User login
This conflict between state and federal law has been the subject of considerable discussion in the professional literature and popular media, even reaching the Supreme Court.3,4 Much less attention has been paid to the parallel, but in some ways even more complicated, ethical, legal, and policy dilemmas facing administrators and practitioners in the Veterans Health Administration (VHA). Federal law governs VA health care facilities and clinical practice, yet there are VA hospitals and clinics in every state that have passed medical marijuana legislation, and veterans are eligible to obtain medical marijuana as residents of their respective states.
This article examines the evolution of VA policy regarding the use of medical marijuana within the confines of federal law and the nature of the VA as a beneficiary system with a mission to provide comprehensive health care to veterans and the legal, clinical, and ethical issues these often opposing obligations present to VA practitioners.
Completion of State Medical Marijuana Forms
In 2008, the VA Office of the General Counsel (OGC) issued to VA physicians the first official directions regarding state medical marijuana programs.5 The ruling of the VA OGC pertained to state medical marijuana registration forms and was addressed to the Under Secretary for Health. The VHA had requested guidance on how VA staff should respond when patients ask them to fill out state forms used to access medical marijuana; specifically, whether VA physicians are permitted or required to complete state medical marijuana registration forms.
The VA OGC was further asked to address the legal issues involved when a VA physician is requested to complete such a form and whether completion of such a form could result in criminal action or other penalties against the physician.
The opinion of the VA OGC issued in a memorandum on May 21, 2008, held that “VA should not authorize the completion of forms seeking recommendation or opinions regarding participation in such a program. Applicable statutes and regulations do not require VA physicians to complete such forms.”5 In response to the first question posed, the VA OGC identified the legal issues involved in the completion of the forms, arguing that the CSA designated marijuana as a Schedule 1 drug, meaning it had no accepted medical use but does have high potential for abuse. The Schedule 1 classification carried with it penalties for the dispensing, manufacturing, distributing, and possession of marijuana that were the responsibility of the Drug Enforcement Agency (DEA) to enforce.
In response to the second question, the VA OGC held that if a VA physician did complete a form permitting a patient to participate in a state medical marijuana program, this could result in DEA action, including revocation of the physician’s registration to prescribe controlled substances, as well as possible criminal charges.6 The VA OGC cited several landmark medical marijuana cases as the background to its issued opinion.
The first case cited in the VA OGC’s opinion was Pearson v McCaffrey, a 2001 ruling pertaining to the U.S. District Court of the District of Columbia.7 Barry McCaffrey, then-director of the Office of National Drug Control Policy, Donna Shalala, the secretary for the U.S. Department of Health and Human Services, and Janet Reno, attorney general, promulgated a policy that allowed the federal government to prosecute or revoke the controlled substance registration of any physician who prescribed or, more relevant to the VA situation, recommended medical marijuana to patients.
Physicians and patients in states with medical marijuana laws sought an injunction against the federal government prohibiting them from initiating civil, criminal, or administrative actions against physicians who recommended and prescribed or patients who obtained and used medical marijuana. The court refused to enforce the injunction the plaintiffs filed against the policy, finding that the federal position did not violate the First Amendment rights of the plaintiffs and, more pertinent, that Congress did have the authority under the Commerce Clause to regulate medical marijuana as a matter of public health and safety.7
Article 1, section 8, clause 3 of the U.S. Constitution grants that the U.S. Congress has the authority “To regulate Commerce with foreign Nations, and among the several states, and with the Indian tribes.”8 The Commerce Clause is often at issue in cases where the scope of federal power toward the states is challenged. The Commerce Clause is especially relevant to the legal status of state medical marijuana laws examined here because it is cited as the legal authority for the CSA, and the CSA governs practitioner prescribing.9
At the same time, an injunction against enforcement was filed in the District Court for the Northern District of California. A group of patients and physicians again initiated the legal action; this time, they were successful in obtaining a permanent injunction of the policy: The court prohibited the federal government from revoking the controlled substance registration or investigating any physician who recommended medical marijuana on the basis of a sincere medical judgment. The Supreme Court declined to hear the case.10
The U.S. Supreme Court did accept the third case, Gonzales v Raich, which did not address whether the individual physician would be prosecuted for recommending a state medical marijuana program but instead whether the federal government possessed the authority under the Commerce Clause to regulate intrastate use of marijuana for medical purposes, including revoking physicians’ controlled substance licenses.
The facts of the Raich case and legal background leading to the Supreme Court decision are as follows: In 1996, California voters passed the Compassionate Use Act, making California the first state in the country to legalize the medical use of marijuana. The law conflicted with the classification of marijuana as a Schedule 1 drug. This conflict between state and federal law rendered the case highly relevant to the question of VA physicians’ completion of medical marijuana forms for patients in states where medical marijuana is legal. The DEA had acted in California, not against a physician’s prescribing authority but against a patient, Angel Raich, for possession of medical marijuana. The DEA agents confiscated the medical marijuana from the patient’s home. In response, a group of medical marijuana users sued the DEA and California Attorney General Roberto Gonzales in federal district court.11
Raich’s attorneys argued that the constitutional basis of the federal government’s power to regulate interstate commerce, which formed the legal claim of the CSA, overreached Congress’s Commerce Clause powers. The district court ruled in favor of the attorney general, but the Ninth Circuit Court of Appeals reversed the decision, ruling that the application of the CSA to the intrastate transactions involved in California’s medical marijuana program was unconstitutional. The Ninth Circuit Court ruling cited 2 important prior cases not involving medical marijuana that also limited the Commerce Clause, although not with reference to marijuana: U.S. v Lopez in 1995 and U.S. v Morrison in 2000.12,13
The Supreme Court agreed to hear the case in June 2004 and in a 6-3 decision ruled that the application of the CSA to intrastate cultivation and possession of marijuana for medical use does not exceed Congress’s power under the Commerce Clause. Supreme Court Justice John Paul Stevens wrote the majority opinion, arguing that the power of the Commerce Clause did extend to the regulation of a “class of activities” that had a substantial effect on interstate commerce. Because marijuana use, even for medical purposes, confined to a local area, such as a state, materially affected the supply and demand market for marijuana in the nation, the regulation of state use of marijuana was required to govern the interstate traffic of marijuana.11
The VA OGC opinion referenced these cases in its analysis of the question VHA providers raised regarding the completion of state medical marijuana forms, particularly those in states such as Colorado and New Mexico where completing forms is not equivalent to providing a prescription yet does constitute a medical recommendation for the use of marijuana.14 The OGC noted that recommendation is not a term of art contained within the CSA and that Pearson ruled that there was no salient distinction between a prescription and a recommendation, where a recommendation was necessary for a patient to be able to obtain medical marijuana, which is the requirement in most states.5
The VA OGC concluded, “While some states may provide for the use of medical marijuana, such programs are in violation of federal law.”5 In formulating its judgment, the VA OGC cited the Supremacy Clause as the key to all subsequent VHA directives regarding medical marijuana. “The Supremacy Clause is the most important guarantor of national union. It assures that the Constitution and federal laws and treaties take precedence over state law and binds all judges to adhere to that principle in their courts.”8
Quoting an informal communication from the Department of Justice (DOJ), the VA OGC warned that the DOJ “may seek civil or criminal penalties for federal physicians and practitioners who completed forms that either recommend the use of medical marijuana or forms that describe the patient’s physical condition in order to facilitate the patient’s procurement of medical marijuana pursuant to state law.”5
Local vs Federal Policy
By 2009, 15 states had passed legislation allowing the medical use of marijuana. Many VA hospitals and clinics continued to regard marijuana, whether prescribed or not, as an illicit drug that violated opioid contracts or agreements. The clinical justification for these denials or other treatment plan modifications was to ensure that veterans used marijuana safely, for example, through detecting and preventing drug interactions or impairment of driving ability.
A group called Veterans for Medical Marijuana Access, founded by veteran Michael Krawitz, was the most politically active among veterans’ organizations on the issue of medical marijuana. Astutely, Mr. Krawitz and other advocates did not aim to change federal law and the Supremacy Clause or the court’s interpretations of the Commerce Clause as it applied to medical marijuana. Instead, their strategy was to expand veterans’ access to state programs, and their tactic was to work directly with the VA to formulate a policy. Mr. Krawitz adroitly used the media to champion his cause.
On March 5, 2010, Krawitz received a letter from Col. Will A. Gunn of the VA OGC. Mr. Krawitz had written the VA OGC regarding the inequities in VA policy regarding the provision of opioid medications for pain management to veterans enrolled in state medical marijuana programs. Mr. Krawitz informed Col. Gunn that the directors of some facilities had issued policies explicitly stating that veterans who provide medical marijuana registration in accordance with state programs and who tested positive for the drug would not be considered in violation of opioid contracts. Mr. Krawitz asked for official confirmation that these local policies were valid. On July 6, 2010, Under Secretary for Health Dr. Robert Petzel wrote Mr. Krawitz a memorandum stating, “If a veteran obtains and uses medical marijuana in a manner consistent with state law, testing positive for marijuana would not preclude the veteran from receiving opioids for pain management in a Department of Veterans Affairs facility.”
Dr. Petzel also outlined what would become the clinical ethics principles VA would employ to manage the federal-state law conflict regarding medical marijuana. First, a patient must inform his provider of medical marijuana use to ensure safety. Second, opioid agreements must make a clear distinction between illegal drugs, including the recreational use of marijuana, and medical marijuana. Third, the practitioner has the discretion to make the opioid prescribing decision and must make that decision on clinical grounds. Fourth, the prescribing decision should be made on a case-by-case basis “based upon the provider’s judgment and the needs of the patient.”
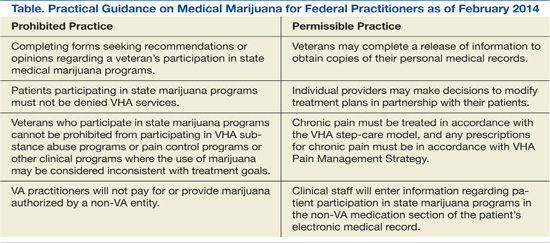
Following these letters was a highly publicized article in The New York Times in which Principal Deputy Under Secretary for Health Dr. Robert L. Jesse confirmed the new policy.15 The article included comments from Mr. Krawitz on the change in VA’s approach to medical marijuana. The VHA codified these less formal communications in VHA Directive 2010-035 issued on July 22, 2010.16 This directive was rescinded and replaced in January 2011 by VHA Directive 2011-004, which remains in effect as of this article’s publication.17 The provisions of this directive titled “Access to Clinical Programs for Veterans Participating in State-Approved Medical Marijuana Programs” are summarized in the Table as practical guidance for federal practitioners.
In contrast to the VA, the DoD has not revised its position that the use and possession of marijuana for any purpose is a violation of the Uniform Code of Military Justice.18 There is no indication that the DoD plans to change its ruling that military personnel who use or possess marijuana are subject to court martial, even in states where marijuana is available for therapeutic purposes.
Clinical Considerations
Concerns and questions from practitioners in the field about how to practically implement the opinion of VA OGC and VHA Directive 2010-035 led the Office of Patient Care Services (PCS) in August 2010 to issue clinical guidance that has significant ethical implications.2
Veterans who are certified to use medical marijuana should present evidence of their registration, often a medical marijuana card, to their VA provider. The provider is then advised to ask the patient to sign a release of information to enable the VA practitioner to speak to the non-VA counterpart who is prescribing the medical marijuana. This approach respects the patient’s confidentiality and obtains informed consent for coordinated treatment. One limitation of this guidance is that it does not advise the practitioner how to proceed if the patient refuses to sign the release. The VA confidentiality regulations regarding substance use information are the strictest of all federal privacy laws. Under 38 USC 7332, this information cannot be released without the explicit written consent of the veteran in order to prevent stigma and discrimination.19 The ethical objective of this communication between VA and community practitioners is nonmaleficence and thus is focused on “adherence monitoring, treatment effectiveness, safety, and impact on cognitive, emotional, social and physical functioning, and side-effects.”20
Clinicians at VA are expected to know the dosage, frequency, and form of marijuana prescribed and the medical condition for which it is approved. The directive identifies but does not officially recognize as clinical indications for the use of medical marijuana a number of medical conditions for which marijuana is commonly prescribed—glaucoma, chemotherapy-induced nausea, multiple sclerosis, epilepsy, and chronic pain—but it is the specific state laws that determine what medical and psychiatric conditions are approved for the use of medical marijuana.16,21 The PCS clearly states that it is the VA clinician, presumptively the primary care provider (PCP), who is responsible for and directs the patient’s care, just as with any consultant or provider outside VA auspices. Some clinicians find this arrangement problematic, in that they may be potentially liable for bad outcomes and may not refuse a clinically reasonable request for opioids for chronic pain, yet are unable to control the secondary prescribing of marijuana. Clinicians with political, scientific, or moral objections to any use of marijuana for medical purpose may have little recourse under the policy, as there is no indication that such objections would fall under a conscience clause.
The use of medical marijuana is an area of intense research and cultural controversy, and the empirical data to support ethical refusal by a clinician to care for a patient using medical marijuana is often difficult to separate from social attitudes and political positions.22 The VA practitioner has a duty to “adjust treatment plans to promote effective management of these conditions” for which the veteran is using medical marijuana, such as offering adjunctive medications for pain or counseling for substance use.2
The VA clinician in the service of integrated care is required to document all clinical information regarding medical marijuana, including entering the substance as a non-VA prescription in the Computerized Patient Record System. This requirement is essential to protect the veteran from having necessary and appropriate care restricted if the results of toxicology screens are positive for marijuana. One gap in the guidance is that VA clinicians have no ready means of distinguishing prescribed marijuana from illegal marijuana in a standard toxicology screen, and if the patient has a state medical marijuana registration, the clinician must assume the source is prescribed and not illicit. Since the federal practitioner cannot prescribe marijuana, there is even more uncertainty and concern regarding a positive result. Laws passed in 2013 in Colorado and Washington states, which make the recreational use of medical marijuana legal, render toxicology interpretation and medical decision-making even more complex.23
The practitioner is directed to counsel and educate the patient from a nonjudgmental and beneficence-based orientation, which fosters the patient’s autonomy and informed consent. The VA clinician’s discussion of the evidence-base for the health benefits and risks of marijuana should include criteria for a marijuana substance use disorder, emerging data on marijuana withdrawal syndrome and empirical treatment, and most important effective alternative treatments for the target symptoms or conditions for which marijuana is being used.2
Along with this general guidance for the appropriate treatment of patients who use medical marijuana, specific advice is proffered on the 2 most strongly impacted areas of clinical care: pain management and substance use disorders. Practitioners on the ground struggle to reconcile the conflict between state and federal law and policy on medical marijuana in these 2 key domains. Ethics consultation is advised as potentially helpful in resolving ethical dilemmas that arise in patient care.
Pain Management
The PCS articulates the ethical principles surrounding chronic pain treatment with a focus on opioid prescribing for veterans approved to use medical marijuana. A multimodal and stepped-care approach to pain management is endorsed that “should be based on principles of shared medical decision-making and patient autonomy.”2 In this context, veteran safety and minimizing risk to the public are high priorities. Decisions about the use of opioid analgesics need to balance the veteran’s right to pain management and veteran well-being. The informed consent discussion regarding the use of opioids and marijuana should encompass benefits and risks of each substance and its interaction, especially those related to psychomotor impairment, such as driving and memory deficits, which could affect daily functioning. Practitioners are strongly advised to cogently record the clinical evaluation and treatment rationale for prescribing opioids to patients who use medical marijuana.2
Substance Use Disorders
It is the position of the American Society of Addiction Medicine that medical marijuana is not clinically appropriate for patients with substance use disorders.24 The VA policy clearly states that no veteran participating in a state-approved program will be denied substance use treatment or stigmatized for their use of medical marijuana, which is paradoxically a substance of abuse that is illegal in many states outside of these programs. Veterans being treated for other substance use disorders may also develop a marijuana use disorder, even if the drug is medically prescribed, or may concurrently use both legal and recreational marijuana. Just as the principle of justice requires patients who use medical marijuana are not denied participation in substance use treatment, so must veterans who develop abuse of marijuana have equal access to treatment when the addiction risks outweigh the health benefits of marijuana. Central to fairness is the identification of alternative treatments for the conditions for which marijuana is prescribed.2 Unfortunately, diagnosing a marijuana use disorder in a patient using the drug for medical purposes is neither easy nor clear.
There may also be situations in which appropriate use of medical marijuana may interfere with recovery from other substances of abuse, such as benzodiazepines or alcohol, or contravene employment of the optimal therapies for comorbid medical or psychiatric conditions, for example, other sedating psychoactive medications. Medical marijuana use could in theory lead a patient or other patients in a program to relapse to the substance of choice, although preliminary evidence suggests this may not necessarily be the case.25
Self-medication with medical marijuana for symptoms other than those for which the drug is approved may become an obstacle to efficacious treatment of other psychiatric problems. For instance, a veteran being treated for depression with cognitive behavioral therapy (CBT) may find the apathy chronic marijuana often induces to be an obstacle to the homework and activation exercises used in CBT.2
Patient-Physician Partnership
The nature of VA as a beneficiary health care system precludes the organization from denying VA services to veterans participating in state medical marijuana programs. However, the system does allow providers to make decisions to modify treatment plans on clinical grounds so long as those modifications are made in partnership with patients in accordance with VA’s emphasis on shared decision-making in medical care.
It should be noted that despite this emphasis, the autonomy of both patient and physician is legally and administratively circumscribed. If a clinician’s independent reading of the medical literature and professional judgment regarding the patient’s specific clinical circumstances determine medical marijuana is clinically indicated, the clinician is not free to communicate this recommendation to the patient without risking criminal prosecution or institutional sanctions. These considerations may weigh heavily on practitioners who think that medical marijuana would benefit patients, especially in states where it is legally available.
Conversely, patients residing in states with medical marijuana laws who believe the substance would relieve their symptoms can seek out a community provider to assist them in obtaining registration. However, patients’ self-determination is limited in that they do not have the choice to have their PCP, who presumably is most familiar with their medical history, recommend or prescribe medical marijuana. Veterans also are not permitted to use VA pharmacy benefits to have VA pharmacists fill the prescription.
This is a clear statement of the limit of veteran entitlement: VA will not pay for medical marijuana. No exception is made if the veteran is using medical marijuana to treat service-connected injuries or illnesses. Directive 2010-035 (now rescinded) and the original VA OGC opinion assert that medical marijuana does not meet criteria as a core health benefit that VHA as an entitlement program must provide as an aspect of basic care.5,20 The justification for this exclusion is that non-Food and Drug Administration (FDA) approved drugs are not encompassed in the medical benefits package outside either an Investigational New Drug Application or compassionate use FDA provision. Veterans may experience this as a social justice issue and a violation of the VA fiduciary duty to its beneficiaries. A sharp demarcation is made between the private use and public possession of marijuana. Veterans who carry marijuana on VA property, even if they are certified to carry medical marijuana, will be prosecuted under CSA.
Conclusion
Studies estimate that 50% of veterans experience chronic pain, and nearly half of these patients receive prescription opioids.26 Conversely, up to 35% of VA patients are diagnosed with both substance use and mental health disorders.27
The one aspect of the controversy that stakeholders on the pro and con sides of the medical marijuana question agree on is the need for more empirical data.28 There is an urgent need for more study of the use of medical marijuana as a treatment for posttraumatic stress disorder, which is a qualifying health condition in a growing number of states.29
Along with federal law, it is federal agencies, including the DEA, FDA, and the National Institute on Drug Abuse, that may be the biggest obstacle to conducting this vital research.30 These regulatory obstacles must be removed before researchers can conduct the scientific studies needed to provide a factual foundation to inform what has too often been a political debate. Solid science grounding legal reform and shaping public policy toward medical marijuana may be the only means of resolving the ethical dilemmas that confront veterans daily and the VA clinicians committed to caring for them.31,32
In the interim, VA practitioners should be provided effective training in educating and counseling patients about the implications of VA policy regarding state-approved medical marijuana programs for their individual health care. Such a patient-centered approach represents the most ethically acceptable means of mediating the conflict between state and federal law regarding medical marijuana in its current stage of evolution.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. State Medical Marijuana Laws. National Conference of State Legislators Website. http://www.ncsl.org/issues-research/health/state-medical-marijuana-laws.aspx. Updated January 2014. Accessed February 1, 2014.
2. Veterans Health Administration. Clinical Considerations Regarding Veteran Patients Who Participate in State-Approved Medical Marijuana Programs. Washington, DC: Department of Veterans Affairs; 2010.
3. The Associated Press. Supreme Court is set to consider medical marijuana. New York Times. November 28, 2004. http://www.nytimes.com/2004/11/28/politics/28marijuana.html?fta=y. Accessed February 5, 2014.
4. Dresser R. Irrational basis: The legal status of medical marijuana. Hastings Cent Rep. 2009;39(6):7-8.
5. Office of General Counsel. Opinion on State Medical Marijuana Registration Forms. Washington, DC: Department of Veterans Affairs; 2008. VAOPGCADV 9-2008.
6. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part one of two. J Pain Palliat Care Pharmacother. 2009;23(1):4-25.
7. Pearson v McCaffrey, 139 F Supp 2d 772 (D DC 2001).
8. Constitution of the United States. United States Senate Website. http://www.senate.gov/civics/constitution_item/constitution.htm. Accessed January 22, 2012.
9. White BD. New York, NY: Informa Healthcare; 2007.
10. Conant v Walters, 309 F3d 629 (9th Cir 2002).
11. Gonzales v Raich, 545 US 1, 125 SCt, 2195 (2005).
12. United States v Lopez, 514 US 549, 115 SCt, 1624 (1995).
13. United States v Morrison, 529 US 598, 120 SCt, 1740 (2000).
14. The Lynn and Erin Compassionate Use Act, NMSA 1978 §26-2B (2007).
15. Frosch D. V.A. Easing rules for users of medical marijuana. New York Times. July 24, 2010:A1.
16. Medical Marijuana. Washington, DC: Dept of Veterans Affairs; 2010. VHA Directive 2010-035.
17. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
18. Uniform Code of Military Justice, 10 USC § 912A (2011).
19. Confidentiality of Certain Medical Records, 38 USC § 7332 (1991).
20. Petzel RA. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
21. Institute of Medicine. Marijuana and Medicine: Assessing the Science. Joy JE, Watson SJ Jr, Benson JA Jr, eds. Washington, DC: National Academy Press; 1999.
22. Charuvastra A, Friedmann PD, Stein MD. Physician attitudes regarding the prescription of medical marijuana. J Addict Dis. 2005;24(3):87-93.
23. Healy J. Up early and in line for a medical marijuana milestone in Colorado. New York Times. January 1, 2014:A1.
24. Public Policy Statement on Medical Marijuana. Chevy Chase, MD: American Society of Addiction Medicine; 2010.
25. Swartz R. Medical marijuana users in substance abuse treatment. Harm Reduct J. 2010;7:3.
26. Clark JD. Chronic pain prevalence and analgesic prescribing in a general medical population. J Pain Symptom Manage. 2002;23(2):131-137.
27. Petrakis IL, Rosenheck R, Desai R. Substance use comorbidity among veterans with posttraumatic stress disorder and other psychiatric illness. Am J Addict. 2011;20(3):185-189.
28. Medical Marijuana. ProCon.org Website. http://medicalmarijuana.procon.org. Updated February 3, 2014. Accessed February 5, 2014.
29. Busemeyer D. Cannabis catch-22. Santa Fe New Mexican. October 14, 2012:A1, A4-A5.
30. Harris G. Researchers find study of medical marijuana discouraged. New York Times. January 18, 2010:A14.
31. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part two of two. J Pain Palliat Care Pharmacother. 2009;23(2):120-140.
32. Daigle L. Medical Marijuana. Bethesda, MD: American Society of Health-System Pharmacists; 2011.
This conflict between state and federal law has been the subject of considerable discussion in the professional literature and popular media, even reaching the Supreme Court.3,4 Much less attention has been paid to the parallel, but in some ways even more complicated, ethical, legal, and policy dilemmas facing administrators and practitioners in the Veterans Health Administration (VHA). Federal law governs VA health care facilities and clinical practice, yet there are VA hospitals and clinics in every state that have passed medical marijuana legislation, and veterans are eligible to obtain medical marijuana as residents of their respective states.
This article examines the evolution of VA policy regarding the use of medical marijuana within the confines of federal law and the nature of the VA as a beneficiary system with a mission to provide comprehensive health care to veterans and the legal, clinical, and ethical issues these often opposing obligations present to VA practitioners.
Completion of State Medical Marijuana Forms
In 2008, the VA Office of the General Counsel (OGC) issued to VA physicians the first official directions regarding state medical marijuana programs.5 The ruling of the VA OGC pertained to state medical marijuana registration forms and was addressed to the Under Secretary for Health. The VHA had requested guidance on how VA staff should respond when patients ask them to fill out state forms used to access medical marijuana; specifically, whether VA physicians are permitted or required to complete state medical marijuana registration forms.
The VA OGC was further asked to address the legal issues involved when a VA physician is requested to complete such a form and whether completion of such a form could result in criminal action or other penalties against the physician.
The opinion of the VA OGC issued in a memorandum on May 21, 2008, held that “VA should not authorize the completion of forms seeking recommendation or opinions regarding participation in such a program. Applicable statutes and regulations do not require VA physicians to complete such forms.”5 In response to the first question posed, the VA OGC identified the legal issues involved in the completion of the forms, arguing that the CSA designated marijuana as a Schedule 1 drug, meaning it had no accepted medical use but does have high potential for abuse. The Schedule 1 classification carried with it penalties for the dispensing, manufacturing, distributing, and possession of marijuana that were the responsibility of the Drug Enforcement Agency (DEA) to enforce.
In response to the second question, the VA OGC held that if a VA physician did complete a form permitting a patient to participate in a state medical marijuana program, this could result in DEA action, including revocation of the physician’s registration to prescribe controlled substances, as well as possible criminal charges.6 The VA OGC cited several landmark medical marijuana cases as the background to its issued opinion.
The first case cited in the VA OGC’s opinion was Pearson v McCaffrey, a 2001 ruling pertaining to the U.S. District Court of the District of Columbia.7 Barry McCaffrey, then-director of the Office of National Drug Control Policy, Donna Shalala, the secretary for the U.S. Department of Health and Human Services, and Janet Reno, attorney general, promulgated a policy that allowed the federal government to prosecute or revoke the controlled substance registration of any physician who prescribed or, more relevant to the VA situation, recommended medical marijuana to patients.
Physicians and patients in states with medical marijuana laws sought an injunction against the federal government prohibiting them from initiating civil, criminal, or administrative actions against physicians who recommended and prescribed or patients who obtained and used medical marijuana. The court refused to enforce the injunction the plaintiffs filed against the policy, finding that the federal position did not violate the First Amendment rights of the plaintiffs and, more pertinent, that Congress did have the authority under the Commerce Clause to regulate medical marijuana as a matter of public health and safety.7
Article 1, section 8, clause 3 of the U.S. Constitution grants that the U.S. Congress has the authority “To regulate Commerce with foreign Nations, and among the several states, and with the Indian tribes.”8 The Commerce Clause is often at issue in cases where the scope of federal power toward the states is challenged. The Commerce Clause is especially relevant to the legal status of state medical marijuana laws examined here because it is cited as the legal authority for the CSA, and the CSA governs practitioner prescribing.9
At the same time, an injunction against enforcement was filed in the District Court for the Northern District of California. A group of patients and physicians again initiated the legal action; this time, they were successful in obtaining a permanent injunction of the policy: The court prohibited the federal government from revoking the controlled substance registration or investigating any physician who recommended medical marijuana on the basis of a sincere medical judgment. The Supreme Court declined to hear the case.10
The U.S. Supreme Court did accept the third case, Gonzales v Raich, which did not address whether the individual physician would be prosecuted for recommending a state medical marijuana program but instead whether the federal government possessed the authority under the Commerce Clause to regulate intrastate use of marijuana for medical purposes, including revoking physicians’ controlled substance licenses.
The facts of the Raich case and legal background leading to the Supreme Court decision are as follows: In 1996, California voters passed the Compassionate Use Act, making California the first state in the country to legalize the medical use of marijuana. The law conflicted with the classification of marijuana as a Schedule 1 drug. This conflict between state and federal law rendered the case highly relevant to the question of VA physicians’ completion of medical marijuana forms for patients in states where medical marijuana is legal. The DEA had acted in California, not against a physician’s prescribing authority but against a patient, Angel Raich, for possession of medical marijuana. The DEA agents confiscated the medical marijuana from the patient’s home. In response, a group of medical marijuana users sued the DEA and California Attorney General Roberto Gonzales in federal district court.11
Raich’s attorneys argued that the constitutional basis of the federal government’s power to regulate interstate commerce, which formed the legal claim of the CSA, overreached Congress’s Commerce Clause powers. The district court ruled in favor of the attorney general, but the Ninth Circuit Court of Appeals reversed the decision, ruling that the application of the CSA to the intrastate transactions involved in California’s medical marijuana program was unconstitutional. The Ninth Circuit Court ruling cited 2 important prior cases not involving medical marijuana that also limited the Commerce Clause, although not with reference to marijuana: U.S. v Lopez in 1995 and U.S. v Morrison in 2000.12,13
The Supreme Court agreed to hear the case in June 2004 and in a 6-3 decision ruled that the application of the CSA to intrastate cultivation and possession of marijuana for medical use does not exceed Congress’s power under the Commerce Clause. Supreme Court Justice John Paul Stevens wrote the majority opinion, arguing that the power of the Commerce Clause did extend to the regulation of a “class of activities” that had a substantial effect on interstate commerce. Because marijuana use, even for medical purposes, confined to a local area, such as a state, materially affected the supply and demand market for marijuana in the nation, the regulation of state use of marijuana was required to govern the interstate traffic of marijuana.11
The VA OGC opinion referenced these cases in its analysis of the question VHA providers raised regarding the completion of state medical marijuana forms, particularly those in states such as Colorado and New Mexico where completing forms is not equivalent to providing a prescription yet does constitute a medical recommendation for the use of marijuana.14 The OGC noted that recommendation is not a term of art contained within the CSA and that Pearson ruled that there was no salient distinction between a prescription and a recommendation, where a recommendation was necessary for a patient to be able to obtain medical marijuana, which is the requirement in most states.5
The VA OGC concluded, “While some states may provide for the use of medical marijuana, such programs are in violation of federal law.”5 In formulating its judgment, the VA OGC cited the Supremacy Clause as the key to all subsequent VHA directives regarding medical marijuana. “The Supremacy Clause is the most important guarantor of national union. It assures that the Constitution and federal laws and treaties take precedence over state law and binds all judges to adhere to that principle in their courts.”8
Quoting an informal communication from the Department of Justice (DOJ), the VA OGC warned that the DOJ “may seek civil or criminal penalties for federal physicians and practitioners who completed forms that either recommend the use of medical marijuana or forms that describe the patient’s physical condition in order to facilitate the patient’s procurement of medical marijuana pursuant to state law.”5
Local vs Federal Policy
By 2009, 15 states had passed legislation allowing the medical use of marijuana. Many VA hospitals and clinics continued to regard marijuana, whether prescribed or not, as an illicit drug that violated opioid contracts or agreements. The clinical justification for these denials or other treatment plan modifications was to ensure that veterans used marijuana safely, for example, through detecting and preventing drug interactions or impairment of driving ability.
A group called Veterans for Medical Marijuana Access, founded by veteran Michael Krawitz, was the most politically active among veterans’ organizations on the issue of medical marijuana. Astutely, Mr. Krawitz and other advocates did not aim to change federal law and the Supremacy Clause or the court’s interpretations of the Commerce Clause as it applied to medical marijuana. Instead, their strategy was to expand veterans’ access to state programs, and their tactic was to work directly with the VA to formulate a policy. Mr. Krawitz adroitly used the media to champion his cause.
On March 5, 2010, Krawitz received a letter from Col. Will A. Gunn of the VA OGC. Mr. Krawitz had written the VA OGC regarding the inequities in VA policy regarding the provision of opioid medications for pain management to veterans enrolled in state medical marijuana programs. Mr. Krawitz informed Col. Gunn that the directors of some facilities had issued policies explicitly stating that veterans who provide medical marijuana registration in accordance with state programs and who tested positive for the drug would not be considered in violation of opioid contracts. Mr. Krawitz asked for official confirmation that these local policies were valid. On July 6, 2010, Under Secretary for Health Dr. Robert Petzel wrote Mr. Krawitz a memorandum stating, “If a veteran obtains and uses medical marijuana in a manner consistent with state law, testing positive for marijuana would not preclude the veteran from receiving opioids for pain management in a Department of Veterans Affairs facility.”
Dr. Petzel also outlined what would become the clinical ethics principles VA would employ to manage the federal-state law conflict regarding medical marijuana. First, a patient must inform his provider of medical marijuana use to ensure safety. Second, opioid agreements must make a clear distinction between illegal drugs, including the recreational use of marijuana, and medical marijuana. Third, the practitioner has the discretion to make the opioid prescribing decision and must make that decision on clinical grounds. Fourth, the prescribing decision should be made on a case-by-case basis “based upon the provider’s judgment and the needs of the patient.”
Following these letters was a highly publicized article in The New York Times in which Principal Deputy Under Secretary for Health Dr. Robert L. Jesse confirmed the new policy.15 The article included comments from Mr. Krawitz on the change in VA’s approach to medical marijuana. The VHA codified these less formal communications in VHA Directive 2010-035 issued on July 22, 2010.16 This directive was rescinded and replaced in January 2011 by VHA Directive 2011-004, which remains in effect as of this article’s publication.17 The provisions of this directive titled “Access to Clinical Programs for Veterans Participating in State-Approved Medical Marijuana Programs” are summarized in the Table as practical guidance for federal practitioners.
In contrast to the VA, the DoD has not revised its position that the use and possession of marijuana for any purpose is a violation of the Uniform Code of Military Justice.18 There is no indication that the DoD plans to change its ruling that military personnel who use or possess marijuana are subject to court martial, even in states where marijuana is available for therapeutic purposes.
Clinical Considerations
Concerns and questions from practitioners in the field about how to practically implement the opinion of VA OGC and VHA Directive 2010-035 led the Office of Patient Care Services (PCS) in August 2010 to issue clinical guidance that has significant ethical implications.2
Veterans who are certified to use medical marijuana should present evidence of their registration, often a medical marijuana card, to their VA provider. The provider is then advised to ask the patient to sign a release of information to enable the VA practitioner to speak to the non-VA counterpart who is prescribing the medical marijuana. This approach respects the patient’s confidentiality and obtains informed consent for coordinated treatment. One limitation of this guidance is that it does not advise the practitioner how to proceed if the patient refuses to sign the release. The VA confidentiality regulations regarding substance use information are the strictest of all federal privacy laws. Under 38 USC 7332, this information cannot be released without the explicit written consent of the veteran in order to prevent stigma and discrimination.19 The ethical objective of this communication between VA and community practitioners is nonmaleficence and thus is focused on “adherence monitoring, treatment effectiveness, safety, and impact on cognitive, emotional, social and physical functioning, and side-effects.”20
Clinicians at VA are expected to know the dosage, frequency, and form of marijuana prescribed and the medical condition for which it is approved. The directive identifies but does not officially recognize as clinical indications for the use of medical marijuana a number of medical conditions for which marijuana is commonly prescribed—glaucoma, chemotherapy-induced nausea, multiple sclerosis, epilepsy, and chronic pain—but it is the specific state laws that determine what medical and psychiatric conditions are approved for the use of medical marijuana.16,21 The PCS clearly states that it is the VA clinician, presumptively the primary care provider (PCP), who is responsible for and directs the patient’s care, just as with any consultant or provider outside VA auspices. Some clinicians find this arrangement problematic, in that they may be potentially liable for bad outcomes and may not refuse a clinically reasonable request for opioids for chronic pain, yet are unable to control the secondary prescribing of marijuana. Clinicians with political, scientific, or moral objections to any use of marijuana for medical purpose may have little recourse under the policy, as there is no indication that such objections would fall under a conscience clause.
The use of medical marijuana is an area of intense research and cultural controversy, and the empirical data to support ethical refusal by a clinician to care for a patient using medical marijuana is often difficult to separate from social attitudes and political positions.22 The VA practitioner has a duty to “adjust treatment plans to promote effective management of these conditions” for which the veteran is using medical marijuana, such as offering adjunctive medications for pain or counseling for substance use.2
The VA clinician in the service of integrated care is required to document all clinical information regarding medical marijuana, including entering the substance as a non-VA prescription in the Computerized Patient Record System. This requirement is essential to protect the veteran from having necessary and appropriate care restricted if the results of toxicology screens are positive for marijuana. One gap in the guidance is that VA clinicians have no ready means of distinguishing prescribed marijuana from illegal marijuana in a standard toxicology screen, and if the patient has a state medical marijuana registration, the clinician must assume the source is prescribed and not illicit. Since the federal practitioner cannot prescribe marijuana, there is even more uncertainty and concern regarding a positive result. Laws passed in 2013 in Colorado and Washington states, which make the recreational use of medical marijuana legal, render toxicology interpretation and medical decision-making even more complex.23
The practitioner is directed to counsel and educate the patient from a nonjudgmental and beneficence-based orientation, which fosters the patient’s autonomy and informed consent. The VA clinician’s discussion of the evidence-base for the health benefits and risks of marijuana should include criteria for a marijuana substance use disorder, emerging data on marijuana withdrawal syndrome and empirical treatment, and most important effective alternative treatments for the target symptoms or conditions for which marijuana is being used.2
Along with this general guidance for the appropriate treatment of patients who use medical marijuana, specific advice is proffered on the 2 most strongly impacted areas of clinical care: pain management and substance use disorders. Practitioners on the ground struggle to reconcile the conflict between state and federal law and policy on medical marijuana in these 2 key domains. Ethics consultation is advised as potentially helpful in resolving ethical dilemmas that arise in patient care.
Pain Management
The PCS articulates the ethical principles surrounding chronic pain treatment with a focus on opioid prescribing for veterans approved to use medical marijuana. A multimodal and stepped-care approach to pain management is endorsed that “should be based on principles of shared medical decision-making and patient autonomy.”2 In this context, veteran safety and minimizing risk to the public are high priorities. Decisions about the use of opioid analgesics need to balance the veteran’s right to pain management and veteran well-being. The informed consent discussion regarding the use of opioids and marijuana should encompass benefits and risks of each substance and its interaction, especially those related to psychomotor impairment, such as driving and memory deficits, which could affect daily functioning. Practitioners are strongly advised to cogently record the clinical evaluation and treatment rationale for prescribing opioids to patients who use medical marijuana.2
Substance Use Disorders
It is the position of the American Society of Addiction Medicine that medical marijuana is not clinically appropriate for patients with substance use disorders.24 The VA policy clearly states that no veteran participating in a state-approved program will be denied substance use treatment or stigmatized for their use of medical marijuana, which is paradoxically a substance of abuse that is illegal in many states outside of these programs. Veterans being treated for other substance use disorders may also develop a marijuana use disorder, even if the drug is medically prescribed, or may concurrently use both legal and recreational marijuana. Just as the principle of justice requires patients who use medical marijuana are not denied participation in substance use treatment, so must veterans who develop abuse of marijuana have equal access to treatment when the addiction risks outweigh the health benefits of marijuana. Central to fairness is the identification of alternative treatments for the conditions for which marijuana is prescribed.2 Unfortunately, diagnosing a marijuana use disorder in a patient using the drug for medical purposes is neither easy nor clear.
There may also be situations in which appropriate use of medical marijuana may interfere with recovery from other substances of abuse, such as benzodiazepines or alcohol, or contravene employment of the optimal therapies for comorbid medical or psychiatric conditions, for example, other sedating psychoactive medications. Medical marijuana use could in theory lead a patient or other patients in a program to relapse to the substance of choice, although preliminary evidence suggests this may not necessarily be the case.25
Self-medication with medical marijuana for symptoms other than those for which the drug is approved may become an obstacle to efficacious treatment of other psychiatric problems. For instance, a veteran being treated for depression with cognitive behavioral therapy (CBT) may find the apathy chronic marijuana often induces to be an obstacle to the homework and activation exercises used in CBT.2
Patient-Physician Partnership
The nature of VA as a beneficiary health care system precludes the organization from denying VA services to veterans participating in state medical marijuana programs. However, the system does allow providers to make decisions to modify treatment plans on clinical grounds so long as those modifications are made in partnership with patients in accordance with VA’s emphasis on shared decision-making in medical care.
It should be noted that despite this emphasis, the autonomy of both patient and physician is legally and administratively circumscribed. If a clinician’s independent reading of the medical literature and professional judgment regarding the patient’s specific clinical circumstances determine medical marijuana is clinically indicated, the clinician is not free to communicate this recommendation to the patient without risking criminal prosecution or institutional sanctions. These considerations may weigh heavily on practitioners who think that medical marijuana would benefit patients, especially in states where it is legally available.
Conversely, patients residing in states with medical marijuana laws who believe the substance would relieve their symptoms can seek out a community provider to assist them in obtaining registration. However, patients’ self-determination is limited in that they do not have the choice to have their PCP, who presumably is most familiar with their medical history, recommend or prescribe medical marijuana. Veterans also are not permitted to use VA pharmacy benefits to have VA pharmacists fill the prescription.
This is a clear statement of the limit of veteran entitlement: VA will not pay for medical marijuana. No exception is made if the veteran is using medical marijuana to treat service-connected injuries or illnesses. Directive 2010-035 (now rescinded) and the original VA OGC opinion assert that medical marijuana does not meet criteria as a core health benefit that VHA as an entitlement program must provide as an aspect of basic care.5,20 The justification for this exclusion is that non-Food and Drug Administration (FDA) approved drugs are not encompassed in the medical benefits package outside either an Investigational New Drug Application or compassionate use FDA provision. Veterans may experience this as a social justice issue and a violation of the VA fiduciary duty to its beneficiaries. A sharp demarcation is made between the private use and public possession of marijuana. Veterans who carry marijuana on VA property, even if they are certified to carry medical marijuana, will be prosecuted under CSA.
Conclusion
Studies estimate that 50% of veterans experience chronic pain, and nearly half of these patients receive prescription opioids.26 Conversely, up to 35% of VA patients are diagnosed with both substance use and mental health disorders.27
The one aspect of the controversy that stakeholders on the pro and con sides of the medical marijuana question agree on is the need for more empirical data.28 There is an urgent need for more study of the use of medical marijuana as a treatment for posttraumatic stress disorder, which is a qualifying health condition in a growing number of states.29
Along with federal law, it is federal agencies, including the DEA, FDA, and the National Institute on Drug Abuse, that may be the biggest obstacle to conducting this vital research.30 These regulatory obstacles must be removed before researchers can conduct the scientific studies needed to provide a factual foundation to inform what has too often been a political debate. Solid science grounding legal reform and shaping public policy toward medical marijuana may be the only means of resolving the ethical dilemmas that confront veterans daily and the VA clinicians committed to caring for them.31,32
In the interim, VA practitioners should be provided effective training in educating and counseling patients about the implications of VA policy regarding state-approved medical marijuana programs for their individual health care. Such a patient-centered approach represents the most ethically acceptable means of mediating the conflict between state and federal law regarding medical marijuana in its current stage of evolution.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. State Medical Marijuana Laws. National Conference of State Legislators Website. http://www.ncsl.org/issues-research/health/state-medical-marijuana-laws.aspx. Updated January 2014. Accessed February 1, 2014.
2. Veterans Health Administration. Clinical Considerations Regarding Veteran Patients Who Participate in State-Approved Medical Marijuana Programs. Washington, DC: Department of Veterans Affairs; 2010.
3. The Associated Press. Supreme Court is set to consider medical marijuana. New York Times. November 28, 2004. http://www.nytimes.com/2004/11/28/politics/28marijuana.html?fta=y. Accessed February 5, 2014.
4. Dresser R. Irrational basis: The legal status of medical marijuana. Hastings Cent Rep. 2009;39(6):7-8.
5. Office of General Counsel. Opinion on State Medical Marijuana Registration Forms. Washington, DC: Department of Veterans Affairs; 2008. VAOPGCADV 9-2008.
6. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part one of two. J Pain Palliat Care Pharmacother. 2009;23(1):4-25.
7. Pearson v McCaffrey, 139 F Supp 2d 772 (D DC 2001).
8. Constitution of the United States. United States Senate Website. http://www.senate.gov/civics/constitution_item/constitution.htm. Accessed January 22, 2012.
9. White BD. New York, NY: Informa Healthcare; 2007.
10. Conant v Walters, 309 F3d 629 (9th Cir 2002).
11. Gonzales v Raich, 545 US 1, 125 SCt, 2195 (2005).
12. United States v Lopez, 514 US 549, 115 SCt, 1624 (1995).
13. United States v Morrison, 529 US 598, 120 SCt, 1740 (2000).
14. The Lynn and Erin Compassionate Use Act, NMSA 1978 §26-2B (2007).
15. Frosch D. V.A. Easing rules for users of medical marijuana. New York Times. July 24, 2010:A1.
16. Medical Marijuana. Washington, DC: Dept of Veterans Affairs; 2010. VHA Directive 2010-035.
17. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
18. Uniform Code of Military Justice, 10 USC § 912A (2011).
19. Confidentiality of Certain Medical Records, 38 USC § 7332 (1991).
20. Petzel RA. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
21. Institute of Medicine. Marijuana and Medicine: Assessing the Science. Joy JE, Watson SJ Jr, Benson JA Jr, eds. Washington, DC: National Academy Press; 1999.
22. Charuvastra A, Friedmann PD, Stein MD. Physician attitudes regarding the prescription of medical marijuana. J Addict Dis. 2005;24(3):87-93.
23. Healy J. Up early and in line for a medical marijuana milestone in Colorado. New York Times. January 1, 2014:A1.
24. Public Policy Statement on Medical Marijuana. Chevy Chase, MD: American Society of Addiction Medicine; 2010.
25. Swartz R. Medical marijuana users in substance abuse treatment. Harm Reduct J. 2010;7:3.
26. Clark JD. Chronic pain prevalence and analgesic prescribing in a general medical population. J Pain Symptom Manage. 2002;23(2):131-137.
27. Petrakis IL, Rosenheck R, Desai R. Substance use comorbidity among veterans with posttraumatic stress disorder and other psychiatric illness. Am J Addict. 2011;20(3):185-189.
28. Medical Marijuana. ProCon.org Website. http://medicalmarijuana.procon.org. Updated February 3, 2014. Accessed February 5, 2014.
29. Busemeyer D. Cannabis catch-22. Santa Fe New Mexican. October 14, 2012:A1, A4-A5.
30. Harris G. Researchers find study of medical marijuana discouraged. New York Times. January 18, 2010:A14.
31. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part two of two. J Pain Palliat Care Pharmacother. 2009;23(2):120-140.
32. Daigle L. Medical Marijuana. Bethesda, MD: American Society of Health-System Pharmacists; 2011.
This conflict between state and federal law has been the subject of considerable discussion in the professional literature and popular media, even reaching the Supreme Court.3,4 Much less attention has been paid to the parallel, but in some ways even more complicated, ethical, legal, and policy dilemmas facing administrators and practitioners in the Veterans Health Administration (VHA). Federal law governs VA health care facilities and clinical practice, yet there are VA hospitals and clinics in every state that have passed medical marijuana legislation, and veterans are eligible to obtain medical marijuana as residents of their respective states.
This article examines the evolution of VA policy regarding the use of medical marijuana within the confines of federal law and the nature of the VA as a beneficiary system with a mission to provide comprehensive health care to veterans and the legal, clinical, and ethical issues these often opposing obligations present to VA practitioners.
Completion of State Medical Marijuana Forms
In 2008, the VA Office of the General Counsel (OGC) issued to VA physicians the first official directions regarding state medical marijuana programs.5 The ruling of the VA OGC pertained to state medical marijuana registration forms and was addressed to the Under Secretary for Health. The VHA had requested guidance on how VA staff should respond when patients ask them to fill out state forms used to access medical marijuana; specifically, whether VA physicians are permitted or required to complete state medical marijuana registration forms.
The VA OGC was further asked to address the legal issues involved when a VA physician is requested to complete such a form and whether completion of such a form could result in criminal action or other penalties against the physician.
The opinion of the VA OGC issued in a memorandum on May 21, 2008, held that “VA should not authorize the completion of forms seeking recommendation or opinions regarding participation in such a program. Applicable statutes and regulations do not require VA physicians to complete such forms.”5 In response to the first question posed, the VA OGC identified the legal issues involved in the completion of the forms, arguing that the CSA designated marijuana as a Schedule 1 drug, meaning it had no accepted medical use but does have high potential for abuse. The Schedule 1 classification carried with it penalties for the dispensing, manufacturing, distributing, and possession of marijuana that were the responsibility of the Drug Enforcement Agency (DEA) to enforce.
In response to the second question, the VA OGC held that if a VA physician did complete a form permitting a patient to participate in a state medical marijuana program, this could result in DEA action, including revocation of the physician’s registration to prescribe controlled substances, as well as possible criminal charges.6 The VA OGC cited several landmark medical marijuana cases as the background to its issued opinion.
The first case cited in the VA OGC’s opinion was Pearson v McCaffrey, a 2001 ruling pertaining to the U.S. District Court of the District of Columbia.7 Barry McCaffrey, then-director of the Office of National Drug Control Policy, Donna Shalala, the secretary for the U.S. Department of Health and Human Services, and Janet Reno, attorney general, promulgated a policy that allowed the federal government to prosecute or revoke the controlled substance registration of any physician who prescribed or, more relevant to the VA situation, recommended medical marijuana to patients.
Physicians and patients in states with medical marijuana laws sought an injunction against the federal government prohibiting them from initiating civil, criminal, or administrative actions against physicians who recommended and prescribed or patients who obtained and used medical marijuana. The court refused to enforce the injunction the plaintiffs filed against the policy, finding that the federal position did not violate the First Amendment rights of the plaintiffs and, more pertinent, that Congress did have the authority under the Commerce Clause to regulate medical marijuana as a matter of public health and safety.7
Article 1, section 8, clause 3 of the U.S. Constitution grants that the U.S. Congress has the authority “To regulate Commerce with foreign Nations, and among the several states, and with the Indian tribes.”8 The Commerce Clause is often at issue in cases where the scope of federal power toward the states is challenged. The Commerce Clause is especially relevant to the legal status of state medical marijuana laws examined here because it is cited as the legal authority for the CSA, and the CSA governs practitioner prescribing.9
At the same time, an injunction against enforcement was filed in the District Court for the Northern District of California. A group of patients and physicians again initiated the legal action; this time, they were successful in obtaining a permanent injunction of the policy: The court prohibited the federal government from revoking the controlled substance registration or investigating any physician who recommended medical marijuana on the basis of a sincere medical judgment. The Supreme Court declined to hear the case.10
The U.S. Supreme Court did accept the third case, Gonzales v Raich, which did not address whether the individual physician would be prosecuted for recommending a state medical marijuana program but instead whether the federal government possessed the authority under the Commerce Clause to regulate intrastate use of marijuana for medical purposes, including revoking physicians’ controlled substance licenses.
The facts of the Raich case and legal background leading to the Supreme Court decision are as follows: In 1996, California voters passed the Compassionate Use Act, making California the first state in the country to legalize the medical use of marijuana. The law conflicted with the classification of marijuana as a Schedule 1 drug. This conflict between state and federal law rendered the case highly relevant to the question of VA physicians’ completion of medical marijuana forms for patients in states where medical marijuana is legal. The DEA had acted in California, not against a physician’s prescribing authority but against a patient, Angel Raich, for possession of medical marijuana. The DEA agents confiscated the medical marijuana from the patient’s home. In response, a group of medical marijuana users sued the DEA and California Attorney General Roberto Gonzales in federal district court.11
Raich’s attorneys argued that the constitutional basis of the federal government’s power to regulate interstate commerce, which formed the legal claim of the CSA, overreached Congress’s Commerce Clause powers. The district court ruled in favor of the attorney general, but the Ninth Circuit Court of Appeals reversed the decision, ruling that the application of the CSA to the intrastate transactions involved in California’s medical marijuana program was unconstitutional. The Ninth Circuit Court ruling cited 2 important prior cases not involving medical marijuana that also limited the Commerce Clause, although not with reference to marijuana: U.S. v Lopez in 1995 and U.S. v Morrison in 2000.12,13
The Supreme Court agreed to hear the case in June 2004 and in a 6-3 decision ruled that the application of the CSA to intrastate cultivation and possession of marijuana for medical use does not exceed Congress’s power under the Commerce Clause. Supreme Court Justice John Paul Stevens wrote the majority opinion, arguing that the power of the Commerce Clause did extend to the regulation of a “class of activities” that had a substantial effect on interstate commerce. Because marijuana use, even for medical purposes, confined to a local area, such as a state, materially affected the supply and demand market for marijuana in the nation, the regulation of state use of marijuana was required to govern the interstate traffic of marijuana.11
The VA OGC opinion referenced these cases in its analysis of the question VHA providers raised regarding the completion of state medical marijuana forms, particularly those in states such as Colorado and New Mexico where completing forms is not equivalent to providing a prescription yet does constitute a medical recommendation for the use of marijuana.14 The OGC noted that recommendation is not a term of art contained within the CSA and that Pearson ruled that there was no salient distinction between a prescription and a recommendation, where a recommendation was necessary for a patient to be able to obtain medical marijuana, which is the requirement in most states.5
The VA OGC concluded, “While some states may provide for the use of medical marijuana, such programs are in violation of federal law.”5 In formulating its judgment, the VA OGC cited the Supremacy Clause as the key to all subsequent VHA directives regarding medical marijuana. “The Supremacy Clause is the most important guarantor of national union. It assures that the Constitution and federal laws and treaties take precedence over state law and binds all judges to adhere to that principle in their courts.”8
Quoting an informal communication from the Department of Justice (DOJ), the VA OGC warned that the DOJ “may seek civil or criminal penalties for federal physicians and practitioners who completed forms that either recommend the use of medical marijuana or forms that describe the patient’s physical condition in order to facilitate the patient’s procurement of medical marijuana pursuant to state law.”5
Local vs Federal Policy
By 2009, 15 states had passed legislation allowing the medical use of marijuana. Many VA hospitals and clinics continued to regard marijuana, whether prescribed or not, as an illicit drug that violated opioid contracts or agreements. The clinical justification for these denials or other treatment plan modifications was to ensure that veterans used marijuana safely, for example, through detecting and preventing drug interactions or impairment of driving ability.
A group called Veterans for Medical Marijuana Access, founded by veteran Michael Krawitz, was the most politically active among veterans’ organizations on the issue of medical marijuana. Astutely, Mr. Krawitz and other advocates did not aim to change federal law and the Supremacy Clause or the court’s interpretations of the Commerce Clause as it applied to medical marijuana. Instead, their strategy was to expand veterans’ access to state programs, and their tactic was to work directly with the VA to formulate a policy. Mr. Krawitz adroitly used the media to champion his cause.
On March 5, 2010, Krawitz received a letter from Col. Will A. Gunn of the VA OGC. Mr. Krawitz had written the VA OGC regarding the inequities in VA policy regarding the provision of opioid medications for pain management to veterans enrolled in state medical marijuana programs. Mr. Krawitz informed Col. Gunn that the directors of some facilities had issued policies explicitly stating that veterans who provide medical marijuana registration in accordance with state programs and who tested positive for the drug would not be considered in violation of opioid contracts. Mr. Krawitz asked for official confirmation that these local policies were valid. On July 6, 2010, Under Secretary for Health Dr. Robert Petzel wrote Mr. Krawitz a memorandum stating, “If a veteran obtains and uses medical marijuana in a manner consistent with state law, testing positive for marijuana would not preclude the veteran from receiving opioids for pain management in a Department of Veterans Affairs facility.”
Dr. Petzel also outlined what would become the clinical ethics principles VA would employ to manage the federal-state law conflict regarding medical marijuana. First, a patient must inform his provider of medical marijuana use to ensure safety. Second, opioid agreements must make a clear distinction between illegal drugs, including the recreational use of marijuana, and medical marijuana. Third, the practitioner has the discretion to make the opioid prescribing decision and must make that decision on clinical grounds. Fourth, the prescribing decision should be made on a case-by-case basis “based upon the provider’s judgment and the needs of the patient.”
Following these letters was a highly publicized article in The New York Times in which Principal Deputy Under Secretary for Health Dr. Robert L. Jesse confirmed the new policy.15 The article included comments from Mr. Krawitz on the change in VA’s approach to medical marijuana. The VHA codified these less formal communications in VHA Directive 2010-035 issued on July 22, 2010.16 This directive was rescinded and replaced in January 2011 by VHA Directive 2011-004, which remains in effect as of this article’s publication.17 The provisions of this directive titled “Access to Clinical Programs for Veterans Participating in State-Approved Medical Marijuana Programs” are summarized in the Table as practical guidance for federal practitioners.
In contrast to the VA, the DoD has not revised its position that the use and possession of marijuana for any purpose is a violation of the Uniform Code of Military Justice.18 There is no indication that the DoD plans to change its ruling that military personnel who use or possess marijuana are subject to court martial, even in states where marijuana is available for therapeutic purposes.
Clinical Considerations
Concerns and questions from practitioners in the field about how to practically implement the opinion of VA OGC and VHA Directive 2010-035 led the Office of Patient Care Services (PCS) in August 2010 to issue clinical guidance that has significant ethical implications.2
Veterans who are certified to use medical marijuana should present evidence of their registration, often a medical marijuana card, to their VA provider. The provider is then advised to ask the patient to sign a release of information to enable the VA practitioner to speak to the non-VA counterpart who is prescribing the medical marijuana. This approach respects the patient’s confidentiality and obtains informed consent for coordinated treatment. One limitation of this guidance is that it does not advise the practitioner how to proceed if the patient refuses to sign the release. The VA confidentiality regulations regarding substance use information are the strictest of all federal privacy laws. Under 38 USC 7332, this information cannot be released without the explicit written consent of the veteran in order to prevent stigma and discrimination.19 The ethical objective of this communication between VA and community practitioners is nonmaleficence and thus is focused on “adherence monitoring, treatment effectiveness, safety, and impact on cognitive, emotional, social and physical functioning, and side-effects.”20
Clinicians at VA are expected to know the dosage, frequency, and form of marijuana prescribed and the medical condition for which it is approved. The directive identifies but does not officially recognize as clinical indications for the use of medical marijuana a number of medical conditions for which marijuana is commonly prescribed—glaucoma, chemotherapy-induced nausea, multiple sclerosis, epilepsy, and chronic pain—but it is the specific state laws that determine what medical and psychiatric conditions are approved for the use of medical marijuana.16,21 The PCS clearly states that it is the VA clinician, presumptively the primary care provider (PCP), who is responsible for and directs the patient’s care, just as with any consultant or provider outside VA auspices. Some clinicians find this arrangement problematic, in that they may be potentially liable for bad outcomes and may not refuse a clinically reasonable request for opioids for chronic pain, yet are unable to control the secondary prescribing of marijuana. Clinicians with political, scientific, or moral objections to any use of marijuana for medical purpose may have little recourse under the policy, as there is no indication that such objections would fall under a conscience clause.
The use of medical marijuana is an area of intense research and cultural controversy, and the empirical data to support ethical refusal by a clinician to care for a patient using medical marijuana is often difficult to separate from social attitudes and political positions.22 The VA practitioner has a duty to “adjust treatment plans to promote effective management of these conditions” for which the veteran is using medical marijuana, such as offering adjunctive medications for pain or counseling for substance use.2
The VA clinician in the service of integrated care is required to document all clinical information regarding medical marijuana, including entering the substance as a non-VA prescription in the Computerized Patient Record System. This requirement is essential to protect the veteran from having necessary and appropriate care restricted if the results of toxicology screens are positive for marijuana. One gap in the guidance is that VA clinicians have no ready means of distinguishing prescribed marijuana from illegal marijuana in a standard toxicology screen, and if the patient has a state medical marijuana registration, the clinician must assume the source is prescribed and not illicit. Since the federal practitioner cannot prescribe marijuana, there is even more uncertainty and concern regarding a positive result. Laws passed in 2013 in Colorado and Washington states, which make the recreational use of medical marijuana legal, render toxicology interpretation and medical decision-making even more complex.23
The practitioner is directed to counsel and educate the patient from a nonjudgmental and beneficence-based orientation, which fosters the patient’s autonomy and informed consent. The VA clinician’s discussion of the evidence-base for the health benefits and risks of marijuana should include criteria for a marijuana substance use disorder, emerging data on marijuana withdrawal syndrome and empirical treatment, and most important effective alternative treatments for the target symptoms or conditions for which marijuana is being used.2
Along with this general guidance for the appropriate treatment of patients who use medical marijuana, specific advice is proffered on the 2 most strongly impacted areas of clinical care: pain management and substance use disorders. Practitioners on the ground struggle to reconcile the conflict between state and federal law and policy on medical marijuana in these 2 key domains. Ethics consultation is advised as potentially helpful in resolving ethical dilemmas that arise in patient care.
Pain Management
The PCS articulates the ethical principles surrounding chronic pain treatment with a focus on opioid prescribing for veterans approved to use medical marijuana. A multimodal and stepped-care approach to pain management is endorsed that “should be based on principles of shared medical decision-making and patient autonomy.”2 In this context, veteran safety and minimizing risk to the public are high priorities. Decisions about the use of opioid analgesics need to balance the veteran’s right to pain management and veteran well-being. The informed consent discussion regarding the use of opioids and marijuana should encompass benefits and risks of each substance and its interaction, especially those related to psychomotor impairment, such as driving and memory deficits, which could affect daily functioning. Practitioners are strongly advised to cogently record the clinical evaluation and treatment rationale for prescribing opioids to patients who use medical marijuana.2
Substance Use Disorders
It is the position of the American Society of Addiction Medicine that medical marijuana is not clinically appropriate for patients with substance use disorders.24 The VA policy clearly states that no veteran participating in a state-approved program will be denied substance use treatment or stigmatized for their use of medical marijuana, which is paradoxically a substance of abuse that is illegal in many states outside of these programs. Veterans being treated for other substance use disorders may also develop a marijuana use disorder, even if the drug is medically prescribed, or may concurrently use both legal and recreational marijuana. Just as the principle of justice requires patients who use medical marijuana are not denied participation in substance use treatment, so must veterans who develop abuse of marijuana have equal access to treatment when the addiction risks outweigh the health benefits of marijuana. Central to fairness is the identification of alternative treatments for the conditions for which marijuana is prescribed.2 Unfortunately, diagnosing a marijuana use disorder in a patient using the drug for medical purposes is neither easy nor clear.
There may also be situations in which appropriate use of medical marijuana may interfere with recovery from other substances of abuse, such as benzodiazepines or alcohol, or contravene employment of the optimal therapies for comorbid medical or psychiatric conditions, for example, other sedating psychoactive medications. Medical marijuana use could in theory lead a patient or other patients in a program to relapse to the substance of choice, although preliminary evidence suggests this may not necessarily be the case.25
Self-medication with medical marijuana for symptoms other than those for which the drug is approved may become an obstacle to efficacious treatment of other psychiatric problems. For instance, a veteran being treated for depression with cognitive behavioral therapy (CBT) may find the apathy chronic marijuana often induces to be an obstacle to the homework and activation exercises used in CBT.2
Patient-Physician Partnership
The nature of VA as a beneficiary health care system precludes the organization from denying VA services to veterans participating in state medical marijuana programs. However, the system does allow providers to make decisions to modify treatment plans on clinical grounds so long as those modifications are made in partnership with patients in accordance with VA’s emphasis on shared decision-making in medical care.
It should be noted that despite this emphasis, the autonomy of both patient and physician is legally and administratively circumscribed. If a clinician’s independent reading of the medical literature and professional judgment regarding the patient’s specific clinical circumstances determine medical marijuana is clinically indicated, the clinician is not free to communicate this recommendation to the patient without risking criminal prosecution or institutional sanctions. These considerations may weigh heavily on practitioners who think that medical marijuana would benefit patients, especially in states where it is legally available.
Conversely, patients residing in states with medical marijuana laws who believe the substance would relieve their symptoms can seek out a community provider to assist them in obtaining registration. However, patients’ self-determination is limited in that they do not have the choice to have their PCP, who presumably is most familiar with their medical history, recommend or prescribe medical marijuana. Veterans also are not permitted to use VA pharmacy benefits to have VA pharmacists fill the prescription.
This is a clear statement of the limit of veteran entitlement: VA will not pay for medical marijuana. No exception is made if the veteran is using medical marijuana to treat service-connected injuries or illnesses. Directive 2010-035 (now rescinded) and the original VA OGC opinion assert that medical marijuana does not meet criteria as a core health benefit that VHA as an entitlement program must provide as an aspect of basic care.5,20 The justification for this exclusion is that non-Food and Drug Administration (FDA) approved drugs are not encompassed in the medical benefits package outside either an Investigational New Drug Application or compassionate use FDA provision. Veterans may experience this as a social justice issue and a violation of the VA fiduciary duty to its beneficiaries. A sharp demarcation is made between the private use and public possession of marijuana. Veterans who carry marijuana on VA property, even if they are certified to carry medical marijuana, will be prosecuted under CSA.
Conclusion
Studies estimate that 50% of veterans experience chronic pain, and nearly half of these patients receive prescription opioids.26 Conversely, up to 35% of VA patients are diagnosed with both substance use and mental health disorders.27
The one aspect of the controversy that stakeholders on the pro and con sides of the medical marijuana question agree on is the need for more empirical data.28 There is an urgent need for more study of the use of medical marijuana as a treatment for posttraumatic stress disorder, which is a qualifying health condition in a growing number of states.29
Along with federal law, it is federal agencies, including the DEA, FDA, and the National Institute on Drug Abuse, that may be the biggest obstacle to conducting this vital research.30 These regulatory obstacles must be removed before researchers can conduct the scientific studies needed to provide a factual foundation to inform what has too often been a political debate. Solid science grounding legal reform and shaping public policy toward medical marijuana may be the only means of resolving the ethical dilemmas that confront veterans daily and the VA clinicians committed to caring for them.31,32
In the interim, VA practitioners should be provided effective training in educating and counseling patients about the implications of VA policy regarding state-approved medical marijuana programs for their individual health care. Such a patient-centered approach represents the most ethically acceptable means of mediating the conflict between state and federal law regarding medical marijuana in its current stage of evolution.
Author disclosures
The author reports no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the author and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
References
1. State Medical Marijuana Laws. National Conference of State Legislators Website. http://www.ncsl.org/issues-research/health/state-medical-marijuana-laws.aspx. Updated January 2014. Accessed February 1, 2014.
2. Veterans Health Administration. Clinical Considerations Regarding Veteran Patients Who Participate in State-Approved Medical Marijuana Programs. Washington, DC: Department of Veterans Affairs; 2010.
3. The Associated Press. Supreme Court is set to consider medical marijuana. New York Times. November 28, 2004. http://www.nytimes.com/2004/11/28/politics/28marijuana.html?fta=y. Accessed February 5, 2014.
4. Dresser R. Irrational basis: The legal status of medical marijuana. Hastings Cent Rep. 2009;39(6):7-8.
5. Office of General Counsel. Opinion on State Medical Marijuana Registration Forms. Washington, DC: Department of Veterans Affairs; 2008. VAOPGCADV 9-2008.
6. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part one of two. J Pain Palliat Care Pharmacother. 2009;23(1):4-25.
7. Pearson v McCaffrey, 139 F Supp 2d 772 (D DC 2001).
8. Constitution of the United States. United States Senate Website. http://www.senate.gov/civics/constitution_item/constitution.htm. Accessed January 22, 2012.
9. White BD. New York, NY: Informa Healthcare; 2007.
10. Conant v Walters, 309 F3d 629 (9th Cir 2002).
11. Gonzales v Raich, 545 US 1, 125 SCt, 2195 (2005).
12. United States v Lopez, 514 US 549, 115 SCt, 1624 (1995).
13. United States v Morrison, 529 US 598, 120 SCt, 1740 (2000).
14. The Lynn and Erin Compassionate Use Act, NMSA 1978 §26-2B (2007).
15. Frosch D. V.A. Easing rules for users of medical marijuana. New York Times. July 24, 2010:A1.
16. Medical Marijuana. Washington, DC: Dept of Veterans Affairs; 2010. VHA Directive 2010-035.
17. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
18. Uniform Code of Military Justice, 10 USC § 912A (2011).
19. Confidentiality of Certain Medical Records, 38 USC § 7332 (1991).
20. Petzel RA. Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs. Washington, DC: Dept of Veterans Affairs; 2011. VHA Directive 2011-004.
21. Institute of Medicine. Marijuana and Medicine: Assessing the Science. Joy JE, Watson SJ Jr, Benson JA Jr, eds. Washington, DC: National Academy Press; 1999.
22. Charuvastra A, Friedmann PD, Stein MD. Physician attitudes regarding the prescription of medical marijuana. J Addict Dis. 2005;24(3):87-93.
23. Healy J. Up early and in line for a medical marijuana milestone in Colorado. New York Times. January 1, 2014:A1.
24. Public Policy Statement on Medical Marijuana. Chevy Chase, MD: American Society of Addiction Medicine; 2010.
25. Swartz R. Medical marijuana users in substance abuse treatment. Harm Reduct J. 2010;7:3.
26. Clark JD. Chronic pain prevalence and analgesic prescribing in a general medical population. J Pain Symptom Manage. 2002;23(2):131-137.
27. Petrakis IL, Rosenheck R, Desai R. Substance use comorbidity among veterans with posttraumatic stress disorder and other psychiatric illness. Am J Addict. 2011;20(3):185-189.
28. Medical Marijuana. ProCon.org Website. http://medicalmarijuana.procon.org. Updated February 3, 2014. Accessed February 5, 2014.
29. Busemeyer D. Cannabis catch-22. Santa Fe New Mexican. October 14, 2012:A1, A4-A5.
30. Harris G. Researchers find study of medical marijuana discouraged. New York Times. January 18, 2010:A14.
31. Cohen PJ. Medical marijuana: The conflict between scientific evidence and political ideology. Part two of two. J Pain Palliat Care Pharmacother. 2009;23(2):120-140.
32. Daigle L. Medical Marijuana. Bethesda, MD: American Society of Health-System Pharmacists; 2011.
