User login

› Aim for a glycated hemoglobin of <7% for most nonpregnant patients with type 2 diabetes, with a less stringent target for those with severe hypoglycemia, limited life expectancy, advanced micro- or macrovascular complications, and/or extensive comorbidities. B
› Attempt to treat patients with diabetes and hypertension to a target blood pressure<140/90mm Hg. B
› Prescribe statin therapy regardless of baseline lipid levels for all patients
who have diabetes and are between the ages of 40 and 75years. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Dennis D, age 63, was recently diagnosed with diabetes. his glycated hemoglobin (HbA1c) is 7.8%, his blood pressure (BP) is mildly elevated (145/95 mm Hg), and his body mass index (BMI) is 28.5, but his low-density lipoprotein (LDL) cholesterol is 100 mg/dl, his high-density lipoprotein (HDL) cholesterol is 52 mg/dL, and he has no history of cardiovascular disease (CVD). After an unsuccessful attempt to treat him with lifestyle modification, it is time to initiate diabetes therapy.
Other than an alpha-blocker for benign prostatic hyperplasia and a prostaglandin for glaucoma, Mr. D takes no other medications. You prescribe metformin 500 mg twice daily and consider what else to add to keep his diabetes well controlled. Should you prescribe an antihypertensive? And, despite the patient’s normal lipid levels, should he begin taking a statin?
Type 2 diabetes has been extensively studied in rigorous randomized controlled trials (RCTs). While studies have provided ample evidence in support of optimal treatment, differing interpretations of the findings are reflected in consensus guidelines developed by expert panels that don’t always see eye to eye on what diabetes treatment targets should be and how best to prevent micro- and macrovascular complications.
What’s more, recommendations continue to be updated as new data emerge. In February 2014, the Joint Committee on Prevention, Evaluation, and Treatment of High Blood Pressure (JCN 8) revised its target for patients with diabetes to <140/90 mm Hg (from <130/80 mm Hg).1 This is likely to lead to revisions in other leading consensus guidelines, as well.
Thus, primary care physicians managing the care of patients with diabetes face the challenge of using the latest recommendations in a manner that addresses the entire clinical picture, considering each patient’s age and overall health status, priorities, and preferences. We developed this evidence-based review and guide- line summary with that in mind.
HbA1c target: How low should you go?
The Diabetes Control and Complications Trial (DCCT), published nearly 20 years ago, studied patients with type 1 diabetes, and found that intensive insulin therapy (HbA1c ≤6%) delayed the onset of retinopathy, nephropathy, and neuropathy.2 However, there was an important adverse effect of such intensive therapy: Patients in this group suffered from severe hypoglycemic episodes 3 times more frequently than those in the usual care group. Nonetheless, the microvascular benefits of intensive control observed in those with type 1 diabetes were thought to be similar for patients with type 2 diabetes.
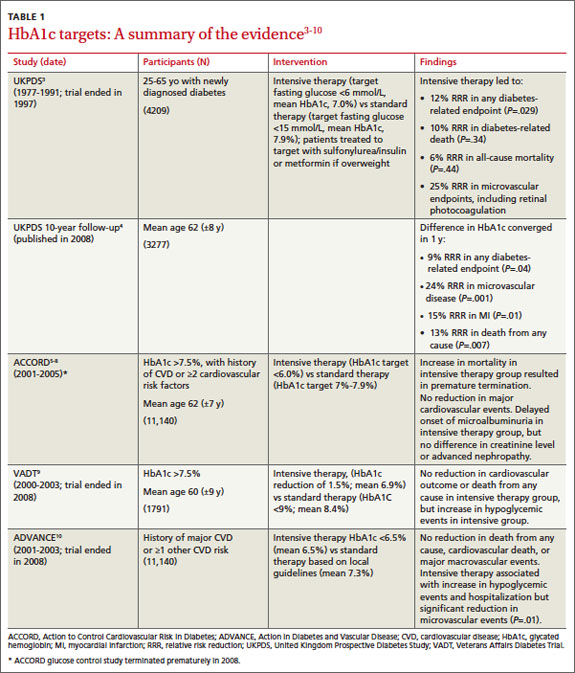
The United Kingdom Prospective Diabetes Study (UKPDS), published in 1999, was the first major study to investigate targets for glucose control in patients with type 2 diabetes.3 Participants treated intensively (mean HbA1c goal, 7%) had a 25% reduction in microvascular complications, including the need for retinal photocoagulation, com- pared with those on standard control (mean HbA1c, 7.9%). There was also a nonsignificant trend toward a reduction in macrovascular complications in the intensive therapy group, but no difference in overall mortality rate.3
A 10-year follow-up of the UKPDS showed that while baseline differences in HbA1c between the 2 groups were lost by one year, reductions in microvascular complications continued to occur in the intensive treatment group.4 Reductions in myocardial infarction (MI) and death emerged over time, a possible legacy effect (ie, the result of intense treatment early in the course of the disease).
The Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial, published in 2008, studied patients at risk for CVD, defined by either a prior history of CVD or ≥2 other cardiovascular risk factors.5 Participants, all of whom had poorly controlled type 2 diabetes (mean HbA1c, 8.1%), were randomized to either intensive treatment (HbA1c goal, <6%) or standard therapy (HbA1c goal, 7%-7.9%). The study was discontinued after a mean follow-up of 3.5 years, when those in the intensive therapy group were found to have a higher mortality rate.5
The rate of nonfatal MI reported by the ACCORD trial was lower in the intensive therapy group, however, and participants in this group also had delayed onset of microalbuminuria.6 No differences were seen in serum creatinine concentrations, advanced nephropathy, diabetic eye complications, or nonfatal stroke. Five-year follow up confirmed an increased mortality rate in the intensive therapy group,7 the result of severe hypoglycemia.8
The Veterans Affairs Diabetes Trial (VADT) randomized patients with poorly controlled type 2 diabetes to intensive or standard therapy.9 At 6 months, the intensive therapy group’s HbA1c averaged 6.9%, compared with 8.4% for the standard therapy group. Except for a delay in the progression of albuminuria, no significant effects of intensive therapy were found: Rates of other microvascular complications, major cardiovascular events, and death were similar.9 It should be noted that the VADT involved fewer participants and shorter follow-up than the other trials cited (TABLE 1),3-10 which may have affected its findings.
The Action in Diabetes and Vascular Disease (ADVANCE) trial, which included participants with either a history of major CVD or ≥1 other CVD risk factors, compared an intensive control group (mean HbA1c, 6.5%) with a standard care group (mean HbA1c, 7.3%)—with mixed results.10 Microalbuminuria occurred less frequently in the intensive therapy group, but hypoglycemia and hospitalization increased. No reduction in death from any cause, in cardiovascular death, or in major macrovascular events was found.
How to proceed? What the experts recommend
In updated standards for the medical care of diabetes released in January 2013,11 the American Diabetes Association (ADA) calls for an HbA1c goal <7% for most nonpregnant adults with type 2 diabetes. This is in line with the 2012 International Diabetes Federation (IDF) guideline.12
The 2011 guideline from the American Association of Clinical Endocrinologists (AACE),13 however, recommends tighter control—an HbA1c of ≤6.5% for most patients. For patients with diabetes of short duration, a long life expectancy, and no significant history of CVD, the AACE believes that this more aggressive goal has the potential to further reduce the risk of microvascular complications.
A less stringent target (eg, <8%) may be more appropriate for patients with a higher risk of adverse effects. That would apply to those with a history of severe hypoglycemia, a limited life expectancy, advanced micro- or macrovascular complications, or extensive comorbid conditions, as well as to any patient for whom stricter control is difficult to attain even with intensive therapy.13
Setting a BP target
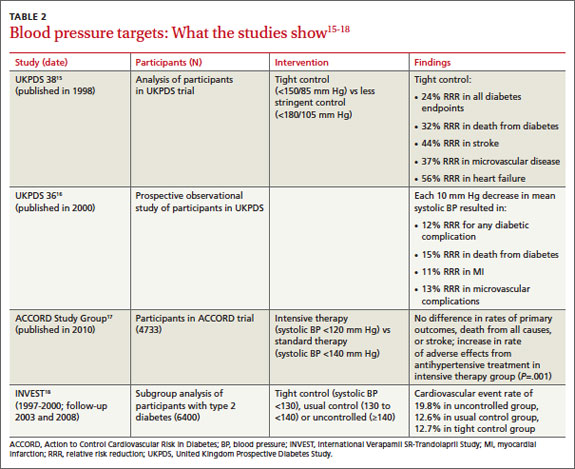
In 2003, the 7th report of the Joint Committee on Prevention, Evaluation, and Treatment of High Blood Pressure (JCN 7) recommended a target BP <130/80 mm Hg for diabetes patients.14 Most major diabetes guidelines, including those of the AACE13 and IDF,12 echoed this recommendation. As noted earlier, JNC 8, published earlier this year, loosened the recommendation to <140/90 mm Hg.1 Although evidence has shown that treatment to a systolic BP <150 mm Hg improves cardiovascular and cerebrovascular outcomes for patients with diabetes,15 no RCTs have addressed whether more intensive treatment to achieve a systolic BP <140 mm Hg provides further benefit.
The BP of participants in the UKPDS has been examined, with patients with tighter control (<150/85 mm Hg) compared with those with less stringent control (<180/105 mm Hg). The tight control group showed a significant reduction in both death and complications related to diabetes, progression of diabetic retinopathy, and deterioration in visual acuity.15 Further investigation found that each 10 mm Hg reduction in systolic pressure was associated with a risk reduction of 15% for death related to diabetes, 12% for diabetes-related complications, 11% for MI, and 13% for microvascular complications.16
The ACCORD trial randomized participants to more intensive control (systolic BP <120 mm Hg, with a mean of 119.3) or standard therapy (systolic BP <140 mm Hg, mean 133.).17 After 4.7 years, no difference was found in the rates of MI, stroke, or death. However, a significant increase in the rate of serious adverse effects from antihypertensive treatment (including hypotension, syncope, bradycardia, hypokalemia, angioedema, and renal failure) occurred in the intensive control group.17
A subgroup analysis of patients with type 2 diabetes enrolled in the International Verapamil SR-Trandolapril Study (INVEST) evaluated systolic BP control and cardiovascular outcomes in those with preexisting coronary artery disease.18 Participants were categorized as having tight control if their systolic BP <130 mm Hg; usual control, if systolic pressure was between 130 and <140 mm Hg; and uncontrolled, if systolic BP ≥140 mm Hg. Those in the usual control group had lower risks of death, nonfatal MI, and stroke compared with those in the uncontrolled group, but little difference was found between patients in the usual control and tight control groups. The studies are summarized in TABLE 2.15-18
Interpreting the results: The experts disagree
The ADA recommends that patients with diabetes and hypertension be treated to a goal <140 mm Hg systolic and <80 mm Hg diastolic pressure11—more lenient than the recommendations of either the AACE or the IDF. It is not clear whether these recommendations will change, however, given the recent JNC 8 report.1 A lower systolic target may be appropriate for certain patients, if it can be achieved without undue adverse effects from antihypertensive medication. Older patients in particular may be at risk for orthostasis or falls as a result of more aggressive treatment.
CASE › Mr. D’s most recent BP is 145/95. Given that his goal is <140/90, you elect to start lisinopril 10 mg daily, advise him to monitor his BP at home, and refer him to a dietician to discuss the Dietary Approaches to Stop Hypertension diet.
Lipid levels: When to add statin therapy
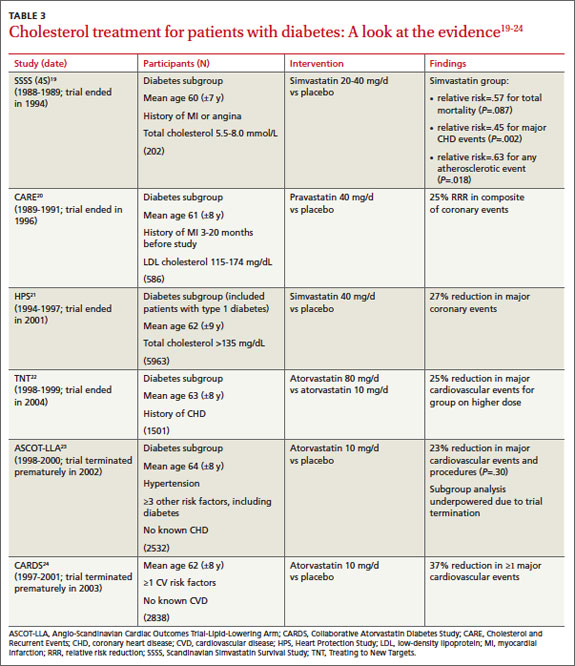
Like glucose and BP control, lipid control and, concomitantly, the benefit of statin therapy for patients with type 2 diabetes has been studied extensively (TABLE 3).19-24
The Scandinavian Simvastatin Survival Study (4S) recruited participants with a history of MI or angina, and included a small diabetes subgroup.19 Participants were randomized to simvastatin 20 mg daily, with blinded titration up to 40 mg/d, or placebo. Among those with diabetes, patients on simvastatin had a 55% reduction in risk for major coronary heart disease events and a 43% reduction in total mortality. The risk reduction did not depend on baseline levels of total cholesterol, LDL cholesterol, HDL cholesterol, or triglycerides.
Cholesterol and Recurrent Events (CARE), which studied participants with a history of MI 3 to 20 months prior to the start of the study and also included a diabetes subgroup, had a similar outcome.20 Compared with placebo, treatment with pravastatin 40 mg/d reduced the risk of both coronary events and revascularization procedures by 25%.
The Heart Protection Study randomized patients with either diabetes or a history of occlusive arterial disease to receive simvastatin 40 mg daily or placebo.21 In the treatment group, the risk of major vascular events was reduced in patients with diabetes by 27%. Improvements were seen in patients with LDL cholesterol levels both above and below 116 mg/dL.
Multiple studies have evaluated the benefits of atorvastatin for patients with diabetes. All have demonstrated a significant reduction in the risk of MI and death in those on statin therapy. The Treating to New Targets study showed a 25% reduction in major cardiovascular events in those treated with 80 mg atorvastatin daily (mean LDL, 77 mg/dL) vs those treated with 10 mg of the drug (mean LDL, 86 mg/dL).22 The Anglo-Scandinavian Cardiac Outcomes Trial–Lipid-Lowering Arm (ASCOT-LLA)23 and the Collaborative Atorvastatin Diabetes Study (CARDS)24 were both terminated early due to the magnitude of benefit seen with statin therapy. In contrast to LDL, evidence for non-LDL treatment goals is lacking in the diabetes literature. Also, there is little evidence to support nonstatin cholesterol-lowering therapy for the management of diabetes patients.
Statin use is widely recommended
In 2008, the ADA and the American College of Cardiology Foundation (ACCF) produced a joint consensus statement regarding lipoprotein management for patients with diabetes and multiple CVD risk factors.25 Target LDL was recommended at <100 mg/dL for moderately high-risk primary prevention patients, including those with diabetes. For patients with diabetes and ≥1 other risk factors, the ADA/ACCF recommended an LDL goal <70 mg/dL. The 2011 AACE guideline has the same treatment goals,13 while the 2012 IDF guidelines are more aggressive.12 For primary prevention, the AACE endorses an LDL goal <80 mg/dL, and <70 mg/dL for those with known CVD.13
The updated standards released by the ADA in January 2013 recommend statin therapy regardless of LDL level for patients who have diabetes and known CVD, as well as for those ages 40 years and older who do not have CVD but have ≥1 other risk factors. Specific risk factors include hypertension, dyslipidemia, albuminuria, and a family history of CVD.11
The latest statin guideline. In November 2013, the American College of Cardiology and American Heart Association (ACC/AHA) published a new guideline for the treatment of cholesterol to reduce cardiovascular risk,26 but said nothing for or against specific LDL or non-HDL cholesterol targets. The ACC/AHA recommends that all patients who have diabetes and are between the ages of 40 and 75 years be treated with a moderate dose of a statin—a target supported with strong (strength of recommendation: A) evidence.
Patients with diabetes and an estimated 10-year risk of CVD >7.5% should be considered for high-intensity statin therapy, according to the ACC/AHA.26 For patients younger than 40 or older than 75, the decision to initiate statin therapy should be made by weighing the potential cardiovascular benefits, the risk of adverse effects, and the potential for drug-drug-interactions, as well as patient preference.
CASE › You discuss the need for moderate-dose statin therapy with Mr. D. He is hesitant at first, referring to a coworker who had “leg cramps” when he was taking a statin. You emphasize the importance of prevention in the care of his diabetes and convince the patient to begin a trial of atorvastatin 40 mg daily.
You warn Mr. D of the possibility of an allergic reaction, rash, or cough from lisinopril and loose stools from metformin, and advise him to call if he develops muscle cramps that could be associated with the statin. Finally, you stress the importance of lifestyle modification, including diet and weight loss, and schedule a follow-up visit in 3 months.
At Mr. D’s next visit, you will check his HbA1c and BP. If his HbA1c is still >7.0%, you may increase the dose of metformin or add a sulfonylurea. The dose of lisinopril could be increased if the patient’s BP continues to be elevated. There will be no need to recheck Mr. D’s cholesterol levels, however, because the purpose of the statin therapy is to improve overall outcomes, rather than to achieve a target goal.
CORRESPONDENCE
Kathryn M. Harmes, MD, Department of Family Medicine, University of Michigan Medical School, 1150 West Medical Center Drive, M7300 Med Sci I, SPC 5625, Ann Arbor, MI 48109-5625; jordankm@med.umich.edu
1. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507-520.
2. The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329:977-986.
3. King P, Peacock I, Donnelly R. The UK Prospective Diabetes Study (UKPDS): clinical and therapeutic implications for type 2 diabetes. Br J Clin Pharmacol. 1999;48:643-648.
4. Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359:1577-1589.
5. Gerstein HC, Miller ME, Byington RP, et al; Action to Con- trol Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358:2545-2559.
6. Ismail-Beigi F, Craven T, Banerji MA, et al; ACCORD Trial Group. Effect of intensive treatment of hyperglycaemia on microvascular outcomes in type 2 diabetes: an analysis of the ACCORD randomised trial. Lancet. 2010;376:419-430.
7. Gerstein HC, Miller ME, Genuth S, et al; ACCORD Study Group. Long-term effects of intensive glucose lowering on cardiovascular outcomes. N Engl J Med. 2011;364:818-828.
8. Bonds DE, Miller ME, Bergenstal RM, et al. The association between symptomatic, severe hypoglycaemia and mortality in type 2 diabetes: retrospective epidemiological analysis of the ACCORD study. BMJ. 2010;340:b4909.
9. Duckworth W, Abraira C, Moritz T, et al; VADT Investigators. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360:129-139.
10. Patel A, MacMahon S, Chalmers J, et al; ADVANCE Collab- orative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358:2560-2572.
11. American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care. 2013;36(suppl 1):S11-S66.
12. International Diabetes Foundation Clinical Guidelines Task Force. Global Guideline for Type 2 Diabetes. International Diabetes Federation. Brussels, Belgium; 2012.
13. Handelsman Y, Mechanick JI, Blonde L, et al; AACE Task Force for Developing Diabetes Comprehensive Care Plan. Ameri- can Association of Clinical Endocrinologists Medical Guidelines for clinical practice for developing a diabetes mellitus comprehensive care plan: executive summary. Endocr Pract. 2011;17(suppl 2):S1-S53
14. Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
15. UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ. 1998;317:703-713.
16. Adler AI, Stratton IM, Neil HA, et al. Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational study. BMJ. 2000;321:412-419.
17. Cushman WC, Evans GW, Byington RP, et al; ACCORD Study Group. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362:1575-1585.
18. Cooper-DeHoff RM, Gong Y, Handberg EM, et al. Tight blood pressure control and cardiovascular outcomes among hypertensive patients with diabetes and coronary artery disease. JAMA. 2010;304:61-68.
19. Pyörälä K, Pedersen TR, Kjekshus J, et al. Cholesterol lowering with simvastatin improves prognosis of diabetic patients with coronary heart disease. A subgroup analysis of the Scandinavian Simvastatin Survival Study (4S). Diabetes Care. 1997;20:614-620.
20. Goldberg RB, Mellies MJ, Sacks FM, et al; The Care Investigators. Cardiovascular events and their reduction with pravastatin in diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels: subgroup analyses in the cholesterol and recurrent events (CARE) trial. The Care Investigators. Circulation. 1998;98:2513-2519.
21. Collins R, Armitage J, Parish S, et al; Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet. 2003;361:2005-2016.
22. Shepherd J, Barter P, Carmena R, et al. Effect of lowering LDL cholesterol substantially below currently recommended levels in patients with coronary heart disease and diabetes: the Treating to New Targets (TNT) study. Diabetes Care. 2006;29:1220-1226.
23. Sever PS, Poulter NR, Dahlöf B, et al. Reduction in cardiovascular events with atorvastatin in 2,532 patients with type 2 diabetes: Anglo-Scandinavian Cardiac Outcomes Trial—lipid-lowering arm (ASCOT-LLA). Diabetes Care. 2005;28:1151-1157.
24. Colhoun HM, Betteridge DJ, Durrington PN, et al; CARDS investigators. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomized placebo-controlled trial. Lancet. 2004;364:685-696.
25. Brunzell JD, Davidson M, Furberg CD, et al; American Diabetes Association; American College of Cardiology Foundation. Lipoprotein management in patients with cardiometabolic risk: consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care. 2008;31:811-822.
26. Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2889-2934.
› Aim for a glycated hemoglobin of <7% for most nonpregnant patients with type 2 diabetes, with a less stringent target for those with severe hypoglycemia, limited life expectancy, advanced micro- or macrovascular complications, and/or extensive comorbidities. B
› Attempt to treat patients with diabetes and hypertension to a target blood pressure<140/90mm Hg. B
› Prescribe statin therapy regardless of baseline lipid levels for all patients
who have diabetes and are between the ages of 40 and 75years. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Dennis D, age 63, was recently diagnosed with diabetes. his glycated hemoglobin (HbA1c) is 7.8%, his blood pressure (BP) is mildly elevated (145/95 mm Hg), and his body mass index (BMI) is 28.5, but his low-density lipoprotein (LDL) cholesterol is 100 mg/dl, his high-density lipoprotein (HDL) cholesterol is 52 mg/dL, and he has no history of cardiovascular disease (CVD). After an unsuccessful attempt to treat him with lifestyle modification, it is time to initiate diabetes therapy.
Other than an alpha-blocker for benign prostatic hyperplasia and a prostaglandin for glaucoma, Mr. D takes no other medications. You prescribe metformin 500 mg twice daily and consider what else to add to keep his diabetes well controlled. Should you prescribe an antihypertensive? And, despite the patient’s normal lipid levels, should he begin taking a statin?
Type 2 diabetes has been extensively studied in rigorous randomized controlled trials (RCTs). While studies have provided ample evidence in support of optimal treatment, differing interpretations of the findings are reflected in consensus guidelines developed by expert panels that don’t always see eye to eye on what diabetes treatment targets should be and how best to prevent micro- and macrovascular complications.
What’s more, recommendations continue to be updated as new data emerge. In February 2014, the Joint Committee on Prevention, Evaluation, and Treatment of High Blood Pressure (JCN 8) revised its target for patients with diabetes to <140/90 mm Hg (from <130/80 mm Hg).1 This is likely to lead to revisions in other leading consensus guidelines, as well.
Thus, primary care physicians managing the care of patients with diabetes face the challenge of using the latest recommendations in a manner that addresses the entire clinical picture, considering each patient’s age and overall health status, priorities, and preferences. We developed this evidence-based review and guide- line summary with that in mind.
HbA1c target: How low should you go?
The Diabetes Control and Complications Trial (DCCT), published nearly 20 years ago, studied patients with type 1 diabetes, and found that intensive insulin therapy (HbA1c ≤6%) delayed the onset of retinopathy, nephropathy, and neuropathy.2 However, there was an important adverse effect of such intensive therapy: Patients in this group suffered from severe hypoglycemic episodes 3 times more frequently than those in the usual care group. Nonetheless, the microvascular benefits of intensive control observed in those with type 1 diabetes were thought to be similar for patients with type 2 diabetes.
The United Kingdom Prospective Diabetes Study (UKPDS), published in 1999, was the first major study to investigate targets for glucose control in patients with type 2 diabetes.3 Participants treated intensively (mean HbA1c goal, 7%) had a 25% reduction in microvascular complications, including the need for retinal photocoagulation, com- pared with those on standard control (mean HbA1c, 7.9%). There was also a nonsignificant trend toward a reduction in macrovascular complications in the intensive therapy group, but no difference in overall mortality rate.3
A 10-year follow-up of the UKPDS showed that while baseline differences in HbA1c between the 2 groups were lost by one year, reductions in microvascular complications continued to occur in the intensive treatment group.4 Reductions in myocardial infarction (MI) and death emerged over time, a possible legacy effect (ie, the result of intense treatment early in the course of the disease).
The Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial, published in 2008, studied patients at risk for CVD, defined by either a prior history of CVD or ≥2 other cardiovascular risk factors.5 Participants, all of whom had poorly controlled type 2 diabetes (mean HbA1c, 8.1%), were randomized to either intensive treatment (HbA1c goal, <6%) or standard therapy (HbA1c goal, 7%-7.9%). The study was discontinued after a mean follow-up of 3.5 years, when those in the intensive therapy group were found to have a higher mortality rate.5
The rate of nonfatal MI reported by the ACCORD trial was lower in the intensive therapy group, however, and participants in this group also had delayed onset of microalbuminuria.6 No differences were seen in serum creatinine concentrations, advanced nephropathy, diabetic eye complications, or nonfatal stroke. Five-year follow up confirmed an increased mortality rate in the intensive therapy group,7 the result of severe hypoglycemia.8
The Veterans Affairs Diabetes Trial (VADT) randomized patients with poorly controlled type 2 diabetes to intensive or standard therapy.9 At 6 months, the intensive therapy group’s HbA1c averaged 6.9%, compared with 8.4% for the standard therapy group. Except for a delay in the progression of albuminuria, no significant effects of intensive therapy were found: Rates of other microvascular complications, major cardiovascular events, and death were similar.9 It should be noted that the VADT involved fewer participants and shorter follow-up than the other trials cited (TABLE 1),3-10 which may have affected its findings.
The Action in Diabetes and Vascular Disease (ADVANCE) trial, which included participants with either a history of major CVD or ≥1 other CVD risk factors, compared an intensive control group (mean HbA1c, 6.5%) with a standard care group (mean HbA1c, 7.3%)—with mixed results.10 Microalbuminuria occurred less frequently in the intensive therapy group, but hypoglycemia and hospitalization increased. No reduction in death from any cause, in cardiovascular death, or in major macrovascular events was found.
How to proceed? What the experts recommend
In updated standards for the medical care of diabetes released in January 2013,11 the American Diabetes Association (ADA) calls for an HbA1c goal <7% for most nonpregnant adults with type 2 diabetes. This is in line with the 2012 International Diabetes Federation (IDF) guideline.12
The 2011 guideline from the American Association of Clinical Endocrinologists (AACE),13 however, recommends tighter control—an HbA1c of ≤6.5% for most patients. For patients with diabetes of short duration, a long life expectancy, and no significant history of CVD, the AACE believes that this more aggressive goal has the potential to further reduce the risk of microvascular complications.
A less stringent target (eg, <8%) may be more appropriate for patients with a higher risk of adverse effects. That would apply to those with a history of severe hypoglycemia, a limited life expectancy, advanced micro- or macrovascular complications, or extensive comorbid conditions, as well as to any patient for whom stricter control is difficult to attain even with intensive therapy.13
Setting a BP target
In 2003, the 7th report of the Joint Committee on Prevention, Evaluation, and Treatment of High Blood Pressure (JCN 7) recommended a target BP <130/80 mm Hg for diabetes patients.14 Most major diabetes guidelines, including those of the AACE13 and IDF,12 echoed this recommendation. As noted earlier, JNC 8, published earlier this year, loosened the recommendation to <140/90 mm Hg.1 Although evidence has shown that treatment to a systolic BP <150 mm Hg improves cardiovascular and cerebrovascular outcomes for patients with diabetes,15 no RCTs have addressed whether more intensive treatment to achieve a systolic BP <140 mm Hg provides further benefit.
The BP of participants in the UKPDS has been examined, with patients with tighter control (<150/85 mm Hg) compared with those with less stringent control (<180/105 mm Hg). The tight control group showed a significant reduction in both death and complications related to diabetes, progression of diabetic retinopathy, and deterioration in visual acuity.15 Further investigation found that each 10 mm Hg reduction in systolic pressure was associated with a risk reduction of 15% for death related to diabetes, 12% for diabetes-related complications, 11% for MI, and 13% for microvascular complications.16
The ACCORD trial randomized participants to more intensive control (systolic BP <120 mm Hg, with a mean of 119.3) or standard therapy (systolic BP <140 mm Hg, mean 133.).17 After 4.7 years, no difference was found in the rates of MI, stroke, or death. However, a significant increase in the rate of serious adverse effects from antihypertensive treatment (including hypotension, syncope, bradycardia, hypokalemia, angioedema, and renal failure) occurred in the intensive control group.17
A subgroup analysis of patients with type 2 diabetes enrolled in the International Verapamil SR-Trandolapril Study (INVEST) evaluated systolic BP control and cardiovascular outcomes in those with preexisting coronary artery disease.18 Participants were categorized as having tight control if their systolic BP <130 mm Hg; usual control, if systolic pressure was between 130 and <140 mm Hg; and uncontrolled, if systolic BP ≥140 mm Hg. Those in the usual control group had lower risks of death, nonfatal MI, and stroke compared with those in the uncontrolled group, but little difference was found between patients in the usual control and tight control groups. The studies are summarized in TABLE 2.15-18
Interpreting the results: The experts disagree
The ADA recommends that patients with diabetes and hypertension be treated to a goal <140 mm Hg systolic and <80 mm Hg diastolic pressure11—more lenient than the recommendations of either the AACE or the IDF. It is not clear whether these recommendations will change, however, given the recent JNC 8 report.1 A lower systolic target may be appropriate for certain patients, if it can be achieved without undue adverse effects from antihypertensive medication. Older patients in particular may be at risk for orthostasis or falls as a result of more aggressive treatment.
CASE › Mr. D’s most recent BP is 145/95. Given that his goal is <140/90, you elect to start lisinopril 10 mg daily, advise him to monitor his BP at home, and refer him to a dietician to discuss the Dietary Approaches to Stop Hypertension diet.
Lipid levels: When to add statin therapy
Like glucose and BP control, lipid control and, concomitantly, the benefit of statin therapy for patients with type 2 diabetes has been studied extensively (TABLE 3).19-24
The Scandinavian Simvastatin Survival Study (4S) recruited participants with a history of MI or angina, and included a small diabetes subgroup.19 Participants were randomized to simvastatin 20 mg daily, with blinded titration up to 40 mg/d, or placebo. Among those with diabetes, patients on simvastatin had a 55% reduction in risk for major coronary heart disease events and a 43% reduction in total mortality. The risk reduction did not depend on baseline levels of total cholesterol, LDL cholesterol, HDL cholesterol, or triglycerides.
Cholesterol and Recurrent Events (CARE), which studied participants with a history of MI 3 to 20 months prior to the start of the study and also included a diabetes subgroup, had a similar outcome.20 Compared with placebo, treatment with pravastatin 40 mg/d reduced the risk of both coronary events and revascularization procedures by 25%.
The Heart Protection Study randomized patients with either diabetes or a history of occlusive arterial disease to receive simvastatin 40 mg daily or placebo.21 In the treatment group, the risk of major vascular events was reduced in patients with diabetes by 27%. Improvements were seen in patients with LDL cholesterol levels both above and below 116 mg/dL.
Multiple studies have evaluated the benefits of atorvastatin for patients with diabetes. All have demonstrated a significant reduction in the risk of MI and death in those on statin therapy. The Treating to New Targets study showed a 25% reduction in major cardiovascular events in those treated with 80 mg atorvastatin daily (mean LDL, 77 mg/dL) vs those treated with 10 mg of the drug (mean LDL, 86 mg/dL).22 The Anglo-Scandinavian Cardiac Outcomes Trial–Lipid-Lowering Arm (ASCOT-LLA)23 and the Collaborative Atorvastatin Diabetes Study (CARDS)24 were both terminated early due to the magnitude of benefit seen with statin therapy. In contrast to LDL, evidence for non-LDL treatment goals is lacking in the diabetes literature. Also, there is little evidence to support nonstatin cholesterol-lowering therapy for the management of diabetes patients.
Statin use is widely recommended
In 2008, the ADA and the American College of Cardiology Foundation (ACCF) produced a joint consensus statement regarding lipoprotein management for patients with diabetes and multiple CVD risk factors.25 Target LDL was recommended at <100 mg/dL for moderately high-risk primary prevention patients, including those with diabetes. For patients with diabetes and ≥1 other risk factors, the ADA/ACCF recommended an LDL goal <70 mg/dL. The 2011 AACE guideline has the same treatment goals,13 while the 2012 IDF guidelines are more aggressive.12 For primary prevention, the AACE endorses an LDL goal <80 mg/dL, and <70 mg/dL for those with known CVD.13
The updated standards released by the ADA in January 2013 recommend statin therapy regardless of LDL level for patients who have diabetes and known CVD, as well as for those ages 40 years and older who do not have CVD but have ≥1 other risk factors. Specific risk factors include hypertension, dyslipidemia, albuminuria, and a family history of CVD.11
The latest statin guideline. In November 2013, the American College of Cardiology and American Heart Association (ACC/AHA) published a new guideline for the treatment of cholesterol to reduce cardiovascular risk,26 but said nothing for or against specific LDL or non-HDL cholesterol targets. The ACC/AHA recommends that all patients who have diabetes and are between the ages of 40 and 75 years be treated with a moderate dose of a statin—a target supported with strong (strength of recommendation: A) evidence.
Patients with diabetes and an estimated 10-year risk of CVD >7.5% should be considered for high-intensity statin therapy, according to the ACC/AHA.26 For patients younger than 40 or older than 75, the decision to initiate statin therapy should be made by weighing the potential cardiovascular benefits, the risk of adverse effects, and the potential for drug-drug-interactions, as well as patient preference.
CASE › You discuss the need for moderate-dose statin therapy with Mr. D. He is hesitant at first, referring to a coworker who had “leg cramps” when he was taking a statin. You emphasize the importance of prevention in the care of his diabetes and convince the patient to begin a trial of atorvastatin 40 mg daily.
You warn Mr. D of the possibility of an allergic reaction, rash, or cough from lisinopril and loose stools from metformin, and advise him to call if he develops muscle cramps that could be associated with the statin. Finally, you stress the importance of lifestyle modification, including diet and weight loss, and schedule a follow-up visit in 3 months.
At Mr. D’s next visit, you will check his HbA1c and BP. If his HbA1c is still >7.0%, you may increase the dose of metformin or add a sulfonylurea. The dose of lisinopril could be increased if the patient’s BP continues to be elevated. There will be no need to recheck Mr. D’s cholesterol levels, however, because the purpose of the statin therapy is to improve overall outcomes, rather than to achieve a target goal.
CORRESPONDENCE
Kathryn M. Harmes, MD, Department of Family Medicine, University of Michigan Medical School, 1150 West Medical Center Drive, M7300 Med Sci I, SPC 5625, Ann Arbor, MI 48109-5625; jordankm@med.umich.edu
› Aim for a glycated hemoglobin of <7% for most nonpregnant patients with type 2 diabetes, with a less stringent target for those with severe hypoglycemia, limited life expectancy, advanced micro- or macrovascular complications, and/or extensive comorbidities. B
› Attempt to treat patients with diabetes and hypertension to a target blood pressure<140/90mm Hg. B
› Prescribe statin therapy regardless of baseline lipid levels for all patients
who have diabetes and are between the ages of 40 and 75years. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Dennis D, age 63, was recently diagnosed with diabetes. his glycated hemoglobin (HbA1c) is 7.8%, his blood pressure (BP) is mildly elevated (145/95 mm Hg), and his body mass index (BMI) is 28.5, but his low-density lipoprotein (LDL) cholesterol is 100 mg/dl, his high-density lipoprotein (HDL) cholesterol is 52 mg/dL, and he has no history of cardiovascular disease (CVD). After an unsuccessful attempt to treat him with lifestyle modification, it is time to initiate diabetes therapy.
Other than an alpha-blocker for benign prostatic hyperplasia and a prostaglandin for glaucoma, Mr. D takes no other medications. You prescribe metformin 500 mg twice daily and consider what else to add to keep his diabetes well controlled. Should you prescribe an antihypertensive? And, despite the patient’s normal lipid levels, should he begin taking a statin?
Type 2 diabetes has been extensively studied in rigorous randomized controlled trials (RCTs). While studies have provided ample evidence in support of optimal treatment, differing interpretations of the findings are reflected in consensus guidelines developed by expert panels that don’t always see eye to eye on what diabetes treatment targets should be and how best to prevent micro- and macrovascular complications.
What’s more, recommendations continue to be updated as new data emerge. In February 2014, the Joint Committee on Prevention, Evaluation, and Treatment of High Blood Pressure (JCN 8) revised its target for patients with diabetes to <140/90 mm Hg (from <130/80 mm Hg).1 This is likely to lead to revisions in other leading consensus guidelines, as well.
Thus, primary care physicians managing the care of patients with diabetes face the challenge of using the latest recommendations in a manner that addresses the entire clinical picture, considering each patient’s age and overall health status, priorities, and preferences. We developed this evidence-based review and guide- line summary with that in mind.
HbA1c target: How low should you go?
The Diabetes Control and Complications Trial (DCCT), published nearly 20 years ago, studied patients with type 1 diabetes, and found that intensive insulin therapy (HbA1c ≤6%) delayed the onset of retinopathy, nephropathy, and neuropathy.2 However, there was an important adverse effect of such intensive therapy: Patients in this group suffered from severe hypoglycemic episodes 3 times more frequently than those in the usual care group. Nonetheless, the microvascular benefits of intensive control observed in those with type 1 diabetes were thought to be similar for patients with type 2 diabetes.
The United Kingdom Prospective Diabetes Study (UKPDS), published in 1999, was the first major study to investigate targets for glucose control in patients with type 2 diabetes.3 Participants treated intensively (mean HbA1c goal, 7%) had a 25% reduction in microvascular complications, including the need for retinal photocoagulation, com- pared with those on standard control (mean HbA1c, 7.9%). There was also a nonsignificant trend toward a reduction in macrovascular complications in the intensive therapy group, but no difference in overall mortality rate.3
A 10-year follow-up of the UKPDS showed that while baseline differences in HbA1c between the 2 groups were lost by one year, reductions in microvascular complications continued to occur in the intensive treatment group.4 Reductions in myocardial infarction (MI) and death emerged over time, a possible legacy effect (ie, the result of intense treatment early in the course of the disease).
The Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial, published in 2008, studied patients at risk for CVD, defined by either a prior history of CVD or ≥2 other cardiovascular risk factors.5 Participants, all of whom had poorly controlled type 2 diabetes (mean HbA1c, 8.1%), were randomized to either intensive treatment (HbA1c goal, <6%) or standard therapy (HbA1c goal, 7%-7.9%). The study was discontinued after a mean follow-up of 3.5 years, when those in the intensive therapy group were found to have a higher mortality rate.5
The rate of nonfatal MI reported by the ACCORD trial was lower in the intensive therapy group, however, and participants in this group also had delayed onset of microalbuminuria.6 No differences were seen in serum creatinine concentrations, advanced nephropathy, diabetic eye complications, or nonfatal stroke. Five-year follow up confirmed an increased mortality rate in the intensive therapy group,7 the result of severe hypoglycemia.8
The Veterans Affairs Diabetes Trial (VADT) randomized patients with poorly controlled type 2 diabetes to intensive or standard therapy.9 At 6 months, the intensive therapy group’s HbA1c averaged 6.9%, compared with 8.4% for the standard therapy group. Except for a delay in the progression of albuminuria, no significant effects of intensive therapy were found: Rates of other microvascular complications, major cardiovascular events, and death were similar.9 It should be noted that the VADT involved fewer participants and shorter follow-up than the other trials cited (TABLE 1),3-10 which may have affected its findings.
The Action in Diabetes and Vascular Disease (ADVANCE) trial, which included participants with either a history of major CVD or ≥1 other CVD risk factors, compared an intensive control group (mean HbA1c, 6.5%) with a standard care group (mean HbA1c, 7.3%)—with mixed results.10 Microalbuminuria occurred less frequently in the intensive therapy group, but hypoglycemia and hospitalization increased. No reduction in death from any cause, in cardiovascular death, or in major macrovascular events was found.
How to proceed? What the experts recommend
In updated standards for the medical care of diabetes released in January 2013,11 the American Diabetes Association (ADA) calls for an HbA1c goal <7% for most nonpregnant adults with type 2 diabetes. This is in line with the 2012 International Diabetes Federation (IDF) guideline.12
The 2011 guideline from the American Association of Clinical Endocrinologists (AACE),13 however, recommends tighter control—an HbA1c of ≤6.5% for most patients. For patients with diabetes of short duration, a long life expectancy, and no significant history of CVD, the AACE believes that this more aggressive goal has the potential to further reduce the risk of microvascular complications.
A less stringent target (eg, <8%) may be more appropriate for patients with a higher risk of adverse effects. That would apply to those with a history of severe hypoglycemia, a limited life expectancy, advanced micro- or macrovascular complications, or extensive comorbid conditions, as well as to any patient for whom stricter control is difficult to attain even with intensive therapy.13
Setting a BP target
In 2003, the 7th report of the Joint Committee on Prevention, Evaluation, and Treatment of High Blood Pressure (JCN 7) recommended a target BP <130/80 mm Hg for diabetes patients.14 Most major diabetes guidelines, including those of the AACE13 and IDF,12 echoed this recommendation. As noted earlier, JNC 8, published earlier this year, loosened the recommendation to <140/90 mm Hg.1 Although evidence has shown that treatment to a systolic BP <150 mm Hg improves cardiovascular and cerebrovascular outcomes for patients with diabetes,15 no RCTs have addressed whether more intensive treatment to achieve a systolic BP <140 mm Hg provides further benefit.
The BP of participants in the UKPDS has been examined, with patients with tighter control (<150/85 mm Hg) compared with those with less stringent control (<180/105 mm Hg). The tight control group showed a significant reduction in both death and complications related to diabetes, progression of diabetic retinopathy, and deterioration in visual acuity.15 Further investigation found that each 10 mm Hg reduction in systolic pressure was associated with a risk reduction of 15% for death related to diabetes, 12% for diabetes-related complications, 11% for MI, and 13% for microvascular complications.16
The ACCORD trial randomized participants to more intensive control (systolic BP <120 mm Hg, with a mean of 119.3) or standard therapy (systolic BP <140 mm Hg, mean 133.).17 After 4.7 years, no difference was found in the rates of MI, stroke, or death. However, a significant increase in the rate of serious adverse effects from antihypertensive treatment (including hypotension, syncope, bradycardia, hypokalemia, angioedema, and renal failure) occurred in the intensive control group.17
A subgroup analysis of patients with type 2 diabetes enrolled in the International Verapamil SR-Trandolapril Study (INVEST) evaluated systolic BP control and cardiovascular outcomes in those with preexisting coronary artery disease.18 Participants were categorized as having tight control if their systolic BP <130 mm Hg; usual control, if systolic pressure was between 130 and <140 mm Hg; and uncontrolled, if systolic BP ≥140 mm Hg. Those in the usual control group had lower risks of death, nonfatal MI, and stroke compared with those in the uncontrolled group, but little difference was found between patients in the usual control and tight control groups. The studies are summarized in TABLE 2.15-18
Interpreting the results: The experts disagree
The ADA recommends that patients with diabetes and hypertension be treated to a goal <140 mm Hg systolic and <80 mm Hg diastolic pressure11—more lenient than the recommendations of either the AACE or the IDF. It is not clear whether these recommendations will change, however, given the recent JNC 8 report.1 A lower systolic target may be appropriate for certain patients, if it can be achieved without undue adverse effects from antihypertensive medication. Older patients in particular may be at risk for orthostasis or falls as a result of more aggressive treatment.
CASE › Mr. D’s most recent BP is 145/95. Given that his goal is <140/90, you elect to start lisinopril 10 mg daily, advise him to monitor his BP at home, and refer him to a dietician to discuss the Dietary Approaches to Stop Hypertension diet.
Lipid levels: When to add statin therapy
Like glucose and BP control, lipid control and, concomitantly, the benefit of statin therapy for patients with type 2 diabetes has been studied extensively (TABLE 3).19-24
The Scandinavian Simvastatin Survival Study (4S) recruited participants with a history of MI or angina, and included a small diabetes subgroup.19 Participants were randomized to simvastatin 20 mg daily, with blinded titration up to 40 mg/d, or placebo. Among those with diabetes, patients on simvastatin had a 55% reduction in risk for major coronary heart disease events and a 43% reduction in total mortality. The risk reduction did not depend on baseline levels of total cholesterol, LDL cholesterol, HDL cholesterol, or triglycerides.
Cholesterol and Recurrent Events (CARE), which studied participants with a history of MI 3 to 20 months prior to the start of the study and also included a diabetes subgroup, had a similar outcome.20 Compared with placebo, treatment with pravastatin 40 mg/d reduced the risk of both coronary events and revascularization procedures by 25%.
The Heart Protection Study randomized patients with either diabetes or a history of occlusive arterial disease to receive simvastatin 40 mg daily or placebo.21 In the treatment group, the risk of major vascular events was reduced in patients with diabetes by 27%. Improvements were seen in patients with LDL cholesterol levels both above and below 116 mg/dL.
Multiple studies have evaluated the benefits of atorvastatin for patients with diabetes. All have demonstrated a significant reduction in the risk of MI and death in those on statin therapy. The Treating to New Targets study showed a 25% reduction in major cardiovascular events in those treated with 80 mg atorvastatin daily (mean LDL, 77 mg/dL) vs those treated with 10 mg of the drug (mean LDL, 86 mg/dL).22 The Anglo-Scandinavian Cardiac Outcomes Trial–Lipid-Lowering Arm (ASCOT-LLA)23 and the Collaborative Atorvastatin Diabetes Study (CARDS)24 were both terminated early due to the magnitude of benefit seen with statin therapy. In contrast to LDL, evidence for non-LDL treatment goals is lacking in the diabetes literature. Also, there is little evidence to support nonstatin cholesterol-lowering therapy for the management of diabetes patients.
Statin use is widely recommended
In 2008, the ADA and the American College of Cardiology Foundation (ACCF) produced a joint consensus statement regarding lipoprotein management for patients with diabetes and multiple CVD risk factors.25 Target LDL was recommended at <100 mg/dL for moderately high-risk primary prevention patients, including those with diabetes. For patients with diabetes and ≥1 other risk factors, the ADA/ACCF recommended an LDL goal <70 mg/dL. The 2011 AACE guideline has the same treatment goals,13 while the 2012 IDF guidelines are more aggressive.12 For primary prevention, the AACE endorses an LDL goal <80 mg/dL, and <70 mg/dL for those with known CVD.13
The updated standards released by the ADA in January 2013 recommend statin therapy regardless of LDL level for patients who have diabetes and known CVD, as well as for those ages 40 years and older who do not have CVD but have ≥1 other risk factors. Specific risk factors include hypertension, dyslipidemia, albuminuria, and a family history of CVD.11
The latest statin guideline. In November 2013, the American College of Cardiology and American Heart Association (ACC/AHA) published a new guideline for the treatment of cholesterol to reduce cardiovascular risk,26 but said nothing for or against specific LDL or non-HDL cholesterol targets. The ACC/AHA recommends that all patients who have diabetes and are between the ages of 40 and 75 years be treated with a moderate dose of a statin—a target supported with strong (strength of recommendation: A) evidence.
Patients with diabetes and an estimated 10-year risk of CVD >7.5% should be considered for high-intensity statin therapy, according to the ACC/AHA.26 For patients younger than 40 or older than 75, the decision to initiate statin therapy should be made by weighing the potential cardiovascular benefits, the risk of adverse effects, and the potential for drug-drug-interactions, as well as patient preference.
CASE › You discuss the need for moderate-dose statin therapy with Mr. D. He is hesitant at first, referring to a coworker who had “leg cramps” when he was taking a statin. You emphasize the importance of prevention in the care of his diabetes and convince the patient to begin a trial of atorvastatin 40 mg daily.
You warn Mr. D of the possibility of an allergic reaction, rash, or cough from lisinopril and loose stools from metformin, and advise him to call if he develops muscle cramps that could be associated with the statin. Finally, you stress the importance of lifestyle modification, including diet and weight loss, and schedule a follow-up visit in 3 months.
At Mr. D’s next visit, you will check his HbA1c and BP. If his HbA1c is still >7.0%, you may increase the dose of metformin or add a sulfonylurea. The dose of lisinopril could be increased if the patient’s BP continues to be elevated. There will be no need to recheck Mr. D’s cholesterol levels, however, because the purpose of the statin therapy is to improve overall outcomes, rather than to achieve a target goal.
CORRESPONDENCE
Kathryn M. Harmes, MD, Department of Family Medicine, University of Michigan Medical School, 1150 West Medical Center Drive, M7300 Med Sci I, SPC 5625, Ann Arbor, MI 48109-5625; jordankm@med.umich.edu
1. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507-520.
2. The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329:977-986.
3. King P, Peacock I, Donnelly R. The UK Prospective Diabetes Study (UKPDS): clinical and therapeutic implications for type 2 diabetes. Br J Clin Pharmacol. 1999;48:643-648.
4. Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359:1577-1589.
5. Gerstein HC, Miller ME, Byington RP, et al; Action to Con- trol Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358:2545-2559.
6. Ismail-Beigi F, Craven T, Banerji MA, et al; ACCORD Trial Group. Effect of intensive treatment of hyperglycaemia on microvascular outcomes in type 2 diabetes: an analysis of the ACCORD randomised trial. Lancet. 2010;376:419-430.
7. Gerstein HC, Miller ME, Genuth S, et al; ACCORD Study Group. Long-term effects of intensive glucose lowering on cardiovascular outcomes. N Engl J Med. 2011;364:818-828.
8. Bonds DE, Miller ME, Bergenstal RM, et al. The association between symptomatic, severe hypoglycaemia and mortality in type 2 diabetes: retrospective epidemiological analysis of the ACCORD study. BMJ. 2010;340:b4909.
9. Duckworth W, Abraira C, Moritz T, et al; VADT Investigators. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360:129-139.
10. Patel A, MacMahon S, Chalmers J, et al; ADVANCE Collab- orative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358:2560-2572.
11. American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care. 2013;36(suppl 1):S11-S66.
12. International Diabetes Foundation Clinical Guidelines Task Force. Global Guideline for Type 2 Diabetes. International Diabetes Federation. Brussels, Belgium; 2012.
13. Handelsman Y, Mechanick JI, Blonde L, et al; AACE Task Force for Developing Diabetes Comprehensive Care Plan. Ameri- can Association of Clinical Endocrinologists Medical Guidelines for clinical practice for developing a diabetes mellitus comprehensive care plan: executive summary. Endocr Pract. 2011;17(suppl 2):S1-S53
14. Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
15. UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ. 1998;317:703-713.
16. Adler AI, Stratton IM, Neil HA, et al. Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational study. BMJ. 2000;321:412-419.
17. Cushman WC, Evans GW, Byington RP, et al; ACCORD Study Group. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362:1575-1585.
18. Cooper-DeHoff RM, Gong Y, Handberg EM, et al. Tight blood pressure control and cardiovascular outcomes among hypertensive patients with diabetes and coronary artery disease. JAMA. 2010;304:61-68.
19. Pyörälä K, Pedersen TR, Kjekshus J, et al. Cholesterol lowering with simvastatin improves prognosis of diabetic patients with coronary heart disease. A subgroup analysis of the Scandinavian Simvastatin Survival Study (4S). Diabetes Care. 1997;20:614-620.
20. Goldberg RB, Mellies MJ, Sacks FM, et al; The Care Investigators. Cardiovascular events and their reduction with pravastatin in diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels: subgroup analyses in the cholesterol and recurrent events (CARE) trial. The Care Investigators. Circulation. 1998;98:2513-2519.
21. Collins R, Armitage J, Parish S, et al; Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet. 2003;361:2005-2016.
22. Shepherd J, Barter P, Carmena R, et al. Effect of lowering LDL cholesterol substantially below currently recommended levels in patients with coronary heart disease and diabetes: the Treating to New Targets (TNT) study. Diabetes Care. 2006;29:1220-1226.
23. Sever PS, Poulter NR, Dahlöf B, et al. Reduction in cardiovascular events with atorvastatin in 2,532 patients with type 2 diabetes: Anglo-Scandinavian Cardiac Outcomes Trial—lipid-lowering arm (ASCOT-LLA). Diabetes Care. 2005;28:1151-1157.
24. Colhoun HM, Betteridge DJ, Durrington PN, et al; CARDS investigators. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomized placebo-controlled trial. Lancet. 2004;364:685-696.
25. Brunzell JD, Davidson M, Furberg CD, et al; American Diabetes Association; American College of Cardiology Foundation. Lipoprotein management in patients with cardiometabolic risk: consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care. 2008;31:811-822.
26. Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2889-2934.
1. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507-520.
2. The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993;329:977-986.
3. King P, Peacock I, Donnelly R. The UK Prospective Diabetes Study (UKPDS): clinical and therapeutic implications for type 2 diabetes. Br J Clin Pharmacol. 1999;48:643-648.
4. Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359:1577-1589.
5. Gerstein HC, Miller ME, Byington RP, et al; Action to Con- trol Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358:2545-2559.
6. Ismail-Beigi F, Craven T, Banerji MA, et al; ACCORD Trial Group. Effect of intensive treatment of hyperglycaemia on microvascular outcomes in type 2 diabetes: an analysis of the ACCORD randomised trial. Lancet. 2010;376:419-430.
7. Gerstein HC, Miller ME, Genuth S, et al; ACCORD Study Group. Long-term effects of intensive glucose lowering on cardiovascular outcomes. N Engl J Med. 2011;364:818-828.
8. Bonds DE, Miller ME, Bergenstal RM, et al. The association between symptomatic, severe hypoglycaemia and mortality in type 2 diabetes: retrospective epidemiological analysis of the ACCORD study. BMJ. 2010;340:b4909.
9. Duckworth W, Abraira C, Moritz T, et al; VADT Investigators. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360:129-139.
10. Patel A, MacMahon S, Chalmers J, et al; ADVANCE Collab- orative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358:2560-2572.
11. American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care. 2013;36(suppl 1):S11-S66.
12. International Diabetes Foundation Clinical Guidelines Task Force. Global Guideline for Type 2 Diabetes. International Diabetes Federation. Brussels, Belgium; 2012.
13. Handelsman Y, Mechanick JI, Blonde L, et al; AACE Task Force for Developing Diabetes Comprehensive Care Plan. Ameri- can Association of Clinical Endocrinologists Medical Guidelines for clinical practice for developing a diabetes mellitus comprehensive care plan: executive summary. Endocr Pract. 2011;17(suppl 2):S1-S53
14. Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
15. UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ. 1998;317:703-713.
16. Adler AI, Stratton IM, Neil HA, et al. Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational study. BMJ. 2000;321:412-419.
17. Cushman WC, Evans GW, Byington RP, et al; ACCORD Study Group. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362:1575-1585.
18. Cooper-DeHoff RM, Gong Y, Handberg EM, et al. Tight blood pressure control and cardiovascular outcomes among hypertensive patients with diabetes and coronary artery disease. JAMA. 2010;304:61-68.
19. Pyörälä K, Pedersen TR, Kjekshus J, et al. Cholesterol lowering with simvastatin improves prognosis of diabetic patients with coronary heart disease. A subgroup analysis of the Scandinavian Simvastatin Survival Study (4S). Diabetes Care. 1997;20:614-620.
20. Goldberg RB, Mellies MJ, Sacks FM, et al; The Care Investigators. Cardiovascular events and their reduction with pravastatin in diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels: subgroup analyses in the cholesterol and recurrent events (CARE) trial. The Care Investigators. Circulation. 1998;98:2513-2519.
21. Collins R, Armitage J, Parish S, et al; Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: a randomised placebo-controlled trial. Lancet. 2003;361:2005-2016.
22. Shepherd J, Barter P, Carmena R, et al. Effect of lowering LDL cholesterol substantially below currently recommended levels in patients with coronary heart disease and diabetes: the Treating to New Targets (TNT) study. Diabetes Care. 2006;29:1220-1226.
23. Sever PS, Poulter NR, Dahlöf B, et al. Reduction in cardiovascular events with atorvastatin in 2,532 patients with type 2 diabetes: Anglo-Scandinavian Cardiac Outcomes Trial—lipid-lowering arm (ASCOT-LLA). Diabetes Care. 2005;28:1151-1157.
24. Colhoun HM, Betteridge DJ, Durrington PN, et al; CARDS investigators. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomized placebo-controlled trial. Lancet. 2004;364:685-696.
25. Brunzell JD, Davidson M, Furberg CD, et al; American Diabetes Association; American College of Cardiology Foundation. Lipoprotein management in patients with cardiometabolic risk: consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care. 2008;31:811-822.
26. Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2889-2934.