User login
Depletive Fluid Management Strategy During Weaning from Mechanical Ventilation Can Lower VAP Rates
Clinical question: What is the benefit associated with a depletive fluid management strategy on ventilator-associated complication (VAC) and ventilator-associated pneumonia (VAP) during weaning from mechanical ventilation?
Background: VAP is common in the ICU. Pulmonary edema predisposes patients to pneumonia by altering the alveolar microenvironment through enhancement of bacterial colonization and infectivity and a decrease in host bactericidal capacities. A fluid management strategy aimed at lowering lung fluid balance may prove useful in reducing both VAC and VAP.
Study design: Randomized controlled trial.
Setting: Nine ICUs in Europe and South America, between May 2007 and July 2009.
Synopsis: Data from the B-type Natriuretic Peptide for the Management of Weaning (BMW) trial was used to compare the cumulative incidence of VAC and VAP between the biomarker-driven, depletive fluid management group and the usual care group during the 14 days following randomization. The trial enrolled 304 randomized patients, 152 in each group.
Compared with usual care, the interventional strategy was associated with a higher proportion of patients receiving diuretics, in higher doses, resulting in a significantly more negative fluid balance during weaning and a shorter duration of mechanical ventilation. VAC (as defined by worsening oxygenation) occurred in 13.2% of patients during the 14 days following randomization: 17.8% in the usual care group and 8.6% in the interventional group. VAP occurred in 13.5% during the 14 days following randomization: 17.8% in the usual care group and 9.2% in the interventional group.
Bottom line: A biomarker-driven, depletive fluid strategy decreases the cumulative incidence of VAC and VAP.
Citation: Mekontso Dessap A, Katsahian S, Roche-Campo F, et al. Ventilator-associated pneumonia during weaning from mechanical ventilation: role of fluid management. Chest. 2014;146(1):58-65.
Visit our website for more physician reviews of HM-related research.
Clinical question: What is the benefit associated with a depletive fluid management strategy on ventilator-associated complication (VAC) and ventilator-associated pneumonia (VAP) during weaning from mechanical ventilation?
Background: VAP is common in the ICU. Pulmonary edema predisposes patients to pneumonia by altering the alveolar microenvironment through enhancement of bacterial colonization and infectivity and a decrease in host bactericidal capacities. A fluid management strategy aimed at lowering lung fluid balance may prove useful in reducing both VAC and VAP.
Study design: Randomized controlled trial.
Setting: Nine ICUs in Europe and South America, between May 2007 and July 2009.
Synopsis: Data from the B-type Natriuretic Peptide for the Management of Weaning (BMW) trial was used to compare the cumulative incidence of VAC and VAP between the biomarker-driven, depletive fluid management group and the usual care group during the 14 days following randomization. The trial enrolled 304 randomized patients, 152 in each group.
Compared with usual care, the interventional strategy was associated with a higher proportion of patients receiving diuretics, in higher doses, resulting in a significantly more negative fluid balance during weaning and a shorter duration of mechanical ventilation. VAC (as defined by worsening oxygenation) occurred in 13.2% of patients during the 14 days following randomization: 17.8% in the usual care group and 8.6% in the interventional group. VAP occurred in 13.5% during the 14 days following randomization: 17.8% in the usual care group and 9.2% in the interventional group.
Bottom line: A biomarker-driven, depletive fluid strategy decreases the cumulative incidence of VAC and VAP.
Citation: Mekontso Dessap A, Katsahian S, Roche-Campo F, et al. Ventilator-associated pneumonia during weaning from mechanical ventilation: role of fluid management. Chest. 2014;146(1):58-65.
Visit our website for more physician reviews of HM-related research.
Clinical question: What is the benefit associated with a depletive fluid management strategy on ventilator-associated complication (VAC) and ventilator-associated pneumonia (VAP) during weaning from mechanical ventilation?
Background: VAP is common in the ICU. Pulmonary edema predisposes patients to pneumonia by altering the alveolar microenvironment through enhancement of bacterial colonization and infectivity and a decrease in host bactericidal capacities. A fluid management strategy aimed at lowering lung fluid balance may prove useful in reducing both VAC and VAP.
Study design: Randomized controlled trial.
Setting: Nine ICUs in Europe and South America, between May 2007 and July 2009.
Synopsis: Data from the B-type Natriuretic Peptide for the Management of Weaning (BMW) trial was used to compare the cumulative incidence of VAC and VAP between the biomarker-driven, depletive fluid management group and the usual care group during the 14 days following randomization. The trial enrolled 304 randomized patients, 152 in each group.
Compared with usual care, the interventional strategy was associated with a higher proportion of patients receiving diuretics, in higher doses, resulting in a significantly more negative fluid balance during weaning and a shorter duration of mechanical ventilation. VAC (as defined by worsening oxygenation) occurred in 13.2% of patients during the 14 days following randomization: 17.8% in the usual care group and 8.6% in the interventional group. VAP occurred in 13.5% during the 14 days following randomization: 17.8% in the usual care group and 9.2% in the interventional group.
Bottom line: A biomarker-driven, depletive fluid strategy decreases the cumulative incidence of VAC and VAP.
Citation: Mekontso Dessap A, Katsahian S, Roche-Campo F, et al. Ventilator-associated pneumonia during weaning from mechanical ventilation: role of fluid management. Chest. 2014;146(1):58-65.
Visit our website for more physician reviews of HM-related research.
Epidemiology, Consequences of Non-Leg VTE in Critically Ill Patients
Clinical question: Which risk factors are key in the development of non-leg deep vein thromboses (NLDVTs), and what are the expected clinical sequelae from these events?
Background: Critically ill patients are at increased risk of venous thrombosis. Despite adherence to recommended daily thromboprophylaxis, many patients will develop a venous thrombosis in a vein other than the lower extremity. The association between NLDVT and pulmonary embolism (PE) or death is less clearly identified.
Study design: The PROphylaxis for ThromboEmbolism in Critical Care Trial (PROTECT), a multicenter, randomized, blinded, and concealed prospective cohort study occurring between May 2006 and June 2010.
Setting: Sixty-seven international secondary and tertiary care ICUs in both academic and community settings.
Synopsis: Researchers enrolled 3,746 ICU patients in a randomized controlled trial of dalteparin versus standard heparin for thromboprophylaxis. Of these patients, 84 (2.2%) developed a NLDVT. These thromboses were more likely to be deep and located proximally.
Risk factors were assessed using five selected variables: APACHE (acute physiology and chronic health evaluation), BMI, malignancy, and treatment with vasopressors or statins. Outside of indwelling upper extremity central venous catheters, cancer was the only independent predictor of NLDVT.
Compared to patients without any VTE, those with NLDVT were more likely to develop PE (14.9% versus 1.9%) and have longer ICU stays (19 versus nine days). On average, one in seven patients with NLDVT developed PE during the hospital stay. Despite the association with PE, NLDVT was not associated with an increased ICU mortality in an adjusted model. However, the PROTECT trial may have been underpowered to detect a difference. Additional limitations of the study included a relatively small total number of NLDVTs and a lack of standardized screening protocols for both NLDVT and PE.
Bottom line: Despite universal heparin thromboprophylaxis, many medical-surgical critically ill patients may develop NLDVT, placing them at higher risk for longer ICU stays and PE. TH
Citation: Lamontagne F, McIntyre L, Dodek P, et al. Nonleg venous thrombosis in critically ill adults: a nested prospective cohort study. JAMA Intern Med. 2014;174(5):689-696.
Clinical question: Which risk factors are key in the development of non-leg deep vein thromboses (NLDVTs), and what are the expected clinical sequelae from these events?
Background: Critically ill patients are at increased risk of venous thrombosis. Despite adherence to recommended daily thromboprophylaxis, many patients will develop a venous thrombosis in a vein other than the lower extremity. The association between NLDVT and pulmonary embolism (PE) or death is less clearly identified.
Study design: The PROphylaxis for ThromboEmbolism in Critical Care Trial (PROTECT), a multicenter, randomized, blinded, and concealed prospective cohort study occurring between May 2006 and June 2010.
Setting: Sixty-seven international secondary and tertiary care ICUs in both academic and community settings.
Synopsis: Researchers enrolled 3,746 ICU patients in a randomized controlled trial of dalteparin versus standard heparin for thromboprophylaxis. Of these patients, 84 (2.2%) developed a NLDVT. These thromboses were more likely to be deep and located proximally.
Risk factors were assessed using five selected variables: APACHE (acute physiology and chronic health evaluation), BMI, malignancy, and treatment with vasopressors or statins. Outside of indwelling upper extremity central venous catheters, cancer was the only independent predictor of NLDVT.
Compared to patients without any VTE, those with NLDVT were more likely to develop PE (14.9% versus 1.9%) and have longer ICU stays (19 versus nine days). On average, one in seven patients with NLDVT developed PE during the hospital stay. Despite the association with PE, NLDVT was not associated with an increased ICU mortality in an adjusted model. However, the PROTECT trial may have been underpowered to detect a difference. Additional limitations of the study included a relatively small total number of NLDVTs and a lack of standardized screening protocols for both NLDVT and PE.
Bottom line: Despite universal heparin thromboprophylaxis, many medical-surgical critically ill patients may develop NLDVT, placing them at higher risk for longer ICU stays and PE. TH
Citation: Lamontagne F, McIntyre L, Dodek P, et al. Nonleg venous thrombosis in critically ill adults: a nested prospective cohort study. JAMA Intern Med. 2014;174(5):689-696.
Clinical question: Which risk factors are key in the development of non-leg deep vein thromboses (NLDVTs), and what are the expected clinical sequelae from these events?
Background: Critically ill patients are at increased risk of venous thrombosis. Despite adherence to recommended daily thromboprophylaxis, many patients will develop a venous thrombosis in a vein other than the lower extremity. The association between NLDVT and pulmonary embolism (PE) or death is less clearly identified.
Study design: The PROphylaxis for ThromboEmbolism in Critical Care Trial (PROTECT), a multicenter, randomized, blinded, and concealed prospective cohort study occurring between May 2006 and June 2010.
Setting: Sixty-seven international secondary and tertiary care ICUs in both academic and community settings.
Synopsis: Researchers enrolled 3,746 ICU patients in a randomized controlled trial of dalteparin versus standard heparin for thromboprophylaxis. Of these patients, 84 (2.2%) developed a NLDVT. These thromboses were more likely to be deep and located proximally.
Risk factors were assessed using five selected variables: APACHE (acute physiology and chronic health evaluation), BMI, malignancy, and treatment with vasopressors or statins. Outside of indwelling upper extremity central venous catheters, cancer was the only independent predictor of NLDVT.
Compared to patients without any VTE, those with NLDVT were more likely to develop PE (14.9% versus 1.9%) and have longer ICU stays (19 versus nine days). On average, one in seven patients with NLDVT developed PE during the hospital stay. Despite the association with PE, NLDVT was not associated with an increased ICU mortality in an adjusted model. However, the PROTECT trial may have been underpowered to detect a difference. Additional limitations of the study included a relatively small total number of NLDVTs and a lack of standardized screening protocols for both NLDVT and PE.
Bottom line: Despite universal heparin thromboprophylaxis, many medical-surgical critically ill patients may develop NLDVT, placing them at higher risk for longer ICU stays and PE. TH
Citation: Lamontagne F, McIntyre L, Dodek P, et al. Nonleg venous thrombosis in critically ill adults: a nested prospective cohort study. JAMA Intern Med. 2014;174(5):689-696.
In the Literature: Hospital-Based Research You Need to Know
Clinical question: Is routine preoperative urine screening beneficial?
Background: The value of preoperative urine screening is unproven, except before urologic procedures. Furthermore, treatment of asymptomatic bacteriuria may lead to adverse events, including diarrhea, allergic reactions, and Clostridium difficile infection (CDI).
Study design: Retrospective chart review.
Setting: Patients who underwent cardiothoracic, orthopedic, and vascular surgeries at the Minneapolis Veterans Affairs Medical Center in 2010.
Synopsis: A total of 1,934 procedures were performed on 1,699 patients, most of which were orthopedics procedures (1,291 in 1,115 patients). A urine culture was obtained before 25% of procedures with significant variation by service (cardiothoracic, 85%; vascular, 48%; orthopedic, 4%). Bacteriuria was detected in 11% of urine cultures (54 of 489), but antimicrobial drugs were dispensed to just 16 patients.
To identify correlates of preoperative urine culture use, patients with and without urine cultures were compared. The rate of surgical-site infection was similar for both groups. Postoperative UTI was more frequent among patients with bacteriuria. Rates of diarrhea, allergy, and CDI did not differ. Paradoxically, patients treated for preoperative UTI were more likely to develop surgical-site infections (45% vs. 14%; P=0.03). Postoperative UTI was also more frequent among treated patients versus untreated patients (18% vs. 7%).
Bottom line: This is the largest study to assess outcomes for routine preoperative urine cultures. These findings demonstrate that preoperative screening for, and treatment of, asymptomatic bacteriuria should be avoided in patients undergoing nonurologic surgical procedures.
Citation: Drekonja DM, Zarmbinski B, Johnson JR. Preoperative urine culture at a veterans affairs medical center. JAMA Intern Med. 2013;173(1):71-72.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Is routine preoperative urine screening beneficial?
Background: The value of preoperative urine screening is unproven, except before urologic procedures. Furthermore, treatment of asymptomatic bacteriuria may lead to adverse events, including diarrhea, allergic reactions, and Clostridium difficile infection (CDI).
Study design: Retrospective chart review.
Setting: Patients who underwent cardiothoracic, orthopedic, and vascular surgeries at the Minneapolis Veterans Affairs Medical Center in 2010.
Synopsis: A total of 1,934 procedures were performed on 1,699 patients, most of which were orthopedics procedures (1,291 in 1,115 patients). A urine culture was obtained before 25% of procedures with significant variation by service (cardiothoracic, 85%; vascular, 48%; orthopedic, 4%). Bacteriuria was detected in 11% of urine cultures (54 of 489), but antimicrobial drugs were dispensed to just 16 patients.
To identify correlates of preoperative urine culture use, patients with and without urine cultures were compared. The rate of surgical-site infection was similar for both groups. Postoperative UTI was more frequent among patients with bacteriuria. Rates of diarrhea, allergy, and CDI did not differ. Paradoxically, patients treated for preoperative UTI were more likely to develop surgical-site infections (45% vs. 14%; P=0.03). Postoperative UTI was also more frequent among treated patients versus untreated patients (18% vs. 7%).
Bottom line: This is the largest study to assess outcomes for routine preoperative urine cultures. These findings demonstrate that preoperative screening for, and treatment of, asymptomatic bacteriuria should be avoided in patients undergoing nonurologic surgical procedures.
Citation: Drekonja DM, Zarmbinski B, Johnson JR. Preoperative urine culture at a veterans affairs medical center. JAMA Intern Med. 2013;173(1):71-72.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Is routine preoperative urine screening beneficial?
Background: The value of preoperative urine screening is unproven, except before urologic procedures. Furthermore, treatment of asymptomatic bacteriuria may lead to adverse events, including diarrhea, allergic reactions, and Clostridium difficile infection (CDI).
Study design: Retrospective chart review.
Setting: Patients who underwent cardiothoracic, orthopedic, and vascular surgeries at the Minneapolis Veterans Affairs Medical Center in 2010.
Synopsis: A total of 1,934 procedures were performed on 1,699 patients, most of which were orthopedics procedures (1,291 in 1,115 patients). A urine culture was obtained before 25% of procedures with significant variation by service (cardiothoracic, 85%; vascular, 48%; orthopedic, 4%). Bacteriuria was detected in 11% of urine cultures (54 of 489), but antimicrobial drugs were dispensed to just 16 patients.
To identify correlates of preoperative urine culture use, patients with and without urine cultures were compared. The rate of surgical-site infection was similar for both groups. Postoperative UTI was more frequent among patients with bacteriuria. Rates of diarrhea, allergy, and CDI did not differ. Paradoxically, patients treated for preoperative UTI were more likely to develop surgical-site infections (45% vs. 14%; P=0.03). Postoperative UTI was also more frequent among treated patients versus untreated patients (18% vs. 7%).
Bottom line: This is the largest study to assess outcomes for routine preoperative urine cultures. These findings demonstrate that preoperative screening for, and treatment of, asymptomatic bacteriuria should be avoided in patients undergoing nonurologic surgical procedures.
Citation: Drekonja DM, Zarmbinski B, Johnson JR. Preoperative urine culture at a veterans affairs medical center. JAMA Intern Med. 2013;173(1):71-72.
Visit our website for more physician reviews of recent HM-relevant literature.
ITL: Physician Reviews of HM-Relevant Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Value of routine preoperative urine screening assessed
- Impact of hospitalist-led intermediate care on patient survival
- Risks of blood transfusion to treat upper GI bleeding
- Low-dose steroids and increased mortality in sepsis
- Reduced length of stay and hospital readmission rates
- Restrictive blood transfusion strategies better for acute myocardial infarction
- Trends in GI illnesses and their associated costs
- Apixaban as a stand-alone anticoagulant in patients with VTE
- Guidelines for upper endoscopy use in gastroesophageal reflux disease
Avoid Preoperative Urine Culture in Nonurologic Surgical Procedures
Clinical question: Is routine preoperative urine screening beneficial?
Background: The value of preoperative urine screening is unproven, except before urologic procedures. Furthermore, treatment of asymptomatic bacteriuria may lead to adverse events, including diarrhea, allergic reactions, and Clostridium difficile infection (CDI).
Study design: Retrospective chart review.
Setting: Patients who underwent cardiothoracic, orthopedic, and vascular surgeries at the Minneapolis Veterans Affairs Medical Center in 2010.
Synopsis: A total of 1,934 procedures were performed on 1,699 patients, most of which were orthopedics procedures (1,291 in 1,115 patients). A urine culture was obtained before 25% of procedures with significant variation by service (cardiothoracic, 85%; vascular, 48%; orthopedic, 4%). Bacteriuria was detected in 11% of urine cultures (54 of 489), but antimicrobial drugs were dispensed to just 16 patients.
To identify correlates of preoperative urine culture use, patients with and without urine cultures were compared. The rate of surgical-site infection was similar for both groups. Postoperative UTI was more frequent among patients with bacteriuria. Rates of diarrhea, allergy, and CDI did not differ. Paradoxically, patients treated for preoperative UTI were more likely to develop surgical-site infections (45% vs. 14%; P=0.03). Postoperative UTI was also more frequent among treated patients versus untreated patients (18% vs. 7%).
Bottom line: This is the largest study to assess outcomes for routine preoperative urine cultures. These findings demonstrate that preoperative screening for, and treatment of, asymptomatic bacteriuria should be avoided in patients undergoing nonurologic surgical procedures.
Citation: Drekonja DM, Zarmbinski B, Johnson JR. Preoperative urine culture at a veterans affairs medical center. JAMA Intern Med. 2013;173(1):71-72.
Intermediate Care Staffed by Hospitalists: Impact on Mortality, Comanagement, and Teaching
Clinical question: Does a hospitalist-led intermediate-care unit improve patient survival?
Background: Hospitalized patients are complex, and institutions often have to balance matching patient acuity to either an ICU or a regular ward. However, an intermediate-care setting might be an attractive strategy to provide rational care according to patient needs while expanding comanagement and teaching services.
Study design: Retrospective observational study.
Setting: Intermediate-care unit of a single academic hospital.
Synopsis: In-hospital mortality in this intermediate-care unit was 20.6%, whereas the expected mortality was 23.2% based on Simplified Acute Physiology Score II (SAPS II) score. The correlation between SAPS II predicted and observed death rates was accurate and statistically significant (P<0.001). Comanagement was performed with several medical and surgical teams, with an increase in perioperative comanagement of 22.7% (P=0.014). The number of training residents in the intermediate-care unit increased to 30.4% from 4.3% (P=0.002).
Bottom line: An intermediate-care unit led by hospitalists showed encouraging results in patient mortality, as well as comanagement and teaching opportunities.
Citation: Lucena JF, Alegre F, Rodil R, et al. Results of a retrospective observational study of intermediate care staffed by hospitalists: impact on mortality, co-management, and teaching. J Hosp Med. 2012;7(5):411-415.
Blood Transfusion Associated with Increased Risk of Rebleeding in Patients with Nonvariceal Upper GI Bleeding
Clinical question: Does more liberal use of blood transfusions in the setting of nonvariceal upper GI bleeding result in patient harm?
Background: Randomized controlled trials have demonstrated that a more liberal approach to blood transfusions for patients in the medical intensive-care unit results in higher mortality. However, the potential harmful effect of blood transfusions in the setting of GI bleeding has not been demonstrated.
Study design: Retrospective cohort study.
Setting: Canadian hospitals.
Synopsis: Based on a retrospective analysis of the Canadian Registry of patients with Upper Gastrointestinal Bleeding and Endoscopy (RUGBE), the authors determined there was a statistically significant association between patients who received a blood transfusion for the management of nonvariceal upper GI bleeding and the risk of rebleeding. The rate of rebleeding in patients who received a blood transfusion was 23.6% compared with 11.3% in patients who were not transfused (P<0.01). There was no statistically significant difference in mortality.
Although this was a reasonably large observational study that included 1,677 patients with nonvariceal upper GI bleeding, it is vulnerable to confounding. It suggests the need to further study potential harm of blood transfusion in the setting of GI bleeding, but it should not result in a change in clinical practice at this time.
Bottom line: Prospective randomized studies are needed to determine if there are harmful effects of blood transfusions in the setting of GI bleeding and to better define a threshold for transfusion.
Citation: Restellini S, Kherad O, Jairath V, Martel M, Barkun AN. Red blood cell transfusion is associated with increased rebleeding in patients with nonvariceal upper gastrointestinal bleeding. Aliment Pharmacol Ther. 2013;37:316-322.
Low-Dose Steroids in Sepsis Associated with Increase in Mortality
Clinical question: What is the role of steroids in the treatment of adult patients with sepsis?
Background: The Surviving Sepsis Campaign guidelines have previously recommended administering steroids to patients with septic shock not responsive to fluid resuscitation and who require vasopressors. However, prior randomized clinical trials studying the use of steroids in these settings have produced conflicting results.
Study design: Retrospective cohort study.
Setting: Two hundred fifty-two hospitals in North America, South America, and Europe.
Synopsis: The Surviving Sepsis Campaign management bundle has been shown to reduce mortality in patients with sepsis. However, it is not known which particular elements of the management bundle result in improved mortality. The Surviving Sepsis Campaign database included 17,847 patients who required vasopressor therapy after adequate fluid resuscitation. This subgroup was analyzed to see if there was a difference in mortality between patients who received low-dose steroids versus those who did not receive steroids. The mortality rate among those who received steroids was statistically higher (with odds ratio of 1.18 and P<0.001) compared with those who did not receive steroids. This finding adds to the body of evidence that calls into question the commonplace practice of administrating steroids to septic patients on vasopressor therapy.
The most recent campaign guidelines recommend the use of steroids in septic patients only if both adequate fluid resuscitation and vasopressor therapy are not able to restore hemodynamic stability.
Bottom line: Further studies are needed to better define the role of steroids in the treatment of sepsis.
Citation: Casserly B, Gerlach H, Phillips GS, et al. Low-dose steroids in adult septic shock: results of the Surviving Sepsis Campaign. Intensive Care Med. 2012;38:1946-1954.
Link Between Length of Stay and Readmission Rates
Clinical question: How has reducing length of stay affected hospital readmission rates?
Background: There are ongoing concerns that improving a hospital’s efficiency by reducing length of stay (LOS) could be associated with higher hospital readmission rates. However, no studies evaluating the relationship between LOS and readmission rates have been done using recent data.
Study design: Retrospective observational study.
Setting: All acute-care Veterans Affairs (VA) hospitals in the U.S.
Synopsis: A total of 4,124,907 index admissions were included in the final sample from all acute medical admissions in 129 acute-care VA hospitals from October 1996 to September 2010. The primary outcomes were the hospital LOS and the 30-day readmission rate. Index admissions for heart failure, chronic obstructive pulmonary disease (COPD), acute myocardial infarction (AMI), community-acquired pneumonia, and gastrointestinal hemorrhage were also analyzed separately.
The risk-adjusted analysis of LOS demonstrated significant reductions for all admissions over the 14-year period, to 3.98 days from 5.44 days, and for all of the individual conditions with reductions ranging from 1.40 days for gastrointestinal hemorrhage to 2.85 days for AMI. There were similar significant reductions in 30-day readmission rates for all admissions to 13.8% from 16.5% and within the individual conditions ranging from 0.9% in community-acquired pneumonia to 3.3% in COPD. These results show that the reductions in LOS did not increase the risk of readmissions. The major limitation of the study was that these data are only from a single healthcare system.
Bottom line: Data from VA hospitals show that reductions in LOS do not have adverse effects on 30-day readmission rates; instead, both LOS and readmission rates improved over the same time period.
Citation: Kaboli PJ, Go JT, Hockenberry J, et al. Associations between reduced hospital length of stay and 30-day readmission rate and mortality: 14-year experience in 129 Veterans Affairs hospitals. Ann Intern Med. 2012;157:837-845.
Better to Restrict Blood Transfusions in Acute Myocardial Infarction
Clinical question: Is a liberal or restrictive blood transfusion strategy better in patients with anemia and acute myocardial infarction?
Background: Patients with acute myocardial infarction (AMI) are often given therapies that can increase their risk for bleeding and anemia, and it is known that AMI patients have a worse prognosis if they have concomitant anemia. No clear consensus exists on the benefit or harm of blood transfusions in AMI patients.
Study design: Systematic review and meta-analysis.
Setting: Ten articles included in the qualitative and quantitative analyses out of 729 screened articles from Jan. 1, 1966, to March 31, 2012, using the search terms “transfusion,” “myocardial infarction,” and “mortality” in English language.
Synopsis: A total of 203,665 study participants were identified from the 10 studies (one randomized and nine observational) that met the inclusion and exclusion criteria. All-cause mortality was significantly higher in AMI patients who received a blood transfusion compared with those who did not (18.2% vs. 10.2%). However, this difference was not statistically significant in patients that had a STEMI or in patients with a baseline hematocrit less than 30%. A multivariate meta-regression with several covariates, excluding demographics, also showed that blood transfusion was associated with higher mortality and higher risk for subsequent myocardial infarction. There was significant heterogeneity in all results, but no single study was found as the source of the heterogeneity, and no significant publication bias was identified. The major limitations to this study are that there is a paucity of randomized trials available that pertain to this specific topic and the authors did not have patient-level covariates to include in their analyses.
Bottom line: There appears to be an increased risk of mortality and subsequent myocardial infarction in AMI patients who receive blood transfusions versus those who do not.
Citation: Chatterjee S, Wetterslev J, Sharma A, Lichstein E, Mukherjee D. Association of blood transfusion with increased mortality in myocardial infarction: a meta-analysis and diversity-adjusted study sequential analysis. JAMA Intern Med. 2013;173(2):132-139.
Trends in GI Illnesses and Their Associated Costs
Clinical question: What are the new trends in GI illnesses and their associated costs?
Background: The frequency of illnesses and their treatment costs have changed over the last decade. In order to help healthcare providers focus their attention on these new trends, a new compilation of data is needed.
Study design: Epidemiological analysis.
Setting: Various governmental and private databases representing outpatient clinics, hospitals, and death certificates from multiple regions of the U.S.
Synopsis: The analysis was blinded to patient identifiers but represented multiple regions of the U.S. Symptoms were abstracted from patient surveys, and the rest of the data were collected from record review. The most common reported symptoms were abdominal pain, followed by nausea, vomiting, diarrhea, constipation, and heartburn. The most common clinic diagnoses were reflux, abdominal pain, enteritis/dyspepsia, and constipation. The most common inpatient discharge primary diagnoses included acute pancreatitis, cholecystitis, and diverticulitis. Impressive increases were seen in the number of morbidly obese, C. diff, and fatty liver diagnoses.
Colon cancer was the most common GI malignancy and had the highest mortality. C. diff was the ninth-leading cause of GI-related deaths. All types of scopes (except endoscopic retrograde cholangiopancreatography) were performed more commonly now than in the past, with colonoscopy being the most common. The most common indication for an upper endoscopy was reflux, which was also the most common outpatient GI diagnosis.
Bottom line: Healthcare providers need to be aware of new GI illness trends and their associated costs.
Citation: Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterol. 2012;143:1179-1187.
Is Apixaban a Good Stand-Alone Anticoagulant for Extended Treatment in VTE Patients?
Clinical question: Is apixaban an option for the extended treatment of VTE in a simple, fixed-dose regimen?
Background: Apixaban is an oral factor Xa inhibitor that is administered in fixed doses without the need for laboratory monitoring. In the Apixaban after the Initial Management of Pulmonary Embolism and Deep Vein Thrombosis with First-Line Therapy—Extended Treatment (AMPLIFY-EXT) study, investigators compared the efficacy and safety of two doses of apixaban (2.5 mg and 5 mg) with those of placebo in patients with VTE who had completed six to 12 months of anticoagulation therapy and for whom treating physicians were uncertain about continuing therapy. Additional aims of the study were to determine whether the lower dose of apixaban was effective and whether it was associated with less bleeding than the higher dose, and to examine the effect of treatment on arterial thrombotic outcomes.
Study design: Randomized, double-blind study.
Synopsis: A total of 2,486 patients underwent randomization, 2,482 of whom were included in the intention-to-treat analyses. Symptomatic recurrent VTE or death from VTE occurred in 73 of the 829 patients (8.8%) who were receiving placebo, compared with 14 of the 840 patients (1.7%) who were receiving 2.5 mg of apixaban (a difference of 7.2 percentage points; 95% confidence interval [CI], 5.0 to 9.3) and 14 of the 813 patients (1.7%) who were receiving 5 mg of apixaban (a difference of 7.0 percentage points; 95% CI, 4.9 to 9.1) (P<0.001 for both comparisons). The rates of major bleeding were 0.5% in the placebo group, 0.2% in the 2.5-mg apixaban group, and 0.1% in the 5-mg apixaban group. The rates of clinically relevant nonmajor bleeding were 2.3% in the placebo group, 3.0% in the 2.5-mg apixaban group, and 4.2% in the 5-mg apixaban group. The rate of death from any cause was 1.7% in the placebo group, compared with 0.8% in the 2.5-mg apixaban group and 0.5% in the 5-mg apixaban group.
Bottom line: Apixaban is a safe and effective anticoagulant for extended anticoagulation in patients with VTE initially treated with six to 12 months of warfarin.
Citation: Agnelli GM, Buller HR, Cohen A, et al. Apixaban for extended treatment of venous thromboembolism. N Engl J Med. 2013;368(8):699-708.
ACP Guideline Review: Upper Endoscopy for Gastroesophageal Reflux Disease
Clinical question: What are the indications of upper endoscopy in the setting of gastroesophageal reflux disease (GERD)?
Background: GERD is a common condition. Upper endoscopy is widely available and routinely used for diagnosis and management of GERD and its complications. The indications for this procedure are not clearly defined. Overuse of upper endoscopy contributes to higher healthcare costs without improving patient outcomes.
Study design: Literature review and comparison of clinical guidelines from professional organizations by a team of general internists, gastroenterologists, and clinical epidemiologists. The document was not based on a formal systemic review but was intended to provide practical advice based on the best available evidence.
Synopsis: Best practice advice No. 1: Upper endoscopy is indicated in men and women with heartburn and alarm symptoms (dysphagia, bleeding, anemia, weight loss, and recurrent vomiting).
Best practice advice No. 2: Upper endoscopy is indicated in men and women with typical GERD symptoms that persist despite a therapeutic trial of four to eight weeks of twice-daily proton-pump inhibitor therapy, severe erosive esophagitis after a two-month course of proton-pump inhibitor therapy to assess healing and rule out Barrett esophagus, and history of esophageal stricture who have recurrent symptoms of dysphagia.
Best practice advice No. 3: Upper endoscopy might be indicated in men older than 50 with chronic GERD symptoms (symptoms for more than five years) and additional risk factors (nocturnal reflux symptoms, hiatal hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat) to detect esophageal adenocarcinoma and Barrett esophagus. It might also be indicated for surveillance evaluation in men and women with a history of Barrett esophagus. In men and women with Barrett esophagus and no dysplasia, surveillance examinations should occur at intervals no more frequently than three to five years. More frequent intervals are indicated in patients with Barrett esophagus and dysplasia.
Bottom line: Use upper endoscopy selectively for patients with GERD.
Citation: Shaheen NJ, Weinberg DS, Denberg TD, et al. Upper endoscopy for gastroesophageal reflux disease: best practice advice from the Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med. 2012;157(11):808-816.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Value of routine preoperative urine screening assessed
- Impact of hospitalist-led intermediate care on patient survival
- Risks of blood transfusion to treat upper GI bleeding
- Low-dose steroids and increased mortality in sepsis
- Reduced length of stay and hospital readmission rates
- Restrictive blood transfusion strategies better for acute myocardial infarction
- Trends in GI illnesses and their associated costs
- Apixaban as a stand-alone anticoagulant in patients with VTE
- Guidelines for upper endoscopy use in gastroesophageal reflux disease
Avoid Preoperative Urine Culture in Nonurologic Surgical Procedures
Clinical question: Is routine preoperative urine screening beneficial?
Background: The value of preoperative urine screening is unproven, except before urologic procedures. Furthermore, treatment of asymptomatic bacteriuria may lead to adverse events, including diarrhea, allergic reactions, and Clostridium difficile infection (CDI).
Study design: Retrospective chart review.
Setting: Patients who underwent cardiothoracic, orthopedic, and vascular surgeries at the Minneapolis Veterans Affairs Medical Center in 2010.
Synopsis: A total of 1,934 procedures were performed on 1,699 patients, most of which were orthopedics procedures (1,291 in 1,115 patients). A urine culture was obtained before 25% of procedures with significant variation by service (cardiothoracic, 85%; vascular, 48%; orthopedic, 4%). Bacteriuria was detected in 11% of urine cultures (54 of 489), but antimicrobial drugs were dispensed to just 16 patients.
To identify correlates of preoperative urine culture use, patients with and without urine cultures were compared. The rate of surgical-site infection was similar for both groups. Postoperative UTI was more frequent among patients with bacteriuria. Rates of diarrhea, allergy, and CDI did not differ. Paradoxically, patients treated for preoperative UTI were more likely to develop surgical-site infections (45% vs. 14%; P=0.03). Postoperative UTI was also more frequent among treated patients versus untreated patients (18% vs. 7%).
Bottom line: This is the largest study to assess outcomes for routine preoperative urine cultures. These findings demonstrate that preoperative screening for, and treatment of, asymptomatic bacteriuria should be avoided in patients undergoing nonurologic surgical procedures.
Citation: Drekonja DM, Zarmbinski B, Johnson JR. Preoperative urine culture at a veterans affairs medical center. JAMA Intern Med. 2013;173(1):71-72.
Intermediate Care Staffed by Hospitalists: Impact on Mortality, Comanagement, and Teaching
Clinical question: Does a hospitalist-led intermediate-care unit improve patient survival?
Background: Hospitalized patients are complex, and institutions often have to balance matching patient acuity to either an ICU or a regular ward. However, an intermediate-care setting might be an attractive strategy to provide rational care according to patient needs while expanding comanagement and teaching services.
Study design: Retrospective observational study.
Setting: Intermediate-care unit of a single academic hospital.
Synopsis: In-hospital mortality in this intermediate-care unit was 20.6%, whereas the expected mortality was 23.2% based on Simplified Acute Physiology Score II (SAPS II) score. The correlation between SAPS II predicted and observed death rates was accurate and statistically significant (P<0.001). Comanagement was performed with several medical and surgical teams, with an increase in perioperative comanagement of 22.7% (P=0.014). The number of training residents in the intermediate-care unit increased to 30.4% from 4.3% (P=0.002).
Bottom line: An intermediate-care unit led by hospitalists showed encouraging results in patient mortality, as well as comanagement and teaching opportunities.
Citation: Lucena JF, Alegre F, Rodil R, et al. Results of a retrospective observational study of intermediate care staffed by hospitalists: impact on mortality, co-management, and teaching. J Hosp Med. 2012;7(5):411-415.
Blood Transfusion Associated with Increased Risk of Rebleeding in Patients with Nonvariceal Upper GI Bleeding
Clinical question: Does more liberal use of blood transfusions in the setting of nonvariceal upper GI bleeding result in patient harm?
Background: Randomized controlled trials have demonstrated that a more liberal approach to blood transfusions for patients in the medical intensive-care unit results in higher mortality. However, the potential harmful effect of blood transfusions in the setting of GI bleeding has not been demonstrated.
Study design: Retrospective cohort study.
Setting: Canadian hospitals.
Synopsis: Based on a retrospective analysis of the Canadian Registry of patients with Upper Gastrointestinal Bleeding and Endoscopy (RUGBE), the authors determined there was a statistically significant association between patients who received a blood transfusion for the management of nonvariceal upper GI bleeding and the risk of rebleeding. The rate of rebleeding in patients who received a blood transfusion was 23.6% compared with 11.3% in patients who were not transfused (P<0.01). There was no statistically significant difference in mortality.
Although this was a reasonably large observational study that included 1,677 patients with nonvariceal upper GI bleeding, it is vulnerable to confounding. It suggests the need to further study potential harm of blood transfusion in the setting of GI bleeding, but it should not result in a change in clinical practice at this time.
Bottom line: Prospective randomized studies are needed to determine if there are harmful effects of blood transfusions in the setting of GI bleeding and to better define a threshold for transfusion.
Citation: Restellini S, Kherad O, Jairath V, Martel M, Barkun AN. Red blood cell transfusion is associated with increased rebleeding in patients with nonvariceal upper gastrointestinal bleeding. Aliment Pharmacol Ther. 2013;37:316-322.
Low-Dose Steroids in Sepsis Associated with Increase in Mortality
Clinical question: What is the role of steroids in the treatment of adult patients with sepsis?
Background: The Surviving Sepsis Campaign guidelines have previously recommended administering steroids to patients with septic shock not responsive to fluid resuscitation and who require vasopressors. However, prior randomized clinical trials studying the use of steroids in these settings have produced conflicting results.
Study design: Retrospective cohort study.
Setting: Two hundred fifty-two hospitals in North America, South America, and Europe.
Synopsis: The Surviving Sepsis Campaign management bundle has been shown to reduce mortality in patients with sepsis. However, it is not known which particular elements of the management bundle result in improved mortality. The Surviving Sepsis Campaign database included 17,847 patients who required vasopressor therapy after adequate fluid resuscitation. This subgroup was analyzed to see if there was a difference in mortality between patients who received low-dose steroids versus those who did not receive steroids. The mortality rate among those who received steroids was statistically higher (with odds ratio of 1.18 and P<0.001) compared with those who did not receive steroids. This finding adds to the body of evidence that calls into question the commonplace practice of administrating steroids to septic patients on vasopressor therapy.
The most recent campaign guidelines recommend the use of steroids in septic patients only if both adequate fluid resuscitation and vasopressor therapy are not able to restore hemodynamic stability.
Bottom line: Further studies are needed to better define the role of steroids in the treatment of sepsis.
Citation: Casserly B, Gerlach H, Phillips GS, et al. Low-dose steroids in adult septic shock: results of the Surviving Sepsis Campaign. Intensive Care Med. 2012;38:1946-1954.
Link Between Length of Stay and Readmission Rates
Clinical question: How has reducing length of stay affected hospital readmission rates?
Background: There are ongoing concerns that improving a hospital’s efficiency by reducing length of stay (LOS) could be associated with higher hospital readmission rates. However, no studies evaluating the relationship between LOS and readmission rates have been done using recent data.
Study design: Retrospective observational study.
Setting: All acute-care Veterans Affairs (VA) hospitals in the U.S.
Synopsis: A total of 4,124,907 index admissions were included in the final sample from all acute medical admissions in 129 acute-care VA hospitals from October 1996 to September 2010. The primary outcomes were the hospital LOS and the 30-day readmission rate. Index admissions for heart failure, chronic obstructive pulmonary disease (COPD), acute myocardial infarction (AMI), community-acquired pneumonia, and gastrointestinal hemorrhage were also analyzed separately.
The risk-adjusted analysis of LOS demonstrated significant reductions for all admissions over the 14-year period, to 3.98 days from 5.44 days, and for all of the individual conditions with reductions ranging from 1.40 days for gastrointestinal hemorrhage to 2.85 days for AMI. There were similar significant reductions in 30-day readmission rates for all admissions to 13.8% from 16.5% and within the individual conditions ranging from 0.9% in community-acquired pneumonia to 3.3% in COPD. These results show that the reductions in LOS did not increase the risk of readmissions. The major limitation of the study was that these data are only from a single healthcare system.
Bottom line: Data from VA hospitals show that reductions in LOS do not have adverse effects on 30-day readmission rates; instead, both LOS and readmission rates improved over the same time period.
Citation: Kaboli PJ, Go JT, Hockenberry J, et al. Associations between reduced hospital length of stay and 30-day readmission rate and mortality: 14-year experience in 129 Veterans Affairs hospitals. Ann Intern Med. 2012;157:837-845.
Better to Restrict Blood Transfusions in Acute Myocardial Infarction
Clinical question: Is a liberal or restrictive blood transfusion strategy better in patients with anemia and acute myocardial infarction?
Background: Patients with acute myocardial infarction (AMI) are often given therapies that can increase their risk for bleeding and anemia, and it is known that AMI patients have a worse prognosis if they have concomitant anemia. No clear consensus exists on the benefit or harm of blood transfusions in AMI patients.
Study design: Systematic review and meta-analysis.
Setting: Ten articles included in the qualitative and quantitative analyses out of 729 screened articles from Jan. 1, 1966, to March 31, 2012, using the search terms “transfusion,” “myocardial infarction,” and “mortality” in English language.
Synopsis: A total of 203,665 study participants were identified from the 10 studies (one randomized and nine observational) that met the inclusion and exclusion criteria. All-cause mortality was significantly higher in AMI patients who received a blood transfusion compared with those who did not (18.2% vs. 10.2%). However, this difference was not statistically significant in patients that had a STEMI or in patients with a baseline hematocrit less than 30%. A multivariate meta-regression with several covariates, excluding demographics, also showed that blood transfusion was associated with higher mortality and higher risk for subsequent myocardial infarction. There was significant heterogeneity in all results, but no single study was found as the source of the heterogeneity, and no significant publication bias was identified. The major limitations to this study are that there is a paucity of randomized trials available that pertain to this specific topic and the authors did not have patient-level covariates to include in their analyses.
Bottom line: There appears to be an increased risk of mortality and subsequent myocardial infarction in AMI patients who receive blood transfusions versus those who do not.
Citation: Chatterjee S, Wetterslev J, Sharma A, Lichstein E, Mukherjee D. Association of blood transfusion with increased mortality in myocardial infarction: a meta-analysis and diversity-adjusted study sequential analysis. JAMA Intern Med. 2013;173(2):132-139.
Trends in GI Illnesses and Their Associated Costs
Clinical question: What are the new trends in GI illnesses and their associated costs?
Background: The frequency of illnesses and their treatment costs have changed over the last decade. In order to help healthcare providers focus their attention on these new trends, a new compilation of data is needed.
Study design: Epidemiological analysis.
Setting: Various governmental and private databases representing outpatient clinics, hospitals, and death certificates from multiple regions of the U.S.
Synopsis: The analysis was blinded to patient identifiers but represented multiple regions of the U.S. Symptoms were abstracted from patient surveys, and the rest of the data were collected from record review. The most common reported symptoms were abdominal pain, followed by nausea, vomiting, diarrhea, constipation, and heartburn. The most common clinic diagnoses were reflux, abdominal pain, enteritis/dyspepsia, and constipation. The most common inpatient discharge primary diagnoses included acute pancreatitis, cholecystitis, and diverticulitis. Impressive increases were seen in the number of morbidly obese, C. diff, and fatty liver diagnoses.
Colon cancer was the most common GI malignancy and had the highest mortality. C. diff was the ninth-leading cause of GI-related deaths. All types of scopes (except endoscopic retrograde cholangiopancreatography) were performed more commonly now than in the past, with colonoscopy being the most common. The most common indication for an upper endoscopy was reflux, which was also the most common outpatient GI diagnosis.
Bottom line: Healthcare providers need to be aware of new GI illness trends and their associated costs.
Citation: Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterol. 2012;143:1179-1187.
Is Apixaban a Good Stand-Alone Anticoagulant for Extended Treatment in VTE Patients?
Clinical question: Is apixaban an option for the extended treatment of VTE in a simple, fixed-dose regimen?
Background: Apixaban is an oral factor Xa inhibitor that is administered in fixed doses without the need for laboratory monitoring. In the Apixaban after the Initial Management of Pulmonary Embolism and Deep Vein Thrombosis with First-Line Therapy—Extended Treatment (AMPLIFY-EXT) study, investigators compared the efficacy and safety of two doses of apixaban (2.5 mg and 5 mg) with those of placebo in patients with VTE who had completed six to 12 months of anticoagulation therapy and for whom treating physicians were uncertain about continuing therapy. Additional aims of the study were to determine whether the lower dose of apixaban was effective and whether it was associated with less bleeding than the higher dose, and to examine the effect of treatment on arterial thrombotic outcomes.
Study design: Randomized, double-blind study.
Synopsis: A total of 2,486 patients underwent randomization, 2,482 of whom were included in the intention-to-treat analyses. Symptomatic recurrent VTE or death from VTE occurred in 73 of the 829 patients (8.8%) who were receiving placebo, compared with 14 of the 840 patients (1.7%) who were receiving 2.5 mg of apixaban (a difference of 7.2 percentage points; 95% confidence interval [CI], 5.0 to 9.3) and 14 of the 813 patients (1.7%) who were receiving 5 mg of apixaban (a difference of 7.0 percentage points; 95% CI, 4.9 to 9.1) (P<0.001 for both comparisons). The rates of major bleeding were 0.5% in the placebo group, 0.2% in the 2.5-mg apixaban group, and 0.1% in the 5-mg apixaban group. The rates of clinically relevant nonmajor bleeding were 2.3% in the placebo group, 3.0% in the 2.5-mg apixaban group, and 4.2% in the 5-mg apixaban group. The rate of death from any cause was 1.7% in the placebo group, compared with 0.8% in the 2.5-mg apixaban group and 0.5% in the 5-mg apixaban group.
Bottom line: Apixaban is a safe and effective anticoagulant for extended anticoagulation in patients with VTE initially treated with six to 12 months of warfarin.
Citation: Agnelli GM, Buller HR, Cohen A, et al. Apixaban for extended treatment of venous thromboembolism. N Engl J Med. 2013;368(8):699-708.
ACP Guideline Review: Upper Endoscopy for Gastroesophageal Reflux Disease
Clinical question: What are the indications of upper endoscopy in the setting of gastroesophageal reflux disease (GERD)?
Background: GERD is a common condition. Upper endoscopy is widely available and routinely used for diagnosis and management of GERD and its complications. The indications for this procedure are not clearly defined. Overuse of upper endoscopy contributes to higher healthcare costs without improving patient outcomes.
Study design: Literature review and comparison of clinical guidelines from professional organizations by a team of general internists, gastroenterologists, and clinical epidemiologists. The document was not based on a formal systemic review but was intended to provide practical advice based on the best available evidence.
Synopsis: Best practice advice No. 1: Upper endoscopy is indicated in men and women with heartburn and alarm symptoms (dysphagia, bleeding, anemia, weight loss, and recurrent vomiting).
Best practice advice No. 2: Upper endoscopy is indicated in men and women with typical GERD symptoms that persist despite a therapeutic trial of four to eight weeks of twice-daily proton-pump inhibitor therapy, severe erosive esophagitis after a two-month course of proton-pump inhibitor therapy to assess healing and rule out Barrett esophagus, and history of esophageal stricture who have recurrent symptoms of dysphagia.
Best practice advice No. 3: Upper endoscopy might be indicated in men older than 50 with chronic GERD symptoms (symptoms for more than five years) and additional risk factors (nocturnal reflux symptoms, hiatal hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat) to detect esophageal adenocarcinoma and Barrett esophagus. It might also be indicated for surveillance evaluation in men and women with a history of Barrett esophagus. In men and women with Barrett esophagus and no dysplasia, surveillance examinations should occur at intervals no more frequently than three to five years. More frequent intervals are indicated in patients with Barrett esophagus and dysplasia.
Bottom line: Use upper endoscopy selectively for patients with GERD.
Citation: Shaheen NJ, Weinberg DS, Denberg TD, et al. Upper endoscopy for gastroesophageal reflux disease: best practice advice from the Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med. 2012;157(11):808-816.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Value of routine preoperative urine screening assessed
- Impact of hospitalist-led intermediate care on patient survival
- Risks of blood transfusion to treat upper GI bleeding
- Low-dose steroids and increased mortality in sepsis
- Reduced length of stay and hospital readmission rates
- Restrictive blood transfusion strategies better for acute myocardial infarction
- Trends in GI illnesses and their associated costs
- Apixaban as a stand-alone anticoagulant in patients with VTE
- Guidelines for upper endoscopy use in gastroesophageal reflux disease
Avoid Preoperative Urine Culture in Nonurologic Surgical Procedures
Clinical question: Is routine preoperative urine screening beneficial?
Background: The value of preoperative urine screening is unproven, except before urologic procedures. Furthermore, treatment of asymptomatic bacteriuria may lead to adverse events, including diarrhea, allergic reactions, and Clostridium difficile infection (CDI).
Study design: Retrospective chart review.
Setting: Patients who underwent cardiothoracic, orthopedic, and vascular surgeries at the Minneapolis Veterans Affairs Medical Center in 2010.
Synopsis: A total of 1,934 procedures were performed on 1,699 patients, most of which were orthopedics procedures (1,291 in 1,115 patients). A urine culture was obtained before 25% of procedures with significant variation by service (cardiothoracic, 85%; vascular, 48%; orthopedic, 4%). Bacteriuria was detected in 11% of urine cultures (54 of 489), but antimicrobial drugs were dispensed to just 16 patients.
To identify correlates of preoperative urine culture use, patients with and without urine cultures were compared. The rate of surgical-site infection was similar for both groups. Postoperative UTI was more frequent among patients with bacteriuria. Rates of diarrhea, allergy, and CDI did not differ. Paradoxically, patients treated for preoperative UTI were more likely to develop surgical-site infections (45% vs. 14%; P=0.03). Postoperative UTI was also more frequent among treated patients versus untreated patients (18% vs. 7%).
Bottom line: This is the largest study to assess outcomes for routine preoperative urine cultures. These findings demonstrate that preoperative screening for, and treatment of, asymptomatic bacteriuria should be avoided in patients undergoing nonurologic surgical procedures.
Citation: Drekonja DM, Zarmbinski B, Johnson JR. Preoperative urine culture at a veterans affairs medical center. JAMA Intern Med. 2013;173(1):71-72.
Intermediate Care Staffed by Hospitalists: Impact on Mortality, Comanagement, and Teaching
Clinical question: Does a hospitalist-led intermediate-care unit improve patient survival?
Background: Hospitalized patients are complex, and institutions often have to balance matching patient acuity to either an ICU or a regular ward. However, an intermediate-care setting might be an attractive strategy to provide rational care according to patient needs while expanding comanagement and teaching services.
Study design: Retrospective observational study.
Setting: Intermediate-care unit of a single academic hospital.
Synopsis: In-hospital mortality in this intermediate-care unit was 20.6%, whereas the expected mortality was 23.2% based on Simplified Acute Physiology Score II (SAPS II) score. The correlation between SAPS II predicted and observed death rates was accurate and statistically significant (P<0.001). Comanagement was performed with several medical and surgical teams, with an increase in perioperative comanagement of 22.7% (P=0.014). The number of training residents in the intermediate-care unit increased to 30.4% from 4.3% (P=0.002).
Bottom line: An intermediate-care unit led by hospitalists showed encouraging results in patient mortality, as well as comanagement and teaching opportunities.
Citation: Lucena JF, Alegre F, Rodil R, et al. Results of a retrospective observational study of intermediate care staffed by hospitalists: impact on mortality, co-management, and teaching. J Hosp Med. 2012;7(5):411-415.
Blood Transfusion Associated with Increased Risk of Rebleeding in Patients with Nonvariceal Upper GI Bleeding
Clinical question: Does more liberal use of blood transfusions in the setting of nonvariceal upper GI bleeding result in patient harm?
Background: Randomized controlled trials have demonstrated that a more liberal approach to blood transfusions for patients in the medical intensive-care unit results in higher mortality. However, the potential harmful effect of blood transfusions in the setting of GI bleeding has not been demonstrated.
Study design: Retrospective cohort study.
Setting: Canadian hospitals.
Synopsis: Based on a retrospective analysis of the Canadian Registry of patients with Upper Gastrointestinal Bleeding and Endoscopy (RUGBE), the authors determined there was a statistically significant association between patients who received a blood transfusion for the management of nonvariceal upper GI bleeding and the risk of rebleeding. The rate of rebleeding in patients who received a blood transfusion was 23.6% compared with 11.3% in patients who were not transfused (P<0.01). There was no statistically significant difference in mortality.
Although this was a reasonably large observational study that included 1,677 patients with nonvariceal upper GI bleeding, it is vulnerable to confounding. It suggests the need to further study potential harm of blood transfusion in the setting of GI bleeding, but it should not result in a change in clinical practice at this time.
Bottom line: Prospective randomized studies are needed to determine if there are harmful effects of blood transfusions in the setting of GI bleeding and to better define a threshold for transfusion.
Citation: Restellini S, Kherad O, Jairath V, Martel M, Barkun AN. Red blood cell transfusion is associated with increased rebleeding in patients with nonvariceal upper gastrointestinal bleeding. Aliment Pharmacol Ther. 2013;37:316-322.
Low-Dose Steroids in Sepsis Associated with Increase in Mortality
Clinical question: What is the role of steroids in the treatment of adult patients with sepsis?
Background: The Surviving Sepsis Campaign guidelines have previously recommended administering steroids to patients with septic shock not responsive to fluid resuscitation and who require vasopressors. However, prior randomized clinical trials studying the use of steroids in these settings have produced conflicting results.
Study design: Retrospective cohort study.
Setting: Two hundred fifty-two hospitals in North America, South America, and Europe.
Synopsis: The Surviving Sepsis Campaign management bundle has been shown to reduce mortality in patients with sepsis. However, it is not known which particular elements of the management bundle result in improved mortality. The Surviving Sepsis Campaign database included 17,847 patients who required vasopressor therapy after adequate fluid resuscitation. This subgroup was analyzed to see if there was a difference in mortality between patients who received low-dose steroids versus those who did not receive steroids. The mortality rate among those who received steroids was statistically higher (with odds ratio of 1.18 and P<0.001) compared with those who did not receive steroids. This finding adds to the body of evidence that calls into question the commonplace practice of administrating steroids to septic patients on vasopressor therapy.
The most recent campaign guidelines recommend the use of steroids in septic patients only if both adequate fluid resuscitation and vasopressor therapy are not able to restore hemodynamic stability.
Bottom line: Further studies are needed to better define the role of steroids in the treatment of sepsis.
Citation: Casserly B, Gerlach H, Phillips GS, et al. Low-dose steroids in adult septic shock: results of the Surviving Sepsis Campaign. Intensive Care Med. 2012;38:1946-1954.
Link Between Length of Stay and Readmission Rates
Clinical question: How has reducing length of stay affected hospital readmission rates?
Background: There are ongoing concerns that improving a hospital’s efficiency by reducing length of stay (LOS) could be associated with higher hospital readmission rates. However, no studies evaluating the relationship between LOS and readmission rates have been done using recent data.
Study design: Retrospective observational study.
Setting: All acute-care Veterans Affairs (VA) hospitals in the U.S.
Synopsis: A total of 4,124,907 index admissions were included in the final sample from all acute medical admissions in 129 acute-care VA hospitals from October 1996 to September 2010. The primary outcomes were the hospital LOS and the 30-day readmission rate. Index admissions for heart failure, chronic obstructive pulmonary disease (COPD), acute myocardial infarction (AMI), community-acquired pneumonia, and gastrointestinal hemorrhage were also analyzed separately.
The risk-adjusted analysis of LOS demonstrated significant reductions for all admissions over the 14-year period, to 3.98 days from 5.44 days, and for all of the individual conditions with reductions ranging from 1.40 days for gastrointestinal hemorrhage to 2.85 days for AMI. There were similar significant reductions in 30-day readmission rates for all admissions to 13.8% from 16.5% and within the individual conditions ranging from 0.9% in community-acquired pneumonia to 3.3% in COPD. These results show that the reductions in LOS did not increase the risk of readmissions. The major limitation of the study was that these data are only from a single healthcare system.
Bottom line: Data from VA hospitals show that reductions in LOS do not have adverse effects on 30-day readmission rates; instead, both LOS and readmission rates improved over the same time period.
Citation: Kaboli PJ, Go JT, Hockenberry J, et al. Associations between reduced hospital length of stay and 30-day readmission rate and mortality: 14-year experience in 129 Veterans Affairs hospitals. Ann Intern Med. 2012;157:837-845.
Better to Restrict Blood Transfusions in Acute Myocardial Infarction
Clinical question: Is a liberal or restrictive blood transfusion strategy better in patients with anemia and acute myocardial infarction?
Background: Patients with acute myocardial infarction (AMI) are often given therapies that can increase their risk for bleeding and anemia, and it is known that AMI patients have a worse prognosis if they have concomitant anemia. No clear consensus exists on the benefit or harm of blood transfusions in AMI patients.
Study design: Systematic review and meta-analysis.
Setting: Ten articles included in the qualitative and quantitative analyses out of 729 screened articles from Jan. 1, 1966, to March 31, 2012, using the search terms “transfusion,” “myocardial infarction,” and “mortality” in English language.
Synopsis: A total of 203,665 study participants were identified from the 10 studies (one randomized and nine observational) that met the inclusion and exclusion criteria. All-cause mortality was significantly higher in AMI patients who received a blood transfusion compared with those who did not (18.2% vs. 10.2%). However, this difference was not statistically significant in patients that had a STEMI or in patients with a baseline hematocrit less than 30%. A multivariate meta-regression with several covariates, excluding demographics, also showed that blood transfusion was associated with higher mortality and higher risk for subsequent myocardial infarction. There was significant heterogeneity in all results, but no single study was found as the source of the heterogeneity, and no significant publication bias was identified. The major limitations to this study are that there is a paucity of randomized trials available that pertain to this specific topic and the authors did not have patient-level covariates to include in their analyses.
Bottom line: There appears to be an increased risk of mortality and subsequent myocardial infarction in AMI patients who receive blood transfusions versus those who do not.
Citation: Chatterjee S, Wetterslev J, Sharma A, Lichstein E, Mukherjee D. Association of blood transfusion with increased mortality in myocardial infarction: a meta-analysis and diversity-adjusted study sequential analysis. JAMA Intern Med. 2013;173(2):132-139.
Trends in GI Illnesses and Their Associated Costs
Clinical question: What are the new trends in GI illnesses and their associated costs?
Background: The frequency of illnesses and their treatment costs have changed over the last decade. In order to help healthcare providers focus their attention on these new trends, a new compilation of data is needed.
Study design: Epidemiological analysis.
Setting: Various governmental and private databases representing outpatient clinics, hospitals, and death certificates from multiple regions of the U.S.
Synopsis: The analysis was blinded to patient identifiers but represented multiple regions of the U.S. Symptoms were abstracted from patient surveys, and the rest of the data were collected from record review. The most common reported symptoms were abdominal pain, followed by nausea, vomiting, diarrhea, constipation, and heartburn. The most common clinic diagnoses were reflux, abdominal pain, enteritis/dyspepsia, and constipation. The most common inpatient discharge primary diagnoses included acute pancreatitis, cholecystitis, and diverticulitis. Impressive increases were seen in the number of morbidly obese, C. diff, and fatty liver diagnoses.
Colon cancer was the most common GI malignancy and had the highest mortality. C. diff was the ninth-leading cause of GI-related deaths. All types of scopes (except endoscopic retrograde cholangiopancreatography) were performed more commonly now than in the past, with colonoscopy being the most common. The most common indication for an upper endoscopy was reflux, which was also the most common outpatient GI diagnosis.
Bottom line: Healthcare providers need to be aware of new GI illness trends and their associated costs.
Citation: Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterol. 2012;143:1179-1187.
Is Apixaban a Good Stand-Alone Anticoagulant for Extended Treatment in VTE Patients?
Clinical question: Is apixaban an option for the extended treatment of VTE in a simple, fixed-dose regimen?
Background: Apixaban is an oral factor Xa inhibitor that is administered in fixed doses without the need for laboratory monitoring. In the Apixaban after the Initial Management of Pulmonary Embolism and Deep Vein Thrombosis with First-Line Therapy—Extended Treatment (AMPLIFY-EXT) study, investigators compared the efficacy and safety of two doses of apixaban (2.5 mg and 5 mg) with those of placebo in patients with VTE who had completed six to 12 months of anticoagulation therapy and for whom treating physicians were uncertain about continuing therapy. Additional aims of the study were to determine whether the lower dose of apixaban was effective and whether it was associated with less bleeding than the higher dose, and to examine the effect of treatment on arterial thrombotic outcomes.
Study design: Randomized, double-blind study.
Synopsis: A total of 2,486 patients underwent randomization, 2,482 of whom were included in the intention-to-treat analyses. Symptomatic recurrent VTE or death from VTE occurred in 73 of the 829 patients (8.8%) who were receiving placebo, compared with 14 of the 840 patients (1.7%) who were receiving 2.5 mg of apixaban (a difference of 7.2 percentage points; 95% confidence interval [CI], 5.0 to 9.3) and 14 of the 813 patients (1.7%) who were receiving 5 mg of apixaban (a difference of 7.0 percentage points; 95% CI, 4.9 to 9.1) (P<0.001 for both comparisons). The rates of major bleeding were 0.5% in the placebo group, 0.2% in the 2.5-mg apixaban group, and 0.1% in the 5-mg apixaban group. The rates of clinically relevant nonmajor bleeding were 2.3% in the placebo group, 3.0% in the 2.5-mg apixaban group, and 4.2% in the 5-mg apixaban group. The rate of death from any cause was 1.7% in the placebo group, compared with 0.8% in the 2.5-mg apixaban group and 0.5% in the 5-mg apixaban group.
Bottom line: Apixaban is a safe and effective anticoagulant for extended anticoagulation in patients with VTE initially treated with six to 12 months of warfarin.
Citation: Agnelli GM, Buller HR, Cohen A, et al. Apixaban for extended treatment of venous thromboembolism. N Engl J Med. 2013;368(8):699-708.
ACP Guideline Review: Upper Endoscopy for Gastroesophageal Reflux Disease
Clinical question: What are the indications of upper endoscopy in the setting of gastroesophageal reflux disease (GERD)?
Background: GERD is a common condition. Upper endoscopy is widely available and routinely used for diagnosis and management of GERD and its complications. The indications for this procedure are not clearly defined. Overuse of upper endoscopy contributes to higher healthcare costs without improving patient outcomes.
Study design: Literature review and comparison of clinical guidelines from professional organizations by a team of general internists, gastroenterologists, and clinical epidemiologists. The document was not based on a formal systemic review but was intended to provide practical advice based on the best available evidence.
Synopsis: Best practice advice No. 1: Upper endoscopy is indicated in men and women with heartburn and alarm symptoms (dysphagia, bleeding, anemia, weight loss, and recurrent vomiting).
Best practice advice No. 2: Upper endoscopy is indicated in men and women with typical GERD symptoms that persist despite a therapeutic trial of four to eight weeks of twice-daily proton-pump inhibitor therapy, severe erosive esophagitis after a two-month course of proton-pump inhibitor therapy to assess healing and rule out Barrett esophagus, and history of esophageal stricture who have recurrent symptoms of dysphagia.
Best practice advice No. 3: Upper endoscopy might be indicated in men older than 50 with chronic GERD symptoms (symptoms for more than five years) and additional risk factors (nocturnal reflux symptoms, hiatal hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat) to detect esophageal adenocarcinoma and Barrett esophagus. It might also be indicated for surveillance evaluation in men and women with a history of Barrett esophagus. In men and women with Barrett esophagus and no dysplasia, surveillance examinations should occur at intervals no more frequently than three to five years. More frequent intervals are indicated in patients with Barrett esophagus and dysplasia.
Bottom line: Use upper endoscopy selectively for patients with GERD.
Citation: Shaheen NJ, Weinberg DS, Denberg TD, et al. Upper endoscopy for gastroesophageal reflux disease: best practice advice from the Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med. 2012;157(11):808-816.
ITL: Physician Reviews of HM-Relevant Research
Clinical question: Is there a difference between aspirin and warfarin in preventing thromboembolic complications and risk of bleeding in patients with chronic kidney disease (CKD) and nonvalvular atrial fibrillation (NVAF)?
Background: Data are lacking on risks and benefits of aspirin and warfarin in CKD, as this group of patients largely has been excluded from anticoagulation therapy trials for NVAF. This study examined the risks and benefits of aspirin and warfarin in patients with CKD with NVAF.
Study design: Retrospective, observational cohort study.
Setting: Danish National Registries.
Synopsis: Of 132,372 patients with NVAF, 2.7% had CKD and 0.7% had end-stage renal disease (ESRD). Compared to patients with no CKD, there was increased risk of stroke or systemic thromboembolism in patients with ESRD (HR, 1.83; 95% CI, 1.57-2.14) and with non-end-stage CKD (HR 1.49; 95% CI 1.38-1.59).
In patients with CKD, warfarin significantly reduced stroke risk (HR, 0.76; 95% CI, 0.64-0.91) and significantly increased bleeding risk (HR, 1.33; 95% CI, 1.16-1.53); aspirin significantly increased bleeding risk (HR, 1.17; 95% CI, 1.02-1.34), with no reduction in stroke risk.
Bottom line: CKD was associated with an increased risk of stroke among NVAF patients. While both aspirin and warfarin were associated with increased risk of bleeding, there was a reduction in the risk of stroke with warfarin, but not with aspirin.
Citation: Olesen JB, Lip GY, Kamper AL, et al. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N Engl J Med. 2012;367(7):625-635.
Click here for more physician reviews of HM-relevant literature.
Clinical question: Is there a difference between aspirin and warfarin in preventing thromboembolic complications and risk of bleeding in patients with chronic kidney disease (CKD) and nonvalvular atrial fibrillation (NVAF)?
Background: Data are lacking on risks and benefits of aspirin and warfarin in CKD, as this group of patients largely has been excluded from anticoagulation therapy trials for NVAF. This study examined the risks and benefits of aspirin and warfarin in patients with CKD with NVAF.
Study design: Retrospective, observational cohort study.
Setting: Danish National Registries.
Synopsis: Of 132,372 patients with NVAF, 2.7% had CKD and 0.7% had end-stage renal disease (ESRD). Compared to patients with no CKD, there was increased risk of stroke or systemic thromboembolism in patients with ESRD (HR, 1.83; 95% CI, 1.57-2.14) and with non-end-stage CKD (HR 1.49; 95% CI 1.38-1.59).
In patients with CKD, warfarin significantly reduced stroke risk (HR, 0.76; 95% CI, 0.64-0.91) and significantly increased bleeding risk (HR, 1.33; 95% CI, 1.16-1.53); aspirin significantly increased bleeding risk (HR, 1.17; 95% CI, 1.02-1.34), with no reduction in stroke risk.
Bottom line: CKD was associated with an increased risk of stroke among NVAF patients. While both aspirin and warfarin were associated with increased risk of bleeding, there was a reduction in the risk of stroke with warfarin, but not with aspirin.
Citation: Olesen JB, Lip GY, Kamper AL, et al. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N Engl J Med. 2012;367(7):625-635.
Click here for more physician reviews of HM-relevant literature.
Clinical question: Is there a difference between aspirin and warfarin in preventing thromboembolic complications and risk of bleeding in patients with chronic kidney disease (CKD) and nonvalvular atrial fibrillation (NVAF)?
Background: Data are lacking on risks and benefits of aspirin and warfarin in CKD, as this group of patients largely has been excluded from anticoagulation therapy trials for NVAF. This study examined the risks and benefits of aspirin and warfarin in patients with CKD with NVAF.
Study design: Retrospective, observational cohort study.
Setting: Danish National Registries.
Synopsis: Of 132,372 patients with NVAF, 2.7% had CKD and 0.7% had end-stage renal disease (ESRD). Compared to patients with no CKD, there was increased risk of stroke or systemic thromboembolism in patients with ESRD (HR, 1.83; 95% CI, 1.57-2.14) and with non-end-stage CKD (HR 1.49; 95% CI 1.38-1.59).
In patients with CKD, warfarin significantly reduced stroke risk (HR, 0.76; 95% CI, 0.64-0.91) and significantly increased bleeding risk (HR, 1.33; 95% CI, 1.16-1.53); aspirin significantly increased bleeding risk (HR, 1.17; 95% CI, 1.02-1.34), with no reduction in stroke risk.
Bottom line: CKD was associated with an increased risk of stroke among NVAF patients. While both aspirin and warfarin were associated with increased risk of bleeding, there was a reduction in the risk of stroke with warfarin, but not with aspirin.
Citation: Olesen JB, Lip GY, Kamper AL, et al. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N Engl J Med. 2012;367(7):625-635.
Click here for more physician reviews of HM-relevant literature.
ITL: Physician Reviews of HM-Relevant Research
Clinical question: What are the relative predictive values of the HEMORR2HAGES, ATRIA, and HAS-BLED risk-prediction schemes?
Background: The tools predict bleeding risk in patients anticoagulated for atrial fibrillation (afib), but it is unknown which is the best for predicting clinically relevant bleeding.
Study design: Post-hoc analysis.
Setting: Data previously collected for the AMADEUS trial (2,293 patients taking warfarin; 251 had at least one clinically relevant bleeding event) were used to test each of the three bleeding-risk-prediction schemes on the same data set.
Synopsis: Using three analysis methods (net reclassification improvement, receiver-operating characteristic [ROC], and decision-curve analysis), the researchers compared the three schemes’ performance. HAS-BLED performed best in all three of the analysis methods.
The HAS-BLED score calculation requires the following patient information: history of hypertension, renal disease, liver disease, stroke, prior major bleeding event, and labile INR; age >65; and use of antiplatelet agents, aspirin, and alcohol.
Bottom line: HAS-BLED was the best of the three schemes, although all three had only modest ability to predict clinically relevant bleeding.
Citation: Apostolakis S, Lane DA, Guo Y, et al. Performance of the HEMORR2HAGES, ATRIA and HAS-BLED bleeding risk-prediction scores in patients with atrial fibrillation undergoing anticoagulation. J Am Coll Cardiol. 2012;60(9):861-867.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: What are the relative predictive values of the HEMORR2HAGES, ATRIA, and HAS-BLED risk-prediction schemes?
Background: The tools predict bleeding risk in patients anticoagulated for atrial fibrillation (afib), but it is unknown which is the best for predicting clinically relevant bleeding.
Study design: Post-hoc analysis.
Setting: Data previously collected for the AMADEUS trial (2,293 patients taking warfarin; 251 had at least one clinically relevant bleeding event) were used to test each of the three bleeding-risk-prediction schemes on the same data set.
Synopsis: Using three analysis methods (net reclassification improvement, receiver-operating characteristic [ROC], and decision-curve analysis), the researchers compared the three schemes’ performance. HAS-BLED performed best in all three of the analysis methods.
The HAS-BLED score calculation requires the following patient information: history of hypertension, renal disease, liver disease, stroke, prior major bleeding event, and labile INR; age >65; and use of antiplatelet agents, aspirin, and alcohol.
Bottom line: HAS-BLED was the best of the three schemes, although all three had only modest ability to predict clinically relevant bleeding.
Citation: Apostolakis S, Lane DA, Guo Y, et al. Performance of the HEMORR2HAGES, ATRIA and HAS-BLED bleeding risk-prediction scores in patients with atrial fibrillation undergoing anticoagulation. J Am Coll Cardiol. 2012;60(9):861-867.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: What are the relative predictive values of the HEMORR2HAGES, ATRIA, and HAS-BLED risk-prediction schemes?
Background: The tools predict bleeding risk in patients anticoagulated for atrial fibrillation (afib), but it is unknown which is the best for predicting clinically relevant bleeding.
Study design: Post-hoc analysis.
Setting: Data previously collected for the AMADEUS trial (2,293 patients taking warfarin; 251 had at least one clinically relevant bleeding event) were used to test each of the three bleeding-risk-prediction schemes on the same data set.
Synopsis: Using three analysis methods (net reclassification improvement, receiver-operating characteristic [ROC], and decision-curve analysis), the researchers compared the three schemes’ performance. HAS-BLED performed best in all three of the analysis methods.
The HAS-BLED score calculation requires the following patient information: history of hypertension, renal disease, liver disease, stroke, prior major bleeding event, and labile INR; age >65; and use of antiplatelet agents, aspirin, and alcohol.
Bottom line: HAS-BLED was the best of the three schemes, although all three had only modest ability to predict clinically relevant bleeding.
Citation: Apostolakis S, Lane DA, Guo Y, et al. Performance of the HEMORR2HAGES, ATRIA and HAS-BLED bleeding risk-prediction scores in patients with atrial fibrillation undergoing anticoagulation. J Am Coll Cardiol. 2012;60(9):861-867.
Visit our website for more physician reviews of recent HM-relevant literature.
ITL: Physician Reviews of HM-Relevant Research
Clinical question: Does the addition of clopidogrel to aspirin reduce the risk of any type of recurrent stroke, or affect the risk of bleeding or death, in patients who recently suffered a lacunar stroke?
Background: There are no prior randomized, multicenter trials on secondary prevention of lacunar stroke; aspirin is the standard antiplatelet therapy in this setting.
Study design: Double-blind, randomized, multicenter trial.
Setting: Eighty-two clinical centers in North America, Latin America, and Spain.
Synopsis: Researchers enrolled 3,020 patients from 2003 to 2011; criteria included age >30 years old and symptomatic lacunar stroke (proven by MRI) in the preceding 180 days.
Results showed no significant difference between recurrent strokes (any type) in the aspirin-only group (2.7% per year) versus the aspirin-plus-clopidogrel group (2.5% per year). Major hemorrhage risk was much higher in the aspirin-plus-clopidogrel group (2.1% per year) versus aspirin-only group (1.1% per year). All-cause mortality also was much higher in the aspirin-plus-clopidogrel group (N=113) versus the aspirin-only group (N=77).
Bottom line: The addition of clopidogrel to aspirin for secondary prevention does not significantly reduce the risk of recurrent stroke, but it does significantly increase the risk of bleeding and death.
Citation: Benavente OR, Hart RG, McClure LA, et al. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. N Engl J Med. 2012;367:817-825.
For more physician reviews of recent HM-relevant literature, visit our website.
Clinical question: Does the addition of clopidogrel to aspirin reduce the risk of any type of recurrent stroke, or affect the risk of bleeding or death, in patients who recently suffered a lacunar stroke?
Background: There are no prior randomized, multicenter trials on secondary prevention of lacunar stroke; aspirin is the standard antiplatelet therapy in this setting.
Study design: Double-blind, randomized, multicenter trial.
Setting: Eighty-two clinical centers in North America, Latin America, and Spain.
Synopsis: Researchers enrolled 3,020 patients from 2003 to 2011; criteria included age >30 years old and symptomatic lacunar stroke (proven by MRI) in the preceding 180 days.
Results showed no significant difference between recurrent strokes (any type) in the aspirin-only group (2.7% per year) versus the aspirin-plus-clopidogrel group (2.5% per year). Major hemorrhage risk was much higher in the aspirin-plus-clopidogrel group (2.1% per year) versus aspirin-only group (1.1% per year). All-cause mortality also was much higher in the aspirin-plus-clopidogrel group (N=113) versus the aspirin-only group (N=77).
Bottom line: The addition of clopidogrel to aspirin for secondary prevention does not significantly reduce the risk of recurrent stroke, but it does significantly increase the risk of bleeding and death.
Citation: Benavente OR, Hart RG, McClure LA, et al. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. N Engl J Med. 2012;367:817-825.
For more physician reviews of recent HM-relevant literature, visit our website.
Clinical question: Does the addition of clopidogrel to aspirin reduce the risk of any type of recurrent stroke, or affect the risk of bleeding or death, in patients who recently suffered a lacunar stroke?
Background: There are no prior randomized, multicenter trials on secondary prevention of lacunar stroke; aspirin is the standard antiplatelet therapy in this setting.
Study design: Double-blind, randomized, multicenter trial.
Setting: Eighty-two clinical centers in North America, Latin America, and Spain.
Synopsis: Researchers enrolled 3,020 patients from 2003 to 2011; criteria included age >30 years old and symptomatic lacunar stroke (proven by MRI) in the preceding 180 days.
Results showed no significant difference between recurrent strokes (any type) in the aspirin-only group (2.7% per year) versus the aspirin-plus-clopidogrel group (2.5% per year). Major hemorrhage risk was much higher in the aspirin-plus-clopidogrel group (2.1% per year) versus aspirin-only group (1.1% per year). All-cause mortality also was much higher in the aspirin-plus-clopidogrel group (N=113) versus the aspirin-only group (N=77).
Bottom line: The addition of clopidogrel to aspirin for secondary prevention does not significantly reduce the risk of recurrent stroke, but it does significantly increase the risk of bleeding and death.
Citation: Benavente OR, Hart RG, McClure LA, et al. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. N Engl J Med. 2012;367:817-825.
For more physician reviews of recent HM-relevant literature, visit our website.
In the Literature: Research You Need to Know
Clinical question: Can the aortic dissection detection (ADD) risk score be used to screen patients for acute aortic dissection at the bedside?
Background: AAD, a life-threatening condition, often is missed due to relatively low incidence, varied presentation, and need for advanced imaging studies. The American Heart Association and the American College of Cardiology have published guidelines on thoracic aortic disease from which the ADD risk score has been adapted to identify high-risk patients and to suggest additional testing based on pretest probability of disease.
Study design: Retrospective application of ADD risk score to the International Registry of Acute Aortic Dissection (IRAD) database.
Setting: Multinational medical registry compiled from 24 medical centers.
Synopsis: A total of 2,538 patients with confirmed ADD were reviewed. The number of patients presenting with one or more of 12 proposed clinical risk markers was determined. An ADD risk score of 0 to 3 was calculated based on the number of risk categories (high-risk predisposing conditions, pain features, examination features) in which patients met criteria.
Among 108 (4.3%) patients found to be low-risk (ADD score 0), 72 had a chest X-ray, 35 of which were found to have a widened mediastinum. High-risk features (ADD score 2 or 3) were found in 1,503 (59.2%) patients, and the remaining 927 (36.5%) patients had intermediate risk (ADD score 1).
The guidelines recommend further imaging for all intermediate- and high-risk patients and for low-risk patients with a wide mediastinum resulting in very good sensitivity.
Bottom line: The ADD risk score is a sensitive bedside screening tool for aortic dissection, ensuring that more than 95% patients with true dissection undergo further investigation, but it may lead to overinvestigation due to unknown specificity.
Citation: Rogers AM, Hermann LK, Booher AM, et al. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: results from the international registry of acute aortic dissection. Circ. 2011;123:2213-2218.
For more physician reviews of HM-related literature, visit our website and search "Literature."
Clinical question: Can the aortic dissection detection (ADD) risk score be used to screen patients for acute aortic dissection at the bedside?
Background: AAD, a life-threatening condition, often is missed due to relatively low incidence, varied presentation, and need for advanced imaging studies. The American Heart Association and the American College of Cardiology have published guidelines on thoracic aortic disease from which the ADD risk score has been adapted to identify high-risk patients and to suggest additional testing based on pretest probability of disease.
Study design: Retrospective application of ADD risk score to the International Registry of Acute Aortic Dissection (IRAD) database.
Setting: Multinational medical registry compiled from 24 medical centers.
Synopsis: A total of 2,538 patients with confirmed ADD were reviewed. The number of patients presenting with one or more of 12 proposed clinical risk markers was determined. An ADD risk score of 0 to 3 was calculated based on the number of risk categories (high-risk predisposing conditions, pain features, examination features) in which patients met criteria.
Among 108 (4.3%) patients found to be low-risk (ADD score 0), 72 had a chest X-ray, 35 of which were found to have a widened mediastinum. High-risk features (ADD score 2 or 3) were found in 1,503 (59.2%) patients, and the remaining 927 (36.5%) patients had intermediate risk (ADD score 1).
The guidelines recommend further imaging for all intermediate- and high-risk patients and for low-risk patients with a wide mediastinum resulting in very good sensitivity.
Bottom line: The ADD risk score is a sensitive bedside screening tool for aortic dissection, ensuring that more than 95% patients with true dissection undergo further investigation, but it may lead to overinvestigation due to unknown specificity.
Citation: Rogers AM, Hermann LK, Booher AM, et al. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: results from the international registry of acute aortic dissection. Circ. 2011;123:2213-2218.
For more physician reviews of HM-related literature, visit our website and search "Literature."
Clinical question: Can the aortic dissection detection (ADD) risk score be used to screen patients for acute aortic dissection at the bedside?
Background: AAD, a life-threatening condition, often is missed due to relatively low incidence, varied presentation, and need for advanced imaging studies. The American Heart Association and the American College of Cardiology have published guidelines on thoracic aortic disease from which the ADD risk score has been adapted to identify high-risk patients and to suggest additional testing based on pretest probability of disease.
Study design: Retrospective application of ADD risk score to the International Registry of Acute Aortic Dissection (IRAD) database.
Setting: Multinational medical registry compiled from 24 medical centers.
Synopsis: A total of 2,538 patients with confirmed ADD were reviewed. The number of patients presenting with one or more of 12 proposed clinical risk markers was determined. An ADD risk score of 0 to 3 was calculated based on the number of risk categories (high-risk predisposing conditions, pain features, examination features) in which patients met criteria.
Among 108 (4.3%) patients found to be low-risk (ADD score 0), 72 had a chest X-ray, 35 of which were found to have a widened mediastinum. High-risk features (ADD score 2 or 3) were found in 1,503 (59.2%) patients, and the remaining 927 (36.5%) patients had intermediate risk (ADD score 1).
The guidelines recommend further imaging for all intermediate- and high-risk patients and for low-risk patients with a wide mediastinum resulting in very good sensitivity.
Bottom line: The ADD risk score is a sensitive bedside screening tool for aortic dissection, ensuring that more than 95% patients with true dissection undergo further investigation, but it may lead to overinvestigation due to unknown specificity.
Citation: Rogers AM, Hermann LK, Booher AM, et al. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: results from the international registry of acute aortic dissection. Circ. 2011;123:2213-2218.
For more physician reviews of HM-related literature, visit our website and search "Literature."
In the Literature: Research You Need to Know
Clinical question: In patients with candidemia, what are the incidence, risk factors, and antifungal treatment outcomes for ocular candidiasis?
Background: The incidence and treatment outcomes of ocular candidiasis have not been studied extensively.
Study design: Randomized noninferiority trial.
Setting: Multicenter study of 370 patients.
Synopsis: This study randomized 370 non-neutropenic patients with candidemia in a 2:1 ratio to receive voriconazole monotherapy or amphotericin B followed by fluconazole. Patients were treated for at least two weeks after the last positive blood culture, for a maximum duration of eight weeks. Baseline and follow-up fundoscopic examinations were performed.
Sixty (16%) patients were diagnosed with ocular candidiasis, of which six (1.6%) were diagnosed with endophthalmitis and 34 (9%) with chorioretinitis. Patients with ocular candidiasis had a longer duration of candidemia, and were more likely to be infected with Candida albicans.
Outcomes were not available in 19 patients with ocular candidiasis due to death or loss of follow-up. There was no significant difference between the cure rate of voriconazole (93.5% [29/31]), compared with the amphotericin B group (100% [10/10]).
Bottom line: Ocular candidiasis occurs in approximately 16% of non-neutropenic patients with candidemia. A longer duration of candidemia and infection with C. albicans were associated with ocular candidiasis. Both voriconazole and amphotericin B/fluconazole are effective in patients with ocular candidiasis.
Citation: Oude Lashof AM, Rothova A, Sobel JD, et al. Ocular manifestations of candidemia. Clin Infect Dis. 2011;53:262-268.
For more physician reviews of HM-related literature, check out our website.
Clinical question: In patients with candidemia, what are the incidence, risk factors, and antifungal treatment outcomes for ocular candidiasis?
Background: The incidence and treatment outcomes of ocular candidiasis have not been studied extensively.
Study design: Randomized noninferiority trial.
Setting: Multicenter study of 370 patients.
Synopsis: This study randomized 370 non-neutropenic patients with candidemia in a 2:1 ratio to receive voriconazole monotherapy or amphotericin B followed by fluconazole. Patients were treated for at least two weeks after the last positive blood culture, for a maximum duration of eight weeks. Baseline and follow-up fundoscopic examinations were performed.
Sixty (16%) patients were diagnosed with ocular candidiasis, of which six (1.6%) were diagnosed with endophthalmitis and 34 (9%) with chorioretinitis. Patients with ocular candidiasis had a longer duration of candidemia, and were more likely to be infected with Candida albicans.
Outcomes were not available in 19 patients with ocular candidiasis due to death or loss of follow-up. There was no significant difference between the cure rate of voriconazole (93.5% [29/31]), compared with the amphotericin B group (100% [10/10]).
Bottom line: Ocular candidiasis occurs in approximately 16% of non-neutropenic patients with candidemia. A longer duration of candidemia and infection with C. albicans were associated with ocular candidiasis. Both voriconazole and amphotericin B/fluconazole are effective in patients with ocular candidiasis.
Citation: Oude Lashof AM, Rothova A, Sobel JD, et al. Ocular manifestations of candidemia. Clin Infect Dis. 2011;53:262-268.
For more physician reviews of HM-related literature, check out our website.
Clinical question: In patients with candidemia, what are the incidence, risk factors, and antifungal treatment outcomes for ocular candidiasis?
Background: The incidence and treatment outcomes of ocular candidiasis have not been studied extensively.
Study design: Randomized noninferiority trial.
Setting: Multicenter study of 370 patients.
Synopsis: This study randomized 370 non-neutropenic patients with candidemia in a 2:1 ratio to receive voriconazole monotherapy or amphotericin B followed by fluconazole. Patients were treated for at least two weeks after the last positive blood culture, for a maximum duration of eight weeks. Baseline and follow-up fundoscopic examinations were performed.
Sixty (16%) patients were diagnosed with ocular candidiasis, of which six (1.6%) were diagnosed with endophthalmitis and 34 (9%) with chorioretinitis. Patients with ocular candidiasis had a longer duration of candidemia, and were more likely to be infected with Candida albicans.
Outcomes were not available in 19 patients with ocular candidiasis due to death or loss of follow-up. There was no significant difference between the cure rate of voriconazole (93.5% [29/31]), compared with the amphotericin B group (100% [10/10]).
Bottom line: Ocular candidiasis occurs in approximately 16% of non-neutropenic patients with candidemia. A longer duration of candidemia and infection with C. albicans were associated with ocular candidiasis. Both voriconazole and amphotericin B/fluconazole are effective in patients with ocular candidiasis.
Citation: Oude Lashof AM, Rothova A, Sobel JD, et al. Ocular manifestations of candidemia. Clin Infect Dis. 2011;53:262-268.
For more physician reviews of HM-related literature, check out our website.
How Do I Determine if My Patient has Decision-Making Capacity?
Case
A 79-year-old male with coronary artery disease, hypertension, non-insulin-dependent mellitus, moderate dementia, and chronic renal insufficiency is admitted after a fall evaluation. He is widowed and lives in an assisted living facility. He’s accompanied by his niece, is alert, and oriented to person. He thinks he is in a clinic and is unable to state the year, but the remainder of the examination is unremarkable. His labs are notable for potassium of 6.3 mmol/L, BUN of 78 mg/dL, and Cr of 3.7 mg/dL. The niece reports that the patient is not fond of medical care, thus the most recent labs are from two years ago (and indicate a BUN of 39 and Cr of 2.8, with an upward trend over the past decade). You discuss possible long-term need for dialysis with the patient and niece, and the patient clearly states "no." However, he also states that it is 1988. How do you determine if he has the capacity to make decisions?
Overview
Hospitalists are familiar with the doctrine of informed consent—describing a disease, treatment options, associated risks and benefits, potential for complications, and alternatives, including no treatment. Not only must the patient be informed, and the decision free from any coercion, but the patient also must have capacity to make the decision.
Hospitalists often care for patients in whom decision-making capacity comes into question. This includes populations with depression, psychosis, dementia, stroke, severe personality disorders, developmental delay, comatose patients, as well as those with impaired attentional capacity (e.g. acute pain) or general debility (e.g. metastatic cancer).1,2
ave for the comatose patient, whether the patient has capacity might not be obvious. However, addressing the components of capacity (communication, understanding, appreciation, and rationalization) by using a validated clinical tool, such as the MacCAT-T, or more simply by systematically applying those four components to the clinical scenario under consideration, hospitalists can make this determination.
Review of the Literature
It is important to differentiate capacity from competency. Competency is a global assessment and a legal determination made by a judge in court. Capacity, on the other hand, is a functional assessment regarding a particular decision. Capacity is not static, and it can be performed by any clinician familiar with the patient. A hospitalist often is well positioned to make a capacity determination given established rapport with the patient and familiarity with the details of the case.
To make this determination, a hospitalist needs to know how to assess capacity. Although capacity usually is defined by state law and varies by jurisdiction, clinicians generally can assume it includes one or more of the four key components:
- Communication. The patient needs to be able to express a treatment choice, and this decision needs to be stable enough for the treatment to be implemented. Changing one’s decision in itself would not bring a patient’s capacity into question, so long as the patient was able to explain the rationale behind the switch. Frequent changes back and forth in the decision-making, however, could be indicative of an underlying psychiatric disorder or extreme indecision, which could bring capacity into question.
- Understanding. The patient needs to recall conversations about treatment, to make the link between causal relationships, and to process probabilities for outcomes. Problems with memory, attention span, and intelligence can affect one’s understanding.
- Appreciation. The patient should be able to identify the illness, treatment options, and likely outcomes as things that will affect him or her directly. A lack of appreciation usually stems from a denial based on intelligence (lack of a capability to understand) or emotion, or a delusion that the patient is not affected by this situation the same way and will have a different outcome.
- Rationalization or reasoning. The patient needs to be able to weigh the risks and benefits of the treatment options presented to come to a conclusion in keeping with their goals and best interests, as defined by their personal set of values. This often is affected in psychosis, depression, anxiety, phobias, delirium, and dementia.3
Several clinical capacity tools have been developed to assess these components:
Clinical tools.
The Mini-Mental Status Examination (MMSE) is a bedside test of a patient’s cognitive function, with scores ranging from 0 to 30.4 Although it wasn’t developed for assessing decision-making capacity, it has been compared with expert evaluation for assessment of capacity; the test performs reasonably well, particularly with high and low scores. Specifically, a MMSE >24 has a negative likelihood ratio (LR) of 0.05 for lack of capacity, while a MMSE <16 has a positive LR of 15.5 Scores from 17 to 23 do not correlate well with capacity, and further testing would be necessary. It is easy to administer, requires no formal training, and is familiar to most hospitalists. However, it does not address any specific aspects of informed consent, such as understanding or choice, and has not been validated in patients with mental illness.
The MacArthur Competence Assessment Tools for Treatment (MacCAT-T) is regarded as the gold standard for capacity assessment aids. It utilizes hospital chart review followed by a semi-structured interview to address clinical issues relevant to the patient being assessed; it takes 15 to 20 minutes to complete.6 The test provides scores in each of the four domains (choice, understanding, appreciation, and reasoning) of capacity. It has been validated in patients with dementia, schizophrenia, and depression. Limiting its clinical applicability is the fact that the MacCAT-T requires training to administer and interpret the results, though this is a relatively brief process.
The Capacity to Consent to Treatment Instrument (CCTI) uses hypothetical clinical vignettes in a structured interview to assess capacity across all four domains. The tool was developed and validated in patients with dementia and Parkinson’s disease, and takes 20 to 25 minutes to complete.7 A potential limitation is the CCTI’s use of vignettes as opposed to a patient-specific discussion, which could lead to different patient answers and a false assessment of the patient’s capacity.
The Hopemont Capacity Assessment Interview (HCAI) utilizes hypothetical vignettes in a semi-structured interview format to assess understanding, appreciation, choice, and likely reasoning.8,9 Similar to CCTI, HCAI is not modified for individual patients. Rather, it uses clinical vignettes to gauge a patient’s ability to make decisions. The test takes 30 to 60 minutes to administer and performs less well in assessing appreciation and reasoning than the MacCAT-T and CCTI.10
It is not necessary to perform a formal assessment of capacity on every inpatient. For most, there is no reasonable concern for impaired capacity, obviating the need for formal testing. Likewise, in patients who clearly lack capacity, such as those with end-stage dementia or established guardians, formal reassessment usually is not required. Formal testing is most useful in situations in which capacity is unclear, disagreement amongst surrogate decision-makers exists, or judicial involvement is anticipated.
The MacCAT-T has been validated in the broadest population and is probably the most clinically useful tool currently available. The MMSE is an attractive alternative because of its widespread use and familiarity; however, it is imprecise with scores from 17 to 23, limiting its applicability.
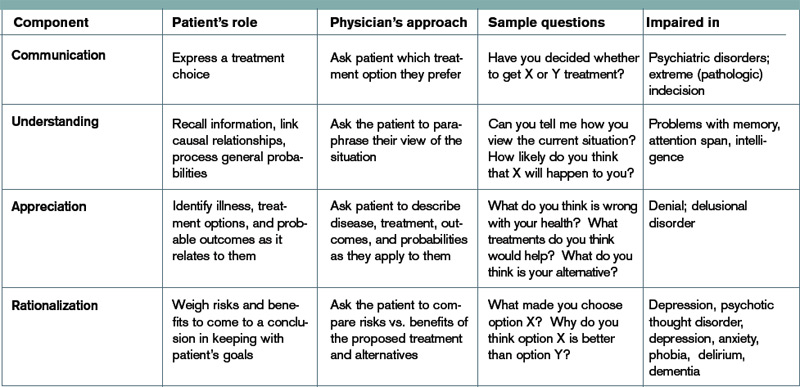
At a minimum, familiarity with the core legal standards of capacity (communication of choice, understanding, appreciation, and reasoning) will improve a hospitalist’s ability to identify patients who lack capacity. Understanding and applying the defined markers most often provides a sufficient capacity evaluation in itself. As capacity is not static, the decision usually requires more than one assessment.
Equally, deciding that a patient lacks capacity is not an end in itself, and the underlying cause should be addressed. Certain factors, such as infection, medication, time of day, and relationship with the clinician doing the assessment, can affect a patient’s capacity. These should be addressed through treatment, education, and social support whenever possible in order to optimize a patient’s performance during the capacity evaluation. If the decision can be delayed until a time when the patient can regain capacity, this should be done in order to maximize the patient’s autonomy.11
Risk-related standards of capacity.
Although some question the notion, given our desire to facilitate management beneficial to the patient, the general consensus is that we have a lower threshold for capacity for consent to treatments that are low-risk and high-benefit.12,13 We would then have a somewhat higher threshold for capacity to refuse that same treatment. Stemming from a desire to protect patients from harm, we have a relatively higher threshold for capacity to make decisions regarding high-risk, low-benefit treatments. For the remainder of cases (low risk/low benefit; high risk/high benefit), as well as treatments that significantly impact a patient’s lifestyle (e.g. dialysis, amputation), we have a low capacity to let patients decide for themselves.11,14
Other considerations.
Clinicians should be thorough in documenting details in coming to a capacity determination, both as a means to formalize the thought process running through the four determinants of capacity, and in order to document for future reference. Cases in which it could be reasonable to call a consultant for those familiar with the assessment basics include:
- Cases in which a determination of lack of capacity could adversely affect the hospitalist’s relationship with the patient;
- Cases in which the hospitalist lacks the time to properly perform the evaluation;
- Particularly difficult or high-stakes cases (e.g. cases that might involve legal proceedings); and
- Cases in which significant mental illness affects a patient’s capacity.11
Early involvement of potential surrogate decision-makers is wise for patients in whom capacity is questioned, both for obtaining collateral history as well as initiating dialogue as to the patient’s wishes. When a patient is found to lack capacity, resources to utilize to help make a treatment decision include existing advance directives and substitute decision-makers, such as durable power of attorneys (DPOAs) and family members. In those rare cases in which clinicians are unable to reach a consensus about a patient’s capacity, an ethics consult should be considered.
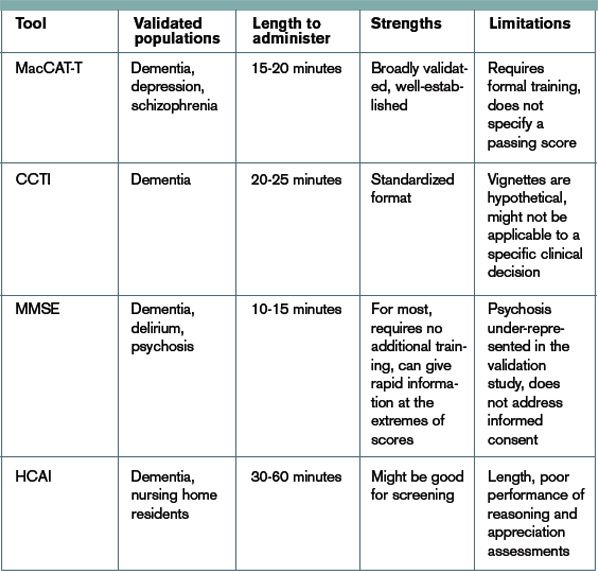
Back to the Case.
Following the patient’s declaration that dialysis is not something he is interested in, his niece reports that he is a minimalist when it comes to interventions, and that he had similarly refused a cardiac catheterization in the 1990s. You review with the patient and niece that dialysis would be a procedure to replace his failing kidney function, and that failure to pursue this would ultimately be life-threatening and likely result in death, especially in regard to electrolyte abnormalities and his lack of any other terminal illness.
The consulting nephrologist reviews their recommendations with the patient and niece as well, and the patient consistently refuses. Having clearly communicated his choice, you ask the patient if he understands the situation. He says, "My kidneys are failing. That’s how I got the high potassium." You ask him what that means. "They aren’t going to function on their own much longer," he says. "I could die from it."
You confirm his ideas, and ask him why he doesn’t want dialysis. "I don’t want dialysis because I don’t want to spend my life hooked up to machines three times a week," the patient explains. "I just want to let things run their natural course." The niece says her uncle wouldn’t have wanted dialysis even if it were 10 years ago, so she’s not surprised he is refusing now.
Following this discussion, you feel comfortable that the patient has capacity to make this decision. Having documented this discussion, you discharge him to a subacute rehabilitation facility.
Bottom Line.
In cases in which capacity is in question, a hospitalist’s case-by-case review of the four components of capacity—communicating a choice, understanding, appreciation, and rationalization and reasoning—is warranted to help determine whether a patient has capacity. In cases in which a second opinion is warranted, psychiatry, geriatrics, or ethics consults could be utilized.
Drs. Dastidar and Odden are hospitalists at the University of Michigan in Ann Arbor.
References
- Buchanan A, Brock DW. Deciding for others. Milbank Q. 1986;64(Suppl. 2):17-94.
- Guidelines for assessing the decision-making capacities of potential research subjects with cognitive impairment. American Psychiatric Association. Am J Psychiatry. 1998;155(11):1649-50.
- Appelbaum PS, Grisso T. Assessing patients’ capacities to consent to treatment. N Engl J Med. 1988;319(25):1635-1638.
- Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189-198.
- Etchells E, Darzins P, Silberfeld M, et al. Assessment of patient capacity to consent to treatment. J Gen Intern Med. 1999;14:27-34.
- Grisso T, Appelbaum PS, Hill-Fotouhi C. The MacCAT-T: a clinical tool to assess patients’ capacities to make treatment decisions. Psychiatr Serv. 1997;48:1415- 1419.
- Marson DC, Ingram KK, Cody HA, Harrell LE. Assessing the competency of patients with Alzheimer’s disease under different legal standards. A prototype instrument. Arch Neurol. 1995;52:949-954.
- Edelstein B. Hopemont Capacity Assessment Interview Manual and Scoring Guide. 1999: Morgantown, W.V.: West Virginia University.
- Pruchno RA, Smyer MA, Rose MS, Hartman-Stein PE, Henderson-Laribee DL. Competence of long-term care residents to participate in decisions about their medical care: a brief, objective assessment. Gerontologist. 1995;35:622-629.
- Moye J, Karel M, Azar AR, Gurrera R. Capacity to consent to treatment: empirical comparison of three instruments in older adults with and without dementia. Gerontologist. 2004;44:166-175.
- Grisso T, Appelbaum PS. Assessing competence to consent to treatment: a guide for physicians and other health professionals. 1998; New York: Oxford University Press, 211.
- Cale GS. Risk-related standards of competence: continuing the debate over risk-related standards of competence. Bioethics. 1999;13(2):131-148.
- Checkland D. On risk and decisional capacity. J Med Philos. 2001;26(1):35-59.
- Wilks I. The debate over risk-related standards of competence. Bioethics. 1997;11(5):413-426.
- Ganzini L, Volicer L, Nelson WA, Fox E, Derse AR. Ten myths about decision-making capacity. J Am Med Dir Assoc. 2004;5(4):263-267.
Acknowledgements:The authors would like to thank Dr. Jeff Rohde for reviewing a copy of the manuscript, and Dr. Amy Rosinski for providing direction from the psychiatry standpoint
Case
A 79-year-old male with coronary artery disease, hypertension, non-insulin-dependent mellitus, moderate dementia, and chronic renal insufficiency is admitted after a fall evaluation. He is widowed and lives in an assisted living facility. He’s accompanied by his niece, is alert, and oriented to person. He thinks he is in a clinic and is unable to state the year, but the remainder of the examination is unremarkable. His labs are notable for potassium of 6.3 mmol/L, BUN of 78 mg/dL, and Cr of 3.7 mg/dL. The niece reports that the patient is not fond of medical care, thus the most recent labs are from two years ago (and indicate a BUN of 39 and Cr of 2.8, with an upward trend over the past decade). You discuss possible long-term need for dialysis with the patient and niece, and the patient clearly states "no." However, he also states that it is 1988. How do you determine if he has the capacity to make decisions?
Overview
Hospitalists are familiar with the doctrine of informed consent—describing a disease, treatment options, associated risks and benefits, potential for complications, and alternatives, including no treatment. Not only must the patient be informed, and the decision free from any coercion, but the patient also must have capacity to make the decision.
Hospitalists often care for patients in whom decision-making capacity comes into question. This includes populations with depression, psychosis, dementia, stroke, severe personality disorders, developmental delay, comatose patients, as well as those with impaired attentional capacity (e.g. acute pain) or general debility (e.g. metastatic cancer).1,2
ave for the comatose patient, whether the patient has capacity might not be obvious. However, addressing the components of capacity (communication, understanding, appreciation, and rationalization) by using a validated clinical tool, such as the MacCAT-T, or more simply by systematically applying those four components to the clinical scenario under consideration, hospitalists can make this determination.
Review of the Literature
It is important to differentiate capacity from competency. Competency is a global assessment and a legal determination made by a judge in court. Capacity, on the other hand, is a functional assessment regarding a particular decision. Capacity is not static, and it can be performed by any clinician familiar with the patient. A hospitalist often is well positioned to make a capacity determination given established rapport with the patient and familiarity with the details of the case.
To make this determination, a hospitalist needs to know how to assess capacity. Although capacity usually is defined by state law and varies by jurisdiction, clinicians generally can assume it includes one or more of the four key components:
- Communication. The patient needs to be able to express a treatment choice, and this decision needs to be stable enough for the treatment to be implemented. Changing one’s decision in itself would not bring a patient’s capacity into question, so long as the patient was able to explain the rationale behind the switch. Frequent changes back and forth in the decision-making, however, could be indicative of an underlying psychiatric disorder or extreme indecision, which could bring capacity into question.
- Understanding. The patient needs to recall conversations about treatment, to make the link between causal relationships, and to process probabilities for outcomes. Problems with memory, attention span, and intelligence can affect one’s understanding.
- Appreciation. The patient should be able to identify the illness, treatment options, and likely outcomes as things that will affect him or her directly. A lack of appreciation usually stems from a denial based on intelligence (lack of a capability to understand) or emotion, or a delusion that the patient is not affected by this situation the same way and will have a different outcome.
- Rationalization or reasoning. The patient needs to be able to weigh the risks and benefits of the treatment options presented to come to a conclusion in keeping with their goals and best interests, as defined by their personal set of values. This often is affected in psychosis, depression, anxiety, phobias, delirium, and dementia.3
Several clinical capacity tools have been developed to assess these components:
Clinical tools.
The Mini-Mental Status Examination (MMSE) is a bedside test of a patient’s cognitive function, with scores ranging from 0 to 30.4 Although it wasn’t developed for assessing decision-making capacity, it has been compared with expert evaluation for assessment of capacity; the test performs reasonably well, particularly with high and low scores. Specifically, a MMSE >24 has a negative likelihood ratio (LR) of 0.05 for lack of capacity, while a MMSE <16 has a positive LR of 15.5 Scores from 17 to 23 do not correlate well with capacity, and further testing would be necessary. It is easy to administer, requires no formal training, and is familiar to most hospitalists. However, it does not address any specific aspects of informed consent, such as understanding or choice, and has not been validated in patients with mental illness.
The MacArthur Competence Assessment Tools for Treatment (MacCAT-T) is regarded as the gold standard for capacity assessment aids. It utilizes hospital chart review followed by a semi-structured interview to address clinical issues relevant to the patient being assessed; it takes 15 to 20 minutes to complete.6 The test provides scores in each of the four domains (choice, understanding, appreciation, and reasoning) of capacity. It has been validated in patients with dementia, schizophrenia, and depression. Limiting its clinical applicability is the fact that the MacCAT-T requires training to administer and interpret the results, though this is a relatively brief process.
The Capacity to Consent to Treatment Instrument (CCTI) uses hypothetical clinical vignettes in a structured interview to assess capacity across all four domains. The tool was developed and validated in patients with dementia and Parkinson’s disease, and takes 20 to 25 minutes to complete.7 A potential limitation is the CCTI’s use of vignettes as opposed to a patient-specific discussion, which could lead to different patient answers and a false assessment of the patient’s capacity.
The Hopemont Capacity Assessment Interview (HCAI) utilizes hypothetical vignettes in a semi-structured interview format to assess understanding, appreciation, choice, and likely reasoning.8,9 Similar to CCTI, HCAI is not modified for individual patients. Rather, it uses clinical vignettes to gauge a patient’s ability to make decisions. The test takes 30 to 60 minutes to administer and performs less well in assessing appreciation and reasoning than the MacCAT-T and CCTI.10
It is not necessary to perform a formal assessment of capacity on every inpatient. For most, there is no reasonable concern for impaired capacity, obviating the need for formal testing. Likewise, in patients who clearly lack capacity, such as those with end-stage dementia or established guardians, formal reassessment usually is not required. Formal testing is most useful in situations in which capacity is unclear, disagreement amongst surrogate decision-makers exists, or judicial involvement is anticipated.
The MacCAT-T has been validated in the broadest population and is probably the most clinically useful tool currently available. The MMSE is an attractive alternative because of its widespread use and familiarity; however, it is imprecise with scores from 17 to 23, limiting its applicability.
At a minimum, familiarity with the core legal standards of capacity (communication of choice, understanding, appreciation, and reasoning) will improve a hospitalist’s ability to identify patients who lack capacity. Understanding and applying the defined markers most often provides a sufficient capacity evaluation in itself. As capacity is not static, the decision usually requires more than one assessment.
Equally, deciding that a patient lacks capacity is not an end in itself, and the underlying cause should be addressed. Certain factors, such as infection, medication, time of day, and relationship with the clinician doing the assessment, can affect a patient’s capacity. These should be addressed through treatment, education, and social support whenever possible in order to optimize a patient’s performance during the capacity evaluation. If the decision can be delayed until a time when the patient can regain capacity, this should be done in order to maximize the patient’s autonomy.11
Risk-related standards of capacity.
Although some question the notion, given our desire to facilitate management beneficial to the patient, the general consensus is that we have a lower threshold for capacity for consent to treatments that are low-risk and high-benefit.12,13 We would then have a somewhat higher threshold for capacity to refuse that same treatment. Stemming from a desire to protect patients from harm, we have a relatively higher threshold for capacity to make decisions regarding high-risk, low-benefit treatments. For the remainder of cases (low risk/low benefit; high risk/high benefit), as well as treatments that significantly impact a patient’s lifestyle (e.g. dialysis, amputation), we have a low capacity to let patients decide for themselves.11,14
Other considerations.
Clinicians should be thorough in documenting details in coming to a capacity determination, both as a means to formalize the thought process running through the four determinants of capacity, and in order to document for future reference. Cases in which it could be reasonable to call a consultant for those familiar with the assessment basics include:
- Cases in which a determination of lack of capacity could adversely affect the hospitalist’s relationship with the patient;
- Cases in which the hospitalist lacks the time to properly perform the evaluation;
- Particularly difficult or high-stakes cases (e.g. cases that might involve legal proceedings); and
- Cases in which significant mental illness affects a patient’s capacity.11
Early involvement of potential surrogate decision-makers is wise for patients in whom capacity is questioned, both for obtaining collateral history as well as initiating dialogue as to the patient’s wishes. When a patient is found to lack capacity, resources to utilize to help make a treatment decision include existing advance directives and substitute decision-makers, such as durable power of attorneys (DPOAs) and family members. In those rare cases in which clinicians are unable to reach a consensus about a patient’s capacity, an ethics consult should be considered.
Back to the Case.
Following the patient’s declaration that dialysis is not something he is interested in, his niece reports that he is a minimalist when it comes to interventions, and that he had similarly refused a cardiac catheterization in the 1990s. You review with the patient and niece that dialysis would be a procedure to replace his failing kidney function, and that failure to pursue this would ultimately be life-threatening and likely result in death, especially in regard to electrolyte abnormalities and his lack of any other terminal illness.
The consulting nephrologist reviews their recommendations with the patient and niece as well, and the patient consistently refuses. Having clearly communicated his choice, you ask the patient if he understands the situation. He says, "My kidneys are failing. That’s how I got the high potassium." You ask him what that means. "They aren’t going to function on their own much longer," he says. "I could die from it."
You confirm his ideas, and ask him why he doesn’t want dialysis. "I don’t want dialysis because I don’t want to spend my life hooked up to machines three times a week," the patient explains. "I just want to let things run their natural course." The niece says her uncle wouldn’t have wanted dialysis even if it were 10 years ago, so she’s not surprised he is refusing now.
Following this discussion, you feel comfortable that the patient has capacity to make this decision. Having documented this discussion, you discharge him to a subacute rehabilitation facility.
Bottom Line.
In cases in which capacity is in question, a hospitalist’s case-by-case review of the four components of capacity—communicating a choice, understanding, appreciation, and rationalization and reasoning—is warranted to help determine whether a patient has capacity. In cases in which a second opinion is warranted, psychiatry, geriatrics, or ethics consults could be utilized.
Drs. Dastidar and Odden are hospitalists at the University of Michigan in Ann Arbor.
References
- Buchanan A, Brock DW. Deciding for others. Milbank Q. 1986;64(Suppl. 2):17-94.
- Guidelines for assessing the decision-making capacities of potential research subjects with cognitive impairment. American Psychiatric Association. Am J Psychiatry. 1998;155(11):1649-50.
- Appelbaum PS, Grisso T. Assessing patients’ capacities to consent to treatment. N Engl J Med. 1988;319(25):1635-1638.
- Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189-198.
- Etchells E, Darzins P, Silberfeld M, et al. Assessment of patient capacity to consent to treatment. J Gen Intern Med. 1999;14:27-34.
- Grisso T, Appelbaum PS, Hill-Fotouhi C. The MacCAT-T: a clinical tool to assess patients’ capacities to make treatment decisions. Psychiatr Serv. 1997;48:1415- 1419.
- Marson DC, Ingram KK, Cody HA, Harrell LE. Assessing the competency of patients with Alzheimer’s disease under different legal standards. A prototype instrument. Arch Neurol. 1995;52:949-954.
- Edelstein B. Hopemont Capacity Assessment Interview Manual and Scoring Guide. 1999: Morgantown, W.V.: West Virginia University.
- Pruchno RA, Smyer MA, Rose MS, Hartman-Stein PE, Henderson-Laribee DL. Competence of long-term care residents to participate in decisions about their medical care: a brief, objective assessment. Gerontologist. 1995;35:622-629.
- Moye J, Karel M, Azar AR, Gurrera R. Capacity to consent to treatment: empirical comparison of three instruments in older adults with and without dementia. Gerontologist. 2004;44:166-175.
- Grisso T, Appelbaum PS. Assessing competence to consent to treatment: a guide for physicians and other health professionals. 1998; New York: Oxford University Press, 211.
- Cale GS. Risk-related standards of competence: continuing the debate over risk-related standards of competence. Bioethics. 1999;13(2):131-148.
- Checkland D. On risk and decisional capacity. J Med Philos. 2001;26(1):35-59.
- Wilks I. The debate over risk-related standards of competence. Bioethics. 1997;11(5):413-426.
- Ganzini L, Volicer L, Nelson WA, Fox E, Derse AR. Ten myths about decision-making capacity. J Am Med Dir Assoc. 2004;5(4):263-267.
Acknowledgements:The authors would like to thank Dr. Jeff Rohde for reviewing a copy of the manuscript, and Dr. Amy Rosinski for providing direction from the psychiatry standpoint
Case
A 79-year-old male with coronary artery disease, hypertension, non-insulin-dependent mellitus, moderate dementia, and chronic renal insufficiency is admitted after a fall evaluation. He is widowed and lives in an assisted living facility. He’s accompanied by his niece, is alert, and oriented to person. He thinks he is in a clinic and is unable to state the year, but the remainder of the examination is unremarkable. His labs are notable for potassium of 6.3 mmol/L, BUN of 78 mg/dL, and Cr of 3.7 mg/dL. The niece reports that the patient is not fond of medical care, thus the most recent labs are from two years ago (and indicate a BUN of 39 and Cr of 2.8, with an upward trend over the past decade). You discuss possible long-term need for dialysis with the patient and niece, and the patient clearly states "no." However, he also states that it is 1988. How do you determine if he has the capacity to make decisions?
Overview
Hospitalists are familiar with the doctrine of informed consent—describing a disease, treatment options, associated risks and benefits, potential for complications, and alternatives, including no treatment. Not only must the patient be informed, and the decision free from any coercion, but the patient also must have capacity to make the decision.
Hospitalists often care for patients in whom decision-making capacity comes into question. This includes populations with depression, psychosis, dementia, stroke, severe personality disorders, developmental delay, comatose patients, as well as those with impaired attentional capacity (e.g. acute pain) or general debility (e.g. metastatic cancer).1,2
ave for the comatose patient, whether the patient has capacity might not be obvious. However, addressing the components of capacity (communication, understanding, appreciation, and rationalization) by using a validated clinical tool, such as the MacCAT-T, or more simply by systematically applying those four components to the clinical scenario under consideration, hospitalists can make this determination.
Review of the Literature
It is important to differentiate capacity from competency. Competency is a global assessment and a legal determination made by a judge in court. Capacity, on the other hand, is a functional assessment regarding a particular decision. Capacity is not static, and it can be performed by any clinician familiar with the patient. A hospitalist often is well positioned to make a capacity determination given established rapport with the patient and familiarity with the details of the case.
To make this determination, a hospitalist needs to know how to assess capacity. Although capacity usually is defined by state law and varies by jurisdiction, clinicians generally can assume it includes one or more of the four key components:
- Communication. The patient needs to be able to express a treatment choice, and this decision needs to be stable enough for the treatment to be implemented. Changing one’s decision in itself would not bring a patient’s capacity into question, so long as the patient was able to explain the rationale behind the switch. Frequent changes back and forth in the decision-making, however, could be indicative of an underlying psychiatric disorder or extreme indecision, which could bring capacity into question.
- Understanding. The patient needs to recall conversations about treatment, to make the link between causal relationships, and to process probabilities for outcomes. Problems with memory, attention span, and intelligence can affect one’s understanding.
- Appreciation. The patient should be able to identify the illness, treatment options, and likely outcomes as things that will affect him or her directly. A lack of appreciation usually stems from a denial based on intelligence (lack of a capability to understand) or emotion, or a delusion that the patient is not affected by this situation the same way and will have a different outcome.
- Rationalization or reasoning. The patient needs to be able to weigh the risks and benefits of the treatment options presented to come to a conclusion in keeping with their goals and best interests, as defined by their personal set of values. This often is affected in psychosis, depression, anxiety, phobias, delirium, and dementia.3
Several clinical capacity tools have been developed to assess these components:
Clinical tools.
The Mini-Mental Status Examination (MMSE) is a bedside test of a patient’s cognitive function, with scores ranging from 0 to 30.4 Although it wasn’t developed for assessing decision-making capacity, it has been compared with expert evaluation for assessment of capacity; the test performs reasonably well, particularly with high and low scores. Specifically, a MMSE >24 has a negative likelihood ratio (LR) of 0.05 for lack of capacity, while a MMSE <16 has a positive LR of 15.5 Scores from 17 to 23 do not correlate well with capacity, and further testing would be necessary. It is easy to administer, requires no formal training, and is familiar to most hospitalists. However, it does not address any specific aspects of informed consent, such as understanding or choice, and has not been validated in patients with mental illness.
The MacArthur Competence Assessment Tools for Treatment (MacCAT-T) is regarded as the gold standard for capacity assessment aids. It utilizes hospital chart review followed by a semi-structured interview to address clinical issues relevant to the patient being assessed; it takes 15 to 20 minutes to complete.6 The test provides scores in each of the four domains (choice, understanding, appreciation, and reasoning) of capacity. It has been validated in patients with dementia, schizophrenia, and depression. Limiting its clinical applicability is the fact that the MacCAT-T requires training to administer and interpret the results, though this is a relatively brief process.
The Capacity to Consent to Treatment Instrument (CCTI) uses hypothetical clinical vignettes in a structured interview to assess capacity across all four domains. The tool was developed and validated in patients with dementia and Parkinson’s disease, and takes 20 to 25 minutes to complete.7 A potential limitation is the CCTI’s use of vignettes as opposed to a patient-specific discussion, which could lead to different patient answers and a false assessment of the patient’s capacity.
The Hopemont Capacity Assessment Interview (HCAI) utilizes hypothetical vignettes in a semi-structured interview format to assess understanding, appreciation, choice, and likely reasoning.8,9 Similar to CCTI, HCAI is not modified for individual patients. Rather, it uses clinical vignettes to gauge a patient’s ability to make decisions. The test takes 30 to 60 minutes to administer and performs less well in assessing appreciation and reasoning than the MacCAT-T and CCTI.10
It is not necessary to perform a formal assessment of capacity on every inpatient. For most, there is no reasonable concern for impaired capacity, obviating the need for formal testing. Likewise, in patients who clearly lack capacity, such as those with end-stage dementia or established guardians, formal reassessment usually is not required. Formal testing is most useful in situations in which capacity is unclear, disagreement amongst surrogate decision-makers exists, or judicial involvement is anticipated.
The MacCAT-T has been validated in the broadest population and is probably the most clinically useful tool currently available. The MMSE is an attractive alternative because of its widespread use and familiarity; however, it is imprecise with scores from 17 to 23, limiting its applicability.
At a minimum, familiarity with the core legal standards of capacity (communication of choice, understanding, appreciation, and reasoning) will improve a hospitalist’s ability to identify patients who lack capacity. Understanding and applying the defined markers most often provides a sufficient capacity evaluation in itself. As capacity is not static, the decision usually requires more than one assessment.
Equally, deciding that a patient lacks capacity is not an end in itself, and the underlying cause should be addressed. Certain factors, such as infection, medication, time of day, and relationship with the clinician doing the assessment, can affect a patient’s capacity. These should be addressed through treatment, education, and social support whenever possible in order to optimize a patient’s performance during the capacity evaluation. If the decision can be delayed until a time when the patient can regain capacity, this should be done in order to maximize the patient’s autonomy.11
Risk-related standards of capacity.
Although some question the notion, given our desire to facilitate management beneficial to the patient, the general consensus is that we have a lower threshold for capacity for consent to treatments that are low-risk and high-benefit.12,13 We would then have a somewhat higher threshold for capacity to refuse that same treatment. Stemming from a desire to protect patients from harm, we have a relatively higher threshold for capacity to make decisions regarding high-risk, low-benefit treatments. For the remainder of cases (low risk/low benefit; high risk/high benefit), as well as treatments that significantly impact a patient’s lifestyle (e.g. dialysis, amputation), we have a low capacity to let patients decide for themselves.11,14
Other considerations.
Clinicians should be thorough in documenting details in coming to a capacity determination, both as a means to formalize the thought process running through the four determinants of capacity, and in order to document for future reference. Cases in which it could be reasonable to call a consultant for those familiar with the assessment basics include:
- Cases in which a determination of lack of capacity could adversely affect the hospitalist’s relationship with the patient;
- Cases in which the hospitalist lacks the time to properly perform the evaluation;
- Particularly difficult or high-stakes cases (e.g. cases that might involve legal proceedings); and
- Cases in which significant mental illness affects a patient’s capacity.11
Early involvement of potential surrogate decision-makers is wise for patients in whom capacity is questioned, both for obtaining collateral history as well as initiating dialogue as to the patient’s wishes. When a patient is found to lack capacity, resources to utilize to help make a treatment decision include existing advance directives and substitute decision-makers, such as durable power of attorneys (DPOAs) and family members. In those rare cases in which clinicians are unable to reach a consensus about a patient’s capacity, an ethics consult should be considered.
Back to the Case.
Following the patient’s declaration that dialysis is not something he is interested in, his niece reports that he is a minimalist when it comes to interventions, and that he had similarly refused a cardiac catheterization in the 1990s. You review with the patient and niece that dialysis would be a procedure to replace his failing kidney function, and that failure to pursue this would ultimately be life-threatening and likely result in death, especially in regard to electrolyte abnormalities and his lack of any other terminal illness.
The consulting nephrologist reviews their recommendations with the patient and niece as well, and the patient consistently refuses. Having clearly communicated his choice, you ask the patient if he understands the situation. He says, "My kidneys are failing. That’s how I got the high potassium." You ask him what that means. "They aren’t going to function on their own much longer," he says. "I could die from it."
You confirm his ideas, and ask him why he doesn’t want dialysis. "I don’t want dialysis because I don’t want to spend my life hooked up to machines three times a week," the patient explains. "I just want to let things run their natural course." The niece says her uncle wouldn’t have wanted dialysis even if it were 10 years ago, so she’s not surprised he is refusing now.
Following this discussion, you feel comfortable that the patient has capacity to make this decision. Having documented this discussion, you discharge him to a subacute rehabilitation facility.
Bottom Line.
In cases in which capacity is in question, a hospitalist’s case-by-case review of the four components of capacity—communicating a choice, understanding, appreciation, and rationalization and reasoning—is warranted to help determine whether a patient has capacity. In cases in which a second opinion is warranted, psychiatry, geriatrics, or ethics consults could be utilized.
Drs. Dastidar and Odden are hospitalists at the University of Michigan in Ann Arbor.
References
- Buchanan A, Brock DW. Deciding for others. Milbank Q. 1986;64(Suppl. 2):17-94.
- Guidelines for assessing the decision-making capacities of potential research subjects with cognitive impairment. American Psychiatric Association. Am J Psychiatry. 1998;155(11):1649-50.
- Appelbaum PS, Grisso T. Assessing patients’ capacities to consent to treatment. N Engl J Med. 1988;319(25):1635-1638.
- Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189-198.
- Etchells E, Darzins P, Silberfeld M, et al. Assessment of patient capacity to consent to treatment. J Gen Intern Med. 1999;14:27-34.
- Grisso T, Appelbaum PS, Hill-Fotouhi C. The MacCAT-T: a clinical tool to assess patients’ capacities to make treatment decisions. Psychiatr Serv. 1997;48:1415- 1419.
- Marson DC, Ingram KK, Cody HA, Harrell LE. Assessing the competency of patients with Alzheimer’s disease under different legal standards. A prototype instrument. Arch Neurol. 1995;52:949-954.
- Edelstein B. Hopemont Capacity Assessment Interview Manual and Scoring Guide. 1999: Morgantown, W.V.: West Virginia University.
- Pruchno RA, Smyer MA, Rose MS, Hartman-Stein PE, Henderson-Laribee DL. Competence of long-term care residents to participate in decisions about their medical care: a brief, objective assessment. Gerontologist. 1995;35:622-629.
- Moye J, Karel M, Azar AR, Gurrera R. Capacity to consent to treatment: empirical comparison of three instruments in older adults with and without dementia. Gerontologist. 2004;44:166-175.
- Grisso T, Appelbaum PS. Assessing competence to consent to treatment: a guide for physicians and other health professionals. 1998; New York: Oxford University Press, 211.
- Cale GS. Risk-related standards of competence: continuing the debate over risk-related standards of competence. Bioethics. 1999;13(2):131-148.
- Checkland D. On risk and decisional capacity. J Med Philos. 2001;26(1):35-59.
- Wilks I. The debate over risk-related standards of competence. Bioethics. 1997;11(5):413-426.
- Ganzini L, Volicer L, Nelson WA, Fox E, Derse AR. Ten myths about decision-making capacity. J Am Med Dir Assoc. 2004;5(4):263-267.
Acknowledgements:The authors would like to thank Dr. Jeff Rohde for reviewing a copy of the manuscript, and Dr. Amy Rosinski for providing direction from the psychiatry standpoint