s and 2000s – and in recent years, the increasing need for discussions to address vaccine concerns, mental and behavioral health issues, and obesity and overweight problems – there are real pulls and tugs.
The time allotted to well-child visits may have increased slightly for some pediatricians – to just over 20 minutes – but overall, visit length hasn’t changed much over the past few decades. “It has pretty much stayed the same, averaging between 15 and 20 minutes,” said Dr. Schor.
Offering guidance to clinicians in prioritizing questions and issues has been a goal in the last two editions (2008 and 2016) of the Bright Futures recommendations – formally called the Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. “The joke was that if you did a Bright Futures well-child visit according to the old Bright Futures, you’d do one in the morning and one in the afternoon,” said Dr. Hagan.
The first edition came out in 1994, after a multidisciplinary group convened by the Maternal and Child Health Bureau at the Health Resources and Services Administration, and the Medicaid Bureau (then part of the Health Care Financing Administration) established the Bright Futures Children’s Health Charter to improve children’s health. The second edition was released in 2000 and updated in 2002, at which point the AAP established the Bright Futures National Center.
Previsit screening tools included in the new edition are aimed at assessing and prioritizing anticipatory guidance issues, Dr. Hagan said, noting too that the Periodicity Schedule and Bright Futures recommendations make distinctions between universal and selective screening. “By design,” he emphasized, “there’s more anticipatory guidance than you might ever accomplish in one visit, because we want to be thorough enough to provide a context – a schema – to deal with the issues.”
Oftentimes, he said, “what parents want to talk about is what you want to talk about.” And pediatricians “develop a skill set to temporize, to figure out what needs to be covered today, and what can be dealt with better at a later time,” Dr. Hagan said. “If you tell kids, for instance, ‘I can help you with this, I just have to get more information,’ they hear that there’s help on the way. Then you follow through.”
Overall, his well-child visits “have gotten much more involved with the emotional well-being of children.” Given that emotional issues and behavioral issues “tend to take a longer time to discuss and unravel,” he sets aside consultation times near the end of the day for families who need to discuss these issues.
And he routinely devotes time – starting at the 2-month visit – to discuss screen time and media use. “I believe that technology is making our children sick,” he said, noting that in his nearly 17 years of practice he has seen increasing numbers of children and adolescents with depression, anxiety, anger, and attention deficit/hyperactivity disorder. “The AAP has done a pretty good job of raising the point, but I don’t think it has hit home with parents yet.”
For Dr. Chung, electronic medical records and systems have enabled him to better flag issues for follow-up over the course of well-child visits, leading to “better longitudinal care.”
Surveys and questionnaires filled out by parents in his practice’s waiting room are scanned into charts, he noted, and adolescents can mark answers on a proprietary confidential risk questionnaire that subsequently gets scrambled so that no one but the provider can understand the responses.
Other potential impacts of electronic systems have yet to be realized, he and others said. Some pediatric practices, Dr. Schor said, have begun engaging with families ahead of well-child visits through the use of a computerized questionnaire that elicits areas and issues of interest. Such outreach may help families feel more invested and committed to attending the visits, particularly those that don’t involve immunizations or school/sport forms, he said.
Families are “not [always] buying what we’re selling [for well-child care],” said Dr. Schor, who has served on AAP committees and has written several well-cited articles on preventive pediatrics care.
Insurance coverage for well-child care got a boost in 2010 when Bright Futures was cited in the Affordable Care Act as the standard of what well-child care should accomplish, and its recommended screenings and services were required to be covered by insurers without cost-sharing.
In the long-run, he said, rethinking the roles of nonphysicians in anticipatory guidance and developmental and psychosocial screening – in interpreting results of questionnaires, for instance – may be essential for well-child care. Outside of large health care systems, “the use of personnel [has been] pretty much been unchanged over the years,” he said. “We need to ask, how can we use each individual’s skills and training most efficiently? How can we retrain and reorganize our patient flow?”
This may be especially important as well-child care increasingly considers family psychosocial issues such as housing, food insecurity, family violence, and other family social stressors. Maternal depression screening made its way into the Periodicity Schedule in February 2016, and Dr. Schor predicts that the schedule will include “family psychosocial risk screening” in another several years.
For now, the newly revised Bright Futures guidelines – and much of well-child care – places an increased emphasis on the social determinants of health, which Dr. Hagan said reflects the “long-standing, logical conclusion that we reached back in the 1990s – that if families are healthy, kids will be healthy … and that family health is also linked to community health.”
50 years of child psychiatry, developmental-behavioral pediatrics
The 50th anniversary of Pediatric News prompts us to look back on the past 50 years in child psychiatry and developmental-behavioral pediatrics, and reflect on the evolution of the field. This includes the approach to diagnosis, the thinking about development and family, and the approach and access to treatment during this dynamic period.
While some historians identify the establishment of the first juvenile court in Chicago in 1899 and the work to help judges evaluate juvenile delinquency as the origin of child psychiatry in the United States, it was not until after World War II that the field really began to take root here, largely based on psychiatrists fleeing Europe and the seminal work of Anna Freud. Some of the earliest connections between pediatrics and child psychiatry were based on the work in England of Donald W. Winnicott, a practicing pediatrician and child psychiatrist, Albert J. Solnit, MD, at the Yale Child Study Center, and psychologically informed work of pediatrician Benjamin M. Spock, MD.
The first Diagnostic and Statistical Manual (DSM) was published in 1952, based on a codification of mental disorders established by the Navy during WWII. The American Academy of Child & Adolescent Psychiatry was established in 1953, the same year that the first “tranquilizer,” chlorpromazine (Thorazine) was introduced (in France), marking the start of a revolution in psychiatric care. In 1959, the first candidates sat for a licensing examination in child psychiatry. The Section on Developmental and Behavioral Pediatrics was established as part of the American Academy of Pediatrics in 1960 to support training in this area. The AACAP established a journal in 1961. Child guidance clinics started affiliating with hospitals and universities in the 1960’s, after the Community Mental Health Act of 1963. Then, in 1965, Julius B. Richmond, MD, (a pediatrician) and Uri Bronfenbrenner, PhD, (a developmental psychologist), recognizing the importance of ecological systems to child development, were involved in the creation of Head Start, and the first Joint Commission on Mental Health for Children was established by federal legislation in 1965. The field was truly coalescing into a distinct discipline of medicine, one that bridged pediatrics, psychiatry, and neurology with nonmedical disciplines such as justice and education.
The decade between 1967 and 1977 was a period of transition from the focus on psychoanalytic concepts typical of the first half of the century to a more systematic approach to diagnosis. Children in psychiatric treatment had commonly been seen for extended individual treatments, and those with more disruptive disorders often were hospitalized for long periods. Psychoanalysis focused on the unconscious (theoretical drives and conflicts) to guide treatment. Treatment often focused on the role (causal) of parents, and family treatment was common, even on inpatient units. The second edition of the DSM (DSM-II) was published in 1968, with its first distinct section for disorders of childhood and adolescence, and an overarching focus on psychodynamics. In 1974, the decision was made to publish a new edition of the DSM that would establish a multiaxial assessment system (separating “biological” mental health problems from personality disorders, medical illnesses, and psychosocial stressors) and research-oriented diagnostic criteria that would attempt to facilitate reliable diagnoses based on common clusters of symptoms. Field trials sponsored by the National Institute of Mental Health began in 1977 to establish the reliability of the new diagnoses.
The year 1977 saw the first Apple computer, the New York City blackout, the release of the first “Star Wars” movie, and also the start of a momentous decade in general and child psychiatry. The third edition of the DSM (DSM-III) was published in 1980, the beginning of a revolution in psychiatric diagnosis and treatments. It created reliable, reproducible diagnostic constructs to serve as the basis for studies on epidemiology and treatment. Implications of causality were replaced by description; for example, hyperkinetic reaction of childhood was redefined and labeled attention-deficit disorder. Recognizing the importance of research and training in this rapidly changing field, W.T. Grant Foundation funded 11 fellowship programs in 1977, and the Society for Developmental and Behavioral Pediatrics was founded in 1982 by the leaders of those programs.
In 1983, The AACAP published “Child Psychiatry: A Plan for the Coming Decades.” It was the result of 5 years’ work by 100 child psychiatrists, general psychiatrists, pediatricians, epidemiologists, nurses, leaders of the NIMH, and various child advocates. This report laid out a challenge for child psychiatry to develop research strategies that would allow evidence-based understanding and treatment of the mental illnesses of children. The established focus on individual experience and anecdotal data, particularly about social and psychodynamic influences, would shift towards a more scientific approach to diagnosis and treatment. This decade started an explosion in epidemiologic research, medication trials, and controlled studies of nonbiological treatments in child psychiatry. At the same time, the political landscape changed, and an ascendant conservatism began the process of closing publicly funded residential treatment centers that had offered care to the more chronically mentally ill and children with profound developmental disorders. This would accelerate the shift towards outpatient psychiatric care of children. Ironically, as research would accelerate in child psychiatry, access to effective treatments would become more difficult.
The decade from 1987 to 1997 was a period of dramatic growth in medication use in child psychiatry. Prozac was approved by the Food and Drug Administration for use in the United States in 1988 and soon followed by other selective serotonin reuptake inhibitors (Zoloft in 1991 and Paxil in 1992). The journal of the AACAP began to publish more randomized controlled trials of medication treatments in children with DSM-codified diagnoses, and clinicians became more comfortable using stimulants, antidepressants, and even antipsychotic medications in the outpatient setting. This trend was enhanced by the emergence of managed care and the denial of coverage for alleged “nonbiological” diagnoses and for many psychiatric treatments. Loss of reimbursement led to a significant decline in resources, particularly inpatient child psychiatry beds and specialized clinics. This, in turn, contributed to the growing emphasis on medication treatments for children’s mental health problems. For-profit managed care companies underbid each other to provide mental health coverage and incentivized medication visits. Of note, the medical budgets, not the mental health carve outs, were billed for the medication prescribed.
The Americans with Disabilities Act was passed in 1990, increasing the funding for school-based mental health resources for children, and in 1996, Congress passed the Mental Health Parity Act, the first of several legislative attempts to ensure parity between insurance coverage for medical and psychiatric illnesses – legislation that to this day has not achieved parity of access to care. As pediatricians took on more of mental health care, a multidisciplinary team created a primary care version of DSM IV, the DSM-IV-PC, in 1995, to assist with defining levels of symptoms less than disorder to facilitate earlier intervention. A formal subspecialty of developmental-behavioral pediatrics was established in 1999 to educate leaders. Pediatric residents have had required training in developmental-behavioral pediatrics since 2008.
The year 1997 saw the first nationwide survey of parents about attention-deficit/hyperactivity disorder, kicking off what could be called the decade of ADHD, in which prevalence rates steadily climbed, from 5.7% in 1997 to 9.5% in 2007. The prevalence of stimulant treatment in children skyrocketed in this period. According to the NIMH, stimulants were prescribed to 4.2% of 6- to 12-year-olds in 1996, and that number grew to 5.1% in 2008. For 13- to 18-year-olds, the rate more than doubled during this time, from 2.3% in 1996 to 4.9% in 2008. The prevalence of autism also grew dramatically during this time, from 1.9 per 1,000 in 1997-1999 to 7.4 per 1,000 in 2006-2008, probably based on an evolving understanding of the disorder and this diagnosis providing special access to resources in schools.
Research during this decade became increasingly focused on imaging studies of children (and adults), as leaders in the field were trying to move from symptom clusters to anatomic and physiologic correlates of psychiatric illness. The great increase in medication use in children hit a speed bump in October 2004, when the Food and Drug Administration issued a controversial public warning about an increased risk of suicidal thoughts or behaviors in youth being treated with SSRI antidepressants. As access to child psychiatric treatment had become more difficult over the preceding decades, pediatricians had assumed much of the medication treatment of common psychiatric problems. The FDA’s black box warning complicated pediatricians’ efforts to fill this void.
The last decade has been the decade of genetics and efforts to improve access to care. It started in 2007 with the FDA expanding its SSRI warning to acknowledge that depression itself increased the risk for suicide, in an effort to not discourage needed depression treatment in young people. But studies demonstrated that the rates of diagnosing and treating depression dropped dramatically in the years following the warning: Diagnoses of depression declined by as much as 42% in children, and the rate of antidepressant treatment in adolescents dropped by as much as 32% in the 2 years following the warning (N Engl J Med. 2014 Oct 30;371(18):1666-8). There was no compensatory increase in utilization of other kinds of treatments. While suicide rates in young people had been stubbornly steady from the mid-1970’s to the mid-1990’s, they began to decline in 1996, according to the Centers for Disease Control and Prevention. But that trend was broken in 2004, with a jump in attempted and completed suicides in young people. The rate stabilized later in the decade, but has never returned to the lows that were being achieved prior to the warning.
This decade was marked by the passage of the Affordable Care Act, including – again – an unfulfilled mandate for mental health parity for any insurance plans in the marketplace. Although diagnosis is still symptom based, the effort to define psychiatric disorders based on brain anatomy, neurotransmitters, and genomics continues to intensify. There is growing evidence that psychiatric disorders are not nature or nurture, but nature and nurture. Epigenetic findings show that environment impacts gene expression and brain functioning. These findings promise to deepen our understanding of the critical role of early experiences (consider Adverse Childhood Experiences [ACE] scores) and the promise of protective relationships, in schools and parenting.
And what will come next? We believe that silos – medical, psychiatric, parenting, school, environment – will be bridged to understand the many factors that impact behavior and treatment, but the need to advocate for policies that support funding for the education and mental health care of children and the training of professionals to provide that care is never ending. As our knowledge of the genome marches forward, we may discover effective strategies for preventing the emergence of mental illness in children or create individualized treatments. We may learn more about the role of nutrition and the microbiome in health and disease, about autoimmunity and mental illness. Our focus may return to parents, not as culprits, but as the mediators of health from the prenatal period on. Technology may enable us to improve access to effective treatments, with teens monitoring their sleep and mood, and accessing therapy on their smart phones. And our understanding of development and vulnerability may help us stem the rise in autism or collaborate with educators so that education could better put every child on their healthiest possible path. We look forward to experiencing it – and writing about it – with you!
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. They said they had no relevant financial disclosures. Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email them at pdnews@frontlinemedcom.com.
The 50th anniversary of Pediatric News prompts us to look back on the past 50 years in child psychiatry and developmental-behavioral pediatrics, and reflect on the evolution of the field. This includes the approach to diagnosis, the thinking about development and family, and the approach and access to treatment during this dynamic period.
While some historians identify the establishment of the first juvenile court in Chicago in 1899 and the work to help judges evaluate juvenile delinquency as the origin of child psychiatry in the United States, it was not until after World War II that the field really began to take root here, largely based on psychiatrists fleeing Europe and the seminal work of Anna Freud. Some of the earliest connections between pediatrics and child psychiatry were based on the work in England of Donald W. Winnicott, a practicing pediatrician and child psychiatrist, Albert J. Solnit, MD, at the Yale Child Study Center, and psychologically informed work of pediatrician Benjamin M. Spock, MD.
The first Diagnostic and Statistical Manual (DSM) was published in 1952, based on a codification of mental disorders established by the Navy during WWII. The American Academy of Child & Adolescent Psychiatry was established in 1953, the same year that the first “tranquilizer,” chlorpromazine (Thorazine) was introduced (in France), marking the start of a revolution in psychiatric care. In 1959, the first candidates sat for a licensing examination in child psychiatry. The Section on Developmental and Behavioral Pediatrics was established as part of the American Academy of Pediatrics in 1960 to support training in this area. The AACAP established a journal in 1961. Child guidance clinics started affiliating with hospitals and universities in the 1960’s, after the Community Mental Health Act of 1963. Then, in 1965, Julius B. Richmond, MD, (a pediatrician) and Uri Bronfenbrenner, PhD, (a developmental psychologist), recognizing the importance of ecological systems to child development, were involved in the creation of Head Start, and the first Joint Commission on Mental Health for Children was established by federal legislation in 1965. The field was truly coalescing into a distinct discipline of medicine, one that bridged pediatrics, psychiatry, and neurology with nonmedical disciplines such as justice and education.
The decade between 1967 and 1977 was a period of transition from the focus on psychoanalytic concepts typical of the first half of the century to a more systematic approach to diagnosis. Children in psychiatric treatment had commonly been seen for extended individual treatments, and those with more disruptive disorders often were hospitalized for long periods. Psychoanalysis focused on the unconscious (theoretical drives and conflicts) to guide treatment. Treatment often focused on the role (causal) of parents, and family treatment was common, even on inpatient units. The second edition of the DSM (DSM-II) was published in 1968, with its first distinct section for disorders of childhood and adolescence, and an overarching focus on psychodynamics. In 1974, the decision was made to publish a new edition of the DSM that would establish a multiaxial assessment system (separating “biological” mental health problems from personality disorders, medical illnesses, and psychosocial stressors) and research-oriented diagnostic criteria that would attempt to facilitate reliable diagnoses based on common clusters of symptoms. Field trials sponsored by the National Institute of Mental Health began in 1977 to establish the reliability of the new diagnoses.
The year 1977 saw the first Apple computer, the New York City blackout, the release of the first “Star Wars” movie, and also the start of a momentous decade in general and child psychiatry. The third edition of the DSM (DSM-III) was published in 1980, the beginning of a revolution in psychiatric diagnosis and treatments. It created reliable, reproducible diagnostic constructs to serve as the basis for studies on epidemiology and treatment. Implications of causality were replaced by description; for example, hyperkinetic reaction of childhood was redefined and labeled attention-deficit disorder. Recognizing the importance of research and training in this rapidly changing field, W.T. Grant Foundation funded 11 fellowship programs in 1977, and the Society for Developmental and Behavioral Pediatrics was founded in 1982 by the leaders of those programs.
In 1983, The AACAP published “Child Psychiatry: A Plan for the Coming Decades.” It was the result of 5 years’ work by 100 child psychiatrists, general psychiatrists, pediatricians, epidemiologists, nurses, leaders of the NIMH, and various child advocates. This report laid out a challenge for child psychiatry to develop research strategies that would allow evidence-based understanding and treatment of the mental illnesses of children. The established focus on individual experience and anecdotal data, particularly about social and psychodynamic influences, would shift towards a more scientific approach to diagnosis and treatment. This decade started an explosion in epidemiologic research, medication trials, and controlled studies of nonbiological treatments in child psychiatry. At the same time, the political landscape changed, and an ascendant conservatism began the process of closing publicly funded residential treatment centers that had offered care to the more chronically mentally ill and children with profound developmental disorders. This would accelerate the shift towards outpatient psychiatric care of children. Ironically, as research would accelerate in child psychiatry, access to effective treatments would become more difficult.
The decade from 1987 to 1997 was a period of dramatic growth in medication use in child psychiatry. Prozac was approved by the Food and Drug Administration for use in the United States in 1988 and soon followed by other selective serotonin reuptake inhibitors (Zoloft in 1991 and Paxil in 1992). The journal of the AACAP began to publish more randomized controlled trials of medication treatments in children with DSM-codified diagnoses, and clinicians became more comfortable using stimulants, antidepressants, and even antipsychotic medications in the outpatient setting. This trend was enhanced by the emergence of managed care and the denial of coverage for alleged “nonbiological” diagnoses and for many psychiatric treatments. Loss of reimbursement led to a significant decline in resources, particularly inpatient child psychiatry beds and specialized clinics. This, in turn, contributed to the growing emphasis on medication treatments for children’s mental health problems. For-profit managed care companies underbid each other to provide mental health coverage and incentivized medication visits. Of note, the medical budgets, not the mental health carve outs, were billed for the medication prescribed.
The Americans with Disabilities Act was passed in 1990, increasing the funding for school-based mental health resources for children, and in 1996, Congress passed the Mental Health Parity Act, the first of several legislative attempts to ensure parity between insurance coverage for medical and psychiatric illnesses – legislation that to this day has not achieved parity of access to care. As pediatricians took on more of mental health care, a multidisciplinary team created a primary care version of DSM IV, the DSM-IV-PC, in 1995, to assist with defining levels of symptoms less than disorder to facilitate earlier intervention. A formal subspecialty of developmental-behavioral pediatrics was established in 1999 to educate leaders. Pediatric residents have had required training in developmental-behavioral pediatrics since 2008.
The year 1997 saw the first nationwide survey of parents about attention-deficit/hyperactivity disorder, kicking off what could be called the decade of ADHD, in which prevalence rates steadily climbed, from 5.7% in 1997 to 9.5% in 2007. The prevalence of stimulant treatment in children skyrocketed in this period. According to the NIMH, stimulants were prescribed to 4.2% of 6- to 12-year-olds in 1996, and that number grew to 5.1% in 2008. For 13- to 18-year-olds, the rate more than doubled during this time, from 2.3% in 1996 to 4.9% in 2008. The prevalence of autism also grew dramatically during this time, from 1.9 per 1,000 in 1997-1999 to 7.4 per 1,000 in 2006-2008, probably based on an evolving understanding of the disorder and this diagnosis providing special access to resources in schools.
Research during this decade became increasingly focused on imaging studies of children (and adults), as leaders in the field were trying to move from symptom clusters to anatomic and physiologic correlates of psychiatric illness. The great increase in medication use in children hit a speed bump in October 2004, when the Food and Drug Administration issued a controversial public warning about an increased risk of suicidal thoughts or behaviors in youth being treated with SSRI antidepressants. As access to child psychiatric treatment had become more difficult over the preceding decades, pediatricians had assumed much of the medication treatment of common psychiatric problems. The FDA’s black box warning complicated pediatricians’ efforts to fill this void.
The last decade has been the decade of genetics and efforts to improve access to care. It started in 2007 with the FDA expanding its SSRI warning to acknowledge that depression itself increased the risk for suicide, in an effort to not discourage needed depression treatment in young people. But studies demonstrated that the rates of diagnosing and treating depression dropped dramatically in the years following the warning: Diagnoses of depression declined by as much as 42% in children, and the rate of antidepressant treatment in adolescents dropped by as much as 32% in the 2 years following the warning (N Engl J Med. 2014 Oct 30;371(18):1666-8). There was no compensatory increase in utilization of other kinds of treatments. While suicide rates in young people had been stubbornly steady from the mid-1970’s to the mid-1990’s, they began to decline in 1996, according to the Centers for Disease Control and Prevention. But that trend was broken in 2004, with a jump in attempted and completed suicides in young people. The rate stabilized later in the decade, but has never returned to the lows that were being achieved prior to the warning.
This decade was marked by the passage of the Affordable Care Act, including – again – an unfulfilled mandate for mental health parity for any insurance plans in the marketplace. Although diagnosis is still symptom based, the effort to define psychiatric disorders based on brain anatomy, neurotransmitters, and genomics continues to intensify. There is growing evidence that psychiatric disorders are not nature or nurture, but nature and nurture. Epigenetic findings show that environment impacts gene expression and brain functioning. These findings promise to deepen our understanding of the critical role of early experiences (consider Adverse Childhood Experiences [ACE] scores) and the promise of protective relationships, in schools and parenting.
And what will come next? We believe that silos – medical, psychiatric, parenting, school, environment – will be bridged to understand the many factors that impact behavior and treatment, but the need to advocate for policies that support funding for the education and mental health care of children and the training of professionals to provide that care is never ending. As our knowledge of the genome marches forward, we may discover effective strategies for preventing the emergence of mental illness in children or create individualized treatments. We may learn more about the role of nutrition and the microbiome in health and disease, about autoimmunity and mental illness. Our focus may return to parents, not as culprits, but as the mediators of health from the prenatal period on. Technology may enable us to improve access to effective treatments, with teens monitoring their sleep and mood, and accessing therapy on their smart phones. And our understanding of development and vulnerability may help us stem the rise in autism or collaborate with educators so that education could better put every child on their healthiest possible path. We look forward to experiencing it – and writing about it – with you!
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. They said they had no relevant financial disclosures. Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email them at pdnews@frontlinemedcom.com.
The 50th anniversary of Pediatric News prompts us to look back on the past 50 years in child psychiatry and developmental-behavioral pediatrics, and reflect on the evolution of the field. This includes the approach to diagnosis, the thinking about development and family, and the approach and access to treatment during this dynamic period.
While some historians identify the establishment of the first juvenile court in Chicago in 1899 and the work to help judges evaluate juvenile delinquency as the origin of child psychiatry in the United States, it was not until after World War II that the field really began to take root here, largely based on psychiatrists fleeing Europe and the seminal work of Anna Freud. Some of the earliest connections between pediatrics and child psychiatry were based on the work in England of Donald W. Winnicott, a practicing pediatrician and child psychiatrist, Albert J. Solnit, MD, at the Yale Child Study Center, and psychologically informed work of pediatrician Benjamin M. Spock, MD.
The first Diagnostic and Statistical Manual (DSM) was published in 1952, based on a codification of mental disorders established by the Navy during WWII. The American Academy of Child & Adolescent Psychiatry was established in 1953, the same year that the first “tranquilizer,” chlorpromazine (Thorazine) was introduced (in France), marking the start of a revolution in psychiatric care. In 1959, the first candidates sat for a licensing examination in child psychiatry. The Section on Developmental and Behavioral Pediatrics was established as part of the American Academy of Pediatrics in 1960 to support training in this area. The AACAP established a journal in 1961. Child guidance clinics started affiliating with hospitals and universities in the 1960’s, after the Community Mental Health Act of 1963. Then, in 1965, Julius B. Richmond, MD, (a pediatrician) and Uri Bronfenbrenner, PhD, (a developmental psychologist), recognizing the importance of ecological systems to child development, were involved in the creation of Head Start, and the first Joint Commission on Mental Health for Children was established by federal legislation in 1965. The field was truly coalescing into a distinct discipline of medicine, one that bridged pediatrics, psychiatry, and neurology with nonmedical disciplines such as justice and education.
The decade between 1967 and 1977 was a period of transition from the focus on psychoanalytic concepts typical of the first half of the century to a more systematic approach to diagnosis. Children in psychiatric treatment had commonly been seen for extended individual treatments, and those with more disruptive disorders often were hospitalized for long periods. Psychoanalysis focused on the unconscious (theoretical drives and conflicts) to guide treatment. Treatment often focused on the role (causal) of parents, and family treatment was common, even on inpatient units. The second edition of the DSM (DSM-II) was published in 1968, with its first distinct section for disorders of childhood and adolescence, and an overarching focus on psychodynamics. In 1974, the decision was made to publish a new edition of the DSM that would establish a multiaxial assessment system (separating “biological” mental health problems from personality disorders, medical illnesses, and psychosocial stressors) and research-oriented diagnostic criteria that would attempt to facilitate reliable diagnoses based on common clusters of symptoms. Field trials sponsored by the National Institute of Mental Health began in 1977 to establish the reliability of the new diagnoses.
The year 1977 saw the first Apple computer, the New York City blackout, the release of the first “Star Wars” movie, and also the start of a momentous decade in general and child psychiatry. The third edition of the DSM (DSM-III) was published in 1980, the beginning of a revolution in psychiatric diagnosis and treatments. It created reliable, reproducible diagnostic constructs to serve as the basis for studies on epidemiology and treatment. Implications of causality were replaced by description; for example, hyperkinetic reaction of childhood was redefined and labeled attention-deficit disorder. Recognizing the importance of research and training in this rapidly changing field, W.T. Grant Foundation funded 11 fellowship programs in 1977, and the Society for Developmental and Behavioral Pediatrics was founded in 1982 by the leaders of those programs.
In 1983, The AACAP published “Child Psychiatry: A Plan for the Coming Decades.” It was the result of 5 years’ work by 100 child psychiatrists, general psychiatrists, pediatricians, epidemiologists, nurses, leaders of the NIMH, and various child advocates. This report laid out a challenge for child psychiatry to develop research strategies that would allow evidence-based understanding and treatment of the mental illnesses of children. The established focus on individual experience and anecdotal data, particularly about social and psychodynamic influences, would shift towards a more scientific approach to diagnosis and treatment. This decade started an explosion in epidemiologic research, medication trials, and controlled studies of nonbiological treatments in child psychiatry. At the same time, the political landscape changed, and an ascendant conservatism began the process of closing publicly funded residential treatment centers that had offered care to the more chronically mentally ill and children with profound developmental disorders. This would accelerate the shift towards outpatient psychiatric care of children. Ironically, as research would accelerate in child psychiatry, access to effective treatments would become more difficult.
The decade from 1987 to 1997 was a period of dramatic growth in medication use in child psychiatry. Prozac was approved by the Food and Drug Administration for use in the United States in 1988 and soon followed by other selective serotonin reuptake inhibitors (Zoloft in 1991 and Paxil in 1992). The journal of the AACAP began to publish more randomized controlled trials of medication treatments in children with DSM-codified diagnoses, and clinicians became more comfortable using stimulants, antidepressants, and even antipsychotic medications in the outpatient setting. This trend was enhanced by the emergence of managed care and the denial of coverage for alleged “nonbiological” diagnoses and for many psychiatric treatments. Loss of reimbursement led to a significant decline in resources, particularly inpatient child psychiatry beds and specialized clinics. This, in turn, contributed to the growing emphasis on medication treatments for children’s mental health problems. For-profit managed care companies underbid each other to provide mental health coverage and incentivized medication visits. Of note, the medical budgets, not the mental health carve outs, were billed for the medication prescribed.
The Americans with Disabilities Act was passed in 1990, increasing the funding for school-based mental health resources for children, and in 1996, Congress passed the Mental Health Parity Act, the first of several legislative attempts to ensure parity between insurance coverage for medical and psychiatric illnesses – legislation that to this day has not achieved parity of access to care. As pediatricians took on more of mental health care, a multidisciplinary team created a primary care version of DSM IV, the DSM-IV-PC, in 1995, to assist with defining levels of symptoms less than disorder to facilitate earlier intervention. A formal subspecialty of developmental-behavioral pediatrics was established in 1999 to educate leaders. Pediatric residents have had required training in developmental-behavioral pediatrics since 2008.
The year 1997 saw the first nationwide survey of parents about attention-deficit/hyperactivity disorder, kicking off what could be called the decade of ADHD, in which prevalence rates steadily climbed, from 5.7% in 1997 to 9.5% in 2007. The prevalence of stimulant treatment in children skyrocketed in this period. According to the NIMH, stimulants were prescribed to 4.2% of 6- to 12-year-olds in 1996, and that number grew to 5.1% in 2008. For 13- to 18-year-olds, the rate more than doubled during this time, from 2.3% in 1996 to 4.9% in 2008. The prevalence of autism also grew dramatically during this time, from 1.9 per 1,000 in 1997-1999 to 7.4 per 1,000 in 2006-2008, probably based on an evolving understanding of the disorder and this diagnosis providing special access to resources in schools.
Research during this decade became increasingly focused on imaging studies of children (and adults), as leaders in the field were trying to move from symptom clusters to anatomic and physiologic correlates of psychiatric illness. The great increase in medication use in children hit a speed bump in October 2004, when the Food and Drug Administration issued a controversial public warning about an increased risk of suicidal thoughts or behaviors in youth being treated with SSRI antidepressants. As access to child psychiatric treatment had become more difficult over the preceding decades, pediatricians had assumed much of the medication treatment of common psychiatric problems. The FDA’s black box warning complicated pediatricians’ efforts to fill this void.
The last decade has been the decade of genetics and efforts to improve access to care. It started in 2007 with the FDA expanding its SSRI warning to acknowledge that depression itself increased the risk for suicide, in an effort to not discourage needed depression treatment in young people. But studies demonstrated that the rates of diagnosing and treating depression dropped dramatically in the years following the warning: Diagnoses of depression declined by as much as 42% in children, and the rate of antidepressant treatment in adolescents dropped by as much as 32% in the 2 years following the warning (N Engl J Med. 2014 Oct 30;371(18):1666-8). There was no compensatory increase in utilization of other kinds of treatments. While suicide rates in young people had been stubbornly steady from the mid-1970’s to the mid-1990’s, they began to decline in 1996, according to the Centers for Disease Control and Prevention. But that trend was broken in 2004, with a jump in attempted and completed suicides in young people. The rate stabilized later in the decade, but has never returned to the lows that were being achieved prior to the warning.
This decade was marked by the passage of the Affordable Care Act, including – again – an unfulfilled mandate for mental health parity for any insurance plans in the marketplace. Although diagnosis is still symptom based, the effort to define psychiatric disorders based on brain anatomy, neurotransmitters, and genomics continues to intensify. There is growing evidence that psychiatric disorders are not nature or nurture, but nature and nurture. Epigenetic findings show that environment impacts gene expression and brain functioning. These findings promise to deepen our understanding of the critical role of early experiences (consider Adverse Childhood Experiences [ACE] scores) and the promise of protective relationships, in schools and parenting.
And what will come next? We believe that silos – medical, psychiatric, parenting, school, environment – will be bridged to understand the many factors that impact behavior and treatment, but the need to advocate for policies that support funding for the education and mental health care of children and the training of professionals to provide that care is never ending. As our knowledge of the genome marches forward, we may discover effective strategies for preventing the emergence of mental illness in children or create individualized treatments. We may learn more about the role of nutrition and the microbiome in health and disease, about autoimmunity and mental illness. Our focus may return to parents, not as culprits, but as the mediators of health from the prenatal period on. Technology may enable us to improve access to effective treatments, with teens monitoring their sleep and mood, and accessing therapy on their smart phones. And our understanding of development and vulnerability may help us stem the rise in autism or collaborate with educators so that education could better put every child on their healthiest possible path. We look forward to experiencing it – and writing about it – with you!
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. They said they had no relevant financial disclosures. Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email them at pdnews@frontlinemedcom.com.
50 years in pediatrics: ‘You have to get involved’
A few years before the launch of Pediatric News in 1967, Dr. Henry Kempe and his colleagues at the University of Colorado, Denver, published a groundbreaking report on child abuse, “The Battered Child Syndrome,” in JAMA.
It had a major impact on Calvin C.J. Sia, MD, a now-retired pediatrician in Hawaii, not only because it was pioneering work and one of the milestones of 20th century pediatrics, but also because Dr. Kempe was a close friend and mentor of Dr. Sia, going back to when Dr. Sia was a resident in the 1950s.
Dr. Kempe “alerted me to the battered child syndrome and taught me the importance of looking at the whole child within the context of the family, and he repeatedly reminded me of the importance of preventive care. He taught me how to make preventive change, with the emphasis on the first 3 years” of life, Dr. Sia said in an interview from his home in Honolulu.
To celebrate the 50th anniversary of Pediatric News, it seemed appropriate to turn to Dr. Sia. His practice, launched in 1958, not only spanned our 50 years, but also illustrated one of the major themes in pediatrics over the past half-century. With the old scourges of infectious disease, malnutrition, and infant mortality largely brought under control, pediatrics turned to the broader struggles of childhood, including learning, poverty, and abusive parenting.
Dr. Sia has been president of the Hawaii Medical Association; president of the Hawaii chapter of the American Academy of Pediatrics; chief of staff at the Kauikeolani Children’s Hospital, Honolulu (now the Kapi‘olani Medical Center for Women and Children); chair of the American Medical Association Pediatric Delegation; and founder of the AMA’s Section Council on Pediatrics.
Positions like these eventually led him to contacts with legislators willing to listen and fund child abuse prevention, immunization programs, and other initiatives to help children. It often meant lobbying politicians for money.
“It doesn’t occur overnight; it takes chance and dedication,” said Dr. Sia, whose name, as one of its earliest champions, is now nearly synonymous with the concept of the medical home – an ideal of cradling children in a physician, family, and social services safety net of coordinated care.
Dr. Sia’s career spanned all of the developments that Pediatric News has covered over its 50 years, including the increasing recognition of autism, the earlier survival of premature infants, and phenylketonuria and other screenings at birth. He remembers all of them, and took action on many at the state and federal level.
Taking a step took courage, even when he wasn’t quite sure what to do. “I recognized autism back in the 60s. Children looked normal, were born normal, but then had trouble. I didn’t know what to do with them. That’s how I got involved with learning disabilities. I didn’t know anything, but I got involved,” he said.
With the advice of Robert Cooke, MD, another mentor and an eventual founder of the Head Start program, Dr. Sia cofounded Honolulu’s Variety School for Learning Disabilities in 1967. It’s still in operation; Don Ho and other local “variety hour” entertainers helped with early fundraising.
Dr. Sia also helped launch Healthy Start, one of the nation’s first home visit programs for at-risk kids, and an amendment to the federal Education of the Handicapped Act to extend aid to children with family and developmental challenges.
He convinced Sen. Daniel Inouye, another personal friend, to introduce the Emergency Medical Services for Children Act in the 1980s, which funded states to develop emergency medical services for children. “It was really important because kids need special instruments, IVs, and medications. I had to lobby. It was under Reaganomics,” Dr. Sia said.
At 89 years of age and recovering from a recent heart attack and open heart bypass, he is still trying to help children. Dr. Sia, who was born in Beijing, has been promoting the medical home concept in Asia. Meanwhile, he said he is worried about the fragmentation of health care in the United States, and the likely cutback in federal and state spending on kids.
Even so, “I believe in the future. I see in the generation coming up much more awareness of the whole child. I think they are going to do a much better job than I did,” but they need to learn “how to work the system.” Young physicians also must be mentored to believe in themselves, and take up the torch, he said.
A few years before the launch of Pediatric News in 1967, Dr. Henry Kempe and his colleagues at the University of Colorado, Denver, published a groundbreaking report on child abuse, “The Battered Child Syndrome,” in JAMA.
It had a major impact on Calvin C.J. Sia, MD, a now-retired pediatrician in Hawaii, not only because it was pioneering work and one of the milestones of 20th century pediatrics, but also because Dr. Kempe was a close friend and mentor of Dr. Sia, going back to when Dr. Sia was a resident in the 1950s.
Dr. Kempe “alerted me to the battered child syndrome and taught me the importance of looking at the whole child within the context of the family, and he repeatedly reminded me of the importance of preventive care. He taught me how to make preventive change, with the emphasis on the first 3 years” of life, Dr. Sia said in an interview from his home in Honolulu.
To celebrate the 50th anniversary of Pediatric News, it seemed appropriate to turn to Dr. Sia. His practice, launched in 1958, not only spanned our 50 years, but also illustrated one of the major themes in pediatrics over the past half-century. With the old scourges of infectious disease, malnutrition, and infant mortality largely brought under control, pediatrics turned to the broader struggles of childhood, including learning, poverty, and abusive parenting.
Dr. Sia has been president of the Hawaii Medical Association; president of the Hawaii chapter of the American Academy of Pediatrics; chief of staff at the Kauikeolani Children’s Hospital, Honolulu (now the Kapi‘olani Medical Center for Women and Children); chair of the American Medical Association Pediatric Delegation; and founder of the AMA’s Section Council on Pediatrics.
Positions like these eventually led him to contacts with legislators willing to listen and fund child abuse prevention, immunization programs, and other initiatives to help children. It often meant lobbying politicians for money.
“It doesn’t occur overnight; it takes chance and dedication,” said Dr. Sia, whose name, as one of its earliest champions, is now nearly synonymous with the concept of the medical home – an ideal of cradling children in a physician, family, and social services safety net of coordinated care.
Dr. Sia’s career spanned all of the developments that Pediatric News has covered over its 50 years, including the increasing recognition of autism, the earlier survival of premature infants, and phenylketonuria and other screenings at birth. He remembers all of them, and took action on many at the state and federal level.
Taking a step took courage, even when he wasn’t quite sure what to do. “I recognized autism back in the 60s. Children looked normal, were born normal, but then had trouble. I didn’t know what to do with them. That’s how I got involved with learning disabilities. I didn’t know anything, but I got involved,” he said.
With the advice of Robert Cooke, MD, another mentor and an eventual founder of the Head Start program, Dr. Sia cofounded Honolulu’s Variety School for Learning Disabilities in 1967. It’s still in operation; Don Ho and other local “variety hour” entertainers helped with early fundraising.
Dr. Sia also helped launch Healthy Start, one of the nation’s first home visit programs for at-risk kids, and an amendment to the federal Education of the Handicapped Act to extend aid to children with family and developmental challenges.
He convinced Sen. Daniel Inouye, another personal friend, to introduce the Emergency Medical Services for Children Act in the 1980s, which funded states to develop emergency medical services for children. “It was really important because kids need special instruments, IVs, and medications. I had to lobby. It was under Reaganomics,” Dr. Sia said.
At 89 years of age and recovering from a recent heart attack and open heart bypass, he is still trying to help children. Dr. Sia, who was born in Beijing, has been promoting the medical home concept in Asia. Meanwhile, he said he is worried about the fragmentation of health care in the United States, and the likely cutback in federal and state spending on kids.
Even so, “I believe in the future. I see in the generation coming up much more awareness of the whole child. I think they are going to do a much better job than I did,” but they need to learn “how to work the system.” Young physicians also must be mentored to believe in themselves, and take up the torch, he said.
A few years before the launch of Pediatric News in 1967, Dr. Henry Kempe and his colleagues at the University of Colorado, Denver, published a groundbreaking report on child abuse, “The Battered Child Syndrome,” in JAMA.
It had a major impact on Calvin C.J. Sia, MD, a now-retired pediatrician in Hawaii, not only because it was pioneering work and one of the milestones of 20th century pediatrics, but also because Dr. Kempe was a close friend and mentor of Dr. Sia, going back to when Dr. Sia was a resident in the 1950s.
Dr. Kempe “alerted me to the battered child syndrome and taught me the importance of looking at the whole child within the context of the family, and he repeatedly reminded me of the importance of preventive care. He taught me how to make preventive change, with the emphasis on the first 3 years” of life, Dr. Sia said in an interview from his home in Honolulu.
To celebrate the 50th anniversary of Pediatric News, it seemed appropriate to turn to Dr. Sia. His practice, launched in 1958, not only spanned our 50 years, but also illustrated one of the major themes in pediatrics over the past half-century. With the old scourges of infectious disease, malnutrition, and infant mortality largely brought under control, pediatrics turned to the broader struggles of childhood, including learning, poverty, and abusive parenting.
Dr. Sia has been president of the Hawaii Medical Association; president of the Hawaii chapter of the American Academy of Pediatrics; chief of staff at the Kauikeolani Children’s Hospital, Honolulu (now the Kapi‘olani Medical Center for Women and Children); chair of the American Medical Association Pediatric Delegation; and founder of the AMA’s Section Council on Pediatrics.
Positions like these eventually led him to contacts with legislators willing to listen and fund child abuse prevention, immunization programs, and other initiatives to help children. It often meant lobbying politicians for money.
“It doesn’t occur overnight; it takes chance and dedication,” said Dr. Sia, whose name, as one of its earliest champions, is now nearly synonymous with the concept of the medical home – an ideal of cradling children in a physician, family, and social services safety net of coordinated care.
Dr. Sia’s career spanned all of the developments that Pediatric News has covered over its 50 years, including the increasing recognition of autism, the earlier survival of premature infants, and phenylketonuria and other screenings at birth. He remembers all of them, and took action on many at the state and federal level.
Taking a step took courage, even when he wasn’t quite sure what to do. “I recognized autism back in the 60s. Children looked normal, were born normal, but then had trouble. I didn’t know what to do with them. That’s how I got involved with learning disabilities. I didn’t know anything, but I got involved,” he said.
With the advice of Robert Cooke, MD, another mentor and an eventual founder of the Head Start program, Dr. Sia cofounded Honolulu’s Variety School for Learning Disabilities in 1967. It’s still in operation; Don Ho and other local “variety hour” entertainers helped with early fundraising.
Dr. Sia also helped launch Healthy Start, one of the nation’s first home visit programs for at-risk kids, and an amendment to the federal Education of the Handicapped Act to extend aid to children with family and developmental challenges.
He convinced Sen. Daniel Inouye, another personal friend, to introduce the Emergency Medical Services for Children Act in the 1980s, which funded states to develop emergency medical services for children. “It was really important because kids need special instruments, IVs, and medications. I had to lobby. It was under Reaganomics,” Dr. Sia said.
At 89 years of age and recovering from a recent heart attack and open heart bypass, he is still trying to help children. Dr. Sia, who was born in Beijing, has been promoting the medical home concept in Asia. Meanwhile, he said he is worried about the fragmentation of health care in the United States, and the likely cutback in federal and state spending on kids.
Even so, “I believe in the future. I see in the generation coming up much more awareness of the whole child. I think they are going to do a much better job than I did,” but they need to learn “how to work the system.” Young physicians also must be mentored to believe in themselves, and take up the torch, he said.
1967 at a glance
• The Early and Periodic Screening, Diagnostic and Treatment (EPSDT) program was enacted as the child health component of Medicaid. Children under 21 years enrolled in Medicaid are entitled to EPSDT benefits, and states must cover a “broad array of preventive and treatment services.”
• By 1967, all states had laws requiring that physicians report child abuse.
• Field trials of experimental respiratory syncytial virus vaccines were performed but stalled. Currently, 65 RSV vaccines are being studied, and 13 are in phase III trials.
• The World Health Association declared a war on smallpox with a worldwide vaccination campaign. Twelve years later the disease was eradicated.
• The Public Health Service issued the second Surgeon General’s report on the health consequences of smoking.
• The first heart transplant was performed by Christian Barnard.
• The Early and Periodic Screening, Diagnostic and Treatment (EPSDT) program was enacted as the child health component of Medicaid. Children under 21 years enrolled in Medicaid are entitled to EPSDT benefits, and states must cover a “broad array of preventive and treatment services.”
• By 1967, all states had laws requiring that physicians report child abuse.
• Field trials of experimental respiratory syncytial virus vaccines were performed but stalled. Currently, 65 RSV vaccines are being studied, and 13 are in phase III trials.
• The World Health Association declared a war on smallpox with a worldwide vaccination campaign. Twelve years later the disease was eradicated.
• The Public Health Service issued the second Surgeon General’s report on the health consequences of smoking.
• The first heart transplant was performed by Christian Barnard.
• The Early and Periodic Screening, Diagnostic and Treatment (EPSDT) program was enacted as the child health component of Medicaid. Children under 21 years enrolled in Medicaid are entitled to EPSDT benefits, and states must cover a “broad array of preventive and treatment services.”
• By 1967, all states had laws requiring that physicians report child abuse.
• Field trials of experimental respiratory syncytial virus vaccines were performed but stalled. Currently, 65 RSV vaccines are being studied, and 13 are in phase III trials.
• The World Health Association declared a war on smallpox with a worldwide vaccination campaign. Twelve years later the disease was eradicated.
• The Public Health Service issued the second Surgeon General’s report on the health consequences of smoking.
• The first heart transplant was performed by Christian Barnard.
A look back at 1967
As Pediatric News celebrates 50 years of publication, we’re taking a look back at our first year: 1967.
A review of the 1967 issues of the journal Pediatrics offers a snapshot of the state of the science and some surprising similarities with pediatric medicine today.
A commentary in the November issue entitled “Pediatrics at a Crossroad” described an accelerating trend toward pediatric group practice and noted that full-time hospital employment of pediatricians was an emerging pattern of pediatric practice. The author, Richard Smith, MD, of the University of Florida, Gainesville, expressed concern about certain practices, such as the wide employment of antibiotics for uncomplicated respiratory infections and “routine use of gamma globulin in community hospital nurseries supposedly to treat sepsis or its regular injection in putatively allergic children.” He also was concerned about a quality gap in pediatric specialty education (Pediatrics. 1967 Nov;40[5]:783-7).
Articles of interest in the infectious disease area included an article demonstrating the response of infants to trivalent polio vaccine (Dec;40[6]:980-5); a new antibody test for rubella (Dec;40[5]:787-8, 789-97); and a live attenuated mumps vaccine (Dec;40[5]:798-803). And as we deal with emerging infectious diseases on a large scale, a fatal case of dengue hemorrhagic fever was reported in an American child (Dec;40[5]:804-7).
In a commentary, Starkey D. Davis, MD, and Ralph J. Wedgwood, MD, of the University of Washington, Seattle, said that the annual tuberculosis infection rate was low and falling, and that new cases were decreasing. Sufficient beds were available to isolate infectious cases, and effective chemotherapy made most cases noninfectious quickly. Isoniazid was cheap and effective, and it decreased complications of asymptomatic primary tuberculosis in children by 85%. “Pediatricians can expect to see tuberculosis in children become a medical curiosity in this country as infection rates continue to fall, if isoniazid prophylaxis is energetically used,” they predicted (Jun;39[6]:809-10).
D. Holdaway of the Royal Victoria Infirmary in Newcastle Upon Tyne, England, and associates reported on 211 children with acute bronchiolitis and 295 controls with nonrespiratory illness. Of the children with bronchiolitis, 59% had respiratory syncytial virus (RSV), compared with 1% of the controls, which confirmed the etiological significance of RSV in bronchiolitis, the researchers said. They also maintained that “oxygen is vitally important in bronchiolitis and there is little conclusive evidence that any other therapy is consistently or even occasionally useful” (Jun;39[6]:924-8).
In a commentary, Leon Eisenberg, MD, of the division of child psychiatry at the Johns Hopkins Hospital, Baltimore, called for more training in child development for pediatricians (May;39[5];645-7). Today, pediatricians are calling for more training in child psychiatry.
A report by the American Academy of Pediatrics Committee on Nutrition on obesity in childhood was prescient. They said, despite much research, that “our ignorance concerning the etiology, pathogenesis, and treatment is remarkable” (Sep;40[3]:455-67). The committee acknowledged that morbidity and mortality for diabetes and cardiovascular disease were higher in obese adults than in those of average weight, and that obese children tended to remain obese as adults. The committee also wrote that no treatments had achieved more than minor success of weight reduction. It suggested prevention of weight gain as the likely best approach, with initiation by the pediatrician in high-risk families – advice that still holds true today 50 years later.
Throughout 2017, Pediatric News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including changes in child psychiatry, pediatric dermatology, and infectious disease medicine, changes in residency training, and the transformation of the well-child visit. Look for these articles and more special features on the pages of Pediatric News and here online.
As Pediatric News celebrates 50 years of publication, we’re taking a look back at our first year: 1967.
A review of the 1967 issues of the journal Pediatrics offers a snapshot of the state of the science and some surprising similarities with pediatric medicine today.
A commentary in the November issue entitled “Pediatrics at a Crossroad” described an accelerating trend toward pediatric group practice and noted that full-time hospital employment of pediatricians was an emerging pattern of pediatric practice. The author, Richard Smith, MD, of the University of Florida, Gainesville, expressed concern about certain practices, such as the wide employment of antibiotics for uncomplicated respiratory infections and “routine use of gamma globulin in community hospital nurseries supposedly to treat sepsis or its regular injection in putatively allergic children.” He also was concerned about a quality gap in pediatric specialty education (Pediatrics. 1967 Nov;40[5]:783-7).
Articles of interest in the infectious disease area included an article demonstrating the response of infants to trivalent polio vaccine (Dec;40[6]:980-5); a new antibody test for rubella (Dec;40[5]:787-8, 789-97); and a live attenuated mumps vaccine (Dec;40[5]:798-803). And as we deal with emerging infectious diseases on a large scale, a fatal case of dengue hemorrhagic fever was reported in an American child (Dec;40[5]:804-7).
In a commentary, Starkey D. Davis, MD, and Ralph J. Wedgwood, MD, of the University of Washington, Seattle, said that the annual tuberculosis infection rate was low and falling, and that new cases were decreasing. Sufficient beds were available to isolate infectious cases, and effective chemotherapy made most cases noninfectious quickly. Isoniazid was cheap and effective, and it decreased complications of asymptomatic primary tuberculosis in children by 85%. “Pediatricians can expect to see tuberculosis in children become a medical curiosity in this country as infection rates continue to fall, if isoniazid prophylaxis is energetically used,” they predicted (Jun;39[6]:809-10).
D. Holdaway of the Royal Victoria Infirmary in Newcastle Upon Tyne, England, and associates reported on 211 children with acute bronchiolitis and 295 controls with nonrespiratory illness. Of the children with bronchiolitis, 59% had respiratory syncytial virus (RSV), compared with 1% of the controls, which confirmed the etiological significance of RSV in bronchiolitis, the researchers said. They also maintained that “oxygen is vitally important in bronchiolitis and there is little conclusive evidence that any other therapy is consistently or even occasionally useful” (Jun;39[6]:924-8).
In a commentary, Leon Eisenberg, MD, of the division of child psychiatry at the Johns Hopkins Hospital, Baltimore, called for more training in child development for pediatricians (May;39[5];645-7). Today, pediatricians are calling for more training in child psychiatry.
A report by the American Academy of Pediatrics Committee on Nutrition on obesity in childhood was prescient. They said, despite much research, that “our ignorance concerning the etiology, pathogenesis, and treatment is remarkable” (Sep;40[3]:455-67). The committee acknowledged that morbidity and mortality for diabetes and cardiovascular disease were higher in obese adults than in those of average weight, and that obese children tended to remain obese as adults. The committee also wrote that no treatments had achieved more than minor success of weight reduction. It suggested prevention of weight gain as the likely best approach, with initiation by the pediatrician in high-risk families – advice that still holds true today 50 years later.
Throughout 2017, Pediatric News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including changes in child psychiatry, pediatric dermatology, and infectious disease medicine, changes in residency training, and the transformation of the well-child visit. Look for these articles and more special features on the pages of Pediatric News and here online.
As Pediatric News celebrates 50 years of publication, we’re taking a look back at our first year: 1967.
A review of the 1967 issues of the journal Pediatrics offers a snapshot of the state of the science and some surprising similarities with pediatric medicine today.
A commentary in the November issue entitled “Pediatrics at a Crossroad” described an accelerating trend toward pediatric group practice and noted that full-time hospital employment of pediatricians was an emerging pattern of pediatric practice. The author, Richard Smith, MD, of the University of Florida, Gainesville, expressed concern about certain practices, such as the wide employment of antibiotics for uncomplicated respiratory infections and “routine use of gamma globulin in community hospital nurseries supposedly to treat sepsis or its regular injection in putatively allergic children.” He also was concerned about a quality gap in pediatric specialty education (Pediatrics. 1967 Nov;40[5]:783-7).
Articles of interest in the infectious disease area included an article demonstrating the response of infants to trivalent polio vaccine (Dec;40[6]:980-5); a new antibody test for rubella (Dec;40[5]:787-8, 789-97); and a live attenuated mumps vaccine (Dec;40[5]:798-803). And as we deal with emerging infectious diseases on a large scale, a fatal case of dengue hemorrhagic fever was reported in an American child (Dec;40[5]:804-7).
In a commentary, Starkey D. Davis, MD, and Ralph J. Wedgwood, MD, of the University of Washington, Seattle, said that the annual tuberculosis infection rate was low and falling, and that new cases were decreasing. Sufficient beds were available to isolate infectious cases, and effective chemotherapy made most cases noninfectious quickly. Isoniazid was cheap and effective, and it decreased complications of asymptomatic primary tuberculosis in children by 85%. “Pediatricians can expect to see tuberculosis in children become a medical curiosity in this country as infection rates continue to fall, if isoniazid prophylaxis is energetically used,” they predicted (Jun;39[6]:809-10).
D. Holdaway of the Royal Victoria Infirmary in Newcastle Upon Tyne, England, and associates reported on 211 children with acute bronchiolitis and 295 controls with nonrespiratory illness. Of the children with bronchiolitis, 59% had respiratory syncytial virus (RSV), compared with 1% of the controls, which confirmed the etiological significance of RSV in bronchiolitis, the researchers said. They also maintained that “oxygen is vitally important in bronchiolitis and there is little conclusive evidence that any other therapy is consistently or even occasionally useful” (Jun;39[6]:924-8).
In a commentary, Leon Eisenberg, MD, of the division of child psychiatry at the Johns Hopkins Hospital, Baltimore, called for more training in child development for pediatricians (May;39[5];645-7). Today, pediatricians are calling for more training in child psychiatry.
A report by the American Academy of Pediatrics Committee on Nutrition on obesity in childhood was prescient. They said, despite much research, that “our ignorance concerning the etiology, pathogenesis, and treatment is remarkable” (Sep;40[3]:455-67). The committee acknowledged that morbidity and mortality for diabetes and cardiovascular disease were higher in obese adults than in those of average weight, and that obese children tended to remain obese as adults. The committee also wrote that no treatments had achieved more than minor success of weight reduction. It suggested prevention of weight gain as the likely best approach, with initiation by the pediatrician in high-risk families – advice that still holds true today 50 years later.
Throughout 2017, Pediatric News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including changes in child psychiatry, pediatric dermatology, and infectious disease medicine, changes in residency training, and the transformation of the well-child visit. Look for these articles and more special features on the pages of Pediatric News and here online.