User login
European Society of Cardiology (ESC): EuroPRevent 2013
Cardiac rehabilitation benefits elderly heart failure patients
ROME – A multiweek program of cardiac rehabilitation is as beneficial in elderly patients with chronic heart failure as it is in younger heart failure patients, according to a review of 243 patients at one Belgium center.
"Although they have lower exercise capacity at baseline, older patients have at least as much benefit from an exercise program as younger patients with chronic heart failure," Ms. Sofie Pardaens* reported in a poster at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation.
A second analysis by Ms. Pardaens, a researcher at Ghent (Belgium) University, and her associates, reported in a separate poster, showed that a prolonged cardiac rehabilitation program was as effective in patients recently discharged from a heart failure hospitalization as it was in patients following cardiac surgery or after an acute coronary syndrome (ACS) event.

Their assessment of cardiac rehabilitation relative to a patient’s age included 243 patients who participated in a rehabilitation program at the University of Ghent, who had chronic heart failure, and who had an amino-terminal pro-B-type natriuretic peptide value of at least 400 pg/mL, a level very suggestive of heart failure (Circulation 2011;123:2015-9). The group included 43 patients (18%) who were at least 75 years old (average, 78 years) and 68 patients younger than 60 (average, 51 years), with the remaining 132 patients evenly distributed across the range of 60-74 years old.
All participants had just been hospitalized, for an ACS event, cardiac surgery, or heart failure.
The hospital-based rehabilitation program combined aerobic and strength training, and was designed to bring a patient’s heart rate to his anaerobic threshold during each session. Sessions occurred two or three times a week, and the full program included 45 sessions over a period of 4-5 months. The patients studied averaged 34 sessions each; patients aged 75 or older averaged 32 sessions each, while those younger than 60 averaged 35 sessions each.
The researchers measured peak exercise capacity using cardiopulmonary exercise testing at baseline and at the end of the rehabilitation session sequence, and found that the 16% average level of improvement among patients at least 75 years old closely matched the average 19% improvement among the patients younger than 60, and the 17% average improvement among everyone else, Ms. Pardaens and her associates reported. All age groups also showed similar improvements in their average ventilatory equivalence ratio, as well as their average 6-minute walk distance; however, the 29% average increased distance among patients younger than 60 years significantly exceeded the 19% average increase among those aged 75 or older.
The group’s second analysis focused on the 371 patients who underwent cardiac rehabilitation at the University of Ghent during January 2010 through May 2012 from among the 1,253 patients hospitalized during this period for an acute coronary syndrome event, cardiac surgery, or heart failure. In this pool of more than 1,000 patients who were potentially eligible to participate, only 30% actually enrolled in the rehabilitation program. The cardiac rehabilitation program again involved two to three sessions per week, with a goal for patients to complete 45 sessions within 5 months.
The sign-up rate for rehabilitation lagged even more among the 428 patients from the larger group whose index hospitalization had been for heart failure, with 37 of the acute heart failure patients (9%) actually engaging in rehabilitation. Rehabilitation participation was highest, a 56% rate, among the 358 patients who had been hospitalized for cardiac surgery, with a 28% uptake rate among 467 patients who had an ACS event.
Despite the low, 9% uptake of cardiac rehabilitation in heart failure patients, their benefit from participation closely tracked the benefit seen in surgery and ACS patients. Improvement in peak exercise capacity over baseline at the end of rehabilitation averaged 19% in the heart failure patients, 17% in the ACS patients, and 24% in the surgery patients, differences that were not statistically significant, reported Ms. Pardaens. All three subgroups also had similar average improvements in their 6-minute walk distance, which rose by an average of 21% in the heart failure patients and by averages of 27% and 28% in the other two subgroups.
Based on the efficacy but low usage of cardiac rehabilitation, future research should examine ways to boost its use by heart failure patients, concluded Ms. Pardaens.
Ms. Pardaens and her associates said they had no relevant financial disclosures.
On Twitter @mitchelzoler
*Correction 6/28/13: An earlier version of this article incorrectly reported researcher Sofie Pardaens' title. She is currently studying for her PhD in the department of internal medicine at Ghent University.
Cardiac rehabilitation is undoubtedly an essential component of the contemporary treatment of patients with coronary disease and heart failure.
Exercise training has the potential to act as a catalyst for promoting other aspects of rehabilitation, including risk factor modification through therapeutic lifestyle changes and optimization of psychosocial support. Similarly, among patients who are elderly, such outcome measures may include the achievement of functional independence, the prevention of premature disability, and a reduction in the need for custodial care.
Despite limited data, older patients have shown improvement in their exercise tolerance comparable to that of younger patients participating in equivalent exercise programs. In addition, the safety of exercise within cardiac rehabilitation programs is well accepted and established.
Dr. Jun Chiong is associate professor of medicine at Loma Linda (Calif.) University Medical Center. He is on the on the advisory board of CHEST Physician.
Cardiac rehabilitation is undoubtedly an essential component of the contemporary treatment of patients with coronary disease and heart failure.
Exercise training has the potential to act as a catalyst for promoting other aspects of rehabilitation, including risk factor modification through therapeutic lifestyle changes and optimization of psychosocial support. Similarly, among patients who are elderly, such outcome measures may include the achievement of functional independence, the prevention of premature disability, and a reduction in the need for custodial care.
Despite limited data, older patients have shown improvement in their exercise tolerance comparable to that of younger patients participating in equivalent exercise programs. In addition, the safety of exercise within cardiac rehabilitation programs is well accepted and established.
Dr. Jun Chiong is associate professor of medicine at Loma Linda (Calif.) University Medical Center. He is on the on the advisory board of CHEST Physician.
Cardiac rehabilitation is undoubtedly an essential component of the contemporary treatment of patients with coronary disease and heart failure.
Exercise training has the potential to act as a catalyst for promoting other aspects of rehabilitation, including risk factor modification through therapeutic lifestyle changes and optimization of psychosocial support. Similarly, among patients who are elderly, such outcome measures may include the achievement of functional independence, the prevention of premature disability, and a reduction in the need for custodial care.
Despite limited data, older patients have shown improvement in their exercise tolerance comparable to that of younger patients participating in equivalent exercise programs. In addition, the safety of exercise within cardiac rehabilitation programs is well accepted and established.
Dr. Jun Chiong is associate professor of medicine at Loma Linda (Calif.) University Medical Center. He is on the on the advisory board of CHEST Physician.
ROME – A multiweek program of cardiac rehabilitation is as beneficial in elderly patients with chronic heart failure as it is in younger heart failure patients, according to a review of 243 patients at one Belgium center.
"Although they have lower exercise capacity at baseline, older patients have at least as much benefit from an exercise program as younger patients with chronic heart failure," Ms. Sofie Pardaens* reported in a poster at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation.
A second analysis by Ms. Pardaens, a researcher at Ghent (Belgium) University, and her associates, reported in a separate poster, showed that a prolonged cardiac rehabilitation program was as effective in patients recently discharged from a heart failure hospitalization as it was in patients following cardiac surgery or after an acute coronary syndrome (ACS) event.
Their assessment of cardiac rehabilitation relative to a patient’s age included 243 patients who participated in a rehabilitation program at the University of Ghent, who had chronic heart failure, and who had an amino-terminal pro-B-type natriuretic peptide value of at least 400 pg/mL, a level very suggestive of heart failure (Circulation 2011;123:2015-9). The group included 43 patients (18%) who were at least 75 years old (average, 78 years) and 68 patients younger than 60 (average, 51 years), with the remaining 132 patients evenly distributed across the range of 60-74 years old.
All participants had just been hospitalized, for an ACS event, cardiac surgery, or heart failure.
The hospital-based rehabilitation program combined aerobic and strength training, and was designed to bring a patient’s heart rate to his anaerobic threshold during each session. Sessions occurred two or three times a week, and the full program included 45 sessions over a period of 4-5 months. The patients studied averaged 34 sessions each; patients aged 75 or older averaged 32 sessions each, while those younger than 60 averaged 35 sessions each.
The researchers measured peak exercise capacity using cardiopulmonary exercise testing at baseline and at the end of the rehabilitation session sequence, and found that the 16% average level of improvement among patients at least 75 years old closely matched the average 19% improvement among the patients younger than 60, and the 17% average improvement among everyone else, Ms. Pardaens and her associates reported. All age groups also showed similar improvements in their average ventilatory equivalence ratio, as well as their average 6-minute walk distance; however, the 29% average increased distance among patients younger than 60 years significantly exceeded the 19% average increase among those aged 75 or older.
The group’s second analysis focused on the 371 patients who underwent cardiac rehabilitation at the University of Ghent during January 2010 through May 2012 from among the 1,253 patients hospitalized during this period for an acute coronary syndrome event, cardiac surgery, or heart failure. In this pool of more than 1,000 patients who were potentially eligible to participate, only 30% actually enrolled in the rehabilitation program. The cardiac rehabilitation program again involved two to three sessions per week, with a goal for patients to complete 45 sessions within 5 months.
The sign-up rate for rehabilitation lagged even more among the 428 patients from the larger group whose index hospitalization had been for heart failure, with 37 of the acute heart failure patients (9%) actually engaging in rehabilitation. Rehabilitation participation was highest, a 56% rate, among the 358 patients who had been hospitalized for cardiac surgery, with a 28% uptake rate among 467 patients who had an ACS event.
Despite the low, 9% uptake of cardiac rehabilitation in heart failure patients, their benefit from participation closely tracked the benefit seen in surgery and ACS patients. Improvement in peak exercise capacity over baseline at the end of rehabilitation averaged 19% in the heart failure patients, 17% in the ACS patients, and 24% in the surgery patients, differences that were not statistically significant, reported Ms. Pardaens. All three subgroups also had similar average improvements in their 6-minute walk distance, which rose by an average of 21% in the heart failure patients and by averages of 27% and 28% in the other two subgroups.
Based on the efficacy but low usage of cardiac rehabilitation, future research should examine ways to boost its use by heart failure patients, concluded Ms. Pardaens.
Ms. Pardaens and her associates said they had no relevant financial disclosures.
On Twitter @mitchelzoler
*Correction 6/28/13: An earlier version of this article incorrectly reported researcher Sofie Pardaens' title. She is currently studying for her PhD in the department of internal medicine at Ghent University.
ROME – A multiweek program of cardiac rehabilitation is as beneficial in elderly patients with chronic heart failure as it is in younger heart failure patients, according to a review of 243 patients at one Belgium center.
"Although they have lower exercise capacity at baseline, older patients have at least as much benefit from an exercise program as younger patients with chronic heart failure," Ms. Sofie Pardaens* reported in a poster at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation.
A second analysis by Ms. Pardaens, a researcher at Ghent (Belgium) University, and her associates, reported in a separate poster, showed that a prolonged cardiac rehabilitation program was as effective in patients recently discharged from a heart failure hospitalization as it was in patients following cardiac surgery or after an acute coronary syndrome (ACS) event.
Their assessment of cardiac rehabilitation relative to a patient’s age included 243 patients who participated in a rehabilitation program at the University of Ghent, who had chronic heart failure, and who had an amino-terminal pro-B-type natriuretic peptide value of at least 400 pg/mL, a level very suggestive of heart failure (Circulation 2011;123:2015-9). The group included 43 patients (18%) who were at least 75 years old (average, 78 years) and 68 patients younger than 60 (average, 51 years), with the remaining 132 patients evenly distributed across the range of 60-74 years old.
All participants had just been hospitalized, for an ACS event, cardiac surgery, or heart failure.
The hospital-based rehabilitation program combined aerobic and strength training, and was designed to bring a patient’s heart rate to his anaerobic threshold during each session. Sessions occurred two or three times a week, and the full program included 45 sessions over a period of 4-5 months. The patients studied averaged 34 sessions each; patients aged 75 or older averaged 32 sessions each, while those younger than 60 averaged 35 sessions each.
The researchers measured peak exercise capacity using cardiopulmonary exercise testing at baseline and at the end of the rehabilitation session sequence, and found that the 16% average level of improvement among patients at least 75 years old closely matched the average 19% improvement among the patients younger than 60, and the 17% average improvement among everyone else, Ms. Pardaens and her associates reported. All age groups also showed similar improvements in their average ventilatory equivalence ratio, as well as their average 6-minute walk distance; however, the 29% average increased distance among patients younger than 60 years significantly exceeded the 19% average increase among those aged 75 or older.
The group’s second analysis focused on the 371 patients who underwent cardiac rehabilitation at the University of Ghent during January 2010 through May 2012 from among the 1,253 patients hospitalized during this period for an acute coronary syndrome event, cardiac surgery, or heart failure. In this pool of more than 1,000 patients who were potentially eligible to participate, only 30% actually enrolled in the rehabilitation program. The cardiac rehabilitation program again involved two to three sessions per week, with a goal for patients to complete 45 sessions within 5 months.
The sign-up rate for rehabilitation lagged even more among the 428 patients from the larger group whose index hospitalization had been for heart failure, with 37 of the acute heart failure patients (9%) actually engaging in rehabilitation. Rehabilitation participation was highest, a 56% rate, among the 358 patients who had been hospitalized for cardiac surgery, with a 28% uptake rate among 467 patients who had an ACS event.
Despite the low, 9% uptake of cardiac rehabilitation in heart failure patients, their benefit from participation closely tracked the benefit seen in surgery and ACS patients. Improvement in peak exercise capacity over baseline at the end of rehabilitation averaged 19% in the heart failure patients, 17% in the ACS patients, and 24% in the surgery patients, differences that were not statistically significant, reported Ms. Pardaens. All three subgroups also had similar average improvements in their 6-minute walk distance, which rose by an average of 21% in the heart failure patients and by averages of 27% and 28% in the other two subgroups.
Based on the efficacy but low usage of cardiac rehabilitation, future research should examine ways to boost its use by heart failure patients, concluded Ms. Pardaens.
Ms. Pardaens and her associates said they had no relevant financial disclosures.
On Twitter @mitchelzoler
*Correction 6/28/13: An earlier version of this article incorrectly reported researcher Sofie Pardaens' title. She is currently studying for her PhD in the department of internal medicine at Ghent University.
AT EUROPREVENT 2013
Major finding: Cardiac rehabilitation boosted exercise capacity by an average 16% in elderly patients and an average 19% in younger patients.
Data source: Data came from a review of 243 patients with chronic heart failure who participated in cardiac rehabilitation at one Belgium center.
Disclosures: Dr. Pardaens and her associates said they had no relevant financial disclosures.

Exercise-capacity decline hastened by congenital heart disease
ROME – Young adults with congenital heart disease lose roughly 1% of their predicted exercise capacity each year, based on follow-up of more than 500 patients at one German center.
The "slow but persistent decline" in patients with congenital heart disease "exceeds the decline of reference values for age" compiled in 2009 from the general German population, Jan Müller, Ph.D., said at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
Results from prior, smaller studies also showed greater-than-expected progressive loss of exercise capacity in adults with congenital heart disease, but those had been smaller studies, and had not involved as diversified a range of congenital heart diseases as the new study. The 522 patients reviewed by Dr. Müller and his associates included 29% with pulmonary valve dysfunction and 26% with a left-ventricular outflow obstruction, congenital defects not previously covered in longitudinal reports on exercise capacity, said Dr. Müller, a researcher in sports science at the German Heart Center in Munich.
"We don’t know whether the rate of decline is prognostic, but we know that patients with lower exercise capacity have worse outcomes," he said in an interview. He also believes that these patients would benefit from a training-program intervention, but that has not yet been proven in a study.
Dr. Müller and his associates reviewed records from more than 5,000 cardiopulmonary exercise tests done on patients with congenital heart disease at the Heart Center between July 2001 and August 2012. The series included 522 patients who had serial, validated tests run at least 6 months apart and who did not undergo any medical or surgical intervention during the inter-test period. The average interval between the initial and subsequent test was about 2.5 years. The patients averaged about 25 years of age at baseline and about 27 years old at the time of their second test, and 59% were men.
The next most common congenital disorder following pulmonary valve dysfunction and left-ventricular outflow obstruction was need for arterial switch or congenitally corrected transposition of the great arteries, in 18%, followed by Fontan circulation in 11%, Epstein’s anomaly in 8%, and less common defects in the remaining patients.
Although the group overall lost an average of about 1% of their predicted peak oxygen uptake per year during follow-up, the rate of loss varied substantially by type of congenital defect. Patients with Epstein’s anomaly lost an average of 1.54% of predicted annually, those with a left-ventricular outflow obstruction averaged a 1.28% decline from predicted per year, and patients with pulmonary valve dysfunction averaged a 1.12% loss per year. Patients with lower than average annual loses included those with an arterial switch or transposition, with an average 0.67% loss per year, and patients with Fontan circulation, with an annual loss that averaged only 0.02%. Because exercise capacities were calculated as a percent of predicted values, they included adjustment for age, sex, weight, and height.
The analysis also showed other statistically significant functional declines in the entire group during follow-up, including an average annual fall of 0.76% in peak oxygen delivery per heartbeat, and a 1.49-beat/min decline in peak heart rate.
The rate of decline in exercise capacity was about the same regardless of patient age. And in a multivariate analysis, patients with a pacemaker were significantly more likely to have a larger average annual decline in exercise capacity, he said.
Dr. Müller said that he had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
ROME – Young adults with congenital heart disease lose roughly 1% of their predicted exercise capacity each year, based on follow-up of more than 500 patients at one German center.
The "slow but persistent decline" in patients with congenital heart disease "exceeds the decline of reference values for age" compiled in 2009 from the general German population, Jan Müller, Ph.D., said at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
Results from prior, smaller studies also showed greater-than-expected progressive loss of exercise capacity in adults with congenital heart disease, but those had been smaller studies, and had not involved as diversified a range of congenital heart diseases as the new study. The 522 patients reviewed by Dr. Müller and his associates included 29% with pulmonary valve dysfunction and 26% with a left-ventricular outflow obstruction, congenital defects not previously covered in longitudinal reports on exercise capacity, said Dr. Müller, a researcher in sports science at the German Heart Center in Munich.
"We don’t know whether the rate of decline is prognostic, but we know that patients with lower exercise capacity have worse outcomes," he said in an interview. He also believes that these patients would benefit from a training-program intervention, but that has not yet been proven in a study.
Dr. Müller and his associates reviewed records from more than 5,000 cardiopulmonary exercise tests done on patients with congenital heart disease at the Heart Center between July 2001 and August 2012. The series included 522 patients who had serial, validated tests run at least 6 months apart and who did not undergo any medical or surgical intervention during the inter-test period. The average interval between the initial and subsequent test was about 2.5 years. The patients averaged about 25 years of age at baseline and about 27 years old at the time of their second test, and 59% were men.
The next most common congenital disorder following pulmonary valve dysfunction and left-ventricular outflow obstruction was need for arterial switch or congenitally corrected transposition of the great arteries, in 18%, followed by Fontan circulation in 11%, Epstein’s anomaly in 8%, and less common defects in the remaining patients.
Although the group overall lost an average of about 1% of their predicted peak oxygen uptake per year during follow-up, the rate of loss varied substantially by type of congenital defect. Patients with Epstein’s anomaly lost an average of 1.54% of predicted annually, those with a left-ventricular outflow obstruction averaged a 1.28% decline from predicted per year, and patients with pulmonary valve dysfunction averaged a 1.12% loss per year. Patients with lower than average annual loses included those with an arterial switch or transposition, with an average 0.67% loss per year, and patients with Fontan circulation, with an annual loss that averaged only 0.02%. Because exercise capacities were calculated as a percent of predicted values, they included adjustment for age, sex, weight, and height.
The analysis also showed other statistically significant functional declines in the entire group during follow-up, including an average annual fall of 0.76% in peak oxygen delivery per heartbeat, and a 1.49-beat/min decline in peak heart rate.
The rate of decline in exercise capacity was about the same regardless of patient age. And in a multivariate analysis, patients with a pacemaker were significantly more likely to have a larger average annual decline in exercise capacity, he said.
Dr. Müller said that he had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
ROME – Young adults with congenital heart disease lose roughly 1% of their predicted exercise capacity each year, based on follow-up of more than 500 patients at one German center.
The "slow but persistent decline" in patients with congenital heart disease "exceeds the decline of reference values for age" compiled in 2009 from the general German population, Jan Müller, Ph.D., said at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
Results from prior, smaller studies also showed greater-than-expected progressive loss of exercise capacity in adults with congenital heart disease, but those had been smaller studies, and had not involved as diversified a range of congenital heart diseases as the new study. The 522 patients reviewed by Dr. Müller and his associates included 29% with pulmonary valve dysfunction and 26% with a left-ventricular outflow obstruction, congenital defects not previously covered in longitudinal reports on exercise capacity, said Dr. Müller, a researcher in sports science at the German Heart Center in Munich.
"We don’t know whether the rate of decline is prognostic, but we know that patients with lower exercise capacity have worse outcomes," he said in an interview. He also believes that these patients would benefit from a training-program intervention, but that has not yet been proven in a study.
Dr. Müller and his associates reviewed records from more than 5,000 cardiopulmonary exercise tests done on patients with congenital heart disease at the Heart Center between July 2001 and August 2012. The series included 522 patients who had serial, validated tests run at least 6 months apart and who did not undergo any medical or surgical intervention during the inter-test period. The average interval between the initial and subsequent test was about 2.5 years. The patients averaged about 25 years of age at baseline and about 27 years old at the time of their second test, and 59% were men.
The next most common congenital disorder following pulmonary valve dysfunction and left-ventricular outflow obstruction was need for arterial switch or congenitally corrected transposition of the great arteries, in 18%, followed by Fontan circulation in 11%, Epstein’s anomaly in 8%, and less common defects in the remaining patients.
Although the group overall lost an average of about 1% of their predicted peak oxygen uptake per year during follow-up, the rate of loss varied substantially by type of congenital defect. Patients with Epstein’s anomaly lost an average of 1.54% of predicted annually, those with a left-ventricular outflow obstruction averaged a 1.28% decline from predicted per year, and patients with pulmonary valve dysfunction averaged a 1.12% loss per year. Patients with lower than average annual loses included those with an arterial switch or transposition, with an average 0.67% loss per year, and patients with Fontan circulation, with an annual loss that averaged only 0.02%. Because exercise capacities were calculated as a percent of predicted values, they included adjustment for age, sex, weight, and height.
The analysis also showed other statistically significant functional declines in the entire group during follow-up, including an average annual fall of 0.76% in peak oxygen delivery per heartbeat, and a 1.49-beat/min decline in peak heart rate.
The rate of decline in exercise capacity was about the same regardless of patient age. And in a multivariate analysis, patients with a pacemaker were significantly more likely to have a larger average annual decline in exercise capacity, he said.
Dr. Müller said that he had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
AT EUROPREVENT 2013
Major finding: Exercise capacity fell by an average of 1% per year among young adults with congenital heart disease.
Data source: A review of 522 young adults with congenital heart disease who underwent serial exercise-capacity testing at one German center.
Disclosures: Dr. Müller said that he had no disclosures.
Treadmill 1-km walk test predicts prognosis in cardiac disease
ROME – A moderate walk on a treadmill for 1 km proved useful for calculating a patient’s peak oxygen uptake and cardiopulmonary exercise capacity, and provided significant prognostic information for patients with cardiac disease, in a study with more than 1,200 Italian men.
The treadmill walk test "is a low-cost and simple tool for the indirect evaluation of cardiorespiratory fitness in cardiac outpatients," Dr. Giorgio Chiaranda said in a poster at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation.
Cardiac patients in the highest quartile for cardiorespiratory fitness measured by the walk test had a two-thirds reduction in their mortality, compared with patients in the lowest fitness quartile during a median follow-up of 8 years.
The researchers had previously reported the development of a new submaximal protocol to predict peak oxygen uptake using a moderate, perceptually regulated 1-km treadmill walk test (J. Cardiopulm. Rehabil. Prev. 2012;32:262-9). They developed the walk test as an alternative to the standard maximal cardiopulmonary exercise test, which is relatively expensive and can be impractical in some settings. The investigators initially developed the walk test in 178 men with cardiac disease; the new study was performed to validate the walk test using prospectively collected follow-up data.
After a cardiac event, 1,255 outpatient men were referred to a cardiac rehabilitation program. They averaged 61 years of age, with a range from 25 to 85 years. Their average body mass index was 27.6 kg/m2, and their average left ventricular ejection fraction was 56%(range, 21%-80%. Their index cardiac disease event was coronary artery bypass surgery in 49%, myocardial infarction in 28%, percutaneous coronary intervention in 9%, valve replacement in 9%, and other procedures in 5%.
All patients underwent a 1-km treadmill walk test, during which they were reminded to maintain a moderate pace. Testing produced no complications. Patients in the lowest quartile for their predicted peak oxygen uptake had a level of 19.6 mL/kg per minute or less. Patients in the highest quartile had a rate of at least 25.1 mL/kg per minute.
During a median follow-up of 8 years, 141 (11%) of the patients died. A multivariate analysis adjusted for several demographic and clinical factors including age, body mass index, ejection fraction, smoking status, hypertension, family history, cholesterol levels, glucose level, and renal function. Patients in the fittest quartile had a follow-up mortality rate that was 67% lower than that of patients in the least-fit quartile. Patients in the next most-fit quartile had a mortality rate that was 50% lower than that of the least-fit group. Both between-group differences were statistically significant, Dr. Chiaranda of the University of Ferrara (Italy) Center for Sports Medicine and his associates found. Cardiorespiratory fitness could account for 71% of the variability in mortality during follow-up.
The researchers found the lowest mortality rate among patients from the fittest quartile who further improved their peak oxygen uptake during follow-up, based on a second 1-km walk test performed 1 year following their baseline test in 964 patients. Patients with increased fitness on follow-up had an 89% reduced mortality rate compared with patients from the least-fit quartile who did not show improvement in their fitness after the first follow-up year.
Dr. Chiaranda and his associates said they had no relevant financial disclosures.
On Twitter @mitchelzoler
ROME – A moderate walk on a treadmill for 1 km proved useful for calculating a patient’s peak oxygen uptake and cardiopulmonary exercise capacity, and provided significant prognostic information for patients with cardiac disease, in a study with more than 1,200 Italian men.
The treadmill walk test "is a low-cost and simple tool for the indirect evaluation of cardiorespiratory fitness in cardiac outpatients," Dr. Giorgio Chiaranda said in a poster at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation.
Cardiac patients in the highest quartile for cardiorespiratory fitness measured by the walk test had a two-thirds reduction in their mortality, compared with patients in the lowest fitness quartile during a median follow-up of 8 years.
The researchers had previously reported the development of a new submaximal protocol to predict peak oxygen uptake using a moderate, perceptually regulated 1-km treadmill walk test (J. Cardiopulm. Rehabil. Prev. 2012;32:262-9). They developed the walk test as an alternative to the standard maximal cardiopulmonary exercise test, which is relatively expensive and can be impractical in some settings. The investigators initially developed the walk test in 178 men with cardiac disease; the new study was performed to validate the walk test using prospectively collected follow-up data.
After a cardiac event, 1,255 outpatient men were referred to a cardiac rehabilitation program. They averaged 61 years of age, with a range from 25 to 85 years. Their average body mass index was 27.6 kg/m2, and their average left ventricular ejection fraction was 56%(range, 21%-80%. Their index cardiac disease event was coronary artery bypass surgery in 49%, myocardial infarction in 28%, percutaneous coronary intervention in 9%, valve replacement in 9%, and other procedures in 5%.
All patients underwent a 1-km treadmill walk test, during which they were reminded to maintain a moderate pace. Testing produced no complications. Patients in the lowest quartile for their predicted peak oxygen uptake had a level of 19.6 mL/kg per minute or less. Patients in the highest quartile had a rate of at least 25.1 mL/kg per minute.
During a median follow-up of 8 years, 141 (11%) of the patients died. A multivariate analysis adjusted for several demographic and clinical factors including age, body mass index, ejection fraction, smoking status, hypertension, family history, cholesterol levels, glucose level, and renal function. Patients in the fittest quartile had a follow-up mortality rate that was 67% lower than that of patients in the least-fit quartile. Patients in the next most-fit quartile had a mortality rate that was 50% lower than that of the least-fit group. Both between-group differences were statistically significant, Dr. Chiaranda of the University of Ferrara (Italy) Center for Sports Medicine and his associates found. Cardiorespiratory fitness could account for 71% of the variability in mortality during follow-up.
The researchers found the lowest mortality rate among patients from the fittest quartile who further improved their peak oxygen uptake during follow-up, based on a second 1-km walk test performed 1 year following their baseline test in 964 patients. Patients with increased fitness on follow-up had an 89% reduced mortality rate compared with patients from the least-fit quartile who did not show improvement in their fitness after the first follow-up year.
Dr. Chiaranda and his associates said they had no relevant financial disclosures.
On Twitter @mitchelzoler
ROME – A moderate walk on a treadmill for 1 km proved useful for calculating a patient’s peak oxygen uptake and cardiopulmonary exercise capacity, and provided significant prognostic information for patients with cardiac disease, in a study with more than 1,200 Italian men.
The treadmill walk test "is a low-cost and simple tool for the indirect evaluation of cardiorespiratory fitness in cardiac outpatients," Dr. Giorgio Chiaranda said in a poster at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation.
Cardiac patients in the highest quartile for cardiorespiratory fitness measured by the walk test had a two-thirds reduction in their mortality, compared with patients in the lowest fitness quartile during a median follow-up of 8 years.
The researchers had previously reported the development of a new submaximal protocol to predict peak oxygen uptake using a moderate, perceptually regulated 1-km treadmill walk test (J. Cardiopulm. Rehabil. Prev. 2012;32:262-9). They developed the walk test as an alternative to the standard maximal cardiopulmonary exercise test, which is relatively expensive and can be impractical in some settings. The investigators initially developed the walk test in 178 men with cardiac disease; the new study was performed to validate the walk test using prospectively collected follow-up data.
After a cardiac event, 1,255 outpatient men were referred to a cardiac rehabilitation program. They averaged 61 years of age, with a range from 25 to 85 years. Their average body mass index was 27.6 kg/m2, and their average left ventricular ejection fraction was 56%(range, 21%-80%. Their index cardiac disease event was coronary artery bypass surgery in 49%, myocardial infarction in 28%, percutaneous coronary intervention in 9%, valve replacement in 9%, and other procedures in 5%.
All patients underwent a 1-km treadmill walk test, during which they were reminded to maintain a moderate pace. Testing produced no complications. Patients in the lowest quartile for their predicted peak oxygen uptake had a level of 19.6 mL/kg per minute or less. Patients in the highest quartile had a rate of at least 25.1 mL/kg per minute.
During a median follow-up of 8 years, 141 (11%) of the patients died. A multivariate analysis adjusted for several demographic and clinical factors including age, body mass index, ejection fraction, smoking status, hypertension, family history, cholesterol levels, glucose level, and renal function. Patients in the fittest quartile had a follow-up mortality rate that was 67% lower than that of patients in the least-fit quartile. Patients in the next most-fit quartile had a mortality rate that was 50% lower than that of the least-fit group. Both between-group differences were statistically significant, Dr. Chiaranda of the University of Ferrara (Italy) Center for Sports Medicine and his associates found. Cardiorespiratory fitness could account for 71% of the variability in mortality during follow-up.
The researchers found the lowest mortality rate among patients from the fittest quartile who further improved their peak oxygen uptake during follow-up, based on a second 1-km walk test performed 1 year following their baseline test in 964 patients. Patients with increased fitness on follow-up had an 89% reduced mortality rate compared with patients from the least-fit quartile who did not show improvement in their fitness after the first follow-up year.
Dr. Chiaranda and his associates said they had no relevant financial disclosures.
On Twitter @mitchelzoler
AT EUROPREVENT 2013
Major finding: During a median follow-up of 8 years, 11% of the patients died. Patients in the fittest quartile had a follow-up mortality rate that was 67% lower than that of patients in the least-fit quartile.
Data source: A prospective follow-up study of 1,255 men with cardiac disease who underwent a 1-km treadmill walk test at baseline at a single Italian center.
Disclosures: Dr. Chiaranda and his associates said they had no relevant financial disclosures.
Type 2 diabetics often harbor undiagnosed heart failure
ROME – Unrecognized heart failure is common among older patients with type 2 diabetes, on the basis of a study of 581 Dutch diabetes patients.
A comprehensive screening examination and assessment of Dutch patients with type 2 diabetes who were at least 60 years old and had no prior history of heart failure identified 161 patients (28%) with heart failure, Dr. Leandra J.M. Boonman-de Winter and her associates reported in a poster at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
The newly identified heart failure patients included 28 (5% of the total group screened) with reduced left ventricular function and 133 (23%) with preserved left ventricular function, said Dr. Boonman-de Winter, a researcher at University Medical Center in Utrecht, the Netherlands, and her associates.
To identify these heart failure cases, the researchers performed an extensive work-up on each patient with type 2 diabetes, including a medical history, physical examination, ECG, and echocardiography. A panel of expert cardiologists made the diagnosis of heart failure using criteria of the European Society for Cardiology (Eur. Heart J. 2012;33:1787-847).
The researchers also performed a multivariate analysis to identify demographic and clinical factors that significantly linked with the presence of heart failure in the patients with diabetes. Dyspnea or fatigue linked with a sixfold increased prevalence of heart failure; ankle edema or nocturia, a history of ischemic heart disease, and age greater than 75 years old each linked with a doubled heart-failure prevalence; and hypertension linked with a 70% increased prevalence of heart failure.
These five factors together could account for 80% of the heart failure cases found among the patients with type 2 diabetes, the researchers reported. They recommended using these five factors to identify older patients with diabetes to more thoroughly screen for heart failure.
Dr. Boonman-de Winter and her associates said that they had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
ROME – Unrecognized heart failure is common among older patients with type 2 diabetes, on the basis of a study of 581 Dutch diabetes patients.
A comprehensive screening examination and assessment of Dutch patients with type 2 diabetes who were at least 60 years old and had no prior history of heart failure identified 161 patients (28%) with heart failure, Dr. Leandra J.M. Boonman-de Winter and her associates reported in a poster at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
The newly identified heart failure patients included 28 (5% of the total group screened) with reduced left ventricular function and 133 (23%) with preserved left ventricular function, said Dr. Boonman-de Winter, a researcher at University Medical Center in Utrecht, the Netherlands, and her associates.
To identify these heart failure cases, the researchers performed an extensive work-up on each patient with type 2 diabetes, including a medical history, physical examination, ECG, and echocardiography. A panel of expert cardiologists made the diagnosis of heart failure using criteria of the European Society for Cardiology (Eur. Heart J. 2012;33:1787-847).
The researchers also performed a multivariate analysis to identify demographic and clinical factors that significantly linked with the presence of heart failure in the patients with diabetes. Dyspnea or fatigue linked with a sixfold increased prevalence of heart failure; ankle edema or nocturia, a history of ischemic heart disease, and age greater than 75 years old each linked with a doubled heart-failure prevalence; and hypertension linked with a 70% increased prevalence of heart failure.
These five factors together could account for 80% of the heart failure cases found among the patients with type 2 diabetes, the researchers reported. They recommended using these five factors to identify older patients with diabetes to more thoroughly screen for heart failure.
Dr. Boonman-de Winter and her associates said that they had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
ROME – Unrecognized heart failure is common among older patients with type 2 diabetes, on the basis of a study of 581 Dutch diabetes patients.
A comprehensive screening examination and assessment of Dutch patients with type 2 diabetes who were at least 60 years old and had no prior history of heart failure identified 161 patients (28%) with heart failure, Dr. Leandra J.M. Boonman-de Winter and her associates reported in a poster at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
The newly identified heart failure patients included 28 (5% of the total group screened) with reduced left ventricular function and 133 (23%) with preserved left ventricular function, said Dr. Boonman-de Winter, a researcher at University Medical Center in Utrecht, the Netherlands, and her associates.
To identify these heart failure cases, the researchers performed an extensive work-up on each patient with type 2 diabetes, including a medical history, physical examination, ECG, and echocardiography. A panel of expert cardiologists made the diagnosis of heart failure using criteria of the European Society for Cardiology (Eur. Heart J. 2012;33:1787-847).
The researchers also performed a multivariate analysis to identify demographic and clinical factors that significantly linked with the presence of heart failure in the patients with diabetes. Dyspnea or fatigue linked with a sixfold increased prevalence of heart failure; ankle edema or nocturia, a history of ischemic heart disease, and age greater than 75 years old each linked with a doubled heart-failure prevalence; and hypertension linked with a 70% increased prevalence of heart failure.
These five factors together could account for 80% of the heart failure cases found among the patients with type 2 diabetes, the researchers reported. They recommended using these five factors to identify older patients with diabetes to more thoroughly screen for heart failure.
Dr. Boonman-de Winter and her associates said that they had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
AT EUROPREVENT 2013
Major finding: Undiagnosed heart failure was found in 28% of type 2 diabetes patients aged 60 years and older.
Data source: A single-center screening study of 581 Dutch patients with type 2 diabetes who were at least 60 years old.
Disclosures: Dr. Boonman-de Winter and her associates said that they had no disclosures.
Dietary antioxidants linked to reduced postoperative atrial fib
ROME – Patients undergoing cardiac surgery who ate a diet rich in antioxidants developed significantly fewer episodes of atrial fibrillation, compared with patients who consumed fewer antioxidants, in a review of 217 patients from one Italian center.
Patients in the top tertile for antioxidant consumption in their diet had roughly half the rate of new-onset atrial fibrillation following open cardiac surgery compared with the remaining patients in a multivariate adjusted analysis, Dr. Licia Iacoviello reported in a poster at the annual the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
The next step will be a prospective trial with about 700 patients to test the efficacy of an antioxidant supplement to cut the development of postoperative atrial fibrillation in patients undergoing cardiac surgery, said Dr. Iacoviello, head of the laboratory of genetic and environmental epidemiology at Catholic University, Campobasso, Italy.

She said that she is planning such a trial with her colleagues, but she acknowledged that an antioxidant supplement may not deliver the same materials as a diet rich in antioxidant-containing nutrients. However, intervention based on a controlled diet is difficult to standardize and run, she said in an interview.
Her report involved 217 consecutive patients who underwent coronary artery bypass grafting (CABG), cardiac valve repair or replacement surgery, or a combination of both procedures during January 2010–June 2012. The patients agreed to participate in the study and supplied full information on their diet during the year before surgery. Dr. Iacoviello and her associates analyzed the dietary questionnaire results with several tools that assess antioxidant content, including the trolox equivalent antioxidant capacity (TEAC) (J. Nutr. 2007;137:93-8). The most commonly consumed antioxidant-containing item in their diet was wine, which supplied 46% of antioxidant content, followed by coffee, which kicked in another 30%, and then fruit and fruit juices, which supplied 8% of everyone’s antioxidant consumption. The average age of the patients was 68 years; 110 (51%) underwent isolated CABG, 54 (25%) underwent isolated valve surgery, and the remaining patients had a combined procedure.
During follow-up, 84 patients (39%) developed atrial fibrillation that produced either clinically identifiable symptoms or persisted for more than 5 minutes on an ECG recording. Incident atrial fibrillation occurred in 20 (27%) of 73 patients in the highest tertile for antioxidant consumption based on their TEAC, and in 64 (44%) of the other 144 patients.
In a multivariable analysis that controlled for age, sex, diabetes treatment, a prior diagnosis of atrial fibrillation, and total energy intake, patients in the highest TEAC tertile had a statistically significant, 51% lower risk for developing atrial fibrillation, compared with patients with lower TEAC levels, Dr. Iacoviello reported.
A second analysis that focused only on the 110 patients who underwent isolated CABG showed a similar relationship. In this subgroup, the 39 patients with higher TEAC scores had a 73% reduced risk for new-onset atrial fibrillation following CABG, compared with the remaining 71 with TEAC levels in the two lowest tertiles for the overall group, a statistically significant difference.
These findings provide the first clinical evidence that high dietary levels of antioxidants may play a role in suppressing development of atrial fibrillation following cardiac surgery, said Dr. Giovanni de Gaetano, a coinvestigator on the study and director of research laboratories at Catholic University in Campobasso.
Dr. Iacoviello and Dr. de Gaetano said that they had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
ROME – Patients undergoing cardiac surgery who ate a diet rich in antioxidants developed significantly fewer episodes of atrial fibrillation, compared with patients who consumed fewer antioxidants, in a review of 217 patients from one Italian center.
Patients in the top tertile for antioxidant consumption in their diet had roughly half the rate of new-onset atrial fibrillation following open cardiac surgery compared with the remaining patients in a multivariate adjusted analysis, Dr. Licia Iacoviello reported in a poster at the annual the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
The next step will be a prospective trial with about 700 patients to test the efficacy of an antioxidant supplement to cut the development of postoperative atrial fibrillation in patients undergoing cardiac surgery, said Dr. Iacoviello, head of the laboratory of genetic and environmental epidemiology at Catholic University, Campobasso, Italy.
She said that she is planning such a trial with her colleagues, but she acknowledged that an antioxidant supplement may not deliver the same materials as a diet rich in antioxidant-containing nutrients. However, intervention based on a controlled diet is difficult to standardize and run, she said in an interview.
Her report involved 217 consecutive patients who underwent coronary artery bypass grafting (CABG), cardiac valve repair or replacement surgery, or a combination of both procedures during January 2010–June 2012. The patients agreed to participate in the study and supplied full information on their diet during the year before surgery. Dr. Iacoviello and her associates analyzed the dietary questionnaire results with several tools that assess antioxidant content, including the trolox equivalent antioxidant capacity (TEAC) (J. Nutr. 2007;137:93-8). The most commonly consumed antioxidant-containing item in their diet was wine, which supplied 46% of antioxidant content, followed by coffee, which kicked in another 30%, and then fruit and fruit juices, which supplied 8% of everyone’s antioxidant consumption. The average age of the patients was 68 years; 110 (51%) underwent isolated CABG, 54 (25%) underwent isolated valve surgery, and the remaining patients had a combined procedure.
During follow-up, 84 patients (39%) developed atrial fibrillation that produced either clinically identifiable symptoms or persisted for more than 5 minutes on an ECG recording. Incident atrial fibrillation occurred in 20 (27%) of 73 patients in the highest tertile for antioxidant consumption based on their TEAC, and in 64 (44%) of the other 144 patients.
In a multivariable analysis that controlled for age, sex, diabetes treatment, a prior diagnosis of atrial fibrillation, and total energy intake, patients in the highest TEAC tertile had a statistically significant, 51% lower risk for developing atrial fibrillation, compared with patients with lower TEAC levels, Dr. Iacoviello reported.
A second analysis that focused only on the 110 patients who underwent isolated CABG showed a similar relationship. In this subgroup, the 39 patients with higher TEAC scores had a 73% reduced risk for new-onset atrial fibrillation following CABG, compared with the remaining 71 with TEAC levels in the two lowest tertiles for the overall group, a statistically significant difference.
These findings provide the first clinical evidence that high dietary levels of antioxidants may play a role in suppressing development of atrial fibrillation following cardiac surgery, said Dr. Giovanni de Gaetano, a coinvestigator on the study and director of research laboratories at Catholic University in Campobasso.
Dr. Iacoviello and Dr. de Gaetano said that they had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
ROME – Patients undergoing cardiac surgery who ate a diet rich in antioxidants developed significantly fewer episodes of atrial fibrillation, compared with patients who consumed fewer antioxidants, in a review of 217 patients from one Italian center.
Patients in the top tertile for antioxidant consumption in their diet had roughly half the rate of new-onset atrial fibrillation following open cardiac surgery compared with the remaining patients in a multivariate adjusted analysis, Dr. Licia Iacoviello reported in a poster at the annual the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
The next step will be a prospective trial with about 700 patients to test the efficacy of an antioxidant supplement to cut the development of postoperative atrial fibrillation in patients undergoing cardiac surgery, said Dr. Iacoviello, head of the laboratory of genetic and environmental epidemiology at Catholic University, Campobasso, Italy.
She said that she is planning such a trial with her colleagues, but she acknowledged that an antioxidant supplement may not deliver the same materials as a diet rich in antioxidant-containing nutrients. However, intervention based on a controlled diet is difficult to standardize and run, she said in an interview.
Her report involved 217 consecutive patients who underwent coronary artery bypass grafting (CABG), cardiac valve repair or replacement surgery, or a combination of both procedures during January 2010–June 2012. The patients agreed to participate in the study and supplied full information on their diet during the year before surgery. Dr. Iacoviello and her associates analyzed the dietary questionnaire results with several tools that assess antioxidant content, including the trolox equivalent antioxidant capacity (TEAC) (J. Nutr. 2007;137:93-8). The most commonly consumed antioxidant-containing item in their diet was wine, which supplied 46% of antioxidant content, followed by coffee, which kicked in another 30%, and then fruit and fruit juices, which supplied 8% of everyone’s antioxidant consumption. The average age of the patients was 68 years; 110 (51%) underwent isolated CABG, 54 (25%) underwent isolated valve surgery, and the remaining patients had a combined procedure.
During follow-up, 84 patients (39%) developed atrial fibrillation that produced either clinically identifiable symptoms or persisted for more than 5 minutes on an ECG recording. Incident atrial fibrillation occurred in 20 (27%) of 73 patients in the highest tertile for antioxidant consumption based on their TEAC, and in 64 (44%) of the other 144 patients.
In a multivariable analysis that controlled for age, sex, diabetes treatment, a prior diagnosis of atrial fibrillation, and total energy intake, patients in the highest TEAC tertile had a statistically significant, 51% lower risk for developing atrial fibrillation, compared with patients with lower TEAC levels, Dr. Iacoviello reported.
A second analysis that focused only on the 110 patients who underwent isolated CABG showed a similar relationship. In this subgroup, the 39 patients with higher TEAC scores had a 73% reduced risk for new-onset atrial fibrillation following CABG, compared with the remaining 71 with TEAC levels in the two lowest tertiles for the overall group, a statistically significant difference.
These findings provide the first clinical evidence that high dietary levels of antioxidants may play a role in suppressing development of atrial fibrillation following cardiac surgery, said Dr. Giovanni de Gaetano, a coinvestigator on the study and director of research laboratories at Catholic University in Campobasso.
Dr. Iacoviello and Dr. de Gaetano said that they had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
AT EUROPREVENT 2013
Major finding: Patients in the top tertile for dietary antioxidant consumption developed 51% fewer postoperative atrial fibrillation cases, compared with other patients.
Data source: A review of 217 consecutive patients who underwent cardiac surgery at one Italian center.
Disclosures: Dr. Iacoviello and Dr. de Gaetano said that they had no disclosures.

Telemonitored cardiac rehabilitation boosts compliance
ROME – A home-based cardiac rehabilitation program that relies on telemonitoring safely allowed effective training of about 800 elderly cardiac patients at one center in Poland since 2006.
"The advantages of telerehabilitation are the convenience and easy access for elderly patients," Dr. Ewa Piotrowicz said at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*. Telerehabilitation "fosters greater patient independence than hospital-based exercise training, and may reduce patient commute time and costs. Telemedicine may overcome some of the barriers related to aging.
"In our opinion, home-based cardiac rehabilitation is the best option" for older patients, said Dr. Piotrowicz, a cardiologist and head of the telecardiology center of the Institute of Cardiology in Warsaw.

A key to safe and successful home-based rehabilitation training for elderly cardiac patients is a thorough baseline examination to assess cardiac stability. "We don’t do telerehabilitation on unstable patients," she said in an interview. The other major feature is thorough monitoring by a telephone conversation and telephone transmission of vital recordings immediately before and after each at-home rehabilitation session. "Before and after every session the patient sends an ECG recording and answers a series of questions," she explained.
During the 7 years that the institute has run the program, it has enrolled about 500 lower-risk and 300 higher-risk patients, with about 50 in the program at any given time. At entry, each patient undergoes assessment by ECG, an echocardiography examination, 24-hour Holter blood pressure monitoring, and a cardiopulmonary exercise test.
The rehabilitation program involves an individualized exercise training program, and launches with a few sessions at the hospital along with educational sessions. The patient then continues the basic phase of the program with five daily sessions per week for 8 weeks. The program includes walking, running, interval training, and breathing training. Before and immediately after each daily session the patient speaks with a physician at the center, answering questions and sending information on ECG, heart rate, blood pressure, weight, oxygen saturation, respiration rate, and medications taken. Patients must receive approval from a physician before each exercise session starts.
The program achieved a high compliance level. Dr. Piotrowicz said that 95% of the 800 participants completed their 8-week programs. Following that, patients are encouraged to continue exercising on their own.
In 2010, she and her associates reported results from a formal, controlled assessment of compliance among 152 patients with heart failure who were randomized to either a home-based, telemonitored rehabilitation program or a more conventional outpatient program. The home-based telemonitored program produced similar clinical and quality of life improvements compared with the program for the control patients, and the 77 patients randomized to telemonitoring had 100% compliance with the 8-week rehabilitation program, compared with a 20% attrition rate among the patients enrolled in a standard outpatient rehabilitation program (Eur. J. Heart Fail. 2010;12:164-71). Dr. Piotrowicz attributed the high compliance to the daily contact that patients maintain with their health care providers.
"Telerehabilitation is a chance for implementing cardiac rehabilitation, especially in chronic heart failure patients," she said. The next step is a multicenter study of this approach, she added.
Dr. Piotrowicz said that she had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation.
ROME – A home-based cardiac rehabilitation program that relies on telemonitoring safely allowed effective training of about 800 elderly cardiac patients at one center in Poland since 2006.
"The advantages of telerehabilitation are the convenience and easy access for elderly patients," Dr. Ewa Piotrowicz said at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*. Telerehabilitation "fosters greater patient independence than hospital-based exercise training, and may reduce patient commute time and costs. Telemedicine may overcome some of the barriers related to aging.
"In our opinion, home-based cardiac rehabilitation is the best option" for older patients, said Dr. Piotrowicz, a cardiologist and head of the telecardiology center of the Institute of Cardiology in Warsaw.
A key to safe and successful home-based rehabilitation training for elderly cardiac patients is a thorough baseline examination to assess cardiac stability. "We don’t do telerehabilitation on unstable patients," she said in an interview. The other major feature is thorough monitoring by a telephone conversation and telephone transmission of vital recordings immediately before and after each at-home rehabilitation session. "Before and after every session the patient sends an ECG recording and answers a series of questions," she explained.
During the 7 years that the institute has run the program, it has enrolled about 500 lower-risk and 300 higher-risk patients, with about 50 in the program at any given time. At entry, each patient undergoes assessment by ECG, an echocardiography examination, 24-hour Holter blood pressure monitoring, and a cardiopulmonary exercise test.
The rehabilitation program involves an individualized exercise training program, and launches with a few sessions at the hospital along with educational sessions. The patient then continues the basic phase of the program with five daily sessions per week for 8 weeks. The program includes walking, running, interval training, and breathing training. Before and immediately after each daily session the patient speaks with a physician at the center, answering questions and sending information on ECG, heart rate, blood pressure, weight, oxygen saturation, respiration rate, and medications taken. Patients must receive approval from a physician before each exercise session starts.
The program achieved a high compliance level. Dr. Piotrowicz said that 95% of the 800 participants completed their 8-week programs. Following that, patients are encouraged to continue exercising on their own.
In 2010, she and her associates reported results from a formal, controlled assessment of compliance among 152 patients with heart failure who were randomized to either a home-based, telemonitored rehabilitation program or a more conventional outpatient program. The home-based telemonitored program produced similar clinical and quality of life improvements compared with the program for the control patients, and the 77 patients randomized to telemonitoring had 100% compliance with the 8-week rehabilitation program, compared with a 20% attrition rate among the patients enrolled in a standard outpatient rehabilitation program (Eur. J. Heart Fail. 2010;12:164-71). Dr. Piotrowicz attributed the high compliance to the daily contact that patients maintain with their health care providers.
"Telerehabilitation is a chance for implementing cardiac rehabilitation, especially in chronic heart failure patients," she said. The next step is a multicenter study of this approach, she added.
Dr. Piotrowicz said that she had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation.
ROME – A home-based cardiac rehabilitation program that relies on telemonitoring safely allowed effective training of about 800 elderly cardiac patients at one center in Poland since 2006.
"The advantages of telerehabilitation are the convenience and easy access for elderly patients," Dr. Ewa Piotrowicz said at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*. Telerehabilitation "fosters greater patient independence than hospital-based exercise training, and may reduce patient commute time and costs. Telemedicine may overcome some of the barriers related to aging.
"In our opinion, home-based cardiac rehabilitation is the best option" for older patients, said Dr. Piotrowicz, a cardiologist and head of the telecardiology center of the Institute of Cardiology in Warsaw.
A key to safe and successful home-based rehabilitation training for elderly cardiac patients is a thorough baseline examination to assess cardiac stability. "We don’t do telerehabilitation on unstable patients," she said in an interview. The other major feature is thorough monitoring by a telephone conversation and telephone transmission of vital recordings immediately before and after each at-home rehabilitation session. "Before and after every session the patient sends an ECG recording and answers a series of questions," she explained.
During the 7 years that the institute has run the program, it has enrolled about 500 lower-risk and 300 higher-risk patients, with about 50 in the program at any given time. At entry, each patient undergoes assessment by ECG, an echocardiography examination, 24-hour Holter blood pressure monitoring, and a cardiopulmonary exercise test.
The rehabilitation program involves an individualized exercise training program, and launches with a few sessions at the hospital along with educational sessions. The patient then continues the basic phase of the program with five daily sessions per week for 8 weeks. The program includes walking, running, interval training, and breathing training. Before and immediately after each daily session the patient speaks with a physician at the center, answering questions and sending information on ECG, heart rate, blood pressure, weight, oxygen saturation, respiration rate, and medications taken. Patients must receive approval from a physician before each exercise session starts.
The program achieved a high compliance level. Dr. Piotrowicz said that 95% of the 800 participants completed their 8-week programs. Following that, patients are encouraged to continue exercising on their own.
In 2010, she and her associates reported results from a formal, controlled assessment of compliance among 152 patients with heart failure who were randomized to either a home-based, telemonitored rehabilitation program or a more conventional outpatient program. The home-based telemonitored program produced similar clinical and quality of life improvements compared with the program for the control patients, and the 77 patients randomized to telemonitoring had 100% compliance with the 8-week rehabilitation program, compared with a 20% attrition rate among the patients enrolled in a standard outpatient rehabilitation program (Eur. J. Heart Fail. 2010;12:164-71). Dr. Piotrowicz attributed the high compliance to the daily contact that patients maintain with their health care providers.
"Telerehabilitation is a chance for implementing cardiac rehabilitation, especially in chronic heart failure patients," she said. The next step is a multicenter study of this approach, she added.
Dr. Piotrowicz said that she had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation.
AT EUROPREVENT 2013
Major finding: Telemedicine achieved 95% compliance with at-home cardiac rehabilitation among elderly cardiac patients.
Data source: A review of about 800 patients treated by home-based telerehabilitation at one center in Poland during 7 years.
Disclosures: Dr. Piotrowicz said that she had no disclosures.

Acute MI patients benefit from early rehabilitation
ROME – Starting cardiac rehabilitation sessions within 2 weeks of an acute myocardial infarction is safe and can improve cardiac perfusion and function, according to results of a randomized, controlled study of 46 patients who had residual myocardial ischemia following an MI and percutaneous coronary revascularization.
"Exercise-induced changes in myocardial perfusion and function were associated with an absence of unfavorable left-ventricular remodeling and an improved cardiovascular functional capacity," Dr. Francesco Giallauria said at the European Association for Cardiovascular Prevention and Rehabilitation* annual meeting. He hypothesized that exercise training begun soon after an MI improves myocardial perfusion by inducing coronary vascular adaptation or enhancing development of collateral cardiac vessels.

The study began with patients who underwent percutaneous coronary intervention (PCI) following an acute ST-elevation MI who were then assessed by dipyridamole stress and gated single-photon emission CT (SPECT) using labeled sestamibi. All 46 included patients had a significant amount of residual myocardial ischemia despite PCI, presumably caused by inadequate perfusion in myocardial regions not vascularized by the PCI-treated coronaries, said Dr. Giallauria, a cardiologist at the University of Naples (Italy). All patients also underwent a cardiopulmonary exercise test at baseline to determine their peak exercise capacity.
The researchers then randomized the patients. Twenty-five entered a hospital outpatient program of supervised, 30-minutes sessions of bicycle exercise three times a week, with an exercise target during each session of 60%-70% of their peak exercise capacity. The program began within 2 weeks of their acute MI. The remaining 21 patients served as controls and received just instructions about maintaining physical exercise and lifestyle modification.
The exercise rehabilitation program continued for 6 months, when all 46 patients underwent a follow-up examination of their myocardial perfusion with gated SPECT and follow-up cardiopulmonary stress testing. The average age of the patients was 54 years, and 87% were men.
The results showed that after 6 months, patients who underwent exercise training had an average 29% increase in peak exercise capacity and a 10% average rise in their peak heart rate compared with baseline, both statistically significant differences. Results from the serial SPECT studies showed that left ventricular ejection fraction rose from an average of 48% at baseline to 52% in the patients who underwent exercise training, a statistically significant rise, and their wall motion and wall thickness scores showed improvements in cardiac shape and function compared with baseline, all differences that were statistically significant. In contrast, the control patients had no significant changes for any of these exercise or cardiac measures during the 6 months of follow-up.
In addition, the SPECT imaging showed that at follow-up the extent of myocardial perfusion defect and ischemia fell by about 50% in the exercise group while remaining virtually unchanged in the control patients.
Dr. Giallauria said that he had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation annual conference.
ROME – Starting cardiac rehabilitation sessions within 2 weeks of an acute myocardial infarction is safe and can improve cardiac perfusion and function, according to results of a randomized, controlled study of 46 patients who had residual myocardial ischemia following an MI and percutaneous coronary revascularization.
"Exercise-induced changes in myocardial perfusion and function were associated with an absence of unfavorable left-ventricular remodeling and an improved cardiovascular functional capacity," Dr. Francesco Giallauria said at the European Association for Cardiovascular Prevention and Rehabilitation* annual meeting. He hypothesized that exercise training begun soon after an MI improves myocardial perfusion by inducing coronary vascular adaptation or enhancing development of collateral cardiac vessels.
The study began with patients who underwent percutaneous coronary intervention (PCI) following an acute ST-elevation MI who were then assessed by dipyridamole stress and gated single-photon emission CT (SPECT) using labeled sestamibi. All 46 included patients had a significant amount of residual myocardial ischemia despite PCI, presumably caused by inadequate perfusion in myocardial regions not vascularized by the PCI-treated coronaries, said Dr. Giallauria, a cardiologist at the University of Naples (Italy). All patients also underwent a cardiopulmonary exercise test at baseline to determine their peak exercise capacity.
The researchers then randomized the patients. Twenty-five entered a hospital outpatient program of supervised, 30-minutes sessions of bicycle exercise three times a week, with an exercise target during each session of 60%-70% of their peak exercise capacity. The program began within 2 weeks of their acute MI. The remaining 21 patients served as controls and received just instructions about maintaining physical exercise and lifestyle modification.
The exercise rehabilitation program continued for 6 months, when all 46 patients underwent a follow-up examination of their myocardial perfusion with gated SPECT and follow-up cardiopulmonary stress testing. The average age of the patients was 54 years, and 87% were men.
The results showed that after 6 months, patients who underwent exercise training had an average 29% increase in peak exercise capacity and a 10% average rise in their peak heart rate compared with baseline, both statistically significant differences. Results from the serial SPECT studies showed that left ventricular ejection fraction rose from an average of 48% at baseline to 52% in the patients who underwent exercise training, a statistically significant rise, and their wall motion and wall thickness scores showed improvements in cardiac shape and function compared with baseline, all differences that were statistically significant. In contrast, the control patients had no significant changes for any of these exercise or cardiac measures during the 6 months of follow-up.
In addition, the SPECT imaging showed that at follow-up the extent of myocardial perfusion defect and ischemia fell by about 50% in the exercise group while remaining virtually unchanged in the control patients.
Dr. Giallauria said that he had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation annual conference.
ROME – Starting cardiac rehabilitation sessions within 2 weeks of an acute myocardial infarction is safe and can improve cardiac perfusion and function, according to results of a randomized, controlled study of 46 patients who had residual myocardial ischemia following an MI and percutaneous coronary revascularization.
"Exercise-induced changes in myocardial perfusion and function were associated with an absence of unfavorable left-ventricular remodeling and an improved cardiovascular functional capacity," Dr. Francesco Giallauria said at the European Association for Cardiovascular Prevention and Rehabilitation* annual meeting. He hypothesized that exercise training begun soon after an MI improves myocardial perfusion by inducing coronary vascular adaptation or enhancing development of collateral cardiac vessels.
The study began with patients who underwent percutaneous coronary intervention (PCI) following an acute ST-elevation MI who were then assessed by dipyridamole stress and gated single-photon emission CT (SPECT) using labeled sestamibi. All 46 included patients had a significant amount of residual myocardial ischemia despite PCI, presumably caused by inadequate perfusion in myocardial regions not vascularized by the PCI-treated coronaries, said Dr. Giallauria, a cardiologist at the University of Naples (Italy). All patients also underwent a cardiopulmonary exercise test at baseline to determine their peak exercise capacity.
The researchers then randomized the patients. Twenty-five entered a hospital outpatient program of supervised, 30-minutes sessions of bicycle exercise three times a week, with an exercise target during each session of 60%-70% of their peak exercise capacity. The program began within 2 weeks of their acute MI. The remaining 21 patients served as controls and received just instructions about maintaining physical exercise and lifestyle modification.
The exercise rehabilitation program continued for 6 months, when all 46 patients underwent a follow-up examination of their myocardial perfusion with gated SPECT and follow-up cardiopulmonary stress testing. The average age of the patients was 54 years, and 87% were men.
The results showed that after 6 months, patients who underwent exercise training had an average 29% increase in peak exercise capacity and a 10% average rise in their peak heart rate compared with baseline, both statistically significant differences. Results from the serial SPECT studies showed that left ventricular ejection fraction rose from an average of 48% at baseline to 52% in the patients who underwent exercise training, a statistically significant rise, and their wall motion and wall thickness scores showed improvements in cardiac shape and function compared with baseline, all differences that were statistically significant. In contrast, the control patients had no significant changes for any of these exercise or cardiac measures during the 6 months of follow-up.
In addition, the SPECT imaging showed that at follow-up the extent of myocardial perfusion defect and ischemia fell by about 50% in the exercise group while remaining virtually unchanged in the control patients.
Dr. Giallauria said that he had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation annual conference.
AT EUROPREVENT 2013
Major finding: Six months of exercise cardiac rehabilitation, started soon after an acute MI, safely boosted exercise capacity by 29%.
Data source: A randomized, controlled, single-center study of 46 patients.
Disclosures: Dr. Giallauria said that he had no disclosures.

ECG keys pre-sport participation screening
ROME – Efficient screening for potentially dangerous arrhythmias in adolescent and young-adult athletes requires the participant’s history, a physical examination, and results from a 12-lead ECG examination, based on experience with more than 15,000 screenings at one U.K. center.
"You need to use symptoms and the ECG results together," Jakir Ullah said at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation. "Either technique by itself is not best." Symptoms in sport participants who underwent screening were not associated with underlying cardiac pathology unless they occurred along with a group 2 ECG abnormality, said Mr. Ullah, a researcher at St. George’s University in London.
Most potentially dangerous cardiac abnormalities in adolescent or young-adult sport participants are asymptomatic, said Dr. Saqib Ghani, a cardiologist at St. George’s and a coinvestigator on the study. "ECG is more helpful than symptoms because you can miss the condition if it’s asymptomatic, and symptoms are very subjective," Dr. Ghani said in an interview.
An expert panel organized by the European Association for Cardiovascular Prevention and Rehabilitation and the European Society of Cardiology compiled a list of 13 uncommon, potentially pathological ECG abnormalities, known as group 2 abnormalities, in 2010 (Eur. J. Cardiol. 2010;31:243-59). The list includes T-wave inversion, left atrial enlargement, a long QT interval, and right ventricular hypertrophy.
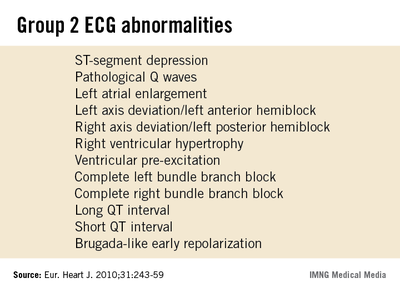
Together, these abnormalities occur in fewer than 5% of people screened by ECG prior to starting sport participation, according to data collected on more than 32,000 Italians aged 8-78 years who underwent pre–sport participation screening during 2003 (Eur. Heart J. 2007:28:2006-10).
Although many sports organizations call for preparticipation screening regardless of age or intensity level, cardiologists at St. George’s focused on people 14-35 years old because children under age 14 often show transient ECG abnormalities, while among adults over age 35 the main cardiac threat during sport participation comes from coronary artery disease rather than an abnormality, Dr. Ghani said.

The St. George’s series consisted of 15,027 people who were examined during 2007-2012. More than half of them were free of any ECG abnormality or symptoms and received immediate clearance for participation. But 6,598 people required further assessment, with 5,415 reporting symptoms, and 1,183 found with a group 2 ECG abnormality. The 8% prevalence rate for a group 2 abnormality, higher than in Italy, matches the somewhat higher U.K. prevalence rates reported by others, he added.
Among the 5,415 people investigated because of symptoms, none were found to have any underlying pathology that precluded sports participation, Mr. Ullah said. Symptoms included chest pain, syncope, palpitations, and dyspnea.
In contrast, among the 1,183 people identified for further assessment because of a group 2 ECG abnormality, the examination identified a clinically important underlying pathology in 67, 0.4% of everyone screened; another 44 people continue to undergo evaluations, and 1,072 people were found free of any sports-limiting condition. Among the 67 with an ECG abnormality and confirmed cardiac pathology, 25 (37%) also had symptoms. The most common cardiac pathology was Wolff-Parkinson-White syndrome, in 29 people, followed by a long QT interval in 8.
Dr. Ghani also stressed that ideally, pre–sport participation screening should occur for all sport participants regardless of the intensity of training or competition. "You only hear about sudden death in high-level athletes, but that is just the tip of the iceberg," he said. "We never know about the sudden death that happens to someone who is just running on the road."
Dr. Ghani and Mr. Ullah had no disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting during which these presentations were given. This story has been updated.
ROME – Efficient screening for potentially dangerous arrhythmias in adolescent and young-adult athletes requires the participant’s history, a physical examination, and results from a 12-lead ECG examination, based on experience with more than 15,000 screenings at one U.K. center.
"You need to use symptoms and the ECG results together," Jakir Ullah said at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation. "Either technique by itself is not best." Symptoms in sport participants who underwent screening were not associated with underlying cardiac pathology unless they occurred along with a group 2 ECG abnormality, said Mr. Ullah, a researcher at St. George’s University in London.
Most potentially dangerous cardiac abnormalities in adolescent or young-adult sport participants are asymptomatic, said Dr. Saqib Ghani, a cardiologist at St. George’s and a coinvestigator on the study. "ECG is more helpful than symptoms because you can miss the condition if it’s asymptomatic, and symptoms are very subjective," Dr. Ghani said in an interview.
An expert panel organized by the European Association for Cardiovascular Prevention and Rehabilitation and the European Society of Cardiology compiled a list of 13 uncommon, potentially pathological ECG abnormalities, known as group 2 abnormalities, in 2010 (Eur. J. Cardiol. 2010;31:243-59). The list includes T-wave inversion, left atrial enlargement, a long QT interval, and right ventricular hypertrophy.
Together, these abnormalities occur in fewer than 5% of people screened by ECG prior to starting sport participation, according to data collected on more than 32,000 Italians aged 8-78 years who underwent pre–sport participation screening during 2003 (Eur. Heart J. 2007:28:2006-10).
Although many sports organizations call for preparticipation screening regardless of age or intensity level, cardiologists at St. George’s focused on people 14-35 years old because children under age 14 often show transient ECG abnormalities, while among adults over age 35 the main cardiac threat during sport participation comes from coronary artery disease rather than an abnormality, Dr. Ghani said.
The St. George’s series consisted of 15,027 people who were examined during 2007-2012. More than half of them were free of any ECG abnormality or symptoms and received immediate clearance for participation. But 6,598 people required further assessment, with 5,415 reporting symptoms, and 1,183 found with a group 2 ECG abnormality. The 8% prevalence rate for a group 2 abnormality, higher than in Italy, matches the somewhat higher U.K. prevalence rates reported by others, he added.
Among the 5,415 people investigated because of symptoms, none were found to have any underlying pathology that precluded sports participation, Mr. Ullah said. Symptoms included chest pain, syncope, palpitations, and dyspnea.
In contrast, among the 1,183 people identified for further assessment because of a group 2 ECG abnormality, the examination identified a clinically important underlying pathology in 67, 0.4% of everyone screened; another 44 people continue to undergo evaluations, and 1,072 people were found free of any sports-limiting condition. Among the 67 with an ECG abnormality and confirmed cardiac pathology, 25 (37%) also had symptoms. The most common cardiac pathology was Wolff-Parkinson-White syndrome, in 29 people, followed by a long QT interval in 8.
Dr. Ghani also stressed that ideally, pre–sport participation screening should occur for all sport participants regardless of the intensity of training or competition. "You only hear about sudden death in high-level athletes, but that is just the tip of the iceberg," he said. "We never know about the sudden death that happens to someone who is just running on the road."
Dr. Ghani and Mr. Ullah had no disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting during which these presentations were given. This story has been updated.
ROME – Efficient screening for potentially dangerous arrhythmias in adolescent and young-adult athletes requires the participant’s history, a physical examination, and results from a 12-lead ECG examination, based on experience with more than 15,000 screenings at one U.K. center.
"You need to use symptoms and the ECG results together," Jakir Ullah said at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation. "Either technique by itself is not best." Symptoms in sport participants who underwent screening were not associated with underlying cardiac pathology unless they occurred along with a group 2 ECG abnormality, said Mr. Ullah, a researcher at St. George’s University in London.
Most potentially dangerous cardiac abnormalities in adolescent or young-adult sport participants are asymptomatic, said Dr. Saqib Ghani, a cardiologist at St. George’s and a coinvestigator on the study. "ECG is more helpful than symptoms because you can miss the condition if it’s asymptomatic, and symptoms are very subjective," Dr. Ghani said in an interview.
An expert panel organized by the European Association for Cardiovascular Prevention and Rehabilitation and the European Society of Cardiology compiled a list of 13 uncommon, potentially pathological ECG abnormalities, known as group 2 abnormalities, in 2010 (Eur. J. Cardiol. 2010;31:243-59). The list includes T-wave inversion, left atrial enlargement, a long QT interval, and right ventricular hypertrophy.
Together, these abnormalities occur in fewer than 5% of people screened by ECG prior to starting sport participation, according to data collected on more than 32,000 Italians aged 8-78 years who underwent pre–sport participation screening during 2003 (Eur. Heart J. 2007:28:2006-10).
Although many sports organizations call for preparticipation screening regardless of age or intensity level, cardiologists at St. George’s focused on people 14-35 years old because children under age 14 often show transient ECG abnormalities, while among adults over age 35 the main cardiac threat during sport participation comes from coronary artery disease rather than an abnormality, Dr. Ghani said.
The St. George’s series consisted of 15,027 people who were examined during 2007-2012. More than half of them were free of any ECG abnormality or symptoms and received immediate clearance for participation. But 6,598 people required further assessment, with 5,415 reporting symptoms, and 1,183 found with a group 2 ECG abnormality. The 8% prevalence rate for a group 2 abnormality, higher than in Italy, matches the somewhat higher U.K. prevalence rates reported by others, he added.
Among the 5,415 people investigated because of symptoms, none were found to have any underlying pathology that precluded sports participation, Mr. Ullah said. Symptoms included chest pain, syncope, palpitations, and dyspnea.
In contrast, among the 1,183 people identified for further assessment because of a group 2 ECG abnormality, the examination identified a clinically important underlying pathology in 67, 0.4% of everyone screened; another 44 people continue to undergo evaluations, and 1,072 people were found free of any sports-limiting condition. Among the 67 with an ECG abnormality and confirmed cardiac pathology, 25 (37%) also had symptoms. The most common cardiac pathology was Wolff-Parkinson-White syndrome, in 29 people, followed by a long QT interval in 8.
Dr. Ghani also stressed that ideally, pre–sport participation screening should occur for all sport participants regardless of the intensity of training or competition. "You only hear about sudden death in high-level athletes, but that is just the tip of the iceberg," he said. "We never know about the sudden death that happens to someone who is just running on the road."
Dr. Ghani and Mr. Ullah had no disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting during which these presentations were given. This story has been updated.
AT EUROPREVENT 2013
Major finding: Cardiac symptoms with no group 2 ECG abnormality were associated with no cases of dangerous cardiac pathology.
Data source: Data came from screening 15,027 people 14-35 years old at one U.K. hospital during 2007-2012.
Disclosures: Dr. Ghani and Mr. Ullah had no disclosures.
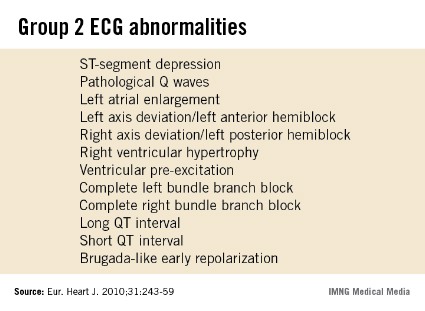
Heart rate linked to men's heart failure
ROME – Otherwise healthy, older men with a heart rate of 79 beats per minute or higher had a roughly 50% increased risk of developing heart failure, compared with men with slower heart rates, in a population-based cohort of more than 1,800 Dutch men.
The finding suggests that heart rate, independent of any other cardiovascular risk factor, could boost the risk for developing heart failure, and raises the possibility of trying to dampen this effect by using interventions to reduce heart rate, Dr. David Nanchen said at the annual meeting of the * European Association for Cardiovascular Prevention and Rehabilitation.

But the apparent link between resting heart rate and a boosted incidence of heart failure during follow-up occurred only in men. The analysis also included 2,939 women, who showed no suggestion of an association between baseline heart rate and subsequent development of heart failure.
The work reported by Dr. Nanchen also included an analysis that censored men who had an incident myocardial infarction during a median follow-up of 15 years, thereby eliminating cases of heart failure that occurred following an MI. In this analysis, men with a baseline heart rate of 79 beats per minute or greater had a statistically significant, 56% increased incidence of heart failure compared with men with an entry heart rate of less than 69 beats per minute, said Dr. Nanchen, head of the cardiovascular preventative clinic of the University of Lausanne (Switzerland).
Ruling out MI as a mediator between high heart rate and the development of heart failure means some other pathologic sequence is involved. One possibility is that patients with high heart rates develop tachycardia-induced cardiomyopathy that progresses to heart failure, Dr. Nanchen said in an interview."
His study included 4,768 people aged 55 or older enrolled in the Rotterdam Study from among apparently healthy people living in the Rotterdam area. During a median follow-up of 15 years, 656 enrollees developed heart failure. The analysis excluded people who at baseline had heart failure, coronary heart disease, atrial fibrillation, atrioventricular block, or a pacemaker, or were taking a beta-blocker or calcium channel blocker.
Among the 1,829 men in the study, every increment of 10 beats per minute in resting heart rate at entry into the study was linked with a statistically significant, 16% relative increase in the incidence of heart failure, an association not seen in women. When the researchers divided the men into tertiles based on their baseline heart rate, those in the top tertile with a rate of 79 beats per minute or greater had a 51% increased incidence of heart failure during follow-up, compared with men in the lowest tertile, with a rate of less than 69 beats per minute.
The analysis adjusted for age, smoking status, systolic blood pressure, diabetes, body mass index, total cholesterol level, HDL cholesterol level, and antihypertensive treatment.
The absence of this heart rate and heart failure link in women was a "surprise," Dr. Nanchen said. It’s possible that women’s hearts are more resilient to high heart rates, he suggested.
For the time being, the only intervention to offer otherwise healthy men older than 55 with a high heart rate is intensified control of lifestyle risk factors. Trial results showed that treatment with the heart rate–lowering drug ivabradine (Prooralan) in heart failure patients led to a reduction in heart failure–related hospitalizations (Lancet 2010;376:875-85).That experience makes it attractive to speculate that ivabradine treatment might also improve outcomes in men with high heart rates and no heart failure, but Dr. Nanchen said he had no immediate plans to test that hypothesis.
U.S. physicians won’t get the chance to study ivabradine in clinical practice for some time. Its manufacturer, Servier, has not disclosed any plans to submit a new drug application to the Food and Drug Administration.
Dr. Nanchen said he had no relevant financial disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting from which this presentation was made. This version has been updated.
ROME – Otherwise healthy, older men with a heart rate of 79 beats per minute or higher had a roughly 50% increased risk of developing heart failure, compared with men with slower heart rates, in a population-based cohort of more than 1,800 Dutch men.
The finding suggests that heart rate, independent of any other cardiovascular risk factor, could boost the risk for developing heart failure, and raises the possibility of trying to dampen this effect by using interventions to reduce heart rate, Dr. David Nanchen said at the annual meeting of the * European Association for Cardiovascular Prevention and Rehabilitation.
But the apparent link between resting heart rate and a boosted incidence of heart failure during follow-up occurred only in men. The analysis also included 2,939 women, who showed no suggestion of an association between baseline heart rate and subsequent development of heart failure.
The work reported by Dr. Nanchen also included an analysis that censored men who had an incident myocardial infarction during a median follow-up of 15 years, thereby eliminating cases of heart failure that occurred following an MI. In this analysis, men with a baseline heart rate of 79 beats per minute or greater had a statistically significant, 56% increased incidence of heart failure compared with men with an entry heart rate of less than 69 beats per minute, said Dr. Nanchen, head of the cardiovascular preventative clinic of the University of Lausanne (Switzerland).
Ruling out MI as a mediator between high heart rate and the development of heart failure means some other pathologic sequence is involved. One possibility is that patients with high heart rates develop tachycardia-induced cardiomyopathy that progresses to heart failure, Dr. Nanchen said in an interview."
His study included 4,768 people aged 55 or older enrolled in the Rotterdam Study from among apparently healthy people living in the Rotterdam area. During a median follow-up of 15 years, 656 enrollees developed heart failure. The analysis excluded people who at baseline had heart failure, coronary heart disease, atrial fibrillation, atrioventricular block, or a pacemaker, or were taking a beta-blocker or calcium channel blocker.
Among the 1,829 men in the study, every increment of 10 beats per minute in resting heart rate at entry into the study was linked with a statistically significant, 16% relative increase in the incidence of heart failure, an association not seen in women. When the researchers divided the men into tertiles based on their baseline heart rate, those in the top tertile with a rate of 79 beats per minute or greater had a 51% increased incidence of heart failure during follow-up, compared with men in the lowest tertile, with a rate of less than 69 beats per minute.
The analysis adjusted for age, smoking status, systolic blood pressure, diabetes, body mass index, total cholesterol level, HDL cholesterol level, and antihypertensive treatment.
The absence of this heart rate and heart failure link in women was a "surprise," Dr. Nanchen said. It’s possible that women’s hearts are more resilient to high heart rates, he suggested.
For the time being, the only intervention to offer otherwise healthy men older than 55 with a high heart rate is intensified control of lifestyle risk factors. Trial results showed that treatment with the heart rate–lowering drug ivabradine (Prooralan) in heart failure patients led to a reduction in heart failure–related hospitalizations (Lancet 2010;376:875-85).That experience makes it attractive to speculate that ivabradine treatment might also improve outcomes in men with high heart rates and no heart failure, but Dr. Nanchen said he had no immediate plans to test that hypothesis.
U.S. physicians won’t get the chance to study ivabradine in clinical practice for some time. Its manufacturer, Servier, has not disclosed any plans to submit a new drug application to the Food and Drug Administration.
Dr. Nanchen said he had no relevant financial disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting from which this presentation was made. This version has been updated.
ROME – Otherwise healthy, older men with a heart rate of 79 beats per minute or higher had a roughly 50% increased risk of developing heart failure, compared with men with slower heart rates, in a population-based cohort of more than 1,800 Dutch men.
The finding suggests that heart rate, independent of any other cardiovascular risk factor, could boost the risk for developing heart failure, and raises the possibility of trying to dampen this effect by using interventions to reduce heart rate, Dr. David Nanchen said at the annual meeting of the * European Association for Cardiovascular Prevention and Rehabilitation.
But the apparent link between resting heart rate and a boosted incidence of heart failure during follow-up occurred only in men. The analysis also included 2,939 women, who showed no suggestion of an association between baseline heart rate and subsequent development of heart failure.
The work reported by Dr. Nanchen also included an analysis that censored men who had an incident myocardial infarction during a median follow-up of 15 years, thereby eliminating cases of heart failure that occurred following an MI. In this analysis, men with a baseline heart rate of 79 beats per minute or greater had a statistically significant, 56% increased incidence of heart failure compared with men with an entry heart rate of less than 69 beats per minute, said Dr. Nanchen, head of the cardiovascular preventative clinic of the University of Lausanne (Switzerland).
Ruling out MI as a mediator between high heart rate and the development of heart failure means some other pathologic sequence is involved. One possibility is that patients with high heart rates develop tachycardia-induced cardiomyopathy that progresses to heart failure, Dr. Nanchen said in an interview."
His study included 4,768 people aged 55 or older enrolled in the Rotterdam Study from among apparently healthy people living in the Rotterdam area. During a median follow-up of 15 years, 656 enrollees developed heart failure. The analysis excluded people who at baseline had heart failure, coronary heart disease, atrial fibrillation, atrioventricular block, or a pacemaker, or were taking a beta-blocker or calcium channel blocker.
Among the 1,829 men in the study, every increment of 10 beats per minute in resting heart rate at entry into the study was linked with a statistically significant, 16% relative increase in the incidence of heart failure, an association not seen in women. When the researchers divided the men into tertiles based on their baseline heart rate, those in the top tertile with a rate of 79 beats per minute or greater had a 51% increased incidence of heart failure during follow-up, compared with men in the lowest tertile, with a rate of less than 69 beats per minute.
The analysis adjusted for age, smoking status, systolic blood pressure, diabetes, body mass index, total cholesterol level, HDL cholesterol level, and antihypertensive treatment.
The absence of this heart rate and heart failure link in women was a "surprise," Dr. Nanchen said. It’s possible that women’s hearts are more resilient to high heart rates, he suggested.
For the time being, the only intervention to offer otherwise healthy men older than 55 with a high heart rate is intensified control of lifestyle risk factors. Trial results showed that treatment with the heart rate–lowering drug ivabradine (Prooralan) in heart failure patients led to a reduction in heart failure–related hospitalizations (Lancet 2010;376:875-85).That experience makes it attractive to speculate that ivabradine treatment might also improve outcomes in men with high heart rates and no heart failure, but Dr. Nanchen said he had no immediate plans to test that hypothesis.
U.S. physicians won’t get the chance to study ivabradine in clinical practice for some time. Its manufacturer, Servier, has not disclosed any plans to submit a new drug application to the Food and Drug Administration.
Dr. Nanchen said he had no relevant financial disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting from which this presentation was made. This version has been updated.
AT EUROPREVENT 2013
Major finding: Among healthy men, heart rates of at least 79 beats per minute were linked with a 51% increased incidence of heart failure.
Data source: A prospective follow-up of a population-based cohort of 4,768 people enrolled in the Rotterdam Study.
Disclosures: Dr. Nanchen said he had no relevant financial disclosures.

European hypertension group endorses broad preeclampsia prophylaxis
ROME – The European Society of Hypertension is poised to endorse low-dose aspirin prophylaxis against preeclampsia for a large percent of pregnant women, according to a report at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation.
Endorsement of aspirin treatment for prophylaxis of preeclampsia in moderate- and high-risk women is part of new guidelines for managing hypertension prepared jointly by the European Society of Hypertension (ESH) and the European Society of Cardiology that will be unveiled at the hypertension society’s annual meeting in Milan in June, Dr. Renata Cifková said at the meeting.

"Aspirin, at a dosage of 75 mg/day, is recommended for the prevention of preeclampsia in women at high or moderate risk of preeclampsia from 12 weeks’ gestation until delivery," said Dr. Cifková, professor and head of the department of preventive cardiology at Thomayer University Hospital in Prague. The high- and moderate-risk categories together define a large proportion of women who become pregnant today.
The new guidelines define women at high risk who should receive aspirin prophylaxis as those who had gestational hypertension during a prior pregnancy, or women with chronic kidney disease, an autoimmune disease such as systemic lupus erythematosus or antiphospholipid syndrome, type 1 or 2 diabetes, or chronic hypertension. The guidelines also say that women should receive aspirin prophylaxis if they have two or more of these moderate-risk factors for preeclampsia: first pregnancy, age 40 years or older, a prior pregnancy interval of more than 10 years, a body mass index of 30 kg/m2 or greater, a family history of preeclampsia, or a multiple pregnancy.
These new ESH guidelines for preeclampsia prevention with aspirin follow exactly the recommendations made in August 2010 by the U.K.’s National Institute for Health and Clinical Excellence (NICE), noted Dr. Cifková. The most notable evidence supporting this approach came from a meta-analysis published in 2010 that included 27 studies involving more than 11,000 women and found that low-dose aspirin begun early in pregnancy cut the incidence of preeclampsia by about 50% (Ob.Gyn. 2010;116:402-14).
Another soon-to-appear guidance from the ESH, on appropriate patients for ambulatory blood pressure monitoring (ABPM), received a preview from Dr. Gianfranco Parati, professor of cardiovascular medicine at the University of Milan.

The new revision comes from an expert panel first convened 2 years ago by the ESH, Dr. Parati said at the meeting. The soon-to-be-published position on ABPM will not make recommendations that are as well defined as the ones for preeclampsia prophylaxis. "Is ABPM needed for every patient with hypertension? No, but it should be used in more patients," he said. Routine use of ABPM to confirm hypertension in all patients "is not suitable for every country because of its cost," he added.
Nonetheless, the new ESH consensus statement calls for using ABPM to confirm a diagnosis of hypertension or its absence, and thereby better avoid the twin nemeses of accurate hypertension assessment: white coat hypertension and masked hypertension, he said. ABPM also allows assessment of blood pressure control throughout 24 hours. The new guidelines say that ABPM is appropriate for selected elderly, children, and adolescent patients, and during pregnancy.
When high-risk patients or patients with nocturnal hypertension undergo ABPM, a follow-up, repeat examination should be done in 6 months. In most other patients, follow-up ABPM can occur after 1-2 years, Dr. Parati said.
Dr. Cifková reported no relevant financial disclosures. Dr. Parati has received honoraria from Bayer, Boegringer Ingelheim, Daiichi-Sankyo, Merck Serono, Menarini, Novartis, Recordati, Sanofi Aventis, and Takeda, and research support from Boehringer Ingelheim, Bayer, and Sanofi Aventis.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the meeting name during which these presentations were made. This version has been updated.
ROME – The European Society of Hypertension is poised to endorse low-dose aspirin prophylaxis against preeclampsia for a large percent of pregnant women, according to a report at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation.
Endorsement of aspirin treatment for prophylaxis of preeclampsia in moderate- and high-risk women is part of new guidelines for managing hypertension prepared jointly by the European Society of Hypertension (ESH) and the European Society of Cardiology that will be unveiled at the hypertension society’s annual meeting in Milan in June, Dr. Renata Cifková said at the meeting.
"Aspirin, at a dosage of 75 mg/day, is recommended for the prevention of preeclampsia in women at high or moderate risk of preeclampsia from 12 weeks’ gestation until delivery," said Dr. Cifková, professor and head of the department of preventive cardiology at Thomayer University Hospital in Prague. The high- and moderate-risk categories together define a large proportion of women who become pregnant today.
The new guidelines define women at high risk who should receive aspirin prophylaxis as those who had gestational hypertension during a prior pregnancy, or women with chronic kidney disease, an autoimmune disease such as systemic lupus erythematosus or antiphospholipid syndrome, type 1 or 2 diabetes, or chronic hypertension. The guidelines also say that women should receive aspirin prophylaxis if they have two or more of these moderate-risk factors for preeclampsia: first pregnancy, age 40 years or older, a prior pregnancy interval of more than 10 years, a body mass index of 30 kg/m2 or greater, a family history of preeclampsia, or a multiple pregnancy.
These new ESH guidelines for preeclampsia prevention with aspirin follow exactly the recommendations made in August 2010 by the U.K.’s National Institute for Health and Clinical Excellence (NICE), noted Dr. Cifková. The most notable evidence supporting this approach came from a meta-analysis published in 2010 that included 27 studies involving more than 11,000 women and found that low-dose aspirin begun early in pregnancy cut the incidence of preeclampsia by about 50% (Ob.Gyn. 2010;116:402-14).
Another soon-to-appear guidance from the ESH, on appropriate patients for ambulatory blood pressure monitoring (ABPM), received a preview from Dr. Gianfranco Parati, professor of cardiovascular medicine at the University of Milan.
The new revision comes from an expert panel first convened 2 years ago by the ESH, Dr. Parati said at the meeting. The soon-to-be-published position on ABPM will not make recommendations that are as well defined as the ones for preeclampsia prophylaxis. "Is ABPM needed for every patient with hypertension? No, but it should be used in more patients," he said. Routine use of ABPM to confirm hypertension in all patients "is not suitable for every country because of its cost," he added.
Nonetheless, the new ESH consensus statement calls for using ABPM to confirm a diagnosis of hypertension or its absence, and thereby better avoid the twin nemeses of accurate hypertension assessment: white coat hypertension and masked hypertension, he said. ABPM also allows assessment of blood pressure control throughout 24 hours. The new guidelines say that ABPM is appropriate for selected elderly, children, and adolescent patients, and during pregnancy.
When high-risk patients or patients with nocturnal hypertension undergo ABPM, a follow-up, repeat examination should be done in 6 months. In most other patients, follow-up ABPM can occur after 1-2 years, Dr. Parati said.
Dr. Cifková reported no relevant financial disclosures. Dr. Parati has received honoraria from Bayer, Boegringer Ingelheim, Daiichi-Sankyo, Merck Serono, Menarini, Novartis, Recordati, Sanofi Aventis, and Takeda, and research support from Boehringer Ingelheim, Bayer, and Sanofi Aventis.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the meeting name during which these presentations were made. This version has been updated.
ROME – The European Society of Hypertension is poised to endorse low-dose aspirin prophylaxis against preeclampsia for a large percent of pregnant women, according to a report at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation.
Endorsement of aspirin treatment for prophylaxis of preeclampsia in moderate- and high-risk women is part of new guidelines for managing hypertension prepared jointly by the European Society of Hypertension (ESH) and the European Society of Cardiology that will be unveiled at the hypertension society’s annual meeting in Milan in June, Dr. Renata Cifková said at the meeting.
"Aspirin, at a dosage of 75 mg/day, is recommended for the prevention of preeclampsia in women at high or moderate risk of preeclampsia from 12 weeks’ gestation until delivery," said Dr. Cifková, professor and head of the department of preventive cardiology at Thomayer University Hospital in Prague. The high- and moderate-risk categories together define a large proportion of women who become pregnant today.
The new guidelines define women at high risk who should receive aspirin prophylaxis as those who had gestational hypertension during a prior pregnancy, or women with chronic kidney disease, an autoimmune disease such as systemic lupus erythematosus or antiphospholipid syndrome, type 1 or 2 diabetes, or chronic hypertension. The guidelines also say that women should receive aspirin prophylaxis if they have two or more of these moderate-risk factors for preeclampsia: first pregnancy, age 40 years or older, a prior pregnancy interval of more than 10 years, a body mass index of 30 kg/m2 or greater, a family history of preeclampsia, or a multiple pregnancy.
These new ESH guidelines for preeclampsia prevention with aspirin follow exactly the recommendations made in August 2010 by the U.K.’s National Institute for Health and Clinical Excellence (NICE), noted Dr. Cifková. The most notable evidence supporting this approach came from a meta-analysis published in 2010 that included 27 studies involving more than 11,000 women and found that low-dose aspirin begun early in pregnancy cut the incidence of preeclampsia by about 50% (Ob.Gyn. 2010;116:402-14).
Another soon-to-appear guidance from the ESH, on appropriate patients for ambulatory blood pressure monitoring (ABPM), received a preview from Dr. Gianfranco Parati, professor of cardiovascular medicine at the University of Milan.
The new revision comes from an expert panel first convened 2 years ago by the ESH, Dr. Parati said at the meeting. The soon-to-be-published position on ABPM will not make recommendations that are as well defined as the ones for preeclampsia prophylaxis. "Is ABPM needed for every patient with hypertension? No, but it should be used in more patients," he said. Routine use of ABPM to confirm hypertension in all patients "is not suitable for every country because of its cost," he added.
Nonetheless, the new ESH consensus statement calls for using ABPM to confirm a diagnosis of hypertension or its absence, and thereby better avoid the twin nemeses of accurate hypertension assessment: white coat hypertension and masked hypertension, he said. ABPM also allows assessment of blood pressure control throughout 24 hours. The new guidelines say that ABPM is appropriate for selected elderly, children, and adolescent patients, and during pregnancy.
When high-risk patients or patients with nocturnal hypertension undergo ABPM, a follow-up, repeat examination should be done in 6 months. In most other patients, follow-up ABPM can occur after 1-2 years, Dr. Parati said.
Dr. Cifková reported no relevant financial disclosures. Dr. Parati has received honoraria from Bayer, Boegringer Ingelheim, Daiichi-Sankyo, Merck Serono, Menarini, Novartis, Recordati, Sanofi Aventis, and Takeda, and research support from Boehringer Ingelheim, Bayer, and Sanofi Aventis.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the meeting name during which these presentations were made. This version has been updated.
AT EUROPREVENT 2013
