User login
BOSTON – Many female physicians say that if they had to do it over again, they might have tried to have children sooner, chosen a different specialty, or elected to have embryos frozen "just in case" they had later fertility problems, an investigator said at the conjoint meeting of the International Federation of Fertility Societies and the American Society for Reproductive Medicine.
Dr. Natalie A. Clark and her colleagues surveyed a random sample of female physicians in the United States to ask about their choices for timing of conception, their basic knowledge of reproductive limitations, and how reproductive choices factor into their professional and personal decision making. The investigators randomly selected 600 women who graduated from medical school from 1995 through 2000 from the American Medical Association (AMA) physicians’ database, and mailed surveys to them. A total of 333 (55.5%) responded.
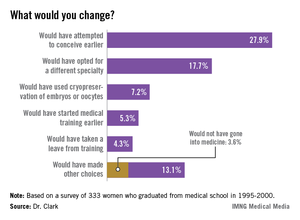
Asked whether they would in retrospect have changed anything about their reproductive choices, 27.9% said they would have attempted to conceive earlier, 17.7% would have opted for a different specialty, 7.2% would have used cryopreservation of embryos or oocytes, 5.3% would have started medical training earlier, and 4.3% would have taken a leave from training. Of the 13.1% who said they would have made other, unspecified choices, 3.6% independently reported that they would not have gone into medicine.
The survey of female physicians highlights the unique challenges that women of childbearing age face when trying to balance the demands of education, training, and career advancement, said Dr. Clark, a third-year resident at the University of Michigan department of obstetrics and gynecology in Ann Arbor.
"We have a number of highly educated patients who come into our clinic who have finished their MDs or PhDs, and have done a great amount of postgraduate work, and they present at very late reproductive ages. They say, "I’m ready to start reproducing, and I don’t want to be too aggressive, but what can I do?’ – not fully realizing that they’ve missed their ideal reproductive window," Dr. Clark said in an interview.
The majority of respondents (55%) work in specialties for women, children, and families, including family medicine, obstetrics and gynecology, and pediatrics; 31% work in other medical specialties; 10% in hospital-based specialties; and 4% in surgical specialties.
In all, 80% of the respondents said they had attempted to conceive, and 77% had at least one biological child. The physicians on average had their first child 7.4 years later than did women in the general population, according to data from the Centers for Disease Control and Prevention.
One-fourth (25%) of all respondents had been diagnosed with infertility. Ovulatory dysfunction was the most common cause, followed by male factor, age-related diminished ovarian reserve, endometriosis, tubal factor, and uterine factor.
"Despite having a medical background, 44% of infertile respondents were surprised about their diagnosis of infertility," Dr. Clark said. In every age range, physicians consistently underestimated their chances for conceiving, she added.
"I think that if we can change the culture of medicine such that we can support those decisions at a biologically advantageous time point, it could change the field of medicine," Dr. Clark said.
The study was supported by a grant from the AMA Joan F. Giambalvo Memorial Scholarship Fund. Dr. Clark was a 2012 recipient of a research award from the fund.
The fact that 25% of physicians have infertility is a slight increase over the percentage of general population (15%), and it reinforces to physicians that they are not immune to the diseases we treat.
The study utilizes graduates from medical school between 1995 and 2000, and it doesn't reflect the working environment that today's graduates face, 13-18 years later. Duty hours, Gen X graduates, and the increasing number of women in medicine, especially in obstetrics and gynecology, have changed the workplace. Residents and young physicians in practice are no longer willing to work the hours that their predecessors did. To me, this is mostly a positive trend, as the desire for work-life balance is something young physicians are teaching older physicians, by example. In my own department, we see many physicians of all ages leading fuller, happier lives because of these changes. That is not to say that being a resident or young physician in practice and being pregnant is easy. It is just more acceptable than it was for the physicians in the study cohort.
 |
| Dr. David Forstein |
As to the option of oocyte freezing early in their career, this option is becoming more and more available to women. We have seen a number of women in their mid- to late 20s, with no partner in place, freeze oocytes "just in case." As the technology improves and allows higher pregnancy rates from unstimulated oocytes, more women will choose this option. Currently, the best pregnancy rates come from frozen embryos, then from oocytes frozen following an ovarian stimulation cycle. The stimulation still requires multiple medication injections, and ultrasound and hormone-level monitoring. These requirements are an additional hurdle for women with busy schedules to navigate.
The cost of an oocyte harvest is significant and not often covered by insurance or, even if it is covered, there are copays and deductibles that make it difficult for residents to manage. This is a challenge to which there are no easy answers.
In my residency program director's role, I have frequently been challenged by resident and attending physicians about what the response to "another pregnant resident" should be. Often frustration ensues amongst the team because a maternity leave stretches the manpower of a program. In my mind, the appropriate response is that as ob.gyns., we should celebrate every pregnancy! If we can't lead by example about how to treat professional women during pregnancy and with their young families, who is going to do it? Respect for the challenge of multitasking a residency or a practice and a family is the way forward.
David Forstein, D.O., is an infertility specialist who is associate professor of obstetrics and gynecology at the University of South Carolina, Greenville. He said he had no financial disclosures relevant to this commentary.
Ob.Gyns. should be leading the way
Regarding this intriguing research performed by Clark and her colleagues, these women physicians had their first child about 7 years later than women in the general population, and just over a quarter of respondents indicated, in retrospect, that they would have attempted to conceive earlier. This paper highlights the bind that professional women often find themselves in - that there is no "ideal" time to have a child.
 |
| Dr. Eve Espey |
Women pursuing professions may be discouraged from childbearing during their education and may hear the message that it is irresponsible to detract from their study time or professional development by having children during their undergraduate education or medical school. During residency, the "system" is not designed to accommodate absences, and fellow residents usually absorb the workload for women taking maternity leave, sometimes leading to resentment and an unspoken bias against childbearing.
Our society is only beginning to accommodate the women who wish to "have it all," both professional fulfillment in a rewarding career and the personal happiness that comes with parenthood.
As women's physicians, ob.gyns. should lead the way in encouraging women professionals to have children whenever during their professional development or careers they see fit, whether that be in college, medical school, residency, or beyond. Because there is no "ideal" time, we should support women in their personal and professional fulfillment, and develop flexible systems that do not punish women for electing to have children at any point in their reproductive lives.
Eve Espey, M.D., is an associate professor of obstetrics and gynecology at the University of New Mexico, Albuquerque. She said she had no financial disclosures relevant to this commentary.
The fact that 25% of physicians have infertility is a slight increase over the percentage of general population (15%), and it reinforces to physicians that they are not immune to the diseases we treat.
The study utilizes graduates from medical school between 1995 and 2000, and it doesn't reflect the working environment that today's graduates face, 13-18 years later. Duty hours, Gen X graduates, and the increasing number of women in medicine, especially in obstetrics and gynecology, have changed the workplace. Residents and young physicians in practice are no longer willing to work the hours that their predecessors did. To me, this is mostly a positive trend, as the desire for work-life balance is something young physicians are teaching older physicians, by example. In my own department, we see many physicians of all ages leading fuller, happier lives because of these changes. That is not to say that being a resident or young physician in practice and being pregnant is easy. It is just more acceptable than it was for the physicians in the study cohort.
|
| Dr. David Forstein |
As to the option of oocyte freezing early in their career, this option is becoming more and more available to women. We have seen a number of women in their mid- to late 20s, with no partner in place, freeze oocytes "just in case." As the technology improves and allows higher pregnancy rates from unstimulated oocytes, more women will choose this option. Currently, the best pregnancy rates come from frozen embryos, then from oocytes frozen following an ovarian stimulation cycle. The stimulation still requires multiple medication injections, and ultrasound and hormone-level monitoring. These requirements are an additional hurdle for women with busy schedules to navigate.
The cost of an oocyte harvest is significant and not often covered by insurance or, even if it is covered, there are copays and deductibles that make it difficult for residents to manage. This is a challenge to which there are no easy answers.
In my residency program director's role, I have frequently been challenged by resident and attending physicians about what the response to "another pregnant resident" should be. Often frustration ensues amongst the team because a maternity leave stretches the manpower of a program. In my mind, the appropriate response is that as ob.gyns., we should celebrate every pregnancy! If we can't lead by example about how to treat professional women during pregnancy and with their young families, who is going to do it? Respect for the challenge of multitasking a residency or a practice and a family is the way forward.
David Forstein, D.O., is an infertility specialist who is associate professor of obstetrics and gynecology at the University of South Carolina, Greenville. He said he had no financial disclosures relevant to this commentary.
Ob.Gyns. should be leading the way
Regarding this intriguing research performed by Clark and her colleagues, these women physicians had their first child about 7 years later than women in the general population, and just over a quarter of respondents indicated, in retrospect, that they would have attempted to conceive earlier. This paper highlights the bind that professional women often find themselves in - that there is no "ideal" time to have a child.
|
| Dr. Eve Espey |
Women pursuing professions may be discouraged from childbearing during their education and may hear the message that it is irresponsible to detract from their study time or professional development by having children during their undergraduate education or medical school. During residency, the "system" is not designed to accommodate absences, and fellow residents usually absorb the workload for women taking maternity leave, sometimes leading to resentment and an unspoken bias against childbearing.
Our society is only beginning to accommodate the women who wish to "have it all," both professional fulfillment in a rewarding career and the personal happiness that comes with parenthood.
As women's physicians, ob.gyns. should lead the way in encouraging women professionals to have children whenever during their professional development or careers they see fit, whether that be in college, medical school, residency, or beyond. Because there is no "ideal" time, we should support women in their personal and professional fulfillment, and develop flexible systems that do not punish women for electing to have children at any point in their reproductive lives.
Eve Espey, M.D., is an associate professor of obstetrics and gynecology at the University of New Mexico, Albuquerque. She said she had no financial disclosures relevant to this commentary.
The fact that 25% of physicians have infertility is a slight increase over the percentage of general population (15%), and it reinforces to physicians that they are not immune to the diseases we treat.
The study utilizes graduates from medical school between 1995 and 2000, and it doesn't reflect the working environment that today's graduates face, 13-18 years later. Duty hours, Gen X graduates, and the increasing number of women in medicine, especially in obstetrics and gynecology, have changed the workplace. Residents and young physicians in practice are no longer willing to work the hours that their predecessors did. To me, this is mostly a positive trend, as the desire for work-life balance is something young physicians are teaching older physicians, by example. In my own department, we see many physicians of all ages leading fuller, happier lives because of these changes. That is not to say that being a resident or young physician in practice and being pregnant is easy. It is just more acceptable than it was for the physicians in the study cohort.
|
| Dr. David Forstein |
As to the option of oocyte freezing early in their career, this option is becoming more and more available to women. We have seen a number of women in their mid- to late 20s, with no partner in place, freeze oocytes "just in case." As the technology improves and allows higher pregnancy rates from unstimulated oocytes, more women will choose this option. Currently, the best pregnancy rates come from frozen embryos, then from oocytes frozen following an ovarian stimulation cycle. The stimulation still requires multiple medication injections, and ultrasound and hormone-level monitoring. These requirements are an additional hurdle for women with busy schedules to navigate.
The cost of an oocyte harvest is significant and not often covered by insurance or, even if it is covered, there are copays and deductibles that make it difficult for residents to manage. This is a challenge to which there are no easy answers.
In my residency program director's role, I have frequently been challenged by resident and attending physicians about what the response to "another pregnant resident" should be. Often frustration ensues amongst the team because a maternity leave stretches the manpower of a program. In my mind, the appropriate response is that as ob.gyns., we should celebrate every pregnancy! If we can't lead by example about how to treat professional women during pregnancy and with their young families, who is going to do it? Respect for the challenge of multitasking a residency or a practice and a family is the way forward.
David Forstein, D.O., is an infertility specialist who is associate professor of obstetrics and gynecology at the University of South Carolina, Greenville. He said he had no financial disclosures relevant to this commentary.
Ob.Gyns. should be leading the way
Regarding this intriguing research performed by Clark and her colleagues, these women physicians had their first child about 7 years later than women in the general population, and just over a quarter of respondents indicated, in retrospect, that they would have attempted to conceive earlier. This paper highlights the bind that professional women often find themselves in - that there is no "ideal" time to have a child.
|
| Dr. Eve Espey |
Women pursuing professions may be discouraged from childbearing during their education and may hear the message that it is irresponsible to detract from their study time or professional development by having children during their undergraduate education or medical school. During residency, the "system" is not designed to accommodate absences, and fellow residents usually absorb the workload for women taking maternity leave, sometimes leading to resentment and an unspoken bias against childbearing.
Our society is only beginning to accommodate the women who wish to "have it all," both professional fulfillment in a rewarding career and the personal happiness that comes with parenthood.
As women's physicians, ob.gyns. should lead the way in encouraging women professionals to have children whenever during their professional development or careers they see fit, whether that be in college, medical school, residency, or beyond. Because there is no "ideal" time, we should support women in their personal and professional fulfillment, and develop flexible systems that do not punish women for electing to have children at any point in their reproductive lives.
Eve Espey, M.D., is an associate professor of obstetrics and gynecology at the University of New Mexico, Albuquerque. She said she had no financial disclosures relevant to this commentary.
BOSTON – Many female physicians say that if they had to do it over again, they might have tried to have children sooner, chosen a different specialty, or elected to have embryos frozen "just in case" they had later fertility problems, an investigator said at the conjoint meeting of the International Federation of Fertility Societies and the American Society for Reproductive Medicine.
Dr. Natalie A. Clark and her colleagues surveyed a random sample of female physicians in the United States to ask about their choices for timing of conception, their basic knowledge of reproductive limitations, and how reproductive choices factor into their professional and personal decision making. The investigators randomly selected 600 women who graduated from medical school from 1995 through 2000 from the American Medical Association (AMA) physicians’ database, and mailed surveys to them. A total of 333 (55.5%) responded.
Asked whether they would in retrospect have changed anything about their reproductive choices, 27.9% said they would have attempted to conceive earlier, 17.7% would have opted for a different specialty, 7.2% would have used cryopreservation of embryos or oocytes, 5.3% would have started medical training earlier, and 4.3% would have taken a leave from training. Of the 13.1% who said they would have made other, unspecified choices, 3.6% independently reported that they would not have gone into medicine.
The survey of female physicians highlights the unique challenges that women of childbearing age face when trying to balance the demands of education, training, and career advancement, said Dr. Clark, a third-year resident at the University of Michigan department of obstetrics and gynecology in Ann Arbor.
"We have a number of highly educated patients who come into our clinic who have finished their MDs or PhDs, and have done a great amount of postgraduate work, and they present at very late reproductive ages. They say, "I’m ready to start reproducing, and I don’t want to be too aggressive, but what can I do?’ – not fully realizing that they’ve missed their ideal reproductive window," Dr. Clark said in an interview.
The majority of respondents (55%) work in specialties for women, children, and families, including family medicine, obstetrics and gynecology, and pediatrics; 31% work in other medical specialties; 10% in hospital-based specialties; and 4% in surgical specialties.
In all, 80% of the respondents said they had attempted to conceive, and 77% had at least one biological child. The physicians on average had their first child 7.4 years later than did women in the general population, according to data from the Centers for Disease Control and Prevention.
One-fourth (25%) of all respondents had been diagnosed with infertility. Ovulatory dysfunction was the most common cause, followed by male factor, age-related diminished ovarian reserve, endometriosis, tubal factor, and uterine factor.
"Despite having a medical background, 44% of infertile respondents were surprised about their diagnosis of infertility," Dr. Clark said. In every age range, physicians consistently underestimated their chances for conceiving, she added.
"I think that if we can change the culture of medicine such that we can support those decisions at a biologically advantageous time point, it could change the field of medicine," Dr. Clark said.
The study was supported by a grant from the AMA Joan F. Giambalvo Memorial Scholarship Fund. Dr. Clark was a 2012 recipient of a research award from the fund.
BOSTON – Many female physicians say that if they had to do it over again, they might have tried to have children sooner, chosen a different specialty, or elected to have embryos frozen "just in case" they had later fertility problems, an investigator said at the conjoint meeting of the International Federation of Fertility Societies and the American Society for Reproductive Medicine.
Dr. Natalie A. Clark and her colleagues surveyed a random sample of female physicians in the United States to ask about their choices for timing of conception, their basic knowledge of reproductive limitations, and how reproductive choices factor into their professional and personal decision making. The investigators randomly selected 600 women who graduated from medical school from 1995 through 2000 from the American Medical Association (AMA) physicians’ database, and mailed surveys to them. A total of 333 (55.5%) responded.
Asked whether they would in retrospect have changed anything about their reproductive choices, 27.9% said they would have attempted to conceive earlier, 17.7% would have opted for a different specialty, 7.2% would have used cryopreservation of embryos or oocytes, 5.3% would have started medical training earlier, and 4.3% would have taken a leave from training. Of the 13.1% who said they would have made other, unspecified choices, 3.6% independently reported that they would not have gone into medicine.
The survey of female physicians highlights the unique challenges that women of childbearing age face when trying to balance the demands of education, training, and career advancement, said Dr. Clark, a third-year resident at the University of Michigan department of obstetrics and gynecology in Ann Arbor.
"We have a number of highly educated patients who come into our clinic who have finished their MDs or PhDs, and have done a great amount of postgraduate work, and they present at very late reproductive ages. They say, "I’m ready to start reproducing, and I don’t want to be too aggressive, but what can I do?’ – not fully realizing that they’ve missed their ideal reproductive window," Dr. Clark said in an interview.
The majority of respondents (55%) work in specialties for women, children, and families, including family medicine, obstetrics and gynecology, and pediatrics; 31% work in other medical specialties; 10% in hospital-based specialties; and 4% in surgical specialties.
In all, 80% of the respondents said they had attempted to conceive, and 77% had at least one biological child. The physicians on average had their first child 7.4 years later than did women in the general population, according to data from the Centers for Disease Control and Prevention.
One-fourth (25%) of all respondents had been diagnosed with infertility. Ovulatory dysfunction was the most common cause, followed by male factor, age-related diminished ovarian reserve, endometriosis, tubal factor, and uterine factor.
"Despite having a medical background, 44% of infertile respondents were surprised about their diagnosis of infertility," Dr. Clark said. In every age range, physicians consistently underestimated their chances for conceiving, she added.
"I think that if we can change the culture of medicine such that we can support those decisions at a biologically advantageous time point, it could change the field of medicine," Dr. Clark said.
The study was supported by a grant from the AMA Joan F. Giambalvo Memorial Scholarship Fund. Dr. Clark was a 2012 recipient of a research award from the fund.
AT THE JOINT IFFS/ASRM MEETING
Major finding: Asked whether they would in retrospect have changed anything about their reproductive choices, 27.9% of female physicians said they would have attempted to conceive earlier, 17.7% would have opted for a different specialty, 7.2% would have used cryopreservation of embryos or oocytes, 5.3% would have started medical training earlier, and 4.3% would have taken a leave from training.
Data source: Mailed survey of 333 U.S. women physicians who graduated from medical school from 1995 through 2000.
Disclosures: The study was supported by a grant from the AMA Joan F. Giambalvo Memorial Scholarship Fund. Dr. Clark was a 2012 recipient of a research award from the fund.
