User login
Inpatient Portals for Hospitalized Patients and Caregivers: A Systematic Review
Engaging patients and their caregivers in care improves health outcomes1-3 and is endorsed by leading healthcare organizations as essential to improving care quality and safety.4-6 Patient engagement emphasizes that patients, caregivers, and healthcare providers work together to “promote and support active patient and public involvement in health and healthcare and to strengthen their influence on healthcare decisions.”7 Patient portals, web-based personal health records linked to electronic health record (EHR) data, are intended to promote engagement by providing patients and their caregivers with timely electronic access to their healthcare information and supporting communication through secure messaging with their healthcare team.8 The use of patient portals has also been suggested as a way for patients and/or caregivers to identify and intercept medical errors, thus having the potential to also improve patient safety.8,9
As a requirement for meaningful use, access to health information through patient portals in the ambulatory setting has increased dramatically.10 Studies evaluating the use of these patient portals to promote patient-centered care are growing, but evidence supporting their impact on improved health outcomes is currently insufficient.11-15 Although research and policy focus on the use of patient portals in the ambulatory setting, recent literature suggests that patient portals may be used to share inpatient clinical information to engage patients and their caregivers during their hospitalization.16-18 Before the widespread use of patient portals in the inpatient setting is endorsed, systematic research is needed to understand optimal portal design requirements, if and how these portals are used, and whether their use provides value to the hospitalized patient and/or caregiver.8
Prior literature summarized early findings regarding the use of various technologies designed to engage hospitalized patients.17,19,20 In this systematic review, we describe the emerging literature examining the design, use, and impact of inpatient portals for hospitalized patients and/or caregivers over the last 10 years. Inpatient portals are defined here as electronic patient portals tethered to EHRs that are designed to provide hospitalized patients and/or caregivers secure access to personalized, inpatient clinical information with the intent of engaging them in their hospital care. After analyzing and summarizing these data, we then identify knowledge gaps and potential future research directions.
METHODS
Search Strategy, Study Selection, and Analysis
This systematic review included available, peer-reviewed, and grey literature published from January 1, 2006, to August 8, 2017, in PubMed, Web of Science (including the Institute of Electrical and Electronics Engineers Xplore), Cochrane, CINAHLPlus, and Scopus databases. Terms and phrases, including those found in the Medical Subject Heading (MeSH) index, were used to identify studies evaluating (1) patient portals (“health record, personal [MeSH],” “personal health record,” “patient portal,” “inpatient portal,” “ipad,” “tablet,” or “bedside information technology”), (2) engagement (“engagement,” “empowerment,” “participation,” “activation,” or “self-efficacy”), and (3) in the hospital (“inpatient [MeSH],” “hospital [MeSH],” “hospitalized patient [MeSH],” or “unit”). MeSH terms were used when applicable. Based on previous literature, free-text terms were also used when subject headings were not applied consistently, such as with terms related to engagement.17,21 Studies were excluded if they were not written in English, if they evaluated portals exclusively in the emergency department or ambulatory setting, and/or if they described future study protocols. Studies describing general inpatient technology or evaluating portals used in the hospital but not tethered to inpatient EHR clinical data were also excluded.
By using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines,22 2 researchers (M.K. and P.H.) completed the literature search and potential article screening. Results were aggregated and studies were screened and excluded from full review based on title and abstract information. Additional studies were included after reference list review. During a full review of included studies, 2 researchers independently extracted data, including the study objective, design, setting, sample, data collection instruments, outcomes, and a description of results. Guided by our study objective, findings were reconciled by consensus and analyzed and described according to the following 3 themes: (1) inpatient portal design, (2) inpatient portal use and usability, and (3) the impact of inpatient portal use on patient or caregiver and healthcare team outcomes as defined by retrieved studies.
The quality of studies was evaluated by the same 2 researchers independently by using the Downs and Black checklist for assessing the methodological quality of randomized and nonrandomized healthcare interventions.23 Qualitative studies describing the development of portal prototypes and/or portal redesign efforts were excluded from these analyses. Discrepancies were resolved by consensus.Because of the wide variability in study designs, populations, and outcomes, a meta-analysis of pooled data was not performed.
RESULTS
Of the 731 studies identified through database searching and reference review, 36 were included for full-text review and 17 met inclusion criteria (Figure; Table 1). Studies excluded after full-text review described portal use outside of the inpatient setting, portals not linked to hospital EHR clinical data, portals not designed for inpatients, and/or inpatient technology in general. The inpatient portal platforms, hardware used, and functionalities varied within included studies (Table 2). The majority of studies used custom, web-based inpatient portal applications on tablet computers. Most provided information about the patients’ hospital medications, healthcare team, and education about their condition and/or a medical glossary. Many included the patient’s schedule, hospital problem list, discharge information, and a way to keep notes.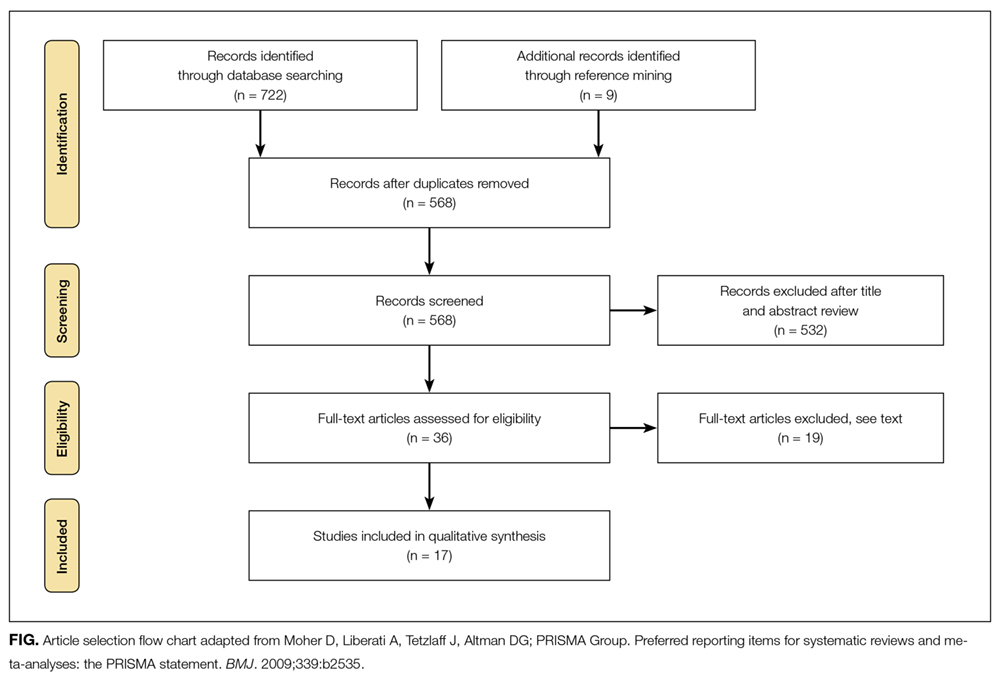
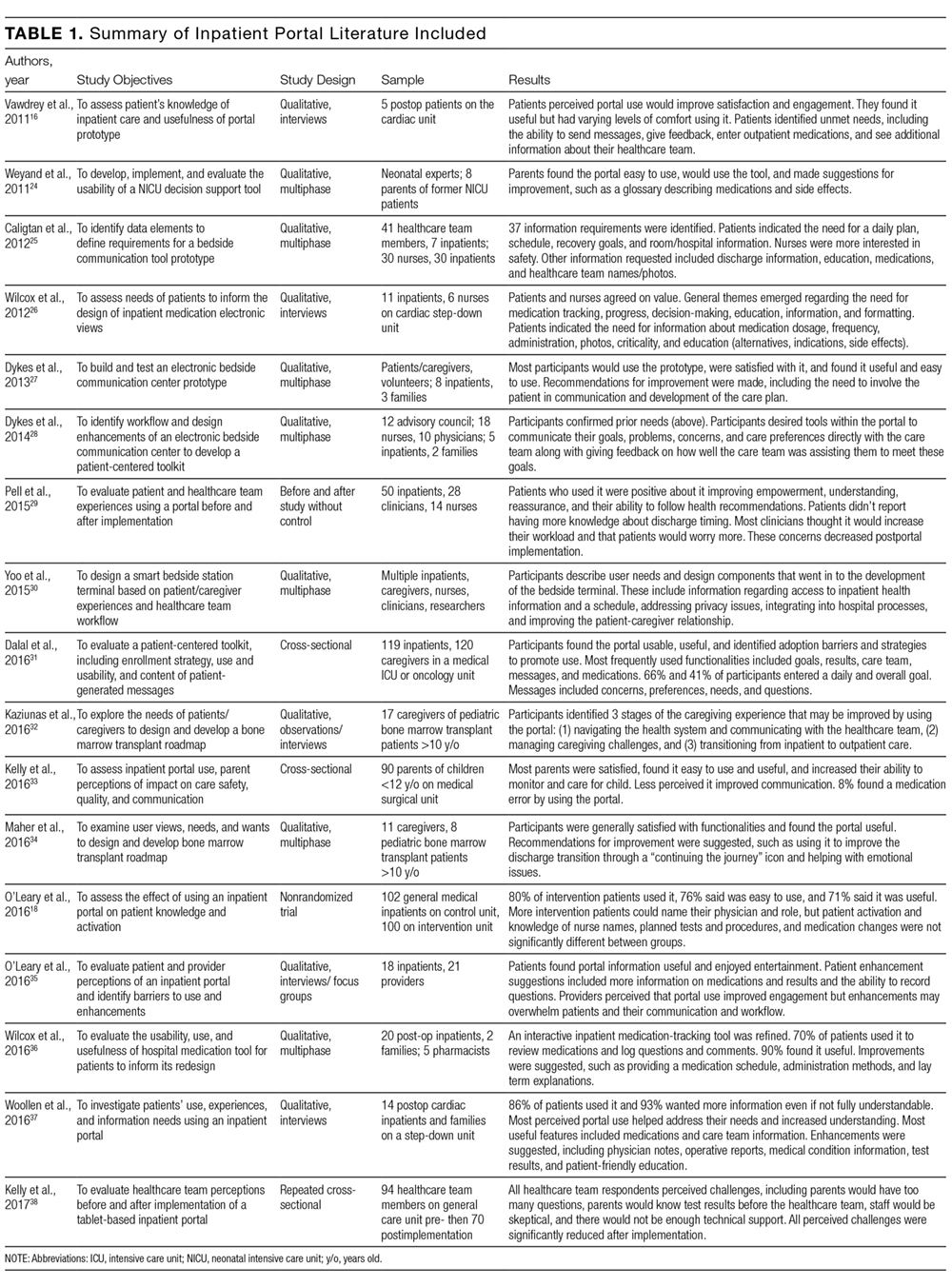
There has been a recent increase in inpatient portal study publication, with 9 studies published during or after 2016. Five were conducted in the pediatric setting and all but 130 with English-speaking participants. Twelve studies were qualitative, many of which were conducted in multiple phases by using semi-structured interviews and/or focus groups to develop or redesign inpatient portals. Of the remaining studies, 3 used a cross-sectional design, 1 used a before and after design without a control group, and 1 was a nonrandomized trial. Studies were rated as having medium-to-high risk of bias because of design flaws (Table 1 in supplementary Appendix). Because many studies were small pilot studies and all were single-centered studies, the generalizability of findings to different healthcare settings or patient populations is limited.
Inpatient Portal Design
Most included studies evaluated patient and/or caregiver information needs to design and/or enhance inpatient portals.16,24-37 In 1 study, patients described an overall lack of information provided in the hospital and insufficient time to understand and remember information, which, when shared, was often presented by using medical terminology.30 They wanted information to help them understand their daily hospital routine, confirm and compare medications and test results, learn about care, and prepare for discharge. Participants in multiple studies echoed these results, indicating the need for a schedule of upcoming clinical events (eg, medication administration, procedures, imaging), secure and timely clinical information (eg, list of diagnoses and medications, test results), personalized education, a medical glossary, discharge information, and a way to take notes and recognize and communicate with providers.
Patients also requested further information transparency,34,37 including physicians’ notes, radiology results, operative reports, and billing information, along with general hospital information,16 meal ordering,33 and video conferencing.27 ln designing and refining an inpatient medication-tracking tool, participants identified the need for information about medication dosage, frequency, timing, administration method, criticality, alternative medications or forms, and education.26,36 Patients and/or caregivers also indicated interest in communicating with inpatient providers by using the portal.16,27,28,30-37 In 1 study, patients highlighted the need to be involved in care plan development,27 which led to portal refinement to allow for patient-generated data entry, including care goals and a way to communicate real-time concerns and feedback.28
Studies also considered healthcare team perspectives to inform portal design.25,26,28,30,35,37 Although information needs usually overlapped, patient and healthcare team priorities differed in some areas. Although patients wanted to “know what was going to happen to them,” nurses in 1 study were more concerned about providing information to protect patients, such as safety and precaution materials.25 Similarly, when designing a medication-tracking tool, patients sought information that helped them understand what to expect, while pharmacists focused on medication safety and providing information that fit their workflow (eg, abstract medication schedules).36
Identified study data raised important portal interface design considerations. Results suggested clinical data should be presented by using simple displays,28 accommodating real-time information. Participants recommended links16,29 to personalized patient-friendly37 education accessed with minimal steps.26 Interfaces may be personalized for target users, such as patient or proxy and younger or older individuals. For example, older patients reported less familiarity with touch screens, internal keyboards, and handwriting recognition, favoring voice recognition for recording notes.27 This raised questions about how portals can be designed to best maintain patient privacy.25 Interface design, such as navigation, also relied heavily on hardware choice, such as tablet versus mobile phone.28
Inpatient Portal Use and Usability
Most patient and/or caregiver participants in included studies were interested in using an inpatient portal, used it when offered, found it easy to use, useful, and/or were satisfied with it.16,18,24-37 Most used and liked functionalities that provided healthcare team, test result, and medication information.22,33,37 In the 1 identified controlled trial,18 researchers evaluated an inpatient portal given to adult inpatients that included a problem list, schedule, medication list, and healthcare team information. Of the intervention unit patients, 80% used the portal, 76% indicated it was easy to use, and 71% thought it provided useful information. When a portal was given to 239 adult patients and caregivers in another study, 66% sent a total of 291 messages to the healthcare team.31 Of these, 153 provided feedback, 76 expressed preferences, and 16 communicated concerns. In a pediatric study, an inpatient portal was given to 296 parents who sent a total of 36 messages and 176 requests.33 Messages sent included information regarding caregiver needs, questions, updates, and/or positive endorsements of the healthcare team and/or care.
Impact of Inpatient Portal Use
Multiple studies evaluated the impact of inpatient portal use on patient and/or caregiver engagement, empowerment, activation, and/or knowledge, which had mixed results. Most adult patients interviewed in one study had positive experiences using a portal to answer their questions between physician visits and learn about, remember, and engage in care.37 A majority of adult inpatient portal users in another study agreed that portal use helped them feel in control and understand their condition; however, they did not report having improved discharge timing knowledge.29 In a pediatric study, most parent inpatient portal users agreed use improved their ability to monitor, understand, and make decisions about their child’s care.33 In the controlled trial,18 a higher percentage of portal intervention patients could identify their physician or role; however, patient activation was not statistically different between intervention and control patients.
Results from included studies also evaluated the impact of portal use on communication. Some suggest inpatient portal use may replace and/or facilitate verbal communication between patients, caregivers, and providers.35 In a pediatric study, 51% of parent portal users reported it gave them the information they needed, reducing the amount of questions they had for their healthcare team.33 Similarly 43% of 14 adult inpatient portal users in another study thought the portal could replace at least some face-to-face communication.37 Some providers indicated portal use enhanced rounding discussion quality.35 Another study suggested that patient-provider communication via electronic messaging may provide benefits for some patients and not others.37
Multiple studies evaluated patient, caregiver, and/or healthcare team perceptions of the impact of inpatient portal use on detection of errors and patient safety.29,31,33,35 In adult inpatients, 6% agreed portal use could help them find errors.29 In a pediatric study, 8% reported finding at least 1 medication error by using the portal, and 89% thought use reduced errors in their child’s care.33 One patient in a qualitative study of adult inpatients cited an example of a dosing error discovered by using the portal.37 Healthcare providers in another study also reported that use facilitated patient error identification.35
Included studies evaluated the potential impact of portal use on patient anxiety, confusion, and/or worry, and the work of healthcare teams. In 1 study, nurses voiced concerns about giving information subject to change or that couldn’t always be achieved because of competing hospital priorities, such as discharge timing.25 They also worried about giving medical information that would create cognitive overload for patients and/or require professional interpretation. Although providers in another study perceived little negative impact on their workflow after portal implementation, they worried about the potential of adding other information to the portal.35 For example, they were concerned that the future release of abnormal test results or sensitive data would lead to confusion and more time spent answering patient questions. Physicians also worried that secure messaging could be overused by patients, would be used to inappropriately express acute concerns, or might adversely affect verbal communication. Providers in 2 studies expressed concerns about potential negative implications of portal use on their work before implementation, which were subsequently reduced after portal implementation.29,38 Conversely, no parent portal users in another study thought portal information was confusing.33 One parent participant noted portal use may actually decrease anxiety: “Access to their medical information gives patients and their caregivers perspective and insight into their hospital care and empowers them with knowledge about [what is going on], which reduces anxiety.”37
DISCUSSION
We identified multiple studies evaluating the design, use, and impact of inpatient patient portals for hospitalized patients and caregivers. Based on the information needs identified by patients and healthcare team participants, multiple key content and design recommendations are suggested, including presenting (1) timely, personalized clinical and educational information in lay terms, (2) the care trajectory, including care plan and patient schedule, and (3) a way to recognize and communicate with the inpatient healthcare team. Design challenges still exist, such as translating medical terminology from EHRs into patient-friendly language, proxy access, and portal integration across transitions. Data from identified studies suggest hospitalized patients and caregivers are interested in and willing to use inpatient portals, but there is less information about the use of each functionality. Evidence supporting the role of inpatient portal use in improving patient and/or caregiver engagement, knowledge, communication, and the quality and safety of care is currently limited. Included studies indicate that healthcare team members had concerns about using portals to share clinical information and communicate electronically in the hospital. The extent to which these concerns translate to demonstrable problems remains to be seen.
Early studies focus on patient and caregiver information needs and portal interface design. Although the necessity for certain core functionalities and design requirements are becoming clear,20 best practices regarding the amount and timing of information released (eg, physician notes, lab results), optimal hardware decisions (eg, large-screen displays, hospital-owned tablets, bring-your-own-device model), and details around secure-messaging implementation in the acute hospital setting are still lacking. Future work is needed to understand optimal patient-provider communication architectures that support improved synchronous and asynchronous messaging and privacy-preserving approaches to the design of these systems to handle patient-generated data as it becomes more commonplace. Although patient participants in these studies were generally satisfied using inpatient portals, many indicated the need for even more transparency, such as the release of results in real time and inclusion of physician notes (even if they could not be fully comprehended).37 As the movement of sharing notes with patients in the ambulatory setting grows,39 it will inevitably extend to the inpatient setting.40 Further research is needed to understand the impact of increased transparency on health outcomes, patient anxiety, and inpatient healthcare team workload. Although the majority of studies described the design and/or use of custom portal platforms, EHR vendors are now developing inpatient portals that integrate into preexisting systems (eg, MyChart Bedside, Epic Systems). This will increase the likelihood of broad inpatient portal adoption and may facilitate multicenter trials evaluating the impact of their use.
The next steps will need to focus on the evaluation of specific inpatient portal functionalities and the impact of their use on objective process and outcome measures by using rigorous, experimental study designs. Akin to ambulatory portal research, measures of interest will include patient activation,41,42 patient and/or caregiver satisfaction,43 care processes (eg, length of stay, readmissions), and patient safety (eg, safety perceptions, adverse drug events, hospital-acquired conditions, and diagnostic errors). More than a mechanism for unidirectional sharing information from providers to the patient, inpatient portals will also provide a platform for the reciprocal exchange of information from the patient to the provider through patient-generated data, such as goal setting and feedback. Patients may play a larger role in reporting hospital satisfaction in real time, reconciling medications, contributing to the treatment plan, and identifying medical errors. As portals are integrated across the care continuum,20 our understanding of their impact may become more clear.
In this review, only 5 studies were conducted in the pediatric hospital setting.24,32-34,38 With hospitalized children experiencing 3 times more harm from medical errors than adults,44 engaging parents in inpatient care to improve safety has become a national priority.45 Giving patient portals, or “parent portals,” to parents of hospitalized children may provide a unique opportunity to share healthcare information and promote engagement, a direction for future study. There is also a research gap in evaluating adolescent inpatient portal use. Future portals may be designed to incentivize young children to learn about their hospitalization through games linked to health-related education.
Finally, as patients and caregivers begin using inpatient portals, there will almost certainly be consequences for healthcare teams. Understanding and anticipating human and work system factors influencing inpatient portal adoption and use from the perspectives of both patients and healthcare teams are needed.46,47 Engaging healthcare team members as valuable stakeholders during implementation and measuring the impact of portal use on their workload is necessary, especially as portal use spreads beyond pilot units. The success of inpatient portals is dependent upon both the positive benefits for patients and their acceptance by healthcare teams.48
Limitations exist in conducting a systematic literature review.49 The conceptual definition of a portal for hospitalized patients and patient/caregiver engagement is evolving; therefore, our definition may not have captured all relevant studies. We intentionally did not include all inpatient technology, as we were interested in a narrow definition of portals designed for inpatients that provided clinical information from the inpatient EHR. Because of rapid technology changes, we also limited our search to studies published within the last 10 years; prior literature has been described elsewhere.17 We excluded non-English language studies, limiting our ability to capture the full scope of inpatient portal research. These patients already experience healthcare delivery disparities, widened by the inaccessibility of innovative health information technologies.50 Future studies would be enhanced with the inclusion of these participants.
Inpatient portal research is in its infancy but growing rapidly. Studies to date are primarily focused on portal design and have small sample sizes. Early findings suggest that patients and caregivers are, in general, enthusiastic about using inpatient portals. Further research is needed, however, to determine the impact of inpatient portal use on patient engagement and hospital-care quality, safety, and cost.
Disclosure
This work was supported by a Department of Pediatrics Research and Development Grant at the University of Wisconsin School of Medicine and Public Health. This publication was also supported by the Clinical and Translational Science Award program through the National Center for Advancing Translational Sciences, grant UL1TR000427. Dr. Hoonakker’s involvement was also partially supported by the National Science Foundation, grant CMMI 1536987. Funding sources had no involvement in study design, analysis, or interpretation of data. The authors have no conflicts of interest to declare.
1. Stewart M, Brown JB, Donner A, et al. The impact of patient-centered care on outcomes. J Fam Pract. 2000;49(9):796-804. PubMed
2. Little P, Everitt H, Williamson I, et al. Observational study of effect of patient centredness and positive approach on outcomes of general practice consultations. BMJ. 2001;323(7318):908-911. PubMed
3. Maeng DD, Graf TR, Davis DE, Tomcavage J, Bloom FJ, Jr. Can a patient-centered medical home lead to better patient outcomes? The Quality Implications of Geisinger’s ProvenHealth Navigator. Am J Med Qual. 2012;27(3):210-216. PubMed
4. Joint Commision on Accreditation of Healthcare Organizations. Speak up: Prevent errors in your child’s care. http://www.jointcommission.org/Speak_Up_Prevent_Errors_in_Your_Childs_Care/. Accessed June 10, 2017.
5. Committee on Hospital Care and Institute for Patient and Family-centered Care. Patient- and family-centered care and the pediatrician’s role. Pediatrics. 2012;129(2):394-404. PubMed
6. Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001. PubMed
7. Coulter A. Engaging Patients in Healthcare. New York: McGraw-Hill Education; 2011. PubMed
8. Tang PC, Ash JS, Bates DW, Overhage JM, Sands DZ. Personal health records: definitions, benefits, and strategies for overcoming barriers to adoption. J Am Med Inform Assoc. 2006;13(2):121-126. PubMed
9. Schnipper JL, Gandhi TK, Wald JS, et al. Design and implementation of a web-based patient portal linked to an electronic health record designed to improve medication safety: the Patient Gateway medications module. Inform Prim Care. 2008;16(2):147-155. PubMed
10. Blumenthal D, Tavenner M. The “meaningful use” regulation for electronic health records. N Engl J Med. 2010;363(6):501-504. PubMed
11. Ammenwerth E, Schnell-Inderst P, Hoerbst A. The impact of electronic patient portals on patient care: a systematic review of controlled trials. J Med Internet Res. 2012;14(6):e162. PubMed
12. Goldzweig CL, Orshansky G, Paige NM, et al. Electronic patient portals: evidence on health utcomes, satisfaction, efficiency, and attitudes: a systematic review. Ann Intern Med. 2013;159(10):677-687. PubMed
13. Davis Giardina T, Menon S, Parrish DE, Sittig DF, Singh H. Patient access to medical records and healthcare outcomes: a systematic review. J Am Med Inform Assoc. 2014;21(4):737-741. PubMed
14. Kalra D, Fernando B. A review of the empirical evidence of the healthcare benefits of personal health records. Yearb Med Inform. 2013;8(1):93-102. PubMed
15. Kruse CS, Bolton K, Freriks G. The effect of patient portals on quality outcomes and its implications to meaningful use: a systematic review. J Med Internet Res. 2015;17(2):e44. PubMed
16. Vawdrey DK, Wilcox LG, Collins SA, et al. A tablet computer application for patients to participate in their hospital care. AMIA Annu Symp Proc. 2011:1428-1435. PubMed
17. Prey JE, Woollen J, Wilcox L, et al. Patient engagement in the inpatient setting: a systematic review. J Am Med Inform Assoc. 2014;21(4):742-750. PubMed
18. O’Leary KJ, Lohman ME, Culver E, et al. The effect of tablet computers with a mobile patient portal application on hospitalized patients’ knowledge and activation. J Am Med Inform Assoc. 2016;23(1):159-165. PubMed
19. Skeels M, Tan DS. Identifying opportunities for inpatient-centric technology. Proceedings of the 1st ACM International Health Informatics Symposium. Arlington: ACM; 2010:580-589.
20. Collins SA, Rozenblum R, Leung WY, et al. Acute care patient portals: a qualitative study of stakeholder perspectives on current practices. J Am Med Inform Assoc. 2017;24(e1):e9-e17. PubMed
21. Morris D, Karlson A. Dynamic Accessibility Requirements for Hospital Patients. SIGCHI Conference on Human Factors in Computing Systems. Vancouver, BC, Canada: ACM; 2011.
22. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. PubMed
23. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
24. Weyand SA, Frize M, Bariciak E, Dunn S. Development and usability testing of a parent decision support tool for the neonatal intensive care unit. Conf Proc IEEE Eng Med Biol Soc. 2011:6430-6433. PubMed
25. Caligtan CA, Carroll DL, Hurley AC, Gersh-Zaremski R, Dykes PC. Bedside information technology to support patient-centered care. Int J Med Inform. 2012;81(7):442-451. PubMed
26. Wilcox L, Feiner S, Liu A, Restaino S, Collins S, Vawdrey D. Designing inpatient technology to meet the medication information needs of cardiology patients. Proceedings of the 2nd ACM SIGHIT International Health Informatics Symposium. Miami: ACM; 2012:831-836. PubMed
27. Dykes PC, Carroll DL, Hurley AC, et al. Building and testing a patient-centric electronic bedside communication center. J Gerontol Nurs. 2013;39(1):15-19. PubMed
28. Dykes PC, Stade D, Chang F, et al. Participatory design and development of a patient-centered toolkit to engage hospitalized patients and care partners in their plan of care. AMIA Annu Symp Proc. 2014:486-495. PubMed
29. Pell JM, Mancuso M, Limon S, Oman K, Lin CT. Patient access to electronic health records during hospitalization. JAMA Intern Med. 2015;175(5):856-858. PubMed
30. Yoo S, Lee KH, Baek H, et al. Development and user research of a smart bedside station system toward patient-centered healthcare system. J Med Syst. 2015;39(9):86. PubMed
31. Dalal AK, Dykes PC, Collins S, et al. A web-based, patient-centered toolkit to engage patients and caregivers in the acute care setting: a preliminary evaluation. J Am Med Inform Assoc. 2016;23(1):80-87. PubMed
32. Kaziunas E, Hanauer DA, Ackerman MS, Choi SW. Identifying unmet informational needs in the inpatient setting to increase patient and caregiver engagement in the context of pediatric hematopoietic stem cell transplantation. J Am Med Inform Assoc. 2016;23(1):94-104. PubMed
33. Kelly MM, Hoonakker PLT, Dean SM. Using an inpatient portal to engage families in pediatric hospital care. J Am Med Inform Assoc. 2016;24(1):153-161. PubMed
34. Maher M, Kaziunas E, Ackerman M, et al. User-centered design groups to engage patients and caregivers with a personalized health information technology tool. Biol Blood Marrow Transplant. 2016;22(2):349-358. PubMed
35. O’Leary KJ, Sharma RK, Killarney A, et al. Patients’ and healthcare providers’ perceptions of a mobile portal application for hospitalized patients. BMC Med Inform Decis Mak. 2016;16(1):123-130. PubMed
36. Wilcox L, Woollen J, Prey J, et al. Interactive tools for inpatient medication tracking: a multi-phase study with cardiothoracic surgery patients. J Am Med Inform Assoc. 2016;23(1):144-158. PubMed
37. Woollen J, Prey J, Wilcox L, et al. Patient experiences using an inpatient personal health record. Appl Clin Inform. 2016;7(2):446-460. PubMed
38. Kelly MM, Dean SM, Carayon P, Wetterneck TB, Hoonakker PLT. Healthcare team perceptions of a portal for parents of hospitalized children before and after implementation. Appl Clin Inform. 2017;8(1):265-278. PubMed
39. Wolff JL, Darer JD, Berger A, et al. Inviting patients and care partners to read doctors’ notes: OpenNotes and shared access to electronic medical records. J Am Med Inform Assoc. 2017;24(e1):e166-e172. PubMed
40. Feldman HJ, Walker J, Li J, Delbanco T. OpenNotes:hospitalists’ challenge and opportunity. J Hosp Med. 2013;8(7):414-417. PubMed
41. Hibbard JH, Stockard J, Mahoney ER, Tusler M. Development of the Patient Activation Measure (PAM): conceptualizing and measuring activation in patients and consumers. Health Serv Res. 2004;39(4 Pt 1):1005-1026. PubMed
42. Prey JE, Qian M, Restaino S, et al. Reliability and validity of the patient activation measure in hospitalized patients. Patient Educ Couns. 2016;99(12):2026-2033. PubMed
43. Toomey SL, Zaslavsky AM, Elliott MN, et al. The development of a pediatric inpatient experience of care measure: Child HCAHPS. Pediatrics. 2015;136(2):360-369. PubMed
44. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285(16):2114-2120. PubMed
45. Agency for Healthcare Research and Quality. 20 Tips to help prevent medical errors in children. Secondary 20 Tips to help prevent medical errors in children. http://www.ahrq.gov/patients-consumers/care-planning/errors/20tips/index.html. Accessed on June 10, 2017.
46. Thompson MJ, Reilly JD, Valdez RS. Work system barriers to patient, provider, and caregiver use of personal health records: A systematic review. Appl Ergon. 2016;54:218-242. PubMed
47. Holden RJ, Carayon P, Gurses AP, et al. SEIPS 2.0: a human factors framework for studying and improving the work of healthcare professionals and patients. Ergonomics. 2013;56(11):1669-1686. PubMed
48. Gagnon MP, Ngangue P, Payne-Gagnon J, Desmartis M. m-Health adoption by healthcare professionals: a systematic review. J Am Med Inform Assoc. 2016;23(1):212-220. PubMed
49. Russell CL. An overview of the integrative research review. Prog Transplant. 2005;15(1):8-13. PubMed
50. Yamin CK, Emani S, Williams DH, et al. The digital divide in adoption and use of a personal health record. Arch Intern Med. 2011;171(6):568-574. PubMed
Engaging patients and their caregivers in care improves health outcomes1-3 and is endorsed by leading healthcare organizations as essential to improving care quality and safety.4-6 Patient engagement emphasizes that patients, caregivers, and healthcare providers work together to “promote and support active patient and public involvement in health and healthcare and to strengthen their influence on healthcare decisions.”7 Patient portals, web-based personal health records linked to electronic health record (EHR) data, are intended to promote engagement by providing patients and their caregivers with timely electronic access to their healthcare information and supporting communication through secure messaging with their healthcare team.8 The use of patient portals has also been suggested as a way for patients and/or caregivers to identify and intercept medical errors, thus having the potential to also improve patient safety.8,9
As a requirement for meaningful use, access to health information through patient portals in the ambulatory setting has increased dramatically.10 Studies evaluating the use of these patient portals to promote patient-centered care are growing, but evidence supporting their impact on improved health outcomes is currently insufficient.11-15 Although research and policy focus on the use of patient portals in the ambulatory setting, recent literature suggests that patient portals may be used to share inpatient clinical information to engage patients and their caregivers during their hospitalization.16-18 Before the widespread use of patient portals in the inpatient setting is endorsed, systematic research is needed to understand optimal portal design requirements, if and how these portals are used, and whether their use provides value to the hospitalized patient and/or caregiver.8
Prior literature summarized early findings regarding the use of various technologies designed to engage hospitalized patients.17,19,20 In this systematic review, we describe the emerging literature examining the design, use, and impact of inpatient portals for hospitalized patients and/or caregivers over the last 10 years. Inpatient portals are defined here as electronic patient portals tethered to EHRs that are designed to provide hospitalized patients and/or caregivers secure access to personalized, inpatient clinical information with the intent of engaging them in their hospital care. After analyzing and summarizing these data, we then identify knowledge gaps and potential future research directions.
METHODS
Search Strategy, Study Selection, and Analysis
This systematic review included available, peer-reviewed, and grey literature published from January 1, 2006, to August 8, 2017, in PubMed, Web of Science (including the Institute of Electrical and Electronics Engineers Xplore), Cochrane, CINAHLPlus, and Scopus databases. Terms and phrases, including those found in the Medical Subject Heading (MeSH) index, were used to identify studies evaluating (1) patient portals (“health record, personal [MeSH],” “personal health record,” “patient portal,” “inpatient portal,” “ipad,” “tablet,” or “bedside information technology”), (2) engagement (“engagement,” “empowerment,” “participation,” “activation,” or “self-efficacy”), and (3) in the hospital (“inpatient [MeSH],” “hospital [MeSH],” “hospitalized patient [MeSH],” or “unit”). MeSH terms were used when applicable. Based on previous literature, free-text terms were also used when subject headings were not applied consistently, such as with terms related to engagement.17,21 Studies were excluded if they were not written in English, if they evaluated portals exclusively in the emergency department or ambulatory setting, and/or if they described future study protocols. Studies describing general inpatient technology or evaluating portals used in the hospital but not tethered to inpatient EHR clinical data were also excluded.
By using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines,22 2 researchers (M.K. and P.H.) completed the literature search and potential article screening. Results were aggregated and studies were screened and excluded from full review based on title and abstract information. Additional studies were included after reference list review. During a full review of included studies, 2 researchers independently extracted data, including the study objective, design, setting, sample, data collection instruments, outcomes, and a description of results. Guided by our study objective, findings were reconciled by consensus and analyzed and described according to the following 3 themes: (1) inpatient portal design, (2) inpatient portal use and usability, and (3) the impact of inpatient portal use on patient or caregiver and healthcare team outcomes as defined by retrieved studies.
The quality of studies was evaluated by the same 2 researchers independently by using the Downs and Black checklist for assessing the methodological quality of randomized and nonrandomized healthcare interventions.23 Qualitative studies describing the development of portal prototypes and/or portal redesign efforts were excluded from these analyses. Discrepancies were resolved by consensus.Because of the wide variability in study designs, populations, and outcomes, a meta-analysis of pooled data was not performed.
RESULTS
Of the 731 studies identified through database searching and reference review, 36 were included for full-text review and 17 met inclusion criteria (Figure; Table 1). Studies excluded after full-text review described portal use outside of the inpatient setting, portals not linked to hospital EHR clinical data, portals not designed for inpatients, and/or inpatient technology in general. The inpatient portal platforms, hardware used, and functionalities varied within included studies (Table 2). The majority of studies used custom, web-based inpatient portal applications on tablet computers. Most provided information about the patients’ hospital medications, healthcare team, and education about their condition and/or a medical glossary. Many included the patient’s schedule, hospital problem list, discharge information, and a way to keep notes.
There has been a recent increase in inpatient portal study publication, with 9 studies published during or after 2016. Five were conducted in the pediatric setting and all but 130 with English-speaking participants. Twelve studies were qualitative, many of which were conducted in multiple phases by using semi-structured interviews and/or focus groups to develop or redesign inpatient portals. Of the remaining studies, 3 used a cross-sectional design, 1 used a before and after design without a control group, and 1 was a nonrandomized trial. Studies were rated as having medium-to-high risk of bias because of design flaws (Table 1 in supplementary Appendix). Because many studies were small pilot studies and all were single-centered studies, the generalizability of findings to different healthcare settings or patient populations is limited.
Inpatient Portal Design
Most included studies evaluated patient and/or caregiver information needs to design and/or enhance inpatient portals.16,24-37 In 1 study, patients described an overall lack of information provided in the hospital and insufficient time to understand and remember information, which, when shared, was often presented by using medical terminology.30 They wanted information to help them understand their daily hospital routine, confirm and compare medications and test results, learn about care, and prepare for discharge. Participants in multiple studies echoed these results, indicating the need for a schedule of upcoming clinical events (eg, medication administration, procedures, imaging), secure and timely clinical information (eg, list of diagnoses and medications, test results), personalized education, a medical glossary, discharge information, and a way to take notes and recognize and communicate with providers.
Patients also requested further information transparency,34,37 including physicians’ notes, radiology results, operative reports, and billing information, along with general hospital information,16 meal ordering,33 and video conferencing.27 ln designing and refining an inpatient medication-tracking tool, participants identified the need for information about medication dosage, frequency, timing, administration method, criticality, alternative medications or forms, and education.26,36 Patients and/or caregivers also indicated interest in communicating with inpatient providers by using the portal.16,27,28,30-37 In 1 study, patients highlighted the need to be involved in care plan development,27 which led to portal refinement to allow for patient-generated data entry, including care goals and a way to communicate real-time concerns and feedback.28
Studies also considered healthcare team perspectives to inform portal design.25,26,28,30,35,37 Although information needs usually overlapped, patient and healthcare team priorities differed in some areas. Although patients wanted to “know what was going to happen to them,” nurses in 1 study were more concerned about providing information to protect patients, such as safety and precaution materials.25 Similarly, when designing a medication-tracking tool, patients sought information that helped them understand what to expect, while pharmacists focused on medication safety and providing information that fit their workflow (eg, abstract medication schedules).36
Identified study data raised important portal interface design considerations. Results suggested clinical data should be presented by using simple displays,28 accommodating real-time information. Participants recommended links16,29 to personalized patient-friendly37 education accessed with minimal steps.26 Interfaces may be personalized for target users, such as patient or proxy and younger or older individuals. For example, older patients reported less familiarity with touch screens, internal keyboards, and handwriting recognition, favoring voice recognition for recording notes.27 This raised questions about how portals can be designed to best maintain patient privacy.25 Interface design, such as navigation, also relied heavily on hardware choice, such as tablet versus mobile phone.28
Inpatient Portal Use and Usability
Most patient and/or caregiver participants in included studies were interested in using an inpatient portal, used it when offered, found it easy to use, useful, and/or were satisfied with it.16,18,24-37 Most used and liked functionalities that provided healthcare team, test result, and medication information.22,33,37 In the 1 identified controlled trial,18 researchers evaluated an inpatient portal given to adult inpatients that included a problem list, schedule, medication list, and healthcare team information. Of the intervention unit patients, 80% used the portal, 76% indicated it was easy to use, and 71% thought it provided useful information. When a portal was given to 239 adult patients and caregivers in another study, 66% sent a total of 291 messages to the healthcare team.31 Of these, 153 provided feedback, 76 expressed preferences, and 16 communicated concerns. In a pediatric study, an inpatient portal was given to 296 parents who sent a total of 36 messages and 176 requests.33 Messages sent included information regarding caregiver needs, questions, updates, and/or positive endorsements of the healthcare team and/or care.
Impact of Inpatient Portal Use
Multiple studies evaluated the impact of inpatient portal use on patient and/or caregiver engagement, empowerment, activation, and/or knowledge, which had mixed results. Most adult patients interviewed in one study had positive experiences using a portal to answer their questions between physician visits and learn about, remember, and engage in care.37 A majority of adult inpatient portal users in another study agreed that portal use helped them feel in control and understand their condition; however, they did not report having improved discharge timing knowledge.29 In a pediatric study, most parent inpatient portal users agreed use improved their ability to monitor, understand, and make decisions about their child’s care.33 In the controlled trial,18 a higher percentage of portal intervention patients could identify their physician or role; however, patient activation was not statistically different between intervention and control patients.
Results from included studies also evaluated the impact of portal use on communication. Some suggest inpatient portal use may replace and/or facilitate verbal communication between patients, caregivers, and providers.35 In a pediatric study, 51% of parent portal users reported it gave them the information they needed, reducing the amount of questions they had for their healthcare team.33 Similarly 43% of 14 adult inpatient portal users in another study thought the portal could replace at least some face-to-face communication.37 Some providers indicated portal use enhanced rounding discussion quality.35 Another study suggested that patient-provider communication via electronic messaging may provide benefits for some patients and not others.37
Multiple studies evaluated patient, caregiver, and/or healthcare team perceptions of the impact of inpatient portal use on detection of errors and patient safety.29,31,33,35 In adult inpatients, 6% agreed portal use could help them find errors.29 In a pediatric study, 8% reported finding at least 1 medication error by using the portal, and 89% thought use reduced errors in their child’s care.33 One patient in a qualitative study of adult inpatients cited an example of a dosing error discovered by using the portal.37 Healthcare providers in another study also reported that use facilitated patient error identification.35
Included studies evaluated the potential impact of portal use on patient anxiety, confusion, and/or worry, and the work of healthcare teams. In 1 study, nurses voiced concerns about giving information subject to change or that couldn’t always be achieved because of competing hospital priorities, such as discharge timing.25 They also worried about giving medical information that would create cognitive overload for patients and/or require professional interpretation. Although providers in another study perceived little negative impact on their workflow after portal implementation, they worried about the potential of adding other information to the portal.35 For example, they were concerned that the future release of abnormal test results or sensitive data would lead to confusion and more time spent answering patient questions. Physicians also worried that secure messaging could be overused by patients, would be used to inappropriately express acute concerns, or might adversely affect verbal communication. Providers in 2 studies expressed concerns about potential negative implications of portal use on their work before implementation, which were subsequently reduced after portal implementation.29,38 Conversely, no parent portal users in another study thought portal information was confusing.33 One parent participant noted portal use may actually decrease anxiety: “Access to their medical information gives patients and their caregivers perspective and insight into their hospital care and empowers them with knowledge about [what is going on], which reduces anxiety.”37
DISCUSSION
We identified multiple studies evaluating the design, use, and impact of inpatient patient portals for hospitalized patients and caregivers. Based on the information needs identified by patients and healthcare team participants, multiple key content and design recommendations are suggested, including presenting (1) timely, personalized clinical and educational information in lay terms, (2) the care trajectory, including care plan and patient schedule, and (3) a way to recognize and communicate with the inpatient healthcare team. Design challenges still exist, such as translating medical terminology from EHRs into patient-friendly language, proxy access, and portal integration across transitions. Data from identified studies suggest hospitalized patients and caregivers are interested in and willing to use inpatient portals, but there is less information about the use of each functionality. Evidence supporting the role of inpatient portal use in improving patient and/or caregiver engagement, knowledge, communication, and the quality and safety of care is currently limited. Included studies indicate that healthcare team members had concerns about using portals to share clinical information and communicate electronically in the hospital. The extent to which these concerns translate to demonstrable problems remains to be seen.
Early studies focus on patient and caregiver information needs and portal interface design. Although the necessity for certain core functionalities and design requirements are becoming clear,20 best practices regarding the amount and timing of information released (eg, physician notes, lab results), optimal hardware decisions (eg, large-screen displays, hospital-owned tablets, bring-your-own-device model), and details around secure-messaging implementation in the acute hospital setting are still lacking. Future work is needed to understand optimal patient-provider communication architectures that support improved synchronous and asynchronous messaging and privacy-preserving approaches to the design of these systems to handle patient-generated data as it becomes more commonplace. Although patient participants in these studies were generally satisfied using inpatient portals, many indicated the need for even more transparency, such as the release of results in real time and inclusion of physician notes (even if they could not be fully comprehended).37 As the movement of sharing notes with patients in the ambulatory setting grows,39 it will inevitably extend to the inpatient setting.40 Further research is needed to understand the impact of increased transparency on health outcomes, patient anxiety, and inpatient healthcare team workload. Although the majority of studies described the design and/or use of custom portal platforms, EHR vendors are now developing inpatient portals that integrate into preexisting systems (eg, MyChart Bedside, Epic Systems). This will increase the likelihood of broad inpatient portal adoption and may facilitate multicenter trials evaluating the impact of their use.
The next steps will need to focus on the evaluation of specific inpatient portal functionalities and the impact of their use on objective process and outcome measures by using rigorous, experimental study designs. Akin to ambulatory portal research, measures of interest will include patient activation,41,42 patient and/or caregiver satisfaction,43 care processes (eg, length of stay, readmissions), and patient safety (eg, safety perceptions, adverse drug events, hospital-acquired conditions, and diagnostic errors). More than a mechanism for unidirectional sharing information from providers to the patient, inpatient portals will also provide a platform for the reciprocal exchange of information from the patient to the provider through patient-generated data, such as goal setting and feedback. Patients may play a larger role in reporting hospital satisfaction in real time, reconciling medications, contributing to the treatment plan, and identifying medical errors. As portals are integrated across the care continuum,20 our understanding of their impact may become more clear.
In this review, only 5 studies were conducted in the pediatric hospital setting.24,32-34,38 With hospitalized children experiencing 3 times more harm from medical errors than adults,44 engaging parents in inpatient care to improve safety has become a national priority.45 Giving patient portals, or “parent portals,” to parents of hospitalized children may provide a unique opportunity to share healthcare information and promote engagement, a direction for future study. There is also a research gap in evaluating adolescent inpatient portal use. Future portals may be designed to incentivize young children to learn about their hospitalization through games linked to health-related education.
Finally, as patients and caregivers begin using inpatient portals, there will almost certainly be consequences for healthcare teams. Understanding and anticipating human and work system factors influencing inpatient portal adoption and use from the perspectives of both patients and healthcare teams are needed.46,47 Engaging healthcare team members as valuable stakeholders during implementation and measuring the impact of portal use on their workload is necessary, especially as portal use spreads beyond pilot units. The success of inpatient portals is dependent upon both the positive benefits for patients and their acceptance by healthcare teams.48
Limitations exist in conducting a systematic literature review.49 The conceptual definition of a portal for hospitalized patients and patient/caregiver engagement is evolving; therefore, our definition may not have captured all relevant studies. We intentionally did not include all inpatient technology, as we were interested in a narrow definition of portals designed for inpatients that provided clinical information from the inpatient EHR. Because of rapid technology changes, we also limited our search to studies published within the last 10 years; prior literature has been described elsewhere.17 We excluded non-English language studies, limiting our ability to capture the full scope of inpatient portal research. These patients already experience healthcare delivery disparities, widened by the inaccessibility of innovative health information technologies.50 Future studies would be enhanced with the inclusion of these participants.
Inpatient portal research is in its infancy but growing rapidly. Studies to date are primarily focused on portal design and have small sample sizes. Early findings suggest that patients and caregivers are, in general, enthusiastic about using inpatient portals. Further research is needed, however, to determine the impact of inpatient portal use on patient engagement and hospital-care quality, safety, and cost.
Disclosure
This work was supported by a Department of Pediatrics Research and Development Grant at the University of Wisconsin School of Medicine and Public Health. This publication was also supported by the Clinical and Translational Science Award program through the National Center for Advancing Translational Sciences, grant UL1TR000427. Dr. Hoonakker’s involvement was also partially supported by the National Science Foundation, grant CMMI 1536987. Funding sources had no involvement in study design, analysis, or interpretation of data. The authors have no conflicts of interest to declare.
Engaging patients and their caregivers in care improves health outcomes1-3 and is endorsed by leading healthcare organizations as essential to improving care quality and safety.4-6 Patient engagement emphasizes that patients, caregivers, and healthcare providers work together to “promote and support active patient and public involvement in health and healthcare and to strengthen their influence on healthcare decisions.”7 Patient portals, web-based personal health records linked to electronic health record (EHR) data, are intended to promote engagement by providing patients and their caregivers with timely electronic access to their healthcare information and supporting communication through secure messaging with their healthcare team.8 The use of patient portals has also been suggested as a way for patients and/or caregivers to identify and intercept medical errors, thus having the potential to also improve patient safety.8,9
As a requirement for meaningful use, access to health information through patient portals in the ambulatory setting has increased dramatically.10 Studies evaluating the use of these patient portals to promote patient-centered care are growing, but evidence supporting their impact on improved health outcomes is currently insufficient.11-15 Although research and policy focus on the use of patient portals in the ambulatory setting, recent literature suggests that patient portals may be used to share inpatient clinical information to engage patients and their caregivers during their hospitalization.16-18 Before the widespread use of patient portals in the inpatient setting is endorsed, systematic research is needed to understand optimal portal design requirements, if and how these portals are used, and whether their use provides value to the hospitalized patient and/or caregiver.8
Prior literature summarized early findings regarding the use of various technologies designed to engage hospitalized patients.17,19,20 In this systematic review, we describe the emerging literature examining the design, use, and impact of inpatient portals for hospitalized patients and/or caregivers over the last 10 years. Inpatient portals are defined here as electronic patient portals tethered to EHRs that are designed to provide hospitalized patients and/or caregivers secure access to personalized, inpatient clinical information with the intent of engaging them in their hospital care. After analyzing and summarizing these data, we then identify knowledge gaps and potential future research directions.
METHODS
Search Strategy, Study Selection, and Analysis
This systematic review included available, peer-reviewed, and grey literature published from January 1, 2006, to August 8, 2017, in PubMed, Web of Science (including the Institute of Electrical and Electronics Engineers Xplore), Cochrane, CINAHLPlus, and Scopus databases. Terms and phrases, including those found in the Medical Subject Heading (MeSH) index, were used to identify studies evaluating (1) patient portals (“health record, personal [MeSH],” “personal health record,” “patient portal,” “inpatient portal,” “ipad,” “tablet,” or “bedside information technology”), (2) engagement (“engagement,” “empowerment,” “participation,” “activation,” or “self-efficacy”), and (3) in the hospital (“inpatient [MeSH],” “hospital [MeSH],” “hospitalized patient [MeSH],” or “unit”). MeSH terms were used when applicable. Based on previous literature, free-text terms were also used when subject headings were not applied consistently, such as with terms related to engagement.17,21 Studies were excluded if they were not written in English, if they evaluated portals exclusively in the emergency department or ambulatory setting, and/or if they described future study protocols. Studies describing general inpatient technology or evaluating portals used in the hospital but not tethered to inpatient EHR clinical data were also excluded.
By using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines,22 2 researchers (M.K. and P.H.) completed the literature search and potential article screening. Results were aggregated and studies were screened and excluded from full review based on title and abstract information. Additional studies were included after reference list review. During a full review of included studies, 2 researchers independently extracted data, including the study objective, design, setting, sample, data collection instruments, outcomes, and a description of results. Guided by our study objective, findings were reconciled by consensus and analyzed and described according to the following 3 themes: (1) inpatient portal design, (2) inpatient portal use and usability, and (3) the impact of inpatient portal use on patient or caregiver and healthcare team outcomes as defined by retrieved studies.
The quality of studies was evaluated by the same 2 researchers independently by using the Downs and Black checklist for assessing the methodological quality of randomized and nonrandomized healthcare interventions.23 Qualitative studies describing the development of portal prototypes and/or portal redesign efforts were excluded from these analyses. Discrepancies were resolved by consensus.Because of the wide variability in study designs, populations, and outcomes, a meta-analysis of pooled data was not performed.
RESULTS
Of the 731 studies identified through database searching and reference review, 36 were included for full-text review and 17 met inclusion criteria (Figure; Table 1). Studies excluded after full-text review described portal use outside of the inpatient setting, portals not linked to hospital EHR clinical data, portals not designed for inpatients, and/or inpatient technology in general. The inpatient portal platforms, hardware used, and functionalities varied within included studies (Table 2). The majority of studies used custom, web-based inpatient portal applications on tablet computers. Most provided information about the patients’ hospital medications, healthcare team, and education about their condition and/or a medical glossary. Many included the patient’s schedule, hospital problem list, discharge information, and a way to keep notes.
There has been a recent increase in inpatient portal study publication, with 9 studies published during or after 2016. Five were conducted in the pediatric setting and all but 130 with English-speaking participants. Twelve studies were qualitative, many of which were conducted in multiple phases by using semi-structured interviews and/or focus groups to develop or redesign inpatient portals. Of the remaining studies, 3 used a cross-sectional design, 1 used a before and after design without a control group, and 1 was a nonrandomized trial. Studies were rated as having medium-to-high risk of bias because of design flaws (Table 1 in supplementary Appendix). Because many studies were small pilot studies and all were single-centered studies, the generalizability of findings to different healthcare settings or patient populations is limited.
Inpatient Portal Design
Most included studies evaluated patient and/or caregiver information needs to design and/or enhance inpatient portals.16,24-37 In 1 study, patients described an overall lack of information provided in the hospital and insufficient time to understand and remember information, which, when shared, was often presented by using medical terminology.30 They wanted information to help them understand their daily hospital routine, confirm and compare medications and test results, learn about care, and prepare for discharge. Participants in multiple studies echoed these results, indicating the need for a schedule of upcoming clinical events (eg, medication administration, procedures, imaging), secure and timely clinical information (eg, list of diagnoses and medications, test results), personalized education, a medical glossary, discharge information, and a way to take notes and recognize and communicate with providers.
Patients also requested further information transparency,34,37 including physicians’ notes, radiology results, operative reports, and billing information, along with general hospital information,16 meal ordering,33 and video conferencing.27 ln designing and refining an inpatient medication-tracking tool, participants identified the need for information about medication dosage, frequency, timing, administration method, criticality, alternative medications or forms, and education.26,36 Patients and/or caregivers also indicated interest in communicating with inpatient providers by using the portal.16,27,28,30-37 In 1 study, patients highlighted the need to be involved in care plan development,27 which led to portal refinement to allow for patient-generated data entry, including care goals and a way to communicate real-time concerns and feedback.28
Studies also considered healthcare team perspectives to inform portal design.25,26,28,30,35,37 Although information needs usually overlapped, patient and healthcare team priorities differed in some areas. Although patients wanted to “know what was going to happen to them,” nurses in 1 study were more concerned about providing information to protect patients, such as safety and precaution materials.25 Similarly, when designing a medication-tracking tool, patients sought information that helped them understand what to expect, while pharmacists focused on medication safety and providing information that fit their workflow (eg, abstract medication schedules).36
Identified study data raised important portal interface design considerations. Results suggested clinical data should be presented by using simple displays,28 accommodating real-time information. Participants recommended links16,29 to personalized patient-friendly37 education accessed with minimal steps.26 Interfaces may be personalized for target users, such as patient or proxy and younger or older individuals. For example, older patients reported less familiarity with touch screens, internal keyboards, and handwriting recognition, favoring voice recognition for recording notes.27 This raised questions about how portals can be designed to best maintain patient privacy.25 Interface design, such as navigation, also relied heavily on hardware choice, such as tablet versus mobile phone.28
Inpatient Portal Use and Usability
Most patient and/or caregiver participants in included studies were interested in using an inpatient portal, used it when offered, found it easy to use, useful, and/or were satisfied with it.16,18,24-37 Most used and liked functionalities that provided healthcare team, test result, and medication information.22,33,37 In the 1 identified controlled trial,18 researchers evaluated an inpatient portal given to adult inpatients that included a problem list, schedule, medication list, and healthcare team information. Of the intervention unit patients, 80% used the portal, 76% indicated it was easy to use, and 71% thought it provided useful information. When a portal was given to 239 adult patients and caregivers in another study, 66% sent a total of 291 messages to the healthcare team.31 Of these, 153 provided feedback, 76 expressed preferences, and 16 communicated concerns. In a pediatric study, an inpatient portal was given to 296 parents who sent a total of 36 messages and 176 requests.33 Messages sent included information regarding caregiver needs, questions, updates, and/or positive endorsements of the healthcare team and/or care.
Impact of Inpatient Portal Use
Multiple studies evaluated the impact of inpatient portal use on patient and/or caregiver engagement, empowerment, activation, and/or knowledge, which had mixed results. Most adult patients interviewed in one study had positive experiences using a portal to answer their questions between physician visits and learn about, remember, and engage in care.37 A majority of adult inpatient portal users in another study agreed that portal use helped them feel in control and understand their condition; however, they did not report having improved discharge timing knowledge.29 In a pediatric study, most parent inpatient portal users agreed use improved their ability to monitor, understand, and make decisions about their child’s care.33 In the controlled trial,18 a higher percentage of portal intervention patients could identify their physician or role; however, patient activation was not statistically different between intervention and control patients.
Results from included studies also evaluated the impact of portal use on communication. Some suggest inpatient portal use may replace and/or facilitate verbal communication between patients, caregivers, and providers.35 In a pediatric study, 51% of parent portal users reported it gave them the information they needed, reducing the amount of questions they had for their healthcare team.33 Similarly 43% of 14 adult inpatient portal users in another study thought the portal could replace at least some face-to-face communication.37 Some providers indicated portal use enhanced rounding discussion quality.35 Another study suggested that patient-provider communication via electronic messaging may provide benefits for some patients and not others.37
Multiple studies evaluated patient, caregiver, and/or healthcare team perceptions of the impact of inpatient portal use on detection of errors and patient safety.29,31,33,35 In adult inpatients, 6% agreed portal use could help them find errors.29 In a pediatric study, 8% reported finding at least 1 medication error by using the portal, and 89% thought use reduced errors in their child’s care.33 One patient in a qualitative study of adult inpatients cited an example of a dosing error discovered by using the portal.37 Healthcare providers in another study also reported that use facilitated patient error identification.35
Included studies evaluated the potential impact of portal use on patient anxiety, confusion, and/or worry, and the work of healthcare teams. In 1 study, nurses voiced concerns about giving information subject to change or that couldn’t always be achieved because of competing hospital priorities, such as discharge timing.25 They also worried about giving medical information that would create cognitive overload for patients and/or require professional interpretation. Although providers in another study perceived little negative impact on their workflow after portal implementation, they worried about the potential of adding other information to the portal.35 For example, they were concerned that the future release of abnormal test results or sensitive data would lead to confusion and more time spent answering patient questions. Physicians also worried that secure messaging could be overused by patients, would be used to inappropriately express acute concerns, or might adversely affect verbal communication. Providers in 2 studies expressed concerns about potential negative implications of portal use on their work before implementation, which were subsequently reduced after portal implementation.29,38 Conversely, no parent portal users in another study thought portal information was confusing.33 One parent participant noted portal use may actually decrease anxiety: “Access to their medical information gives patients and their caregivers perspective and insight into their hospital care and empowers them with knowledge about [what is going on], which reduces anxiety.”37
DISCUSSION
We identified multiple studies evaluating the design, use, and impact of inpatient patient portals for hospitalized patients and caregivers. Based on the information needs identified by patients and healthcare team participants, multiple key content and design recommendations are suggested, including presenting (1) timely, personalized clinical and educational information in lay terms, (2) the care trajectory, including care plan and patient schedule, and (3) a way to recognize and communicate with the inpatient healthcare team. Design challenges still exist, such as translating medical terminology from EHRs into patient-friendly language, proxy access, and portal integration across transitions. Data from identified studies suggest hospitalized patients and caregivers are interested in and willing to use inpatient portals, but there is less information about the use of each functionality. Evidence supporting the role of inpatient portal use in improving patient and/or caregiver engagement, knowledge, communication, and the quality and safety of care is currently limited. Included studies indicate that healthcare team members had concerns about using portals to share clinical information and communicate electronically in the hospital. The extent to which these concerns translate to demonstrable problems remains to be seen.
Early studies focus on patient and caregiver information needs and portal interface design. Although the necessity for certain core functionalities and design requirements are becoming clear,20 best practices regarding the amount and timing of information released (eg, physician notes, lab results), optimal hardware decisions (eg, large-screen displays, hospital-owned tablets, bring-your-own-device model), and details around secure-messaging implementation in the acute hospital setting are still lacking. Future work is needed to understand optimal patient-provider communication architectures that support improved synchronous and asynchronous messaging and privacy-preserving approaches to the design of these systems to handle patient-generated data as it becomes more commonplace. Although patient participants in these studies were generally satisfied using inpatient portals, many indicated the need for even more transparency, such as the release of results in real time and inclusion of physician notes (even if they could not be fully comprehended).37 As the movement of sharing notes with patients in the ambulatory setting grows,39 it will inevitably extend to the inpatient setting.40 Further research is needed to understand the impact of increased transparency on health outcomes, patient anxiety, and inpatient healthcare team workload. Although the majority of studies described the design and/or use of custom portal platforms, EHR vendors are now developing inpatient portals that integrate into preexisting systems (eg, MyChart Bedside, Epic Systems). This will increase the likelihood of broad inpatient portal adoption and may facilitate multicenter trials evaluating the impact of their use.
The next steps will need to focus on the evaluation of specific inpatient portal functionalities and the impact of their use on objective process and outcome measures by using rigorous, experimental study designs. Akin to ambulatory portal research, measures of interest will include patient activation,41,42 patient and/or caregiver satisfaction,43 care processes (eg, length of stay, readmissions), and patient safety (eg, safety perceptions, adverse drug events, hospital-acquired conditions, and diagnostic errors). More than a mechanism for unidirectional sharing information from providers to the patient, inpatient portals will also provide a platform for the reciprocal exchange of information from the patient to the provider through patient-generated data, such as goal setting and feedback. Patients may play a larger role in reporting hospital satisfaction in real time, reconciling medications, contributing to the treatment plan, and identifying medical errors. As portals are integrated across the care continuum,20 our understanding of their impact may become more clear.
In this review, only 5 studies were conducted in the pediatric hospital setting.24,32-34,38 With hospitalized children experiencing 3 times more harm from medical errors than adults,44 engaging parents in inpatient care to improve safety has become a national priority.45 Giving patient portals, or “parent portals,” to parents of hospitalized children may provide a unique opportunity to share healthcare information and promote engagement, a direction for future study. There is also a research gap in evaluating adolescent inpatient portal use. Future portals may be designed to incentivize young children to learn about their hospitalization through games linked to health-related education.
Finally, as patients and caregivers begin using inpatient portals, there will almost certainly be consequences for healthcare teams. Understanding and anticipating human and work system factors influencing inpatient portal adoption and use from the perspectives of both patients and healthcare teams are needed.46,47 Engaging healthcare team members as valuable stakeholders during implementation and measuring the impact of portal use on their workload is necessary, especially as portal use spreads beyond pilot units. The success of inpatient portals is dependent upon both the positive benefits for patients and their acceptance by healthcare teams.48
Limitations exist in conducting a systematic literature review.49 The conceptual definition of a portal for hospitalized patients and patient/caregiver engagement is evolving; therefore, our definition may not have captured all relevant studies. We intentionally did not include all inpatient technology, as we were interested in a narrow definition of portals designed for inpatients that provided clinical information from the inpatient EHR. Because of rapid technology changes, we also limited our search to studies published within the last 10 years; prior literature has been described elsewhere.17 We excluded non-English language studies, limiting our ability to capture the full scope of inpatient portal research. These patients already experience healthcare delivery disparities, widened by the inaccessibility of innovative health information technologies.50 Future studies would be enhanced with the inclusion of these participants.
Inpatient portal research is in its infancy but growing rapidly. Studies to date are primarily focused on portal design and have small sample sizes. Early findings suggest that patients and caregivers are, in general, enthusiastic about using inpatient portals. Further research is needed, however, to determine the impact of inpatient portal use on patient engagement and hospital-care quality, safety, and cost.
Disclosure
This work was supported by a Department of Pediatrics Research and Development Grant at the University of Wisconsin School of Medicine and Public Health. This publication was also supported by the Clinical and Translational Science Award program through the National Center for Advancing Translational Sciences, grant UL1TR000427. Dr. Hoonakker’s involvement was also partially supported by the National Science Foundation, grant CMMI 1536987. Funding sources had no involvement in study design, analysis, or interpretation of data. The authors have no conflicts of interest to declare.
1. Stewart M, Brown JB, Donner A, et al. The impact of patient-centered care on outcomes. J Fam Pract. 2000;49(9):796-804. PubMed
2. Little P, Everitt H, Williamson I, et al. Observational study of effect of patient centredness and positive approach on outcomes of general practice consultations. BMJ. 2001;323(7318):908-911. PubMed
3. Maeng DD, Graf TR, Davis DE, Tomcavage J, Bloom FJ, Jr. Can a patient-centered medical home lead to better patient outcomes? The Quality Implications of Geisinger’s ProvenHealth Navigator. Am J Med Qual. 2012;27(3):210-216. PubMed
4. Joint Commision on Accreditation of Healthcare Organizations. Speak up: Prevent errors in your child’s care. http://www.jointcommission.org/Speak_Up_Prevent_Errors_in_Your_Childs_Care/. Accessed June 10, 2017.
5. Committee on Hospital Care and Institute for Patient and Family-centered Care. Patient- and family-centered care and the pediatrician’s role. Pediatrics. 2012;129(2):394-404. PubMed
6. Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001. PubMed
7. Coulter A. Engaging Patients in Healthcare. New York: McGraw-Hill Education; 2011. PubMed
8. Tang PC, Ash JS, Bates DW, Overhage JM, Sands DZ. Personal health records: definitions, benefits, and strategies for overcoming barriers to adoption. J Am Med Inform Assoc. 2006;13(2):121-126. PubMed
9. Schnipper JL, Gandhi TK, Wald JS, et al. Design and implementation of a web-based patient portal linked to an electronic health record designed to improve medication safety: the Patient Gateway medications module. Inform Prim Care. 2008;16(2):147-155. PubMed
10. Blumenthal D, Tavenner M. The “meaningful use” regulation for electronic health records. N Engl J Med. 2010;363(6):501-504. PubMed
11. Ammenwerth E, Schnell-Inderst P, Hoerbst A. The impact of electronic patient portals on patient care: a systematic review of controlled trials. J Med Internet Res. 2012;14(6):e162. PubMed
12. Goldzweig CL, Orshansky G, Paige NM, et al. Electronic patient portals: evidence on health utcomes, satisfaction, efficiency, and attitudes: a systematic review. Ann Intern Med. 2013;159(10):677-687. PubMed
13. Davis Giardina T, Menon S, Parrish DE, Sittig DF, Singh H. Patient access to medical records and healthcare outcomes: a systematic review. J Am Med Inform Assoc. 2014;21(4):737-741. PubMed
14. Kalra D, Fernando B. A review of the empirical evidence of the healthcare benefits of personal health records. Yearb Med Inform. 2013;8(1):93-102. PubMed
15. Kruse CS, Bolton K, Freriks G. The effect of patient portals on quality outcomes and its implications to meaningful use: a systematic review. J Med Internet Res. 2015;17(2):e44. PubMed
16. Vawdrey DK, Wilcox LG, Collins SA, et al. A tablet computer application for patients to participate in their hospital care. AMIA Annu Symp Proc. 2011:1428-1435. PubMed
17. Prey JE, Woollen J, Wilcox L, et al. Patient engagement in the inpatient setting: a systematic review. J Am Med Inform Assoc. 2014;21(4):742-750. PubMed
18. O’Leary KJ, Lohman ME, Culver E, et al. The effect of tablet computers with a mobile patient portal application on hospitalized patients’ knowledge and activation. J Am Med Inform Assoc. 2016;23(1):159-165. PubMed
19. Skeels M, Tan DS. Identifying opportunities for inpatient-centric technology. Proceedings of the 1st ACM International Health Informatics Symposium. Arlington: ACM; 2010:580-589.
20. Collins SA, Rozenblum R, Leung WY, et al. Acute care patient portals: a qualitative study of stakeholder perspectives on current practices. J Am Med Inform Assoc. 2017;24(e1):e9-e17. PubMed
21. Morris D, Karlson A. Dynamic Accessibility Requirements for Hospital Patients. SIGCHI Conference on Human Factors in Computing Systems. Vancouver, BC, Canada: ACM; 2011.
22. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. PubMed
23. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
24. Weyand SA, Frize M, Bariciak E, Dunn S. Development and usability testing of a parent decision support tool for the neonatal intensive care unit. Conf Proc IEEE Eng Med Biol Soc. 2011:6430-6433. PubMed
25. Caligtan CA, Carroll DL, Hurley AC, Gersh-Zaremski R, Dykes PC. Bedside information technology to support patient-centered care. Int J Med Inform. 2012;81(7):442-451. PubMed
26. Wilcox L, Feiner S, Liu A, Restaino S, Collins S, Vawdrey D. Designing inpatient technology to meet the medication information needs of cardiology patients. Proceedings of the 2nd ACM SIGHIT International Health Informatics Symposium. Miami: ACM; 2012:831-836. PubMed
27. Dykes PC, Carroll DL, Hurley AC, et al. Building and testing a patient-centric electronic bedside communication center. J Gerontol Nurs. 2013;39(1):15-19. PubMed
28. Dykes PC, Stade D, Chang F, et al. Participatory design and development of a patient-centered toolkit to engage hospitalized patients and care partners in their plan of care. AMIA Annu Symp Proc. 2014:486-495. PubMed
29. Pell JM, Mancuso M, Limon S, Oman K, Lin CT. Patient access to electronic health records during hospitalization. JAMA Intern Med. 2015;175(5):856-858. PubMed
30. Yoo S, Lee KH, Baek H, et al. Development and user research of a smart bedside station system toward patient-centered healthcare system. J Med Syst. 2015;39(9):86. PubMed
31. Dalal AK, Dykes PC, Collins S, et al. A web-based, patient-centered toolkit to engage patients and caregivers in the acute care setting: a preliminary evaluation. J Am Med Inform Assoc. 2016;23(1):80-87. PubMed
32. Kaziunas E, Hanauer DA, Ackerman MS, Choi SW. Identifying unmet informational needs in the inpatient setting to increase patient and caregiver engagement in the context of pediatric hematopoietic stem cell transplantation. J Am Med Inform Assoc. 2016;23(1):94-104. PubMed
33. Kelly MM, Hoonakker PLT, Dean SM. Using an inpatient portal to engage families in pediatric hospital care. J Am Med Inform Assoc. 2016;24(1):153-161. PubMed
34. Maher M, Kaziunas E, Ackerman M, et al. User-centered design groups to engage patients and caregivers with a personalized health information technology tool. Biol Blood Marrow Transplant. 2016;22(2):349-358. PubMed
35. O’Leary KJ, Sharma RK, Killarney A, et al. Patients’ and healthcare providers’ perceptions of a mobile portal application for hospitalized patients. BMC Med Inform Decis Mak. 2016;16(1):123-130. PubMed
36. Wilcox L, Woollen J, Prey J, et al. Interactive tools for inpatient medication tracking: a multi-phase study with cardiothoracic surgery patients. J Am Med Inform Assoc. 2016;23(1):144-158. PubMed
37. Woollen J, Prey J, Wilcox L, et al. Patient experiences using an inpatient personal health record. Appl Clin Inform. 2016;7(2):446-460. PubMed
38. Kelly MM, Dean SM, Carayon P, Wetterneck TB, Hoonakker PLT. Healthcare team perceptions of a portal for parents of hospitalized children before and after implementation. Appl Clin Inform. 2017;8(1):265-278. PubMed
39. Wolff JL, Darer JD, Berger A, et al. Inviting patients and care partners to read doctors’ notes: OpenNotes and shared access to electronic medical records. J Am Med Inform Assoc. 2017;24(e1):e166-e172. PubMed
40. Feldman HJ, Walker J, Li J, Delbanco T. OpenNotes:hospitalists’ challenge and opportunity. J Hosp Med. 2013;8(7):414-417. PubMed
41. Hibbard JH, Stockard J, Mahoney ER, Tusler M. Development of the Patient Activation Measure (PAM): conceptualizing and measuring activation in patients and consumers. Health Serv Res. 2004;39(4 Pt 1):1005-1026. PubMed
42. Prey JE, Qian M, Restaino S, et al. Reliability and validity of the patient activation measure in hospitalized patients. Patient Educ Couns. 2016;99(12):2026-2033. PubMed
43. Toomey SL, Zaslavsky AM, Elliott MN, et al. The development of a pediatric inpatient experience of care measure: Child HCAHPS. Pediatrics. 2015;136(2):360-369. PubMed
44. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285(16):2114-2120. PubMed
45. Agency for Healthcare Research and Quality. 20 Tips to help prevent medical errors in children. Secondary 20 Tips to help prevent medical errors in children. http://www.ahrq.gov/patients-consumers/care-planning/errors/20tips/index.html. Accessed on June 10, 2017.
46. Thompson MJ, Reilly JD, Valdez RS. Work system barriers to patient, provider, and caregiver use of personal health records: A systematic review. Appl Ergon. 2016;54:218-242. PubMed
47. Holden RJ, Carayon P, Gurses AP, et al. SEIPS 2.0: a human factors framework for studying and improving the work of healthcare professionals and patients. Ergonomics. 2013;56(11):1669-1686. PubMed
48. Gagnon MP, Ngangue P, Payne-Gagnon J, Desmartis M. m-Health adoption by healthcare professionals: a systematic review. J Am Med Inform Assoc. 2016;23(1):212-220. PubMed
49. Russell CL. An overview of the integrative research review. Prog Transplant. 2005;15(1):8-13. PubMed
50. Yamin CK, Emani S, Williams DH, et al. The digital divide in adoption and use of a personal health record. Arch Intern Med. 2011;171(6):568-574. PubMed
1. Stewart M, Brown JB, Donner A, et al. The impact of patient-centered care on outcomes. J Fam Pract. 2000;49(9):796-804. PubMed
2. Little P, Everitt H, Williamson I, et al. Observational study of effect of patient centredness and positive approach on outcomes of general practice consultations. BMJ. 2001;323(7318):908-911. PubMed
3. Maeng DD, Graf TR, Davis DE, Tomcavage J, Bloom FJ, Jr. Can a patient-centered medical home lead to better patient outcomes? The Quality Implications of Geisinger’s ProvenHealth Navigator. Am J Med Qual. 2012;27(3):210-216. PubMed
4. Joint Commision on Accreditation of Healthcare Organizations. Speak up: Prevent errors in your child’s care. http://www.jointcommission.org/Speak_Up_Prevent_Errors_in_Your_Childs_Care/. Accessed June 10, 2017.
5. Committee on Hospital Care and Institute for Patient and Family-centered Care. Patient- and family-centered care and the pediatrician’s role. Pediatrics. 2012;129(2):394-404. PubMed
6. Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001. PubMed
7. Coulter A. Engaging Patients in Healthcare. New York: McGraw-Hill Education; 2011. PubMed
8. Tang PC, Ash JS, Bates DW, Overhage JM, Sands DZ. Personal health records: definitions, benefits, and strategies for overcoming barriers to adoption. J Am Med Inform Assoc. 2006;13(2):121-126. PubMed
9. Schnipper JL, Gandhi TK, Wald JS, et al. Design and implementation of a web-based patient portal linked to an electronic health record designed to improve medication safety: the Patient Gateway medications module. Inform Prim Care. 2008;16(2):147-155. PubMed
10. Blumenthal D, Tavenner M. The “meaningful use” regulation for electronic health records. N Engl J Med. 2010;363(6):501-504. PubMed
11. Ammenwerth E, Schnell-Inderst P, Hoerbst A. The impact of electronic patient portals on patient care: a systematic review of controlled trials. J Med Internet Res. 2012;14(6):e162. PubMed
12. Goldzweig CL, Orshansky G, Paige NM, et al. Electronic patient portals: evidence on health utcomes, satisfaction, efficiency, and attitudes: a systematic review. Ann Intern Med. 2013;159(10):677-687. PubMed
13. Davis Giardina T, Menon S, Parrish DE, Sittig DF, Singh H. Patient access to medical records and healthcare outcomes: a systematic review. J Am Med Inform Assoc. 2014;21(4):737-741. PubMed
14. Kalra D, Fernando B. A review of the empirical evidence of the healthcare benefits of personal health records. Yearb Med Inform. 2013;8(1):93-102. PubMed
15. Kruse CS, Bolton K, Freriks G. The effect of patient portals on quality outcomes and its implications to meaningful use: a systematic review. J Med Internet Res. 2015;17(2):e44. PubMed
16. Vawdrey DK, Wilcox LG, Collins SA, et al. A tablet computer application for patients to participate in their hospital care. AMIA Annu Symp Proc. 2011:1428-1435. PubMed
17. Prey JE, Woollen J, Wilcox L, et al. Patient engagement in the inpatient setting: a systematic review. J Am Med Inform Assoc. 2014;21(4):742-750. PubMed
18. O’Leary KJ, Lohman ME, Culver E, et al. The effect of tablet computers with a mobile patient portal application on hospitalized patients’ knowledge and activation. J Am Med Inform Assoc. 2016;23(1):159-165. PubMed
19. Skeels M, Tan DS. Identifying opportunities for inpatient-centric technology. Proceedings of the 1st ACM International Health Informatics Symposium. Arlington: ACM; 2010:580-589.
20. Collins SA, Rozenblum R, Leung WY, et al. Acute care patient portals: a qualitative study of stakeholder perspectives on current practices. J Am Med Inform Assoc. 2017;24(e1):e9-e17. PubMed
21. Morris D, Karlson A. Dynamic Accessibility Requirements for Hospital Patients. SIGCHI Conference on Human Factors in Computing Systems. Vancouver, BC, Canada: ACM; 2011.
22. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. PubMed
23. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377-384. PubMed
24. Weyand SA, Frize M, Bariciak E, Dunn S. Development and usability testing of a parent decision support tool for the neonatal intensive care unit. Conf Proc IEEE Eng Med Biol Soc. 2011:6430-6433. PubMed
25. Caligtan CA, Carroll DL, Hurley AC, Gersh-Zaremski R, Dykes PC. Bedside information technology to support patient-centered care. Int J Med Inform. 2012;81(7):442-451. PubMed
26. Wilcox L, Feiner S, Liu A, Restaino S, Collins S, Vawdrey D. Designing inpatient technology to meet the medication information needs of cardiology patients. Proceedings of the 2nd ACM SIGHIT International Health Informatics Symposium. Miami: ACM; 2012:831-836. PubMed
27. Dykes PC, Carroll DL, Hurley AC, et al. Building and testing a patient-centric electronic bedside communication center. J Gerontol Nurs. 2013;39(1):15-19. PubMed
28. Dykes PC, Stade D, Chang F, et al. Participatory design and development of a patient-centered toolkit to engage hospitalized patients and care partners in their plan of care. AMIA Annu Symp Proc. 2014:486-495. PubMed
29. Pell JM, Mancuso M, Limon S, Oman K, Lin CT. Patient access to electronic health records during hospitalization. JAMA Intern Med. 2015;175(5):856-858. PubMed
30. Yoo S, Lee KH, Baek H, et al. Development and user research of a smart bedside station system toward patient-centered healthcare system. J Med Syst. 2015;39(9):86. PubMed
31. Dalal AK, Dykes PC, Collins S, et al. A web-based, patient-centered toolkit to engage patients and caregivers in the acute care setting: a preliminary evaluation. J Am Med Inform Assoc. 2016;23(1):80-87. PubMed
32. Kaziunas E, Hanauer DA, Ackerman MS, Choi SW. Identifying unmet informational needs in the inpatient setting to increase patient and caregiver engagement in the context of pediatric hematopoietic stem cell transplantation. J Am Med Inform Assoc. 2016;23(1):94-104. PubMed
33. Kelly MM, Hoonakker PLT, Dean SM. Using an inpatient portal to engage families in pediatric hospital care. J Am Med Inform Assoc. 2016;24(1):153-161. PubMed
34. Maher M, Kaziunas E, Ackerman M, et al. User-centered design groups to engage patients and caregivers with a personalized health information technology tool. Biol Blood Marrow Transplant. 2016;22(2):349-358. PubMed
35. O’Leary KJ, Sharma RK, Killarney A, et al. Patients’ and healthcare providers’ perceptions of a mobile portal application for hospitalized patients. BMC Med Inform Decis Mak. 2016;16(1):123-130. PubMed
36. Wilcox L, Woollen J, Prey J, et al. Interactive tools for inpatient medication tracking: a multi-phase study with cardiothoracic surgery patients. J Am Med Inform Assoc. 2016;23(1):144-158. PubMed
37. Woollen J, Prey J, Wilcox L, et al. Patient experiences using an inpatient personal health record. Appl Clin Inform. 2016;7(2):446-460. PubMed
38. Kelly MM, Dean SM, Carayon P, Wetterneck TB, Hoonakker PLT. Healthcare team perceptions of a portal for parents of hospitalized children before and after implementation. Appl Clin Inform. 2017;8(1):265-278. PubMed
39. Wolff JL, Darer JD, Berger A, et al. Inviting patients and care partners to read doctors’ notes: OpenNotes and shared access to electronic medical records. J Am Med Inform Assoc. 2017;24(e1):e166-e172. PubMed
40. Feldman HJ, Walker J, Li J, Delbanco T. OpenNotes:hospitalists’ challenge and opportunity. J Hosp Med. 2013;8(7):414-417. PubMed
41. Hibbard JH, Stockard J, Mahoney ER, Tusler M. Development of the Patient Activation Measure (PAM): conceptualizing and measuring activation in patients and consumers. Health Serv Res. 2004;39(4 Pt 1):1005-1026. PubMed
42. Prey JE, Qian M, Restaino S, et al. Reliability and validity of the patient activation measure in hospitalized patients. Patient Educ Couns. 2016;99(12):2026-2033. PubMed
43. Toomey SL, Zaslavsky AM, Elliott MN, et al. The development of a pediatric inpatient experience of care measure: Child HCAHPS. Pediatrics. 2015;136(2):360-369. PubMed
44. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285(16):2114-2120. PubMed
45. Agency for Healthcare Research and Quality. 20 Tips to help prevent medical errors in children. Secondary 20 Tips to help prevent medical errors in children. http://www.ahrq.gov/patients-consumers/care-planning/errors/20tips/index.html. Accessed on June 10, 2017.
46. Thompson MJ, Reilly JD, Valdez RS. Work system barriers to patient, provider, and caregiver use of personal health records: A systematic review. Appl Ergon. 2016;54:218-242. PubMed
47. Holden RJ, Carayon P, Gurses AP, et al. SEIPS 2.0: a human factors framework for studying and improving the work of healthcare professionals and patients. Ergonomics. 2013;56(11):1669-1686. PubMed
48. Gagnon MP, Ngangue P, Payne-Gagnon J, Desmartis M. m-Health adoption by healthcare professionals: a systematic review. J Am Med Inform Assoc. 2016;23(1):212-220. PubMed
49. Russell CL. An overview of the integrative research review. Prog Transplant. 2005;15(1):8-13. PubMed
50. Yamin CK, Emani S, Williams DH, et al. The digital divide in adoption and use of a personal health record. Arch Intern Med. 2011;171(6):568-574. PubMed
© 2017 Society of Hospital Medicine
Improving Family Engagement During FCR
A growing body of literature suggests that patient‐ and family‐centered care can improve patient outcomes[1, 2, 3, 4, 5] as well as patient, family, and provider satisfaction.[6, 7, 8, 9, 10] Engaging patients and families as a way to improve the quality and safety of care has been widely endorsed by leading healthcare organizations,[11, 12, 13] including the Institute of Medicine.[14] In the pediatric inpatient setting, family‐centered rounds (FCR), defined as bedside rounds in which the patient and family share in the control of the management plan as well as in the evaluation of the process itself,[15] potentially provide a consistent venue for family engagement and are recommended by the American Academy of Pediatrics as standard practice.[13]
According to a recent study by Mittal et al.,[16] FCR are the most common type of rounds practiced among pediatric hospitalists surveyed in the United States and Canada. Despite this widespread shift from rounding in a conference room to the bedside with patients and families, there exist only a few studies that provide specific recommendations on conducting FCR.[15, 17, 18] This research has been limited, primarily focusing how rounds are conducted, and further investigation is needed to identify the impact of other processes and elements within the hospital work system that may also affect family engagement during rounds.
The objectives of this study were to: 1) identify strategies to enhance family engagement during FCR drawing from the viewpoints of the various stakeholders on rounds, and 2) characterize these strategies into known elements of hospital work systems and rounding processes using a recognized human factors engineering approach, The Systems Engineering Initiative for Patient Safety (SEIPS) model.[19] According to the SEIPS model, barriers and facilitators to family engagement during FCR are likely embedded in the design of the hospital work systems and rounding process; therefore, we hypothesized that strategies that influence engagement will target all work system and process elements. This work is part of a larger study in which, after prioritization of this group of strategies based on feasibility and sustainability, a bundle of best practices for conducting FCR will be developed, implemented, and evaluated.
METHODS
Study Design
Semistructured interviews using the stimulated recall approach[20, 21] were conducted to understand the cognitive processes of families and healthcare team (HCT) members during FCR. This qualitative study design allowed us to capture comprehensive information from the perspectives of a diverse group of stakeholders on strategies for improving family engagement during FCR.
Setting and Participants
This study was conducted at a children's hospital in Wisconsin, where FCR were initiated in 2007 with the transition to a new hospital facility. The expectation is that FCR are conducted daily with the family and the patient's HCT, consisting of at least an attending physician and nurse. Typically, multiple residents, interns, and medical students are present along with a combination of other providers, including consulting subspecialists, a fellow, nurse practitioner, respiratory therapist, or pharmacist. When this study was conducted, attendees received little to no formal training regarding their role on FCR. As part of a larger study, English‐speaking patients and/or families admitted to 1 of 4 inpatient services (2 hospitalist, 1 pulmonary, and 1 hematology/oncology), and their associated HCT members were enrolled and their bedside rounds were video recorded. A purposive sampling technique[22, 23] was employed, recruiting interviewees that represented the various groups of stakeholders of rounds, including parents, children, attending physicians, resident physicians, medical students, and nurses. For child interviews, we restricted selection to children aged 8 to 17 years to ensure the ability to understand the interviewing process and provide feedback. Families were consented and children were assented. The University of Wisconsin‐Madison Health Sciences Institutional Review Board approved this study.
Interviews and analysis occurred concurrently in an iterative process, informing each other. Thus, recruitment continued until we reached theoretical saturation,[24, 25] the point at which additional interviews did not provide new information or further conceptual development.
Study Procedures
All interviews were conducted by trained researchers, who used the same semistructured interview guide. During each interview, the interviewee was instructed to watch his/her own rounding video and pause when noticing something that made it easy (facilitator) or hard (barrier) to engage the family. Every time the interviewee paused the video to describe what was noticed, the interviewer then asked follow‐up, open‐ended questions to solicit specific information that focused on strategies for enhancing family engagement during FCR. For instance, if the issue identified was a barrier, the interviewer asked, What would you have wanted to happen differently? and if the issue identified was a facilitator, the interviewer asked, How could we ensure that would happen for everyone? The interviewee rewound the video as needed. If the interviewee had not stopped the video by the halfway point, the interviewer would pause the video and review the instructions. After the interviewee had viewed and commented on the entire rounding video, an opportunity was offered to reflect on other factors that influence family engagement during rounds, and additional questions were asked as necessary to fully understand the interviewee's views. All interviews were audio recorded and personal identifiers were removed prior to data analysis.
Data Analysis
Two research assistants reviewed the audio recordings and identified all instances related to strategies for improving family engagement during FCR. There was no screening of strategies (ie, if an interviewee suggested a strategy was related to improving family engagement, it was categorized as such). To ensure intercoder reliability, these assistants, under the supervision of a researcher (L.D.), reviewed the coding process together, held consensus meetings, and crosschecked interviews for coding consensus. A researcher (A.X.) transcribed all strategy‐related instances, which were then reviewed by two additional researchers (M.K., P.C.). To organize, sort, and code the data, interview transcripts were imported in the NVivo qualitative data analysis software (QSR International, Doncaster, Victoria, Australia). The research group then performed a qualitative content analysis of the transcripts[26] and categorized the strategies in an iterative process (information provided on request).
To ensure that all strategies remained conceptually similar within categories, the constant comparative method[27, 28] was applied to the coding process. This involved comparing: 1) strategy‐related instances from the same participants, 2) strategy‐related instances from different participants in the same groups, 3) strategy‐related instances from different participants in different groups, 4) a coded strategy with other coded strategies, 5) coded strategies with categories, and 6) a category with other categories. A strategy‐related instance could be coded under more than one strategy or category. For instance, one interviewee said conducting things that can be done without family beforehand, and presenting and reviewing the plan with family. This was coded under both the strategy conducting rounds in another location without family and then at the bedside with family in the location of FCR category and the strategy focusing presentation on assessment and plan in the communication style category.
RESULTS
A total of 37 interviews were conducted with 11 parents, 4 children, and 22 HCT members (8 attending physicians, 6 resident physicians, 5 medical students, and 3 nurses) in 24 videos of rounding sessions. The duration of the interviews ranged from 30 to 60 minutes.
A total of 338 separate instances related to strategies for improving family engagement on FCR were identified and sorted into 21 categories. Using the SEIPS model, these categories were organized into 2 themes: the work system and process of FCR (Figure 1). Of the 21 categories, 12 were mentioned by both families (parents and/or children) and HCT members and 9 were solely mentioned by the HCT.
Work System of FCR
Table 1 shows the categories of strategies related to the 5 elements of the FCR work system.[29, 30] Illustrative quotes from the interviews (Q) are presented in Table 2.
| Work System Elements | Categories | Strategies | P (11) | C (4) | Att. (8) | Res. (6) | MS (5) | RN (3) |
|---|---|---|---|---|---|---|---|---|
| ||||||||
| People | 1. Size and composition of HCT | Have a smaller HCT conduct FCR | X | X | X | X | ||
| Ensure all relevant disciplines present on FCR | X | X | X | X | X | |||
| Task | 2. Roles and duties of HCT members | Define roles/duties of HCT members on FCR | X | X | ||||
| Organization | 3. Timing and scheduling of FCR | Schedule FCR, inform participants beforehand | X | X | X | |||
| 4. Training of HCT for FCR | Train HCT on how to present on FCR | X | X | |||||
| Environment | 5. Location of FCR | At bedside with family and patient | X | X | ||||
| In another location with HCT, then at bedside | X | X | X | X | ||||
| In another location with family but without child | X | |||||||
| 6. Positioning of HCT members on FCR | Sit down with family | X | X | X | X | X | ||
| Stand close to or in a semicircle around family | X | X | X | X | X | |||
| Tools and technologies | 7. Use of computers on FCR | Use computer to support family interaction | X | X | X | X | ||
| Don't use a computer | X | X | ||||||
|
| Q1: I'm intimidated to ask a question. It seems like there are too many peopleI like a smaller group. (P5) |
| Q2: Sometimes rounds are the only time that the parents are there to see the entire teamso in that way, including [the entire team] at the rounds makes more sense. (MS1) |
| Q3: There needs to be much more clear roles about who is supposed to do what, and it should be predictable. (Att.2) |
| Q4: ([T]iming of rounds) is a huge source of frustration for families. If [physicians] know in which order they will go for patients, they can call our charge nurse or unit clerk or page nurses with that information. (RN1) |
| Q5: ([W]ith a notice of the rounding schedule), I can be ahead of time, trying to think of questions. (P10) |
| Q6: [I]t would be really nice to see somebody do a presentation in a medical eye's version and then also in the family‐centered version. (MS5) |
| Q7: [H]aving the medical students practice with the senior residentis a good way of doing it. (Res.4) |
| Q8: [M]aybe some small groups where you practice this among students. (MS5) |
| Q9: It would be better to be in the room for communication. (Att.1) |
| Q10: You could have sort of hallway rounds, which is much more medical oriented, and inside‐the‐room rounds, which is much more talking with the parent. (P1) |
| Q11: [H]ave sit‐down rounds with parents and families. (Res.5) |
| Q12: I've seen some attending physicians who sat down. I think that could be helpful to be on the same level as the patient and family. (Res.2) |
| Q13: [M]aybe formation of semicircle or something like that, where we can see everybody a little more clearly, I think that would be very helpful. (P10) |
| Q14: I find the presence of a computer incredibly offensive and obstructivewhen you are supposed to be able to interact with the patient. (Att.6) |
| Q15: One of the things I started doing is having one of the other resident physicians have the computer, so just relying on them to do the orders, and me just being there mainly for being the presenter of rounds. (Res.4) |
People
Two seemingly contradictory strategies were proposed. Some interviewees suggested a smaller HCT with members most familiar to the family (Q1), whereas other interviewees stressed the need to involve different relevant disciplines (eg, social worker, nutritionist) during rounds (Q2).
Tasks
Both attending and resident physicians emphasized the importance of defining the role of each HCT member before rounding (Q3). Interviewees also suggested these roles should be explained to families, ideally at admission.
Organization
Many interviewees suggested the need to consistently schedule rounds (Q4) and to inform families and nurses of the schedule so all parties could plan ahead (Q5). Some resident physicians and medical students recommended training of learners on how to give a family‐centered presentation using methods such as role modeling (Q6) and practicing with the senior resident physician (Q7) or in small groups (Q8).
Environment
Some interviewees suggested conducting rounds in patient rooms (Q9). Others suggested conducting rounds first in another location (eg, hallway) without the family and then going to the bedside to round with the family (Q10). There were also interviewees who suggested conducting rounds in another location (eg, conference room) with the family (Q11). When conducting rounds in the patient room, some interviewees suggested that some HCT members (eg, attending and senior resident physicians) could sit down with the family (Q12), with the rest of the HCT standing close to the family in a semicircle (Q13).
Tools and Technologies
Some interviewees thought that conversation with families could be negatively affected by the use of computers, and therefore suggested not using them on FCR (Q14). Alternatively, other interviewees considered computers a tool to facilitate the interaction between the HCT and families, such as showing x‐rays or lab values. Several interviewees suggested that computers should not be positioned to block eye contact between HCT members and families; therefore, only HCT members not presenting should use computers (Q15).
Process of FCR
Table 3 shows the categories of strategies related to the process of FCR, which were categorized into 3 phases. Illustrative quotes are presented in Table 4.
| Process Phases | Categories | Strategies | P (11) | C (4) | Att. (8) | Res. (6) | MS (5) | RN (3) |
|---|---|---|---|---|---|---|---|---|
| ||||||||
| Before FCR | 8. HCT preparation | Collect and prepare pertinent information | X | X | X | X | ||
| 9. Family preparation | Orient family to rounding process | X | X | X | X | X | ||
| Build relationship with family | X | X | X | |||||
| Ask family for permission and preferences | X | X | X | |||||
| During FCR | 10. Introduction and explanation of FCR | Introduce HCT and family to each other | X | X | X | X | X | |
| Explain interactive rounding process | X | X | X | |||||
| 11. Active involvement of nurse | Giving nurse opportunity to actively participate | X | X | |||||
| 12. Communication with family | Give family opportunity to actively participate | X | X | X | X | X | X | |
| Address family's questions/concerns | X | X | X | X | X | |||
| Explain tests, findings and results to family | X | X | X | X | X | |||
| Confirm family understanding | X | X | X | |||||
| 13. Giving presentation | Restructure the presentation | X | X | |||||
| Shorten the presentation | X | X | X | |||||
| Focus presentation on assessment and plan | X | X | X | X | X | |||
| Summarize plan for family | X | X | X | |||||
| Avoid discussion of sensitive topics | X | X | X | |||||
| 14. Communication style | Present in a conversational manner | X | X | X | ||||
| Use an engaging communication style | X | X | X | X | X | |||
| 15. Language used | Use qualitative language | X | X | X | ||||
| Use plain language | X | X | X | X | X | |||
| 16. Performing physical exam | Pause and confirm physical exam | X | ||||||
| 17. Managing distractions | Minimize distractions and interruptions | X | X | X | X | X | X | |
| 18. Senior physician leading/role modeling | Attending/senior resident physician should lead, direct and be a role model on FCR rounds | X | X | |||||
| 19. Teaching | Ask family permission and involve in teaching | X | X | |||||
| 20. Customizing FCR for family | Adapt rounds to family's needs | X | X | X | X | |||
| After FCR | 21. Following up with family | HCT members follow up with family | X | X | X | |||
|
| Q1: [Medical students and residents] actually had a chance to do a quick round, an abbreviated presentation to put together an outline of what we're going to talk about before we even do it. (MS2) |
| Q2: I would like to know exactly what's going onbefore I walk in. (Att.6) |
| Q3: [T]he nurse did give me the fore‐warning that rounds would be coming and it was usually like a group of 8 to 10so I was prepared for that. (P7) |
| Q4: What went well is that I had already connected with this mom and the daughter prior to this rounding encounter. (Res.3) |
| Q5: [Y]ou could ask the patient or the parents if they want the child there. (P3) |
| Q6: [Families] really want to know what your role is on the team. (Att.5) |
| Q7: I guess it would be easier to figure out who you need to direct questions to. (P3) |
| Q8: [L]etting the family anticipate what rounding is going to be like and when the opportunity is going to come up to talk. I think that can help. (Res.2) |
| Q9: I think the decision making is probably the most critical partthere is really no substitute for [families] being involved in the decisionwithout a lot of medical conversation and analysis. (P1) |
| Q10: The family was proactive enough to ask questions, but they were never really given entrance to ask questions.No one had said do you have any questions?' (Res.4) |
| Q11: It is really important for the doctors to listen to them, to know that they are the parents and they know their children best. (RN3) |
| Q12: I think sometimes when you are teaching, some of the information could potentially be scary to the family. What I would hope is letting the family feel like they are part of the education process. (Res.2) |
| Q13: Sometimes nurses are asked initially, do you have anything to add,' which I think is a good way to startbecause we have probably the most current and updated information. (RN1) |
| Q14: When I was talking about the physical exam partmaybe at that point, if I could just stop talking, we couldconfirm that exam. (Res.3) |
| Q15: It's distracting if different groups have individual discussions when you are trying to keep the group focused on this particular patient for rounds. (Att.7) |
| Q16: It's just the basic thing that I try to tell residents. I do this hopefully at least once every time I am on services with the team. (Att.1) |
| Q17: ([C]hanging rounds depending on the families) would be the ideal situationthinking about what's helpful for a family. (Att.6) |
| Q18: What I usually see when things work well after we leave is that the nurse can still stick around the family. (Res.4) |
| Q19: [T]he students have to go back in the afternoon to talk with the family about what the treatment point is and answer any questions. (MS2) |
Before FCR
To engage families during FCR, many interviewees suggested that both the HCT and families need preparation. HCT members suggested that medical students should collect up‐to‐date patient information and review it with the senior resident physicians (Q1) to reach a consensus before starting FCR (Q2). To prepare families for rounds, parents and HCT members suggested that the HCT should orient families to the rounding process (Q3), build relationships with families (Q4), and ask for their permission and preference regarding participation in rounds (Q5).
During FCR
A number of strategies focused on the beginning of rounds. Parents, children, and HCT members stressed the need to introduce HCT members by role (Q6) and inform families to whom to direct questions (Q7). It was also suggested that parents introduce themselves to the team. Some interviewees recommended that the HCT explain the rounding process to families at this time (Q8).
Interviewees recommended strategies related to communication between the HCT and families during rounds. Many interviewees suggested restructuring and shortening the presentation by focusing on the assessment and plan (Q9). According to all interviewees, the HCT should present in a conversational manner and use an engaging communication style (eg, smiling, making eye contact, using appropriate humor) and appropriate language (eg, qualitative trend instead of numbers, plain language instead of medical jargon) to communicate with families. To ensure families understanding, HCT members should encourage and address their questions and concerns (Q10). In addition, families should be given the opportunity to provide information (eg, patient history and overnight events) and to express their opinions about the plan (Q11). If teaching is done during rounds, the HCT should involve families and ask for permission (Q12).
Other strategies on rounds were suggested, such as giving nurses the opportunity to actively participate (Q13), pausing and confirming physical exam findings (Q14), minimizing distractions and interruptions (Q15), attending and/or senior resident physicians leading and being role models for FCR (Q16), and adapting rounds to families' needs (Q17).
After FCR
Some HCT members talked about the importance of following up with families after rounds. Specifically, suggestions that nurses could stay with families immediately after rounds (Q18) were made, whereas physicians could return to families later in the day (Q19).
DISCUSSION
Using recognized qualitative systems engineering methods, we identified a broad range of strategies for enhancing family engagement on FCR from the perspectives of a diverse group of stakeholders on rounds and described how these strategies target known fundamental elements in both the hospital work system and rounding process. We highlight recommendations on the content and style of communication during rounds with families, but also introduce more complex system‐wide elements that likely play a role in family engagement, such as the composition of the HCT; organization and environment of rounds; tools and technologies used; and preparation of the HCT, families, and patients beforehand.
Our research both confirms and builds upon practices previously described in the FCR literature.[17, 31, 32] In a case report by Muething et al.,[17] recommendations were developed using a series of plan‐do‐study‐act cycles to determine the components needed to conduct FCR. These components included: 1) determining family preference prior to rounds, 2) defining HCT roles, 3) introducing HCT to family and explaining the purpose of rounds, 4) describing what is shared and how it is said on rounds, 5) describing the contribution of families, nurses, and ancillary staff, and 6) providing teaching recommendations to senior physicians on rounds. All of these components are suggested by one or more of the participants in our study. In addition, our research identifies a variety of new work system‐related strategies, such as scheduling rounds, using computers appropriately on rounds, and providing training of HCT members beforehand.
Of particular interest was the discordance between strategies mentioned by families and the various members of the HCT. Although HCT members mentioned all identified strategies, families were interested in certain ones. Regarding the structure of FCR, families showed particular interest in HCT composition, timing and scheduling of rounds, location of rounds, and positioning of the HCT. In comparison, families did not mention the importance of the roles and duties of HCT members, HCT preparation for rounds, and use of computers during rounds. With respect to the FCR process, families stressed the importance of family preparation beforehand, introduction and explanation of rounds at the beginning, presentation style and communication style, customization, and management of distractions during rounds. None of the families, however, mentioned the rest of the strategies, including HCT preparation before rounds, involvement of the nurse, teaching and performing the physical exam, the role of the attending and senior resident roles during rounds, and following up with the family after rounds. These different perspectives are likely, in part, inherent to the different roles and experiences of parents and HCT members. For example, parents' knowledge of what goes on in the hospital outside of FCR, such as orientation and preparation of HCT members for rounds, is relatively limited. Future research using methods to evaluate and prioritize strategies as well as understanding reasons for contradicting strategies is warranted.
We recognize that, although family engagement is recommended as a critical component of care, strategies to improve engagement may be in direct opposition to other goals of the HCT. For example, some of our participants suggest having a smaller team may be more beneficial for family engagement on rounds. In some settings, it may be feasible to have a small team; however, in institutions that accommodate a large number of learners, excluding students from the teaching opportunity of rounds may actually compromise educational experiences. In patients with chronic and/or complex care, a larger multidisciplinary team may better facilitate information exchange among disciplines and expedite discharge planning. Moreover, one might speculate that it may not be that the size affects family engagement as much as the composition of the team, especially if tailored to the needs of the patient. For example, a large team consisting of primarily physicians and trainees may not be as engaging as the same sized team with one attending physician and a respiratory therapist, case manager, and consulting subspecialist. Finding a balance between engaging families, teaching learners, and maintaining efficiency is paramount and needs to be studied further.
This study has several limitations. Our data are from a single academic children's hospital, which may limit generalizability due to a small sampling of multiple stakeholders on different services, our specific patient population, HCT composition and roles, and teaching needs. However, we face similar barriers to engaging families during rounds as those published from both another single institution[17] and a national sampling of pediatric hospitalists.[16] Furthermore, our recommended strategies to address the FCR process are supported by prior work.[17] Because this study was voluntary, our interviewees were likely more engaged participants in general. Specifically, the viewpoints of engaged families and HCT members may not represent the viewpoints of those who are less engaged or supportive of FCR. We did not enroll nonEnglish‐speaking patients and families, which is a potential direction for future research. In our interviews, we also relied solely on the perceptions of rounding participants, rather than those of outside observers or researchers, which may only provide a partial perspective of potential strategies to improve family engagement. Last, this qualitative research approach does not provide quantitative information regarding whether certain strategies are preferred by a majority of participants, which we hope to address in future research.
This work is part of a larger study that aims to implement a bundle of these strategies after stakeholder prioritization based on impact on family engagement, feasibility, and sustainability. We plan to systematically evaluate the implementation process of these strategies and measure their impact on family engagement and, ultimately, patient safety. One or more of these strategies could be implemented in a similar manner at other hospitals depending on specific institutional needs.
In conclusion, as recently reflected by Barry et al. in The New England Journal of Medicine, Although talk about patient‐centered care is ubiquitous in modern health care, one of the greatest challenges of turning the rhetoric into reality continues to be routinely engaging patients in decision making.[33] FCR provide a crucial opportunity for family involvement in daily care decisions in the pediatric inpatient setting. This study highlights the importance of prior work defining the components of involving families in this process, while emphasizing new systems‐based strategies that further facilitate the expectation of family engagement in the care of hospitalized children.
Disclosures
This work was funded through an Agency for Healthcare Research and Quality Health Services Research Dissemination and Demonstration Grant, R18 HS018680, and also supported by the Arthur Vining Davis Foundation and the National Patient Safety Foundation through the James S. Todd Memorial Research Award. Funding organizations did not contribute to the design and conduct of study; collection, management, analysis, and interpretation of data; or preparation, review, or approval of the manuscript. The authors report no conflicts of interest.
- , , , et al. The impact of patient‐centered care on outcomes. J Fam Pract. 2000;49:796–804.
- , , , et al. Observational study of effect of patient centredness and positive approach on outcomes of general practice consultations. BMJ. 2001;323:908–911.
- , , . Improvement in the family‐centered medical home enhances outcomes for children and youth with special healthcare needs. J Ambul Care Manage. 2009;32:188–196.
- , , . Associations of family‐centered care with health care outcomes for children with special health care needs. Matern Child Health J. 2011;15:794–805.
- , , , , Can a patient‐centered medical home lead to better patient outcomes? The quality implications of Geisinger's ProvenHealth Navigator. Am J Med Qual. 2012;27:210–216.
- , , . Perceptions of health care providers' communication: relationships between patient‐centered communication and satisfaction. Health Commun. 2004;16:363–383.
- , . Satisfaction with care and ease of using health care services among parents of children with special health care needs: the roles of race/ethnicity, insurance, language, and adequacy of family‐centered care. Pediatrics. 2006;117:1184–1196.
- , , , . A randomized, controlled trial of bedside versus conference‐room case presentation in a pediatric intensive care unit. Pediatrics. 2007;120:275–280.
- , , , , . Effect of patient‐centered care on patient satisfaction and quality of care. J Nurs Care Qual. 2008;23:316–321.
- , , . Implementing family‐centered rounds: pediatric residents' perceptions. Clin Pediatr (Phila) 2010;49:228–234.
- ACGME Program Requirements for Graduate Medical Education in Pediatrics. 2007. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq320_pediatrics_07012007.pdf. Accessed February 10, 2012.
- Speak up: prevent errors in your child's care. 2011. The Joint Commission Web site. Available at: http://www.jointcommission.org/Speak_Up_Prevent_Errors_in_Your_Childs_Care/. Accessed May 11, 2012.
- Patient‐ and family‐centered care and the pediatrician's role. Pediatrics. 2012;129:394–404.
- Committee on Quality of Health Care in America, Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: The National Academies Press; 2001.
- , , , . Defining family‐centered rounds. Teach Learn Med. 2007;19:319–322.
- , , , et al. Family‐centered rounds on pediatric wards: A PRIS network survey of US and Canadian hospitalists. Pediatrics. 2010;126:37–43.
- , , , , . Family‐centered bedside rounds: a new approach to patient care and teaching. Pediatrics. 2007;119:829–832.
- , , , . Parental responses to involvement in rounds on a pediatric inpatient unit at a teaching hospital: a qualitative study. Acad Med. 2008;83:292–297.
- , , , et al. Work system design for patient safety: the SEIPS model. Qual Saf Health Care. 2006;15:i50–i58.
- , . IPR—a validated model for the 1990s and beyond. Couns Psychol. 1990;18:436–440.
- , . Auto‐ and allo‐confrontation as tools for reflective activities. Appl Ergon. 2004;35:531–540.
- . Qualitative Research and Evaluation Methods. 3rd ed. Thousand Oaks, CA: Sage Publications; 2002.
- , . Doing Qualitative Research. 2nd ed. Thousand Oaks, CA: Sage Publications; 1999.
- . Sample size in qualitative research. Res Nurs Health. 1995;18:179–183.
- , . Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. Newbury Park, CA: Sage Publications; 1998.
- , . Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24:105–112.
- . A purposeful approach to the constant comparative method in the analysis of qualitative interviews. Qual Quant. 2002;36:391–409.
- . Theoretical Sensitivity: Advances in the Methodology of Grounded Theory. Mill Valley, CA: Sociology Press; 1978.
- , . Balance theory of job design. In: Karwowski W, ed. International Encyclopedia of Ergonomics and Human Factors. London: Taylor 2000:1181–1184.
- , . A balance theory of job design for stress reduction. Int J Ind Ergon. 1989;4:67–79.
- Institute for Patient‐ and Family‐Centered Care. Applying patient‐ and family‐centered concepts to bedside rounds. 2010. Available at: http://www.ipfcc.org/advance/topics/PH_RD_Applying_PFCC_Rounds_012009.pdf. Accessed May 11, 2012.
- . A fundamental shift: family‐centered rounds in an academic medical center. Hospitalist. 2006;10:45–46.
- , Shared decision making—pinnacle of patient‐centered care. N Engl J Med. 2012;366:780–781.
A growing body of literature suggests that patient‐ and family‐centered care can improve patient outcomes[1, 2, 3, 4, 5] as well as patient, family, and provider satisfaction.[6, 7, 8, 9, 10] Engaging patients and families as a way to improve the quality and safety of care has been widely endorsed by leading healthcare organizations,[11, 12, 13] including the Institute of Medicine.[14] In the pediatric inpatient setting, family‐centered rounds (FCR), defined as bedside rounds in which the patient and family share in the control of the management plan as well as in the evaluation of the process itself,[15] potentially provide a consistent venue for family engagement and are recommended by the American Academy of Pediatrics as standard practice.[13]
According to a recent study by Mittal et al.,[16] FCR are the most common type of rounds practiced among pediatric hospitalists surveyed in the United States and Canada. Despite this widespread shift from rounding in a conference room to the bedside with patients and families, there exist only a few studies that provide specific recommendations on conducting FCR.[15, 17, 18] This research has been limited, primarily focusing how rounds are conducted, and further investigation is needed to identify the impact of other processes and elements within the hospital work system that may also affect family engagement during rounds.
The objectives of this study were to: 1) identify strategies to enhance family engagement during FCR drawing from the viewpoints of the various stakeholders on rounds, and 2) characterize these strategies into known elements of hospital work systems and rounding processes using a recognized human factors engineering approach, The Systems Engineering Initiative for Patient Safety (SEIPS) model.[19] According to the SEIPS model, barriers and facilitators to family engagement during FCR are likely embedded in the design of the hospital work systems and rounding process; therefore, we hypothesized that strategies that influence engagement will target all work system and process elements. This work is part of a larger study in which, after prioritization of this group of strategies based on feasibility and sustainability, a bundle of best practices for conducting FCR will be developed, implemented, and evaluated.
METHODS
Study Design
Semistructured interviews using the stimulated recall approach[20, 21] were conducted to understand the cognitive processes of families and healthcare team (HCT) members during FCR. This qualitative study design allowed us to capture comprehensive information from the perspectives of a diverse group of stakeholders on strategies for improving family engagement during FCR.
Setting and Participants
This study was conducted at a children's hospital in Wisconsin, where FCR were initiated in 2007 with the transition to a new hospital facility. The expectation is that FCR are conducted daily with the family and the patient's HCT, consisting of at least an attending physician and nurse. Typically, multiple residents, interns, and medical students are present along with a combination of other providers, including consulting subspecialists, a fellow, nurse practitioner, respiratory therapist, or pharmacist. When this study was conducted, attendees received little to no formal training regarding their role on FCR. As part of a larger study, English‐speaking patients and/or families admitted to 1 of 4 inpatient services (2 hospitalist, 1 pulmonary, and 1 hematology/oncology), and their associated HCT members were enrolled and their bedside rounds were video recorded. A purposive sampling technique[22, 23] was employed, recruiting interviewees that represented the various groups of stakeholders of rounds, including parents, children, attending physicians, resident physicians, medical students, and nurses. For child interviews, we restricted selection to children aged 8 to 17 years to ensure the ability to understand the interviewing process and provide feedback. Families were consented and children were assented. The University of Wisconsin‐Madison Health Sciences Institutional Review Board approved this study.
Interviews and analysis occurred concurrently in an iterative process, informing each other. Thus, recruitment continued until we reached theoretical saturation,[24, 25] the point at which additional interviews did not provide new information or further conceptual development.
Study Procedures
All interviews were conducted by trained researchers, who used the same semistructured interview guide. During each interview, the interviewee was instructed to watch his/her own rounding video and pause when noticing something that made it easy (facilitator) or hard (barrier) to engage the family. Every time the interviewee paused the video to describe what was noticed, the interviewer then asked follow‐up, open‐ended questions to solicit specific information that focused on strategies for enhancing family engagement during FCR. For instance, if the issue identified was a barrier, the interviewer asked, What would you have wanted to happen differently? and if the issue identified was a facilitator, the interviewer asked, How could we ensure that would happen for everyone? The interviewee rewound the video as needed. If the interviewee had not stopped the video by the halfway point, the interviewer would pause the video and review the instructions. After the interviewee had viewed and commented on the entire rounding video, an opportunity was offered to reflect on other factors that influence family engagement during rounds, and additional questions were asked as necessary to fully understand the interviewee's views. All interviews were audio recorded and personal identifiers were removed prior to data analysis.
Data Analysis
Two research assistants reviewed the audio recordings and identified all instances related to strategies for improving family engagement during FCR. There was no screening of strategies (ie, if an interviewee suggested a strategy was related to improving family engagement, it was categorized as such). To ensure intercoder reliability, these assistants, under the supervision of a researcher (L.D.), reviewed the coding process together, held consensus meetings, and crosschecked interviews for coding consensus. A researcher (A.X.) transcribed all strategy‐related instances, which were then reviewed by two additional researchers (M.K., P.C.). To organize, sort, and code the data, interview transcripts were imported in the NVivo qualitative data analysis software (QSR International, Doncaster, Victoria, Australia). The research group then performed a qualitative content analysis of the transcripts[26] and categorized the strategies in an iterative process (information provided on request).
To ensure that all strategies remained conceptually similar within categories, the constant comparative method[27, 28] was applied to the coding process. This involved comparing: 1) strategy‐related instances from the same participants, 2) strategy‐related instances from different participants in the same groups, 3) strategy‐related instances from different participants in different groups, 4) a coded strategy with other coded strategies, 5) coded strategies with categories, and 6) a category with other categories. A strategy‐related instance could be coded under more than one strategy or category. For instance, one interviewee said conducting things that can be done without family beforehand, and presenting and reviewing the plan with family. This was coded under both the strategy conducting rounds in another location without family and then at the bedside with family in the location of FCR category and the strategy focusing presentation on assessment and plan in the communication style category.
RESULTS
A total of 37 interviews were conducted with 11 parents, 4 children, and 22 HCT members (8 attending physicians, 6 resident physicians, 5 medical students, and 3 nurses) in 24 videos of rounding sessions. The duration of the interviews ranged from 30 to 60 minutes.
A total of 338 separate instances related to strategies for improving family engagement on FCR were identified and sorted into 21 categories. Using the SEIPS model, these categories were organized into 2 themes: the work system and process of FCR (Figure 1). Of the 21 categories, 12 were mentioned by both families (parents and/or children) and HCT members and 9 were solely mentioned by the HCT.
Work System of FCR
Table 1 shows the categories of strategies related to the 5 elements of the FCR work system.[29, 30] Illustrative quotes from the interviews (Q) are presented in Table 2.
| Work System Elements | Categories | Strategies | P (11) | C (4) | Att. (8) | Res. (6) | MS (5) | RN (3) |
|---|---|---|---|---|---|---|---|---|
| ||||||||
| People | 1. Size and composition of HCT | Have a smaller HCT conduct FCR | X | X | X | X | ||
| Ensure all relevant disciplines present on FCR | X | X | X | X | X | |||
| Task | 2. Roles and duties of HCT members | Define roles/duties of HCT members on FCR | X | X | ||||
| Organization | 3. Timing and scheduling of FCR | Schedule FCR, inform participants beforehand | X | X | X | |||
| 4. Training of HCT for FCR | Train HCT on how to present on FCR | X | X | |||||
| Environment | 5. Location of FCR | At bedside with family and patient | X | X | ||||
| In another location with HCT, then at bedside | X | X | X | X | ||||
| In another location with family but without child | X | |||||||
| 6. Positioning of HCT members on FCR | Sit down with family | X | X | X | X | X | ||
| Stand close to or in a semicircle around family | X | X | X | X | X | |||
| Tools and technologies | 7. Use of computers on FCR | Use computer to support family interaction | X | X | X | X | ||
| Don't use a computer | X | X | ||||||
|
| Q1: I'm intimidated to ask a question. It seems like there are too many peopleI like a smaller group. (P5) |
| Q2: Sometimes rounds are the only time that the parents are there to see the entire teamso in that way, including [the entire team] at the rounds makes more sense. (MS1) |
| Q3: There needs to be much more clear roles about who is supposed to do what, and it should be predictable. (Att.2) |
| Q4: ([T]iming of rounds) is a huge source of frustration for families. If [physicians] know in which order they will go for patients, they can call our charge nurse or unit clerk or page nurses with that information. (RN1) |
| Q5: ([W]ith a notice of the rounding schedule), I can be ahead of time, trying to think of questions. (P10) |
| Q6: [I]t would be really nice to see somebody do a presentation in a medical eye's version and then also in the family‐centered version. (MS5) |
| Q7: [H]aving the medical students practice with the senior residentis a good way of doing it. (Res.4) |
| Q8: [M]aybe some small groups where you practice this among students. (MS5) |
| Q9: It would be better to be in the room for communication. (Att.1) |
| Q10: You could have sort of hallway rounds, which is much more medical oriented, and inside‐the‐room rounds, which is much more talking with the parent. (P1) |
| Q11: [H]ave sit‐down rounds with parents and families. (Res.5) |
| Q12: I've seen some attending physicians who sat down. I think that could be helpful to be on the same level as the patient and family. (Res.2) |
| Q13: [M]aybe formation of semicircle or something like that, where we can see everybody a little more clearly, I think that would be very helpful. (P10) |
| Q14: I find the presence of a computer incredibly offensive and obstructivewhen you are supposed to be able to interact with the patient. (Att.6) |
| Q15: One of the things I started doing is having one of the other resident physicians have the computer, so just relying on them to do the orders, and me just being there mainly for being the presenter of rounds. (Res.4) |
People
Two seemingly contradictory strategies were proposed. Some interviewees suggested a smaller HCT with members most familiar to the family (Q1), whereas other interviewees stressed the need to involve different relevant disciplines (eg, social worker, nutritionist) during rounds (Q2).
Tasks
Both attending and resident physicians emphasized the importance of defining the role of each HCT member before rounding (Q3). Interviewees also suggested these roles should be explained to families, ideally at admission.
Organization
Many interviewees suggested the need to consistently schedule rounds (Q4) and to inform families and nurses of the schedule so all parties could plan ahead (Q5). Some resident physicians and medical students recommended training of learners on how to give a family‐centered presentation using methods such as role modeling (Q6) and practicing with the senior resident physician (Q7) or in small groups (Q8).
Environment
Some interviewees suggested conducting rounds in patient rooms (Q9). Others suggested conducting rounds first in another location (eg, hallway) without the family and then going to the bedside to round with the family (Q10). There were also interviewees who suggested conducting rounds in another location (eg, conference room) with the family (Q11). When conducting rounds in the patient room, some interviewees suggested that some HCT members (eg, attending and senior resident physicians) could sit down with the family (Q12), with the rest of the HCT standing close to the family in a semicircle (Q13).
Tools and Technologies
Some interviewees thought that conversation with families could be negatively affected by the use of computers, and therefore suggested not using them on FCR (Q14). Alternatively, other interviewees considered computers a tool to facilitate the interaction between the HCT and families, such as showing x‐rays or lab values. Several interviewees suggested that computers should not be positioned to block eye contact between HCT members and families; therefore, only HCT members not presenting should use computers (Q15).
Process of FCR
Table 3 shows the categories of strategies related to the process of FCR, which were categorized into 3 phases. Illustrative quotes are presented in Table 4.
| Process Phases | Categories | Strategies | P (11) | C (4) | Att. (8) | Res. (6) | MS (5) | RN (3) |
|---|---|---|---|---|---|---|---|---|
| ||||||||
| Before FCR | 8. HCT preparation | Collect and prepare pertinent information | X | X | X | X | ||
| 9. Family preparation | Orient family to rounding process | X | X | X | X | X | ||
| Build relationship with family | X | X | X | |||||
| Ask family for permission and preferences | X | X | X | |||||
| During FCR | 10. Introduction and explanation of FCR | Introduce HCT and family to each other | X | X | X | X | X | |
| Explain interactive rounding process | X | X | X | |||||
| 11. Active involvement of nurse | Giving nurse opportunity to actively participate | X | X | |||||
| 12. Communication with family | Give family opportunity to actively participate | X | X | X | X | X | X | |
| Address family's questions/concerns | X | X | X | X | X | |||
| Explain tests, findings and results to family | X | X | X | X | X | |||
| Confirm family understanding | X | X | X | |||||
| 13. Giving presentation | Restructure the presentation | X | X | |||||
| Shorten the presentation | X | X | X | |||||
| Focus presentation on assessment and plan | X | X | X | X | X | |||
| Summarize plan for family | X | X | X | |||||
| Avoid discussion of sensitive topics | X | X | X | |||||
| 14. Communication style | Present in a conversational manner | X | X | X | ||||
| Use an engaging communication style | X | X | X | X | X | |||
| 15. Language used | Use qualitative language | X | X | X | ||||
| Use plain language | X | X | X | X | X | |||
| 16. Performing physical exam | Pause and confirm physical exam | X | ||||||
| 17. Managing distractions | Minimize distractions and interruptions | X | X | X | X | X | X | |
| 18. Senior physician leading/role modeling | Attending/senior resident physician should lead, direct and be a role model on FCR rounds | X | X | |||||
| 19. Teaching | Ask family permission and involve in teaching | X | X | |||||
| 20. Customizing FCR for family | Adapt rounds to family's needs | X | X | X | X | |||
| After FCR | 21. Following up with family | HCT members follow up with family | X | X | X | |||
|
| Q1: [Medical students and residents] actually had a chance to do a quick round, an abbreviated presentation to put together an outline of what we're going to talk about before we even do it. (MS2) |
| Q2: I would like to know exactly what's going onbefore I walk in. (Att.6) |
| Q3: [T]he nurse did give me the fore‐warning that rounds would be coming and it was usually like a group of 8 to 10so I was prepared for that. (P7) |
| Q4: What went well is that I had already connected with this mom and the daughter prior to this rounding encounter. (Res.3) |
| Q5: [Y]ou could ask the patient or the parents if they want the child there. (P3) |
| Q6: [Families] really want to know what your role is on the team. (Att.5) |
| Q7: I guess it would be easier to figure out who you need to direct questions to. (P3) |
| Q8: [L]etting the family anticipate what rounding is going to be like and when the opportunity is going to come up to talk. I think that can help. (Res.2) |
| Q9: I think the decision making is probably the most critical partthere is really no substitute for [families] being involved in the decisionwithout a lot of medical conversation and analysis. (P1) |
| Q10: The family was proactive enough to ask questions, but they were never really given entrance to ask questions.No one had said do you have any questions?' (Res.4) |
| Q11: It is really important for the doctors to listen to them, to know that they are the parents and they know their children best. (RN3) |
| Q12: I think sometimes when you are teaching, some of the information could potentially be scary to the family. What I would hope is letting the family feel like they are part of the education process. (Res.2) |
| Q13: Sometimes nurses are asked initially, do you have anything to add,' which I think is a good way to startbecause we have probably the most current and updated information. (RN1) |
| Q14: When I was talking about the physical exam partmaybe at that point, if I could just stop talking, we couldconfirm that exam. (Res.3) |
| Q15: It's distracting if different groups have individual discussions when you are trying to keep the group focused on this particular patient for rounds. (Att.7) |
| Q16: It's just the basic thing that I try to tell residents. I do this hopefully at least once every time I am on services with the team. (Att.1) |
| Q17: ([C]hanging rounds depending on the families) would be the ideal situationthinking about what's helpful for a family. (Att.6) |
| Q18: What I usually see when things work well after we leave is that the nurse can still stick around the family. (Res.4) |
| Q19: [T]he students have to go back in the afternoon to talk with the family about what the treatment point is and answer any questions. (MS2) |
Before FCR
To engage families during FCR, many interviewees suggested that both the HCT and families need preparation. HCT members suggested that medical students should collect up‐to‐date patient information and review it with the senior resident physicians (Q1) to reach a consensus before starting FCR (Q2). To prepare families for rounds, parents and HCT members suggested that the HCT should orient families to the rounding process (Q3), build relationships with families (Q4), and ask for their permission and preference regarding participation in rounds (Q5).
During FCR
A number of strategies focused on the beginning of rounds. Parents, children, and HCT members stressed the need to introduce HCT members by role (Q6) and inform families to whom to direct questions (Q7). It was also suggested that parents introduce themselves to the team. Some interviewees recommended that the HCT explain the rounding process to families at this time (Q8).
Interviewees recommended strategies related to communication between the HCT and families during rounds. Many interviewees suggested restructuring and shortening the presentation by focusing on the assessment and plan (Q9). According to all interviewees, the HCT should present in a conversational manner and use an engaging communication style (eg, smiling, making eye contact, using appropriate humor) and appropriate language (eg, qualitative trend instead of numbers, plain language instead of medical jargon) to communicate with families. To ensure families understanding, HCT members should encourage and address their questions and concerns (Q10). In addition, families should be given the opportunity to provide information (eg, patient history and overnight events) and to express their opinions about the plan (Q11). If teaching is done during rounds, the HCT should involve families and ask for permission (Q12).
Other strategies on rounds were suggested, such as giving nurses the opportunity to actively participate (Q13), pausing and confirming physical exam findings (Q14), minimizing distractions and interruptions (Q15), attending and/or senior resident physicians leading and being role models for FCR (Q16), and adapting rounds to families' needs (Q17).
After FCR
Some HCT members talked about the importance of following up with families after rounds. Specifically, suggestions that nurses could stay with families immediately after rounds (Q18) were made, whereas physicians could return to families later in the day (Q19).
DISCUSSION
Using recognized qualitative systems engineering methods, we identified a broad range of strategies for enhancing family engagement on FCR from the perspectives of a diverse group of stakeholders on rounds and described how these strategies target known fundamental elements in both the hospital work system and rounding process. We highlight recommendations on the content and style of communication during rounds with families, but also introduce more complex system‐wide elements that likely play a role in family engagement, such as the composition of the HCT; organization and environment of rounds; tools and technologies used; and preparation of the HCT, families, and patients beforehand.
Our research both confirms and builds upon practices previously described in the FCR literature.[17, 31, 32] In a case report by Muething et al.,[17] recommendations were developed using a series of plan‐do‐study‐act cycles to determine the components needed to conduct FCR. These components included: 1) determining family preference prior to rounds, 2) defining HCT roles, 3) introducing HCT to family and explaining the purpose of rounds, 4) describing what is shared and how it is said on rounds, 5) describing the contribution of families, nurses, and ancillary staff, and 6) providing teaching recommendations to senior physicians on rounds. All of these components are suggested by one or more of the participants in our study. In addition, our research identifies a variety of new work system‐related strategies, such as scheduling rounds, using computers appropriately on rounds, and providing training of HCT members beforehand.
Of particular interest was the discordance between strategies mentioned by families and the various members of the HCT. Although HCT members mentioned all identified strategies, families were interested in certain ones. Regarding the structure of FCR, families showed particular interest in HCT composition, timing and scheduling of rounds, location of rounds, and positioning of the HCT. In comparison, families did not mention the importance of the roles and duties of HCT members, HCT preparation for rounds, and use of computers during rounds. With respect to the FCR process, families stressed the importance of family preparation beforehand, introduction and explanation of rounds at the beginning, presentation style and communication style, customization, and management of distractions during rounds. None of the families, however, mentioned the rest of the strategies, including HCT preparation before rounds, involvement of the nurse, teaching and performing the physical exam, the role of the attending and senior resident roles during rounds, and following up with the family after rounds. These different perspectives are likely, in part, inherent to the different roles and experiences of parents and HCT members. For example, parents' knowledge of what goes on in the hospital outside of FCR, such as orientation and preparation of HCT members for rounds, is relatively limited. Future research using methods to evaluate and prioritize strategies as well as understanding reasons for contradicting strategies is warranted.
We recognize that, although family engagement is recommended as a critical component of care, strategies to improve engagement may be in direct opposition to other goals of the HCT. For example, some of our participants suggest having a smaller team may be more beneficial for family engagement on rounds. In some settings, it may be feasible to have a small team; however, in institutions that accommodate a large number of learners, excluding students from the teaching opportunity of rounds may actually compromise educational experiences. In patients with chronic and/or complex care, a larger multidisciplinary team may better facilitate information exchange among disciplines and expedite discharge planning. Moreover, one might speculate that it may not be that the size affects family engagement as much as the composition of the team, especially if tailored to the needs of the patient. For example, a large team consisting of primarily physicians and trainees may not be as engaging as the same sized team with one attending physician and a respiratory therapist, case manager, and consulting subspecialist. Finding a balance between engaging families, teaching learners, and maintaining efficiency is paramount and needs to be studied further.
This study has several limitations. Our data are from a single academic children's hospital, which may limit generalizability due to a small sampling of multiple stakeholders on different services, our specific patient population, HCT composition and roles, and teaching needs. However, we face similar barriers to engaging families during rounds as those published from both another single institution[17] and a national sampling of pediatric hospitalists.[16] Furthermore, our recommended strategies to address the FCR process are supported by prior work.[17] Because this study was voluntary, our interviewees were likely more engaged participants in general. Specifically, the viewpoints of engaged families and HCT members may not represent the viewpoints of those who are less engaged or supportive of FCR. We did not enroll nonEnglish‐speaking patients and families, which is a potential direction for future research. In our interviews, we also relied solely on the perceptions of rounding participants, rather than those of outside observers or researchers, which may only provide a partial perspective of potential strategies to improve family engagement. Last, this qualitative research approach does not provide quantitative information regarding whether certain strategies are preferred by a majority of participants, which we hope to address in future research.
This work is part of a larger study that aims to implement a bundle of these strategies after stakeholder prioritization based on impact on family engagement, feasibility, and sustainability. We plan to systematically evaluate the implementation process of these strategies and measure their impact on family engagement and, ultimately, patient safety. One or more of these strategies could be implemented in a similar manner at other hospitals depending on specific institutional needs.
In conclusion, as recently reflected by Barry et al. in The New England Journal of Medicine, Although talk about patient‐centered care is ubiquitous in modern health care, one of the greatest challenges of turning the rhetoric into reality continues to be routinely engaging patients in decision making.[33] FCR provide a crucial opportunity for family involvement in daily care decisions in the pediatric inpatient setting. This study highlights the importance of prior work defining the components of involving families in this process, while emphasizing new systems‐based strategies that further facilitate the expectation of family engagement in the care of hospitalized children.
Disclosures
This work was funded through an Agency for Healthcare Research and Quality Health Services Research Dissemination and Demonstration Grant, R18 HS018680, and also supported by the Arthur Vining Davis Foundation and the National Patient Safety Foundation through the James S. Todd Memorial Research Award. Funding organizations did not contribute to the design and conduct of study; collection, management, analysis, and interpretation of data; or preparation, review, or approval of the manuscript. The authors report no conflicts of interest.
A growing body of literature suggests that patient‐ and family‐centered care can improve patient outcomes[1, 2, 3, 4, 5] as well as patient, family, and provider satisfaction.[6, 7, 8, 9, 10] Engaging patients and families as a way to improve the quality and safety of care has been widely endorsed by leading healthcare organizations,[11, 12, 13] including the Institute of Medicine.[14] In the pediatric inpatient setting, family‐centered rounds (FCR), defined as bedside rounds in which the patient and family share in the control of the management plan as well as in the evaluation of the process itself,[15] potentially provide a consistent venue for family engagement and are recommended by the American Academy of Pediatrics as standard practice.[13]
According to a recent study by Mittal et al.,[16] FCR are the most common type of rounds practiced among pediatric hospitalists surveyed in the United States and Canada. Despite this widespread shift from rounding in a conference room to the bedside with patients and families, there exist only a few studies that provide specific recommendations on conducting FCR.[15, 17, 18] This research has been limited, primarily focusing how rounds are conducted, and further investigation is needed to identify the impact of other processes and elements within the hospital work system that may also affect family engagement during rounds.
The objectives of this study were to: 1) identify strategies to enhance family engagement during FCR drawing from the viewpoints of the various stakeholders on rounds, and 2) characterize these strategies into known elements of hospital work systems and rounding processes using a recognized human factors engineering approach, The Systems Engineering Initiative for Patient Safety (SEIPS) model.[19] According to the SEIPS model, barriers and facilitators to family engagement during FCR are likely embedded in the design of the hospital work systems and rounding process; therefore, we hypothesized that strategies that influence engagement will target all work system and process elements. This work is part of a larger study in which, after prioritization of this group of strategies based on feasibility and sustainability, a bundle of best practices for conducting FCR will be developed, implemented, and evaluated.
METHODS
Study Design
Semistructured interviews using the stimulated recall approach[20, 21] were conducted to understand the cognitive processes of families and healthcare team (HCT) members during FCR. This qualitative study design allowed us to capture comprehensive information from the perspectives of a diverse group of stakeholders on strategies for improving family engagement during FCR.
Setting and Participants
This study was conducted at a children's hospital in Wisconsin, where FCR were initiated in 2007 with the transition to a new hospital facility. The expectation is that FCR are conducted daily with the family and the patient's HCT, consisting of at least an attending physician and nurse. Typically, multiple residents, interns, and medical students are present along with a combination of other providers, including consulting subspecialists, a fellow, nurse practitioner, respiratory therapist, or pharmacist. When this study was conducted, attendees received little to no formal training regarding their role on FCR. As part of a larger study, English‐speaking patients and/or families admitted to 1 of 4 inpatient services (2 hospitalist, 1 pulmonary, and 1 hematology/oncology), and their associated HCT members were enrolled and their bedside rounds were video recorded. A purposive sampling technique[22, 23] was employed, recruiting interviewees that represented the various groups of stakeholders of rounds, including parents, children, attending physicians, resident physicians, medical students, and nurses. For child interviews, we restricted selection to children aged 8 to 17 years to ensure the ability to understand the interviewing process and provide feedback. Families were consented and children were assented. The University of Wisconsin‐Madison Health Sciences Institutional Review Board approved this study.
Interviews and analysis occurred concurrently in an iterative process, informing each other. Thus, recruitment continued until we reached theoretical saturation,[24, 25] the point at which additional interviews did not provide new information or further conceptual development.
Study Procedures
All interviews were conducted by trained researchers, who used the same semistructured interview guide. During each interview, the interviewee was instructed to watch his/her own rounding video and pause when noticing something that made it easy (facilitator) or hard (barrier) to engage the family. Every time the interviewee paused the video to describe what was noticed, the interviewer then asked follow‐up, open‐ended questions to solicit specific information that focused on strategies for enhancing family engagement during FCR. For instance, if the issue identified was a barrier, the interviewer asked, What would you have wanted to happen differently? and if the issue identified was a facilitator, the interviewer asked, How could we ensure that would happen for everyone? The interviewee rewound the video as needed. If the interviewee had not stopped the video by the halfway point, the interviewer would pause the video and review the instructions. After the interviewee had viewed and commented on the entire rounding video, an opportunity was offered to reflect on other factors that influence family engagement during rounds, and additional questions were asked as necessary to fully understand the interviewee's views. All interviews were audio recorded and personal identifiers were removed prior to data analysis.
Data Analysis
Two research assistants reviewed the audio recordings and identified all instances related to strategies for improving family engagement during FCR. There was no screening of strategies (ie, if an interviewee suggested a strategy was related to improving family engagement, it was categorized as such). To ensure intercoder reliability, these assistants, under the supervision of a researcher (L.D.), reviewed the coding process together, held consensus meetings, and crosschecked interviews for coding consensus. A researcher (A.X.) transcribed all strategy‐related instances, which were then reviewed by two additional researchers (M.K., P.C.). To organize, sort, and code the data, interview transcripts were imported in the NVivo qualitative data analysis software (QSR International, Doncaster, Victoria, Australia). The research group then performed a qualitative content analysis of the transcripts[26] and categorized the strategies in an iterative process (information provided on request).
To ensure that all strategies remained conceptually similar within categories, the constant comparative method[27, 28] was applied to the coding process. This involved comparing: 1) strategy‐related instances from the same participants, 2) strategy‐related instances from different participants in the same groups, 3) strategy‐related instances from different participants in different groups, 4) a coded strategy with other coded strategies, 5) coded strategies with categories, and 6) a category with other categories. A strategy‐related instance could be coded under more than one strategy or category. For instance, one interviewee said conducting things that can be done without family beforehand, and presenting and reviewing the plan with family. This was coded under both the strategy conducting rounds in another location without family and then at the bedside with family in the location of FCR category and the strategy focusing presentation on assessment and plan in the communication style category.
RESULTS
A total of 37 interviews were conducted with 11 parents, 4 children, and 22 HCT members (8 attending physicians, 6 resident physicians, 5 medical students, and 3 nurses) in 24 videos of rounding sessions. The duration of the interviews ranged from 30 to 60 minutes.
A total of 338 separate instances related to strategies for improving family engagement on FCR were identified and sorted into 21 categories. Using the SEIPS model, these categories were organized into 2 themes: the work system and process of FCR (Figure 1). Of the 21 categories, 12 were mentioned by both families (parents and/or children) and HCT members and 9 were solely mentioned by the HCT.
Work System of FCR
Table 1 shows the categories of strategies related to the 5 elements of the FCR work system.[29, 30] Illustrative quotes from the interviews (Q) are presented in Table 2.
| Work System Elements | Categories | Strategies | P (11) | C (4) | Att. (8) | Res. (6) | MS (5) | RN (3) |
|---|---|---|---|---|---|---|---|---|
| ||||||||
| People | 1. Size and composition of HCT | Have a smaller HCT conduct FCR | X | X | X | X | ||
| Ensure all relevant disciplines present on FCR | X | X | X | X | X | |||
| Task | 2. Roles and duties of HCT members | Define roles/duties of HCT members on FCR | X | X | ||||
| Organization | 3. Timing and scheduling of FCR | Schedule FCR, inform participants beforehand | X | X | X | |||
| 4. Training of HCT for FCR | Train HCT on how to present on FCR | X | X | |||||
| Environment | 5. Location of FCR | At bedside with family and patient | X | X | ||||
| In another location with HCT, then at bedside | X | X | X | X | ||||
| In another location with family but without child | X | |||||||
| 6. Positioning of HCT members on FCR | Sit down with family | X | X | X | X | X | ||
| Stand close to or in a semicircle around family | X | X | X | X | X | |||
| Tools and technologies | 7. Use of computers on FCR | Use computer to support family interaction | X | X | X | X | ||
| Don't use a computer | X | X | ||||||
|
| Q1: I'm intimidated to ask a question. It seems like there are too many peopleI like a smaller group. (P5) |
| Q2: Sometimes rounds are the only time that the parents are there to see the entire teamso in that way, including [the entire team] at the rounds makes more sense. (MS1) |
| Q3: There needs to be much more clear roles about who is supposed to do what, and it should be predictable. (Att.2) |
| Q4: ([T]iming of rounds) is a huge source of frustration for families. If [physicians] know in which order they will go for patients, they can call our charge nurse or unit clerk or page nurses with that information. (RN1) |
| Q5: ([W]ith a notice of the rounding schedule), I can be ahead of time, trying to think of questions. (P10) |
| Q6: [I]t would be really nice to see somebody do a presentation in a medical eye's version and then also in the family‐centered version. (MS5) |
| Q7: [H]aving the medical students practice with the senior residentis a good way of doing it. (Res.4) |
| Q8: [M]aybe some small groups where you practice this among students. (MS5) |
| Q9: It would be better to be in the room for communication. (Att.1) |
| Q10: You could have sort of hallway rounds, which is much more medical oriented, and inside‐the‐room rounds, which is much more talking with the parent. (P1) |
| Q11: [H]ave sit‐down rounds with parents and families. (Res.5) |
| Q12: I've seen some attending physicians who sat down. I think that could be helpful to be on the same level as the patient and family. (Res.2) |
| Q13: [M]aybe formation of semicircle or something like that, where we can see everybody a little more clearly, I think that would be very helpful. (P10) |
| Q14: I find the presence of a computer incredibly offensive and obstructivewhen you are supposed to be able to interact with the patient. (Att.6) |
| Q15: One of the things I started doing is having one of the other resident physicians have the computer, so just relying on them to do the orders, and me just being there mainly for being the presenter of rounds. (Res.4) |
People
Two seemingly contradictory strategies were proposed. Some interviewees suggested a smaller HCT with members most familiar to the family (Q1), whereas other interviewees stressed the need to involve different relevant disciplines (eg, social worker, nutritionist) during rounds (Q2).
Tasks
Both attending and resident physicians emphasized the importance of defining the role of each HCT member before rounding (Q3). Interviewees also suggested these roles should be explained to families, ideally at admission.
Organization
Many interviewees suggested the need to consistently schedule rounds (Q4) and to inform families and nurses of the schedule so all parties could plan ahead (Q5). Some resident physicians and medical students recommended training of learners on how to give a family‐centered presentation using methods such as role modeling (Q6) and practicing with the senior resident physician (Q7) or in small groups (Q8).
Environment
Some interviewees suggested conducting rounds in patient rooms (Q9). Others suggested conducting rounds first in another location (eg, hallway) without the family and then going to the bedside to round with the family (Q10). There were also interviewees who suggested conducting rounds in another location (eg, conference room) with the family (Q11). When conducting rounds in the patient room, some interviewees suggested that some HCT members (eg, attending and senior resident physicians) could sit down with the family (Q12), with the rest of the HCT standing close to the family in a semicircle (Q13).
Tools and Technologies
Some interviewees thought that conversation with families could be negatively affected by the use of computers, and therefore suggested not using them on FCR (Q14). Alternatively, other interviewees considered computers a tool to facilitate the interaction between the HCT and families, such as showing x‐rays or lab values. Several interviewees suggested that computers should not be positioned to block eye contact between HCT members and families; therefore, only HCT members not presenting should use computers (Q15).
Process of FCR
Table 3 shows the categories of strategies related to the process of FCR, which were categorized into 3 phases. Illustrative quotes are presented in Table 4.
| Process Phases | Categories | Strategies | P (11) | C (4) | Att. (8) | Res. (6) | MS (5) | RN (3) |
|---|---|---|---|---|---|---|---|---|
| ||||||||
| Before FCR | 8. HCT preparation | Collect and prepare pertinent information | X | X | X | X | ||
| 9. Family preparation | Orient family to rounding process | X | X | X | X | X | ||
| Build relationship with family | X | X | X | |||||
| Ask family for permission and preferences | X | X | X | |||||
| During FCR | 10. Introduction and explanation of FCR | Introduce HCT and family to each other | X | X | X | X | X | |
| Explain interactive rounding process | X | X | X | |||||
| 11. Active involvement of nurse | Giving nurse opportunity to actively participate | X | X | |||||
| 12. Communication with family | Give family opportunity to actively participate | X | X | X | X | X | X | |
| Address family's questions/concerns | X | X | X | X | X | |||
| Explain tests, findings and results to family | X | X | X | X | X | |||
| Confirm family understanding | X | X | X | |||||
| 13. Giving presentation | Restructure the presentation | X | X | |||||
| Shorten the presentation | X | X | X | |||||
| Focus presentation on assessment and plan | X | X | X | X | X | |||
| Summarize plan for family | X | X | X | |||||
| Avoid discussion of sensitive topics | X | X | X | |||||
| 14. Communication style | Present in a conversational manner | X | X | X | ||||
| Use an engaging communication style | X | X | X | X | X | |||
| 15. Language used | Use qualitative language | X | X | X | ||||
| Use plain language | X | X | X | X | X | |||
| 16. Performing physical exam | Pause and confirm physical exam | X | ||||||
| 17. Managing distractions | Minimize distractions and interruptions | X | X | X | X | X | X | |
| 18. Senior physician leading/role modeling | Attending/senior resident physician should lead, direct and be a role model on FCR rounds | X | X | |||||
| 19. Teaching | Ask family permission and involve in teaching | X | X | |||||
| 20. Customizing FCR for family | Adapt rounds to family's needs | X | X | X | X | |||
| After FCR | 21. Following up with family | HCT members follow up with family | X | X | X | |||
|
| Q1: [Medical students and residents] actually had a chance to do a quick round, an abbreviated presentation to put together an outline of what we're going to talk about before we even do it. (MS2) |
| Q2: I would like to know exactly what's going onbefore I walk in. (Att.6) |
| Q3: [T]he nurse did give me the fore‐warning that rounds would be coming and it was usually like a group of 8 to 10so I was prepared for that. (P7) |
| Q4: What went well is that I had already connected with this mom and the daughter prior to this rounding encounter. (Res.3) |
| Q5: [Y]ou could ask the patient or the parents if they want the child there. (P3) |
| Q6: [Families] really want to know what your role is on the team. (Att.5) |
| Q7: I guess it would be easier to figure out who you need to direct questions to. (P3) |
| Q8: [L]etting the family anticipate what rounding is going to be like and when the opportunity is going to come up to talk. I think that can help. (Res.2) |
| Q9: I think the decision making is probably the most critical partthere is really no substitute for [families] being involved in the decisionwithout a lot of medical conversation and analysis. (P1) |
| Q10: The family was proactive enough to ask questions, but they were never really given entrance to ask questions.No one had said do you have any questions?' (Res.4) |
| Q11: It is really important for the doctors to listen to them, to know that they are the parents and they know their children best. (RN3) |
| Q12: I think sometimes when you are teaching, some of the information could potentially be scary to the family. What I would hope is letting the family feel like they are part of the education process. (Res.2) |
| Q13: Sometimes nurses are asked initially, do you have anything to add,' which I think is a good way to startbecause we have probably the most current and updated information. (RN1) |
| Q14: When I was talking about the physical exam partmaybe at that point, if I could just stop talking, we couldconfirm that exam. (Res.3) |
| Q15: It's distracting if different groups have individual discussions when you are trying to keep the group focused on this particular patient for rounds. (Att.7) |
| Q16: It's just the basic thing that I try to tell residents. I do this hopefully at least once every time I am on services with the team. (Att.1) |
| Q17: ([C]hanging rounds depending on the families) would be the ideal situationthinking about what's helpful for a family. (Att.6) |
| Q18: What I usually see when things work well after we leave is that the nurse can still stick around the family. (Res.4) |
| Q19: [T]he students have to go back in the afternoon to talk with the family about what the treatment point is and answer any questions. (MS2) |
Before FCR
To engage families during FCR, many interviewees suggested that both the HCT and families need preparation. HCT members suggested that medical students should collect up‐to‐date patient information and review it with the senior resident physicians (Q1) to reach a consensus before starting FCR (Q2). To prepare families for rounds, parents and HCT members suggested that the HCT should orient families to the rounding process (Q3), build relationships with families (Q4), and ask for their permission and preference regarding participation in rounds (Q5).
During FCR
A number of strategies focused on the beginning of rounds. Parents, children, and HCT members stressed the need to introduce HCT members by role (Q6) and inform families to whom to direct questions (Q7). It was also suggested that parents introduce themselves to the team. Some interviewees recommended that the HCT explain the rounding process to families at this time (Q8).
Interviewees recommended strategies related to communication between the HCT and families during rounds. Many interviewees suggested restructuring and shortening the presentation by focusing on the assessment and plan (Q9). According to all interviewees, the HCT should present in a conversational manner and use an engaging communication style (eg, smiling, making eye contact, using appropriate humor) and appropriate language (eg, qualitative trend instead of numbers, plain language instead of medical jargon) to communicate with families. To ensure families understanding, HCT members should encourage and address their questions and concerns (Q10). In addition, families should be given the opportunity to provide information (eg, patient history and overnight events) and to express their opinions about the plan (Q11). If teaching is done during rounds, the HCT should involve families and ask for permission (Q12).
Other strategies on rounds were suggested, such as giving nurses the opportunity to actively participate (Q13), pausing and confirming physical exam findings (Q14), minimizing distractions and interruptions (Q15), attending and/or senior resident physicians leading and being role models for FCR (Q16), and adapting rounds to families' needs (Q17).
After FCR
Some HCT members talked about the importance of following up with families after rounds. Specifically, suggestions that nurses could stay with families immediately after rounds (Q18) were made, whereas physicians could return to families later in the day (Q19).
DISCUSSION
Using recognized qualitative systems engineering methods, we identified a broad range of strategies for enhancing family engagement on FCR from the perspectives of a diverse group of stakeholders on rounds and described how these strategies target known fundamental elements in both the hospital work system and rounding process. We highlight recommendations on the content and style of communication during rounds with families, but also introduce more complex system‐wide elements that likely play a role in family engagement, such as the composition of the HCT; organization and environment of rounds; tools and technologies used; and preparation of the HCT, families, and patients beforehand.
Our research both confirms and builds upon practices previously described in the FCR literature.[17, 31, 32] In a case report by Muething et al.,[17] recommendations were developed using a series of plan‐do‐study‐act cycles to determine the components needed to conduct FCR. These components included: 1) determining family preference prior to rounds, 2) defining HCT roles, 3) introducing HCT to family and explaining the purpose of rounds, 4) describing what is shared and how it is said on rounds, 5) describing the contribution of families, nurses, and ancillary staff, and 6) providing teaching recommendations to senior physicians on rounds. All of these components are suggested by one or more of the participants in our study. In addition, our research identifies a variety of new work system‐related strategies, such as scheduling rounds, using computers appropriately on rounds, and providing training of HCT members beforehand.
Of particular interest was the discordance between strategies mentioned by families and the various members of the HCT. Although HCT members mentioned all identified strategies, families were interested in certain ones. Regarding the structure of FCR, families showed particular interest in HCT composition, timing and scheduling of rounds, location of rounds, and positioning of the HCT. In comparison, families did not mention the importance of the roles and duties of HCT members, HCT preparation for rounds, and use of computers during rounds. With respect to the FCR process, families stressed the importance of family preparation beforehand, introduction and explanation of rounds at the beginning, presentation style and communication style, customization, and management of distractions during rounds. None of the families, however, mentioned the rest of the strategies, including HCT preparation before rounds, involvement of the nurse, teaching and performing the physical exam, the role of the attending and senior resident roles during rounds, and following up with the family after rounds. These different perspectives are likely, in part, inherent to the different roles and experiences of parents and HCT members. For example, parents' knowledge of what goes on in the hospital outside of FCR, such as orientation and preparation of HCT members for rounds, is relatively limited. Future research using methods to evaluate and prioritize strategies as well as understanding reasons for contradicting strategies is warranted.
We recognize that, although family engagement is recommended as a critical component of care, strategies to improve engagement may be in direct opposition to other goals of the HCT. For example, some of our participants suggest having a smaller team may be more beneficial for family engagement on rounds. In some settings, it may be feasible to have a small team; however, in institutions that accommodate a large number of learners, excluding students from the teaching opportunity of rounds may actually compromise educational experiences. In patients with chronic and/or complex care, a larger multidisciplinary team may better facilitate information exchange among disciplines and expedite discharge planning. Moreover, one might speculate that it may not be that the size affects family engagement as much as the composition of the team, especially if tailored to the needs of the patient. For example, a large team consisting of primarily physicians and trainees may not be as engaging as the same sized team with one attending physician and a respiratory therapist, case manager, and consulting subspecialist. Finding a balance between engaging families, teaching learners, and maintaining efficiency is paramount and needs to be studied further.
This study has several limitations. Our data are from a single academic children's hospital, which may limit generalizability due to a small sampling of multiple stakeholders on different services, our specific patient population, HCT composition and roles, and teaching needs. However, we face similar barriers to engaging families during rounds as those published from both another single institution[17] and a national sampling of pediatric hospitalists.[16] Furthermore, our recommended strategies to address the FCR process are supported by prior work.[17] Because this study was voluntary, our interviewees were likely more engaged participants in general. Specifically, the viewpoints of engaged families and HCT members may not represent the viewpoints of those who are less engaged or supportive of FCR. We did not enroll nonEnglish‐speaking patients and families, which is a potential direction for future research. In our interviews, we also relied solely on the perceptions of rounding participants, rather than those of outside observers or researchers, which may only provide a partial perspective of potential strategies to improve family engagement. Last, this qualitative research approach does not provide quantitative information regarding whether certain strategies are preferred by a majority of participants, which we hope to address in future research.
This work is part of a larger study that aims to implement a bundle of these strategies after stakeholder prioritization based on impact on family engagement, feasibility, and sustainability. We plan to systematically evaluate the implementation process of these strategies and measure their impact on family engagement and, ultimately, patient safety. One or more of these strategies could be implemented in a similar manner at other hospitals depending on specific institutional needs.
In conclusion, as recently reflected by Barry et al. in The New England Journal of Medicine, Although talk about patient‐centered care is ubiquitous in modern health care, one of the greatest challenges of turning the rhetoric into reality continues to be routinely engaging patients in decision making.[33] FCR provide a crucial opportunity for family involvement in daily care decisions in the pediatric inpatient setting. This study highlights the importance of prior work defining the components of involving families in this process, while emphasizing new systems‐based strategies that further facilitate the expectation of family engagement in the care of hospitalized children.
Disclosures
This work was funded through an Agency for Healthcare Research and Quality Health Services Research Dissemination and Demonstration Grant, R18 HS018680, and also supported by the Arthur Vining Davis Foundation and the National Patient Safety Foundation through the James S. Todd Memorial Research Award. Funding organizations did not contribute to the design and conduct of study; collection, management, analysis, and interpretation of data; or preparation, review, or approval of the manuscript. The authors report no conflicts of interest.
- , , , et al. The impact of patient‐centered care on outcomes. J Fam Pract. 2000;49:796–804.
- , , , et al. Observational study of effect of patient centredness and positive approach on outcomes of general practice consultations. BMJ. 2001;323:908–911.
- , , . Improvement in the family‐centered medical home enhances outcomes for children and youth with special healthcare needs. J Ambul Care Manage. 2009;32:188–196.
- , , . Associations of family‐centered care with health care outcomes for children with special health care needs. Matern Child Health J. 2011;15:794–805.
- , , , , Can a patient‐centered medical home lead to better patient outcomes? The quality implications of Geisinger's ProvenHealth Navigator. Am J Med Qual. 2012;27:210–216.
- , , . Perceptions of health care providers' communication: relationships between patient‐centered communication and satisfaction. Health Commun. 2004;16:363–383.
- , . Satisfaction with care and ease of using health care services among parents of children with special health care needs: the roles of race/ethnicity, insurance, language, and adequacy of family‐centered care. Pediatrics. 2006;117:1184–1196.
- , , , . A randomized, controlled trial of bedside versus conference‐room case presentation in a pediatric intensive care unit. Pediatrics. 2007;120:275–280.
- , , , , . Effect of patient‐centered care on patient satisfaction and quality of care. J Nurs Care Qual. 2008;23:316–321.
- , , . Implementing family‐centered rounds: pediatric residents' perceptions. Clin Pediatr (Phila) 2010;49:228–234.
- ACGME Program Requirements for Graduate Medical Education in Pediatrics. 2007. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq320_pediatrics_07012007.pdf. Accessed February 10, 2012.
- Speak up: prevent errors in your child's care. 2011. The Joint Commission Web site. Available at: http://www.jointcommission.org/Speak_Up_Prevent_Errors_in_Your_Childs_Care/. Accessed May 11, 2012.
- Patient‐ and family‐centered care and the pediatrician's role. Pediatrics. 2012;129:394–404.
- Committee on Quality of Health Care in America, Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: The National Academies Press; 2001.
- , , , . Defining family‐centered rounds. Teach Learn Med. 2007;19:319–322.
- , , , et al. Family‐centered rounds on pediatric wards: A PRIS network survey of US and Canadian hospitalists. Pediatrics. 2010;126:37–43.
- , , , , . Family‐centered bedside rounds: a new approach to patient care and teaching. Pediatrics. 2007;119:829–832.
- , , , . Parental responses to involvement in rounds on a pediatric inpatient unit at a teaching hospital: a qualitative study. Acad Med. 2008;83:292–297.
- , , , et al. Work system design for patient safety: the SEIPS model. Qual Saf Health Care. 2006;15:i50–i58.
- , . IPR—a validated model for the 1990s and beyond. Couns Psychol. 1990;18:436–440.
- , . Auto‐ and allo‐confrontation as tools for reflective activities. Appl Ergon. 2004;35:531–540.
- . Qualitative Research and Evaluation Methods. 3rd ed. Thousand Oaks, CA: Sage Publications; 2002.
- , . Doing Qualitative Research. 2nd ed. Thousand Oaks, CA: Sage Publications; 1999.
- . Sample size in qualitative research. Res Nurs Health. 1995;18:179–183.
- , . Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. Newbury Park, CA: Sage Publications; 1998.
- , . Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24:105–112.
- . A purposeful approach to the constant comparative method in the analysis of qualitative interviews. Qual Quant. 2002;36:391–409.
- . Theoretical Sensitivity: Advances in the Methodology of Grounded Theory. Mill Valley, CA: Sociology Press; 1978.
- , . Balance theory of job design. In: Karwowski W, ed. International Encyclopedia of Ergonomics and Human Factors. London: Taylor 2000:1181–1184.
- , . A balance theory of job design for stress reduction. Int J Ind Ergon. 1989;4:67–79.
- Institute for Patient‐ and Family‐Centered Care. Applying patient‐ and family‐centered concepts to bedside rounds. 2010. Available at: http://www.ipfcc.org/advance/topics/PH_RD_Applying_PFCC_Rounds_012009.pdf. Accessed May 11, 2012.
- . A fundamental shift: family‐centered rounds in an academic medical center. Hospitalist. 2006;10:45–46.
- , Shared decision making—pinnacle of patient‐centered care. N Engl J Med. 2012;366:780–781.
- , , , et al. The impact of patient‐centered care on outcomes. J Fam Pract. 2000;49:796–804.
- , , , et al. Observational study of effect of patient centredness and positive approach on outcomes of general practice consultations. BMJ. 2001;323:908–911.
- , , . Improvement in the family‐centered medical home enhances outcomes for children and youth with special healthcare needs. J Ambul Care Manage. 2009;32:188–196.
- , , . Associations of family‐centered care with health care outcomes for children with special health care needs. Matern Child Health J. 2011;15:794–805.
- , , , , Can a patient‐centered medical home lead to better patient outcomes? The quality implications of Geisinger's ProvenHealth Navigator. Am J Med Qual. 2012;27:210–216.
- , , . Perceptions of health care providers' communication: relationships between patient‐centered communication and satisfaction. Health Commun. 2004;16:363–383.
- , . Satisfaction with care and ease of using health care services among parents of children with special health care needs: the roles of race/ethnicity, insurance, language, and adequacy of family‐centered care. Pediatrics. 2006;117:1184–1196.
- , , , . A randomized, controlled trial of bedside versus conference‐room case presentation in a pediatric intensive care unit. Pediatrics. 2007;120:275–280.
- , , , , . Effect of patient‐centered care on patient satisfaction and quality of care. J Nurs Care Qual. 2008;23:316–321.
- , , . Implementing family‐centered rounds: pediatric residents' perceptions. Clin Pediatr (Phila) 2010;49:228–234.
- ACGME Program Requirements for Graduate Medical Education in Pediatrics. 2007. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq320_pediatrics_07012007.pdf. Accessed February 10, 2012.
- Speak up: prevent errors in your child's care. 2011. The Joint Commission Web site. Available at: http://www.jointcommission.org/Speak_Up_Prevent_Errors_in_Your_Childs_Care/. Accessed May 11, 2012.
- Patient‐ and family‐centered care and the pediatrician's role. Pediatrics. 2012;129:394–404.
- Committee on Quality of Health Care in America, Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: The National Academies Press; 2001.
- , , , . Defining family‐centered rounds. Teach Learn Med. 2007;19:319–322.
- , , , et al. Family‐centered rounds on pediatric wards: A PRIS network survey of US and Canadian hospitalists. Pediatrics. 2010;126:37–43.
- , , , , . Family‐centered bedside rounds: a new approach to patient care and teaching. Pediatrics. 2007;119:829–832.
- , , , . Parental responses to involvement in rounds on a pediatric inpatient unit at a teaching hospital: a qualitative study. Acad Med. 2008;83:292–297.
- , , , et al. Work system design for patient safety: the SEIPS model. Qual Saf Health Care. 2006;15:i50–i58.
- , . IPR—a validated model for the 1990s and beyond. Couns Psychol. 1990;18:436–440.
- , . Auto‐ and allo‐confrontation as tools for reflective activities. Appl Ergon. 2004;35:531–540.
- . Qualitative Research and Evaluation Methods. 3rd ed. Thousand Oaks, CA: Sage Publications; 2002.
- , . Doing Qualitative Research. 2nd ed. Thousand Oaks, CA: Sage Publications; 1999.
- . Sample size in qualitative research. Res Nurs Health. 1995;18:179–183.
- , . Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. Newbury Park, CA: Sage Publications; 1998.
- , . Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24:105–112.
- . A purposeful approach to the constant comparative method in the analysis of qualitative interviews. Qual Quant. 2002;36:391–409.
- . Theoretical Sensitivity: Advances in the Methodology of Grounded Theory. Mill Valley, CA: Sociology Press; 1978.
- , . Balance theory of job design. In: Karwowski W, ed. International Encyclopedia of Ergonomics and Human Factors. London: Taylor 2000:1181–1184.
- , . A balance theory of job design for stress reduction. Int J Ind Ergon. 1989;4:67–79.
- Institute for Patient‐ and Family‐Centered Care. Applying patient‐ and family‐centered concepts to bedside rounds. 2010. Available at: http://www.ipfcc.org/advance/topics/PH_RD_Applying_PFCC_Rounds_012009.pdf. Accessed May 11, 2012.
- . A fundamental shift: family‐centered rounds in an academic medical center. Hospitalist. 2006;10:45–46.
- , Shared decision making—pinnacle of patient‐centered care. N Engl J Med. 2012;366:780–781.
Copyright © 2013 Society of Hospital Medicine