User login
Danielle Scheurer, MD, MSCR, SFHM, is a hospitalist and the chief quality officer at the Medical University of South Carolina (MUSC) in Charleston. She is former SHM physician advisor, an SHM blogger, and member of SHM's Education Committee. She also serves as faculty of SHM's annual meeting "ABIM Maintenance of Certification (MOC) Learning Session" pre-course. Dr. Scheurer earned her undergraduate degree at Emory University in Atlanta, graduated medical school from the University of Tennessee in Knoxville, and trained at Duke University in Durham, N.C. She has served as physician editor of The Hospitalist since 2012.
HealthKit Wellness App Could Prove Helpful to Hospitalists

The Institute for Healthcare Improvement (IHI) released its Triple Aim Initiative in 2008, challenging the healthcare industry to undergo extensive systematic change, with the following goals:1
- Reduce the per capita cost of healthcare;
- Improve the patient experience of care, including quality and satisfaction; and
- Improve the health of populations.
The first two aims are difficult enough, but the third involves engaging and empowering patients and their families to take ownership of their own health and wellness. This is much more than just understanding what your diagnoses are and which medications to take; it is about getting and staying well. Keeping patients and their families well is a goal that has eluded the healthcare industry since before Hippocrates and is an extremely challenging one for hospitalists, whose time with patients is usually limited to an acute care hospital stay.
Naturally, when one industry cannot figure out how to do something well, another industry will develop a breakthrough innovation. Enter Apple Inc., which has officially moved into the health and wellness business. Apple Health is a new app that will share multiple inputs of patient information in a cloud platform called “HealthKit.” HealthKit will allow a user to view a personalized dashboard of health and fitness metrics, which conglomerates information from a myriad of different health and wellness apps, helping them “communicate” with one another.2
The breadth and choice of health and wellness apps available to users is astounding. In a five-minute browse through the app store on my iPhone, I found the following free options to help patients track and understand their health and wellness:
- MyPlate Calorie Tracker, Calorie Counter, and Fooducate help educate and monitor caloric intake.
- iTriage, WebMD, and Mango Health Medication Manager, which can answer questions about symptoms you may be experiencing, will save a list of medications, conditions, procedures, physicians, appointments, and more, and can help you manage your medications.
- Nexercise, MapMyRun, MapMyRide, MapMyFitness, Pacer, and Health Mate track physical activity.
- Fitness Buddy and Daily Workout allow users to view daily workout options and target muscle groups for appropriate exercises.
- ShopWell allows you to scan food labels and evaluate ingredients, calories, gluten, and so on in most store-bought food products.
What Apple proposes to do with its new HealthKit is coordinate the input of these types of apps to synthesize a patient’s health and wellness onto a single platform, which can be shared with caretakers and healthcare providers as needed. The company, as only Apple can, actually declared that its app might be “the beginning of a health revolution.”
A New Day
What HealthKit offers is truly unique from a data security standpoint, which will appeal to Orwellian paranoids. Traditionally, when customers use services such as Google or Yahoo, these services use your personal identity—gathered in pieces of data such as your location and your browsing histories—and then use that data to collect, store, or sell such information on their terms. But Apple promises to help manage health and wellness data on the users’ terms. The purpose is to enable easy but secure sharing of complex health information, which can be updated by users or by other devices. Apple has coordinated with other developers to import information to HealthKit from multiple platforms and devices (such as Nike+, Withings Scale, and Fitbit Flex), acting as a central repository of personalized information.
With this technology, it’s easy to envision hospitals, clinics, pharmacies, laboratories, and even insurers integrating bilaterally with any patient information housed on HealthKit, at the discretion of the user. Mayo Clinic, Cleveland Clinic, Kaiser Permanente, Stanford, UCLA, and Mount Sinai Hospital are all rumored to be working with Apple to figure out how to exchange relevant patient information to enhance the continuity of a patient’s care. In addition to these potential collaborators, electronic health record providers Epic Systems and Allscripts are rumored to be working with Apple in some sort of partnership.3,4
Not only will HealthKit be a secure repository of information, but it will constantly monitor all the metrics and can be programmed to send alerts to key stakeholders, such as family members or healthcare providers, when any of the metrics veer outside predetermined boundaries.4
This “new revolution” in healthcare and wellness should prove extremely helpful to hospitalists, who are often caught in the crosshairs of disjointed patient care delivery systems, and patients who need someone (or something) to track their health and wellness. Imagine a late afternoon admission of a patient who knows exactly what medications she is taking, who can outline several months’ history of caloric intake, physical activity, and basic vital signs, who has an accurate and updated inventory of laboratory exams from other medical centers, and who has a list of all recent physicians and appointments. Although this may seem too good to be true, such an admission may not be too far in the future.
What would be even better is if a patient’s health and wellness tracking keeps him out of the hospital altogether. After all, an Apple a day keeps the doctors away.

Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Institute for Healthcare Improvement. IHI Triple Aim Initiative. Available at: http://www.ihi.org/Engage/Initiatives/TripleAim/Pages/default.aspx. Accessed August 31, 2014.
- Apple Inc. Healthkit information page. Available at: https://developer.apple.com/healthkit/. Accessed August 31, 2014.
- The Advisory Board Company. Daily Briefing: Apple in talks with top hospitals to become ‘hub of health data.’ Available at: http://www.advisory.com/daily-briefing/2014/08/12/apple-in-talks-with-top-hospitals-to-become-hub-of-health-data. Accessed August 31, 2014.
- Sullivan M. VentureBeat News. Apple announces HealthKit platform and new health app. Available at: http://venturebeat.com/2014/06/02/apple-announces-heath-kit-platform-and-health-app/. Accessed August 31, 2014.
The Institute for Healthcare Improvement (IHI) released its Triple Aim Initiative in 2008, challenging the healthcare industry to undergo extensive systematic change, with the following goals:1
- Reduce the per capita cost of healthcare;
- Improve the patient experience of care, including quality and satisfaction; and
- Improve the health of populations.
The first two aims are difficult enough, but the third involves engaging and empowering patients and their families to take ownership of their own health and wellness. This is much more than just understanding what your diagnoses are and which medications to take; it is about getting and staying well. Keeping patients and their families well is a goal that has eluded the healthcare industry since before Hippocrates and is an extremely challenging one for hospitalists, whose time with patients is usually limited to an acute care hospital stay.
Naturally, when one industry cannot figure out how to do something well, another industry will develop a breakthrough innovation. Enter Apple Inc., which has officially moved into the health and wellness business. Apple Health is a new app that will share multiple inputs of patient information in a cloud platform called “HealthKit.” HealthKit will allow a user to view a personalized dashboard of health and fitness metrics, which conglomerates information from a myriad of different health and wellness apps, helping them “communicate” with one another.2
The breadth and choice of health and wellness apps available to users is astounding. In a five-minute browse through the app store on my iPhone, I found the following free options to help patients track and understand their health and wellness:
- MyPlate Calorie Tracker, Calorie Counter, and Fooducate help educate and monitor caloric intake.
- iTriage, WebMD, and Mango Health Medication Manager, which can answer questions about symptoms you may be experiencing, will save a list of medications, conditions, procedures, physicians, appointments, and more, and can help you manage your medications.
- Nexercise, MapMyRun, MapMyRide, MapMyFitness, Pacer, and Health Mate track physical activity.
- Fitness Buddy and Daily Workout allow users to view daily workout options and target muscle groups for appropriate exercises.
- ShopWell allows you to scan food labels and evaluate ingredients, calories, gluten, and so on in most store-bought food products.
What Apple proposes to do with its new HealthKit is coordinate the input of these types of apps to synthesize a patient’s health and wellness onto a single platform, which can be shared with caretakers and healthcare providers as needed. The company, as only Apple can, actually declared that its app might be “the beginning of a health revolution.”
A New Day
What HealthKit offers is truly unique from a data security standpoint, which will appeal to Orwellian paranoids. Traditionally, when customers use services such as Google or Yahoo, these services use your personal identity—gathered in pieces of data such as your location and your browsing histories—and then use that data to collect, store, or sell such information on their terms. But Apple promises to help manage health and wellness data on the users’ terms. The purpose is to enable easy but secure sharing of complex health information, which can be updated by users or by other devices. Apple has coordinated with other developers to import information to HealthKit from multiple platforms and devices (such as Nike+, Withings Scale, and Fitbit Flex), acting as a central repository of personalized information.
With this technology, it’s easy to envision hospitals, clinics, pharmacies, laboratories, and even insurers integrating bilaterally with any patient information housed on HealthKit, at the discretion of the user. Mayo Clinic, Cleveland Clinic, Kaiser Permanente, Stanford, UCLA, and Mount Sinai Hospital are all rumored to be working with Apple to figure out how to exchange relevant patient information to enhance the continuity of a patient’s care. In addition to these potential collaborators, electronic health record providers Epic Systems and Allscripts are rumored to be working with Apple in some sort of partnership.3,4
Not only will HealthKit be a secure repository of information, but it will constantly monitor all the metrics and can be programmed to send alerts to key stakeholders, such as family members or healthcare providers, when any of the metrics veer outside predetermined boundaries.4
This “new revolution” in healthcare and wellness should prove extremely helpful to hospitalists, who are often caught in the crosshairs of disjointed patient care delivery systems, and patients who need someone (or something) to track their health and wellness. Imagine a late afternoon admission of a patient who knows exactly what medications she is taking, who can outline several months’ history of caloric intake, physical activity, and basic vital signs, who has an accurate and updated inventory of laboratory exams from other medical centers, and who has a list of all recent physicians and appointments. Although this may seem too good to be true, such an admission may not be too far in the future.
What would be even better is if a patient’s health and wellness tracking keeps him out of the hospital altogether. After all, an Apple a day keeps the doctors away.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Institute for Healthcare Improvement. IHI Triple Aim Initiative. Available at: http://www.ihi.org/Engage/Initiatives/TripleAim/Pages/default.aspx. Accessed August 31, 2014.
- Apple Inc. Healthkit information page. Available at: https://developer.apple.com/healthkit/. Accessed August 31, 2014.
- The Advisory Board Company. Daily Briefing: Apple in talks with top hospitals to become ‘hub of health data.’ Available at: http://www.advisory.com/daily-briefing/2014/08/12/apple-in-talks-with-top-hospitals-to-become-hub-of-health-data. Accessed August 31, 2014.
- Sullivan M. VentureBeat News. Apple announces HealthKit platform and new health app. Available at: http://venturebeat.com/2014/06/02/apple-announces-heath-kit-platform-and-health-app/. Accessed August 31, 2014.
The Institute for Healthcare Improvement (IHI) released its Triple Aim Initiative in 2008, challenging the healthcare industry to undergo extensive systematic change, with the following goals:1
- Reduce the per capita cost of healthcare;
- Improve the patient experience of care, including quality and satisfaction; and
- Improve the health of populations.
The first two aims are difficult enough, but the third involves engaging and empowering patients and their families to take ownership of their own health and wellness. This is much more than just understanding what your diagnoses are and which medications to take; it is about getting and staying well. Keeping patients and their families well is a goal that has eluded the healthcare industry since before Hippocrates and is an extremely challenging one for hospitalists, whose time with patients is usually limited to an acute care hospital stay.
Naturally, when one industry cannot figure out how to do something well, another industry will develop a breakthrough innovation. Enter Apple Inc., which has officially moved into the health and wellness business. Apple Health is a new app that will share multiple inputs of patient information in a cloud platform called “HealthKit.” HealthKit will allow a user to view a personalized dashboard of health and fitness metrics, which conglomerates information from a myriad of different health and wellness apps, helping them “communicate” with one another.2
The breadth and choice of health and wellness apps available to users is astounding. In a five-minute browse through the app store on my iPhone, I found the following free options to help patients track and understand their health and wellness:
- MyPlate Calorie Tracker, Calorie Counter, and Fooducate help educate and monitor caloric intake.
- iTriage, WebMD, and Mango Health Medication Manager, which can answer questions about symptoms you may be experiencing, will save a list of medications, conditions, procedures, physicians, appointments, and more, and can help you manage your medications.
- Nexercise, MapMyRun, MapMyRide, MapMyFitness, Pacer, and Health Mate track physical activity.
- Fitness Buddy and Daily Workout allow users to view daily workout options and target muscle groups for appropriate exercises.
- ShopWell allows you to scan food labels and evaluate ingredients, calories, gluten, and so on in most store-bought food products.
What Apple proposes to do with its new HealthKit is coordinate the input of these types of apps to synthesize a patient’s health and wellness onto a single platform, which can be shared with caretakers and healthcare providers as needed. The company, as only Apple can, actually declared that its app might be “the beginning of a health revolution.”
A New Day
What HealthKit offers is truly unique from a data security standpoint, which will appeal to Orwellian paranoids. Traditionally, when customers use services such as Google or Yahoo, these services use your personal identity—gathered in pieces of data such as your location and your browsing histories—and then use that data to collect, store, or sell such information on their terms. But Apple promises to help manage health and wellness data on the users’ terms. The purpose is to enable easy but secure sharing of complex health information, which can be updated by users or by other devices. Apple has coordinated with other developers to import information to HealthKit from multiple platforms and devices (such as Nike+, Withings Scale, and Fitbit Flex), acting as a central repository of personalized information.
With this technology, it’s easy to envision hospitals, clinics, pharmacies, laboratories, and even insurers integrating bilaterally with any patient information housed on HealthKit, at the discretion of the user. Mayo Clinic, Cleveland Clinic, Kaiser Permanente, Stanford, UCLA, and Mount Sinai Hospital are all rumored to be working with Apple to figure out how to exchange relevant patient information to enhance the continuity of a patient’s care. In addition to these potential collaborators, electronic health record providers Epic Systems and Allscripts are rumored to be working with Apple in some sort of partnership.3,4
Not only will HealthKit be a secure repository of information, but it will constantly monitor all the metrics and can be programmed to send alerts to key stakeholders, such as family members or healthcare providers, when any of the metrics veer outside predetermined boundaries.4
This “new revolution” in healthcare and wellness should prove extremely helpful to hospitalists, who are often caught in the crosshairs of disjointed patient care delivery systems, and patients who need someone (or something) to track their health and wellness. Imagine a late afternoon admission of a patient who knows exactly what medications she is taking, who can outline several months’ history of caloric intake, physical activity, and basic vital signs, who has an accurate and updated inventory of laboratory exams from other medical centers, and who has a list of all recent physicians and appointments. Although this may seem too good to be true, such an admission may not be too far in the future.
What would be even better is if a patient’s health and wellness tracking keeps him out of the hospital altogether. After all, an Apple a day keeps the doctors away.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Institute for Healthcare Improvement. IHI Triple Aim Initiative. Available at: http://www.ihi.org/Engage/Initiatives/TripleAim/Pages/default.aspx. Accessed August 31, 2014.
- Apple Inc. Healthkit information page. Available at: https://developer.apple.com/healthkit/. Accessed August 31, 2014.
- The Advisory Board Company. Daily Briefing: Apple in talks with top hospitals to become ‘hub of health data.’ Available at: http://www.advisory.com/daily-briefing/2014/08/12/apple-in-talks-with-top-hospitals-to-become-hub-of-health-data. Accessed August 31, 2014.
- Sullivan M. VentureBeat News. Apple announces HealthKit platform and new health app. Available at: http://venturebeat.com/2014/06/02/apple-announces-heath-kit-platform-and-health-app/. Accessed August 31, 2014.
Medicare Billing Practices More Transparent as CMS Cracks Down on Overchargers

The U.S. Department of Health and Human Services (HHS) is putting forth stricter interventions and penalties aimed at curbing acts of careless billing by physicians it refers to as “recalcitrant providers.” Webster’s defines recalcitrant as “obstinately defiant of authority or restraint…difficult to manage or operate.” According to Medicare, these “recalcitrants” are providers who routinely and repeatedly overcharge for services billed through Medicare, despite proper training on how to bill appropriately for these services.1
Medicare has long battled the issue of finding and curbing overcharging and overpayment. CMS estimates that such defiance accounts for up to $6 billion a year in unnecessary Medicare costs, which makes up about 10% of all physician fee payments, given the fact that total Medicare Part B payments are about $65 billion a year.2
Medicare has systems in place to prevent, detect, and/or mitigate improper payments, whether they result from mistakes or from intentional fraud. In 2011, CMS’ Center for Program Integrity implemented sophisticated technology, called the Fraud Prevention System (FPS), which uses predictive analytics to detect provider irregularities warranting further inspection. According to their 2012 report, the FPS generated 536 new investigations, assisted in providing additional information for 511 active investigations, and initiated thousands of verification interviews of beneficiaries and providers to validate the legitimate receipt of services and items. The center estimates that in the first year of this program, FPS prevented about $115 million in payments.3
So what is Medicare’s response to providers who are identified as outliers? For overpayments from mistakes, CMS generally aims to recover the overpayments and educate the providers. Tactics range from educational letters and phone calls to on-site reviews and “prepayment medical reviews.” For fraud, on the other hand, Medicare (obviously) pursues more disciplinary sanctions, including criminal or civil penalties.
A New Paradigm
Now CMS is stepping up its expectations of provider accountability, adding heftier penalties for infractions, including higher financial penalties and even expulsion from Medicare, Medicaid, and other federal programs. In addition to these disciplinary actions, the agency plans to utilize recently changed laws to maximize public transparency around provider billing practices.
As of March 2014, Medicare will be able to publicly report all federal payments that have been paid out to individual providers. Although it has not yet disclosed how or when these will be reported, CMS now has the authority, for the first time since 1979, to display this information publicly. The history on this topic is that a federal district judge in Florida in 1979 prohibited the disclosure of individual payments to physicians, based on the contention that such disclosure would be an invasion of physician privacy. This longstanding mandate, which was reversed in May 2012, now allows Medicare to weigh the risks and benefits of individual requests for information on charges/payments by individual physicians. According to a New York Times article, Medicare is now being pressured by advocacy groups (insurers, employers, consumers) to release as much of the data as possible, to aid in data dissection and analysis and prompt early identification of abusive providers.4
Understandably, many physician advocacy groups, such as the American Medical Association, are concerned that such unfiltered access to this raw data may lead to inaccurate and unnecessary conclusions about physician practice and billing patterns.
The good news is that the federal government currently estimates that the recalcitrant provider list comprises a relatively small group of providers, roughly 300 or so. Some of these providers have received up to $3 million in Medicare payments a year. They estimate that, overall, about 2% of total Medicare licensed providers charged 25% of total payments, and that the total volume of these high-charging outliers increased by 78% between the years 2008 to 2011. A 2009 audit found that more than half of these recalcitrants were internists; other “high offenders” were ophthalmology and radiation oncology.
The list of these particular high-outlier offenders will be turned over to the Office of the Inspector General (OIG) at HHS to impose the appropriate degree of penalty. Then the federal government will determine an appropriate process of “screening” for providers that may meet the criteria for penalties and will start with those at the highest levels of cumulative payments. The OIG acknowledges that high payments do not necessarily imply fraud or abuse but believes it is reasonable to start there when analyzing and investigating potential areas of fraud or abuse.
Transparency Is Coming
So, while it is not exactly clear when or how the data will be released, what is clear is that the federal government has been granted the authority to dissect and release the data as it sees fit, opening up a new era of transparency in pricing, cost, charges, billing, and payments.
This change should affect all types of providers that bill Medicare part B, including hospitalists and other physicians, as well as nurse practitioners and physical therapists.5 While this is likely to cause some degree of discomfort and generate many questions from the public, hospitalists should be willing to embrace such transparency and engage in the dialogue needed to help the lay public understand the data. Most hospitalists work in practices that routinely share their data about billing, at least among the group, if not with a larger audience.
This is just one of many examples of how transparency can and should identify those providers considered “recalcitrant” in a number of realms, including patient satisfaction, quality, utilization, or cost. And, similar to other publicly reported “metrics,” release of this data will likely generate more questions than answers in the short run. In the long run, we should all be prepared for the release of data that is coming, one that will usher us into a whole new era of transparency.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. CMS Manual System. Pub 100-08 Medicare program integrity. December 13, 2013. Available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R495PI.pdf. Accessed April 6, 2014.
- Levinson DR. Department of Health and Human Services. Office of Inspector General. Reviews of clinicians associated with high cumulative payments could improve Medicare program integrity efforts. December 2013. Available at: http://oig.hhs.gov/oas/reports/region1/11100511.pdf. Accessed April 6, 2014.
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. Report to Congress: fraud prevention system—first implementation year, 2012. Available at: http://www.stopmedicarefraud.gov/fraud-rtc12142012.pdf. Accessed April 6, 2014.
- Pear R. Doctors abusing Medicare face fines and expulsion. January 25, 2014. The New York Times website. Available at: http://www.nytimes.com/2014/01/26/us/doctors-abusing-medicare-to-face-fines.html. Accessed April 6, 2014.
- Steinbrook R. Public disclosure of Medicare payments to individual physicians. The Journal of the American Medical Association website. April 2, 2014. Available at: http://jama.jamanetwork.com/article.aspx?articleID=1832217&utm_source=Silverchair%20Information%20Systems&utm_medium=email&utm_campaign=JAMA%3AOnlineFirst02%2F17%2F2014. Accessed April 6,
2014.
The U.S. Department of Health and Human Services (HHS) is putting forth stricter interventions and penalties aimed at curbing acts of careless billing by physicians it refers to as “recalcitrant providers.” Webster’s defines recalcitrant as “obstinately defiant of authority or restraint…difficult to manage or operate.” According to Medicare, these “recalcitrants” are providers who routinely and repeatedly overcharge for services billed through Medicare, despite proper training on how to bill appropriately for these services.1
Medicare has long battled the issue of finding and curbing overcharging and overpayment. CMS estimates that such defiance accounts for up to $6 billion a year in unnecessary Medicare costs, which makes up about 10% of all physician fee payments, given the fact that total Medicare Part B payments are about $65 billion a year.2
Medicare has systems in place to prevent, detect, and/or mitigate improper payments, whether they result from mistakes or from intentional fraud. In 2011, CMS’ Center for Program Integrity implemented sophisticated technology, called the Fraud Prevention System (FPS), which uses predictive analytics to detect provider irregularities warranting further inspection. According to their 2012 report, the FPS generated 536 new investigations, assisted in providing additional information for 511 active investigations, and initiated thousands of verification interviews of beneficiaries and providers to validate the legitimate receipt of services and items. The center estimates that in the first year of this program, FPS prevented about $115 million in payments.3
So what is Medicare’s response to providers who are identified as outliers? For overpayments from mistakes, CMS generally aims to recover the overpayments and educate the providers. Tactics range from educational letters and phone calls to on-site reviews and “prepayment medical reviews.” For fraud, on the other hand, Medicare (obviously) pursues more disciplinary sanctions, including criminal or civil penalties.
A New Paradigm
Now CMS is stepping up its expectations of provider accountability, adding heftier penalties for infractions, including higher financial penalties and even expulsion from Medicare, Medicaid, and other federal programs. In addition to these disciplinary actions, the agency plans to utilize recently changed laws to maximize public transparency around provider billing practices.
As of March 2014, Medicare will be able to publicly report all federal payments that have been paid out to individual providers. Although it has not yet disclosed how or when these will be reported, CMS now has the authority, for the first time since 1979, to display this information publicly. The history on this topic is that a federal district judge in Florida in 1979 prohibited the disclosure of individual payments to physicians, based on the contention that such disclosure would be an invasion of physician privacy. This longstanding mandate, which was reversed in May 2012, now allows Medicare to weigh the risks and benefits of individual requests for information on charges/payments by individual physicians. According to a New York Times article, Medicare is now being pressured by advocacy groups (insurers, employers, consumers) to release as much of the data as possible, to aid in data dissection and analysis and prompt early identification of abusive providers.4
Understandably, many physician advocacy groups, such as the American Medical Association, are concerned that such unfiltered access to this raw data may lead to inaccurate and unnecessary conclusions about physician practice and billing patterns.
The good news is that the federal government currently estimates that the recalcitrant provider list comprises a relatively small group of providers, roughly 300 or so. Some of these providers have received up to $3 million in Medicare payments a year. They estimate that, overall, about 2% of total Medicare licensed providers charged 25% of total payments, and that the total volume of these high-charging outliers increased by 78% between the years 2008 to 2011. A 2009 audit found that more than half of these recalcitrants were internists; other “high offenders” were ophthalmology and radiation oncology.
The list of these particular high-outlier offenders will be turned over to the Office of the Inspector General (OIG) at HHS to impose the appropriate degree of penalty. Then the federal government will determine an appropriate process of “screening” for providers that may meet the criteria for penalties and will start with those at the highest levels of cumulative payments. The OIG acknowledges that high payments do not necessarily imply fraud or abuse but believes it is reasonable to start there when analyzing and investigating potential areas of fraud or abuse.
Transparency Is Coming
So, while it is not exactly clear when or how the data will be released, what is clear is that the federal government has been granted the authority to dissect and release the data as it sees fit, opening up a new era of transparency in pricing, cost, charges, billing, and payments.
This change should affect all types of providers that bill Medicare part B, including hospitalists and other physicians, as well as nurse practitioners and physical therapists.5 While this is likely to cause some degree of discomfort and generate many questions from the public, hospitalists should be willing to embrace such transparency and engage in the dialogue needed to help the lay public understand the data. Most hospitalists work in practices that routinely share their data about billing, at least among the group, if not with a larger audience.
This is just one of many examples of how transparency can and should identify those providers considered “recalcitrant” in a number of realms, including patient satisfaction, quality, utilization, or cost. And, similar to other publicly reported “metrics,” release of this data will likely generate more questions than answers in the short run. In the long run, we should all be prepared for the release of data that is coming, one that will usher us into a whole new era of transparency.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. CMS Manual System. Pub 100-08 Medicare program integrity. December 13, 2013. Available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R495PI.pdf. Accessed April 6, 2014.
- Levinson DR. Department of Health and Human Services. Office of Inspector General. Reviews of clinicians associated with high cumulative payments could improve Medicare program integrity efforts. December 2013. Available at: http://oig.hhs.gov/oas/reports/region1/11100511.pdf. Accessed April 6, 2014.
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. Report to Congress: fraud prevention system—first implementation year, 2012. Available at: http://www.stopmedicarefraud.gov/fraud-rtc12142012.pdf. Accessed April 6, 2014.
- Pear R. Doctors abusing Medicare face fines and expulsion. January 25, 2014. The New York Times website. Available at: http://www.nytimes.com/2014/01/26/us/doctors-abusing-medicare-to-face-fines.html. Accessed April 6, 2014.
- Steinbrook R. Public disclosure of Medicare payments to individual physicians. The Journal of the American Medical Association website. April 2, 2014. Available at: http://jama.jamanetwork.com/article.aspx?articleID=1832217&utm_source=Silverchair%20Information%20Systems&utm_medium=email&utm_campaign=JAMA%3AOnlineFirst02%2F17%2F2014. Accessed April 6,
2014.
The U.S. Department of Health and Human Services (HHS) is putting forth stricter interventions and penalties aimed at curbing acts of careless billing by physicians it refers to as “recalcitrant providers.” Webster’s defines recalcitrant as “obstinately defiant of authority or restraint…difficult to manage or operate.” According to Medicare, these “recalcitrants” are providers who routinely and repeatedly overcharge for services billed through Medicare, despite proper training on how to bill appropriately for these services.1
Medicare has long battled the issue of finding and curbing overcharging and overpayment. CMS estimates that such defiance accounts for up to $6 billion a year in unnecessary Medicare costs, which makes up about 10% of all physician fee payments, given the fact that total Medicare Part B payments are about $65 billion a year.2
Medicare has systems in place to prevent, detect, and/or mitigate improper payments, whether they result from mistakes or from intentional fraud. In 2011, CMS’ Center for Program Integrity implemented sophisticated technology, called the Fraud Prevention System (FPS), which uses predictive analytics to detect provider irregularities warranting further inspection. According to their 2012 report, the FPS generated 536 new investigations, assisted in providing additional information for 511 active investigations, and initiated thousands of verification interviews of beneficiaries and providers to validate the legitimate receipt of services and items. The center estimates that in the first year of this program, FPS prevented about $115 million in payments.3
So what is Medicare’s response to providers who are identified as outliers? For overpayments from mistakes, CMS generally aims to recover the overpayments and educate the providers. Tactics range from educational letters and phone calls to on-site reviews and “prepayment medical reviews.” For fraud, on the other hand, Medicare (obviously) pursues more disciplinary sanctions, including criminal or civil penalties.
A New Paradigm
Now CMS is stepping up its expectations of provider accountability, adding heftier penalties for infractions, including higher financial penalties and even expulsion from Medicare, Medicaid, and other federal programs. In addition to these disciplinary actions, the agency plans to utilize recently changed laws to maximize public transparency around provider billing practices.
As of March 2014, Medicare will be able to publicly report all federal payments that have been paid out to individual providers. Although it has not yet disclosed how or when these will be reported, CMS now has the authority, for the first time since 1979, to display this information publicly. The history on this topic is that a federal district judge in Florida in 1979 prohibited the disclosure of individual payments to physicians, based on the contention that such disclosure would be an invasion of physician privacy. This longstanding mandate, which was reversed in May 2012, now allows Medicare to weigh the risks and benefits of individual requests for information on charges/payments by individual physicians. According to a New York Times article, Medicare is now being pressured by advocacy groups (insurers, employers, consumers) to release as much of the data as possible, to aid in data dissection and analysis and prompt early identification of abusive providers.4
Understandably, many physician advocacy groups, such as the American Medical Association, are concerned that such unfiltered access to this raw data may lead to inaccurate and unnecessary conclusions about physician practice and billing patterns.
The good news is that the federal government currently estimates that the recalcitrant provider list comprises a relatively small group of providers, roughly 300 or so. Some of these providers have received up to $3 million in Medicare payments a year. They estimate that, overall, about 2% of total Medicare licensed providers charged 25% of total payments, and that the total volume of these high-charging outliers increased by 78% between the years 2008 to 2011. A 2009 audit found that more than half of these recalcitrants were internists; other “high offenders” were ophthalmology and radiation oncology.
The list of these particular high-outlier offenders will be turned over to the Office of the Inspector General (OIG) at HHS to impose the appropriate degree of penalty. Then the federal government will determine an appropriate process of “screening” for providers that may meet the criteria for penalties and will start with those at the highest levels of cumulative payments. The OIG acknowledges that high payments do not necessarily imply fraud or abuse but believes it is reasonable to start there when analyzing and investigating potential areas of fraud or abuse.
Transparency Is Coming
So, while it is not exactly clear when or how the data will be released, what is clear is that the federal government has been granted the authority to dissect and release the data as it sees fit, opening up a new era of transparency in pricing, cost, charges, billing, and payments.
This change should affect all types of providers that bill Medicare part B, including hospitalists and other physicians, as well as nurse practitioners and physical therapists.5 While this is likely to cause some degree of discomfort and generate many questions from the public, hospitalists should be willing to embrace such transparency and engage in the dialogue needed to help the lay public understand the data. Most hospitalists work in practices that routinely share their data about billing, at least among the group, if not with a larger audience.
This is just one of many examples of how transparency can and should identify those providers considered “recalcitrant” in a number of realms, including patient satisfaction, quality, utilization, or cost. And, similar to other publicly reported “metrics,” release of this data will likely generate more questions than answers in the short run. In the long run, we should all be prepared for the release of data that is coming, one that will usher us into a whole new era of transparency.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. CMS Manual System. Pub 100-08 Medicare program integrity. December 13, 2013. Available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R495PI.pdf. Accessed April 6, 2014.
- Levinson DR. Department of Health and Human Services. Office of Inspector General. Reviews of clinicians associated with high cumulative payments could improve Medicare program integrity efforts. December 2013. Available at: http://oig.hhs.gov/oas/reports/region1/11100511.pdf. Accessed April 6, 2014.
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. Report to Congress: fraud prevention system—first implementation year, 2012. Available at: http://www.stopmedicarefraud.gov/fraud-rtc12142012.pdf. Accessed April 6, 2014.
- Pear R. Doctors abusing Medicare face fines and expulsion. January 25, 2014. The New York Times website. Available at: http://www.nytimes.com/2014/01/26/us/doctors-abusing-medicare-to-face-fines.html. Accessed April 6, 2014.
- Steinbrook R. Public disclosure of Medicare payments to individual physicians. The Journal of the American Medical Association website. April 2, 2014. Available at: http://jama.jamanetwork.com/article.aspx?articleID=1832217&utm_source=Silverchair%20Information%20Systems&utm_medium=email&utm_campaign=JAMA%3AOnlineFirst02%2F17%2F2014. Accessed April 6,
2014.
Why Hospitalists Should Heed Choosing Wisely Recommendations

By now, most hospitalists are at least familiar with the Choosing Wisely campaign, which has been widely published and embraced by numerous medical societies, including the Society of Hospital Medicine.1 This campaign was conceived in 2009 by the National Physicians Alliance, which developed simple lists for three primary care specialties—internal medicine, pediatrics, and family medicine—to help them become more effective in utilizing specific resources.
The effort was first published in the Archives of Internal Medicine in 2011 by the “Good Stewardship Working Group,” which outlined the five most overutilized types of care by the three groups, including items such as routinely ordering complete blood counts or electrocardiograms, prescribing brand name versus generic statin drugs, and prescribing antibiotics for pediatric pharyngitis. From this small list alone, they found incredible variability among primary care practices, with utilization of these services ranging from 1% to 56% and resulting in an estimated annual cost of $6.8 billion. Although this first pilot found simple reductions in utilization can have a powerful impact on cost, the group estimated that this overutilization in primary care is only a very small fraction of overutilization cost in the U.S. As such, they called upon other specialties outside of primary care to identify their own sets of targets to reduce unnecessary utilization of low-value services.
Many specialty groups heeded this call to action, which resulted in the Choosing Wisely campaign, launched in April 2012. In just two short years, this simple effort has expanded to published recommendations about resource use in more than 60 specialty societies.2 Like the original primary care list, most recommendations have focused on overutilization of diagnostic testing (imaging, cardiac testing, labs, pathology) and medication use. Later this year, the campaign will expand to include non-physician provider organizations, including the American Dental Association, the American Physical Therapy Association, and the American Academy of Nursing.
The Next Phase
The program has evolved from asking specialty groups to develop consensus and abide by their lists to targeting patients and their families so that they can understand and abide by those same lists. In fact, one of the major aims of the campaign is empowering patients to insist on care that is evidence based, necessary, not duplicative, and more beneficial than harmful. To do this, Consumer Reports has partnered up with the Choosing Wisely campaign to develop patient-friendly educational materials and with multiple consumer groups to help these materials reach their target audience. Major funding for the project has been provided by the American Board of Internal Medicine (ABIM) Foundation and the Robert Wood Johnson Foundation (RWJF). So far, they have awarded 21 projects.
These grants have been awarded to medical societies (see “SHM Choosing Wisely Case Study Competition,” p. 4), regional health organizations, and consumer advocate groups. Many of the tactics will include educational campaigns to teach practitioners about the content of the recommendations, programs aimed to enhance physician communication skills geared toward practicing physicians, other educational campaigns geared toward patients and families, and the establishment of a learning network to assist practices in quickly and effectively learning from one another how to implement the various recommendations.3
The three major assets of the Choosing Wisely campaign are:
- It attacks a core issue within the medical industry: Healthcare costs are higher here than in any other industrialized nation in the world, without clear evidence of higher quality to justify that cost;
- The lists are created by those who are responsible for most of the spending; and
- The campaign is spending resources to get information to the patients and their families so that there will be bilateral exchange and acceptance of the recommendations.
Without widespread patient education, overutilization will likely continue; a recent survey sponsored by the Choosing Wisely campaign found about half of physicians admitted they would order a test they know is unnecessary if the patient is insistent.4
Variable Outcomes
While there are many reasons to celebrate the success of the campaign, there is some concern that the Choosing Wisely campaign may have unintended consequences. Although a major driver in the success of the program is the fact that the lists have been created and endorsed by physician societies, a sort of “self-governance,” with no influence or impact from payers, critics of the program note the variability that each list has on the actual practice or revenue of the physician groups enacting the lists.
For example, a recent New England Journal of Medicine (NEJM) essay notes that the list produced by the American Academy of Orthopedic Surgeons does not include procedures that are high volume and variably valuable (such as knee arthoplasty) but does include over-the-counter medication use and low-volume procedures (such as needle lavage for knee osteoarthritis).5 Some societies list specialty services that need to be curbed but neglect to mention their own.
And, although the campaign specifically states on its website that the “recommendations should not be used to establish coverage decisions or exclusions,” some are legitimately concerned that these Choosing Wisely lists might very well be used by payers and/or quality reporting bodies to determine payments. This is undeniably tempting: How can practitioners argue against public display and reimbursement schemes being tightly tethered to their performance on metrics that they themselves have deemed unnecessary? As the NEJM editorial summarizes, these efforts should be embraced as long as there is thoughtful discussion about inclusion criteria, exclusion criteria, and measurement beforehand.5
In Sum
Despite concerns, the impact of the Choosing Wisely campaign has been widespread and impressive. The full extent to which this will have an impact on utilization and healthcare cost remains to be seen, but this yeoman’s attempt to reduce waste by providers is long overdue. Whether the program will be used for unintended purposes, such as public reporting, financial penalties, or incentives for performance, is still unknown, but physician groups should be paying close attention to the lists that we can impact, and we should pledge to be good stewards of the finite healthcare resources available to our patients.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Choosing Wisely Campaign. Available at: http://www.choosingwisely.org. Accessed May 11, 2014.
- Choosing Wisely Consumer Partners. Available at: http://www.choosingwisely.org/partners. Access May 11, 2014.
- Choosing Wisely Grantees. Available at: http://www.choosingwisely.org/grantees. Accessed May 11, 2014.
- Choosing Wisely & Consumer Reports. Available at: http://consumerhealthchoices.org/wp-content/uploads/2014/03/ChoosingWiselyAndConsumerHealthChoices.pdf. Accessed May 11, 2014.
- Morden ME, Colla CH, Sequist TD, Rosenthal MB. Choosing Wisely—the politics and economics of labeling low-value services. Available at: http://www.nejm.org/doi/full/10.1056/NEJMp1314965. Accessed May 11, 2014.
By now, most hospitalists are at least familiar with the Choosing Wisely campaign, which has been widely published and embraced by numerous medical societies, including the Society of Hospital Medicine.1 This campaign was conceived in 2009 by the National Physicians Alliance, which developed simple lists for three primary care specialties—internal medicine, pediatrics, and family medicine—to help them become more effective in utilizing specific resources.
The effort was first published in the Archives of Internal Medicine in 2011 by the “Good Stewardship Working Group,” which outlined the five most overutilized types of care by the three groups, including items such as routinely ordering complete blood counts or electrocardiograms, prescribing brand name versus generic statin drugs, and prescribing antibiotics for pediatric pharyngitis. From this small list alone, they found incredible variability among primary care practices, with utilization of these services ranging from 1% to 56% and resulting in an estimated annual cost of $6.8 billion. Although this first pilot found simple reductions in utilization can have a powerful impact on cost, the group estimated that this overutilization in primary care is only a very small fraction of overutilization cost in the U.S. As such, they called upon other specialties outside of primary care to identify their own sets of targets to reduce unnecessary utilization of low-value services.
Many specialty groups heeded this call to action, which resulted in the Choosing Wisely campaign, launched in April 2012. In just two short years, this simple effort has expanded to published recommendations about resource use in more than 60 specialty societies.2 Like the original primary care list, most recommendations have focused on overutilization of diagnostic testing (imaging, cardiac testing, labs, pathology) and medication use. Later this year, the campaign will expand to include non-physician provider organizations, including the American Dental Association, the American Physical Therapy Association, and the American Academy of Nursing.
The Next Phase
The program has evolved from asking specialty groups to develop consensus and abide by their lists to targeting patients and their families so that they can understand and abide by those same lists. In fact, one of the major aims of the campaign is empowering patients to insist on care that is evidence based, necessary, not duplicative, and more beneficial than harmful. To do this, Consumer Reports has partnered up with the Choosing Wisely campaign to develop patient-friendly educational materials and with multiple consumer groups to help these materials reach their target audience. Major funding for the project has been provided by the American Board of Internal Medicine (ABIM) Foundation and the Robert Wood Johnson Foundation (RWJF). So far, they have awarded 21 projects.
These grants have been awarded to medical societies (see “SHM Choosing Wisely Case Study Competition,” p. 4), regional health organizations, and consumer advocate groups. Many of the tactics will include educational campaigns to teach practitioners about the content of the recommendations, programs aimed to enhance physician communication skills geared toward practicing physicians, other educational campaigns geared toward patients and families, and the establishment of a learning network to assist practices in quickly and effectively learning from one another how to implement the various recommendations.3
The three major assets of the Choosing Wisely campaign are:
- It attacks a core issue within the medical industry: Healthcare costs are higher here than in any other industrialized nation in the world, without clear evidence of higher quality to justify that cost;
- The lists are created by those who are responsible for most of the spending; and
- The campaign is spending resources to get information to the patients and their families so that there will be bilateral exchange and acceptance of the recommendations.
Without widespread patient education, overutilization will likely continue; a recent survey sponsored by the Choosing Wisely campaign found about half of physicians admitted they would order a test they know is unnecessary if the patient is insistent.4
Variable Outcomes
While there are many reasons to celebrate the success of the campaign, there is some concern that the Choosing Wisely campaign may have unintended consequences. Although a major driver in the success of the program is the fact that the lists have been created and endorsed by physician societies, a sort of “self-governance,” with no influence or impact from payers, critics of the program note the variability that each list has on the actual practice or revenue of the physician groups enacting the lists.
For example, a recent New England Journal of Medicine (NEJM) essay notes that the list produced by the American Academy of Orthopedic Surgeons does not include procedures that are high volume and variably valuable (such as knee arthoplasty) but does include over-the-counter medication use and low-volume procedures (such as needle lavage for knee osteoarthritis).5 Some societies list specialty services that need to be curbed but neglect to mention their own.
And, although the campaign specifically states on its website that the “recommendations should not be used to establish coverage decisions or exclusions,” some are legitimately concerned that these Choosing Wisely lists might very well be used by payers and/or quality reporting bodies to determine payments. This is undeniably tempting: How can practitioners argue against public display and reimbursement schemes being tightly tethered to their performance on metrics that they themselves have deemed unnecessary? As the NEJM editorial summarizes, these efforts should be embraced as long as there is thoughtful discussion about inclusion criteria, exclusion criteria, and measurement beforehand.5
In Sum
Despite concerns, the impact of the Choosing Wisely campaign has been widespread and impressive. The full extent to which this will have an impact on utilization and healthcare cost remains to be seen, but this yeoman’s attempt to reduce waste by providers is long overdue. Whether the program will be used for unintended purposes, such as public reporting, financial penalties, or incentives for performance, is still unknown, but physician groups should be paying close attention to the lists that we can impact, and we should pledge to be good stewards of the finite healthcare resources available to our patients.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Choosing Wisely Campaign. Available at: http://www.choosingwisely.org. Accessed May 11, 2014.
- Choosing Wisely Consumer Partners. Available at: http://www.choosingwisely.org/partners. Access May 11, 2014.
- Choosing Wisely Grantees. Available at: http://www.choosingwisely.org/grantees. Accessed May 11, 2014.
- Choosing Wisely & Consumer Reports. Available at: http://consumerhealthchoices.org/wp-content/uploads/2014/03/ChoosingWiselyAndConsumerHealthChoices.pdf. Accessed May 11, 2014.
- Morden ME, Colla CH, Sequist TD, Rosenthal MB. Choosing Wisely—the politics and economics of labeling low-value services. Available at: http://www.nejm.org/doi/full/10.1056/NEJMp1314965. Accessed May 11, 2014.
By now, most hospitalists are at least familiar with the Choosing Wisely campaign, which has been widely published and embraced by numerous medical societies, including the Society of Hospital Medicine.1 This campaign was conceived in 2009 by the National Physicians Alliance, which developed simple lists for three primary care specialties—internal medicine, pediatrics, and family medicine—to help them become more effective in utilizing specific resources.
The effort was first published in the Archives of Internal Medicine in 2011 by the “Good Stewardship Working Group,” which outlined the five most overutilized types of care by the three groups, including items such as routinely ordering complete blood counts or electrocardiograms, prescribing brand name versus generic statin drugs, and prescribing antibiotics for pediatric pharyngitis. From this small list alone, they found incredible variability among primary care practices, with utilization of these services ranging from 1% to 56% and resulting in an estimated annual cost of $6.8 billion. Although this first pilot found simple reductions in utilization can have a powerful impact on cost, the group estimated that this overutilization in primary care is only a very small fraction of overutilization cost in the U.S. As such, they called upon other specialties outside of primary care to identify their own sets of targets to reduce unnecessary utilization of low-value services.
Many specialty groups heeded this call to action, which resulted in the Choosing Wisely campaign, launched in April 2012. In just two short years, this simple effort has expanded to published recommendations about resource use in more than 60 specialty societies.2 Like the original primary care list, most recommendations have focused on overutilization of diagnostic testing (imaging, cardiac testing, labs, pathology) and medication use. Later this year, the campaign will expand to include non-physician provider organizations, including the American Dental Association, the American Physical Therapy Association, and the American Academy of Nursing.
The Next Phase
The program has evolved from asking specialty groups to develop consensus and abide by their lists to targeting patients and their families so that they can understand and abide by those same lists. In fact, one of the major aims of the campaign is empowering patients to insist on care that is evidence based, necessary, not duplicative, and more beneficial than harmful. To do this, Consumer Reports has partnered up with the Choosing Wisely campaign to develop patient-friendly educational materials and with multiple consumer groups to help these materials reach their target audience. Major funding for the project has been provided by the American Board of Internal Medicine (ABIM) Foundation and the Robert Wood Johnson Foundation (RWJF). So far, they have awarded 21 projects.
These grants have been awarded to medical societies (see “SHM Choosing Wisely Case Study Competition,” p. 4), regional health organizations, and consumer advocate groups. Many of the tactics will include educational campaigns to teach practitioners about the content of the recommendations, programs aimed to enhance physician communication skills geared toward practicing physicians, other educational campaigns geared toward patients and families, and the establishment of a learning network to assist practices in quickly and effectively learning from one another how to implement the various recommendations.3
The three major assets of the Choosing Wisely campaign are:
- It attacks a core issue within the medical industry: Healthcare costs are higher here than in any other industrialized nation in the world, without clear evidence of higher quality to justify that cost;
- The lists are created by those who are responsible for most of the spending; and
- The campaign is spending resources to get information to the patients and their families so that there will be bilateral exchange and acceptance of the recommendations.
Without widespread patient education, overutilization will likely continue; a recent survey sponsored by the Choosing Wisely campaign found about half of physicians admitted they would order a test they know is unnecessary if the patient is insistent.4
Variable Outcomes
While there are many reasons to celebrate the success of the campaign, there is some concern that the Choosing Wisely campaign may have unintended consequences. Although a major driver in the success of the program is the fact that the lists have been created and endorsed by physician societies, a sort of “self-governance,” with no influence or impact from payers, critics of the program note the variability that each list has on the actual practice or revenue of the physician groups enacting the lists.
For example, a recent New England Journal of Medicine (NEJM) essay notes that the list produced by the American Academy of Orthopedic Surgeons does not include procedures that are high volume and variably valuable (such as knee arthoplasty) but does include over-the-counter medication use and low-volume procedures (such as needle lavage for knee osteoarthritis).5 Some societies list specialty services that need to be curbed but neglect to mention their own.
And, although the campaign specifically states on its website that the “recommendations should not be used to establish coverage decisions or exclusions,” some are legitimately concerned that these Choosing Wisely lists might very well be used by payers and/or quality reporting bodies to determine payments. This is undeniably tempting: How can practitioners argue against public display and reimbursement schemes being tightly tethered to their performance on metrics that they themselves have deemed unnecessary? As the NEJM editorial summarizes, these efforts should be embraced as long as there is thoughtful discussion about inclusion criteria, exclusion criteria, and measurement beforehand.5
In Sum
Despite concerns, the impact of the Choosing Wisely campaign has been widespread and impressive. The full extent to which this will have an impact on utilization and healthcare cost remains to be seen, but this yeoman’s attempt to reduce waste by providers is long overdue. Whether the program will be used for unintended purposes, such as public reporting, financial penalties, or incentives for performance, is still unknown, but physician groups should be paying close attention to the lists that we can impact, and we should pledge to be good stewards of the finite healthcare resources available to our patients.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Choosing Wisely Campaign. Available at: http://www.choosingwisely.org. Accessed May 11, 2014.
- Choosing Wisely Consumer Partners. Available at: http://www.choosingwisely.org/partners. Access May 11, 2014.
- Choosing Wisely Grantees. Available at: http://www.choosingwisely.org/grantees. Accessed May 11, 2014.
- Choosing Wisely & Consumer Reports. Available at: http://consumerhealthchoices.org/wp-content/uploads/2014/03/ChoosingWiselyAndConsumerHealthChoices.pdf. Accessed May 11, 2014.
- Morden ME, Colla CH, Sequist TD, Rosenthal MB. Choosing Wisely—the politics and economics of labeling low-value services. Available at: http://www.nejm.org/doi/full/10.1056/NEJMp1314965. Accessed May 11, 2014.
MERS Cases Put Hospitalists on Alert for Infectious Disease
Patients diagnosed with Middle East Respiratory Syndrome (MERS) in Indiana and Florida have healthcare workers and hospitalists on the lookout for additional cases of the potentially fatal respiratory infection.
Hospitalists should pay attention to patients exhibiting fever and respiratory symptoms who traveled to the Arabian Peninsula in the 14 days prior to disease onset, and contact the hospital epidemiologist if MERS is suspected, says James Pile, MD, vice chair of the department of hospital medicine at the Cleveland Clinic.
The CDC has reported three cases of MERS this month. The first, reported on May 2, involved a healthcare worker from Saudi Arabia who traveled to Indiana to visit family. The second was reported on May 11, when another visiting healthcare worker from Saudi Arabia checked into the emergency department in Orlando, Fla., after he fell ill with fever, chills, and a slight cough. Both patients are considered to be fully recovered.
The third MERS case is in an Illinois man who had a business meeting with the patient from Indiana and represents the first case of the virus being contracted in the U.S. A blood test confirmed that the Illinois man had been infected with the virus, but he’s reported that he no longer feels sick.
Caused by a coronavirus called MERS-CoV, MERS was first reported in Saudi Arabia in 2012. So far, there have been more than 600 confirmed cases around the world and 181 people have died, according to the World Health Organization.
"The CDC suggests that the index U.S. case represents a very low threat to the general population in this country, and my sense is that that this will not turn out to be a major issue for the U.S. healthcare system, but there’s still a lot we don’t know about MERS," Dr. Pile says. “The scope of the issue should become much clearer over the next couple of months.”
For more information on MERS, check out this CDC fact sheet.
Read physician editor Danielle Scheurer's recent blog post on the MERS situation.
Visit our website for more information about hospitalists and infectious disease care.
Patients diagnosed with Middle East Respiratory Syndrome (MERS) in Indiana and Florida have healthcare workers and hospitalists on the lookout for additional cases of the potentially fatal respiratory infection.
Hospitalists should pay attention to patients exhibiting fever and respiratory symptoms who traveled to the Arabian Peninsula in the 14 days prior to disease onset, and contact the hospital epidemiologist if MERS is suspected, says James Pile, MD, vice chair of the department of hospital medicine at the Cleveland Clinic.
The CDC has reported three cases of MERS this month. The first, reported on May 2, involved a healthcare worker from Saudi Arabia who traveled to Indiana to visit family. The second was reported on May 11, when another visiting healthcare worker from Saudi Arabia checked into the emergency department in Orlando, Fla., after he fell ill with fever, chills, and a slight cough. Both patients are considered to be fully recovered.
The third MERS case is in an Illinois man who had a business meeting with the patient from Indiana and represents the first case of the virus being contracted in the U.S. A blood test confirmed that the Illinois man had been infected with the virus, but he’s reported that he no longer feels sick.
Caused by a coronavirus called MERS-CoV, MERS was first reported in Saudi Arabia in 2012. So far, there have been more than 600 confirmed cases around the world and 181 people have died, according to the World Health Organization.
"The CDC suggests that the index U.S. case represents a very low threat to the general population in this country, and my sense is that that this will not turn out to be a major issue for the U.S. healthcare system, but there’s still a lot we don’t know about MERS," Dr. Pile says. “The scope of the issue should become much clearer over the next couple of months.”
For more information on MERS, check out this CDC fact sheet.
Read physician editor Danielle Scheurer's recent blog post on the MERS situation.
Visit our website for more information about hospitalists and infectious disease care.
Patients diagnosed with Middle East Respiratory Syndrome (MERS) in Indiana and Florida have healthcare workers and hospitalists on the lookout for additional cases of the potentially fatal respiratory infection.
Hospitalists should pay attention to patients exhibiting fever and respiratory symptoms who traveled to the Arabian Peninsula in the 14 days prior to disease onset, and contact the hospital epidemiologist if MERS is suspected, says James Pile, MD, vice chair of the department of hospital medicine at the Cleveland Clinic.
The CDC has reported three cases of MERS this month. The first, reported on May 2, involved a healthcare worker from Saudi Arabia who traveled to Indiana to visit family. The second was reported on May 11, when another visiting healthcare worker from Saudi Arabia checked into the emergency department in Orlando, Fla., after he fell ill with fever, chills, and a slight cough. Both patients are considered to be fully recovered.
The third MERS case is in an Illinois man who had a business meeting with the patient from Indiana and represents the first case of the virus being contracted in the U.S. A blood test confirmed that the Illinois man had been infected with the virus, but he’s reported that he no longer feels sick.
Caused by a coronavirus called MERS-CoV, MERS was first reported in Saudi Arabia in 2012. So far, there have been more than 600 confirmed cases around the world and 181 people have died, according to the World Health Organization.
"The CDC suggests that the index U.S. case represents a very low threat to the general population in this country, and my sense is that that this will not turn out to be a major issue for the U.S. healthcare system, but there’s still a lot we don’t know about MERS," Dr. Pile says. “The scope of the issue should become much clearer over the next couple of months.”
For more information on MERS, check out this CDC fact sheet.
Read physician editor Danielle Scheurer's recent blog post on the MERS situation.
Visit our website for more information about hospitalists and infectious disease care.
Hospitalists Can Help Bridge Gaps in Healthcare Access as Hospitals Cope with Mounting Financial Pressures

There has been a fair amount of media coverage lately about “medical deserts.”1 What exactly is a medical desert, and how big of a problem do they pose for hospital medicine? Wikipedia defines a desert as “a barren area of land where little precipitation occurs and consequently living conditions are hostile for plant and animal life.”2 There are definitely areas in the U.S., both urban and rural, lacking adequate emergency and inpatient medical care.
Based on the latest American Hospital Association (AHA) statistics, there are still >5,700 registered hospitals in the U.S. with almost one million staffed beds combined, which accommodate >36 million admissions every year.3 However, of all U.S. hospitals, only about 35% are located in rural areas, and these tend to be the ones most likely affected by declining reimbursements and tight operating margins.1
Here is some evidence:
— A recent study in the Annals of Emergency Medicine found that only half of the population in the state of Pennsylvania had access to appropriate care within 60 minutes for four time-sensitive conditions (i.e., STEMI, stroke, septic shock, and cardiac arrest).4
— Another study from the Office of Rural Health Policy estimates that approximately 20% of all residential areas do not have rapid access to an acute care medical facility.1
— A recent online story about medical deserts described the devastating case of an 18-month-old girl who died of asphyxiation when a grape became lodged in her throat; their local county’s only hospital with an emergency room had closed months earlier, leaving the closest ED more than 20 miles away.1 This particular hospital, Shelby Regional Medical Center, was a 54-bed hospital in Center, Texas, which suddenly closed in July 2013 amid allegations of fraud from CMS. In addition, a nearby 49-bed Texas hospital (Renaissance Hospital Groves), owned and operated by the same company, had closed in May 2013.
But the list of hospital closures in the past year goes on:
- Lakeside Memorial Hospital in Brockport, N.Y. (61-bed hospital);
- Earl K. Long Medical Center in Baton Rouge, La. (116-bed hospital);
- Stewart-Webster Hospital in Richland, Ga. (25-bed, critical access hospital);
- Calhoun Memorial Hospital in Arlington, Ga. (85-bed hospital);
- Charlton Memorial Hospital in Folkston, Ga. (25-bed hospital);
- The Los Angeles-based Pacific Health Corporation closed all four of its hospitals in California: Anaheim General Hospital (142 beds), Bellflower Medical Center (142 beds), Los Angeles Metropolitan Medical Center (212 beds), and Newport Specialty Hospital (177 beds).
As the CEO of Calhoun Memorial Hospital stated at the closure of his hospital: “It’s a sad day for the community it’s just a sign of the times.”5
Staff, Service Reductions
These hospital closures do not even start to address the nearly ubiquitous reductions in staff and services that many hospitals are resorting to, including workforce reductions experienced by many high-profile academic medical centers like Wake Forest, Denver Health, Emory Health, and Vanderbilt University Medical Centers. According to the Bureau of Labor Statistics, hospitals cut 4,400 jobs in July 2013 alone, while the U.S. overall added 162,000 jobs.1
These acute medical care deserts are primarily a result of declining reimbursements from Medicare and Medicaid, combined with a lack of newly insured Americans, a group that was expected to increase at a much faster pace than it has. The introduction of high-dollar withholds tethered to pay-for-performance programs, such as value-based purchasing and readmission reduction penalties, has also contributed to the financial instability in some hospitals.
In addition, the reduction in disproportionate share hospital (DSH) payments has occurred long before any substantial increase in funded patients through the Affordable Care Act health exchanges. Particularly hard-hit are hospitals in the states that have still elected not to expand Medicaid (primarily in the Southeast and Midwest). And forecasters have every reason to believe that these medical deserts will expand, unless limping hospitals are merged and/or acquired by larger hospital systems.
Should You Be Concerned?
These statistics probably should raise some concern for hospitalists and hospital medicine groups, as the number of hospital-employed physicians is already relatively high (26% according to a recent survey) and rises every year, including an increase of 6% from 2012 to 2013 alone.6 In order to survive in these tenuous conditions, healthcare systems, including hospitalists, will have to be much more involved in the “spectrum of care,” including population health, as opposed to only being involved in discrete acute care episodes. There undoubtedly will be a heavy reliance on telemedicine, seamless electronic medical records, and alternative treatment settings to bridge the gap between medical oases and medical deserts. All of these acute medical care extensions will very likely involve hospitalists.
For the most part, as long as the specialty of hospital medicine keeps its ear to the ground on what is coming, ensuring that we can all be flexible and responsive in meeting the needs of the population we serve, our specialty will be prepped and ready for the “sign of the times.” That way, even when medical deserts do appear, they are not “hostile for life” but are reasonably connected to a suitable oasis.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Williams JP. What happens when a town’s only hospital shuts down? U.S. News and World Report online. November 8, 2013. Available at: http://health.usnews.com/health-news/hospital-of-tomorrow/articles/2013/11/08/what-happens-when-the-only-hospital-closes. Accessed March 5, 2014.
- Wikipedia. Desert. Available at: http://en.wikipedia.org/wiki/Desert. Accessed March 5, 2014.
- American Hospital Association. Fast facts on U.S. hospitals. Available at: http://www.aha.org/research/rc/stat-studies/fast-facts.shtml. Accessed March 5, 2014.
- Salhi RA, Edwards JM, Gaieski DF, Band RA, Abella BS, Carr BG. Access to Care for patients with time-sensitive conditions in Pennsylvania [published online ahead of print December 21, 2013]. Ann Emerg Med.
- Parks JM. Calhoun Memorial Hospital shuts down. Albany Herald online. February 4, 2013. Available at: http://www.albanyherald.com/news/2013/feb/04/calhoun-memorial-hospital-shuts-down. Accessed March 5, 2014.
- Vaidya A. Survey: number of hospital-employed physicians up 6%. Becker’s Hospital Review online. June 18, 2013. Available at: http://www.beckershospitalreview.com/hospital-physician-relationships/survey-number-of-hospital-employed-physicians-up-6.html. Accessed March 5, 2014.
There has been a fair amount of media coverage lately about “medical deserts.”1 What exactly is a medical desert, and how big of a problem do they pose for hospital medicine? Wikipedia defines a desert as “a barren area of land where little precipitation occurs and consequently living conditions are hostile for plant and animal life.”2 There are definitely areas in the U.S., both urban and rural, lacking adequate emergency and inpatient medical care.
Based on the latest American Hospital Association (AHA) statistics, there are still >5,700 registered hospitals in the U.S. with almost one million staffed beds combined, which accommodate >36 million admissions every year.3 However, of all U.S. hospitals, only about 35% are located in rural areas, and these tend to be the ones most likely affected by declining reimbursements and tight operating margins.1
Here is some evidence:
— A recent study in the Annals of Emergency Medicine found that only half of the population in the state of Pennsylvania had access to appropriate care within 60 minutes for four time-sensitive conditions (i.e., STEMI, stroke, septic shock, and cardiac arrest).4
— Another study from the Office of Rural Health Policy estimates that approximately 20% of all residential areas do not have rapid access to an acute care medical facility.1
— A recent online story about medical deserts described the devastating case of an 18-month-old girl who died of asphyxiation when a grape became lodged in her throat; their local county’s only hospital with an emergency room had closed months earlier, leaving the closest ED more than 20 miles away.1 This particular hospital, Shelby Regional Medical Center, was a 54-bed hospital in Center, Texas, which suddenly closed in July 2013 amid allegations of fraud from CMS. In addition, a nearby 49-bed Texas hospital (Renaissance Hospital Groves), owned and operated by the same company, had closed in May 2013.
But the list of hospital closures in the past year goes on:
- Lakeside Memorial Hospital in Brockport, N.Y. (61-bed hospital);
- Earl K. Long Medical Center in Baton Rouge, La. (116-bed hospital);
- Stewart-Webster Hospital in Richland, Ga. (25-bed, critical access hospital);
- Calhoun Memorial Hospital in Arlington, Ga. (85-bed hospital);
- Charlton Memorial Hospital in Folkston, Ga. (25-bed hospital);
- The Los Angeles-based Pacific Health Corporation closed all four of its hospitals in California: Anaheim General Hospital (142 beds), Bellflower Medical Center (142 beds), Los Angeles Metropolitan Medical Center (212 beds), and Newport Specialty Hospital (177 beds).
As the CEO of Calhoun Memorial Hospital stated at the closure of his hospital: “It’s a sad day for the community it’s just a sign of the times.”5
Staff, Service Reductions
These hospital closures do not even start to address the nearly ubiquitous reductions in staff and services that many hospitals are resorting to, including workforce reductions experienced by many high-profile academic medical centers like Wake Forest, Denver Health, Emory Health, and Vanderbilt University Medical Centers. According to the Bureau of Labor Statistics, hospitals cut 4,400 jobs in July 2013 alone, while the U.S. overall added 162,000 jobs.1
These acute medical care deserts are primarily a result of declining reimbursements from Medicare and Medicaid, combined with a lack of newly insured Americans, a group that was expected to increase at a much faster pace than it has. The introduction of high-dollar withholds tethered to pay-for-performance programs, such as value-based purchasing and readmission reduction penalties, has also contributed to the financial instability in some hospitals.
In addition, the reduction in disproportionate share hospital (DSH) payments has occurred long before any substantial increase in funded patients through the Affordable Care Act health exchanges. Particularly hard-hit are hospitals in the states that have still elected not to expand Medicaid (primarily in the Southeast and Midwest). And forecasters have every reason to believe that these medical deserts will expand, unless limping hospitals are merged and/or acquired by larger hospital systems.
Should You Be Concerned?
These statistics probably should raise some concern for hospitalists and hospital medicine groups, as the number of hospital-employed physicians is already relatively high (26% according to a recent survey) and rises every year, including an increase of 6% from 2012 to 2013 alone.6 In order to survive in these tenuous conditions, healthcare systems, including hospitalists, will have to be much more involved in the “spectrum of care,” including population health, as opposed to only being involved in discrete acute care episodes. There undoubtedly will be a heavy reliance on telemedicine, seamless electronic medical records, and alternative treatment settings to bridge the gap between medical oases and medical deserts. All of these acute medical care extensions will very likely involve hospitalists.
For the most part, as long as the specialty of hospital medicine keeps its ear to the ground on what is coming, ensuring that we can all be flexible and responsive in meeting the needs of the population we serve, our specialty will be prepped and ready for the “sign of the times.” That way, even when medical deserts do appear, they are not “hostile for life” but are reasonably connected to a suitable oasis.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Williams JP. What happens when a town’s only hospital shuts down? U.S. News and World Report online. November 8, 2013. Available at: http://health.usnews.com/health-news/hospital-of-tomorrow/articles/2013/11/08/what-happens-when-the-only-hospital-closes. Accessed March 5, 2014.
- Wikipedia. Desert. Available at: http://en.wikipedia.org/wiki/Desert. Accessed March 5, 2014.
- American Hospital Association. Fast facts on U.S. hospitals. Available at: http://www.aha.org/research/rc/stat-studies/fast-facts.shtml. Accessed March 5, 2014.
- Salhi RA, Edwards JM, Gaieski DF, Band RA, Abella BS, Carr BG. Access to Care for patients with time-sensitive conditions in Pennsylvania [published online ahead of print December 21, 2013]. Ann Emerg Med.
- Parks JM. Calhoun Memorial Hospital shuts down. Albany Herald online. February 4, 2013. Available at: http://www.albanyherald.com/news/2013/feb/04/calhoun-memorial-hospital-shuts-down. Accessed March 5, 2014.
- Vaidya A. Survey: number of hospital-employed physicians up 6%. Becker’s Hospital Review online. June 18, 2013. Available at: http://www.beckershospitalreview.com/hospital-physician-relationships/survey-number-of-hospital-employed-physicians-up-6.html. Accessed March 5, 2014.
There has been a fair amount of media coverage lately about “medical deserts.”1 What exactly is a medical desert, and how big of a problem do they pose for hospital medicine? Wikipedia defines a desert as “a barren area of land where little precipitation occurs and consequently living conditions are hostile for plant and animal life.”2 There are definitely areas in the U.S., both urban and rural, lacking adequate emergency and inpatient medical care.
Based on the latest American Hospital Association (AHA) statistics, there are still >5,700 registered hospitals in the U.S. with almost one million staffed beds combined, which accommodate >36 million admissions every year.3 However, of all U.S. hospitals, only about 35% are located in rural areas, and these tend to be the ones most likely affected by declining reimbursements and tight operating margins.1
Here is some evidence:
— A recent study in the Annals of Emergency Medicine found that only half of the population in the state of Pennsylvania had access to appropriate care within 60 minutes for four time-sensitive conditions (i.e., STEMI, stroke, septic shock, and cardiac arrest).4
— Another study from the Office of Rural Health Policy estimates that approximately 20% of all residential areas do not have rapid access to an acute care medical facility.1
— A recent online story about medical deserts described the devastating case of an 18-month-old girl who died of asphyxiation when a grape became lodged in her throat; their local county’s only hospital with an emergency room had closed months earlier, leaving the closest ED more than 20 miles away.1 This particular hospital, Shelby Regional Medical Center, was a 54-bed hospital in Center, Texas, which suddenly closed in July 2013 amid allegations of fraud from CMS. In addition, a nearby 49-bed Texas hospital (Renaissance Hospital Groves), owned and operated by the same company, had closed in May 2013.
But the list of hospital closures in the past year goes on:
- Lakeside Memorial Hospital in Brockport, N.Y. (61-bed hospital);
- Earl K. Long Medical Center in Baton Rouge, La. (116-bed hospital);
- Stewart-Webster Hospital in Richland, Ga. (25-bed, critical access hospital);
- Calhoun Memorial Hospital in Arlington, Ga. (85-bed hospital);
- Charlton Memorial Hospital in Folkston, Ga. (25-bed hospital);
- The Los Angeles-based Pacific Health Corporation closed all four of its hospitals in California: Anaheim General Hospital (142 beds), Bellflower Medical Center (142 beds), Los Angeles Metropolitan Medical Center (212 beds), and Newport Specialty Hospital (177 beds).
As the CEO of Calhoun Memorial Hospital stated at the closure of his hospital: “It’s a sad day for the community it’s just a sign of the times.”5
Staff, Service Reductions
These hospital closures do not even start to address the nearly ubiquitous reductions in staff and services that many hospitals are resorting to, including workforce reductions experienced by many high-profile academic medical centers like Wake Forest, Denver Health, Emory Health, and Vanderbilt University Medical Centers. According to the Bureau of Labor Statistics, hospitals cut 4,400 jobs in July 2013 alone, while the U.S. overall added 162,000 jobs.1
These acute medical care deserts are primarily a result of declining reimbursements from Medicare and Medicaid, combined with a lack of newly insured Americans, a group that was expected to increase at a much faster pace than it has. The introduction of high-dollar withholds tethered to pay-for-performance programs, such as value-based purchasing and readmission reduction penalties, has also contributed to the financial instability in some hospitals.
In addition, the reduction in disproportionate share hospital (DSH) payments has occurred long before any substantial increase in funded patients through the Affordable Care Act health exchanges. Particularly hard-hit are hospitals in the states that have still elected not to expand Medicaid (primarily in the Southeast and Midwest). And forecasters have every reason to believe that these medical deserts will expand, unless limping hospitals are merged and/or acquired by larger hospital systems.
Should You Be Concerned?
These statistics probably should raise some concern for hospitalists and hospital medicine groups, as the number of hospital-employed physicians is already relatively high (26% according to a recent survey) and rises every year, including an increase of 6% from 2012 to 2013 alone.6 In order to survive in these tenuous conditions, healthcare systems, including hospitalists, will have to be much more involved in the “spectrum of care,” including population health, as opposed to only being involved in discrete acute care episodes. There undoubtedly will be a heavy reliance on telemedicine, seamless electronic medical records, and alternative treatment settings to bridge the gap between medical oases and medical deserts. All of these acute medical care extensions will very likely involve hospitalists.
For the most part, as long as the specialty of hospital medicine keeps its ear to the ground on what is coming, ensuring that we can all be flexible and responsive in meeting the needs of the population we serve, our specialty will be prepped and ready for the “sign of the times.” That way, even when medical deserts do appear, they are not “hostile for life” but are reasonably connected to a suitable oasis.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- Williams JP. What happens when a town’s only hospital shuts down? U.S. News and World Report online. November 8, 2013. Available at: http://health.usnews.com/health-news/hospital-of-tomorrow/articles/2013/11/08/what-happens-when-the-only-hospital-closes. Accessed March 5, 2014.
- Wikipedia. Desert. Available at: http://en.wikipedia.org/wiki/Desert. Accessed March 5, 2014.
- American Hospital Association. Fast facts on U.S. hospitals. Available at: http://www.aha.org/research/rc/stat-studies/fast-facts.shtml. Accessed March 5, 2014.
- Salhi RA, Edwards JM, Gaieski DF, Band RA, Abella BS, Carr BG. Access to Care for patients with time-sensitive conditions in Pennsylvania [published online ahead of print December 21, 2013]. Ann Emerg Med.
- Parks JM. Calhoun Memorial Hospital shuts down. Albany Herald online. February 4, 2013. Available at: http://www.albanyherald.com/news/2013/feb/04/calhoun-memorial-hospital-shuts-down. Accessed March 5, 2014.
- Vaidya A. Survey: number of hospital-employed physicians up 6%. Becker’s Hospital Review online. June 18, 2013. Available at: http://www.beckershospitalreview.com/hospital-physician-relationships/survey-number-of-hospital-employed-physicians-up-6.html. Accessed March 5, 2014.
How Will New Physician Value-Based Payment Modifier Affect Medicare Reimbursements?

We talk a lot about value in healthcare—about how to enhance quality and reduce cost—because we all know both need an incredible amount of work. One tactic Medicare is using to improve the value equation on a large scale is aggregating and displaying physician-specific “value” metrics. These metrics, which will be used to deduct or enhance reimbursement for physicians, are known as the Physician Value-Based Payment Modifier (PVBM).
This program has been enacted fairly rapidly since the passage of the Affordable Care Act; it is being rolled out first to large physician practices, then to all groups by 2017. Those with superior performance in both quality and cost will experience as much as a 2% higher reimbursement, while groups with average performance will remain financially neutral and those who show lower performance or choose not to report will be penalized up to 1% of Medicare reimbursement. This first round, for larger groups of 100-plus physicians, will affect about 30% of all U.S. physicians. The second round, for groups of 10 or more physicians, will affect about another third of physicians. The last round, for groups with fewer than 10 physicians, will be applicable to the remaining physicians practicing in the U.S.
On the face of it, the program does seem to be a potentially effective tactic for improving value on a large scale, holding individual physicians accountable for their own individual patient-care performance. A few fatal flaws in the program as it currently stands make it extraordinarily unlikely to be universally adopted by all physicians, however. Here are a few of those flaws:1,2
1 Uncertain yield: Because it is essentially a “zero-sum game” for Medicare, the incentive or penalty for a physician (or the physician’s group) depends on the performance of all the other physicians’ or groups’ performance. As a result, there is incredible uncertainty as to how strong a physician’s performance actually needs to be, year to year, to result in a bonus payment. Given that many of the metrics will require some type of investment to perform well, such as information technology infrastructure or a quality coordinator, there is an equal amount of uncertainty about how much investment will be needed to get a certain budgetary yield. For smaller physician practices, taking a 1% to 2% reduction in Medicare reimbursements may be easier to weather financially than investing in the infrastructure needed to reliably hit the quality metrics for every relevant patient.
2 Uncertain benchmarks: Unlike many hospital quality metrics, which have been publicly displayed for years, physician-level value metrics are just now being reported publicly. This leaves uncertainty about how strong a physician’s performance needs to be in order to be better than average. In the hospital value-based purchasing program, “average” performance is extremely good, in the 98% to 99% compliance range for most metrics. It is less clear what compliance range will be “average” in the physician-based program.
3 Physician variability: More than a half million physicians in the U.S. bill Medicare, and their practice types range from primary care solo practice to multi-group specialty practice. Motivating all brands to understand, measure, report, and improve quality metrics is a yeoman’s task, unlikely to be successful in the short term. Most physicians have not received any formal education or training in quality improvement, so they may not even have the skill set required to improve their metrics into a highly reliable range, worthy of bonus designation.
4 Metric identity and attribution: Because the repertoire of physician types is broad, the ability of each physician type to have a set of metrics that they understand and can identify with is extremely unlikely. In addition, attribution of patients and their associated metrics to any single physician is complicated, especially for patients who are cared for by many different physicians across a number of settings. For hospitalists, the attribution issue is a fatal flaw, as many groups routinely “hand off” patients among other hospitalists in their group, at least once if not several times during a typical hospital stay. The same is true of many other hospital-based specialty physicians.
5 Playing to the test: As with other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to play to the test, so that their efforts to perform exceedingly well at a few metrics will crowd out and hinder their performance on unmeasured metrics. This tendency can result in lower-value care in the sum total, even if the metrics show stellar performance.
6 Reducing the risk: As seen in other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to avoid caring for patients who are likely to be unpredictable, including those with multiple co-morbid conditions or with complex social situations; these patients are likely to perform less well on any metric, despite risk adjusting (which is inherently imperfect). This is a well-known and documented risk of publicly reported programs, and there is no reason to believe the PVBM program will be immune to this risk.
In Sum
Because these flaws seem so daunting at first glance, many physicians and physician groups will be tempted to reject the program outright and take the financial hit induced by nonparticipation. An alternative approach is to embrace all of the value programs outright, investing time and energy in improving the metrics that are truly valuable to both patients and providers.
Regardless of which regulatory agency is demanding performance, we need to be active participants in foraging out what metrics and attribution logic are most appropriate. For hospitalists, these could include risk-adjusted device days, appropriate prescribing and unprescribing of antibiotics, judicious utilization of diagnostic testing, and measurements of patient functional status and/or mobility.
Value metrics are here to stay, including those attributable to individual physicians; our job now is to advocate for meaningful metrics and meaningful attribution, which can and should motivate hospitalists to enhance their patients’ quality of life at a lower cost.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
We talk a lot about value in healthcare—about how to enhance quality and reduce cost—because we all know both need an incredible amount of work. One tactic Medicare is using to improve the value equation on a large scale is aggregating and displaying physician-specific “value” metrics. These metrics, which will be used to deduct or enhance reimbursement for physicians, are known as the Physician Value-Based Payment Modifier (PVBM).
This program has been enacted fairly rapidly since the passage of the Affordable Care Act; it is being rolled out first to large physician practices, then to all groups by 2017. Those with superior performance in both quality and cost will experience as much as a 2% higher reimbursement, while groups with average performance will remain financially neutral and those who show lower performance or choose not to report will be penalized up to 1% of Medicare reimbursement. This first round, for larger groups of 100-plus physicians, will affect about 30% of all U.S. physicians. The second round, for groups of 10 or more physicians, will affect about another third of physicians. The last round, for groups with fewer than 10 physicians, will be applicable to the remaining physicians practicing in the U.S.
On the face of it, the program does seem to be a potentially effective tactic for improving value on a large scale, holding individual physicians accountable for their own individual patient-care performance. A few fatal flaws in the program as it currently stands make it extraordinarily unlikely to be universally adopted by all physicians, however. Here are a few of those flaws:1,2
1 Uncertain yield: Because it is essentially a “zero-sum game” for Medicare, the incentive or penalty for a physician (or the physician’s group) depends on the performance of all the other physicians’ or groups’ performance. As a result, there is incredible uncertainty as to how strong a physician’s performance actually needs to be, year to year, to result in a bonus payment. Given that many of the metrics will require some type of investment to perform well, such as information technology infrastructure or a quality coordinator, there is an equal amount of uncertainty about how much investment will be needed to get a certain budgetary yield. For smaller physician practices, taking a 1% to 2% reduction in Medicare reimbursements may be easier to weather financially than investing in the infrastructure needed to reliably hit the quality metrics for every relevant patient.
2 Uncertain benchmarks: Unlike many hospital quality metrics, which have been publicly displayed for years, physician-level value metrics are just now being reported publicly. This leaves uncertainty about how strong a physician’s performance needs to be in order to be better than average. In the hospital value-based purchasing program, “average” performance is extremely good, in the 98% to 99% compliance range for most metrics. It is less clear what compliance range will be “average” in the physician-based program.
3 Physician variability: More than a half million physicians in the U.S. bill Medicare, and their practice types range from primary care solo practice to multi-group specialty practice. Motivating all brands to understand, measure, report, and improve quality metrics is a yeoman’s task, unlikely to be successful in the short term. Most physicians have not received any formal education or training in quality improvement, so they may not even have the skill set required to improve their metrics into a highly reliable range, worthy of bonus designation.
4 Metric identity and attribution: Because the repertoire of physician types is broad, the ability of each physician type to have a set of metrics that they understand and can identify with is extremely unlikely. In addition, attribution of patients and their associated metrics to any single physician is complicated, especially for patients who are cared for by many different physicians across a number of settings. For hospitalists, the attribution issue is a fatal flaw, as many groups routinely “hand off” patients among other hospitalists in their group, at least once if not several times during a typical hospital stay. The same is true of many other hospital-based specialty physicians.
5 Playing to the test: As with other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to play to the test, so that their efforts to perform exceedingly well at a few metrics will crowd out and hinder their performance on unmeasured metrics. This tendency can result in lower-value care in the sum total, even if the metrics show stellar performance.
6 Reducing the risk: As seen in other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to avoid caring for patients who are likely to be unpredictable, including those with multiple co-morbid conditions or with complex social situations; these patients are likely to perform less well on any metric, despite risk adjusting (which is inherently imperfect). This is a well-known and documented risk of publicly reported programs, and there is no reason to believe the PVBM program will be immune to this risk.
In Sum
Because these flaws seem so daunting at first glance, many physicians and physician groups will be tempted to reject the program outright and take the financial hit induced by nonparticipation. An alternative approach is to embrace all of the value programs outright, investing time and energy in improving the metrics that are truly valuable to both patients and providers.
Regardless of which regulatory agency is demanding performance, we need to be active participants in foraging out what metrics and attribution logic are most appropriate. For hospitalists, these could include risk-adjusted device days, appropriate prescribing and unprescribing of antibiotics, judicious utilization of diagnostic testing, and measurements of patient functional status and/or mobility.
Value metrics are here to stay, including those attributable to individual physicians; our job now is to advocate for meaningful metrics and meaningful attribution, which can and should motivate hospitalists to enhance their patients’ quality of life at a lower cost.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
We talk a lot about value in healthcare—about how to enhance quality and reduce cost—because we all know both need an incredible amount of work. One tactic Medicare is using to improve the value equation on a large scale is aggregating and displaying physician-specific “value” metrics. These metrics, which will be used to deduct or enhance reimbursement for physicians, are known as the Physician Value-Based Payment Modifier (PVBM).
This program has been enacted fairly rapidly since the passage of the Affordable Care Act; it is being rolled out first to large physician practices, then to all groups by 2017. Those with superior performance in both quality and cost will experience as much as a 2% higher reimbursement, while groups with average performance will remain financially neutral and those who show lower performance or choose not to report will be penalized up to 1% of Medicare reimbursement. This first round, for larger groups of 100-plus physicians, will affect about 30% of all U.S. physicians. The second round, for groups of 10 or more physicians, will affect about another third of physicians. The last round, for groups with fewer than 10 physicians, will be applicable to the remaining physicians practicing in the U.S.
On the face of it, the program does seem to be a potentially effective tactic for improving value on a large scale, holding individual physicians accountable for their own individual patient-care performance. A few fatal flaws in the program as it currently stands make it extraordinarily unlikely to be universally adopted by all physicians, however. Here are a few of those flaws:1,2
1 Uncertain yield: Because it is essentially a “zero-sum game” for Medicare, the incentive or penalty for a physician (or the physician’s group) depends on the performance of all the other physicians’ or groups’ performance. As a result, there is incredible uncertainty as to how strong a physician’s performance actually needs to be, year to year, to result in a bonus payment. Given that many of the metrics will require some type of investment to perform well, such as information technology infrastructure or a quality coordinator, there is an equal amount of uncertainty about how much investment will be needed to get a certain budgetary yield. For smaller physician practices, taking a 1% to 2% reduction in Medicare reimbursements may be easier to weather financially than investing in the infrastructure needed to reliably hit the quality metrics for every relevant patient.
2 Uncertain benchmarks: Unlike many hospital quality metrics, which have been publicly displayed for years, physician-level value metrics are just now being reported publicly. This leaves uncertainty about how strong a physician’s performance needs to be in order to be better than average. In the hospital value-based purchasing program, “average” performance is extremely good, in the 98% to 99% compliance range for most metrics. It is less clear what compliance range will be “average” in the physician-based program.
3 Physician variability: More than a half million physicians in the U.S. bill Medicare, and their practice types range from primary care solo practice to multi-group specialty practice. Motivating all brands to understand, measure, report, and improve quality metrics is a yeoman’s task, unlikely to be successful in the short term. Most physicians have not received any formal education or training in quality improvement, so they may not even have the skill set required to improve their metrics into a highly reliable range, worthy of bonus designation.
4 Metric identity and attribution: Because the repertoire of physician types is broad, the ability of each physician type to have a set of metrics that they understand and can identify with is extremely unlikely. In addition, attribution of patients and their associated metrics to any single physician is complicated, especially for patients who are cared for by many different physicians across a number of settings. For hospitalists, the attribution issue is a fatal flaw, as many groups routinely “hand off” patients among other hospitalists in their group, at least once if not several times during a typical hospital stay. The same is true of many other hospital-based specialty physicians.
5 Playing to the test: As with other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to play to the test, so that their efforts to perform exceedingly well at a few metrics will crowd out and hinder their performance on unmeasured metrics. This tendency can result in lower-value care in the sum total, even if the metrics show stellar performance.
6 Reducing the risk: As seen in other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to avoid caring for patients who are likely to be unpredictable, including those with multiple co-morbid conditions or with complex social situations; these patients are likely to perform less well on any metric, despite risk adjusting (which is inherently imperfect). This is a well-known and documented risk of publicly reported programs, and there is no reason to believe the PVBM program will be immune to this risk.
In Sum
Because these flaws seem so daunting at first glance, many physicians and physician groups will be tempted to reject the program outright and take the financial hit induced by nonparticipation. An alternative approach is to embrace all of the value programs outright, investing time and energy in improving the metrics that are truly valuable to both patients and providers.
Regardless of which regulatory agency is demanding performance, we need to be active participants in foraging out what metrics and attribution logic are most appropriate. For hospitalists, these could include risk-adjusted device days, appropriate prescribing and unprescribing of antibiotics, judicious utilization of diagnostic testing, and measurements of patient functional status and/or mobility.
Value metrics are here to stay, including those attributable to individual physicians; our job now is to advocate for meaningful metrics and meaningful attribution, which can and should motivate hospitalists to enhance their patients’ quality of life at a lower cost.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
HM14 Sessions Hospitalists Should Not Miss

HM14 offers something for every hospitalist, from procedures training to special interest forums to practice management pearls. The four-day annual meeting, coming up March 24-27 at the Mandalay Bay in Las Vegas, caters to young, old, and every doctor in between.
So how will you get the most value out of the conference?
“The highest-yield content is going to depend on what your background is and how to spend that time in a way that augments your knowledge, your perspective, or your exposure to like-minded colleagues in a very individual way,” says HM14 course director Daniel Brotman, MD, FACP, SFHM, director of the hospitalist program at Johns Hopkins Hospital in Baltimore. “One of the things that’s so cool about hospital medicine is its diversity.”
But don’t take Dr. Brotman’s well-educated word for it. Here’s a list of recommendations from Team Hospitalist, the only reader-involvement group of its kind in HM, on events they would not miss this year.
Team Hospitalist contributors: Danielle Scheurer, MD, MSCR, SFHM, hospitalist, chief quality officer, Medical University of South Carolina; Edward Ma, MD, hospitalist, Coatesville (Pa.) VA Medical Center; Nick Fitterman, MD, FACP, SFHM, vice chair of hospital medicine, Hofstra North Shore-LIJ School of Medicine, Manhasset, N.Y.; James O’Callaghan, MD, FHM, clinical assistant professor of pediatrics, Seattle Children’s Hospital, University of Washington, and EvergreenHealth, Kirkland, Wash.; Klaus Suehler, MD, FHM, Mercy Hospital, Allina Health, Minneapolis, Minn.
1 “When Time is Brain (or Cord): Neurological Emergencies for the Hospitalist”
Tuesday, March 25
10:35-11:15 am
Dr. Suehler: As hospitalists, we often are the first ones to see patients with such neurological emergencies, and it is crucial to know when to get the neurologist or neurosurgeon involved. These are opportunities with a brief window of time to save or restore a patient’s neurological function.
2 “The ACA at 4: Impact on Costs, Quality, Lifestyle, and Payment”
Tuesday, March 25
10:35-11:50 am
Dr. Scheurer: This will be a packed session and will discuss all angles of the Affordable Care Act: how it will play out in hospitals around the country and, particularly, what it will mean to hospitalists. The complexity of the ACA is dizzying, so it will be time well spent to hear from several leaders in the field on how the major components of the ACA can and will impact us.
Dr. Ma: The ACA is nearly four years old, so I’m looking forward to a review on what precisely has been accomplished in medicine thus far and what can we anticipate down the road. The lawyers bantered about the constitutionality of the policy for the first two years. Politicians have been ranting about death panels, repeals, and amendments [for] the past four years. The public endured the latter part of 2013 reading about (or experiencing firsthand) the disastrous rollout of the healthcare.gov website. I want a clearer idea, beyond the fear and loathing, beyond the inane rhetoric, of the real impact that ACA has had and will have on the two most important components of healthcare: physicians and patients.
3 “Rate, Rhythm, Rivaroxaban, Ablation: Update in Atrial Fibrillation”
Tuesday, March 25
11:20 am-Noon
Dr. Suehler: This is a standard situation for hospitalists. We often admit patients with atrial fibrillation or get consulted when patients who are hospitalized for other reasons develop atrial fibrillation. It is very important for hospitalists to provide optimal care and counseling to patients with this arrhythmia, whether or not cardiologists get involved down the road.
4 “How ICD-10 Will Affect Hospitalists”
Tuesday, March 25
1:10-2:25 pm
Dr. Scheurer: Whether we like it or not, ICD-10 is right around the corner. This session will give an overview of what impact ICD-10 will have on our medical record documentation and coding, including how it can and will affect reimbursement. The more you know now, the better off you will be when your hospital implements it.
5 “Controversies in Perioperative Medicine”
Wednesday, March 26
11 am-Noon
Dr. Scheurer: We all know how much our surgeons depend on us to give them sound and evidence-based advice on how to manage surgical patients in the perioperative period. This session will review some controversial topics, from [the perspective of] two of the leaders in the field of perioperative medicine.
6 “Is It OK if I Sit Down?: Improving Patient Communication and Satisfaction at the Bedside”
Wednesday, March 26
11:45 am-12:25 pm
Dr. Fitterman: Any hospitalist or HM program leader struggling to raise patient satisfaction scores must attend this session. Recognizing that 30% of the value-based incentive pool for hospitals is directly linked to these scores, we all have “skin in the game.” Most hospitalists have part of their salary tied to patient satisfaction; however, many still lack the desired improvement in rankings despite multiple initiatives to address this issue. Four of the top five drivers of the patient experience are related to nursing, making our responsibility to impact this quite challenging. There is a correlation between the hospitals with the best satisfaction scores and lower patient mortality, so this is not just about the “chocolate on the pillow” but about filling gaps in care. I anticipate the discussion leaders will help us navigate this challenge with tips to bring back to our programs.
7 “Ending the Benevolent Dictatorship: Shared Decision-Making in the Hospital”
Wednesday, March 26
2:50-3:30 pm
Dr. Fitterman: This is a must attend for anyone interested in the “next blockbuster drug.” That is how patient activation and shared decision-making are being referred to (Health Affairs, February 2013). Where this has been implemented, patients have recognized better health outcomes, and there has been less decisional conflict (which likely equates to better satisfaction)—and all at lower costs. Sounds like a blockbuster drug, doesn’t it? The challenges I hope to see answered in this breakout session: First, most evidence wrapped around this topic is in the outpatient arena. Second, how do we overcome a lack of training in this field? Finally, how can we fit this into our busy workflows? Save me a seat.
8 “What Keeps Your CFO Awake at Night”
Wednesday, March 26
2:50-4:05 pm
Dr. Scheurer: The complexity of hospital finances can confuse even the brightest of hospitalists. This session will focus on the basics of what hospitalists should know and care about, as it relates to hospital finances. You won’t want to miss the concise opportunity to get informed.
9 “Different Generation/Different Concerns: Managing Boomers, Gen-Xers, and Gen Ys”
Thursday, March 27
8:45-9:40 am
Dr. Ma: This will likely be a contentious yet humorous session. The generational differences in attitude toward the practice of medicine can be very pronounced at times and certainly can lead to conflict in the workplace between the older and younger physicians. It’s important to recognize these differences without passing judgment and understand how they impact a practice.
10 “Effective, Efficient, and Prudent Syncope Evaluation”
Thursday, March 27
10:30-11:10 am
Dr. Suehler: Syncope is a frequent admission diagnosis for hospitalists. There is a wide spectrum of how hospitalists manage such patients (how long to monitor on telemetry, what additional tests to order). Hospitalists need to know how to provide a rational and cost-effective evaluation of patients with syncope and be able to identify patients who have a serious or life-threatening cause for their syncope.
–Nick Fitterman, MD, FACP, SFHM, vice chair of hospital medicine, Hofstra North Shore-LIJ School of Medicine, Manhasset, N.Y.
11 “The Leadership Imperative: Building a Culture of Engagement and Ownership”
Thursday, March 27
10:55-11:50 am
Dr. O’Callaghan: Hospital practices, and the systems to which they belong, are complex organizations with their own culture. Producing long-term, sustainable change and improvement usually means changing this culture. Practices and their leaders need to develop hospitalists who think about improving the system of care, not just the patients in front of them. Successful practices are able to provide physicians with the freedom and responsibility to develop an ownership-mindset toward the practice. This lecture will help leaders develop the skills needed to support the development and maintenance of a culture of ownership.
12 “HFNC in Bronchiolitis: Best Thing Since Sliced Bread?”
Thursday, March 25
1:10-2:25 pm
Dr. O’Callaghan: Shawn Ralston, MD, is well known in pediatric hospital medicine for having both expertise and passion around the diagnosis of bronchiolitis. In the past year, she was lead author of a multi-site voluntary QI collaborative study that demonstrated that benchmarking decreased utilization of bronchodilators and chest physiotherapy in bronchiolitis (J Hosp Med. 2013;8:25-30). In addition, she was one of the authors of SHM’s Choosing Wisely Pediatric Hospital Medicine Recommendations (J Hosp Med. 2013;8(9):479-485). Dr. Ralston is a strong proponent of “doing more by doing less,” with regard to bronchiolitis, which is a self-limiting disease in pediatrics; however, along comes a potential new therapy—high flow nasal cannula therapy. I am very excited to see Dr. Ralston explore this new treatment. Will she have a debate with herself, and if so, which Ralston wins—doing-less Ralston or doing-more Ralston? I anticipate this session to be both highly informative and highly entertaining.
Richard Quinn is a freelance writer in New Jersey.
HM14 offers something for every hospitalist, from procedures training to special interest forums to practice management pearls. The four-day annual meeting, coming up March 24-27 at the Mandalay Bay in Las Vegas, caters to young, old, and every doctor in between.
So how will you get the most value out of the conference?
“The highest-yield content is going to depend on what your background is and how to spend that time in a way that augments your knowledge, your perspective, or your exposure to like-minded colleagues in a very individual way,” says HM14 course director Daniel Brotman, MD, FACP, SFHM, director of the hospitalist program at Johns Hopkins Hospital in Baltimore. “One of the things that’s so cool about hospital medicine is its diversity.”
But don’t take Dr. Brotman’s well-educated word for it. Here’s a list of recommendations from Team Hospitalist, the only reader-involvement group of its kind in HM, on events they would not miss this year.
Team Hospitalist contributors: Danielle Scheurer, MD, MSCR, SFHM, hospitalist, chief quality officer, Medical University of South Carolina; Edward Ma, MD, hospitalist, Coatesville (Pa.) VA Medical Center; Nick Fitterman, MD, FACP, SFHM, vice chair of hospital medicine, Hofstra North Shore-LIJ School of Medicine, Manhasset, N.Y.; James O’Callaghan, MD, FHM, clinical assistant professor of pediatrics, Seattle Children’s Hospital, University of Washington, and EvergreenHealth, Kirkland, Wash.; Klaus Suehler, MD, FHM, Mercy Hospital, Allina Health, Minneapolis, Minn.
1 “When Time is Brain (or Cord): Neurological Emergencies for the Hospitalist”
Tuesday, March 25
10:35-11:15 am
Dr. Suehler: As hospitalists, we often are the first ones to see patients with such neurological emergencies, and it is crucial to know when to get the neurologist or neurosurgeon involved. These are opportunities with a brief window of time to save or restore a patient’s neurological function.
2 “The ACA at 4: Impact on Costs, Quality, Lifestyle, and Payment”
Tuesday, March 25
10:35-11:50 am
Dr. Scheurer: This will be a packed session and will discuss all angles of the Affordable Care Act: how it will play out in hospitals around the country and, particularly, what it will mean to hospitalists. The complexity of the ACA is dizzying, so it will be time well spent to hear from several leaders in the field on how the major components of the ACA can and will impact us.
Dr. Ma: The ACA is nearly four years old, so I’m looking forward to a review on what precisely has been accomplished in medicine thus far and what can we anticipate down the road. The lawyers bantered about the constitutionality of the policy for the first two years. Politicians have been ranting about death panels, repeals, and amendments [for] the past four years. The public endured the latter part of 2013 reading about (or experiencing firsthand) the disastrous rollout of the healthcare.gov website. I want a clearer idea, beyond the fear and loathing, beyond the inane rhetoric, of the real impact that ACA has had and will have on the two most important components of healthcare: physicians and patients.
3 “Rate, Rhythm, Rivaroxaban, Ablation: Update in Atrial Fibrillation”
Tuesday, March 25
11:20 am-Noon
Dr. Suehler: This is a standard situation for hospitalists. We often admit patients with atrial fibrillation or get consulted when patients who are hospitalized for other reasons develop atrial fibrillation. It is very important for hospitalists to provide optimal care and counseling to patients with this arrhythmia, whether or not cardiologists get involved down the road.
4 “How ICD-10 Will Affect Hospitalists”
Tuesday, March 25
1:10-2:25 pm
Dr. Scheurer: Whether we like it or not, ICD-10 is right around the corner. This session will give an overview of what impact ICD-10 will have on our medical record documentation and coding, including how it can and will affect reimbursement. The more you know now, the better off you will be when your hospital implements it.
5 “Controversies in Perioperative Medicine”
Wednesday, March 26
11 am-Noon
Dr. Scheurer: We all know how much our surgeons depend on us to give them sound and evidence-based advice on how to manage surgical patients in the perioperative period. This session will review some controversial topics, from [the perspective of] two of the leaders in the field of perioperative medicine.
6 “Is It OK if I Sit Down?: Improving Patient Communication and Satisfaction at the Bedside”
Wednesday, March 26
11:45 am-12:25 pm
Dr. Fitterman: Any hospitalist or HM program leader struggling to raise patient satisfaction scores must attend this session. Recognizing that 30% of the value-based incentive pool for hospitals is directly linked to these scores, we all have “skin in the game.” Most hospitalists have part of their salary tied to patient satisfaction; however, many still lack the desired improvement in rankings despite multiple initiatives to address this issue. Four of the top five drivers of the patient experience are related to nursing, making our responsibility to impact this quite challenging. There is a correlation between the hospitals with the best satisfaction scores and lower patient mortality, so this is not just about the “chocolate on the pillow” but about filling gaps in care. I anticipate the discussion leaders will help us navigate this challenge with tips to bring back to our programs.
7 “Ending the Benevolent Dictatorship: Shared Decision-Making in the Hospital”
Wednesday, March 26
2:50-3:30 pm
Dr. Fitterman: This is a must attend for anyone interested in the “next blockbuster drug.” That is how patient activation and shared decision-making are being referred to (Health Affairs, February 2013). Where this has been implemented, patients have recognized better health outcomes, and there has been less decisional conflict (which likely equates to better satisfaction)—and all at lower costs. Sounds like a blockbuster drug, doesn’t it? The challenges I hope to see answered in this breakout session: First, most evidence wrapped around this topic is in the outpatient arena. Second, how do we overcome a lack of training in this field? Finally, how can we fit this into our busy workflows? Save me a seat.
8 “What Keeps Your CFO Awake at Night”
Wednesday, March 26
2:50-4:05 pm
Dr. Scheurer: The complexity of hospital finances can confuse even the brightest of hospitalists. This session will focus on the basics of what hospitalists should know and care about, as it relates to hospital finances. You won’t want to miss the concise opportunity to get informed.
9 “Different Generation/Different Concerns: Managing Boomers, Gen-Xers, and Gen Ys”
Thursday, March 27
8:45-9:40 am
Dr. Ma: This will likely be a contentious yet humorous session. The generational differences in attitude toward the practice of medicine can be very pronounced at times and certainly can lead to conflict in the workplace between the older and younger physicians. It’s important to recognize these differences without passing judgment and understand how they impact a practice.
10 “Effective, Efficient, and Prudent Syncope Evaluation”
Thursday, March 27
10:30-11:10 am
Dr. Suehler: Syncope is a frequent admission diagnosis for hospitalists. There is a wide spectrum of how hospitalists manage such patients (how long to monitor on telemetry, what additional tests to order). Hospitalists need to know how to provide a rational and cost-effective evaluation of patients with syncope and be able to identify patients who have a serious or life-threatening cause for their syncope.
–Nick Fitterman, MD, FACP, SFHM, vice chair of hospital medicine, Hofstra North Shore-LIJ School of Medicine, Manhasset, N.Y.
11 “The Leadership Imperative: Building a Culture of Engagement and Ownership”
Thursday, March 27
10:55-11:50 am
Dr. O’Callaghan: Hospital practices, and the systems to which they belong, are complex organizations with their own culture. Producing long-term, sustainable change and improvement usually means changing this culture. Practices and their leaders need to develop hospitalists who think about improving the system of care, not just the patients in front of them. Successful practices are able to provide physicians with the freedom and responsibility to develop an ownership-mindset toward the practice. This lecture will help leaders develop the skills needed to support the development and maintenance of a culture of ownership.
12 “HFNC in Bronchiolitis: Best Thing Since Sliced Bread?”
Thursday, March 25
1:10-2:25 pm
Dr. O’Callaghan: Shawn Ralston, MD, is well known in pediatric hospital medicine for having both expertise and passion around the diagnosis of bronchiolitis. In the past year, she was lead author of a multi-site voluntary QI collaborative study that demonstrated that benchmarking decreased utilization of bronchodilators and chest physiotherapy in bronchiolitis (J Hosp Med. 2013;8:25-30). In addition, she was one of the authors of SHM’s Choosing Wisely Pediatric Hospital Medicine Recommendations (J Hosp Med. 2013;8(9):479-485). Dr. Ralston is a strong proponent of “doing more by doing less,” with regard to bronchiolitis, which is a self-limiting disease in pediatrics; however, along comes a potential new therapy—high flow nasal cannula therapy. I am very excited to see Dr. Ralston explore this new treatment. Will she have a debate with herself, and if so, which Ralston wins—doing-less Ralston or doing-more Ralston? I anticipate this session to be both highly informative and highly entertaining.
Richard Quinn is a freelance writer in New Jersey.
HM14 offers something for every hospitalist, from procedures training to special interest forums to practice management pearls. The four-day annual meeting, coming up March 24-27 at the Mandalay Bay in Las Vegas, caters to young, old, and every doctor in between.
So how will you get the most value out of the conference?
“The highest-yield content is going to depend on what your background is and how to spend that time in a way that augments your knowledge, your perspective, or your exposure to like-minded colleagues in a very individual way,” says HM14 course director Daniel Brotman, MD, FACP, SFHM, director of the hospitalist program at Johns Hopkins Hospital in Baltimore. “One of the things that’s so cool about hospital medicine is its diversity.”
But don’t take Dr. Brotman’s well-educated word for it. Here’s a list of recommendations from Team Hospitalist, the only reader-involvement group of its kind in HM, on events they would not miss this year.
Team Hospitalist contributors: Danielle Scheurer, MD, MSCR, SFHM, hospitalist, chief quality officer, Medical University of South Carolina; Edward Ma, MD, hospitalist, Coatesville (Pa.) VA Medical Center; Nick Fitterman, MD, FACP, SFHM, vice chair of hospital medicine, Hofstra North Shore-LIJ School of Medicine, Manhasset, N.Y.; James O’Callaghan, MD, FHM, clinical assistant professor of pediatrics, Seattle Children’s Hospital, University of Washington, and EvergreenHealth, Kirkland, Wash.; Klaus Suehler, MD, FHM, Mercy Hospital, Allina Health, Minneapolis, Minn.
1 “When Time is Brain (or Cord): Neurological Emergencies for the Hospitalist”
Tuesday, March 25
10:35-11:15 am
Dr. Suehler: As hospitalists, we often are the first ones to see patients with such neurological emergencies, and it is crucial to know when to get the neurologist or neurosurgeon involved. These are opportunities with a brief window of time to save or restore a patient’s neurological function.
2 “The ACA at 4: Impact on Costs, Quality, Lifestyle, and Payment”
Tuesday, March 25
10:35-11:50 am
Dr. Scheurer: This will be a packed session and will discuss all angles of the Affordable Care Act: how it will play out in hospitals around the country and, particularly, what it will mean to hospitalists. The complexity of the ACA is dizzying, so it will be time well spent to hear from several leaders in the field on how the major components of the ACA can and will impact us.
Dr. Ma: The ACA is nearly four years old, so I’m looking forward to a review on what precisely has been accomplished in medicine thus far and what can we anticipate down the road. The lawyers bantered about the constitutionality of the policy for the first two years. Politicians have been ranting about death panels, repeals, and amendments [for] the past four years. The public endured the latter part of 2013 reading about (or experiencing firsthand) the disastrous rollout of the healthcare.gov website. I want a clearer idea, beyond the fear and loathing, beyond the inane rhetoric, of the real impact that ACA has had and will have on the two most important components of healthcare: physicians and patients.
3 “Rate, Rhythm, Rivaroxaban, Ablation: Update in Atrial Fibrillation”
Tuesday, March 25
11:20 am-Noon
Dr. Suehler: This is a standard situation for hospitalists. We often admit patients with atrial fibrillation or get consulted when patients who are hospitalized for other reasons develop atrial fibrillation. It is very important for hospitalists to provide optimal care and counseling to patients with this arrhythmia, whether or not cardiologists get involved down the road.
4 “How ICD-10 Will Affect Hospitalists”
Tuesday, March 25
1:10-2:25 pm
Dr. Scheurer: Whether we like it or not, ICD-10 is right around the corner. This session will give an overview of what impact ICD-10 will have on our medical record documentation and coding, including how it can and will affect reimbursement. The more you know now, the better off you will be when your hospital implements it.
5 “Controversies in Perioperative Medicine”
Wednesday, March 26
11 am-Noon
Dr. Scheurer: We all know how much our surgeons depend on us to give them sound and evidence-based advice on how to manage surgical patients in the perioperative period. This session will review some controversial topics, from [the perspective of] two of the leaders in the field of perioperative medicine.
6 “Is It OK if I Sit Down?: Improving Patient Communication and Satisfaction at the Bedside”
Wednesday, March 26
11:45 am-12:25 pm
Dr. Fitterman: Any hospitalist or HM program leader struggling to raise patient satisfaction scores must attend this session. Recognizing that 30% of the value-based incentive pool for hospitals is directly linked to these scores, we all have “skin in the game.” Most hospitalists have part of their salary tied to patient satisfaction; however, many still lack the desired improvement in rankings despite multiple initiatives to address this issue. Four of the top five drivers of the patient experience are related to nursing, making our responsibility to impact this quite challenging. There is a correlation between the hospitals with the best satisfaction scores and lower patient mortality, so this is not just about the “chocolate on the pillow” but about filling gaps in care. I anticipate the discussion leaders will help us navigate this challenge with tips to bring back to our programs.
7 “Ending the Benevolent Dictatorship: Shared Decision-Making in the Hospital”
Wednesday, March 26
2:50-3:30 pm
Dr. Fitterman: This is a must attend for anyone interested in the “next blockbuster drug.” That is how patient activation and shared decision-making are being referred to (Health Affairs, February 2013). Where this has been implemented, patients have recognized better health outcomes, and there has been less decisional conflict (which likely equates to better satisfaction)—and all at lower costs. Sounds like a blockbuster drug, doesn’t it? The challenges I hope to see answered in this breakout session: First, most evidence wrapped around this topic is in the outpatient arena. Second, how do we overcome a lack of training in this field? Finally, how can we fit this into our busy workflows? Save me a seat.
8 “What Keeps Your CFO Awake at Night”
Wednesday, March 26
2:50-4:05 pm
Dr. Scheurer: The complexity of hospital finances can confuse even the brightest of hospitalists. This session will focus on the basics of what hospitalists should know and care about, as it relates to hospital finances. You won’t want to miss the concise opportunity to get informed.
9 “Different Generation/Different Concerns: Managing Boomers, Gen-Xers, and Gen Ys”
Thursday, March 27
8:45-9:40 am
Dr. Ma: This will likely be a contentious yet humorous session. The generational differences in attitude toward the practice of medicine can be very pronounced at times and certainly can lead to conflict in the workplace between the older and younger physicians. It’s important to recognize these differences without passing judgment and understand how they impact a practice.
10 “Effective, Efficient, and Prudent Syncope Evaluation”
Thursday, March 27
10:30-11:10 am
Dr. Suehler: Syncope is a frequent admission diagnosis for hospitalists. There is a wide spectrum of how hospitalists manage such patients (how long to monitor on telemetry, what additional tests to order). Hospitalists need to know how to provide a rational and cost-effective evaluation of patients with syncope and be able to identify patients who have a serious or life-threatening cause for their syncope.
–Nick Fitterman, MD, FACP, SFHM, vice chair of hospital medicine, Hofstra North Shore-LIJ School of Medicine, Manhasset, N.Y.
11 “The Leadership Imperative: Building a Culture of Engagement and Ownership”
Thursday, March 27
10:55-11:50 am
Dr. O’Callaghan: Hospital practices, and the systems to which they belong, are complex organizations with their own culture. Producing long-term, sustainable change and improvement usually means changing this culture. Practices and their leaders need to develop hospitalists who think about improving the system of care, not just the patients in front of them. Successful practices are able to provide physicians with the freedom and responsibility to develop an ownership-mindset toward the practice. This lecture will help leaders develop the skills needed to support the development and maintenance of a culture of ownership.
12 “HFNC in Bronchiolitis: Best Thing Since Sliced Bread?”
Thursday, March 25
1:10-2:25 pm
Dr. O’Callaghan: Shawn Ralston, MD, is well known in pediatric hospital medicine for having both expertise and passion around the diagnosis of bronchiolitis. In the past year, she was lead author of a multi-site voluntary QI collaborative study that demonstrated that benchmarking decreased utilization of bronchodilators and chest physiotherapy in bronchiolitis (J Hosp Med. 2013;8:25-30). In addition, she was one of the authors of SHM’s Choosing Wisely Pediatric Hospital Medicine Recommendations (J Hosp Med. 2013;8(9):479-485). Dr. Ralston is a strong proponent of “doing more by doing less,” with regard to bronchiolitis, which is a self-limiting disease in pediatrics; however, along comes a potential new therapy—high flow nasal cannula therapy. I am very excited to see Dr. Ralston explore this new treatment. Will she have a debate with herself, and if so, which Ralston wins—doing-less Ralston or doing-more Ralston? I anticipate this session to be both highly informative and highly entertaining.
Richard Quinn is a freelance writer in New Jersey.
Five Reasons To Pursue ABIM's Hospitalist-Focused MOC

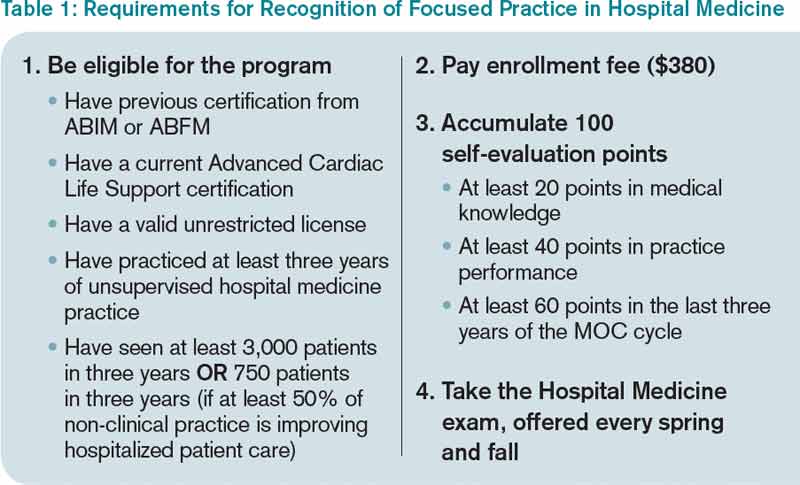
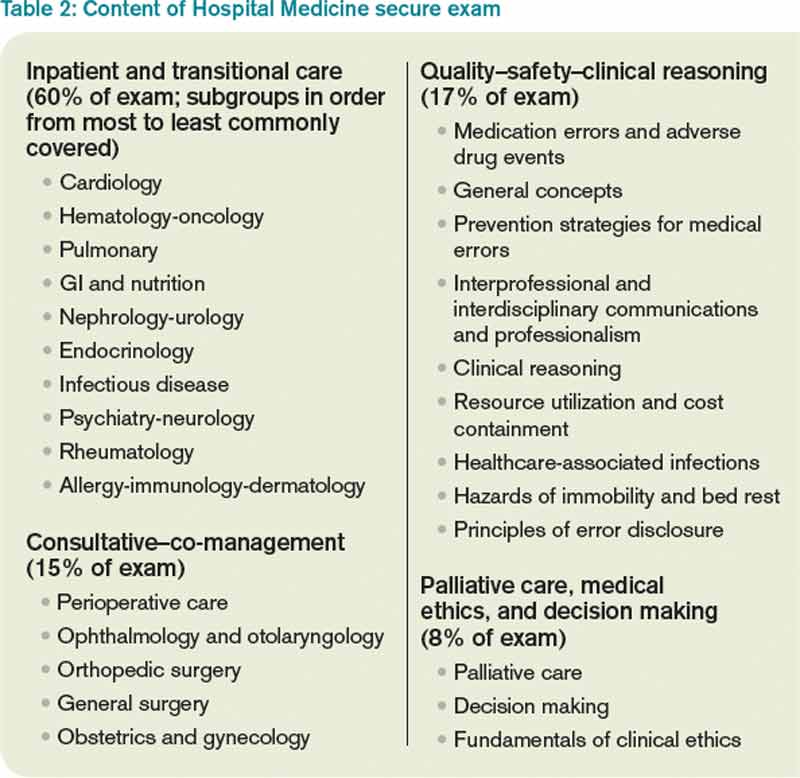
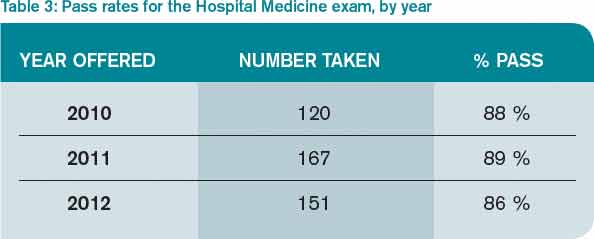
By now, most hospitalists have at least heard about the Recognition in Focused Practice in Hospital Medicine (RFPHM), which is offered as a variation in certification for internal medicine- and family medicine-trained graduates who are pursuing Maintenance of Certification (MOC). Although the requirements are relatively straightforward, it may not be abundantly clear exactly why a hospitalist would pursue this pathway. As a recent “graduate” of the first cycle of the program, I can testify it is wholly worth the time and energy for the following reasons:
1. The requirements are relatively easy. Table 1 outlines the requirements for eligibility for enrolling in the program through the American Board of Internal Medicine (ABIM); enrollment through the American Board of Family Medicine (ABFM) also is available. These are basic requirements, and most practicing hospitalists will easily qualify simply by doing their daily jobs. Enrollment does require an administrative fee, but many HM programs can—and should—reimburse you for these fees, so be sure to ask if your program will cover the cost.
After enrolling and paying the fee, your next step is to accumulate points toward certification. Of note, the 100 points do not all have to be accumulated prior to sitting for the exam, but accumulating these points generally prepares you for the exam, so it is a good idea to complete this task before the exam, in most circumstances.
The medical knowledge modules can be completed through ABIM/ABFM, the Society of Hospital Medicine (SHM), or the New England Journal of Medicine.1 A repertoire of clinical and non-clinical modules are offered by ABIM, and there are two modules on quality-patient safety offered by SHM. You can attend a number of pre-courses offered at local-regional-national HM meetings; these modules can be completed individually or in a group setting. A list of available group learning sessions can be found at www.abim.org. You can earn CME credit for completing these modules. Not only are the medical knowledge modules readily available, but they are also well written, are easy to complete, and prepare you well for the exam.
The practice performance modules can be completed through ABIM/ABFM or through a number of medical centers that participate in the American Board of Medical Specialties “Portfolio Program.” For organizations that participate in the program, hospitalists within the organizational network who have completed a quality improvement project may qualify for module credit. A list of these sponsoring organizations can be found at http://mocportfolioprogram.org/approved-portfolio-sponsors.
Hospitalists can earn practice improvement module (PIM) credit for being involved in a number of large collaborative projects, including SHM’s mentored implementation programs (e.g. glycemic control, VTE, and Project BOOST).3
For those completing a PIM through the ABIM, the most straightforward are the self-directed PIM or the completed project PIM.2
2. The exam content is known. Table 2 lists the content categories of the secure exam, published by ABIM, with approximate percentages of the content within overall categories and subcategories. This information helps you focus your efforts in preparing for the exam and is aligned with what most hospitalists practice on a daily basis.
3. The exam preparation is easy. Not only is the content outlined in the blueprint in Table 2, but practice exams are available online from the ABIM and a tutorial can be found at www.abim.org/hospital-medicine-tutorial. This tutorial simulates the actual exam, to enhance preparation and reduce testing anxiety.
4. The exam pass rate is high. Table 3 lists pass rates from the 2010-2012 hospital medicine exam. These pass rates are equivalent to the general medicine exam, and they exceed some of the other specialty exam pass rates.
5. RFPHM is gaining more of the recognition it deserves. Given this growth in recognition, from employers, peers, patients, and maybe even payors, it would serve you well to start the process early, because it is highly likely to gain traction in the coming years.
Join Us
All told, RFPHM enrollment, preparation, and exam completion are straightforward, relatively easy, and worth the time and energy. I hope you join me and the 418 other hospitalists who have pursued this recognition. You will be glad you invested in your future.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- American Board of Internal Medicine. List of self-evaluation modules. Available at: http://www.abim.org/maintenance-of-certification/medical-knowledge/modules.aspx#hosp. Accessed November 27, 2013.
- American Board of Internal Medicine. List of PIMs from ABIM. Available at: http://www.abim.org/moc/earning-points.aspx. Accessed November 27, 2013.
- American Board of Internal Medicine. List of PIMs from sponsoring institutions. Available at: http://www.abim.org/moc/earning-points/productinfo-demo-ordering.aspx#aqi. Accessed November 27, 2013.
By now, most hospitalists have at least heard about the Recognition in Focused Practice in Hospital Medicine (RFPHM), which is offered as a variation in certification for internal medicine- and family medicine-trained graduates who are pursuing Maintenance of Certification (MOC). Although the requirements are relatively straightforward, it may not be abundantly clear exactly why a hospitalist would pursue this pathway. As a recent “graduate” of the first cycle of the program, I can testify it is wholly worth the time and energy for the following reasons:
1. The requirements are relatively easy. Table 1 outlines the requirements for eligibility for enrolling in the program through the American Board of Internal Medicine (ABIM); enrollment through the American Board of Family Medicine (ABFM) also is available. These are basic requirements, and most practicing hospitalists will easily qualify simply by doing their daily jobs. Enrollment does require an administrative fee, but many HM programs can—and should—reimburse you for these fees, so be sure to ask if your program will cover the cost.
After enrolling and paying the fee, your next step is to accumulate points toward certification. Of note, the 100 points do not all have to be accumulated prior to sitting for the exam, but accumulating these points generally prepares you for the exam, so it is a good idea to complete this task before the exam, in most circumstances.
The medical knowledge modules can be completed through ABIM/ABFM, the Society of Hospital Medicine (SHM), or the New England Journal of Medicine.1 A repertoire of clinical and non-clinical modules are offered by ABIM, and there are two modules on quality-patient safety offered by SHM. You can attend a number of pre-courses offered at local-regional-national HM meetings; these modules can be completed individually or in a group setting. A list of available group learning sessions can be found at www.abim.org. You can earn CME credit for completing these modules. Not only are the medical knowledge modules readily available, but they are also well written, are easy to complete, and prepare you well for the exam.
The practice performance modules can be completed through ABIM/ABFM or through a number of medical centers that participate in the American Board of Medical Specialties “Portfolio Program.” For organizations that participate in the program, hospitalists within the organizational network who have completed a quality improvement project may qualify for module credit. A list of these sponsoring organizations can be found at http://mocportfolioprogram.org/approved-portfolio-sponsors.
Hospitalists can earn practice improvement module (PIM) credit for being involved in a number of large collaborative projects, including SHM’s mentored implementation programs (e.g. glycemic control, VTE, and Project BOOST).3
For those completing a PIM through the ABIM, the most straightforward are the self-directed PIM or the completed project PIM.2
2. The exam content is known. Table 2 lists the content categories of the secure exam, published by ABIM, with approximate percentages of the content within overall categories and subcategories. This information helps you focus your efforts in preparing for the exam and is aligned with what most hospitalists practice on a daily basis.
3. The exam preparation is easy. Not only is the content outlined in the blueprint in Table 2, but practice exams are available online from the ABIM and a tutorial can be found at www.abim.org/hospital-medicine-tutorial. This tutorial simulates the actual exam, to enhance preparation and reduce testing anxiety.
4. The exam pass rate is high. Table 3 lists pass rates from the 2010-2012 hospital medicine exam. These pass rates are equivalent to the general medicine exam, and they exceed some of the other specialty exam pass rates.
5. RFPHM is gaining more of the recognition it deserves. Given this growth in recognition, from employers, peers, patients, and maybe even payors, it would serve you well to start the process early, because it is highly likely to gain traction in the coming years.
Join Us
All told, RFPHM enrollment, preparation, and exam completion are straightforward, relatively easy, and worth the time and energy. I hope you join me and the 418 other hospitalists who have pursued this recognition. You will be glad you invested in your future.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- American Board of Internal Medicine. List of self-evaluation modules. Available at: http://www.abim.org/maintenance-of-certification/medical-knowledge/modules.aspx#hosp. Accessed November 27, 2013.
- American Board of Internal Medicine. List of PIMs from ABIM. Available at: http://www.abim.org/moc/earning-points.aspx. Accessed November 27, 2013.
- American Board of Internal Medicine. List of PIMs from sponsoring institutions. Available at: http://www.abim.org/moc/earning-points/productinfo-demo-ordering.aspx#aqi. Accessed November 27, 2013.
By now, most hospitalists have at least heard about the Recognition in Focused Practice in Hospital Medicine (RFPHM), which is offered as a variation in certification for internal medicine- and family medicine-trained graduates who are pursuing Maintenance of Certification (MOC). Although the requirements are relatively straightforward, it may not be abundantly clear exactly why a hospitalist would pursue this pathway. As a recent “graduate” of the first cycle of the program, I can testify it is wholly worth the time and energy for the following reasons:
1. The requirements are relatively easy. Table 1 outlines the requirements for eligibility for enrolling in the program through the American Board of Internal Medicine (ABIM); enrollment through the American Board of Family Medicine (ABFM) also is available. These are basic requirements, and most practicing hospitalists will easily qualify simply by doing their daily jobs. Enrollment does require an administrative fee, but many HM programs can—and should—reimburse you for these fees, so be sure to ask if your program will cover the cost.
After enrolling and paying the fee, your next step is to accumulate points toward certification. Of note, the 100 points do not all have to be accumulated prior to sitting for the exam, but accumulating these points generally prepares you for the exam, so it is a good idea to complete this task before the exam, in most circumstances.
The medical knowledge modules can be completed through ABIM/ABFM, the Society of Hospital Medicine (SHM), or the New England Journal of Medicine.1 A repertoire of clinical and non-clinical modules are offered by ABIM, and there are two modules on quality-patient safety offered by SHM. You can attend a number of pre-courses offered at local-regional-national HM meetings; these modules can be completed individually or in a group setting. A list of available group learning sessions can be found at www.abim.org. You can earn CME credit for completing these modules. Not only are the medical knowledge modules readily available, but they are also well written, are easy to complete, and prepare you well for the exam.
The practice performance modules can be completed through ABIM/ABFM or through a number of medical centers that participate in the American Board of Medical Specialties “Portfolio Program.” For organizations that participate in the program, hospitalists within the organizational network who have completed a quality improvement project may qualify for module credit. A list of these sponsoring organizations can be found at http://mocportfolioprogram.org/approved-portfolio-sponsors.
Hospitalists can earn practice improvement module (PIM) credit for being involved in a number of large collaborative projects, including SHM’s mentored implementation programs (e.g. glycemic control, VTE, and Project BOOST).3
For those completing a PIM through the ABIM, the most straightforward are the self-directed PIM or the completed project PIM.2
2. The exam content is known. Table 2 lists the content categories of the secure exam, published by ABIM, with approximate percentages of the content within overall categories and subcategories. This information helps you focus your efforts in preparing for the exam and is aligned with what most hospitalists practice on a daily basis.
3. The exam preparation is easy. Not only is the content outlined in the blueprint in Table 2, but practice exams are available online from the ABIM and a tutorial can be found at www.abim.org/hospital-medicine-tutorial. This tutorial simulates the actual exam, to enhance preparation and reduce testing anxiety.
4. The exam pass rate is high. Table 3 lists pass rates from the 2010-2012 hospital medicine exam. These pass rates are equivalent to the general medicine exam, and they exceed some of the other specialty exam pass rates.
5. RFPHM is gaining more of the recognition it deserves. Given this growth in recognition, from employers, peers, patients, and maybe even payors, it would serve you well to start the process early, because it is highly likely to gain traction in the coming years.
Join Us
All told, RFPHM enrollment, preparation, and exam completion are straightforward, relatively easy, and worth the time and energy. I hope you join me and the 418 other hospitalists who have pursued this recognition. You will be glad you invested in your future.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
- American Board of Internal Medicine. List of self-evaluation modules. Available at: http://www.abim.org/maintenance-of-certification/medical-knowledge/modules.aspx#hosp. Accessed November 27, 2013.
- American Board of Internal Medicine. List of PIMs from ABIM. Available at: http://www.abim.org/moc/earning-points.aspx. Accessed November 27, 2013.
- American Board of Internal Medicine. List of PIMs from sponsoring institutions. Available at: http://www.abim.org/moc/earning-points/productinfo-demo-ordering.aspx#aqi. Accessed November 27, 2013.
Six Interventions To Radically Improve the U.S. Healthcare System

We talk a lot about value in healthcare these days. Most everyone in healthcare knows the infamous quality/cost equation: the lower the cost and the higher the quality, the higher the value. Seems like a pretty straightforward equation; there aren’t even any coefficients, factorials, exponents, or square roots. Just two simple terms: quality and cost. How complicated could that possibly be?
The problem with the value equation is not its complexity on paper but the reinforcing barriers in our healthcare system that have made it impossible to improve the value equation on a large scale. Despite millions of hard-working, well-intentioned people in the healthcare industry, quality continues to be variable at best, and cost continues to rise. Healthcare currently consumes nearly 18% of the U.S. gross domestic product, threatening other aspects of the American economy, notably education and other federally subsidized programs.
A series of articles published between The New England Journal of Medicine and the Harvard Business Review aims to discover and suggest solutions to the issues currently ailing the U.S. healthcare system.1 The first installment focused on how to improve value on a large scale. The authors discuss the major barriers to realizing the value equation, along with some propositions for overcoming these barriers on a large scale.2 Although all six barriers are extremely difficult to surmount, the authors argue that because they are all mutually reinforcing in the current state, all will need to be addressed swiftly, tenaciously, and simultaneously.
Outlined here is a summary of the proposed interventions, and how these can and will affect hospitalists.
1
Providers need to organize themselves around what patients need, instead of around what providers do and how they are reimbursed. This will entail a shift from individual, discrete services to comprehensive, patient-focused care of medical conditions. The authors term these “Integrated Practice Units (IPU),” in which an entire team of providers organize themselves around the patient’s disease and provide comprehensive care across the range of the severity of the disease and the locations in which that disease is best served.
For hospitalists, working in multidisciplinary teams will come as second nature, but this also will require hospitalists to enhance the flexibility with which they see the patients and provide services exactly as the patients need, rather than based on arbitrary schedules and conveniences. Many hospitalists are already involved in comprehensive specialty care of high-volume surgical conditions, such as total hip and total knee patients, who usually come with a relatively predictable set of co-morbid conditions, such as hypertension, diabetes, rheumatologic disease, or sickle cell anemia. The literature has clearly established the fact that high-volume specialty care centers can and do deliver higher value care (higher quality at lower cost), compared to lower volume, less “well-oiled” centers.
2
Providers need transparent and readily available information on quality and cost to move the value equation. As we all know, you can’t improve what you don’t measure. Hospitalists need to work collaboratively with their hospital systems to collect and widely report on quality and cost metrics for the patients they serve. These quality metrics should not only focus on those process and outcome measures that must currently be reported (internally or externally); hospitalists should seek out the metrics that really matter to patients, such as achieving functional status (ambulating, eating, being pain free), shortening recovery time (getting back to work, playing with the grandchildren), and sustaining recovery for as long as possible (relapse, readmission, reoperation).
Hospitalists should embrace the transparency of these metrics and encourage attribution of the metrics to individual providers or provider groups. Metric transparency stimulates rapid improvements and fosters goal alignment. Measurement and reporting of cost is absolutely essential in moving the value equation. Hospitalists should advocate for widespread transparency of the costs of tests, products, supplies, and manpower, and these should be freely and openly shared with patients and their families, to engage them in discussions about value.
3
Reimbursement for services should reflect the actual cost of the service and should be bundled. Many hospitalists are likely already involved in some demonstration projects around bundled payments for care across a continuum. Many CMS demonstration projects have focused on high-volume, predictable conditions (total hip arthroplasty, for instance) or high-volume, less predictable but costly conditions (such as congestive heart failure or COPD). Some large employers also are contracting with high volume hospitals to perform semi-elective procedures such as coronary artery bypass grafting, and sending their employees out of state to these centers of excellence. Most hospitalists are already at least conceptually comfortable with being held accountable for the cost and quality of certain patient types, including reducing unnecessary variation and spending and avoiding preventable complications.
4
Care should be integrated into a smaller number of large delivery systems, instead of a large number of small, “do-it-all” systems. These large systems have to actually work for the good of the patients, integrating their care and not just providing duplicate services in each location. Each center should be able to deliver excellent care in some conditions, not adequate care in all conditions. The more complicated, complex care should be delivered in tertiary care centers, and the more predictable, less heterogeneous care conditions should be addressed in lower-cost, community settings. Integrated systems can direct the right patients to the right location, to enhance both quality and cost.
5
On a related thread, healthcare systems need to focus patients on getting the right care in the right location and teach them to be less concerned about geography. In the days when hospital length of stays were routinely in the double digits, patients naturally opted to receive any and all care in a location close to their home and family. But now that hospital stays are generally in single digits, proximity to home is less important than good value of care, and healthcare systems need to steer patients to the best care delivery site, even if it is not near their homes. Some large employers have started reimbursing patients and their families for the cost associated with traveling to the correct site of care. With the availability of easy, low-cost travel options, this can and should be feasible for most patients and their families.
6
Information technology systems need to enable patient-centered care. Although this seemed to be the premise of EHRs, in reality, most have focused on enhancing billing, revenue, and documentation, rather than closely tracking the health, wellness, outcomes, and cost of individual patients throughout the care continuum. In the healthcare system of the future, the patient-centered EHR has to be readily accessible to all care providers, as well as to the patients themselves; it has to be easy to input and extract data; and it has to use common definitions for data.
Hospitalists would welcome such EHRs and should work tirelessly to achieve them within the healthcare system.
Conclusion
Although no single suggestion is wholly unappealing to the field of hospital medicine, accomplishing all of these quickly and simultaneously will be extremely challenging. It will take tremendous leadership and a bit of faith in the end goal. But the status quo is not an option, and current healthcare spending threatens the American Dream. Hospitalists can—and should—be pivotal in leading, or at least cooperating in, the achievement of this future-state, high-value healthcare system.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
We talk a lot about value in healthcare these days. Most everyone in healthcare knows the infamous quality/cost equation: the lower the cost and the higher the quality, the higher the value. Seems like a pretty straightforward equation; there aren’t even any coefficients, factorials, exponents, or square roots. Just two simple terms: quality and cost. How complicated could that possibly be?
The problem with the value equation is not its complexity on paper but the reinforcing barriers in our healthcare system that have made it impossible to improve the value equation on a large scale. Despite millions of hard-working, well-intentioned people in the healthcare industry, quality continues to be variable at best, and cost continues to rise. Healthcare currently consumes nearly 18% of the U.S. gross domestic product, threatening other aspects of the American economy, notably education and other federally subsidized programs.
A series of articles published between The New England Journal of Medicine and the Harvard Business Review aims to discover and suggest solutions to the issues currently ailing the U.S. healthcare system.1 The first installment focused on how to improve value on a large scale. The authors discuss the major barriers to realizing the value equation, along with some propositions for overcoming these barriers on a large scale.2 Although all six barriers are extremely difficult to surmount, the authors argue that because they are all mutually reinforcing in the current state, all will need to be addressed swiftly, tenaciously, and simultaneously.
Outlined here is a summary of the proposed interventions, and how these can and will affect hospitalists.
1
Providers need to organize themselves around what patients need, instead of around what providers do and how they are reimbursed. This will entail a shift from individual, discrete services to comprehensive, patient-focused care of medical conditions. The authors term these “Integrated Practice Units (IPU),” in which an entire team of providers organize themselves around the patient’s disease and provide comprehensive care across the range of the severity of the disease and the locations in which that disease is best served.
For hospitalists, working in multidisciplinary teams will come as second nature, but this also will require hospitalists to enhance the flexibility with which they see the patients and provide services exactly as the patients need, rather than based on arbitrary schedules and conveniences. Many hospitalists are already involved in comprehensive specialty care of high-volume surgical conditions, such as total hip and total knee patients, who usually come with a relatively predictable set of co-morbid conditions, such as hypertension, diabetes, rheumatologic disease, or sickle cell anemia. The literature has clearly established the fact that high-volume specialty care centers can and do deliver higher value care (higher quality at lower cost), compared to lower volume, less “well-oiled” centers.
2
Providers need transparent and readily available information on quality and cost to move the value equation. As we all know, you can’t improve what you don’t measure. Hospitalists need to work collaboratively with their hospital systems to collect and widely report on quality and cost metrics for the patients they serve. These quality metrics should not only focus on those process and outcome measures that must currently be reported (internally or externally); hospitalists should seek out the metrics that really matter to patients, such as achieving functional status (ambulating, eating, being pain free), shortening recovery time (getting back to work, playing with the grandchildren), and sustaining recovery for as long as possible (relapse, readmission, reoperation).
Hospitalists should embrace the transparency of these metrics and encourage attribution of the metrics to individual providers or provider groups. Metric transparency stimulates rapid improvements and fosters goal alignment. Measurement and reporting of cost is absolutely essential in moving the value equation. Hospitalists should advocate for widespread transparency of the costs of tests, products, supplies, and manpower, and these should be freely and openly shared with patients and their families, to engage them in discussions about value.
3
Reimbursement for services should reflect the actual cost of the service and should be bundled. Many hospitalists are likely already involved in some demonstration projects around bundled payments for care across a continuum. Many CMS demonstration projects have focused on high-volume, predictable conditions (total hip arthroplasty, for instance) or high-volume, less predictable but costly conditions (such as congestive heart failure or COPD). Some large employers also are contracting with high volume hospitals to perform semi-elective procedures such as coronary artery bypass grafting, and sending their employees out of state to these centers of excellence. Most hospitalists are already at least conceptually comfortable with being held accountable for the cost and quality of certain patient types, including reducing unnecessary variation and spending and avoiding preventable complications.
4
Care should be integrated into a smaller number of large delivery systems, instead of a large number of small, “do-it-all” systems. These large systems have to actually work for the good of the patients, integrating their care and not just providing duplicate services in each location. Each center should be able to deliver excellent care in some conditions, not adequate care in all conditions. The more complicated, complex care should be delivered in tertiary care centers, and the more predictable, less heterogeneous care conditions should be addressed in lower-cost, community settings. Integrated systems can direct the right patients to the right location, to enhance both quality and cost.
5
On a related thread, healthcare systems need to focus patients on getting the right care in the right location and teach them to be less concerned about geography. In the days when hospital length of stays were routinely in the double digits, patients naturally opted to receive any and all care in a location close to their home and family. But now that hospital stays are generally in single digits, proximity to home is less important than good value of care, and healthcare systems need to steer patients to the best care delivery site, even if it is not near their homes. Some large employers have started reimbursing patients and their families for the cost associated with traveling to the correct site of care. With the availability of easy, low-cost travel options, this can and should be feasible for most patients and their families.
6
Information technology systems need to enable patient-centered care. Although this seemed to be the premise of EHRs, in reality, most have focused on enhancing billing, revenue, and documentation, rather than closely tracking the health, wellness, outcomes, and cost of individual patients throughout the care continuum. In the healthcare system of the future, the patient-centered EHR has to be readily accessible to all care providers, as well as to the patients themselves; it has to be easy to input and extract data; and it has to use common definitions for data.
Hospitalists would welcome such EHRs and should work tirelessly to achieve them within the healthcare system.
Conclusion
Although no single suggestion is wholly unappealing to the field of hospital medicine, accomplishing all of these quickly and simultaneously will be extremely challenging. It will take tremendous leadership and a bit of faith in the end goal. But the status quo is not an option, and current healthcare spending threatens the American Dream. Hospitalists can—and should—be pivotal in leading, or at least cooperating in, the achievement of this future-state, high-value healthcare system.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
We talk a lot about value in healthcare these days. Most everyone in healthcare knows the infamous quality/cost equation: the lower the cost and the higher the quality, the higher the value. Seems like a pretty straightforward equation; there aren’t even any coefficients, factorials, exponents, or square roots. Just two simple terms: quality and cost. How complicated could that possibly be?
The problem with the value equation is not its complexity on paper but the reinforcing barriers in our healthcare system that have made it impossible to improve the value equation on a large scale. Despite millions of hard-working, well-intentioned people in the healthcare industry, quality continues to be variable at best, and cost continues to rise. Healthcare currently consumes nearly 18% of the U.S. gross domestic product, threatening other aspects of the American economy, notably education and other federally subsidized programs.
A series of articles published between The New England Journal of Medicine and the Harvard Business Review aims to discover and suggest solutions to the issues currently ailing the U.S. healthcare system.1 The first installment focused on how to improve value on a large scale. The authors discuss the major barriers to realizing the value equation, along with some propositions for overcoming these barriers on a large scale.2 Although all six barriers are extremely difficult to surmount, the authors argue that because they are all mutually reinforcing in the current state, all will need to be addressed swiftly, tenaciously, and simultaneously.
Outlined here is a summary of the proposed interventions, and how these can and will affect hospitalists.
1
Providers need to organize themselves around what patients need, instead of around what providers do and how they are reimbursed. This will entail a shift from individual, discrete services to comprehensive, patient-focused care of medical conditions. The authors term these “Integrated Practice Units (IPU),” in which an entire team of providers organize themselves around the patient’s disease and provide comprehensive care across the range of the severity of the disease and the locations in which that disease is best served.
For hospitalists, working in multidisciplinary teams will come as second nature, but this also will require hospitalists to enhance the flexibility with which they see the patients and provide services exactly as the patients need, rather than based on arbitrary schedules and conveniences. Many hospitalists are already involved in comprehensive specialty care of high-volume surgical conditions, such as total hip and total knee patients, who usually come with a relatively predictable set of co-morbid conditions, such as hypertension, diabetes, rheumatologic disease, or sickle cell anemia. The literature has clearly established the fact that high-volume specialty care centers can and do deliver higher value care (higher quality at lower cost), compared to lower volume, less “well-oiled” centers.
2
Providers need transparent and readily available information on quality and cost to move the value equation. As we all know, you can’t improve what you don’t measure. Hospitalists need to work collaboratively with their hospital systems to collect and widely report on quality and cost metrics for the patients they serve. These quality metrics should not only focus on those process and outcome measures that must currently be reported (internally or externally); hospitalists should seek out the metrics that really matter to patients, such as achieving functional status (ambulating, eating, being pain free), shortening recovery time (getting back to work, playing with the grandchildren), and sustaining recovery for as long as possible (relapse, readmission, reoperation).
Hospitalists should embrace the transparency of these metrics and encourage attribution of the metrics to individual providers or provider groups. Metric transparency stimulates rapid improvements and fosters goal alignment. Measurement and reporting of cost is absolutely essential in moving the value equation. Hospitalists should advocate for widespread transparency of the costs of tests, products, supplies, and manpower, and these should be freely and openly shared with patients and their families, to engage them in discussions about value.
3
Reimbursement for services should reflect the actual cost of the service and should be bundled. Many hospitalists are likely already involved in some demonstration projects around bundled payments for care across a continuum. Many CMS demonstration projects have focused on high-volume, predictable conditions (total hip arthroplasty, for instance) or high-volume, less predictable but costly conditions (such as congestive heart failure or COPD). Some large employers also are contracting with high volume hospitals to perform semi-elective procedures such as coronary artery bypass grafting, and sending their employees out of state to these centers of excellence. Most hospitalists are already at least conceptually comfortable with being held accountable for the cost and quality of certain patient types, including reducing unnecessary variation and spending and avoiding preventable complications.
4
Care should be integrated into a smaller number of large delivery systems, instead of a large number of small, “do-it-all” systems. These large systems have to actually work for the good of the patients, integrating their care and not just providing duplicate services in each location. Each center should be able to deliver excellent care in some conditions, not adequate care in all conditions. The more complicated, complex care should be delivered in tertiary care centers, and the more predictable, less heterogeneous care conditions should be addressed in lower-cost, community settings. Integrated systems can direct the right patients to the right location, to enhance both quality and cost.
5
On a related thread, healthcare systems need to focus patients on getting the right care in the right location and teach them to be less concerned about geography. In the days when hospital length of stays were routinely in the double digits, patients naturally opted to receive any and all care in a location close to their home and family. But now that hospital stays are generally in single digits, proximity to home is less important than good value of care, and healthcare systems need to steer patients to the best care delivery site, even if it is not near their homes. Some large employers have started reimbursing patients and their families for the cost associated with traveling to the correct site of care. With the availability of easy, low-cost travel options, this can and should be feasible for most patients and their families.
6
Information technology systems need to enable patient-centered care. Although this seemed to be the premise of EHRs, in reality, most have focused on enhancing billing, revenue, and documentation, rather than closely tracking the health, wellness, outcomes, and cost of individual patients throughout the care continuum. In the healthcare system of the future, the patient-centered EHR has to be readily accessible to all care providers, as well as to the patients themselves; it has to be easy to input and extract data; and it has to use common definitions for data.
Hospitalists would welcome such EHRs and should work tirelessly to achieve them within the healthcare system.
Conclusion
Although no single suggestion is wholly unappealing to the field of hospital medicine, accomplishing all of these quickly and simultaneously will be extremely challenging. It will take tremendous leadership and a bit of faith in the end goal. But the status quo is not an option, and current healthcare spending threatens the American Dream. Hospitalists can—and should—be pivotal in leading, or at least cooperating in, the achievement of this future-state, high-value healthcare system.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
References
Report on England’s Health System Mirrors Need for Improvement in U.S.

Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.
Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at scheured@musc.edu.