User login
Good evidence supports the use of surgery for carpal tunnel syndrome over nonsurgical therapies such as wrist splints, nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, occupational therapy, local steroid injections, work modification, and oral vitamin B6 (Grade of Recommendation: A, based on extrapolation from a systematic review of 1 randomized controlled trial [RCT], 1 additional recent RCT, and 2 cohort studies). Surgery is likely worth the extra costs when conservative therapy (up to 3 months) fails to improve symptoms and return of function, because delayed surgery is as successful as surgery performed shortly after diagnosis. Closed endoscopic release and open release surgery are equally effective therapies for controlling symptoms (Grade of Recommendation: C, based on extrapolation from a systematic review of RCTs). However, whether endoscopic release results in more rapid regain of function and return to work is unclear.
See the Patient Information at the end of this article.
Evidence summary
A recent Cochrane review based on only 1 RCT of 22 patients published in 1964 concluded that surgical treatment of carpal tunnel syndrome appears to be more effective than wrist splinting.1 A well-designed RCT of 176 patients published since that Cochrane review stated that with regard to overall improvement of symptoms and function status, surgical treatment of carpal tunnel syndrome was more effective than wrist splinting 18 months posttreatment.2 The investigators found that surgery resulted in worse short-term outcomes at 1 month follow-up (29% vs 42% success), but by 3 months the improvement in all outcomes was greater in the surgery group (80% vs 54% success). The number needed to treat (NNT) over 18 months was only 2 patients in the treatment-received (per protocol) analysis (92% vs 37% success) and 7 in the intention-to-treat analysis (90% vs 75% success). Patients in the conservative treatment group who underwent surgery after splinting had failed had a higher success rate after 18 months follow-up than patients who did not have surgery (94% vs 62% success rate; NNT = 3).
One cohort study of 90 patients concluded that with respect to symptom control and return to function, open release surgery was as effective as local steroid injection at 1 month follow-up.3 However, at 4 to 6 months after the operation, surgery patients were found to have significantly improved symptom and function scores, with continued improvement compared with patients who received the steroid injection. One other cohort study of 429 patients found that surgery (open or closed endoscopic) was more effective with respect to symptom relief and functional status than various nonsurgical therapies (NSAIDs, splints, physical or occupational therapy, local steroid injections, work modification, or vitamin B6) at 30 months follow-up.4 In both cohort studies, the patients’ pretreatment symptom and functioning scores were worse in the surgery group than in the nonsurgical group. The investigators in the first study3 did not report controlling for these scores. In the second study,4 the authors controlled for functional status scores, but not for symptom severity.
One recent systematic review of 14 RCTs comparing types of surgical therapies for carpal tunnel syndrome concluded that none of the alternative surgical procedures, including closed endoscopic release, appeared to give better symptom relief than open release; and that the evidence is conflicting as to whether endoscopic release results in earlier return to work or improved level of function.5
Recommendations from others
The American Society of Plastic and Reconstructive Surgeons recommends surgical release in the following situations6: (1) failed or incomplete conservative therapy; (2) motor weakness or thenar atrophy; (3) lumbrical pattern symptoms (occur when the metacarpophalangeal joints are held at 90 degrees, eg, driving, letter writing, holding a magazine, pinching, using a small tool); (4) severe pattern on electrical studies (not defined); (5) space-occupying lesions requiring excision; (6) acute carpal tunnel syndrome with symptoms lasting longer than 6 to 8 hours; and (7) progressive or severe symptoms lasting longer than 12 months. The Society did not recommend one surgical procedure over another.
Maureen O’Reilly Brown, MD, MPH
Swedish Family Medicine Residency Program Seattle, Washington
In my practice, many patients have carpal tunnel syndrome and we regularly struggle with the question of whether and when to suggest surgical consultation. This review will make that struggle easier. With at least 33% of cases responding to splinting alone, an initial trial of conservative treatment seems appropriate for most patients. However, early surgical referral when a conservative approach has failed can now be easily justified, given the 90% or better success rate with surgery. The authors also include guidelines from the American Society of Plastic and Reconstructive Surgeons, which may be helpful in selecting which patients should go directly to surgical release.
Patient Information
What is carpal tunnel syndrome?
Carpal tunnel syndrome is felt as pain, tingling, a burning sensation, or loss of sensation that occurs throughout all or part of the hand. These symptoms may be worse at night and can wake you from sleep. You may feel the pain in just the hand, or it may travel up the arm.
How it’s diagnosed
Carpal tunnel syndrome can be challenging to diagnose.
Your doctor will ask you to describe your symptoms and may ask you to perform specific motions with your hand or wrist to see how they affect your symptoms.
Your doctor may arrange for a nerve conduction study—a test to determine how well the nerves in your hand are working. The test can detect if the pressure on the nerve is enough to affect how well it works.
How it’s treated
Your doctor may ask you to wear wrist splints at night or during work, and may advise you to reduce those activities that make the problem worse. Steroid injections into the carpal tunnel may also help. If such conservative treatment does not help, your doctor may talk to you about a simple surgical procedure to relieve pressure on the nerve. The surgeon cuts the ligament over the carpal tunnel, which releases the pressure on the nerve. This surgery works well to relieve the symptoms of carpal tunnel syndrome.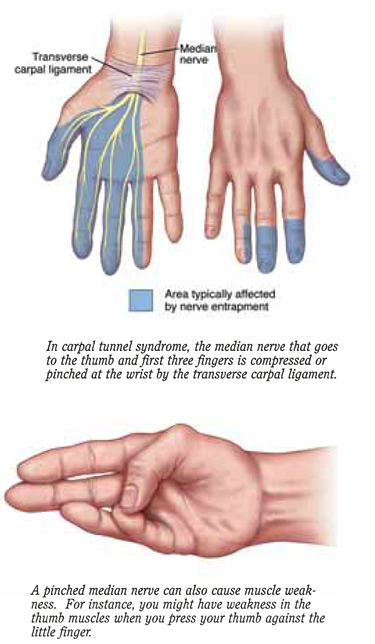
The carpal “tunnel” is the space in which nerves, tendons, and blood vessels pass through the bones of the wrist. Anything that narrows the tunnel, such as swelling of tendons, can compress the nerve and cause carpal tunnel syndrome.
1. Verdugo RJ, Salinas RS, Castillo J, Cea JG. Surgical versus non-surgical treatment for carpal tunnel syndrome. Cochrane Database Syst Rev 2002;(2):CD001552.-
2. Gerritsen AA, de Vet HC, Scholten RJ, Bertelsmann FW, de Krom MC, Bouter LM. Splinting vs surgery in the treatment of carpal tunnel syndrome: a randomized controlled trial. JAMA 2002;288:1245-51.
3. Demirci S, Kutluhan S, Koyuncuoglu HR, et al. Comparison of open carpal tunnel release and local steroid treatment outcomes in idiopathic carpal tunnel syndrome. Rheumatol Int 2002;22:33-7.
4. Katz JN, Keller RB, Simmons BP, et al. Maine carpal tunnel study: outcomes of operative and nonoperative therapy for carpal tunnel syndrome in a community-based cohort. J Hand Surg [Am] 1998;23:697-710.
5. Gerritsen AA, Uitdehaag BM, van Geldere D, Scholten RJ, de Vet HC, Bouter LM. Systematic review of randomized clinical trials of surgical treatment for carpal tunnel syndrome. Br J Surg 2001;88:1285-95.
6. American Society of Plastic and Reconstructive Surgeons. Carpal Tunnel Syndrome (Guidelines). Arlington Heights, IL: American Society of Plastic and Reconstructive Surgeons; 1998.
Good evidence supports the use of surgery for carpal tunnel syndrome over nonsurgical therapies such as wrist splints, nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, occupational therapy, local steroid injections, work modification, and oral vitamin B6 (Grade of Recommendation: A, based on extrapolation from a systematic review of 1 randomized controlled trial [RCT], 1 additional recent RCT, and 2 cohort studies). Surgery is likely worth the extra costs when conservative therapy (up to 3 months) fails to improve symptoms and return of function, because delayed surgery is as successful as surgery performed shortly after diagnosis. Closed endoscopic release and open release surgery are equally effective therapies for controlling symptoms (Grade of Recommendation: C, based on extrapolation from a systematic review of RCTs). However, whether endoscopic release results in more rapid regain of function and return to work is unclear.
See the Patient Information at the end of this article.
Evidence summary
A recent Cochrane review based on only 1 RCT of 22 patients published in 1964 concluded that surgical treatment of carpal tunnel syndrome appears to be more effective than wrist splinting.1 A well-designed RCT of 176 patients published since that Cochrane review stated that with regard to overall improvement of symptoms and function status, surgical treatment of carpal tunnel syndrome was more effective than wrist splinting 18 months posttreatment.2 The investigators found that surgery resulted in worse short-term outcomes at 1 month follow-up (29% vs 42% success), but by 3 months the improvement in all outcomes was greater in the surgery group (80% vs 54% success). The number needed to treat (NNT) over 18 months was only 2 patients in the treatment-received (per protocol) analysis (92% vs 37% success) and 7 in the intention-to-treat analysis (90% vs 75% success). Patients in the conservative treatment group who underwent surgery after splinting had failed had a higher success rate after 18 months follow-up than patients who did not have surgery (94% vs 62% success rate; NNT = 3).
One cohort study of 90 patients concluded that with respect to symptom control and return to function, open release surgery was as effective as local steroid injection at 1 month follow-up.3 However, at 4 to 6 months after the operation, surgery patients were found to have significantly improved symptom and function scores, with continued improvement compared with patients who received the steroid injection. One other cohort study of 429 patients found that surgery (open or closed endoscopic) was more effective with respect to symptom relief and functional status than various nonsurgical therapies (NSAIDs, splints, physical or occupational therapy, local steroid injections, work modification, or vitamin B6) at 30 months follow-up.4 In both cohort studies, the patients’ pretreatment symptom and functioning scores were worse in the surgery group than in the nonsurgical group. The investigators in the first study3 did not report controlling for these scores. In the second study,4 the authors controlled for functional status scores, but not for symptom severity.
One recent systematic review of 14 RCTs comparing types of surgical therapies for carpal tunnel syndrome concluded that none of the alternative surgical procedures, including closed endoscopic release, appeared to give better symptom relief than open release; and that the evidence is conflicting as to whether endoscopic release results in earlier return to work or improved level of function.5
Recommendations from others
The American Society of Plastic and Reconstructive Surgeons recommends surgical release in the following situations6: (1) failed or incomplete conservative therapy; (2) motor weakness or thenar atrophy; (3) lumbrical pattern symptoms (occur when the metacarpophalangeal joints are held at 90 degrees, eg, driving, letter writing, holding a magazine, pinching, using a small tool); (4) severe pattern on electrical studies (not defined); (5) space-occupying lesions requiring excision; (6) acute carpal tunnel syndrome with symptoms lasting longer than 6 to 8 hours; and (7) progressive or severe symptoms lasting longer than 12 months. The Society did not recommend one surgical procedure over another.
Maureen O’Reilly Brown, MD, MPH
Swedish Family Medicine Residency Program Seattle, Washington
In my practice, many patients have carpal tunnel syndrome and we regularly struggle with the question of whether and when to suggest surgical consultation. This review will make that struggle easier. With at least 33% of cases responding to splinting alone, an initial trial of conservative treatment seems appropriate for most patients. However, early surgical referral when a conservative approach has failed can now be easily justified, given the 90% or better success rate with surgery. The authors also include guidelines from the American Society of Plastic and Reconstructive Surgeons, which may be helpful in selecting which patients should go directly to surgical release.
Patient Information
What is carpal tunnel syndrome?
Carpal tunnel syndrome is felt as pain, tingling, a burning sensation, or loss of sensation that occurs throughout all or part of the hand. These symptoms may be worse at night and can wake you from sleep. You may feel the pain in just the hand, or it may travel up the arm.
How it’s diagnosed
Carpal tunnel syndrome can be challenging to diagnose.
Your doctor will ask you to describe your symptoms and may ask you to perform specific motions with your hand or wrist to see how they affect your symptoms.
Your doctor may arrange for a nerve conduction study—a test to determine how well the nerves in your hand are working. The test can detect if the pressure on the nerve is enough to affect how well it works.
How it’s treated
Your doctor may ask you to wear wrist splints at night or during work, and may advise you to reduce those activities that make the problem worse. Steroid injections into the carpal tunnel may also help. If such conservative treatment does not help, your doctor may talk to you about a simple surgical procedure to relieve pressure on the nerve. The surgeon cuts the ligament over the carpal tunnel, which releases the pressure on the nerve. This surgery works well to relieve the symptoms of carpal tunnel syndrome.
The carpal “tunnel” is the space in which nerves, tendons, and blood vessels pass through the bones of the wrist. Anything that narrows the tunnel, such as swelling of tendons, can compress the nerve and cause carpal tunnel syndrome.
Good evidence supports the use of surgery for carpal tunnel syndrome over nonsurgical therapies such as wrist splints, nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, occupational therapy, local steroid injections, work modification, and oral vitamin B6 (Grade of Recommendation: A, based on extrapolation from a systematic review of 1 randomized controlled trial [RCT], 1 additional recent RCT, and 2 cohort studies). Surgery is likely worth the extra costs when conservative therapy (up to 3 months) fails to improve symptoms and return of function, because delayed surgery is as successful as surgery performed shortly after diagnosis. Closed endoscopic release and open release surgery are equally effective therapies for controlling symptoms (Grade of Recommendation: C, based on extrapolation from a systematic review of RCTs). However, whether endoscopic release results in more rapid regain of function and return to work is unclear.
See the Patient Information at the end of this article.
Evidence summary
A recent Cochrane review based on only 1 RCT of 22 patients published in 1964 concluded that surgical treatment of carpal tunnel syndrome appears to be more effective than wrist splinting.1 A well-designed RCT of 176 patients published since that Cochrane review stated that with regard to overall improvement of symptoms and function status, surgical treatment of carpal tunnel syndrome was more effective than wrist splinting 18 months posttreatment.2 The investigators found that surgery resulted in worse short-term outcomes at 1 month follow-up (29% vs 42% success), but by 3 months the improvement in all outcomes was greater in the surgery group (80% vs 54% success). The number needed to treat (NNT) over 18 months was only 2 patients in the treatment-received (per protocol) analysis (92% vs 37% success) and 7 in the intention-to-treat analysis (90% vs 75% success). Patients in the conservative treatment group who underwent surgery after splinting had failed had a higher success rate after 18 months follow-up than patients who did not have surgery (94% vs 62% success rate; NNT = 3).
One cohort study of 90 patients concluded that with respect to symptom control and return to function, open release surgery was as effective as local steroid injection at 1 month follow-up.3 However, at 4 to 6 months after the operation, surgery patients were found to have significantly improved symptom and function scores, with continued improvement compared with patients who received the steroid injection. One other cohort study of 429 patients found that surgery (open or closed endoscopic) was more effective with respect to symptom relief and functional status than various nonsurgical therapies (NSAIDs, splints, physical or occupational therapy, local steroid injections, work modification, or vitamin B6) at 30 months follow-up.4 In both cohort studies, the patients’ pretreatment symptom and functioning scores were worse in the surgery group than in the nonsurgical group. The investigators in the first study3 did not report controlling for these scores. In the second study,4 the authors controlled for functional status scores, but not for symptom severity.
One recent systematic review of 14 RCTs comparing types of surgical therapies for carpal tunnel syndrome concluded that none of the alternative surgical procedures, including closed endoscopic release, appeared to give better symptom relief than open release; and that the evidence is conflicting as to whether endoscopic release results in earlier return to work or improved level of function.5
Recommendations from others
The American Society of Plastic and Reconstructive Surgeons recommends surgical release in the following situations6: (1) failed or incomplete conservative therapy; (2) motor weakness or thenar atrophy; (3) lumbrical pattern symptoms (occur when the metacarpophalangeal joints are held at 90 degrees, eg, driving, letter writing, holding a magazine, pinching, using a small tool); (4) severe pattern on electrical studies (not defined); (5) space-occupying lesions requiring excision; (6) acute carpal tunnel syndrome with symptoms lasting longer than 6 to 8 hours; and (7) progressive or severe symptoms lasting longer than 12 months. The Society did not recommend one surgical procedure over another.
Maureen O’Reilly Brown, MD, MPH
Swedish Family Medicine Residency Program Seattle, Washington
In my practice, many patients have carpal tunnel syndrome and we regularly struggle with the question of whether and when to suggest surgical consultation. This review will make that struggle easier. With at least 33% of cases responding to splinting alone, an initial trial of conservative treatment seems appropriate for most patients. However, early surgical referral when a conservative approach has failed can now be easily justified, given the 90% or better success rate with surgery. The authors also include guidelines from the American Society of Plastic and Reconstructive Surgeons, which may be helpful in selecting which patients should go directly to surgical release.
Patient Information
What is carpal tunnel syndrome?
Carpal tunnel syndrome is felt as pain, tingling, a burning sensation, or loss of sensation that occurs throughout all or part of the hand. These symptoms may be worse at night and can wake you from sleep. You may feel the pain in just the hand, or it may travel up the arm.
How it’s diagnosed
Carpal tunnel syndrome can be challenging to diagnose.
Your doctor will ask you to describe your symptoms and may ask you to perform specific motions with your hand or wrist to see how they affect your symptoms.
Your doctor may arrange for a nerve conduction study—a test to determine how well the nerves in your hand are working. The test can detect if the pressure on the nerve is enough to affect how well it works.
How it’s treated
Your doctor may ask you to wear wrist splints at night or during work, and may advise you to reduce those activities that make the problem worse. Steroid injections into the carpal tunnel may also help. If such conservative treatment does not help, your doctor may talk to you about a simple surgical procedure to relieve pressure on the nerve. The surgeon cuts the ligament over the carpal tunnel, which releases the pressure on the nerve. This surgery works well to relieve the symptoms of carpal tunnel syndrome.
The carpal “tunnel” is the space in which nerves, tendons, and blood vessels pass through the bones of the wrist. Anything that narrows the tunnel, such as swelling of tendons, can compress the nerve and cause carpal tunnel syndrome.
1. Verdugo RJ, Salinas RS, Castillo J, Cea JG. Surgical versus non-surgical treatment for carpal tunnel syndrome. Cochrane Database Syst Rev 2002;(2):CD001552.-
2. Gerritsen AA, de Vet HC, Scholten RJ, Bertelsmann FW, de Krom MC, Bouter LM. Splinting vs surgery in the treatment of carpal tunnel syndrome: a randomized controlled trial. JAMA 2002;288:1245-51.
3. Demirci S, Kutluhan S, Koyuncuoglu HR, et al. Comparison of open carpal tunnel release and local steroid treatment outcomes in idiopathic carpal tunnel syndrome. Rheumatol Int 2002;22:33-7.
4. Katz JN, Keller RB, Simmons BP, et al. Maine carpal tunnel study: outcomes of operative and nonoperative therapy for carpal tunnel syndrome in a community-based cohort. J Hand Surg [Am] 1998;23:697-710.
5. Gerritsen AA, Uitdehaag BM, van Geldere D, Scholten RJ, de Vet HC, Bouter LM. Systematic review of randomized clinical trials of surgical treatment for carpal tunnel syndrome. Br J Surg 2001;88:1285-95.
6. American Society of Plastic and Reconstructive Surgeons. Carpal Tunnel Syndrome (Guidelines). Arlington Heights, IL: American Society of Plastic and Reconstructive Surgeons; 1998.
1. Verdugo RJ, Salinas RS, Castillo J, Cea JG. Surgical versus non-surgical treatment for carpal tunnel syndrome. Cochrane Database Syst Rev 2002;(2):CD001552.-
2. Gerritsen AA, de Vet HC, Scholten RJ, Bertelsmann FW, de Krom MC, Bouter LM. Splinting vs surgery in the treatment of carpal tunnel syndrome: a randomized controlled trial. JAMA 2002;288:1245-51.
3. Demirci S, Kutluhan S, Koyuncuoglu HR, et al. Comparison of open carpal tunnel release and local steroid treatment outcomes in idiopathic carpal tunnel syndrome. Rheumatol Int 2002;22:33-7.
4. Katz JN, Keller RB, Simmons BP, et al. Maine carpal tunnel study: outcomes of operative and nonoperative therapy for carpal tunnel syndrome in a community-based cohort. J Hand Surg [Am] 1998;23:697-710.
5. Gerritsen AA, Uitdehaag BM, van Geldere D, Scholten RJ, de Vet HC, Bouter LM. Systematic review of randomized clinical trials of surgical treatment for carpal tunnel syndrome. Br J Surg 2001;88:1285-95.
6. American Society of Plastic and Reconstructive Surgeons. Carpal Tunnel Syndrome (Guidelines). Arlington Heights, IL: American Society of Plastic and Reconstructive Surgeons; 1998.
Evidence-based answers from the Family Physicians Inquiries Network