User login
Step 1 scoring moves to pass/fail: Hospitalists’ role and unintended consequences
The National Board of Medical Examiners recently announced a change in the United States Medical Licensing Examination (USMLE) Step 1 score reporting from a 3-digit score to a pass/fail score beginning in 2022.1 Endorsed by a broad coalition of organizations involved in undergraduate (UME) and graduate medical education (GME), this change is intended as a first step toward systemic improvements in the UME-GME transition to residency by promoting holistic reviews of applicants. Additionally, it is meant to tackle widespread concerns about medical student distress brought about by the residency selection process. For example, switching to pass/fail preclinical curricula has resulted in an improvement in medical student well-being at many medical schools.2 It is the hope that a mirrored change in Step 1 may similarly improve mental health and encourage a growth mindset towards learning.

On the other hand, many residency programs rely on USMLE scores for screening potential candidates, especially as application inflation has burdened programs with thousands of applications.3 The change to a pass/fail Step 1 score will likely shift emphasis and stress to the Step 2 CK Exam, essentially negating the intended effect. Furthermore, for schools still reporting NBME Subject (shelf) Exam scores and Clerkship grades, there will likely be a greater emphasis placed on these metrics as well. The need for objective assessment methods are seen by many as so critical that some GME leaders have advocated for instituting entrance exams or requiring a Standardized Letter of Evaluation as a prerequisite to residency application. Finally, medical students jockeying for competitive residency positions may also feel pressured to distinguish themselves by boosting other aspects of their portfolio by taking a research year or applying for away electives, which risks marginalizing students of lesser means or with family responsibilities.
Ultimately, the change to a pass/fail Step 1 exam will likely do little to address the expanding gulf between the UME and GME communities. Residency program directors are searching for students with qualities of a good physician, such as interpersonal skills, “teamsmanship,” compassion, and professionalism, but reliable, objective, and standardized assessment tools are not available. Currently our best tools are clinical evaluations which are subject to grade inflation and implicit racial and gender biases. Furthermore, other components of a residency application, such as letters of recommendation, Chair’s letters, and the Medical Student Performance Evaluation (Dean’s letter), are regarded to be less informative as schools move toward no student rankings, pass/fail grading schemes, and nonstandardized summative adjectives to describe medical students overall medical school performance.
Finally, medical student distress in the residency application process may stem from the perpetuation of elitism that extends from medical school to fellowship training and academic hospital medicine. Rankings of medical schools, residencies, fellowships, and hospitals serve to create a hierarchical system. Competitive residency applicants see admittance into the best training programs as opening doors to opportunities, while not getting into these programs is seen as closing doors to career paths and opportunities.
With this change in Step 1 score reporting, where do we as hospitalists fit in? Hospitalists are at the forefront of educating and evaluating medical students in academic medical centers, and we are often asked to write letters of recommendation and serve as mentors. If done well, these activities can have a positive impact on medical student applications to residency by alleviating some of the stresses and mitigating the downsides to the new Step 1 scoring system. Writing impactful letters and thoughtful evaluations are all skills that should be incorporated in hospitalist faculty development programs. Moreover, in order to serve as better advocates for our students, it is important that academic hospitalists understand the evolving landscape of the residency application process and are mindful of the stresses that medical students face. Changing Step 1 scoring to pass/fail will likely have unintended consequences for our medical students, and we as hospitalists must be ready to improve our knowledge and skills in order to continue to support and advocate for our medical students.
Dr. Esquivel is a hospitalist and assistant professor at Weill Cornell Medical College in New York; Dr. Chang is associate professor and interprofessional education thread director (MD curriculum) at Washington University, St. Louis; Dr. Ricotta is a hospitalist at Beth Israel Deaconess Medical Center, Boston, and instructor in medicine at Harvard Medical School; Dr. Rendon is a hospitalist at the University of New Mexico in Albuquerque; Dr. Kwan is a hospitalist at the Veterans Affairs San Diego Healthcare System and associate professor at the University of California, San Diego. He is the chair of SHM’s Physicians in Training committee.
References
1. United States Medical Licensing Examination (2020 Feb). Change to pass/fail score reporting for Step 1.
2. Slavin SJ and Chibnall JT. Finding the why, changing the how: Improving the mental health of medical students, residents, and physicians. Academic Medicine. 2016;91(9):1194‐6.
3. Pereira AG, Chelminski PR, et al. Application inflation for internal medicine applicants in the Match: Drivers, consequences, and potential solutions. Am J Med. 2016 Aug;129(8): 885-91.
The National Board of Medical Examiners recently announced a change in the United States Medical Licensing Examination (USMLE) Step 1 score reporting from a 3-digit score to a pass/fail score beginning in 2022.1 Endorsed by a broad coalition of organizations involved in undergraduate (UME) and graduate medical education (GME), this change is intended as a first step toward systemic improvements in the UME-GME transition to residency by promoting holistic reviews of applicants. Additionally, it is meant to tackle widespread concerns about medical student distress brought about by the residency selection process. For example, switching to pass/fail preclinical curricula has resulted in an improvement in medical student well-being at many medical schools.2 It is the hope that a mirrored change in Step 1 may similarly improve mental health and encourage a growth mindset towards learning.
On the other hand, many residency programs rely on USMLE scores for screening potential candidates, especially as application inflation has burdened programs with thousands of applications.3 The change to a pass/fail Step 1 score will likely shift emphasis and stress to the Step 2 CK Exam, essentially negating the intended effect. Furthermore, for schools still reporting NBME Subject (shelf) Exam scores and Clerkship grades, there will likely be a greater emphasis placed on these metrics as well. The need for objective assessment methods are seen by many as so critical that some GME leaders have advocated for instituting entrance exams or requiring a Standardized Letter of Evaluation as a prerequisite to residency application. Finally, medical students jockeying for competitive residency positions may also feel pressured to distinguish themselves by boosting other aspects of their portfolio by taking a research year or applying for away electives, which risks marginalizing students of lesser means or with family responsibilities.
Ultimately, the change to a pass/fail Step 1 exam will likely do little to address the expanding gulf between the UME and GME communities. Residency program directors are searching for students with qualities of a good physician, such as interpersonal skills, “teamsmanship,” compassion, and professionalism, but reliable, objective, and standardized assessment tools are not available. Currently our best tools are clinical evaluations which are subject to grade inflation and implicit racial and gender biases. Furthermore, other components of a residency application, such as letters of recommendation, Chair’s letters, and the Medical Student Performance Evaluation (Dean’s letter), are regarded to be less informative as schools move toward no student rankings, pass/fail grading schemes, and nonstandardized summative adjectives to describe medical students overall medical school performance.
Finally, medical student distress in the residency application process may stem from the perpetuation of elitism that extends from medical school to fellowship training and academic hospital medicine. Rankings of medical schools, residencies, fellowships, and hospitals serve to create a hierarchical system. Competitive residency applicants see admittance into the best training programs as opening doors to opportunities, while not getting into these programs is seen as closing doors to career paths and opportunities.
With this change in Step 1 score reporting, where do we as hospitalists fit in? Hospitalists are at the forefront of educating and evaluating medical students in academic medical centers, and we are often asked to write letters of recommendation and serve as mentors. If done well, these activities can have a positive impact on medical student applications to residency by alleviating some of the stresses and mitigating the downsides to the new Step 1 scoring system. Writing impactful letters and thoughtful evaluations are all skills that should be incorporated in hospitalist faculty development programs. Moreover, in order to serve as better advocates for our students, it is important that academic hospitalists understand the evolving landscape of the residency application process and are mindful of the stresses that medical students face. Changing Step 1 scoring to pass/fail will likely have unintended consequences for our medical students, and we as hospitalists must be ready to improve our knowledge and skills in order to continue to support and advocate for our medical students.
Dr. Esquivel is a hospitalist and assistant professor at Weill Cornell Medical College in New York; Dr. Chang is associate professor and interprofessional education thread director (MD curriculum) at Washington University, St. Louis; Dr. Ricotta is a hospitalist at Beth Israel Deaconess Medical Center, Boston, and instructor in medicine at Harvard Medical School; Dr. Rendon is a hospitalist at the University of New Mexico in Albuquerque; Dr. Kwan is a hospitalist at the Veterans Affairs San Diego Healthcare System and associate professor at the University of California, San Diego. He is the chair of SHM’s Physicians in Training committee.
References
1. United States Medical Licensing Examination (2020 Feb). Change to pass/fail score reporting for Step 1.
2. Slavin SJ and Chibnall JT. Finding the why, changing the how: Improving the mental health of medical students, residents, and physicians. Academic Medicine. 2016;91(9):1194‐6.
3. Pereira AG, Chelminski PR, et al. Application inflation for internal medicine applicants in the Match: Drivers, consequences, and potential solutions. Am J Med. 2016 Aug;129(8): 885-91.
The National Board of Medical Examiners recently announced a change in the United States Medical Licensing Examination (USMLE) Step 1 score reporting from a 3-digit score to a pass/fail score beginning in 2022.1 Endorsed by a broad coalition of organizations involved in undergraduate (UME) and graduate medical education (GME), this change is intended as a first step toward systemic improvements in the UME-GME transition to residency by promoting holistic reviews of applicants. Additionally, it is meant to tackle widespread concerns about medical student distress brought about by the residency selection process. For example, switching to pass/fail preclinical curricula has resulted in an improvement in medical student well-being at many medical schools.2 It is the hope that a mirrored change in Step 1 may similarly improve mental health and encourage a growth mindset towards learning.
On the other hand, many residency programs rely on USMLE scores for screening potential candidates, especially as application inflation has burdened programs with thousands of applications.3 The change to a pass/fail Step 1 score will likely shift emphasis and stress to the Step 2 CK Exam, essentially negating the intended effect. Furthermore, for schools still reporting NBME Subject (shelf) Exam scores and Clerkship grades, there will likely be a greater emphasis placed on these metrics as well. The need for objective assessment methods are seen by many as so critical that some GME leaders have advocated for instituting entrance exams or requiring a Standardized Letter of Evaluation as a prerequisite to residency application. Finally, medical students jockeying for competitive residency positions may also feel pressured to distinguish themselves by boosting other aspects of their portfolio by taking a research year or applying for away electives, which risks marginalizing students of lesser means or with family responsibilities.
Ultimately, the change to a pass/fail Step 1 exam will likely do little to address the expanding gulf between the UME and GME communities. Residency program directors are searching for students with qualities of a good physician, such as interpersonal skills, “teamsmanship,” compassion, and professionalism, but reliable, objective, and standardized assessment tools are not available. Currently our best tools are clinical evaluations which are subject to grade inflation and implicit racial and gender biases. Furthermore, other components of a residency application, such as letters of recommendation, Chair’s letters, and the Medical Student Performance Evaluation (Dean’s letter), are regarded to be less informative as schools move toward no student rankings, pass/fail grading schemes, and nonstandardized summative adjectives to describe medical students overall medical school performance.
Finally, medical student distress in the residency application process may stem from the perpetuation of elitism that extends from medical school to fellowship training and academic hospital medicine. Rankings of medical schools, residencies, fellowships, and hospitals serve to create a hierarchical system. Competitive residency applicants see admittance into the best training programs as opening doors to opportunities, while not getting into these programs is seen as closing doors to career paths and opportunities.
With this change in Step 1 score reporting, where do we as hospitalists fit in? Hospitalists are at the forefront of educating and evaluating medical students in academic medical centers, and we are often asked to write letters of recommendation and serve as mentors. If done well, these activities can have a positive impact on medical student applications to residency by alleviating some of the stresses and mitigating the downsides to the new Step 1 scoring system. Writing impactful letters and thoughtful evaluations are all skills that should be incorporated in hospitalist faculty development programs. Moreover, in order to serve as better advocates for our students, it is important that academic hospitalists understand the evolving landscape of the residency application process and are mindful of the stresses that medical students face. Changing Step 1 scoring to pass/fail will likely have unintended consequences for our medical students, and we as hospitalists must be ready to improve our knowledge and skills in order to continue to support and advocate for our medical students.
Dr. Esquivel is a hospitalist and assistant professor at Weill Cornell Medical College in New York; Dr. Chang is associate professor and interprofessional education thread director (MD curriculum) at Washington University, St. Louis; Dr. Ricotta is a hospitalist at Beth Israel Deaconess Medical Center, Boston, and instructor in medicine at Harvard Medical School; Dr. Rendon is a hospitalist at the University of New Mexico in Albuquerque; Dr. Kwan is a hospitalist at the Veterans Affairs San Diego Healthcare System and associate professor at the University of California, San Diego. He is the chair of SHM’s Physicians in Training committee.
References
1. United States Medical Licensing Examination (2020 Feb). Change to pass/fail score reporting for Step 1.
2. Slavin SJ and Chibnall JT. Finding the why, changing the how: Improving the mental health of medical students, residents, and physicians. Academic Medicine. 2016;91(9):1194‐6.
3. Pereira AG, Chelminski PR, et al. Application inflation for internal medicine applicants in the Match: Drivers, consequences, and potential solutions. Am J Med. 2016 Aug;129(8): 885-91.
The branching tree of hospital medicine
Diversity of training backgrounds
You’ve probably heard of a “nocturnist,” but have you ever heard of a “weekendist?”

The field of hospital medicine (HM) has evolved dramatically since the term “hospitalist” was introduced in the literature in 1996.1 There is a saying in HM that “if you know one HM program, you know one HM program,” alluding to the fact that every HM program is unique. The diversity of individual HM programs combined with the overall evolution of the field has expanded the range of jobs available in HM.
The nomenclature of adding an -ist to the end of the specific roles (e.g., nocturnist, weekendist) has become commonplace. These roles have developed with the increasing need for day and night staffing at many hospitals secondary to increased and more complex patients, less availability of residents because of work hour restrictions, and the Accreditation Council for Graduate Medical Education (ACGME) rules that require overnight supervision of residents
Additionally, the field of HM increasingly includes physicians trained in internal medicine, family medicine, pediatrics, and medicine-pediatrics (med-peds). In this article, we describe the variety of roles available to trainees joining HM and the multitude of different training backgrounds hospitalists come from.
Nocturnists
The 2018 State of Hospital Medicine Report notes that 76.1% of adult-only HM groups have nocturnists, hospitalists who work primarily at night to admit and to provide coverage for admitted patients.2 Nocturnists often provide benefit to the rest of their hospitalist group by allowing fewer required night shifts for those that prefer to work during the day.

Nocturnists may choose a nighttime schedule for several reasons, including the ability to be home more during the day. They also have the potential to work fewer total hours or shifts while still earning a similar or increased income, compared with predominantly daytime hospitalists, increasing their flexibility to pursue other interests. These nocturnists become experts in navigating the admission process and responding to inpatient emergencies often with less support when compared with daytime hospitalists.
In addition to career nocturnist work, nocturnist jobs can be a great fit for those residency graduates who are undecided about fellowship and enjoy the acuity of inpatient medicine. It provides an opportunity to hone their clinical skill set prior to specialized training while earning an attending salary, and offers flexible hours which may allow for research or other endeavors. In academic centers, nocturnist educational roles take on a different character as well and may involve more 1:1 educational experiences. The role of nocturnists as educators is expanding as ACGME rules call for more oversight and educational opportunities for residents who are working at night.
However, challenges exist for nocturnists, including keeping abreast of new changes in their HM groups and hospital systems and engaging in quality initiatives, given that most meetings occur during the day. Additionally, nocturnists must adapt to sleeping during the day, potentially getting less sleep then they would otherwise and being “off cycle” with family and friends. For nocturnists raising children, being off cycle may be advantageous as it can allow them to be home with their children after school.
Weekendists
Another common hospitalist role is the weekendist, hospitalists who spend much of their clinical time preferentially working weekends. Similar to nocturnists, weekendists provide benefit to their hospitalist group by allowing others to have more weekends off.

Weekendists may prefer working weekends because of fewer total shifts or hours and/or higher compensation per shift. Additionally, weekendists have the flexibility to do other work on weekdays, such as research or another hospitalist job. For those that do nonclinical work during the week, a weekendist position may allow them to keep their clinical skills up to date. However, weekendists may face intense clinical days with a higher census because of fewer hospitalists rounding on the weekends.
Weekendists must balance having more potential time available during the weekdays but less time on the weekends to devote to family and friends. Furthermore, weekendists may feel less engaged with nonclinical opportunities, including quality improvement, educational offerings, and teaching opportunities.
SNFists
With increasing emphasis on transitions of care and the desire to avoid readmission penalties, some hospitalists have transitioned to work partly or primarily in skilled nursing facilities (SNF) and have been referred to as “SNFists.” Some of these hospitalists may split their clinical time between SNFs and acute care hospitals, while others may work exclusively at SNFs.

SNFists have the potential to be invaluable in improving transitions of care after discharge to post–acute care facilities because of increased provider presence in these facilities, comfort with medically complex patients, and appreciation of government regulations.4 SNFists may face potential challenges of needing to staff more than one post–acute care hospital and of having less resources available, compared with an acute care hospital.
Specific specialty hospitalists
For a variety of reasons including clinical interest, many hospitalists have become specialized with regards to their primary inpatient population. Some hospitalists spend the majority of their clinical time on a specific service in the hospital, often working closely with the subspecialist caring for that patient. These hospitalists may focus on hematology, oncology, bone-marrow transplant, neurology, cardiology, surgery services, or critical care, among others. Hospitalists focused on a specific service often become knowledge experts in that specialty. Conversely, by focusing on a specific service, certain pathologies may be less commonly seen, which may narrow the breadth of the hospital medicine job.
Hospitalist training
Internal medicine hospitalists may be the most common hospitalists encountered in many hospitals and at each Society of Hospital Medicine annual conference, but there has also been rapid growth in hospitalists from other specialties and backgrounds.
Family medicine hospitalists are a part of 64.9% of HM groups and about 9% of family medicine graduates are choosing HM as a career path.2,3 Most family medicine hospitalists work in adult HM groups, but some, particularly in rural or academic settings, care for pediatric, newborn, and/or maternity patients. Similarly, pediatric hospitalists have become entrenched at many hospitals where children are admitted. These pediatric hospitalists, like adult hospitalists, may work in a variety of different clinical roles including in EDs, newborn nurseries, and inpatient wards or ICUs; they may also provide consult, sedation, or procedural services.
Med-peds hospitalists that split time between internal medicine and pediatrics are becoming more commonplace in the field. Many work at academic centers where they often work on each side separately, doing the same work as their internal medicine or pediatrics colleagues, and then switching to the other side after a period of time. Some centers offer unique roles for med-peds hospitalists including working on adult consult teams in children’s hospitals, where they provide consult care to older patients that may still receive their care at a children’s hospital. There are also nonacademic hospitals that primarily staff med-peds hospitalists, where they can provide the full spectrum of care from the newborn nursery to the inpatient pediatric and adult wards.
Hospital medicine is a young field that is constantly changing with new and developing roles for hospitalists from a wide variety of backgrounds. Stick around to see which “-ist” will come next in HM.
Dr. Hall is a med-peds hospitalist and assistant professor at the University of Kentucky, Lexington. Dr. Sanyal-Dey is an academic hospitalist at Zuckerberg San Francisco General Hospital and Trauma Center and the University of California, San Francisco, where she is the director of clinical operations, and director of the faculty inpatient service. Dr. Chang is associate professor and interprofessional education thread director (MD curriculum) at Washington University, St. Louis. Dr. Kwan is a hospitalist at the Veterans Affairs San Diego Healthcare System and associate professor at the University of California, San Diego. He is the chair of SHM’s Physicians in Training committee. Dr. Seymour is family medicine hospitalist education director at the University of Massachusetts Memorial Medical Center, Worcester, and associate professor at the University of Massachusetts.
References
1. Wachter RM, Goldman L. The Emerging Role of “Hospitalists” in the American Health Care System. N Engl J Med. 1996;335(7):514-7.
2. 2018 State of Hospital Medicine Report. Philadelphia: Society of Hospital Medicine, 2018.
3. Weaver SP, Hill J. Academician Attitudes and Beliefs Regarding the Use of Hospitalists: A CERA Study. Fam Med. 2015;47(5):357-61.
4. Teno JM et al. Temporal Trends in the Numbers of Skilled Nursing Facility Specialists From 2007 Through 2014. JAMA Intern Med. 2017;177(9):1376-8.
Diversity of training backgrounds
Diversity of training backgrounds
You’ve probably heard of a “nocturnist,” but have you ever heard of a “weekendist?”
The field of hospital medicine (HM) has evolved dramatically since the term “hospitalist” was introduced in the literature in 1996.1 There is a saying in HM that “if you know one HM program, you know one HM program,” alluding to the fact that every HM program is unique. The diversity of individual HM programs combined with the overall evolution of the field has expanded the range of jobs available in HM.
The nomenclature of adding an -ist to the end of the specific roles (e.g., nocturnist, weekendist) has become commonplace. These roles have developed with the increasing need for day and night staffing at many hospitals secondary to increased and more complex patients, less availability of residents because of work hour restrictions, and the Accreditation Council for Graduate Medical Education (ACGME) rules that require overnight supervision of residents
Additionally, the field of HM increasingly includes physicians trained in internal medicine, family medicine, pediatrics, and medicine-pediatrics (med-peds). In this article, we describe the variety of roles available to trainees joining HM and the multitude of different training backgrounds hospitalists come from.
Nocturnists
The 2018 State of Hospital Medicine Report notes that 76.1% of adult-only HM groups have nocturnists, hospitalists who work primarily at night to admit and to provide coverage for admitted patients.2 Nocturnists often provide benefit to the rest of their hospitalist group by allowing fewer required night shifts for those that prefer to work during the day.
Nocturnists may choose a nighttime schedule for several reasons, including the ability to be home more during the day. They also have the potential to work fewer total hours or shifts while still earning a similar or increased income, compared with predominantly daytime hospitalists, increasing their flexibility to pursue other interests. These nocturnists become experts in navigating the admission process and responding to inpatient emergencies often with less support when compared with daytime hospitalists.
In addition to career nocturnist work, nocturnist jobs can be a great fit for those residency graduates who are undecided about fellowship and enjoy the acuity of inpatient medicine. It provides an opportunity to hone their clinical skill set prior to specialized training while earning an attending salary, and offers flexible hours which may allow for research or other endeavors. In academic centers, nocturnist educational roles take on a different character as well and may involve more 1:1 educational experiences. The role of nocturnists as educators is expanding as ACGME rules call for more oversight and educational opportunities for residents who are working at night.
However, challenges exist for nocturnists, including keeping abreast of new changes in their HM groups and hospital systems and engaging in quality initiatives, given that most meetings occur during the day. Additionally, nocturnists must adapt to sleeping during the day, potentially getting less sleep then they would otherwise and being “off cycle” with family and friends. For nocturnists raising children, being off cycle may be advantageous as it can allow them to be home with their children after school.
Weekendists
Another common hospitalist role is the weekendist, hospitalists who spend much of their clinical time preferentially working weekends. Similar to nocturnists, weekendists provide benefit to their hospitalist group by allowing others to have more weekends off.
Weekendists may prefer working weekends because of fewer total shifts or hours and/or higher compensation per shift. Additionally, weekendists have the flexibility to do other work on weekdays, such as research or another hospitalist job. For those that do nonclinical work during the week, a weekendist position may allow them to keep their clinical skills up to date. However, weekendists may face intense clinical days with a higher census because of fewer hospitalists rounding on the weekends.
Weekendists must balance having more potential time available during the weekdays but less time on the weekends to devote to family and friends. Furthermore, weekendists may feel less engaged with nonclinical opportunities, including quality improvement, educational offerings, and teaching opportunities.
SNFists
With increasing emphasis on transitions of care and the desire to avoid readmission penalties, some hospitalists have transitioned to work partly or primarily in skilled nursing facilities (SNF) and have been referred to as “SNFists.” Some of these hospitalists may split their clinical time between SNFs and acute care hospitals, while others may work exclusively at SNFs.
SNFists have the potential to be invaluable in improving transitions of care after discharge to post–acute care facilities because of increased provider presence in these facilities, comfort with medically complex patients, and appreciation of government regulations.4 SNFists may face potential challenges of needing to staff more than one post–acute care hospital and of having less resources available, compared with an acute care hospital.
Specific specialty hospitalists
For a variety of reasons including clinical interest, many hospitalists have become specialized with regards to their primary inpatient population. Some hospitalists spend the majority of their clinical time on a specific service in the hospital, often working closely with the subspecialist caring for that patient. These hospitalists may focus on hematology, oncology, bone-marrow transplant, neurology, cardiology, surgery services, or critical care, among others. Hospitalists focused on a specific service often become knowledge experts in that specialty. Conversely, by focusing on a specific service, certain pathologies may be less commonly seen, which may narrow the breadth of the hospital medicine job.
Hospitalist training
Internal medicine hospitalists may be the most common hospitalists encountered in many hospitals and at each Society of Hospital Medicine annual conference, but there has also been rapid growth in hospitalists from other specialties and backgrounds.
Family medicine hospitalists are a part of 64.9% of HM groups and about 9% of family medicine graduates are choosing HM as a career path.2,3 Most family medicine hospitalists work in adult HM groups, but some, particularly in rural or academic settings, care for pediatric, newborn, and/or maternity patients. Similarly, pediatric hospitalists have become entrenched at many hospitals where children are admitted. These pediatric hospitalists, like adult hospitalists, may work in a variety of different clinical roles including in EDs, newborn nurseries, and inpatient wards or ICUs; they may also provide consult, sedation, or procedural services.
Med-peds hospitalists that split time between internal medicine and pediatrics are becoming more commonplace in the field. Many work at academic centers where they often work on each side separately, doing the same work as their internal medicine or pediatrics colleagues, and then switching to the other side after a period of time. Some centers offer unique roles for med-peds hospitalists including working on adult consult teams in children’s hospitals, where they provide consult care to older patients that may still receive their care at a children’s hospital. There are also nonacademic hospitals that primarily staff med-peds hospitalists, where they can provide the full spectrum of care from the newborn nursery to the inpatient pediatric and adult wards.
Hospital medicine is a young field that is constantly changing with new and developing roles for hospitalists from a wide variety of backgrounds. Stick around to see which “-ist” will come next in HM.
Dr. Hall is a med-peds hospitalist and assistant professor at the University of Kentucky, Lexington. Dr. Sanyal-Dey is an academic hospitalist at Zuckerberg San Francisco General Hospital and Trauma Center and the University of California, San Francisco, where she is the director of clinical operations, and director of the faculty inpatient service. Dr. Chang is associate professor and interprofessional education thread director (MD curriculum) at Washington University, St. Louis. Dr. Kwan is a hospitalist at the Veterans Affairs San Diego Healthcare System and associate professor at the University of California, San Diego. He is the chair of SHM’s Physicians in Training committee. Dr. Seymour is family medicine hospitalist education director at the University of Massachusetts Memorial Medical Center, Worcester, and associate professor at the University of Massachusetts.
References
1. Wachter RM, Goldman L. The Emerging Role of “Hospitalists” in the American Health Care System. N Engl J Med. 1996;335(7):514-7.
2. 2018 State of Hospital Medicine Report. Philadelphia: Society of Hospital Medicine, 2018.
3. Weaver SP, Hill J. Academician Attitudes and Beliefs Regarding the Use of Hospitalists: A CERA Study. Fam Med. 2015;47(5):357-61.
4. Teno JM et al. Temporal Trends in the Numbers of Skilled Nursing Facility Specialists From 2007 Through 2014. JAMA Intern Med. 2017;177(9):1376-8.
You’ve probably heard of a “nocturnist,” but have you ever heard of a “weekendist?”
The field of hospital medicine (HM) has evolved dramatically since the term “hospitalist” was introduced in the literature in 1996.1 There is a saying in HM that “if you know one HM program, you know one HM program,” alluding to the fact that every HM program is unique. The diversity of individual HM programs combined with the overall evolution of the field has expanded the range of jobs available in HM.
The nomenclature of adding an -ist to the end of the specific roles (e.g., nocturnist, weekendist) has become commonplace. These roles have developed with the increasing need for day and night staffing at many hospitals secondary to increased and more complex patients, less availability of residents because of work hour restrictions, and the Accreditation Council for Graduate Medical Education (ACGME) rules that require overnight supervision of residents
Additionally, the field of HM increasingly includes physicians trained in internal medicine, family medicine, pediatrics, and medicine-pediatrics (med-peds). In this article, we describe the variety of roles available to trainees joining HM and the multitude of different training backgrounds hospitalists come from.
Nocturnists
The 2018 State of Hospital Medicine Report notes that 76.1% of adult-only HM groups have nocturnists, hospitalists who work primarily at night to admit and to provide coverage for admitted patients.2 Nocturnists often provide benefit to the rest of their hospitalist group by allowing fewer required night shifts for those that prefer to work during the day.
Nocturnists may choose a nighttime schedule for several reasons, including the ability to be home more during the day. They also have the potential to work fewer total hours or shifts while still earning a similar or increased income, compared with predominantly daytime hospitalists, increasing their flexibility to pursue other interests. These nocturnists become experts in navigating the admission process and responding to inpatient emergencies often with less support when compared with daytime hospitalists.
In addition to career nocturnist work, nocturnist jobs can be a great fit for those residency graduates who are undecided about fellowship and enjoy the acuity of inpatient medicine. It provides an opportunity to hone their clinical skill set prior to specialized training while earning an attending salary, and offers flexible hours which may allow for research or other endeavors. In academic centers, nocturnist educational roles take on a different character as well and may involve more 1:1 educational experiences. The role of nocturnists as educators is expanding as ACGME rules call for more oversight and educational opportunities for residents who are working at night.
However, challenges exist for nocturnists, including keeping abreast of new changes in their HM groups and hospital systems and engaging in quality initiatives, given that most meetings occur during the day. Additionally, nocturnists must adapt to sleeping during the day, potentially getting less sleep then they would otherwise and being “off cycle” with family and friends. For nocturnists raising children, being off cycle may be advantageous as it can allow them to be home with their children after school.
Weekendists
Another common hospitalist role is the weekendist, hospitalists who spend much of their clinical time preferentially working weekends. Similar to nocturnists, weekendists provide benefit to their hospitalist group by allowing others to have more weekends off.
Weekendists may prefer working weekends because of fewer total shifts or hours and/or higher compensation per shift. Additionally, weekendists have the flexibility to do other work on weekdays, such as research or another hospitalist job. For those that do nonclinical work during the week, a weekendist position may allow them to keep their clinical skills up to date. However, weekendists may face intense clinical days with a higher census because of fewer hospitalists rounding on the weekends.
Weekendists must balance having more potential time available during the weekdays but less time on the weekends to devote to family and friends. Furthermore, weekendists may feel less engaged with nonclinical opportunities, including quality improvement, educational offerings, and teaching opportunities.
SNFists
With increasing emphasis on transitions of care and the desire to avoid readmission penalties, some hospitalists have transitioned to work partly or primarily in skilled nursing facilities (SNF) and have been referred to as “SNFists.” Some of these hospitalists may split their clinical time between SNFs and acute care hospitals, while others may work exclusively at SNFs.
SNFists have the potential to be invaluable in improving transitions of care after discharge to post–acute care facilities because of increased provider presence in these facilities, comfort with medically complex patients, and appreciation of government regulations.4 SNFists may face potential challenges of needing to staff more than one post–acute care hospital and of having less resources available, compared with an acute care hospital.
Specific specialty hospitalists
For a variety of reasons including clinical interest, many hospitalists have become specialized with regards to their primary inpatient population. Some hospitalists spend the majority of their clinical time on a specific service in the hospital, often working closely with the subspecialist caring for that patient. These hospitalists may focus on hematology, oncology, bone-marrow transplant, neurology, cardiology, surgery services, or critical care, among others. Hospitalists focused on a specific service often become knowledge experts in that specialty. Conversely, by focusing on a specific service, certain pathologies may be less commonly seen, which may narrow the breadth of the hospital medicine job.
Hospitalist training
Internal medicine hospitalists may be the most common hospitalists encountered in many hospitals and at each Society of Hospital Medicine annual conference, but there has also been rapid growth in hospitalists from other specialties and backgrounds.
Family medicine hospitalists are a part of 64.9% of HM groups and about 9% of family medicine graduates are choosing HM as a career path.2,3 Most family medicine hospitalists work in adult HM groups, but some, particularly in rural or academic settings, care for pediatric, newborn, and/or maternity patients. Similarly, pediatric hospitalists have become entrenched at many hospitals where children are admitted. These pediatric hospitalists, like adult hospitalists, may work in a variety of different clinical roles including in EDs, newborn nurseries, and inpatient wards or ICUs; they may also provide consult, sedation, or procedural services.
Med-peds hospitalists that split time between internal medicine and pediatrics are becoming more commonplace in the field. Many work at academic centers where they often work on each side separately, doing the same work as their internal medicine or pediatrics colleagues, and then switching to the other side after a period of time. Some centers offer unique roles for med-peds hospitalists including working on adult consult teams in children’s hospitals, where they provide consult care to older patients that may still receive their care at a children’s hospital. There are also nonacademic hospitals that primarily staff med-peds hospitalists, where they can provide the full spectrum of care from the newborn nursery to the inpatient pediatric and adult wards.
Hospital medicine is a young field that is constantly changing with new and developing roles for hospitalists from a wide variety of backgrounds. Stick around to see which “-ist” will come next in HM.
Dr. Hall is a med-peds hospitalist and assistant professor at the University of Kentucky, Lexington. Dr. Sanyal-Dey is an academic hospitalist at Zuckerberg San Francisco General Hospital and Trauma Center and the University of California, San Francisco, where she is the director of clinical operations, and director of the faculty inpatient service. Dr. Chang is associate professor and interprofessional education thread director (MD curriculum) at Washington University, St. Louis. Dr. Kwan is a hospitalist at the Veterans Affairs San Diego Healthcare System and associate professor at the University of California, San Diego. He is the chair of SHM’s Physicians in Training committee. Dr. Seymour is family medicine hospitalist education director at the University of Massachusetts Memorial Medical Center, Worcester, and associate professor at the University of Massachusetts.
References
1. Wachter RM, Goldman L. The Emerging Role of “Hospitalists” in the American Health Care System. N Engl J Med. 1996;335(7):514-7.
2. 2018 State of Hospital Medicine Report. Philadelphia: Society of Hospital Medicine, 2018.
3. Weaver SP, Hill J. Academician Attitudes and Beliefs Regarding the Use of Hospitalists: A CERA Study. Fam Med. 2015;47(5):357-61.
4. Teno JM et al. Temporal Trends in the Numbers of Skilled Nursing Facility Specialists From 2007 Through 2014. JAMA Intern Med. 2017;177(9):1376-8.
10 Tips for Hospitalists to Achieve an Effective Medical Consult
A medical consult is an amazing way to learn. Consultation challenges us to practice our best medicine while also exposing us to innovations in other specialties. It can forge new and productive relationships with physicians from all specialties. At its best, it is the purest of medicine or, as some put it, “medicine without the drama.”
As hospitalists, we are increasingly asked to be medical consultants and co-managers. Yet most training programs spend very little time educating residents on what makes a high-quality consultation. One of the first articles written on this subject was by Lee Goldman and colleagues in 1983. In this article, Goldman sets out 10 commandments for effective consultation.1
Many of the lessons in these 10 commandments continue to ring true today. As primary providers, we know that consulting another service can run the gamut from being pleasant, helpful, and enlightening to being the most frustrating, slam-the-phone-down experience of the day. In this article, we update these commandments to create five golden rules for medical consultations that ensure that your referring providers’ experiences are purely positive.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
Five Golden Rules
1 Listen and determine the needs of your customer.
Understanding the needs of your requesting physician is paramount to being an effective consultant, and the first step is to determine the physician’s question. Some referring providers want the bird’s eye view of a general medicine consult, whereas others have just one specific question. In one study stratified by specialty, 59% of surgeons preferred a general medicine consult, while most non-surgeons preferred a focused consult.2
Next, establish the timeframe: Is it emergent, urgent, or routine? One rule of thumb is that all consults should be seen within 24 hours. But many consults need to be seen more quickly, or even immediately. For example, you may be correct to assume that a patient is stable enough to wait for your consult, but perhaps the lack of pre-operative medical assessment will cause her to lose her spot on the OR schedule. The orthopedic surgeon now operates late into the night. Truly understanding the needs of your referring provider might have avoided that scenario.
There are of course times when you really can’t get to a consult expeditiously, but you must let the referring provider know. Ultimately, once you agree upon the urgency, all parties, including the patient, will know when to expect the consultant at the bedside.
2 Look for yourself, and do it yourself.
We practice in an age in which we spend more time in front of computers than in front of patients. As Lee and colleagues write, “A consultant should not expect to make brilliant diagnostic conclusions based on an assessment of data that are already in the chart. Usually, if the answer could be deduced from this information, the consultations would not have been called.”1 Effective consultants always obtain their own history and physical—your special expertise may allow you to extract overlooked information.
In addition, simply leaving recommendations to repeat tests or obtain records often delays care. If you feel the information is vital, take it upon yourself to obtain it. This may include contacting outside primary care providers or medicine subspecialists, or getting outside records.
Although we are not the primary provider, our goal must always be to do what is best for our patients.
3 Make brief, detailed plans with contingencies.
Recommendations can easily be lost in the deluge of information bombarding the primary care team. Our goal is not only to make recommendations, but also to have them followed.
In a study looking at which aspects of a consultation lead to increased compliance, researchers noted that if dose and duration of therapy were not specified, 64% of recommendations were implemented.3 When only one was specified, implementation increased to 85%, and when both were specified, implementation rates increased to 100%. Sadly, only 15% of over 200 consults had both duration and dose in their recommendations. Another study on compliance found that when five or fewer recommendations were specified, compliance increased from 79% to 96%.4
Contingency plans are a way of life for hospitalists when we sign out. Consultations are no different. Patients we consult on are often critically ill, and their status is dynamic. Anticipating problems and giving recommendations if those problems arise can save valuable time later for both you and your colleagues.
As consultants, we often feel compelled to “do something,” yet we know as primary providers how frustrating it is to have a consultant ask for a battery of tests or treatments that don’t address the big picture. Never be afraid to recommend continuing current management if it is appropriate or even to recommend stopping treatment or avoiding additional testing when it does not help the patient.
In summary, consults are most effective when they are brief (five or fewer recommendations), are detailed, and provide contingency plans. What good is a great consultation if it is not followed?
4 Communicate, communicate, communicate.
When 323 surgeons and non-surgeons were surveyed, both groups agreed that initial recommendations should be discussed verbally. Direct verbal communication allows the primary team to provide important information that you may have missed. In addition, discussing recommendations improves compliance and allows everyone to agree on the next plan of action and provide a unified plan to the patient, improving patient satisfaction and adherence.
Lastly and most importantly, opening the lines of communication between consultant and requesting physician creates effective consulting relationships.
Developing this relationship with other services may mean that the next time you call them for a consult, you will already have good rapport to build on.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
5 Follow up.
Several studies have shown that follow-up notes improve compliance with recommendations.3,5 Follow-up is also important to ensure that critical recommendations are followed and that any changes in patient status can be addressed. Furthermore, following up can provide valuable feedback on your own initial clinical judgment. Finally, it is bad practice to recommend testing and then sign off before these tests are completed. Either you feel they are important to patient care and worth obtaining, or they are not needed.
Following these five golden rules can ensure that you are the consultant who gives other physicians the satisfying experience of an effective and great consult. If it’s done right, the experience of a general medicine consult is the purest of medicine.
Dr. Chang is assistant professor, inpatient medicine clerkship director, and director of education in the division of hospital medicine at Mount Sinai Medical Center in New York City. Dr. Gabriel is assistant professor and director of medicine consult preoperative services in the division of hospital medicine at Mount Sinai.
References
- Goldman L, Lee T, Rudd P. Ten commandments for effective consultations. Arch Intern Med. 1983;143(9):1753-1755.
- Salerno SM, Hurst FP, Halvorson S, Mercado DL. Principles of effective consultation: an update for the 21st-century consultant. Arch Intern Med. 2007;167(3):271-275.
- Horwitz RI, Henes CG, Horwitz SM. Developing strategies for improving the diagnostic and management efficacy of medical consultations. J Chron Dis. 1983;36(2):213-218.
- Sears CL, Charlson ME. The effectiveness of a consultation: compliance with initial recommendations. Am J Med. 1983;74(5):870-876.
- MacKenzie TB, Popkin MK, Callies AL, Jorgensen CR, Cohn JN. The effectiveness of cardiology consultations. Concordance with diagnostic and drug recommendations. Chest. 1981;79(1):16-22.
A medical consult is an amazing way to learn. Consultation challenges us to practice our best medicine while also exposing us to innovations in other specialties. It can forge new and productive relationships with physicians from all specialties. At its best, it is the purest of medicine or, as some put it, “medicine without the drama.”
As hospitalists, we are increasingly asked to be medical consultants and co-managers. Yet most training programs spend very little time educating residents on what makes a high-quality consultation. One of the first articles written on this subject was by Lee Goldman and colleagues in 1983. In this article, Goldman sets out 10 commandments for effective consultation.1
Many of the lessons in these 10 commandments continue to ring true today. As primary providers, we know that consulting another service can run the gamut from being pleasant, helpful, and enlightening to being the most frustrating, slam-the-phone-down experience of the day. In this article, we update these commandments to create five golden rules for medical consultations that ensure that your referring providers’ experiences are purely positive.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
Five Golden Rules
1 Listen and determine the needs of your customer.
Understanding the needs of your requesting physician is paramount to being an effective consultant, and the first step is to determine the physician’s question. Some referring providers want the bird’s eye view of a general medicine consult, whereas others have just one specific question. In one study stratified by specialty, 59% of surgeons preferred a general medicine consult, while most non-surgeons preferred a focused consult.2
Next, establish the timeframe: Is it emergent, urgent, or routine? One rule of thumb is that all consults should be seen within 24 hours. But many consults need to be seen more quickly, or even immediately. For example, you may be correct to assume that a patient is stable enough to wait for your consult, but perhaps the lack of pre-operative medical assessment will cause her to lose her spot on the OR schedule. The orthopedic surgeon now operates late into the night. Truly understanding the needs of your referring provider might have avoided that scenario.
There are of course times when you really can’t get to a consult expeditiously, but you must let the referring provider know. Ultimately, once you agree upon the urgency, all parties, including the patient, will know when to expect the consultant at the bedside.
2 Look for yourself, and do it yourself.
We practice in an age in which we spend more time in front of computers than in front of patients. As Lee and colleagues write, “A consultant should not expect to make brilliant diagnostic conclusions based on an assessment of data that are already in the chart. Usually, if the answer could be deduced from this information, the consultations would not have been called.”1 Effective consultants always obtain their own history and physical—your special expertise may allow you to extract overlooked information.
In addition, simply leaving recommendations to repeat tests or obtain records often delays care. If you feel the information is vital, take it upon yourself to obtain it. This may include contacting outside primary care providers or medicine subspecialists, or getting outside records.
Although we are not the primary provider, our goal must always be to do what is best for our patients.
3 Make brief, detailed plans with contingencies.
Recommendations can easily be lost in the deluge of information bombarding the primary care team. Our goal is not only to make recommendations, but also to have them followed.
In a study looking at which aspects of a consultation lead to increased compliance, researchers noted that if dose and duration of therapy were not specified, 64% of recommendations were implemented.3 When only one was specified, implementation increased to 85%, and when both were specified, implementation rates increased to 100%. Sadly, only 15% of over 200 consults had both duration and dose in their recommendations. Another study on compliance found that when five or fewer recommendations were specified, compliance increased from 79% to 96%.4
Contingency plans are a way of life for hospitalists when we sign out. Consultations are no different. Patients we consult on are often critically ill, and their status is dynamic. Anticipating problems and giving recommendations if those problems arise can save valuable time later for both you and your colleagues.
As consultants, we often feel compelled to “do something,” yet we know as primary providers how frustrating it is to have a consultant ask for a battery of tests or treatments that don’t address the big picture. Never be afraid to recommend continuing current management if it is appropriate or even to recommend stopping treatment or avoiding additional testing when it does not help the patient.
In summary, consults are most effective when they are brief (five or fewer recommendations), are detailed, and provide contingency plans. What good is a great consultation if it is not followed?
4 Communicate, communicate, communicate.
When 323 surgeons and non-surgeons were surveyed, both groups agreed that initial recommendations should be discussed verbally. Direct verbal communication allows the primary team to provide important information that you may have missed. In addition, discussing recommendations improves compliance and allows everyone to agree on the next plan of action and provide a unified plan to the patient, improving patient satisfaction and adherence.
Lastly and most importantly, opening the lines of communication between consultant and requesting physician creates effective consulting relationships.
Developing this relationship with other services may mean that the next time you call them for a consult, you will already have good rapport to build on.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
5 Follow up.
Several studies have shown that follow-up notes improve compliance with recommendations.3,5 Follow-up is also important to ensure that critical recommendations are followed and that any changes in patient status can be addressed. Furthermore, following up can provide valuable feedback on your own initial clinical judgment. Finally, it is bad practice to recommend testing and then sign off before these tests are completed. Either you feel they are important to patient care and worth obtaining, or they are not needed.
Following these five golden rules can ensure that you are the consultant who gives other physicians the satisfying experience of an effective and great consult. If it’s done right, the experience of a general medicine consult is the purest of medicine.
Dr. Chang is assistant professor, inpatient medicine clerkship director, and director of education in the division of hospital medicine at Mount Sinai Medical Center in New York City. Dr. Gabriel is assistant professor and director of medicine consult preoperative services in the division of hospital medicine at Mount Sinai.
References
- Goldman L, Lee T, Rudd P. Ten commandments for effective consultations. Arch Intern Med. 1983;143(9):1753-1755.
- Salerno SM, Hurst FP, Halvorson S, Mercado DL. Principles of effective consultation: an update for the 21st-century consultant. Arch Intern Med. 2007;167(3):271-275.
- Horwitz RI, Henes CG, Horwitz SM. Developing strategies for improving the diagnostic and management efficacy of medical consultations. J Chron Dis. 1983;36(2):213-218.
- Sears CL, Charlson ME. The effectiveness of a consultation: compliance with initial recommendations. Am J Med. 1983;74(5):870-876.
- MacKenzie TB, Popkin MK, Callies AL, Jorgensen CR, Cohn JN. The effectiveness of cardiology consultations. Concordance with diagnostic and drug recommendations. Chest. 1981;79(1):16-22.
A medical consult is an amazing way to learn. Consultation challenges us to practice our best medicine while also exposing us to innovations in other specialties. It can forge new and productive relationships with physicians from all specialties. At its best, it is the purest of medicine or, as some put it, “medicine without the drama.”
As hospitalists, we are increasingly asked to be medical consultants and co-managers. Yet most training programs spend very little time educating residents on what makes a high-quality consultation. One of the first articles written on this subject was by Lee Goldman and colleagues in 1983. In this article, Goldman sets out 10 commandments for effective consultation.1
Many of the lessons in these 10 commandments continue to ring true today. As primary providers, we know that consulting another service can run the gamut from being pleasant, helpful, and enlightening to being the most frustrating, slam-the-phone-down experience of the day. In this article, we update these commandments to create five golden rules for medical consultations that ensure that your referring providers’ experiences are purely positive.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
Five Golden Rules
1 Listen and determine the needs of your customer.
Understanding the needs of your requesting physician is paramount to being an effective consultant, and the first step is to determine the physician’s question. Some referring providers want the bird’s eye view of a general medicine consult, whereas others have just one specific question. In one study stratified by specialty, 59% of surgeons preferred a general medicine consult, while most non-surgeons preferred a focused consult.2
Next, establish the timeframe: Is it emergent, urgent, or routine? One rule of thumb is that all consults should be seen within 24 hours. But many consults need to be seen more quickly, or even immediately. For example, you may be correct to assume that a patient is stable enough to wait for your consult, but perhaps the lack of pre-operative medical assessment will cause her to lose her spot on the OR schedule. The orthopedic surgeon now operates late into the night. Truly understanding the needs of your referring provider might have avoided that scenario.
There are of course times when you really can’t get to a consult expeditiously, but you must let the referring provider know. Ultimately, once you agree upon the urgency, all parties, including the patient, will know when to expect the consultant at the bedside.
2 Look for yourself, and do it yourself.
We practice in an age in which we spend more time in front of computers than in front of patients. As Lee and colleagues write, “A consultant should not expect to make brilliant diagnostic conclusions based on an assessment of data that are already in the chart. Usually, if the answer could be deduced from this information, the consultations would not have been called.”1 Effective consultants always obtain their own history and physical—your special expertise may allow you to extract overlooked information.
In addition, simply leaving recommendations to repeat tests or obtain records often delays care. If you feel the information is vital, take it upon yourself to obtain it. This may include contacting outside primary care providers or medicine subspecialists, or getting outside records.
Although we are not the primary provider, our goal must always be to do what is best for our patients.
3 Make brief, detailed plans with contingencies.
Recommendations can easily be lost in the deluge of information bombarding the primary care team. Our goal is not only to make recommendations, but also to have them followed.
In a study looking at which aspects of a consultation lead to increased compliance, researchers noted that if dose and duration of therapy were not specified, 64% of recommendations were implemented.3 When only one was specified, implementation increased to 85%, and when both were specified, implementation rates increased to 100%. Sadly, only 15% of over 200 consults had both duration and dose in their recommendations. Another study on compliance found that when five or fewer recommendations were specified, compliance increased from 79% to 96%.4
Contingency plans are a way of life for hospitalists when we sign out. Consultations are no different. Patients we consult on are often critically ill, and their status is dynamic. Anticipating problems and giving recommendations if those problems arise can save valuable time later for both you and your colleagues.
As consultants, we often feel compelled to “do something,” yet we know as primary providers how frustrating it is to have a consultant ask for a battery of tests or treatments that don’t address the big picture. Never be afraid to recommend continuing current management if it is appropriate or even to recommend stopping treatment or avoiding additional testing when it does not help the patient.
In summary, consults are most effective when they are brief (five or fewer recommendations), are detailed, and provide contingency plans. What good is a great consultation if it is not followed?
4 Communicate, communicate, communicate.
When 323 surgeons and non-surgeons were surveyed, both groups agreed that initial recommendations should be discussed verbally. Direct verbal communication allows the primary team to provide important information that you may have missed. In addition, discussing recommendations improves compliance and allows everyone to agree on the next plan of action and provide a unified plan to the patient, improving patient satisfaction and adherence.
Lastly and most importantly, opening the lines of communication between consultant and requesting physician creates effective consulting relationships.
Developing this relationship with other services may mean that the next time you call them for a consult, you will already have good rapport to build on.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
5 Follow up.
Several studies have shown that follow-up notes improve compliance with recommendations.3,5 Follow-up is also important to ensure that critical recommendations are followed and that any changes in patient status can be addressed. Furthermore, following up can provide valuable feedback on your own initial clinical judgment. Finally, it is bad practice to recommend testing and then sign off before these tests are completed. Either you feel they are important to patient care and worth obtaining, or they are not needed.
Following these five golden rules can ensure that you are the consultant who gives other physicians the satisfying experience of an effective and great consult. If it’s done right, the experience of a general medicine consult is the purest of medicine.
Dr. Chang is assistant professor, inpatient medicine clerkship director, and director of education in the division of hospital medicine at Mount Sinai Medical Center in New York City. Dr. Gabriel is assistant professor and director of medicine consult preoperative services in the division of hospital medicine at Mount Sinai.
References
- Goldman L, Lee T, Rudd P. Ten commandments for effective consultations. Arch Intern Med. 1983;143(9):1753-1755.
- Salerno SM, Hurst FP, Halvorson S, Mercado DL. Principles of effective consultation: an update for the 21st-century consultant. Arch Intern Med. 2007;167(3):271-275.
- Horwitz RI, Henes CG, Horwitz SM. Developing strategies for improving the diagnostic and management efficacy of medical consultations. J Chron Dis. 1983;36(2):213-218.
- Sears CL, Charlson ME. The effectiveness of a consultation: compliance with initial recommendations. Am J Med. 1983;74(5):870-876.
- MacKenzie TB, Popkin MK, Callies AL, Jorgensen CR, Cohn JN. The effectiveness of cardiology consultations. Concordance with diagnostic and drug recommendations. Chest. 1981;79(1):16-22.
Risk of Perioperative Morbidity, Post-Op Mortality Higher for Current Smokers
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day postoperative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10–1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51–1.81 vs. OR 1.20; CI, 1.09–1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40–1.51 vs. OR, 1.13; CI, 1.08–1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease postoperative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013;148:755-762.
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day postoperative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10–1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51–1.81 vs. OR 1.20; CI, 1.09–1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40–1.51 vs. OR, 1.13; CI, 1.08–1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease postoperative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013;148:755-762.
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day postoperative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10–1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51–1.81 vs. OR 1.20; CI, 1.09–1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40–1.51 vs. OR, 1.13; CI, 1.08–1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease postoperative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013;148:755-762.
Reviews of Reseach on Perioperative Morbidity, Capnography with Diabetic Ketoacidosis in the ED, Mortality Rate for Elective Surgeries
In This Edition
Literature At A Glance
A guide to this month’s studies
- Early treatment with intravenous tPA for acute stroke
- Perioperative morbidity, mortality for current smokers
- Statins associated with musculoskeletal conditions
- Antithrombotic medications in patients with history of stroke
- Extended prophylaxis with aspirin for patients after total hip arthroplasty
- Prognosis for symptomatic subsegmental pulmonary embolism
- Video-based educational workshops for academic hospitalists
- Increased mortality for elective surgeries on Fridays, weekends
- Basal plus correction insulin regimen and Type 2 diabetes
- Capnography to diagnose diabetic ketoacidosis in the ED
- How publicly reported mortality rates correlate with hospitals’ overall mortality
- Cost savings and preventable acute-care visits for Medicare patients
Early tPA in Acute Stroke Is Associated with Better Short-Term Outcomes in Routine Clinical Practice
Clinical question: Does early treatment with intravenous (IV) tissue plasminogen activator (tPA) result in better outcomes among patients with acute ischemic stroke in routine clinical practice?
Background: IV tPA for acute ischemic stroke is beneficial if given in the first 4.5 hours after symptom onset. However, pooled data from clinical trials have been limited in characterizing the extent to which onset-to-treatment (OTT) with IV tPA influences outcomes and how effective tPA is in routine clinical practice.
Study design: Data analysis from a stroke registry.
Setting: One thousand three hundred ninety-five U.S. hospitals participating in the Get with the Guidelines—Stroke Program.
Synopsis: Data were analyzed from 58,353 tPA-treated patients within 4.5 hours of symptom onset. Clinical outcomes were compared among patients treated in the 0-90-, 91-180-, and 181-270-minute OTT windows. Patient factors strongly associated with shorter OTT were greater stroke severity (odds ratio [OR] 2.8; 95% confidence interval [CI], 2.5-3.1 per five-point increase), arrival by ambulance (OR 5.9; 95% CI, 4.5-7.3), and arrival during regular hours (OR 4.6; 95% CI, 3.8-5.4). Faster OTT, in 15-minute increments, was associated with reduced in-hospital mortality (OR 0.96; 95% CI, 0.95-0.98; P<.001), reduced symptomatic intracranial hemorrhage (OR 0.96; 95% CI, 0.95-0.98; P<.001), increased achievement of independent ambulation at discharge (OR 1.04; 95% CI, 1.03-1.05; P<.001), and increased discharge to home (OR 1.03; 95% CI, 1.02-1.04; P<.001).
Data collected were dependent on the accuracy and completeness of the chart abstraction, and only short-term outcomes were reported. Although no post-discharge outcomes were reported, previous studies have shown that functional status at discharge strongly correlates with three-month disability outcomes.
Bottom line: In routine clinical practice, earlier tPA for acute ischemic strokes results in better short-term clinical outcomes.
Citation: Saver JL, Fonarow GC, Smith EE, et al. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA. 2013;309:2480-2488.
Current Smokers Have Higher Perioperative Morbidity and Mortality Compared to Past Smokers
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day post-operative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10-1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51-1.81 vs. OR 1.20; CI, 1.09-1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40-1.51 vs. OR, 1.13; CI, 1.08-1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease post-operative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013 Jun 19:1-8. doi: 10.1001/jamasurg.2013.2360 [Epub ahead of print].
Statins Associated with Several Musculoskeletal Conditions
Clinical question: Is statin use associated with musculoskeletal adverse events, including arthropathy and injury, in physically active individuals?
Background: Statin-induced musculoskeletal adverse events (AEs) include myalgias, muscle weakness, cramps, rhabdomyolysis, and tendinous disease. The full spectrum of AEs is unknown because randomized clinical trials have not been powered to detect uncommon AEs.
Study design: Retrospective cohort study with propensity score matching.
Setting: San Antonio military area.
Synopsis: A total of 46,249 patients aged 30 to 85 years who met study criteria were propensity-matched into 6,967 statin users and 6,967 nonusers. The occurrence of musculoskeletal conditions were categorized using ICD-9 codes: Msk1, all musculoskeletal diseases; Msk1a, arthropathies and related diseases; Msk1b, injury-related diseases; and Msk2, drug-associated musculoskeletal pain. Of these, statin users had a higher odds ratio (OR) for Msk1 (OR 1.19; 95% CI, 1.08-1.30), Msk1b (1.13; 1.05-1.21), and Msk2 (1.09; 1.02-1.18). Msk1b (arthropathies) had an OR of 1.07 (0.9-1.16, P=0.07). Simvastatin was used by 73.5% of patients, and years of simvastatin use was not a significant predictor of any of the outcome measures. Secondary and sensitivity analyses showed higher adjusted ORs for statin users in all groups. This study was limited by the use of ICD-9-CM codes for identification of baseline characteristics, and the musculoskeletal diagnosis groups used were not validated.
Bottom line: Statin use is associated with an increased likelihood of musculoskeletal conditions, arthropathies, injuries, and pain.
Citation: Mansi I, Frei CR, Pugh M, Makris U, Mortensen EM. Statins and musculoskeletal conditions, arthropathies, and injuries. JAMA Intern Med. 2013;173:1318-1326.
Evidence-Based Guidelines on Periprocedural Management of Antithrombotic Medications in Patients with History of Stroke
Clinical question: What is the evidence for the periprocedural management of antithrombotics in patients with ischemic cerebrovascular accidents (CVAs)?
Background: Evidence-based guidelines are needed to help clinicians determine the thromboembolic risk of temporary discontinuation of antithrombotic medications, the perioperative bleeding risks of continuing antithrombotic agents, whether bridging therapy should be used, and the appropriate timing of antithrombotic agent discontinuation.
Study design: Systematic literature review with practice recommendations.
Setting: American Academy of Neurology Guideline Development Subcommittee convened an expert panel to review and provide recommendations.
Synopsis: Researchers analyzed 133 literature reviews via MEDLINE and EMBASE. Aspirin in stroke patients:
- Should routinely be continued for dental procedures (Level A);
- Should probably be continued for invasive ocular anesthesia, cataract surgery, dermatologic procedures, transrectal ultrasound-guided prostate biopsy, spinal/epidural procedures, and carpal tunnel surgery (Level B); and
- Should possibly be continued for vitreoretinal surgery, electromyogram (EMG), transbronchial lung biopsy, colonoscopic polypectomy, upper endoscopy and biopsy/sphincterotomy, and abdominal ultrasound-guided biopsies (Level C).
Warfarin in stroke patients:
- Should routinely be continued for dental procedures (Level A); and
- Should possibly continued for dermatologic procedures (Level B) and EMG, prostate procedures, inguinal hemiorrhaphy, and endothermal ablation of great saphenous vein (Level C).
- There is a lack of evidence on warfarin for ophthalmologic procedures, with the exception of ocular anesthesia, where it probably does not increase clinically significant bleeding (Level B).
There was not enough evidence to support or refute a recommendation regarding heparin bridge therapy in reducing thromboembolism in chronically anticoagulated patients (Level B).
Bottom line: These are the most up-to-date guidelines for anticoagulant and antiplatelet agents in patients with transient ischemic attacks and strokes undergoing procedures, but further research is needed in many areas.
Citation: Armstrong MJ, Gronseth G Anderson DC, et al. Summary of evidence-based guideline: periprocedural management of antithrombotic medications in patients with ischemic cerebrovascular disease: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2065-2069.
Extended Prophylaxis with Aspirin Was Noninferior to Extended Prophylaxis with Low-Molecular-Weight Heparin
Clinical question: Is aspirin as effective as low-molecular-weight heparin (LMWH) for the extended prophylaxis of venous thromboembolism (VTE) after total hip arthroplasty (THA)?
Background: Deep vein thrombosis (DVT) and pulmonary embolism (PE) are common complications after THA. After initial prophylaxis, LMWH given for up to 30 days has been shown to reduce VTE compared with placebo. However, LMWH is costly and may increase the risk of minor bleeding. Aspirin is a potentially simple, low-cost alternative.
Study design: Randomized, placebo-controlled trial.
Setting: Twelve university-affiliated orthopedic hospitals in Canada.
Synopsis: Patients undergoing elective THA without hip fracture, metastatic cancer, or bleeding precluding anticoagulants were eligible. All patients received dalteparin for 10 days and were then randomized to aspirin 81 mg daily or to continue dalteparin. The primary outcome was symptomatic proximal DVT or PE during 90 days’ follow-up. The study was terminated early due to slow enrollment. At that time, 2,364 patients had been enrolled, and an analysis by an independent data safety and monitoring board determined that continuing the study was unlikely to alter the main findings. Extended prophylaxis with aspirin was noninferior to LMWH for the primary outcome, which occurred in 0.3% vs. 1.3%, respectively (95% CI, -0.5% to 2.5%, P<.001 for noninferiority). There were no significant differences in major or minor bleeding.
Though the early termination is a concern, the sample size was large and the results do not suggest inadequate power as a reason for lack of superiority for LMWH. Also, all patients received 10 days of LMWH, which indicates a period of LMWH after discharge will still be needed for most patients prior to initiating aspirin.
Bottom line: After initial LMWH prophylaxis for 10 days, extended prophylaxis with aspirin can be considered, particularly for patients for whom LMWH may not be feasible.
Citation: Anderson DR, Dunbar MJ, Bohm ER, et al. Aspirin versus low-molecular-weight heparin for extended venous thromboembolism prophylaxis after total hip arthroplasty: a randomized trial. Ann Intern Med. 2013;158:800-806.
Symptomatic Subsegmental Pulmonary Embolism (PE) Has a Prognosis Similar to Proximal PE
Clinical question: Is the prognosis of a symptomatic subsegmental pulmonary embolism (PE) similar to that of a more proximal PE?
Background: The use of multidetector computed tomography angiography (CTA) has allowed for better assessment of the pulmonary vasculature and increased detection of distal emboli. Prior studies have raised questions on the clinical importance of subsegmental PE but have been limited by small size or retrospective design.
Study design: Combined data from two prospective trials of management of suspected PE.
Setting: Twelve hospitals in the Netherlands and four tertiary-care emergency departments in Canada.
Synopsis: The study cohort consisted of 3,769 patients with suspected PE, of which 2,688 underwent CTA. Of patients diagnosed with PE, 15.5% had isolated subsegmental emboli. All patients were treated with anticoagulation. During three months of follow-up, the incidence of symptomatic recurrence for subsegmental PE was similar to patients with proximal PE (3.6% vs. 2.5%, respectively). The mortality rates for patients with subsegmental and proximal PE were also similar (10.3% vs. 6.3%, respectively).
The study may have been underpowered to detect small differences in event rates; however, there was no trend suggesting that subsegmental PE had better outcomes than more proximal PE. Also, the study did not specifically investigate whether any management strategy is preferred based on thrombus location on CTA.
Bottom line: Clinicians should continue to anticoagulate patients with subsegmental PE as the prognosis is similar to those with proximal PE.
Citation: Den Exter PL, van Es J, Klok FA, et al. Risk profile and clinical outcome of symptomatic subsegmental pulmonary embolism. Blood. 2013;122:1144-1149.
Video-Based Educational Workshop for Academic Hospitalists and House Staff May Improve Professionalism
Clinical question: Can video-based education promote professionalism among academic hospitalists and house staff?
Background: Unprofessional behavior by academic hospitalists and residents can negatively impact the learning environment and patient safety. This behavior increases throughout training, and faculty behavior can be influential. There is a paucity of educational materials to train hospitalists and house staff to recognize and ameliorate unprofessional behaviors.
Study design: Educational survey study.
Setting: University of Chicago, Northwestern University, and NorthShore University Health System teaching hospitals.
Synopsis: Three videos were developed displaying three types of unprofessional behavior: disparaging other physicians, “blocking” admissions, and misrepresenting tests to expedite their completion. There were 44 hospitalists and 244 house staff who received a 60-minute workshop in which they watched the videos using a viewing tool and discussed the videos in small groups.
For all three videos, more than three-quarters of both hospitalists and house staff felt the behavior was unprofessional or somewhat unprofessional. Hospitalists and house staff found the workshop useful and effective (65.9% and 77.1%, respectively) and would change their behavior as a result of the workshop (65.9% and 67.2%, respectively). Those who perceived the videos as “very realistic” were more likely to report intent to change behavior (93% vs. 53%, P=0.01).
This study is limited by its small sample size and possible selection bias. Those interested or concerned about unprofessional behavior may have been more likely to attend the workshop.
Bottom line: Video-based professionalism education is a feasible and well-received way to educate hospitalists and residents about unprofessional behavior and may even affect their future behavior.
Citation: Farnan JM, O’Leary KJ, Didwania A, et al. Promoting professionalism via a video-based educational workshop for academic hospitalists and housestaff. J Hosp Med. 2013;8:386-389.
Friday and Weekend Elective Surgeries Have Increased Mortality
Clinical question: How can the association between mortality and the day of elective surgical procedures be assessed?
Background: Several studies have described the “weekend effect” for both surgical and medical patients, with higher mortality and length of stay in patients admitted on the weekend compared to weekdays. Two potential explanations are poorer quality of care being delivered on the weekend or more severely ill patients being operated on or admitted on the weekend.
Study design: Retrospective analysis of national hospital administrative data.
Setting: All acute-care and specialist hospitals in England from 2008 to 2011.
Synopsis: There were 4,133,346 elective, inpatient surgical procedures studied. Friday surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.44 [95% CI, 1.39-1.50] and 1.42 [95% CI, 1.26-1.60], respectively, when compared with Monday. Weekend surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.82 [95% CI, 1.71-1.94] and 2.67 [95% CI, 2.30-3.09], respectively, when compared with Monday. There were significant trends toward higher mortality at the end of the workweek and weekends for four high-risk procedures: esophagus and/or stomach excision, colon and/or rectum excisions, coronary artery bypass graft, and lung excision. For lower-risk procedures, there was a significant increase in mortality for Friday surgeries but not weekend surgeries. As with all studies using administrative data, inherent selection biases could not be adjusted for Friday or weekend procedures.
Bottom line: Elective surgeries that occur on the weekend and later in the week have an increased risk of mortality, implying that the weekend effect is due to poorer quality of care during weekends, rather than higher-acuity patients presenting on weekends.
Citation: Aylin P, Alexandrescu R, Jen MH, Mayer EK, Bottle A. Day of week of procedure and 30 day mortality for elective surgery: retrospective analysis of hospital episode statistics. BMJ. 2013;346:f2424.
Basal Plus Correction Insulin Regimen Is Effective in Hospitalized Patients with Type 2 Diabetes
Clinical question: Does a basal plus correction insulin regimen (as needed with meals) result in similar glycemic control and lower rates of hypoglycemia compared to a basal-bolus regimen?
Background: Basal bolus is the preferred insulin regimen for non-critically-ill hospitalized patients as per clinical guidelines. But use is limited due to the complexity of the regimen and the fear of inducing hypoglycemia. A less complex, easier-to-implement basal plus correction insulin regimen may be an effective alternative.
Study design: Multicenter, prospective, open-label, randomized study.
Setting: Six hospitals in the U.S.
Synopsis: A group of 375 medical and surgical patients with Type 2 diabetes treated with diet, oral anti-diabetic agents, or low-dose insulin (≤ 0.4 units/kg/day) were randomized to:
- Basal-bolus insulin regimen with glargine once daily and fixed doses of glusiline before meals;
- Basal plus correction insulin (“basal plus”) regimen with glargine once daily and glusiline sliding scale insulin (SSI) before meals; or
- Regular SSI alone.
After the first day of therapy, treatment with basal-bolus and basal-plus regimens resulted in similar improvements in daily blood glucose (BG) (P=0.16), and both were superior to SSI alone (P=0.04). Both regimens also resulted in less treatment failure (defined as mean daily BG of >240 mg/dl or >2 consecutive BG >240 mg/dl) than did treatment with SSI. Hypoglycemia (BG <70 mg/dl) occurred in 16%, 13%, and 3% of patients in the basal-bolus, basal-plus, and SSI groups, respectively (P=0.02). There were no between-group differences in the frequency of severe hypoglycemia (<40 mg/dl; P=0.76).
The study was not powered to evaluate hospital complications (infection, mortality, hospital stay, and readmissions) across groups.
Bottom line: The basal-plus regimen resulted in glycemic control similar to standard basal-bolus regimen and is an effective alternative for the initial management of hyperglycemia in general medical and surgical patients with Type 2 diabetes.
Citation: Umpierrez GE, Smiley D, Hermayer K, et al. Randomized study comparing a basal-bolus with a basal plus correction insulin regimen for the hospital management of medical and surgical patients with type 2 diabetes: Basal plus trial. Diabetes Care. 2013;36:2169-2174.
Capnography Can Help Diagnose Diabetic Ketoacidosis in the ED
Clinical question: Can capnography be used as a screening tool to identify patients with diabetic ketoacidosis (DKA)?
Background: Metabolic acidosis is a major criterion for diagnosing DKA. Previous studies have shown that end-tidal carbon dioxide (ETCO2) measurement by capnography can provide an accurate estimation of arterial carbon dioxide tension (PaCO2) and may be a noninvasive, fast, inexpensive measurement of acidosis in DKA. However, those studies were in pediatric patients and had small sample sizes.
Study design: Cross-sectional, prospective descriptive-analytic study.
Setting: The ED of Imam Reza Medical Research and Training Hospital, Tabriz, East Azarbaijan, Iran.
Synopsis: A total of 181 adult patients older than 18 with suspected DKA and blood sugar >250 mg/dl were included in the study. Simultaneous capnography and arterial blood gas (ABG) were obtained on all patients. Urine ketones, complete blood count, serum levels of potassium, urea, and creatinine were collected. Sixty-two patients were found to have DKA, while 119 had other conditions associated with metabolic acidosis. There was a significant linear relationship between pH and ETCO2 (P>0.0001, relative risk (R)=0.253), PaCO2 and ETCO2 (P>0.0001, R=0.572), and bicarbonate (HCO3) and ETCO2 (P>0.0001, R=0.730). ETCO2 values >24.5 mmHg had a sensitivity and specificity of 0.90 for ruling out DKA. No cutoff point could be determined for ruling in DKA.
The study was open to selection bias as patient collection was only done during the day, so eligible subjects may have been missed. Moreover, though the study suggests that capnography has a role in ruling out DKA, the exact cutoff value is unclear. Other studies found that higher values were needed to exclude diagnosis.
Bottom line: Using ETCO2 values >24.5 mmHg, capnography can help exclude the diagnosis of DKA in adult patients with elevated BG.
Citation: Soleimanour H, Taghizadieh A, Niafar M, Rahmani F, Golzari S, Esfanjani RM. Predictive value of capnography for diagnosis in patients with suspected diabetic ketoacidosis in the emergency department. West J Emerg Med. 2013. doi: 10.5811/westjem.2013.4.14296.
Publicly Reported Mortality Correlates with Overall Mortality
Clinical question: Are publicly reported mortality rates associated with a hospital’s overall medical and surgical mortality rate?
Background: Public reporting of mortality has become an important strategy in Medicare’s quality-improvement initiative. However, the mortality rate for only three conditions, acute myocardial infarction, congestive heart failure, and pneumonia are reported. It is unclear if these rates correlate to a hospital’s overall mortality rate.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Using 2008-2009 data from 2,322 acute-care hospitals with 6.7 million admissions, an aggregate mortality rate for the three publicly reported conditions, a standardized 30-day mortality rate for selected medical and surgical conditions, and an overall average composite mortality score was calculated for each hospital. Based on their mortality for the three publicly reported conditions, hospitals were grouped into quartiles from highest (top-performing hospitals) to lowest mortality (poor-performing hospitals).
Top-performing hospitals had a 3.6% (9.4%vs 13.0%; P<.001) lower mortality rate than poor-performing hospitals and an odds ratio >5 of being a top performer in overall mortality (OR 5.3; 95% CI, 4.3-6.5). They also had an 81% lower chance of being in the worst-performing quartile in overall mortality (OR 0.19; 95% CI, 0.14-0.27). Conversely, poor-performing hospitals had a 4.5 times higher risk of being in the lowest quartile in overall mortality. The study is limited by the use of administrative data, which limits the ability to adjust for severity of illness, overall health, and socioeconomic status of each hospital’s population.
Bottom line: A hospital’s mortality performance on the three publicly reported conditions may predict mortality rates across a wide range of medical and surgical conditions.
Citation: McCrum ML, Joynt KE, Orav EJ, Gawande AA, Jha AK. Mortality for publicly reported conditions and overall hospital mortality rates. JAMA Intern Med. 2013;173:1351-1357.
Cost Savings in Decreasing Preventable Acute-Care Visits Are Limited among High-Cost Medicare Utilizers
Clinical question: What role do preventable acute-care visits play in the overall costs of care for the highest Medicare utilizers?
Background: Some 10% of Medicare patients account for more than half the costs. Interventions targeted at decreasing acute-care costs (ED visits and inpatient hospitalizations) for this high-cost population are widespread, but it is unknown what impact they can have.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Standardized total costs were created for fee-for-service Medicare patients for 2009 and 2010 in order to identify high-cost and persistently high-cost patients. Algorithms were used to identify preventable ED visits and hospitalizations in both the high-cost and non-high-cost cohorts.
Of the more than 1 million patients in the sample Medicare population, as many as 113,341 were high-cost. As much as 73% of acute-care spending was attributable to this cohort. Overall, 10% of acute-care costs were felt to be preventable in the high-cost group, 13.5% in the persistently high-cost group, and 19% in the non-high-cost group for 2010. The most common reasons for preventable acute care in the high-cost cohort were heart failure, bacterial pneumonia, and chronic obstructive pulmonary disease. Catastrophic events (myocardial infarction, stroke, sepsis), cancer, and orthopedic procedures drove overall inpatient costs in the high-cost group.
Preventable costs were higher per capita in areas with higher numbers of primary-care and specialist physicians, but it’s unclear if this was a supply or demand issue. The study also used algorithms that possibly overestimate the amount of preventable acute care.
Bottom line: In the highest Medicare utilizers, cost savings aimed at preventable acute care may be limited and might be better targeted at efficiency during acute-care episodes.
Citation: Joynt KE, Gawande AA, Orav EJ, Jha AK. Contribution of preventable acute care spending to total spending for high-cost Medicare patients. JAMA. 2013;309:2572-2578.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Early treatment with intravenous tPA for acute stroke
- Perioperative morbidity, mortality for current smokers
- Statins associated with musculoskeletal conditions
- Antithrombotic medications in patients with history of stroke
- Extended prophylaxis with aspirin for patients after total hip arthroplasty
- Prognosis for symptomatic subsegmental pulmonary embolism
- Video-based educational workshops for academic hospitalists
- Increased mortality for elective surgeries on Fridays, weekends
- Basal plus correction insulin regimen and Type 2 diabetes
- Capnography to diagnose diabetic ketoacidosis in the ED
- How publicly reported mortality rates correlate with hospitals’ overall mortality
- Cost savings and preventable acute-care visits for Medicare patients
Early tPA in Acute Stroke Is Associated with Better Short-Term Outcomes in Routine Clinical Practice
Clinical question: Does early treatment with intravenous (IV) tissue plasminogen activator (tPA) result in better outcomes among patients with acute ischemic stroke in routine clinical practice?
Background: IV tPA for acute ischemic stroke is beneficial if given in the first 4.5 hours after symptom onset. However, pooled data from clinical trials have been limited in characterizing the extent to which onset-to-treatment (OTT) with IV tPA influences outcomes and how effective tPA is in routine clinical practice.
Study design: Data analysis from a stroke registry.
Setting: One thousand three hundred ninety-five U.S. hospitals participating in the Get with the Guidelines—Stroke Program.
Synopsis: Data were analyzed from 58,353 tPA-treated patients within 4.5 hours of symptom onset. Clinical outcomes were compared among patients treated in the 0-90-, 91-180-, and 181-270-minute OTT windows. Patient factors strongly associated with shorter OTT were greater stroke severity (odds ratio [OR] 2.8; 95% confidence interval [CI], 2.5-3.1 per five-point increase), arrival by ambulance (OR 5.9; 95% CI, 4.5-7.3), and arrival during regular hours (OR 4.6; 95% CI, 3.8-5.4). Faster OTT, in 15-minute increments, was associated with reduced in-hospital mortality (OR 0.96; 95% CI, 0.95-0.98; P<.001), reduced symptomatic intracranial hemorrhage (OR 0.96; 95% CI, 0.95-0.98; P<.001), increased achievement of independent ambulation at discharge (OR 1.04; 95% CI, 1.03-1.05; P<.001), and increased discharge to home (OR 1.03; 95% CI, 1.02-1.04; P<.001).
Data collected were dependent on the accuracy and completeness of the chart abstraction, and only short-term outcomes were reported. Although no post-discharge outcomes were reported, previous studies have shown that functional status at discharge strongly correlates with three-month disability outcomes.
Bottom line: In routine clinical practice, earlier tPA for acute ischemic strokes results in better short-term clinical outcomes.
Citation: Saver JL, Fonarow GC, Smith EE, et al. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA. 2013;309:2480-2488.
Current Smokers Have Higher Perioperative Morbidity and Mortality Compared to Past Smokers
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day post-operative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10-1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51-1.81 vs. OR 1.20; CI, 1.09-1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40-1.51 vs. OR, 1.13; CI, 1.08-1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease post-operative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013 Jun 19:1-8. doi: 10.1001/jamasurg.2013.2360 [Epub ahead of print].
Statins Associated with Several Musculoskeletal Conditions
Clinical question: Is statin use associated with musculoskeletal adverse events, including arthropathy and injury, in physically active individuals?
Background: Statin-induced musculoskeletal adverse events (AEs) include myalgias, muscle weakness, cramps, rhabdomyolysis, and tendinous disease. The full spectrum of AEs is unknown because randomized clinical trials have not been powered to detect uncommon AEs.
Study design: Retrospective cohort study with propensity score matching.
Setting: San Antonio military area.
Synopsis: A total of 46,249 patients aged 30 to 85 years who met study criteria were propensity-matched into 6,967 statin users and 6,967 nonusers. The occurrence of musculoskeletal conditions were categorized using ICD-9 codes: Msk1, all musculoskeletal diseases; Msk1a, arthropathies and related diseases; Msk1b, injury-related diseases; and Msk2, drug-associated musculoskeletal pain. Of these, statin users had a higher odds ratio (OR) for Msk1 (OR 1.19; 95% CI, 1.08-1.30), Msk1b (1.13; 1.05-1.21), and Msk2 (1.09; 1.02-1.18). Msk1b (arthropathies) had an OR of 1.07 (0.9-1.16, P=0.07). Simvastatin was used by 73.5% of patients, and years of simvastatin use was not a significant predictor of any of the outcome measures. Secondary and sensitivity analyses showed higher adjusted ORs for statin users in all groups. This study was limited by the use of ICD-9-CM codes for identification of baseline characteristics, and the musculoskeletal diagnosis groups used were not validated.
Bottom line: Statin use is associated with an increased likelihood of musculoskeletal conditions, arthropathies, injuries, and pain.
Citation: Mansi I, Frei CR, Pugh M, Makris U, Mortensen EM. Statins and musculoskeletal conditions, arthropathies, and injuries. JAMA Intern Med. 2013;173:1318-1326.
Evidence-Based Guidelines on Periprocedural Management of Antithrombotic Medications in Patients with History of Stroke
Clinical question: What is the evidence for the periprocedural management of antithrombotics in patients with ischemic cerebrovascular accidents (CVAs)?
Background: Evidence-based guidelines are needed to help clinicians determine the thromboembolic risk of temporary discontinuation of antithrombotic medications, the perioperative bleeding risks of continuing antithrombotic agents, whether bridging therapy should be used, and the appropriate timing of antithrombotic agent discontinuation.
Study design: Systematic literature review with practice recommendations.
Setting: American Academy of Neurology Guideline Development Subcommittee convened an expert panel to review and provide recommendations.
Synopsis: Researchers analyzed 133 literature reviews via MEDLINE and EMBASE. Aspirin in stroke patients:
- Should routinely be continued for dental procedures (Level A);
- Should probably be continued for invasive ocular anesthesia, cataract surgery, dermatologic procedures, transrectal ultrasound-guided prostate biopsy, spinal/epidural procedures, and carpal tunnel surgery (Level B); and
- Should possibly be continued for vitreoretinal surgery, electromyogram (EMG), transbronchial lung biopsy, colonoscopic polypectomy, upper endoscopy and biopsy/sphincterotomy, and abdominal ultrasound-guided biopsies (Level C).
Warfarin in stroke patients:
- Should routinely be continued for dental procedures (Level A); and
- Should possibly continued for dermatologic procedures (Level B) and EMG, prostate procedures, inguinal hemiorrhaphy, and endothermal ablation of great saphenous vein (Level C).
- There is a lack of evidence on warfarin for ophthalmologic procedures, with the exception of ocular anesthesia, where it probably does not increase clinically significant bleeding (Level B).
There was not enough evidence to support or refute a recommendation regarding heparin bridge therapy in reducing thromboembolism in chronically anticoagulated patients (Level B).
Bottom line: These are the most up-to-date guidelines for anticoagulant and antiplatelet agents in patients with transient ischemic attacks and strokes undergoing procedures, but further research is needed in many areas.
Citation: Armstrong MJ, Gronseth G Anderson DC, et al. Summary of evidence-based guideline: periprocedural management of antithrombotic medications in patients with ischemic cerebrovascular disease: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2065-2069.
Extended Prophylaxis with Aspirin Was Noninferior to Extended Prophylaxis with Low-Molecular-Weight Heparin
Clinical question: Is aspirin as effective as low-molecular-weight heparin (LMWH) for the extended prophylaxis of venous thromboembolism (VTE) after total hip arthroplasty (THA)?
Background: Deep vein thrombosis (DVT) and pulmonary embolism (PE) are common complications after THA. After initial prophylaxis, LMWH given for up to 30 days has been shown to reduce VTE compared with placebo. However, LMWH is costly and may increase the risk of minor bleeding. Aspirin is a potentially simple, low-cost alternative.
Study design: Randomized, placebo-controlled trial.
Setting: Twelve university-affiliated orthopedic hospitals in Canada.
Synopsis: Patients undergoing elective THA without hip fracture, metastatic cancer, or bleeding precluding anticoagulants were eligible. All patients received dalteparin for 10 days and were then randomized to aspirin 81 mg daily or to continue dalteparin. The primary outcome was symptomatic proximal DVT or PE during 90 days’ follow-up. The study was terminated early due to slow enrollment. At that time, 2,364 patients had been enrolled, and an analysis by an independent data safety and monitoring board determined that continuing the study was unlikely to alter the main findings. Extended prophylaxis with aspirin was noninferior to LMWH for the primary outcome, which occurred in 0.3% vs. 1.3%, respectively (95% CI, -0.5% to 2.5%, P<.001 for noninferiority). There were no significant differences in major or minor bleeding.
Though the early termination is a concern, the sample size was large and the results do not suggest inadequate power as a reason for lack of superiority for LMWH. Also, all patients received 10 days of LMWH, which indicates a period of LMWH after discharge will still be needed for most patients prior to initiating aspirin.
Bottom line: After initial LMWH prophylaxis for 10 days, extended prophylaxis with aspirin can be considered, particularly for patients for whom LMWH may not be feasible.
Citation: Anderson DR, Dunbar MJ, Bohm ER, et al. Aspirin versus low-molecular-weight heparin for extended venous thromboembolism prophylaxis after total hip arthroplasty: a randomized trial. Ann Intern Med. 2013;158:800-806.
Symptomatic Subsegmental Pulmonary Embolism (PE) Has a Prognosis Similar to Proximal PE
Clinical question: Is the prognosis of a symptomatic subsegmental pulmonary embolism (PE) similar to that of a more proximal PE?
Background: The use of multidetector computed tomography angiography (CTA) has allowed for better assessment of the pulmonary vasculature and increased detection of distal emboli. Prior studies have raised questions on the clinical importance of subsegmental PE but have been limited by small size or retrospective design.
Study design: Combined data from two prospective trials of management of suspected PE.
Setting: Twelve hospitals in the Netherlands and four tertiary-care emergency departments in Canada.
Synopsis: The study cohort consisted of 3,769 patients with suspected PE, of which 2,688 underwent CTA. Of patients diagnosed with PE, 15.5% had isolated subsegmental emboli. All patients were treated with anticoagulation. During three months of follow-up, the incidence of symptomatic recurrence for subsegmental PE was similar to patients with proximal PE (3.6% vs. 2.5%, respectively). The mortality rates for patients with subsegmental and proximal PE were also similar (10.3% vs. 6.3%, respectively).
The study may have been underpowered to detect small differences in event rates; however, there was no trend suggesting that subsegmental PE had better outcomes than more proximal PE. Also, the study did not specifically investigate whether any management strategy is preferred based on thrombus location on CTA.
Bottom line: Clinicians should continue to anticoagulate patients with subsegmental PE as the prognosis is similar to those with proximal PE.
Citation: Den Exter PL, van Es J, Klok FA, et al. Risk profile and clinical outcome of symptomatic subsegmental pulmonary embolism. Blood. 2013;122:1144-1149.
Video-Based Educational Workshop for Academic Hospitalists and House Staff May Improve Professionalism
Clinical question: Can video-based education promote professionalism among academic hospitalists and house staff?
Background: Unprofessional behavior by academic hospitalists and residents can negatively impact the learning environment and patient safety. This behavior increases throughout training, and faculty behavior can be influential. There is a paucity of educational materials to train hospitalists and house staff to recognize and ameliorate unprofessional behaviors.
Study design: Educational survey study.
Setting: University of Chicago, Northwestern University, and NorthShore University Health System teaching hospitals.
Synopsis: Three videos were developed displaying three types of unprofessional behavior: disparaging other physicians, “blocking” admissions, and misrepresenting tests to expedite their completion. There were 44 hospitalists and 244 house staff who received a 60-minute workshop in which they watched the videos using a viewing tool and discussed the videos in small groups.
For all three videos, more than three-quarters of both hospitalists and house staff felt the behavior was unprofessional or somewhat unprofessional. Hospitalists and house staff found the workshop useful and effective (65.9% and 77.1%, respectively) and would change their behavior as a result of the workshop (65.9% and 67.2%, respectively). Those who perceived the videos as “very realistic” were more likely to report intent to change behavior (93% vs. 53%, P=0.01).
This study is limited by its small sample size and possible selection bias. Those interested or concerned about unprofessional behavior may have been more likely to attend the workshop.
Bottom line: Video-based professionalism education is a feasible and well-received way to educate hospitalists and residents about unprofessional behavior and may even affect their future behavior.
Citation: Farnan JM, O’Leary KJ, Didwania A, et al. Promoting professionalism via a video-based educational workshop for academic hospitalists and housestaff. J Hosp Med. 2013;8:386-389.
Friday and Weekend Elective Surgeries Have Increased Mortality
Clinical question: How can the association between mortality and the day of elective surgical procedures be assessed?
Background: Several studies have described the “weekend effect” for both surgical and medical patients, with higher mortality and length of stay in patients admitted on the weekend compared to weekdays. Two potential explanations are poorer quality of care being delivered on the weekend or more severely ill patients being operated on or admitted on the weekend.
Study design: Retrospective analysis of national hospital administrative data.
Setting: All acute-care and specialist hospitals in England from 2008 to 2011.
Synopsis: There were 4,133,346 elective, inpatient surgical procedures studied. Friday surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.44 [95% CI, 1.39-1.50] and 1.42 [95% CI, 1.26-1.60], respectively, when compared with Monday. Weekend surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.82 [95% CI, 1.71-1.94] and 2.67 [95% CI, 2.30-3.09], respectively, when compared with Monday. There were significant trends toward higher mortality at the end of the workweek and weekends for four high-risk procedures: esophagus and/or stomach excision, colon and/or rectum excisions, coronary artery bypass graft, and lung excision. For lower-risk procedures, there was a significant increase in mortality for Friday surgeries but not weekend surgeries. As with all studies using administrative data, inherent selection biases could not be adjusted for Friday or weekend procedures.
Bottom line: Elective surgeries that occur on the weekend and later in the week have an increased risk of mortality, implying that the weekend effect is due to poorer quality of care during weekends, rather than higher-acuity patients presenting on weekends.
Citation: Aylin P, Alexandrescu R, Jen MH, Mayer EK, Bottle A. Day of week of procedure and 30 day mortality for elective surgery: retrospective analysis of hospital episode statistics. BMJ. 2013;346:f2424.
Basal Plus Correction Insulin Regimen Is Effective in Hospitalized Patients with Type 2 Diabetes
Clinical question: Does a basal plus correction insulin regimen (as needed with meals) result in similar glycemic control and lower rates of hypoglycemia compared to a basal-bolus regimen?
Background: Basal bolus is the preferred insulin regimen for non-critically-ill hospitalized patients as per clinical guidelines. But use is limited due to the complexity of the regimen and the fear of inducing hypoglycemia. A less complex, easier-to-implement basal plus correction insulin regimen may be an effective alternative.
Study design: Multicenter, prospective, open-label, randomized study.
Setting: Six hospitals in the U.S.
Synopsis: A group of 375 medical and surgical patients with Type 2 diabetes treated with diet, oral anti-diabetic agents, or low-dose insulin (≤ 0.4 units/kg/day) were randomized to:
- Basal-bolus insulin regimen with glargine once daily and fixed doses of glusiline before meals;
- Basal plus correction insulin (“basal plus”) regimen with glargine once daily and glusiline sliding scale insulin (SSI) before meals; or
- Regular SSI alone.
After the first day of therapy, treatment with basal-bolus and basal-plus regimens resulted in similar improvements in daily blood glucose (BG) (P=0.16), and both were superior to SSI alone (P=0.04). Both regimens also resulted in less treatment failure (defined as mean daily BG of >240 mg/dl or >2 consecutive BG >240 mg/dl) than did treatment with SSI. Hypoglycemia (BG <70 mg/dl) occurred in 16%, 13%, and 3% of patients in the basal-bolus, basal-plus, and SSI groups, respectively (P=0.02). There were no between-group differences in the frequency of severe hypoglycemia (<40 mg/dl; P=0.76).
The study was not powered to evaluate hospital complications (infection, mortality, hospital stay, and readmissions) across groups.
Bottom line: The basal-plus regimen resulted in glycemic control similar to standard basal-bolus regimen and is an effective alternative for the initial management of hyperglycemia in general medical and surgical patients with Type 2 diabetes.
Citation: Umpierrez GE, Smiley D, Hermayer K, et al. Randomized study comparing a basal-bolus with a basal plus correction insulin regimen for the hospital management of medical and surgical patients with type 2 diabetes: Basal plus trial. Diabetes Care. 2013;36:2169-2174.
Capnography Can Help Diagnose Diabetic Ketoacidosis in the ED
Clinical question: Can capnography be used as a screening tool to identify patients with diabetic ketoacidosis (DKA)?
Background: Metabolic acidosis is a major criterion for diagnosing DKA. Previous studies have shown that end-tidal carbon dioxide (ETCO2) measurement by capnography can provide an accurate estimation of arterial carbon dioxide tension (PaCO2) and may be a noninvasive, fast, inexpensive measurement of acidosis in DKA. However, those studies were in pediatric patients and had small sample sizes.
Study design: Cross-sectional, prospective descriptive-analytic study.
Setting: The ED of Imam Reza Medical Research and Training Hospital, Tabriz, East Azarbaijan, Iran.
Synopsis: A total of 181 adult patients older than 18 with suspected DKA and blood sugar >250 mg/dl were included in the study. Simultaneous capnography and arterial blood gas (ABG) were obtained on all patients. Urine ketones, complete blood count, serum levels of potassium, urea, and creatinine were collected. Sixty-two patients were found to have DKA, while 119 had other conditions associated with metabolic acidosis. There was a significant linear relationship between pH and ETCO2 (P>0.0001, relative risk (R)=0.253), PaCO2 and ETCO2 (P>0.0001, R=0.572), and bicarbonate (HCO3) and ETCO2 (P>0.0001, R=0.730). ETCO2 values >24.5 mmHg had a sensitivity and specificity of 0.90 for ruling out DKA. No cutoff point could be determined for ruling in DKA.
The study was open to selection bias as patient collection was only done during the day, so eligible subjects may have been missed. Moreover, though the study suggests that capnography has a role in ruling out DKA, the exact cutoff value is unclear. Other studies found that higher values were needed to exclude diagnosis.
Bottom line: Using ETCO2 values >24.5 mmHg, capnography can help exclude the diagnosis of DKA in adult patients with elevated BG.
Citation: Soleimanour H, Taghizadieh A, Niafar M, Rahmani F, Golzari S, Esfanjani RM. Predictive value of capnography for diagnosis in patients with suspected diabetic ketoacidosis in the emergency department. West J Emerg Med. 2013. doi: 10.5811/westjem.2013.4.14296.
Publicly Reported Mortality Correlates with Overall Mortality
Clinical question: Are publicly reported mortality rates associated with a hospital’s overall medical and surgical mortality rate?
Background: Public reporting of mortality has become an important strategy in Medicare’s quality-improvement initiative. However, the mortality rate for only three conditions, acute myocardial infarction, congestive heart failure, and pneumonia are reported. It is unclear if these rates correlate to a hospital’s overall mortality rate.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Using 2008-2009 data from 2,322 acute-care hospitals with 6.7 million admissions, an aggregate mortality rate for the three publicly reported conditions, a standardized 30-day mortality rate for selected medical and surgical conditions, and an overall average composite mortality score was calculated for each hospital. Based on their mortality for the three publicly reported conditions, hospitals were grouped into quartiles from highest (top-performing hospitals) to lowest mortality (poor-performing hospitals).
Top-performing hospitals had a 3.6% (9.4%vs 13.0%; P<.001) lower mortality rate than poor-performing hospitals and an odds ratio >5 of being a top performer in overall mortality (OR 5.3; 95% CI, 4.3-6.5). They also had an 81% lower chance of being in the worst-performing quartile in overall mortality (OR 0.19; 95% CI, 0.14-0.27). Conversely, poor-performing hospitals had a 4.5 times higher risk of being in the lowest quartile in overall mortality. The study is limited by the use of administrative data, which limits the ability to adjust for severity of illness, overall health, and socioeconomic status of each hospital’s population.
Bottom line: A hospital’s mortality performance on the three publicly reported conditions may predict mortality rates across a wide range of medical and surgical conditions.
Citation: McCrum ML, Joynt KE, Orav EJ, Gawande AA, Jha AK. Mortality for publicly reported conditions and overall hospital mortality rates. JAMA Intern Med. 2013;173:1351-1357.
Cost Savings in Decreasing Preventable Acute-Care Visits Are Limited among High-Cost Medicare Utilizers
Clinical question: What role do preventable acute-care visits play in the overall costs of care for the highest Medicare utilizers?
Background: Some 10% of Medicare patients account for more than half the costs. Interventions targeted at decreasing acute-care costs (ED visits and inpatient hospitalizations) for this high-cost population are widespread, but it is unknown what impact they can have.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Standardized total costs were created for fee-for-service Medicare patients for 2009 and 2010 in order to identify high-cost and persistently high-cost patients. Algorithms were used to identify preventable ED visits and hospitalizations in both the high-cost and non-high-cost cohorts.
Of the more than 1 million patients in the sample Medicare population, as many as 113,341 were high-cost. As much as 73% of acute-care spending was attributable to this cohort. Overall, 10% of acute-care costs were felt to be preventable in the high-cost group, 13.5% in the persistently high-cost group, and 19% in the non-high-cost group for 2010. The most common reasons for preventable acute care in the high-cost cohort were heart failure, bacterial pneumonia, and chronic obstructive pulmonary disease. Catastrophic events (myocardial infarction, stroke, sepsis), cancer, and orthopedic procedures drove overall inpatient costs in the high-cost group.
Preventable costs were higher per capita in areas with higher numbers of primary-care and specialist physicians, but it’s unclear if this was a supply or demand issue. The study also used algorithms that possibly overestimate the amount of preventable acute care.
Bottom line: In the highest Medicare utilizers, cost savings aimed at preventable acute care may be limited and might be better targeted at efficiency during acute-care episodes.
Citation: Joynt KE, Gawande AA, Orav EJ, Jha AK. Contribution of preventable acute care spending to total spending for high-cost Medicare patients. JAMA. 2013;309:2572-2578.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Early treatment with intravenous tPA for acute stroke
- Perioperative morbidity, mortality for current smokers
- Statins associated with musculoskeletal conditions
- Antithrombotic medications in patients with history of stroke
- Extended prophylaxis with aspirin for patients after total hip arthroplasty
- Prognosis for symptomatic subsegmental pulmonary embolism
- Video-based educational workshops for academic hospitalists
- Increased mortality for elective surgeries on Fridays, weekends
- Basal plus correction insulin regimen and Type 2 diabetes
- Capnography to diagnose diabetic ketoacidosis in the ED
- How publicly reported mortality rates correlate with hospitals’ overall mortality
- Cost savings and preventable acute-care visits for Medicare patients
Early tPA in Acute Stroke Is Associated with Better Short-Term Outcomes in Routine Clinical Practice
Clinical question: Does early treatment with intravenous (IV) tissue plasminogen activator (tPA) result in better outcomes among patients with acute ischemic stroke in routine clinical practice?
Background: IV tPA for acute ischemic stroke is beneficial if given in the first 4.5 hours after symptom onset. However, pooled data from clinical trials have been limited in characterizing the extent to which onset-to-treatment (OTT) with IV tPA influences outcomes and how effective tPA is in routine clinical practice.
Study design: Data analysis from a stroke registry.
Setting: One thousand three hundred ninety-five U.S. hospitals participating in the Get with the Guidelines—Stroke Program.
Synopsis: Data were analyzed from 58,353 tPA-treated patients within 4.5 hours of symptom onset. Clinical outcomes were compared among patients treated in the 0-90-, 91-180-, and 181-270-minute OTT windows. Patient factors strongly associated with shorter OTT were greater stroke severity (odds ratio [OR] 2.8; 95% confidence interval [CI], 2.5-3.1 per five-point increase), arrival by ambulance (OR 5.9; 95% CI, 4.5-7.3), and arrival during regular hours (OR 4.6; 95% CI, 3.8-5.4). Faster OTT, in 15-minute increments, was associated with reduced in-hospital mortality (OR 0.96; 95% CI, 0.95-0.98; P<.001), reduced symptomatic intracranial hemorrhage (OR 0.96; 95% CI, 0.95-0.98; P<.001), increased achievement of independent ambulation at discharge (OR 1.04; 95% CI, 1.03-1.05; P<.001), and increased discharge to home (OR 1.03; 95% CI, 1.02-1.04; P<.001).
Data collected were dependent on the accuracy and completeness of the chart abstraction, and only short-term outcomes were reported. Although no post-discharge outcomes were reported, previous studies have shown that functional status at discharge strongly correlates with three-month disability outcomes.
Bottom line: In routine clinical practice, earlier tPA for acute ischemic strokes results in better short-term clinical outcomes.
Citation: Saver JL, Fonarow GC, Smith EE, et al. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA. 2013;309:2480-2488.
Current Smokers Have Higher Perioperative Morbidity and Mortality Compared to Past Smokers
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day post-operative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10-1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51-1.81 vs. OR 1.20; CI, 1.09-1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40-1.51 vs. OR, 1.13; CI, 1.08-1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease post-operative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013 Jun 19:1-8. doi: 10.1001/jamasurg.2013.2360 [Epub ahead of print].
Statins Associated with Several Musculoskeletal Conditions
Clinical question: Is statin use associated with musculoskeletal adverse events, including arthropathy and injury, in physically active individuals?
Background: Statin-induced musculoskeletal adverse events (AEs) include myalgias, muscle weakness, cramps, rhabdomyolysis, and tendinous disease. The full spectrum of AEs is unknown because randomized clinical trials have not been powered to detect uncommon AEs.
Study design: Retrospective cohort study with propensity score matching.
Setting: San Antonio military area.
Synopsis: A total of 46,249 patients aged 30 to 85 years who met study criteria were propensity-matched into 6,967 statin users and 6,967 nonusers. The occurrence of musculoskeletal conditions were categorized using ICD-9 codes: Msk1, all musculoskeletal diseases; Msk1a, arthropathies and related diseases; Msk1b, injury-related diseases; and Msk2, drug-associated musculoskeletal pain. Of these, statin users had a higher odds ratio (OR) for Msk1 (OR 1.19; 95% CI, 1.08-1.30), Msk1b (1.13; 1.05-1.21), and Msk2 (1.09; 1.02-1.18). Msk1b (arthropathies) had an OR of 1.07 (0.9-1.16, P=0.07). Simvastatin was used by 73.5% of patients, and years of simvastatin use was not a significant predictor of any of the outcome measures. Secondary and sensitivity analyses showed higher adjusted ORs for statin users in all groups. This study was limited by the use of ICD-9-CM codes for identification of baseline characteristics, and the musculoskeletal diagnosis groups used were not validated.
Bottom line: Statin use is associated with an increased likelihood of musculoskeletal conditions, arthropathies, injuries, and pain.
Citation: Mansi I, Frei CR, Pugh M, Makris U, Mortensen EM. Statins and musculoskeletal conditions, arthropathies, and injuries. JAMA Intern Med. 2013;173:1318-1326.
Evidence-Based Guidelines on Periprocedural Management of Antithrombotic Medications in Patients with History of Stroke
Clinical question: What is the evidence for the periprocedural management of antithrombotics in patients with ischemic cerebrovascular accidents (CVAs)?
Background: Evidence-based guidelines are needed to help clinicians determine the thromboembolic risk of temporary discontinuation of antithrombotic medications, the perioperative bleeding risks of continuing antithrombotic agents, whether bridging therapy should be used, and the appropriate timing of antithrombotic agent discontinuation.
Study design: Systematic literature review with practice recommendations.
Setting: American Academy of Neurology Guideline Development Subcommittee convened an expert panel to review and provide recommendations.
Synopsis: Researchers analyzed 133 literature reviews via MEDLINE and EMBASE. Aspirin in stroke patients:
- Should routinely be continued for dental procedures (Level A);
- Should probably be continued for invasive ocular anesthesia, cataract surgery, dermatologic procedures, transrectal ultrasound-guided prostate biopsy, spinal/epidural procedures, and carpal tunnel surgery (Level B); and
- Should possibly be continued for vitreoretinal surgery, electromyogram (EMG), transbronchial lung biopsy, colonoscopic polypectomy, upper endoscopy and biopsy/sphincterotomy, and abdominal ultrasound-guided biopsies (Level C).
Warfarin in stroke patients:
- Should routinely be continued for dental procedures (Level A); and
- Should possibly continued for dermatologic procedures (Level B) and EMG, prostate procedures, inguinal hemiorrhaphy, and endothermal ablation of great saphenous vein (Level C).
- There is a lack of evidence on warfarin for ophthalmologic procedures, with the exception of ocular anesthesia, where it probably does not increase clinically significant bleeding (Level B).
There was not enough evidence to support or refute a recommendation regarding heparin bridge therapy in reducing thromboembolism in chronically anticoagulated patients (Level B).
Bottom line: These are the most up-to-date guidelines for anticoagulant and antiplatelet agents in patients with transient ischemic attacks and strokes undergoing procedures, but further research is needed in many areas.
Citation: Armstrong MJ, Gronseth G Anderson DC, et al. Summary of evidence-based guideline: periprocedural management of antithrombotic medications in patients with ischemic cerebrovascular disease: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2065-2069.
Extended Prophylaxis with Aspirin Was Noninferior to Extended Prophylaxis with Low-Molecular-Weight Heparin
Clinical question: Is aspirin as effective as low-molecular-weight heparin (LMWH) for the extended prophylaxis of venous thromboembolism (VTE) after total hip arthroplasty (THA)?
Background: Deep vein thrombosis (DVT) and pulmonary embolism (PE) are common complications after THA. After initial prophylaxis, LMWH given for up to 30 days has been shown to reduce VTE compared with placebo. However, LMWH is costly and may increase the risk of minor bleeding. Aspirin is a potentially simple, low-cost alternative.
Study design: Randomized, placebo-controlled trial.
Setting: Twelve university-affiliated orthopedic hospitals in Canada.
Synopsis: Patients undergoing elective THA without hip fracture, metastatic cancer, or bleeding precluding anticoagulants were eligible. All patients received dalteparin for 10 days and were then randomized to aspirin 81 mg daily or to continue dalteparin. The primary outcome was symptomatic proximal DVT or PE during 90 days’ follow-up. The study was terminated early due to slow enrollment. At that time, 2,364 patients had been enrolled, and an analysis by an independent data safety and monitoring board determined that continuing the study was unlikely to alter the main findings. Extended prophylaxis with aspirin was noninferior to LMWH for the primary outcome, which occurred in 0.3% vs. 1.3%, respectively (95% CI, -0.5% to 2.5%, P<.001 for noninferiority). There were no significant differences in major or minor bleeding.
Though the early termination is a concern, the sample size was large and the results do not suggest inadequate power as a reason for lack of superiority for LMWH. Also, all patients received 10 days of LMWH, which indicates a period of LMWH after discharge will still be needed for most patients prior to initiating aspirin.
Bottom line: After initial LMWH prophylaxis for 10 days, extended prophylaxis with aspirin can be considered, particularly for patients for whom LMWH may not be feasible.
Citation: Anderson DR, Dunbar MJ, Bohm ER, et al. Aspirin versus low-molecular-weight heparin for extended venous thromboembolism prophylaxis after total hip arthroplasty: a randomized trial. Ann Intern Med. 2013;158:800-806.
Symptomatic Subsegmental Pulmonary Embolism (PE) Has a Prognosis Similar to Proximal PE
Clinical question: Is the prognosis of a symptomatic subsegmental pulmonary embolism (PE) similar to that of a more proximal PE?
Background: The use of multidetector computed tomography angiography (CTA) has allowed for better assessment of the pulmonary vasculature and increased detection of distal emboli. Prior studies have raised questions on the clinical importance of subsegmental PE but have been limited by small size or retrospective design.
Study design: Combined data from two prospective trials of management of suspected PE.
Setting: Twelve hospitals in the Netherlands and four tertiary-care emergency departments in Canada.
Synopsis: The study cohort consisted of 3,769 patients with suspected PE, of which 2,688 underwent CTA. Of patients diagnosed with PE, 15.5% had isolated subsegmental emboli. All patients were treated with anticoagulation. During three months of follow-up, the incidence of symptomatic recurrence for subsegmental PE was similar to patients with proximal PE (3.6% vs. 2.5%, respectively). The mortality rates for patients with subsegmental and proximal PE were also similar (10.3% vs. 6.3%, respectively).
The study may have been underpowered to detect small differences in event rates; however, there was no trend suggesting that subsegmental PE had better outcomes than more proximal PE. Also, the study did not specifically investigate whether any management strategy is preferred based on thrombus location on CTA.
Bottom line: Clinicians should continue to anticoagulate patients with subsegmental PE as the prognosis is similar to those with proximal PE.
Citation: Den Exter PL, van Es J, Klok FA, et al. Risk profile and clinical outcome of symptomatic subsegmental pulmonary embolism. Blood. 2013;122:1144-1149.
Video-Based Educational Workshop for Academic Hospitalists and House Staff May Improve Professionalism
Clinical question: Can video-based education promote professionalism among academic hospitalists and house staff?
Background: Unprofessional behavior by academic hospitalists and residents can negatively impact the learning environment and patient safety. This behavior increases throughout training, and faculty behavior can be influential. There is a paucity of educational materials to train hospitalists and house staff to recognize and ameliorate unprofessional behaviors.
Study design: Educational survey study.
Setting: University of Chicago, Northwestern University, and NorthShore University Health System teaching hospitals.
Synopsis: Three videos were developed displaying three types of unprofessional behavior: disparaging other physicians, “blocking” admissions, and misrepresenting tests to expedite their completion. There were 44 hospitalists and 244 house staff who received a 60-minute workshop in which they watched the videos using a viewing tool and discussed the videos in small groups.
For all three videos, more than three-quarters of both hospitalists and house staff felt the behavior was unprofessional or somewhat unprofessional. Hospitalists and house staff found the workshop useful and effective (65.9% and 77.1%, respectively) and would change their behavior as a result of the workshop (65.9% and 67.2%, respectively). Those who perceived the videos as “very realistic” were more likely to report intent to change behavior (93% vs. 53%, P=0.01).
This study is limited by its small sample size and possible selection bias. Those interested or concerned about unprofessional behavior may have been more likely to attend the workshop.
Bottom line: Video-based professionalism education is a feasible and well-received way to educate hospitalists and residents about unprofessional behavior and may even affect their future behavior.
Citation: Farnan JM, O’Leary KJ, Didwania A, et al. Promoting professionalism via a video-based educational workshop for academic hospitalists and housestaff. J Hosp Med. 2013;8:386-389.
Friday and Weekend Elective Surgeries Have Increased Mortality
Clinical question: How can the association between mortality and the day of elective surgical procedures be assessed?
Background: Several studies have described the “weekend effect” for both surgical and medical patients, with higher mortality and length of stay in patients admitted on the weekend compared to weekdays. Two potential explanations are poorer quality of care being delivered on the weekend or more severely ill patients being operated on or admitted on the weekend.
Study design: Retrospective analysis of national hospital administrative data.
Setting: All acute-care and specialist hospitals in England from 2008 to 2011.
Synopsis: There were 4,133,346 elective, inpatient surgical procedures studied. Friday surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.44 [95% CI, 1.39-1.50] and 1.42 [95% CI, 1.26-1.60], respectively, when compared with Monday. Weekend surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.82 [95% CI, 1.71-1.94] and 2.67 [95% CI, 2.30-3.09], respectively, when compared with Monday. There were significant trends toward higher mortality at the end of the workweek and weekends for four high-risk procedures: esophagus and/or stomach excision, colon and/or rectum excisions, coronary artery bypass graft, and lung excision. For lower-risk procedures, there was a significant increase in mortality for Friday surgeries but not weekend surgeries. As with all studies using administrative data, inherent selection biases could not be adjusted for Friday or weekend procedures.
Bottom line: Elective surgeries that occur on the weekend and later in the week have an increased risk of mortality, implying that the weekend effect is due to poorer quality of care during weekends, rather than higher-acuity patients presenting on weekends.
Citation: Aylin P, Alexandrescu R, Jen MH, Mayer EK, Bottle A. Day of week of procedure and 30 day mortality for elective surgery: retrospective analysis of hospital episode statistics. BMJ. 2013;346:f2424.
Basal Plus Correction Insulin Regimen Is Effective in Hospitalized Patients with Type 2 Diabetes
Clinical question: Does a basal plus correction insulin regimen (as needed with meals) result in similar glycemic control and lower rates of hypoglycemia compared to a basal-bolus regimen?
Background: Basal bolus is the preferred insulin regimen for non-critically-ill hospitalized patients as per clinical guidelines. But use is limited due to the complexity of the regimen and the fear of inducing hypoglycemia. A less complex, easier-to-implement basal plus correction insulin regimen may be an effective alternative.
Study design: Multicenter, prospective, open-label, randomized study.
Setting: Six hospitals in the U.S.
Synopsis: A group of 375 medical and surgical patients with Type 2 diabetes treated with diet, oral anti-diabetic agents, or low-dose insulin (≤ 0.4 units/kg/day) were randomized to:
- Basal-bolus insulin regimen with glargine once daily and fixed doses of glusiline before meals;
- Basal plus correction insulin (“basal plus”) regimen with glargine once daily and glusiline sliding scale insulin (SSI) before meals; or
- Regular SSI alone.
After the first day of therapy, treatment with basal-bolus and basal-plus regimens resulted in similar improvements in daily blood glucose (BG) (P=0.16), and both were superior to SSI alone (P=0.04). Both regimens also resulted in less treatment failure (defined as mean daily BG of >240 mg/dl or >2 consecutive BG >240 mg/dl) than did treatment with SSI. Hypoglycemia (BG <70 mg/dl) occurred in 16%, 13%, and 3% of patients in the basal-bolus, basal-plus, and SSI groups, respectively (P=0.02). There were no between-group differences in the frequency of severe hypoglycemia (<40 mg/dl; P=0.76).
The study was not powered to evaluate hospital complications (infection, mortality, hospital stay, and readmissions) across groups.
Bottom line: The basal-plus regimen resulted in glycemic control similar to standard basal-bolus regimen and is an effective alternative for the initial management of hyperglycemia in general medical and surgical patients with Type 2 diabetes.
Citation: Umpierrez GE, Smiley D, Hermayer K, et al. Randomized study comparing a basal-bolus with a basal plus correction insulin regimen for the hospital management of medical and surgical patients with type 2 diabetes: Basal plus trial. Diabetes Care. 2013;36:2169-2174.
Capnography Can Help Diagnose Diabetic Ketoacidosis in the ED
Clinical question: Can capnography be used as a screening tool to identify patients with diabetic ketoacidosis (DKA)?
Background: Metabolic acidosis is a major criterion for diagnosing DKA. Previous studies have shown that end-tidal carbon dioxide (ETCO2) measurement by capnography can provide an accurate estimation of arterial carbon dioxide tension (PaCO2) and may be a noninvasive, fast, inexpensive measurement of acidosis in DKA. However, those studies were in pediatric patients and had small sample sizes.
Study design: Cross-sectional, prospective descriptive-analytic study.
Setting: The ED of Imam Reza Medical Research and Training Hospital, Tabriz, East Azarbaijan, Iran.
Synopsis: A total of 181 adult patients older than 18 with suspected DKA and blood sugar >250 mg/dl were included in the study. Simultaneous capnography and arterial blood gas (ABG) were obtained on all patients. Urine ketones, complete blood count, serum levels of potassium, urea, and creatinine were collected. Sixty-two patients were found to have DKA, while 119 had other conditions associated with metabolic acidosis. There was a significant linear relationship between pH and ETCO2 (P>0.0001, relative risk (R)=0.253), PaCO2 and ETCO2 (P>0.0001, R=0.572), and bicarbonate (HCO3) and ETCO2 (P>0.0001, R=0.730). ETCO2 values >24.5 mmHg had a sensitivity and specificity of 0.90 for ruling out DKA. No cutoff point could be determined for ruling in DKA.
The study was open to selection bias as patient collection was only done during the day, so eligible subjects may have been missed. Moreover, though the study suggests that capnography has a role in ruling out DKA, the exact cutoff value is unclear. Other studies found that higher values were needed to exclude diagnosis.
Bottom line: Using ETCO2 values >24.5 mmHg, capnography can help exclude the diagnosis of DKA in adult patients with elevated BG.
Citation: Soleimanour H, Taghizadieh A, Niafar M, Rahmani F, Golzari S, Esfanjani RM. Predictive value of capnography for diagnosis in patients with suspected diabetic ketoacidosis in the emergency department. West J Emerg Med. 2013. doi: 10.5811/westjem.2013.4.14296.
Publicly Reported Mortality Correlates with Overall Mortality
Clinical question: Are publicly reported mortality rates associated with a hospital’s overall medical and surgical mortality rate?
Background: Public reporting of mortality has become an important strategy in Medicare’s quality-improvement initiative. However, the mortality rate for only three conditions, acute myocardial infarction, congestive heart failure, and pneumonia are reported. It is unclear if these rates correlate to a hospital’s overall mortality rate.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Using 2008-2009 data from 2,322 acute-care hospitals with 6.7 million admissions, an aggregate mortality rate for the three publicly reported conditions, a standardized 30-day mortality rate for selected medical and surgical conditions, and an overall average composite mortality score was calculated for each hospital. Based on their mortality for the three publicly reported conditions, hospitals were grouped into quartiles from highest (top-performing hospitals) to lowest mortality (poor-performing hospitals).
Top-performing hospitals had a 3.6% (9.4%vs 13.0%; P<.001) lower mortality rate than poor-performing hospitals and an odds ratio >5 of being a top performer in overall mortality (OR 5.3; 95% CI, 4.3-6.5). They also had an 81% lower chance of being in the worst-performing quartile in overall mortality (OR 0.19; 95% CI, 0.14-0.27). Conversely, poor-performing hospitals had a 4.5 times higher risk of being in the lowest quartile in overall mortality. The study is limited by the use of administrative data, which limits the ability to adjust for severity of illness, overall health, and socioeconomic status of each hospital’s population.
Bottom line: A hospital’s mortality performance on the three publicly reported conditions may predict mortality rates across a wide range of medical and surgical conditions.
Citation: McCrum ML, Joynt KE, Orav EJ, Gawande AA, Jha AK. Mortality for publicly reported conditions and overall hospital mortality rates. JAMA Intern Med. 2013;173:1351-1357.
Cost Savings in Decreasing Preventable Acute-Care Visits Are Limited among High-Cost Medicare Utilizers
Clinical question: What role do preventable acute-care visits play in the overall costs of care for the highest Medicare utilizers?
Background: Some 10% of Medicare patients account for more than half the costs. Interventions targeted at decreasing acute-care costs (ED visits and inpatient hospitalizations) for this high-cost population are widespread, but it is unknown what impact they can have.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Standardized total costs were created for fee-for-service Medicare patients for 2009 and 2010 in order to identify high-cost and persistently high-cost patients. Algorithms were used to identify preventable ED visits and hospitalizations in both the high-cost and non-high-cost cohorts.
Of the more than 1 million patients in the sample Medicare population, as many as 113,341 were high-cost. As much as 73% of acute-care spending was attributable to this cohort. Overall, 10% of acute-care costs were felt to be preventable in the high-cost group, 13.5% in the persistently high-cost group, and 19% in the non-high-cost group for 2010. The most common reasons for preventable acute care in the high-cost cohort were heart failure, bacterial pneumonia, and chronic obstructive pulmonary disease. Catastrophic events (myocardial infarction, stroke, sepsis), cancer, and orthopedic procedures drove overall inpatient costs in the high-cost group.
Preventable costs were higher per capita in areas with higher numbers of primary-care and specialist physicians, but it’s unclear if this was a supply or demand issue. The study also used algorithms that possibly overestimate the amount of preventable acute care.
Bottom line: In the highest Medicare utilizers, cost savings aimed at preventable acute care may be limited and might be better targeted at efficiency during acute-care episodes.
Citation: Joynt KE, Gawande AA, Orav EJ, Jha AK. Contribution of preventable acute care spending to total spending for high-cost Medicare patients. JAMA. 2013;309:2572-2578.
What Are the Indications for a Blood Transfusion?

Case
A 65-year-old man with a history of coronary artery disease (CAD) presents to the ED after a mechanical fall. He was found to have a hip fracture, admitted to orthopedic service, and underwent an uneventful hip repair. His post-operative course was uncomplicated, except for his hemoglobin level of 7.5 g/dL, which had decreased from his pre-operative hemoglobin of 11.2 g/dL. The patient was without cardiac symptoms, was ambulating with assistance, had normal vital signs, and was otherwise having an unremarkable recovery. The orthopedic surgeon, who recently heard that you do not have to transfuse patients unless their hemoglobin is less than 7 g/dL, consulted the hospitalist to help make the decision. What would your recommendation be?
Overview
Blood transfusions are a common medical procedure routinely given in the hospital.1 An estimated 15 million red blood cell (RBC) units are transfused each year in the United States.2 Despite its common use, the clinical indications for transfusion continue to be the subject of considerable debate. Most clinicians would agree that treating a patient with a low hemoglobin level and symptoms of anemia is reasonable.1,3 However, in the absence of overt symptoms, there is debate about when transfusions are appropriate.2,3
Because tissue oxygen delivery is dependent on hemoglobin and cardiac output, past medical practice has supported the use of the “golden 10/30 rule,” by which patients are transfused to a hemoglobin concentration of 10 g/dL or a hematocrit of 30%, regardless of symptoms. The rationale for this approach is based on physiologic evidence that cardiac output increases when hemoglobin falls below 7 g/dl. In patients with cardiac disease, the ability to increase cardiac output is compromised. Therefore, in order to reduce strain on the heart, hemoglobin levels historically have been kept higher than this threshold.
However, several studies have forced us to re-evaluate this old paradigm, including increasing concern for the infectious and noninfectious complications associated with blood transfusions and the need for cost containment (see Table 1).1,2,4 Due to improved blood screening, infectious complications from transfusions have been greatly reduced; noninfectious complications are 1,000 times more likely than infectious ones.
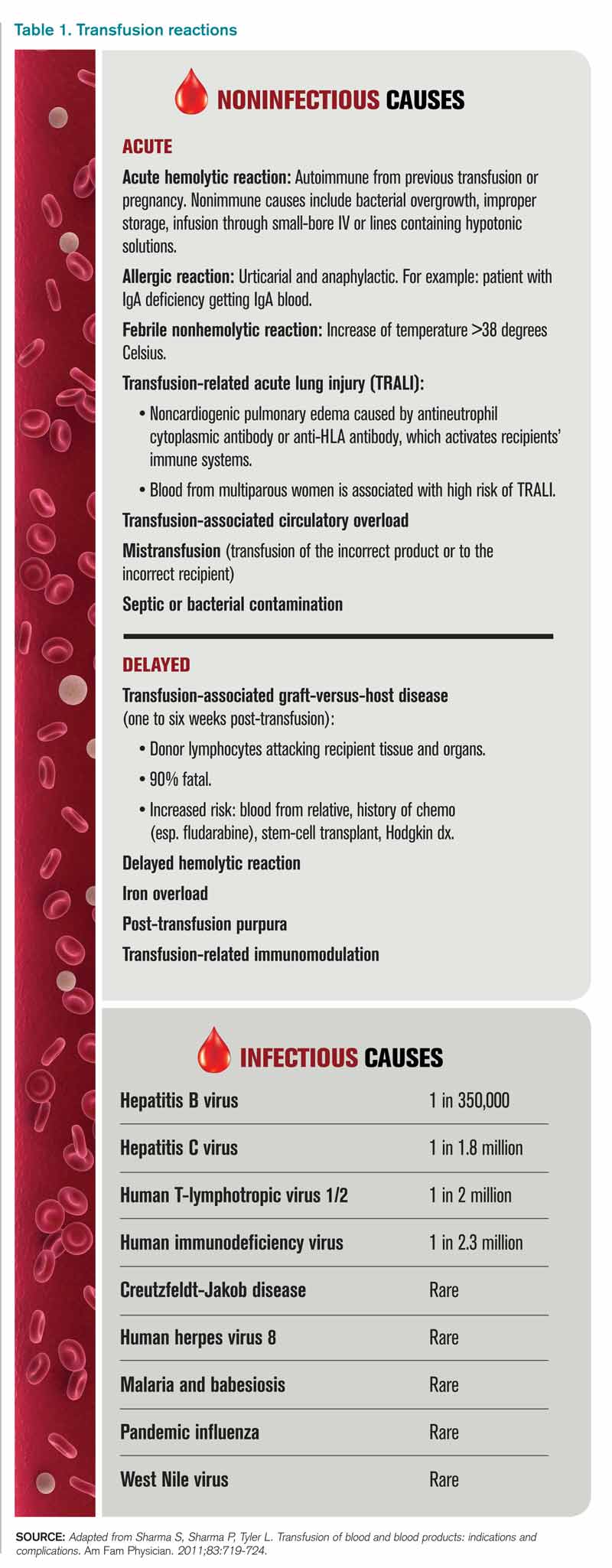
Review of Data
Although a number of studies have been performed on the indications for blood transfusions, many of the trials conducted in the past were too small to substantiate a certain practice. However, three trials with a large number of participants have allowed for a more evidence-based approach to blood transfusions. The studies address different patient populations to help broaden the restrictive transfusion approach to a larger range of patients.
TRICC trial: critically ill patients5. The TRICC trial was the first major study that compared a liberal transfusion strategy (transfuse when Hb <10 g/dL) to a more conservative approach (transfuse when Hb <7 g/dL). In this multicenter, randomized controlled trial, Hébert et al enrolled 418 critically ill patients and found that there was no significant difference in 30-day all-cause mortality between the restrictive-strategy group (18.7%) and the liberal-strategy group (23.3%).
However, in the pre-determined subgroup analysis, patients who were less severely ill (APACHE II scores of <20) had 30-day all-cause mortality of 8.7%, compared with 16.1% in the liberal-strategy group. Interestingly, there were more cardiac complications (pulmonary edema, angina, MI, and cardiac arrest) in the liberal-strategy group (21%) compared with the restrictive-strategy group (13%). Despite this finding, 30-day mortality was not significantly different in patients with clinically significant cardiac disease (primary or secondary diagnosis of cardiac disease [20.5% restrictive versus 22.9% liberal]).
An average of 2.6 units of RBCs per patient were given in the restrictive group, while 5.6 units were given to patients in the liberal group. This reflects a 54% decrease in the number of transfusions used in the conservative group. All the patients in the liberal group received transfusions, while 33% of the restrictive group’s patients received no blood at all.
The results of this trial suggested that there is no clinical advantage in transfusing ICU patients to Hb values above 9 g/dL, even if they have a history of cardiac disease. In fact, it may be harmful to practice a liberal transfusion strategy in critically ill younger patients (<55 years old) and those who are less severely ill (APACHE II <20).5
FOCUS trial: hip surgery and history of cardiac disease6. The FOCUS trial is a recent study that looked at the optimal hemoglobin level at which an RBC transfusion is beneficial for patients undergoing hip surgery. This study enrolled patients aged 50 or older who had a history or risk factors for cardiovascular disease (clinical evidence of cardiovascular disease: h/o ischemic heart disease, EKG evidence of previous MI, h/o CHF/PVD, h/o stroke/TIA, h/o HTN, DM, hyperlipidemia (TC >200/LDL >130), current tobacco use, or Cr>2.0), who were undergoing primary surgical repair of a hip fracture, and who had Hb <10g/dL within three days after surgery.
More than 2,000 patients were assigned randomly to a liberal-strategy group (transfuse to maintain a Hb >10g/dL) or a restrictive strategy group (transfuse to maintain Hg >8g/dl or for symptoms or signs of anemia). These signs/symptoms included chest pain that was possibly cardiac-related, congestive heart failure, tachycardia, and unresponsive hypotension. The primary outcomes were mortality or inability to walk 10 feet without assistance at 60-day follow-up.
The FOCUS trial found no statistically significant difference in mortality rate (7.6% in the liberal group versus 6.6% in the restrictive group) or in the ability to walk at 60 days (35.2% in the liberal group versus 34.7% in the restrictive group). There were no significant differences in the rates of in-hospital acute MI, unstable angina, or death between the two groups.
Patients in the restrictive-strategy group received 65% fewer units of blood than the liberal group, with 59% receiving no blood after surgery compared with 3% of the liberal group. Overall, the liberal group received 1,866 units of blood, compared with 652 units in the restrictive group.
This trial helps support the findings in previous trials, such as TRICC, by showing that a restrictive transfusion strategy using a trigger point of 8 g/dl does not increase mortality or cardiovascular complications and does not decrease functional ability after orthopedic surgery.
TRAC trial: patients after cardiac surgery7. The TRAC trial was a prospective randomized trial in 502 patients undergoing cardiac surgery that assigned 253 patients to the liberal-transfusion-strategy group (Hb >10g/dl) and 249 to the restrictive-strategy group (Hb >8 g/dl). In this study, the primary endpoint of all-cause 30-day mortality occurred in 10% of the liberal group and 11% of the restrictive group. This difference was not significant.
Subanalysis showed that blood transfusion in both groups was an independent risk factor for the occurrence of respiratory, cardiac, renal, and infectious complications, in addition to the composite end point of 30-day mortality—again highlighting the risk involved in of blood transfusions.
These results support the other trial conclusions that a restrictive transfusion strategy of maintaining a hematocrit of 24% (Hb 8 g/dL) is as safe as a more liberal strategy with a hematocrit of 30% (Hb 10 g/dL). It also offers further evidence of the risks of blood transfusions and supports the view that blood transfusions should never be given simply to correct low hemoglobin levels.
Cochrane Review. A recent Cochrane Review that comprised 19 trials with a combined total of 6,264 patients also supported a restrictive-strategy approach.8 In this review, no difference in mortality was established between the restrictive and liberal transfusion groups, with a trend toward decreased hospital mortality in the restrictive-transfusion group. The authors of the study felt that for most patients, blood transfusion is not necessary until hemoglobin levels drop below 7-8 g/dL but emphasized that this criteria should not be generalized to patients with an acute cardiac issue.
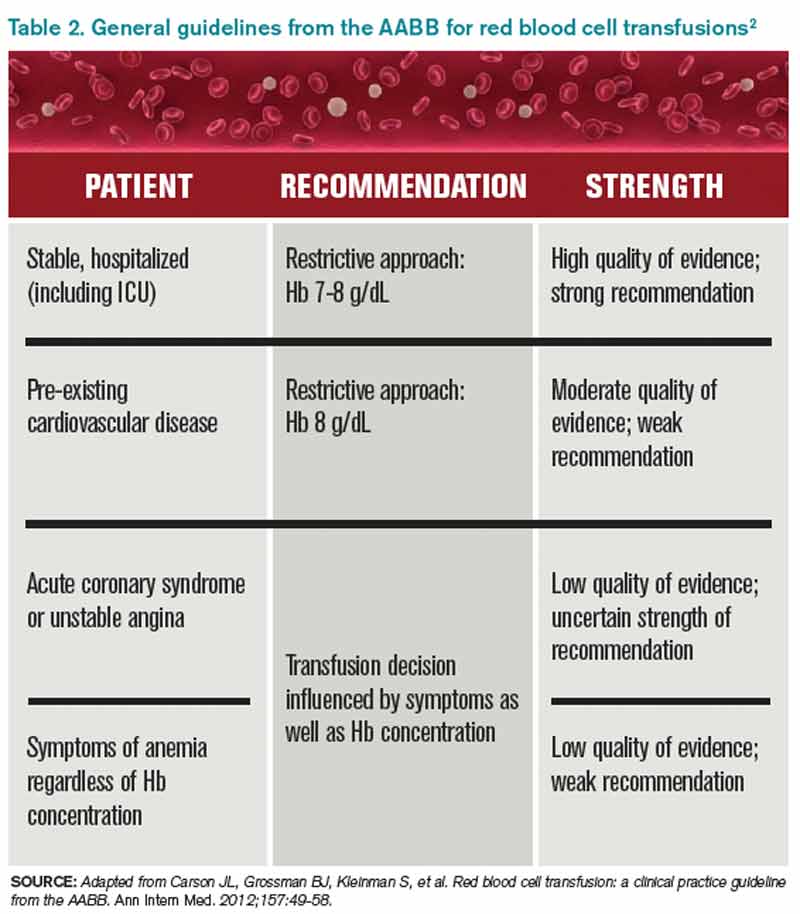
Back to the Case
In this case, the patient is doing well post-operatively and has no cardiac symptoms or hypotension. However, based on the new available data from the FOCUS trial, given the patient’s history of CAD, and the threshold of 8 g/dL used in the study, it was recommended that the patient be transfused.
Bottom Line
Current practice guidelines clearly support clinical judgment as the primary determinant in the decision to transfuse.2 However, current evidence is growing that our threshold for blood transfusions should be a hemoglobin level of 7-8 g/dl.
Dr. Chang is a hospitalist and assistant professor at Mount Sinai Medical Center in New York City, and is co-director of the medicine-geriatrics clerkship at the Icahn School of Medicine at Mount Sinai. Dr. Torgalkar is a hospitalist and assistant professor at Mount Sinai Medical Center.
References
- Sharma S, Sharma P, Tyler L. Transfusion of blood and blood products: indications and complications. Am Fam Physician. 2011;83:719-724.
- Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2012;157:49-58.
- Valeri CR, Crowley JP, Loscalzo J. The red cell transfusion trigger: has a sin of commission now become a sin of omission? Transfusion. 1998;38:602-610.
- Klein HG, Spahn DR, Carson JL. Red blood cell transfusion in clinical practice. Lancet. 2007;370(9585):415-426.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409-17.
- Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365:2453-2462.
- Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial. JAMA. 2010;304:1559-1567.
- Carson JL, Carless PA, Hébert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012; 4:CD002042.
Case
A 65-year-old man with a history of coronary artery disease (CAD) presents to the ED after a mechanical fall. He was found to have a hip fracture, admitted to orthopedic service, and underwent an uneventful hip repair. His post-operative course was uncomplicated, except for his hemoglobin level of 7.5 g/dL, which had decreased from his pre-operative hemoglobin of 11.2 g/dL. The patient was without cardiac symptoms, was ambulating with assistance, had normal vital signs, and was otherwise having an unremarkable recovery. The orthopedic surgeon, who recently heard that you do not have to transfuse patients unless their hemoglobin is less than 7 g/dL, consulted the hospitalist to help make the decision. What would your recommendation be?
Overview
Blood transfusions are a common medical procedure routinely given in the hospital.1 An estimated 15 million red blood cell (RBC) units are transfused each year in the United States.2 Despite its common use, the clinical indications for transfusion continue to be the subject of considerable debate. Most clinicians would agree that treating a patient with a low hemoglobin level and symptoms of anemia is reasonable.1,3 However, in the absence of overt symptoms, there is debate about when transfusions are appropriate.2,3
Because tissue oxygen delivery is dependent on hemoglobin and cardiac output, past medical practice has supported the use of the “golden 10/30 rule,” by which patients are transfused to a hemoglobin concentration of 10 g/dL or a hematocrit of 30%, regardless of symptoms. The rationale for this approach is based on physiologic evidence that cardiac output increases when hemoglobin falls below 7 g/dl. In patients with cardiac disease, the ability to increase cardiac output is compromised. Therefore, in order to reduce strain on the heart, hemoglobin levels historically have been kept higher than this threshold.
However, several studies have forced us to re-evaluate this old paradigm, including increasing concern for the infectious and noninfectious complications associated with blood transfusions and the need for cost containment (see Table 1).1,2,4 Due to improved blood screening, infectious complications from transfusions have been greatly reduced; noninfectious complications are 1,000 times more likely than infectious ones.
Review of Data
Although a number of studies have been performed on the indications for blood transfusions, many of the trials conducted in the past were too small to substantiate a certain practice. However, three trials with a large number of participants have allowed for a more evidence-based approach to blood transfusions. The studies address different patient populations to help broaden the restrictive transfusion approach to a larger range of patients.
TRICC trial: critically ill patients5. The TRICC trial was the first major study that compared a liberal transfusion strategy (transfuse when Hb <10 g/dL) to a more conservative approach (transfuse when Hb <7 g/dL). In this multicenter, randomized controlled trial, Hébert et al enrolled 418 critically ill patients and found that there was no significant difference in 30-day all-cause mortality between the restrictive-strategy group (18.7%) and the liberal-strategy group (23.3%).
However, in the pre-determined subgroup analysis, patients who were less severely ill (APACHE II scores of <20) had 30-day all-cause mortality of 8.7%, compared with 16.1% in the liberal-strategy group. Interestingly, there were more cardiac complications (pulmonary edema, angina, MI, and cardiac arrest) in the liberal-strategy group (21%) compared with the restrictive-strategy group (13%). Despite this finding, 30-day mortality was not significantly different in patients with clinically significant cardiac disease (primary or secondary diagnosis of cardiac disease [20.5% restrictive versus 22.9% liberal]).
An average of 2.6 units of RBCs per patient were given in the restrictive group, while 5.6 units were given to patients in the liberal group. This reflects a 54% decrease in the number of transfusions used in the conservative group. All the patients in the liberal group received transfusions, while 33% of the restrictive group’s patients received no blood at all.
The results of this trial suggested that there is no clinical advantage in transfusing ICU patients to Hb values above 9 g/dL, even if they have a history of cardiac disease. In fact, it may be harmful to practice a liberal transfusion strategy in critically ill younger patients (<55 years old) and those who are less severely ill (APACHE II <20).5
FOCUS trial: hip surgery and history of cardiac disease6. The FOCUS trial is a recent study that looked at the optimal hemoglobin level at which an RBC transfusion is beneficial for patients undergoing hip surgery. This study enrolled patients aged 50 or older who had a history or risk factors for cardiovascular disease (clinical evidence of cardiovascular disease: h/o ischemic heart disease, EKG evidence of previous MI, h/o CHF/PVD, h/o stroke/TIA, h/o HTN, DM, hyperlipidemia (TC >200/LDL >130), current tobacco use, or Cr>2.0), who were undergoing primary surgical repair of a hip fracture, and who had Hb <10g/dL within three days after surgery.
More than 2,000 patients were assigned randomly to a liberal-strategy group (transfuse to maintain a Hb >10g/dL) or a restrictive strategy group (transfuse to maintain Hg >8g/dl or for symptoms or signs of anemia). These signs/symptoms included chest pain that was possibly cardiac-related, congestive heart failure, tachycardia, and unresponsive hypotension. The primary outcomes were mortality or inability to walk 10 feet without assistance at 60-day follow-up.
The FOCUS trial found no statistically significant difference in mortality rate (7.6% in the liberal group versus 6.6% in the restrictive group) or in the ability to walk at 60 days (35.2% in the liberal group versus 34.7% in the restrictive group). There were no significant differences in the rates of in-hospital acute MI, unstable angina, or death between the two groups.
Patients in the restrictive-strategy group received 65% fewer units of blood than the liberal group, with 59% receiving no blood after surgery compared with 3% of the liberal group. Overall, the liberal group received 1,866 units of blood, compared with 652 units in the restrictive group.
This trial helps support the findings in previous trials, such as TRICC, by showing that a restrictive transfusion strategy using a trigger point of 8 g/dl does not increase mortality or cardiovascular complications and does not decrease functional ability after orthopedic surgery.
TRAC trial: patients after cardiac surgery7. The TRAC trial was a prospective randomized trial in 502 patients undergoing cardiac surgery that assigned 253 patients to the liberal-transfusion-strategy group (Hb >10g/dl) and 249 to the restrictive-strategy group (Hb >8 g/dl). In this study, the primary endpoint of all-cause 30-day mortality occurred in 10% of the liberal group and 11% of the restrictive group. This difference was not significant.
Subanalysis showed that blood transfusion in both groups was an independent risk factor for the occurrence of respiratory, cardiac, renal, and infectious complications, in addition to the composite end point of 30-day mortality—again highlighting the risk involved in of blood transfusions.
These results support the other trial conclusions that a restrictive transfusion strategy of maintaining a hematocrit of 24% (Hb 8 g/dL) is as safe as a more liberal strategy with a hematocrit of 30% (Hb 10 g/dL). It also offers further evidence of the risks of blood transfusions and supports the view that blood transfusions should never be given simply to correct low hemoglobin levels.
Cochrane Review. A recent Cochrane Review that comprised 19 trials with a combined total of 6,264 patients also supported a restrictive-strategy approach.8 In this review, no difference in mortality was established between the restrictive and liberal transfusion groups, with a trend toward decreased hospital mortality in the restrictive-transfusion group. The authors of the study felt that for most patients, blood transfusion is not necessary until hemoglobin levels drop below 7-8 g/dL but emphasized that this criteria should not be generalized to patients with an acute cardiac issue.
Back to the Case
In this case, the patient is doing well post-operatively and has no cardiac symptoms or hypotension. However, based on the new available data from the FOCUS trial, given the patient’s history of CAD, and the threshold of 8 g/dL used in the study, it was recommended that the patient be transfused.
Bottom Line
Current practice guidelines clearly support clinical judgment as the primary determinant in the decision to transfuse.2 However, current evidence is growing that our threshold for blood transfusions should be a hemoglobin level of 7-8 g/dl.
Dr. Chang is a hospitalist and assistant professor at Mount Sinai Medical Center in New York City, and is co-director of the medicine-geriatrics clerkship at the Icahn School of Medicine at Mount Sinai. Dr. Torgalkar is a hospitalist and assistant professor at Mount Sinai Medical Center.
References
- Sharma S, Sharma P, Tyler L. Transfusion of blood and blood products: indications and complications. Am Fam Physician. 2011;83:719-724.
- Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2012;157:49-58.
- Valeri CR, Crowley JP, Loscalzo J. The red cell transfusion trigger: has a sin of commission now become a sin of omission? Transfusion. 1998;38:602-610.
- Klein HG, Spahn DR, Carson JL. Red blood cell transfusion in clinical practice. Lancet. 2007;370(9585):415-426.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409-17.
- Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365:2453-2462.
- Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial. JAMA. 2010;304:1559-1567.
- Carson JL, Carless PA, Hébert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012; 4:CD002042.
Case
A 65-year-old man with a history of coronary artery disease (CAD) presents to the ED after a mechanical fall. He was found to have a hip fracture, admitted to orthopedic service, and underwent an uneventful hip repair. His post-operative course was uncomplicated, except for his hemoglobin level of 7.5 g/dL, which had decreased from his pre-operative hemoglobin of 11.2 g/dL. The patient was without cardiac symptoms, was ambulating with assistance, had normal vital signs, and was otherwise having an unremarkable recovery. The orthopedic surgeon, who recently heard that you do not have to transfuse patients unless their hemoglobin is less than 7 g/dL, consulted the hospitalist to help make the decision. What would your recommendation be?
Overview
Blood transfusions are a common medical procedure routinely given in the hospital.1 An estimated 15 million red blood cell (RBC) units are transfused each year in the United States.2 Despite its common use, the clinical indications for transfusion continue to be the subject of considerable debate. Most clinicians would agree that treating a patient with a low hemoglobin level and symptoms of anemia is reasonable.1,3 However, in the absence of overt symptoms, there is debate about when transfusions are appropriate.2,3
Because tissue oxygen delivery is dependent on hemoglobin and cardiac output, past medical practice has supported the use of the “golden 10/30 rule,” by which patients are transfused to a hemoglobin concentration of 10 g/dL or a hematocrit of 30%, regardless of symptoms. The rationale for this approach is based on physiologic evidence that cardiac output increases when hemoglobin falls below 7 g/dl. In patients with cardiac disease, the ability to increase cardiac output is compromised. Therefore, in order to reduce strain on the heart, hemoglobin levels historically have been kept higher than this threshold.
However, several studies have forced us to re-evaluate this old paradigm, including increasing concern for the infectious and noninfectious complications associated with blood transfusions and the need for cost containment (see Table 1).1,2,4 Due to improved blood screening, infectious complications from transfusions have been greatly reduced; noninfectious complications are 1,000 times more likely than infectious ones.
Review of Data
Although a number of studies have been performed on the indications for blood transfusions, many of the trials conducted in the past were too small to substantiate a certain practice. However, three trials with a large number of participants have allowed for a more evidence-based approach to blood transfusions. The studies address different patient populations to help broaden the restrictive transfusion approach to a larger range of patients.
TRICC trial: critically ill patients5. The TRICC trial was the first major study that compared a liberal transfusion strategy (transfuse when Hb <10 g/dL) to a more conservative approach (transfuse when Hb <7 g/dL). In this multicenter, randomized controlled trial, Hébert et al enrolled 418 critically ill patients and found that there was no significant difference in 30-day all-cause mortality between the restrictive-strategy group (18.7%) and the liberal-strategy group (23.3%).
However, in the pre-determined subgroup analysis, patients who were less severely ill (APACHE II scores of <20) had 30-day all-cause mortality of 8.7%, compared with 16.1% in the liberal-strategy group. Interestingly, there were more cardiac complications (pulmonary edema, angina, MI, and cardiac arrest) in the liberal-strategy group (21%) compared with the restrictive-strategy group (13%). Despite this finding, 30-day mortality was not significantly different in patients with clinically significant cardiac disease (primary or secondary diagnosis of cardiac disease [20.5% restrictive versus 22.9% liberal]).
An average of 2.6 units of RBCs per patient were given in the restrictive group, while 5.6 units were given to patients in the liberal group. This reflects a 54% decrease in the number of transfusions used in the conservative group. All the patients in the liberal group received transfusions, while 33% of the restrictive group’s patients received no blood at all.
The results of this trial suggested that there is no clinical advantage in transfusing ICU patients to Hb values above 9 g/dL, even if they have a history of cardiac disease. In fact, it may be harmful to practice a liberal transfusion strategy in critically ill younger patients (<55 years old) and those who are less severely ill (APACHE II <20).5
FOCUS trial: hip surgery and history of cardiac disease6. The FOCUS trial is a recent study that looked at the optimal hemoglobin level at which an RBC transfusion is beneficial for patients undergoing hip surgery. This study enrolled patients aged 50 or older who had a history or risk factors for cardiovascular disease (clinical evidence of cardiovascular disease: h/o ischemic heart disease, EKG evidence of previous MI, h/o CHF/PVD, h/o stroke/TIA, h/o HTN, DM, hyperlipidemia (TC >200/LDL >130), current tobacco use, or Cr>2.0), who were undergoing primary surgical repair of a hip fracture, and who had Hb <10g/dL within three days after surgery.
More than 2,000 patients were assigned randomly to a liberal-strategy group (transfuse to maintain a Hb >10g/dL) or a restrictive strategy group (transfuse to maintain Hg >8g/dl or for symptoms or signs of anemia). These signs/symptoms included chest pain that was possibly cardiac-related, congestive heart failure, tachycardia, and unresponsive hypotension. The primary outcomes were mortality or inability to walk 10 feet without assistance at 60-day follow-up.
The FOCUS trial found no statistically significant difference in mortality rate (7.6% in the liberal group versus 6.6% in the restrictive group) or in the ability to walk at 60 days (35.2% in the liberal group versus 34.7% in the restrictive group). There were no significant differences in the rates of in-hospital acute MI, unstable angina, or death between the two groups.
Patients in the restrictive-strategy group received 65% fewer units of blood than the liberal group, with 59% receiving no blood after surgery compared with 3% of the liberal group. Overall, the liberal group received 1,866 units of blood, compared with 652 units in the restrictive group.
This trial helps support the findings in previous trials, such as TRICC, by showing that a restrictive transfusion strategy using a trigger point of 8 g/dl does not increase mortality or cardiovascular complications and does not decrease functional ability after orthopedic surgery.
TRAC trial: patients after cardiac surgery7. The TRAC trial was a prospective randomized trial in 502 patients undergoing cardiac surgery that assigned 253 patients to the liberal-transfusion-strategy group (Hb >10g/dl) and 249 to the restrictive-strategy group (Hb >8 g/dl). In this study, the primary endpoint of all-cause 30-day mortality occurred in 10% of the liberal group and 11% of the restrictive group. This difference was not significant.
Subanalysis showed that blood transfusion in both groups was an independent risk factor for the occurrence of respiratory, cardiac, renal, and infectious complications, in addition to the composite end point of 30-day mortality—again highlighting the risk involved in of blood transfusions.
These results support the other trial conclusions that a restrictive transfusion strategy of maintaining a hematocrit of 24% (Hb 8 g/dL) is as safe as a more liberal strategy with a hematocrit of 30% (Hb 10 g/dL). It also offers further evidence of the risks of blood transfusions and supports the view that blood transfusions should never be given simply to correct low hemoglobin levels.
Cochrane Review. A recent Cochrane Review that comprised 19 trials with a combined total of 6,264 patients also supported a restrictive-strategy approach.8 In this review, no difference in mortality was established between the restrictive and liberal transfusion groups, with a trend toward decreased hospital mortality in the restrictive-transfusion group. The authors of the study felt that for most patients, blood transfusion is not necessary until hemoglobin levels drop below 7-8 g/dL but emphasized that this criteria should not be generalized to patients with an acute cardiac issue.
Back to the Case
In this case, the patient is doing well post-operatively and has no cardiac symptoms or hypotension. However, based on the new available data from the FOCUS trial, given the patient’s history of CAD, and the threshold of 8 g/dL used in the study, it was recommended that the patient be transfused.
Bottom Line
Current practice guidelines clearly support clinical judgment as the primary determinant in the decision to transfuse.2 However, current evidence is growing that our threshold for blood transfusions should be a hemoglobin level of 7-8 g/dl.
Dr. Chang is a hospitalist and assistant professor at Mount Sinai Medical Center in New York City, and is co-director of the medicine-geriatrics clerkship at the Icahn School of Medicine at Mount Sinai. Dr. Torgalkar is a hospitalist and assistant professor at Mount Sinai Medical Center.
References
- Sharma S, Sharma P, Tyler L. Transfusion of blood and blood products: indications and complications. Am Fam Physician. 2011;83:719-724.
- Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2012;157:49-58.
- Valeri CR, Crowley JP, Loscalzo J. The red cell transfusion trigger: has a sin of commission now become a sin of omission? Transfusion. 1998;38:602-610.
- Klein HG, Spahn DR, Carson JL. Red blood cell transfusion in clinical practice. Lancet. 2007;370(9585):415-426.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409-17.
- Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365:2453-2462.
- Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial. JAMA. 2010;304:1559-1567.
- Carson JL, Carless PA, Hébert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012; 4:CD002042.