User login
While febrile seizures are common in early childhood and generally benign, prolonged febrile seizures of 30 minutes or longer have been associated with a greatly increased risk of later epilepsy, particularly temporal lobe epilepsy.
To better understand the pathogenesis of epilepsy among children presenting with febrile status epilepticus (FSE) and to guide the development of interventions that could prevent it following a first episode of FSE, a group of clinical researchers has been working with a cohort of 199 children aged 1 month to 6 years (median age, 15.8 months) who presented with FSE between 2003 and 2010.
The study, being conducted at five clinical sites in the United States under funding from the National Institutes of Health (NIH), is designed with a considerable follow-up, with data collection planned for 1, 5, 10, and 15 years after the initial acute episode.
But even with the first-year results yet to be published, the Consequences of Prolonged Febrile Seizures in Childhood, or FEBSTAT, study has already generated some important findings.
Human herpes viruses 6 and 7 are strongly associated with FSE, the FEBSTAT team revealed this June, with HHV-6b or 7 infections occurring in 32% of 169 children in the cohort (Epilepsia 2012;53:1481-8). Whether there is a relationship between HHV infection at baseline and subsequent epilepsy will take years to establish.
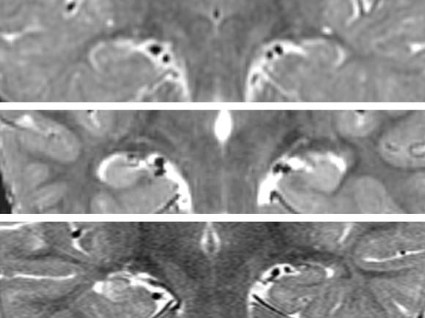
In July, the FEBSTAT investigators published results of a study showing that 11.5% of 191 children in the cohort had MRI (magnetic resonance imaging) evidence of an acute injury to one hippocampus following FSE (Neurology 2012;79:871-7), compared with none in a control group of children presenting with benign febrile seizures. A substantial number of cases also had developmental abnormalities of the hippocampus (10.5%); but some children in the control group also had abnormalities (2.1%).
In November, the researchers revealed that of acute EEG findings following FSE, 45.2% were abnormal, with the most common abnormality being focal slowing or attenuation. Epileptiform abnormalities also were seen in 6.5% of the full cohort of 199 children (Neurology 2012 Nov. 7 [doi: 10.1212/WNL.0b013e3182759766]). The EEG findings are highly associated with MRI evidence of acute hippocampal injury, and may also reveal injuries too subtle to be picked up by MRI imaging.
FEBSTAT principal investigator Dr. Shlomo Shinnar, professor of neurology, pediatrics, and epidemiology at Montefiore Medical Center and Albert Einstein College of Medicine in New York, said in an interview that MRI and EEG are used in tandem to offer the most complete picture possible.
"Sometimes the EEG will show you’re evolving into epilepsy when the MRI doesn’t; sometimes the MRI will show changes before the EEG. We want multimodal assessments, so whenever we do an MRI we do an EEG. EEG is noninvasive and minimal risk; it turns out to be quite predictive and it is very easy to get."
At this point in the FEBSTAT study, the MRI and EEG study results cannot fully clarify whether FSE results in damage to the hippocampus and later epilepsy, or whether children with hippocampal abnormalities are more likely to present with FSE. However, it is already clear that while children with hippocampal abnormalities may be more susceptible to prolonged febrile seizure, these can result in acute injury.
The researchers conduct MRIs and EEGs on all subjects at the predetermined follow-up points, which will help reveal evidence of injuries or abnormalities that may have been undetectable at baseline. At 5 years, investigators collect extensive data on cognition, memory, executive function, attention, and behavior and psychiatric morbidity, in addition to imaging. "Our hypothesis is that when 5-year follow-up data are complete, kids with smaller hippocampi will have memory impairment," said Dr. Shinnar, lead author on the MRI study and coauthor on the EEG and HHV studies.
Dr. Shinnar said that one goal of the prospective cohort study is to identify biomarkers that will be useful in indicating preventive therapies for the children most at risk. Right now, he said, prophylaxis would be limited to antiseizure drugs; however, "the hope is that if we can identify that if you have this MRI or that EEG and are determined to be at high risk, you can find some agent that you can give for a couple weeks and prevent the development of epilepsy."

"The NIH has just funded a planning grant in which they’re testing agents in animals to prevent epileptogenesis," Dr. Shinnar said. "We are going to provide them some data from FEBSTAT to assist the modeling. There is a lot of interest in developing an agent that will prevent epilepsy, but of the candidate agents, none has so far passed muster."
The HHV study offered another clue to a potential route of intervention. HHV-6b and HHV-7, both found to be common in FSE, have potential for reactivation after primary infection. Evidence of infection with HHV-6b or HHV-7 was present in 85% of the cohort, with viremia in 32%.
What the FEBSTAT team still doesn’t know, Dr. Shinnar said, "is whether HHV-6b is a common cause of high fever in young children and therefore of febrile status, but that nothing about it could cause further epilepsy down the road; or whether it is a common cause of fever but because of the properties of virus is more likely to cause you to have status. We’re adequately powered to answer these questions, but you’ll have to tune in 10 years from now." A long-term aim of the FEBSTAT study is to determine whether FSE due to HHV-6 or HHV-7 infection is more likely to result in hippocampal injury, hippocampal sclerosis, and temporal lobe epilepsy than FSE without HHV-6 or HHV-7 infection.
The long follow-up of the cohort, which is powered to withstand some attrition over time, should prove one of its greatest strengths. The first 10-year data will be collected next year, and hopefully will reveal even more about the role of hippocampal injury, hippocampal abnormality, and HHV-6b and 7 in the pathogenesis of epilepsy.
"God and NIH willing," Dr. Shinnar said, he’ll be around for the 15-year results, by which time many of his earliest recruits will be headed off to college.
Dr. Shinnar disclosed past service on an advisory board for King Pharmaceuticals, and past financial relationships with Questcor, Sunovion, Eisai, Neuronex, and UCB. Several of Dr. Shinnar’s coinvestigators on the EEG and MRI studies also disclosed past and ongoing financial relationships with pharmaceutical manufacturers.
Dr. Yu-Tze Ng comments: The FEBSTAT study team should be congratulated for working their way toward determining the acute and long-term consequences of FSE in childhood. Their preliminary results for MRI scans and EEGs possibly performed in the post-ictal period (within 72 hours of the FSE episode) suggest the evolution of mesial temporal sclerosis (MTS) in a small but significant number of affected children. To date, 17 (8.5%) children had definitely abnormal T2 signal in the hippocampus and a further 5 (2.5%) had equivocal findings. Significant focal non-epileptiform findings were seen in 60 (30.2%) acute EEGs. Perhaps not unexpectedly, epileptiform discharges were noted in only 13 (6.5%) tracings. It will be of particular interest to watch the (possibly expected) evolution of more MTS cases from this cohort of patients. However, that may be offset with expected normalization of many of the EEGs and also possible resolution of MRI T2 signal changes, some of which may simply have been (sub-)acute post-ictal findings.
To date, PubMed reveals eight major publications related to FEBSTAT.
Besides examining post-ictal MRI and EEG results, other issues being studied include the association between FSE and human herpesvirus (HHV) 6 and 7 infections, although it is a long way from being proved causative. About one-third of the children in the study had HHV infection: predominantly HHV-6b, less frequently HHV-7, and none with HHV-6a. Possibly more significant was the FEBSTAT group’s recent finding that 136 children with FSE who underwent lumbar puncture had essentially normal cerebrospinal fluid results without pleocytosis (J. Pediatr. 2012 Sept. 14 [doi:10.1016/j.jpeds.2012.08.008]). Hence, caregivers should not ignore a "positive" lumbar puncture result in a patient with FSE.
There are a few clinical and pragmatic limitations to the conclusions that can be drawn so far. The FEBSTAT study is predominantly concentrating on patients with FSE, not those with simple febrile seizures. Although febrile seizures may affect nearly 1 in 20 children, less than a third (and probably closer to only 10%-20%) have complex febrile seizures. Hence, for current and future extrapolations, the majority of practitioners will probably not be fully aware of this very significant difference in the subset group of patients who are being studied.
Although temporal lobe epilepsy (TLE) is the commonest form of adult epilepsy, and MTS is found predominantly in refractory TLE patients, only a minority of these patients report having had febrile seizures and nearly always the subtle distinction of FSE is not made.
The authors also acknowledge that it remains to be proven that some of these findings are incidental and not causative (pre-FSE MRIs were not available), because MTS in children certainly exists (J. Child Neurol. 2006;21:512-7).
We await further results from this cohort of FSE patients.
It is possible that more questions rather than answers may arise. The next major step will be to try to develop preventive interventions for febrile seizures and TLE from the information gathered.
Yu-Tze Ng, M.D., is director of epilepsy and chair of child neurology at the University of Oklahoma Health Sciences Center, Oklahoma City. He serves on the scientific advisory board for Lundbeck and receives honoraria for speaking engagements or educational activities from Lundbeck, UCB Pharma, and Cyberonics. He is not involved in the FEBSTAT study.
Dr. Yu-Tze Ng comments: The FEBSTAT study team should be congratulated for working their way toward determining the acute and long-term consequences of FSE in childhood. Their preliminary results for MRI scans and EEGs possibly performed in the post-ictal period (within 72 hours of the FSE episode) suggest the evolution of mesial temporal sclerosis (MTS) in a small but significant number of affected children. To date, 17 (8.5%) children had definitely abnormal T2 signal in the hippocampus and a further 5 (2.5%) had equivocal findings. Significant focal non-epileptiform findings were seen in 60 (30.2%) acute EEGs. Perhaps not unexpectedly, epileptiform discharges were noted in only 13 (6.5%) tracings. It will be of particular interest to watch the (possibly expected) evolution of more MTS cases from this cohort of patients. However, that may be offset with expected normalization of many of the EEGs and also possible resolution of MRI T2 signal changes, some of which may simply have been (sub-)acute post-ictal findings.
To date, PubMed reveals eight major publications related to FEBSTAT.
Besides examining post-ictal MRI and EEG results, other issues being studied include the association between FSE and human herpesvirus (HHV) 6 and 7 infections, although it is a long way from being proved causative. About one-third of the children in the study had HHV infection: predominantly HHV-6b, less frequently HHV-7, and none with HHV-6a. Possibly more significant was the FEBSTAT group’s recent finding that 136 children with FSE who underwent lumbar puncture had essentially normal cerebrospinal fluid results without pleocytosis (J. Pediatr. 2012 Sept. 14 [doi:10.1016/j.jpeds.2012.08.008]). Hence, caregivers should not ignore a "positive" lumbar puncture result in a patient with FSE.
There are a few clinical and pragmatic limitations to the conclusions that can be drawn so far. The FEBSTAT study is predominantly concentrating on patients with FSE, not those with simple febrile seizures. Although febrile seizures may affect nearly 1 in 20 children, less than a third (and probably closer to only 10%-20%) have complex febrile seizures. Hence, for current and future extrapolations, the majority of practitioners will probably not be fully aware of this very significant difference in the subset group of patients who are being studied.
Although temporal lobe epilepsy (TLE) is the commonest form of adult epilepsy, and MTS is found predominantly in refractory TLE patients, only a minority of these patients report having had febrile seizures and nearly always the subtle distinction of FSE is not made.
The authors also acknowledge that it remains to be proven that some of these findings are incidental and not causative (pre-FSE MRIs were not available), because MTS in children certainly exists (J. Child Neurol. 2006;21:512-7).
We await further results from this cohort of FSE patients.
It is possible that more questions rather than answers may arise. The next major step will be to try to develop preventive interventions for febrile seizures and TLE from the information gathered.
Yu-Tze Ng, M.D., is director of epilepsy and chair of child neurology at the University of Oklahoma Health Sciences Center, Oklahoma City. He serves on the scientific advisory board for Lundbeck and receives honoraria for speaking engagements or educational activities from Lundbeck, UCB Pharma, and Cyberonics. He is not involved in the FEBSTAT study.
Dr. Yu-Tze Ng comments: The FEBSTAT study team should be congratulated for working their way toward determining the acute and long-term consequences of FSE in childhood. Their preliminary results for MRI scans and EEGs possibly performed in the post-ictal period (within 72 hours of the FSE episode) suggest the evolution of mesial temporal sclerosis (MTS) in a small but significant number of affected children. To date, 17 (8.5%) children had definitely abnormal T2 signal in the hippocampus and a further 5 (2.5%) had equivocal findings. Significant focal non-epileptiform findings were seen in 60 (30.2%) acute EEGs. Perhaps not unexpectedly, epileptiform discharges were noted in only 13 (6.5%) tracings. It will be of particular interest to watch the (possibly expected) evolution of more MTS cases from this cohort of patients. However, that may be offset with expected normalization of many of the EEGs and also possible resolution of MRI T2 signal changes, some of which may simply have been (sub-)acute post-ictal findings.
To date, PubMed reveals eight major publications related to FEBSTAT.
Besides examining post-ictal MRI and EEG results, other issues being studied include the association between FSE and human herpesvirus (HHV) 6 and 7 infections, although it is a long way from being proved causative. About one-third of the children in the study had HHV infection: predominantly HHV-6b, less frequently HHV-7, and none with HHV-6a. Possibly more significant was the FEBSTAT group’s recent finding that 136 children with FSE who underwent lumbar puncture had essentially normal cerebrospinal fluid results without pleocytosis (J. Pediatr. 2012 Sept. 14 [doi:10.1016/j.jpeds.2012.08.008]). Hence, caregivers should not ignore a "positive" lumbar puncture result in a patient with FSE.
There are a few clinical and pragmatic limitations to the conclusions that can be drawn so far. The FEBSTAT study is predominantly concentrating on patients with FSE, not those with simple febrile seizures. Although febrile seizures may affect nearly 1 in 20 children, less than a third (and probably closer to only 10%-20%) have complex febrile seizures. Hence, for current and future extrapolations, the majority of practitioners will probably not be fully aware of this very significant difference in the subset group of patients who are being studied.
Although temporal lobe epilepsy (TLE) is the commonest form of adult epilepsy, and MTS is found predominantly in refractory TLE patients, only a minority of these patients report having had febrile seizures and nearly always the subtle distinction of FSE is not made.
The authors also acknowledge that it remains to be proven that some of these findings are incidental and not causative (pre-FSE MRIs were not available), because MTS in children certainly exists (J. Child Neurol. 2006;21:512-7).
We await further results from this cohort of FSE patients.
It is possible that more questions rather than answers may arise. The next major step will be to try to develop preventive interventions for febrile seizures and TLE from the information gathered.
Yu-Tze Ng, M.D., is director of epilepsy and chair of child neurology at the University of Oklahoma Health Sciences Center, Oklahoma City. He serves on the scientific advisory board for Lundbeck and receives honoraria for speaking engagements or educational activities from Lundbeck, UCB Pharma, and Cyberonics. He is not involved in the FEBSTAT study.
While febrile seizures are common in early childhood and generally benign, prolonged febrile seizures of 30 minutes or longer have been associated with a greatly increased risk of later epilepsy, particularly temporal lobe epilepsy.
To better understand the pathogenesis of epilepsy among children presenting with febrile status epilepticus (FSE) and to guide the development of interventions that could prevent it following a first episode of FSE, a group of clinical researchers has been working with a cohort of 199 children aged 1 month to 6 years (median age, 15.8 months) who presented with FSE between 2003 and 2010.
The study, being conducted at five clinical sites in the United States under funding from the National Institutes of Health (NIH), is designed with a considerable follow-up, with data collection planned for 1, 5, 10, and 15 years after the initial acute episode.
But even with the first-year results yet to be published, the Consequences of Prolonged Febrile Seizures in Childhood, or FEBSTAT, study has already generated some important findings.
Human herpes viruses 6 and 7 are strongly associated with FSE, the FEBSTAT team revealed this June, with HHV-6b or 7 infections occurring in 32% of 169 children in the cohort (Epilepsia 2012;53:1481-8). Whether there is a relationship between HHV infection at baseline and subsequent epilepsy will take years to establish.
In July, the FEBSTAT investigators published results of a study showing that 11.5% of 191 children in the cohort had MRI (magnetic resonance imaging) evidence of an acute injury to one hippocampus following FSE (Neurology 2012;79:871-7), compared with none in a control group of children presenting with benign febrile seizures. A substantial number of cases also had developmental abnormalities of the hippocampus (10.5%); but some children in the control group also had abnormalities (2.1%).
In November, the researchers revealed that of acute EEG findings following FSE, 45.2% were abnormal, with the most common abnormality being focal slowing or attenuation. Epileptiform abnormalities also were seen in 6.5% of the full cohort of 199 children (Neurology 2012 Nov. 7 [doi: 10.1212/WNL.0b013e3182759766]). The EEG findings are highly associated with MRI evidence of acute hippocampal injury, and may also reveal injuries too subtle to be picked up by MRI imaging.
FEBSTAT principal investigator Dr. Shlomo Shinnar, professor of neurology, pediatrics, and epidemiology at Montefiore Medical Center and Albert Einstein College of Medicine in New York, said in an interview that MRI and EEG are used in tandem to offer the most complete picture possible.
"Sometimes the EEG will show you’re evolving into epilepsy when the MRI doesn’t; sometimes the MRI will show changes before the EEG. We want multimodal assessments, so whenever we do an MRI we do an EEG. EEG is noninvasive and minimal risk; it turns out to be quite predictive and it is very easy to get."
At this point in the FEBSTAT study, the MRI and EEG study results cannot fully clarify whether FSE results in damage to the hippocampus and later epilepsy, or whether children with hippocampal abnormalities are more likely to present with FSE. However, it is already clear that while children with hippocampal abnormalities may be more susceptible to prolonged febrile seizure, these can result in acute injury.
The researchers conduct MRIs and EEGs on all subjects at the predetermined follow-up points, which will help reveal evidence of injuries or abnormalities that may have been undetectable at baseline. At 5 years, investigators collect extensive data on cognition, memory, executive function, attention, and behavior and psychiatric morbidity, in addition to imaging. "Our hypothesis is that when 5-year follow-up data are complete, kids with smaller hippocampi will have memory impairment," said Dr. Shinnar, lead author on the MRI study and coauthor on the EEG and HHV studies.
Dr. Shinnar said that one goal of the prospective cohort study is to identify biomarkers that will be useful in indicating preventive therapies for the children most at risk. Right now, he said, prophylaxis would be limited to antiseizure drugs; however, "the hope is that if we can identify that if you have this MRI or that EEG and are determined to be at high risk, you can find some agent that you can give for a couple weeks and prevent the development of epilepsy."
"The NIH has just funded a planning grant in which they’re testing agents in animals to prevent epileptogenesis," Dr. Shinnar said. "We are going to provide them some data from FEBSTAT to assist the modeling. There is a lot of interest in developing an agent that will prevent epilepsy, but of the candidate agents, none has so far passed muster."
The HHV study offered another clue to a potential route of intervention. HHV-6b and HHV-7, both found to be common in FSE, have potential for reactivation after primary infection. Evidence of infection with HHV-6b or HHV-7 was present in 85% of the cohort, with viremia in 32%.
What the FEBSTAT team still doesn’t know, Dr. Shinnar said, "is whether HHV-6b is a common cause of high fever in young children and therefore of febrile status, but that nothing about it could cause further epilepsy down the road; or whether it is a common cause of fever but because of the properties of virus is more likely to cause you to have status. We’re adequately powered to answer these questions, but you’ll have to tune in 10 years from now." A long-term aim of the FEBSTAT study is to determine whether FSE due to HHV-6 or HHV-7 infection is more likely to result in hippocampal injury, hippocampal sclerosis, and temporal lobe epilepsy than FSE without HHV-6 or HHV-7 infection.
The long follow-up of the cohort, which is powered to withstand some attrition over time, should prove one of its greatest strengths. The first 10-year data will be collected next year, and hopefully will reveal even more about the role of hippocampal injury, hippocampal abnormality, and HHV-6b and 7 in the pathogenesis of epilepsy.
"God and NIH willing," Dr. Shinnar said, he’ll be around for the 15-year results, by which time many of his earliest recruits will be headed off to college.
Dr. Shinnar disclosed past service on an advisory board for King Pharmaceuticals, and past financial relationships with Questcor, Sunovion, Eisai, Neuronex, and UCB. Several of Dr. Shinnar’s coinvestigators on the EEG and MRI studies also disclosed past and ongoing financial relationships with pharmaceutical manufacturers.
While febrile seizures are common in early childhood and generally benign, prolonged febrile seizures of 30 minutes or longer have been associated with a greatly increased risk of later epilepsy, particularly temporal lobe epilepsy.
To better understand the pathogenesis of epilepsy among children presenting with febrile status epilepticus (FSE) and to guide the development of interventions that could prevent it following a first episode of FSE, a group of clinical researchers has been working with a cohort of 199 children aged 1 month to 6 years (median age, 15.8 months) who presented with FSE between 2003 and 2010.
The study, being conducted at five clinical sites in the United States under funding from the National Institutes of Health (NIH), is designed with a considerable follow-up, with data collection planned for 1, 5, 10, and 15 years after the initial acute episode.
But even with the first-year results yet to be published, the Consequences of Prolonged Febrile Seizures in Childhood, or FEBSTAT, study has already generated some important findings.
Human herpes viruses 6 and 7 are strongly associated with FSE, the FEBSTAT team revealed this June, with HHV-6b or 7 infections occurring in 32% of 169 children in the cohort (Epilepsia 2012;53:1481-8). Whether there is a relationship between HHV infection at baseline and subsequent epilepsy will take years to establish.
In July, the FEBSTAT investigators published results of a study showing that 11.5% of 191 children in the cohort had MRI (magnetic resonance imaging) evidence of an acute injury to one hippocampus following FSE (Neurology 2012;79:871-7), compared with none in a control group of children presenting with benign febrile seizures. A substantial number of cases also had developmental abnormalities of the hippocampus (10.5%); but some children in the control group also had abnormalities (2.1%).
In November, the researchers revealed that of acute EEG findings following FSE, 45.2% were abnormal, with the most common abnormality being focal slowing or attenuation. Epileptiform abnormalities also were seen in 6.5% of the full cohort of 199 children (Neurology 2012 Nov. 7 [doi: 10.1212/WNL.0b013e3182759766]). The EEG findings are highly associated with MRI evidence of acute hippocampal injury, and may also reveal injuries too subtle to be picked up by MRI imaging.
FEBSTAT principal investigator Dr. Shlomo Shinnar, professor of neurology, pediatrics, and epidemiology at Montefiore Medical Center and Albert Einstein College of Medicine in New York, said in an interview that MRI and EEG are used in tandem to offer the most complete picture possible.
"Sometimes the EEG will show you’re evolving into epilepsy when the MRI doesn’t; sometimes the MRI will show changes before the EEG. We want multimodal assessments, so whenever we do an MRI we do an EEG. EEG is noninvasive and minimal risk; it turns out to be quite predictive and it is very easy to get."
At this point in the FEBSTAT study, the MRI and EEG study results cannot fully clarify whether FSE results in damage to the hippocampus and later epilepsy, or whether children with hippocampal abnormalities are more likely to present with FSE. However, it is already clear that while children with hippocampal abnormalities may be more susceptible to prolonged febrile seizure, these can result in acute injury.
The researchers conduct MRIs and EEGs on all subjects at the predetermined follow-up points, which will help reveal evidence of injuries or abnormalities that may have been undetectable at baseline. At 5 years, investigators collect extensive data on cognition, memory, executive function, attention, and behavior and psychiatric morbidity, in addition to imaging. "Our hypothesis is that when 5-year follow-up data are complete, kids with smaller hippocampi will have memory impairment," said Dr. Shinnar, lead author on the MRI study and coauthor on the EEG and HHV studies.
Dr. Shinnar said that one goal of the prospective cohort study is to identify biomarkers that will be useful in indicating preventive therapies for the children most at risk. Right now, he said, prophylaxis would be limited to antiseizure drugs; however, "the hope is that if we can identify that if you have this MRI or that EEG and are determined to be at high risk, you can find some agent that you can give for a couple weeks and prevent the development of epilepsy."
"The NIH has just funded a planning grant in which they’re testing agents in animals to prevent epileptogenesis," Dr. Shinnar said. "We are going to provide them some data from FEBSTAT to assist the modeling. There is a lot of interest in developing an agent that will prevent epilepsy, but of the candidate agents, none has so far passed muster."
The HHV study offered another clue to a potential route of intervention. HHV-6b and HHV-7, both found to be common in FSE, have potential for reactivation after primary infection. Evidence of infection with HHV-6b or HHV-7 was present in 85% of the cohort, with viremia in 32%.
What the FEBSTAT team still doesn’t know, Dr. Shinnar said, "is whether HHV-6b is a common cause of high fever in young children and therefore of febrile status, but that nothing about it could cause further epilepsy down the road; or whether it is a common cause of fever but because of the properties of virus is more likely to cause you to have status. We’re adequately powered to answer these questions, but you’ll have to tune in 10 years from now." A long-term aim of the FEBSTAT study is to determine whether FSE due to HHV-6 or HHV-7 infection is more likely to result in hippocampal injury, hippocampal sclerosis, and temporal lobe epilepsy than FSE without HHV-6 or HHV-7 infection.
The long follow-up of the cohort, which is powered to withstand some attrition over time, should prove one of its greatest strengths. The first 10-year data will be collected next year, and hopefully will reveal even more about the role of hippocampal injury, hippocampal abnormality, and HHV-6b and 7 in the pathogenesis of epilepsy.
"God and NIH willing," Dr. Shinnar said, he’ll be around for the 15-year results, by which time many of his earliest recruits will be headed off to college.
Dr. Shinnar disclosed past service on an advisory board for King Pharmaceuticals, and past financial relationships with Questcor, Sunovion, Eisai, Neuronex, and UCB. Several of Dr. Shinnar’s coinvestigators on the EEG and MRI studies also disclosed past and ongoing financial relationships with pharmaceutical manufacturers.