User login

More questions than answers?
The data presented by Wright and colleagues on the prevalence of underlying cancer in women who undergo myomectomy is disturbing and thought-provoking.
Are those in the 50-and-older age group who undergo myomectomy different from their same-aged peers with fibroids who do not undergo myomectomy? If so, why? If not, then with a 1 in 154 to 1 in 31 risk of occult malignancy, should not all women 50 years and older with fibroids undergo hysterectomy for this occult risk? This certainly has not been the standard of care for women 50 and older with asymptomatic fibroids. Thoughts?
In conclusion, it appears that power morcellation, or should I say the morcellation issue, has brought forth more questions than answers.
Richard L. Myers, MD
Jacksonville, Florida
Dr. Barbieri responds
I agree with Dr. Myers: Women aged 50 and older who have fibroids and undergo myomectomy must be clinically different than women of the same age who have fibroids but do not undergo myomectomy. It is likely that the women who undergo myomectomy have larger pelvic tumors or are more symptomatic than those who do not undergo myomectomy. I think this demonstrates that gynecologists are successfully identifying those women with a pelvic mass thought to be due to fibroids with the greatest risk of occult cancer and recommending that those women undergo surgery, while simultaneously recommending expectant management for those at lowest risk of an occult cancer.
“UPDATE ON MINIMALLY INVASIVE gynecologic SURGERY”
AMY L. GARCIA, MD (APRIL 2015)
Additional tips for in-office hysteroscopy
Thank you for the excellent coverage of hysteroscopy in the April issue. For me, patient trust is extremely important. Before I begin in-office hysteroscopy, I explain how the procedure is performed and answer all questions. I reassure the patient that, if it is too painful, I will stop and we will move to the operating room. I find music to be distracting to me as I am talking and constantly reassuring her.
In addition, I don’t perform the procedure when the patient is menstruating as it decreases visibility and I don’t want the intrauterine lidocaine to enter open vessels. It is helpful to perform this procedure shortly after menses and prior to ovulation to avoid instrumenting a pregnant uterus. Even if the menses is normal in timing and flow, a pregnancy test is still performed prior to the procedure. Doing it in this time period also can offer better visibility, as the endometrium is thinner.
I prescribe oral misoprostol the night before (400 mg, or 200 mg if she has undergone a cesarean delivery). The patient also is instructed to take ibuprofen 800 mg 1 hour prior to the procedure.
I continuously tell the patient what to expect. First, I perform a bimanual exam to determine the uterine position. Then local anesthesia placed on the anterior lip of the cervix prevents pain when placing the tenaculum. A paracervical block is performed and lidocaine jelly is placed in the cervix. Using an angiocatheter, I inject 4 mL of 2% lidocaine into the uterus and then wait 3 minutes.
It is important to only use the amount of fluid necessary to avoid overdistending the uterus. I take care to avoid touching the fundus, as this increases pain. I use a 4-mm 30˚ scope. I agree that the pain is dependent on physician expertise and procedure length.
If the cavity is clean, I perform a thorough endometrial biopsy that causes minimal pain because of the intrauterine lidocaine. I recently started doing in-office diagnostic hysteroscopy again. When I did it years ago without intrauterine lidocaine, it was unacceptably painful. I have performed 25 cases, all of which were successful, including on postmenopausal patients. All of the patients reported being highly satisfied and glad to have had the procedure performed in the office.
Ray Wertheim, MD
Fairfax, Virginia
Would you approve this candidate for uterus transplantation?
Instant Poll
Dr. Barbieri presented 3 cases to readers in his recent editorial on uterus transplantation and asked, “Would you approve or disapprove of transplantation of the uterus in these cases?”
- 23-year-old Army sergeant (G0) injured by improvised explosive device. To save her life, military surgeons removed her uterus, which had been lacerated in the explosion. She requested uterus transplantation to pursue a pregnancy. The Department of Defense has approved her request.
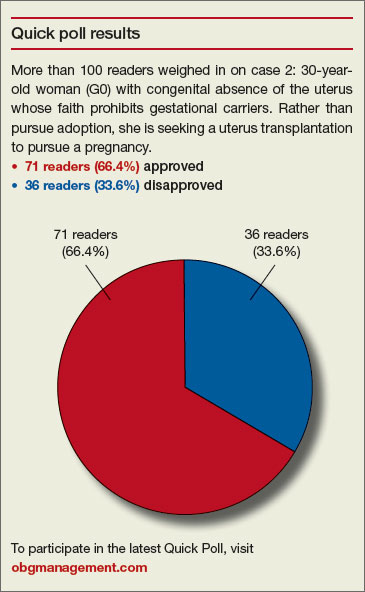
- 30-year-old woman (G0) with congenital absence of the uterus who is a devout member of a religious community in which the tenets of faith prohibit gestational carriers. Rather than pursue adoption, she is seeking a uterus transplantation to pursue a pregnancy.
- 35-year-old woman (G1P1) who had her uterus removed to treat cervical cancer. She has been disease-free for 3 years. She would like a uterus transplant to pursue a pregnancy.
READERS WEIGH IN:
Concentrate on saving lives
We should be concentrating our resources on saving lives rather than on satisfying the wishes of some very genuine people.
Where will it end? Let us not compare uterine transplant with kidney, heart, and lung transplants.
Ram A. Singh, MD
Oklahoma City, Oklahoma
No to 35-year-old patient
Assuming, as stated, that the women are healthy and psychosocially approved, to which I would add, they are fully informed on the preparation, medications, procedure, postoperative recovery, and potential complications,I would approve the first 2 cases and disapprove of the last. My reasoning for denying a uterus transplant to the 35-year-old woman is that, after she goes through the process of screening and evaluation, she will be an “elderly gravida,” which in itself has risks. I would also be concerned that all the family members fully understand the potential risks of her undertaking.
Helen T. Jackson, MD
Brookline, Massachusetts
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
More questions than answers?
The data presented by Wright and colleagues on the prevalence of underlying cancer in women who undergo myomectomy is disturbing and thought-provoking.
Are those in the 50-and-older age group who undergo myomectomy different from their same-aged peers with fibroids who do not undergo myomectomy? If so, why? If not, then with a 1 in 154 to 1 in 31 risk of occult malignancy, should not all women 50 years and older with fibroids undergo hysterectomy for this occult risk? This certainly has not been the standard of care for women 50 and older with asymptomatic fibroids. Thoughts?
In conclusion, it appears that power morcellation, or should I say the morcellation issue, has brought forth more questions than answers.
Richard L. Myers, MD
Jacksonville, Florida
Dr. Barbieri responds
I agree with Dr. Myers: Women aged 50 and older who have fibroids and undergo myomectomy must be clinically different than women of the same age who have fibroids but do not undergo myomectomy. It is likely that the women who undergo myomectomy have larger pelvic tumors or are more symptomatic than those who do not undergo myomectomy. I think this demonstrates that gynecologists are successfully identifying those women with a pelvic mass thought to be due to fibroids with the greatest risk of occult cancer and recommending that those women undergo surgery, while simultaneously recommending expectant management for those at lowest risk of an occult cancer.
“UPDATE ON MINIMALLY INVASIVE gynecologic SURGERY”
AMY L. GARCIA, MD (APRIL 2015)
Additional tips for in-office hysteroscopy
Thank you for the excellent coverage of hysteroscopy in the April issue. For me, patient trust is extremely important. Before I begin in-office hysteroscopy, I explain how the procedure is performed and answer all questions. I reassure the patient that, if it is too painful, I will stop and we will move to the operating room. I find music to be distracting to me as I am talking and constantly reassuring her.
In addition, I don’t perform the procedure when the patient is menstruating as it decreases visibility and I don’t want the intrauterine lidocaine to enter open vessels. It is helpful to perform this procedure shortly after menses and prior to ovulation to avoid instrumenting a pregnant uterus. Even if the menses is normal in timing and flow, a pregnancy test is still performed prior to the procedure. Doing it in this time period also can offer better visibility, as the endometrium is thinner.
I prescribe oral misoprostol the night before (400 mg, or 200 mg if she has undergone a cesarean delivery). The patient also is instructed to take ibuprofen 800 mg 1 hour prior to the procedure.
I continuously tell the patient what to expect. First, I perform a bimanual exam to determine the uterine position. Then local anesthesia placed on the anterior lip of the cervix prevents pain when placing the tenaculum. A paracervical block is performed and lidocaine jelly is placed in the cervix. Using an angiocatheter, I inject 4 mL of 2% lidocaine into the uterus and then wait 3 minutes.
It is important to only use the amount of fluid necessary to avoid overdistending the uterus. I take care to avoid touching the fundus, as this increases pain. I use a 4-mm 30˚ scope. I agree that the pain is dependent on physician expertise and procedure length.
If the cavity is clean, I perform a thorough endometrial biopsy that causes minimal pain because of the intrauterine lidocaine. I recently started doing in-office diagnostic hysteroscopy again. When I did it years ago without intrauterine lidocaine, it was unacceptably painful. I have performed 25 cases, all of which were successful, including on postmenopausal patients. All of the patients reported being highly satisfied and glad to have had the procedure performed in the office.
Ray Wertheim, MD
Fairfax, Virginia
Would you approve this candidate for uterus transplantation?
Instant Poll
Dr. Barbieri presented 3 cases to readers in his recent editorial on uterus transplantation and asked, “Would you approve or disapprove of transplantation of the uterus in these cases?”
- 23-year-old Army sergeant (G0) injured by improvised explosive device. To save her life, military surgeons removed her uterus, which had been lacerated in the explosion. She requested uterus transplantation to pursue a pregnancy. The Department of Defense has approved her request.
- 30-year-old woman (G0) with congenital absence of the uterus who is a devout member of a religious community in which the tenets of faith prohibit gestational carriers. Rather than pursue adoption, she is seeking a uterus transplantation to pursue a pregnancy.
- 35-year-old woman (G1P1) who had her uterus removed to treat cervical cancer. She has been disease-free for 3 years. She would like a uterus transplant to pursue a pregnancy.
READERS WEIGH IN:
Concentrate on saving lives
We should be concentrating our resources on saving lives rather than on satisfying the wishes of some very genuine people.
Where will it end? Let us not compare uterine transplant with kidney, heart, and lung transplants.
Ram A. Singh, MD
Oklahoma City, Oklahoma
No to 35-year-old patient
Assuming, as stated, that the women are healthy and psychosocially approved, to which I would add, they are fully informed on the preparation, medications, procedure, postoperative recovery, and potential complications,I would approve the first 2 cases and disapprove of the last. My reasoning for denying a uterus transplant to the 35-year-old woman is that, after she goes through the process of screening and evaluation, she will be an “elderly gravida,” which in itself has risks. I would also be concerned that all the family members fully understand the potential risks of her undertaking.
Helen T. Jackson, MD
Brookline, Massachusetts
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
More questions than answers?
The data presented by Wright and colleagues on the prevalence of underlying cancer in women who undergo myomectomy is disturbing and thought-provoking.
Are those in the 50-and-older age group who undergo myomectomy different from their same-aged peers with fibroids who do not undergo myomectomy? If so, why? If not, then with a 1 in 154 to 1 in 31 risk of occult malignancy, should not all women 50 years and older with fibroids undergo hysterectomy for this occult risk? This certainly has not been the standard of care for women 50 and older with asymptomatic fibroids. Thoughts?
In conclusion, it appears that power morcellation, or should I say the morcellation issue, has brought forth more questions than answers.
Richard L. Myers, MD
Jacksonville, Florida
Dr. Barbieri responds
I agree with Dr. Myers: Women aged 50 and older who have fibroids and undergo myomectomy must be clinically different than women of the same age who have fibroids but do not undergo myomectomy. It is likely that the women who undergo myomectomy have larger pelvic tumors or are more symptomatic than those who do not undergo myomectomy. I think this demonstrates that gynecologists are successfully identifying those women with a pelvic mass thought to be due to fibroids with the greatest risk of occult cancer and recommending that those women undergo surgery, while simultaneously recommending expectant management for those at lowest risk of an occult cancer.
“UPDATE ON MINIMALLY INVASIVE gynecologic SURGERY”
AMY L. GARCIA, MD (APRIL 2015)
Additional tips for in-office hysteroscopy
Thank you for the excellent coverage of hysteroscopy in the April issue. For me, patient trust is extremely important. Before I begin in-office hysteroscopy, I explain how the procedure is performed and answer all questions. I reassure the patient that, if it is too painful, I will stop and we will move to the operating room. I find music to be distracting to me as I am talking and constantly reassuring her.
In addition, I don’t perform the procedure when the patient is menstruating as it decreases visibility and I don’t want the intrauterine lidocaine to enter open vessels. It is helpful to perform this procedure shortly after menses and prior to ovulation to avoid instrumenting a pregnant uterus. Even if the menses is normal in timing and flow, a pregnancy test is still performed prior to the procedure. Doing it in this time period also can offer better visibility, as the endometrium is thinner.
I prescribe oral misoprostol the night before (400 mg, or 200 mg if she has undergone a cesarean delivery). The patient also is instructed to take ibuprofen 800 mg 1 hour prior to the procedure.
I continuously tell the patient what to expect. First, I perform a bimanual exam to determine the uterine position. Then local anesthesia placed on the anterior lip of the cervix prevents pain when placing the tenaculum. A paracervical block is performed and lidocaine jelly is placed in the cervix. Using an angiocatheter, I inject 4 mL of 2% lidocaine into the uterus and then wait 3 minutes.
It is important to only use the amount of fluid necessary to avoid overdistending the uterus. I take care to avoid touching the fundus, as this increases pain. I use a 4-mm 30˚ scope. I agree that the pain is dependent on physician expertise and procedure length.
If the cavity is clean, I perform a thorough endometrial biopsy that causes minimal pain because of the intrauterine lidocaine. I recently started doing in-office diagnostic hysteroscopy again. When I did it years ago without intrauterine lidocaine, it was unacceptably painful. I have performed 25 cases, all of which were successful, including on postmenopausal patients. All of the patients reported being highly satisfied and glad to have had the procedure performed in the office.
Ray Wertheim, MD
Fairfax, Virginia
Would you approve this candidate for uterus transplantation?
Instant Poll
Dr. Barbieri presented 3 cases to readers in his recent editorial on uterus transplantation and asked, “Would you approve or disapprove of transplantation of the uterus in these cases?”
- 23-year-old Army sergeant (G0) injured by improvised explosive device. To save her life, military surgeons removed her uterus, which had been lacerated in the explosion. She requested uterus transplantation to pursue a pregnancy. The Department of Defense has approved her request.
- 30-year-old woman (G0) with congenital absence of the uterus who is a devout member of a religious community in which the tenets of faith prohibit gestational carriers. Rather than pursue adoption, she is seeking a uterus transplantation to pursue a pregnancy.
- 35-year-old woman (G1P1) who had her uterus removed to treat cervical cancer. She has been disease-free for 3 years. She would like a uterus transplant to pursue a pregnancy.
READERS WEIGH IN:
Concentrate on saving lives
We should be concentrating our resources on saving lives rather than on satisfying the wishes of some very genuine people.
Where will it end? Let us not compare uterine transplant with kidney, heart, and lung transplants.
Ram A. Singh, MD
Oklahoma City, Oklahoma
No to 35-year-old patient
Assuming, as stated, that the women are healthy and psychosocially approved, to which I would add, they are fully informed on the preparation, medications, procedure, postoperative recovery, and potential complications,I would approve the first 2 cases and disapprove of the last. My reasoning for denying a uterus transplant to the 35-year-old woman is that, after she goes through the process of screening and evaluation, she will be an “elderly gravida,” which in itself has risks. I would also be concerned that all the family members fully understand the potential risks of her undertaking.
Helen T. Jackson, MD
Brookline, Massachusetts
Share your thoughts on this article! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.