User login
When it can be done safely, most people prefer to be treated and recover from illness at home.1,2 Home-based services have improved considerably since Brickner called the homebound aged “a medically unreached group.”3 Still, home care has not achieved its full potential and scientific investigation of home care models is scant compared with that of other therapeutic approaches.
The challenges of studying home care include variability in interventions, difficulty defining treatment and comparison groups, and high research costs. The care itself can be demanding, requiring providers to mobilize processes that have become institution-based and immobile, integrate care across insular settings, incorporate complex social issues into the care plan, and develop a viable home care financing model.
This article reviews evidence favoring investment in advanced home care and adds perspective from 3 decades’ experience at Virginia Commonwealth University (VCU), Richmond, Virginia.
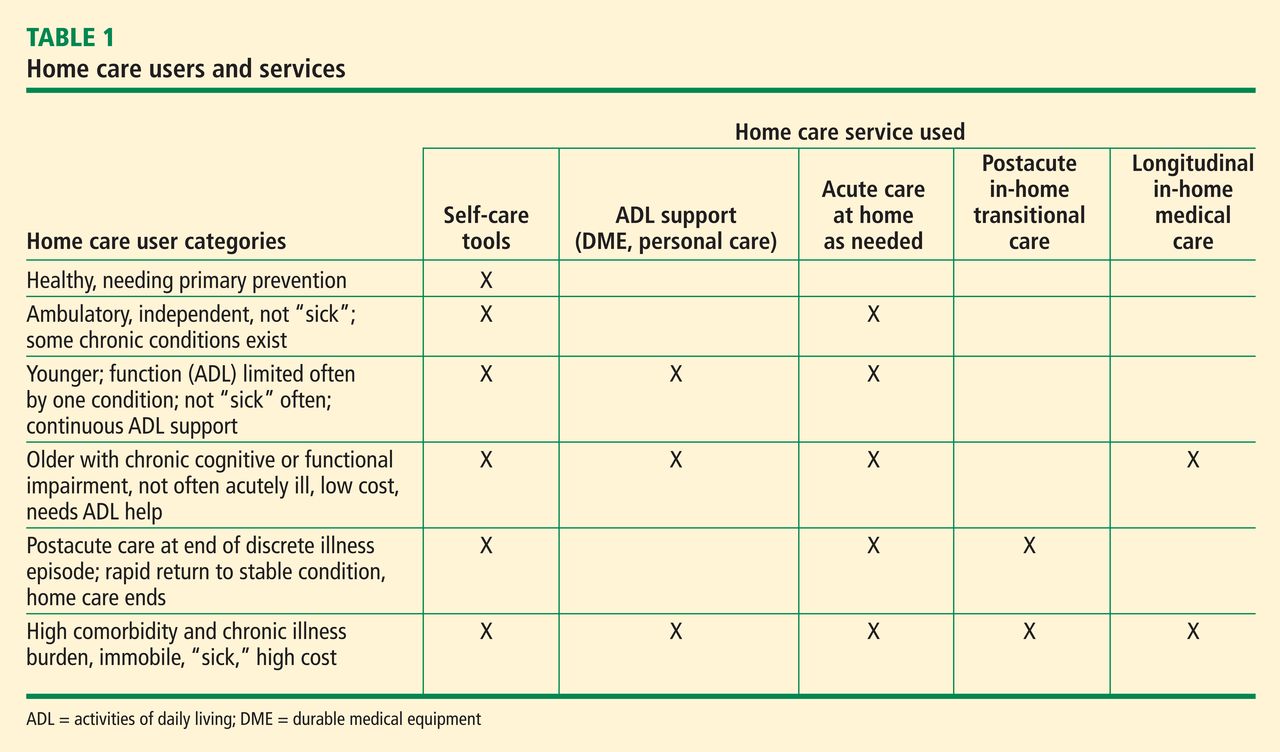
The term home care has a broad scope, ranging from basic support to highly technical care involving intravenous lines, ventilators, portable diagnostic tests, and remote monitors.4 Patients cared for at home range from those who are ambulatory to those who are permanently bedfast and seriously ill. The home care user population can be categorized based on the types of health care resources they consume (Table 1). Much attention has been paid to home-based care during recuperation after acute illness. The aim has been to foster recovery and prevent further need for institutional care. Lately the term transitional care has been used in this context.
TRANSITIONAL CARE
Transitional care has long been a priority for visiting nurse agencies. In 1965, Medicare Part A, building from the tradition of urban parish nursing services, created an interdisciplinary industry. Medicare now certifies more than 10,000 agencies with more than 250,000 professional staff.5 For several reasons, beginning in the 1970s, US physicians have become less integrated into in-home care. Despite this and the challenge of managing medically complex patients with minimal active physician involvement, home health agencies provide a vital service. Further, they have demonstrated improved outcomes and cost savings.
Transitional care refers to specialized, short-term care for selected high-risk patients after an acute illness. The original objective of transitional care was to reduce hospital readmissions. Tested models include an approach developed by Coleman et al,6 based on four pillars: assistance with medication self-management, patient-centered and -owned medical record, timely follow-up with primary or specialty care, and “red flags” that indicate a worsening condition. This model, which yielded one-third fewer hospital readmissions and a savings of about $500 per patient in 6 months, is being adopted in many locations nationally.
Naylor and colleagues7,8 collaborated with hospital-based nurse practitioners (NPs) for 2 decades on a more intensive model. In the Naylor model, the NPs form a health care bridge from hospital to home for 4 weeks after hospital care and add an active medical care component to the home care team. Naylor et al7 reported a 50% reduction in the rehospitalization rate and a cost savings of approximately $3,000 per patient over 24 weeks. Naylor’s team observed these results among frail, elderly patients with a variety of conditions and comorbidities. The 2010 federal health care reform law as well as state and private insurer initiatives now encourage use of this and other integrated care models.
In a national demonstration program using performance improvement methods and careful data collection, 73 US home health agencies improved targeted clinical outcomes and reduced hospitalizations from baseline rates by approximately 7% within 3 to 4 years.9 The study included approximately 158,000 patients in the intervention group and 249,000 in the comparison group. However, in general the success demonstrated in this study has not been reflected nationally, and home health agencies have been weakly integrated with the remainder of the health care delivery system.
Medicare home health agency care has evolved rapidly in the past 15 years, with reporting of numerous quality measures that has created direct accountability of physicians to the public. Until as recently as the 1990s, many important measures of quality in medicine were available only to physicians and physician and hospital organizations through governmental and, in some cases, legal routes. This new quality-based accountability, along with fiscal pressure to reduce lengths of stay and to limit visits under prospective payment, are among the changes that are transforming the home health industry.
THE VCU TRANSITIONAL CARE EXPERIENCE
The VCU Medical Center implemented a Naylor-model hospital-based transitional care program (TCP) 12 years ago that has served more than 500 patients. Targeted patients have histories similar to those observed by Naylor et al7: multiple hospitalizations, prolonged inpatient stays, many comorbidities and medications, complex care plans, and poor social support. Referrals come from physician teams, care coordinators, nurses, and social workers. The electronic medical record (EMR) has triggers for referrals.
Transitional care NPs meet patients in the hospital to ensure the appropriateness of their referral, introduce the program, and verify information. As shown in the Naylor model and later in the Coleman model,6 inpatient contact creates rapport with the patient and with family caregivers.
The first home visit is made on a weekday within 24 to 72 hours of discharge. At this initial visit, which takes a considerable amount of time, we attempt to reconcile medications, clarify social needs and resources, conduct physical assessments, modify medical regimens, educate the patient and his or her caregivers, and run diagnostic laboratory tests as needed. What we see in the home on this first visit often does not correspond with what was previously reported by hospital-based clinicians. For example, we have found that many patients are not taking medications as prescribed.
Typically, we visit homes weekly for 4 to 8 weeks. Some patients remain in transitional care for longer periods due to medical and social reasons. The NPs maintain close contact with home health agency staff via mobile phones. In some cases we conduct joint visits with home health agency staff in order to facilitate adjustments to medical care plans. Regular communication with primary care providers via the EMR, fax, and phone helps close the follow-up gap. The NP’s ability to observe the home setting, identify barriers to medical compliance (including literacy), and address social issues offers a clearer picture to care providers and fosters better outcomes. As patients improve and become more mobile, they return to the care of the primary provider.
Positive results with some limitations
We collected data between 2003 and 2006 on patients enrolled in the VCU Medical Center TCP. Our demographic results were similar to those reported by Naylor et al.7 Prevalent diseases included heart failure (HF), coronary artery disease, diabetes, and chronic obstructive pulmonary disease (COPD). The mean age was 71 years. The patient population was 63% female and 77% African American. About 73% of patients returned to the care of their primary physicians, 13% enrolled in the VCU House Calls program, 12% died, and 3% were admitted to nursing homes.10
A comparison of utilization data for 199 patients 6 months before and after their enrollment in the TCP over a period of 4 years showed decreased use of hospital resources—ie, fewer inpatient days, shorter lengths of stay, and fewer intensive care unit days— after enrollment. Aggregate cost after TCP enrollment reduction was $2,251,34410 which is 38% less than the 6-month pre-enrollment baseline (Table 2). Regression to the mean played a role, but most patients had a sustained high-use pattern for 6 months before enrollment. The high rate of consumption of health care resources dropped quickly following implementation of the TCP and stayed down for many months.
We largely concur with Naylor’s description of transitional care implementation.11 However, we have found that many transitional care patients are unable return to the clinic after 2 months, as suggested by Naylor. In our system, these patients default to our House Calls program for continuing care. Thus, in our estimation, transitional care is an important but incomplete response to population-based health needs. Supporting this conclusion is the Congressional Budget Office report, which states that among high-cost Medicare patients in an index year (2001), those who lived for 5 years were high-cost patients on a month-by-month basis in 22 of the next 60 months, reflecting chronic illness and cyclical service use patterns.12
Extension of the TCP to outpatients
Because of the favorable effect observed in the hospital-based TCP, we created a role for transitional care in our outpatient geriatric practice. Transitional care NPs from the clinic practice have the option of making home visits in a variety of scenarios. In the least serious cases a single “diagnostic” home visit provides invaluable insight. For example, we evaluate support systems and compliance with medication instructions and put systems in place to help patients maintain independence and safety at home, including nutrition and fall prevention programs. Patients with poor social support benefit especially from home visits.
We find that high-risk patients recently discharged from facilities, including those outside our health system, benefit from NP visits. When a high-risk clinic patient is hospitalized, we maintain a connection with the inpatient team, follow the patient’s progress, and assist with discharge planning. Based on our relationship with the patient prior to admission, we are able to anticipate problems and to address them promptly after discharge. The NP functions as the “hub of the wheel” to coordinate the multidisciplinary plan among primary care providers; specialists; and support services such as home health, social work, and physical therapy.
We also initiate periodic NP home visits as chronic diseases progress and as clinic patients become increasingly frail. Interim visits are made to monitor the medical plan and perform follow-up blood testing. Once patients are no longer able to use the office practice, they transition into the House Calls program.
HOSPITAL AT HOME
The ultimate in substitutive, intensive home care occurs when one replaces acute care hospital admission with care delivered entirely at home. Robust research has shown comparable or better clinical outcomes with fewer complications and lower costs when home care is applied to common conditions such as pneumonia, COPD, cellulitis, and HF.13,14 Rapidly advancing technology now supports increasingly sophisticated care at home. For example, with low molecular weight heparin, the care of deep vein thrombosis and stable pulmonary embolism—which always required inpatient care 25 years ago—can now be delivered entirely at home in many cases. Soon, these conditions may be managed solely with oral medication.15,16 The range of conditions that are now being managed at home is extensive, and the transformation of health care by portable technology is just beginning.17
LONGITUDINAL IN-HOME PRIMARY CARE
In the United States, patients who are immobile and cannot easily access office-based care often suffer with suboptimal mobile primary care. This represents a major limitation in care access for these patients. There is good evidence that longitudinal medical care, primarily delivered at home for periods lasting many months to several years, is effective and that it makes clinical sense. In the home, providers can accurately assess the patient’s living situation, engender trust, and respond in a timely manner when a patient’s condition changes. The Geriatric Resources for Assessment and Care of Elders (GRACE) program and the Veterans Affairs (VA) home-based primary care model are two examples of the benefits of longitudinal in-home care.
In the GRACE model, patients receive comprehensive in-home assessment by NPs with quarterly follow-up, and recommendations are given to primary care providers. The program’s clinical trial demonstrated markedly improved treatment of a variety of common geriatric ailments and reduced costs in a high-risk subset of patients.18 GRACE was not designed for urgent care but the approach was linked to lower costs in high-risk cases, likely due to better care and improved access.
The VA home-based primary care model has grown rapidly in the past decade, now operating at more than 200 medical centers, each with a full interprofessional team. House calls by physicians and NPs are part of the model, although the frequency varies across sites. Every team includes actively engaged physicians. Medicoeconomic evaluation based on tens of thousands of patient-years has shown an overall reduction in health care costs of 15% to 25% compared with historical values and prospectively modeled dollars.19,20 Home-based primary care teams are emerging across the United States at many academic centers and in the private sector.
To fund comprehensive longitudinal home care services for patients with complex health problems, the Independence at Home21 demonstration program was created under section 3024 of the Patient Protection and Affordable Care Act, using robust gain-sharing from demonstrated cost savings to reward house call teams. This multisite 3-year program started in June 2012. Rapid growth of this model is likely as private insurers have also taken an active interest in mobile medical care designs, using a variety of reward structures.
TELEMEDICINE
A debate continues over the use of communication technology in home care. It seems intuitive that “virtual visits” would be more efficient than clinicians visiting patients at home. Yet, the challenges of improving care by telemedicine alone are underestimated. For example, a recent large randomized trial, in which 33 cardiology practice sites provided at-home postdis-charge telemonitoring for HF patients, demonstrated no difference in clinical outcomes compared with patients monitored in the hospital or clinic.22
Proponents of telemedicine cite integrated models where data are managed proactively by a physician-led team that is engaged in care. This view seems valid, but other than anecdotal reports from integrated health systems, the published evidence of reduced costs is sparse. Some combination of in-person care and telemedicine is likely to be the optimal design and will emerge in coming years.
PACE: SYSTEM-BASED HOME CARE
In the 1980s, health maintenance organization risk contracts seemed a likely context for developing advanced home care models, but this did not happen. However, the Program for All-Inclusive Care of the Elderly (PACE) was tested and became a defined federal benefit in 1997. There are now nearly 100 PACE centers nationwide. PACE offers comprehensive care for people aged 55 years and older who are nursing home–eligible. The program appears to effectively help people stay home.23
An interdisciplinary team (IDT) coordinates PACE medical and social services to promote independence and quality of life. The program has been referred to as “a nursing home without walls.” Services include primary and specialty care, adult day care, case management, nursing, home health care, assistance with activities of daily living (ADL), medications, social work, rehabilitation, hospitalization, nursing facility care, nutritional support, caregiver respite, and transportation to and from the PACE adult day health center (ADHC) and medical appointments. The ADHC is the cornerstone and coordinating center for most care provided to PACE participants. Home-based care is provided in several ways:
- Home nursing care may be provided by external agencies, including skilled care, personal care, and hospice care, under contract with PACE. In Richmond, the home care manager oversees care after it is approved by the IDT. Weekly hours of care are changed often according to the participant’s need (eg, increased hours after hospital discharge and decreased hours when a family member visits and can provide more care). Home care provides assistance with ADLs and instrumental ADLs; “sitter” services are provided at the ADHC.
- The program supports home modifications and provides durable medical equipment (DME). Assessment is done by one or more team members upon enrollment and then at least every 6 months. PACE provides all DME the participant needs to remain safely in the community. At disenrollment or death, some equipment can be returned to PACE after review by the rehabilitation department.
- Primary care, basic laboratory services, and medical specialty care can be provided to the participant at home if for any reason he or she is unable to travel to the ADHC. PACE physicians make house calls to better understand patients’ living situations and needs. On-call nurses make home visits after hours or on weekends for clinical assessments, point-of-care diagnostic testing, specimen collection (stool or urine), and participant and family education on proper use of medications or equipment.
- As PACE participants approach the end of life, they transition to a palliative care model. A decision is made by the family and the IDT to discontinue attendance at the ADHC and to focus on care at home,24 allowing the participant to spend the last days or weeks in the relative comfort of home. Nurses make home visits when needed and educate families on symptom palliation.
- Additional in-home respite services can be provided to decrease caregiver burden.
- Skilled rehabilitation services are delivered either at home or in the ADHC depending on the judgment of the rehabilitation department and the IDT. The PACE site offers advanced transportation and full onsite therapy services 5 days per week.
The PACE sites become the insurers, receive defined capitation payments from Medicare and Medicaid that are adjusted for patient complexity, and assume the risk for all health care costs. Because of a 5% withholding in the capitation amount relative to projected Medicare expenses, PACE should reduce governmental costs. PACE must provide or pay for all usual Medicare and Medicaid services, and it may provide other services deemed necessary by the PACE team. Within PACE, hospital use is markedly reduced compared with conventional Medicare,25 and home care is one of several strategies employed. The PACE experience shows that care can be safely shifted from hospitals to other settings.
IMPACT ON MEDICAL EDUCATION
Since 1984, several thousand medical students; internal medicine residents; geriatric fellows; and N P, social work, and pharmacy students have participated in the VCU House Calls program and have come to see home care as a viable care model. House calls have been mandatory in the VCU School of Medicine curriculum since 2002. Qualitative evidence from these encounters demonstrates that learners value the experience and gain a better understanding of health care as a result.
Medical students’ interest in geriatrics is low,26,27 but positive, intense, or unique experiences with elders, and interactions with positive role models may improve the outlook for the specialty. The home setting gives learners an opportunity to observe the care of medically complex patients in the community, exposes the students to the team of professionals needed for comprehensive care, and enhances learners’ awareness of the challenges in providing continuity of care for this population.
We previously reported on a qualitative study of comments of second-year medical students who participated in our House Calls program.28 Students frequently noted the apparent comfort and positive attitude of the patients; the dedication, patience, compassion, commitment, and hard work of the caregivers; and the personalized and comprehensive care provided. The students identified both the challenges and the rewards for the doctors and expressed increased interest in conducting house calls in the future.
The training of competent and caring physicians and other health professionals is the goal of medical education. Fourth-year medical students were surveyed nationally regarding the qualities of a humanistic doctor.29 The students noted the importance of role models and participatory experiences. House calls provide an opportunity for learners to see health care in the community. Such experiences can create a memorable lesson in care delivery and in doctor-patient-caregiver relationships.
PALLIATIVE CARE AND HOME CARE
Ideally, care plans would gradually shift in focus from curative therapy to palliative care as patients with significant chronic illness advance in age and debility. In our geriatric practice, palliation is always important throughout extended chronic illness. Care plans progress and palliation becomes the primary focus in the final months of life. This transition may take years. Hospice referral is frequently a final step because the payment system reimburses for comprehensive team-based hospice care only when life expectancy is less than 6 months. The reason for this is economic: comprehensive team-based care is costly, and lengthening the hospice benefit as it is now structured could be prohibitively expensive. Our patients may live for years in a state of advanced debility, yet need intensive team care only at intervals. Optimally, the care model, team intensity, and related payments should flex with clinical need. This is what we have experienced by making house calls the mode of longitudinal primary care delivery, supported by our institution. Our teams help patients and families shift focus and decide when to accept hospice care; this requires more art than science and usually involves a gradual process of adaptation.
Our approach is consistent with the definition of palliative care published by the Centers for Medicare & Medicaid Services in 2008: patient- and family-centered care that optimizes quality of life by anticipating, preventing, and treating suffering. Palliative care addresses physical, intellectual, emotional, social, and spiritual needs and facilitates patient autonomy, access to information, and choice.30 Geriatric clinicians seek to help patients and families maximize quality of life and to maintain function by focusing on symptom management and clarification of patient and family goals rather than on specific diseases. This approach is applied without regard to patient age, condition, or stage of disease, and it can coexist with curative treatments. Thus it is distinguished in concept from “what we do when there is nothing more we can do.”31
In ways that are less clear when working in other care settings, home visits reveal patient goals, true rehabilitative potential, and family capacity for care-giving. Home visits take longer than office encounters, but make the provider’s job easier. By observing the patient at home, providers can better assess barriers to comfort and devise strategies to improve function, while also evaluating whether life is truly nearing the end. The home care clinician often engages in palliative care even if he or she did not initially intend to do so.
Furthermore, compared with the hospital or office setting, a home is more conducive to reasonably paced discussions about goals of care. Patients are more physically and emotionally comfortable and may talk more easily about potentially disturbing subjects. The clinician may be able to engage the patient by referring to pictures or mementos that help the patient to reflect on life values. And, a patient who is seen at home will more readily trust that the clinician places patients’ needs first. This opens the door to difficult discussions about code status, health care proxies, dialysis and ventilator support, or whether the patient would ever want to go to a hospital or a nursing home. Preferences change with time; patients ultimately feel less need to rely on ambulances and emergency care, given a timely response at home from a clinician who is familiar.32
Most dying patients are at home with their families during most of their final year of life; yet, despite studies showing that most patients prefer to die at home33–35 about 60% of all deaths still occur in the hospital.36 In our House Calls program’s experience, the percentage of patients who die at home is closer to 60.
Cherin and colleagues32 described a successful end-of-life home care program demonstrating a significant benefit to patients over usual care. The program integrated curative and palliative therapies. Similarly, Brumley and colleagues37 demonstrated that, compared with usual care, patients receiving in-home palliative care reported greater satisfaction, had fewer emergency department and hospital visits, and were more likely to die at home, with significantly lower overall costs. These findings conform to our experience. (Also see “Innovative models of home-based palliative care”)
CONCLUSION
Advanced home care with a strong medical component is an important part of the supportive and recuperative care options in the United States. For these programs to reach their full potential, we must expand on the successful in-home medical care models and create responsible financing methods that control overall costs while rewarding providers appropriately. We must broaden the application of portable and information technologies and develop an interdisciplinary workforce. These approaches will lead us toward our overall goals of optimal care at minimal cost.
- Levine SA, Boal J, Boling PA. Home care. JAMA 2003; 290:1203–1207.
- Boling PA. Home care: the first option. In:Cornwell T, Schwartz-berg JGeds. Medical Management of the Home Care Patient: Guidelines for Physicians. 4th ed. Chicago, IL: American Medical Association; 2012:1–14.
- Brickner PW, Duque Sister Teresita, Kaufman A, et al. The homebound aged: a medically unreached group. Ann Intern Med 1975; 82:1–6.
- Boling PA. Effects of policy, reimbursement, and regulation on home health care. In:Olson S. The Role of Human Factors in Home Health Care: Workshop Summary. Washington, DC: The National Academies Press; 2010:275–302.
- Basic statistics about home care. National Association for Home Care & Hospice Web site. http://www.nahc.org/facts/10HC_Stats.pdf. Updated 2010. Accessed October 11, 2012.
- Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 2006; 166:1822–1828.
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home follow-up of hospitalized elders: a randomized clinical trial. JAMA 1999; 281:613–620.
- Naylor MD, Brooten DA, Campbell RL, Maislin G, McCauley KM, Schwartz JS. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial. J Am Geriatr Soc 2004; 52:675–684.
- Shaughnessy PW, Hittle DF, Crisler KS, et al. Improving patient outcomes of home health care: findings from two demonstration trials of outcome-based quality improvement. J Am Geriatr Soc 2002; 50:1354–1364.
- Smigelski C, Hungate B, Holdren J, Goodloe L, Boling PA. Transitional model of care at VCU Medical Center—6 years’ experience. J Am Geriatr Soc 2008; 56 suppl 1:S197.
- Naylor MD. Advancing high value transitional care: the central role of nursing and its leadership. Nurs Adm Q 2012; 36:115–126.
- Holtz-Eakin D. High-cost medicare beneficiaries. Congressional Budget Office Web site. http://www.cbo.gov/sites/default/fles/cbofles/ftpdocs/63xx/doc6332/05-03-medispending.pdf. Published May 2005. Accessed October 11, 2012.
- Cryer L, Shannon SB, Van Amsterdam M, Leff B. Costs for “hospital at home” patients were 19 percent lower, with equal or better outcomes compared to similar inpatients. Health Aff (Millwood) 2012; 31:1237–1243.
- Leff B, Burton L, Mader SL, et al. Hospital at home: feasibility and outcomes of a program to provide hospital-level care at home for acutely ill older patients. Ann Intern Med 2005; 143:798–808.
- Aujesky D, Roy PM, Verschuren F, et al. Outpatient versus inpatient treatment for patients with acute pulmonary embolism: an international, open-label, randomised, non-inferiority trial [published online ahead of print June 22, 2011]. Lancet 2011; 378 9785:41–48. 10.1016/S0140-6736 1160824–6
- Büller HR, Prins MH, Lensing AWA, et al the EINSTEIN– PE Investigators. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 2012; 366:1287–1297.
- Landers SH. Why health care is going home [published online ahead of print October 20, 2010]. N Engl J Med 2010; 363:1690–1691. 10.1056/NEJMp1000401
- Counsell SR, Callahan CM, Clark DO, et al. Geriatric care management for low-income seniors: a randomized controlled trial. JAMA 2007; 298:2623–2633.
- Beales JL, Edes T. Veteran’s Affairs home based primary care. Clin Geriatr Med 2009; 25:149–154.
- Kinosian B, Edes T, Davis D, Hossain M. Financial savings of home based primary care for frail veterans with chronic disabling disease. J Am Geriatr Soc 2010; 589 (suppl s1):S3. Abstract P7.
- DeJonge KE, Taler G, Boling PA. Independence at home: community-based care for older adults with severe chronic illness. Clin Geriatr Med 2009; 25:155–169.
- Chaudhry SI, Mattera JA, Curtis JP, et al. Telemonitoring in patients with heart failure [published online ahead of print November 16, 2010]. N Engl J Med 2010; 363:2301–2309. 10.1056/NEJMoa1010029
- Wieland D, Boland R, Baskins J, Kinosian B. Five-year survival in a Program of All-inclusive Care for Elderly compared with alternative institutional and home- and community-based care [published online ahead of print March 30, 2010]. J Gerontol A Biol Sci Med Sci 2010; 65:721–726. 10.1093/gerona/glq040
- Schamp R, Tenkku L. Managed death in a PACE: pathways in present and advance directives [published online ahead of print May 30, 2006]. J Am Med Dir Assoc 2006; 7:339–344. 10.1016/j.jamda.2006.01.022
- Meret-Hanke LA. Effects of the Program of All-inclusive Care for the Elderly on hospital use [published online ahead of print July 6, 2011]. Gerontologist 2011; 51:774–785. 10.1093/geront/gnr040
- Fitzgerald JT, Wray LA, Halter JB, Williams BC, Supiano MA. Relating medical students’ knowledge, attitudes, and experience to an interest in geriatric medicine. Gerontologist 2003; 43:849–855.
- Voogt SJ, Mickus M, Santiago O, Herman SE. Attitudes, experiences, and interest in geriatrics of first-year allopathic and osteopathic medical students [published online ahead of print December 11, 2007]. J Am Geriatr Soc 2008; 56:339–344. 10.1111/j.1532-5415.2007.01541.
- Abbey L, Willett R, Selby-Penczak R, McKnight R. Social learning: medical student perceptions of geriatric house calls. Gerontol Geriatr Educ 2010; 31:149–162.
- Moyer CA, Arnold L, Quaintance J, et al. What factors create a humanistic doctor? A nationwide survey of fourth-year medical students. Acad Med 2010; 85:1800–1807.
- Centers for Medicare & Medicaid Services. Medicare and Medicaid programs: hospice conditions of participation. Federal Register 2008; 73:32204–32220.
- Meier DE, Brawley OW. Palliative care and the quality of life [published online ahead of print June 13, 2011]. J Clin Oncol 2011; 29:2750–2752. 10.1200/JCO.2011.35.9729
- Cherin DA, Enguidanos SM, Jamison P. Physicians as medical center “extenders” in end-of-life care: physician home visits as the lynch pin in creating an end-of-life care system. Home Health Care Serv Q 2004; 23:41–53.
- Hays JC, Galanos AN, Palmer TA, McQuoid DR, Flint EP. Preference for place of death in a continuing care retirement community. Gerontologist 2001; 41:123–128.
- Karlsen S, Addington-Hall J. How do cancer patients who die at home differ from those who die elsewhere? Palliat Med 1998; 12:279–286.
- Townsend J, Frank AO, Fermont D, et al. Terminal cancer care and patients’ preference for place of death: a prospective study. BMJ 1990; 301:415–417.
- Weitzen S, Teno JM, Fennell M, Mor V. Factors associated with site of death: a national study of where people die. Med Care 2003; 41:323–335.
- Brumley R, Enguidanos S, Jamison P, et al. Increased satisfaction with care and lower costs: results of a randomized trial of in-home palliative care. J Am Geriatr Soc 2007; 55:993–1000.
When it can be done safely, most people prefer to be treated and recover from illness at home.1,2 Home-based services have improved considerably since Brickner called the homebound aged “a medically unreached group.”3 Still, home care has not achieved its full potential and scientific investigation of home care models is scant compared with that of other therapeutic approaches.
The challenges of studying home care include variability in interventions, difficulty defining treatment and comparison groups, and high research costs. The care itself can be demanding, requiring providers to mobilize processes that have become institution-based and immobile, integrate care across insular settings, incorporate complex social issues into the care plan, and develop a viable home care financing model.
This article reviews evidence favoring investment in advanced home care and adds perspective from 3 decades’ experience at Virginia Commonwealth University (VCU), Richmond, Virginia.
The term home care has a broad scope, ranging from basic support to highly technical care involving intravenous lines, ventilators, portable diagnostic tests, and remote monitors.4 Patients cared for at home range from those who are ambulatory to those who are permanently bedfast and seriously ill. The home care user population can be categorized based on the types of health care resources they consume (Table 1). Much attention has been paid to home-based care during recuperation after acute illness. The aim has been to foster recovery and prevent further need for institutional care. Lately the term transitional care has been used in this context.
TRANSITIONAL CARE
Transitional care has long been a priority for visiting nurse agencies. In 1965, Medicare Part A, building from the tradition of urban parish nursing services, created an interdisciplinary industry. Medicare now certifies more than 10,000 agencies with more than 250,000 professional staff.5 For several reasons, beginning in the 1970s, US physicians have become less integrated into in-home care. Despite this and the challenge of managing medically complex patients with minimal active physician involvement, home health agencies provide a vital service. Further, they have demonstrated improved outcomes and cost savings.
Transitional care refers to specialized, short-term care for selected high-risk patients after an acute illness. The original objective of transitional care was to reduce hospital readmissions. Tested models include an approach developed by Coleman et al,6 based on four pillars: assistance with medication self-management, patient-centered and -owned medical record, timely follow-up with primary or specialty care, and “red flags” that indicate a worsening condition. This model, which yielded one-third fewer hospital readmissions and a savings of about $500 per patient in 6 months, is being adopted in many locations nationally.
Naylor and colleagues7,8 collaborated with hospital-based nurse practitioners (NPs) for 2 decades on a more intensive model. In the Naylor model, the NPs form a health care bridge from hospital to home for 4 weeks after hospital care and add an active medical care component to the home care team. Naylor et al7 reported a 50% reduction in the rehospitalization rate and a cost savings of approximately $3,000 per patient over 24 weeks. Naylor’s team observed these results among frail, elderly patients with a variety of conditions and comorbidities. The 2010 federal health care reform law as well as state and private insurer initiatives now encourage use of this and other integrated care models.
In a national demonstration program using performance improvement methods and careful data collection, 73 US home health agencies improved targeted clinical outcomes and reduced hospitalizations from baseline rates by approximately 7% within 3 to 4 years.9 The study included approximately 158,000 patients in the intervention group and 249,000 in the comparison group. However, in general the success demonstrated in this study has not been reflected nationally, and home health agencies have been weakly integrated with the remainder of the health care delivery system.
Medicare home health agency care has evolved rapidly in the past 15 years, with reporting of numerous quality measures that has created direct accountability of physicians to the public. Until as recently as the 1990s, many important measures of quality in medicine were available only to physicians and physician and hospital organizations through governmental and, in some cases, legal routes. This new quality-based accountability, along with fiscal pressure to reduce lengths of stay and to limit visits under prospective payment, are among the changes that are transforming the home health industry.
THE VCU TRANSITIONAL CARE EXPERIENCE
The VCU Medical Center implemented a Naylor-model hospital-based transitional care program (TCP) 12 years ago that has served more than 500 patients. Targeted patients have histories similar to those observed by Naylor et al7: multiple hospitalizations, prolonged inpatient stays, many comorbidities and medications, complex care plans, and poor social support. Referrals come from physician teams, care coordinators, nurses, and social workers. The electronic medical record (EMR) has triggers for referrals.
Transitional care NPs meet patients in the hospital to ensure the appropriateness of their referral, introduce the program, and verify information. As shown in the Naylor model and later in the Coleman model,6 inpatient contact creates rapport with the patient and with family caregivers.
The first home visit is made on a weekday within 24 to 72 hours of discharge. At this initial visit, which takes a considerable amount of time, we attempt to reconcile medications, clarify social needs and resources, conduct physical assessments, modify medical regimens, educate the patient and his or her caregivers, and run diagnostic laboratory tests as needed. What we see in the home on this first visit often does not correspond with what was previously reported by hospital-based clinicians. For example, we have found that many patients are not taking medications as prescribed.
Typically, we visit homes weekly for 4 to 8 weeks. Some patients remain in transitional care for longer periods due to medical and social reasons. The NPs maintain close contact with home health agency staff via mobile phones. In some cases we conduct joint visits with home health agency staff in order to facilitate adjustments to medical care plans. Regular communication with primary care providers via the EMR, fax, and phone helps close the follow-up gap. The NP’s ability to observe the home setting, identify barriers to medical compliance (including literacy), and address social issues offers a clearer picture to care providers and fosters better outcomes. As patients improve and become more mobile, they return to the care of the primary provider.
Positive results with some limitations
We collected data between 2003 and 2006 on patients enrolled in the VCU Medical Center TCP. Our demographic results were similar to those reported by Naylor et al.7 Prevalent diseases included heart failure (HF), coronary artery disease, diabetes, and chronic obstructive pulmonary disease (COPD). The mean age was 71 years. The patient population was 63% female and 77% African American. About 73% of patients returned to the care of their primary physicians, 13% enrolled in the VCU House Calls program, 12% died, and 3% were admitted to nursing homes.10
A comparison of utilization data for 199 patients 6 months before and after their enrollment in the TCP over a period of 4 years showed decreased use of hospital resources—ie, fewer inpatient days, shorter lengths of stay, and fewer intensive care unit days— after enrollment. Aggregate cost after TCP enrollment reduction was $2,251,34410 which is 38% less than the 6-month pre-enrollment baseline (Table 2). Regression to the mean played a role, but most patients had a sustained high-use pattern for 6 months before enrollment. The high rate of consumption of health care resources dropped quickly following implementation of the TCP and stayed down for many months.
We largely concur with Naylor’s description of transitional care implementation.11 However, we have found that many transitional care patients are unable return to the clinic after 2 months, as suggested by Naylor. In our system, these patients default to our House Calls program for continuing care. Thus, in our estimation, transitional care is an important but incomplete response to population-based health needs. Supporting this conclusion is the Congressional Budget Office report, which states that among high-cost Medicare patients in an index year (2001), those who lived for 5 years were high-cost patients on a month-by-month basis in 22 of the next 60 months, reflecting chronic illness and cyclical service use patterns.12
Extension of the TCP to outpatients
Because of the favorable effect observed in the hospital-based TCP, we created a role for transitional care in our outpatient geriatric practice. Transitional care NPs from the clinic practice have the option of making home visits in a variety of scenarios. In the least serious cases a single “diagnostic” home visit provides invaluable insight. For example, we evaluate support systems and compliance with medication instructions and put systems in place to help patients maintain independence and safety at home, including nutrition and fall prevention programs. Patients with poor social support benefit especially from home visits.
We find that high-risk patients recently discharged from facilities, including those outside our health system, benefit from NP visits. When a high-risk clinic patient is hospitalized, we maintain a connection with the inpatient team, follow the patient’s progress, and assist with discharge planning. Based on our relationship with the patient prior to admission, we are able to anticipate problems and to address them promptly after discharge. The NP functions as the “hub of the wheel” to coordinate the multidisciplinary plan among primary care providers; specialists; and support services such as home health, social work, and physical therapy.
We also initiate periodic NP home visits as chronic diseases progress and as clinic patients become increasingly frail. Interim visits are made to monitor the medical plan and perform follow-up blood testing. Once patients are no longer able to use the office practice, they transition into the House Calls program.
HOSPITAL AT HOME
The ultimate in substitutive, intensive home care occurs when one replaces acute care hospital admission with care delivered entirely at home. Robust research has shown comparable or better clinical outcomes with fewer complications and lower costs when home care is applied to common conditions such as pneumonia, COPD, cellulitis, and HF.13,14 Rapidly advancing technology now supports increasingly sophisticated care at home. For example, with low molecular weight heparin, the care of deep vein thrombosis and stable pulmonary embolism—which always required inpatient care 25 years ago—can now be delivered entirely at home in many cases. Soon, these conditions may be managed solely with oral medication.15,16 The range of conditions that are now being managed at home is extensive, and the transformation of health care by portable technology is just beginning.17
LONGITUDINAL IN-HOME PRIMARY CARE
In the United States, patients who are immobile and cannot easily access office-based care often suffer with suboptimal mobile primary care. This represents a major limitation in care access for these patients. There is good evidence that longitudinal medical care, primarily delivered at home for periods lasting many months to several years, is effective and that it makes clinical sense. In the home, providers can accurately assess the patient’s living situation, engender trust, and respond in a timely manner when a patient’s condition changes. The Geriatric Resources for Assessment and Care of Elders (GRACE) program and the Veterans Affairs (VA) home-based primary care model are two examples of the benefits of longitudinal in-home care.
In the GRACE model, patients receive comprehensive in-home assessment by NPs with quarterly follow-up, and recommendations are given to primary care providers. The program’s clinical trial demonstrated markedly improved treatment of a variety of common geriatric ailments and reduced costs in a high-risk subset of patients.18 GRACE was not designed for urgent care but the approach was linked to lower costs in high-risk cases, likely due to better care and improved access.
The VA home-based primary care model has grown rapidly in the past decade, now operating at more than 200 medical centers, each with a full interprofessional team. House calls by physicians and NPs are part of the model, although the frequency varies across sites. Every team includes actively engaged physicians. Medicoeconomic evaluation based on tens of thousands of patient-years has shown an overall reduction in health care costs of 15% to 25% compared with historical values and prospectively modeled dollars.19,20 Home-based primary care teams are emerging across the United States at many academic centers and in the private sector.
To fund comprehensive longitudinal home care services for patients with complex health problems, the Independence at Home21 demonstration program was created under section 3024 of the Patient Protection and Affordable Care Act, using robust gain-sharing from demonstrated cost savings to reward house call teams. This multisite 3-year program started in June 2012. Rapid growth of this model is likely as private insurers have also taken an active interest in mobile medical care designs, using a variety of reward structures.
TELEMEDICINE
A debate continues over the use of communication technology in home care. It seems intuitive that “virtual visits” would be more efficient than clinicians visiting patients at home. Yet, the challenges of improving care by telemedicine alone are underestimated. For example, a recent large randomized trial, in which 33 cardiology practice sites provided at-home postdis-charge telemonitoring for HF patients, demonstrated no difference in clinical outcomes compared with patients monitored in the hospital or clinic.22
Proponents of telemedicine cite integrated models where data are managed proactively by a physician-led team that is engaged in care. This view seems valid, but other than anecdotal reports from integrated health systems, the published evidence of reduced costs is sparse. Some combination of in-person care and telemedicine is likely to be the optimal design and will emerge in coming years.
PACE: SYSTEM-BASED HOME CARE
In the 1980s, health maintenance organization risk contracts seemed a likely context for developing advanced home care models, but this did not happen. However, the Program for All-Inclusive Care of the Elderly (PACE) was tested and became a defined federal benefit in 1997. There are now nearly 100 PACE centers nationwide. PACE offers comprehensive care for people aged 55 years and older who are nursing home–eligible. The program appears to effectively help people stay home.23
An interdisciplinary team (IDT) coordinates PACE medical and social services to promote independence and quality of life. The program has been referred to as “a nursing home without walls.” Services include primary and specialty care, adult day care, case management, nursing, home health care, assistance with activities of daily living (ADL), medications, social work, rehabilitation, hospitalization, nursing facility care, nutritional support, caregiver respite, and transportation to and from the PACE adult day health center (ADHC) and medical appointments. The ADHC is the cornerstone and coordinating center for most care provided to PACE participants. Home-based care is provided in several ways:
- Home nursing care may be provided by external agencies, including skilled care, personal care, and hospice care, under contract with PACE. In Richmond, the home care manager oversees care after it is approved by the IDT. Weekly hours of care are changed often according to the participant’s need (eg, increased hours after hospital discharge and decreased hours when a family member visits and can provide more care). Home care provides assistance with ADLs and instrumental ADLs; “sitter” services are provided at the ADHC.
- The program supports home modifications and provides durable medical equipment (DME). Assessment is done by one or more team members upon enrollment and then at least every 6 months. PACE provides all DME the participant needs to remain safely in the community. At disenrollment or death, some equipment can be returned to PACE after review by the rehabilitation department.
- Primary care, basic laboratory services, and medical specialty care can be provided to the participant at home if for any reason he or she is unable to travel to the ADHC. PACE physicians make house calls to better understand patients’ living situations and needs. On-call nurses make home visits after hours or on weekends for clinical assessments, point-of-care diagnostic testing, specimen collection (stool or urine), and participant and family education on proper use of medications or equipment.
- As PACE participants approach the end of life, they transition to a palliative care model. A decision is made by the family and the IDT to discontinue attendance at the ADHC and to focus on care at home,24 allowing the participant to spend the last days or weeks in the relative comfort of home. Nurses make home visits when needed and educate families on symptom palliation.
- Additional in-home respite services can be provided to decrease caregiver burden.
- Skilled rehabilitation services are delivered either at home or in the ADHC depending on the judgment of the rehabilitation department and the IDT. The PACE site offers advanced transportation and full onsite therapy services 5 days per week.
The PACE sites become the insurers, receive defined capitation payments from Medicare and Medicaid that are adjusted for patient complexity, and assume the risk for all health care costs. Because of a 5% withholding in the capitation amount relative to projected Medicare expenses, PACE should reduce governmental costs. PACE must provide or pay for all usual Medicare and Medicaid services, and it may provide other services deemed necessary by the PACE team. Within PACE, hospital use is markedly reduced compared with conventional Medicare,25 and home care is one of several strategies employed. The PACE experience shows that care can be safely shifted from hospitals to other settings.
IMPACT ON MEDICAL EDUCATION
Since 1984, several thousand medical students; internal medicine residents; geriatric fellows; and N P, social work, and pharmacy students have participated in the VCU House Calls program and have come to see home care as a viable care model. House calls have been mandatory in the VCU School of Medicine curriculum since 2002. Qualitative evidence from these encounters demonstrates that learners value the experience and gain a better understanding of health care as a result.
Medical students’ interest in geriatrics is low,26,27 but positive, intense, or unique experiences with elders, and interactions with positive role models may improve the outlook for the specialty. The home setting gives learners an opportunity to observe the care of medically complex patients in the community, exposes the students to the team of professionals needed for comprehensive care, and enhances learners’ awareness of the challenges in providing continuity of care for this population.
We previously reported on a qualitative study of comments of second-year medical students who participated in our House Calls program.28 Students frequently noted the apparent comfort and positive attitude of the patients; the dedication, patience, compassion, commitment, and hard work of the caregivers; and the personalized and comprehensive care provided. The students identified both the challenges and the rewards for the doctors and expressed increased interest in conducting house calls in the future.
The training of competent and caring physicians and other health professionals is the goal of medical education. Fourth-year medical students were surveyed nationally regarding the qualities of a humanistic doctor.29 The students noted the importance of role models and participatory experiences. House calls provide an opportunity for learners to see health care in the community. Such experiences can create a memorable lesson in care delivery and in doctor-patient-caregiver relationships.
PALLIATIVE CARE AND HOME CARE
Ideally, care plans would gradually shift in focus from curative therapy to palliative care as patients with significant chronic illness advance in age and debility. In our geriatric practice, palliation is always important throughout extended chronic illness. Care plans progress and palliation becomes the primary focus in the final months of life. This transition may take years. Hospice referral is frequently a final step because the payment system reimburses for comprehensive team-based hospice care only when life expectancy is less than 6 months. The reason for this is economic: comprehensive team-based care is costly, and lengthening the hospice benefit as it is now structured could be prohibitively expensive. Our patients may live for years in a state of advanced debility, yet need intensive team care only at intervals. Optimally, the care model, team intensity, and related payments should flex with clinical need. This is what we have experienced by making house calls the mode of longitudinal primary care delivery, supported by our institution. Our teams help patients and families shift focus and decide when to accept hospice care; this requires more art than science and usually involves a gradual process of adaptation.
Our approach is consistent with the definition of palliative care published by the Centers for Medicare & Medicaid Services in 2008: patient- and family-centered care that optimizes quality of life by anticipating, preventing, and treating suffering. Palliative care addresses physical, intellectual, emotional, social, and spiritual needs and facilitates patient autonomy, access to information, and choice.30 Geriatric clinicians seek to help patients and families maximize quality of life and to maintain function by focusing on symptom management and clarification of patient and family goals rather than on specific diseases. This approach is applied without regard to patient age, condition, or stage of disease, and it can coexist with curative treatments. Thus it is distinguished in concept from “what we do when there is nothing more we can do.”31
In ways that are less clear when working in other care settings, home visits reveal patient goals, true rehabilitative potential, and family capacity for care-giving. Home visits take longer than office encounters, but make the provider’s job easier. By observing the patient at home, providers can better assess barriers to comfort and devise strategies to improve function, while also evaluating whether life is truly nearing the end. The home care clinician often engages in palliative care even if he or she did not initially intend to do so.
Furthermore, compared with the hospital or office setting, a home is more conducive to reasonably paced discussions about goals of care. Patients are more physically and emotionally comfortable and may talk more easily about potentially disturbing subjects. The clinician may be able to engage the patient by referring to pictures or mementos that help the patient to reflect on life values. And, a patient who is seen at home will more readily trust that the clinician places patients’ needs first. This opens the door to difficult discussions about code status, health care proxies, dialysis and ventilator support, or whether the patient would ever want to go to a hospital or a nursing home. Preferences change with time; patients ultimately feel less need to rely on ambulances and emergency care, given a timely response at home from a clinician who is familiar.32
Most dying patients are at home with their families during most of their final year of life; yet, despite studies showing that most patients prefer to die at home33–35 about 60% of all deaths still occur in the hospital.36 In our House Calls program’s experience, the percentage of patients who die at home is closer to 60.
Cherin and colleagues32 described a successful end-of-life home care program demonstrating a significant benefit to patients over usual care. The program integrated curative and palliative therapies. Similarly, Brumley and colleagues37 demonstrated that, compared with usual care, patients receiving in-home palliative care reported greater satisfaction, had fewer emergency department and hospital visits, and were more likely to die at home, with significantly lower overall costs. These findings conform to our experience. (Also see “Innovative models of home-based palliative care”)
CONCLUSION
Advanced home care with a strong medical component is an important part of the supportive and recuperative care options in the United States. For these programs to reach their full potential, we must expand on the successful in-home medical care models and create responsible financing methods that control overall costs while rewarding providers appropriately. We must broaden the application of portable and information technologies and develop an interdisciplinary workforce. These approaches will lead us toward our overall goals of optimal care at minimal cost.
When it can be done safely, most people prefer to be treated and recover from illness at home.1,2 Home-based services have improved considerably since Brickner called the homebound aged “a medically unreached group.”3 Still, home care has not achieved its full potential and scientific investigation of home care models is scant compared with that of other therapeutic approaches.
The challenges of studying home care include variability in interventions, difficulty defining treatment and comparison groups, and high research costs. The care itself can be demanding, requiring providers to mobilize processes that have become institution-based and immobile, integrate care across insular settings, incorporate complex social issues into the care plan, and develop a viable home care financing model.
This article reviews evidence favoring investment in advanced home care and adds perspective from 3 decades’ experience at Virginia Commonwealth University (VCU), Richmond, Virginia.
The term home care has a broad scope, ranging from basic support to highly technical care involving intravenous lines, ventilators, portable diagnostic tests, and remote monitors.4 Patients cared for at home range from those who are ambulatory to those who are permanently bedfast and seriously ill. The home care user population can be categorized based on the types of health care resources they consume (Table 1). Much attention has been paid to home-based care during recuperation after acute illness. The aim has been to foster recovery and prevent further need for institutional care. Lately the term transitional care has been used in this context.
TRANSITIONAL CARE
Transitional care has long been a priority for visiting nurse agencies. In 1965, Medicare Part A, building from the tradition of urban parish nursing services, created an interdisciplinary industry. Medicare now certifies more than 10,000 agencies with more than 250,000 professional staff.5 For several reasons, beginning in the 1970s, US physicians have become less integrated into in-home care. Despite this and the challenge of managing medically complex patients with minimal active physician involvement, home health agencies provide a vital service. Further, they have demonstrated improved outcomes and cost savings.
Transitional care refers to specialized, short-term care for selected high-risk patients after an acute illness. The original objective of transitional care was to reduce hospital readmissions. Tested models include an approach developed by Coleman et al,6 based on four pillars: assistance with medication self-management, patient-centered and -owned medical record, timely follow-up with primary or specialty care, and “red flags” that indicate a worsening condition. This model, which yielded one-third fewer hospital readmissions and a savings of about $500 per patient in 6 months, is being adopted in many locations nationally.
Naylor and colleagues7,8 collaborated with hospital-based nurse practitioners (NPs) for 2 decades on a more intensive model. In the Naylor model, the NPs form a health care bridge from hospital to home for 4 weeks after hospital care and add an active medical care component to the home care team. Naylor et al7 reported a 50% reduction in the rehospitalization rate and a cost savings of approximately $3,000 per patient over 24 weeks. Naylor’s team observed these results among frail, elderly patients with a variety of conditions and comorbidities. The 2010 federal health care reform law as well as state and private insurer initiatives now encourage use of this and other integrated care models.
In a national demonstration program using performance improvement methods and careful data collection, 73 US home health agencies improved targeted clinical outcomes and reduced hospitalizations from baseline rates by approximately 7% within 3 to 4 years.9 The study included approximately 158,000 patients in the intervention group and 249,000 in the comparison group. However, in general the success demonstrated in this study has not been reflected nationally, and home health agencies have been weakly integrated with the remainder of the health care delivery system.
Medicare home health agency care has evolved rapidly in the past 15 years, with reporting of numerous quality measures that has created direct accountability of physicians to the public. Until as recently as the 1990s, many important measures of quality in medicine were available only to physicians and physician and hospital organizations through governmental and, in some cases, legal routes. This new quality-based accountability, along with fiscal pressure to reduce lengths of stay and to limit visits under prospective payment, are among the changes that are transforming the home health industry.
THE VCU TRANSITIONAL CARE EXPERIENCE
The VCU Medical Center implemented a Naylor-model hospital-based transitional care program (TCP) 12 years ago that has served more than 500 patients. Targeted patients have histories similar to those observed by Naylor et al7: multiple hospitalizations, prolonged inpatient stays, many comorbidities and medications, complex care plans, and poor social support. Referrals come from physician teams, care coordinators, nurses, and social workers. The electronic medical record (EMR) has triggers for referrals.
Transitional care NPs meet patients in the hospital to ensure the appropriateness of their referral, introduce the program, and verify information. As shown in the Naylor model and later in the Coleman model,6 inpatient contact creates rapport with the patient and with family caregivers.
The first home visit is made on a weekday within 24 to 72 hours of discharge. At this initial visit, which takes a considerable amount of time, we attempt to reconcile medications, clarify social needs and resources, conduct physical assessments, modify medical regimens, educate the patient and his or her caregivers, and run diagnostic laboratory tests as needed. What we see in the home on this first visit often does not correspond with what was previously reported by hospital-based clinicians. For example, we have found that many patients are not taking medications as prescribed.
Typically, we visit homes weekly for 4 to 8 weeks. Some patients remain in transitional care for longer periods due to medical and social reasons. The NPs maintain close contact with home health agency staff via mobile phones. In some cases we conduct joint visits with home health agency staff in order to facilitate adjustments to medical care plans. Regular communication with primary care providers via the EMR, fax, and phone helps close the follow-up gap. The NP’s ability to observe the home setting, identify barriers to medical compliance (including literacy), and address social issues offers a clearer picture to care providers and fosters better outcomes. As patients improve and become more mobile, they return to the care of the primary provider.
Positive results with some limitations
We collected data between 2003 and 2006 on patients enrolled in the VCU Medical Center TCP. Our demographic results were similar to those reported by Naylor et al.7 Prevalent diseases included heart failure (HF), coronary artery disease, diabetes, and chronic obstructive pulmonary disease (COPD). The mean age was 71 years. The patient population was 63% female and 77% African American. About 73% of patients returned to the care of their primary physicians, 13% enrolled in the VCU House Calls program, 12% died, and 3% were admitted to nursing homes.10
A comparison of utilization data for 199 patients 6 months before and after their enrollment in the TCP over a period of 4 years showed decreased use of hospital resources—ie, fewer inpatient days, shorter lengths of stay, and fewer intensive care unit days— after enrollment. Aggregate cost after TCP enrollment reduction was $2,251,34410 which is 38% less than the 6-month pre-enrollment baseline (Table 2). Regression to the mean played a role, but most patients had a sustained high-use pattern for 6 months before enrollment. The high rate of consumption of health care resources dropped quickly following implementation of the TCP and stayed down for many months.
We largely concur with Naylor’s description of transitional care implementation.11 However, we have found that many transitional care patients are unable return to the clinic after 2 months, as suggested by Naylor. In our system, these patients default to our House Calls program for continuing care. Thus, in our estimation, transitional care is an important but incomplete response to population-based health needs. Supporting this conclusion is the Congressional Budget Office report, which states that among high-cost Medicare patients in an index year (2001), those who lived for 5 years were high-cost patients on a month-by-month basis in 22 of the next 60 months, reflecting chronic illness and cyclical service use patterns.12
Extension of the TCP to outpatients
Because of the favorable effect observed in the hospital-based TCP, we created a role for transitional care in our outpatient geriatric practice. Transitional care NPs from the clinic practice have the option of making home visits in a variety of scenarios. In the least serious cases a single “diagnostic” home visit provides invaluable insight. For example, we evaluate support systems and compliance with medication instructions and put systems in place to help patients maintain independence and safety at home, including nutrition and fall prevention programs. Patients with poor social support benefit especially from home visits.
We find that high-risk patients recently discharged from facilities, including those outside our health system, benefit from NP visits. When a high-risk clinic patient is hospitalized, we maintain a connection with the inpatient team, follow the patient’s progress, and assist with discharge planning. Based on our relationship with the patient prior to admission, we are able to anticipate problems and to address them promptly after discharge. The NP functions as the “hub of the wheel” to coordinate the multidisciplinary plan among primary care providers; specialists; and support services such as home health, social work, and physical therapy.
We also initiate periodic NP home visits as chronic diseases progress and as clinic patients become increasingly frail. Interim visits are made to monitor the medical plan and perform follow-up blood testing. Once patients are no longer able to use the office practice, they transition into the House Calls program.
HOSPITAL AT HOME
The ultimate in substitutive, intensive home care occurs when one replaces acute care hospital admission with care delivered entirely at home. Robust research has shown comparable or better clinical outcomes with fewer complications and lower costs when home care is applied to common conditions such as pneumonia, COPD, cellulitis, and HF.13,14 Rapidly advancing technology now supports increasingly sophisticated care at home. For example, with low molecular weight heparin, the care of deep vein thrombosis and stable pulmonary embolism—which always required inpatient care 25 years ago—can now be delivered entirely at home in many cases. Soon, these conditions may be managed solely with oral medication.15,16 The range of conditions that are now being managed at home is extensive, and the transformation of health care by portable technology is just beginning.17
LONGITUDINAL IN-HOME PRIMARY CARE
In the United States, patients who are immobile and cannot easily access office-based care often suffer with suboptimal mobile primary care. This represents a major limitation in care access for these patients. There is good evidence that longitudinal medical care, primarily delivered at home for periods lasting many months to several years, is effective and that it makes clinical sense. In the home, providers can accurately assess the patient’s living situation, engender trust, and respond in a timely manner when a patient’s condition changes. The Geriatric Resources for Assessment and Care of Elders (GRACE) program and the Veterans Affairs (VA) home-based primary care model are two examples of the benefits of longitudinal in-home care.
In the GRACE model, patients receive comprehensive in-home assessment by NPs with quarterly follow-up, and recommendations are given to primary care providers. The program’s clinical trial demonstrated markedly improved treatment of a variety of common geriatric ailments and reduced costs in a high-risk subset of patients.18 GRACE was not designed for urgent care but the approach was linked to lower costs in high-risk cases, likely due to better care and improved access.
The VA home-based primary care model has grown rapidly in the past decade, now operating at more than 200 medical centers, each with a full interprofessional team. House calls by physicians and NPs are part of the model, although the frequency varies across sites. Every team includes actively engaged physicians. Medicoeconomic evaluation based on tens of thousands of patient-years has shown an overall reduction in health care costs of 15% to 25% compared with historical values and prospectively modeled dollars.19,20 Home-based primary care teams are emerging across the United States at many academic centers and in the private sector.
To fund comprehensive longitudinal home care services for patients with complex health problems, the Independence at Home21 demonstration program was created under section 3024 of the Patient Protection and Affordable Care Act, using robust gain-sharing from demonstrated cost savings to reward house call teams. This multisite 3-year program started in June 2012. Rapid growth of this model is likely as private insurers have also taken an active interest in mobile medical care designs, using a variety of reward structures.
TELEMEDICINE
A debate continues over the use of communication technology in home care. It seems intuitive that “virtual visits” would be more efficient than clinicians visiting patients at home. Yet, the challenges of improving care by telemedicine alone are underestimated. For example, a recent large randomized trial, in which 33 cardiology practice sites provided at-home postdis-charge telemonitoring for HF patients, demonstrated no difference in clinical outcomes compared with patients monitored in the hospital or clinic.22
Proponents of telemedicine cite integrated models where data are managed proactively by a physician-led team that is engaged in care. This view seems valid, but other than anecdotal reports from integrated health systems, the published evidence of reduced costs is sparse. Some combination of in-person care and telemedicine is likely to be the optimal design and will emerge in coming years.
PACE: SYSTEM-BASED HOME CARE
In the 1980s, health maintenance organization risk contracts seemed a likely context for developing advanced home care models, but this did not happen. However, the Program for All-Inclusive Care of the Elderly (PACE) was tested and became a defined federal benefit in 1997. There are now nearly 100 PACE centers nationwide. PACE offers comprehensive care for people aged 55 years and older who are nursing home–eligible. The program appears to effectively help people stay home.23
An interdisciplinary team (IDT) coordinates PACE medical and social services to promote independence and quality of life. The program has been referred to as “a nursing home without walls.” Services include primary and specialty care, adult day care, case management, nursing, home health care, assistance with activities of daily living (ADL), medications, social work, rehabilitation, hospitalization, nursing facility care, nutritional support, caregiver respite, and transportation to and from the PACE adult day health center (ADHC) and medical appointments. The ADHC is the cornerstone and coordinating center for most care provided to PACE participants. Home-based care is provided in several ways:
- Home nursing care may be provided by external agencies, including skilled care, personal care, and hospice care, under contract with PACE. In Richmond, the home care manager oversees care after it is approved by the IDT. Weekly hours of care are changed often according to the participant’s need (eg, increased hours after hospital discharge and decreased hours when a family member visits and can provide more care). Home care provides assistance with ADLs and instrumental ADLs; “sitter” services are provided at the ADHC.
- The program supports home modifications and provides durable medical equipment (DME). Assessment is done by one or more team members upon enrollment and then at least every 6 months. PACE provides all DME the participant needs to remain safely in the community. At disenrollment or death, some equipment can be returned to PACE after review by the rehabilitation department.
- Primary care, basic laboratory services, and medical specialty care can be provided to the participant at home if for any reason he or she is unable to travel to the ADHC. PACE physicians make house calls to better understand patients’ living situations and needs. On-call nurses make home visits after hours or on weekends for clinical assessments, point-of-care diagnostic testing, specimen collection (stool or urine), and participant and family education on proper use of medications or equipment.
- As PACE participants approach the end of life, they transition to a palliative care model. A decision is made by the family and the IDT to discontinue attendance at the ADHC and to focus on care at home,24 allowing the participant to spend the last days or weeks in the relative comfort of home. Nurses make home visits when needed and educate families on symptom palliation.
- Additional in-home respite services can be provided to decrease caregiver burden.
- Skilled rehabilitation services are delivered either at home or in the ADHC depending on the judgment of the rehabilitation department and the IDT. The PACE site offers advanced transportation and full onsite therapy services 5 days per week.
The PACE sites become the insurers, receive defined capitation payments from Medicare and Medicaid that are adjusted for patient complexity, and assume the risk for all health care costs. Because of a 5% withholding in the capitation amount relative to projected Medicare expenses, PACE should reduce governmental costs. PACE must provide or pay for all usual Medicare and Medicaid services, and it may provide other services deemed necessary by the PACE team. Within PACE, hospital use is markedly reduced compared with conventional Medicare,25 and home care is one of several strategies employed. The PACE experience shows that care can be safely shifted from hospitals to other settings.
IMPACT ON MEDICAL EDUCATION
Since 1984, several thousand medical students; internal medicine residents; geriatric fellows; and N P, social work, and pharmacy students have participated in the VCU House Calls program and have come to see home care as a viable care model. House calls have been mandatory in the VCU School of Medicine curriculum since 2002. Qualitative evidence from these encounters demonstrates that learners value the experience and gain a better understanding of health care as a result.
Medical students’ interest in geriatrics is low,26,27 but positive, intense, or unique experiences with elders, and interactions with positive role models may improve the outlook for the specialty. The home setting gives learners an opportunity to observe the care of medically complex patients in the community, exposes the students to the team of professionals needed for comprehensive care, and enhances learners’ awareness of the challenges in providing continuity of care for this population.
We previously reported on a qualitative study of comments of second-year medical students who participated in our House Calls program.28 Students frequently noted the apparent comfort and positive attitude of the patients; the dedication, patience, compassion, commitment, and hard work of the caregivers; and the personalized and comprehensive care provided. The students identified both the challenges and the rewards for the doctors and expressed increased interest in conducting house calls in the future.
The training of competent and caring physicians and other health professionals is the goal of medical education. Fourth-year medical students were surveyed nationally regarding the qualities of a humanistic doctor.29 The students noted the importance of role models and participatory experiences. House calls provide an opportunity for learners to see health care in the community. Such experiences can create a memorable lesson in care delivery and in doctor-patient-caregiver relationships.
PALLIATIVE CARE AND HOME CARE
Ideally, care plans would gradually shift in focus from curative therapy to palliative care as patients with significant chronic illness advance in age and debility. In our geriatric practice, palliation is always important throughout extended chronic illness. Care plans progress and palliation becomes the primary focus in the final months of life. This transition may take years. Hospice referral is frequently a final step because the payment system reimburses for comprehensive team-based hospice care only when life expectancy is less than 6 months. The reason for this is economic: comprehensive team-based care is costly, and lengthening the hospice benefit as it is now structured could be prohibitively expensive. Our patients may live for years in a state of advanced debility, yet need intensive team care only at intervals. Optimally, the care model, team intensity, and related payments should flex with clinical need. This is what we have experienced by making house calls the mode of longitudinal primary care delivery, supported by our institution. Our teams help patients and families shift focus and decide when to accept hospice care; this requires more art than science and usually involves a gradual process of adaptation.
Our approach is consistent with the definition of palliative care published by the Centers for Medicare & Medicaid Services in 2008: patient- and family-centered care that optimizes quality of life by anticipating, preventing, and treating suffering. Palliative care addresses physical, intellectual, emotional, social, and spiritual needs and facilitates patient autonomy, access to information, and choice.30 Geriatric clinicians seek to help patients and families maximize quality of life and to maintain function by focusing on symptom management and clarification of patient and family goals rather than on specific diseases. This approach is applied without regard to patient age, condition, or stage of disease, and it can coexist with curative treatments. Thus it is distinguished in concept from “what we do when there is nothing more we can do.”31
In ways that are less clear when working in other care settings, home visits reveal patient goals, true rehabilitative potential, and family capacity for care-giving. Home visits take longer than office encounters, but make the provider’s job easier. By observing the patient at home, providers can better assess barriers to comfort and devise strategies to improve function, while also evaluating whether life is truly nearing the end. The home care clinician often engages in palliative care even if he or she did not initially intend to do so.
Furthermore, compared with the hospital or office setting, a home is more conducive to reasonably paced discussions about goals of care. Patients are more physically and emotionally comfortable and may talk more easily about potentially disturbing subjects. The clinician may be able to engage the patient by referring to pictures or mementos that help the patient to reflect on life values. And, a patient who is seen at home will more readily trust that the clinician places patients’ needs first. This opens the door to difficult discussions about code status, health care proxies, dialysis and ventilator support, or whether the patient would ever want to go to a hospital or a nursing home. Preferences change with time; patients ultimately feel less need to rely on ambulances and emergency care, given a timely response at home from a clinician who is familiar.32
Most dying patients are at home with their families during most of their final year of life; yet, despite studies showing that most patients prefer to die at home33–35 about 60% of all deaths still occur in the hospital.36 In our House Calls program’s experience, the percentage of patients who die at home is closer to 60.
Cherin and colleagues32 described a successful end-of-life home care program demonstrating a significant benefit to patients over usual care. The program integrated curative and palliative therapies. Similarly, Brumley and colleagues37 demonstrated that, compared with usual care, patients receiving in-home palliative care reported greater satisfaction, had fewer emergency department and hospital visits, and were more likely to die at home, with significantly lower overall costs. These findings conform to our experience. (Also see “Innovative models of home-based palliative care”)
CONCLUSION
Advanced home care with a strong medical component is an important part of the supportive and recuperative care options in the United States. For these programs to reach their full potential, we must expand on the successful in-home medical care models and create responsible financing methods that control overall costs while rewarding providers appropriately. We must broaden the application of portable and information technologies and develop an interdisciplinary workforce. These approaches will lead us toward our overall goals of optimal care at minimal cost.
- Levine SA, Boal J, Boling PA. Home care. JAMA 2003; 290:1203–1207.
- Boling PA. Home care: the first option. In:Cornwell T, Schwartz-berg JGeds. Medical Management of the Home Care Patient: Guidelines for Physicians. 4th ed. Chicago, IL: American Medical Association; 2012:1–14.
- Brickner PW, Duque Sister Teresita, Kaufman A, et al. The homebound aged: a medically unreached group. Ann Intern Med 1975; 82:1–6.
- Boling PA. Effects of policy, reimbursement, and regulation on home health care. In:Olson S. The Role of Human Factors in Home Health Care: Workshop Summary. Washington, DC: The National Academies Press; 2010:275–302.
- Basic statistics about home care. National Association for Home Care & Hospice Web site. http://www.nahc.org/facts/10HC_Stats.pdf. Updated 2010. Accessed October 11, 2012.
- Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 2006; 166:1822–1828.
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home follow-up of hospitalized elders: a randomized clinical trial. JAMA 1999; 281:613–620.
- Naylor MD, Brooten DA, Campbell RL, Maislin G, McCauley KM, Schwartz JS. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial. J Am Geriatr Soc 2004; 52:675–684.
- Shaughnessy PW, Hittle DF, Crisler KS, et al. Improving patient outcomes of home health care: findings from two demonstration trials of outcome-based quality improvement. J Am Geriatr Soc 2002; 50:1354–1364.
- Smigelski C, Hungate B, Holdren J, Goodloe L, Boling PA. Transitional model of care at VCU Medical Center—6 years’ experience. J Am Geriatr Soc 2008; 56 suppl 1:S197.
- Naylor MD. Advancing high value transitional care: the central role of nursing and its leadership. Nurs Adm Q 2012; 36:115–126.
- Holtz-Eakin D. High-cost medicare beneficiaries. Congressional Budget Office Web site. http://www.cbo.gov/sites/default/fles/cbofles/ftpdocs/63xx/doc6332/05-03-medispending.pdf. Published May 2005. Accessed October 11, 2012.
- Cryer L, Shannon SB, Van Amsterdam M, Leff B. Costs for “hospital at home” patients were 19 percent lower, with equal or better outcomes compared to similar inpatients. Health Aff (Millwood) 2012; 31:1237–1243.
- Leff B, Burton L, Mader SL, et al. Hospital at home: feasibility and outcomes of a program to provide hospital-level care at home for acutely ill older patients. Ann Intern Med 2005; 143:798–808.
- Aujesky D, Roy PM, Verschuren F, et al. Outpatient versus inpatient treatment for patients with acute pulmonary embolism: an international, open-label, randomised, non-inferiority trial [published online ahead of print June 22, 2011]. Lancet 2011; 378 9785:41–48. 10.1016/S0140-6736 1160824–6
- Büller HR, Prins MH, Lensing AWA, et al the EINSTEIN– PE Investigators. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 2012; 366:1287–1297.
- Landers SH. Why health care is going home [published online ahead of print October 20, 2010]. N Engl J Med 2010; 363:1690–1691. 10.1056/NEJMp1000401
- Counsell SR, Callahan CM, Clark DO, et al. Geriatric care management for low-income seniors: a randomized controlled trial. JAMA 2007; 298:2623–2633.
- Beales JL, Edes T. Veteran’s Affairs home based primary care. Clin Geriatr Med 2009; 25:149–154.
- Kinosian B, Edes T, Davis D, Hossain M. Financial savings of home based primary care for frail veterans with chronic disabling disease. J Am Geriatr Soc 2010; 589 (suppl s1):S3. Abstract P7.
- DeJonge KE, Taler G, Boling PA. Independence at home: community-based care for older adults with severe chronic illness. Clin Geriatr Med 2009; 25:155–169.
- Chaudhry SI, Mattera JA, Curtis JP, et al. Telemonitoring in patients with heart failure [published online ahead of print November 16, 2010]. N Engl J Med 2010; 363:2301–2309. 10.1056/NEJMoa1010029
- Wieland D, Boland R, Baskins J, Kinosian B. Five-year survival in a Program of All-inclusive Care for Elderly compared with alternative institutional and home- and community-based care [published online ahead of print March 30, 2010]. J Gerontol A Biol Sci Med Sci 2010; 65:721–726. 10.1093/gerona/glq040
- Schamp R, Tenkku L. Managed death in a PACE: pathways in present and advance directives [published online ahead of print May 30, 2006]. J Am Med Dir Assoc 2006; 7:339–344. 10.1016/j.jamda.2006.01.022
- Meret-Hanke LA. Effects of the Program of All-inclusive Care for the Elderly on hospital use [published online ahead of print July 6, 2011]. Gerontologist 2011; 51:774–785. 10.1093/geront/gnr040
- Fitzgerald JT, Wray LA, Halter JB, Williams BC, Supiano MA. Relating medical students’ knowledge, attitudes, and experience to an interest in geriatric medicine. Gerontologist 2003; 43:849–855.
- Voogt SJ, Mickus M, Santiago O, Herman SE. Attitudes, experiences, and interest in geriatrics of first-year allopathic and osteopathic medical students [published online ahead of print December 11, 2007]. J Am Geriatr Soc 2008; 56:339–344. 10.1111/j.1532-5415.2007.01541.
- Abbey L, Willett R, Selby-Penczak R, McKnight R. Social learning: medical student perceptions of geriatric house calls. Gerontol Geriatr Educ 2010; 31:149–162.
- Moyer CA, Arnold L, Quaintance J, et al. What factors create a humanistic doctor? A nationwide survey of fourth-year medical students. Acad Med 2010; 85:1800–1807.
- Centers for Medicare & Medicaid Services. Medicare and Medicaid programs: hospice conditions of participation. Federal Register 2008; 73:32204–32220.
- Meier DE, Brawley OW. Palliative care and the quality of life [published online ahead of print June 13, 2011]. J Clin Oncol 2011; 29:2750–2752. 10.1200/JCO.2011.35.9729
- Cherin DA, Enguidanos SM, Jamison P. Physicians as medical center “extenders” in end-of-life care: physician home visits as the lynch pin in creating an end-of-life care system. Home Health Care Serv Q 2004; 23:41–53.
- Hays JC, Galanos AN, Palmer TA, McQuoid DR, Flint EP. Preference for place of death in a continuing care retirement community. Gerontologist 2001; 41:123–128.
- Karlsen S, Addington-Hall J. How do cancer patients who die at home differ from those who die elsewhere? Palliat Med 1998; 12:279–286.
- Townsend J, Frank AO, Fermont D, et al. Terminal cancer care and patients’ preference for place of death: a prospective study. BMJ 1990; 301:415–417.
- Weitzen S, Teno JM, Fennell M, Mor V. Factors associated with site of death: a national study of where people die. Med Care 2003; 41:323–335.
- Brumley R, Enguidanos S, Jamison P, et al. Increased satisfaction with care and lower costs: results of a randomized trial of in-home palliative care. J Am Geriatr Soc 2007; 55:993–1000.
- Levine SA, Boal J, Boling PA. Home care. JAMA 2003; 290:1203–1207.
- Boling PA. Home care: the first option. In:Cornwell T, Schwartz-berg JGeds. Medical Management of the Home Care Patient: Guidelines for Physicians. 4th ed. Chicago, IL: American Medical Association; 2012:1–14.
- Brickner PW, Duque Sister Teresita, Kaufman A, et al. The homebound aged: a medically unreached group. Ann Intern Med 1975; 82:1–6.
- Boling PA. Effects of policy, reimbursement, and regulation on home health care. In:Olson S. The Role of Human Factors in Home Health Care: Workshop Summary. Washington, DC: The National Academies Press; 2010:275–302.
- Basic statistics about home care. National Association for Home Care & Hospice Web site. http://www.nahc.org/facts/10HC_Stats.pdf. Updated 2010. Accessed October 11, 2012.
- Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 2006; 166:1822–1828.
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home follow-up of hospitalized elders: a randomized clinical trial. JAMA 1999; 281:613–620.
- Naylor MD, Brooten DA, Campbell RL, Maislin G, McCauley KM, Schwartz JS. Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial. J Am Geriatr Soc 2004; 52:675–684.
- Shaughnessy PW, Hittle DF, Crisler KS, et al. Improving patient outcomes of home health care: findings from two demonstration trials of outcome-based quality improvement. J Am Geriatr Soc 2002; 50:1354–1364.
- Smigelski C, Hungate B, Holdren J, Goodloe L, Boling PA. Transitional model of care at VCU Medical Center—6 years’ experience. J Am Geriatr Soc 2008; 56 suppl 1:S197.
- Naylor MD. Advancing high value transitional care: the central role of nursing and its leadership. Nurs Adm Q 2012; 36:115–126.
- Holtz-Eakin D. High-cost medicare beneficiaries. Congressional Budget Office Web site. http://www.cbo.gov/sites/default/fles/cbofles/ftpdocs/63xx/doc6332/05-03-medispending.pdf. Published May 2005. Accessed October 11, 2012.
- Cryer L, Shannon SB, Van Amsterdam M, Leff B. Costs for “hospital at home” patients were 19 percent lower, with equal or better outcomes compared to similar inpatients. Health Aff (Millwood) 2012; 31:1237–1243.
- Leff B, Burton L, Mader SL, et al. Hospital at home: feasibility and outcomes of a program to provide hospital-level care at home for acutely ill older patients. Ann Intern Med 2005; 143:798–808.
- Aujesky D, Roy PM, Verschuren F, et al. Outpatient versus inpatient treatment for patients with acute pulmonary embolism: an international, open-label, randomised, non-inferiority trial [published online ahead of print June 22, 2011]. Lancet 2011; 378 9785:41–48. 10.1016/S0140-6736 1160824–6
- Büller HR, Prins MH, Lensing AWA, et al the EINSTEIN– PE Investigators. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 2012; 366:1287–1297.
- Landers SH. Why health care is going home [published online ahead of print October 20, 2010]. N Engl J Med 2010; 363:1690–1691. 10.1056/NEJMp1000401
- Counsell SR, Callahan CM, Clark DO, et al. Geriatric care management for low-income seniors: a randomized controlled trial. JAMA 2007; 298:2623–2633.
- Beales JL, Edes T. Veteran’s Affairs home based primary care. Clin Geriatr Med 2009; 25:149–154.
- Kinosian B, Edes T, Davis D, Hossain M. Financial savings of home based primary care for frail veterans with chronic disabling disease. J Am Geriatr Soc 2010; 589 (suppl s1):S3. Abstract P7.
- DeJonge KE, Taler G, Boling PA. Independence at home: community-based care for older adults with severe chronic illness. Clin Geriatr Med 2009; 25:155–169.
- Chaudhry SI, Mattera JA, Curtis JP, et al. Telemonitoring in patients with heart failure [published online ahead of print November 16, 2010]. N Engl J Med 2010; 363:2301–2309. 10.1056/NEJMoa1010029
- Wieland D, Boland R, Baskins J, Kinosian B. Five-year survival in a Program of All-inclusive Care for Elderly compared with alternative institutional and home- and community-based care [published online ahead of print March 30, 2010]. J Gerontol A Biol Sci Med Sci 2010; 65:721–726. 10.1093/gerona/glq040
- Schamp R, Tenkku L. Managed death in a PACE: pathways in present and advance directives [published online ahead of print May 30, 2006]. J Am Med Dir Assoc 2006; 7:339–344. 10.1016/j.jamda.2006.01.022
- Meret-Hanke LA. Effects of the Program of All-inclusive Care for the Elderly on hospital use [published online ahead of print July 6, 2011]. Gerontologist 2011; 51:774–785. 10.1093/geront/gnr040
- Fitzgerald JT, Wray LA, Halter JB, Williams BC, Supiano MA. Relating medical students’ knowledge, attitudes, and experience to an interest in geriatric medicine. Gerontologist 2003; 43:849–855.
- Voogt SJ, Mickus M, Santiago O, Herman SE. Attitudes, experiences, and interest in geriatrics of first-year allopathic and osteopathic medical students [published online ahead of print December 11, 2007]. J Am Geriatr Soc 2008; 56:339–344. 10.1111/j.1532-5415.2007.01541.
- Abbey L, Willett R, Selby-Penczak R, McKnight R. Social learning: medical student perceptions of geriatric house calls. Gerontol Geriatr Educ 2010; 31:149–162.
- Moyer CA, Arnold L, Quaintance J, et al. What factors create a humanistic doctor? A nationwide survey of fourth-year medical students. Acad Med 2010; 85:1800–1807.
- Centers for Medicare & Medicaid Services. Medicare and Medicaid programs: hospice conditions of participation. Federal Register 2008; 73:32204–32220.
- Meier DE, Brawley OW. Palliative care and the quality of life [published online ahead of print June 13, 2011]. J Clin Oncol 2011; 29:2750–2752. 10.1200/JCO.2011.35.9729
- Cherin DA, Enguidanos SM, Jamison P. Physicians as medical center “extenders” in end-of-life care: physician home visits as the lynch pin in creating an end-of-life care system. Home Health Care Serv Q 2004; 23:41–53.
- Hays JC, Galanos AN, Palmer TA, McQuoid DR, Flint EP. Preference for place of death in a continuing care retirement community. Gerontologist 2001; 41:123–128.
- Karlsen S, Addington-Hall J. How do cancer patients who die at home differ from those who die elsewhere? Palliat Med 1998; 12:279–286.
- Townsend J, Frank AO, Fermont D, et al. Terminal cancer care and patients’ preference for place of death: a prospective study. BMJ 1990; 301:415–417.
- Weitzen S, Teno JM, Fennell M, Mor V. Factors associated with site of death: a national study of where people die. Med Care 2003; 41:323–335.
- Brumley R, Enguidanos S, Jamison P, et al. Increased satisfaction with care and lower costs: results of a randomized trial of in-home palliative care. J Am Geriatr Soc 2007; 55:993–1000.