User login
Blepharoplasty, or surgical manipulation of the upper and/or lower eyelids, is a commonly performed cosmetic procedure to improve the appearance and function of the eyelids by repositioning and/or removing excess skin and soft tissue from the eyelids, most often through external incisions that minimize scarring and maximize the aesthetic outcomes of the surgery. Therefore, the placement of the incisions is an important determinant of the surgical outcome, and the preoperative marking of the eyelids to indicate where the incisions should be placed is a crucial part of preparation for the surgery.
Preoperative marking has unique challenges due to the dynamicity of the eyelids and the delicate nature of the surgery. The mark must be narrow to minimize the risk of placing the incision higher or lower than intended. The mark also must dry quickly because the patient may blink and create multiple impressions of the marking on skinfolds in contact with the wet ink. Fast drying of the ink used to create the marks improves the efficiency and clarity of the presurgical planning.
We present data on the performance of the various blepharoplasty markers regarding drying time and ink spread width based on an evaluation of 13 surgical markers.
Methods
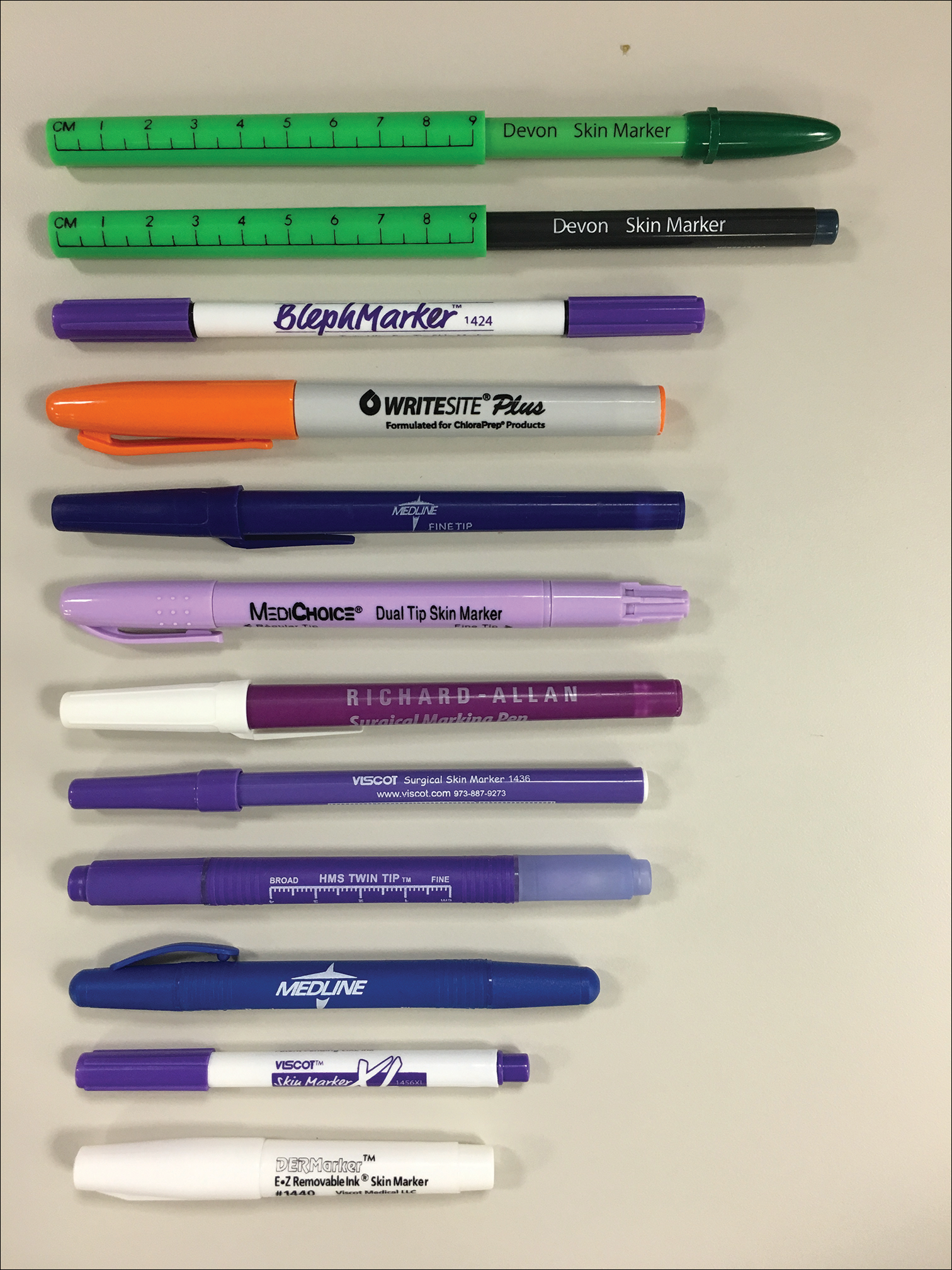
Eleven unique fine tip (FT) markers and 2 standard tip (ST) markers were obtained based on their accessibility at the researchers’ home institution and availability for direct purchase in small quantities from the distributors (Figure 1). Four markers were double tipped with one FT end and one ST end; for these markers, only the FT end was studied. The experiments were conducted on the bilateral upper eyelids and on hairless patches of skin of a single patient in a minor procedure room with surgical lighting and minimal draft of air. The sole experimenter (J.M.K.) conducting the study was not blinded.
The drying time of each marker was measured by marking 1-in lines on a patch of hairless skin that was first cleaned with an alcohol pad, then dried. Drying time for each marking was measured in increments of 5 seconds; at each time point, the markings were wiped with a single-ply, light-duty tissue under the weight of 10 US quarters to ensure that the same weight/pressure was applied when wiping the skin. Smudges observed with the naked eye on either the wipe or the patients’ skin were interpreted as nondry status of the marking. The first time point at which a marking was found to have no visible smudges either on the skin or the wipe was recorded as the drying time of the respective marker.
Ink spread was measured on clean eyelid skin by drawing curved lines along the natural crease as would be done for actual blepharoplasty planning. Each line was allowed to dry for 2 minutes. The greatest perpendicular spread width along the line observed with the naked eye was measured using a digital Vernier caliper with 0.01-mm graduations. Three measurements were obtained per marker and the values averaged to arrive at the final spread width.
Results
Drying time among the 13 total markers (11 FT and 2 ST) ranged from 5 to 70 seconds, with a mean of 20.8 seconds and median of 5 seconds (Table). The drying time for the DERMarker E-Z Removable Ink Mini Skin Marker (Delasco, LLC) with an ST was 5 seconds, while the drying time for the other ST marker, WriteSite Plus Surgical Skin Marker (Aspen Surgical, Inc), was 70 seconds. The FT markers spanned the entire range of drying times. The ink spread width among the markers ranged from 0.53 to 2.27 mm with a median of 0.9 mm and mean of 1.13 mm (Table). The 2 ST markers were found to make some of the widest marks measured, including the WriteSite Plus Surgical Skin Marker, a nonsterile ST marker that created the widest ink marks. The second widest mark was made by an FT marker (Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker [Viscot Medical, LLC]).
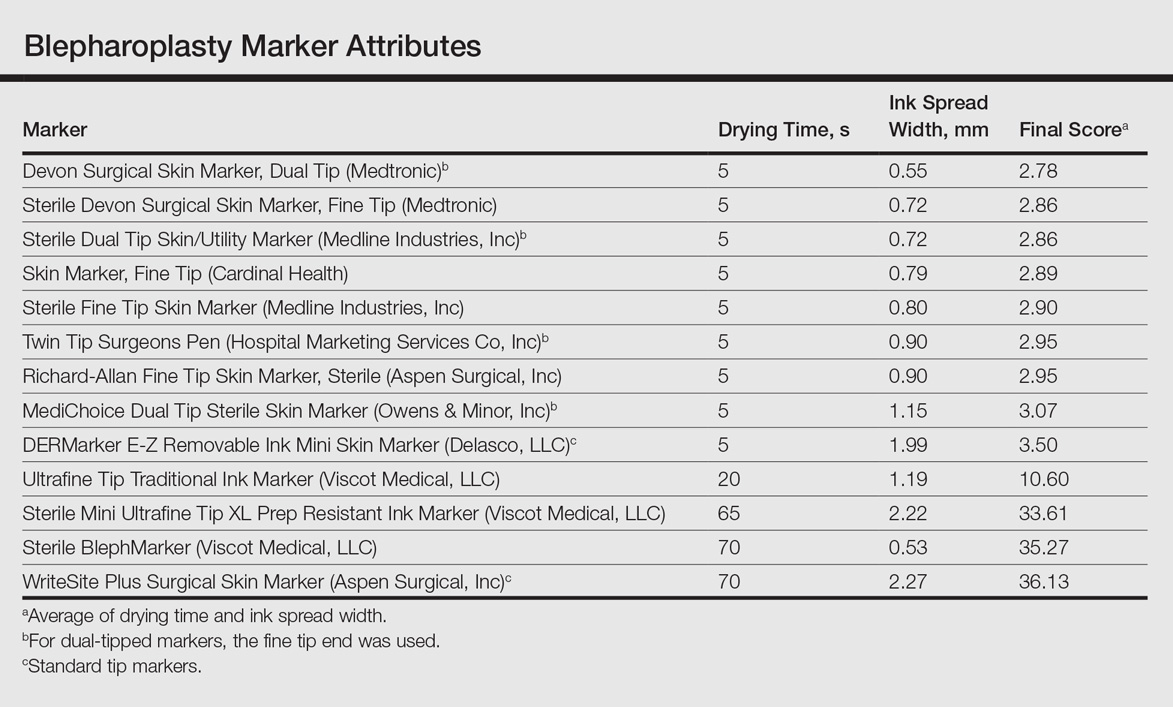
To prioritize short drying time coupled with minimal ink spread width, the values associated with each marker were averaged to arrive at the overall score for each marker. The smaller the overall score, the higher we ranked the marker. The Devon Surgical Skin Marker, Dual Tip (Medtronic) ranked the highest among the 13 markers with a final score of 2.78. Runner-up markers included the Sterile Devon Surgical Skin marker, Fine Tip (Medtronic)(final score, 2.86); the Sterile Dual Tip Skin/Utility Marker (Medline Industries, Inc)(final score, 2.86); and the Skin Marker, Fine Tip (Cardinal Health)(final score, 2.89). The 2 lowest-ranking markers were the WriteSite Plus Surgical Skin Marker, an ST marker (final score, 36.13), followed by the Sterile BlephMarker (Viscot Medical, LLC)(final score, 35.27).
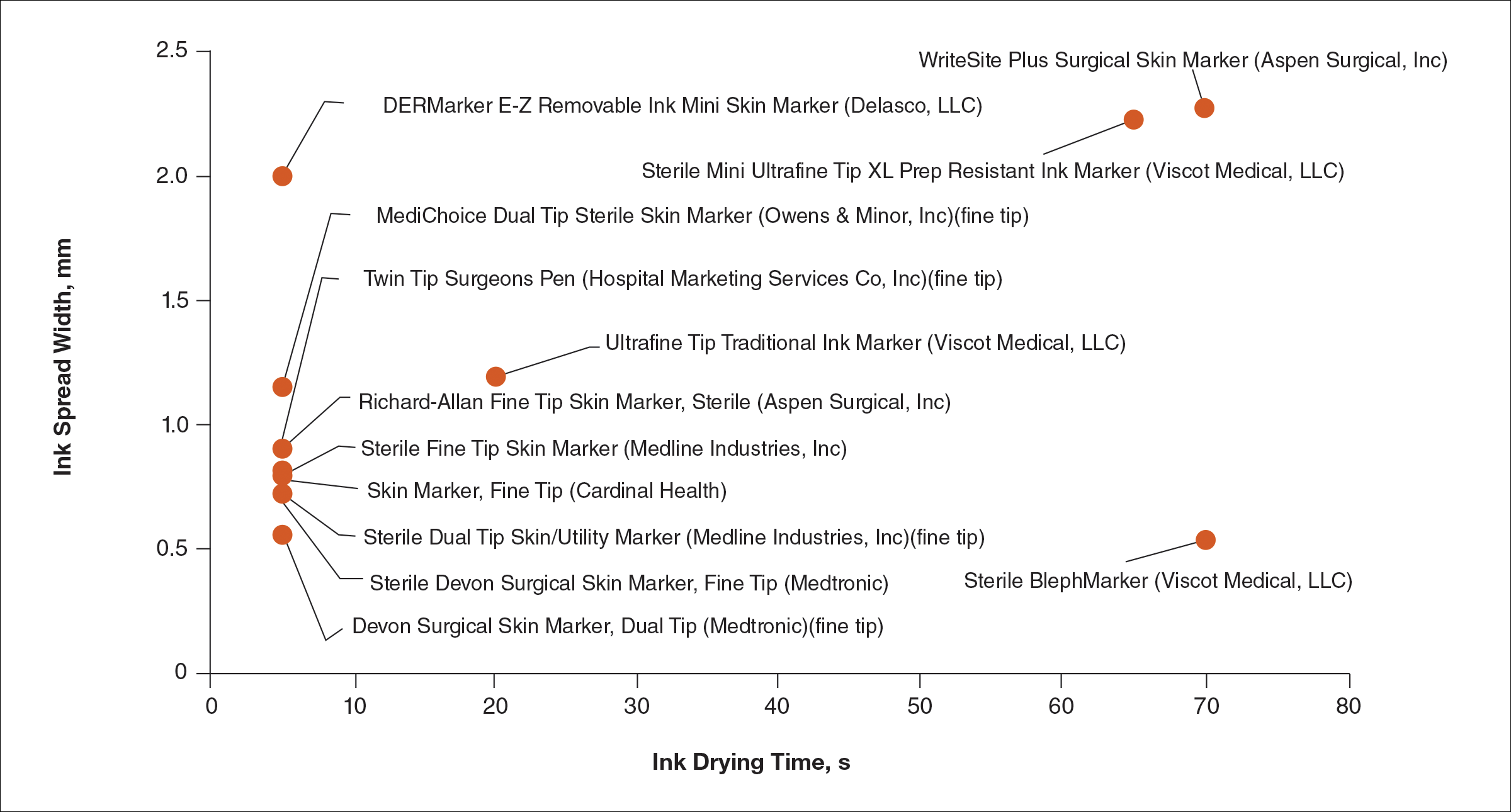
Figure 2 shows the drying time and ink spread width for all 13 markers.
Comment
Blepharoplasty surgeons generally agree that meticulous presurgical planning with marking of the eyelids is critical for successful surgical outcomes.1,2 Fine tip markers have been recommended for this purpose due to the relative precision of the marks, but the prerequisite of these markers is that the marks must have minimal ink spread through skinfolds to allow for precision as well as short drying time to avoid unintentional duplication of the ink on overlapping skin, especially with the likely chance of reflexive blinking by the patient. The associated assumption is that FT markers automatically leave precise marks with minimal drying time. This study systemically compared these 2 qualities for 13 markers, and the results are notable for the unexpected wide range of performance. Although most of the FT markers had ink spread width of less than 1 mm, the Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker was an outlier among FT markers, with ink spread greater than 2 mm, making it too broad and imprecise for practical use. This result indicates that not every FT marker actually makes fine marks. The 2 ST markers in the study—DERMarker E-Z Removable Ink Mini Skin Marker and WriteSite Plus Surgical Skin Marker—left broad marks as anticipated.
The drying time of the markers also ranged from 5 to 70 seconds among both FT and ST markers. Indeed, most of the FT markers were dry at or before 5 seconds of marking, but 2 FT markers—Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker and Sterile BlephMarker—dried at 65 and 70 seconds, respectively. Such a long drying time would be considered impractical for use in blepharoplasty marking and also unexpected of FT markers, which usually are marketed for their precision and efficiency. Notable in the discussion of drying time is that one of the 2 ST markers in the study, the DERMarker E-Z Removable Ink Mini Skin Marker, had the shortest possible drying time of 5 seconds, while the other ST marker, WriteSite Plus Surgical Skin Marker, dried at 70 seconds. This observation coupled with the unexpected results of broad marks and long drying time for some of the FT markers indicates that a surgeon cannot simply assume that a FT marker would provide marks with precision and fast drying time, or that an ST marker would be the opposite.
Future directions for study include the addition of other markers and the extent of resistance to antiseptic routines that can fade the markings.
Conclusion
Among the 13 markers studied, FT markers typically had the shortest drying time and least ink
Acknowledgement
The authors would like to thank Laura B. Hall, MD (New Haven, Connecticut), for her participation as the volunteer in this study.
- Hartstein ME, Massry GG, Holds JB. Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. New York, NY: Springer New York; 2015.
- Gladstone G, Black EH. Oculoplastic Surgery Atlas. New York, NY: Springer New York; 2005.
Blepharoplasty, or surgical manipulation of the upper and/or lower eyelids, is a commonly performed cosmetic procedure to improve the appearance and function of the eyelids by repositioning and/or removing excess skin and soft tissue from the eyelids, most often through external incisions that minimize scarring and maximize the aesthetic outcomes of the surgery. Therefore, the placement of the incisions is an important determinant of the surgical outcome, and the preoperative marking of the eyelids to indicate where the incisions should be placed is a crucial part of preparation for the surgery.
Preoperative marking has unique challenges due to the dynamicity of the eyelids and the delicate nature of the surgery. The mark must be narrow to minimize the risk of placing the incision higher or lower than intended. The mark also must dry quickly because the patient may blink and create multiple impressions of the marking on skinfolds in contact with the wet ink. Fast drying of the ink used to create the marks improves the efficiency and clarity of the presurgical planning.
We present data on the performance of the various blepharoplasty markers regarding drying time and ink spread width based on an evaluation of 13 surgical markers.
Methods
Eleven unique fine tip (FT) markers and 2 standard tip (ST) markers were obtained based on their accessibility at the researchers’ home institution and availability for direct purchase in small quantities from the distributors (Figure 1). Four markers were double tipped with one FT end and one ST end; for these markers, only the FT end was studied. The experiments were conducted on the bilateral upper eyelids and on hairless patches of skin of a single patient in a minor procedure room with surgical lighting and minimal draft of air. The sole experimenter (J.M.K.) conducting the study was not blinded.
The drying time of each marker was measured by marking 1-in lines on a patch of hairless skin that was first cleaned with an alcohol pad, then dried. Drying time for each marking was measured in increments of 5 seconds; at each time point, the markings were wiped with a single-ply, light-duty tissue under the weight of 10 US quarters to ensure that the same weight/pressure was applied when wiping the skin. Smudges observed with the naked eye on either the wipe or the patients’ skin were interpreted as nondry status of the marking. The first time point at which a marking was found to have no visible smudges either on the skin or the wipe was recorded as the drying time of the respective marker.
Ink spread was measured on clean eyelid skin by drawing curved lines along the natural crease as would be done for actual blepharoplasty planning. Each line was allowed to dry for 2 minutes. The greatest perpendicular spread width along the line observed with the naked eye was measured using a digital Vernier caliper with 0.01-mm graduations. Three measurements were obtained per marker and the values averaged to arrive at the final spread width.
Results
Drying time among the 13 total markers (11 FT and 2 ST) ranged from 5 to 70 seconds, with a mean of 20.8 seconds and median of 5 seconds (Table). The drying time for the DERMarker E-Z Removable Ink Mini Skin Marker (Delasco, LLC) with an ST was 5 seconds, while the drying time for the other ST marker, WriteSite Plus Surgical Skin Marker (Aspen Surgical, Inc), was 70 seconds. The FT markers spanned the entire range of drying times. The ink spread width among the markers ranged from 0.53 to 2.27 mm with a median of 0.9 mm and mean of 1.13 mm (Table). The 2 ST markers were found to make some of the widest marks measured, including the WriteSite Plus Surgical Skin Marker, a nonsterile ST marker that created the widest ink marks. The second widest mark was made by an FT marker (Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker [Viscot Medical, LLC]).
To prioritize short drying time coupled with minimal ink spread width, the values associated with each marker were averaged to arrive at the overall score for each marker. The smaller the overall score, the higher we ranked the marker. The Devon Surgical Skin Marker, Dual Tip (Medtronic) ranked the highest among the 13 markers with a final score of 2.78. Runner-up markers included the Sterile Devon Surgical Skin marker, Fine Tip (Medtronic)(final score, 2.86); the Sterile Dual Tip Skin/Utility Marker (Medline Industries, Inc)(final score, 2.86); and the Skin Marker, Fine Tip (Cardinal Health)(final score, 2.89). The 2 lowest-ranking markers were the WriteSite Plus Surgical Skin Marker, an ST marker (final score, 36.13), followed by the Sterile BlephMarker (Viscot Medical, LLC)(final score, 35.27).
Figure 2 shows the drying time and ink spread width for all 13 markers.
Comment
Blepharoplasty surgeons generally agree that meticulous presurgical planning with marking of the eyelids is critical for successful surgical outcomes.1,2 Fine tip markers have been recommended for this purpose due to the relative precision of the marks, but the prerequisite of these markers is that the marks must have minimal ink spread through skinfolds to allow for precision as well as short drying time to avoid unintentional duplication of the ink on overlapping skin, especially with the likely chance of reflexive blinking by the patient. The associated assumption is that FT markers automatically leave precise marks with minimal drying time. This study systemically compared these 2 qualities for 13 markers, and the results are notable for the unexpected wide range of performance. Although most of the FT markers had ink spread width of less than 1 mm, the Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker was an outlier among FT markers, with ink spread greater than 2 mm, making it too broad and imprecise for practical use. This result indicates that not every FT marker actually makes fine marks. The 2 ST markers in the study—DERMarker E-Z Removable Ink Mini Skin Marker and WriteSite Plus Surgical Skin Marker—left broad marks as anticipated.
The drying time of the markers also ranged from 5 to 70 seconds among both FT and ST markers. Indeed, most of the FT markers were dry at or before 5 seconds of marking, but 2 FT markers—Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker and Sterile BlephMarker—dried at 65 and 70 seconds, respectively. Such a long drying time would be considered impractical for use in blepharoplasty marking and also unexpected of FT markers, which usually are marketed for their precision and efficiency. Notable in the discussion of drying time is that one of the 2 ST markers in the study, the DERMarker E-Z Removable Ink Mini Skin Marker, had the shortest possible drying time of 5 seconds, while the other ST marker, WriteSite Plus Surgical Skin Marker, dried at 70 seconds. This observation coupled with the unexpected results of broad marks and long drying time for some of the FT markers indicates that a surgeon cannot simply assume that a FT marker would provide marks with precision and fast drying time, or that an ST marker would be the opposite.
Future directions for study include the addition of other markers and the extent of resistance to antiseptic routines that can fade the markings.
Conclusion
Among the 13 markers studied, FT markers typically had the shortest drying time and least ink
Acknowledgement
The authors would like to thank Laura B. Hall, MD (New Haven, Connecticut), for her participation as the volunteer in this study.
Blepharoplasty, or surgical manipulation of the upper and/or lower eyelids, is a commonly performed cosmetic procedure to improve the appearance and function of the eyelids by repositioning and/or removing excess skin and soft tissue from the eyelids, most often through external incisions that minimize scarring and maximize the aesthetic outcomes of the surgery. Therefore, the placement of the incisions is an important determinant of the surgical outcome, and the preoperative marking of the eyelids to indicate where the incisions should be placed is a crucial part of preparation for the surgery.
Preoperative marking has unique challenges due to the dynamicity of the eyelids and the delicate nature of the surgery. The mark must be narrow to minimize the risk of placing the incision higher or lower than intended. The mark also must dry quickly because the patient may blink and create multiple impressions of the marking on skinfolds in contact with the wet ink. Fast drying of the ink used to create the marks improves the efficiency and clarity of the presurgical planning.
We present data on the performance of the various blepharoplasty markers regarding drying time and ink spread width based on an evaluation of 13 surgical markers.
Methods
Eleven unique fine tip (FT) markers and 2 standard tip (ST) markers were obtained based on their accessibility at the researchers’ home institution and availability for direct purchase in small quantities from the distributors (Figure 1). Four markers were double tipped with one FT end and one ST end; for these markers, only the FT end was studied. The experiments were conducted on the bilateral upper eyelids and on hairless patches of skin of a single patient in a minor procedure room with surgical lighting and minimal draft of air. The sole experimenter (J.M.K.) conducting the study was not blinded.
The drying time of each marker was measured by marking 1-in lines on a patch of hairless skin that was first cleaned with an alcohol pad, then dried. Drying time for each marking was measured in increments of 5 seconds; at each time point, the markings were wiped with a single-ply, light-duty tissue under the weight of 10 US quarters to ensure that the same weight/pressure was applied when wiping the skin. Smudges observed with the naked eye on either the wipe or the patients’ skin were interpreted as nondry status of the marking. The first time point at which a marking was found to have no visible smudges either on the skin or the wipe was recorded as the drying time of the respective marker.
Ink spread was measured on clean eyelid skin by drawing curved lines along the natural crease as would be done for actual blepharoplasty planning. Each line was allowed to dry for 2 minutes. The greatest perpendicular spread width along the line observed with the naked eye was measured using a digital Vernier caliper with 0.01-mm graduations. Three measurements were obtained per marker and the values averaged to arrive at the final spread width.
Results
Drying time among the 13 total markers (11 FT and 2 ST) ranged from 5 to 70 seconds, with a mean of 20.8 seconds and median of 5 seconds (Table). The drying time for the DERMarker E-Z Removable Ink Mini Skin Marker (Delasco, LLC) with an ST was 5 seconds, while the drying time for the other ST marker, WriteSite Plus Surgical Skin Marker (Aspen Surgical, Inc), was 70 seconds. The FT markers spanned the entire range of drying times. The ink spread width among the markers ranged from 0.53 to 2.27 mm with a median of 0.9 mm and mean of 1.13 mm (Table). The 2 ST markers were found to make some of the widest marks measured, including the WriteSite Plus Surgical Skin Marker, a nonsterile ST marker that created the widest ink marks. The second widest mark was made by an FT marker (Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker [Viscot Medical, LLC]).
To prioritize short drying time coupled with minimal ink spread width, the values associated with each marker were averaged to arrive at the overall score for each marker. The smaller the overall score, the higher we ranked the marker. The Devon Surgical Skin Marker, Dual Tip (Medtronic) ranked the highest among the 13 markers with a final score of 2.78. Runner-up markers included the Sterile Devon Surgical Skin marker, Fine Tip (Medtronic)(final score, 2.86); the Sterile Dual Tip Skin/Utility Marker (Medline Industries, Inc)(final score, 2.86); and the Skin Marker, Fine Tip (Cardinal Health)(final score, 2.89). The 2 lowest-ranking markers were the WriteSite Plus Surgical Skin Marker, an ST marker (final score, 36.13), followed by the Sterile BlephMarker (Viscot Medical, LLC)(final score, 35.27).
Figure 2 shows the drying time and ink spread width for all 13 markers.
Comment
Blepharoplasty surgeons generally agree that meticulous presurgical planning with marking of the eyelids is critical for successful surgical outcomes.1,2 Fine tip markers have been recommended for this purpose due to the relative precision of the marks, but the prerequisite of these markers is that the marks must have minimal ink spread through skinfolds to allow for precision as well as short drying time to avoid unintentional duplication of the ink on overlapping skin, especially with the likely chance of reflexive blinking by the patient. The associated assumption is that FT markers automatically leave precise marks with minimal drying time. This study systemically compared these 2 qualities for 13 markers, and the results are notable for the unexpected wide range of performance. Although most of the FT markers had ink spread width of less than 1 mm, the Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker was an outlier among FT markers, with ink spread greater than 2 mm, making it too broad and imprecise for practical use. This result indicates that not every FT marker actually makes fine marks. The 2 ST markers in the study—DERMarker E-Z Removable Ink Mini Skin Marker and WriteSite Plus Surgical Skin Marker—left broad marks as anticipated.
The drying time of the markers also ranged from 5 to 70 seconds among both FT and ST markers. Indeed, most of the FT markers were dry at or before 5 seconds of marking, but 2 FT markers—Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker and Sterile BlephMarker—dried at 65 and 70 seconds, respectively. Such a long drying time would be considered impractical for use in blepharoplasty marking and also unexpected of FT markers, which usually are marketed for their precision and efficiency. Notable in the discussion of drying time is that one of the 2 ST markers in the study, the DERMarker E-Z Removable Ink Mini Skin Marker, had the shortest possible drying time of 5 seconds, while the other ST marker, WriteSite Plus Surgical Skin Marker, dried at 70 seconds. This observation coupled with the unexpected results of broad marks and long drying time for some of the FT markers indicates that a surgeon cannot simply assume that a FT marker would provide marks with precision and fast drying time, or that an ST marker would be the opposite.
Future directions for study include the addition of other markers and the extent of resistance to antiseptic routines that can fade the markings.
Conclusion
Among the 13 markers studied, FT markers typically had the shortest drying time and least ink
Acknowledgement
The authors would like to thank Laura B. Hall, MD (New Haven, Connecticut), for her participation as the volunteer in this study.
- Hartstein ME, Massry GG, Holds JB. Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. New York, NY: Springer New York; 2015.
- Gladstone G, Black EH. Oculoplastic Surgery Atlas. New York, NY: Springer New York; 2005.
- Hartstein ME, Massry GG, Holds JB. Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. New York, NY: Springer New York; 2015.
- Gladstone G, Black EH. Oculoplastic Surgery Atlas. New York, NY: Springer New York; 2005.
Resident Pearl
Based on the data presented in this study, blepharoplasty surgeons may choose to use the markers shown to have measurably short drying time and minimal ink spread to maximize efficiency of preincisional lid marking.