User login
Revision total knee arthroplasty (TKA) is frequently complicated by bone loss and ligament instability, necessitating specialized implants to increase constraint and transmit forces away from the joint surface. Femoral stems are commonly used to enhance fixation and distribute force from the condyles to the metaphysis or diaphysis, to higher-quality bone capable of sustaining the forces at the knee joint.
Modular implants are now commonplace in revision surgery, because they allow intraoperative customization of the implant to the patient’s anatomy, degree of bone loss, and need for metaphyseal or diaphyseal fixation. However, these advantages are not without a downside. The modular junction introduces potential weaknesses in the implant, which may lead to early failure.
We report a case of loosening of a Triathlon TS (Stryker) femoral component that was not evident on preoperative radiographs. To our knowledge, this complication has not been reported with this particular revision knee system. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 56-year-old woman underwent 2-stage revision left TKA secondary to infection at an outside institution. She had undergone 17 prior knee surgeries with multiple revisions prior to this most recent revision surgery. A constrained implant was used at her last reimplantation secondary to ligamentous laxity after extensive débridement for infection. A Triathlon TS revision knee system with cemented stemmed tibial and femoral components was implanted; stems designed for uncemented fixation were cemented. She had a history of a quadriceps tendon tear, which was repaired prior to her revision, and quadricepsplasty was performed at the time of revision.
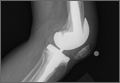
Seven years after this revision surgery, the patient presented to our clinic with progressive global instability, occasional effusions, and 2 documented episodes of frank dislocation. On examination, she was unstable in flexion and extension. Her extensor mechanism was intact, although with 7º active lag. She had a palpable quadriceps tendon defect. Her passive range of motion was 0º to 130º. Her active range of motion was 7º to 130º. Her erythrocyte sedimentation rate and C-reactive protein levels were within normal limits, and aspiration was negative for infection. Radiographs showed apparently well-fixed components with cemented femoral and tibial stems (Figures 1A, 1B).

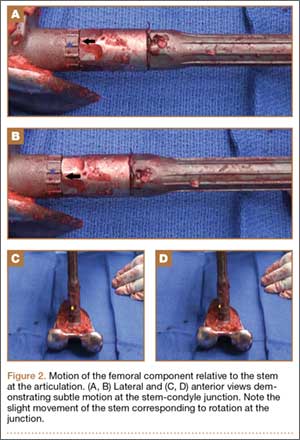
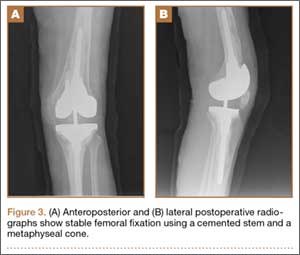
The patient underwent revision surgery for global instability with the surgical goal to upsize the polyethylene insert and advance the quadriceps to improve stability. In the operating room, a defect in the quadriceps mechanism was seen between the vastus medialis obliquus (VMO) and the patella, as well as a large effusion. Upon removal of the polyethylene insert, the tibial and patellar components were examined and found to be well fixed. The femoral component was grossly loose. On closer inspection, the condylar portion was found to be rotating in the axial plane freely on the well-fixed cemented stem in the femoral canal (Figures 2A-2D). The entire femoral component was removed with some difficulty because the well-fixed uncemented stem design was cemented in place. This required a small, anterior episiotomy of the femur. Reconstruction of the femur was performed using a trabecular metal cone, a cemented stem, and condylar component with distal and posterior augments (Figures 3A, 3B). A shorter, thinner stem was implanted and cemented into the previous cement mantle. A 19-mm constrained polyethylene liner was selected (the prior liner was 13 mm), which gave adequate stability with range of motion 0º to 130º. The VMO was advanced approximately 1.5 cm at the time of closure of the arthrotomy. The patient was implanted with the same Triathlon TS system, because the tibial component was well fixed, well positioned, and did not require revision.
Discussion
The need and use of stemmed, modular femoral components for revision TKA is neither questioned nor a novel concept in arthroplasty.1 Femoral bone defects encountered in revision arthroplasty generally lack sufficient cortical integrity to support an unstemmed component. Biomechanical analyses have reliably demonstrated improved initial stability and reduced relative motion provided by femoral stem extension.2,3 Correspondingly, significant translational and rotational movements of the femoral component when disconnected from the stem presumably correspond with clinical observations of instability.3 We report a unique case of failure of the modular junction of a stemmed femoral component in revision TKA that was not readily apparent on plain radiographs.
Dissociation of a cemented stem from the condylar portion of the component has been described at our institution with a different implant design.4 To our knowledge, we describe the first report of failure at the modular junction of the Triathlon TS femoral component.
Interestingly, relative motion has been shown to increase with increasing flexion in a biomechanical study2 using the same Triathlon TS system. The authors of that study found they were unable to complete testing at flexion greater than 30º because, absent the stabilizing influence of surrounding ligament and muscle, the sample deformation was so significant that it caused fracture.2 In the case of our patient, the incompetence of her extensor mechanism likely resulted in increased forces transmitted through the implant than might be expected in more physiologic circumstances. This higher stress may account in part for the failure of the implant at the known weakest point, the stem-condyle modular junction.
Modular implants are routinely used, given the variability of scenarios encountered in revision surgery and the need for customization to provide the best approximation of physiologic functioning of the joint. However, modular components introduce junctional points, which are potential points of failure. Stresses on the femoral component occur in multiple dimensions besides the axial loading and medial-lateral, anterior-posterior rocking seen with the tibial component. The maximum stress is observed at the distal-most aspect of the stiffest or most well-fixed components, in this case, the articulation between the cemented stem and the cemented condylar component. Poor distal femoral fixation compounds the problem.
Numerous case reports have documented such failures in other knee systems. Issack and colleagues5 described 2 cases of fracture through the taper lock between the femoral component and the stem extension in the Optetrak stemmed-constrained condylar knee prosthesis (Exactech). Westrich and colleagues6 reported disengagement of the locking bolt of the Insall-Burstein II Constrained Condylar Knee (Zimmer) leading to failure. Lim and colleagues4 reported stem-condyle junctional failure of the Total Condylar III (DePuy, Johnson & Johnson) due to locking-screw failure. Butt and colleagues7 reported a case of failure at the femoral component–stem junction caused by screw breakage. All of these cases involved failure at the condylar-stem junction that was readily apparent on routine preoperative imaging.
Our case is noteworthy because there was no preoperative radiographic evidence that the components were loose or the junction had failed. As with many revision systems observed by Fehring and colleagues,8 determination of fixation is often based on the appearance of the stem because the distal femoral interfaces may be obscured by the intercondylar box. This suggests that a loose component at the stem-condylar junction could easily be overlooked and not appropriately revised based on imaging alone. A solution for achieving stability at the time of revision surgery is to obtain good distal bone apposition and fixation. In this case, a cemented stem with a metaphyseal cone was used for femoral fixation (Figures 3A, 3B).
While long-term, abnormally high stress transmitted through the modular junction may account for the implant’s failure, to our knowledge, this is the first report of its kind related to this particular implant. If quadriceps weakness contributed to this failure, it is worth considering that quadriceps weakness is common after TKA and may persist without appropriate rehabilitation and activity. Furthermore, the lack of evidence on plain radiographs makes this particular form of failure very difficult to screen. A high degree of suspicion for loosening should be maintained in patients with pain and instability after revision TKA with this implant as well as with other modular revision knee systems.
1. Kurtz S, Mowat F, Ong K, Chan N, Lau E, Halpern M. Prevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002. J Bone Joint Surg Am. 2005;87(7):1487-1497.
2. Conlisk N, Gray H, Pankaj P, Howie CR. The influence of stem length and fixation on initial femoral component stability in revision total knee replacement. Bone Joint Res. 2012;1(11):281-288.
3. van Loon CJ, Kyriazopoulos A, Verdonschot N, de Waal Malefijt MC, Huiskes R, Buma P. The role of femoral stem extension in total knee arthroplasty. Clin Orthop Relat Res. 2000;(378):282-289.
4. Lim LA, Trousdale RT, Berry DJ, Hanssen AD. Failure of the stem-condyle junction of a modular femoral stem in revision total knee arthroplasty: a report of five cases. J Arthroplasty. 2001;16(1):128-132.
5. Issack PS, Cottrell JM, Delgado S, Wright TM, Sculco TP, Su EP. Failure at the taper lock of a modular stemmed femoral implant in revision knee arthroplasty. A report of two cases and a retrieval analysis. J Bone Joint Surg Am. 2007;89(10):2271-2274.
6. Westrich GH, Hidaka C, Windsor RE. Disengagement of a locking screw from a modular stem in revision total knee arthroplasty. A report of three cases. J Bone Joint Surg Am. 1997;79(2):254-258.
7. Butt AJ, Shaikh AH, Cameron HU. Coupling failure between stem and femoral component in a constrained revision total knee arthroplasty. J Coll Physicians Surg Pak. 2013;23(2):162-163.
8. Fehring TK, Odum S, Olekson C, Griffin WL, Mason JB, McCoy TH. Stem fixation in revision total knee arthroplasty: a comparative analysis. Clin Orthop Relat Res. 2003;(416):217-224.
Revision total knee arthroplasty (TKA) is frequently complicated by bone loss and ligament instability, necessitating specialized implants to increase constraint and transmit forces away from the joint surface. Femoral stems are commonly used to enhance fixation and distribute force from the condyles to the metaphysis or diaphysis, to higher-quality bone capable of sustaining the forces at the knee joint.
Modular implants are now commonplace in revision surgery, because they allow intraoperative customization of the implant to the patient’s anatomy, degree of bone loss, and need for metaphyseal or diaphyseal fixation. However, these advantages are not without a downside. The modular junction introduces potential weaknesses in the implant, which may lead to early failure.
We report a case of loosening of a Triathlon TS (Stryker) femoral component that was not evident on preoperative radiographs. To our knowledge, this complication has not been reported with this particular revision knee system. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 56-year-old woman underwent 2-stage revision left TKA secondary to infection at an outside institution. She had undergone 17 prior knee surgeries with multiple revisions prior to this most recent revision surgery. A constrained implant was used at her last reimplantation secondary to ligamentous laxity after extensive débridement for infection. A Triathlon TS revision knee system with cemented stemmed tibial and femoral components was implanted; stems designed for uncemented fixation were cemented. She had a history of a quadriceps tendon tear, which was repaired prior to her revision, and quadricepsplasty was performed at the time of revision.
Seven years after this revision surgery, the patient presented to our clinic with progressive global instability, occasional effusions, and 2 documented episodes of frank dislocation. On examination, she was unstable in flexion and extension. Her extensor mechanism was intact, although with 7º active lag. She had a palpable quadriceps tendon defect. Her passive range of motion was 0º to 130º. Her active range of motion was 7º to 130º. Her erythrocyte sedimentation rate and C-reactive protein levels were within normal limits, and aspiration was negative for infection. Radiographs showed apparently well-fixed components with cemented femoral and tibial stems (Figures 1A, 1B).
The patient underwent revision surgery for global instability with the surgical goal to upsize the polyethylene insert and advance the quadriceps to improve stability. In the operating room, a defect in the quadriceps mechanism was seen between the vastus medialis obliquus (VMO) and the patella, as well as a large effusion. Upon removal of the polyethylene insert, the tibial and patellar components were examined and found to be well fixed. The femoral component was grossly loose. On closer inspection, the condylar portion was found to be rotating in the axial plane freely on the well-fixed cemented stem in the femoral canal (Figures 2A-2D). The entire femoral component was removed with some difficulty because the well-fixed uncemented stem design was cemented in place. This required a small, anterior episiotomy of the femur. Reconstruction of the femur was performed using a trabecular metal cone, a cemented stem, and condylar component with distal and posterior augments (Figures 3A, 3B). A shorter, thinner stem was implanted and cemented into the previous cement mantle. A 19-mm constrained polyethylene liner was selected (the prior liner was 13 mm), which gave adequate stability with range of motion 0º to 130º. The VMO was advanced approximately 1.5 cm at the time of closure of the arthrotomy. The patient was implanted with the same Triathlon TS system, because the tibial component was well fixed, well positioned, and did not require revision.
Discussion
The need and use of stemmed, modular femoral components for revision TKA is neither questioned nor a novel concept in arthroplasty.1 Femoral bone defects encountered in revision arthroplasty generally lack sufficient cortical integrity to support an unstemmed component. Biomechanical analyses have reliably demonstrated improved initial stability and reduced relative motion provided by femoral stem extension.2,3 Correspondingly, significant translational and rotational movements of the femoral component when disconnected from the stem presumably correspond with clinical observations of instability.3 We report a unique case of failure of the modular junction of a stemmed femoral component in revision TKA that was not readily apparent on plain radiographs.
Dissociation of a cemented stem from the condylar portion of the component has been described at our institution with a different implant design.4 To our knowledge, we describe the first report of failure at the modular junction of the Triathlon TS femoral component.
Interestingly, relative motion has been shown to increase with increasing flexion in a biomechanical study2 using the same Triathlon TS system. The authors of that study found they were unable to complete testing at flexion greater than 30º because, absent the stabilizing influence of surrounding ligament and muscle, the sample deformation was so significant that it caused fracture.2 In the case of our patient, the incompetence of her extensor mechanism likely resulted in increased forces transmitted through the implant than might be expected in more physiologic circumstances. This higher stress may account in part for the failure of the implant at the known weakest point, the stem-condyle modular junction.
Modular implants are routinely used, given the variability of scenarios encountered in revision surgery and the need for customization to provide the best approximation of physiologic functioning of the joint. However, modular components introduce junctional points, which are potential points of failure. Stresses on the femoral component occur in multiple dimensions besides the axial loading and medial-lateral, anterior-posterior rocking seen with the tibial component. The maximum stress is observed at the distal-most aspect of the stiffest or most well-fixed components, in this case, the articulation between the cemented stem and the cemented condylar component. Poor distal femoral fixation compounds the problem.
Numerous case reports have documented such failures in other knee systems. Issack and colleagues5 described 2 cases of fracture through the taper lock between the femoral component and the stem extension in the Optetrak stemmed-constrained condylar knee prosthesis (Exactech). Westrich and colleagues6 reported disengagement of the locking bolt of the Insall-Burstein II Constrained Condylar Knee (Zimmer) leading to failure. Lim and colleagues4 reported stem-condyle junctional failure of the Total Condylar III (DePuy, Johnson & Johnson) due to locking-screw failure. Butt and colleagues7 reported a case of failure at the femoral component–stem junction caused by screw breakage. All of these cases involved failure at the condylar-stem junction that was readily apparent on routine preoperative imaging.
Our case is noteworthy because there was no preoperative radiographic evidence that the components were loose or the junction had failed. As with many revision systems observed by Fehring and colleagues,8 determination of fixation is often based on the appearance of the stem because the distal femoral interfaces may be obscured by the intercondylar box. This suggests that a loose component at the stem-condylar junction could easily be overlooked and not appropriately revised based on imaging alone. A solution for achieving stability at the time of revision surgery is to obtain good distal bone apposition and fixation. In this case, a cemented stem with a metaphyseal cone was used for femoral fixation (Figures 3A, 3B).
While long-term, abnormally high stress transmitted through the modular junction may account for the implant’s failure, to our knowledge, this is the first report of its kind related to this particular implant. If quadriceps weakness contributed to this failure, it is worth considering that quadriceps weakness is common after TKA and may persist without appropriate rehabilitation and activity. Furthermore, the lack of evidence on plain radiographs makes this particular form of failure very difficult to screen. A high degree of suspicion for loosening should be maintained in patients with pain and instability after revision TKA with this implant as well as with other modular revision knee systems.
Revision total knee arthroplasty (TKA) is frequently complicated by bone loss and ligament instability, necessitating specialized implants to increase constraint and transmit forces away from the joint surface. Femoral stems are commonly used to enhance fixation and distribute force from the condyles to the metaphysis or diaphysis, to higher-quality bone capable of sustaining the forces at the knee joint.
Modular implants are now commonplace in revision surgery, because they allow intraoperative customization of the implant to the patient’s anatomy, degree of bone loss, and need for metaphyseal or diaphyseal fixation. However, these advantages are not without a downside. The modular junction introduces potential weaknesses in the implant, which may lead to early failure.
We report a case of loosening of a Triathlon TS (Stryker) femoral component that was not evident on preoperative radiographs. To our knowledge, this complication has not been reported with this particular revision knee system. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A 56-year-old woman underwent 2-stage revision left TKA secondary to infection at an outside institution. She had undergone 17 prior knee surgeries with multiple revisions prior to this most recent revision surgery. A constrained implant was used at her last reimplantation secondary to ligamentous laxity after extensive débridement for infection. A Triathlon TS revision knee system with cemented stemmed tibial and femoral components was implanted; stems designed for uncemented fixation were cemented. She had a history of a quadriceps tendon tear, which was repaired prior to her revision, and quadricepsplasty was performed at the time of revision.
Seven years after this revision surgery, the patient presented to our clinic with progressive global instability, occasional effusions, and 2 documented episodes of frank dislocation. On examination, she was unstable in flexion and extension. Her extensor mechanism was intact, although with 7º active lag. She had a palpable quadriceps tendon defect. Her passive range of motion was 0º to 130º. Her active range of motion was 7º to 130º. Her erythrocyte sedimentation rate and C-reactive protein levels were within normal limits, and aspiration was negative for infection. Radiographs showed apparently well-fixed components with cemented femoral and tibial stems (Figures 1A, 1B).
The patient underwent revision surgery for global instability with the surgical goal to upsize the polyethylene insert and advance the quadriceps to improve stability. In the operating room, a defect in the quadriceps mechanism was seen between the vastus medialis obliquus (VMO) and the patella, as well as a large effusion. Upon removal of the polyethylene insert, the tibial and patellar components were examined and found to be well fixed. The femoral component was grossly loose. On closer inspection, the condylar portion was found to be rotating in the axial plane freely on the well-fixed cemented stem in the femoral canal (Figures 2A-2D). The entire femoral component was removed with some difficulty because the well-fixed uncemented stem design was cemented in place. This required a small, anterior episiotomy of the femur. Reconstruction of the femur was performed using a trabecular metal cone, a cemented stem, and condylar component with distal and posterior augments (Figures 3A, 3B). A shorter, thinner stem was implanted and cemented into the previous cement mantle. A 19-mm constrained polyethylene liner was selected (the prior liner was 13 mm), which gave adequate stability with range of motion 0º to 130º. The VMO was advanced approximately 1.5 cm at the time of closure of the arthrotomy. The patient was implanted with the same Triathlon TS system, because the tibial component was well fixed, well positioned, and did not require revision.
Discussion
The need and use of stemmed, modular femoral components for revision TKA is neither questioned nor a novel concept in arthroplasty.1 Femoral bone defects encountered in revision arthroplasty generally lack sufficient cortical integrity to support an unstemmed component. Biomechanical analyses have reliably demonstrated improved initial stability and reduced relative motion provided by femoral stem extension.2,3 Correspondingly, significant translational and rotational movements of the femoral component when disconnected from the stem presumably correspond with clinical observations of instability.3 We report a unique case of failure of the modular junction of a stemmed femoral component in revision TKA that was not readily apparent on plain radiographs.
Dissociation of a cemented stem from the condylar portion of the component has been described at our institution with a different implant design.4 To our knowledge, we describe the first report of failure at the modular junction of the Triathlon TS femoral component.
Interestingly, relative motion has been shown to increase with increasing flexion in a biomechanical study2 using the same Triathlon TS system. The authors of that study found they were unable to complete testing at flexion greater than 30º because, absent the stabilizing influence of surrounding ligament and muscle, the sample deformation was so significant that it caused fracture.2 In the case of our patient, the incompetence of her extensor mechanism likely resulted in increased forces transmitted through the implant than might be expected in more physiologic circumstances. This higher stress may account in part for the failure of the implant at the known weakest point, the stem-condyle modular junction.
Modular implants are routinely used, given the variability of scenarios encountered in revision surgery and the need for customization to provide the best approximation of physiologic functioning of the joint. However, modular components introduce junctional points, which are potential points of failure. Stresses on the femoral component occur in multiple dimensions besides the axial loading and medial-lateral, anterior-posterior rocking seen with the tibial component. The maximum stress is observed at the distal-most aspect of the stiffest or most well-fixed components, in this case, the articulation between the cemented stem and the cemented condylar component. Poor distal femoral fixation compounds the problem.
Numerous case reports have documented such failures in other knee systems. Issack and colleagues5 described 2 cases of fracture through the taper lock between the femoral component and the stem extension in the Optetrak stemmed-constrained condylar knee prosthesis (Exactech). Westrich and colleagues6 reported disengagement of the locking bolt of the Insall-Burstein II Constrained Condylar Knee (Zimmer) leading to failure. Lim and colleagues4 reported stem-condyle junctional failure of the Total Condylar III (DePuy, Johnson & Johnson) due to locking-screw failure. Butt and colleagues7 reported a case of failure at the femoral component–stem junction caused by screw breakage. All of these cases involved failure at the condylar-stem junction that was readily apparent on routine preoperative imaging.
Our case is noteworthy because there was no preoperative radiographic evidence that the components were loose or the junction had failed. As with many revision systems observed by Fehring and colleagues,8 determination of fixation is often based on the appearance of the stem because the distal femoral interfaces may be obscured by the intercondylar box. This suggests that a loose component at the stem-condylar junction could easily be overlooked and not appropriately revised based on imaging alone. A solution for achieving stability at the time of revision surgery is to obtain good distal bone apposition and fixation. In this case, a cemented stem with a metaphyseal cone was used for femoral fixation (Figures 3A, 3B).
While long-term, abnormally high stress transmitted through the modular junction may account for the implant’s failure, to our knowledge, this is the first report of its kind related to this particular implant. If quadriceps weakness contributed to this failure, it is worth considering that quadriceps weakness is common after TKA and may persist without appropriate rehabilitation and activity. Furthermore, the lack of evidence on plain radiographs makes this particular form of failure very difficult to screen. A high degree of suspicion for loosening should be maintained in patients with pain and instability after revision TKA with this implant as well as with other modular revision knee systems.
1. Kurtz S, Mowat F, Ong K, Chan N, Lau E, Halpern M. Prevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002. J Bone Joint Surg Am. 2005;87(7):1487-1497.
2. Conlisk N, Gray H, Pankaj P, Howie CR. The influence of stem length and fixation on initial femoral component stability in revision total knee replacement. Bone Joint Res. 2012;1(11):281-288.
3. van Loon CJ, Kyriazopoulos A, Verdonschot N, de Waal Malefijt MC, Huiskes R, Buma P. The role of femoral stem extension in total knee arthroplasty. Clin Orthop Relat Res. 2000;(378):282-289.
4. Lim LA, Trousdale RT, Berry DJ, Hanssen AD. Failure of the stem-condyle junction of a modular femoral stem in revision total knee arthroplasty: a report of five cases. J Arthroplasty. 2001;16(1):128-132.
5. Issack PS, Cottrell JM, Delgado S, Wright TM, Sculco TP, Su EP. Failure at the taper lock of a modular stemmed femoral implant in revision knee arthroplasty. A report of two cases and a retrieval analysis. J Bone Joint Surg Am. 2007;89(10):2271-2274.
6. Westrich GH, Hidaka C, Windsor RE. Disengagement of a locking screw from a modular stem in revision total knee arthroplasty. A report of three cases. J Bone Joint Surg Am. 1997;79(2):254-258.
7. Butt AJ, Shaikh AH, Cameron HU. Coupling failure between stem and femoral component in a constrained revision total knee arthroplasty. J Coll Physicians Surg Pak. 2013;23(2):162-163.
8. Fehring TK, Odum S, Olekson C, Griffin WL, Mason JB, McCoy TH. Stem fixation in revision total knee arthroplasty: a comparative analysis. Clin Orthop Relat Res. 2003;(416):217-224.
1. Kurtz S, Mowat F, Ong K, Chan N, Lau E, Halpern M. Prevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002. J Bone Joint Surg Am. 2005;87(7):1487-1497.
2. Conlisk N, Gray H, Pankaj P, Howie CR. The influence of stem length and fixation on initial femoral component stability in revision total knee replacement. Bone Joint Res. 2012;1(11):281-288.
3. van Loon CJ, Kyriazopoulos A, Verdonschot N, de Waal Malefijt MC, Huiskes R, Buma P. The role of femoral stem extension in total knee arthroplasty. Clin Orthop Relat Res. 2000;(378):282-289.
4. Lim LA, Trousdale RT, Berry DJ, Hanssen AD. Failure of the stem-condyle junction of a modular femoral stem in revision total knee arthroplasty: a report of five cases. J Arthroplasty. 2001;16(1):128-132.
5. Issack PS, Cottrell JM, Delgado S, Wright TM, Sculco TP, Su EP. Failure at the taper lock of a modular stemmed femoral implant in revision knee arthroplasty. A report of two cases and a retrieval analysis. J Bone Joint Surg Am. 2007;89(10):2271-2274.
6. Westrich GH, Hidaka C, Windsor RE. Disengagement of a locking screw from a modular stem in revision total knee arthroplasty. A report of three cases. J Bone Joint Surg Am. 1997;79(2):254-258.
7. Butt AJ, Shaikh AH, Cameron HU. Coupling failure between stem and femoral component in a constrained revision total knee arthroplasty. J Coll Physicians Surg Pak. 2013;23(2):162-163.
8. Fehring TK, Odum S, Olekson C, Griffin WL, Mason JB, McCoy TH. Stem fixation in revision total knee arthroplasty: a comparative analysis. Clin Orthop Relat Res. 2003;(416):217-224.