User login
Risk Evaluation and Mitigation Strategies (REMS): red tape, or a remedy for opioid abuse?
Are you aware that a significant change is coming to the way you prescribe opioid pain relievers for your patients? After 3 years of debate among the Food and Drug Administration (FDA), drug industry stakeholders, members of the pain and addiction communities, patient advocacy groups, and the public, the first large-scale, class-wide REMS is here. REMS is the acronym for Risk Evaluation and Mitigation Strategies. There is a good chance you are prescribing one or more of the affected medications, and adherence to the REMS requirements will be essential if you wish to continue prescribing them.
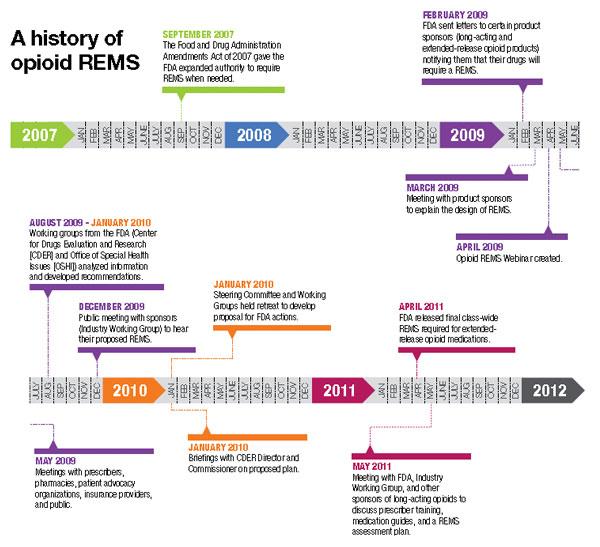
Before getting into the fine points of the opioid REMS, a little background about how it came into being is in order. On March 25, 2008, the Food and Drug Administration Amendments Act went into effect, granting the FDA authority to require a REMS for any product or product class it deemed to be a public health, safety, or welfare threat. Basically, REMS is an FDA-imposed “safety” program. The first medication to now have a single or class REMS is the class of extended-release (ER) and long-acting (LA) opioid analgesics.
Why opioid analgesics? In 2007, attempts to mitigate targeted risks associated with 30 drugs using RISKMaps were cited as inadequate by the FDA. RISKMaps are safety programs designed to minimize significant risks of certain medicines through FDA-approved labeling, reporting of adverse events, prescriber and patient education about risks, reminders, and performance-linked access systems that tie access to medications with documentation and laboratory testing.1 Passage of the FDA Amendments Act allowed the FDA to use its REMS authority to “improve” existing risk plans.
Forces for change
The FDA cites many good reasons for this change, primarily to ensure that the benefits of prescribing opioid analgesics outweigh the risks, and that patients in pain who need these drugs have access to them. Driving factors behind this move centered on the highly visible consequences associated with what FDA experts describe as misuse, abuse, and improper prescribing of 12 ER/LA opioid analgesics. According to FDA estimates, in 2007 more than 33 million Americans age 12 and older misused ER/LA opioids. Of the almost 28,000 Americans who died from unintended consequences of drug use, nearly 12,000 were associated with prescription analgesics.2
In my opinion, voluntary continuing medical education (CME) and professional organization guidelines added to the problem by failing to decrease overdoses and unintended deaths. This may come as no surprise, as such deaths often stem from diversion, and diverters typically are not subject to a CME requirement.
The ER/LA segment of the class was targeted for a variety of reasons. First, higher doses of ER/LA opiates packed into single units are believed to pose a greater threat than the millions of short-acting, immediate-release (IR) opioid analgesics units abused annually.3 Another reason for the move focused on the burden to the health system caused by more than 24 similar individual REMS existing in this class. That alone created a virtual paper, regulatory, and health system encumbrance that is expected to be alleviated by a class-wide REMS.
Increasing numbers of prescriptions were an additional consideration. The number of outpatient retail prescriptions dispensed for ER/LA and IR opiates rose dramatically between 2000 and 2009, from 9.3 million to 22.9 million ER/LA opioids and from 164.8 million to 234 million IR opioids [Figure 1].3 Who is prescribing them? You are. In 2009, primary care physicians were the top prescribers of ER/LA (43.8%) and IR (42.1%) opioid analgesics [Figure 2].3 Who are you prescribing them for? Not the elderly age group you might expect. The largest number of prescriptions were written for men and women between ages 50and 59 [Figure 3].3
| FIGURE 1: Total number of prescriptions dispensed for ER/LA and IR opioids from US outpatient retail pharmacies, 2000-2009. |
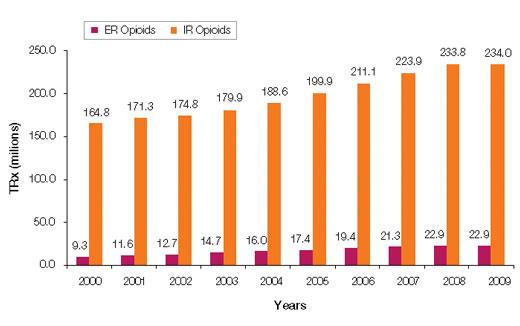
| ER, extended release; IR, immediate release; LA, long acting; TRx, total prescriptions. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterial/Drug/AnestheticAndLifeSupportDrugsAdvisory Committee/UCM220950.pdf. |
| FIGURE 2: Total number of prescriptions dispensed in the United States by top 10 prescribing specialties for IR and ER/LA opioids, 2009 |
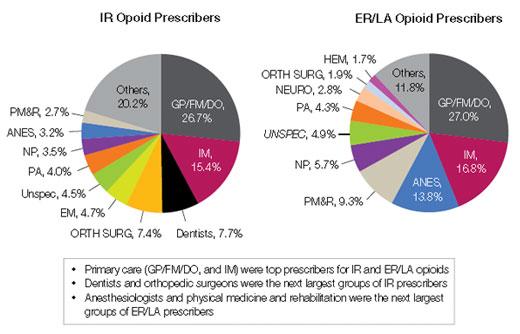
| ANES, anesthesiologists; DO, doctor of osteopathy; EM, emergency medicine; ER, extended release; FM, family medicine; GP, general practitioner; HEM, hematologists; IM, internal medicine; IR, immediate release; LA, long acting; NP, nurse practitioners; ORTH SURG, orthopedic surgeons; NEURO, neurologists; PA, physician assistants; PM&R, physical medicine and rehabilitation; TRx, total prescriptions. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drug/AnestheticAndLifeSupportDrugsAdvisoryCommittee/UCM220950.pdf. |
| FIGURE 3: Total number of unique patients, stratified by age and sex, receiving a dispensed prescription for an ER/LA opioid product from US outpatient retail pharmacies, 2009 |
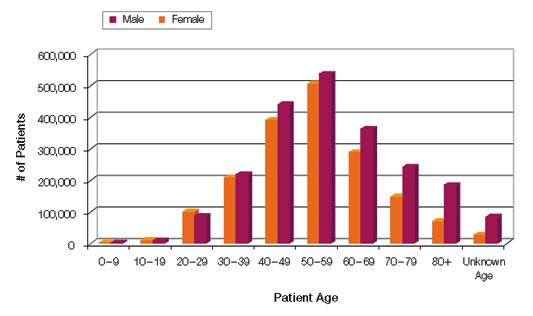
| ER, extended release; LA, long acting. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndLifeSupportDrugsAdvisoryCommittee/UCM220950.pdf. |
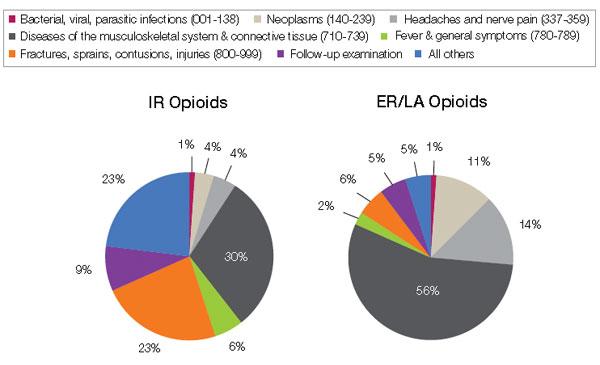
And what are you prescribing them for? Data from a 2009 survey of the prescribing habits of 3200 office-based physicians in 30 specialties showed that most prescriptions written for ER/LA and IR opioids are associated with diagnoses related to pain in the musculoskeletal system and connective tissue (56% [ER/LA] and 30% [IR]). For ER/LA
prescriptions the second most common diagnoses were headaches and nerve pain (14%), while for IR prescriptions they were fractures, sprains, and contusions (23%) [Figure 4].3
| FIGURE 4: Diagnoses associated with use (by grouped ICD-9 codes) for IR and ER/LA opioids as reported by office-based physicians in the United States, 2009 |
| ER, extended release; IR, immediate release; LA, long acting. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndLifeSupportDrugs AdvisoryCommittee/UCM220950.pdf. |
According to Janet Woodcock, MD, Director of the FDA’s Center for Drug Evaluation and Research, some physicians may not be clear about who should receive these drugs or how to manage patients in pain. As a result, some physicians may be reluctant to prescribe opioid analgesics, leaving patients without adequate pain relief. At the same time, other physicians overprescribe them, putting patients—and anyone with access to the family medicine cabinet—at risk.4
A REMS by any other name
And so REMS was conceived. On February 6, 2009, manufacturers of certain opioid drug products received a letter from the FDA informing them that their drugs would be required to have a risk management program, and inviting them to meet to discuss the design and development of such a REMS.5
Two years later, on April 19, 2011, an alarm in the form of an action plan was released by the Obama administration through the Office of National Drug Control Policy. The plan,
Epidemic: Responding to America’s Prescription Drug Abuse Crisis, outlined a set of measures to remedy the problem through education, monitoring, proper disposal of prescription drugs, and enforcement.6
REMS for opioids was the FDA’s response in support of the President’s plan. On the same day in April, 32 manufacturers of ER/LA opioids received a letter from the FDA informing them that they must meet new safety requirements concerning these medications under a single shared, standardized system [Table].
| TABLE: Long-acting and extended-release opioids requiring an opioid REMS |
| Brand Name Products |
| Trade Name | Generic Name | Sponsor | |
| 1 | Duragesic | Fentanyl transdermal system | Ortho-McNeil-Janssen |
| 2 | Dolophine | Methadone HCI tablets | Roxanne Laboratories |
| 3 | Avinza | Morphine sulfate extended-release capsules | King Pharmaceuticals/Pfizer |
| 4 | Kadian capsules | Morphine sulfate extended-release capsules | Actavis |
| 5 | MS Contin | Morphine sulfate controlled-release tablets | Purdue Pharma |
| 6 | Oramorph | Morphine sulfate sustained-release tablets | Xanodyne Pharmaceuticals |
| 7 | OxyContin | Oxycodone HCI controlled-release tablets | Purdue Pharma |
| 8 | Opana ER | Oxymorphone HCI extended-release tablets | Endo Pharmaceuticals |
| 9 | Exalgo | Hydromorphone HCI extendedrelease tablets | Mallinckrodt Inc/Covidien |
| 10 | Butrans | Buprenorphine transdermal system | Purdue Pharma |
| Generic Products |
| Drug Name | Generic Name | Sponsor | |
| 1 | Fentanyl | Fentanyl extended-release transdermal system | Actavis |
| 2 | Fentanyl | Fentanyl extended-release transdermal system | Lavipharm Labs |
| 3 | Fentanyl | Fentanyl extended-release transdermal system | Mallinckrodt Inc/Covidien |
| 4 | Fentanyl | Fentanyl extended-release transdermal system | Mylan Technologies |
| 5 | Fentanyl | Fentanyl extended-release transdermal system | Noven Pharmaceuticals |
| 6 | Fentanyl | Fentanyl extended-release transdermal system | Teva Pharmaceutical Industries |
| 7 | Fentanyl | Fentanyl extended-release transdermal system | Watson Pharmaceuticals |
| 8 | Methadone hydrochloride | Methadone HCl oral solution | The Pharmanetwork |
| 9 | Methadone hydrochloride | Methadone HCl oral solution | Mallinckrodt Inc/Covidien |
| 10 | Methadone hydrochloride | Methadone HCl oral solution | Sandoz |
| 11 | Methadone hydrochloride | Methadone HCl oral solution | Roxane Laboratories |
| 12 | Methadone hydrochloride | Methadone HCl oral solution | VistaPharm |
| 13 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Endo Pharmaceuticals |
| 14 | Morphine sulfate | Morphine sulfate extendedrelease tablets | KV Pharmaceuticals |
| 15 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Mallinckrodt Inc/Covidien |
| 16 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Watson Pharmaceuticals |
| 17 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Rhodes Pharmaceuticals |
| 18 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Mallinckrodt Inc/Covidien |
| 19 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Impax Laboratories |
| 20 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Teva Pharmaceutical Industries |
| 21 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Endo Pharmaceuticals |
| 22 | Oxycodone hydrochloride | Oxymorphone HCl extendedrelease tablets | Impax Laboratories |
| 23 | Oxycodone hydrochloride | Oxymorphone HCl extendedrelease tablets | Actavis |
| *Tentatively approved products. Source: U.S. Food & Drug Administration Web site. http://www.fda.gov/Drugs/DrugSafet/InformationbyDrugClass/ucm251735.htm. |
As outlined in this REMS, manufacturers must provide for the training of prescribers of opioid medications—training that covers proper patient selection, patient counseling in specific product use and risk, and assessment for addiction and tolerance. Manufacturers must also develop factual, nonpromotional patient information and medication guides that will be FDA regulated and approved. Finally, they will be asked to adhere to a timetable to assess whether REMS is meetings its goals.4,5
In May 2011, the FDA met with manufacturers to expand on how to coordinate and implement the REMS requirements.
Hope for a “new normal”
Will REMS for other large medication classes eventually reach beyond opioid analgesics, perhaps warranting practitioners to view REMS as being a good thing as opposed to a nuisance? Your decision to participate in REMS or pass and alter your care approach will need to be made soon. What will you do?
For you as an opioid prescriber, education is the focus, and you will soon be presented with voluntary prescriber education programs. The “hope” is that you will volunteer to take the opioid education program, fill out an electronic or fax form, and send it in to an administrator who will track all those who participate. Since “hope” will unlikely drive large-scale participation, when hope finally runs out the education will become mandatory. This will occur in a year or 2, and will likely become a Drug Enforcement Administration requirement for you to procure CII scheduling.
Unfortunately, there is no guarantee that deaths and overdoses will stop with the opioid REMS. The only guarantee is you will not be able to prescribe these medications at some point if you do not participate in the REMS.
So act now. To be notified when the opioid REMS training becomes available go to www.opioidREMS.com and register. It’s vital that you do ... and relatively painless.
REFERENCES
1. U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality, Food and Drug Administration. Summary of public workshop. Implementation of risk minimization action plans (RiskMAPs) to support quality use of pharmaceuticals: opportunities and challenges. June 25-26, 2007.
2. US. Food and Drug Administration. FDA acts to reduce harm from opioid drugs. Consumer Updates. Available at: http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm251830.htm.
3. Governale L. Outpatient Prescription Opioid Utilization in the U.S., Years 2000 – 2009. Food and Drug Administration, Division of Epidemiology. July 22, 2010. Avilable at: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndLifeSupportDrugsAdvisoryCommittee/UCM220950.pdf
4. Marchand H, moderator. Opioid drugs and risk evaluation and mitigation strategies (REMS) Podcast/transcript. April 20, 2011. Available at: http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm252649.htm.
5. U.S. Food and Drug Administration. Opioid drugs and risk mitigation strategies (REMS) Available at: http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm163647.htm.
6. Epidemic: responding to America’s prescription drug abuse crisis. Available at: http://www.whitehousedrugpolicy.gov/publications/pdf/rx_abuse_plan.pdf.
Are you aware that a significant change is coming to the way you prescribe opioid pain relievers for your patients? After 3 years of debate among the Food and Drug Administration (FDA), drug industry stakeholders, members of the pain and addiction communities, patient advocacy groups, and the public, the first large-scale, class-wide REMS is here. REMS is the acronym for Risk Evaluation and Mitigation Strategies. There is a good chance you are prescribing one or more of the affected medications, and adherence to the REMS requirements will be essential if you wish to continue prescribing them.
Before getting into the fine points of the opioid REMS, a little background about how it came into being is in order. On March 25, 2008, the Food and Drug Administration Amendments Act went into effect, granting the FDA authority to require a REMS for any product or product class it deemed to be a public health, safety, or welfare threat. Basically, REMS is an FDA-imposed “safety” program. The first medication to now have a single or class REMS is the class of extended-release (ER) and long-acting (LA) opioid analgesics.
Why opioid analgesics? In 2007, attempts to mitigate targeted risks associated with 30 drugs using RISKMaps were cited as inadequate by the FDA. RISKMaps are safety programs designed to minimize significant risks of certain medicines through FDA-approved labeling, reporting of adverse events, prescriber and patient education about risks, reminders, and performance-linked access systems that tie access to medications with documentation and laboratory testing.1 Passage of the FDA Amendments Act allowed the FDA to use its REMS authority to “improve” existing risk plans.
Forces for change
The FDA cites many good reasons for this change, primarily to ensure that the benefits of prescribing opioid analgesics outweigh the risks, and that patients in pain who need these drugs have access to them. Driving factors behind this move centered on the highly visible consequences associated with what FDA experts describe as misuse, abuse, and improper prescribing of 12 ER/LA opioid analgesics. According to FDA estimates, in 2007 more than 33 million Americans age 12 and older misused ER/LA opioids. Of the almost 28,000 Americans who died from unintended consequences of drug use, nearly 12,000 were associated with prescription analgesics.2
In my opinion, voluntary continuing medical education (CME) and professional organization guidelines added to the problem by failing to decrease overdoses and unintended deaths. This may come as no surprise, as such deaths often stem from diversion, and diverters typically are not subject to a CME requirement.
The ER/LA segment of the class was targeted for a variety of reasons. First, higher doses of ER/LA opiates packed into single units are believed to pose a greater threat than the millions of short-acting, immediate-release (IR) opioid analgesics units abused annually.3 Another reason for the move focused on the burden to the health system caused by more than 24 similar individual REMS existing in this class. That alone created a virtual paper, regulatory, and health system encumbrance that is expected to be alleviated by a class-wide REMS.
Increasing numbers of prescriptions were an additional consideration. The number of outpatient retail prescriptions dispensed for ER/LA and IR opiates rose dramatically between 2000 and 2009, from 9.3 million to 22.9 million ER/LA opioids and from 164.8 million to 234 million IR opioids [Figure 1].3 Who is prescribing them? You are. In 2009, primary care physicians were the top prescribers of ER/LA (43.8%) and IR (42.1%) opioid analgesics [Figure 2].3 Who are you prescribing them for? Not the elderly age group you might expect. The largest number of prescriptions were written for men and women between ages 50and 59 [Figure 3].3
| FIGURE 1: Total number of prescriptions dispensed for ER/LA and IR opioids from US outpatient retail pharmacies, 2000-2009. |
| ER, extended release; IR, immediate release; LA, long acting; TRx, total prescriptions. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterial/Drug/AnestheticAndLifeSupportDrugsAdvisory Committee/UCM220950.pdf. |
| FIGURE 2: Total number of prescriptions dispensed in the United States by top 10 prescribing specialties for IR and ER/LA opioids, 2009 |
| ANES, anesthesiologists; DO, doctor of osteopathy; EM, emergency medicine; ER, extended release; FM, family medicine; GP, general practitioner; HEM, hematologists; IM, internal medicine; IR, immediate release; LA, long acting; NP, nurse practitioners; ORTH SURG, orthopedic surgeons; NEURO, neurologists; PA, physician assistants; PM&R, physical medicine and rehabilitation; TRx, total prescriptions. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drug/AnestheticAndLifeSupportDrugsAdvisoryCommittee/UCM220950.pdf. |
| FIGURE 3: Total number of unique patients, stratified by age and sex, receiving a dispensed prescription for an ER/LA opioid product from US outpatient retail pharmacies, 2009 |
| ER, extended release; LA, long acting. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndLifeSupportDrugsAdvisoryCommittee/UCM220950.pdf. |
And what are you prescribing them for? Data from a 2009 survey of the prescribing habits of 3200 office-based physicians in 30 specialties showed that most prescriptions written for ER/LA and IR opioids are associated with diagnoses related to pain in the musculoskeletal system and connective tissue (56% [ER/LA] and 30% [IR]). For ER/LA
prescriptions the second most common diagnoses were headaches and nerve pain (14%), while for IR prescriptions they were fractures, sprains, and contusions (23%) [Figure 4].3
| FIGURE 4: Diagnoses associated with use (by grouped ICD-9 codes) for IR and ER/LA opioids as reported by office-based physicians in the United States, 2009 |
| ER, extended release; IR, immediate release; LA, long acting. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndLifeSupportDrugs AdvisoryCommittee/UCM220950.pdf. |
According to Janet Woodcock, MD, Director of the FDA’s Center for Drug Evaluation and Research, some physicians may not be clear about who should receive these drugs or how to manage patients in pain. As a result, some physicians may be reluctant to prescribe opioid analgesics, leaving patients without adequate pain relief. At the same time, other physicians overprescribe them, putting patients—and anyone with access to the family medicine cabinet—at risk.4
A REMS by any other name
And so REMS was conceived. On February 6, 2009, manufacturers of certain opioid drug products received a letter from the FDA informing them that their drugs would be required to have a risk management program, and inviting them to meet to discuss the design and development of such a REMS.5
Two years later, on April 19, 2011, an alarm in the form of an action plan was released by the Obama administration through the Office of National Drug Control Policy. The plan,
Epidemic: Responding to America’s Prescription Drug Abuse Crisis, outlined a set of measures to remedy the problem through education, monitoring, proper disposal of prescription drugs, and enforcement.6
REMS for opioids was the FDA’s response in support of the President’s plan. On the same day in April, 32 manufacturers of ER/LA opioids received a letter from the FDA informing them that they must meet new safety requirements concerning these medications under a single shared, standardized system [Table].
| TABLE: Long-acting and extended-release opioids requiring an opioid REMS |
| Brand Name Products |
| Trade Name | Generic Name | Sponsor | |
| 1 | Duragesic | Fentanyl transdermal system | Ortho-McNeil-Janssen |
| 2 | Dolophine | Methadone HCI tablets | Roxanne Laboratories |
| 3 | Avinza | Morphine sulfate extended-release capsules | King Pharmaceuticals/Pfizer |
| 4 | Kadian capsules | Morphine sulfate extended-release capsules | Actavis |
| 5 | MS Contin | Morphine sulfate controlled-release tablets | Purdue Pharma |
| 6 | Oramorph | Morphine sulfate sustained-release tablets | Xanodyne Pharmaceuticals |
| 7 | OxyContin | Oxycodone HCI controlled-release tablets | Purdue Pharma |
| 8 | Opana ER | Oxymorphone HCI extended-release tablets | Endo Pharmaceuticals |
| 9 | Exalgo | Hydromorphone HCI extendedrelease tablets | Mallinckrodt Inc/Covidien |
| 10 | Butrans | Buprenorphine transdermal system | Purdue Pharma |
| Generic Products |
| Drug Name | Generic Name | Sponsor | |
| 1 | Fentanyl | Fentanyl extended-release transdermal system | Actavis |
| 2 | Fentanyl | Fentanyl extended-release transdermal system | Lavipharm Labs |
| 3 | Fentanyl | Fentanyl extended-release transdermal system | Mallinckrodt Inc/Covidien |
| 4 | Fentanyl | Fentanyl extended-release transdermal system | Mylan Technologies |
| 5 | Fentanyl | Fentanyl extended-release transdermal system | Noven Pharmaceuticals |
| 6 | Fentanyl | Fentanyl extended-release transdermal system | Teva Pharmaceutical Industries |
| 7 | Fentanyl | Fentanyl extended-release transdermal system | Watson Pharmaceuticals |
| 8 | Methadone hydrochloride | Methadone HCl oral solution | The Pharmanetwork |
| 9 | Methadone hydrochloride | Methadone HCl oral solution | Mallinckrodt Inc/Covidien |
| 10 | Methadone hydrochloride | Methadone HCl oral solution | Sandoz |
| 11 | Methadone hydrochloride | Methadone HCl oral solution | Roxane Laboratories |
| 12 | Methadone hydrochloride | Methadone HCl oral solution | VistaPharm |
| 13 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Endo Pharmaceuticals |
| 14 | Morphine sulfate | Morphine sulfate extendedrelease tablets | KV Pharmaceuticals |
| 15 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Mallinckrodt Inc/Covidien |
| 16 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Watson Pharmaceuticals |
| 17 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Rhodes Pharmaceuticals |
| 18 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Mallinckrodt Inc/Covidien |
| 19 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Impax Laboratories |
| 20 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Teva Pharmaceutical Industries |
| 21 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Endo Pharmaceuticals |
| 22 | Oxycodone hydrochloride | Oxymorphone HCl extendedrelease tablets | Impax Laboratories |
| 23 | Oxycodone hydrochloride | Oxymorphone HCl extendedrelease tablets | Actavis |
| *Tentatively approved products. Source: U.S. Food & Drug Administration Web site. http://www.fda.gov/Drugs/DrugSafet/InformationbyDrugClass/ucm251735.htm. |
As outlined in this REMS, manufacturers must provide for the training of prescribers of opioid medications—training that covers proper patient selection, patient counseling in specific product use and risk, and assessment for addiction and tolerance. Manufacturers must also develop factual, nonpromotional patient information and medication guides that will be FDA regulated and approved. Finally, they will be asked to adhere to a timetable to assess whether REMS is meetings its goals.4,5
In May 2011, the FDA met with manufacturers to expand on how to coordinate and implement the REMS requirements.
Hope for a “new normal”
Will REMS for other large medication classes eventually reach beyond opioid analgesics, perhaps warranting practitioners to view REMS as being a good thing as opposed to a nuisance? Your decision to participate in REMS or pass and alter your care approach will need to be made soon. What will you do?
For you as an opioid prescriber, education is the focus, and you will soon be presented with voluntary prescriber education programs. The “hope” is that you will volunteer to take the opioid education program, fill out an electronic or fax form, and send it in to an administrator who will track all those who participate. Since “hope” will unlikely drive large-scale participation, when hope finally runs out the education will become mandatory. This will occur in a year or 2, and will likely become a Drug Enforcement Administration requirement for you to procure CII scheduling.
Unfortunately, there is no guarantee that deaths and overdoses will stop with the opioid REMS. The only guarantee is you will not be able to prescribe these medications at some point if you do not participate in the REMS.
So act now. To be notified when the opioid REMS training becomes available go to www.opioidREMS.com and register. It’s vital that you do ... and relatively painless.
REFERENCES
1. U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality, Food and Drug Administration. Summary of public workshop. Implementation of risk minimization action plans (RiskMAPs) to support quality use of pharmaceuticals: opportunities and challenges. June 25-26, 2007.
2. US. Food and Drug Administration. FDA acts to reduce harm from opioid drugs. Consumer Updates. Available at: http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm251830.htm.
3. Governale L. Outpatient Prescription Opioid Utilization in the U.S., Years 2000 – 2009. Food and Drug Administration, Division of Epidemiology. July 22, 2010. Avilable at: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndLifeSupportDrugsAdvisoryCommittee/UCM220950.pdf
4. Marchand H, moderator. Opioid drugs and risk evaluation and mitigation strategies (REMS) Podcast/transcript. April 20, 2011. Available at: http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm252649.htm.
5. U.S. Food and Drug Administration. Opioid drugs and risk mitigation strategies (REMS) Available at: http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm163647.htm.
6. Epidemic: responding to America’s prescription drug abuse crisis. Available at: http://www.whitehousedrugpolicy.gov/publications/pdf/rx_abuse_plan.pdf.
Are you aware that a significant change is coming to the way you prescribe opioid pain relievers for your patients? After 3 years of debate among the Food and Drug Administration (FDA), drug industry stakeholders, members of the pain and addiction communities, patient advocacy groups, and the public, the first large-scale, class-wide REMS is here. REMS is the acronym for Risk Evaluation and Mitigation Strategies. There is a good chance you are prescribing one or more of the affected medications, and adherence to the REMS requirements will be essential if you wish to continue prescribing them.
Before getting into the fine points of the opioid REMS, a little background about how it came into being is in order. On March 25, 2008, the Food and Drug Administration Amendments Act went into effect, granting the FDA authority to require a REMS for any product or product class it deemed to be a public health, safety, or welfare threat. Basically, REMS is an FDA-imposed “safety” program. The first medication to now have a single or class REMS is the class of extended-release (ER) and long-acting (LA) opioid analgesics.
Why opioid analgesics? In 2007, attempts to mitigate targeted risks associated with 30 drugs using RISKMaps were cited as inadequate by the FDA. RISKMaps are safety programs designed to minimize significant risks of certain medicines through FDA-approved labeling, reporting of adverse events, prescriber and patient education about risks, reminders, and performance-linked access systems that tie access to medications with documentation and laboratory testing.1 Passage of the FDA Amendments Act allowed the FDA to use its REMS authority to “improve” existing risk plans.
Forces for change
The FDA cites many good reasons for this change, primarily to ensure that the benefits of prescribing opioid analgesics outweigh the risks, and that patients in pain who need these drugs have access to them. Driving factors behind this move centered on the highly visible consequences associated with what FDA experts describe as misuse, abuse, and improper prescribing of 12 ER/LA opioid analgesics. According to FDA estimates, in 2007 more than 33 million Americans age 12 and older misused ER/LA opioids. Of the almost 28,000 Americans who died from unintended consequences of drug use, nearly 12,000 were associated with prescription analgesics.2
In my opinion, voluntary continuing medical education (CME) and professional organization guidelines added to the problem by failing to decrease overdoses and unintended deaths. This may come as no surprise, as such deaths often stem from diversion, and diverters typically are not subject to a CME requirement.
The ER/LA segment of the class was targeted for a variety of reasons. First, higher doses of ER/LA opiates packed into single units are believed to pose a greater threat than the millions of short-acting, immediate-release (IR) opioid analgesics units abused annually.3 Another reason for the move focused on the burden to the health system caused by more than 24 similar individual REMS existing in this class. That alone created a virtual paper, regulatory, and health system encumbrance that is expected to be alleviated by a class-wide REMS.
Increasing numbers of prescriptions were an additional consideration. The number of outpatient retail prescriptions dispensed for ER/LA and IR opiates rose dramatically between 2000 and 2009, from 9.3 million to 22.9 million ER/LA opioids and from 164.8 million to 234 million IR opioids [Figure 1].3 Who is prescribing them? You are. In 2009, primary care physicians were the top prescribers of ER/LA (43.8%) and IR (42.1%) opioid analgesics [Figure 2].3 Who are you prescribing them for? Not the elderly age group you might expect. The largest number of prescriptions were written for men and women between ages 50and 59 [Figure 3].3
| FIGURE 1: Total number of prescriptions dispensed for ER/LA and IR opioids from US outpatient retail pharmacies, 2000-2009. |
| ER, extended release; IR, immediate release; LA, long acting; TRx, total prescriptions. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterial/Drug/AnestheticAndLifeSupportDrugsAdvisory Committee/UCM220950.pdf. |
| FIGURE 2: Total number of prescriptions dispensed in the United States by top 10 prescribing specialties for IR and ER/LA opioids, 2009 |
| ANES, anesthesiologists; DO, doctor of osteopathy; EM, emergency medicine; ER, extended release; FM, family medicine; GP, general practitioner; HEM, hematologists; IM, internal medicine; IR, immediate release; LA, long acting; NP, nurse practitioners; ORTH SURG, orthopedic surgeons; NEURO, neurologists; PA, physician assistants; PM&R, physical medicine and rehabilitation; TRx, total prescriptions. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drug/AnestheticAndLifeSupportDrugsAdvisoryCommittee/UCM220950.pdf. |
| FIGURE 3: Total number of unique patients, stratified by age and sex, receiving a dispensed prescription for an ER/LA opioid product from US outpatient retail pharmacies, 2009 |
| ER, extended release; LA, long acting. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndLifeSupportDrugsAdvisoryCommittee/UCM220950.pdf. |
And what are you prescribing them for? Data from a 2009 survey of the prescribing habits of 3200 office-based physicians in 30 specialties showed that most prescriptions written for ER/LA and IR opioids are associated with diagnoses related to pain in the musculoskeletal system and connective tissue (56% [ER/LA] and 30% [IR]). For ER/LA
prescriptions the second most common diagnoses were headaches and nerve pain (14%), while for IR prescriptions they were fractures, sprains, and contusions (23%) [Figure 4].3
| FIGURE 4: Diagnoses associated with use (by grouped ICD-9 codes) for IR and ER/LA opioids as reported by office-based physicians in the United States, 2009 |
| ER, extended release; IR, immediate release; LA, long acting. Source: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndLifeSupportDrugs AdvisoryCommittee/UCM220950.pdf. |
According to Janet Woodcock, MD, Director of the FDA’s Center for Drug Evaluation and Research, some physicians may not be clear about who should receive these drugs or how to manage patients in pain. As a result, some physicians may be reluctant to prescribe opioid analgesics, leaving patients without adequate pain relief. At the same time, other physicians overprescribe them, putting patients—and anyone with access to the family medicine cabinet—at risk.4
A REMS by any other name
And so REMS was conceived. On February 6, 2009, manufacturers of certain opioid drug products received a letter from the FDA informing them that their drugs would be required to have a risk management program, and inviting them to meet to discuss the design and development of such a REMS.5
Two years later, on April 19, 2011, an alarm in the form of an action plan was released by the Obama administration through the Office of National Drug Control Policy. The plan,
Epidemic: Responding to America’s Prescription Drug Abuse Crisis, outlined a set of measures to remedy the problem through education, monitoring, proper disposal of prescription drugs, and enforcement.6
REMS for opioids was the FDA’s response in support of the President’s plan. On the same day in April, 32 manufacturers of ER/LA opioids received a letter from the FDA informing them that they must meet new safety requirements concerning these medications under a single shared, standardized system [Table].
| TABLE: Long-acting and extended-release opioids requiring an opioid REMS |
| Brand Name Products |
| Trade Name | Generic Name | Sponsor | |
| 1 | Duragesic | Fentanyl transdermal system | Ortho-McNeil-Janssen |
| 2 | Dolophine | Methadone HCI tablets | Roxanne Laboratories |
| 3 | Avinza | Morphine sulfate extended-release capsules | King Pharmaceuticals/Pfizer |
| 4 | Kadian capsules | Morphine sulfate extended-release capsules | Actavis |
| 5 | MS Contin | Morphine sulfate controlled-release tablets | Purdue Pharma |
| 6 | Oramorph | Morphine sulfate sustained-release tablets | Xanodyne Pharmaceuticals |
| 7 | OxyContin | Oxycodone HCI controlled-release tablets | Purdue Pharma |
| 8 | Opana ER | Oxymorphone HCI extended-release tablets | Endo Pharmaceuticals |
| 9 | Exalgo | Hydromorphone HCI extendedrelease tablets | Mallinckrodt Inc/Covidien |
| 10 | Butrans | Buprenorphine transdermal system | Purdue Pharma |
| Generic Products |
| Drug Name | Generic Name | Sponsor | |
| 1 | Fentanyl | Fentanyl extended-release transdermal system | Actavis |
| 2 | Fentanyl | Fentanyl extended-release transdermal system | Lavipharm Labs |
| 3 | Fentanyl | Fentanyl extended-release transdermal system | Mallinckrodt Inc/Covidien |
| 4 | Fentanyl | Fentanyl extended-release transdermal system | Mylan Technologies |
| 5 | Fentanyl | Fentanyl extended-release transdermal system | Noven Pharmaceuticals |
| 6 | Fentanyl | Fentanyl extended-release transdermal system | Teva Pharmaceutical Industries |
| 7 | Fentanyl | Fentanyl extended-release transdermal system | Watson Pharmaceuticals |
| 8 | Methadone hydrochloride | Methadone HCl oral solution | The Pharmanetwork |
| 9 | Methadone hydrochloride | Methadone HCl oral solution | Mallinckrodt Inc/Covidien |
| 10 | Methadone hydrochloride | Methadone HCl oral solution | Sandoz |
| 11 | Methadone hydrochloride | Methadone HCl oral solution | Roxane Laboratories |
| 12 | Methadone hydrochloride | Methadone HCl oral solution | VistaPharm |
| 13 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Endo Pharmaceuticals |
| 14 | Morphine sulfate | Morphine sulfate extendedrelease tablets | KV Pharmaceuticals |
| 15 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Mallinckrodt Inc/Covidien |
| 16 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Watson Pharmaceuticals |
| 17 | Morphine sulfate | Morphine sulfate extendedrelease tablets | Rhodes Pharmaceuticals |
| 18 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Mallinckrodt Inc/Covidien |
| 19 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Impax Laboratories |
| 20 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Teva Pharmaceutical Industries |
| 21 | Oxycodone hydrochloride | *Oxycodone HCl extendedrelease tablets | Endo Pharmaceuticals |
| 22 | Oxycodone hydrochloride | Oxymorphone HCl extendedrelease tablets | Impax Laboratories |
| 23 | Oxycodone hydrochloride | Oxymorphone HCl extendedrelease tablets | Actavis |
| *Tentatively approved products. Source: U.S. Food & Drug Administration Web site. http://www.fda.gov/Drugs/DrugSafet/InformationbyDrugClass/ucm251735.htm. |
As outlined in this REMS, manufacturers must provide for the training of prescribers of opioid medications—training that covers proper patient selection, patient counseling in specific product use and risk, and assessment for addiction and tolerance. Manufacturers must also develop factual, nonpromotional patient information and medication guides that will be FDA regulated and approved. Finally, they will be asked to adhere to a timetable to assess whether REMS is meetings its goals.4,5
In May 2011, the FDA met with manufacturers to expand on how to coordinate and implement the REMS requirements.
Hope for a “new normal”
Will REMS for other large medication classes eventually reach beyond opioid analgesics, perhaps warranting practitioners to view REMS as being a good thing as opposed to a nuisance? Your decision to participate in REMS or pass and alter your care approach will need to be made soon. What will you do?
For you as an opioid prescriber, education is the focus, and you will soon be presented with voluntary prescriber education programs. The “hope” is that you will volunteer to take the opioid education program, fill out an electronic or fax form, and send it in to an administrator who will track all those who participate. Since “hope” will unlikely drive large-scale participation, when hope finally runs out the education will become mandatory. This will occur in a year or 2, and will likely become a Drug Enforcement Administration requirement for you to procure CII scheduling.
Unfortunately, there is no guarantee that deaths and overdoses will stop with the opioid REMS. The only guarantee is you will not be able to prescribe these medications at some point if you do not participate in the REMS.
So act now. To be notified when the opioid REMS training becomes available go to www.opioidREMS.com and register. It’s vital that you do ... and relatively painless.
REFERENCES
1. U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality, Food and Drug Administration. Summary of public workshop. Implementation of risk minimization action plans (RiskMAPs) to support quality use of pharmaceuticals: opportunities and challenges. June 25-26, 2007.
2. US. Food and Drug Administration. FDA acts to reduce harm from opioid drugs. Consumer Updates. Available at: http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm251830.htm.
3. Governale L. Outpatient Prescription Opioid Utilization in the U.S., Years 2000 – 2009. Food and Drug Administration, Division of Epidemiology. July 22, 2010. Avilable at: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndLifeSupportDrugsAdvisoryCommittee/UCM220950.pdf
4. Marchand H, moderator. Opioid drugs and risk evaluation and mitigation strategies (REMS) Podcast/transcript. April 20, 2011. Available at: http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm252649.htm.
5. U.S. Food and Drug Administration. Opioid drugs and risk mitigation strategies (REMS) Available at: http://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm163647.htm.
6. Epidemic: responding to America’s prescription drug abuse crisis. Available at: http://www.whitehousedrugpolicy.gov/publications/pdf/rx_abuse_plan.pdf.