User login
Richard Pizzi is editor of The Hospitalist. He has been an editor at Frontline Medical Communications since 2015, and previously served as editor of MDedge publications Hospitalist News and ID Practitioner. He has also worked as an editor and in editorial management roles for HIMSS Media, MedTech Media, and the American Association for Clinical Chemistry. Follow him on Twitter @richpizzi
Afghanistan still struggling with poliovirus
Afghanistan experienced a “major setback” in its efforts to eradicate polio in 2014, after having made significant progress towards elimination of the disease the prior year, a new study reveals.
The number of reported polio cases in Afghanistan doubled in 2014 over 2013 figures, and the country’s routine immunization system remains weak and unable to reach recommended benchmarks in most regions, according to Dr. Chukwuma Mbaeyi of the Center for Global Health at the Centers for Disease Control and Prevention, and coauthors. Afghanistan is one of the two remaining countries (the other being Pakistan) where indigenous wild poliovirus transmission has never been interrupted.

During 2014, a total of 28 wild polio virus (WPV1) cases were reported in Afghanistan, compared with 14 cases in 2013, while nine cases were reported during January‒August 2015, the same number as during the identical period in 2014. Childhood immunization efforts have been hampered by ongoing conflict and insecurity in the region, especially in parts of southern and eastern Afghanistan, as well as one province in the western region (MMWR. 2015 Oct. 23; 64[41]:1166-70).
The report says there is an urgent need to improve on the level of coordination and oversight of polio eradication activities in the country, particularly with respect to supplementary immunization, to eliminate poliovirus transmission in Afghanistan.
“Emergency operations centers (EOCs) need to be established at the national level and in critical regions without delay to improve overall coordination and oversight of polio eradication activities,” Dr. Mbaeyi and coauthors wrote. “The recently revised National Emergency Action Plan for polio eradication needs to be fully implemented, including detailed microplanning and enhanced monitoring and supervision of [supplementary immunization activities], as well as improved cross-border coordination with Pakistan.”
The researchers say improving the quality of SIAs in Afghanistan will require better preparation through proper staff training and detailed microplanning, and ensuring adequate monitoring and supervision during the course of immunization campaigns.
Read the entire report on the CDC website.
On Twitter @richpizzi
Afghanistan experienced a “major setback” in its efforts to eradicate polio in 2014, after having made significant progress towards elimination of the disease the prior year, a new study reveals.
The number of reported polio cases in Afghanistan doubled in 2014 over 2013 figures, and the country’s routine immunization system remains weak and unable to reach recommended benchmarks in most regions, according to Dr. Chukwuma Mbaeyi of the Center for Global Health at the Centers for Disease Control and Prevention, and coauthors. Afghanistan is one of the two remaining countries (the other being Pakistan) where indigenous wild poliovirus transmission has never been interrupted.
During 2014, a total of 28 wild polio virus (WPV1) cases were reported in Afghanistan, compared with 14 cases in 2013, while nine cases were reported during January‒August 2015, the same number as during the identical period in 2014. Childhood immunization efforts have been hampered by ongoing conflict and insecurity in the region, especially in parts of southern and eastern Afghanistan, as well as one province in the western region (MMWR. 2015 Oct. 23; 64[41]:1166-70).
The report says there is an urgent need to improve on the level of coordination and oversight of polio eradication activities in the country, particularly with respect to supplementary immunization, to eliminate poliovirus transmission in Afghanistan.
“Emergency operations centers (EOCs) need to be established at the national level and in critical regions without delay to improve overall coordination and oversight of polio eradication activities,” Dr. Mbaeyi and coauthors wrote. “The recently revised National Emergency Action Plan for polio eradication needs to be fully implemented, including detailed microplanning and enhanced monitoring and supervision of [supplementary immunization activities], as well as improved cross-border coordination with Pakistan.”
The researchers say improving the quality of SIAs in Afghanistan will require better preparation through proper staff training and detailed microplanning, and ensuring adequate monitoring and supervision during the course of immunization campaigns.
Read the entire report on the CDC website.
On Twitter @richpizzi
Afghanistan experienced a “major setback” in its efforts to eradicate polio in 2014, after having made significant progress towards elimination of the disease the prior year, a new study reveals.
The number of reported polio cases in Afghanistan doubled in 2014 over 2013 figures, and the country’s routine immunization system remains weak and unable to reach recommended benchmarks in most regions, according to Dr. Chukwuma Mbaeyi of the Center for Global Health at the Centers for Disease Control and Prevention, and coauthors. Afghanistan is one of the two remaining countries (the other being Pakistan) where indigenous wild poliovirus transmission has never been interrupted.
During 2014, a total of 28 wild polio virus (WPV1) cases were reported in Afghanistan, compared with 14 cases in 2013, while nine cases were reported during January‒August 2015, the same number as during the identical period in 2014. Childhood immunization efforts have been hampered by ongoing conflict and insecurity in the region, especially in parts of southern and eastern Afghanistan, as well as one province in the western region (MMWR. 2015 Oct. 23; 64[41]:1166-70).
The report says there is an urgent need to improve on the level of coordination and oversight of polio eradication activities in the country, particularly with respect to supplementary immunization, to eliminate poliovirus transmission in Afghanistan.
“Emergency operations centers (EOCs) need to be established at the national level and in critical regions without delay to improve overall coordination and oversight of polio eradication activities,” Dr. Mbaeyi and coauthors wrote. “The recently revised National Emergency Action Plan for polio eradication needs to be fully implemented, including detailed microplanning and enhanced monitoring and supervision of [supplementary immunization activities], as well as improved cross-border coordination with Pakistan.”
The researchers say improving the quality of SIAs in Afghanistan will require better preparation through proper staff training and detailed microplanning, and ensuring adequate monitoring and supervision during the course of immunization campaigns.
Read the entire report on the CDC website.
On Twitter @richpizzi
FROM MMWR

Improved supply chain, immunization rates key to global vaccination success
The key element to achieving global vaccination coverage goals may be improving vaccine stock management, suggests a recent report by the Centers for Disease Control and Prevention.
Vaccine stock management is a critical component to ensuring vaccine access, said Dr. Saleena Subaiya of the CDC’s Global Immunization Division, and her coauthors in the Nov. 13, 2015 edition of the Morbidity and Mortality Weekly Report (MMWR. 2015 Nov 13;64[44]:1252-55). The large proportion of countries experiencing district level “stockouts” as a result of a national level stockout provides evidence that shortage of vaccines at the national level can affect the supply chain and interrupt immunization services. Dr. Subaiya said improved and timely demand forecasts to the vaccine industry are integral to help secure sufficient supplies of vaccines.
During 2014, a total of 50 (26%) of the 194 World Health Organization (WHO) countries reported experiencing a national level stockout, or shortage of supply, of at least one vaccine lasting at least 1 month. Overall 110 national stockout events were reported in 2014, with a mean of 2.2 events per country and a maximum of six events per country. Shortages involving diphtheria-tetanus-pertussis (DTP) vaccines represented 40% of the reported stockout events, followed by Bacille Calmette-Guérin vaccine for protection against tuberculosis (25%), and measles-containing vaccine representing 14% of stockout events.
At the subnational level, 88% of countries with a national level stockout experienced a district level stockout. In 38 (86%) countries with a district level stockout, the primary cause identified was a national level stockout.
In addition to adequate vaccine stock management, strengthening immunization programs and achieving global vaccination coverage goals requires “additional opportunities for immunization,” such as routine child medical visits in the second year of life, the researchers said.
In 2014, estimated DTP3 coverage (vaccination with the 3rd dose of DTP) was 86% worldwide among infants aged ≤12 months, while estimated global coverage with BCG, polio3, and MCV1 was 91%, 86%, and 85%, respectively. During 2014, a total of 129 (66%) of 194 WHO countries achieved ≥90% national DTP3 coverage. National DTP3 coverage was 80%–89% in 30 countries, 70%–79% in 20 countries, and <70% in 15 countries.
To read the complete report in MMWR, click here.
On Twitter @richpizzi
The key element to achieving global vaccination coverage goals may be improving vaccine stock management, suggests a recent report by the Centers for Disease Control and Prevention.
Vaccine stock management is a critical component to ensuring vaccine access, said Dr. Saleena Subaiya of the CDC’s Global Immunization Division, and her coauthors in the Nov. 13, 2015 edition of the Morbidity and Mortality Weekly Report (MMWR. 2015 Nov 13;64[44]:1252-55). The large proportion of countries experiencing district level “stockouts” as a result of a national level stockout provides evidence that shortage of vaccines at the national level can affect the supply chain and interrupt immunization services. Dr. Subaiya said improved and timely demand forecasts to the vaccine industry are integral to help secure sufficient supplies of vaccines.
During 2014, a total of 50 (26%) of the 194 World Health Organization (WHO) countries reported experiencing a national level stockout, or shortage of supply, of at least one vaccine lasting at least 1 month. Overall 110 national stockout events were reported in 2014, with a mean of 2.2 events per country and a maximum of six events per country. Shortages involving diphtheria-tetanus-pertussis (DTP) vaccines represented 40% of the reported stockout events, followed by Bacille Calmette-Guérin vaccine for protection against tuberculosis (25%), and measles-containing vaccine representing 14% of stockout events.
At the subnational level, 88% of countries with a national level stockout experienced a district level stockout. In 38 (86%) countries with a district level stockout, the primary cause identified was a national level stockout.
In addition to adequate vaccine stock management, strengthening immunization programs and achieving global vaccination coverage goals requires “additional opportunities for immunization,” such as routine child medical visits in the second year of life, the researchers said.
In 2014, estimated DTP3 coverage (vaccination with the 3rd dose of DTP) was 86% worldwide among infants aged ≤12 months, while estimated global coverage with BCG, polio3, and MCV1 was 91%, 86%, and 85%, respectively. During 2014, a total of 129 (66%) of 194 WHO countries achieved ≥90% national DTP3 coverage. National DTP3 coverage was 80%–89% in 30 countries, 70%–79% in 20 countries, and <70% in 15 countries.
To read the complete report in MMWR, click here.
On Twitter @richpizzi
The key element to achieving global vaccination coverage goals may be improving vaccine stock management, suggests a recent report by the Centers for Disease Control and Prevention.
Vaccine stock management is a critical component to ensuring vaccine access, said Dr. Saleena Subaiya of the CDC’s Global Immunization Division, and her coauthors in the Nov. 13, 2015 edition of the Morbidity and Mortality Weekly Report (MMWR. 2015 Nov 13;64[44]:1252-55). The large proportion of countries experiencing district level “stockouts” as a result of a national level stockout provides evidence that shortage of vaccines at the national level can affect the supply chain and interrupt immunization services. Dr. Subaiya said improved and timely demand forecasts to the vaccine industry are integral to help secure sufficient supplies of vaccines.
During 2014, a total of 50 (26%) of the 194 World Health Organization (WHO) countries reported experiencing a national level stockout, or shortage of supply, of at least one vaccine lasting at least 1 month. Overall 110 national stockout events were reported in 2014, with a mean of 2.2 events per country and a maximum of six events per country. Shortages involving diphtheria-tetanus-pertussis (DTP) vaccines represented 40% of the reported stockout events, followed by Bacille Calmette-Guérin vaccine for protection against tuberculosis (25%), and measles-containing vaccine representing 14% of stockout events.
At the subnational level, 88% of countries with a national level stockout experienced a district level stockout. In 38 (86%) countries with a district level stockout, the primary cause identified was a national level stockout.
In addition to adequate vaccine stock management, strengthening immunization programs and achieving global vaccination coverage goals requires “additional opportunities for immunization,” such as routine child medical visits in the second year of life, the researchers said.
In 2014, estimated DTP3 coverage (vaccination with the 3rd dose of DTP) was 86% worldwide among infants aged ≤12 months, while estimated global coverage with BCG, polio3, and MCV1 was 91%, 86%, and 85%, respectively. During 2014, a total of 129 (66%) of 194 WHO countries achieved ≥90% national DTP3 coverage. National DTP3 coverage was 80%–89% in 30 countries, 70%–79% in 20 countries, and <70% in 15 countries.
To read the complete report in MMWR, click here.
On Twitter @richpizzi
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
FDA approves new single-tablet HIV treatment
The U.S. Food and Drug Administration has approved Genvoya – a fixed-dose combination tablet containing elvitegravir, cobicistat, emtricitabine, and tenofovir alafenamide – as a complete regimen for the treatment of HIV-1 infection in adults and pediatric patients 12 years of age and older.
Genvoya is approved for use in HIV-infected adults and children aged 12 years and older weighing at least 35 kg (77 pounds) who have never taken HIV therapy and HIV-infected adults whose HIV-1 virus is currently suppressed. The FDA does not recommend Genvoya for patients with severe renal impairment, but says those with moderate renal impairment can take the drug.
Genvoya, which is marketed by Gilead Sciences in Foster City, Calif., contains a new form of tenofovir that has not been previously approved. The FDA says this new form of tenofovir was developed to help reduce some drug side effects, and provides lower levels of the drug in the bloodstream but higher levels within the cells where HIV-1 replicates.
According to Gilead Sciences, Genvoya was studied in a phase III HIV clinical program in more than 3,500 patients across 21 countries, including treatment-naive, virologically suppressed, renally impaired, and adolescent patients. The approval is supported by 48-week data from two phase III double-blind studies among 1,733 treatment-naive patients in which the regimen met its primary objective of noninferiority, compared with another FDA-approved HIV treatment. In the combined analysis of the studies, 92.4% of Genvoya patients and 90.4% of patients on the other treatment had HIV-1 RNA levels less than 50 copies/mL at week 48.
The FDA says Genvoya appears to be associated with less kidney toxicity and fewer decreases in bone density than previously approved tenofovir-containing regimens, based on laboratory measures. Patients receiving Genvoya had greater increases in serum lipids (total cholesterol and low-density lipoprotein) than patients receiving other treatment regimens in the studies.
The new treatment carries a boxed warning alerting patients and health care providers that the drug can cause a buildup of lactic acid in the blood and severe liver problems, both of which can be fatal. The boxed warning also states that Genvoya is not approved to treat chronic hepatitis B virus infection.
For more information, see the FDA announcement, and the Genvoya fact sheet from Gilead Sciences.
rpizzi@frontlinemedcom.com
On Twitter @richpizzi
The U.S. Food and Drug Administration has approved Genvoya – a fixed-dose combination tablet containing elvitegravir, cobicistat, emtricitabine, and tenofovir alafenamide – as a complete regimen for the treatment of HIV-1 infection in adults and pediatric patients 12 years of age and older.
Genvoya is approved for use in HIV-infected adults and children aged 12 years and older weighing at least 35 kg (77 pounds) who have never taken HIV therapy and HIV-infected adults whose HIV-1 virus is currently suppressed. The FDA does not recommend Genvoya for patients with severe renal impairment, but says those with moderate renal impairment can take the drug.
Genvoya, which is marketed by Gilead Sciences in Foster City, Calif., contains a new form of tenofovir that has not been previously approved. The FDA says this new form of tenofovir was developed to help reduce some drug side effects, and provides lower levels of the drug in the bloodstream but higher levels within the cells where HIV-1 replicates.
According to Gilead Sciences, Genvoya was studied in a phase III HIV clinical program in more than 3,500 patients across 21 countries, including treatment-naive, virologically suppressed, renally impaired, and adolescent patients. The approval is supported by 48-week data from two phase III double-blind studies among 1,733 treatment-naive patients in which the regimen met its primary objective of noninferiority, compared with another FDA-approved HIV treatment. In the combined analysis of the studies, 92.4% of Genvoya patients and 90.4% of patients on the other treatment had HIV-1 RNA levels less than 50 copies/mL at week 48.
The FDA says Genvoya appears to be associated with less kidney toxicity and fewer decreases in bone density than previously approved tenofovir-containing regimens, based on laboratory measures. Patients receiving Genvoya had greater increases in serum lipids (total cholesterol and low-density lipoprotein) than patients receiving other treatment regimens in the studies.
The new treatment carries a boxed warning alerting patients and health care providers that the drug can cause a buildup of lactic acid in the blood and severe liver problems, both of which can be fatal. The boxed warning also states that Genvoya is not approved to treat chronic hepatitis B virus infection.
For more information, see the FDA announcement, and the Genvoya fact sheet from Gilead Sciences.
rpizzi@frontlinemedcom.com
On Twitter @richpizzi
The U.S. Food and Drug Administration has approved Genvoya – a fixed-dose combination tablet containing elvitegravir, cobicistat, emtricitabine, and tenofovir alafenamide – as a complete regimen for the treatment of HIV-1 infection in adults and pediatric patients 12 years of age and older.
Genvoya is approved for use in HIV-infected adults and children aged 12 years and older weighing at least 35 kg (77 pounds) who have never taken HIV therapy and HIV-infected adults whose HIV-1 virus is currently suppressed. The FDA does not recommend Genvoya for patients with severe renal impairment, but says those with moderate renal impairment can take the drug.
Genvoya, which is marketed by Gilead Sciences in Foster City, Calif., contains a new form of tenofovir that has not been previously approved. The FDA says this new form of tenofovir was developed to help reduce some drug side effects, and provides lower levels of the drug in the bloodstream but higher levels within the cells where HIV-1 replicates.
According to Gilead Sciences, Genvoya was studied in a phase III HIV clinical program in more than 3,500 patients across 21 countries, including treatment-naive, virologically suppressed, renally impaired, and adolescent patients. The approval is supported by 48-week data from two phase III double-blind studies among 1,733 treatment-naive patients in which the regimen met its primary objective of noninferiority, compared with another FDA-approved HIV treatment. In the combined analysis of the studies, 92.4% of Genvoya patients and 90.4% of patients on the other treatment had HIV-1 RNA levels less than 50 copies/mL at week 48.
The FDA says Genvoya appears to be associated with less kidney toxicity and fewer decreases in bone density than previously approved tenofovir-containing regimens, based on laboratory measures. Patients receiving Genvoya had greater increases in serum lipids (total cholesterol and low-density lipoprotein) than patients receiving other treatment regimens in the studies.
The new treatment carries a boxed warning alerting patients and health care providers that the drug can cause a buildup of lactic acid in the blood and severe liver problems, both of which can be fatal. The boxed warning also states that Genvoya is not approved to treat chronic hepatitis B virus infection.
For more information, see the FDA announcement, and the Genvoya fact sheet from Gilead Sciences.
rpizzi@frontlinemedcom.com
On Twitter @richpizzi
Zika virus adds to dengue and chikungunya threat in Brazil
Clusters of acute exanthematous illness in Brazil have been linked since 2014 to the Zika virus, but research also suggests the concurrent transmission of dengue and chikungunya by the same vectors, a new report reveals.
Zika virus is an emerging mosquito-borne flavivirus that causes a denguelike illness characterized by exanthema, low-grade fever, conjunctivitis, and arthralgia. In a letter to the journal Emerging Infectious Diseases published online, Dr. Cristiane W. Cardoso of the Municipality of Health in Salvador, Brazil, and her coauthors describe the challenges Brazilian public health authorities faced in clinically differentiating Zika virus infections from dengue and chikungunya viruses, also circulating in Brazil from February 2015 to June 2015 (Emerg Infect Dis. 2015 Dec. doi: 10.3201/eid2112.151167).

All three viruses are etiologic agents of acute exanthematous illness, which suggests that the three Aedes mosquito−transmitted viruses were co-circulating in the state of Salvador. The research highlights the challenge in clinically differentiating the infections during outbreaks. The researchers were not able to determine the specific incidence of each virus but write that the low frequency of fever and arthralgia, which are indicators of dengue and chikungunya, point to Zika virus as the probable cause of several reported cases in 2015.
Dr. Cardoso says the spread of Zika virus represents a challenge for public health systems because of the risk for concurrent transmission of dengue and chikungunya by the same vectors – Aedes aegypti and Aedes albopictus mosquitoes – which are abundant throughout tropical and subtropical regions. The authors also suggest that an increase in reports of Guillain-Barré syndrome during the outbreak deserves further investigation to determine whether the syndrome is associated with Zika infection.
To read the entire letter, click here.
On Twitter @richpizzi
Clusters of acute exanthematous illness in Brazil have been linked since 2014 to the Zika virus, but research also suggests the concurrent transmission of dengue and chikungunya by the same vectors, a new report reveals.
Zika virus is an emerging mosquito-borne flavivirus that causes a denguelike illness characterized by exanthema, low-grade fever, conjunctivitis, and arthralgia. In a letter to the journal Emerging Infectious Diseases published online, Dr. Cristiane W. Cardoso of the Municipality of Health in Salvador, Brazil, and her coauthors describe the challenges Brazilian public health authorities faced in clinically differentiating Zika virus infections from dengue and chikungunya viruses, also circulating in Brazil from February 2015 to June 2015 (Emerg Infect Dis. 2015 Dec. doi: 10.3201/eid2112.151167).
All three viruses are etiologic agents of acute exanthematous illness, which suggests that the three Aedes mosquito−transmitted viruses were co-circulating in the state of Salvador. The research highlights the challenge in clinically differentiating the infections during outbreaks. The researchers were not able to determine the specific incidence of each virus but write that the low frequency of fever and arthralgia, which are indicators of dengue and chikungunya, point to Zika virus as the probable cause of several reported cases in 2015.
Dr. Cardoso says the spread of Zika virus represents a challenge for public health systems because of the risk for concurrent transmission of dengue and chikungunya by the same vectors – Aedes aegypti and Aedes albopictus mosquitoes – which are abundant throughout tropical and subtropical regions. The authors also suggest that an increase in reports of Guillain-Barré syndrome during the outbreak deserves further investigation to determine whether the syndrome is associated with Zika infection.
To read the entire letter, click here.
On Twitter @richpizzi
Clusters of acute exanthematous illness in Brazil have been linked since 2014 to the Zika virus, but research also suggests the concurrent transmission of dengue and chikungunya by the same vectors, a new report reveals.
Zika virus is an emerging mosquito-borne flavivirus that causes a denguelike illness characterized by exanthema, low-grade fever, conjunctivitis, and arthralgia. In a letter to the journal Emerging Infectious Diseases published online, Dr. Cristiane W. Cardoso of the Municipality of Health in Salvador, Brazil, and her coauthors describe the challenges Brazilian public health authorities faced in clinically differentiating Zika virus infections from dengue and chikungunya viruses, also circulating in Brazil from February 2015 to June 2015 (Emerg Infect Dis. 2015 Dec. doi: 10.3201/eid2112.151167).
All three viruses are etiologic agents of acute exanthematous illness, which suggests that the three Aedes mosquito−transmitted viruses were co-circulating in the state of Salvador. The research highlights the challenge in clinically differentiating the infections during outbreaks. The researchers were not able to determine the specific incidence of each virus but write that the low frequency of fever and arthralgia, which are indicators of dengue and chikungunya, point to Zika virus as the probable cause of several reported cases in 2015.
Dr. Cardoso says the spread of Zika virus represents a challenge for public health systems because of the risk for concurrent transmission of dengue and chikungunya by the same vectors – Aedes aegypti and Aedes albopictus mosquitoes – which are abundant throughout tropical and subtropical regions. The authors also suggest that an increase in reports of Guillain-Barré syndrome during the outbreak deserves further investigation to determine whether the syndrome is associated with Zika infection.
To read the entire letter, click here.
On Twitter @richpizzi
FROM EMERGING INFECTIOUS DISEASES

Louse-borne relapsing fever appears again in Europe
The reemergence of an early-20th-century fever is an example of how increased migration from war-torn and resource-poor countries has created new routes for the spread of vectorborne diseases.

Louse-borne relapsing fever (LBRF) caused by the bacterium Borrelia recurrentis was a major public health problem in Eastern Europe and Northern Africa during World Wars I and II. A new study published online in Emerging Infectious Diseases reveals that several cases of LBRF have been reported in multiple European nations among asylum seekers from Eritrea (Emerg Infect Dis. 2016 Jan. 22[1]. doi: 10.3201/eid2201.151580).
Poor living conditions, famine, war, and refugee camps are major risk factors for epidemics of LBRF, writes Dr. Alessandra Ciervo of the department of infectious, parasitic and immune-mediated diseases at the Istituto Superiore di Sanità in Rome. Indeed, recent cases of LBRF in the Netherlands, Switzerland, and Germany occurred in asylum seekers who had been in refugee camps in Libya or Italy. Dr. Ciervo and her coauthors report on three sample LBRF cases among patients in Italy who migrated from Somalia after traveling in several countries in Africa and crossing the Mediterranean.
The researchers conclude that, because the cases suggest that more migrants and refugees are infected, LBRF should be considered an emerging disease among migrants and refugees, and diagnostic suspicion of LBRF should lead to early diagnosis among refugees from the Horn of Africa and in persons in migrant camps.
To read the entire research letter, click here.
On Twitter @richpizzi
The reemergence of an early-20th-century fever is an example of how increased migration from war-torn and resource-poor countries has created new routes for the spread of vectorborne diseases.
Louse-borne relapsing fever (LBRF) caused by the bacterium Borrelia recurrentis was a major public health problem in Eastern Europe and Northern Africa during World Wars I and II. A new study published online in Emerging Infectious Diseases reveals that several cases of LBRF have been reported in multiple European nations among asylum seekers from Eritrea (Emerg Infect Dis. 2016 Jan. 22[1]. doi: 10.3201/eid2201.151580).
Poor living conditions, famine, war, and refugee camps are major risk factors for epidemics of LBRF, writes Dr. Alessandra Ciervo of the department of infectious, parasitic and immune-mediated diseases at the Istituto Superiore di Sanità in Rome. Indeed, recent cases of LBRF in the Netherlands, Switzerland, and Germany occurred in asylum seekers who had been in refugee camps in Libya or Italy. Dr. Ciervo and her coauthors report on three sample LBRF cases among patients in Italy who migrated from Somalia after traveling in several countries in Africa and crossing the Mediterranean.
The researchers conclude that, because the cases suggest that more migrants and refugees are infected, LBRF should be considered an emerging disease among migrants and refugees, and diagnostic suspicion of LBRF should lead to early diagnosis among refugees from the Horn of Africa and in persons in migrant camps.
To read the entire research letter, click here.
On Twitter @richpizzi
The reemergence of an early-20th-century fever is an example of how increased migration from war-torn and resource-poor countries has created new routes for the spread of vectorborne diseases.
Louse-borne relapsing fever (LBRF) caused by the bacterium Borrelia recurrentis was a major public health problem in Eastern Europe and Northern Africa during World Wars I and II. A new study published online in Emerging Infectious Diseases reveals that several cases of LBRF have been reported in multiple European nations among asylum seekers from Eritrea (Emerg Infect Dis. 2016 Jan. 22[1]. doi: 10.3201/eid2201.151580).
Poor living conditions, famine, war, and refugee camps are major risk factors for epidemics of LBRF, writes Dr. Alessandra Ciervo of the department of infectious, parasitic and immune-mediated diseases at the Istituto Superiore di Sanità in Rome. Indeed, recent cases of LBRF in the Netherlands, Switzerland, and Germany occurred in asylum seekers who had been in refugee camps in Libya or Italy. Dr. Ciervo and her coauthors report on three sample LBRF cases among patients in Italy who migrated from Somalia after traveling in several countries in Africa and crossing the Mediterranean.
The researchers conclude that, because the cases suggest that more migrants and refugees are infected, LBRF should be considered an emerging disease among migrants and refugees, and diagnostic suspicion of LBRF should lead to early diagnosis among refugees from the Horn of Africa and in persons in migrant camps.
To read the entire research letter, click here.
On Twitter @richpizzi
FROM EMERGING INFECTIOUS DISEASES

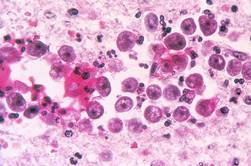
Early diagnosis of primary amebic meningoencephalitis key to treatment
A 2014 Florida case of primary amebic meningoencephalitis (PAM) – a rare, typically fatal infection of the brain – is a reminder to physicians of the need for early diagnosis and prompt treatment of patients with suspected ameba infections.
PAM is a devastating infection caused by Naegleria fowleri, a free-living ameba found in warm, fresh water bodies throughout the world. Amebae like N. fowleri are aspirated into the nasal cavity through swimming, splashing, or nasal irrigation, and after attaching to the nasal mucosa, migrate across the cribriform plate to the brain via the olfactory nerves, causing extensive damage to the frontal lobes of the brain. In fact, only three nonfatal cases have ever been documented in the United States, according to a report in the Nov. 6, 2015, edition of the Morbidity and Mortality Weekly Report (MMWR. 2015 Nov 6;64[43]:1226).
In August 2013, miltefosine, an antiparasitic drug with activity against N. fowleri, became available from the Centers for Disease Control and Prevention as an investigational drug for the treatment of free-living ameba infections in combination with other antimicrobial drugs. Miltefosine was administered as part of the successful treatment of a case of PAM in 2013, and it can be requested from the CDC upon clinical suspicion of PAM infection and before laboratory confirmation.
Peggy J. Booth of the Florida Department of Health and coauthors related the case of an 11-year-old Florida boy hospitalized with a presumptive diagnosis of viral meningitis in June 2014. The initial cerebral spinal fluid (CSF) analysis was negative for motile ameba, but 2 days later – after the boy’s condition deteriorated – a second CSF specimen revealed the presence of motile ameba. Physicians consulted with the CDC and arranged for delivery of miltefosine, but the patient died before its arrival.
Ms. Booth and coauthors recommend that physicians consider a diagnosis of PAM in persons with a clinically compatible illness who have a history of fresh water exposure 1-9 days before illness onset. Early diagnosis and prompt treatment are essential because of the high mortality rate. The CDC is currently considering strategic placement of miltefosine in Texas and Florida, where approximately half of all cases in the United States have been reported, which might reduce the time to initiating treatment associated with transport of the medication.
To read the complete report in MMWR, click here.
On Twitter @richpizzi
A 2014 Florida case of primary amebic meningoencephalitis (PAM) – a rare, typically fatal infection of the brain – is a reminder to physicians of the need for early diagnosis and prompt treatment of patients with suspected ameba infections.
PAM is a devastating infection caused by Naegleria fowleri, a free-living ameba found in warm, fresh water bodies throughout the world. Amebae like N. fowleri are aspirated into the nasal cavity through swimming, splashing, or nasal irrigation, and after attaching to the nasal mucosa, migrate across the cribriform plate to the brain via the olfactory nerves, causing extensive damage to the frontal lobes of the brain. In fact, only three nonfatal cases have ever been documented in the United States, according to a report in the Nov. 6, 2015, edition of the Morbidity and Mortality Weekly Report (MMWR. 2015 Nov 6;64[43]:1226).
In August 2013, miltefosine, an antiparasitic drug with activity against N. fowleri, became available from the Centers for Disease Control and Prevention as an investigational drug for the treatment of free-living ameba infections in combination with other antimicrobial drugs. Miltefosine was administered as part of the successful treatment of a case of PAM in 2013, and it can be requested from the CDC upon clinical suspicion of PAM infection and before laboratory confirmation.
Peggy J. Booth of the Florida Department of Health and coauthors related the case of an 11-year-old Florida boy hospitalized with a presumptive diagnosis of viral meningitis in June 2014. The initial cerebral spinal fluid (CSF) analysis was negative for motile ameba, but 2 days later – after the boy’s condition deteriorated – a second CSF specimen revealed the presence of motile ameba. Physicians consulted with the CDC and arranged for delivery of miltefosine, but the patient died before its arrival.
Ms. Booth and coauthors recommend that physicians consider a diagnosis of PAM in persons with a clinically compatible illness who have a history of fresh water exposure 1-9 days before illness onset. Early diagnosis and prompt treatment are essential because of the high mortality rate. The CDC is currently considering strategic placement of miltefosine in Texas and Florida, where approximately half of all cases in the United States have been reported, which might reduce the time to initiating treatment associated with transport of the medication.
To read the complete report in MMWR, click here.
On Twitter @richpizzi
A 2014 Florida case of primary amebic meningoencephalitis (PAM) – a rare, typically fatal infection of the brain – is a reminder to physicians of the need for early diagnosis and prompt treatment of patients with suspected ameba infections.
PAM is a devastating infection caused by Naegleria fowleri, a free-living ameba found in warm, fresh water bodies throughout the world. Amebae like N. fowleri are aspirated into the nasal cavity through swimming, splashing, or nasal irrigation, and after attaching to the nasal mucosa, migrate across the cribriform plate to the brain via the olfactory nerves, causing extensive damage to the frontal lobes of the brain. In fact, only three nonfatal cases have ever been documented in the United States, according to a report in the Nov. 6, 2015, edition of the Morbidity and Mortality Weekly Report (MMWR. 2015 Nov 6;64[43]:1226).
In August 2013, miltefosine, an antiparasitic drug with activity against N. fowleri, became available from the Centers for Disease Control and Prevention as an investigational drug for the treatment of free-living ameba infections in combination with other antimicrobial drugs. Miltefosine was administered as part of the successful treatment of a case of PAM in 2013, and it can be requested from the CDC upon clinical suspicion of PAM infection and before laboratory confirmation.
Peggy J. Booth of the Florida Department of Health and coauthors related the case of an 11-year-old Florida boy hospitalized with a presumptive diagnosis of viral meningitis in June 2014. The initial cerebral spinal fluid (CSF) analysis was negative for motile ameba, but 2 days later – after the boy’s condition deteriorated – a second CSF specimen revealed the presence of motile ameba. Physicians consulted with the CDC and arranged for delivery of miltefosine, but the patient died before its arrival.
Ms. Booth and coauthors recommend that physicians consider a diagnosis of PAM in persons with a clinically compatible illness who have a history of fresh water exposure 1-9 days before illness onset. Early diagnosis and prompt treatment are essential because of the high mortality rate. The CDC is currently considering strategic placement of miltefosine in Texas and Florida, where approximately half of all cases in the United States have been reported, which might reduce the time to initiating treatment associated with transport of the medication.
To read the complete report in MMWR, click here.
On Twitter @richpizzi
FROM MMWR

Genomic sequencing technology reveals weakness in malaria vaccine
Genetic variability in the surface protein targeted by an experimental malaria vaccine explains why the vaccine provided only moderate protection among children during clinical testing, a new study reveals.

The research, published online in the New England Journal of Medicine (2015 Oct 21. doi: 10.1056/NEJMoa1505819), was intended to determine whether the efficacy of the malaria vaccine candidate RTS,S/AS01 (RTS,S) was specific to certain parasite genotypes at the circumsporozoite (CS) protein locus. The researchers, led by Daniel Neafsey, Ph.D., associate director of the Genomic Center for Infectious Diseases at the Broad Institute of MIT in Boston, used polymerase chain reaction–based next-generation sequencing of DNA to evaluate blood samples from nearly 5,000 infants and children who participated in Phase III clinical testing of the vaccine. They found that the RTS,S vaccine was most effective at preventing malaria in children aged 5-17 months who were infected with parasites with the same protein variant that the RTS,S vaccine targeted, while a mismatch corresponded with a lesser degree of protection.
The RTS,S vaccine was designed to target the CS protein found on the surface of malaria-causing Plasmodium parasites. However, while the CS protein is genetically diverse, the RTS,S vaccine incorporates only one variant. Previous studies examining genetic variations in the CS protein did not suggest that the variations may limit or restrict vaccine protection.
“The overall vaccine efficacy in this age category will depend on the proportion of matched alleles in the local parasite population,” Dr. Neafsey and his coauthors wrote. “In this trial, less than 10% of parasites had matched alleles.”
The authors reported no relevant disclosures.
To read the entire study, click here.
On Twitter @richpizzi
Genetic variability in the surface protein targeted by an experimental malaria vaccine explains why the vaccine provided only moderate protection among children during clinical testing, a new study reveals.
The research, published online in the New England Journal of Medicine (2015 Oct 21. doi: 10.1056/NEJMoa1505819), was intended to determine whether the efficacy of the malaria vaccine candidate RTS,S/AS01 (RTS,S) was specific to certain parasite genotypes at the circumsporozoite (CS) protein locus. The researchers, led by Daniel Neafsey, Ph.D., associate director of the Genomic Center for Infectious Diseases at the Broad Institute of MIT in Boston, used polymerase chain reaction–based next-generation sequencing of DNA to evaluate blood samples from nearly 5,000 infants and children who participated in Phase III clinical testing of the vaccine. They found that the RTS,S vaccine was most effective at preventing malaria in children aged 5-17 months who were infected with parasites with the same protein variant that the RTS,S vaccine targeted, while a mismatch corresponded with a lesser degree of protection.
The RTS,S vaccine was designed to target the CS protein found on the surface of malaria-causing Plasmodium parasites. However, while the CS protein is genetically diverse, the RTS,S vaccine incorporates only one variant. Previous studies examining genetic variations in the CS protein did not suggest that the variations may limit or restrict vaccine protection.
“The overall vaccine efficacy in this age category will depend on the proportion of matched alleles in the local parasite population,” Dr. Neafsey and his coauthors wrote. “In this trial, less than 10% of parasites had matched alleles.”
The authors reported no relevant disclosures.
To read the entire study, click here.
On Twitter @richpizzi
Genetic variability in the surface protein targeted by an experimental malaria vaccine explains why the vaccine provided only moderate protection among children during clinical testing, a new study reveals.
The research, published online in the New England Journal of Medicine (2015 Oct 21. doi: 10.1056/NEJMoa1505819), was intended to determine whether the efficacy of the malaria vaccine candidate RTS,S/AS01 (RTS,S) was specific to certain parasite genotypes at the circumsporozoite (CS) protein locus. The researchers, led by Daniel Neafsey, Ph.D., associate director of the Genomic Center for Infectious Diseases at the Broad Institute of MIT in Boston, used polymerase chain reaction–based next-generation sequencing of DNA to evaluate blood samples from nearly 5,000 infants and children who participated in Phase III clinical testing of the vaccine. They found that the RTS,S vaccine was most effective at preventing malaria in children aged 5-17 months who were infected with parasites with the same protein variant that the RTS,S vaccine targeted, while a mismatch corresponded with a lesser degree of protection.
The RTS,S vaccine was designed to target the CS protein found on the surface of malaria-causing Plasmodium parasites. However, while the CS protein is genetically diverse, the RTS,S vaccine incorporates only one variant. Previous studies examining genetic variations in the CS protein did not suggest that the variations may limit or restrict vaccine protection.
“The overall vaccine efficacy in this age category will depend on the proportion of matched alleles in the local parasite population,” Dr. Neafsey and his coauthors wrote. “In this trial, less than 10% of parasites had matched alleles.”
The authors reported no relevant disclosures.
To read the entire study, click here.
On Twitter @richpizzi
FROM NEW ENGLAND JOURNAL OF MEDICINE

Society of Hospital Medicine targets antibiotic overprescribing
A campaign that specifically targets hospital-based clinicians to address the growing problem of antibiotic-resistant infections is being launched by the Society of Hospital Medicine (SHM).
The “Fight the Resistance” campaign officially launches on Tuesday, Nov. 10 with a webinar featuring Dr. Scott A. Flanders, professor of medicine and director of the hospitalist program at the University of Michigan, and Dr. Melhim Bou Alwan, chair of the antimicrobial stewardship committee at West Georgia Health. Physicians can register to join the webinar. SHM is also offering downloadable posters on the dedicated campaign website – www.fighttheresistance.org – and encouraging hospital-based staff to display the posters in high-traffic areas of their institutions.

The SHM committed to the campaign at a White House forum on antibiotic stewardship in June 2015. The campaign is in conjunction with the Center for Disease Control and Prevention’s “Get Smart About Antibiotics Week,” which is Nov.16-22.
Hospital-based staff are encouraged to work as a team, paying attention to appropriate antibiotic choice and rethinking antibiotic treatment time course, Dr. Eric Howell, SHM senior physician advisor, notes at the new website. Downloading the posters from the website and displaying them in their hospitals is one way to focus on that goal.
Two million people become infected each year with antibiotic-resistant bacteria and at least 23,000 people die as a direct result of these infections, according to the SHM. The organization hopes Fight the Resistance helps to promote culture change in U.S. hospitals that sharply reduces antibiotic overprescribing.
For more information on “Fight the Resistance,” visit the campaign website and follow the conversation on Twitter using the hashtag #FightTheResistance.
On Twitter @richpizzi
A campaign that specifically targets hospital-based clinicians to address the growing problem of antibiotic-resistant infections is being launched by the Society of Hospital Medicine (SHM).
The “Fight the Resistance” campaign officially launches on Tuesday, Nov. 10 with a webinar featuring Dr. Scott A. Flanders, professor of medicine and director of the hospitalist program at the University of Michigan, and Dr. Melhim Bou Alwan, chair of the antimicrobial stewardship committee at West Georgia Health. Physicians can register to join the webinar. SHM is also offering downloadable posters on the dedicated campaign website – www.fighttheresistance.org – and encouraging hospital-based staff to display the posters in high-traffic areas of their institutions.
The SHM committed to the campaign at a White House forum on antibiotic stewardship in June 2015. The campaign is in conjunction with the Center for Disease Control and Prevention’s “Get Smart About Antibiotics Week,” which is Nov.16-22.
Hospital-based staff are encouraged to work as a team, paying attention to appropriate antibiotic choice and rethinking antibiotic treatment time course, Dr. Eric Howell, SHM senior physician advisor, notes at the new website. Downloading the posters from the website and displaying them in their hospitals is one way to focus on that goal.
Two million people become infected each year with antibiotic-resistant bacteria and at least 23,000 people die as a direct result of these infections, according to the SHM. The organization hopes Fight the Resistance helps to promote culture change in U.S. hospitals that sharply reduces antibiotic overprescribing.
For more information on “Fight the Resistance,” visit the campaign website and follow the conversation on Twitter using the hashtag #FightTheResistance.
On Twitter @richpizzi
A campaign that specifically targets hospital-based clinicians to address the growing problem of antibiotic-resistant infections is being launched by the Society of Hospital Medicine (SHM).
The “Fight the Resistance” campaign officially launches on Tuesday, Nov. 10 with a webinar featuring Dr. Scott A. Flanders, professor of medicine and director of the hospitalist program at the University of Michigan, and Dr. Melhim Bou Alwan, chair of the antimicrobial stewardship committee at West Georgia Health. Physicians can register to join the webinar. SHM is also offering downloadable posters on the dedicated campaign website – www.fighttheresistance.org – and encouraging hospital-based staff to display the posters in high-traffic areas of their institutions.
The SHM committed to the campaign at a White House forum on antibiotic stewardship in June 2015. The campaign is in conjunction with the Center for Disease Control and Prevention’s “Get Smart About Antibiotics Week,” which is Nov.16-22.
Hospital-based staff are encouraged to work as a team, paying attention to appropriate antibiotic choice and rethinking antibiotic treatment time course, Dr. Eric Howell, SHM senior physician advisor, notes at the new website. Downloading the posters from the website and displaying them in their hospitals is one way to focus on that goal.
Two million people become infected each year with antibiotic-resistant bacteria and at least 23,000 people die as a direct result of these infections, according to the SHM. The organization hopes Fight the Resistance helps to promote culture change in U.S. hospitals that sharply reduces antibiotic overprescribing.
For more information on “Fight the Resistance,” visit the campaign website and follow the conversation on Twitter using the hashtag #FightTheResistance.
On Twitter @richpizzi

CDC to celebrate best blood clot prevention strategies
The Centers for Disease Control and Prevention has launched a program to honor hospitals, health systems, and managed care organizations that have implemented effective strategies to prevent health care–associated blood clots.
The HA-VTE Prevention Challenge invites provider organizations around the world to submit evidence of demonstrated successful use of venous thromboembolism (VTE) prevention strategies and interventions. VTE leads to approximately 100,000 premature deaths in the United States every year, according to the CDC, yet as many as 70% of HA-VTEs are preventable, although fewer than half of hospital patients receive appropriate prevention. Indeed, about half of all blood clots happen after a recent hospital stay or surgery.
“Doctors and nurses in hospitals and other health care settings can save lives by implementing the best practices discovered through this challenge,” Dr. Tom Frieden, CDC director, said in a statement. “Tell us about what you are doing and what’s helping prevent blood clots, so we can advance science and save lives together.”
The purpose of the challenge is to highlight the systems, processes, and staffing that contribute to exceptional VTE prevention, according to the CDC. Processes may include the implementation of protocols, risk assessments, and the use of health information technology and clinical decision support tools. Seven of the highest scoring U.S. non-federal hospitals, multihospital systems, hospital networks, and managed care organizations will be recognized as HA-VTE Prevention Champions and will receive a cash award of $10,000 each. Winning submissions from U.S. federal and international entities will be eligible for nonmonetary recognition.
The CDC will accept submissions from Nov. 2, 2015, until Jan. 10, 2016. Winners will be announced in March 2016.
For more information, visit the HA-VTE Prevention Challenge website.
On Twitter: @richpizzi
The Centers for Disease Control and Prevention has launched a program to honor hospitals, health systems, and managed care organizations that have implemented effective strategies to prevent health care–associated blood clots.
The HA-VTE Prevention Challenge invites provider organizations around the world to submit evidence of demonstrated successful use of venous thromboembolism (VTE) prevention strategies and interventions. VTE leads to approximately 100,000 premature deaths in the United States every year, according to the CDC, yet as many as 70% of HA-VTEs are preventable, although fewer than half of hospital patients receive appropriate prevention. Indeed, about half of all blood clots happen after a recent hospital stay or surgery.
“Doctors and nurses in hospitals and other health care settings can save lives by implementing the best practices discovered through this challenge,” Dr. Tom Frieden, CDC director, said in a statement. “Tell us about what you are doing and what’s helping prevent blood clots, so we can advance science and save lives together.”
The purpose of the challenge is to highlight the systems, processes, and staffing that contribute to exceptional VTE prevention, according to the CDC. Processes may include the implementation of protocols, risk assessments, and the use of health information technology and clinical decision support tools. Seven of the highest scoring U.S. non-federal hospitals, multihospital systems, hospital networks, and managed care organizations will be recognized as HA-VTE Prevention Champions and will receive a cash award of $10,000 each. Winning submissions from U.S. federal and international entities will be eligible for nonmonetary recognition.
The CDC will accept submissions from Nov. 2, 2015, until Jan. 10, 2016. Winners will be announced in March 2016.
For more information, visit the HA-VTE Prevention Challenge website.
On Twitter: @richpizzi
The Centers for Disease Control and Prevention has launched a program to honor hospitals, health systems, and managed care organizations that have implemented effective strategies to prevent health care–associated blood clots.
The HA-VTE Prevention Challenge invites provider organizations around the world to submit evidence of demonstrated successful use of venous thromboembolism (VTE) prevention strategies and interventions. VTE leads to approximately 100,000 premature deaths in the United States every year, according to the CDC, yet as many as 70% of HA-VTEs are preventable, although fewer than half of hospital patients receive appropriate prevention. Indeed, about half of all blood clots happen after a recent hospital stay or surgery.
“Doctors and nurses in hospitals and other health care settings can save lives by implementing the best practices discovered through this challenge,” Dr. Tom Frieden, CDC director, said in a statement. “Tell us about what you are doing and what’s helping prevent blood clots, so we can advance science and save lives together.”
The purpose of the challenge is to highlight the systems, processes, and staffing that contribute to exceptional VTE prevention, according to the CDC. Processes may include the implementation of protocols, risk assessments, and the use of health information technology and clinical decision support tools. Seven of the highest scoring U.S. non-federal hospitals, multihospital systems, hospital networks, and managed care organizations will be recognized as HA-VTE Prevention Champions and will receive a cash award of $10,000 each. Winning submissions from U.S. federal and international entities will be eligible for nonmonetary recognition.
The CDC will accept submissions from Nov. 2, 2015, until Jan. 10, 2016. Winners will be announced in March 2016.
For more information, visit the HA-VTE Prevention Challenge website.
On Twitter: @richpizzi
2015 Nobel Prize for Medicine honors parasitic disease research
Three biomedical scientists who developed revolutionary therapies for the treatment of parasitic diseases have won the 2015 Nobel Prize in Physiology or Medicine.
Microbiologists William C. Campbell, PhD, and Satoshi Omura, PhD, were honored for the discovery of avermectin, the derivatives of which have radically lowered the incidence of river blindness and lymphatic filariasis, as well as showing efficacy against an expanding number of other parasitic diseases. Dr. Campbell and Dr. Omura shared the award with pharmacologist Youyou Tu, who discovered artemisinin, a drug that has significantly reduced the mortality rates for patients suffering from malaria.
Dr. Campbell, an expert in parasite biology, is based at Drew University in Madison, N.J., while Dr. Omura, renowned for his expertise in isolating natural products, works at Kitasato University in Tokyo. Ms. Tu, the first China-based researcher to win a science Nobel, is chief professor at the China Academy of Traditional Chinese Medical Sciences in Beijing.
According to the prize announcement from the Nobel Assembly at Karolinska Institutet in Stockholm, the research of the 2015 Physiology or Medicine Laureates “represents a paradigm shift in medicine, which has not only provided a revolutionary therapy for patients suffering from devastating parasitic diseases, but it has also promoted well-being and prosperity of both individuals and society. The global impact of their discoveries and the benefit to mankind is immeasurable.”
Read the 2015 Nobel Prize in Physiology or Medicine announcement here, and the complete scientific statement supporting the winners here.
On Twitter @richpizzi
Three biomedical scientists who developed revolutionary therapies for the treatment of parasitic diseases have won the 2015 Nobel Prize in Physiology or Medicine.
Microbiologists William C. Campbell, PhD, and Satoshi Omura, PhD, were honored for the discovery of avermectin, the derivatives of which have radically lowered the incidence of river blindness and lymphatic filariasis, as well as showing efficacy against an expanding number of other parasitic diseases. Dr. Campbell and Dr. Omura shared the award with pharmacologist Youyou Tu, who discovered artemisinin, a drug that has significantly reduced the mortality rates for patients suffering from malaria.
Dr. Campbell, an expert in parasite biology, is based at Drew University in Madison, N.J., while Dr. Omura, renowned for his expertise in isolating natural products, works at Kitasato University in Tokyo. Ms. Tu, the first China-based researcher to win a science Nobel, is chief professor at the China Academy of Traditional Chinese Medical Sciences in Beijing.
According to the prize announcement from the Nobel Assembly at Karolinska Institutet in Stockholm, the research of the 2015 Physiology or Medicine Laureates “represents a paradigm shift in medicine, which has not only provided a revolutionary therapy for patients suffering from devastating parasitic diseases, but it has also promoted well-being and prosperity of both individuals and society. The global impact of their discoveries and the benefit to mankind is immeasurable.”
Read the 2015 Nobel Prize in Physiology or Medicine announcement here, and the complete scientific statement supporting the winners here.
On Twitter @richpizzi
Three biomedical scientists who developed revolutionary therapies for the treatment of parasitic diseases have won the 2015 Nobel Prize in Physiology or Medicine.
Microbiologists William C. Campbell, PhD, and Satoshi Omura, PhD, were honored for the discovery of avermectin, the derivatives of which have radically lowered the incidence of river blindness and lymphatic filariasis, as well as showing efficacy against an expanding number of other parasitic diseases. Dr. Campbell and Dr. Omura shared the award with pharmacologist Youyou Tu, who discovered artemisinin, a drug that has significantly reduced the mortality rates for patients suffering from malaria.
Dr. Campbell, an expert in parasite biology, is based at Drew University in Madison, N.J., while Dr. Omura, renowned for his expertise in isolating natural products, works at Kitasato University in Tokyo. Ms. Tu, the first China-based researcher to win a science Nobel, is chief professor at the China Academy of Traditional Chinese Medical Sciences in Beijing.
According to the prize announcement from the Nobel Assembly at Karolinska Institutet in Stockholm, the research of the 2015 Physiology or Medicine Laureates “represents a paradigm shift in medicine, which has not only provided a revolutionary therapy for patients suffering from devastating parasitic diseases, but it has also promoted well-being and prosperity of both individuals and society. The global impact of their discoveries and the benefit to mankind is immeasurable.”
Read the 2015 Nobel Prize in Physiology or Medicine announcement here, and the complete scientific statement supporting the winners here.
On Twitter @richpizzi