User login
Measles: More than the rash
To the Editor: I read the excellent overview article on measles by Drs. Kumar and Sabella.1 However, there are additional important clinical points regarding measles diagnosis that deserve further comment. Prior to definitive diagnosis, measles is a clinical diagnosis. Properly, much attention is given to the rash, but there are important clinical clues besides the rash that are helpful diagnostically.
Some clinical findings are more characteristic of a disease than others, eg, eye findings in measles, and clinicians should specifically look for them. Other findings not characteristic but consistent with the diagnosis are less helpful, eg, measles with diarrhea.2 Measles is a systemic infection with several extradermatologic manifestations. Characteristically, measles involves the respiratory tract, manifested by runny nose, dry cough, or shortness of breath, ie, measles pneumonia.2
Gastrointestinal involvement may be manifested as nausea, vomiting, diarrhea, or abdominal pain. Abdominal pain, when located in the right lower quadrant, may mimic acute appendicitis, ie, pseudoappendicitis. In patients undergoing appendectomy, pathologically the appendix is normal but contains multinucleated giant cells (Warthin-Finkeldey cells). Measles pseudoappendicitis can be perplexing because it presents before the rash. Even without appendiceal involvement (pseudoappendicitis), Warthin-Finkeldey cells are also present in the nasal mucosa. If nasal swab cytology shows Warthin-Finkeldey cells, an early diagnosis of measles may be made days before IgM measles antibodies are reported.3
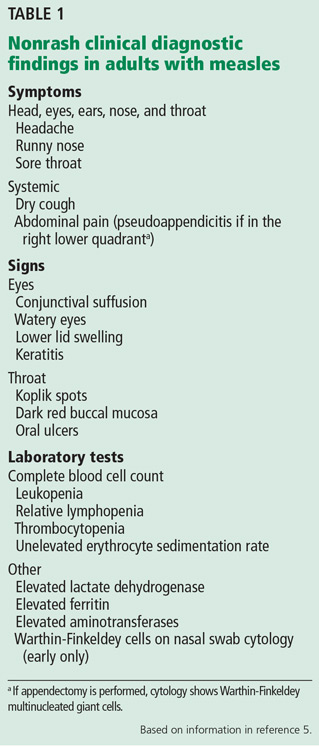
Other often-overlooked important clues are eye findings, eg, watery eyes, lower lid edema, conjunctival suffusion, and keratitis. No other disease in the differential diagnosis of measles presents with watery eyes with bilateral lower lid edema and conjunctival suffusion. Headache, mental confusion or oral ulcers may suggest alternate diagnoses. Typically, nonspecific laboratory abnormalities include leukopenia and thrombocytopenia, and importantly, the erythrocyte sedimentation rate is not elevated (Table 1).4,5
In measles, much is made of Koplik spots, which are found early on dark red buccal mucosa (vs Fordyce spots).1 However, if these are missed or not present, clinicians can use other characteristic findings to make a presumptive diagnosis of measles.
- Kumar D, Sabella C. Measles: back again. Cleve Clin J Med 2016; 83:340–344.
- Leibovici L, Sharir T, Kalter-Leibovici O, Alpert G, Epstein LM. An outbreak of measles among young adults. Clinical and laboratory features in 461 patients. J Adolesc Health Care 1988; 9:203–207.
- Cunha BA, Hage JE, Turi GK. A 45-year-old male with rash, fever and diarrhea. J Clin Microbiol 2012; 50:1835,2184.
- Cunha BA, Mickail N. Fever and rash in an adult traveler: the many masquerades of measles. Travel Med Inf Dis 2011; 9:255–257.
- Cunha CB, Cunha BA. Rash and fever in the intensive care unit. In: Fink MP, Abraham E, Vincent JL, Kochanek P, editors. Textbook of Critical Care Medicine (7th Ed). Elsevier, Philadelphia, 2016:97–115.
To the Editor: I read the excellent overview article on measles by Drs. Kumar and Sabella.1 However, there are additional important clinical points regarding measles diagnosis that deserve further comment. Prior to definitive diagnosis, measles is a clinical diagnosis. Properly, much attention is given to the rash, but there are important clinical clues besides the rash that are helpful diagnostically.
Some clinical findings are more characteristic of a disease than others, eg, eye findings in measles, and clinicians should specifically look for them. Other findings not characteristic but consistent with the diagnosis are less helpful, eg, measles with diarrhea.2 Measles is a systemic infection with several extradermatologic manifestations. Characteristically, measles involves the respiratory tract, manifested by runny nose, dry cough, or shortness of breath, ie, measles pneumonia.2
Gastrointestinal involvement may be manifested as nausea, vomiting, diarrhea, or abdominal pain. Abdominal pain, when located in the right lower quadrant, may mimic acute appendicitis, ie, pseudoappendicitis. In patients undergoing appendectomy, pathologically the appendix is normal but contains multinucleated giant cells (Warthin-Finkeldey cells). Measles pseudoappendicitis can be perplexing because it presents before the rash. Even without appendiceal involvement (pseudoappendicitis), Warthin-Finkeldey cells are also present in the nasal mucosa. If nasal swab cytology shows Warthin-Finkeldey cells, an early diagnosis of measles may be made days before IgM measles antibodies are reported.3
Other often-overlooked important clues are eye findings, eg, watery eyes, lower lid edema, conjunctival suffusion, and keratitis. No other disease in the differential diagnosis of measles presents with watery eyes with bilateral lower lid edema and conjunctival suffusion. Headache, mental confusion or oral ulcers may suggest alternate diagnoses. Typically, nonspecific laboratory abnormalities include leukopenia and thrombocytopenia, and importantly, the erythrocyte sedimentation rate is not elevated (Table 1).4,5
In measles, much is made of Koplik spots, which are found early on dark red buccal mucosa (vs Fordyce spots).1 However, if these are missed or not present, clinicians can use other characteristic findings to make a presumptive diagnosis of measles.
To the Editor: I read the excellent overview article on measles by Drs. Kumar and Sabella.1 However, there are additional important clinical points regarding measles diagnosis that deserve further comment. Prior to definitive diagnosis, measles is a clinical diagnosis. Properly, much attention is given to the rash, but there are important clinical clues besides the rash that are helpful diagnostically.
Some clinical findings are more characteristic of a disease than others, eg, eye findings in measles, and clinicians should specifically look for them. Other findings not characteristic but consistent with the diagnosis are less helpful, eg, measles with diarrhea.2 Measles is a systemic infection with several extradermatologic manifestations. Characteristically, measles involves the respiratory tract, manifested by runny nose, dry cough, or shortness of breath, ie, measles pneumonia.2
Gastrointestinal involvement may be manifested as nausea, vomiting, diarrhea, or abdominal pain. Abdominal pain, when located in the right lower quadrant, may mimic acute appendicitis, ie, pseudoappendicitis. In patients undergoing appendectomy, pathologically the appendix is normal but contains multinucleated giant cells (Warthin-Finkeldey cells). Measles pseudoappendicitis can be perplexing because it presents before the rash. Even without appendiceal involvement (pseudoappendicitis), Warthin-Finkeldey cells are also present in the nasal mucosa. If nasal swab cytology shows Warthin-Finkeldey cells, an early diagnosis of measles may be made days before IgM measles antibodies are reported.3
Other often-overlooked important clues are eye findings, eg, watery eyes, lower lid edema, conjunctival suffusion, and keratitis. No other disease in the differential diagnosis of measles presents with watery eyes with bilateral lower lid edema and conjunctival suffusion. Headache, mental confusion or oral ulcers may suggest alternate diagnoses. Typically, nonspecific laboratory abnormalities include leukopenia and thrombocytopenia, and importantly, the erythrocyte sedimentation rate is not elevated (Table 1).4,5
In measles, much is made of Koplik spots, which are found early on dark red buccal mucosa (vs Fordyce spots).1 However, if these are missed or not present, clinicians can use other characteristic findings to make a presumptive diagnosis of measles.
- Kumar D, Sabella C. Measles: back again. Cleve Clin J Med 2016; 83:340–344.
- Leibovici L, Sharir T, Kalter-Leibovici O, Alpert G, Epstein LM. An outbreak of measles among young adults. Clinical and laboratory features in 461 patients. J Adolesc Health Care 1988; 9:203–207.
- Cunha BA, Hage JE, Turi GK. A 45-year-old male with rash, fever and diarrhea. J Clin Microbiol 2012; 50:1835,2184.
- Cunha BA, Mickail N. Fever and rash in an adult traveler: the many masquerades of measles. Travel Med Inf Dis 2011; 9:255–257.
- Cunha CB, Cunha BA. Rash and fever in the intensive care unit. In: Fink MP, Abraham E, Vincent JL, Kochanek P, editors. Textbook of Critical Care Medicine (7th Ed). Elsevier, Philadelphia, 2016:97–115.
- Kumar D, Sabella C. Measles: back again. Cleve Clin J Med 2016; 83:340–344.
- Leibovici L, Sharir T, Kalter-Leibovici O, Alpert G, Epstein LM. An outbreak of measles among young adults. Clinical and laboratory features in 461 patients. J Adolesc Health Care 1988; 9:203–207.
- Cunha BA, Hage JE, Turi GK. A 45-year-old male with rash, fever and diarrhea. J Clin Microbiol 2012; 50:1835,2184.
- Cunha BA, Mickail N. Fever and rash in an adult traveler: the many masquerades of measles. Travel Med Inf Dis 2011; 9:255–257.
- Cunha CB, Cunha BA. Rash and fever in the intensive care unit. In: Fink MP, Abraham E, Vincent JL, Kochanek P, editors. Textbook of Critical Care Medicine (7th Ed). Elsevier, Philadelphia, 2016:97–115.
Enterovirus D-68 presenting with acute pancreatitis
To the Editor: We read the review on enterovirus D681 (EV-D68) with great interest, and we thought it merited comment.
During the current influenza season, we have had several adult cases of EV-D68 presenting as an influenza-like illness. EV-D68 was diagnosed by nasal swab viral film array polymerase chain reaction (PCR) testing. We agree with the authors that the clinical spectrum of enteroviral infection includes a variety of extraintestinal manifestations, eg, acute pancreatitis. As more cases of EV-D68 are described, the range of clinical manifestations will be increased.2–5
We recently saw a 27-year-old woman who presented with an influenza-like illness, but with a main complaint of right-upper-quadrant abdominal pain. She denied recent travel or contacts with sick children or adults. Her past medical history was unremarkable, and she was not taking any medications. The physical examination was unremarkable except for moderately severe tenderness in the right upper quadrant, with no rebound or guarding.
Results of laboratory testing at hospital admission included a white blood cell count of 7.3 × 109/L (49% neutrophils, 41% lymphocytes, 7% monocytes, 3% eosinophils), a normal platelet count, serum lipase 73 U/L (reference range 5.6–51.3 U/L), and serum amylase 211 U/L (37–121 U/L). Serum aminotransferase and alkaline phosphatase levels were normal. Abdominal ultrasonography was unremarkable. Nasal swab for multiplex PCR testing for respiratory viruses was positive for human rhinovirus-enterovirus. Further PCR testing was positive for EV-D68 (New York State Department of Health, Wadsworth Laboratory). Her abdominal pain was treated symptomatically; she gradually improved and was discharged.
This instance of EV-D68 in a healthy 27-year-old woman presenting with influenza-like illness and acute pain in the right upper quadrant is the first we have seen of EV-D68 presenting as acute pancreatitis. Clinicians should be aware that EV-D68, like influenza, may present with gastrointestinal manifestations.
- Foster CB, Friedman N, Carl J, Piedimonte G. Enterovirus D68: a clinically important respiratory enterovirus. Cleve Clin J Med 2015; 82:26–31.
- Tokarz R, Firth C, Madhi SA, et al. Worldwide emergence of multiple clades of enterovirus 68. J Gen Virol 2012; 93:1952–1958.
- Oberste MS, Maher K, Schnurr D, et al. Enterovirus 68 is associated with respiratory illness and shares biological features with both the enteroviruses and the rhinoviruses. J Gen Virol 2004; 85:2577–2584.
- Rahamat-Langendoen J, Riezebos-Brilman A, Borger R, et al. Upsurge of human enterovirus 68 infections in patients with severe respiratory tract infections. J Clin Virol 2011; 52:103–106.
- Midgley CM, Jackson MA, Selvarangan R, et al. Severe respiratory illness associated with enterovirus D68 – Missouri and Illinois, 2014. MMWR 2014; 63:798–799.
To the Editor: We read the review on enterovirus D681 (EV-D68) with great interest, and we thought it merited comment.
During the current influenza season, we have had several adult cases of EV-D68 presenting as an influenza-like illness. EV-D68 was diagnosed by nasal swab viral film array polymerase chain reaction (PCR) testing. We agree with the authors that the clinical spectrum of enteroviral infection includes a variety of extraintestinal manifestations, eg, acute pancreatitis. As more cases of EV-D68 are described, the range of clinical manifestations will be increased.2–5
We recently saw a 27-year-old woman who presented with an influenza-like illness, but with a main complaint of right-upper-quadrant abdominal pain. She denied recent travel or contacts with sick children or adults. Her past medical history was unremarkable, and she was not taking any medications. The physical examination was unremarkable except for moderately severe tenderness in the right upper quadrant, with no rebound or guarding.
Results of laboratory testing at hospital admission included a white blood cell count of 7.3 × 109/L (49% neutrophils, 41% lymphocytes, 7% monocytes, 3% eosinophils), a normal platelet count, serum lipase 73 U/L (reference range 5.6–51.3 U/L), and serum amylase 211 U/L (37–121 U/L). Serum aminotransferase and alkaline phosphatase levels were normal. Abdominal ultrasonography was unremarkable. Nasal swab for multiplex PCR testing for respiratory viruses was positive for human rhinovirus-enterovirus. Further PCR testing was positive for EV-D68 (New York State Department of Health, Wadsworth Laboratory). Her abdominal pain was treated symptomatically; she gradually improved and was discharged.
This instance of EV-D68 in a healthy 27-year-old woman presenting with influenza-like illness and acute pain in the right upper quadrant is the first we have seen of EV-D68 presenting as acute pancreatitis. Clinicians should be aware that EV-D68, like influenza, may present with gastrointestinal manifestations.
To the Editor: We read the review on enterovirus D681 (EV-D68) with great interest, and we thought it merited comment.
During the current influenza season, we have had several adult cases of EV-D68 presenting as an influenza-like illness. EV-D68 was diagnosed by nasal swab viral film array polymerase chain reaction (PCR) testing. We agree with the authors that the clinical spectrum of enteroviral infection includes a variety of extraintestinal manifestations, eg, acute pancreatitis. As more cases of EV-D68 are described, the range of clinical manifestations will be increased.2–5
We recently saw a 27-year-old woman who presented with an influenza-like illness, but with a main complaint of right-upper-quadrant abdominal pain. She denied recent travel or contacts with sick children or adults. Her past medical history was unremarkable, and she was not taking any medications. The physical examination was unremarkable except for moderately severe tenderness in the right upper quadrant, with no rebound or guarding.
Results of laboratory testing at hospital admission included a white blood cell count of 7.3 × 109/L (49% neutrophils, 41% lymphocytes, 7% monocytes, 3% eosinophils), a normal platelet count, serum lipase 73 U/L (reference range 5.6–51.3 U/L), and serum amylase 211 U/L (37–121 U/L). Serum aminotransferase and alkaline phosphatase levels were normal. Abdominal ultrasonography was unremarkable. Nasal swab for multiplex PCR testing for respiratory viruses was positive for human rhinovirus-enterovirus. Further PCR testing was positive for EV-D68 (New York State Department of Health, Wadsworth Laboratory). Her abdominal pain was treated symptomatically; she gradually improved and was discharged.
This instance of EV-D68 in a healthy 27-year-old woman presenting with influenza-like illness and acute pain in the right upper quadrant is the first we have seen of EV-D68 presenting as acute pancreatitis. Clinicians should be aware that EV-D68, like influenza, may present with gastrointestinal manifestations.
- Foster CB, Friedman N, Carl J, Piedimonte G. Enterovirus D68: a clinically important respiratory enterovirus. Cleve Clin J Med 2015; 82:26–31.
- Tokarz R, Firth C, Madhi SA, et al. Worldwide emergence of multiple clades of enterovirus 68. J Gen Virol 2012; 93:1952–1958.
- Oberste MS, Maher K, Schnurr D, et al. Enterovirus 68 is associated with respiratory illness and shares biological features with both the enteroviruses and the rhinoviruses. J Gen Virol 2004; 85:2577–2584.
- Rahamat-Langendoen J, Riezebos-Brilman A, Borger R, et al. Upsurge of human enterovirus 68 infections in patients with severe respiratory tract infections. J Clin Virol 2011; 52:103–106.
- Midgley CM, Jackson MA, Selvarangan R, et al. Severe respiratory illness associated with enterovirus D68 – Missouri and Illinois, 2014. MMWR 2014; 63:798–799.
- Foster CB, Friedman N, Carl J, Piedimonte G. Enterovirus D68: a clinically important respiratory enterovirus. Cleve Clin J Med 2015; 82:26–31.
- Tokarz R, Firth C, Madhi SA, et al. Worldwide emergence of multiple clades of enterovirus 68. J Gen Virol 2012; 93:1952–1958.
- Oberste MS, Maher K, Schnurr D, et al. Enterovirus 68 is associated with respiratory illness and shares biological features with both the enteroviruses and the rhinoviruses. J Gen Virol 2004; 85:2577–2584.
- Rahamat-Langendoen J, Riezebos-Brilman A, Borger R, et al. Upsurge of human enterovirus 68 infections in patients with severe respiratory tract infections. J Clin Virol 2011; 52:103–106.
- Midgley CM, Jackson MA, Selvarangan R, et al. Severe respiratory illness associated with enterovirus D68 – Missouri and Illinois, 2014. MMWR 2014; 63:798–799.