User login
The number of total hip and knee replacement surgeries is increasing, and consequently, more patients are at risk of venous thromboembolism (VTE).1 Without thromboprophylaxis, the incidence of proximal deep vein thrombosis (DVT) is about 18% to 36% following total hip replacement (THR) and about 5% to 22% following total knee replacement (TKR). The incidence of total pulmonary embolism (PE) has been estimated at 0.9% to 28% in THR and 1.5% to 10% in TKR, and the incidence of fatal PE has been estimated to be as high as 2% following total joint replacement surgery.2 Despite the availability of effective anticoagulant agents for thromboprophylaxis, symptomatic VTE continues to occur in 1.3% to 10.0% of patients in the 3-month period following joint replacement surgery.2
VTE following THR or TKR represents a significant source of morbidity and mortality as well as a financial burden on the health care system. This burden is increased further by the complications of VTE—including a high rate of recurrence, postthrombotic syndrome (PTS), and pulmonary hypertension—which may be more debilitating than the primary event.3-5 Effective prophylaxis of VTE is paramount in reducing the incidence of these consequences.
Rivaroxaban, a Factor Xa inhibitor, is a novel anticoagulant that has recently been approved by the U.S. Food and Drug Administration (FDA) for prophylaxis of DVT in patients undergoing THR or TKR as well as for reduction of the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation (AFib).6 Clinical trials have shown that rivaroxaban is superior to enoxaparin, the standard of care, in preventing VTE after total joint replacement, and cost-effectiveness studies have demonstrated that rivaroxaban may potentially be a cost-saving agent.
This clinical review will address the economic and public health burden of VTE following THR and TKR and evaluate the novel anticoagulants that have been studied for this indication, including rivaroxaban. The safety and efficacy of rivaroxaban will be discussed, along with cost-effectiveness issues and practical management information.
The Economic Burden of VTE
VTE is the most common cause of hospital readmission following THR.2 The occurrence of VTE is reported to significantly increase the length of hospital stays and health care charges in patients undergoing TKR or THR. For example, one study reported health care charges for the index admission that were $9,297 higher for inpatients who experienced VTE compared with patients with TKR who did not have a VTE (P = .02).7 Similarly, for patients with THR, health care charges were $25,853 higher for inpatients who experienced VTE compared with patients who did not (P < .01).7
According to Spyropoulos and Lin, the total annual health care cost of a VTE (not limited to orthopedic patients) is $7,594 to $16,644, depending on the type of VTE (DVT or PE) and whether it was the primary or secondary diagnosis on discharge.8 These costs are significant, especially when multiplied by the number of THR and TKR surgeries performed in the U.S. Furthermore, VTE complications, such as PTS, represent an additional driver of health care expenditures.5,9,10
VTE Prophylaxis Guidelines
Both the American College of Chest Physicians (ACCP) and the American Academy of Orthopaedic Surgeons (AAOS) have published evidence-based guidelines for the prevention of VTE following total joint replacement.2,11 The 2012 version of the ACCP guidelines recommended the routine use of low-molecular-weight heparins (LMWHs), fondaparinux, low-dose unfractionated heparin, aspirin, adjusted-dose warfarin, rivaroxaban, apixaban, or dabigatran for thromboprophylaxis following THR or TKR. In contrast, the 2011 version of the AAOS guidelines makes no specific recommendations for pharmacologic agents.11 Despite the availability of evidence-based guidelines with specific recommendations, physician compliance with these guidelines is low.12
Before the approval of rivaroxaban, the vitamin K antagonist warfarin was the only available oral option for thromboprophylaxis following THR or TKR. The use of warfarin can be challenging, because it requires frequent monitoring and maintaining a patient within a specified international normalized ratio (INR) range. Several factors may influence time-in-therapeutic range, including drug-drug and drug-food interactions and genetic polymorphisms of vitamin K epoxide reductase complex subunit 1 (VKORC1) and cytochrome P450 (CYP)2C9.13 Warfarin does not provide short-term prophylaxis because of its delayed onset of action. It has been reported that 5 days after THR and TKR only about 30% of patients are within an INR of 2.0 to 3.0.14 Patients with an INR below 2.0 are at a 4- to 5-fold increased risk for VTE.14
Low-molecular-weight heparins, such as enoxaparin, do not require routine monitoring and have minimal drug interactions.15 The main drawback of LMWHs is their injectable mode of administration, which may influence prescribing habits and medication adherence. Patient education plays an essential role in ensuring adherence to LMWHs following orthopedic surgery.16
New Oral Anticoagulants
The new oral anticoagulants that have completed phase 3 trials for VTE prophylaxis following total joint replacement surgery include the selective Factor Xa inhibitors rivaroxaban and apixaban and the direct thrombin inhibitor dabigatran etexilate. Unlike warfarin, these agents do not require routine monitoring, a result of their predictable pharmacokinetic/pharmacodynamic (PK/PD) relationship, and they have few clinically significant drug interactions.17 Dabigatran and apixaban are not currently FDA approved for VTE prophylaxis following total joint replacement surgery; however, rivaroxaban was approved by the FDA in July 2011 for this indication.6
Apixaban
The Apixaban or Enoxaparin for Thromboprophylaxis After Knee Replacement (ADVANCE)-1 and ADVANCE-2 trials evaluated the use of Apixaban for thromboprophylaxis in patients undergoing TKR.18,19 In the ADVANCE-1 trial, patients undergoing TKR were randomized to receive either apixaban 2.5 mg orally twice daily or the North American preferred dosing of enoxaparin, 30 mg subcutaneously (SC) twice daily, with both agents started 12 to 24 hours after surgery and then taken for 10 to 14 days.18
Apixaban did not meet the prespecified statistical criteria for noninferiority compared with enoxaparin, although the rates of the primary efficacy endpoint (composite of VTE and all-cause mortality) were similar: 9.0% and 8.8% of patients, respectively. However, apixaban showed lower rates of clinically relevant bleeding and a similar adverse event (AE) profile compared with enoxaparin.
In the ADVANCE-2 trial, patients undergoing TKR received either apixaban 2.5 mg orally twice daily or enoxaparin 40 mg SC once daily for 10 to 14 days.19 The primary efficacy outcome (composite of total VTE and all-cause mortality) occurred at significantly lower rates in patients receiving apixaban (15% and 24%, respectively; relative risk [RR] 0.62; 95% confidence interval [CI] 0.51-0.74; P < .0001). Rates of major or clinically relevant nonmajor bleeding events occurred at similar rates between the 2 groups.
In the ADVANCE-3 trial, patients undergoing THR received either apixaban 2.5 orally twice daily or enoxaparin 40 mg SC once daily for 35 days.20 The primary efficacy outcome (composite of total VTE and all-cause mortality) occurred at significantly lower rates in patients receiving apixaban (1.4% and 3.9%, respectively; RR 0.36; 95% CI 0.22-0.54; P < .001). Rates of major or clinically relevant nonmajor bleeding events occurred at similar rates between both groups.
Dabigatran etexilate
Dabigatran etexilate has been evaluated in patients undergoing TKR in the Oral Dabigatran Etexilate vs Subcutaneous Enoxaparin for the Prevention of Venous Thromboembolism After Total Knee Replacement (RE-MODEL) and Oral Thrombin Inhibitor Dabigatran Etexilate vs North American Enoxaparin Regimen for Prevention of Venous Thromboembolism After Total Knee Replacement (RE-MOBILIZE) studies and in patients undergoing THR in the Oral Dabigatran vs Enoxaparin for Thromboprophylaxis After Primary Total Hip Arthroplasty (RE-NOVATE)-1 and RE-NOVATE‑2 trials.21-24
In RE-MODEL, patients undergoing TKR received either 150 mg or 220 mg of dabigatran etexilate once daily (starting with a half dose 1 to 4 hours after surgery) or enoxaparin 40 mg once daily (started the evening before surgery) for 6 to 10 days.23 Both doses of dabigatran had a similar incidence of the composite of total VTE and mortality and major bleeding. In RE-MOBILIZE, patients undergoing TKR received either 150 mg or 220 mg of dabigatran etexilate once daily or the North American regimen of enoxaparin, 30 mg SC twice daily for 12 to 15 days.24 Both dabigatran regimens had a significantly higher incidence of the composite of total VTE, failing to establish noninferiority to enoxaparin. The incidence of major bleeding was not significantly different among the 3 groups.
In RE-NOVATE I, patients undergoing THR received either dabigatran 150 mg or 220 mg twice daily, or enoxaparin 40 mg SC once daily for 28 to 35 days.21 Both doses of dabigatran had a similar incidence of the composite of total VTE and mortality and major bleeding. Because RE-NOVATE I did not include any study sites in North America, a second phase 3 trial, RE-NOVATE II, was conducted to include North American sites. RE-NOVATE II had an identical trial design to RE-NOVATE I and similar results (noninferior efficacy and comparable safety).22
Rivaroxaban
The phase 3 Rivaroxaban vs Enoxaparin for Thromboprophylaxis After Hip Arthroplasty (RECORD) program consisted of 4 double-blind randomized trials that compared the efficacy and safety of oral rivaroxaban to SC enoxaparin in THR (RECORD1 and 2) and TKR (RECORD3 and 4). The RECORD1 and 2 trials compared rivaroxaban 10 mg orally once daily for 31 to 39 days with enoxaparin 40 mg SC once daily (for 31-39 days in RECORD1 and for 10-14 days followed by placebo in RECORD2). The RECORD3 and 4 trials compared 10- to 14-day regimens of rivaroxaban 10 mg orally once daily with enoxaparin 40 mg SC once daily (RECORD3) and 30 mg twice daily (RECORD4). The 4 trials used the same efficacy and safety outcomes (Table).
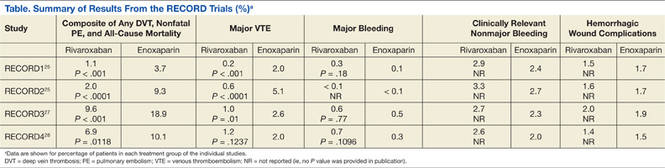
In the RECORD1, 2, and 3 studies, rivaroxaban significantly reduced the composite of DVT, nonfatal PE, and all-cause mortality, as well as major VTE compared with enoxaparin. Major bleeding events as well as clinically relevant nonmajor bleeding and hemorrhagic wound complications were similar across both groups.25-27
In the RECORD4 study, rivaroxaban significantly reduced the composite of DVT, nonfatal PE, and all-cause mortality, but not major VTE, in patients undergoing TKR. Major bleeding events as well as clinically relevant nonmajor bleeding were numerically higher in the rivaroxaban group, but this was not statistically significant. Hemorrhagic wound complications were similar across both groups.28 This study was not required for approval and was not included in the final FDA-approved package insert.29
In a pooled analysis of the 4 RECORD trials presented at the FDA advisory committee, the incidence of major bleeding was significantly higher in the rivaroxaban group (24 events [0.39%]) compared with enoxaparin (13 events [0.21%]), with a nominal P value of .08 (significant at 10% nominal level) in the total treatment duration pool.30 In a pooled analysis by Turpie and colleagues who used the same data, this difference was not determined to be statistically different.31 In addition, this pooled analysis showed that the incidence of treatment-emergent hemorrhagic wound complications was similar in patients receiving rivaroxaban and enoxaparin and that fewer treatment-emergent serious AEs occurred in patients receiving rivaroxaban compared with patients receiving enoxaparin.31
In the FDA advisory committee, an “isolated signal” for a potentially increased risk of ischemic stroke was identified: In the safety population, ischemic stroke occurred in 5 patients who had received rivaroxaban and 1 patient who received enoxaparin.30 Furthermore, cardiovascular events in the safety population were concentrated around discontinuation of rivaroxaban, which was not the case for enoxaparin. The concern of stroke following rivaroxaban discontinuation was much more robust in Rivaroxaban vs Warfarin in Nonvalvular Atrial Fibrillation (ROCKET-AF), the phase 3 trial that compared rivaroxaban and warfarin for stroke prophylaxis in AFib.32 In the study ROCKET-AF, higher rates of stroke and systemic embolism were observed at the end of the trial among patients discontinuing rivaroxaban and switching to open-label warfarin compared with patients who had been taking warfarin and were transitioned to open-label warfarin. This observation led to a black box warning in the label of rivaroxaban regarding discontinuation of this agent.33
rivaroxaban management
The approved dose of rivaroxaban for the prophylaxis of VTE is 10 mg orally once daily with or without food.29 The first dose should be taken 6 to 10 hours after surgery, once hemostasis has been established. Rivaroxaban should be administered for 35 days to patients undergoing THR and for 12 days to patients undergoing TKR. Tablets may be crushed and administered in a gastric feeding tube, but they must not be administered via feeding tubes that deliver the contents into the proximal small intestine, because reduced drug absorption may result.29
The prescribing information for rivaroxaban includes a black box warning stating that epidural or spinal hematomas have occurred in patients treated with rivaroxaban who are receiving neuraxial (ie, spinal or epidural) anesthesia or undergoing spinal puncture. For such patients, the epidural catheter should not be removed earlier than 18 hours after the last administration of rivaroxaban.29 The next rivaroxaban dose should not be administered earlier than 6 hours after the catheter is removed.29 If a traumatic puncture occurs, rivaroxaban administration should be delayed for 24 hours.29 Factors that can increase the risk of developing epidural or spinal hematomas include the use of indwelling epidural catheters, concomitant use of drugs that affect hemostasis (eg, nonsteroidal anti-inflammatory drugs [NSAIDs], platelet inhibitors, and other anticoagulants), a history of traumatic or repeated epidural or spinal punctures, and a history of spinal deformity or spinal surgery.
Rivaroxaban has not been studied in severe hepatic impairment (Child-Pugh C), and in subjects with moderate hepatic impairment (Child-Pugh B), rivaroxaban has led to increased drug exposure, with increased PD effects. Therefore, rivaroxaban should be avoided in patients with moderate to severe hepatic impairment or any hepatic disease associated with coagulopathy.29
Rivaroxaban should also be avoided in patients with severe renal impairment (a creatinine clearance [CrCl] of < 30 mL/min), because increased exposure with increased PD effects is expected. A combined analysis of the RECORD1, 2, and 3 trials did not show an increased bleeding risk for patients with moderate renal impairment (CrCl 30-50 mL/min) taking rivaroxaban. However, such patients should be observed for signs or symptoms of bleeding. Discontinuation should be considered in any patient who develops acute renal failure while taking rivaroxaban.
Drug interaction studies found that the concomitant use of rivaroxaban with drugs that are combined P-glycoprotein (P-gp) and CYP3A4 inhibitors led to increased rivaroxaban exposure and PD effects (ie, Factor Xa inhibition and prolonged prothrombin time). Rivaroxaban exposure was increased significantly when the drug was administered with combined P-gp and strong CYP3A4 inhibitors (eg, azole antifungal agents and protease inhibitors). Therefore, coadministration of rivaroxaban with these agents should be avoided, particularly in patients with any degree of renal impairment, because bleeding risk may increase. In cases where a change in exposure is considered unlikely to affect bleeding risk (ie, coadministration of weaker combined P-gp and CYP3A4 inhibitors, such as clarithromycin and erythromycin), no precautions are necessary.
If bleeding occurs during treatment with rivaroxaban, it may be appropriate to temporarily discontinue the drug and start supportive care. Rivaroxaban has a relatively short half-life (5-9 hours in healthy subjects aged 20-45 years and 11-13 hours in the elderly), meaning that drug effect decreases relatively quickly compared with warfarin. There is currently no direct antidote for rivaroxaban, but a study in healthy human subjects demonstrated that administration of prothrombin complex concentrates may be a potential option.34 Absolute contraindications to rivaroxaban treatment include patients with active pathological bleeding and those with severe hypersensitivity to the drug.
RIVAROXABAN ECONOMICS
Despite its high cost, economic analyses indicate that enoxaparin is a cost-effective agent for VTE prophylaxis compared with warfarin, which is well known to be inexpensive.35 An economic analysis that took into account prophylaxis failures and treatment complications as well as the direct costs associated with medical services, drugs, and laboratory tests showed a cost advantage for enoxaparin over warfarin that lasted for a substantial amount of time (19-31 days after hospital discharge).35
An economic model that followed patients for 1 year postsurgery specifically evaluated the costs associated with symptomatic VTE and major bleeding events in the RECORD trials, assuming the cost of rivaroxaban to be similar to that of enoxaparin 40 mg.36 Cost savings for rivaroxaban over enoxaparin were $82 to $291 per patient, depending on the indication (TKR or THR) and regimen, with cost savings increasing further if the costs of home nursing or training patients to self-administer enoxaparin are included.36 This economic model was also applied to THR and TKR figures from 2005 to show the global cost-effectiveness of rivaroxaban.37 This analysis showed that based on RECORD1, the use of rivaroxaban was associated with an average cost savings of $82 per patient and a reduction of 6 symptomatic events per 1,000 patients undergoing THR. Based on RECORD3, the use of rivaroxaban was associated with a cost savings of $284 per patient and a reduction of 18 symptomatic events per 1,000 patients undergoing TKR.
A later cost-effectiveness analysis by Duran and colleagues, published after FDA approval, included U.S. pricing information.38 In patients receiving extended-duration prophylaxis (35 days) following THR, rivaroxaban was associated with a cost savings of $695 per patient compared with enoxaparin. Compared with 14 days of enoxaparin, extended-duration rivaroxaban (35 days) prevented about 10 additional symptomatic VTE events per 1,000 patients and saved $244 per patient. In patients undergoing TKR, short-duration rivaroxaban
(10-14 days) prevented about 13 additional symptomatic VTE events per 1,000 patients while saving $411 per patient compared with short-duration enoxaparin (10-14 days). It should be noted that statistically significant differences were detected only in the base-case economic analysis, and differences in PE and bleeding events were not captured.
Conclusion
The prevalence of VTE after total joint replacement continues to pose a significant burden to our health care system in terms of morbidity, mortality, and health care costs. Novel anticoagulants such as rivaroxaban, which is now FDA-approved, represent promising alternatives to the traditional agents used for VTE prophylaxis. In addition to its superior efficacy and comparable safety profile to enoxaparin, rivaroxaban’s oral route of administration and straightforward management make it a promising alternative. In particular, the lack of a requirement for routine coagulation monitoring or dose adjustment should simplify treatment with the potential to improve compliance and adherence.
Some questions remain unanswered, such as lack of a direct antidote or widely accepted reversibility technique and how to monitor or assess anticoagulation status in emergency situations, such as overdose or pathologic bleeding. Importantly, early cost-effectiveness analyses indicate that rivaroxaban is cost-effective and potentially even cost-saving compared with enoxaparin and warfarin.Careful postmarketing surveillance will need to be conducted to establish its safety in real-world settings.
Acknowledgments
The authors would like to acknowledge Matthew Romo, PharmD, who provided editorial support with funding from Janssen Scientific Affairs, LLC.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. Iorio R, Robb WJ, Healy WL, et al. Orthopaedic surgeon workforce and volume assessment for total hip and knee replacement in the United States: Preparing for an epidemic. J Bone Joint Surg Am. 2008;90(7):1598-1605.
2. Falck-Ytter Y, Francis CW, Johanson NA, et al; American College of Chest Physicians. Prevention of VTE in Orthopedic Surgery Patients: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines, 9th ed. Chest. 2012(suppl 2);141:e278S-e325S.
3. Fanikos J, Piazza G, Zayaruzny M, Goldhaber SZ. Long-term complications of medical patients with hospital-acquired venous thromboembolism. Thromb Haemost. 2009;102(4):688-693.
4. Pengo V, Lensing AW, Prins MH, et al; Thromboembolic Pulmonary Hypertension Study Group. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350(22):2257-2264.
5. Ruppert A, Lees M, Steinle T. Clinical burden of venous thromboembolism. Curr Med Res Opin. 2010;26(10):2465-2473.
6. FDA approves Xarelto® (rivaroxaban tablets) for the prophylaxis of deep vein thrombosis which may lead to a pulmonary embolism in patients undergoing knee or hip replacement surgery. BayNews.
July 1, 2011.
7. Oster G, Ollendorf DA, Vera-Llonch M, Hagiwara M, Berger A, Edelsberg J. Economic consequences of venous thromboembolism following major orthopedic surgery. Ann Pharmacother. 2004;38(3):377-382.
8. Spyropoulos AC, Lin J. Direct medical costs of venous thromboembolism and subsequent hospital readmission rates: An administrative claims analysis from 30 managed care organizations. J Manag Care Pharm. 2007;13(6):475-486.
9. Ashrani AA, Heit JA. Incidence and cost burden of post-thrombotic syndrome. J Thromb Thrombolysis. 2009;28(4):465-476.
10. MacDougall DA, Feliu AL, Boccuzzi SJ, Lin J. Economic burden of deep-vein thrombosis, pulmonary embolism, and post-thrombotic syndrome.
Am J Health Syst Pharm. 2006;63(suppl 20):S5-S15.
11. American Academy of Orthopaedic Surgeons. Preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty: evidence-based guidelines and evidence report. American Academy of Orthopaedic Surgeons Website. http://www.aaos.org/research/guidelines/VTE/VTE_full_guideline.pdf. Accessed January 29, 2014.
12. Friedman RJ, Gallus A, Gil-Garay E, Fitzgerald G, Cushner F. Practice patterns in the use of venous thromboembolism prophylaxis after total joint arthroplasty—insights from the Multinational Global Orthopaedic Registry (GLORY). Am J Orthop (Belle Mead NJ). 2010;39(suppl 9):14-21.
13. Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G; American College of Chest Physicians. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(suppl 6):160S-198S.
14. Nordstrom BL, Kachroo S, Fraeman KH, et al. Warfarin prophylaxis in patients after total knee or hip arthroplasty—international normalized ratio patterns and venous thromboembolism. Curr Med Res Opin. 2011;27(10):1973-1985.
15. Lovenox [package insert]. Bridgewater, NJ: sanofi-aventis U.S. LLC; 2013.
16. Colwell CW Jr, Pulido P, Hardwick ME, Morris BA. Patient compliance with outpatient prophylaxis: An observational study. Orthopedics. 2005;28(2):143-147.
17. Eriksson BI, Quinlan DJ, Weitz JI. Comparative pharmacodynamics and pharmacokinetics of oral direct thrombin and factor xa inhibitors in development. Clin Pharmacokinet. 2009;48(1):1-22.
18. Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Portman RJ. Apixaban or enoxaparin for thromboprophylaxis after knee replacement. N Engl J Med. 2009;361(6):594-604.
19. Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Hornick P; ADVANCE-2 investigators. Apixaban versus enoxaparin for thromboprophylaxis after knee replacement (ADVANCE-2): A randomised double-blind trial. Lancet. 2010;375(9717):807-815.
20. Lassen MR, Gallus A, Raskob GE, Pineo G, Chen D, Ramirez LM; ADVANCE-3 Investigators. Apixaban versus enoxaparin for thromboprophylaxis after hip replacement. N Engl J Med. 2010;363(26):2487-2498.
21. Eriksson BI, Dahl OE, Rosencher N, et al; RE-NOVATE Study Group. Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: A randomised, double-blind, non-inferiority trial. Lancet. 2007;370(9591):949-956.
22. Eriksson BI, Dahl OE, Huo MH, et al; RE-NOVATE II Study Group. Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE-NOVATE II*). A randomised, double-blind, non-inferiority trial. Thromb Haemost. 2011;105(4):721-729.
23. Eriksson BI, Dahl OE, Rosencher N, et al; RE-MODEL Study Group. Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: The RE-MODEL randomized trial. J Thromb Haemost. 2007;5(11):2178-2185.
24. RE-MOBILIZE Writing Committee, Ginsberg JS, Davidson BL, et al. Oral thrombin inhibitor dabigatran etexilate vs North American enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgery. J Arthroplasty. 2009;24(1):1-9.
25. Eriksson BI, Borris LC, Friedman RJ, et al; RECORD1 Study Group. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty.
N Engl J Med. 2008;358(26):2765-2775.
26. Kakkar AK, Brenner B, Dahl OE, et al; RECORD2 Investigators. Extended duration rivaroxaban versus short-term enoxaparin for the prevention of venous thromboembolism after total hip arthroplasty: A double-blind, randomised controlled trial. Lancet. 2008;372(9632):31-39.
27. Lassen MR, Ageno W, Borris LC, et al; RECORD3 Investigators. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty.
N Engl J Med. 2008;358(26):2776-2786.
28. Turpie AG, Lassen MR, Davidson BL, et al; RECORD4 Investigators. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4): A randomised trial. Lancet. 2009;373(9676):1673-1680.
29. Xarelto [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2009.
30. Cardiovascular and Renal Drugs Advisory Committee. FDA Advisory Committee Briefing Document. 2009. http://www.fda.gov/ohrms/dockets/ac/09/briefing/2009-4418b1-01-FDA.pdf. Accessed January 15, 2012.
31. Turpie AG, Lassen MR, Eriksson BI, et al. Rivaroxaban for the prevention of venous thromboembolism after hip or knee arthroplasty. Pooled analysis of four studies. Thromb Haemost. 2011;105(3):444-453.
32. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883-891.
33. Xarelto [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2011.
34. Eerenberg ES, Kamphuisen PW, Sijpkens MK, Meijers JC, Buller HR, Levi M. Reversal of rivaroxaban and dabigatran by prothrombin complex concentrate: A randomized, placebo-controlled, crossover study in healthy subjects. Circulation. 2011;124(14):1573-1579.
35. Friedman RJ, Dunsworth GA. Cost analyses of extended prophylaxis with enoxaparin after hip arthroplasty. Clin Orthop Rel Res. 2000;370:171-182.
36. Kwong LM. Cost-effectiveness of rivaroxaban after total hip or total knee arthroplasty. Am J Manag Care. 2011;17(suppl 1):S22-S26.
37. Friedman RJ, Sengupta N, Lees M. Economic impact of venous thromboembolism after hip and knee arthroplasty: Potential impact of rivaroxaban. Expert Rev Pharmacoecon Outcomes Res. 2011;11(3):299-306.
38. Duran A, Sengupta N, Diamantopoulos A, Forster F, Kwong L, Lees M. Cost and outcomes associated with rivaroxaban vs enoxaparin for the prevention of postsurgical venous thormboembolism from a US payer’s perspective. J Med Econ. 2011;14(6):824-834.
The number of total hip and knee replacement surgeries is increasing, and consequently, more patients are at risk of venous thromboembolism (VTE).1 Without thromboprophylaxis, the incidence of proximal deep vein thrombosis (DVT) is about 18% to 36% following total hip replacement (THR) and about 5% to 22% following total knee replacement (TKR). The incidence of total pulmonary embolism (PE) has been estimated at 0.9% to 28% in THR and 1.5% to 10% in TKR, and the incidence of fatal PE has been estimated to be as high as 2% following total joint replacement surgery.2 Despite the availability of effective anticoagulant agents for thromboprophylaxis, symptomatic VTE continues to occur in 1.3% to 10.0% of patients in the 3-month period following joint replacement surgery.2
VTE following THR or TKR represents a significant source of morbidity and mortality as well as a financial burden on the health care system. This burden is increased further by the complications of VTE—including a high rate of recurrence, postthrombotic syndrome (PTS), and pulmonary hypertension—which may be more debilitating than the primary event.3-5 Effective prophylaxis of VTE is paramount in reducing the incidence of these consequences.
Rivaroxaban, a Factor Xa inhibitor, is a novel anticoagulant that has recently been approved by the U.S. Food and Drug Administration (FDA) for prophylaxis of DVT in patients undergoing THR or TKR as well as for reduction of the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation (AFib).6 Clinical trials have shown that rivaroxaban is superior to enoxaparin, the standard of care, in preventing VTE after total joint replacement, and cost-effectiveness studies have demonstrated that rivaroxaban may potentially be a cost-saving agent.
This clinical review will address the economic and public health burden of VTE following THR and TKR and evaluate the novel anticoagulants that have been studied for this indication, including rivaroxaban. The safety and efficacy of rivaroxaban will be discussed, along with cost-effectiveness issues and practical management information.
The Economic Burden of VTE
VTE is the most common cause of hospital readmission following THR.2 The occurrence of VTE is reported to significantly increase the length of hospital stays and health care charges in patients undergoing TKR or THR. For example, one study reported health care charges for the index admission that were $9,297 higher for inpatients who experienced VTE compared with patients with TKR who did not have a VTE (P = .02).7 Similarly, for patients with THR, health care charges were $25,853 higher for inpatients who experienced VTE compared with patients who did not (P < .01).7
According to Spyropoulos and Lin, the total annual health care cost of a VTE (not limited to orthopedic patients) is $7,594 to $16,644, depending on the type of VTE (DVT or PE) and whether it was the primary or secondary diagnosis on discharge.8 These costs are significant, especially when multiplied by the number of THR and TKR surgeries performed in the U.S. Furthermore, VTE complications, such as PTS, represent an additional driver of health care expenditures.5,9,10
VTE Prophylaxis Guidelines
Both the American College of Chest Physicians (ACCP) and the American Academy of Orthopaedic Surgeons (AAOS) have published evidence-based guidelines for the prevention of VTE following total joint replacement.2,11 The 2012 version of the ACCP guidelines recommended the routine use of low-molecular-weight heparins (LMWHs), fondaparinux, low-dose unfractionated heparin, aspirin, adjusted-dose warfarin, rivaroxaban, apixaban, or dabigatran for thromboprophylaxis following THR or TKR. In contrast, the 2011 version of the AAOS guidelines makes no specific recommendations for pharmacologic agents.11 Despite the availability of evidence-based guidelines with specific recommendations, physician compliance with these guidelines is low.12
Before the approval of rivaroxaban, the vitamin K antagonist warfarin was the only available oral option for thromboprophylaxis following THR or TKR. The use of warfarin can be challenging, because it requires frequent monitoring and maintaining a patient within a specified international normalized ratio (INR) range. Several factors may influence time-in-therapeutic range, including drug-drug and drug-food interactions and genetic polymorphisms of vitamin K epoxide reductase complex subunit 1 (VKORC1) and cytochrome P450 (CYP)2C9.13 Warfarin does not provide short-term prophylaxis because of its delayed onset of action. It has been reported that 5 days after THR and TKR only about 30% of patients are within an INR of 2.0 to 3.0.14 Patients with an INR below 2.0 are at a 4- to 5-fold increased risk for VTE.14
Low-molecular-weight heparins, such as enoxaparin, do not require routine monitoring and have minimal drug interactions.15 The main drawback of LMWHs is their injectable mode of administration, which may influence prescribing habits and medication adherence. Patient education plays an essential role in ensuring adherence to LMWHs following orthopedic surgery.16
New Oral Anticoagulants
The new oral anticoagulants that have completed phase 3 trials for VTE prophylaxis following total joint replacement surgery include the selective Factor Xa inhibitors rivaroxaban and apixaban and the direct thrombin inhibitor dabigatran etexilate. Unlike warfarin, these agents do not require routine monitoring, a result of their predictable pharmacokinetic/pharmacodynamic (PK/PD) relationship, and they have few clinically significant drug interactions.17 Dabigatran and apixaban are not currently FDA approved for VTE prophylaxis following total joint replacement surgery; however, rivaroxaban was approved by the FDA in July 2011 for this indication.6
Apixaban
The Apixaban or Enoxaparin for Thromboprophylaxis After Knee Replacement (ADVANCE)-1 and ADVANCE-2 trials evaluated the use of Apixaban for thromboprophylaxis in patients undergoing TKR.18,19 In the ADVANCE-1 trial, patients undergoing TKR were randomized to receive either apixaban 2.5 mg orally twice daily or the North American preferred dosing of enoxaparin, 30 mg subcutaneously (SC) twice daily, with both agents started 12 to 24 hours after surgery and then taken for 10 to 14 days.18
Apixaban did not meet the prespecified statistical criteria for noninferiority compared with enoxaparin, although the rates of the primary efficacy endpoint (composite of VTE and all-cause mortality) were similar: 9.0% and 8.8% of patients, respectively. However, apixaban showed lower rates of clinically relevant bleeding and a similar adverse event (AE) profile compared with enoxaparin.
In the ADVANCE-2 trial, patients undergoing TKR received either apixaban 2.5 mg orally twice daily or enoxaparin 40 mg SC once daily for 10 to 14 days.19 The primary efficacy outcome (composite of total VTE and all-cause mortality) occurred at significantly lower rates in patients receiving apixaban (15% and 24%, respectively; relative risk [RR] 0.62; 95% confidence interval [CI] 0.51-0.74; P < .0001). Rates of major or clinically relevant nonmajor bleeding events occurred at similar rates between the 2 groups.
In the ADVANCE-3 trial, patients undergoing THR received either apixaban 2.5 orally twice daily or enoxaparin 40 mg SC once daily for 35 days.20 The primary efficacy outcome (composite of total VTE and all-cause mortality) occurred at significantly lower rates in patients receiving apixaban (1.4% and 3.9%, respectively; RR 0.36; 95% CI 0.22-0.54; P < .001). Rates of major or clinically relevant nonmajor bleeding events occurred at similar rates between both groups.
Dabigatran etexilate
Dabigatran etexilate has been evaluated in patients undergoing TKR in the Oral Dabigatran Etexilate vs Subcutaneous Enoxaparin for the Prevention of Venous Thromboembolism After Total Knee Replacement (RE-MODEL) and Oral Thrombin Inhibitor Dabigatran Etexilate vs North American Enoxaparin Regimen for Prevention of Venous Thromboembolism After Total Knee Replacement (RE-MOBILIZE) studies and in patients undergoing THR in the Oral Dabigatran vs Enoxaparin for Thromboprophylaxis After Primary Total Hip Arthroplasty (RE-NOVATE)-1 and RE-NOVATE‑2 trials.21-24
In RE-MODEL, patients undergoing TKR received either 150 mg or 220 mg of dabigatran etexilate once daily (starting with a half dose 1 to 4 hours after surgery) or enoxaparin 40 mg once daily (started the evening before surgery) for 6 to 10 days.23 Both doses of dabigatran had a similar incidence of the composite of total VTE and mortality and major bleeding. In RE-MOBILIZE, patients undergoing TKR received either 150 mg or 220 mg of dabigatran etexilate once daily or the North American regimen of enoxaparin, 30 mg SC twice daily for 12 to 15 days.24 Both dabigatran regimens had a significantly higher incidence of the composite of total VTE, failing to establish noninferiority to enoxaparin. The incidence of major bleeding was not significantly different among the 3 groups.
In RE-NOVATE I, patients undergoing THR received either dabigatran 150 mg or 220 mg twice daily, or enoxaparin 40 mg SC once daily for 28 to 35 days.21 Both doses of dabigatran had a similar incidence of the composite of total VTE and mortality and major bleeding. Because RE-NOVATE I did not include any study sites in North America, a second phase 3 trial, RE-NOVATE II, was conducted to include North American sites. RE-NOVATE II had an identical trial design to RE-NOVATE I and similar results (noninferior efficacy and comparable safety).22
Rivaroxaban
The phase 3 Rivaroxaban vs Enoxaparin for Thromboprophylaxis After Hip Arthroplasty (RECORD) program consisted of 4 double-blind randomized trials that compared the efficacy and safety of oral rivaroxaban to SC enoxaparin in THR (RECORD1 and 2) and TKR (RECORD3 and 4). The RECORD1 and 2 trials compared rivaroxaban 10 mg orally once daily for 31 to 39 days with enoxaparin 40 mg SC once daily (for 31-39 days in RECORD1 and for 10-14 days followed by placebo in RECORD2). The RECORD3 and 4 trials compared 10- to 14-day regimens of rivaroxaban 10 mg orally once daily with enoxaparin 40 mg SC once daily (RECORD3) and 30 mg twice daily (RECORD4). The 4 trials used the same efficacy and safety outcomes (Table).
In the RECORD1, 2, and 3 studies, rivaroxaban significantly reduced the composite of DVT, nonfatal PE, and all-cause mortality, as well as major VTE compared with enoxaparin. Major bleeding events as well as clinically relevant nonmajor bleeding and hemorrhagic wound complications were similar across both groups.25-27
In the RECORD4 study, rivaroxaban significantly reduced the composite of DVT, nonfatal PE, and all-cause mortality, but not major VTE, in patients undergoing TKR. Major bleeding events as well as clinically relevant nonmajor bleeding were numerically higher in the rivaroxaban group, but this was not statistically significant. Hemorrhagic wound complications were similar across both groups.28 This study was not required for approval and was not included in the final FDA-approved package insert.29
In a pooled analysis of the 4 RECORD trials presented at the FDA advisory committee, the incidence of major bleeding was significantly higher in the rivaroxaban group (24 events [0.39%]) compared with enoxaparin (13 events [0.21%]), with a nominal P value of .08 (significant at 10% nominal level) in the total treatment duration pool.30 In a pooled analysis by Turpie and colleagues who used the same data, this difference was not determined to be statistically different.31 In addition, this pooled analysis showed that the incidence of treatment-emergent hemorrhagic wound complications was similar in patients receiving rivaroxaban and enoxaparin and that fewer treatment-emergent serious AEs occurred in patients receiving rivaroxaban compared with patients receiving enoxaparin.31
In the FDA advisory committee, an “isolated signal” for a potentially increased risk of ischemic stroke was identified: In the safety population, ischemic stroke occurred in 5 patients who had received rivaroxaban and 1 patient who received enoxaparin.30 Furthermore, cardiovascular events in the safety population were concentrated around discontinuation of rivaroxaban, which was not the case for enoxaparin. The concern of stroke following rivaroxaban discontinuation was much more robust in Rivaroxaban vs Warfarin in Nonvalvular Atrial Fibrillation (ROCKET-AF), the phase 3 trial that compared rivaroxaban and warfarin for stroke prophylaxis in AFib.32 In the study ROCKET-AF, higher rates of stroke and systemic embolism were observed at the end of the trial among patients discontinuing rivaroxaban and switching to open-label warfarin compared with patients who had been taking warfarin and were transitioned to open-label warfarin. This observation led to a black box warning in the label of rivaroxaban regarding discontinuation of this agent.33
rivaroxaban management
The approved dose of rivaroxaban for the prophylaxis of VTE is 10 mg orally once daily with or without food.29 The first dose should be taken 6 to 10 hours after surgery, once hemostasis has been established. Rivaroxaban should be administered for 35 days to patients undergoing THR and for 12 days to patients undergoing TKR. Tablets may be crushed and administered in a gastric feeding tube, but they must not be administered via feeding tubes that deliver the contents into the proximal small intestine, because reduced drug absorption may result.29
The prescribing information for rivaroxaban includes a black box warning stating that epidural or spinal hematomas have occurred in patients treated with rivaroxaban who are receiving neuraxial (ie, spinal or epidural) anesthesia or undergoing spinal puncture. For such patients, the epidural catheter should not be removed earlier than 18 hours after the last administration of rivaroxaban.29 The next rivaroxaban dose should not be administered earlier than 6 hours after the catheter is removed.29 If a traumatic puncture occurs, rivaroxaban administration should be delayed for 24 hours.29 Factors that can increase the risk of developing epidural or spinal hematomas include the use of indwelling epidural catheters, concomitant use of drugs that affect hemostasis (eg, nonsteroidal anti-inflammatory drugs [NSAIDs], platelet inhibitors, and other anticoagulants), a history of traumatic or repeated epidural or spinal punctures, and a history of spinal deformity or spinal surgery.
Rivaroxaban has not been studied in severe hepatic impairment (Child-Pugh C), and in subjects with moderate hepatic impairment (Child-Pugh B), rivaroxaban has led to increased drug exposure, with increased PD effects. Therefore, rivaroxaban should be avoided in patients with moderate to severe hepatic impairment or any hepatic disease associated with coagulopathy.29
Rivaroxaban should also be avoided in patients with severe renal impairment (a creatinine clearance [CrCl] of < 30 mL/min), because increased exposure with increased PD effects is expected. A combined analysis of the RECORD1, 2, and 3 trials did not show an increased bleeding risk for patients with moderate renal impairment (CrCl 30-50 mL/min) taking rivaroxaban. However, such patients should be observed for signs or symptoms of bleeding. Discontinuation should be considered in any patient who develops acute renal failure while taking rivaroxaban.
Drug interaction studies found that the concomitant use of rivaroxaban with drugs that are combined P-glycoprotein (P-gp) and CYP3A4 inhibitors led to increased rivaroxaban exposure and PD effects (ie, Factor Xa inhibition and prolonged prothrombin time). Rivaroxaban exposure was increased significantly when the drug was administered with combined P-gp and strong CYP3A4 inhibitors (eg, azole antifungal agents and protease inhibitors). Therefore, coadministration of rivaroxaban with these agents should be avoided, particularly in patients with any degree of renal impairment, because bleeding risk may increase. In cases where a change in exposure is considered unlikely to affect bleeding risk (ie, coadministration of weaker combined P-gp and CYP3A4 inhibitors, such as clarithromycin and erythromycin), no precautions are necessary.
If bleeding occurs during treatment with rivaroxaban, it may be appropriate to temporarily discontinue the drug and start supportive care. Rivaroxaban has a relatively short half-life (5-9 hours in healthy subjects aged 20-45 years and 11-13 hours in the elderly), meaning that drug effect decreases relatively quickly compared with warfarin. There is currently no direct antidote for rivaroxaban, but a study in healthy human subjects demonstrated that administration of prothrombin complex concentrates may be a potential option.34 Absolute contraindications to rivaroxaban treatment include patients with active pathological bleeding and those with severe hypersensitivity to the drug.
RIVAROXABAN ECONOMICS
Despite its high cost, economic analyses indicate that enoxaparin is a cost-effective agent for VTE prophylaxis compared with warfarin, which is well known to be inexpensive.35 An economic analysis that took into account prophylaxis failures and treatment complications as well as the direct costs associated with medical services, drugs, and laboratory tests showed a cost advantage for enoxaparin over warfarin that lasted for a substantial amount of time (19-31 days after hospital discharge).35
An economic model that followed patients for 1 year postsurgery specifically evaluated the costs associated with symptomatic VTE and major bleeding events in the RECORD trials, assuming the cost of rivaroxaban to be similar to that of enoxaparin 40 mg.36 Cost savings for rivaroxaban over enoxaparin were $82 to $291 per patient, depending on the indication (TKR or THR) and regimen, with cost savings increasing further if the costs of home nursing or training patients to self-administer enoxaparin are included.36 This economic model was also applied to THR and TKR figures from 2005 to show the global cost-effectiveness of rivaroxaban.37 This analysis showed that based on RECORD1, the use of rivaroxaban was associated with an average cost savings of $82 per patient and a reduction of 6 symptomatic events per 1,000 patients undergoing THR. Based on RECORD3, the use of rivaroxaban was associated with a cost savings of $284 per patient and a reduction of 18 symptomatic events per 1,000 patients undergoing TKR.
A later cost-effectiveness analysis by Duran and colleagues, published after FDA approval, included U.S. pricing information.38 In patients receiving extended-duration prophylaxis (35 days) following THR, rivaroxaban was associated with a cost savings of $695 per patient compared with enoxaparin. Compared with 14 days of enoxaparin, extended-duration rivaroxaban (35 days) prevented about 10 additional symptomatic VTE events per 1,000 patients and saved $244 per patient. In patients undergoing TKR, short-duration rivaroxaban
(10-14 days) prevented about 13 additional symptomatic VTE events per 1,000 patients while saving $411 per patient compared with short-duration enoxaparin (10-14 days). It should be noted that statistically significant differences were detected only in the base-case economic analysis, and differences in PE and bleeding events were not captured.
Conclusion
The prevalence of VTE after total joint replacement continues to pose a significant burden to our health care system in terms of morbidity, mortality, and health care costs. Novel anticoagulants such as rivaroxaban, which is now FDA-approved, represent promising alternatives to the traditional agents used for VTE prophylaxis. In addition to its superior efficacy and comparable safety profile to enoxaparin, rivaroxaban’s oral route of administration and straightforward management make it a promising alternative. In particular, the lack of a requirement for routine coagulation monitoring or dose adjustment should simplify treatment with the potential to improve compliance and adherence.
Some questions remain unanswered, such as lack of a direct antidote or widely accepted reversibility technique and how to monitor or assess anticoagulation status in emergency situations, such as overdose or pathologic bleeding. Importantly, early cost-effectiveness analyses indicate that rivaroxaban is cost-effective and potentially even cost-saving compared with enoxaparin and warfarin.Careful postmarketing surveillance will need to be conducted to establish its safety in real-world settings.
Acknowledgments
The authors would like to acknowledge Matthew Romo, PharmD, who provided editorial support with funding from Janssen Scientific Affairs, LLC.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. Iorio R, Robb WJ, Healy WL, et al. Orthopaedic surgeon workforce and volume assessment for total hip and knee replacement in the United States: Preparing for an epidemic. J Bone Joint Surg Am. 2008;90(7):1598-1605.
2. Falck-Ytter Y, Francis CW, Johanson NA, et al; American College of Chest Physicians. Prevention of VTE in Orthopedic Surgery Patients: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines, 9th ed. Chest. 2012(suppl 2);141:e278S-e325S.
3. Fanikos J, Piazza G, Zayaruzny M, Goldhaber SZ. Long-term complications of medical patients with hospital-acquired venous thromboembolism. Thromb Haemost. 2009;102(4):688-693.
4. Pengo V, Lensing AW, Prins MH, et al; Thromboembolic Pulmonary Hypertension Study Group. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350(22):2257-2264.
5. Ruppert A, Lees M, Steinle T. Clinical burden of venous thromboembolism. Curr Med Res Opin. 2010;26(10):2465-2473.
6. FDA approves Xarelto® (rivaroxaban tablets) for the prophylaxis of deep vein thrombosis which may lead to a pulmonary embolism in patients undergoing knee or hip replacement surgery. BayNews.
July 1, 2011.
7. Oster G, Ollendorf DA, Vera-Llonch M, Hagiwara M, Berger A, Edelsberg J. Economic consequences of venous thromboembolism following major orthopedic surgery. Ann Pharmacother. 2004;38(3):377-382.
8. Spyropoulos AC, Lin J. Direct medical costs of venous thromboembolism and subsequent hospital readmission rates: An administrative claims analysis from 30 managed care organizations. J Manag Care Pharm. 2007;13(6):475-486.
9. Ashrani AA, Heit JA. Incidence and cost burden of post-thrombotic syndrome. J Thromb Thrombolysis. 2009;28(4):465-476.
10. MacDougall DA, Feliu AL, Boccuzzi SJ, Lin J. Economic burden of deep-vein thrombosis, pulmonary embolism, and post-thrombotic syndrome.
Am J Health Syst Pharm. 2006;63(suppl 20):S5-S15.
11. American Academy of Orthopaedic Surgeons. Preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty: evidence-based guidelines and evidence report. American Academy of Orthopaedic Surgeons Website. http://www.aaos.org/research/guidelines/VTE/VTE_full_guideline.pdf. Accessed January 29, 2014.
12. Friedman RJ, Gallus A, Gil-Garay E, Fitzgerald G, Cushner F. Practice patterns in the use of venous thromboembolism prophylaxis after total joint arthroplasty—insights from the Multinational Global Orthopaedic Registry (GLORY). Am J Orthop (Belle Mead NJ). 2010;39(suppl 9):14-21.
13. Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G; American College of Chest Physicians. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(suppl 6):160S-198S.
14. Nordstrom BL, Kachroo S, Fraeman KH, et al. Warfarin prophylaxis in patients after total knee or hip arthroplasty—international normalized ratio patterns and venous thromboembolism. Curr Med Res Opin. 2011;27(10):1973-1985.
15. Lovenox [package insert]. Bridgewater, NJ: sanofi-aventis U.S. LLC; 2013.
16. Colwell CW Jr, Pulido P, Hardwick ME, Morris BA. Patient compliance with outpatient prophylaxis: An observational study. Orthopedics. 2005;28(2):143-147.
17. Eriksson BI, Quinlan DJ, Weitz JI. Comparative pharmacodynamics and pharmacokinetics of oral direct thrombin and factor xa inhibitors in development. Clin Pharmacokinet. 2009;48(1):1-22.
18. Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Portman RJ. Apixaban or enoxaparin for thromboprophylaxis after knee replacement. N Engl J Med. 2009;361(6):594-604.
19. Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Hornick P; ADVANCE-2 investigators. Apixaban versus enoxaparin for thromboprophylaxis after knee replacement (ADVANCE-2): A randomised double-blind trial. Lancet. 2010;375(9717):807-815.
20. Lassen MR, Gallus A, Raskob GE, Pineo G, Chen D, Ramirez LM; ADVANCE-3 Investigators. Apixaban versus enoxaparin for thromboprophylaxis after hip replacement. N Engl J Med. 2010;363(26):2487-2498.
21. Eriksson BI, Dahl OE, Rosencher N, et al; RE-NOVATE Study Group. Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: A randomised, double-blind, non-inferiority trial. Lancet. 2007;370(9591):949-956.
22. Eriksson BI, Dahl OE, Huo MH, et al; RE-NOVATE II Study Group. Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE-NOVATE II*). A randomised, double-blind, non-inferiority trial. Thromb Haemost. 2011;105(4):721-729.
23. Eriksson BI, Dahl OE, Rosencher N, et al; RE-MODEL Study Group. Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: The RE-MODEL randomized trial. J Thromb Haemost. 2007;5(11):2178-2185.
24. RE-MOBILIZE Writing Committee, Ginsberg JS, Davidson BL, et al. Oral thrombin inhibitor dabigatran etexilate vs North American enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgery. J Arthroplasty. 2009;24(1):1-9.
25. Eriksson BI, Borris LC, Friedman RJ, et al; RECORD1 Study Group. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty.
N Engl J Med. 2008;358(26):2765-2775.
26. Kakkar AK, Brenner B, Dahl OE, et al; RECORD2 Investigators. Extended duration rivaroxaban versus short-term enoxaparin for the prevention of venous thromboembolism after total hip arthroplasty: A double-blind, randomised controlled trial. Lancet. 2008;372(9632):31-39.
27. Lassen MR, Ageno W, Borris LC, et al; RECORD3 Investigators. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty.
N Engl J Med. 2008;358(26):2776-2786.
28. Turpie AG, Lassen MR, Davidson BL, et al; RECORD4 Investigators. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4): A randomised trial. Lancet. 2009;373(9676):1673-1680.
29. Xarelto [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2009.
30. Cardiovascular and Renal Drugs Advisory Committee. FDA Advisory Committee Briefing Document. 2009. http://www.fda.gov/ohrms/dockets/ac/09/briefing/2009-4418b1-01-FDA.pdf. Accessed January 15, 2012.
31. Turpie AG, Lassen MR, Eriksson BI, et al. Rivaroxaban for the prevention of venous thromboembolism after hip or knee arthroplasty. Pooled analysis of four studies. Thromb Haemost. 2011;105(3):444-453.
32. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883-891.
33. Xarelto [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2011.
34. Eerenberg ES, Kamphuisen PW, Sijpkens MK, Meijers JC, Buller HR, Levi M. Reversal of rivaroxaban and dabigatran by prothrombin complex concentrate: A randomized, placebo-controlled, crossover study in healthy subjects. Circulation. 2011;124(14):1573-1579.
35. Friedman RJ, Dunsworth GA. Cost analyses of extended prophylaxis with enoxaparin after hip arthroplasty. Clin Orthop Rel Res. 2000;370:171-182.
36. Kwong LM. Cost-effectiveness of rivaroxaban after total hip or total knee arthroplasty. Am J Manag Care. 2011;17(suppl 1):S22-S26.
37. Friedman RJ, Sengupta N, Lees M. Economic impact of venous thromboembolism after hip and knee arthroplasty: Potential impact of rivaroxaban. Expert Rev Pharmacoecon Outcomes Res. 2011;11(3):299-306.
38. Duran A, Sengupta N, Diamantopoulos A, Forster F, Kwong L, Lees M. Cost and outcomes associated with rivaroxaban vs enoxaparin for the prevention of postsurgical venous thormboembolism from a US payer’s perspective. J Med Econ. 2011;14(6):824-834.
The number of total hip and knee replacement surgeries is increasing, and consequently, more patients are at risk of venous thromboembolism (VTE).1 Without thromboprophylaxis, the incidence of proximal deep vein thrombosis (DVT) is about 18% to 36% following total hip replacement (THR) and about 5% to 22% following total knee replacement (TKR). The incidence of total pulmonary embolism (PE) has been estimated at 0.9% to 28% in THR and 1.5% to 10% in TKR, and the incidence of fatal PE has been estimated to be as high as 2% following total joint replacement surgery.2 Despite the availability of effective anticoagulant agents for thromboprophylaxis, symptomatic VTE continues to occur in 1.3% to 10.0% of patients in the 3-month period following joint replacement surgery.2
VTE following THR or TKR represents a significant source of morbidity and mortality as well as a financial burden on the health care system. This burden is increased further by the complications of VTE—including a high rate of recurrence, postthrombotic syndrome (PTS), and pulmonary hypertension—which may be more debilitating than the primary event.3-5 Effective prophylaxis of VTE is paramount in reducing the incidence of these consequences.
Rivaroxaban, a Factor Xa inhibitor, is a novel anticoagulant that has recently been approved by the U.S. Food and Drug Administration (FDA) for prophylaxis of DVT in patients undergoing THR or TKR as well as for reduction of the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation (AFib).6 Clinical trials have shown that rivaroxaban is superior to enoxaparin, the standard of care, in preventing VTE after total joint replacement, and cost-effectiveness studies have demonstrated that rivaroxaban may potentially be a cost-saving agent.
This clinical review will address the economic and public health burden of VTE following THR and TKR and evaluate the novel anticoagulants that have been studied for this indication, including rivaroxaban. The safety and efficacy of rivaroxaban will be discussed, along with cost-effectiveness issues and practical management information.
The Economic Burden of VTE
VTE is the most common cause of hospital readmission following THR.2 The occurrence of VTE is reported to significantly increase the length of hospital stays and health care charges in patients undergoing TKR or THR. For example, one study reported health care charges for the index admission that were $9,297 higher for inpatients who experienced VTE compared with patients with TKR who did not have a VTE (P = .02).7 Similarly, for patients with THR, health care charges were $25,853 higher for inpatients who experienced VTE compared with patients who did not (P < .01).7
According to Spyropoulos and Lin, the total annual health care cost of a VTE (not limited to orthopedic patients) is $7,594 to $16,644, depending on the type of VTE (DVT or PE) and whether it was the primary or secondary diagnosis on discharge.8 These costs are significant, especially when multiplied by the number of THR and TKR surgeries performed in the U.S. Furthermore, VTE complications, such as PTS, represent an additional driver of health care expenditures.5,9,10
VTE Prophylaxis Guidelines
Both the American College of Chest Physicians (ACCP) and the American Academy of Orthopaedic Surgeons (AAOS) have published evidence-based guidelines for the prevention of VTE following total joint replacement.2,11 The 2012 version of the ACCP guidelines recommended the routine use of low-molecular-weight heparins (LMWHs), fondaparinux, low-dose unfractionated heparin, aspirin, adjusted-dose warfarin, rivaroxaban, apixaban, or dabigatran for thromboprophylaxis following THR or TKR. In contrast, the 2011 version of the AAOS guidelines makes no specific recommendations for pharmacologic agents.11 Despite the availability of evidence-based guidelines with specific recommendations, physician compliance with these guidelines is low.12
Before the approval of rivaroxaban, the vitamin K antagonist warfarin was the only available oral option for thromboprophylaxis following THR or TKR. The use of warfarin can be challenging, because it requires frequent monitoring and maintaining a patient within a specified international normalized ratio (INR) range. Several factors may influence time-in-therapeutic range, including drug-drug and drug-food interactions and genetic polymorphisms of vitamin K epoxide reductase complex subunit 1 (VKORC1) and cytochrome P450 (CYP)2C9.13 Warfarin does not provide short-term prophylaxis because of its delayed onset of action. It has been reported that 5 days after THR and TKR only about 30% of patients are within an INR of 2.0 to 3.0.14 Patients with an INR below 2.0 are at a 4- to 5-fold increased risk for VTE.14
Low-molecular-weight heparins, such as enoxaparin, do not require routine monitoring and have minimal drug interactions.15 The main drawback of LMWHs is their injectable mode of administration, which may influence prescribing habits and medication adherence. Patient education plays an essential role in ensuring adherence to LMWHs following orthopedic surgery.16
New Oral Anticoagulants
The new oral anticoagulants that have completed phase 3 trials for VTE prophylaxis following total joint replacement surgery include the selective Factor Xa inhibitors rivaroxaban and apixaban and the direct thrombin inhibitor dabigatran etexilate. Unlike warfarin, these agents do not require routine monitoring, a result of their predictable pharmacokinetic/pharmacodynamic (PK/PD) relationship, and they have few clinically significant drug interactions.17 Dabigatran and apixaban are not currently FDA approved for VTE prophylaxis following total joint replacement surgery; however, rivaroxaban was approved by the FDA in July 2011 for this indication.6
Apixaban
The Apixaban or Enoxaparin for Thromboprophylaxis After Knee Replacement (ADVANCE)-1 and ADVANCE-2 trials evaluated the use of Apixaban for thromboprophylaxis in patients undergoing TKR.18,19 In the ADVANCE-1 trial, patients undergoing TKR were randomized to receive either apixaban 2.5 mg orally twice daily or the North American preferred dosing of enoxaparin, 30 mg subcutaneously (SC) twice daily, with both agents started 12 to 24 hours after surgery and then taken for 10 to 14 days.18
Apixaban did not meet the prespecified statistical criteria for noninferiority compared with enoxaparin, although the rates of the primary efficacy endpoint (composite of VTE and all-cause mortality) were similar: 9.0% and 8.8% of patients, respectively. However, apixaban showed lower rates of clinically relevant bleeding and a similar adverse event (AE) profile compared with enoxaparin.
In the ADVANCE-2 trial, patients undergoing TKR received either apixaban 2.5 mg orally twice daily or enoxaparin 40 mg SC once daily for 10 to 14 days.19 The primary efficacy outcome (composite of total VTE and all-cause mortality) occurred at significantly lower rates in patients receiving apixaban (15% and 24%, respectively; relative risk [RR] 0.62; 95% confidence interval [CI] 0.51-0.74; P < .0001). Rates of major or clinically relevant nonmajor bleeding events occurred at similar rates between the 2 groups.
In the ADVANCE-3 trial, patients undergoing THR received either apixaban 2.5 orally twice daily or enoxaparin 40 mg SC once daily for 35 days.20 The primary efficacy outcome (composite of total VTE and all-cause mortality) occurred at significantly lower rates in patients receiving apixaban (1.4% and 3.9%, respectively; RR 0.36; 95% CI 0.22-0.54; P < .001). Rates of major or clinically relevant nonmajor bleeding events occurred at similar rates between both groups.
Dabigatran etexilate
Dabigatran etexilate has been evaluated in patients undergoing TKR in the Oral Dabigatran Etexilate vs Subcutaneous Enoxaparin for the Prevention of Venous Thromboembolism After Total Knee Replacement (RE-MODEL) and Oral Thrombin Inhibitor Dabigatran Etexilate vs North American Enoxaparin Regimen for Prevention of Venous Thromboembolism After Total Knee Replacement (RE-MOBILIZE) studies and in patients undergoing THR in the Oral Dabigatran vs Enoxaparin for Thromboprophylaxis After Primary Total Hip Arthroplasty (RE-NOVATE)-1 and RE-NOVATE‑2 trials.21-24
In RE-MODEL, patients undergoing TKR received either 150 mg or 220 mg of dabigatran etexilate once daily (starting with a half dose 1 to 4 hours after surgery) or enoxaparin 40 mg once daily (started the evening before surgery) for 6 to 10 days.23 Both doses of dabigatran had a similar incidence of the composite of total VTE and mortality and major bleeding. In RE-MOBILIZE, patients undergoing TKR received either 150 mg or 220 mg of dabigatran etexilate once daily or the North American regimen of enoxaparin, 30 mg SC twice daily for 12 to 15 days.24 Both dabigatran regimens had a significantly higher incidence of the composite of total VTE, failing to establish noninferiority to enoxaparin. The incidence of major bleeding was not significantly different among the 3 groups.
In RE-NOVATE I, patients undergoing THR received either dabigatran 150 mg or 220 mg twice daily, or enoxaparin 40 mg SC once daily for 28 to 35 days.21 Both doses of dabigatran had a similar incidence of the composite of total VTE and mortality and major bleeding. Because RE-NOVATE I did not include any study sites in North America, a second phase 3 trial, RE-NOVATE II, was conducted to include North American sites. RE-NOVATE II had an identical trial design to RE-NOVATE I and similar results (noninferior efficacy and comparable safety).22
Rivaroxaban
The phase 3 Rivaroxaban vs Enoxaparin for Thromboprophylaxis After Hip Arthroplasty (RECORD) program consisted of 4 double-blind randomized trials that compared the efficacy and safety of oral rivaroxaban to SC enoxaparin in THR (RECORD1 and 2) and TKR (RECORD3 and 4). The RECORD1 and 2 trials compared rivaroxaban 10 mg orally once daily for 31 to 39 days with enoxaparin 40 mg SC once daily (for 31-39 days in RECORD1 and for 10-14 days followed by placebo in RECORD2). The RECORD3 and 4 trials compared 10- to 14-day regimens of rivaroxaban 10 mg orally once daily with enoxaparin 40 mg SC once daily (RECORD3) and 30 mg twice daily (RECORD4). The 4 trials used the same efficacy and safety outcomes (Table).
In the RECORD1, 2, and 3 studies, rivaroxaban significantly reduced the composite of DVT, nonfatal PE, and all-cause mortality, as well as major VTE compared with enoxaparin. Major bleeding events as well as clinically relevant nonmajor bleeding and hemorrhagic wound complications were similar across both groups.25-27
In the RECORD4 study, rivaroxaban significantly reduced the composite of DVT, nonfatal PE, and all-cause mortality, but not major VTE, in patients undergoing TKR. Major bleeding events as well as clinically relevant nonmajor bleeding were numerically higher in the rivaroxaban group, but this was not statistically significant. Hemorrhagic wound complications were similar across both groups.28 This study was not required for approval and was not included in the final FDA-approved package insert.29
In a pooled analysis of the 4 RECORD trials presented at the FDA advisory committee, the incidence of major bleeding was significantly higher in the rivaroxaban group (24 events [0.39%]) compared with enoxaparin (13 events [0.21%]), with a nominal P value of .08 (significant at 10% nominal level) in the total treatment duration pool.30 In a pooled analysis by Turpie and colleagues who used the same data, this difference was not determined to be statistically different.31 In addition, this pooled analysis showed that the incidence of treatment-emergent hemorrhagic wound complications was similar in patients receiving rivaroxaban and enoxaparin and that fewer treatment-emergent serious AEs occurred in patients receiving rivaroxaban compared with patients receiving enoxaparin.31
In the FDA advisory committee, an “isolated signal” for a potentially increased risk of ischemic stroke was identified: In the safety population, ischemic stroke occurred in 5 patients who had received rivaroxaban and 1 patient who received enoxaparin.30 Furthermore, cardiovascular events in the safety population were concentrated around discontinuation of rivaroxaban, which was not the case for enoxaparin. The concern of stroke following rivaroxaban discontinuation was much more robust in Rivaroxaban vs Warfarin in Nonvalvular Atrial Fibrillation (ROCKET-AF), the phase 3 trial that compared rivaroxaban and warfarin for stroke prophylaxis in AFib.32 In the study ROCKET-AF, higher rates of stroke and systemic embolism were observed at the end of the trial among patients discontinuing rivaroxaban and switching to open-label warfarin compared with patients who had been taking warfarin and were transitioned to open-label warfarin. This observation led to a black box warning in the label of rivaroxaban regarding discontinuation of this agent.33
rivaroxaban management
The approved dose of rivaroxaban for the prophylaxis of VTE is 10 mg orally once daily with or without food.29 The first dose should be taken 6 to 10 hours after surgery, once hemostasis has been established. Rivaroxaban should be administered for 35 days to patients undergoing THR and for 12 days to patients undergoing TKR. Tablets may be crushed and administered in a gastric feeding tube, but they must not be administered via feeding tubes that deliver the contents into the proximal small intestine, because reduced drug absorption may result.29
The prescribing information for rivaroxaban includes a black box warning stating that epidural or spinal hematomas have occurred in patients treated with rivaroxaban who are receiving neuraxial (ie, spinal or epidural) anesthesia or undergoing spinal puncture. For such patients, the epidural catheter should not be removed earlier than 18 hours after the last administration of rivaroxaban.29 The next rivaroxaban dose should not be administered earlier than 6 hours after the catheter is removed.29 If a traumatic puncture occurs, rivaroxaban administration should be delayed for 24 hours.29 Factors that can increase the risk of developing epidural or spinal hematomas include the use of indwelling epidural catheters, concomitant use of drugs that affect hemostasis (eg, nonsteroidal anti-inflammatory drugs [NSAIDs], platelet inhibitors, and other anticoagulants), a history of traumatic or repeated epidural or spinal punctures, and a history of spinal deformity or spinal surgery.
Rivaroxaban has not been studied in severe hepatic impairment (Child-Pugh C), and in subjects with moderate hepatic impairment (Child-Pugh B), rivaroxaban has led to increased drug exposure, with increased PD effects. Therefore, rivaroxaban should be avoided in patients with moderate to severe hepatic impairment or any hepatic disease associated with coagulopathy.29
Rivaroxaban should also be avoided in patients with severe renal impairment (a creatinine clearance [CrCl] of < 30 mL/min), because increased exposure with increased PD effects is expected. A combined analysis of the RECORD1, 2, and 3 trials did not show an increased bleeding risk for patients with moderate renal impairment (CrCl 30-50 mL/min) taking rivaroxaban. However, such patients should be observed for signs or symptoms of bleeding. Discontinuation should be considered in any patient who develops acute renal failure while taking rivaroxaban.
Drug interaction studies found that the concomitant use of rivaroxaban with drugs that are combined P-glycoprotein (P-gp) and CYP3A4 inhibitors led to increased rivaroxaban exposure and PD effects (ie, Factor Xa inhibition and prolonged prothrombin time). Rivaroxaban exposure was increased significantly when the drug was administered with combined P-gp and strong CYP3A4 inhibitors (eg, azole antifungal agents and protease inhibitors). Therefore, coadministration of rivaroxaban with these agents should be avoided, particularly in patients with any degree of renal impairment, because bleeding risk may increase. In cases where a change in exposure is considered unlikely to affect bleeding risk (ie, coadministration of weaker combined P-gp and CYP3A4 inhibitors, such as clarithromycin and erythromycin), no precautions are necessary.
If bleeding occurs during treatment with rivaroxaban, it may be appropriate to temporarily discontinue the drug and start supportive care. Rivaroxaban has a relatively short half-life (5-9 hours in healthy subjects aged 20-45 years and 11-13 hours in the elderly), meaning that drug effect decreases relatively quickly compared with warfarin. There is currently no direct antidote for rivaroxaban, but a study in healthy human subjects demonstrated that administration of prothrombin complex concentrates may be a potential option.34 Absolute contraindications to rivaroxaban treatment include patients with active pathological bleeding and those with severe hypersensitivity to the drug.
RIVAROXABAN ECONOMICS
Despite its high cost, economic analyses indicate that enoxaparin is a cost-effective agent for VTE prophylaxis compared with warfarin, which is well known to be inexpensive.35 An economic analysis that took into account prophylaxis failures and treatment complications as well as the direct costs associated with medical services, drugs, and laboratory tests showed a cost advantage for enoxaparin over warfarin that lasted for a substantial amount of time (19-31 days after hospital discharge).35
An economic model that followed patients for 1 year postsurgery specifically evaluated the costs associated with symptomatic VTE and major bleeding events in the RECORD trials, assuming the cost of rivaroxaban to be similar to that of enoxaparin 40 mg.36 Cost savings for rivaroxaban over enoxaparin were $82 to $291 per patient, depending on the indication (TKR or THR) and regimen, with cost savings increasing further if the costs of home nursing or training patients to self-administer enoxaparin are included.36 This economic model was also applied to THR and TKR figures from 2005 to show the global cost-effectiveness of rivaroxaban.37 This analysis showed that based on RECORD1, the use of rivaroxaban was associated with an average cost savings of $82 per patient and a reduction of 6 symptomatic events per 1,000 patients undergoing THR. Based on RECORD3, the use of rivaroxaban was associated with a cost savings of $284 per patient and a reduction of 18 symptomatic events per 1,000 patients undergoing TKR.
A later cost-effectiveness analysis by Duran and colleagues, published after FDA approval, included U.S. pricing information.38 In patients receiving extended-duration prophylaxis (35 days) following THR, rivaroxaban was associated with a cost savings of $695 per patient compared with enoxaparin. Compared with 14 days of enoxaparin, extended-duration rivaroxaban (35 days) prevented about 10 additional symptomatic VTE events per 1,000 patients and saved $244 per patient. In patients undergoing TKR, short-duration rivaroxaban
(10-14 days) prevented about 13 additional symptomatic VTE events per 1,000 patients while saving $411 per patient compared with short-duration enoxaparin (10-14 days). It should be noted that statistically significant differences were detected only in the base-case economic analysis, and differences in PE and bleeding events were not captured.
Conclusion
The prevalence of VTE after total joint replacement continues to pose a significant burden to our health care system in terms of morbidity, mortality, and health care costs. Novel anticoagulants such as rivaroxaban, which is now FDA-approved, represent promising alternatives to the traditional agents used for VTE prophylaxis. In addition to its superior efficacy and comparable safety profile to enoxaparin, rivaroxaban’s oral route of administration and straightforward management make it a promising alternative. In particular, the lack of a requirement for routine coagulation monitoring or dose adjustment should simplify treatment with the potential to improve compliance and adherence.
Some questions remain unanswered, such as lack of a direct antidote or widely accepted reversibility technique and how to monitor or assess anticoagulation status in emergency situations, such as overdose or pathologic bleeding. Importantly, early cost-effectiveness analyses indicate that rivaroxaban is cost-effective and potentially even cost-saving compared with enoxaparin and warfarin.Careful postmarketing surveillance will need to be conducted to establish its safety in real-world settings.
Acknowledgments
The authors would like to acknowledge Matthew Romo, PharmD, who provided editorial support with funding from Janssen Scientific Affairs, LLC.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. Iorio R, Robb WJ, Healy WL, et al. Orthopaedic surgeon workforce and volume assessment for total hip and knee replacement in the United States: Preparing for an epidemic. J Bone Joint Surg Am. 2008;90(7):1598-1605.
2. Falck-Ytter Y, Francis CW, Johanson NA, et al; American College of Chest Physicians. Prevention of VTE in Orthopedic Surgery Patients: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines, 9th ed. Chest. 2012(suppl 2);141:e278S-e325S.
3. Fanikos J, Piazza G, Zayaruzny M, Goldhaber SZ. Long-term complications of medical patients with hospital-acquired venous thromboembolism. Thromb Haemost. 2009;102(4):688-693.
4. Pengo V, Lensing AW, Prins MH, et al; Thromboembolic Pulmonary Hypertension Study Group. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350(22):2257-2264.
5. Ruppert A, Lees M, Steinle T. Clinical burden of venous thromboembolism. Curr Med Res Opin. 2010;26(10):2465-2473.
6. FDA approves Xarelto® (rivaroxaban tablets) for the prophylaxis of deep vein thrombosis which may lead to a pulmonary embolism in patients undergoing knee or hip replacement surgery. BayNews.
July 1, 2011.
7. Oster G, Ollendorf DA, Vera-Llonch M, Hagiwara M, Berger A, Edelsberg J. Economic consequences of venous thromboembolism following major orthopedic surgery. Ann Pharmacother. 2004;38(3):377-382.
8. Spyropoulos AC, Lin J. Direct medical costs of venous thromboembolism and subsequent hospital readmission rates: An administrative claims analysis from 30 managed care organizations. J Manag Care Pharm. 2007;13(6):475-486.
9. Ashrani AA, Heit JA. Incidence and cost burden of post-thrombotic syndrome. J Thromb Thrombolysis. 2009;28(4):465-476.
10. MacDougall DA, Feliu AL, Boccuzzi SJ, Lin J. Economic burden of deep-vein thrombosis, pulmonary embolism, and post-thrombotic syndrome.
Am J Health Syst Pharm. 2006;63(suppl 20):S5-S15.
11. American Academy of Orthopaedic Surgeons. Preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty: evidence-based guidelines and evidence report. American Academy of Orthopaedic Surgeons Website. http://www.aaos.org/research/guidelines/VTE/VTE_full_guideline.pdf. Accessed January 29, 2014.
12. Friedman RJ, Gallus A, Gil-Garay E, Fitzgerald G, Cushner F. Practice patterns in the use of venous thromboembolism prophylaxis after total joint arthroplasty—insights from the Multinational Global Orthopaedic Registry (GLORY). Am J Orthop (Belle Mead NJ). 2010;39(suppl 9):14-21.
13. Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G; American College of Chest Physicians. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(suppl 6):160S-198S.
14. Nordstrom BL, Kachroo S, Fraeman KH, et al. Warfarin prophylaxis in patients after total knee or hip arthroplasty—international normalized ratio patterns and venous thromboembolism. Curr Med Res Opin. 2011;27(10):1973-1985.
15. Lovenox [package insert]. Bridgewater, NJ: sanofi-aventis U.S. LLC; 2013.
16. Colwell CW Jr, Pulido P, Hardwick ME, Morris BA. Patient compliance with outpatient prophylaxis: An observational study. Orthopedics. 2005;28(2):143-147.
17. Eriksson BI, Quinlan DJ, Weitz JI. Comparative pharmacodynamics and pharmacokinetics of oral direct thrombin and factor xa inhibitors in development. Clin Pharmacokinet. 2009;48(1):1-22.
18. Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Portman RJ. Apixaban or enoxaparin for thromboprophylaxis after knee replacement. N Engl J Med. 2009;361(6):594-604.
19. Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Hornick P; ADVANCE-2 investigators. Apixaban versus enoxaparin for thromboprophylaxis after knee replacement (ADVANCE-2): A randomised double-blind trial. Lancet. 2010;375(9717):807-815.
20. Lassen MR, Gallus A, Raskob GE, Pineo G, Chen D, Ramirez LM; ADVANCE-3 Investigators. Apixaban versus enoxaparin for thromboprophylaxis after hip replacement. N Engl J Med. 2010;363(26):2487-2498.
21. Eriksson BI, Dahl OE, Rosencher N, et al; RE-NOVATE Study Group. Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: A randomised, double-blind, non-inferiority trial. Lancet. 2007;370(9591):949-956.
22. Eriksson BI, Dahl OE, Huo MH, et al; RE-NOVATE II Study Group. Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE-NOVATE II*). A randomised, double-blind, non-inferiority trial. Thromb Haemost. 2011;105(4):721-729.
23. Eriksson BI, Dahl OE, Rosencher N, et al; RE-MODEL Study Group. Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: The RE-MODEL randomized trial. J Thromb Haemost. 2007;5(11):2178-2185.
24. RE-MOBILIZE Writing Committee, Ginsberg JS, Davidson BL, et al. Oral thrombin inhibitor dabigatran etexilate vs North American enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgery. J Arthroplasty. 2009;24(1):1-9.
25. Eriksson BI, Borris LC, Friedman RJ, et al; RECORD1 Study Group. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty.
N Engl J Med. 2008;358(26):2765-2775.
26. Kakkar AK, Brenner B, Dahl OE, et al; RECORD2 Investigators. Extended duration rivaroxaban versus short-term enoxaparin for the prevention of venous thromboembolism after total hip arthroplasty: A double-blind, randomised controlled trial. Lancet. 2008;372(9632):31-39.
27. Lassen MR, Ageno W, Borris LC, et al; RECORD3 Investigators. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty.
N Engl J Med. 2008;358(26):2776-2786.
28. Turpie AG, Lassen MR, Davidson BL, et al; RECORD4 Investigators. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4): A randomised trial. Lancet. 2009;373(9676):1673-1680.
29. Xarelto [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2009.
30. Cardiovascular and Renal Drugs Advisory Committee. FDA Advisory Committee Briefing Document. 2009. http://www.fda.gov/ohrms/dockets/ac/09/briefing/2009-4418b1-01-FDA.pdf. Accessed January 15, 2012.
31. Turpie AG, Lassen MR, Eriksson BI, et al. Rivaroxaban for the prevention of venous thromboembolism after hip or knee arthroplasty. Pooled analysis of four studies. Thromb Haemost. 2011;105(3):444-453.
32. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883-891.
33. Xarelto [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2011.
34. Eerenberg ES, Kamphuisen PW, Sijpkens MK, Meijers JC, Buller HR, Levi M. Reversal of rivaroxaban and dabigatran by prothrombin complex concentrate: A randomized, placebo-controlled, crossover study in healthy subjects. Circulation. 2011;124(14):1573-1579.
35. Friedman RJ, Dunsworth GA. Cost analyses of extended prophylaxis with enoxaparin after hip arthroplasty. Clin Orthop Rel Res. 2000;370:171-182.
36. Kwong LM. Cost-effectiveness of rivaroxaban after total hip or total knee arthroplasty. Am J Manag Care. 2011;17(suppl 1):S22-S26.
37. Friedman RJ, Sengupta N, Lees M. Economic impact of venous thromboembolism after hip and knee arthroplasty: Potential impact of rivaroxaban. Expert Rev Pharmacoecon Outcomes Res. 2011;11(3):299-306.
38. Duran A, Sengupta N, Diamantopoulos A, Forster F, Kwong L, Lees M. Cost and outcomes associated with rivaroxaban vs enoxaparin for the prevention of postsurgical venous thormboembolism from a US payer’s perspective. J Med Econ. 2011;14(6):824-834.