User login
Radial Artery Tops Saphenous Vein Graft in CABG
NEW ORLEANS – Long-term data from the Radial Artery Patency Study show that radial arteries, compared with saphenous veins, are associated with reduced rates of functional and complete graft occlusion in patients undergoing coronary artery bypass surgery.
In addition, radial arteries are associated with lower rates of graft disease, lead author Dr. Stephen E. Fremes said during a late-breaking trial session at the annual meeting of the American College of Cardiology.
The issue of which conduit provides the best long-term graft outcomes has been a subject of lengthy debate. Several trials have indicated that radial-artery grafts are no better than saphenous-vein grafts, including a recently published Veterans Affairs (VA) study showing similar 1-year graft patency among 757 patients undergoing first-time, elective coronary artery bypass grafting (JAMA 2011;305:167-74).
One-year data previously published from the Radial Artery Patency Study (RAPS) showed that complete graft occlusion was significantly reduced in radial-artery grafts compared with saphenous-vein grafts (8.2% vs. 13.6%), but that partial graft occlusion was similar (12.3% vs. 14.3%) between the two conduits (N. Engl. J. Med. 2004;351:2302-09).
When Dr. Fremes was asked how to reconcile the results of RAPS with those from the recent VA study, he replied that the VA study was conducted almost exclusively in men (99%), vein grafts performed better than predicted, and there were very high rates of evidence-based medicine. Adherence to evidence-based medicine was good in RAPS, but the trial accrued much earlier, from November 1996 to January 2001. The mean age of the 269 patients in the current analysis was 60 years, and 15% were women.
RAPS enrolled 561 patients with isolated triple-vessel disease and a left ventricular fraction of more than 35% from 12 Canadian centers and one in New Zealand. Randomization was unique in that it was performed within patients and not between patients, explained Dr. Fremes, head of the cardiovascular surgery division at Sunnybrook Health Sciences Centre and research director at the Schulich Heart Centre at Sunnybrook, Toronto. Patients were randomized to receive either a radial artery to the right coronary territory and a saphenous vein to the circumflex territory or a saphenous vein to the right coronary territory and a radial artery to the circumflex territory.
Late angiography was performed on 440 patients at 1 year and on 269 patients at a mean of 7.6 years after surgery. Grafts were considered occluded if they had a TIMI (Thrombolysis in Myocardial Infarction) score of 0-2, and were considered patent with a TIMI score of 3.
At 5 years, the primary end point of functional graft occlusion was significantly decreased in radial-artery grafts at 12%, compared with saphenous-vein grafts at 18.8% (odds ratio, 0.64), Dr. Fremes said. Significantly fewer radial-artery grafts also became completely occluded at 9%, compared with saphenous-vein grafts at 18% (OR 0.50).
Among 164 patients who had completely patent grafts at follow-up, graft stenosis was similar for both conduits for proximal and distal anastomotic lesions. There were fewer graft-body lesions at 6.7% in radial arteries, vs. saphenous veins at 15.2% (OR 0.42). Consequently, radial-artery grafts were significantly less likely to be either stenotic or completely occluded at 22%, compared with saphenous-vein grafts at 34% (OR 0.58), he said.
Target vessel stenosis, an important risk factor for graft occlusion at 1 year, was evaluated in a subgroup analysis. Target vessels with stenosis were classified a priori as those with 70%-89% narrowing and those with at least 90% narrowing. Although graft occlusion was reduced almost 50% for either graft in target vessels with at least 90% narrowing, radial-artery grafts had much lower functional (8.8%) and complete (6.3%) occlusion rates, as did saphenous-vein grafts (14.6% and 14.5%, respectively), in the more severely narrowed vessels.
The incidence of cardiac death beyond 1 year was 5%, of nonfatal myocardial infarction was 1.5%, and of major adverse cardiac events was 15%. Dr. Fremes pointed out that the clinical event findings were descriptive rather than explanatory since each patient received both graft types.
Overall survival in the entire cohort was 96% at 5 years, 91% at 7.5 years, and 78% at 10 years. Event-free survival was 95%, 90%, and 78%, respectively.
During the panel discussion of the study, Dr. James McClurken, professor and vice-chair of surgery at Temple University in Philadelphia, said, "This [study] lends credence to utilizing the radial artery, with obvious caveats that it is important to place it in highly obstructed vessels so there is not competitive flow and to maintain patency for the longest period of time.
"This is not quite as good as internal-mammary artery patency data, but certainly better than vein-graft data."
Fellow discussant Dr. Steven Bolling, a thoracic surgeon at the University of Michigan Medical Center in Ann Arbor, said he expects the data will shift practice and increase utilization of the radial-artery graft.
When asked about this point during a press conference at the meeting, Dr. Fremes said that radial-artery utilization varies by jurisdiction at about 20%, compared with more than 95% for the internal-mammary artery. He noted that the evidence to date on radial-artery grafts has been mixed and comes mainly from observational studies.
"The study we presented is the first multi-institutional, longitudinal, randomized comparison, so this is fairly unique data," he said. "Hopefully, it will be persuasive."
Press briefing moderator Dr. Spencer King III, with St. Joseph’s Heart and Vascular Institute in Atlanta, said RAPS challenges the prevailing attitude that the radial artery is not that much better than vein grafts. RAPS "says maybe it is going to last longer. So I think this is an interesting thing for surgeons to chew on," he noted.
The Canadian Institutes of Health Research funded the study. Dr. Fremes reported no conflicts.
NEW ORLEANS – Long-term data from the Radial Artery Patency Study show that radial arteries, compared with saphenous veins, are associated with reduced rates of functional and complete graft occlusion in patients undergoing coronary artery bypass surgery.
In addition, radial arteries are associated with lower rates of graft disease, lead author Dr. Stephen E. Fremes said during a late-breaking trial session at the annual meeting of the American College of Cardiology.
The issue of which conduit provides the best long-term graft outcomes has been a subject of lengthy debate. Several trials have indicated that radial-artery grafts are no better than saphenous-vein grafts, including a recently published Veterans Affairs (VA) study showing similar 1-year graft patency among 757 patients undergoing first-time, elective coronary artery bypass grafting (JAMA 2011;305:167-74).
One-year data previously published from the Radial Artery Patency Study (RAPS) showed that complete graft occlusion was significantly reduced in radial-artery grafts compared with saphenous-vein grafts (8.2% vs. 13.6%), but that partial graft occlusion was similar (12.3% vs. 14.3%) between the two conduits (N. Engl. J. Med. 2004;351:2302-09).
When Dr. Fremes was asked how to reconcile the results of RAPS with those from the recent VA study, he replied that the VA study was conducted almost exclusively in men (99%), vein grafts performed better than predicted, and there were very high rates of evidence-based medicine. Adherence to evidence-based medicine was good in RAPS, but the trial accrued much earlier, from November 1996 to January 2001. The mean age of the 269 patients in the current analysis was 60 years, and 15% were women.
RAPS enrolled 561 patients with isolated triple-vessel disease and a left ventricular fraction of more than 35% from 12 Canadian centers and one in New Zealand. Randomization was unique in that it was performed within patients and not between patients, explained Dr. Fremes, head of the cardiovascular surgery division at Sunnybrook Health Sciences Centre and research director at the Schulich Heart Centre at Sunnybrook, Toronto. Patients were randomized to receive either a radial artery to the right coronary territory and a saphenous vein to the circumflex territory or a saphenous vein to the right coronary territory and a radial artery to the circumflex territory.
Late angiography was performed on 440 patients at 1 year and on 269 patients at a mean of 7.6 years after surgery. Grafts were considered occluded if they had a TIMI (Thrombolysis in Myocardial Infarction) score of 0-2, and were considered patent with a TIMI score of 3.
At 5 years, the primary end point of functional graft occlusion was significantly decreased in radial-artery grafts at 12%, compared with saphenous-vein grafts at 18.8% (odds ratio, 0.64), Dr. Fremes said. Significantly fewer radial-artery grafts also became completely occluded at 9%, compared with saphenous-vein grafts at 18% (OR 0.50).
Among 164 patients who had completely patent grafts at follow-up, graft stenosis was similar for both conduits for proximal and distal anastomotic lesions. There were fewer graft-body lesions at 6.7% in radial arteries, vs. saphenous veins at 15.2% (OR 0.42). Consequently, radial-artery grafts were significantly less likely to be either stenotic or completely occluded at 22%, compared with saphenous-vein grafts at 34% (OR 0.58), he said.
Target vessel stenosis, an important risk factor for graft occlusion at 1 year, was evaluated in a subgroup analysis. Target vessels with stenosis were classified a priori as those with 70%-89% narrowing and those with at least 90% narrowing. Although graft occlusion was reduced almost 50% for either graft in target vessels with at least 90% narrowing, radial-artery grafts had much lower functional (8.8%) and complete (6.3%) occlusion rates, as did saphenous-vein grafts (14.6% and 14.5%, respectively), in the more severely narrowed vessels.
The incidence of cardiac death beyond 1 year was 5%, of nonfatal myocardial infarction was 1.5%, and of major adverse cardiac events was 15%. Dr. Fremes pointed out that the clinical event findings were descriptive rather than explanatory since each patient received both graft types.
Overall survival in the entire cohort was 96% at 5 years, 91% at 7.5 years, and 78% at 10 years. Event-free survival was 95%, 90%, and 78%, respectively.
During the panel discussion of the study, Dr. James McClurken, professor and vice-chair of surgery at Temple University in Philadelphia, said, "This [study] lends credence to utilizing the radial artery, with obvious caveats that it is important to place it in highly obstructed vessels so there is not competitive flow and to maintain patency for the longest period of time.
"This is not quite as good as internal-mammary artery patency data, but certainly better than vein-graft data."
Fellow discussant Dr. Steven Bolling, a thoracic surgeon at the University of Michigan Medical Center in Ann Arbor, said he expects the data will shift practice and increase utilization of the radial-artery graft.
When asked about this point during a press conference at the meeting, Dr. Fremes said that radial-artery utilization varies by jurisdiction at about 20%, compared with more than 95% for the internal-mammary artery. He noted that the evidence to date on radial-artery grafts has been mixed and comes mainly from observational studies.
"The study we presented is the first multi-institutional, longitudinal, randomized comparison, so this is fairly unique data," he said. "Hopefully, it will be persuasive."
Press briefing moderator Dr. Spencer King III, with St. Joseph’s Heart and Vascular Institute in Atlanta, said RAPS challenges the prevailing attitude that the radial artery is not that much better than vein grafts. RAPS "says maybe it is going to last longer. So I think this is an interesting thing for surgeons to chew on," he noted.
The Canadian Institutes of Health Research funded the study. Dr. Fremes reported no conflicts.
NEW ORLEANS – Long-term data from the Radial Artery Patency Study show that radial arteries, compared with saphenous veins, are associated with reduced rates of functional and complete graft occlusion in patients undergoing coronary artery bypass surgery.
In addition, radial arteries are associated with lower rates of graft disease, lead author Dr. Stephen E. Fremes said during a late-breaking trial session at the annual meeting of the American College of Cardiology.
The issue of which conduit provides the best long-term graft outcomes has been a subject of lengthy debate. Several trials have indicated that radial-artery grafts are no better than saphenous-vein grafts, including a recently published Veterans Affairs (VA) study showing similar 1-year graft patency among 757 patients undergoing first-time, elective coronary artery bypass grafting (JAMA 2011;305:167-74).
One-year data previously published from the Radial Artery Patency Study (RAPS) showed that complete graft occlusion was significantly reduced in radial-artery grafts compared with saphenous-vein grafts (8.2% vs. 13.6%), but that partial graft occlusion was similar (12.3% vs. 14.3%) between the two conduits (N. Engl. J. Med. 2004;351:2302-09).
When Dr. Fremes was asked how to reconcile the results of RAPS with those from the recent VA study, he replied that the VA study was conducted almost exclusively in men (99%), vein grafts performed better than predicted, and there were very high rates of evidence-based medicine. Adherence to evidence-based medicine was good in RAPS, but the trial accrued much earlier, from November 1996 to January 2001. The mean age of the 269 patients in the current analysis was 60 years, and 15% were women.
RAPS enrolled 561 patients with isolated triple-vessel disease and a left ventricular fraction of more than 35% from 12 Canadian centers and one in New Zealand. Randomization was unique in that it was performed within patients and not between patients, explained Dr. Fremes, head of the cardiovascular surgery division at Sunnybrook Health Sciences Centre and research director at the Schulich Heart Centre at Sunnybrook, Toronto. Patients were randomized to receive either a radial artery to the right coronary territory and a saphenous vein to the circumflex territory or a saphenous vein to the right coronary territory and a radial artery to the circumflex territory.
Late angiography was performed on 440 patients at 1 year and on 269 patients at a mean of 7.6 years after surgery. Grafts were considered occluded if they had a TIMI (Thrombolysis in Myocardial Infarction) score of 0-2, and were considered patent with a TIMI score of 3.
At 5 years, the primary end point of functional graft occlusion was significantly decreased in radial-artery grafts at 12%, compared with saphenous-vein grafts at 18.8% (odds ratio, 0.64), Dr. Fremes said. Significantly fewer radial-artery grafts also became completely occluded at 9%, compared with saphenous-vein grafts at 18% (OR 0.50).
Among 164 patients who had completely patent grafts at follow-up, graft stenosis was similar for both conduits for proximal and distal anastomotic lesions. There were fewer graft-body lesions at 6.7% in radial arteries, vs. saphenous veins at 15.2% (OR 0.42). Consequently, radial-artery grafts were significantly less likely to be either stenotic or completely occluded at 22%, compared with saphenous-vein grafts at 34% (OR 0.58), he said.
Target vessel stenosis, an important risk factor for graft occlusion at 1 year, was evaluated in a subgroup analysis. Target vessels with stenosis were classified a priori as those with 70%-89% narrowing and those with at least 90% narrowing. Although graft occlusion was reduced almost 50% for either graft in target vessels with at least 90% narrowing, radial-artery grafts had much lower functional (8.8%) and complete (6.3%) occlusion rates, as did saphenous-vein grafts (14.6% and 14.5%, respectively), in the more severely narrowed vessels.
The incidence of cardiac death beyond 1 year was 5%, of nonfatal myocardial infarction was 1.5%, and of major adverse cardiac events was 15%. Dr. Fremes pointed out that the clinical event findings were descriptive rather than explanatory since each patient received both graft types.
Overall survival in the entire cohort was 96% at 5 years, 91% at 7.5 years, and 78% at 10 years. Event-free survival was 95%, 90%, and 78%, respectively.
During the panel discussion of the study, Dr. James McClurken, professor and vice-chair of surgery at Temple University in Philadelphia, said, "This [study] lends credence to utilizing the radial artery, with obvious caveats that it is important to place it in highly obstructed vessels so there is not competitive flow and to maintain patency for the longest period of time.
"This is not quite as good as internal-mammary artery patency data, but certainly better than vein-graft data."
Fellow discussant Dr. Steven Bolling, a thoracic surgeon at the University of Michigan Medical Center in Ann Arbor, said he expects the data will shift practice and increase utilization of the radial-artery graft.
When asked about this point during a press conference at the meeting, Dr. Fremes said that radial-artery utilization varies by jurisdiction at about 20%, compared with more than 95% for the internal-mammary artery. He noted that the evidence to date on radial-artery grafts has been mixed and comes mainly from observational studies.
"The study we presented is the first multi-institutional, longitudinal, randomized comparison, so this is fairly unique data," he said. "Hopefully, it will be persuasive."
Press briefing moderator Dr. Spencer King III, with St. Joseph’s Heart and Vascular Institute in Atlanta, said RAPS challenges the prevailing attitude that the radial artery is not that much better than vein grafts. RAPS "says maybe it is going to last longer. So I think this is an interesting thing for surgeons to chew on," he noted.
The Canadian Institutes of Health Research funded the study. Dr. Fremes reported no conflicts.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Functional graft occlusion at 5 years was 12% in radial-artery grafts and nearly 19% in saphenous-vein grafts.
Data Source: Multicenter, randomized Radial Artery Patency Study in 269 patients.
Disclosures: The Canadian Institutes of Health Research funded the study. Dr. Fremes reported no conflicts.
Therapeutic Hypothermia Can Treat Cardiac Arrest in Hypertrophic Cardiomyopathy
NEW ORLEANS – Therapeutic hypothermia shows promise as a novel, strikingly effective lifesaving and neuroprotective treatment in patients with hypertrophic cardiomyopathy who experience out-of-hospital cardiac arrest.
In a prospective series of seven consecutive relatively young adult patients with cardiac arrest and hypertrophic cardiomyopathy (HCM) who underwent rapid cooling to a core body temperature of 31.8 -33° F for 24-29 hours followed by gradual rewarming, all seven left the hospital with preserved cognitive, neurologic, and cardiac function. All received implantable cardioverter-defibrillators for secondary prevention and remained asymptomatic 10-56 months post arrest, Dr. Bradley A. Maron said at the annual meeting of the American College of Cardiology.

This experience stands in marked contrast to the outcomes typically seen when cardiac arrest occurs in patients with HCM. In the absence of therapeutic hypothermia, HCM patients are known to have dismal outcomes despite swift cardiopulmonary resuscitation and external defibrillation, noted Dr. Maron of Brigham and Women's Hospital, Boston.
Therapeutic hypothermia is gaining traction as a neuroprotective treatment strategy for out-of-hospital cardiac arrest in unconscious patients, especially those with ischemic heart disease, stroke, or near drowning. But there are no prior reports of it being used in patients with HCM.
Dr. Maron said he got the idea for studying therapeutic hypothermia in patients with HCM and other genetic heart diseases after he noticed that when the therapy is applied in patients with ischemic heart disease and impaired left ventricular function, their LV function tends to worsen because of the increased afterload caused by cold-induced peripheral vasoconstriction.
"I thought, ‘In hypertrophic cardiomyopathy LV function is generally preserved, cardiac index is generally maintained, so maybe this is a population worth looking at to see if they tend to do better with therapeutic hypothermia than other patients [do],’ " he recalled in an interview.
The seven patients, six men and one woman, averaged 47 years of age with a marked mean maximum LV thickness of 23 mm. Four of the seven had LV outflow obstruction of 45-70 mm Hg at rest. Six patients received cardiopulmonary resuscitation within 3 minutes of their cardiac arrest and the other within 6 minutes. The mean time to spontaneous circulation was 19 minutes, with an average of 162 minutes from collapse to initiation of hypothermia. One patient didn’t start therapeutic hypothermia until more than 4 hours had gone by. Each patient was unconscious without meaningful responses at the initiation of therapy. The initial Glasgow Coma Scale score was 3 in all cases.
Prior to their cardiac arrest, none of these patients had risk factors warranting placement of an implantable cardioverter-defibrillator. However, follow-up genetic testing showed that two patients had double sarcomere mutations in the MyBPC3 and TNN13 genes, potentially explaining their high risk for sudden death.
The mean LV ejection fraction was 61% prior to the cardiac arrest and 63% at discharge.
Noting that HCM is the most frequent cause of sudden death in the young, Dr. Maron observed that "since a lot of these deaths are on-field in the athletic arena, we may want to consider the possibility of joining on-field access to an automatic external defibrillator to some form of cooling therapy that can be applied immediately when an athlete goes down."
He said he had no relevant financial disclosures.
NEW ORLEANS – Therapeutic hypothermia shows promise as a novel, strikingly effective lifesaving and neuroprotective treatment in patients with hypertrophic cardiomyopathy who experience out-of-hospital cardiac arrest.
In a prospective series of seven consecutive relatively young adult patients with cardiac arrest and hypertrophic cardiomyopathy (HCM) who underwent rapid cooling to a core body temperature of 31.8 -33° F for 24-29 hours followed by gradual rewarming, all seven left the hospital with preserved cognitive, neurologic, and cardiac function. All received implantable cardioverter-defibrillators for secondary prevention and remained asymptomatic 10-56 months post arrest, Dr. Bradley A. Maron said at the annual meeting of the American College of Cardiology.
This experience stands in marked contrast to the outcomes typically seen when cardiac arrest occurs in patients with HCM. In the absence of therapeutic hypothermia, HCM patients are known to have dismal outcomes despite swift cardiopulmonary resuscitation and external defibrillation, noted Dr. Maron of Brigham and Women's Hospital, Boston.
Therapeutic hypothermia is gaining traction as a neuroprotective treatment strategy for out-of-hospital cardiac arrest in unconscious patients, especially those with ischemic heart disease, stroke, or near drowning. But there are no prior reports of it being used in patients with HCM.
Dr. Maron said he got the idea for studying therapeutic hypothermia in patients with HCM and other genetic heart diseases after he noticed that when the therapy is applied in patients with ischemic heart disease and impaired left ventricular function, their LV function tends to worsen because of the increased afterload caused by cold-induced peripheral vasoconstriction.
"I thought, ‘In hypertrophic cardiomyopathy LV function is generally preserved, cardiac index is generally maintained, so maybe this is a population worth looking at to see if they tend to do better with therapeutic hypothermia than other patients [do],’ " he recalled in an interview.
The seven patients, six men and one woman, averaged 47 years of age with a marked mean maximum LV thickness of 23 mm. Four of the seven had LV outflow obstruction of 45-70 mm Hg at rest. Six patients received cardiopulmonary resuscitation within 3 minutes of their cardiac arrest and the other within 6 minutes. The mean time to spontaneous circulation was 19 minutes, with an average of 162 minutes from collapse to initiation of hypothermia. One patient didn’t start therapeutic hypothermia until more than 4 hours had gone by. Each patient was unconscious without meaningful responses at the initiation of therapy. The initial Glasgow Coma Scale score was 3 in all cases.
Prior to their cardiac arrest, none of these patients had risk factors warranting placement of an implantable cardioverter-defibrillator. However, follow-up genetic testing showed that two patients had double sarcomere mutations in the MyBPC3 and TNN13 genes, potentially explaining their high risk for sudden death.
The mean LV ejection fraction was 61% prior to the cardiac arrest and 63% at discharge.
Noting that HCM is the most frequent cause of sudden death in the young, Dr. Maron observed that "since a lot of these deaths are on-field in the athletic arena, we may want to consider the possibility of joining on-field access to an automatic external defibrillator to some form of cooling therapy that can be applied immediately when an athlete goes down."
He said he had no relevant financial disclosures.
NEW ORLEANS – Therapeutic hypothermia shows promise as a novel, strikingly effective lifesaving and neuroprotective treatment in patients with hypertrophic cardiomyopathy who experience out-of-hospital cardiac arrest.
In a prospective series of seven consecutive relatively young adult patients with cardiac arrest and hypertrophic cardiomyopathy (HCM) who underwent rapid cooling to a core body temperature of 31.8 -33° F for 24-29 hours followed by gradual rewarming, all seven left the hospital with preserved cognitive, neurologic, and cardiac function. All received implantable cardioverter-defibrillators for secondary prevention and remained asymptomatic 10-56 months post arrest, Dr. Bradley A. Maron said at the annual meeting of the American College of Cardiology.
This experience stands in marked contrast to the outcomes typically seen when cardiac arrest occurs in patients with HCM. In the absence of therapeutic hypothermia, HCM patients are known to have dismal outcomes despite swift cardiopulmonary resuscitation and external defibrillation, noted Dr. Maron of Brigham and Women's Hospital, Boston.
Therapeutic hypothermia is gaining traction as a neuroprotective treatment strategy for out-of-hospital cardiac arrest in unconscious patients, especially those with ischemic heart disease, stroke, or near drowning. But there are no prior reports of it being used in patients with HCM.
Dr. Maron said he got the idea for studying therapeutic hypothermia in patients with HCM and other genetic heart diseases after he noticed that when the therapy is applied in patients with ischemic heart disease and impaired left ventricular function, their LV function tends to worsen because of the increased afterload caused by cold-induced peripheral vasoconstriction.
"I thought, ‘In hypertrophic cardiomyopathy LV function is generally preserved, cardiac index is generally maintained, so maybe this is a population worth looking at to see if they tend to do better with therapeutic hypothermia than other patients [do],’ " he recalled in an interview.
The seven patients, six men and one woman, averaged 47 years of age with a marked mean maximum LV thickness of 23 mm. Four of the seven had LV outflow obstruction of 45-70 mm Hg at rest. Six patients received cardiopulmonary resuscitation within 3 minutes of their cardiac arrest and the other within 6 minutes. The mean time to spontaneous circulation was 19 minutes, with an average of 162 minutes from collapse to initiation of hypothermia. One patient didn’t start therapeutic hypothermia until more than 4 hours had gone by. Each patient was unconscious without meaningful responses at the initiation of therapy. The initial Glasgow Coma Scale score was 3 in all cases.
Prior to their cardiac arrest, none of these patients had risk factors warranting placement of an implantable cardioverter-defibrillator. However, follow-up genetic testing showed that two patients had double sarcomere mutations in the MyBPC3 and TNN13 genes, potentially explaining their high risk for sudden death.
The mean LV ejection fraction was 61% prior to the cardiac arrest and 63% at discharge.
Noting that HCM is the most frequent cause of sudden death in the young, Dr. Maron observed that "since a lot of these deaths are on-field in the athletic arena, we may want to consider the possibility of joining on-field access to an automatic external defibrillator to some form of cooling therapy that can be applied immediately when an athlete goes down."
He said he had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Therapeutic Hypothermia Can Treat Cardiac Arrest in Hypertrophic Cardiomyopathy
NEW ORLEANS – Therapeutic hypothermia shows promise as a novel, strikingly effective lifesaving and neuroprotective treatment in patients with hypertrophic cardiomyopathy who experience out-of-hospital cardiac arrest.
In a prospective series of seven consecutive relatively young adult patients with cardiac arrest and hypertrophic cardiomyopathy (HCM) who underwent rapid cooling to a core body temperature of 31.8 -33° F for 24-29 hours followed by gradual rewarming, all seven left the hospital with preserved cognitive, neurologic, and cardiac function. All received implantable cardioverter-defibrillators for secondary prevention and remained asymptomatic 10-56 months post arrest, Dr. Bradley A. Maron said at the annual meeting of the American College of Cardiology.
This experience stands in marked contrast to the outcomes typically seen when cardiac arrest occurs in patients with HCM. In the absence of therapeutic hypothermia, HCM patients are known to have dismal outcomes despite swift cardiopulmonary resuscitation and external defibrillation, noted Dr. Maron of Brigham and Women's Hospital, Boston.
Therapeutic hypothermia is gaining traction as a neuroprotective treatment strategy for out-of-hospital cardiac arrest in unconscious patients, especially those with ischemic heart disease, stroke, or near drowning. But there are no prior reports of it being used in patients with HCM.
Dr. Maron said he got the idea for studying therapeutic hypothermia in patients with HCM and other genetic heart diseases after he noticed that when the therapy is applied in patients with ischemic heart disease and impaired left ventricular function, their LV function tends to worsen because of the increased afterload caused by cold-induced peripheral vasoconstriction.
"I thought, ‘In hypertrophic cardiomyopathy LV function is generally preserved, cardiac index is generally maintained, so maybe this is a population worth looking at to see if they tend to do better with therapeutic hypothermia than other patients [do],’ " he recalled in an interview.
The seven patients, six men and one woman, averaged 47 years of age with a marked mean maximum LV thickness of 23 mm. Four of the seven had LV outflow obstruction of 45-70 mm Hg at rest. Six patients received cardiopulmonary resuscitation within 3 minutes of their cardiac arrest and the other within 6 minutes. The mean time to spontaneous circulation was 19 minutes, with an average of 162 minutes from collapse to initiation of hypothermia. One patient didn’t start therapeutic hypothermia until more than 4 hours had gone by. Each patient was unconscious without meaningful responses at the initiation of therapy. The initial Glasgow Coma Scale score was 3 in all cases.
Prior to their cardiac arrest, none of these patients had risk factors warranting placement of an implantable cardioverter-defibrillator. However, follow-up genetic testing showed that two patients had double sarcomere mutations in the MyBPC3 and TNN13 genes, potentially explaining their high risk for sudden death.
The mean LV ejection fraction was 61% prior to the cardiac arrest and 63% at discharge.
Noting that HCM is the most frequent cause of sudden death in the young, Dr. Maron observed that "since a lot of these deaths are on-field in the athletic arena, we may want to consider the possibility of joining on-field access to an automatic external defibrillator to some form of cooling therapy that can be applied immediately when an athlete goes down."
He said he had no relevant financial disclosures.
NEW ORLEANS – Therapeutic hypothermia shows promise as a novel, strikingly effective lifesaving and neuroprotective treatment in patients with hypertrophic cardiomyopathy who experience out-of-hospital cardiac arrest.
In a prospective series of seven consecutive relatively young adult patients with cardiac arrest and hypertrophic cardiomyopathy (HCM) who underwent rapid cooling to a core body temperature of 31.8 -33° F for 24-29 hours followed by gradual rewarming, all seven left the hospital with preserved cognitive, neurologic, and cardiac function. All received implantable cardioverter-defibrillators for secondary prevention and remained asymptomatic 10-56 months post arrest, Dr. Bradley A. Maron said at the annual meeting of the American College of Cardiology.
This experience stands in marked contrast to the outcomes typically seen when cardiac arrest occurs in patients with HCM. In the absence of therapeutic hypothermia, HCM patients are known to have dismal outcomes despite swift cardiopulmonary resuscitation and external defibrillation, noted Dr. Maron of Brigham and Women's Hospital, Boston.
Therapeutic hypothermia is gaining traction as a neuroprotective treatment strategy for out-of-hospital cardiac arrest in unconscious patients, especially those with ischemic heart disease, stroke, or near drowning. But there are no prior reports of it being used in patients with HCM.
Dr. Maron said he got the idea for studying therapeutic hypothermia in patients with HCM and other genetic heart diseases after he noticed that when the therapy is applied in patients with ischemic heart disease and impaired left ventricular function, their LV function tends to worsen because of the increased afterload caused by cold-induced peripheral vasoconstriction.
"I thought, ‘In hypertrophic cardiomyopathy LV function is generally preserved, cardiac index is generally maintained, so maybe this is a population worth looking at to see if they tend to do better with therapeutic hypothermia than other patients [do],’ " he recalled in an interview.
The seven patients, six men and one woman, averaged 47 years of age with a marked mean maximum LV thickness of 23 mm. Four of the seven had LV outflow obstruction of 45-70 mm Hg at rest. Six patients received cardiopulmonary resuscitation within 3 minutes of their cardiac arrest and the other within 6 minutes. The mean time to spontaneous circulation was 19 minutes, with an average of 162 minutes from collapse to initiation of hypothermia. One patient didn’t start therapeutic hypothermia until more than 4 hours had gone by. Each patient was unconscious without meaningful responses at the initiation of therapy. The initial Glasgow Coma Scale score was 3 in all cases.
Prior to their cardiac arrest, none of these patients had risk factors warranting placement of an implantable cardioverter-defibrillator. However, follow-up genetic testing showed that two patients had double sarcomere mutations in the MyBPC3 and TNN13 genes, potentially explaining their high risk for sudden death.
The mean LV ejection fraction was 61% prior to the cardiac arrest and 63% at discharge.
Noting that HCM is the most frequent cause of sudden death in the young, Dr. Maron observed that "since a lot of these deaths are on-field in the athletic arena, we may want to consider the possibility of joining on-field access to an automatic external defibrillator to some form of cooling therapy that can be applied immediately when an athlete goes down."
He said he had no relevant financial disclosures.
NEW ORLEANS – Therapeutic hypothermia shows promise as a novel, strikingly effective lifesaving and neuroprotective treatment in patients with hypertrophic cardiomyopathy who experience out-of-hospital cardiac arrest.
In a prospective series of seven consecutive relatively young adult patients with cardiac arrest and hypertrophic cardiomyopathy (HCM) who underwent rapid cooling to a core body temperature of 31.8 -33° F for 24-29 hours followed by gradual rewarming, all seven left the hospital with preserved cognitive, neurologic, and cardiac function. All received implantable cardioverter-defibrillators for secondary prevention and remained asymptomatic 10-56 months post arrest, Dr. Bradley A. Maron said at the annual meeting of the American College of Cardiology.
This experience stands in marked contrast to the outcomes typically seen when cardiac arrest occurs in patients with HCM. In the absence of therapeutic hypothermia, HCM patients are known to have dismal outcomes despite swift cardiopulmonary resuscitation and external defibrillation, noted Dr. Maron of Brigham and Women's Hospital, Boston.
Therapeutic hypothermia is gaining traction as a neuroprotective treatment strategy for out-of-hospital cardiac arrest in unconscious patients, especially those with ischemic heart disease, stroke, or near drowning. But there are no prior reports of it being used in patients with HCM.
Dr. Maron said he got the idea for studying therapeutic hypothermia in patients with HCM and other genetic heart diseases after he noticed that when the therapy is applied in patients with ischemic heart disease and impaired left ventricular function, their LV function tends to worsen because of the increased afterload caused by cold-induced peripheral vasoconstriction.
"I thought, ‘In hypertrophic cardiomyopathy LV function is generally preserved, cardiac index is generally maintained, so maybe this is a population worth looking at to see if they tend to do better with therapeutic hypothermia than other patients [do],’ " he recalled in an interview.
The seven patients, six men and one woman, averaged 47 years of age with a marked mean maximum LV thickness of 23 mm. Four of the seven had LV outflow obstruction of 45-70 mm Hg at rest. Six patients received cardiopulmonary resuscitation within 3 minutes of their cardiac arrest and the other within 6 minutes. The mean time to spontaneous circulation was 19 minutes, with an average of 162 minutes from collapse to initiation of hypothermia. One patient didn’t start therapeutic hypothermia until more than 4 hours had gone by. Each patient was unconscious without meaningful responses at the initiation of therapy. The initial Glasgow Coma Scale score was 3 in all cases.
Prior to their cardiac arrest, none of these patients had risk factors warranting placement of an implantable cardioverter-defibrillator. However, follow-up genetic testing showed that two patients had double sarcomere mutations in the MyBPC3 and TNN13 genes, potentially explaining their high risk for sudden death.
The mean LV ejection fraction was 61% prior to the cardiac arrest and 63% at discharge.
Noting that HCM is the most frequent cause of sudden death in the young, Dr. Maron observed that "since a lot of these deaths are on-field in the athletic arena, we may want to consider the possibility of joining on-field access to an automatic external defibrillator to some form of cooling therapy that can be applied immediately when an athlete goes down."
He said he had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Factors Predict Successful Weaning From VAD
NEW ORLEANS – Patients with chronic cardiomyopathy can be successfully weaned from ventricular assist devices, and certain parameters can predict long-term cardiac stability after explantation, according to German investigators.
"Unloading-promoted reversal of heart failure allows for long-term transplant-free outcomes after patients are removed from VADs. However, few patients with chronic cardiomyopathy have been weaned from VADs, and the majority only recently," said principal investigator Dr. Michael Dandel of the German Heart Institute Berlin. "The long-term outcomes of patients, therefore, and the reliability of criteria for making weaning decisions, are not well known."
At his clinic, 91 patients with chronic cardiomyopathy (CCM) as the underlying cause of heart failure were weaned from VADs between 1995 and 2010, including 75 weaned from left ventricular assist devices, 13 weaned from biventricular assist devices, and 3 weaned from right ventricular assist devices. Before VAD implantation, the patients had left ventricular ejection fraction (LVEF) values of 10%-20%.
These patients were evaluated as to the feasibility of weaning and to establish criteria that could predict long-term cardiac stability after VAD removal. "With this information, we can improve future weaning decisions and postweaning patient management," Dr. Dandel said at the annual meeting of the American College of Cardiology.
A total of 47 patients were evaluated. Of these 41 (87.2%) had idiopathic cardiomyopathy, 4 (8.5%) had histologic evidence of chronic myocarditis before VAD implantation, and 2 (4.3%) had chronic ischemic cardiomyopathy with severe left ventricular dilation.
Before VAD insertion, all patients had irreversible end-stage heart failure and required continuous positive inotropic support. No attempts were made to use VADs electively with the aim of myocardial recovery only, he said.
Postweaning results. Cardiac stability lasting at least 15 years was achieved by 2 patients, while 10 patients have been stable at least 10 years and 3 at least 5 years, he reported.
"At 5 years, only five patients, 10.6%, had died due to heart failure recurrence or weaning-related complications. Several patients died of other causes," he said.
Postweaning freedom from heart failure recurrence for all evaluated patients was 74% at 3 years and 66% at 5 years, but these results included nine patients at very high risk for poor outcomes. After 2002, when the investigators tightened their criteria for weaning, freedom from heart failure recurrence reached 100% at 3 years, he noted.
Pre-explantation variables predictive of outcomes. "Echo data obtained during ‘off pump’ trials proved to be reliable for detection of recovery during mechanical unloading," Dr. Dandel said. "In particular, off-pump [left ventricle] size, geometry, and ejection fraction were predictive of outcome after weaning, especially when history of heart failure was also considered."
For cardiac stability lasting at least 5 years, pre-explantation "off pump" LVEF of 50% or more was associated with a positive predictive value of 91.7%, while LVEF of 45% or more had a positive predictive value of 79.1%.
The positive predictive value of LVEF of 45% or more was approximately 90% if additional parameters were considered: pre-explantation left ventricle size and geometry, stability of unloading-induced cardiac improvement before VAD removal, and heart failure duration before VAD implantation.
Time to cardiac recovery seemed important, Dr. Dandel said. "Patients who had recurrences needed more time to show an improvement. They needed twice the duration of VAD support as patients who did not have a recurrence," he said.
"Definite cutoff values for certain parameters – including tissue Doppler-derived LV wall motion velocity – allowed us to formulate weaning criteria with high predictability for postweaning stability," he said.
Risk factors for heart failure recurrence. Dr. Dandel and his colleagues also identified several risk factors that predicted heart failure recurrence during the first 3 years after VAD removal. These factors, and their associated probability for recurrence, were:
• Preweaning off-pump LVEF less than 45% plus history of heart failure longer than 5 years (100%).
• Preweaning LVEF less than 45% (88.9%).
• Preweaning off-pump LVEF less than 50% plus left ventricular internal diastolic diameter greater than 55 mm (90%).
• Pre-explantation LVEF less than 50% and preexisting alteration of greater than 10% best value (87.5%).
• LVEF less than 50% plus relative wall thickness decrease of less than 10% during final off-pump trial (83.3%).
Of these, he emphasized the importance of the final off-pump trial values. "An off-pump ejection fraction less than 45% in patients with a history of heart failure for more than 5 years is an absolute contraindication for VAD removal," he noted. "All such patients in our study had a recurrence of heart failure."
Early instability of ejection fraction and unstable geometry also confer a high probability of recurrence. "A wall thickness increase by more than 10% means the reverse in modeling is not stable enough," he added.
"The notion that we can actually wean patients from VADs is still a fairly new concept, and the European experience is larger than that of the United States. This is still a field that is wide open for determining patient selection and predictors of outcome after VAD removal," session moderator Dr. Gregory A. Ewald, medical director of heart transplantation at Barnes-Jewish Hospital, St. Louis, said in an interview.
"Clearly, the echocardiographic appearance of the heart on and off support is a good predictor," Dr. Ewald said, but he noted that nonechocardiographic factors such as exercise tolerance were not studied. He also noted that the field has moved to continuous-flow pumps rather than pulsatile pumps, which constituted much of the German experience. It remains to be determined if the same parameters are completely applicable to the newer-generation devices.
Dr. Dandel and Dr. Ewald reported having no relevant conflicts of interest.
NEW ORLEANS – Patients with chronic cardiomyopathy can be successfully weaned from ventricular assist devices, and certain parameters can predict long-term cardiac stability after explantation, according to German investigators.
"Unloading-promoted reversal of heart failure allows for long-term transplant-free outcomes after patients are removed from VADs. However, few patients with chronic cardiomyopathy have been weaned from VADs, and the majority only recently," said principal investigator Dr. Michael Dandel of the German Heart Institute Berlin. "The long-term outcomes of patients, therefore, and the reliability of criteria for making weaning decisions, are not well known."
At his clinic, 91 patients with chronic cardiomyopathy (CCM) as the underlying cause of heart failure were weaned from VADs between 1995 and 2010, including 75 weaned from left ventricular assist devices, 13 weaned from biventricular assist devices, and 3 weaned from right ventricular assist devices. Before VAD implantation, the patients had left ventricular ejection fraction (LVEF) values of 10%-20%.
These patients were evaluated as to the feasibility of weaning and to establish criteria that could predict long-term cardiac stability after VAD removal. "With this information, we can improve future weaning decisions and postweaning patient management," Dr. Dandel said at the annual meeting of the American College of Cardiology.
A total of 47 patients were evaluated. Of these 41 (87.2%) had idiopathic cardiomyopathy, 4 (8.5%) had histologic evidence of chronic myocarditis before VAD implantation, and 2 (4.3%) had chronic ischemic cardiomyopathy with severe left ventricular dilation.
Before VAD insertion, all patients had irreversible end-stage heart failure and required continuous positive inotropic support. No attempts were made to use VADs electively with the aim of myocardial recovery only, he said.
Postweaning results. Cardiac stability lasting at least 15 years was achieved by 2 patients, while 10 patients have been stable at least 10 years and 3 at least 5 years, he reported.
"At 5 years, only five patients, 10.6%, had died due to heart failure recurrence or weaning-related complications. Several patients died of other causes," he said.
Postweaning freedom from heart failure recurrence for all evaluated patients was 74% at 3 years and 66% at 5 years, but these results included nine patients at very high risk for poor outcomes. After 2002, when the investigators tightened their criteria for weaning, freedom from heart failure recurrence reached 100% at 3 years, he noted.
Pre-explantation variables predictive of outcomes. "Echo data obtained during ‘off pump’ trials proved to be reliable for detection of recovery during mechanical unloading," Dr. Dandel said. "In particular, off-pump [left ventricle] size, geometry, and ejection fraction were predictive of outcome after weaning, especially when history of heart failure was also considered."
For cardiac stability lasting at least 5 years, pre-explantation "off pump" LVEF of 50% or more was associated with a positive predictive value of 91.7%, while LVEF of 45% or more had a positive predictive value of 79.1%.
The positive predictive value of LVEF of 45% or more was approximately 90% if additional parameters were considered: pre-explantation left ventricle size and geometry, stability of unloading-induced cardiac improvement before VAD removal, and heart failure duration before VAD implantation.
Time to cardiac recovery seemed important, Dr. Dandel said. "Patients who had recurrences needed more time to show an improvement. They needed twice the duration of VAD support as patients who did not have a recurrence," he said.
"Definite cutoff values for certain parameters – including tissue Doppler-derived LV wall motion velocity – allowed us to formulate weaning criteria with high predictability for postweaning stability," he said.
Risk factors for heart failure recurrence. Dr. Dandel and his colleagues also identified several risk factors that predicted heart failure recurrence during the first 3 years after VAD removal. These factors, and their associated probability for recurrence, were:
• Preweaning off-pump LVEF less than 45% plus history of heart failure longer than 5 years (100%).
• Preweaning LVEF less than 45% (88.9%).
• Preweaning off-pump LVEF less than 50% plus left ventricular internal diastolic diameter greater than 55 mm (90%).
• Pre-explantation LVEF less than 50% and preexisting alteration of greater than 10% best value (87.5%).
• LVEF less than 50% plus relative wall thickness decrease of less than 10% during final off-pump trial (83.3%).
Of these, he emphasized the importance of the final off-pump trial values. "An off-pump ejection fraction less than 45% in patients with a history of heart failure for more than 5 years is an absolute contraindication for VAD removal," he noted. "All such patients in our study had a recurrence of heart failure."
Early instability of ejection fraction and unstable geometry also confer a high probability of recurrence. "A wall thickness increase by more than 10% means the reverse in modeling is not stable enough," he added.
"The notion that we can actually wean patients from VADs is still a fairly new concept, and the European experience is larger than that of the United States. This is still a field that is wide open for determining patient selection and predictors of outcome after VAD removal," session moderator Dr. Gregory A. Ewald, medical director of heart transplantation at Barnes-Jewish Hospital, St. Louis, said in an interview.
"Clearly, the echocardiographic appearance of the heart on and off support is a good predictor," Dr. Ewald said, but he noted that nonechocardiographic factors such as exercise tolerance were not studied. He also noted that the field has moved to continuous-flow pumps rather than pulsatile pumps, which constituted much of the German experience. It remains to be determined if the same parameters are completely applicable to the newer-generation devices.
Dr. Dandel and Dr. Ewald reported having no relevant conflicts of interest.
NEW ORLEANS – Patients with chronic cardiomyopathy can be successfully weaned from ventricular assist devices, and certain parameters can predict long-term cardiac stability after explantation, according to German investigators.
"Unloading-promoted reversal of heart failure allows for long-term transplant-free outcomes after patients are removed from VADs. However, few patients with chronic cardiomyopathy have been weaned from VADs, and the majority only recently," said principal investigator Dr. Michael Dandel of the German Heart Institute Berlin. "The long-term outcomes of patients, therefore, and the reliability of criteria for making weaning decisions, are not well known."
At his clinic, 91 patients with chronic cardiomyopathy (CCM) as the underlying cause of heart failure were weaned from VADs between 1995 and 2010, including 75 weaned from left ventricular assist devices, 13 weaned from biventricular assist devices, and 3 weaned from right ventricular assist devices. Before VAD implantation, the patients had left ventricular ejection fraction (LVEF) values of 10%-20%.
These patients were evaluated as to the feasibility of weaning and to establish criteria that could predict long-term cardiac stability after VAD removal. "With this information, we can improve future weaning decisions and postweaning patient management," Dr. Dandel said at the annual meeting of the American College of Cardiology.
A total of 47 patients were evaluated. Of these 41 (87.2%) had idiopathic cardiomyopathy, 4 (8.5%) had histologic evidence of chronic myocarditis before VAD implantation, and 2 (4.3%) had chronic ischemic cardiomyopathy with severe left ventricular dilation.
Before VAD insertion, all patients had irreversible end-stage heart failure and required continuous positive inotropic support. No attempts were made to use VADs electively with the aim of myocardial recovery only, he said.
Postweaning results. Cardiac stability lasting at least 15 years was achieved by 2 patients, while 10 patients have been stable at least 10 years and 3 at least 5 years, he reported.
"At 5 years, only five patients, 10.6%, had died due to heart failure recurrence or weaning-related complications. Several patients died of other causes," he said.
Postweaning freedom from heart failure recurrence for all evaluated patients was 74% at 3 years and 66% at 5 years, but these results included nine patients at very high risk for poor outcomes. After 2002, when the investigators tightened their criteria for weaning, freedom from heart failure recurrence reached 100% at 3 years, he noted.
Pre-explantation variables predictive of outcomes. "Echo data obtained during ‘off pump’ trials proved to be reliable for detection of recovery during mechanical unloading," Dr. Dandel said. "In particular, off-pump [left ventricle] size, geometry, and ejection fraction were predictive of outcome after weaning, especially when history of heart failure was also considered."
For cardiac stability lasting at least 5 years, pre-explantation "off pump" LVEF of 50% or more was associated with a positive predictive value of 91.7%, while LVEF of 45% or more had a positive predictive value of 79.1%.
The positive predictive value of LVEF of 45% or more was approximately 90% if additional parameters were considered: pre-explantation left ventricle size and geometry, stability of unloading-induced cardiac improvement before VAD removal, and heart failure duration before VAD implantation.
Time to cardiac recovery seemed important, Dr. Dandel said. "Patients who had recurrences needed more time to show an improvement. They needed twice the duration of VAD support as patients who did not have a recurrence," he said.
"Definite cutoff values for certain parameters – including tissue Doppler-derived LV wall motion velocity – allowed us to formulate weaning criteria with high predictability for postweaning stability," he said.
Risk factors for heart failure recurrence. Dr. Dandel and his colleagues also identified several risk factors that predicted heart failure recurrence during the first 3 years after VAD removal. These factors, and their associated probability for recurrence, were:
• Preweaning off-pump LVEF less than 45% plus history of heart failure longer than 5 years (100%).
• Preweaning LVEF less than 45% (88.9%).
• Preweaning off-pump LVEF less than 50% plus left ventricular internal diastolic diameter greater than 55 mm (90%).
• Pre-explantation LVEF less than 50% and preexisting alteration of greater than 10% best value (87.5%).
• LVEF less than 50% plus relative wall thickness decrease of less than 10% during final off-pump trial (83.3%).
Of these, he emphasized the importance of the final off-pump trial values. "An off-pump ejection fraction less than 45% in patients with a history of heart failure for more than 5 years is an absolute contraindication for VAD removal," he noted. "All such patients in our study had a recurrence of heart failure."
Early instability of ejection fraction and unstable geometry also confer a high probability of recurrence. "A wall thickness increase by more than 10% means the reverse in modeling is not stable enough," he added.
"The notion that we can actually wean patients from VADs is still a fairly new concept, and the European experience is larger than that of the United States. This is still a field that is wide open for determining patient selection and predictors of outcome after VAD removal," session moderator Dr. Gregory A. Ewald, medical director of heart transplantation at Barnes-Jewish Hospital, St. Louis, said in an interview.
"Clearly, the echocardiographic appearance of the heart on and off support is a good predictor," Dr. Ewald said, but he noted that nonechocardiographic factors such as exercise tolerance were not studied. He also noted that the field has moved to continuous-flow pumps rather than pulsatile pumps, which constituted much of the German experience. It remains to be determined if the same parameters are completely applicable to the newer-generation devices.
Dr. Dandel and Dr. Ewald reported having no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Factors Predict Successful Weaning From VAD
NEW ORLEANS – Patients with chronic cardiomyopathy can be successfully weaned from ventricular assist devices, and certain parameters can predict long-term cardiac stability after explantation, according to German investigators.
"Unloading-promoted reversal of heart failure allows for long-term transplant-free outcomes after patients are removed from VADs. However, few patients with chronic cardiomyopathy have been weaned from VADs, and the majority only recently," said principal investigator Dr. Michael Dandel of the German Heart Institute Berlin. "The long-term outcomes of patients, therefore, and the reliability of criteria for making weaning decisions, are not well known."
At his clinic, 91 patients with chronic cardiomyopathy (CCM) as the underlying cause of heart failure were weaned from VADs between 1995 and 2010, including 75 weaned from left ventricular assist devices, 13 weaned from biventricular assist devices, and 3 weaned from right ventricular assist devices. Before VAD implantation, the patients had left ventricular ejection fraction (LVEF) values of 10%-20%.
These patients were evaluated as to the feasibility of weaning and to establish criteria that could predict long-term cardiac stability after VAD removal. "With this information, we can improve future weaning decisions and postweaning patient management," Dr. Dandel said at the annual meeting of the American College of Cardiology.
A total of 47 patients were evaluated. Of these 41 (87.2%) had idiopathic cardiomyopathy, 4 (8.5%) had histologic evidence of chronic myocarditis before VAD implantation, and 2 (4.3%) had chronic ischemic cardiomyopathy with severe left ventricular dilation.
Before VAD insertion, all patients had irreversible end-stage heart failure and required continuous positive inotropic support. No attempts were made to use VADs electively with the aim of myocardial recovery only, he said.
Postweaning results. Cardiac stability lasting at least 15 years was achieved by 2 patients, while 10 patients have been stable at least 10 years and 3 at least 5 years, he reported.
"At 5 years, only five patients, 10.6%, had died due to heart failure recurrence or weaning-related complications. Several patients died of other causes," he said.
Postweaning freedom from heart failure recurrence for all evaluated patients was 74% at 3 years and 66% at 5 years, but these results included nine patients at very high risk for poor outcomes. After 2002, when the investigators tightened their criteria for weaning, freedom from heart failure recurrence reached 100% at 3 years, he noted.
Pre-explantation variables predictive of outcomes. "Echo data obtained during ‘off pump’ trials proved to be reliable for detection of recovery during mechanical unloading," Dr. Dandel said. "In particular, off-pump [left ventricle] size, geometry, and ejection fraction were predictive of outcome after weaning, especially when history of heart failure was also considered."
For cardiac stability lasting at least 5 years, pre-explantation "off pump" LVEF of 50% or more was associated with a positive predictive value of 91.7%, while LVEF of 45% or more had a positive predictive value of 79.1%.
The positive predictive value of LVEF of 45% or more was approximately 90% if additional parameters were considered: pre-explantation left ventricle size and geometry, stability of unloading-induced cardiac improvement before VAD removal, and heart failure duration before VAD implantation.
Time to cardiac recovery seemed important, Dr. Dandel said. "Patients who had recurrences needed more time to show an improvement. They needed twice the duration of VAD support as patients who did not have a recurrence," he said.
"Definite cutoff values for certain parameters – including tissue Doppler-derived LV wall motion velocity – allowed us to formulate weaning criteria with high predictability for postweaning stability," he said.
Risk factors for heart failure recurrence. Dr. Dandel and his colleagues also identified several risk factors that predicted heart failure recurrence during the first 3 years after VAD removal. These factors, and their associated probability for recurrence, were:
• Preweaning off-pump LVEF less than 45% plus history of heart failure longer than 5 years (100%).
• Preweaning LVEF less than 45% (88.9%).
• Preweaning off-pump LVEF less than 50% plus left ventricular internal diastolic diameter greater than 55 mm (90%).
• Pre-explantation LVEF less than 50% and preexisting alteration of greater than 10% best value (87.5%).
• LVEF less than 50% plus relative wall thickness decrease of less than 10% during final off-pump trial (83.3%).
Of these, he emphasized the importance of the final off-pump trial values. "An off-pump ejection fraction less than 45% in patients with a history of heart failure for more than 5 years is an absolute contraindication for VAD removal," he noted. "All such patients in our study had a recurrence of heart failure."
Early instability of ejection fraction and unstable geometry also confer a high probability of recurrence. "A wall thickness increase by more than 10% means the reverse in modeling is not stable enough," he added.
"The notion that we can actually wean patients from VADs is still a fairly new concept, and the European experience is larger than that of the United States. This is still a field that is wide open for determining patient selection and predictors of outcome after VAD removal," session moderator Dr. Gregory A. Ewald, medical director of heart transplantation at Barnes-Jewish Hospital, St. Louis, said in an interview.
"Clearly, the echocardiographic appearance of the heart on and off support is a good predictor," Dr. Ewald said, but he noted that nonechocardiographic factors such as exercise tolerance were not studied. He also noted that the field has moved to continuous-flow pumps rather than pulsatile pumps, which constituted much of the German experience. It remains to be determined if the same parameters are completely applicable to the newer-generation devices.
Dr. Dandel and Dr. Ewald reported having no relevant conflicts of interest.
NEW ORLEANS – Patients with chronic cardiomyopathy can be successfully weaned from ventricular assist devices, and certain parameters can predict long-term cardiac stability after explantation, according to German investigators.
"Unloading-promoted reversal of heart failure allows for long-term transplant-free outcomes after patients are removed from VADs. However, few patients with chronic cardiomyopathy have been weaned from VADs, and the majority only recently," said principal investigator Dr. Michael Dandel of the German Heart Institute Berlin. "The long-term outcomes of patients, therefore, and the reliability of criteria for making weaning decisions, are not well known."
At his clinic, 91 patients with chronic cardiomyopathy (CCM) as the underlying cause of heart failure were weaned from VADs between 1995 and 2010, including 75 weaned from left ventricular assist devices, 13 weaned from biventricular assist devices, and 3 weaned from right ventricular assist devices. Before VAD implantation, the patients had left ventricular ejection fraction (LVEF) values of 10%-20%.
These patients were evaluated as to the feasibility of weaning and to establish criteria that could predict long-term cardiac stability after VAD removal. "With this information, we can improve future weaning decisions and postweaning patient management," Dr. Dandel said at the annual meeting of the American College of Cardiology.
A total of 47 patients were evaluated. Of these 41 (87.2%) had idiopathic cardiomyopathy, 4 (8.5%) had histologic evidence of chronic myocarditis before VAD implantation, and 2 (4.3%) had chronic ischemic cardiomyopathy with severe left ventricular dilation.
Before VAD insertion, all patients had irreversible end-stage heart failure and required continuous positive inotropic support. No attempts were made to use VADs electively with the aim of myocardial recovery only, he said.
Postweaning results. Cardiac stability lasting at least 15 years was achieved by 2 patients, while 10 patients have been stable at least 10 years and 3 at least 5 years, he reported.
"At 5 years, only five patients, 10.6%, had died due to heart failure recurrence or weaning-related complications. Several patients died of other causes," he said.
Postweaning freedom from heart failure recurrence for all evaluated patients was 74% at 3 years and 66% at 5 years, but these results included nine patients at very high risk for poor outcomes. After 2002, when the investigators tightened their criteria for weaning, freedom from heart failure recurrence reached 100% at 3 years, he noted.
Pre-explantation variables predictive of outcomes. "Echo data obtained during ‘off pump’ trials proved to be reliable for detection of recovery during mechanical unloading," Dr. Dandel said. "In particular, off-pump [left ventricle] size, geometry, and ejection fraction were predictive of outcome after weaning, especially when history of heart failure was also considered."
For cardiac stability lasting at least 5 years, pre-explantation "off pump" LVEF of 50% or more was associated with a positive predictive value of 91.7%, while LVEF of 45% or more had a positive predictive value of 79.1%.
The positive predictive value of LVEF of 45% or more was approximately 90% if additional parameters were considered: pre-explantation left ventricle size and geometry, stability of unloading-induced cardiac improvement before VAD removal, and heart failure duration before VAD implantation.
Time to cardiac recovery seemed important, Dr. Dandel said. "Patients who had recurrences needed more time to show an improvement. They needed twice the duration of VAD support as patients who did not have a recurrence," he said.
"Definite cutoff values for certain parameters – including tissue Doppler-derived LV wall motion velocity – allowed us to formulate weaning criteria with high predictability for postweaning stability," he said.
Risk factors for heart failure recurrence. Dr. Dandel and his colleagues also identified several risk factors that predicted heart failure recurrence during the first 3 years after VAD removal. These factors, and their associated probability for recurrence, were:
• Preweaning off-pump LVEF less than 45% plus history of heart failure longer than 5 years (100%).
• Preweaning LVEF less than 45% (88.9%).
• Preweaning off-pump LVEF less than 50% plus left ventricular internal diastolic diameter greater than 55 mm (90%).
• Pre-explantation LVEF less than 50% and preexisting alteration of greater than 10% best value (87.5%).
• LVEF less than 50% plus relative wall thickness decrease of less than 10% during final off-pump trial (83.3%).
Of these, he emphasized the importance of the final off-pump trial values. "An off-pump ejection fraction less than 45% in patients with a history of heart failure for more than 5 years is an absolute contraindication for VAD removal," he noted. "All such patients in our study had a recurrence of heart failure."
Early instability of ejection fraction and unstable geometry also confer a high probability of recurrence. "A wall thickness increase by more than 10% means the reverse in modeling is not stable enough," he added.
"The notion that we can actually wean patients from VADs is still a fairly new concept, and the European experience is larger than that of the United States. This is still a field that is wide open for determining patient selection and predictors of outcome after VAD removal," session moderator Dr. Gregory A. Ewald, medical director of heart transplantation at Barnes-Jewish Hospital, St. Louis, said in an interview.
"Clearly, the echocardiographic appearance of the heart on and off support is a good predictor," Dr. Ewald said, but he noted that nonechocardiographic factors such as exercise tolerance were not studied. He also noted that the field has moved to continuous-flow pumps rather than pulsatile pumps, which constituted much of the German experience. It remains to be determined if the same parameters are completely applicable to the newer-generation devices.
Dr. Dandel and Dr. Ewald reported having no relevant conflicts of interest.
NEW ORLEANS – Patients with chronic cardiomyopathy can be successfully weaned from ventricular assist devices, and certain parameters can predict long-term cardiac stability after explantation, according to German investigators.
"Unloading-promoted reversal of heart failure allows for long-term transplant-free outcomes after patients are removed from VADs. However, few patients with chronic cardiomyopathy have been weaned from VADs, and the majority only recently," said principal investigator Dr. Michael Dandel of the German Heart Institute Berlin. "The long-term outcomes of patients, therefore, and the reliability of criteria for making weaning decisions, are not well known."
At his clinic, 91 patients with chronic cardiomyopathy (CCM) as the underlying cause of heart failure were weaned from VADs between 1995 and 2010, including 75 weaned from left ventricular assist devices, 13 weaned from biventricular assist devices, and 3 weaned from right ventricular assist devices. Before VAD implantation, the patients had left ventricular ejection fraction (LVEF) values of 10%-20%.
These patients were evaluated as to the feasibility of weaning and to establish criteria that could predict long-term cardiac stability after VAD removal. "With this information, we can improve future weaning decisions and postweaning patient management," Dr. Dandel said at the annual meeting of the American College of Cardiology.
A total of 47 patients were evaluated. Of these 41 (87.2%) had idiopathic cardiomyopathy, 4 (8.5%) had histologic evidence of chronic myocarditis before VAD implantation, and 2 (4.3%) had chronic ischemic cardiomyopathy with severe left ventricular dilation.
Before VAD insertion, all patients had irreversible end-stage heart failure and required continuous positive inotropic support. No attempts were made to use VADs electively with the aim of myocardial recovery only, he said.
Postweaning results. Cardiac stability lasting at least 15 years was achieved by 2 patients, while 10 patients have been stable at least 10 years and 3 at least 5 years, he reported.
"At 5 years, only five patients, 10.6%, had died due to heart failure recurrence or weaning-related complications. Several patients died of other causes," he said.
Postweaning freedom from heart failure recurrence for all evaluated patients was 74% at 3 years and 66% at 5 years, but these results included nine patients at very high risk for poor outcomes. After 2002, when the investigators tightened their criteria for weaning, freedom from heart failure recurrence reached 100% at 3 years, he noted.
Pre-explantation variables predictive of outcomes. "Echo data obtained during ‘off pump’ trials proved to be reliable for detection of recovery during mechanical unloading," Dr. Dandel said. "In particular, off-pump [left ventricle] size, geometry, and ejection fraction were predictive of outcome after weaning, especially when history of heart failure was also considered."
For cardiac stability lasting at least 5 years, pre-explantation "off pump" LVEF of 50% or more was associated with a positive predictive value of 91.7%, while LVEF of 45% or more had a positive predictive value of 79.1%.
The positive predictive value of LVEF of 45% or more was approximately 90% if additional parameters were considered: pre-explantation left ventricle size and geometry, stability of unloading-induced cardiac improvement before VAD removal, and heart failure duration before VAD implantation.
Time to cardiac recovery seemed important, Dr. Dandel said. "Patients who had recurrences needed more time to show an improvement. They needed twice the duration of VAD support as patients who did not have a recurrence," he said.
"Definite cutoff values for certain parameters – including tissue Doppler-derived LV wall motion velocity – allowed us to formulate weaning criteria with high predictability for postweaning stability," he said.
Risk factors for heart failure recurrence. Dr. Dandel and his colleagues also identified several risk factors that predicted heart failure recurrence during the first 3 years after VAD removal. These factors, and their associated probability for recurrence, were:
• Preweaning off-pump LVEF less than 45% plus history of heart failure longer than 5 years (100%).
• Preweaning LVEF less than 45% (88.9%).
• Preweaning off-pump LVEF less than 50% plus left ventricular internal diastolic diameter greater than 55 mm (90%).
• Pre-explantation LVEF less than 50% and preexisting alteration of greater than 10% best value (87.5%).
• LVEF less than 50% plus relative wall thickness decrease of less than 10% during final off-pump trial (83.3%).
Of these, he emphasized the importance of the final off-pump trial values. "An off-pump ejection fraction less than 45% in patients with a history of heart failure for more than 5 years is an absolute contraindication for VAD removal," he noted. "All such patients in our study had a recurrence of heart failure."
Early instability of ejection fraction and unstable geometry also confer a high probability of recurrence. "A wall thickness increase by more than 10% means the reverse in modeling is not stable enough," he added.
"The notion that we can actually wean patients from VADs is still a fairly new concept, and the European experience is larger than that of the United States. This is still a field that is wide open for determining patient selection and predictors of outcome after VAD removal," session moderator Dr. Gregory A. Ewald, medical director of heart transplantation at Barnes-Jewish Hospital, St. Louis, said in an interview.
"Clearly, the echocardiographic appearance of the heart on and off support is a good predictor," Dr. Ewald said, but he noted that nonechocardiographic factors such as exercise tolerance were not studied. He also noted that the field has moved to continuous-flow pumps rather than pulsatile pumps, which constituted much of the German experience. It remains to be determined if the same parameters are completely applicable to the newer-generation devices.
Dr. Dandel and Dr. Ewald reported having no relevant conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Nearly Half of ICDs in Massachusetts Placed for Off – Label Indications
NEW ORLEANS – Nearly half of patients who received an implantable cardioverter defibrillator in Massachusetts during 1998-2008 had at least one clinical factor that categorized them as an off-label recipient, based on the exclusion criteria used in the clinical trials that established the efficacy of these devices.
The most common off-label use occurred in patients aged either 75 or older or 19 or younger, which in both cases put them outside of the age enrollment criteria for the implantable cardioverter defibrillator (ICD) trials, Dr. Norman S. Kato reported while presenting a poster at the annual meeting of the American College of Cardiology.
ICDs given to patients outside the age range that was tested in trials accounted for well over a quarter of all ICD use in Massachusetts during the period studied, and more than half of all off-label use. Other common off-label ICD uses occurred in patients with renal insufficiency or a recent acute MI, reported Dr. Kato, a cardiothoracic surgeon in Encino, Calif., who has consulted with the Food and Drug Administration, and his associates in their poster (J. Am Coll. Cardiol. 2011;57:E184).
Their analysis, which included 15,724 ICD recipients during the 11-year period studied, represents "the first analysis [of ICD use] to encompass all patients who have received this technology in a single state," he said in an interview. But he also cautioned that "it would be incorrect to generalize these results to other states, or to assume anything about practice patterns in Massachusetts" in the years following 2008.
"The key finding from our study was that patients over age 65 represent a significant portion of the population receiving these devices. Our research revealed that about 45% of all patients receiving the devices in the Medicare age group were age 75 or older." In addition, the results showed that 15% of recipients were age 85 or older.
"ICDs may have been implanted when there was little empirical evidence to support their use. Because subjects over age 75 were specifically excluded from the randomized clinical trials [of ICDs,] there is no scientific evidence to support the notion that ICDs are safe or effective in this group," Dr. Kato said. "We really need to conduct randomized clinical trials in the excluded groups to determine safety and efficacy. If there is a lot of off-label use for a specific indication, then it stands to reason that clinical trials should be conducted to determine the safety and efficacy of the device for these specific indications.
"Off-label use does not necessarily mean that the use was without benefit or was unsafe," he noted. "Off-label use is simply the use of the device for conditions that were not tested during the randomized clinical trials."
The Centers for Medicare and Medicaid Services, in a 2005 decision memo on ICD use, noted that only 10% of patients who were enrolled in the two largest ICD trials were aged 75 or older, and as a consequence "the implantation of a defibrillator in the most elderly patients should be carefully considered and not routinely recommended," the memo said (CAG-00157R3).
Dr. Kato’s study of Massachusetts ICD usage also showed disproportionate placement of ICDs in men. During 1998-2008, men received ICDs three- to eightfold more often than did women for primary prevention indications, and three- to ninefold more often for secondary prevention.
These findings raise issues of a sex bias or a disease bias that favored men over women for ICD placement, he said. "In general, men have a higher risk for and greater rates of heart attack and coronary artery disease than women, hence men should probably be more likely to receive an ICD. But this merits consideration since results from other studies have also identified the same frequency differences by gender," said Dr. Kato.
The analyses used data compiled by the Massachusetts Department of Health and Human Services on hospital case mix and charge, as well as population estimates from the National Center for Health Statistics.
During the 11-year period studied, the rate of off-label ICD use for primary prevention indications ranged from 28% to 50%, depending on the year. In 2008, about 45% of Massachusetts patients who received an ICD had at least one off-label clinical feature, with age being an off-label factor for about 28% of all recipients. Primary-prevention use, which totaled 13,801 patients over the 11 years studied, occurred in patients with a diagnosis of heart failure or cardiomyopathy.
In 2008, about 45% of patients who received an ICD for secondary prevention had an off-label feature. Secondary-prevention use, which occurred in a total of 1,923 patients in the 11 years studied, included the indications of a history of cardiac arrest or ventricular arrhythmia during the year prior to ICD placement in patients who did not have a primary-prevention indication.
Criteria that led to exclusion from the ICD efficacy trials and hence constitute markers of off-label use included patients undergoing simultaneous percutaneous coronary intervention or coronary artery bypass surgery, and patients with a recent acute MI, renal failure, liver failure, neurologic failure, solid tumor, or dementia, as well as patients on dialysis, and patients aged 75 or older or aged 19 or younger.
Dr. Kato and his associates on the study said that they had no disclosures.
NEW ORLEANS – Nearly half of patients who received an implantable cardioverter defibrillator in Massachusetts during 1998-2008 had at least one clinical factor that categorized them as an off-label recipient, based on the exclusion criteria used in the clinical trials that established the efficacy of these devices.
The most common off-label use occurred in patients aged either 75 or older or 19 or younger, which in both cases put them outside of the age enrollment criteria for the implantable cardioverter defibrillator (ICD) trials, Dr. Norman S. Kato reported while presenting a poster at the annual meeting of the American College of Cardiology.
ICDs given to patients outside the age range that was tested in trials accounted for well over a quarter of all ICD use in Massachusetts during the period studied, and more than half of all off-label use. Other common off-label ICD uses occurred in patients with renal insufficiency or a recent acute MI, reported Dr. Kato, a cardiothoracic surgeon in Encino, Calif., who has consulted with the Food and Drug Administration, and his associates in their poster (J. Am Coll. Cardiol. 2011;57:E184).
Their analysis, which included 15,724 ICD recipients during the 11-year period studied, represents "the first analysis [of ICD use] to encompass all patients who have received this technology in a single state," he said in an interview. But he also cautioned that "it would be incorrect to generalize these results to other states, or to assume anything about practice patterns in Massachusetts" in the years following 2008.
"The key finding from our study was that patients over age 65 represent a significant portion of the population receiving these devices. Our research revealed that about 45% of all patients receiving the devices in the Medicare age group were age 75 or older." In addition, the results showed that 15% of recipients were age 85 or older.
"ICDs may have been implanted when there was little empirical evidence to support their use. Because subjects over age 75 were specifically excluded from the randomized clinical trials [of ICDs,] there is no scientific evidence to support the notion that ICDs are safe or effective in this group," Dr. Kato said. "We really need to conduct randomized clinical trials in the excluded groups to determine safety and efficacy. If there is a lot of off-label use for a specific indication, then it stands to reason that clinical trials should be conducted to determine the safety and efficacy of the device for these specific indications.
"Off-label use does not necessarily mean that the use was without benefit or was unsafe," he noted. "Off-label use is simply the use of the device for conditions that were not tested during the randomized clinical trials."
The Centers for Medicare and Medicaid Services, in a 2005 decision memo on ICD use, noted that only 10% of patients who were enrolled in the two largest ICD trials were aged 75 or older, and as a consequence "the implantation of a defibrillator in the most elderly patients should be carefully considered and not routinely recommended," the memo said (CAG-00157R3).
Dr. Kato’s study of Massachusetts ICD usage also showed disproportionate placement of ICDs in men. During 1998-2008, men received ICDs three- to eightfold more often than did women for primary prevention indications, and three- to ninefold more often for secondary prevention.
These findings raise issues of a sex bias or a disease bias that favored men over women for ICD placement, he said. "In general, men have a higher risk for and greater rates of heart attack and coronary artery disease than women, hence men should probably be more likely to receive an ICD. But this merits consideration since results from other studies have also identified the same frequency differences by gender," said Dr. Kato.
The analyses used data compiled by the Massachusetts Department of Health and Human Services on hospital case mix and charge, as well as population estimates from the National Center for Health Statistics.
During the 11-year period studied, the rate of off-label ICD use for primary prevention indications ranged from 28% to 50%, depending on the year. In 2008, about 45% of Massachusetts patients who received an ICD had at least one off-label clinical feature, with age being an off-label factor for about 28% of all recipients. Primary-prevention use, which totaled 13,801 patients over the 11 years studied, occurred in patients with a diagnosis of heart failure or cardiomyopathy.
In 2008, about 45% of patients who received an ICD for secondary prevention had an off-label feature. Secondary-prevention use, which occurred in a total of 1,923 patients in the 11 years studied, included the indications of a history of cardiac arrest or ventricular arrhythmia during the year prior to ICD placement in patients who did not have a primary-prevention indication.
Criteria that led to exclusion from the ICD efficacy trials and hence constitute markers of off-label use included patients undergoing simultaneous percutaneous coronary intervention or coronary artery bypass surgery, and patients with a recent acute MI, renal failure, liver failure, neurologic failure, solid tumor, or dementia, as well as patients on dialysis, and patients aged 75 or older or aged 19 or younger.
Dr. Kato and his associates on the study said that they had no disclosures.
NEW ORLEANS – Nearly half of patients who received an implantable cardioverter defibrillator in Massachusetts during 1998-2008 had at least one clinical factor that categorized them as an off-label recipient, based on the exclusion criteria used in the clinical trials that established the efficacy of these devices.
The most common off-label use occurred in patients aged either 75 or older or 19 or younger, which in both cases put them outside of the age enrollment criteria for the implantable cardioverter defibrillator (ICD) trials, Dr. Norman S. Kato reported while presenting a poster at the annual meeting of the American College of Cardiology.
ICDs given to patients outside the age range that was tested in trials accounted for well over a quarter of all ICD use in Massachusetts during the period studied, and more than half of all off-label use. Other common off-label ICD uses occurred in patients with renal insufficiency or a recent acute MI, reported Dr. Kato, a cardiothoracic surgeon in Encino, Calif., who has consulted with the Food and Drug Administration, and his associates in their poster (J. Am Coll. Cardiol. 2011;57:E184).
Their analysis, which included 15,724 ICD recipients during the 11-year period studied, represents "the first analysis [of ICD use] to encompass all patients who have received this technology in a single state," he said in an interview. But he also cautioned that "it would be incorrect to generalize these results to other states, or to assume anything about practice patterns in Massachusetts" in the years following 2008.
"The key finding from our study was that patients over age 65 represent a significant portion of the population receiving these devices. Our research revealed that about 45% of all patients receiving the devices in the Medicare age group were age 75 or older." In addition, the results showed that 15% of recipients were age 85 or older.
"ICDs may have been implanted when there was little empirical evidence to support their use. Because subjects over age 75 were specifically excluded from the randomized clinical trials [of ICDs,] there is no scientific evidence to support the notion that ICDs are safe or effective in this group," Dr. Kato said. "We really need to conduct randomized clinical trials in the excluded groups to determine safety and efficacy. If there is a lot of off-label use for a specific indication, then it stands to reason that clinical trials should be conducted to determine the safety and efficacy of the device for these specific indications.
"Off-label use does not necessarily mean that the use was without benefit or was unsafe," he noted. "Off-label use is simply the use of the device for conditions that were not tested during the randomized clinical trials."
The Centers for Medicare and Medicaid Services, in a 2005 decision memo on ICD use, noted that only 10% of patients who were enrolled in the two largest ICD trials were aged 75 or older, and as a consequence "the implantation of a defibrillator in the most elderly patients should be carefully considered and not routinely recommended," the memo said (CAG-00157R3).
Dr. Kato’s study of Massachusetts ICD usage also showed disproportionate placement of ICDs in men. During 1998-2008, men received ICDs three- to eightfold more often than did women for primary prevention indications, and three- to ninefold more often for secondary prevention.
These findings raise issues of a sex bias or a disease bias that favored men over women for ICD placement, he said. "In general, men have a higher risk for and greater rates of heart attack and coronary artery disease than women, hence men should probably be more likely to receive an ICD. But this merits consideration since results from other studies have also identified the same frequency differences by gender," said Dr. Kato.
The analyses used data compiled by the Massachusetts Department of Health and Human Services on hospital case mix and charge, as well as population estimates from the National Center for Health Statistics.
During the 11-year period studied, the rate of off-label ICD use for primary prevention indications ranged from 28% to 50%, depending on the year. In 2008, about 45% of Massachusetts patients who received an ICD had at least one off-label clinical feature, with age being an off-label factor for about 28% of all recipients. Primary-prevention use, which totaled 13,801 patients over the 11 years studied, occurred in patients with a diagnosis of heart failure or cardiomyopathy.
In 2008, about 45% of patients who received an ICD for secondary prevention had an off-label feature. Secondary-prevention use, which occurred in a total of 1,923 patients in the 11 years studied, included the indications of a history of cardiac arrest or ventricular arrhythmia during the year prior to ICD placement in patients who did not have a primary-prevention indication.
Criteria that led to exclusion from the ICD efficacy trials and hence constitute markers of off-label use included patients undergoing simultaneous percutaneous coronary intervention or coronary artery bypass surgery, and patients with a recent acute MI, renal failure, liver failure, neurologic failure, solid tumor, or dementia, as well as patients on dialysis, and patients aged 75 or older or aged 19 or younger.
Dr. Kato and his associates on the study said that they had no disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: During 1998-2008, off-label placement of ICDs in Massachusetts occurred in 28%-50% of patients who received devices for primary prevention, and in 35%-58% of patients treated for secondary prevention.
Data Source: Hospital case mix and charge data collected by the Massachusetts DHHS for 15,724 patients receiving an ICD during 1998-2008.
Disclosures: Dr. Kato and his associates said that they had no disclosures.
Persistent LV Hypertrophy Worsens Hypertension Outcomes
NEW ORLEANS – Hypertensive patients with persistent left ventricular hypertrophy despite normalized blood pressure faced a substantially higher risk for death and cardiovascular events, compared with patients without hypertrophy on antihypertensive treatment, according to the findings of a study involving 463 patients.
"These results suggest that persistence of left ventricular hypertrophy in a subset of patients with lower achieved blood pressure during treatment may in part explain the lack of benefit seen in hypertensive patients, despite treatment to lower systolic blood pressure," Dr. Peter M. Okin said at the annual meeting of the American College of Cardiology.
Based on these results, it may be necessary to track end-organ damage – in this case, as manifested by ECG left ventricular hypertrophy – in addition to blood pressure to fully assess response to treatment in hypertensive patients. "You can’t just track blood pressure; you need to look at end-organ damage," such as the size of the heart, said Dr. Okin, a cardiologist and professor of medicine at Cornell University in New York.
But currently no evidence exists on the best way to manage patients whose hearts remain enlarged despite blood pressure normalization.
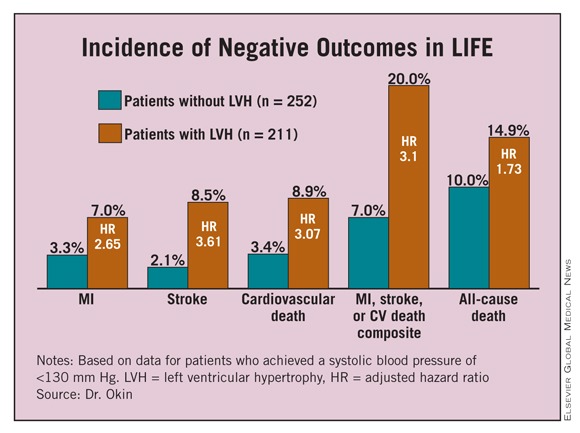
"The data are not there to say you should treat these patients more aggressively," he said in an interview. In fact, an equally plausible approach would be to back off treatment in such patients because of the high hazard they face and the lack of evidence that treatment helps their clinical outcome. Randomized trials must be done to identify the best way to manage these patients, he said.
The analysis Dr. Okin reported came from a subset of patients who were enrolled in the LIFE (Losartan Intervention for End Point Reduction in Hypertension) study, which enrolled 9,193 patients aged 55-80 years with a blood pressure of 160/95 mm Hg to 200/115 mm Hg. The study randomized patients to two different antihypertensive treatment arms, one based primarily on losartan and the control based primarily on atenolol, with a target blood pressure of 140/90 mm Hg or less (Lancet 2002;359:995-1003).
The subgroup that was used for the new analysis included the 463 patients in the study who achieved a systolic blood pressure of 130 mm Hg or less. Their average age was 65 years, and slightly more than half were men. During an average follow-up of more than 4 years, the combined rate of cardiovascular death, MI, or stroke was 15%.
The researchers used data from the 12-lead ECG recordings of these patients, as analyzed by the Cornell product equation and by Sokolow-Lyon voltage to calculate left ventricular size. They considered any patient with a Cornell product greater than 2440 mm x msec to have residual left ventricular hypertrophy. This identified 211 patients (46%) with persistent hypertrophy despite their low achieved systolic blood pressure, and 252 patients without hypertrophy.
Patients with persistent hypertrophy were significantly older (66 years), compared with those without hypertrophy (64 years), and were significantly more likely to be women (53%), compared with the 40% rate of women in the group without hypertrophy. At baseline, the two subgroups had similar average blood pressures, and on treatment the average decline in systolic and diastolic pressures were similar in the two subgroups.
During the average 4.4 years of follow-up, patients with residual hypertrophy had significantly higher rates of MI, strokes, cardiovascular death, and all-cause mortality, as well as a significantly higher rate of the combined end point of MI, stroke, or cardiovascular death, compared with the patients without hypertrophy. (See box.) These significant differences remained after multivariate adjustment for treatment allocation within the study, baseline Framingham risks score, and diastolic blood pressure on treatment.
Dr. Okin said that he receives a financial benefit from GE Medical Systems. The LIFE trial was sponsored by Merck, which markets losartan (Cozaar).
NEW ORLEANS – Hypertensive patients with persistent left ventricular hypertrophy despite normalized blood pressure faced a substantially higher risk for death and cardiovascular events, compared with patients without hypertrophy on antihypertensive treatment, according to the findings of a study involving 463 patients.
"These results suggest that persistence of left ventricular hypertrophy in a subset of patients with lower achieved blood pressure during treatment may in part explain the lack of benefit seen in hypertensive patients, despite treatment to lower systolic blood pressure," Dr. Peter M. Okin said at the annual meeting of the American College of Cardiology.
Based on these results, it may be necessary to track end-organ damage – in this case, as manifested by ECG left ventricular hypertrophy – in addition to blood pressure to fully assess response to treatment in hypertensive patients. "You can’t just track blood pressure; you need to look at end-organ damage," such as the size of the heart, said Dr. Okin, a cardiologist and professor of medicine at Cornell University in New York.
But currently no evidence exists on the best way to manage patients whose hearts remain enlarged despite blood pressure normalization.
"The data are not there to say you should treat these patients more aggressively," he said in an interview. In fact, an equally plausible approach would be to back off treatment in such patients because of the high hazard they face and the lack of evidence that treatment helps their clinical outcome. Randomized trials must be done to identify the best way to manage these patients, he said.
The analysis Dr. Okin reported came from a subset of patients who were enrolled in the LIFE (Losartan Intervention for End Point Reduction in Hypertension) study, which enrolled 9,193 patients aged 55-80 years with a blood pressure of 160/95 mm Hg to 200/115 mm Hg. The study randomized patients to two different antihypertensive treatment arms, one based primarily on losartan and the control based primarily on atenolol, with a target blood pressure of 140/90 mm Hg or less (Lancet 2002;359:995-1003).
The subgroup that was used for the new analysis included the 463 patients in the study who achieved a systolic blood pressure of 130 mm Hg or less. Their average age was 65 years, and slightly more than half were men. During an average follow-up of more than 4 years, the combined rate of cardiovascular death, MI, or stroke was 15%.
The researchers used data from the 12-lead ECG recordings of these patients, as analyzed by the Cornell product equation and by Sokolow-Lyon voltage to calculate left ventricular size. They considered any patient with a Cornell product greater than 2440 mm x msec to have residual left ventricular hypertrophy. This identified 211 patients (46%) with persistent hypertrophy despite their low achieved systolic blood pressure, and 252 patients without hypertrophy.
Patients with persistent hypertrophy were significantly older (66 years), compared with those without hypertrophy (64 years), and were significantly more likely to be women (53%), compared with the 40% rate of women in the group without hypertrophy. At baseline, the two subgroups had similar average blood pressures, and on treatment the average decline in systolic and diastolic pressures were similar in the two subgroups.
During the average 4.4 years of follow-up, patients with residual hypertrophy had significantly higher rates of MI, strokes, cardiovascular death, and all-cause mortality, as well as a significantly higher rate of the combined end point of MI, stroke, or cardiovascular death, compared with the patients without hypertrophy. (See box.) These significant differences remained after multivariate adjustment for treatment allocation within the study, baseline Framingham risks score, and diastolic blood pressure on treatment.
Dr. Okin said that he receives a financial benefit from GE Medical Systems. The LIFE trial was sponsored by Merck, which markets losartan (Cozaar).
NEW ORLEANS – Hypertensive patients with persistent left ventricular hypertrophy despite normalized blood pressure faced a substantially higher risk for death and cardiovascular events, compared with patients without hypertrophy on antihypertensive treatment, according to the findings of a study involving 463 patients.
"These results suggest that persistence of left ventricular hypertrophy in a subset of patients with lower achieved blood pressure during treatment may in part explain the lack of benefit seen in hypertensive patients, despite treatment to lower systolic blood pressure," Dr. Peter M. Okin said at the annual meeting of the American College of Cardiology.
Based on these results, it may be necessary to track end-organ damage – in this case, as manifested by ECG left ventricular hypertrophy – in addition to blood pressure to fully assess response to treatment in hypertensive patients. "You can’t just track blood pressure; you need to look at end-organ damage," such as the size of the heart, said Dr. Okin, a cardiologist and professor of medicine at Cornell University in New York.
But currently no evidence exists on the best way to manage patients whose hearts remain enlarged despite blood pressure normalization.
"The data are not there to say you should treat these patients more aggressively," he said in an interview. In fact, an equally plausible approach would be to back off treatment in such patients because of the high hazard they face and the lack of evidence that treatment helps their clinical outcome. Randomized trials must be done to identify the best way to manage these patients, he said.
The analysis Dr. Okin reported came from a subset of patients who were enrolled in the LIFE (Losartan Intervention for End Point Reduction in Hypertension) study, which enrolled 9,193 patients aged 55-80 years with a blood pressure of 160/95 mm Hg to 200/115 mm Hg. The study randomized patients to two different antihypertensive treatment arms, one based primarily on losartan and the control based primarily on atenolol, with a target blood pressure of 140/90 mm Hg or less (Lancet 2002;359:995-1003).
The subgroup that was used for the new analysis included the 463 patients in the study who achieved a systolic blood pressure of 130 mm Hg or less. Their average age was 65 years, and slightly more than half were men. During an average follow-up of more than 4 years, the combined rate of cardiovascular death, MI, or stroke was 15%.
The researchers used data from the 12-lead ECG recordings of these patients, as analyzed by the Cornell product equation and by Sokolow-Lyon voltage to calculate left ventricular size. They considered any patient with a Cornell product greater than 2440 mm x msec to have residual left ventricular hypertrophy. This identified 211 patients (46%) with persistent hypertrophy despite their low achieved systolic blood pressure, and 252 patients without hypertrophy.
Patients with persistent hypertrophy were significantly older (66 years), compared with those without hypertrophy (64 years), and were significantly more likely to be women (53%), compared with the 40% rate of women in the group without hypertrophy. At baseline, the two subgroups had similar average blood pressures, and on treatment the average decline in systolic and diastolic pressures were similar in the two subgroups.
During the average 4.4 years of follow-up, patients with residual hypertrophy had significantly higher rates of MI, strokes, cardiovascular death, and all-cause mortality, as well as a significantly higher rate of the combined end point of MI, stroke, or cardiovascular death, compared with the patients without hypertrophy. (See box.) These significant differences remained after multivariate adjustment for treatment allocation within the study, baseline Framingham risks score, and diastolic blood pressure on treatment.
Dr. Okin said that he receives a financial benefit from GE Medical Systems. The LIFE trial was sponsored by Merck, which markets losartan (Cozaar).
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Patients with persistent left ventricular hypertrophy had a threefold higher rate of cardiovascular death, MI, or stroke compared with patients without hypertrophy on treatment.
Data Source: Analysis of 463 patients enrolled in the LIFE hypertension-treatment trial who achieved a systolic blood pressure of 130 mm Hg or less on treatment.
Disclosures: Dr. Okin said that he receives a financial benefit from GE Medical Systems. The LIFE trial was sponsored by Merck, which markets losartan (Cozaar).
Persistent LV Hypertrophy Worsens Hypertension Outcomes
NEW ORLEANS – Hypertensive patients with persistent left ventricular hypertrophy despite normalized blood pressure faced a substantially higher risk for death and cardiovascular events, compared with patients without hypertrophy on antihypertensive treatment, according to the findings of a study involving 463 patients.
"These results suggest that persistence of left ventricular hypertrophy in a subset of patients with lower achieved blood pressure during treatment may in part explain the lack of benefit seen in hypertensive patients, despite treatment to lower systolic blood pressure," Dr. Peter M. Okin said at the annual meeting of the American College of Cardiology.
Based on these results, it may be necessary to track end-organ damage – in this case, as manifested by ECG left ventricular hypertrophy – in addition to blood pressure to fully assess response to treatment in hypertensive patients. "You can’t just track blood pressure; you need to look at end-organ damage," such as the size of the heart, said Dr. Okin, a cardiologist and professor of medicine at Cornell University in New York.
But currently no evidence exists on the best way to manage patients whose hearts remain enlarged despite blood pressure normalization.
"The data are not there to say you should treat these patients more aggressively," he said in an interview. In fact, an equally plausible approach would be to back off treatment in such patients because of the high hazard they face and the lack of evidence that treatment helps their clinical outcome. Randomized trials must be done to identify the best way to manage these patients, he said.
The analysis Dr. Okin reported came from a subset of patients who were enrolled in the LIFE (Losartan Intervention for End Point Reduction in Hypertension) study, which enrolled 9,193 patients aged 55-80 years with a blood pressure of 160/95 mm Hg to 200/115 mm Hg. The study randomized patients to two different antihypertensive treatment arms, one based primarily on losartan and the control based primarily on atenolol, with a target blood pressure of 140/90 mm Hg or less (Lancet 2002;359:995-1003).
The subgroup that was used for the new analysis included the 463 patients in the study who achieved a systolic blood pressure of 130 mm Hg or less. Their average age was 65 years, and slightly more than half were men. During an average follow-up of more than 4 years, the combined rate of cardiovascular death, MI, or stroke was 15%.
The researchers used data from the 12-lead ECG recordings of these patients, as analyzed by the Cornell product equation and by Sokolow-Lyon voltage to calculate left ventricular size. They considered any patient with a Cornell product greater than 2440 mm x msec to have residual left ventricular hypertrophy. This identified 211 patients (46%) with persistent hypertrophy despite their low achieved systolic blood pressure, and 252 patients without hypertrophy.
Patients with persistent hypertrophy were significantly older (66 years), compared with those without hypertrophy (64 years), and were significantly more likely to be women (53%), compared with the 40% rate of women in the group without hypertrophy. At baseline, the two subgroups had similar average blood pressures, and on treatment the average decline in systolic and diastolic pressures were similar in the two subgroups.
During the average 4.4 years of follow-up, patients with residual hypertrophy had significantly higher rates of MI, strokes, cardiovascular death, and all-cause mortality, as well as a significantly higher rate of the combined end point of MI, stroke, or cardiovascular death, compared with the patients without hypertrophy. (See box.) These significant differences remained after multivariate adjustment for treatment allocation within the study, baseline Framingham risks score, and diastolic blood pressure on treatment.
Dr. Okin said that he receives a financial benefit from GE Medical Systems. The LIFE trial was sponsored by Merck, which markets losartan (Cozaar).
NEW ORLEANS – Hypertensive patients with persistent left ventricular hypertrophy despite normalized blood pressure faced a substantially higher risk for death and cardiovascular events, compared with patients without hypertrophy on antihypertensive treatment, according to the findings of a study involving 463 patients.
"These results suggest that persistence of left ventricular hypertrophy in a subset of patients with lower achieved blood pressure during treatment may in part explain the lack of benefit seen in hypertensive patients, despite treatment to lower systolic blood pressure," Dr. Peter M. Okin said at the annual meeting of the American College of Cardiology.
Based on these results, it may be necessary to track end-organ damage – in this case, as manifested by ECG left ventricular hypertrophy – in addition to blood pressure to fully assess response to treatment in hypertensive patients. "You can’t just track blood pressure; you need to look at end-organ damage," such as the size of the heart, said Dr. Okin, a cardiologist and professor of medicine at Cornell University in New York.
But currently no evidence exists on the best way to manage patients whose hearts remain enlarged despite blood pressure normalization.
"The data are not there to say you should treat these patients more aggressively," he said in an interview. In fact, an equally plausible approach would be to back off treatment in such patients because of the high hazard they face and the lack of evidence that treatment helps their clinical outcome. Randomized trials must be done to identify the best way to manage these patients, he said.
The analysis Dr. Okin reported came from a subset of patients who were enrolled in the LIFE (Losartan Intervention for End Point Reduction in Hypertension) study, which enrolled 9,193 patients aged 55-80 years with a blood pressure of 160/95 mm Hg to 200/115 mm Hg. The study randomized patients to two different antihypertensive treatment arms, one based primarily on losartan and the control based primarily on atenolol, with a target blood pressure of 140/90 mm Hg or less (Lancet 2002;359:995-1003).
The subgroup that was used for the new analysis included the 463 patients in the study who achieved a systolic blood pressure of 130 mm Hg or less. Their average age was 65 years, and slightly more than half were men. During an average follow-up of more than 4 years, the combined rate of cardiovascular death, MI, or stroke was 15%.
The researchers used data from the 12-lead ECG recordings of these patients, as analyzed by the Cornell product equation and by Sokolow-Lyon voltage to calculate left ventricular size. They considered any patient with a Cornell product greater than 2440 mm x msec to have residual left ventricular hypertrophy. This identified 211 patients (46%) with persistent hypertrophy despite their low achieved systolic blood pressure, and 252 patients without hypertrophy.
Patients with persistent hypertrophy were significantly older (66 years), compared with those without hypertrophy (64 years), and were significantly more likely to be women (53%), compared with the 40% rate of women in the group without hypertrophy. At baseline, the two subgroups had similar average blood pressures, and on treatment the average decline in systolic and diastolic pressures were similar in the two subgroups.
During the average 4.4 years of follow-up, patients with residual hypertrophy had significantly higher rates of MI, strokes, cardiovascular death, and all-cause mortality, as well as a significantly higher rate of the combined end point of MI, stroke, or cardiovascular death, compared with the patients without hypertrophy. (See box.) These significant differences remained after multivariate adjustment for treatment allocation within the study, baseline Framingham risks score, and diastolic blood pressure on treatment.
Dr. Okin said that he receives a financial benefit from GE Medical Systems. The LIFE trial was sponsored by Merck, which markets losartan (Cozaar).
NEW ORLEANS – Hypertensive patients with persistent left ventricular hypertrophy despite normalized blood pressure faced a substantially higher risk for death and cardiovascular events, compared with patients without hypertrophy on antihypertensive treatment, according to the findings of a study involving 463 patients.
"These results suggest that persistence of left ventricular hypertrophy in a subset of patients with lower achieved blood pressure during treatment may in part explain the lack of benefit seen in hypertensive patients, despite treatment to lower systolic blood pressure," Dr. Peter M. Okin said at the annual meeting of the American College of Cardiology.
Based on these results, it may be necessary to track end-organ damage – in this case, as manifested by ECG left ventricular hypertrophy – in addition to blood pressure to fully assess response to treatment in hypertensive patients. "You can’t just track blood pressure; you need to look at end-organ damage," such as the size of the heart, said Dr. Okin, a cardiologist and professor of medicine at Cornell University in New York.
But currently no evidence exists on the best way to manage patients whose hearts remain enlarged despite blood pressure normalization.
"The data are not there to say you should treat these patients more aggressively," he said in an interview. In fact, an equally plausible approach would be to back off treatment in such patients because of the high hazard they face and the lack of evidence that treatment helps their clinical outcome. Randomized trials must be done to identify the best way to manage these patients, he said.
The analysis Dr. Okin reported came from a subset of patients who were enrolled in the LIFE (Losartan Intervention for End Point Reduction in Hypertension) study, which enrolled 9,193 patients aged 55-80 years with a blood pressure of 160/95 mm Hg to 200/115 mm Hg. The study randomized patients to two different antihypertensive treatment arms, one based primarily on losartan and the control based primarily on atenolol, with a target blood pressure of 140/90 mm Hg or less (Lancet 2002;359:995-1003).
The subgroup that was used for the new analysis included the 463 patients in the study who achieved a systolic blood pressure of 130 mm Hg or less. Their average age was 65 years, and slightly more than half were men. During an average follow-up of more than 4 years, the combined rate of cardiovascular death, MI, or stroke was 15%.
The researchers used data from the 12-lead ECG recordings of these patients, as analyzed by the Cornell product equation and by Sokolow-Lyon voltage to calculate left ventricular size. They considered any patient with a Cornell product greater than 2440 mm x msec to have residual left ventricular hypertrophy. This identified 211 patients (46%) with persistent hypertrophy despite their low achieved systolic blood pressure, and 252 patients without hypertrophy.
Patients with persistent hypertrophy were significantly older (66 years), compared with those without hypertrophy (64 years), and were significantly more likely to be women (53%), compared with the 40% rate of women in the group without hypertrophy. At baseline, the two subgroups had similar average blood pressures, and on treatment the average decline in systolic and diastolic pressures were similar in the two subgroups.
During the average 4.4 years of follow-up, patients with residual hypertrophy had significantly higher rates of MI, strokes, cardiovascular death, and all-cause mortality, as well as a significantly higher rate of the combined end point of MI, stroke, or cardiovascular death, compared with the patients without hypertrophy. (See box.) These significant differences remained after multivariate adjustment for treatment allocation within the study, baseline Framingham risks score, and diastolic blood pressure on treatment.
Dr. Okin said that he receives a financial benefit from GE Medical Systems. The LIFE trial was sponsored by Merck, which markets losartan (Cozaar).
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Persistent LV Hypertrophy Worsens Hypertension Outcomes
NEW ORLEANS – Hypertensive patients with persistent left ventricular hypertrophy despite normalized blood pressure faced a substantially higher risk for death and cardiovascular events, compared with patients without hypertrophy on antihypertensive treatment, according to the findings of a study involving 463 patients.
"These results suggest that persistence of left ventricular hypertrophy in a subset of patients with lower achieved blood pressure during treatment may in part explain the lack of benefit seen in hypertensive patients, despite treatment to lower systolic blood pressure," Dr. Peter M. Okin said at the annual meeting of the American College of Cardiology.
Based on these results, it may be necessary to track end-organ damage – in this case, as manifested by ECG left ventricular hypertrophy – in addition to blood pressure to fully assess response to treatment in hypertensive patients. "You can’t just track blood pressure; you need to look at end-organ damage," such as the size of the heart, said Dr. Okin, a cardiologist and professor of medicine at Cornell University in New York.
But currently no evidence exists on the best way to manage patients whose hearts remain enlarged despite blood pressure normalization.
"The data are not there to say you should treat these patients more aggressively," he said in an interview. In fact, an equally plausible approach would be to back off treatment in such patients because of the high hazard they face and the lack of evidence that treatment helps their clinical outcome. Randomized trials must be done to identify the best way to manage these patients, he said.
The analysis Dr. Okin reported came from a subset of patients who were enrolled in the LIFE (Losartan Intervention for End Point Reduction in Hypertension) study, which enrolled 9,193 patients aged 55-80 years with a blood pressure of 160/95 mm Hg to 200/115 mm Hg. The study randomized patients to two different antihypertensive treatment arms, one based primarily on losartan and the control based primarily on atenolol, with a target blood pressure of 140/90 mm Hg or less (Lancet 2002;359:995-1003).
The subgroup that was used for the new analysis included the 463 patients in the study who achieved a systolic blood pressure of 130 mm Hg or less. Their average age was 65 years, and slightly more than half were men. During an average follow-up of more than 4 years, the combined rate of cardiovascular death, MI, or stroke was 15%.
The researchers used data from the 12-lead ECG recordings of these patients, as analyzed by the Cornell product equation and by Sokolow-Lyon voltage to calculate left ventricular size. They considered any patient with a Cornell product greater than 2440 mm x msec to have residual left ventricular hypertrophy. This identified 211 patients (46%) with persistent hypertrophy despite their low achieved systolic blood pressure, and 252 patients without hypertrophy.
Patients with persistent hypertrophy were significantly older (66 years), compared with those without hypertrophy (64 years), and were significantly more likely to be women (53%), compared with the 40% rate of women in the group without hypertrophy. At baseline, the two subgroups had similar average blood pressures, and on treatment the average decline in systolic and diastolic pressures were similar in the two subgroups.
During the average 4.4 years of follow-up, patients with residual hypertrophy had significantly higher rates of MI, strokes, cardiovascular death, and all-cause mortality, as well as a significantly higher rate of the combined end point of MI, stroke, or cardiovascular death, compared with the patients without hypertrophy. (See box.) These significant differences remained after multivariate adjustment for treatment allocation within the study, baseline Framingham risks score, and diastolic blood pressure on treatment.
Dr. Okin said that he receives a financial benefit from GE Medical Systems. The LIFE trial was sponsored by Merck, which markets losartan (Cozaar).
NEW ORLEANS – Hypertensive patients with persistent left ventricular hypertrophy despite normalized blood pressure faced a substantially higher risk for death and cardiovascular events, compared with patients without hypertrophy on antihypertensive treatment, according to the findings of a study involving 463 patients.
"These results suggest that persistence of left ventricular hypertrophy in a subset of patients with lower achieved blood pressure during treatment may in part explain the lack of benefit seen in hypertensive patients, despite treatment to lower systolic blood pressure," Dr. Peter M. Okin said at the annual meeting of the American College of Cardiology.
Based on these results, it may be necessary to track end-organ damage – in this case, as manifested by ECG left ventricular hypertrophy – in addition to blood pressure to fully assess response to treatment in hypertensive patients. "You can’t just track blood pressure; you need to look at end-organ damage," such as the size of the heart, said Dr. Okin, a cardiologist and professor of medicine at Cornell University in New York.
But currently no evidence exists on the best way to manage patients whose hearts remain enlarged despite blood pressure normalization.
"The data are not there to say you should treat these patients more aggressively," he said in an interview. In fact, an equally plausible approach would be to back off treatment in such patients because of the high hazard they face and the lack of evidence that treatment helps their clinical outcome. Randomized trials must be done to identify the best way to manage these patients, he said.
The analysis Dr. Okin reported came from a subset of patients who were enrolled in the LIFE (Losartan Intervention for End Point Reduction in Hypertension) study, which enrolled 9,193 patients aged 55-80 years with a blood pressure of 160/95 mm Hg to 200/115 mm Hg. The study randomized patients to two different antihypertensive treatment arms, one based primarily on losartan and the control based primarily on atenolol, with a target blood pressure of 140/90 mm Hg or less (Lancet 2002;359:995-1003).
The subgroup that was used for the new analysis included the 463 patients in the study who achieved a systolic blood pressure of 130 mm Hg or less. Their average age was 65 years, and slightly more than half were men. During an average follow-up of more than 4 years, the combined rate of cardiovascular death, MI, or stroke was 15%.
The researchers used data from the 12-lead ECG recordings of these patients, as analyzed by the Cornell product equation and by Sokolow-Lyon voltage to calculate left ventricular size. They considered any patient with a Cornell product greater than 2440 mm x msec to have residual left ventricular hypertrophy. This identified 211 patients (46%) with persistent hypertrophy despite their low achieved systolic blood pressure, and 252 patients without hypertrophy.
Patients with persistent hypertrophy were significantly older (66 years), compared with those without hypertrophy (64 years), and were significantly more likely to be women (53%), compared with the 40% rate of women in the group without hypertrophy. At baseline, the two subgroups had similar average blood pressures, and on treatment the average decline in systolic and diastolic pressures were similar in the two subgroups.
During the average 4.4 years of follow-up, patients with residual hypertrophy had significantly higher rates of MI, strokes, cardiovascular death, and all-cause mortality, as well as a significantly higher rate of the combined end point of MI, stroke, or cardiovascular death, compared with the patients without hypertrophy. (See box.) These significant differences remained after multivariate adjustment for treatment allocation within the study, baseline Framingham risks score, and diastolic blood pressure on treatment.
Dr. Okin said that he receives a financial benefit from GE Medical Systems. The LIFE trial was sponsored by Merck, which markets losartan (Cozaar).
NEW ORLEANS – Hypertensive patients with persistent left ventricular hypertrophy despite normalized blood pressure faced a substantially higher risk for death and cardiovascular events, compared with patients without hypertrophy on antihypertensive treatment, according to the findings of a study involving 463 patients.
"These results suggest that persistence of left ventricular hypertrophy in a subset of patients with lower achieved blood pressure during treatment may in part explain the lack of benefit seen in hypertensive patients, despite treatment to lower systolic blood pressure," Dr. Peter M. Okin said at the annual meeting of the American College of Cardiology.
Based on these results, it may be necessary to track end-organ damage – in this case, as manifested by ECG left ventricular hypertrophy – in addition to blood pressure to fully assess response to treatment in hypertensive patients. "You can’t just track blood pressure; you need to look at end-organ damage," such as the size of the heart, said Dr. Okin, a cardiologist and professor of medicine at Cornell University in New York.
But currently no evidence exists on the best way to manage patients whose hearts remain enlarged despite blood pressure normalization.
"The data are not there to say you should treat these patients more aggressively," he said in an interview. In fact, an equally plausible approach would be to back off treatment in such patients because of the high hazard they face and the lack of evidence that treatment helps their clinical outcome. Randomized trials must be done to identify the best way to manage these patients, he said.
The analysis Dr. Okin reported came from a subset of patients who were enrolled in the LIFE (Losartan Intervention for End Point Reduction in Hypertension) study, which enrolled 9,193 patients aged 55-80 years with a blood pressure of 160/95 mm Hg to 200/115 mm Hg. The study randomized patients to two different antihypertensive treatment arms, one based primarily on losartan and the control based primarily on atenolol, with a target blood pressure of 140/90 mm Hg or less (Lancet 2002;359:995-1003).
The subgroup that was used for the new analysis included the 463 patients in the study who achieved a systolic blood pressure of 130 mm Hg or less. Their average age was 65 years, and slightly more than half were men. During an average follow-up of more than 4 years, the combined rate of cardiovascular death, MI, or stroke was 15%.
The researchers used data from the 12-lead ECG recordings of these patients, as analyzed by the Cornell product equation and by Sokolow-Lyon voltage to calculate left ventricular size. They considered any patient with a Cornell product greater than 2440 mm x msec to have residual left ventricular hypertrophy. This identified 211 patients (46%) with persistent hypertrophy despite their low achieved systolic blood pressure, and 252 patients without hypertrophy.
Patients with persistent hypertrophy were significantly older (66 years), compared with those without hypertrophy (64 years), and were significantly more likely to be women (53%), compared with the 40% rate of women in the group without hypertrophy. At baseline, the two subgroups had similar average blood pressures, and on treatment the average decline in systolic and diastolic pressures were similar in the two subgroups.
During the average 4.4 years of follow-up, patients with residual hypertrophy had significantly higher rates of MI, strokes, cardiovascular death, and all-cause mortality, as well as a significantly higher rate of the combined end point of MI, stroke, or cardiovascular death, compared with the patients without hypertrophy. (See box.) These significant differences remained after multivariate adjustment for treatment allocation within the study, baseline Framingham risks score, and diastolic blood pressure on treatment.
Dr. Okin said that he receives a financial benefit from GE Medical Systems. The LIFE trial was sponsored by Merck, which markets losartan (Cozaar).
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Patients with persistent left ventricular hypertrophy had a threefold higher rate of cardiovascular death, MI, or stroke compared with patients without hypertrophy on treatment.
Data Source: Analysis of 463 patients enrolled in the LIFE hypertension-treatment trial who achieved a systolic blood pressure of 130 mm Hg or less on treatment.
Disclosures: Dr. Okin said that he receives a financial benefit from GE Medical Systems. The LIFE trial was sponsored by Merck, which markets losartan (Cozaar).
New LV Assist Device Shows Benefits in High-Risk PCI Patients
NEW ORLEANS – Introduced to the U.S. market in 2008 as an upgraded alternative to the intra-arterial balloon pump, the Impella 2.5 showed clear signs of better performance in high-risk patients undergoing percutaneous coronary intervention in a multicenter, randomized trial with 447 patients.
But once Impella 2.5 entered the U.S. market, enrollment into the study slowed dramatically. Eventually, researchers stopped the trial substantially short of its enrollment target, and the pivotal study’s primary end point did not show a statistically significant benefit for Impella 2.5.

The trial also ran into a second problem with a major confounding issue: Interventional cardiologists used rotational atherectomy more aggressively in Impella-treated patients. They seemingly were emboldened by the added cardiac support, and Impella-treated patients had an unbalanced rate of adverse effects.
Despite these problems, the trial results showed a role for the Impella device in high-risk, low-cardiac-output patients undergoing PCI (percutaneous coronary intervention), Dr. William O’Neill said at the annual meeting of the American College of Cardiology.
"This device produces superb hemodynamic support during high-risk interventions. It really allows a more complete procedure that leads to fewer late events," said Dr. O’Neill, an interventional cardiologist and executive dean for clinical affairs at the University of Miami. "With these [high-risk] patients, we skate rapidly over thin ice. This device allows us the luxury of taking more time and doing a more complete and safer procedure. I think [that capability] will translate into increased use [of the device] in these high-risk patients."
Experts who heard the trial results were split on their interpretation of the findings.
"This was a negative study. What is driving the differences you see? I don’t understand how to reconcile the results with your conclusion to go ahead [with using] this device," commented Dr. Ron Waksman, director of experimental angioplasty at Washington (D.C.) Hospital Center.
PROTECT II was a prospective, multicenter, randomized, controlled trial of the Impella Recover LP 2.5 system vs. IABP (intra-aortic balloon pump) in patients undergoing nonemergent, high-risk PCI. The trial began in November 2007 at 67 U.S. sites, 4 sites in Canada, and 1 site in the Netherlands. It enrolled patients with either unprotected left main coronary disease and a left ventricular ejection fraction of 35% or less, or patients with triple-vessel coronary disease and an ejection fraction of 30% or less. The primary end point was the 30-day rate of death, MI, stroke, need for repeat revascularization, need for cardiovascular surgery or vascular surgery for limb ischemia, acute renal dysfunction, increased aortic insufficiency, severe hypotension, need for cardiopulmonary resuscitation, ventricular tachycardia, or failure to reopen the target coronaries by PCI.
The patients averaged 67 years old, 80% were men, and 56% had New York Heart Association class III or IV heart failure. Their average Society of Thoracic Surgeons (STS) mortality score was 6, their average SYNTAX (Synergy Between PCI With Taxus and Cardiac Surgery) score was 30, and 63% were considered ineligible for surgery. "The population was "extraordinarily high risk, the most complex patients ever enrolled in a multicenter, randomized, controlled trial, Dr. O’Neill said. There were 447 patients enrolled in PROTECT II before the study’s data and safety monitoring board stopped the trial last December. This number was 70% of the number of patients originally identified as needed to produce a statistically significant result for the primary end point. Enrollment into the study sharply slowed once the Impella device came onto the U.S. market in June 2008.
During PCI, the participating operators generally managed the Impella patients more aggressively. Heparin was given to 94% in the Impella arm and to 82% in the IABP control arm. Rotational atherectomy was performed in 15% of the Impella patients and in 10% of patients in the IABP arm, a statistically significant difference. Also, participating operators used atherectomy more aggressively in the Impella patients, with an average of five atherectomy passes per patient, compared with two passes in the IABP patients.
Although this shift in treatment approach may have ultimately benefited some of the Impella patients, it also "increased the major adverse event rate and confounded the analysis," Dr. O’Neill said. "About 70% of patients treated with atherectomy in the Impella group had an adverse event" – primarily rises in the level of creatine kinase–myoglobin – "compared with about 35% treated with atherectomy in the IABP group," he said in an interview. "It was a procedural imbalance that was hard to control for" in the safety and efficacy analysis.
There was no statistically significant difference for the study’s primary outcome, the combined major adverse event rate in the intention-to-treat analysis at 30 days after treatment, as well as at 90 days after treatment. However, at both time points, patients in the Impella arm showed trends toward lower major adverse events rates. At 30 days, the Impella patients had a 36% rate, compared with a 40% rate in the IABP patients. At 90 days, the rates reached 41% and 50%, respectively.
In the per-protocol analysis, at 30 days the Impella patients had a major adverse event rate of 35%, compared with 43% in the IABP patients, which was not a statistically significant difference. At 90 days, the rates reached 41% and 51% respectively, a difference that was statistically significant.
Dr. O’Neill addressed concerns that the major adverse event measure included many elements of sharply differing clinical importance. "What drove the difference [between the two study arms] was death, myocardial infarction, and need for urgent revascularization – not the small stuff. The real major adverse cardiac events were significantly better" when the Impella device was used, he said in an interview.
An analysis of several prespecified subgroups also highlighted certain types of patients who had significant benefit from the Impella device for the study’s primary end point. Among the 88% of patients in the study who were not treated with rotational atherectomy, the 30-day major adverse event rate reached 30%, compared with 42% in the IABP patients, a statistically significant difference. A significant difference in the primary outcome in favor of the Impella patients also occurred in the subgroup that had an STS mortality score lower than 10.
The results also showed a strong trend toward a better primary outcome in the Impella-treated patients when the analysis excluded the first Impella-treated patient for each operator, a finding that highlighted an important learning curve in using the device, Dr. O’Neill said.
Analysis also showed that the 90-day rate of major adverse events in the Impella patients fell from 48% in 2008 to 39% in 2009 and to 37% in 2010. In contrast, the rate in the IABP patients stayed fairly constant (at 47%-52%) in all 3 years, again highlighting the role of experience with the Impella device in achieving better patient outcomes, he said.
"I think many clinicians will see [from these data] that Impella provides a lot of safety," Dr. O’Neill said.
PROTECT II was sponsored by Abiomed, the company marketing the Impella 2.5 assist device. Dr. O’Neill said that he has been a consultant to Medtronic. Dr. Waksman said that he has been a consultant to or received honoraria from Medtronic Vascular, Abbott Vascular, Biotronik, Merck, and Boston Scientific.
The results that Dr. O’Neill presented support the use of the Impella 2.5 device in certain clinical situations, specifically in extremely high-risk patients who have a low left ventricular ejection fraction and need protection when undergoing multivessel PCI. Having access to this type of adjunctive device is important, especially for high-risk patients. I can see myself using this device in patients similar to those enrolled in PROTECT II.
It’s unfortunate that the trial did not give a definitive answer to the questions posed in the study. The trial was designed as a superiority trial and did not meet its primary end point. The results do not give us a scientific answer on when to use the device because the study stopped early. But studies like this can inform us tremendously on how to manage very high-risk patients. It’s a tremendous effort to undertake the study and find the patients who would benefit from this device.
We saw in the results that physicians who used the Impella device had the confidence to more aggressively use atherectomy. That can’t be proved, but it appears to be so. The higher use of rotational atherectomy resulted in more creatine kinase–myoglobin elevations in that arm, but the Impella group had fewer critically important MIs (defined as a CK-MB rise of more than eight times the upper limit of normal).
Roxana Mehran, M.D., is professor of medicine and director of interventional cardiovascular research at Mount Sinai Medical Center in New York. She said that she has been a consultant to or received honoraria from Cardiva, Ortho-McNeil, Regado, the Medicines Company, Abbott Vascular, AstraZeneca, and Cordis. She has received research grants from Bristol-Myers Squibb and Sanofi-Aventis.
The results that Dr. O’Neill presented support the use of the Impella 2.5 device in certain clinical situations, specifically in extremely high-risk patients who have a low left ventricular ejection fraction and need protection when undergoing multivessel PCI. Having access to this type of adjunctive device is important, especially for high-risk patients. I can see myself using this device in patients similar to those enrolled in PROTECT II.
It’s unfortunate that the trial did not give a definitive answer to the questions posed in the study. The trial was designed as a superiority trial and did not meet its primary end point. The results do not give us a scientific answer on when to use the device because the study stopped early. But studies like this can inform us tremendously on how to manage very high-risk patients. It’s a tremendous effort to undertake the study and find the patients who would benefit from this device.
We saw in the results that physicians who used the Impella device had the confidence to more aggressively use atherectomy. That can’t be proved, but it appears to be so. The higher use of rotational atherectomy resulted in more creatine kinase–myoglobin elevations in that arm, but the Impella group had fewer critically important MIs (defined as a CK-MB rise of more than eight times the upper limit of normal).
Roxana Mehran, M.D., is professor of medicine and director of interventional cardiovascular research at Mount Sinai Medical Center in New York. She said that she has been a consultant to or received honoraria from Cardiva, Ortho-McNeil, Regado, the Medicines Company, Abbott Vascular, AstraZeneca, and Cordis. She has received research grants from Bristol-Myers Squibb and Sanofi-Aventis.
The results that Dr. O’Neill presented support the use of the Impella 2.5 device in certain clinical situations, specifically in extremely high-risk patients who have a low left ventricular ejection fraction and need protection when undergoing multivessel PCI. Having access to this type of adjunctive device is important, especially for high-risk patients. I can see myself using this device in patients similar to those enrolled in PROTECT II.
It’s unfortunate that the trial did not give a definitive answer to the questions posed in the study. The trial was designed as a superiority trial and did not meet its primary end point. The results do not give us a scientific answer on when to use the device because the study stopped early. But studies like this can inform us tremendously on how to manage very high-risk patients. It’s a tremendous effort to undertake the study and find the patients who would benefit from this device.
We saw in the results that physicians who used the Impella device had the confidence to more aggressively use atherectomy. That can’t be proved, but it appears to be so. The higher use of rotational atherectomy resulted in more creatine kinase–myoglobin elevations in that arm, but the Impella group had fewer critically important MIs (defined as a CK-MB rise of more than eight times the upper limit of normal).
Roxana Mehran, M.D., is professor of medicine and director of interventional cardiovascular research at Mount Sinai Medical Center in New York. She said that she has been a consultant to or received honoraria from Cardiva, Ortho-McNeil, Regado, the Medicines Company, Abbott Vascular, AstraZeneca, and Cordis. She has received research grants from Bristol-Myers Squibb and Sanofi-Aventis.
NEW ORLEANS – Introduced to the U.S. market in 2008 as an upgraded alternative to the intra-arterial balloon pump, the Impella 2.5 showed clear signs of better performance in high-risk patients undergoing percutaneous coronary intervention in a multicenter, randomized trial with 447 patients.
But once Impella 2.5 entered the U.S. market, enrollment into the study slowed dramatically. Eventually, researchers stopped the trial substantially short of its enrollment target, and the pivotal study’s primary end point did not show a statistically significant benefit for Impella 2.5.
The trial also ran into a second problem with a major confounding issue: Interventional cardiologists used rotational atherectomy more aggressively in Impella-treated patients. They seemingly were emboldened by the added cardiac support, and Impella-treated patients had an unbalanced rate of adverse effects.
Despite these problems, the trial results showed a role for the Impella device in high-risk, low-cardiac-output patients undergoing PCI (percutaneous coronary intervention), Dr. William O’Neill said at the annual meeting of the American College of Cardiology.
"This device produces superb hemodynamic support during high-risk interventions. It really allows a more complete procedure that leads to fewer late events," said Dr. O’Neill, an interventional cardiologist and executive dean for clinical affairs at the University of Miami. "With these [high-risk] patients, we skate rapidly over thin ice. This device allows us the luxury of taking more time and doing a more complete and safer procedure. I think [that capability] will translate into increased use [of the device] in these high-risk patients."
Experts who heard the trial results were split on their interpretation of the findings.
"This was a negative study. What is driving the differences you see? I don’t understand how to reconcile the results with your conclusion to go ahead [with using] this device," commented Dr. Ron Waksman, director of experimental angioplasty at Washington (D.C.) Hospital Center.
PROTECT II was a prospective, multicenter, randomized, controlled trial of the Impella Recover LP 2.5 system vs. IABP (intra-aortic balloon pump) in patients undergoing nonemergent, high-risk PCI. The trial began in November 2007 at 67 U.S. sites, 4 sites in Canada, and 1 site in the Netherlands. It enrolled patients with either unprotected left main coronary disease and a left ventricular ejection fraction of 35% or less, or patients with triple-vessel coronary disease and an ejection fraction of 30% or less. The primary end point was the 30-day rate of death, MI, stroke, need for repeat revascularization, need for cardiovascular surgery or vascular surgery for limb ischemia, acute renal dysfunction, increased aortic insufficiency, severe hypotension, need for cardiopulmonary resuscitation, ventricular tachycardia, or failure to reopen the target coronaries by PCI.
The patients averaged 67 years old, 80% were men, and 56% had New York Heart Association class III or IV heart failure. Their average Society of Thoracic Surgeons (STS) mortality score was 6, their average SYNTAX (Synergy Between PCI With Taxus and Cardiac Surgery) score was 30, and 63% were considered ineligible for surgery. "The population was "extraordinarily high risk, the most complex patients ever enrolled in a multicenter, randomized, controlled trial, Dr. O’Neill said. There were 447 patients enrolled in PROTECT II before the study’s data and safety monitoring board stopped the trial last December. This number was 70% of the number of patients originally identified as needed to produce a statistically significant result for the primary end point. Enrollment into the study sharply slowed once the Impella device came onto the U.S. market in June 2008.
During PCI, the participating operators generally managed the Impella patients more aggressively. Heparin was given to 94% in the Impella arm and to 82% in the IABP control arm. Rotational atherectomy was performed in 15% of the Impella patients and in 10% of patients in the IABP arm, a statistically significant difference. Also, participating operators used atherectomy more aggressively in the Impella patients, with an average of five atherectomy passes per patient, compared with two passes in the IABP patients.
Although this shift in treatment approach may have ultimately benefited some of the Impella patients, it also "increased the major adverse event rate and confounded the analysis," Dr. O’Neill said. "About 70% of patients treated with atherectomy in the Impella group had an adverse event" – primarily rises in the level of creatine kinase–myoglobin – "compared with about 35% treated with atherectomy in the IABP group," he said in an interview. "It was a procedural imbalance that was hard to control for" in the safety and efficacy analysis.
There was no statistically significant difference for the study’s primary outcome, the combined major adverse event rate in the intention-to-treat analysis at 30 days after treatment, as well as at 90 days after treatment. However, at both time points, patients in the Impella arm showed trends toward lower major adverse events rates. At 30 days, the Impella patients had a 36% rate, compared with a 40% rate in the IABP patients. At 90 days, the rates reached 41% and 50%, respectively.
In the per-protocol analysis, at 30 days the Impella patients had a major adverse event rate of 35%, compared with 43% in the IABP patients, which was not a statistically significant difference. At 90 days, the rates reached 41% and 51% respectively, a difference that was statistically significant.
Dr. O’Neill addressed concerns that the major adverse event measure included many elements of sharply differing clinical importance. "What drove the difference [between the two study arms] was death, myocardial infarction, and need for urgent revascularization – not the small stuff. The real major adverse cardiac events were significantly better" when the Impella device was used, he said in an interview.
An analysis of several prespecified subgroups also highlighted certain types of patients who had significant benefit from the Impella device for the study’s primary end point. Among the 88% of patients in the study who were not treated with rotational atherectomy, the 30-day major adverse event rate reached 30%, compared with 42% in the IABP patients, a statistically significant difference. A significant difference in the primary outcome in favor of the Impella patients also occurred in the subgroup that had an STS mortality score lower than 10.
The results also showed a strong trend toward a better primary outcome in the Impella-treated patients when the analysis excluded the first Impella-treated patient for each operator, a finding that highlighted an important learning curve in using the device, Dr. O’Neill said.
Analysis also showed that the 90-day rate of major adverse events in the Impella patients fell from 48% in 2008 to 39% in 2009 and to 37% in 2010. In contrast, the rate in the IABP patients stayed fairly constant (at 47%-52%) in all 3 years, again highlighting the role of experience with the Impella device in achieving better patient outcomes, he said.
"I think many clinicians will see [from these data] that Impella provides a lot of safety," Dr. O’Neill said.
PROTECT II was sponsored by Abiomed, the company marketing the Impella 2.5 assist device. Dr. O’Neill said that he has been a consultant to Medtronic. Dr. Waksman said that he has been a consultant to or received honoraria from Medtronic Vascular, Abbott Vascular, Biotronik, Merck, and Boston Scientific.
NEW ORLEANS – Introduced to the U.S. market in 2008 as an upgraded alternative to the intra-arterial balloon pump, the Impella 2.5 showed clear signs of better performance in high-risk patients undergoing percutaneous coronary intervention in a multicenter, randomized trial with 447 patients.
But once Impella 2.5 entered the U.S. market, enrollment into the study slowed dramatically. Eventually, researchers stopped the trial substantially short of its enrollment target, and the pivotal study’s primary end point did not show a statistically significant benefit for Impella 2.5.
The trial also ran into a second problem with a major confounding issue: Interventional cardiologists used rotational atherectomy more aggressively in Impella-treated patients. They seemingly were emboldened by the added cardiac support, and Impella-treated patients had an unbalanced rate of adverse effects.
Despite these problems, the trial results showed a role for the Impella device in high-risk, low-cardiac-output patients undergoing PCI (percutaneous coronary intervention), Dr. William O’Neill said at the annual meeting of the American College of Cardiology.
"This device produces superb hemodynamic support during high-risk interventions. It really allows a more complete procedure that leads to fewer late events," said Dr. O’Neill, an interventional cardiologist and executive dean for clinical affairs at the University of Miami. "With these [high-risk] patients, we skate rapidly over thin ice. This device allows us the luxury of taking more time and doing a more complete and safer procedure. I think [that capability] will translate into increased use [of the device] in these high-risk patients."
Experts who heard the trial results were split on their interpretation of the findings.
"This was a negative study. What is driving the differences you see? I don’t understand how to reconcile the results with your conclusion to go ahead [with using] this device," commented Dr. Ron Waksman, director of experimental angioplasty at Washington (D.C.) Hospital Center.
PROTECT II was a prospective, multicenter, randomized, controlled trial of the Impella Recover LP 2.5 system vs. IABP (intra-aortic balloon pump) in patients undergoing nonemergent, high-risk PCI. The trial began in November 2007 at 67 U.S. sites, 4 sites in Canada, and 1 site in the Netherlands. It enrolled patients with either unprotected left main coronary disease and a left ventricular ejection fraction of 35% or less, or patients with triple-vessel coronary disease and an ejection fraction of 30% or less. The primary end point was the 30-day rate of death, MI, stroke, need for repeat revascularization, need for cardiovascular surgery or vascular surgery for limb ischemia, acute renal dysfunction, increased aortic insufficiency, severe hypotension, need for cardiopulmonary resuscitation, ventricular tachycardia, or failure to reopen the target coronaries by PCI.
The patients averaged 67 years old, 80% were men, and 56% had New York Heart Association class III or IV heart failure. Their average Society of Thoracic Surgeons (STS) mortality score was 6, their average SYNTAX (Synergy Between PCI With Taxus and Cardiac Surgery) score was 30, and 63% were considered ineligible for surgery. "The population was "extraordinarily high risk, the most complex patients ever enrolled in a multicenter, randomized, controlled trial, Dr. O’Neill said. There were 447 patients enrolled in PROTECT II before the study’s data and safety monitoring board stopped the trial last December. This number was 70% of the number of patients originally identified as needed to produce a statistically significant result for the primary end point. Enrollment into the study sharply slowed once the Impella device came onto the U.S. market in June 2008.
During PCI, the participating operators generally managed the Impella patients more aggressively. Heparin was given to 94% in the Impella arm and to 82% in the IABP control arm. Rotational atherectomy was performed in 15% of the Impella patients and in 10% of patients in the IABP arm, a statistically significant difference. Also, participating operators used atherectomy more aggressively in the Impella patients, with an average of five atherectomy passes per patient, compared with two passes in the IABP patients.
Although this shift in treatment approach may have ultimately benefited some of the Impella patients, it also "increased the major adverse event rate and confounded the analysis," Dr. O’Neill said. "About 70% of patients treated with atherectomy in the Impella group had an adverse event" – primarily rises in the level of creatine kinase–myoglobin – "compared with about 35% treated with atherectomy in the IABP group," he said in an interview. "It was a procedural imbalance that was hard to control for" in the safety and efficacy analysis.
There was no statistically significant difference for the study’s primary outcome, the combined major adverse event rate in the intention-to-treat analysis at 30 days after treatment, as well as at 90 days after treatment. However, at both time points, patients in the Impella arm showed trends toward lower major adverse events rates. At 30 days, the Impella patients had a 36% rate, compared with a 40% rate in the IABP patients. At 90 days, the rates reached 41% and 50%, respectively.
In the per-protocol analysis, at 30 days the Impella patients had a major adverse event rate of 35%, compared with 43% in the IABP patients, which was not a statistically significant difference. At 90 days, the rates reached 41% and 51% respectively, a difference that was statistically significant.
Dr. O’Neill addressed concerns that the major adverse event measure included many elements of sharply differing clinical importance. "What drove the difference [between the two study arms] was death, myocardial infarction, and need for urgent revascularization – not the small stuff. The real major adverse cardiac events were significantly better" when the Impella device was used, he said in an interview.
An analysis of several prespecified subgroups also highlighted certain types of patients who had significant benefit from the Impella device for the study’s primary end point. Among the 88% of patients in the study who were not treated with rotational atherectomy, the 30-day major adverse event rate reached 30%, compared with 42% in the IABP patients, a statistically significant difference. A significant difference in the primary outcome in favor of the Impella patients also occurred in the subgroup that had an STS mortality score lower than 10.
The results also showed a strong trend toward a better primary outcome in the Impella-treated patients when the analysis excluded the first Impella-treated patient for each operator, a finding that highlighted an important learning curve in using the device, Dr. O’Neill said.
Analysis also showed that the 90-day rate of major adverse events in the Impella patients fell from 48% in 2008 to 39% in 2009 and to 37% in 2010. In contrast, the rate in the IABP patients stayed fairly constant (at 47%-52%) in all 3 years, again highlighting the role of experience with the Impella device in achieving better patient outcomes, he said.
"I think many clinicians will see [from these data] that Impella provides a lot of safety," Dr. O’Neill said.
PROTECT II was sponsored by Abiomed, the company marketing the Impella 2.5 assist device. Dr. O’Neill said that he has been a consultant to Medtronic. Dr. Waksman said that he has been a consultant to or received honoraria from Medtronic Vascular, Abbott Vascular, Biotronik, Merck, and Boston Scientific.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OR CARDIOLOGY
Major Finding: High-risk patients who were aided during PCI with an LVAD (Impella 2.5) had a 41% rate of major adverse events at 90 days, significantly better than the 51% rate seen in patients who were treated with a standard intra-aortic balloon pump. But in the intention-to-treat analysis, outcomes did not differ for the two groups at either 30 days or 90 days.
Data Source: PROTECT II, a randomized trial comparing LV support with the Impella 2.5 device and an intra-aortic balloon pump in 447 patients who were treated at 72 sites worldwide.
Disclosures: PROTECT II was funded by Abiomed, the company that markets the Impella device. Dr. O’Neill said that he has been a consultant to Medtronic. Dr. Mehran said that she has been a consultant to or received honoraria from Cardiva, Ortho-McNeil, Regado, the Medicines Company, Abbott Vascular, AstraZeneca, and Cordis. She has received research grants from Bristol-Myers Squibb and Sanofi-Aventis. Dr. Waksman said that he has been a consultant to or received honoraria from Medtronic Vascular, Abbott Vascular, Biotronik, Merck, and Boston Scientific.